Stroke Systems of Care. Sharon Webb, MD, FAANS, FACS, FAHA
|
|
|
- Lilian Lewis
- 5 years ago
- Views:
Transcription
1 Stroke Systems of Care Sharon Webb, MD, FAANS, FACS, FAHA
2 Disclosures No Disclosures
3 Objectives Describe Systems of Care Describe stroke levels of care Discuss SC stroke council state Initiatives
4 What is the systems of care? When it comes to stroke and heart disease, the systems of care incorporates the coordination of care along the following continuum: 1. Primary prevention 2. Notification and response of emergency medical services (911 and EMS) 3. Acute treatment 4. Sub-acute care and secondary prevention 5. Recovery and rehabilitation 6. Continuous quality improvement initiatives
5 Why are systems of care important? To prevent the incidence and death of stroke, it is important to address the whole system from prevention to rehabilitation. The health threats that the systems of care is designed to fight against are some of the leading causes of death in America. For example, stroke, heart attack, trauma. If every state implemented a strong systems of care, we could help reduce heart disease and stroke deaths among Americans by 20 percent by the year 2020.
6 What specific improvements can be made to the systems of care? States can officially recognize the best medical centers to treat stroke to ensure that the best care is delivered promptly States can develop a registry to track the response and outcome of each incident in order to discover and implement future improvements in the systems of care States can mandate the utilization of EMS transport protocols to ensure that all patients having signs or symptoms of stroke be transported to the nearest appropriate certified stroke center. Positive patient outcomes are reliant on specialized care and quick treatment that can be found in certified stroke hospitals
7 Stroke Systems of Care Study Committee Report (S*26) (November 30, 2010) Recommendation summary (Primary Recommendations are listed in bold) 1. Support evidenced-based policy and systems changes which promote stroke prevention such as increasing the number of hypertension specialists in SC. Support campaigns to enhance public education and awareness of stroke. Provide resources to implement strategies to reduce stroke treatment disparities. 2. Establish hospital designation based on level of stroke care through designation by DHEC so that EMS can transport patients to the most appropriate, facility. Fund a full-time position, to be managed through DHEC's EMS Division, to establish and monitor regulations relating to hospital designation. 3. Ensure tele-health coverage through both public and private Insurance providers. 4. Ensure adequate coverage by private and public payers (including Medicaid) to provide stroke rehabilitation in free-standing interdisciplinary rehabilitation hospitals and home health based on need. 5. Offer tax credits, or limited state income tax, for stroke rehabilitation professionals in underserved areas including physiatrists, physical therapists, occupational therapists, and speech therapists. 6. Establish a statewide stroke registry, which will capture and link data on pre-hospital, hospital, and rehabilitation services. 7. Establish a statewide stroke steering committee to evaluate Implementation, adherence, and continuous improvement of the recommended changes. 8. Establish a full-time position, to be managed through DHEC's Heart Disease and Stroke Prevention Division, to implement the state stroke plan.

8 Stroke Systems of Care Act of 2011 Establish hospital designation Establish a statewide stroke registry EMS triage tool EMS transport protocols Establish a statewide stroke steering committee
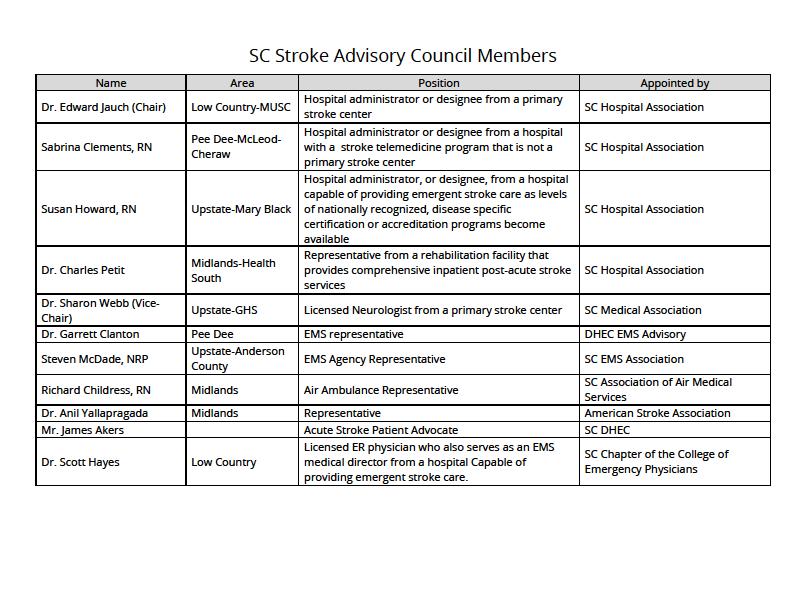
9 Establish a Statewide Stroke Steering Committee
10 Stroke Advisory Council Responsible for advising the department through the Bureau of EMS on all things related to stroke systems of care within the State. Like the EMS advisory Council, the members of the Stroke Advisory Council have the power to bring issues before the Council, make motions, and vote on matters that they see appropriate. Advisory Councils within the State have tremendous power and influence on system development and improvement.
11
12 Establish Hospital Designation
13 Stroke Levels of Care Acute Stroke Ready Hospital Primary Stroke Center Comprehensive Stroke Center
14 Stroke Hospital Certification CSC PSC ASRH Stabilize All Stroke Types Stabilize/Transfer All Stroke Types Role Treat All Stroke Types Treat Most Ischemic Strokes IV tpa for Ischemic Strokes Available 24/7 Available 24/7 Available 24/7 Actue Stroke Team Bedside within 15 min Bedside within 15 min Bedside within 15 min Neuro-ICU Stroke Unit Stroke beds (not ICU) none required with 24/7 neuro-intensivist Routine Imaging CT/MRI (24/7) CT/MRI (24/7) CT/MRI (24/7) 24/7 CTA, MRA, angiogram, not required Advanced Imaging CTP, TC doppler, carotid doppler, not required (except 1 cardiac imaging) TTE & TEE Neurologist Neurosurgery 24/7 in person, able to handle multiple complex pts Available 24/7, able to handle aneurysm clipping, AVM resection, carotid endartectomy 24/7 in person or telemedicine 24/7 in person or telemedicine Access within 2 hours (at center or transfer) Access within 3 hours (at center or transfer) Neurosurgery OR Available 24/7 Available 24/7 only if NSGY at center not required Endovascular Available 24/7 not required not required IV tpa, open neurosurgery, Minimum Treatment endovascular treatments IV tpa IV tpa protocol for transfer to CSC for Transfer Protocols accepts from PSC/ASRH neurosurgery/endovascular protocol for transfer to CSC/PSC Minimum Yearly Volume Education Research SAH aneurysm treatments 25 IV tpa (50/2 years carotid treatment variable Prehospital personnel education Public stroke education (2/yr) Internal educational courses (2/yr) IRB approved patient-centered research none required Prehospital personnel education Public stroke education (2/yr) none required none required Prehospital personnel education none required

15 Accreditation Organizations
16 Primary Stroke Center Mostly urban and suburban Typically 300+ stroke patient admissions per year Same level of care 24/7/365 All attributes of acute stroke ready, plus.
17 Primary Stroke Center Collaboration with EMS providers. Access to stroke treatment & destination protocols. Provide support to remote area hospitals. Transfer protocols to primary or comprehensive stroke center, when needed.


18 Primary Stroke Center Neuroimaging 24/7 basis: Able to obtain brain image within 25 minutes and interpretation within 20 minutes of completion. Advanced imaging: MRI with diffusion Vascular imaging (MRA, CTA, carotid doppler) Cardiac imaging (TTE, TEE, or cardiac MRI)



19 Primary Stroke Center Laboratory Services: Stroke labs within 45 minutes from order on 24/7 basis. ECG and chest x-ray within 45 minutes from order, when clinically indicated. Outcome and quality improvement activities. Community educational programs.

20 Primary Stroke Center Neurosurgeon available within 2 hours of need identified. Or written transfer plan to facility with this capability. Operating room capability 24/7.



21 Primary Stroke Center Stroke Units Does not require specific enclosed unit, but must be a unit where majority of patients are admitted where staff have annual education & specialized experience in caring for the stroke patient.
22 Primary Stroke Center Rehabilitation Services: Speech Language Therapy Physical Therapy Occupational Therapy Assessment and early initiation of a plan.
23 Primary Stroke Center, Metrics Stroke Core Measures Volume of Ischemic, TIA, ICH & SAH admits Acute Stroke workup times: Door to CT Door to lab results Door to EKG & CXR IV tpa volume, door to needle times


24 Must show that you deliver care based on these published guidelines.
25 Comprehensive Stroke Center Everything we ve discussed so far, plus Health care personnel with specific expertise in a number of disciplines, including neurosurgery and vascular neurology. Advanced neuroimaging capabilities, such as MRI and various types of cerebral angiography, 24/7/365, most within 30 minutes of clinical need. Surgical and endovascular techniques, including clipping and coiling of intracranial aneurysm, carotid endarterectomy and stenting, and endovascular treatments for ischemic stroke. Infrastructure and programmatic elements such as a dedicated neuro intensive care unit staffed with neurointensivists. Post hospital care coordination. Extensive data collection and peer review process. Participation in stroke research.

26 Comprehensive Stroke Center Increased data collection requirements. Examples: Ischemic stroke % of patients who received IV tpa in 60 minutes from arrival % who arrive in less than 6 hours of onset who were considered for endovascular tx 90 day modified Rankin scores Hemorrhagic stroke Initial severity scores documented (ICH & SAH) Procoagulant reversal times for ICH Median time from admit to surgical or endovascular tx for aneurysm % of patients who receive nimodipine within 24 hours of admit Serious complication and mortality rates for CEA, aneurysm coiling & clipping, carotid stents, thrombectomies, decompressive cranis, ventriculostomies, EVD s & transduced lines, cerebral angiograms. Follow-up calls on complex stroke patients within 7 days of discharge.

27 Comprehensive Stroke Center Enhances the ability to analyze and optimize how patients move through the system (EMS on through back into community). It allows for more team thinking of how we all work together to provide an efficient & optimal patient experience, rather than just thinking in silos about what occurs in and would work best for my own department. Regular communication among stakeholders through an organized committee/advisory group structure helps to reinforce the team concept, helps to identify common goals, sets clear priorities, and builds positive working relationships.
28 GHS Stroke Team CORE STROKE TEAM Mahmoud Rayes, MD Neuroscience Associates & Southeastern Neurosurgical & Spine System Stroke Medical Director CSC Medical Stroke Director Clinical Lead: Stroke, Research Sharon Webb, MD Southeastern Neurosurgical & Spine Director Cerebrovascular, Endovascular, Neurocritical care CSC Surgical Stroke Director Clinical Lead: Endovascular, NICU Angel Rochester, MD GHS Emergency Medicine Division Chief of Adult Emergency Medicine Clinical Lead: Emergency Department Shannon Sternberg, RN Greenville Memorial Hospital GHS Stroke Program Manager Core Stroke team represents Nursing, Neurology, Neurosurgery, Endovascular, Neurocritical Care & Emergency Medicine STROKE ADVISORY TEAM Physician: Neurology, Neurosurgery, Emergency, Radiology, Physiatry, Hospitalist Nursing: ED, IP, NeuroRadiology Laboratory Pharmacy Radiology Rehab Therapy Nutrition Hospital Case Management Quality Management Referral Center EMS
29 Future of Hospital Certification JCAHO: Thrombectomy-Capable Stroke Center 4 th designation + thrombectomy and ICU care - neurosurgery/endovascular capabilities for other stroke types 12 thrombectomies/year, 2 operators SNIS: Neuro-Endovascular Ready Add on State designation (like Trauma) + thrombectomy capable 36 thrombectomies/year, 2 operators, proper training
30 EMS Triage Tool
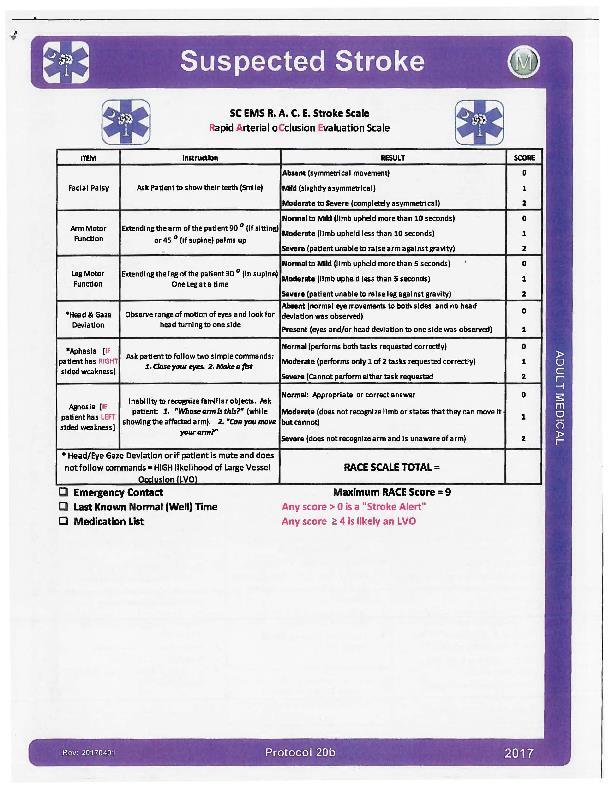
31
32 EMS Transport Protocols

33 GC EMS CVA Protocol
34
35
36 Establish a Statewide Stroke Registry
37 Statewide Stroke Registry Will use the GWTG data but will eventually also include prehospital data from EMS and post hospital stay data from rehab facilities ALL certified hospitals will be required to participate in the state stroke registry and submit data quarterly
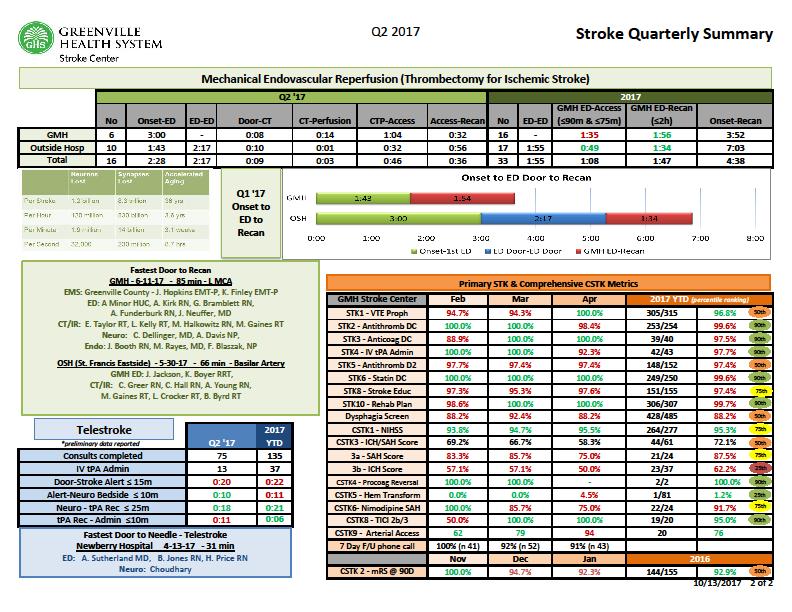
38 Power of Data Stroke Core Measures STK-1 VTE Prophylaxis initiated by hospital day 2 STK-2 Discharged on Antithrombotics STK-3 STK-4 Anticoagulation for Afib % who arrive in ED w/in 120 minutes of onset who received tpa w/in 3 hours of onset STK-5 Antithrombotics started by hospital day 2 STK-6 LDL> 100 discharged on a statin STK-8 Patient/family stroke education provided STK-10 Assessed for rehab needs PSC-7 Bedside swallow screen prior to any PO PSC-9 Tobacco cessation provided during hospital stay
39
40
41 Public Comment Providing public comment to SC DHEC - deadline October 23 Updates/PublicComments/
42 Stroke Systems of Care Does it make a difference? Compared to general hospitals, Primary Stroke Centers have: Higher tpa treatment rates Lower death rates Improved outcomes Being certified by an independent licensing body increases effectiveness of overall stroke care. The focus is on the entire continuum.
43 GHS Leading the Way in the Upstate

44 Cerebrovascular and Stroke Center

45 Cerebrovascular and Stroke Center

46 Cerebrovascular and Stroke Center
47 Cerebrovascular and Stroke Center
48 The Cerebrovascular and Stroke Service Line supports the Neurosciences/Post-Acute Services with the following GHS directives: GHS Vision: Transform health care for the benefit of the people and communities we serve. GHS Mission: Heal compassionately. Teach innovatively. Improve constantly. GHS Values: Together we serve with integrity, respect, trust and openness. CEREBROVASCULAR AND STROKE ADVISORY COUNCIL MISSION -Support Cerebrovascular and Stroke strategy and provide feedback -Improve effectiveness of patient experience -Develop increased capabilities of Caregivers -Advance awareness of Cerebrovascular and Stroke in the community -Explore advocacy engagement of organizations, both internal and external

49 Cerebrovascular and Stroke Fund







50 QUESTIONS?









51 Questions?









52
53 Donations can be made: Office of Philanthropy and Partnership 1. Online: 2. Check payable to: Greenville Health System and mail to: Greenville Health System Office of Philanthropy and Partnership Greenville Health System 300 East McBee, Suite 503 Greenville, SC Call the Office Of Philanthropy: If you want to discuss additional options contact: Dianne Dillon the Neuroscience and Post- Acute Philanthropy Representative at or
Primary Versus Comprehensive: What is the Difference?
 Primary Versus Comprehensive: What is the Difference? April 26, 2018 Bethann Mercanti, PA-C Director of Clinical Practice Stroke Program Coordinator Cooper Neurological Institute Cooper Bon & Joint Institute
Primary Versus Comprehensive: What is the Difference? April 26, 2018 Bethann Mercanti, PA-C Director of Clinical Practice Stroke Program Coordinator Cooper Neurological Institute Cooper Bon & Joint Institute
Moving from a Primary Stroke Center to a Comprehensive Stroke Center
 Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission October 19, 2012 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission October 19, 2012 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs
 The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs WA State Cardiac & Stroke Conference Brian R. Johnson, Ph.D. Associate Director Hospital Business Development
The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs WA State Cardiac & Stroke Conference Brian R. Johnson, Ph.D. Associate Director Hospital Business Development
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
C E R T I FI C AT I O N. Benchmarking Performance in HFAP-certified Primary Stroke Centers
 PRIMARY STROKE C E R T I FI C AT I O N Benchmarking Performance in HFAP-certified Primary Stroke Centers HFAP s mission is to advance high quality patient care and safety through objective application
PRIMARY STROKE C E R T I FI C AT I O N Benchmarking Performance in HFAP-certified Primary Stroke Centers HFAP s mission is to advance high quality patient care and safety through objective application
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes
 Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Neuroscience ICU: A Statewide Critical Care Resource
 Neuroscience ICU: A Statewide Critical Care Resource Ansgar M Brambrink, MD, PhD Director, Neuroscience Intensive Care Unit Oregon Health & Science University Portland, OR Neurocritical care in the US
Neuroscience ICU: A Statewide Critical Care Resource Ansgar M Brambrink, MD, PhD Director, Neuroscience Intensive Care Unit Oregon Health & Science University Portland, OR Neurocritical care in the US
Vote Using Your Phone!
 Update on Stroke Certification Jean Range, MS, RN The Joint Commission February 28, 2014 Vote Using Your Phone! Answer multiple choice questions by texting a code to 22333. Your phone carrier s texting
Update on Stroke Certification Jean Range, MS, RN The Joint Commission February 28, 2014 Vote Using Your Phone! Answer multiple choice questions by texting a code to 22333. Your phone carrier s texting
It is not enough to do your best, you must know what to do and then do your best
 Creating Effective Regional Stroke Systems of Care Stroke Strategies for Success Workshop October 3, 2012 Rick Foster, MD It is not enough to do your best, you must know what to do and then do your best
Creating Effective Regional Stroke Systems of Care Stroke Strategies for Success Workshop October 3, 2012 Rick Foster, MD It is not enough to do your best, you must know what to do and then do your best
Mark J. Alberts, MD. Turning the Wheels of Stroke Care
 Mark J. Alberts, MD Vice-Chair, Clinical Affairs Professor of Neurology Department of Neurology and Neurotherapeutics University of Texas Southwestern Medical Center Dallas, Texas Turning the Wheels of
Mark J. Alberts, MD Vice-Chair, Clinical Affairs Professor of Neurology Department of Neurology and Neurotherapeutics University of Texas Southwestern Medical Center Dallas, Texas Turning the Wheels of
Moving from a Primary Stroke Center to a Comprehensive Stroke Center
 Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission May 3, 2013 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission May 3, 2013 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
Nebraska Medicine Stroke and Neurovascular Center Outcomes
 Nebraska Medicine Stroke and Neurovascular Center Outcomes Stroke Procedure/Treatment Our Performance Joint Commission Benchmark Diagnostic Cerebral Angiogram Stroke within 24 hours post procedure Death
Nebraska Medicine Stroke and Neurovascular Center Outcomes Stroke Procedure/Treatment Our Performance Joint Commission Benchmark Diagnostic Cerebral Angiogram Stroke within 24 hours post procedure Death
Stroke Systems of Care
 Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Standards of excellence
 The Accreditation Canada Stroke Distinction program was launched in March 2010 to offer a rigorous and highly specialized process above and beyond the requirements of Qmentum. The comprehensive Stroke
The Accreditation Canada Stroke Distinction program was launched in March 2010 to offer a rigorous and highly specialized process above and beyond the requirements of Qmentum. The comprehensive Stroke
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center. What do we know?
 Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Antithrombotics: Percent of patients with an ischemic stroke or TIA prescribed antithrombotic therapy at discharge. Corresponding
 Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Pediatric Thrombectomy
 Pediatric Thrombectomy Translating adult standard of care to pediatric patients DATE: September 16, 2016 PRESENTED BY: Ittai Bushlin MD, PhD and Adrienne McDougal, RN Objectives: Review acute management
Pediatric Thrombectomy Translating adult standard of care to pediatric patients DATE: September 16, 2016 PRESENTED BY: Ittai Bushlin MD, PhD and Adrienne McDougal, RN Objectives: Review acute management
UF HEALTH SHANDS CORE POLICY AND PROCEDURE. Stroke Alert Process
 UF HEALTH SHANDS CORE POLICY AND PROCEDURE POLICY NUMBER: CATEGORY: CP02.078 Patient Care TITLE: POLICY: PURPOSE: Stroke Alert Process Patients who present with or develop the cardinal signs of stroke
UF HEALTH SHANDS CORE POLICY AND PROCEDURE POLICY NUMBER: CATEGORY: CP02.078 Patient Care TITLE: POLICY: PURPOSE: Stroke Alert Process Patients who present with or develop the cardinal signs of stroke
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers
 Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
National Stroke Association s Guide to Choosing Stroke. Rehabilitation Services
 National Stroke Association s Guide to Choosing Stroke Rehabilitation Services Rehabilitation, often referred to as rehab, is an important part of stroke recovery. Through rehab, you: Re-learn basic skills
National Stroke Association s Guide to Choosing Stroke Rehabilitation Services Rehabilitation, often referred to as rehab, is an important part of stroke recovery. Through rehab, you: Re-learn basic skills
Stroke Special Project 640 and 740 Resource For Health Information Management Professionals
 Stroke Special Project 640 and 740 Resource For Health Information Management Professionals Linda Gould RPN Erin Kelleher, BA, CHIM Stefan Pagliuso PT, B.A. Kin(Hon.) Overview of this Resource Overview
Stroke Special Project 640 and 740 Resource For Health Information Management Professionals Linda Gould RPN Erin Kelleher, BA, CHIM Stefan Pagliuso PT, B.A. Kin(Hon.) Overview of this Resource Overview
Inpatient Acute Rehabilitation
 Inpatient Acute Rehabilitation A massive stroke. A major illness. A debilitating injury. At first, you can t imagine how life will ever be the same. Affiliated with the renowned Dignity Health Neurological
Inpatient Acute Rehabilitation A massive stroke. A major illness. A debilitating injury. At first, you can t imagine how life will ever be the same. Affiliated with the renowned Dignity Health Neurological
Stroke is a common and serious disorder. Each year in the. Special Report
 Special Report Revised and Updated Recommendations for the Establishment of Primary Stroke Centers A Summary Statement From the Brain Attack Coalition Mark J. Alberts, MD; Richard E. Latchaw, MD; Andy
Special Report Revised and Updated Recommendations for the Establishment of Primary Stroke Centers A Summary Statement From the Brain Attack Coalition Mark J. Alberts, MD; Richard E. Latchaw, MD; Andy
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
STROKE COORDINATOR! RETURN ON INVESTMENT DEBBIE HILL, FAHA! PRINCIPAL! LOMBARDI HILL CONSULTING GROUP!
 STROKE COORDINATOR! v! RETURN ON INVESTMENT DEBBIE HILL, FAHA! PRINCIPAL! LOMBARDI HILL CONSULTING GROUP! DISCLOSURES Principal, Lombardi Hill Consulting Group Member, Gerson Lehman Healthcare Council
STROKE COORDINATOR! v! RETURN ON INVESTMENT DEBBIE HILL, FAHA! PRINCIPAL! LOMBARDI HILL CONSULTING GROUP! DISCLOSURES Principal, Lombardi Hill Consulting Group Member, Gerson Lehman Healthcare Council
Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical Center Dallas, TX
 Interventional Therapies for Cerebrovascular Diease: The Good, The Bad, The Needed, and The Few 1 Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical
Interventional Therapies for Cerebrovascular Diease: The Good, The Bad, The Needed, and The Few 1 Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical
Headline. Objectives. Baptist Health Mission Stroke Core Measures
 Headline 2010 Stroke Core Measures Baptist Medical Center Downtown Baptist Medical Center South Presented by Maria Martinez, RN, BSN May 21, 2010 Objectives 2 Baptist Health Mission To continue the healing
Headline 2010 Stroke Core Measures Baptist Medical Center Downtown Baptist Medical Center South Presented by Maria Martinez, RN, BSN May 21, 2010 Objectives 2 Baptist Health Mission To continue the healing
Stroke Systems of Care Update
 Stroke Systems of Care Update Edward C. Jauch, MD MS FAHA FACEP Professor and Director, Division of Emergency Medicine Professor, Department of Neurosciences Associate Vice Chair, Research, Department
Stroke Systems of Care Update Edward C. Jauch, MD MS FAHA FACEP Professor and Director, Division of Emergency Medicine Professor, Department of Neurosciences Associate Vice Chair, Research, Department
2017 Stroke Statistics
 2017 Stroke Statistics 2017 LUMC Stroke Volumes by Type of Stroke Ischemic Stroke Treatment by Type 2017 17% 8% 75% Ischemic Intracerebral Hemorrhage Aneurysmal Subarachnoid Hemorrhage 31 42 25 r-tpa Administered
2017 Stroke Statistics 2017 LUMC Stroke Volumes by Type of Stroke Ischemic Stroke Treatment by Type 2017 17% 8% 75% Ischemic Intracerebral Hemorrhage Aneurysmal Subarachnoid Hemorrhage 31 42 25 r-tpa Administered
Stroke Rehab Definitions Framework Self-Assessment Tool Acute Integrated Stroke Unit
 rth & East GTA Stroke Network Stroke Rehab Definitions Framework Self-Assessment Tool Acute Integrated Stroke Unit Purpose of the Self-Assessment Tool: The GTA Rehab Network and the GTA regions of the
rth & East GTA Stroke Network Stroke Rehab Definitions Framework Self-Assessment Tool Acute Integrated Stroke Unit Purpose of the Self-Assessment Tool: The GTA Rehab Network and the GTA regions of the
THE TELE-ICU PROGRAM PROCESS
 Tele-ICU Telehealth s Tele-ICU services provide high-quality critical care in rural and underserved communities throughout the country. This service allows hospitals to ensure consistent coverage of the
Tele-ICU Telehealth s Tele-ICU services provide high-quality critical care in rural and underserved communities throughout the country. This service allows hospitals to ensure consistent coverage of the
JOURNEY TO ACUTE STROKE READY CERTIFICATION
 JOURNEY TO ACUTE STROKE READY CERTIFICATION Bernie Oberrecht RN MSN NE-BC Director of Critical Care for St. Elizabeth Healthcare System Stroke Program Coordinator Currently @ St. Elizabeth Healthcare Edgewood
JOURNEY TO ACUTE STROKE READY CERTIFICATION Bernie Oberrecht RN MSN NE-BC Director of Critical Care for St. Elizabeth Healthcare System Stroke Program Coordinator Currently @ St. Elizabeth Healthcare Edgewood
DISCLOSURES. Learning Objectives. David Lee Gordon, MD, FAHA Update in Stroke 2007 FINANCIAL DISCLOSURE UNLABELED/UNAPPROVED USES DISCLOSURE
 Acute Stroke Care and the Role of EMS Ryan Hakimi, DO, MS April 30, 2015 Assistant Professor Director, Critical Care Neurology Department of Neurology University of Oklahoma Health Sciences Center DISCLOSURES
Acute Stroke Care and the Role of EMS Ryan Hakimi, DO, MS April 30, 2015 Assistant Professor Director, Critical Care Neurology Department of Neurology University of Oklahoma Health Sciences Center DISCLOSURES
SOC s Guide to the 2013 CMS New Core Measures for Stroke
 SOC s Guide to the 2013 CMS New Core Measures for Stroke Since 2004, the Centers for Medicare & Medicaid Services (CMS) has collected quality data from acute care hospitals on a voluntary basis under the
SOC s Guide to the 2013 CMS New Core Measures for Stroke Since 2004, the Centers for Medicare & Medicaid Services (CMS) has collected quality data from acute care hospitals on a voluntary basis under the
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
for Stroke Care (Update 2013)
") Overview (Version 1.0) May 23 rd, 2013 Page 1 TAKING ACTION TOWARDS OPTIMAL STROKE CARE 2 Table of Contents Section Content Page About this Resource 3 1.0 Overview 4 1.1 Purpose of the Resource Kit 4 2.0
Overview (Version 1.0) May 23 rd, 2013 Page 1 TAKING ACTION TOWARDS OPTIMAL STROKE CARE 2 Table of Contents Section Content Page About this Resource 3 1.0 Overview 4 1.1 Purpose of the Resource Kit 4 2.0
Stroke Coordinator: ROI. Author: Debbie Roper, RN, MSN (d.r. Stroke) Vice President of Roper Resources, Inc.
 Vice President of Roper Resources, Inc.") Stroke Coordinator: ROI Author: Debbie Roper, RN, MSN (d.r. Stroke) Vice President of Roper Resources, Inc. debbie@roper-resources.com 214-864-8993 Disclosure Debbie Roper is a speaker for: Genentech Activase
Stroke Coordinator: ROI Author: Debbie Roper, RN, MSN (d.r. Stroke) Vice President of Roper Resources, Inc. debbie@roper-resources.com 214-864-8993 Disclosure Debbie Roper is a speaker for: Genentech Activase
STAR- - Stroke Treatment Alliance of Rochester
 STAR- - Stroke Treatment Alliance of Rochester Curtis Benesch, M.D., M.P.H. Medical Director, URMC Comprehensive Stroke Center March 30, 2017 Background of the STAR Consortium What we learned from STAR
STAR- - Stroke Treatment Alliance of Rochester Curtis Benesch, M.D., M.P.H. Medical Director, URMC Comprehensive Stroke Center March 30, 2017 Background of the STAR Consortium What we learned from STAR
TENNESSEE STROKE REGISTRY QUARTERLY REPORT
 TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 2 July 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender distributions,
TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 2 July 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender distributions,
Stroke Distinction Report...
 .................................................................................................................................................... Alberta Health Services, Stroke Program Edmonton Zone
.................................................................................................................................................... Alberta Health Services, Stroke Program Edmonton Zone
Target: STROKE. The Team-Based Approached
 Target: STROKE The Team-Based Approached November 19, 2013 Tuesday 1300 1400 Thank you for joining today s webinar, the presentation will begin shortly. A special thank you to Cornerstone Therapeutics
Target: STROKE The Team-Based Approached November 19, 2013 Tuesday 1300 1400 Thank you for joining today s webinar, the presentation will begin shortly. A special thank you to Cornerstone Therapeutics
Statewide Acute Stroke Triage The Washington Story
 Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
NORTH CAROLINA CARDIOVASCULAR STATE PLAN I N T R O D U C T I O N S, G O A L S, O B J E C T I V E S A N D S T R A T E G I E S
 NORTH CAROLINA CARDIOVASCULAR STATE PLAN 2011-2016 I N T R O D U C T I O N S, G O A L S, O B J E C T I V E S A N D S T R A T E G I E S PRIMARY PREVENTION OF CARDIOVASCULAR DISEASE THROUGH HEALTHY LIVING
NORTH CAROLINA CARDIOVASCULAR STATE PLAN 2011-2016 I N T R O D U C T I O N S, G O A L S, O B J E C T I V E S A N D S T R A T E G I E S PRIMARY PREVENTION OF CARDIOVASCULAR DISEASE THROUGH HEALTHY LIVING
Get With the Guidelines Stroke PMT. Quality Measure Descriptions
 Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Mission: Lifeline Stroke Nebraska
 Mission: Lifeline Stroke Nebraska What is Mission: Lifeline Stroke? Mission: Lifeline Stroke is the American Heart Association s national initiative to transform stroke care by focusing efforts on connecting
Mission: Lifeline Stroke Nebraska What is Mission: Lifeline Stroke? Mission: Lifeline Stroke is the American Heart Association s national initiative to transform stroke care by focusing efforts on connecting
Emergency Department Stroke Registry Process of Care Indicator Specifications (July 1, 2011 June 30, 2012 Dates of Service)
") Specifications Description Methodology NIH Stroke Scale (NIHSS) Performed in Initial Evaluation used to assess the percentage of adult stroke patients who had the NIHSS performed during their initial evaluation
Specifications Description Methodology NIH Stroke Scale (NIHSS) Performed in Initial Evaluation used to assess the percentage of adult stroke patients who had the NIHSS performed during their initial evaluation
Can We Apply Lessons Learned in Stroke Centers to Change Aspects of Cardiac Arrest Care?
 Can We Apply Lessons Learned in Stroke Centers to Change Aspects of Cardiac Arrest Care? 1 Mark J. Alberts, MD, FAHA Professor of Neurology Vice-Chair, Clinical Affairs Department of Neurology and Neurotherapeutics
Can We Apply Lessons Learned in Stroke Centers to Change Aspects of Cardiac Arrest Care? 1 Mark J. Alberts, MD, FAHA Professor of Neurology Vice-Chair, Clinical Affairs Department of Neurology and Neurotherapeutics
LIFE-CHANGING CARE INPATIENT CARE
 LIFE-CHANGING CARE INPATIENT CARE Helping Patients Get the Most out of Rehab When a stroke, accident or other traumatic incident turns a person s world upside down, there s a place in Indiana where he
LIFE-CHANGING CARE INPATIENT CARE Helping Patients Get the Most out of Rehab When a stroke, accident or other traumatic incident turns a person s world upside down, there s a place in Indiana where he
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council
 American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
Requirements for Cerebrovascular Surgery in Comprehensive Stroke Centers in South Korea
 Clinical Article J Korean Neurosurg Soc 61 (4) : 478-484, 2018 https://doi.org/10.3340/jkns.2017.0227 pissn 2005-3711 eissn 1598-7876 Requirements for Cerebrovascular Surgery in Comprehensive Stroke Centers
Clinical Article J Korean Neurosurg Soc 61 (4) : 478-484, 2018 https://doi.org/10.3340/jkns.2017.0227 pissn 2005-3711 eissn 1598-7876 Requirements for Cerebrovascular Surgery in Comprehensive Stroke Centers
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Stroke System of Care Policy
 Emergency Medical Services Division Policy Effective date December 1, 2015 Edward Hill EMS Director Kristopher Lyon, M.D. Medical Director TABLE OF CONTENTS I. PURPOSE... 2 II. AUTHORITY... 2 III. DEFINITIONS...
Emergency Medical Services Division Policy Effective date December 1, 2015 Edward Hill EMS Director Kristopher Lyon, M.D. Medical Director TABLE OF CONTENTS I. PURPOSE... 2 II. AUTHORITY... 2 III. DEFINITIONS...
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Method Hannah Shotton
 #asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
#asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
THE QUARTERLY NEWSLETTER OF THE NEUROVASCULAR STROKE CENTER AT THE OHIO STATE UNIVERSITY
 THE QUARTERLY NEWSLETTER OF THE NEUROVASCULAR STROKE CENTER AT THE OHIO STATE UNIVERSITY SPRING 2012 FROM THE EDITORS Michel T. Torbey, MD, MPH, FCCM, FAHA Professor of Neurology & Neurosurgery Medical
THE QUARTERLY NEWSLETTER OF THE NEUROVASCULAR STROKE CENTER AT THE OHIO STATE UNIVERSITY SPRING 2012 FROM THE EDITORS Michel T. Torbey, MD, MPH, FCCM, FAHA Professor of Neurology & Neurosurgery Medical
SC Stroke System of Care. Learning Objectives 9/15/2011. Director, Heart Disease and Stroke Prevention SC DHEC
 SC Stroke System of Care Joy Brooks, MHA Director, Heart Disease and Stroke Prevention SC DHEC Learning Objectives Describe the burden of stroke in SC Outline the process for the SC Stroke System of Care
SC Stroke System of Care Joy Brooks, MHA Director, Heart Disease and Stroke Prevention SC DHEC Learning Objectives Describe the burden of stroke in SC Outline the process for the SC Stroke System of Care
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke
 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
Human and Fiscal Implications of Heart Disease and Stroke
 1 Texas Council on Cardiovascular Disease and Stroke Report for the 84 th Regular Texas Legislative Session Heart Disease and Stroke in Texas: A Call to Action Enacted by the 76 th Legislature (House Bill
1 Texas Council on Cardiovascular Disease and Stroke Report for the 84 th Regular Texas Legislative Session Heart Disease and Stroke in Texas: A Call to Action Enacted by the 76 th Legislature (House Bill
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Arnold and Mabel Beckman Center of the National Academies of Sciences and Engineering. 100 Academy Way, Irvine, CA 92617
 LOCATION PROGRAM 7:30 am REGISTRATION & CONTINENTAL BREAKFAST 8:00 am Welcome 8:10 am Introductory Remarks Ralph V. Clayman, MD Dean, UC Irvine School of Medicine Ischemic Stroke and TIA 8:20 am Pre-Hospital
LOCATION PROGRAM 7:30 am REGISTRATION & CONTINENTAL BREAKFAST 8:00 am Welcome 8:10 am Introductory Remarks Ralph V. Clayman, MD Dean, UC Irvine School of Medicine Ischemic Stroke and TIA 8:20 am Pre-Hospital
Team Work in Treatment of Acute Ischemic Stroke
 Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Acute Stroke Rescue and Recovery
 Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Your Risk for Stroke and How to Be Prepared
 Your Risk for Stroke and How to Be Prepared TABLE OF CONTENTS 01 / 02 / 03 / 04 / 06 / 07 / 08 / 09 / 14 / Stroke Education Stroke: The No. 5 Cause Of Death In The U.S. Is Stroke Preventable? Stroke Risk
Your Risk for Stroke and How to Be Prepared TABLE OF CONTENTS 01 / 02 / 03 / 04 / 06 / 07 / 08 / 09 / 14 / Stroke Education Stroke: The No. 5 Cause Of Death In The U.S. Is Stroke Preventable? Stroke Risk
Interventions to Improve Acute Ischemic Stroke Treatment Times
 Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 3-19-2018 Interventions to Improve Acute Ischemic Stroke Treatment Times Jayme Strauss Baptist Hospital of
Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 3-19-2018 Interventions to Improve Acute Ischemic Stroke Treatment Times Jayme Strauss Baptist Hospital of
ALL orders are active unless: 1. Order is manually lined through to inactivate 2. Orders with check boxes ( ) are unchecked DRUG AND TREATMENT ORDERS
 are unchecked DRUG AND TREATMENT ORDERS") DRUG AND TREATMENT Available at: BMC-B BMC-D BMC-N BMC-S Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24
DRUG AND TREATMENT Available at: BMC-B BMC-D BMC-N BMC-S Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24
DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Available at: BMC-B BMC-D BMC-N BMC-S Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24
DRUG AND TREATMENT Available at: BMC-B BMC-D BMC-N BMC-S Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24
Illinois Stroke System Policy Overview
 Illinois Stroke System Policy Overview Christopher T. Richards, MD, MS, FAEMS Department of Emergency Medicine, Northwestern Feinberg School of Medicine Associate EMS Medical Director, Region XI EMS System
Illinois Stroke System Policy Overview Christopher T. Richards, MD, MS, FAEMS Department of Emergency Medicine, Northwestern Feinberg School of Medicine Associate EMS Medical Director, Region XI EMS System
Stroke Belt Consortium
 Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Get With The Guidelines: Lessons for National Healthcare Improvement Programs
 Get With The Guidelines: Lessons for National Healthcare Improvement Programs Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of Cardiovascular Medicine and Science UCLA Division of Cardiology
Get With The Guidelines: Lessons for National Healthcare Improvement Programs Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of Cardiovascular Medicine and Science UCLA Division of Cardiology
Do Specialized Units Improve Outcomes?
 Do Specialized Units Improve Outcomes? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
Do Specialized Units Improve Outcomes? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
ICU OF THE FUTURE. Symposium at UCLA. NEUROCRITICAL CARE in the FEBRUARY 21-22, Luxe Hotel Los Angeles, California
 FEBRUARY 21-22, 2013 Luxe Hotel Los Angeles, California Course Director Paul M. Vespa, MD, FCCM, FAAN Professor of Neurosurgery and Neurology David Geffen School of Medicine at UCLA Director, Neurocritical
FEBRUARY 21-22, 2013 Luxe Hotel Los Angeles, California Course Director Paul M. Vespa, MD, FCCM, FAAN Professor of Neurosurgery and Neurology David Geffen School of Medicine at UCLA Director, Neurocritical
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Therapy for Acute Stroke. Systems of Care for TIA
 Therapy for Acute Stroke and Systems of Care for TIA Gregory W. Albers, MD Coyote Foundation Professor of Neurology and Neurological Sciences Director, Stanford Stroke Center Stanford University Medical
Therapy for Acute Stroke and Systems of Care for TIA Gregory W. Albers, MD Coyote Foundation Professor of Neurology and Neurological Sciences Director, Stanford Stroke Center Stanford University Medical
TENNESSEE STROKE REGISTRY QUARTERLY REPORT
 TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 3 September 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender
TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 3 September 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Advances in Acute stroke Management
 Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Mission: Lifeline Addressing the System of STEMI Care
 Mission: Lifeline Addressing the System of STEMI Care Alice K. Jacobs, M.D. Boston University Medical Center Boston, MA, USA ACC West Virginia Chapter, April 2017 Disclosure Information FINANCIAL DISCLOSURE:
Mission: Lifeline Addressing the System of STEMI Care Alice K. Jacobs, M.D. Boston University Medical Center Boston, MA, USA ACC West Virginia Chapter, April 2017 Disclosure Information FINANCIAL DISCLOSURE:
01: EMS Pre-Notification Door-To-Needle Processes for Success:
 01: EMS Pre-Notification Door-To-Needle Processes for Success: Greenville Memorial Hospital Shannon Sternberg, RN, MSN, CNRN Stroke Program Coordinator Greenville Hospital System 500 400 300 200 100 0
01: EMS Pre-Notification Door-To-Needle Processes for Success: Greenville Memorial Hospital Shannon Sternberg, RN, MSN, CNRN Stroke Program Coordinator Greenville Hospital System 500 400 300 200 100 0
Get With The Guidelines - Stroke and Trends in New Jersey
 The Road to Recovery: Get With The Guidelines - Stroke and Trends in New Jersey Zainab Magdon-Ismail, DrPH Vice President, Quality & Systems Improvement Founders Affiliate (NJ-ME) American Heart Association
The Road to Recovery: Get With The Guidelines - Stroke and Trends in New Jersey Zainab Magdon-Ismail, DrPH Vice President, Quality & Systems Improvement Founders Affiliate (NJ-ME) American Heart Association
Identifying Key Players for Early Stroke Management
 Identifying Key Players for Early Stroke Management Cabinet Peaks Medical Center Libby, Montana Presented by: Kimberlee Rebo and John Thornton OBJECTIVES Identify key players in early stroke care & management
Identifying Key Players for Early Stroke Management Cabinet Peaks Medical Center Libby, Montana Presented by: Kimberlee Rebo and John Thornton OBJECTIVES Identify key players in early stroke care & management
Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2
 Measure Set Session 2") Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2 January 28, 2015 1 to 3 PM Central Time Continuing Education Credit This course
Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2 January 28, 2015 1 to 3 PM Central Time Continuing Education Credit This course
Standardization of the Neuroendovascular Lab
 Standardization of the Neuroendovascular Lab Vallabh Janardhan, MD Director, Texas Stroke Institute Stroke & Interventional Neurologist HCA North Texas Division, Dallas-Fort Worth, TX Founding Board of
Standardization of the Neuroendovascular Lab Vallabh Janardhan, MD Director, Texas Stroke Institute Stroke & Interventional Neurologist HCA North Texas Division, Dallas-Fort Worth, TX Founding Board of
ICU OF THE FUTURE. Symposium at UCLA. NEUROCRITICAL CARE in the FEBRUARY 20-21, Luxe Hotel Los Angeles, California NEUROSURGERY
 NEUROCRITICAL CARE in the FEBRUARY 20-21, 2014 Luxe Hotel Los Angeles, California NEUROSURGERY Course Director Paul M. Vespa, MD, FCCM, FAAN Professor of Neurosurgery and Neurology David Geffen School
NEUROCRITICAL CARE in the FEBRUARY 20-21, 2014 Luxe Hotel Los Angeles, California NEUROSURGERY Course Director Paul M. Vespa, MD, FCCM, FAAN Professor of Neurosurgery and Neurology David Geffen School
The Mercy Telehealth Network: Your direct connection to specialized care
 The Mercy Telehealth Network: Your direct connection to specialized care Mercy Telehealth Network Presentation Goal To provide an overview of the Mercy Telehealth Network To suggest that Telehealth is
The Mercy Telehealth Network: Your direct connection to specialized care Mercy Telehealth Network Presentation Goal To provide an overview of the Mercy Telehealth Network To suggest that Telehealth is
San Joaquin County Emergency Medical Services Primary Stroke Center Application and Self Evaluation Form (SECTION II)
") Self Evaluation Form (SECTIO II) Hospital Services A. General Proof of JCAHO accreditation as a Primary Stroke Center Special permit from CDPH for Basic or Comprehensive Emergency Medical Services B. CT
Self Evaluation Form (SECTIO II) Hospital Services A. General Proof of JCAHO accreditation as a Primary Stroke Center Special permit from CDPH for Basic or Comprehensive Emergency Medical Services B. CT
Maximising Delivery of Thrombectomy
 Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
HIE Image Sharing for a Statewide Stroke Network Session #68, March 6, 2018 Karan Mansukhani, MPH, MBA, Program Manager, Chesapeake Regional
 HIE Image Sharing for a Statewide Stroke Network Session #68, March 6, 2018 Karan Mansukhani, MPH, MBA, Program Manager, Chesapeake Regional Information System for our Patients (CRISP) Dr. Michael Phipps,
HIE Image Sharing for a Statewide Stroke Network Session #68, March 6, 2018 Karan Mansukhani, MPH, MBA, Program Manager, Chesapeake Regional Information System for our Patients (CRISP) Dr. Michael Phipps,
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth. May 23, 2018
 Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II
 Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II Gregg C. Fonarow MD, Eric E. Smith MD, MPH, Jeffrey L. Saver MD, Lee H. Schwamm, MD UCLA Division of Cardiology; Department
Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II Gregg C. Fonarow MD, Eric E. Smith MD, MPH, Jeffrey L. Saver MD, Lee H. Schwamm, MD UCLA Division of Cardiology; Department
Difficulties in establishing Neurocritical Care Units Dr.Omar Ayoub Consultant & Assistant Professor of Neurology Stroke, Neurocritical Care RTP
 Difficulties in establishing Neurocritical Care Units Dr.Omar Ayoub Consultant & Assistant Professor of Neurology Stroke, Neurocritical Care RTP Neurology at KAUH Evolution of ICUs ICUs started as specialized
Difficulties in establishing Neurocritical Care Units Dr.Omar Ayoub Consultant & Assistant Professor of Neurology Stroke, Neurocritical Care RTP Neurology at KAUH Evolution of ICUs ICUs started as specialized
Acute Ischaemic Stroke Pathways Drip and Ship
 Acute Ischaemic Stroke Pathways Drip and Ship Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor
Acute Ischaemic Stroke Pathways Drip and Ship Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor