International Journal of Psychosocial Rehabilitation
|
|
|
- Sydney Hood
- 6 years ago
- Views:
Transcription

1 International Journal of Psychosocial Rehabilitation ISSN (Proudly Serving our Web Based, International Readers Since 1996) Volume 20 July December 2016 A WEB BASED PEER REVIEWED PUBLICATION FOR MENTAL HEALTH PRACTITIONERS, CONSUMERS & APPLIED RESEARCHERS This private NON-PROFIT professional publication and associated webbased, information archive service is dedicated to the enhancement of practice, program development, program evaluation and innovations in mental health and substance abuse treatment programs worldwide. Its goal is to provide a public forum for practitioners, consumers and researchers to address the multiple service needs of patients and families and help determine what works, for whom under a variety of circumstances. WWW. PSYCHOSOCIAL. COM
2 IJPR Feature Articles Page Cognitive behavioural treatment for problematic hoarding: A Case Study- Binnie Effectiveness of a Recovery Program for Chinese Psychiatric Inpatients- Lai, Chiu, Tse, Tsui, Cheung, Chen, Chan, Fan, Chan, Cheung, Wong It made me think a little different a qualitative study of young adult cancer survivors experiences of cognitive therapy in cancer rehabilitation Hauken & Viken Efficacy of Social Skills Training among Persons with Schizophrenia- Kapse & Nirmala Empathy in Psychosocial Intervention: a theoretical overview- Stanley & Sethuramalingam Notes in Tune: Arts-based Therapy (ABT) at Schizophrenia Awareness Association in Pune, India Chabukswar Better Eating and Recovery: Addressing Food Insecurity at an urban Better Eating and Community Mental Health Center- Debor, Gallagher, Blinten, Sernyak, Cole, Olsen, & Harper Adherence issues to antipsychotic medication in schizophrenia: results from a Hong Kong survey targeted for psychiatrists and case managers - Mak, Lo, Yeung, Wong, Chung, Chui, Tam, Mui, Chan, & Wong Perceived burden and quality of life in Chinese caregivers of people with serious mental illness: a path analysis - Zeng, Zhou, & Lin Assessing the Suitability of Clinical Programs for Implementation Bartholomew & Birkman Comparing quality of life, stress perception and quality of social networks in a community-based brain injury program - Prudhomme, Wilcox, Kresge, & Couture Copyright ADG, S.A. All Rights Reserved. ~ 2 ~
3 Journal Information This peer reviewed Journal was created in 1996 by practitioners, mental health program managers and mental health consumers to provide international practitioners, scholars and consumers with a forum to publish and discuss their work in program development, evaluation research, policy innovations, and therapeutic practices that have been successful in their particular region and cultures. IJPR is not associated with any university or governmental institution, nor is it part of any old boy or other professional network. It was created to provide information to an international readership about issues related to psychosocial rehabilitation and associated topics. Articles on psychosocial interventions, psychopharmacotherapy, mental health primary care, institutional and community care innovations, decentralization, policy changes, community & regionally based systems, and program evaluation are given particular attention. However, all articles that relate to psychosocial rehabilitation will be considered. We invite comment from all readers on any and all subjects published in this journal, including the journal format itself. Feel free to comment on the Bulletin Board as well. Current Editorial Board A. Anderson, Ph.D. R. Eisenman, Ph.D M. Merlo, M.D. P. Mcgrath, Ph.D. D. Young, Ph.D. K. Yip, Ph.D. A. Johnston, R.N. J. Shankar, Ph.D., RSW United Kingdom United States Honduras Australia Hong Kong Hong Kong United Kingdom Canada Publishing Information The International Journal of Psychosocial Rehabilitation is published byadg, S..A.(ADG) ADG is a private non-profit, limited corporation in Honduras and operating in a limited capacity in the United Kingdom. All information in IJPR is provided for personal use. Reproduction for publication or other use is strictly prohibited. Written permission must be obtained ADG, S.A., to reprint any information contained within the Journal, either in part or its entirety. Such permission may be requested in writing at the address listed below: Dr. A.J. Anderson Managing Editor - IJPR 500 Avebury Boulevard Milton Keynes MK9 2BE United Kingdom ~ 3 ~
4 Feature Articles ~ 4 ~
5 Cognitive behavioural treatment for problematic hoarding: A case study James Binnie Lecturer in Counselling Psychology Senior Cognitive Behavioural Psychotherapist BABCP accredited therapist, supervisor and trainer NMC registered Mental Health Nurse Senior Fellow of the Higher Education Academy Department of Psychology London South Bank University, 103 Borough Road, London, SE1 0AA jamesbinnie@lsbu.ac.uk Citation: Binnie J. (2015) Cognitive behavioural treatment for problematic hoarding: A Case Study. International Journal of Psychosocial Rehabilitation. Vol 20 (1) 5-14 Abstract A fifty one year old man's difficulties associated with hoarding are presented using a case study methodology. A psychological formulation and treatment plan is constructed following the work of a case study by Frost and Steketee, (1998). Despite some improvements in his functioning and clinical scores the overall reduction in clutter did not meet expectations. The focus of the discussion is the lack of published literature on hoarding behaviour, and the implications this has on interventions. Also highlighted are the issues associated with psychiatric diagnosis and the way in which this can influence decision making. Keywords: CBT, Hoarding Case study Introduction: Hoarding is the gathering of, and failure to throw away, large numbers of possessions that appear to be useless, or have limited value. For hoarding to be seen as a disorder living spaces must also be sufficiently cluttered so as to stop activities for which those spaces were designed, the individual also needs to be significantly distressed or to show an impairment in functioning caused by the hoarding (Frost and Hartl, 1996). Frost, Steketee and Williams (2000) performed a scoping exercise by contacting 88 health departments in Massachusetts, USA, serving a population of 1.79 million people. From their study a prevalence of 2.6 people in 10,000 displaying problematic hoarding behaviour can be calculated. The authors concluded that hoarding behaviours were judged to seriously jeopardise the health of the individual and those around them. However, the actual prevalence of problematic hoarding may be a lot higher as the above study only investigated cases that had already come to the attention of the health departments. Hoarding behaviour can be present in a variety of disorders, including anorexia nervosa, organic mental disorders, psychotic disorders, obsessive-compulsive personality disorder and learning disability; however, the majority of research links hoarding to obsessive-compulsive disorder (OCD; Frost and Hartl, 1996). Frost and Hartl (1996) found that compulsive hoarding is a little studied phenomenon within published literature and that the information is diverse ~ 5 ~
6 and not well integrated. The limited research on treatment for hoarding behaviour suggests that medications for OCD are largely ineffective and that the current evidence base concerning treatment supports cognitive and behavioural approaches (Steketee and Frost, 2003). However, the evidence base for individual interventions for problematic hoarding is mainly derived from case studies (e.g. Frost and Steketee, 1998; Hartl and Frost, 1999; Cermele, Melendez-Pallitto and Pandina, 2001; Seedat and Stein, 2002). Of the available research on hoarding found, the majority centres on theory and not practice; most single case studies and reports have been descriptive rather than treatment orientated. It is apparent that to ascertain the effectiveness of cognitive and behavioural treatments in managing hoarding behaviours there is a need for additional research (Seedat and Stein, 2002). The most practice based case report found was the work by Frost and Steketee (1998). Frost and Steketee (1998) suggest that hoarding involves four types of deficits: 1) Information-processing deficits; in particular decision making difficulties, categorisation/organisational issues, and memory problems 2) Problems with emotional attachments to possessions; whether it is sentimental or security based 3) Behavioural avoidance; saving possessions allows the hoarder to avoid the loss of objects that may be needed someday, hoarding prevents emotional upset associated with discarding possessions, and also hoarding avoids decision making. 4) Distorted beliefs about the nature or importance of possessions; i.e. unrealistic beliefs about the probability and severity of negative consequences if possessions are discarded. Frost and Steketee (1998) applied their hoarding model to a single case study, and from this developed a treatment strategy that involves the three processes described above. The first of these is training in decision making and organisational skills: This involves category creation (keep object, sell/donate object, or discard object), the primary goal is to create uncluttered living space, with a secondary goal of increasing the appropriate use of space. This training should be performed in the context of weekly excavation sessions with homework between sessions. The excavation session incorporates the second aspect of the treatment, exposure to discarding: the primary goal being to habituate the associated anxiety. Cognitive restructuring of hoarding related beliefs is the third component: this can also be done during the excavation sessions when unhelpful beliefs are expressed. Frost and Steketee (1998) put forward that each session should begin with a target area being agreed upon, then category creation, excavation can then begin with cognitive restructuring utilised where appropriate. In their study, Frost and Steketee (1998) worked with their client for 35 sessions. With the inherent limitations of basing treatment on case study methodology the current study has tentatively explored existing research in order to find a model and associated treatment plan. How this was applied an individual with problematic hoarding will now be presented. Clinical case presentation Background Fred was a fifty-year-old man living in an inner city area of London. He described his early home atmosphere as difficult, as his father was an alcoholic and suffered from depression. School was hard for Fred as he felt he didn t fit in, like he was a leper. From seven to ten years old Fred went to a boarding school where he suffered physical and sexual abuse, he describes this period as hell. He left school with six O-Levels and begun an art course. After this he worked as a photographer, he worked on and off until the age of thirty-six. He had some relationships but none that lasted long term. Although he had always drunk alcohol heavily since being an adult his alcohol use became out of control in his thirties and he had periods of homelessness. Fred first came into contact with mental health services at the age of forty-four when he was referred to a psychiatrist due to his alcohol misuse. In addition to his problems with alcohol it was suggested that he had a diagnosis of OCD, characterised by ruminatory thinking and hoarding behaviour. He successfully completed a community alcohol ~ 6 ~
7 detoxification and then attended group psychotherapy for two years. He was then referred to a day hospital for further group work and key working. On meeting Fred he had been abstinent from alcohol for two years. He had not had a relationship for many years and rarely contacted his family. He lived alone in a one-bedroom housing association flat and was training in alternative medicine. Although engaged in community activities he was socially isolated and had no real connections apart from at college and with health professionals. He presented as stable throughout our time together, he was relaxed and calm and responded well in conversation, however at times he came across as very intense in regards to his mannerisms. Fred was always on time for our appointments and seemed fully engaged with the process. Presenting problems Fred reported that his flat was full of his possessions and there wasn t enough living space. For years Fred had brought, and also found, lots of items that he took home. Whilst at home he spent his time churning the objects around the house and putting them into different categories. Fred got the urge to go through his possessions, without throwing them out, all the time he was in the flat, he acted on the urge until he distracted himself doing college work, listening to the radio, or by sleeping. What Fred feared most of all was that he would get too anxious when throwing things away as he thought he may need them again in the future. Fred found as a result of his problem that he had less time to do the things he wanted to. He never had people around to the flat; he reported that no one had been there in over 18 months. Fred described the problem as a sense of hopelessness, which lead to a low mood and despair. Practically Fred was unable to bathe or shower at his flat, unable to cook anything but simple meals and had to sleep on a board on top of the clutter. Fred believed that his problem with hoarding went back to childhood, as he had always been messy and his home life was chaotic. Fred stated that the urge to hoard had been with him as long as he could remember; and once he was allocated his own flat a few years ago he was able to act on his urges. He had never had treatment for his hoarding behaviour, only for alcohol misuse. Fred had read books and papers regarding hoarding and he sometimes looked into alternative medicine to find help. Measurement tools and goals for therapy Obsessive Compulsive Inventory The Obsessive Compulsive Inventory (OCI; Foa et al., 1998) is a measure of the frequency of a range of obsessions and compulsions and associated distress. The measure can be used for diagnosis and to determine the severity of OCD. The OCI has 42 items, for each item a rating is made for frequency from 0 (never) to 4 (almost always), and for distress from 0 (not at all) to 4 (extremely). Total frequency and distress scores can be calculated, scores range from 0 (no frequency or distress) to 168 (highest frequency and distress). For an OCD group the mean total frequency score was found to be (SD = 29.4), and for total distress score was (SD = 31.9). For a control group the mean total frequency was (SD = 21.2) and for mean total distress was (SD = 20.8) (Foa et al. 1998). At assessment Fred s total frequency score was found to be 85 and his total distress score was 83. With these scores Fred would compare to the OCD group. Clutter Ratios A visit to Fred s flat was undertaken after the initial meeting to assess the level of hoarding. The flat and the areas of cluttered space were measured. Clutter ratios (Frost and Steketee, 1998) were taken: For floor areas: Living room/kitchen = 92%, Bathroom = 88%, Hallway = 81%, Bedroom = 100%. For all surfaces and furniture = 100% (Clutter ratios are calculated by dividing the area of total room or surface space by the by the area that is cluttered. Mean score for sample populations is 5%). A video recording and still images of the flat were also taken (images can be found in the appendix 1). Goal Statement ~ 7 ~
8 I would like to feel comfortable with having a friend around for dinner. I would also like a 50% reduction in the clutter in my flat; I would like to achieve this in 3 months. Fred rated that to achieve this now would be extremely difficult (8 on a scale of 0-8, 8 being the highest). Psychological formulation Fred believed that he had an unsatisfactory relationship with his parents and therefore had formed relationships with his possessions. It could be hypothesised that the possessions hold an unrealistic value to Fred, as he is so reluctant to throw them away. Furby (1978) developed this notion of relationships with objects by suggesting that there are two types of hoarding; instrumental saving, where the possession fulfils some desire or purpose; and sentimental saving, where the possession serves as an extension of the self (i.e. it has an emotional attachment). From Fred s early experiences of an unsettled home life and abuse it can be speculated that he had difficulties forming appropriate attachments to care givers. He may have seen himself in a negative way and not trusted others. To cope with the difficult feelings this would have produced he turned to alcohol as a way of coping. This eventually led him to being homeless, thus emphasising the importance of security and possessions. Then years later when he stopped drinking and found new accommodation the difficult feelings returned and he started to hoard as a way of fulfilling his need for meaningful attachments. The problem was maintained through Fred s collecting of useful items and his avoidance of throwing away items in his flat. When he was in his flat looking at the clutter, Fred thought I must get rid of all these things. He then mentally pushed these thoughts away, as he began to feel anxious and tired, as a result Fred either left the flat, went to sleep or more often than not spent time churning and categorising the clutter, but not throwing it away as he makes information processing errors. Fred believed that throwing away possessions causes anxiety, if he purposely avoided the discarding then he would not experience the anxiety; therefore he learnt, through negative reinforcement, that avoidance is beneficial as it stopped him becoming anxious. Also, through his avoidant behaviours he did not disconfirm the original unhelpful thought that every object is useful. The development and maintenance of Fred s problems with hoarding can be shown diagrammatically: ~ 8 ~
9 Treatment rationale It has been described how Fred s avoidant behaviours, decision-making deficits and emotional attachments perpetuated his hoarding behaviour, resulting in a disturbance in his lifestyle and distress. For Fred to unlearn his unhelpful behaviour (i.e. his avoidance of discarding possessions), he needed to habituate to the associated anxiety that he experienced when he contemplated discarding possessions and learn that when he discarded possessions, after time his anxiety would decrease naturally. This mechanism intended to enforce change through interrupting the negative reinforcement of Fred s avoidance of discarding possessions. With repeated exposure to the feared situation of discarding possessions, Fred s unhelpful learnt behaviours would become unnecessary and therefore redundant. This technique is supported by Baer (1991) who found a behavioural programme of exposure to discarding beneficial in cases of individuals with hoarding symptoms. ~ 9 ~
10 It was hoped that through the behavioural programme Fred would habituate the associated anxiety. However, he would still have poor decision making abilities and overvalued ideas related to the possessions, and could bring more items back to the flat in the future. To counteract this possibility, it was intended to train Fred in decision making and organisational skills. The purpose of this was that once Fred learnt how to place items into defined categorises, it would become easier and less anxiety provoking to discard them (Frost and Steketee, 1998). To ease this process cognitive restructuring of hoarding related beliefs could be initiated using Beck s (1985) model of cognitive therapy; the aim of which is to propose alternatives to unhelpful beliefs, through techniques such as Socratic questioning, generation of alternative thoughts, behavioural experiments (Beck, Emery and Greenberg, 1985). Interventions Fred was reluctant to let me see his flat, therefore the first treatment session consisted of planning the therapy and explaining the treatment rationale, during this session cognitive re-structuring was begun in regards to his hoarding related ideas. The week after Fred agreed to let me see his flat, base line measurements of the flat were taken to help calculate the clutter ratios. To help increase his daily functioning the bedroom was the first target area. Categories were set (keep object, sell/donate object, or discard object) and excavation began. Fred found this less anxiety producing than expected as he could identify a lot of items as rubbish. Homework was set to continue to discard possessions each day for at least an hour or until anxiety reduced. In the subsequent session it was discovered that although Fred had done some discarding for homework he had not been doing it every day and that he had moved possessions from the bedroom to the bathroom, rather than throwing them away. Practical considerations were discussed as to the best way forward and we agreed that to focus on discarding larger objects first would be better as this would create more room to move about and allow further discarding. A pattern soon developed whereby Fred would ruminate excessively on decisions whether to throw items away and this reduced any possible habituation to discarding. We therefore developed a timetable to help him plan his time and to focus on less emotionally charged items. Fred responded to this well and by the time I saw him next seven bags of clutter had been discarded; however more possessions had been moved from one room to another. To counter-act this behaviour, I witnessed Fred as he cleared areas. I tried to teach him that decisions should not be dwelt on, as one of the purposes of treatment was for him to experience anxiety when throwing away items and for him to experience the anxiety naturally decreasing and therefore habituate it. This process of therapist assisted discarding and decision making training was repeated in subsequent sessions. Fred became more confident in the discarding and the levels of associated anxiety decreased. We therefore set more ambitious targets: 15 bags of clutter per week. This process continued for the remaining sessions. Due to the levels of clutter in his flat Fred was able to identity much that could be discarded. However, when we discussed throwing out items he saw as potentially more useful (e.g. the third broken oven) he was unable to remove them and they became almost a barrier between us. When this occurred I spent time first of all drawing up lists of pros and cons of discarding the object; when this was not effective I would bring Fred back to his goals to allow him to see the object as working against them. Fred was seen for 25 sessions of active treatment over six months, each session took place in his home and followed the structure above. Towards the end of our sessions together it became apparent that, although considerable amounts of clutter were being removed from the flat, progress had plateaued. The main reason for this was the sheer scale of the project and Fred not having access to friends or family that could physically help. As Fred had learnt and practised the excavation routine and also changed his relationship to objects as he had prioritised his goals, we decided to end our sessions and agreed to meet in three months for a follow up session. ~ 10 ~
11 Outcomes Pre Post OCI: Frequency 85/168 50/168 Distress 83/168 43/168 Clutter Ratios: Kitchen 92% 65% Living area 95% 50% Bathroom 95% 70% Bedroom 100% 60% By the end of sessions noticeable changes had been made in the flat; in the kitchen especially, Fred reported that it used to take him four hours to cook dinner before sessions, at the end of sessions it took him an hour. In addition, he was able to use his bathroom facilities and there was considerably more floor space in the bedroom, allowing him to sleep in there. Fred had stopped bringing in new objects into the flat. However, despite his progress there was still a large amount of clutter that impacted on his day to day functioning. At follow up there had been some progress but not the amount that had been expected. Fred reported that he had been removing clutter but was also spending time enjoying his time in his flat and this reduced the amount of time he was devoting to removing clutter. Again, new objects had not been brought back to the flat. His goal of having someone round to dinner had not been realised. By the end of our time together Fred had reduced his clutter by 34% over the nine months. Discussion The cognitive behavioural assessment and treatment of a client with hoarding behaviour has been described. The practical interventions used were based on a specific case study by Frost and Steketee (1998). Integral to the majority of the case studies that focus on hoarding is the implicit assumption made by clinicians and researchers that hoarding tends to be predominately associated with OCD (Grisham and Norberg, 2010). This assumption also influenced Fred s treatment and lead to the focus being on the role of anxiety and exposure (evidence based practice for anxiety disorders). However, some of Fred s symptoms could have been found in other disorders such as anankastic personality disorder (obsessive-compulsive personality disorder). Fred would have also fulfilled the criteria for this as he presented with at least three of the set characteristics: feelings of excessive doubt and caution, preoccupation with details, rules, list or order, and intrusion of insistent and unwelcome thoughts or impulses (ICD-10, W.H.O, 1992). It has been put forward that individuals with OCD and one or more comorbid personality disorders are less responsive to drug and behavioural treatments (Baer and Jenike, 1998). With this in mind this may account for why Fred did not experience the expected levels of anxiety whilst discarding. Therefore, basing his treatment on diagnosis lead to difficulties as one, the diagnosis may have been incorrect, and two because psychiatric diagnosis are in themselves neither valid or reliable (Kutchins and Kirk, 1999; Bentall, 2003). By assuming the validity and reliability of psychiatric diagnosis therapists (including myself at times) often lack a critical perspective and fail to see the client as an individual with individual problems. In addition, hoarding can be seen as a disabling problem in its own right rather than aligning itself to a psychiatric diagnosis which has to cover so many variables and cannot ever account of the rich variation in clinical presentations (Stein, Seedat and Potocnik, 1999). From re-examining Fred s psychological formulation it can be hypothesised that the maintaining factors for Fred may have been more cognitive than behavioural and thus should have been the focus of the sessions. For example if more attention had been given to Fred s beliefs about objects (influenced by his history of trauma) then perhaps Fred s treatment may have progressed differently. This criticism echoes the move to transdiagnostic ways of working and rejecting the dominance of diagnosis driven therapy. ~ 11 ~
12 Conclusion This study aimed to demonstrate how CBT was applied with a particular client. The effectiveness and implications of the assessment have been discussed in detail, as have the treatment outcomes. Focussing clinical practice on the available evidence base has been discussed; it has been found that although certain methodologies may be unscientific they can still provide a framework to help benefit clients with compulsive hoarding if a case conceptualisation leads interventions rather than a diagnosis. References Baer L, Jenike MA (1998). Personality disorders in obsessive-compulsive disorders. In Jenike MA. Baer L, Minichiello WE (Eds). Obsessive-Compulsive Disorders. Practical Management. 3rd edition. (1998) Mosley. St. Louis Beck AT, Emery G, Greenberg RL, (1985) Anxiety disorders and phobias: A cognitive perspective. New York: Basic Books. Cermele JA, Melendez-Pallitto L, Pandina GJ (2001) Intervention in compulsive hoarding: a case study. Behav Modif. 25 (2): Chic SN, Chong HC, Lau SPF (2003). Exploratory study of hoarding behaviour in Hong Kong. Hong Honk Journal of Psychiatry. 13 (3): Foa, B.E., Kozak, M.J., Salkovskis, P.M., Coles, M.E., Amir, N. (1998). The validation of a new obsessive-compulsive disorder scale: The Obsessive-Compulsive Inventory. Psychological Assessment, 10 (3): Frost RO, Hartl TL. (1996) A cognitive-behavioural model of compulsive hoarding. Behav Res Ther. 34: Frost RO, Steketee GS (1998) Hoarding: Clinical aspects and treatment strategies. In Jenike MA. Baer L, Minichiello WE (Eds). Obsessive-Compulsive Disorders. Practical Management. 3rd edition. (1998) Mosley. St. Louis Frost R, Steketee G, Williams L (2000) Hoarding: a community health problem. Health Soc Care Community. 8 (4): Furby L, (1978) Possessions: Toward a theory of their meaning and function throughout the life cycle. As cited in Stein DJ, Seedat S, Potocnik F (1999) Hoarding: a review. Israel Journal of Psychiatry and Related Sciences. 36 (1): Grisham, JR, Norberg, MM (2010) Compulsive hoarding: current controversies and new directions. Dialogues in Clinical Neuroscience. 12(2): Hartl TL, Frost RO (1999) Cognitive behavioural treatment of compulsive hoarding: a multiple baseline experimental case study. Behaviour Research and Therapy. 37: Seedat S, Stein DJ (2002). Hoarding on obsessive-compulsive disorder and related disorders: a preliminary report of 15 cases. Psychiatry Clin Neurosci. 56 (1): Steketee G, Frost R. (2003) Compulsive hoarding: current status of the research. Clin Psychol Rev. 23 (7): Stein DJ, Seedat S, Potocnik F (1999) Hoarding: a review. Israel Journal of Psychiatry and Related Sciences. 36 (1): World Health Organisation (1992) The ICD-10 classification of mental and behavioural disorders. Geneva: WHO Library Cataloguing in Publication Data. ~ 12 ~

13 Appendix 1 ~ 13 ~

14 Appendix 2 ~ 14 ~
15 Effectiveness of a Recovery Program for Chinese Psychiatric Inpatients LAI, Frank Ho-yin CHIU, Julian Chim-keung TSE, Phyllis Lai-Chu TSUI, Jess Wan-man CHEUNG, Jacky Pak-Ho CHEN, Eddie Wei-chieh CHAN, Suki Hoi-yee FAN, Silvia Hiu-ue CHAN, Annie Suk-man CHEUNG, Jonathan Chin-chung WONG, Simon Kam-man Citation: Lai FH, Chiu J C, Tse PL-C, Tsui JP, Cheung JP-H, Chen EW, Chan SH, Fan SH, Chan AS, Cheung JC, Wong SK.. (2015) Effectiveness of a Recovery Program for Chinese Psychiatric Inpatients. International Journal of Psychosocial Rehabilitation. Vol 20 (1) Correspondence Address: lhy180@ha.org.hk Occupational Therapy Department, Tai Po Hospital, Tai Po, HKSAR Abstract This study is a retrospective evaluation study for a 63 Chinese clients with schizophrenia, bipolar affective disorder, depression and adjustment disorder in recovery program. This study is going to note genders specific response to the recovery program and to identify predictors for their length of hospital stay. All recruited subjects would participate in a three-week recovery program. A series of goal setting training, psycho-education and empowerment activities, and therapeutic group sharing were included. Clients level of hope, mental-wellbeing, and ability in recovery and illness management would be assessed by Chinese Hope Scale (CHS), Chinese Short Warwick-Edinburgh Mental Well-being Scale (CSWEMWBS) and Chinese Illness Management and Recovery Scale (CIMRS). Subjects showed improvement in generating routes to recovery goals, enhanced capacity in initiating and maintaining the actions to reach their recovery goals. Moreover, clients showed significant improvement noted in seeking social support. Genders showed their specific characteristics in their pattern of recovery. Key words: Recovery, Well-being, Illness Management Introduction: In late 1900s, psychiatric care was largely based on medical model which focused on medical model (Campbell-Orde et al., 2005), relapse prevention (Anthony et al., 2002),and to maintain clients level of functioning (Frese et al., 2001). It has been emphasized that each individual's journey to recovery is a personal process, as well as being related to an individual's community and society; alike the model by Repper & Perkins (2006) which focused on social inclusion in relation to recovery. With further reference to the work of Campell-Orde and colleagues on 2005, the later recovery model was developed with the input from clients whom diagnosed with different mental illness. They highlighted what supported or blocked them from living with their illnesses and the later development of recovery model focuses more on client s daily life and peer support rather than treatment. In early 2000 s, Frese and his colleagues further developed their recovery model which scrutinize on individual s recovery journey with the person deciding what he or she needs to recover (Frese et al, 2001). Davidson, O Conell, Tondora, Styron and Kangas (2006) further suggested the concept of recovery in, ~ 15 ~
16 which means the client lives in a safe, dignified manner in the community with the accommodations and supports that he or she needs. Since then, mental health practitioners moved to the development of recovery oriented systems and recovery had become a guiding force in developing mental health policy and practice in foreign countries (Davidson et al., 2006). This study adopted the values of recovery by Farkas, Gagner, Anthony and Chamberlin on 2005 as shown in Figure 1.This model of recovery was renowned by conceptualizing recovery-oriented mental health programs to both providing direction to those involved in program implementation of evidence based mental health practices, as well as providing a stimulus for further development of recovery program. (Farkas, 2007; Farkas & Anthony, 2010). These values had been shown to be evidence based and been well studied for years (Rogers & Farkas, 2008; Slade et al., 2014; Lyman et al., 2014). These values included considerations in person orientation, person involvement, self-determination and growth potential (Farkas et al., 2005). Firstly, in person orientation focuses on client as a whole with strengths. Secondly, person involvement focuses on the unique characteristics of each client while developing his/her own expectation in recovery. Thirdly, self-determination focuses on assisting client to make informed choices and to gain or accept responsibility for their own choices. Fourthly, growth potential focuses on client s capacity to grow and to improve functioning. The purpose of this retrospective evaluation was to investigate outcomes for a group of clients who participated in a recovery-based occupational therapy program. Methodology From May 2015 to July 2015, 63 in-patients joined the three weeks program of recovery activities, which were held for sixty minutes, five mornings a week. These groups were conducted by registered occupational therapist, therapy assistants and patient care workers. Groups were held on occupational therapy department. Occupational therapists assess, monitor and treat clients by providing treatments in our inpatient unit. As part of a multidisciplinary team, occupational therapists collaborate to educate clients, their family and also communities. Occupational therapists believe that recovery from mental illness is possible, but the process takes place in a series of small steps. Clients need knowledge, skills and coping strategies to help relieve their symptoms and manage stress to rejoin their uniqueness in the community. Our designed recovery program aimed to promote successful recovery through proper goal setting, positive thinking, taking control and empowering their life and life role rebuilding through a series of education and discussion modules. This program included five elements as therapeutic modules as shown in Figure 2. Firstly, ~ 16 ~
17 in the module of Hope, client would have increased positive thinking and with feelings of healing and hope. Moreover, this is to increase trust in self and others through therapeutic activities. Secondly, in Support and Managing Symptoms module, client would understand how to manage symptoms and advise on healthy lifestyle changes to help prevent relapse. Thirdly, in the module of Empowerment, clients would develop confidence by problem-solving, goal setting and focusing on own strengths, to discuss stigma, to improve social skills, assertiveness and self-awareness. Fourthly, in the module of Relationships, clients would learn how to improve tolerance, anger management and communication skills. Activities include exploring emotions, communication, anger and conflict. Fifthly, in Coping, client would develop personal coping strategies for selfmanagement and stress reduction; cope with feelings of depression, anxiety, frustration and anger. Moreover, to assist client to recognize distorted thinking. Concepts of cognitive behavioral therapy were woven through the program. The group leader could choose from a variety of optional activities of recovery and illness management as considered to be appropriate. Sequence of programmed sessional activities and lessons bellows were modified according to the progress of patients as needed. Concepts to be delivered to patients in the treatment program including: - Session A. Identification of hope and development of faith - Session B. Enhance personal responsibility and productivity - Session C. Promote self-management and autonomy - Session D. Importance peer support and community life - Session E. Frustration tolerance building and to learn forgiveness - Session F. Social acceptance and enhance self-awareness - Session G. Adaptability and capacity to change - Session H. Situational applicability Outcome measures Chinese Hope Scale (CHS) It is a 12-item measure of a client s level of hope. Snyder et al (1991) defined hope is defined as a cognitive set that is based on a reciprocally-derived sense of successful agency (goal directed determination) and pathways (planning to meet goals). It is divided into two subscales that comprise Snyder s cognitive model of hope (Snyder et al., 1991): (1) Agency (i.e., goal-directed energy) and (2) Pathways (i.e., planning to accomplish goals). Of the 12 items, 4 (Items 1,4,6 and 8) make up the Agency subscale and 4 (Items 2,9,10 and 12) make up the Pathways subscale. The remaining 4 items are fillers. Each item is ~ 17 ~
18 answered using an 8-point Likert-type scale ranging from Definitely False to Definitely True. It is internally consistent with Cronbach alpha =.81with p <.001 for agency factors, and Cronbach s alpha, 0.82 with p <. 001 for pathway factors (Snyder et al., 1991), yet the agency and pathways subscales are factorially identifiable as subcomponents of the overall measure, which accounted for 67.2% of the variance. The four agency items load principally on one factor and the four pathways items load principally on another. Chinese Short Warwick-Edinburgh Mental Well-being Scale (CSWEMWBS) The SWEMWBS is measure for mental wellbeing of clients. Responses in the form of a Likert scale included none of the time (scored 1), rarely (2), some of the time (3), often (4), and all of the time (5). Scores ranged from 7 to 35, with a high score reflecting a high level of mental wellbeing. The scale was validated, with good content validity, moderately high correlations with other mental health scales and lower correlations with other scales measuring overall health. The C-SWEMWBS by research team of Ng on 2014, was cross-culturally adapted from the original English version. The C-SWEMWBS is a short 7-item questionnaire C-SWEMWBS showed good internal consistency (Cronbach s alpha, 0.89) and the principal components factor analysis identified a single component (eigenvalues, 4.28; 61.1% variance), which was consistent with that of English version (Ng et al., 2014). Scores of CSWEMWBS were positively correlated with the scores of WHO5 (r = 0.49; p < 0.001), suggesting it came with good concurrent validity (Ng et al., 2014). Chinese Illness Management and Recovery Scale (CIMRS) IMRS have been developed to assess the clients' progress towards recovery and better illness management (Mueser et al., 2005). It contains 15-items to capture different aspects of recovery, such as knowledge about mental illness, social support, treatment adherence, relapse prevention planning, coping efficacy, and substance abuse and dependence. Previous research has established good internal consistency, test retest reliability and convergent validity for the IMRS among clients with severe mental illness (Hasson-Ohayon, 2008). This scale was translated into Chinese by a group of local experts in the field of psychiatric rehabilitation. All these instruments would be used to document patients condition immediate before the implementation and after their completion of recovery-based rehabilitation training. Data Analysis Descriptive statistics were applied to the demographics, number of previous admissions and their primary diagnosis, T-test analysis would be used to measure if there would be any mean difference before and after the recovery program. Moreover, t-test would be used to compare genders responses in the program. ANOVA analysis would be employed to assess if there would be any difference in variance among different diagnostic groups. Results Convenient sampling strategy would be used to recruit subjects for the present study. The participants had to fulfill several selection criteria: 1) Aged between 18 and 60 years old, 2) In-patient status in a regional psychiatric hospital, 3) Are ethnic Chinese who can read and understand Chinese. With consideration on smoothness of program and discussion running, patients cannot read and understand Chinese would be excluded in this study. All selected subjects would be screened by an occupational therapist whom had properly understood the content to the recovery program. In order for the subjects to be prepared to voluntarily participate they were first be informed as to what the purpose of the study was, from whom they could access further information about the researchers and/or the study, how their anonymity would be maintained, how findings would be disseminated, information, if appropriate, about benefits, and a reiteration that participation was voluntary. The potential for harm in this study was considered to be minimal. In order to maintain confidentiality all subjects' names were be changed and let- ~ 18 ~
19 ters were assigned to each participant. Extreme care was taken in the maintaining a secure database and in the reporting of findings in order to preserve the confidentiality of the data collected, as what had been suggested in literature (Neuman, 2003). A convenient sample of 63 clients was recruited, and the demographic information was shown in Table 1 Table 1 Gender Female : 25 Male : 38 Demographic Information Martial Status Single: 42 Married : 11 Divorced / Widowed : 8 Martial Status Single: 42 Married : 11 Divorced / Widowed : 8 Educational Level Primary : 6 Secondary : 46 Tertiary and above : 10 Living With Family : 41 Alone : 14 Hostel : 5 Others : 3 Occupation Status (before admission) Unemployed : 46 Gainfully employed : 12 Vocational Training : 6 Years of Onset New Onset : 7 Onset less than 2 years : 18 Onset btwn 2 to 5 years : 10 Onset more than 5 years : 28 Primary Diagnosis Gp 1 Schizophrenia / Psychosis / Delusional Disorder : 38 Gp 2 Bipolar Affective Disorder : 12 Gp 3-Depression : 10 Gp 4- Adj. Disorder : 3 Assessment on Mental Well-being Clients mental well-being was measured by the Chinese-SWEMWBS. The raw score was displayed in Table 2. Among the whole study population, in t-test analysis, there was significant difference in the Chinese SWEMWBS before and after recovery program (t = 2.15, p <.05). There was significant difference noted in feeling relaxed (t = 2.23, p <.01), dealing with problems well (t = 2.34, p <.05), feeling close to other people (t = 2.32, p <.05), able to make up my own mind about things (t = 1.89, p <.05). Specifically, in male subjects, among the measures by the CSWEMWBS There was significant difference in the item I ve been feeling close to other people (t = 2.63, p <.05) when individual items were investigated. In female subjects, interestingly, there were significant difference in the item I ve been feeling relaxed (t = 3.67, p <.001), I ve been dealing with problems well (t = 2.19, p <.05), and I ve been feeling close to other people (t = 2.53, p <.05) when individual items were investigated. There was no significant difference in CSWEMWBS and the seven subscales among four different diagnostic groups. Assessment on Level of Hope ~ 19 ~
20 Clients level of hope was measured by the Chinese Hope Scale as shown in Table 2. There was significant difference noted in I energetically pursue my goals (t = 1.23, p <.05), my past experience have prepared me for my future (t = 1.65, p <.05), I ve been pretty successful in life (t = 2.23, p <.01) and I meet the goals that I set for myself (t = 2.56, p <.01) Table 2. T-test analysis for CSWEMWBS, Chinese Hope Scale and Illness Management & Recovery Scale (N= 63) Variables Subscales Before After t M SD M SD CSWEMWBS Feeling optimistic about the future Feeling Useful Feeling Relaxed ** Dealing with Problems Well * Thinking Clearly Feeling Close to * Other People Chinese Hope Scale Able to Make up My * Own Mind about Things I can think of many ways to get out of a jam I energetically pursue my goals I feel tired most of the time There are lots of ways around any problem I am easily downed in an argument * I can think of many ways to get the things in life that are most important to me ~ 20 ~
21 I worry about my health Even when others get discouraged, I know I can find a way to solve the problem My past experiences * have prepared me for my future I ve been pretty successful ** in life I usually find myself worrying about something Illness Management and Recovery Scale (IMR) I meet the goals that ** I set for myself 1. Progress towards * personal goals 2. Knowledge * 3. Involvement of family and friends in my mental health treatment * 4. Contact with people outside of my family Time in Structured Roles Symptom distress Impairment of functioning 8. Relapse Prevention Planning * ~ 21 ~
22 9. Relapse of Symptoms 10. Psychiatric Hospitalizations Coping Involvement with self-help Activities 13. Using Medication Effectively 14. Functioning affected by alcohol use 15. Functioning affected by drug use * * *p <.05, **p <.01, ***p <.001 When female subjects were analyzed, there was significant difference between before and after treatment program in both Pathway subscale (t = 2.63, p <.05) and Agency subscale (t = 2.89, p <.05) of the Hope Scale. Nevertheless, in male subjects, there was significant difference in Pathway subscale (t = 2.92, p <.05) but not in Agency subscale (p >.05) when measures between before and after treatment program. Male participants note to have significant higher pathways thinking than females (t = 3.42, p <.001). Moreover, there are no significant difference in the both Pathway subscale (F = 1.49, p >.05) and Agency subscale (F =.202, p >.05) among different diagnostic groups. Assessment on Illness Management Clients illness management and recovery was measured by Illness Management and Recovery Scale as shown in Table 2. In the whole study population, there were significant difference in progress towards personal goals (t = 1.98, p <.05), knowledge (t = 3.72, p <.001), Involvement of family and friends in my mental health treatment (t = 2.08, p <.05), Relapse Prevention Planning (t = 2.30, p <.05), Involvement with selfhelp activities (t = 3.58, p <.001), Use of Medication Effectively (t = 3.14, p <.01). Male clients seem with less improvement in their illness management and recovery. There were significant difference in knowledge (t = 2.14, p <.01) and Involvement with self-help activities (t = 2.51, p <.05). Nevertheless, female clients showed better response in their illness management and recovery, as shown in knowledge (t = 2.14, p <.05), Involvement of family and friends in my mental health treatment (t = 2.22, p ~ 22 ~
23 <.05), Symptom distress (t = 2.21, p <.05), Relapse Prevention Planning (t = 2.30, p <.05), Coping (t = 3.67, p <. 01), Involvement with self-help activities (t = 3.58, p <.001), Use of Medication Effectively (t = 3.14, p <.01). There was no significant difference among different diagnostic group in the IMR, except in Time in Structured Role (p <.05), in which, the group of schizophrenic clients showed lesser time in doing activities for or with another person. Predictors of Recovery A regression analysis was conducted to predict clients length of stay with those recovery measures as shown in Table 3. The regression model was able to predict a significant proportion of variance in intention of helping (R² =.32). Agency subscales in the Chinese Hope Scale contributed significantly to the regression model (β =.21), while the feeling of getting closer to other people contributed (β =.09), feeling relaxed (β =.11), dealing with problems well (β =. 09) in CSWEMWBS showed their significance. Moreover, the involvement of family and friends in recovery (β =.09) and increased in knowledge of recovery (β =.12) showed significant contribution in Illness Management and Recovery Table 3. Prediction of LOS from Recovery Factors (N = 63) Predictor Variables B SE β t Hope Scale Agency Subscale * Illness Management and Recovery Involvement of Family & Friends * Increase knowledge in Recovery * CSWEMWBS Feel closer to other people * Feel Relaxed * Deals with Problem * Note. *p <.05, **p <.01, ***p <.001 [R 2 =.32] Discussion This study is a retrospective evaluation study for a group of in-patient clients who participated in a recovery-based occupational therapy program. There were a number of positive changes noted in our clients throughout and after this recovery program. Firstly, there is significantly positive change noted in identifying and getting social support from clients in our study. It is worth to note that there is significant improvement noted in getting involvement from their family and friend. This was reflected from the significant difference noted in clients self-reported illness management and well-being measure. These positive changes could be attributed by their social network re-activation and more social inclusion, as suggested from findings of Perry and Pescosolido on Interestingly, female clients showed significant awareness in getting social support from their trusted one than male. This phenomenon could be rectified by the study of Davidson on 2003 that male would adopt their recovery journey by involving in a limited social network than female (Repper & Perkins, 2006). Genders specificity in their social collection and getting social support was underscored from this recovery program. Secondly, after the recovery program, both genders showed their enhancement in knowledge and information acquisition in recovery. It partially reflected the effectiveness of psycho-education as an effective media in promoting the concept of recovery for our Chinese Hong Kong population. These findings also shared by previous researches like the one by Petersen et al on Moreover, another study conducted by Mueser on 2002 ~ 23 ~
24 found that psycho-education would increase individuals insight into illness and affected sociability. It was believed that recovery strategies were acquired through knowledge and skills obtained in relationships with therapist, therapy assistants, and other clients with their own experience of mental illness. Thirdly, clients felt more relaxed throughout and after the recovery program. This could be attributed by their acquisition of knowledge in their illness management and strategies in relapse prevention. Moreover, this therapeutic group interaction can enhance their communication between each other in a relaxed but therapeutic environment. A number of coping strategies could be role-played and shared through an error-free and criticism free trial among clients. Furthermore, it is interesting to note that female clients showed better outcome in coping and dealing with problems well after this recovery program. On the other hand, male clients would more likely to accept direct knowledge and instructions by officials (Fitzgerald, 2010). These finding further echoed to the work by Schön, U.K. (2010), which showed that female would be more effective in learning coping strategies than male (Schön, 2010). Fourthly, it is worthy pointing out that female showed significant change in both pathway thinking and agency thinking in the hope scale measure. However, male showed only significant change in pathway thinking. This phenomenon could be explained by the work by Snyder et al (1991). In their study, they hypothesized that both agentic and pathways thinking are necessary for higher levels of hopeful thought (i.e. they are additive). On the other hand, they can reciprocally interact (i.e. they iterate in the thoughts of people as they entertain their goals). Although agentic and pathways thinking are related, they are not synonymous. Therefore, they refer to differing aspects of the goal directed thinking process. This can justify female and male adopt different perspective in formulating their recovery and illness management strategies. Male would have enhanced ability to generate routes to his recovery goals. Apart from the enhance ability in male, female clients would have enhanced capacity for initiating and maintaining the actions necessary to reach a goal. Our findings echoed the work by Schön (2010) that female showed to be an advantage in the recovery process than male. The recovery of female clients would be facilitated by emotionally supportive social relationships with others who listened to them, and who understood and showed engagement. The male recovery process is under the influence by gender constructions both in terms of societal gender expectations and in terms of the men doing gender in their strategies to control the illness (Harding, 1986). Finally, there is significant difference of clients with schizophrenia than other groups of clients in Time in Structured Role as the measure of illness management and recovery. This could be attributed by the fundamental difference in pre-morbid life roles of our clients as shown in previous study (Fitzgerald, 2010). Premorbid life role is considered as a crucial but missed parameter that was missed to address in this study, nevertheless, this is worth to be considered for further study. Moreover, factors like early onset of illness, the predominant negative symptoms and limitation in social skills development of clients with schizophrenia would further impede their use of time in structured role. Conclusion Recovery is a common theme in rehabilitation for clients with mental illness nowadays. Recovery is considered as a journey in clients life, with ups and downs. This study is the pioneer study in showing the effectiveness of a recovery-based occupational therapy program for in-patients in a regional psychiatric hospital. Through the recruitment of 63 clients with diagnosis groups of schizophrenia, bipolar affective disorder, depression and adjustment disorder, their mental well-being and progress towards recovery and illness management were assessed. After a series of planned recovery program in psycho-education program and therapeutic group sharing, clients showed their enhanced knowledge in recovery, enhanced ability to generate routes to recovery goals, enhanced capacity in initiating and maintaining the actions that necessary to reach their recovery goals. Female subjects showed more positive changes than male subjects in getting social involvement in their ~ 24 ~
25 recovery than male subjects. Results provide new insights into gender as an important factor in understanding recovery processes and in providing care to facilitate these processes. Further studies with larger samples from more diversify populations are suggested for generalization of the results. Moreover, the study period would be too short follow up if exploring outcome, more like post-review evaluation without insight into how long the positive effect can sustain References Anthony, W.A., Cohen, M.R., Farkas, M., Gagne, C. (2002). Psychiatric rehabilitation. Boston: Center for Psychiatric Rehabilitation. Campbell-Orde. T., Chamberline, J., Carpenter, J., Leff, H.S. (2005). Measuring the promise: a compendium of recovery measures (vol II). Cambridge, MA: Human Service Research Institute. Davidson, L. (2003). Living Outside Mental Illness: Qualitative Studies of Recovery in Schizophrenia. New York University Press, New York. Davidson, L., O Conell, M., Tondora, J., Styron, T. & Kangas, K. (2006). The top ten concerns about recovery encountered in a mental health system transformation. Psychiatric Services, 57(5): Farkas, M. (2007). The vision of recovery today: What it is and what it means for services. World Psychiatry, 6(2), 1-7. Farkas, M., & Anthony, W. A. (2010). Psychiatric rehabilitation interventions: A review. International Review of Psychiatry, 22(2), Farkas, M., Gagne, C., Anthony, W.A. & Chamberlin, J. (2005). Implementing recovery oriented evidence based programs: identifying the critical dimensions. Community Mental Health Journal, 41(2): Fitzgerald, M.M. (2010). Comparison of recovery style and insight of patients with severe mental illness in secure services with those in community services. Journal of Psychiatric and Mental Health Nursing, 17: Frese, F.J., Stanley, J., Kress, K. & Vogel-Scibilia, S. (2001). Integrating evidence-based practice and the recovery model. Psychiatric Services, 54(11): Harding, S. (1986). The Science Question in Feminism. The Open University Milton Keynes, Milton Keynes, UK. Hasson-Ohayon, I. (2008). The psychometric properties of the Illness Management and Recovery Scale: client and clinician versions. Psychiatry Res, 160(2): Lyman, D.R., Kurtz, M., Farkas M., George, P., Dougherty, R., Daniels, A.,Ghose, S.S., & Delphin-Rittmon, M.E. (2014). Skill building: Assessing the evidence. Psychiatric Services, 65(6), Mueser, K.T., Corrigan, P.W., Hilton, D.W., Tanzman, B., Schaub, A. & Gingerich, S. (2002). Illness management and recovery: a review of the Research. Psychiatric Services, 53(10): Mueser, K.T., Gingerich, S., Salyers, M.P., McGuire, A.B., Reyes, R.U., Cunningham, H. (2005). Illness Management and Recovery (IMR) scales, in measuring the promise. In: Campbell-Orde, T., Chamberlin, J., Carpenter, J., Leff, H.S. (Eds.). A Compendium of Recovery Measures. Evaluation Center and Human Services Research Institute, II. Cambridge, MA, p Ng, S., Lo, A., Leung, T., Chan, F., Wong, A., Lam, R. & Tsang, K. (2014). Translation and validation of the Chinese version of the Short Warwick-Edinburgh mental well-being scale for patients with mental illness in Hong Kong. East Asian Archives of Psychiatry, 24:3-9. Perry, B.L. & Pescosolido, B. (2015). Social network activation: the role of health discussion partners in recovery from mental illness. Social Science & Medicine, 125: ~ 25 ~
26 Petersen, K.S., Friis, V.S., Haxholm, B.L., Nielsen, C.V. & Wind, G. (2015). Recovery from mental illness: a service user perspective on facilitators and barriers. Community Mental Health Journal, 51:1-13. Repper, J. & Perkins, R. (2006) Social Inclusion and Recovery: A Model for Mental Health Practice. Bailliere Tindall, UK. ISBN Rogers, E.S., & Farkas, M.(2008). Making the Grade: Identification of evidence-based communication messages. In: J. Parker and E. Thorson (Eds.) Health Communication in the New Media Landscape, Ch. 13. London: Springer. Schön, U.K. (2010). Recovery from severe mental illness, a gender perspective. Scandinavian Journal of Caring Sciences, 24: doi: /j x Snyder, C.R., Harris, C., Anderson, J.R., Holleran, S.A, Irving, L.M. & Sigmon, S.T. (1991). The will and the ways: Development and validation of an individual-differences measure of hope. Journal of Personality Social Psychology, 60: Slade, M., Amering, M., Farkas, M., Hamilton B., O Hagan M., Panther. G., Perkins, R., Shepherd, G., Tse, S., & Whitley, R. (2014). Uses and abuses of recovery: implementing recovery-oriented practices in mental health systems. World Psychiatry, 13(1), ~ 26 ~
27 It made me think a little different a qualitative study of young adult cancer survivors experiences of cognitive therapy in cancer rehabilitation. May Aasebø Hauken,RN, cand.polit, PhD Center for Crisis Psychology, Bergen, Norway Linda Viken, Physiotherapist, MSci Red Cross Haugland Rehabilitation Center, Norway Citation: Hauken MA & Viken L. (2015) It made me think a little different a qualitative study of young adult cancer survivors experiences of cognitive therapy in cancer rehabilitation. International Journal of Psychosocial Rehabilitation. Vol 20 (1) Correspondence: Center for Crisis Psychology, Fortunen 7, 5013 Bergen, NORWAY. address: may@krisepsyk.no Abstract Young adult cancer survivors (YACS) have increased risk for psychosocial late-effects. Cognitive therapy (CT) aims to enhance coping in survivorship, but research of CT interventions and how YACS experience these lacks. This study s aim was to explore YACS experiences of CT in a rehabilitation program. A phenomenological-hermeneutical design was used, including semi-structured interviews of 17 YACS who completed a rehabilitation program. Two main themes and three corresponding subthemes emerged: The first theme, «CT as a tool», was elaborated by the subthemes «education and practicing», «follow-up» and «internalization». The second theme, «the perceived usefulness of CT» was clarified by the three subthemes «changed thought patterns», «insight and acceptance» and «handling a new life-situation». The participants experienced CT as a useful tool in their rehabilitation process that changed their thought patterns and helped them getting insight and acceptance as an important basis to handle their new life-situation. Keywords: Young adult cancer survivors, cognitive therapy, cancer rehabilitation, qualitative method Introduction: ~ 27 ~
28 Young adult cancer survivors (YACS) are a small and understudied group of survivors, with specific challenges related to their vulnerable period of life, and their increased risk for morbidity and long- term effects (Albritton et al., 2006; Institute of Medicine, 2013). There is a research gap in survivorship-care for YACS, especially related to rehabilitation (Hall et al., 2012; Institute of Medicine, 2013). Cognitive therapy (CT) is seen as a promising intervention for enhancing coping and quality of life in survivorship (Juvet et al., 2009; Osborn, Demoncada, & Feuerstein, 2006), but we have no knowledge of how YACS survivors experience CT in cancer rehabilitation. Previous research Cancer in young adulthood (18-35 years) is rare (Albritton, Barr, & Bleyer, 2009; Cancer Registry of Norway, 2014), where the cancer types, the genetic, biological and physiological characteristics are unique (Bleyer & Barr, 2009; Institute of Medicine, 2013). The treatment is often aggressive, multi- modal and long lasting (Albritton et al., 2009; Bleyer & Barr, 2009). For YACS, being in a vulnerable period of life (Buchmann & Kriesi, 2011), cancer adds a tremendous burden and life disruption (Albritton et al., 2006). Cancer in YACS also includes high risks of severe late-effects, where some are life threatening as cancer recurrence, subsequent cancers, and chronical diseases (Brearley et al., 2011; Woodward, Jessop, Glaser, & Stark, 2011). Other late-effects compromise health and well- being in a long term (Woodward et al., 2011). These range from physical promlems such as pain, lymphedema, infertility and fatigue (Harrington, Hansen, Moskowitz, Todd, & Feuerstein, 2010; Institute of Medicine, 2013), phsycosocial problems as anxiety, depression, fear of recurrence and impaired self-esteem (Albritton et al., 2006; Zebrack, 2011), impairments in social functioning (Hall et al., 2012; Zebrack, 2011), as well as risk of educational delay and financial problems (Brearley et al., 2011; Parsons et al., 2012). Despite these impairments that seriously may jeopardises YACS s ability to move into wellfunctioning adulthood (Sansom-Daly et al., 2012), they report inadequate follow- ups and rehabilitation interventions (Brearley et al., 2011; Hall et al., 2012; Keegan et al., 2012). Studies of rehabilitation interventions for YACS lacks (Johansen, 2007; Juvet et al., 2009), but the two most evident effective elements in cancer rehabilitation for adults are physical activity (Speck, Courneya, Masse, Duval, & Schmitz, 2010) and different psychosocial interventions (Faller et al., 2013; Hersch, Juraskova, Price, & Mullan, 2009; Juvet et al., 2009; Osborn et al., 2006). For the latter, CT is highlighted as an important intervention, showing positive effects on coping, empowerment, self-efficacy, quality of life, depression, anxiety and fear of recurrence (Faller et al., 2013; Fors et al., 2011; Hersch et al., 2009; Juvet et al., 2009; Lebel et al., 2014; Osborn et al., 2006), as well as fatigue (Eichler et al., 2015; Gielissen, Verhagen, Witjes, & Bleijenberg, 2006). In general, the evidence-base of CT is very strong to a wide range of psychological problems (Beck, 2005; Hofmann, Asnaani, Vonk, Sawyer, & Fang, 2012), but the interventions vary greatly with respect to psychological strategies and technics, intervention content and duration. In cancer rehabilitation, CT interventions typically include education, focusing of unhelpful thoughts or behaviours as well as coping skills training (Faller et al., 2013; Hersch et al., 2009; Juvet et al., 2009; Osborn et al., 2006). The majority of these studies are quantitative, including only brief decriptions of the interventions, and it is not evident how these interventions should be designed (Fors et al., 2011). We have not found any studies eloborating how CT is experienced by cancer survivors, neither any studies of CT including YACS, indicating a research gap. In line with this, Sansom-Daly et al. (2012) state that CT is a promising, but mainly untested intervention that may equip YACS with coping skills to successfully manage their survivorship challenges. Theoretical framework Modern cognitive therapy (CT), often used synonymously with cognitive behavioral therapy (CBT), refers to a family of interventions that combine a variety of cognitive, behavioral, and emotion- focused techniques (A.Beck, 2005; Hofmann et al., 2012). ~ 28 ~
29 CT is based on learning- and cognitive psychology, relating on the cognitive model explaining how thoughts, emotions and bodily reactions mutually interacts (A. Beck, 2005; J. Beck, 2006). This model, also called the cognitive diamond, explains that how an individual perceives and interprets a given situation determines the feelings and behaviors associated with the event (Figure 1). Consequently, behaviors are influenced and determined by how an individual structure his or hers world through cognitions stored in memory as schemes, developed from prior experiences (A. Beck, 2005; J. Beck, 2006). These schemes are activated in special situations or states of mind, and will affect emotions, behavior and psychological activation. Maladaptive cognitions may thus contribute to the maintenance of emotional distress and behavioral problems. In contrast, problems can be reduced, or solved, by consciously being aware of these mutual relationships (A. Beck, 2005; J. Beck, 2006; Hofmann et al., 2012). CT typically involves a short time, structured and present-oriented training, aiming to teach individuals to identify and moderate their negative, automatically thoughts (NAT) and maladaptive behaviors, and thus reduce emotional stress (Arendt & Rosenberg, 2012; Hofmann et al., 2012). This presupposes that the individual learn to detect and be conscious of his/hers negative, automatically thoughts (NAT), to explore and questioning misinterpretations, destructive behavior and assumptions, and then find realistic and alternative reevaluations, followed by acting as this reevaluation is true. Aim The aim of this study is to explore YACS experiences of CT in a rehabilitation program after finishing cancer treatment. More specifically, we elaborated the research question: «What experiences do YACS have in using CT in a rehabilitation program?» Methods Study design This study is a part of a larger study of rehabilitation of YACS (Hauken, 2014). Based on the present study s aim, we conducted a phenomenological - hermeneutical research design (Creswell, 2007 ). This design aims to explore the meaning of the lived experiences of individuals about a phenomenon (phe- ~ 29 ~
30 nomenology), here YACS experiences of CT in cancer rehabilitation, and the researcher s interpretations (hermeneutics) in order to gain new insight and understanding of a phenomenon (Creswell, 2007 ; Malterud, 2011). Participants YACS were invited to join the study by different websites and healthcare professionals in hospitals and in primary healthcare in Norway (Hauken, 2014). The eligibility criteria were a) YACS aged years, b) finished cancer treatment within the last 5 years, and c) all cancer diagnoses. An oncologist or general practitioner verified the YACS s rehabilitation need and referred them to the study. The final sample included 17 informants fulfilling the 6-month rehabilitation program. Table 1 outlines the background variables, diagnoses and cancer treatments. Table 1: Demographic and Medical Presentation of Study Population (N=17) Age (years) Gender Female Male Education Senior High School University/University College Social status Married/Cohabitate Single/Divorced Employment Working or Study Full Tim/part timee Full Sick Leave Number Mean or Standard Deviation Percent 17 31,1 3, % 5 29% 6 35% 11 65% 8 47% 9 53% 10 59% 7 41% Type of cancer ~ 30 ~

31 Lymphoma Gynecological Breast Testes Colon Sarcoma Head & neck Months since diagnose Type of treatment Only surgery or chemo Multimodal treatment Months of treatment Month since treatment 3 18 % 5 29 % 3 18 % 2 12 % 2 12 % 1 6 % 1 6 % 27,0 16,7 8 47% 9 53% 22,3 6,8 7,3 6,3 The intervention The rehabilitation program was structured around three weeks of residential rehabilitation with one- week follow-up after three and six months, and based on six elements: 1) individual goal-setting, 2) physical activity 3) individually follow-up, 4) peer-support, 5) psycho-education based on CT and 6) a next of kin-weekend. The intervention is described in detail elsewhere (Hauken, 2014). Here, we will only focus on the psycho-education based on CT. The psycho-education aimed to increase the participants knowledge of survivorship-issues, and to give them tools to cope with their survivorship challenges (Faller et al., 2013; Fors et al., 2011; Luknes & McFarlane, 2004). The YACS participated in seven 90 minutes sessions of psycho-education during their primary stay, covering topics that were particularly relevant to them. Each session included an introduction, a teaching, training and discussion-section, followed by summing up and homework. CT was used consistently throughout all sessions as a method to discover and to cope with negative thoughts, emotions and maladaptive behaviors (Arendt & Rosenberg, 2012; J. Beck, 2006), exemplified by the YACS s own experiences. The 'five-columns-scheme' was used as a practical tool for detecting and revising negative thoughts, emotions and behaviors (Arendt & Rosenberg, 2012) (Figure 2). ~ 31 ~
32 The YACS also practiced CT by writing their own challenges in the scheme as homework between the sessions. For each topic, they received corresponding readings. Table 2 shows the specific content for each session, and homework and literature. Table 2: Organization and content of the psychoeducation Number Title Content Homework Literature 1 Get Started Intro: Purpose, structure, rules Illustrate & present: Who am I? What am I god at? Setting goals: short term & longterm Introduction to Cognitive Therapy (CT), Wilhemsen: Boss in your own life, Chapter Basis of Cognitive Therapy Intro: Summing up from session 1 & homework Teaching & discussion: Intro to CT, The Cognitive Diamond& ABC tool Use ABC on one of the main topics and identify thoughts and attitudes Wilhemsen: Boss in your own life, Chapter 10 3 Education and Work 4 Thoughts and Emotions 5 Exercise and Physical Activity 6 Me and my Network Intro: Summing up from session 2 & homework Teaching & Discussion: Education and Work related to cancer, rights & possibilities Intro: Summing up from session 3 & homework Teaching & discussion: Coping of physical and psychosocial late effects & use of CT Intro: Summing up from session 4 & homework Teaching & discussion: Physical activity & fatigue after cancer treatment. Benefit of physical activity,how & what to exercise (stepwise) Intro: Summing up from session 5 & homework Teaching & discussion: Network. Illustrate& present: «Who are in your network? Cohabitation and sexuality related to cancer Use ABC related to own situation regarded study/work Use ABC related to own situation regarded coping/negative thoughts and emotions Use ABC related to own situation regarded to physical activity Use ABC related to own situation regarded network/sexuality Norwegian Cancer Society: Rights for patients and relatives Wilhemsen: Boss in your own life, Chapter 10 Norwegian Cancer Society: Physical Activity After Cancer Treatment Norwegian Cancer Society: Cancer and Sexuality ~ 32 ~
33 7 The Way Ahead Intro: Summing up from session 6 & homework Teaching & discussion: Summing up on theme 1 6. What learnt? What to bring with you? Goal achievement short time Information on restay The second author, an experienced physiotherapist, specialized in CT, led the psycho-education. In addition, specialists in the different topics conducted the lectures. At the follow-up visits, the participants got one 90 minutes session using CT each week, focusing on their experienced challenges at home. Altogether, the structured psycho-education and CT counted for approximately 15 hours. Data collection The first author collected all data by in-depth interviews at the end of the rehabilitation program. A semi-structured interview guide with open-ended questions was developed to ensure consistency related to the YACS experiences of CT in the rehabilitation program (Creswell, 2007 ). The main question in the guideline was: Can you please tell me how you have experienced using CT in this rehabilitation program? Follow-up questions were related to the different elements of the content and duration of CT, if and how the YACS had used CT, as well as their total experience. The interviews lasted for minutes, and were digitally recorded and transcribed by the authors. Analysis Systematic Text Condensation (STC), a four-step cross-case analyses, was used to analyze the data (Malterud, 2012). However, analyses of qualitative data is not a straight forward process, but engage the researchers in processes moving in analytical (hermeneutical) circles including several facets of analyses (Creswell, 2007 ). Both authors analyzed and coded the transcribed data separately to enhance validity, and then discussed and performed the rest of the analyses together (Creswell, 2007 ; Malterud, 2012). Following the steps in STC, we first read the interviews to obtain a general impression. The general impression revealed that the YACS emphasized different facets of using CT. Second, we re-read the interviews and extracted units of meaning. We used NVivo 9 software package to code and sort data. In this process, we extracted six codes. Third, these codes were condensed into groups and subgroups during an analytic circle between the identified codes, the transcribed interviews and discussions. We concluded with two main units of meaning or themes: CT as a tool and The perceived usefulness of CT. Further analyses revealed that the two meaning units had three subgroups each. Finally, we validated the analyses by comparing the findings against the interviews to ensure that we had captured the informants expressed and intended meanings. All interpretations reached consensus. We summarized by using direct statements. Table 3 outlines the analyses process. Table 3: Overview of the STC analyzes process STEP 1: Getting a total impression STEP 2: Identifying meaning units STEP 3: Abstracting the contents of individual meaning units STEP 4: Summarizing of findings ~ 33 ~
34 Process: a) The authors read the transcribed interviews separately b) Discussed the total impression to consensus Identified total impression: CT used consciously and unconsciously Different elements: - education - process over time - internalization - practical use/effect Process: a) The authors coded the data separately b) Discussed the codes to consensus within the codes Identified meaning units: Code * Used CT/not used CT Use of CT/applications Changed thought patterns Perceived change Education Tools Source ** *Code: Identified meaning units Referen ces *** Process: a) The authors analyzed the contents separately b) Several discussions to consensus Abstracted contents/themes: 1. CT as a tool Subthemes: -education and practicing -follow-up -internalization 2. The perceived usefulness of CT Subthemes: -changed thought patterns -insight and acceptance -handling a new life condition Process: b) The authors discussed the findings against the transcribed interviews c) Each author found direct statements to elucidate units of meaning and discussed to consensus Summarizing: Summarized findings and presenting direct statements within the abstracted contents ** Source: Number of informants talking about the code (N = 17) *** References: Number of quotes related to the code Ethics The Western Norway Regional Committee of Research and Ethics, and The Norwegian Social Science Data ~ 34 ~
35 Services (NSD) approved the study. We followed their guidelines throughout the study. The YACS got written and verbatim information about the study, and all participants gave written consent. Findings The aim of this study was to explore how YACS experienced CT in a rehabilitation program. The analysis reviled two main-themes: «CT as a tool» and «The perceived usefulness of CT». Both themes had several facets, and three sub themes emerged as important elements within each theme. Main theme 1: «CT as a tool» Most YACS experienced that CT was a useful tool in their rehabilitation process, exemplified by these quotes: «In fact, it is a very good tool. Yes, at least it has learnt me a lot. And I will continue to use it. (P 19), and «I think it has been a tool. I dare not think about it if I had not been here» (P 7). Even those few who did not see CT as a useful tool for themselves, still acknowledged it as a suitably tool for others. However, the YACS highlighted that you cannot use a tool without learning how to use it. The analyses revealed that «CT as a tool» was dependent and elaborated by the three subthemes «education and practicing», «follow-up» and «internalization» which described important elements of this learning process. Education and practicing The majority underlined that the use of CT as a tool was dependent of education and practicing to understand how it worked: «Because you get a tool and you have to learn how to use it. This requires practicing. (P 6). The basic knowledge of the cognitive diamond, and how negative automatic thoughts (NAT), emotions, bodily reactions and behavior were connected, was very important: It helped a lot And to have the facts, how it works and to have the knowledge I have realized that knowledge is good and can help me a lot on my way to a life (P 20). Additionally, the participants underlined that using their own and others real life examples and write these in the «five- columns scheme» during the sessions, was an important way to acknowledge the relevance of CT into their own life situation. The scheme was experienced as a practical tool in the learning process, helping them to grasp the structure of how to use CT. However, several participants found it difficult to formulate and write their problems on their own as part of their homework: «It is most just thoughts... I have tried to write it down, but [I] do not get it formulated so... «(P 20) and «To write it down, then I just felt a bit lame» (P 13). As a part of the learning process, the participants also got readings related to the actual topic as homework, but the YACS experienced these differently. Some expressed that the readings filled out the education and practical training in the sessions in a good manner, while others had trouble in concentrating and called for less and more specified literature related to their situation: «Related to the book, then I think a lot of us read it, but reading page up and page down I think it do not give the right understanding...shorter and easier perhaps» (P 6). Summing up, learning to use CT seem to be dependent of an introduction of the basic elements in CT, how the cognitive diamond work, as well as an introduction of the five-column scheme. Furthermore, practicing CT by using the YACS own challenges, as examples seem to be important. The initial practicing by writing their own challenges at home as well as comprehensive readings seemed to be more challenging. «Follow-up» The majority experienced that learning to use CT was a process in need of time and follow-up. The YACS stated that the knowledge had to be internalized, where training and focus over time was essential: «...It has to ~ 35 ~
36 be followed-up over time if you shall learn to use CT. You have to have some time to let it sink in» (P 4). In contrast, a few participants did not like this focus over time because they found it difficult to open up and be confronted with their own challenges: «I did not want to dwell a lot with it and puh go through those [difficult thoughts] (P 8). Still, these participants acknowledged that this was necessary to be able to cope with their present challenges: «I found it very useful to be forced to, yes, to deal with it myself. To address issues and work constructively.» (P 8) The YACS had only one session of CT on each of their two re-stays, focusing on their experiences at home. These challenges were guided on by using the five-column scheme : «I used my problem as an example in CT, so then I got to think of it in a different way» (P 13). However, several informants called for more CT sessions at the re-stays: «You need some time, even if it is very simple. It is not as if you need many hours to understand what it is. You just need practice and maybe more time on the re- stays I would like to have even more focus on this way of thinking. Not just focus, but more follow- up (P 13). Some participants found it difficult to share their problems openly in the group, especially related to sexuality and fertility problems, and thus needed more individual follow-up. Summing up, learning to use CT as a tool seem to be a process over time in need of continuously repetition and professional follow-up. «Internalization» «Internalization» emerged as the third subtheme in using CT as a tool, describing how the participants eventually internalized CT in different ways. The majority worked with CT in line with the program by first writing down actual examples, before they eventually freed themselves from the scheme. At the end of the program, most of the informants expressed that they had internalized CT and used it more or less automatically: «Now I do not write, I wrote in the beginning, but now I think. To say it in a simple way, I try to think alternatively (P 2) and «I use it, have internalized it. I have practiced on myself, inner training I guess» (P 4). Some participants expressed that they had CT back in their minds, but did not use it consciously. In contrast, some YACS used CT consciously and still wrote down their challenges: «Mmmmm, I write too.on the scheme, because at a certain point I discovered that I really thought negatively about myself, that I did not COPE» (P 17). Summing up, the majority of the participants had learned to use CT, and still used it, at the end of the rehabilitation program, even if they had internalized it at different levels. However, the degree of internalization of CT seemed to be connected to which, and the degree of, survivorship challenges they experienced. Main theme 2: «The perceived usefulness of CT» The «The perceived usefulness of CT» emerged as the second main theme. In general, all the YACS expressed that CT was useful in their rehabilitation process. They described several aspects of this usefulness, elaborated in the three subthemes: «changed thought patterns», «insight and acceptance» and «handling a new life condition». «Changed thought patterns» The majority of the participants expressed that CT had changed their way of thinking, by being able to discover and be aware of their own NAT: «At least, now I take myself in thinking wrong.yes, automatic thoughts that comes, and then I take myself» (P 13). The most frequent mentioned NAT were related to fatigue, sexuality and fertility issues, follow-up, and cancer recurrence. The YACS underlined that CT not necessarily was an easy way to solve their challenges, because some problems were very realistic as for example physical alterations, fertility problems and risks for cancer recurrence. But identifying NAT still seemed to be a prerequisite to be able to change their thought pattern and handle the situation in a more appropriate way: «I think that I ~ 36 ~
37 have learned [to use] CT and that has lifted me up from..i was quite down when I came in January dealing with my grief [being infertile]. I feel that I have got a lot of help from it at least up to certain level». (P 3), and «Now, I can recognize them [NAT], but I have to work a lot more with them..» (P17). This work was especially related to reevaluation of NAT, and finding alternative interpretations. Through this process, several participants told that their levels of anxiety, concern and even physical symptoms were eased: «I used it when I was going to the follow-up The difference is that you in a way can try to. You can in a way turn your thoughts. That you Why are you so nervous and.to think a little bit more.that I try to not worry about things I cannot do anything with» (P9). «Insight and acceptance» Most YACS expressed an increased insight and acceptance of their own situation through the CT and psychoeducation. This was important in order to process what they had gone through during the treatment: «Yes, it must have helped while instead of trying to repress the whole situation; I have rather tried to accept it and just let it be» (P 11). By being more consciousness of their own thought patterns, some YACS discovered that they had placed a lid over their present situation, and that CT and the increased insight made room for «open the lid» - even if this was difficult: «Yes, I do not think the lid is as closed anymore. However, it is difficult, because I cry a lot more than I did before. (P I7). The YACS expressed that they were «normalized» through the psychoeducation, using CT and sharing their own experiences and challenges with others. This «normalization» also contributed to an increased insight and acceptance of their present situation: «To be able to process these thoughts and feelings while being here.that s when you have had the time thinking properly. The thoughts still are there afterwards, but to be reassured that you are not alone thinking like that» (I 19). Through this process, several participants expressed that they had regained some if their former security and self-esteem, even if this had been a long and demanding process for some: «I now manage to have the right focus and to avoid negative thoughts... And gradually, yes, you just work steadily with the stuff and reminding that you shall reach the goal, and then you manage..yes, it is simply the self-esteem. Because, the negative and the bad stuff in your head then in a way becomes weaker and weaker» (P 5). «Handling a new life situation» By using CT, and being able to detect NAT and the increased insight and acceptance, «handling a new life situation» emerged as the third subtheme of how the YACS used CT. For most participants, the cancer treatment had caused extensive changes in their present life-situation. Especially, fatigue led to an extensive decrease in their capacity to participate in different areas of life. To cope with and accept this situation, handling the fatigue was crucial, where CT seemed to be an important tool: «CT has helped me to realize that my fatigue is not that un-normal» (P8). By understanding that it was notrealistic to have the same levels of activity as before, several participants expressed that CT was a useful technic to correct their own requirements and to discover their own coping capabilities. «I have learned that I have to listen to my body and (sighs) and not set too high standards for myself, but it takes time and THAT is something I have learned during this rehabilitation.[ I have] LEARNED a lot of myself..and got more self-secure while I can SEE that I can cope.» (P 19). For all the YACS, it was very important to be able to participate in work/studies after a long sick leave. Several used CT to be realistic and adjust their plans in accordance to their new life situation. Here, follow-up and guidance seemed to be essential as well: «Yes, that someone. pointed out my direction, and that I in fact ought to scale down my work and have a greater focus on myself and not that conscience... That was the most important part» (P 12). Handling everyday life also included restarting «normal» activities as for example their social life, but several participants experienced anxiety and NAT in this process. Here, CT seemed to help them to reduce their anxi- ~ 37 ~
38 ety level and to handle different everyday situations: «I have not as much anxiety. Mmmm I strived a lot with negative thoughts or I didn t know how to handle situations» (P 18). Summing up, the YACS found CT useful in several ways, where detecting NAT and changes in thought patterns were especially important. Together with the psychoeducation, and the discussions with the other YACS, it seems that CT helped them to get insight and acceptance of their present situation, and thus handle their new life-situation in a more constructive way than before. Discussion The purpose of this study was to explore YACS experiences of CT in cancer rehabilitation. The findings show that the participants experienced CT as a useful tool, dependent of education, practicing and follow-up before it could be internalized. Additionally, the YACS perceived that CT was useful in their rehabilitation process, as it changed their thought patterns, helped them to get insight and acceptance of their present situation, and thus handle their new life-situation. This is one of the first studies of a CT intervention targeting YACS, and in our knowledge, the first study to explore the learning process of CT and the perceived usefulness for YACS. Using CT needs education, practicing and professional follow-up The first important message is that the YACS experienced and acknowledged CT as an important tool in their rehabilitation process. This is in line with Sansom-Daly et al s (2012) assumption that CT may equip YACS with coping skills to handle their survivorship issues, as well as studies of older cancer survivors where CT has shown positive effects of several survivorship challenges (Faller et al., 2013; Gielissen et al., 2006; Osborn et al., 2006). This is also in line with the theory of CT to promote self- help and being a tool that individuals can use in challenging situations (A. Beck, 2005; J Beck, 2006). We have found no other studies on how cancer survivors learn to use CT, and our findings give important knowledge into this process. The YACS expressed that the education and practice along with repetitions and follow-up were crucial elements in internalizing and using CT. Especially, the knowledge to understand the cognitive diamond and the connections between thoughts, feelings, behavior and body was crucial. Supporting this, J. Beck (2006) states that it is by understanding these connections, that the individual is able to solve or reduce their problems. Likewise, Luknes and McFarlane (2004) state that knowledge is essential to cope with one s own situation. The results revealed that education in itself was not sufficient to learn to use CT. The YACS highlighted that practicing and using their own examples were essential in the learning process, as this helped them to acknowledge the relevance of CT into their situation. Accordingly, Osborn et al (2006) and Sansom-Daley et al (2012) found that targeting specific problems in such interventions more likely bring positive outcomes. Using their own examples, the YACS also expressed that the five- column scheme was a practical tool and important to understand how CT worked. A clear goal in using the five column-scheme is to detect negative thoughts and feelings and to clarify the connection between these (Arendt & Rosenberg, 2012; J. Beck, 2006). According to literature (Arendt & Rosenberg, 2012), the YACS got homework between the sessions to stimulate the learning process. However, several participants found both the writings and readings difficult. This may be due to overload, based on their fatigue and subsequent difficulties in concentrating as described in other studies (Campos, Hassan, Riechelmann, & Del Giglio, 2011; Smith et al., 2013). The readings also seemed to be too comprehensive and not enough tailored to their needs. These results indicate that it is not easy to learn CT by yourself, and that homework should be initiated gradually, not be too comprehensive, and more directly tailored to the YACS situation. The participants also highlighted that learning CT was a process over time in need of professional follow-up. ~ 38 ~
39 This is in line with other studies indicating that CT interventions have to involve more than 6 sessions and last for more than 3 months to achieve positive outcomes (Faller et al., 2013; Juvet et al., 2009; Osborn et al., 2006; Sansom-Daly et al., 2012). However, the participants need for follow-up seemed to vary. Some found that the follow-up in the program were sufficient, while others called for more follow-up, - especially at the restays. The YACS need for follow-up seemed to be connected to the degree and privacy of their challenges. Some participants felt not comfortable sharing their challenges within the group, but preferred to discuss them with a therapist in privacy. In line with this, the literature underlines the importance of addressing cancer survivors individual needs as these are multidimensional and may vary greatly (Brearley et al., 2011; Hall et al., 2012; Institute of Medicine, 2013). However, the literature also illuminate that group based interventions are important in providing positive effects on psychological health and coping, as it promotes social support and positive impact of cancer survivors knowledge about their illness (Austvoll-Dahlgren, Nøstberg, Stensbekk, & Vist, 2011). These results highlights that the program perhaps should have included a few more structured CT sessions on the re-stays, but that the combination of the group sessions and offers of individual follow-up seems to be important. Even if the results from the subthemes training and follow-up indicate some areas for improvements, the results show that the majority internalized CT as tool. However, the degree of internalization varied from using it by the book, to internalized it in their ordinary way of thinking, while other just bared CT in their minds. This indicates that the majority got enough knowledge and practice to use CT as a tool in their rehabilitation process. In line with these results, previous research has shown that education and training in using coping tools are important and useful elements in rehabilitation (Luknes & McFarlane, 2004). These results are also in line with theory of CT, stated to be a tool to increase the individuals understanding and handling their own situation (Arendt & Rosenberg, 2012; A.Beck, 2005; J. Beck, 2006). The perceived usefulness of CT The second important message from this study is that the YACS experienced that CT had been useful in several ways in their rehabilitation process. First, the participants expressed that learning to use CT had changed their though patterns. Here, they expressed that the most important element was to be aware of and to recognize their own negative thoughts (NAT). This result is consistent with theory of CT, pointing out that to discover and be conscious of negative thoughts as a vital element in changing thought patterns and thereby cope with challenging situations (A. Beck, 2005; J. Beck, 2006). This may be special important for YACS in order to cope with survivorship, as they have limited life-experiences and are fronting an unsecure future with potential health risks (Buchmann & Kriesi, 2011; Institute of Medicine, 2013). By discovering their own NAT, the participants expressed CT was a way to rethink and change NAT, and thereby be better able to handle their present challenges. This result support theory of CT, stating that maladaptive cognitions may contribute to maintenance of emotional distress and behavioral problems, while problems can be reduced or solved by consciously being aware of these mutual relationships (Arendt & Rosenberg, 2012; A. Beck, 2005). The YACS especially experienced that CT was useful related to fatigue, fertility problems, anxiety, follow-ups and fear of recurrence. These are common problems reported by YACS, all with potential seriously to jeopardize their health and wellbeing (Hall et al., 2012; Institute of Medicine, 2013; Woodward et al., 2011). In line with our results for YACS, previous research of older cancer survivors have demonstrated to be efficient for similar problems (Eichler et al., 2015; Faller et al., 2013; Gielissen et al., 2006). Other researchers support this, for example Lebel et. al. (2014) who found that group-based CT decreased cancer survivors fear of recurrence. However, the YACS stated that CT did not change their real life challenges as for example infertility or fear of recurrence, but helped them to cope and come to turn with these in a better way. In line with this, CT is about realistic and appropriate thinking, and not a way of positive thinking, as unrealistic thinking may reduce the individual s ability to cope with the actual problem (Arendt & Rosenberg, 2012; J. Beck, 2006). In contrast, CT aims to seek alternative thoughts and ~ 39 ~
40 solutions on perceived and actual challenges (Arendt & Rosenberg, 2012). Second, the YACS experienced that the psychoeducation equipped them with an insight and acceptance of their present situation. As for most CT intervention for cancer survivors (Faller et al., 2013; Hersch et al., 2009; Juvet et al., 2009), this study included education in both theory of CT and issues specially relevant for YACS, focusing of unhelpful thoughts or behaviours as well as coping skills training (Faller et al., 2013; Hersch et al., 2009; Juvet et al., 2009; Osborn et al., 2006). The YACS expressed that using CT in this process, forced them to reflect over different issues. By being concious about the connections in the cognitive model, made room for an insight and acceptance of their present situation. The individual s experiences of being able to affect and change their own NAT and thereby cope with their own challenges, is a basic goal in CT (A. Beck, 2005; J. Beck, 2006). In particular, a normalization of their present situation, feelings and thoughts, seemed to be important. Since the challenges of cancer survivorship in general are unknown, other studies highlights that discussions with other survivor-peers are important in processing experiences and gaining understanding, as well as legitimization and normalizing of their situation (Hansen & Tiornhoj- Thomsen, 2007; Mattson, Demshar, & Daly, 2013). However, as the YACS challanges could be very sensitive, severe as well as quite realistic, this demonstrate the importance of experienced and knowledgable professionals to facilitate the session. In line with this, several researchers state that positive effects of CT are dependent on skilled professionals who are able to address cancer survivors multidimensional needs (Faller et al., 2013; Hofmann et al., 2012; Osborn et al., 2006). Third, the results indicate that the YACS experienced that CT changed their thought pattern that provided an increased insight and acceptance of their present situation, and was thus an important tool in handling their new life situation. Previous research has shown that cancer often represent a serious life disruption, and that YACS are not well prepared to survivorship, lacking information, follow-up and rehabilitation interventions (Albritton et al., 2006; Hauken, Larsen, & Holsen, 2013; Institute of Medicine, 2013). YACS ask for tools to handle their life situation (Albritton et al., 2006; Institute of Medicine, 2013), and in line with research of older cancer survivors (Hofmann et al., 2012; Juvet et al., 2009; Osborn et al., 2006), it seems that the YACS experienced that CT represented such a tool. In particular, CT seemed to help them to normalize their life, for example related to anxiety and self-esteem, but also in making realistic judgements in how to return to work and studies, based on their reduced capacity. Here, several YACS experienced CT especially useful in their reality orientation, and being able to cope with the discomfort they experienced by having to adjust and change their own demands and goals. CT builds upon that individuals structure their world through cognitions based on previous conceptions and experiences stored in their mind, explaining why new challenges can be difficult to handle. By using CT, the goal is to understand and see these connections in order to reduce the stress.(j. Beck, 2006). Even if the results gives new and important knowledge of the learning process of CT and how the YACS used CT in multiple ways, this study has some limitations. Because of its qualitative design, it includes a relatively small sample from which findings cannot be generalized to the broader population of young adult cancer survivors (Creswell, 2007 ). Enrollment in this study was biased toward self-selection into the rehabilitation program, and with an underrepresentation of men and the youngest age group (18-23 years). A significant strength is, however, the enrollment of a diverse population of informants across the country, with varying backgrounds, life circumstances, and cancer diagnoses, age at diagnosis, cancer treatment, and duration of survivorship. Despite these limitations, the common themes were consistent, suggesting that we captured a valid sample of the experiences of using CT in a rehabilitation program directed to YACS that may help direct both future research and clinical practice. Implications clinical practice and recommendations for further research ~ 40 ~
41 The results indicate that CT can be an important tool for YACS to handle unmet needs and survivorship challenges. However, being able to use CT seems to be dependent of education by professionals, where understanding of the cognitive diamond, use of the five-column scheme, relate CT to the YACS own examples, as well as follow-up over time seem to be important factors in the learning process. Group-based education, discussions and follow-up may provide normalization, but based on the degree and sensitivity of the problems, individually sessions may also be necessary. Further research is necessary, both related to larger RCT studies examining the effects of using CT in rehabilitation of YACS, as well as exploring the content of CT to optimize and develop CT intervention for YACS further. Conclusion This study reveals important information about the unique experiences of how YACS experience CT in a rehabilitation program, an issue that has not been explored before. Most importantly, the findings indicate that the YACS experienced CT as a useful tool in their rehabilitation process. This was, however, dependent of adequate training where a combination of education, practicing, connecting CT to YACS s own challenges, as well as professional follow-up where important factors before CT could be internalized. Additionally, the YACS found CT useful in their rehabilitation process, as it changed their thought patterns and helped them to get insight and acceptance of their present life situation, as well as handling their new life-situation. Even if these results cannot be generalized, they suggest that CT could be an important tool for YACS to handle important survivorship challenges, and further research is highly warranted. Acknowledgement, financial disclosure and conflict of interest The authors thank the study respondents for participants for resilient participating and sharing their profoundly experiences. Thanks to Red Cross Haugland Rehabilitation Centre (RCHRC) employees for running the program so carefully according to the protocol; especially Kari Fismen for coordinating the project. Profound thanks to PhD Torill Larsen and PhD Ingrid Holsen at Hemil/University of Bergen, and MD/specialist in rehabilitation medicine Eirik Fismen at RCHRC for supervision. Thanks to Haugland International Research Centre for profoundly support. The research was generously supported by grants from Eckbo's Lagat and The Norwegian Cancer Society. The authors have no funding or conflicts of interest to disclose. Both authors have participated in in the planning, design, analysis, interpretation, writing, revising, and approval of the manuscript. ~ 41 ~
42 References Albritton, K., Barr, R., & Bleyer, A. (2009). The adolescence of young adult oncology. Semin Oncol, 36(5), doi: /j.seminoncol Albritton, K., Caligiuri, M., Anderson, B., Nichols, C., Ulman, D., & Adams, H. (2006). Closing the gap: Research and care imparatives for adolecents and young adults with cancer. In N. Publication (Series Ed.). Retrieved from Arendt, M., & Rosenberg, N. K. (2012). Kognitiv terapi. Nyeste udvikling. (Cognitive Theraphy. Newest Developement) København: Hans Reitzels Forlag. Austvoll-Dahlgren, A., Nøstberg, A. M., Stensbekk, A., & Vist, G. E. (2011). Effekt av gruppeundervisning i pasient- og pårørendeopplæring: en oppsummering av systematiske oversikter (The effect of group education for patients and next of kin). Report ,Vol. 9, ISBN: , Oslo: Nasjonalt kunnskapssenter for helsetjenesten Beck, A. T. (2005). The current state of cognitive therapy: A 40-year retrospective. Archives of General Psychiatry, 62(9), doi: /archpsyc Beck, J. S. (2006). Kognitiv terapi-teori,utøvelse og refleksjon. (Cognitive Theraphy -Theory, practice and reflections). Oslo, Norway: Norsk Akademisk Forlag. Bleyer, A., & Barr, R. (2009). Cancer in young adults 20 to 39 years of age: overview. Semin Oncol, 36(3), doi: /j.seminoncol Brearley, S. G., Stamataki, Z., Addington-Hall, J., Foster, C., Hodges, L., Jarrett, N., Amir, Z. (2011). The physical and practical problems experienced by cancer survivors: a rapid review and synthesis of the literature. Eur J Oncol Nurs, 15(3), doi: /j.ejon Buchmann, M. C., & Kriesi, I. (2011). Transition to Adulthood in Europe. Annual Review of Sociology, 37(1), doi: /annurev-soc Campos, M. P., Hassan, B. J., Riechelmann, R., & Del Giglio, A. (2011). Cancer-related fatigue: a practical review. Ann Oncol, 22(6), doi: /annonc/mdq458 Cancer Registry of Norway. (2014). Cancer in Norway Cancer incidence, mortality, survival and prevalence in Norway. Oslo: Cancer Registry of Norway. Creswell, J. W. (2007 ). Qualitative inquiry and research design: choosing among five traditions (2nd Ed ed.). London: Thousand Oaks, CA: Sage. Eichler, C., Pia, M., Sibylle, M., Sauerwald, A., Friedrich, W., & Warm, M. (2015). Cognitive behavioral therapy in breast cancer patients-a feasibility study of an 8 week intervention for tumor associated fatigue treatment. Asian Pac J Cancer Prev, 16(3), Faller, H., Schuler, M., Richard, M., Heckl, U., Weis, J., & Kuffner, R. (2013). Effects of psycho- oncologic interventions on emotional distress and quality of life in adult patients with cancer: systematic review and meta-analysis. J Clin Oncol, 31(6), doi: /JCO Fors, E. A., Bertheussen, G. F., Thune, I., Juvet, L. K., Elvsaas, I. K., Oldervoll, L., Leivseth, G. (2011). Psychosocial interventions as part of breast cancer rehabilitation programs? Results from a systematic review. Psychooncology, 20(9), doi: /pon.1844 ~ 42 ~
43 Gielissen, M. F. M., Verhagen, S., Witjes, J. A., & Bleijenberg, G. (2006). Positive effects of cognitive behaviour therapy (CBT) for fatigue in cancer survivors, a randomised controlled trial (RCT). Psycho-Oncology, 15(2), Hall, A. E., Boyes, A. W., Bowman, J., Walsh, R. A., James, E. L., & Girgis, A. (2012). Young adult cancer survivors' psychosocial well-being: a cross-sectional study assessing quality of life, unmet needs, and health behaviors. Support Care Cancer, 20(6), doi: /s x Hansen, H. P., & Tiornhoj-Thomsen, T. (2007). Cancer rehabilitation in Denmark: Stigmatization and normalization. Psycho-Oncology, 16(9), Harrington, C. B., Hansen, J. A., Moskowitz, M., Todd, B. L., & Feuerstein, M. (2010). It's Not over When It's Over: Long-Term Symptoms in Cancer Survivors - a Systematic Review. International Journal of Psychiatry in Medicine, 40(2), doi: /pm.40.2.c Hauken, M. A. (2014). The cancer treatment was only half the work. A mixed Method study of rehabilitation among young adult cancer survirvors. (PhD Article based), University of Bergen, University of Bergen. Retrieved from BORA database. Hauken, M. A., Larsen, T. M., & Holsen, I. (2013). Meeting reality: young adult cancer survivors' experiences of reentering everyday life after cancer treatment. Cancer Nurs, 36(5), doi: /NCC.0b013e318278d4fc Hersch, J., Juraskova, I., Price, M., & Mullan, B. (2009). Psychosocial interventions and quality of life in gynaecological cancer patients: a systematic review. Psychooncology, 18(8), doi: /pon.1443 Hofmann, S., Asnaani, A., Vonk, I. J., Sawyer, A., & Fang, A. (2012). The Efficacy of Cognitive Behavioral Therapy: A Review of Meta-analyses. Cognitive Therapy and Research, 36(5), doi: /s Institute of Medicine. (2013). Identifying and addressing the needs of adolescents and young adults with cancer: workshop summary. Retrieved from: doi: Johansen, C. (2007). Rehabilitation of cancer patients - research perspectives. Acta Oncol, 46(4), doi: / Juvet, L. K., Elvsaas, I. K., Leivseth, G., Anker, G., Bertheussen, G. F., Falkmer, U., Norderhaug, I.N. (Eds.). (2009). Rehabilitation of breast cancer patients: A systematic Review. Oslo: Norwegian Knowledge Centre for the Health Services. Keegan, T. H., Lichtensztajn, D. Y., Kato, I., Kent, E. E., Wu, X. C., West, M. M., Group, A. H. S. C. (2012). Unmet adolescent and young adult cancer survivors information and service needs: a population-based cancer registry study. J Cancer Surviv, 6(3), doi: /s Lebel, S., Maheu, C., Lefebvre, M., Secord, S., Courbasson, C., Singh, M., Catton, P. (2014).Addressing fear of cancer recurrence among women with cancer: a feasibility and preliminary outcome study. JOurnal of Cancer Survivorship, doi: /s Luknes, E. P., & McFarlane, W. (2004). Psychoeducation as evidence-based practice: considerations for practice, research, and policy. Brief Treatment and Crisis Intervention, 4(3), doi: /brief-treatment/mhh019 Malterud, K. (2011). Kvalitative metoder i medisinsk forskning: en innføring. (Qualitative methods in medical research: an introduction). Oslo: Universitetsforl. Malterud, K. (2012). Systematic text condensation: A strategy for qualitative analysis. Scandinavian Journal of Public Health, 40(8), doi: / ~ 43 ~
44 Mattson, M. R., Demshar, R. K., & Daly, B. J. (2013). Quality of life of young adult survivors of hematologic malignancies. Cancer Nurs, 36(2), 1-7. doi: /NCC.0b013e dd Osborn, R. L., Demoncada, A. C., & Feuerstein, M. (2006). Psychosocial interventions for depression, anxiety, and quality of life in cancer survivors: meta-analyses. Int J Psychiatry Med, 36(1), doi: /eufn-rv1k-y3tr-fk0l Parsons, H. M., Harlan, L. C., Lynch, C. F., Hamilton, A. S., Wu, X. C., Kato, I., Keegan, T. H. (2012). Impact of cancer on work and education among adolescent and young adult cancer survivors. J Clin Oncol, 30(19), doi: /JCO Sansom-Daly, U. M., Peate, M., Wakefield, C. E., Bryant, R. A., & Cohn, R. J. (2012). A systematic review of psychological interventions for adolescents and young adults living with chronic illness. Health Psychology, 31(3), doi: /a Sansom-Daly, U. M., Wakefield, C. E., Bryant, R. A., Butow, P., Sawyer, S., Patterson, P., Cohn, R. J. (2012). Online group-based cognitive-behavioural therapy for adolescents and young adults after cancer treatment: a multicenter randomised controlled trial of Recapture Life-AYA. BMC Cancer, 12, 339. doi: / Smith, A. W., Parsons, H. M., Kent, E. E., Bellizzi, K., Zebrack, B. J., Keel, G., AYA Group (2013). Unmet Support Service Needs and Health-Related Quality of Life among Adolescents and Young Adults with Cancer: The AYA HOPE Study. Front Oncol, 3, 75.doi: /fonc Speck, R. M., Courneya, K. S., Masse, L. C., Duval, S., & Schmitz, K. H. (2010). An update of controlled physical activity trials in cancer survivors: a systematic review and meta-analysis. J Cancer Surviv, 4(2), doi: /s Woodward, E., Jessop, M., Glaser, A., & Stark, D. (2011). Late effects in survivors of teenage and young adult cancer: does age matter? Ann Oncol, 22(12), doi: /annonc/mdr044 Zebrack, B. J. (2011). Psychological, social, and behavioral issues for young adults with cancer. Cancer, 117(10 Suppl), doi: /cncr ~ 44 ~
45 Efficacy of Social Skills Training among Persons with Schizophrenia Praful P. Kapse Development Officer Mental Health Initiative Sir Ratan Tata Trust Dr. B. P. Nirmala Associate Professor Department of Psychiatric Social Work National Institute of Mental Health and Neuro Sciences Bangaluru. Citation: Kapse PP & Nirmala BP. (2015) Efficacy of Social Skills Training among Persons with Schizophrenia. International Journal of Psychosocial Rehabilitation. Vol 20 (1) Abstract Background: Person with schizophrenia have the deterioration of personal, family, and social life. The illness leads to many disabilities in terms of interpersonal skills, communication skills, coping skills, dealing with emotions, self-care, self-control, occupational skills. Impairments in social functioning are among the most debilitating and treatment refractory aspects of schizophrenia (Bellack et al., 2007). Materials and Methods: The study aimed to know social skills deficits among persons with schizophrenia and to check the efficacy of the social skills training programme. A total number of 12 persons with schizophrenia, who were availing day care rehabilitation services, were selected randomly for the social skills training programme. The researcher adopted quasi experimental design without control, and interview and observer rating method used to collect data. Major Finding: Significant amount of deficits were found in self care, instrumental skills, communication skills, impulse control and social functions of the participants. The post social skills training programme there was significant improvement reported in social skills of the participants, repeated measures shows (F1.65,18.15)=93.26, p=26 significant level of change in social skills in post1 and post2 test. Conclusion: The present study reported the efficacy of social skills training in improving social skills among persons with schizophrenia who are availing day care rehabilitation facility. The model of social skills training programme were found to be effective and can be applied for larger practice in rehabilitation centres in India. Key Words: Social Skills Training, Schizophrenia, Rehabilitation ~ 45 ~
46 Introduction: It is perhaps commonplace to state to human being as social animals, nevertheless it is true. A substantial portion of human lives spent in interactions with one another moreover, the nature quality, and quantity of those interaction have a tremendous impact on behaviour, mood, and the adequacy of adjustment. Faulty interpersonal relationship patterns have unfailingly been associated with a wide variety of behavioural- psychological dysfunction ranging from simple loneliness to schizophrenia. Schizophrenia is a clinical syndrome of variable, but severely disruptive, the psychopathology which involves disturbance in cognition, emotion, perception, and other aspects of behaviour. The expression of these manifestations varies across patients and over time, however the effect of the illness is always stark and is usually long lasting. "Inexpressive faces, blank looks, monotone and monosyllabic speech, few gestures, seeming lack of interest in the world and other people, inability to feel pleasure or act spontaneously." An estimated 25% of people with schizophrenia have "the deficit syndrome", marked by "severe and persistent negative symptoms." These negative symptoms are related to the individuals inability to socialize, and are connected to the cognitive deficits seen in many patients. These negative symptoms are also the markers for any schizophrenia spectrum disorder (such as schizoptypal personality, and schizoid personality), as well as early markers for full schizophrenia prior to the first psychotic break. Not only are these negative symptoms common and detrimental, little is available for treatment. Most antipsychotic medications work mainly on positive symptoms, and patients with mostly negative symptoms are often deemed "treatment resistant". The term skills - in contrast to the term abilities implies that they are predominantly based on learning experiences. Thus, social skills training utilizes behaviour therapy principles and techniques for teaching individuals to communicate their emotions and requests so that they are more likely to achieve their goals and meet their needs for affiliative relationships and roles required for independent living. Social skills are interpersonal behaviours that are normative and/or socially sanctioned. They include such things as dress and behaviour codes, roles about what to say and not to say, and stylistic guidelines about the expression of affect, social reinforcement interpersonal distance and so on and so forth. Whether they have never learned social skills or have lost them, most people with schizophrenia have marked skill deficits. These deficits make it difficult for many clients to establish and maintain social relationship, to fulfil social roles or to have their needs met. In various studies social skills training has found moderately to strongly effective in increasing skill acquisition and reducing psychiatric symptoms. (Melody Nichols Dilk). Skills training are effective for virtually every area of role functioning for persons with severe psychiatric disabilities (Dion and Anthony 1987). Three models of social skills training, all of which involve role playing by the patient and modelling, prompting, feedback, and reinforcement by the therapist. Many patients can benefit from the basic training model. For patients functioning at a higher level, the problem-solving model provides general strategies for dealing with a variety of social situations. (Robert P. Liberman et al.1985). Despite of these many studies, there are very less number of studies found in Indian context. Beliefs and understanding of mental illness is itself a taboo in India. Persons with mental illness perceive as possessed by black magic and other supernatural powers, so the Stigma, discrimination, hostility is attached with person with mental illness. It often found that family mem- ~ 46 ~
47 bers and society is avoids the abilities of these population and does not give chance to their abilities. In this context the purpose of this study is to find out the effectiveness of social skills training among persons with schizophrenia availing day care rehabilitation services. Materials and Methods The study aimed to know social skills deficits among persons with schizophrenia and to check the efficacy of the social skills training programme. The objective stated for study was to study the socio-demographic profile of the participants. 1) To assess the social skills deficits among participants. 2) To design social skills training program to address social skills deficits. 3) To study the efficacy of social skills training program. For present study researcher hypothesized that there will be significant improvement in social skills of the participants who undergo social skills training A total number of 12 persons with schizophrenia, who were availing day care rehabilitation services, were selected randomly for the social skills training programme. The researcher adopted quasi experimental design without control. The interview and standardised instruments were used to collect data. Semi-structured interview schedule used to collect socio-demographic details of the participants, Social Adaptive Functioning Evaluation (SAFE) by Harvey et.al 1997 an observer rated scale used to measure social skills of the participants, Social Skills Checklist were used to check social behaviour and functioning over past month. Results Demographic Demographic results shows that majority of the participants (66.7%) belongs to age group of 31 to 40 years. Majority of the participants (83.3%) were male. Highest number of participants (33.3%) reported to studied up to high school and very few (16.7%) studied up to graduation and above. All the participants belong to Hindu religion. Majority of the participants (91.7%) were never married. And equal number of participants (41.7%) belongs to Nuclear and joint family. Social Skills Deficits Majority of the participants reported deficits in instrumental skills. Many of the respondents had difficulty in self care activities. 50% of the participants had moderate level of impairment in impulse control. Regarding conversation skills 66.7% participants had severe impairment. Majority of the participants reported deficits in social functions. Post Intervention Results Social skills training in current study the mean total score of the participants during pre, post1 and post2 were 38.33, 22, and 5.75 respectively pair wise comparison shows significant level change F = 93.26, p<0.01 and the social skills training reported effect size The study adopted repeated measures of ANOVA were obtained to see effects of intervention there was significant effect of social skills training on social adaptive functioning, F (1.65, 18.15) = 93.26, p=.05 These results show that there was significant change in social skills of participants after social skills training. The study also finds the improvement in social skills is significant at linear level (F=127.75,p<0.001) and quadratic trend found to be non-significant (F=0.001, p>0.05), which indicates the improvement in social skills at each post SST assessment. In the present study, the social skills training analysis shows that various skills have improved in the participants after social skills training. The efficacy can be seen from the differences in the means score, significant level and effect size. The social skills training effect on the various domain namely instrumental skills, self care, impulse control and social function shows significant improvement. There was a decreased mean score in these domains. The effect size shows a large effect on the above four domains. ~ 47 ~
48 Discussion In present study regarding socio-demographic profile of the participants following results were observed majority of the participants were in age group 31 to 40 years, majority of them were male, all participants belong to Hindu religion, majority of them were never married and equal number of participants was in nuclear and joint family. The similar age group were widely studied in other studies related to social skills. This could be because of adulthood in which persons from this age group are most expected to work and earn money so in this way majority of the participants were from this age group the similar studies (William H. et al, 2009) reported older adults with schizophrenia use more services than any other diagnostic elderly group within community mental health organizations (Bartels, Miles, Dain, & Smyer, 1996; Cuffel, Jeste, & Halpain, 1996).and male member accessing the treatment and other allied services is commonly seen in India, the cultural and socio-cultural beliefs may influence accessibility of the services. The present study intends to help in understanding the social skills deficits among persons with schizophrenia who are availing day care rehabilitation services. The present study shows among persons who are availing day care rehabilitation facility has significant level of social skills deficits in pre-training (M=38.33, SD=16.38). These deficits include instrumental and self care skills, impulse control, and social function skills. The similar level of deficits had been found widely (Harvey et al., 1997). In another study the prevalence of social skill deficits in schizophrenia was examined by comparing patients assessed over a 1 year period with a group of non-patient controls recruited from the community. Social skills were assessed using a role play test and were considered deficient when they were below the range of the control sample. Approximately 50% of the patients were consistently unskilled over the one year, whereas 11% were consistently skilled. Deficits in specific social skills were relative rare. Consistent deficits were present for only one of six specific skills 14% of the patients was consistently less appropriate in their conversation. (Kim T. Mueser et al., 1991) This finding found to be similar with current study, the deficits in conversational skills found significant (M = 2.53, SD =.79) which is high among other skills. A large amount of research studies have done regarding social skills training. Social skills training (SST) involves the use of standard behavioural skills training procedures to develop social competencies, and has been used for over three decades in an attempt to remediate poor social skills in schizophrenia patients (Halford & Hayes, 1991). Implicit in the use of SST is the assumption that poor social skills inhibit the development of supportive social networks and decrease patients coping with stressors, and consequently patient s quality of life & prognosis deteriorate (Anthony & Liberman, 1986; Trower, Brgent, & Argyle, 1978; Wallace, Boone, Donohue, & Foy, 1985). Consistent with this assumption low levels of social skills co vary with social isolation, and poor community functioning (Bellack et al. Halford & Hayes, 1995) The literature dealing with social skills training of schizophrenia patients indicates that topographical features and self-reports of anxiety and discomfort can be changed for the better functioning by social skills training. Unfortunately, these changes do not occur for every patient and, when they do occur, often do not generalize to new situations. Research must be directed to determining the interaction between patient characteristics and training procedures as they affect outcome. The scope of the procedures must also be expanded if meaningful changes in patients' quality of life are to be effected. (Charles J. Wallace, Connie J. Nelson, Robert Paul Liberman et al., 1980). In line of these finding current study adopts social skills training for persons with schizophrenia. Social skills training found to be effective in many previous studies, the efficacy of social skills training and day hospital treatment for 20 chronic schizophrenia patients in a 12-week day hospital program and 44 patients in the same program supplemented by comprehensive social skills training. Patient who completed treatment showed improvement immediately following treatment, during the six month post treatment they maintained gains ( Alan ~ 48 ~
49 S. Bellack, et al. 1984). In present study social skills training among schizophrenia patient found to be useful in improving overall social skills. The mean difference in pre-sst and post SST significantly shown improvement, pre SST overall (M = 38.33, SD = 16.38) which was considerably improved in post1 SST (M = 22, SD = 12.96) and further in post 2 SST shown significant improvement (M = 7.58, SD = 9.23). Similar significant improvement were reported in many studies in a study of twenty-eight schizophrenic male patients, diagnosed by the Present State Examination and Catego criteria, and from families high on expressed emotion, were randomly assigned to either intensive social skills training or holistic health therapy. A multidimensional evaluation was conducted before and after 9 weeks of inpatient treatment and for 24 months in the community. Patients exposed to social skills training evidenced significantly greater acquisition, generalization, and durability of social skills and their social adjustment in the community was rated as better by significant others; and they experienced fewer relapses and rehospitalisation (Charles J Wallace et al., 2002). Efficacy of Social Skills In line of the searching efficacy of social skills training in current study the mean total score of the participants during pre, post1 and post2 were 38.33, 22, and 5.75 respectively pair wise comparison shows significant level change F = 93.26, p<0.01 and the social skills training reported effect size Which is large effect among previous similar other studies. For between-group studies, the overall effect size was medium at post test (d. =.40, n = 58, z = 9.18, p <.001) and large at follow-up (d =.56, n = 14, z = 5.34, p <.01). For within-group studies, the overall effect size was also medium at post test (d. =.48, n = 9, z = 7.59, p <.01), but small at follow up (d. =.30, n = 4, z = 2.37, p <.05). Thus, the overall post test effect size for the within-group studies was similar to that for the between-group studies, whereas the overall follow-up effect size was smaller for the within-group studies than the corresponding statistic for the between-group studies. The study adopted repeated measures of ANOVA were obtained to see effects of intervention there was significant effect of social skills training on social adaptive functioning, F (1.65, 18.15) = 93.26, p=.05 These results show that there was significant change in social skills of participants after social skills training. The study also finds the improvement in social skills is significant at linear level (F=127.75,p<0.001) and quadratic trend found to be non-significant (F=0.001, p>0.05). Which indicates the improvement in social skills at each post SST assessment. Conclusion Efficacy of social skills training among persons with schizophrenia was studied in present study. The social skills deficits have been widely found to be obstacle in recovery of persons with mental illness. Many individuals with schizophrenia gradually develop isolated lives, punctuated by lengthy periods in psychiatric hospitals or in community residence. Such events remove clients from their normal peer group, provide few opportunities to engage in appropriate social roles, and limit social contacts to mental health staff and other severely ill clients. Under such circumstances, clients do not have an opportunity to acquire and practice appropriate adult roles. Moreover, skills mastered earlier in life may be lost because of disuse or lack of reinforcement by the environment. Several studies have reported social skills deficits interfere with the development of appropriate social relationship and the acquisition of social skills. Schizophrenia often strikes first in late adolescence or young adulthood, a critical period for mastery of adult social roles and skills, such as dating and sexual behaviours, work related skills, and the ability to form and maintain adult relationships. (Bellack & Muser, 1993) The present study was reported the efficacy of social skills training in improving social skills among persons with schizophrenia who are availing day care rehabilitation facility. Several similar studies also widely reported the efficacy of social skills training (Benton et al., 1990).The model of social skills training programme were found to be effective and can be applied for larger practice in rehabilitation centres in India. ~ 49 ~
50 References Alan, S. B., & Michel, H., (1979). Research and Practice in Social Skills Training. Plenum Press. New York and London. Anderson, J. R. (1982). Acquisition of cognitive skill. Psychological Review, 89, Anthony,W. A. & Liberman,R. P. (1986). The practice of psychiatric rehabilitation: Historical, conceptual and research base. Schizophrenia Bulletin, 12, Alan. S. B., Samuel, M. T., Michel, H., & Raymond, F. L. (1984). An Examination of the efficacy of social skills training for chronic schizophrenic patients. Hospital Community Psychiatry, 35, Bellack, A. S., Mueser, K. T., Wade, J. H., Sayers, S. L., & Morrison, R. L., (1992). The ability of schizophrenics to perceive and cope with negative affect. British Journal of Psychiatry, 160, Bellack, A. S., & Mueser, K. T. (1993). Psychosocial treatment for schizophrenia. Schizophrenia Bulletin, 19, Charles, J. W., Connie, J. N., Robert, P. L., Robert, A. A., David, L., John, P. E. & Chris, F., (1980). A Review and critique of social skills training with schizophrenic patients. Schizophrenia Bulletin, 6(1), Dion, G. L., and Anthony, W. A. (1987). Research in psychiatric Rehabilitation: A review of experimental and quasi-experimental studies. Rehabilitation Counseling Bulletin, 30, DiSisto, M. J., Harding, C.M., McCormick, R.V., Ashikaga, T., & Brooks, G.W., (1995). The Maine and Vermont threedecade studies of serious mental illness: II Longitudinal course comparison. British Journal of Psychiatry, 167, Saraswat, N., Rao K., Subbakrishna, D. K., & Gangadhar, B. N., (2006). The social occupational functioning scale: A brief measure of functional status in persons with schizophrenia. Schizophrenia Research, 81, Lehman, A. F. (1995). Vocational rehabilitation in schizophrenia. Schizophrenia Bulletin 21, Liberman RP, Kopelowicz A. (1994) Recovery from schizophrenia: Is the time right? The Journal of the California Alliance for the Mentally Ill 5(3), 67-69, Louise, H., Priya, D. G. & Gareth, D. (2007).Mental health nurses experiences of schizophrenia rehabilitation in China and India: A preliminary study. International Journal of Mental Health Nursing, 16(1), Strauss, J. S. & Carpenter, W.T., (1977). Prediction of outcome in schizophrenia: III. Five year outcome and its predictors. Archives of General Psychiatry, 34 (2), Takahashi, M., and Kosaka, K. (2003). Efficacy of open-system social skills training in inpatients with mood, neurotic and eating disorders. Psychiatry and clinical neurosciences, 57(3), ~ 50 ~
51 Empathy in Psychosocial Intervention: a theoretical overview *Selwyn Stanley, PhD Senior Lecturer in Social Work Faculty of Education, Health & Wellbeing University of Wolverhampton, UK *Corresponding author selwyn.stanley@wlv.ac.uk & V. Sethuramalingam, PhD Professor of Social Work Bharathidasan University Tiruchirappalli, India Citation: Stanley V. & Sethuramalingam V. (2015) Empathy in Psychosocial Intervention: a theoretical overview International Journal of Psychosocial Rehabilitation. Vol 20 (1) Abstract Empathy is a concept that is found in the lexicon of many of the helping professions be it medicine, nursing, education or social work to name a few. It is a key element that determines professional competence and considered necessary for effective relationship based practice. Almost all training programs within the helping professions strive to incorporate this ability within the skills repertoire of budding professionals. Empathy is not a new concept in practice and reference to it can be traced to the writings of early case workers. It has been considered to be vital in building trust and developing a relationship that will foster growth and change (Pinderhughes, 1979). Carl Roger s person centred approach envisages empathy to be one of the core conditions of the positive, purposeful and professional relationship that practitioners strive to establish with clients. Empathy enables one to see external events through the client s eye lens and thus provides a near accurate subjective perception of distressful environmental stressors and the realities of the client s life situation. This is important to understand how oppression is experienced by the other if one wants to help alleviate distress. Key tasks of capacity building, resource mobilisation and conscientization would only be possible if the practitioner has a near-accurate perception of the client s life scenario. While empathy is certainly a virtue in helping, there are also dangers associated with boundary cross over, an issue that practitioners need to be cautious about. ~ 51 ~
52 This paper looks at the nature, structure and types of empathy and examines its importance in psychosocial intervention. It explores its links with establishing rapport with clients, to resilience, social justice and empowerment; concepts which are of central concern to a psychosocial approach. Finally it discusses barriers in the manifestation of empathy and its relationship to compassion fatigue and burnout. Key words: Psychosocial intervention, Social Justice, Resilience, Empowerment, Self, Professional Boundaries, Professional Relationships, Burnout, Compassion Empathy in Psychosocial Intervention: a theoretical overview No one cares how much you know, until they know how much you care Theodore Roosevelt Introduction: Psychosocial interventions are non-pharmacological therapeutic interventions which address the psychological, social, personal, relational and vocational problems of people. These interventions draw techniques from cognitive behavioural therapies (CBT) and educational theories and are used for instance with people having mental health problems, substance misuse issues, HIV/AIDS, interpersonal adjustment difficulties and a host of other such issues. Empathy is a key ingredient in approaches that seek to understand people and their life situation. It refers to the ability to understand others by imagining what it might feel like to be them; how it might feel to experience the world by being in their shoes or from within their skin. Dymond (1949), one of the earliest writers to define empathy, refers to it as the imaginative transposing of oneself into the thinking, feeling, and acting of another and so structuring the world as he does. Empathy toward others enhances emotional well-being, interpersonal relationships, and life success (Mehrabian, 1996). Empathy is also claimed to be central in promoting pro-social behaviour through increasing positive, helping and thoughtful actions (Natale & Sora, 2010). In fact, it is seen as the glue that holds society together, the capacity without which humans would not have evolved (Fuchsman, 2015). Empathy: its nature and structure Empathy is the act of perceiving, understanding, experiencing and responding to the emotional state and ideas of another person (Barker, 2003). While it is possible to understand another person without feeling with him, true empathic skill includes the capacity for an emotional response (Shantz, 1975). Rogers explains empathy as sensing the client's private world as if it were your own, but without ever losing the 'as if' quality (Rogers, 1957). This implies that though the practitioner strives for a near accurate perception of the client s inner world, he does so without losing his own objectivity and in this sense brings to his perception a degree of detachment. Truax (1967) states it is not necessary- indeed it would seem undesirable-for the therapist to share the client s feelings in any sense that would require the therapist to feel the same emotions that the client feels. According to Cooper (1970) the practitioner temporarily feels at one with the object while maintaining his individuality. Empathy has been described as vicarious introspection (Kohut, 1959). This implies that the practitioner penetrates the inner world of the client while simultaneously reflecting on the feelings that this transposition evokes in him. Empathy has been conceived variously by different authors; to be a dispositional trait or personality attribute (Martin & Clark, 1982), a situation-specific cognitive-affective state (Duan & Hill, 1996), as a facilitative communication skill (Carkhuff, 1969) and as a interpersonal and experiential process (Barrett-Lennard, 1981). ~ 52 ~
53 Zaki & Ochsner (2012) hold that empathy comprises of two related but distinct processes through which perceivers (individuals focusing on another person s internal states) relate to targets (individuals who are the focus of perceivers attention). They have grouped the processes that underlie empathy into three broad classes depicted in Figure 1 alongside some allied terms from the literature. The three classes include (i) experience sharing: vicarious sharing of targets internal states (Gallese, Keysers & Rizzolatti, 2004). (ii) mentalizing: explicitly considering (and perhaps understanding) targets mental states and their sources (Leslie, Friedman & German, 2004) and (iii) prosocial concern: expressing motivation to improve targets experiences (for example, by reducing their suffering) (Batson, 2011). Empathy has been considered to include two basic components: the affective component or the matching of affective experience between a participant and a target individual; and the cognitive component, which is concerned with the ability to take the perspective of others (Lian & Lieberman, 2009). ~ 53 ~
54 Empathy: a framework A framework to understand empathy in social work practice envisages two primary domains viz. affective and cognitive and together lead to behavioural expressions (King, 2011). These three dimensions are broken down into six underlying constructs drawn from the extant literature (Figure 1). The affective dimension includes the constructs of caring and congruence. Professional caring is a form of interpersonal communication whereby one applies the content and principles of a specified knowledge area (e.g., counselling) within the context of a professional relationship for the purpose of rendering a service designed to improve the human condition (Knowlden, 1998). Congruence was proposed as a core condition by Rogers and refers to being open, non-judgemental and honest within the helping relationship (King, 2011). The cognitive dimension of empathy involves IS, intellectual flexibility, and openness to understanding the experiences and taking the perspectives of another. The second construct of cognition, perspective taking, is the ability to accurately perceive another s point of view (Davis, 1980). This involves the internal and cognitive interpretation and understanding of another s mental and emotional state. Behavioural manifestations of empathy involve interpersonal motivations and actions and they demonstrate functional aspects of empathy and its concrete applications within helping relationships. Altruism and the therapeutic relationship are the two constructs within the behavioural dimension. Altruism has been defined as a motivation to benefit others by Batson (2002) and as an action where the goal is to benefit others without any expectation of reward or benefit in return (Monroe, 2002). Empathy versus sympathy and compassion The terms compassion, empathy, altruism, and other similar terms (connectedness, compassionate love, agape) have sometimes been used interchangeably, but refer to somewhat different but possibly over lapping phenomena (Monroe, 2002). Sympathy is important in human relationships as an expression of concern or sorrow about distressful events in a person's life (Monroe, 2002). Through the consideration of four comparative dimensions in the ~ 54 ~
55 counselling experience--aim, appraisal, apprehension, and agreement, empathy has been distinguished from sympathy (Meier & Davis, 2008). In terms of aim, the primary intent in employing empathy is to express understanding of a client (Clark, 2010), whereas a sympathetic response has the more circumscribed function of expressing compassion for an individual's distressful condition or situation (Eisenberg, 2000). From the point of appraisal, empathy entails attunement with a client's feelings and meanings (Pearson, 1999) while sympathy is a reaction to a client's distress that becomes manifest in mild to intense expressions of feelings of sorrow for an individual s plight (Gribble & Oliver, 1973). In terms of apprehension, a deeper way of knowing an individual is more likely to occur when a practitioner attempts to empathically understand a client from multiple perspectives (Switankowsky, 2000). For instance, through their identification and imaginative capacities practitioners can subjectively apprehend what clients are experiencing. In contrast, when expressing sympathy it is not necessary to "enter into" a client's experiencing or to have a deeper knowledge of the person and it is possible only to have a general understanding of a client's plight and still be able to be sympathetic (Clark, 2010). Finally in terms of agreement, accurate and appropriate use of empathy involves expressing an empathic understanding without implying agreement with the client. In contrast, in expressing compassion and commiseration, it is possible to sympathetically convey agreement with the views and perspectives of a client (Gribble & Oliver, 1973). Sympathy may carry connotations of looking down on somebody and pitying them for the plight they are in and may distort the egalitarian nature of the relationship which practitioners strive to establish. Compassion is considered to be more active than empathy in the sense that it involves a tendency for action. Lilius et al. identify three elements of compassion, noticing another person s suffering, empathically feeling that person s pain, and acting in a manner intended to ease their suffering (Egan, 2010). The connection to suffering is seen in theoretical and empirical analyses of compassion and this is also common to empathy as well as altruism (Lilius, et al., 2008). Common to the concepts of empathy, altruism and compassion is the importance placed on the replacing of selfconcern with concern for others and expressing empathy, as opposed to sympathy, is more objective and accurate, intellectual rather than emotional, altruistic, requires more effort but conserves energy, has more positive effects on the clinician (such as personal growth and career satisfaction), and leads to better patient health outcomes (Martins et al., 2013). Relationship in psychosocial intervention The therapeutic relationship is the medium which facilitates exploration of issues, provides hope and nurturance and is the channel through which strategies for intervention are introduced. The nature and quality of the therapeutic relationship has been established as an important variable in determining outcome (Ardito & Rabellino, 2011). It has been acknowledged that client growth depends on the qualities of the helping alliance, and this is a defining variable of the profession (Biestek, 1957). A productive helping alliance is one in which a helper is accepting, nonjudgmental, supportive, and empathic (Lambert & Barley, 2002). Empathy is envisaged to be essential in building trust and developing a relationship that will foster growth and change (Pinderhughes, 1979). Effective practice depends on the interpersonal and empathic skills of the practitioner (Turner, 2009). Empathy is central with regard to the personality of the therapist as well as being important for skilful therapeutic communication (Duan & Hill, 1996). Empathic responses in the helping process bring benefit to both actors in the relationship. It conveys to the client that the professional is there not only listening to him but with him in terms of understanding his perceptions of distress. Empathy may, in itself, have a therapeutic effect, may contribute to relieving patients distress, and may contribute to the deepening of the therapeutic bond (Jurkovitch, Pananen & Rivara, 2000). It has been found to have strong positive therapeutic effects on service users physical, mental and social well-being (Morrison, 2007). It also conveys to the client a sense that he is not alone in dealing with his difficult circumstances and that there is a concerned other who is keen to enable him deal with his situation. Empathic responses strengthen relationship with the client, breaking down defensive behaviours and enlisting client participation in the process. It provides a medium ~ 55 ~
56 for the practitioner to demonstrate concern, offer reassurance and to sustain client engagement. It thus also becomes an important tool with which to collect accurate information from the client which would then enable the formulation of a holistic assessment and potentially lead to effective strategies of intervention. Empirical evidence points to empathy being an important tool for positive therapeutic intervention (Watson, 2002). Empathy has been identified as the single most consistent condition of a productive therapeutic relationship in outcome research (Sinclair & Monk, 2005). Empathy and the self Self-awareness plays a key role in empathic experience as one becomes aware of the feelings and emotional state of others in relation to one s own emotional disposition. There are two view points within the literature on this relational perspective. The first considers empathy as being a result of identification that blurs the distinction between the self and the other (Lerner, 1980). Empathy does not simply entail the matching of feelings, but the adoption of feelings that are more congruent with the other s situation than with one s own (Hoffman, 2000). The second view point considers empathy to result from a self-other distinctness as it allows one to recognise the particularity and uniqueness of the other (Batson, et al., 1997). It would appear that while both experiences relating to the self are different vis-à-vis the manifestation of empathy, they are both important in the context of professional relationships. The astute practitioner would attempt to get as close to the client s inner world as possible while at the same time maintaining an emotional distance. The latter is important to preserve one s own well-being and to prevent compassion fatigue and burn out. Four empathic behaviours characterise the expression of empathy (Keefe, 1976). The first requires perceiving accurately the client's gestalt. The second involves allowing a direct feeling response to arise. Third the practitioner needs to keep distorting cognitive processes in abeyance, and finally an ability to separate one s own feelings from those shared with the client. Accurate and appropriate feedback needs to complement these processes and the professional needs to convey his understanding of the client s state back to him with sensitivity and in a non-hurtful manner. Empathic behaviour requires the worker to be receptive and to transmit accurately to the client his awareness of the client's state of being. Empathy in students has been found to have a positive correlation with self-awareness (Stanley & Bhuvaneswari, 2016a) Resilience Resilience refers to positive adaptation, or the ability to maintain or regain mental health, despite experiencing adversity (Wald et al., 2006). The nature of psychosocial intervention requires practitioners to be high on resilience in order to be able to often deal with elevated levels of distress that is often manifest in their clients, which is likely to have adverse implications for their own mental health and well-being. Resilience has the potential to buffer the negative impact of work stress, especially in challenging working environments (Howard, 2008). In this sense resilience is a particularly important quality for practitioners, as it may help them adapt positively to stressful situations and enhance their professional growth (Howe, 2008). A study of trainee student social workers found that empathetic concern (feelings of warmth, compassion and sympathy) enhanced stress resilience and that empathetic distress (anxiety and discomfort that result from observing another s negative experience) may diminish it (Kinman & Grant, 2011). A study from India shows that entrants to the social work degree and those in the final year of their course experience more stress and anxiety when compared to students in the second year (Stanley & Bhuvaneswari, 2016b). These studies emphasise the importance of building resilience in students training to serve the helping professions. It is thus important that practitioners develop clear emotional boundaries to ensure that healthy empathetic concern does not spill over into empathetic distress, which is likely to have negative implications for clients as well as themselves. Compassion fatigue and Burnout Compassion fatigue refers to the negative consequences of working with traumatized clients and vicariously experiencing the effects of their traumatic life events (Harr & Moore, 2011). It tends to occur as a result of exposure ~ 56 ~
57 to client suffering and can be complicated by a lack of support at work or at home (Figley, 1995). It may also be caused by the moral stress or distress caused by the need to resolve ethical and value conflicts in practice that are often encountered when dealing with clients (Forster, 2009). Empathy for clients may contribute to the risk of compassion fatigue among experienced professionals and it may pose an even greater threat to inexperienced students who initiate their practice during field placement without the benefit of the mediating factors of practice wisdom and experience (Harr & Moore, 2011). Compassion fatigue can result in the caregiver experiencing a reduced capacity for or interest in being empathic (Adams, Boscarino & Figley, 2006). The use of self/otherawareness, emotion regulation, and perspective-taking skills maximize resiliency and allow for empathic engagement with clients that minimizes aversive responses such as compassion fatigue or secondary trauma (Thomas & Otis, 2010). It is important to distinguish between burnout and compassion fatigue while recognizing that they may share similar symptoms (Harr & Moore, 2011). Burnout is defined as a psychological syndrome of emotional exhaustion, depersonalisation and reduced personal accomplishment that occurs among individuals who work with other people, particularly in conflicting or otherwise critical situations (Maslach & Schaufeli, 1993). Affective sharing is crucial in all the helping professions, but as documented in the literature, can also lead to emotional and physical burnout (Eisenberg, 2000). Burnout is not limited to those who work with the traumatized and tends to occur over a prolonged period of time and can be caused by conflict between individual and organizational demands, an overload of responsibilities, a sense of being denied decision-making input, little financial reward and positive recognition, lack of status or respect in the workplace, lack of job fulfilment, or reduced sense of accomplishment and achievement (Harr & Moore, 2011). Compassion fatigue may be treatable, while burnout may result in the necessity of a job or career change (Sabin-Farrell, & Turpin, 2003). A practitioner who cannot turn off the empathic awareness of a client s despair or anxiety after the workday, may experience emotional burnout (Gerdes & Segal, 2011). The high levels of stress and burnout experienced by social workers have been found to contribute to the growing retention problems within the profession (Kinman & Grant (2011). Social empathy: links to social justice and empowerment Psychosocial approaches often focus on the alleviation of needs and mobilisation of resources for marginalised and vulnerable individuals and groups and this requires an empathic understanding of their life situation, needs and priorities. Social empathy is the ability to understand people by perceiving or experiencing their life situations and as a result gain insight into structural inequalities and disparities (Segal, 2011). It is thus an extension of empathy to larger social groups which are vulnerable and exposed to oppressive experiences owing to structural inequities or negative attitudes directed towards them by the majority. An appreciation of difference and diversity and minority experiences would be facilitated through the promotion of social empathy. This then is a prerequisite if practitioners have to engage with advocacy, rights campaigns and social action on behalf of these groups to initiate social change. Empathy is an important contributor in strengthening social interaction through its ability to motivate individuals to cooperate, to share resources and to help others (Van Lange, 2008). Social empathy has been conceived to be a combination of self-reflection and an accurate perspective or understanding of the underlying causes of social problems that can potentially lead to empathic action to improve societal well-being (Segal, 2011). Social empathy promotes not only a tolerance of people and their diverse cultures but also a more deep seated acceptance and non-judgemental attitude towards their uniqueness, all of which are values cherished by the helping professions. Thus stigma towards particular social groups, their behaviour and other associated atypical features and the social alienation experienced by them can be reduced to a large extent. A social empathic perspective from a macro-context can enable the development of services and policies that are socially and economically just, sensitive to people s needs, and based on the realities of actual situations (Gerdes, 2011) and can thus enable a non-discriminatory approach to promote the welfare of the marginalised. ~ 57 ~
58 Barriers to empathy Cognitive distortion includes stereotyping, making value judgments, or analysing perceptions according to a fixed theoretical schema can interfere with a practitioner s ability to empathise with others (Keefe, 1976). A belief in the superiority of the professional self and the I am the expert complex and a fear of letting go some degree of power could be a barrier that prevents practitioners from entering into honest, open and egalitarian relationships with clients. The fear of over identification and the caution exercised in maintaining rigid professional boundaries could also interfere with the establishment of spontaneous and genuine relationships and limit the experience of empathy. A moralistic perspective on social issues about what is right and appropriate could limit acceptance of the other and curtail the expression of genuine empathy. Other external barriers such as high case loads and the pressure of time, resource constraints, work place frustrations and an increasingly bureaucratic ethos are some external factors that could undermine practitioners ability to empathise. Cultural, racial, ethnic and socio-economic differences can also contribute to the gulf between the professional and the client. In the context of medical education, some barriers to empathic practice are owing to lack of appropriate role models, failing to teach empathy as a cognitive skill, negative experiences, time pressures and an overreliance on technology (Hojat et al., 2009). Conclusion Empathy clearly is perhaps one of the most important skills that psychosocial workers bring to their relationship with clients. Judicious use of empathy is mutually beneficial to both client and practitioner and quintessential in furthering the helping process. Education programs need to ensure that training goes beyond theoretical orientation to empathy, to ensure that skill inculcation activities are used to incorporate this vital aspect in the repertoire of budding professionals. The importance of helping students to develop their emotion management and social skills in order to enhance well-being and protect them against professional burnout has been highlighted. In conclusion, it is appropriate to quote Pink (2006) who says that sometimes we need detachment (objectivity); many other times we need attunement (receptivity) and the people who will thrive will be those who can toggle between the two. References Adams, R.E., Boscarino, J.A., & Figley, C.R. (2006). Compassion Fatigue and Psychological Distress Among Social Workers: A Validation Study. American Journal of Orthopsychiatry, 76, 1, Ardito, R.B., & Rabellino, D. (2011). Therapeutic Alliance and Outcome of Psychotherapy: Historical Excursus, Measurements, and Prospects for Research. Frontiers in Psychology, 2, Barker, R.L. (2003).The social work dictionary. 5th ed. Washington, DC: NASW Press. Barrett-Lennard, G.T. (1981). The empathy cycle: refinement of a nuclear concept. Journal of Counselling Psychology, 28, Batson, C.D. (2011). Altruism in Humans. Oxford Univ. Press, New York. Batson, C. D. (2002). Addressing the Altruism Question Experimentally, in Altruism and Altruistic Love: Science, Philosophy, and Religion in Dialogue, ed. S. G. Post, L. G. Underwood, J. P. Schloss, and W. B. Hurlbut, New York: Oxford Univ. Press, pp Batson, D. C., Sager, K., Garst, E., Kang, M., Rubchinsky, K., & Dawson, K. (1997). Is empathy-induced helping due to self ~ 58 ~
59 other merging? Journal of Personality and Social Psychology, 73, Biestek, F.P. (1957) The Casework Relationship. (Chicago: Loyola University Press). Carkhuff, R. R. (1969). Helping and Human Relations (Vols. 1 and 2), New York: Holt Rinehart and Winston. Clark, A. (2010). Empathy and Sympathy: Therapeutic Distinctions in Counseling. Journal of Mental Health Counseling, 32, 2, Cooper, L. (1970). Empathy: A developmental model, Journal of Neruotic and Mental Diseases, 154, Davis, H. M. (1980). A multidimensional approach to individual differences in empathy. JSAS Catalog of Selected Documents in Psychology, 10, 85. Duan, C., & Hill, C. E., (1996). The current state of empathy research. Journal of Counseling Psychology, 43, Dymond, R.F. (1949). The measurement of empathic ability. Journal of Consulting Psychology, 13, Egan, G. (2010). The skilled helper: A problem-management and opportunity-development approach to helping (9th ed.), Belmont, CA: Thompson Brooks/Cole. Eisenberg, N. (2000) Empathy and sympathy, in Handbook of emotions (2nd ed.), edited by M. Lewis & J. M. Haviland-Jones, New York: Guilford Press, pp Figley, C. (1995) ed., Compassion fatigue: Coping with secondary traumatic stress disorder in those who treat the traumatized. New York, NY: Brunner/Mazel. Forster, D. (2009). Rethinking compassion fatigue as moral stress. Journal of Ethics in Mental Health, 4, 1 4. Fuchsman, K. (2015). Empathy and Humanity. Journal of Psychohistory, 42, 3, Gallese, V., Keysers, C. & Rizzolatti, G. (2004). A unifying view of the basis of social cognition. Trends in Cognitive Science, 8, Gerdes, K.E. (2011) Introduction: 21st-Century Conceptualizations of Empathy: Implications for Social Work Practice and Research. Journal of Social Service Research, 37, Gerdes, K.E., & Segal, E. (2011). Importance of Empathy for Social Work Practice: Integrating New Science. Social Work 56, Gribble, J., & Oliver, G. (1973). Empathy and education. Studies in Philosophy, and Education, 8, Harr, C., & Moore, B. (2011). Compassion Fatigue Among Social Work Students in Field Placements. Journal of Teaching in Social Work, 31, Hoffman, L. M. (2000). Empathy and moral development: Implications for caring and justice. London: Cambridge University Press. Hojat, M., Vergare, M.J., Maxwell, K., Brainard, G., Herrine, S.K., Isenberg, G.A., Veloski, J., & Gonnella, J.S. (2009).The devil is in the third year: a longitudinal study of erosion of empathy in medical school. Academic Medicine, 84, 9, doi: /ACM.0b013e3181b17e55. Howard, F. (2008). Managing stress or enhancing wellbeing? Positive psychology s contributions to clinical supervision. Australian Psychologist, 43, ~ 59 ~
60 Howe, D. (2008). The Emotionally Intelligent Social Worker. London: Palgrave McMillan. Jurkovich, G.J., Pierce, B., Pananen, L., & Rivara, F. P. (2000). Giving bad news: the family perspective. Journal of Trauma, 48, 5, Keefe, T. (1976). Empathy: the critical skill. Social Work, 21, H King Jr. S. H. (2011). The Structure of Empathy in Social Work Practice, Journal of Human Behavior in the Social Environment, 21, Kinman, G., & Grant, L. (2011). Exploring Stress Resilience in Trainee Social Workers: The Role of Emotional and Social Competencies. British Journal of Social Work, 41, Knowlden, V. (1998). The communication of caring in nursing. Indianapolis, IN: Center Nursing Press. Kohut, H. (1959). Introspection, empathy, and psychoanalysis: An examination of the relationship between mode of observation and theory. Journal of the American Psychoanalytic Association, 7, Lambert, M.J., & Barley, D.E. (2002). Research summary on the therapeutic relationship and psychotherapy outcome, in Psychotherapy relationships that work: Therapist contributions and responsiveness to patients, ed. J. C. Norcross. New York, NY: Oxford University Press, pp Lerner, M.J. (1980). The Belief in a Just World: A Fundamental Delusion. New York: Plenum. Leslie, A.M., Friedman, O. & German, T.P. (2004). Core mechanisms in theory of mind. Trends in Cognitive Science, 8, Lian, R. T. & Lieberman, M.D. (2009). Empathy: A Social Cognitive Neuroscience Approach. Social and Personality Psychology Compass, 3, Lilius,J.M., Worline, M.C., Maitlis, S., Kanov,J., Dutton, J.E., & Frost, P. (2008). Contours of compassion at work, Journal of Organizational Behavior, 29, Martin, G. B., & Clark, R. D. (1982). Distress crying in neonates: Species and peer specificity. Developmental Psychology, 18, 3-9. Martins, D.N., Nicholas, N.A., Shaheen, M., Jones, L., & Keith Norris, K. (2013). The Development and evaluation of a compassion scale. Journal of Health Care for the Poor and Underserved, 24, Maslach, C., & Schaufeli, W.B. (1993) Historical and conceptual development of burnout, in Professional Burnout: Recent Developments in Theory and Research, ed. Schaufeli W.B., Maslach C. and Marek T. Washington, DC: Taylor & Francis, pp Mehrabian, A. (1996). Manual for the Balanced Emotional Empathy Scale (BEES). Available from Albert Mehrabian, 1130 Alta Mesa Road, Monterey, CA 93040, Meier, S. T., & Davis, S. R. (2008).The elements of counseling (6th ed.). Belmont, CA: Brooks/Cole, Cengage Learning. Monroe, K. R. (2002). Explicating Altruism, in Altruism and Altruistic Love: Science, Philosophy,and Religion in Dialogue, ed. S. G. Post, L. G. Underwood, J. P. Schloss, and W. B. Hurlbut. New York: Oxford Univ. Press. Pp Morrison, T. (2007). Emotional intelligence, emotion and social work: Context, characteristics, complications and contribution. British Journal of Social Work, 37, Natale, S.M., & Sora, A. (2010) Ethics in strategic thinking: Business processes and the global market collapse, Journal of ~ 60 ~
61 Business Ethics, 94, Pearson, Q. M. (1999). Integrative empathy: Training counselors to listen with a theoretical ear. Journal of Humanistic Counseling, Education and Development, 38, Pinderhughes, E.B. (1979). Teaching empathy in crosscultural social work. Social Work, 24, Pink, D. H. (2006). A whole new mind: why right brainers will rule the future. New York, NY: Riverhead books. Rogers, C.R. (1957). The necessary and sufficient conditions of therapeutic personality change. Journal of Consulting Psychology, 21, Sabin-Farrell, R. & Turpin, G. (2003). Vicarious traumatization: Implications for the mental health of health workers? Clinical Psychology Review, 23, Segal, E. A. (2011). Social Empathy: A Model Built on Empathy, Contextual Understanding, and Social Responsibility That Promotes Social Justice. Journal of Social Service Research, 37, Shantz, C.U. (1975). The development of social cognition, in Review of child development research, vol. 5, ed. E. M. Hetherington. Chicago: Chicago Univ. Press. Sinclair, S.L., & Monk, G. (2005). Discursive empathy: A new foundation for therapeutic practice. British Journal of Guidance & Counseling, 33, Stanley, S., & Bhuvaneswari, G.M. (2016a): Reflective ability, empathy, and emotional intelligence in undergraduate social work students: a cross-sectional study from India, Social Work Education, DOI: / Stanley, S., & Bhuvaneswari, G.M. (2016b). Stress, Anxiety, Resilience and Coping in Social Work Students (A Study from India), Social Work Education, 35, 1, DOI: / Switankowsky, I. (2000). Sympathy and empathy. Philosophy Today, 44, Thomas, J.T., & Otis, M.D. (2010). Intrapsychic correlates of professional quality of life: Mindfulness, empathy, and emotional separation. Journal of the Society for Social Work and Research, 1, Truax, C.B. (1967). A scale for the rating of accurate empathy, in The therapeutic relationship and its impact, ed. C. R. Rogers, Westport, CT: Greenwood, pp Turner, K. (2009). Mindfulness: The present moment in clinical social work. Clinical Social Work Journal, 37, Van Lange, P. (2008). Does empathy trigger only altruistic motivation? How about selflessness or justice? Emotion, 8, Wald, J., Taylor, S., Asmundson, G.J.G., Jang, K.L., Stapleton, J. (2006). Literature review of concepts: psychological resiliency. British Columbia Univ., Vancouver. 134p. Report: DRDC-CR Watson, J.C. (2002 ). Re-visioning empathy, in Humanistic psychotherapies: Handbook of research and practice, edited by D. J. Cain and J. Seeman. Washington, DC: American Psychological Association, pp Zaki, J. & Ochsner, K.N. (2012). The neuroscience of empathy: progress, pitfalls and promise. Nature and Neuroscience, 15, 5, ~ 61 ~
62 Notes in Tune: Arts-based Therapy (ABT) at Schizophrenia Awareness Association in Pune, India Aanand Chabukswar World Centre for Creative Learning (WCCL) Foundation 2015 Citation: Chabukswar A. (2016) Notes in Tune: Arts-based Therapy (ABT) at Schizophrenia Awareness Association in Pune, India International Journal of Psychosocial Rehabilitation. Vol 20 (1) Correspondence: Aanand Chabukswar, Project Head (Courses), World Centre for Creative Learning (WCCL) Foundation F 1001, Felicita, Baner-Pashan Link Road, Pune Maharashtra. India. mailto: aanandsc@gmail.com Abstract The use of the arts as therapy is a paradox in India. Despite a long tradition of healing rituals and practices, there is barely any artsbased model consistent used for contemporary mental health needs and settings. With the aim of introducing and investigating use of ABT (Arts-based Therapy), regular sessions were conducted at Schizophrenia Awareness Association s day-care centre in Pune, India over a period of eighteen months. The group was heterogeneous, with varied severity of symptoms of schizophrenia. With therapeutic goals of present moment attention and interpersonal engagement, participant responses were recorded through PANSS (Positive and Negative Syndrome Scale), a Rating Scale, a Checklist and qualitative observations. All data sources show definite though variable response to ABT. PANSS scores noted a decline in negative symptoms and general psychopathology, especially the sub-items marked severe show a clear trend of reduction. The correlations between PANSS, Rating Scale and Checklist are notable though not statistically significant. The qualitative data uncovers the nuances of the process. Despite a small sample size, the study points in the direction of use of ABT in mental health settings, especially within the Indian context. Keywords: ABT, Arts-based Therapy, Schizophrenia in India, arts in mental health, PANSS Introduction: Arts-based Therapy (ABT) sessions were conducted at the day-care centre of Schizophrenia Awareness Association (SAA) in Pune between September 2013 and April 2015 for a group of 14 participants. Of that, data was collated for 7 persons in the age range of 23 to 60 years, all diagnosed with Schizophrenia. The aim of these sessions was to reduce symptom severity, with the therapeutic goals of building present moment attention and interpersonal engagement. ~ 62 ~
63 ABT is evidence-based use of art forms to accomplish individualized goals within a therapeutic relationship. ABT derives theoretical base from a systematic training in Subtle Energy Guide (Pillai-Balsara 2013) drawn from the Indian Mind Traditions, notably Buddhist Psychology and Ethics further interfaced with information from neuroscience and developmental psychology (Balsara et al 2013). The practice of ABT is based on use of multi-arts modality to address the therapeutic goals. Within this framework interventions are designed as per the specific needs of each client. Schizophrenia causes a number of fundamental disturbances and distortions in cognition, perception and behavior of a person. There are an estimated four million people diagnosed with schizophrenia in India, with different degrees of impact on some 25 million family members (WHO 2010). Within India, for those who reach out for help, the first line of treatment is mostly psychotropic medication and institutionalization. Even after medication clients experience persisting symptoms, side effects and need for care and capacity building. Additionally, Long term disabling consequences of lost opportunities, stigma, residual symptoms, and medication side effects are also well documented (Spearing 1999, WHO 2001). The SAA day-care centre is thus a host to a growing number of persons seeking relief and care. Historically within India, like in other native cultures, spirituality, rituals, shamanic rites were used in conjunction with traditional healing and medical systems (Davar and Lohokare 2009, Evers 2008, Simoes 2002). In postindependence in India period the need to develop services beyond mental health institutions (Kumar 2004, p. 174) was recognized, which called for a distinctive approach. However, insights were not followed up with systematic actions and the ground reality thus has been the degeneration of traditional understanding and treatment modalities on the one hand and inadequacy of mental health care institutions and trained personnel in face of high need (Thirunavukarasu and Thirunavukarasu 2010) on the other. A middle way that combines the strengths of traditional healing with contemporary specifics has been mostly unexplored. Interestingly, in what is termed as the outcomes paradox, markedly better outcome for schizophrenia patients in India has been reported in WHO s long-term studies (Jablensky and Sartorius 2008, Padma 2014). The better results are attributed to socio-cultural factors, like family, community and local conditions. WHO s recent programmes in India also clearly report that in the Indian context it is important to have innovative programmes that are strongly anchored in the community and are family-based and family-oriented (WHO 2010, p. 3). Approaches that recognize the differences and nuances of social, cultural and economic variations are extremely important. In this context ABT strives to make way. In ABT, the difference between the person labeled with mental illness and the one without is considered one of degree and intensity of suffering, and its consequent impact on functioning in life. Multiple realities and their coexistence are acknowledged, and the ability of a person to navigate skillfully and meaningfully between different levels of experiences and existence is significant. The arts are uniquely situated as they experientially create alternative realities, yet the boundaries between them are held in awareness. ABT offers a range of artistic tools a rich language of music, rhythm, songs, stories, drama, visual art methods and their numerous combinations. The artistic activities bring the attention onto colours, images, stories, rhythms, musical phrases. Metaphors make things manageable, and possible to understand. Sharing, giving-receiving in a co-creative spirit happens seamlessly in a group. Here, the emphasis is on the process, the artistic outcomes are secondary and playfulness ensures that there is no stress, no pressure. The focus is on the capability of the person no matter how small or insignificant the contribution may seem (Chabukswar and Daniel 2009). The artistic process also presents a complementary counterpoint to mere verbal engagement in therapy that experience can transcend conceptual barriers to reach a person. The creative interactions record nuances of the therapeutic process that otherwise cannot be documented. ABT thus navigates towards symptom relief, supplementing the vital institutional agenda in the rehabilitative process. ~ 63 ~
64 ABT projects in adult mental health from 2006 to 2013 from WCCL Foundation s archives were reviewed (Chabukswar 2013) to note case studies of 129 participants in the age range of 15 to 79 years, all diagnosed with mental health disturbances (depression, schizophrenia, emotional distress, trauma) all engaged with ABT for a minimum period of 6 months. Client-specific individualized therapeutic goals were worked on and overall positive therapeutic outcomes are noted (Table 1). These projects used varied assessment tools, including standardized assessments tools, checklists and observation formats. However, qualitative data (interviews, structured and unstructured feedback, observations) yield more meaningful data. Many projects note the limitations of time, tools and methods and lack of availability or reliability of standardized assessment tools given the specific conditions of work in India. Table 1: ABT projects in adult mental health ( ): Therapeutic outcomes Better mood and affect than before Better comprehension of tasks Clients opening up: showing interest and initiative Higher confidence and self-efficacy Improved communication in the group Improved speech through storytelling and singing Improvement in perception and cognition Increase in attention span Increase in expression of emotions More effective symptom management Overall improvement in somatic memory Sensory integration This paper explores the trajectory of a particular ABT intervention at SAA in Pune, India. How engagement with ABT challenged the symptoms that resulted in a significant decrease in severity, and reflected a decline in negative symptoms and general psychopathology measured on PANSS (Positive and Negative Syndrome Scale). The observations from PANSS further demonstrate a positive correlation with ABT Practitioner s Rating Scale as well as the Checklist on attention and interpersonal engagement. This is further corroborated by qualitative observations made by an independent third person and the ABT Practitioner. The outcomes are significant enough to make a case for ABT as a friendly and accessible therapy that complements the tools for symptom relief and rehabilitation in Schizophrenia. MATERIALS AND METHODS The setting and the group Schizophrenia Awareness Association s (SAA) Swanand Punarvasan Kendra is a day-care centre for people with mental illness. At the centre, such a person comes to an environment that is meant to provide a structure and tools for day-to-day functioning that can support the process of recovery. Activities like yoga, dance, cooking, computer training and vocational activities like making lamps, paper bags etc. are done at the centre. Therapeutic activities include counseling, self-help tools, parents support group and the newly introduced, ABT. 14 participants attended the ABT sessions, of which data was collated for 7 participants who were part of the group for the entire 18 months. Individualized therapeutic goals for each participant were set (Table 2) and common therapeutic goals were identified as keeping attention here and now for reality contact and increasing interpersonal engagement for reduction in isolation. ~ 64 ~
65 Table 2: ABT Group background, symptoms and therapeutic goals Participant Background Symptoms in 2013 Therapeutic Goals (age in 2013) Avinash Male, age 50 Disorganized schizophrenia. Onset ECTs and medication. Tobacco addiction and diabetes. No hygiene, auditory andmake reality contact by visual hallucinations. keeping attention in the Sudden outburst of here and now laughing and muttering. No participation, no Being interaction active/participative in ABT. Arti Female, age 60 Paranoid Schizophrenia. Lack of concentration, Make present reality Onset Given ECTs confidence. Irritation andcontact by being active and medication. suicidal thoughts. Mood in ABT swings, irrelevant talk, poor self-care and Developing strength to hygiene. Persecutory feel worthy of living delusions, OCD about food and touching. Madhu Female, age 32 Schizophrenia. Sudden onset in Obsessive, irritation, poor social interaction. Borderline IQ. Self-talk, auditory and Control and express visual hallucinations, emotions appropriately sometimes violent. Guilt Building interpersonal about past violent skills and interactions behaviour. Sometimes laughing uncontrollably and intense anger at times. Nikash Male, age 23 Pratiksha Female, age 36 Intellectual disability andcatatonic features i.e. Psychosis. Onset stiff muscles, long reaction time, poor finemotor skills. Poor social interaction, barely audible. Delusions and OCD about eating, touching, poor hygiene as a result. Flat affect. Paranoid Schizophrenia, onset On medication. Tactile hallucinations, persecutory delusions. Poor hygiene (no bathing). No interaction at all. Improvement in gross and fine motor coordination Being attentive and audible thereby expressing himself clearly in the ABT sessions Attention to the here and now Improvement in speech (volume and audibility) Meaningful interaction with others Reena Paranoid Schizophrenia, Visual and auditory Reduction in tension and ~ 65 ~
66 Female, age 41 onset ECT (once) & medication. hallucinations, severe persecutory delusion. Not much interaction with others, anxious about her future. Has insight. to be at ease Ease in interactions Vikas Male, age 33 [1] All names changed Epilepsy since age of 6 years, calcium deficiency and low IQ. Onset of schizophrenia in Bursts of uncontrolled laughing, crying, swearing. Heavy (91 kg), very sleepy all the time. Repeating same thing over and over. Very little attention span. To pay attention, to be present Increase span of attention on the here and now Developing some ability to interact with others in a specific, meaningful way All except one participant showed direct signs of visual, tactile hallucinations. Four of them had severe symptoms of social withdrawal, were almost non-verbal, showing no interest in any activity or interaction. To varying extent, all were locked or engaged in alternative reality, lacking external reality contact. Three participants were verbal one of them apprehensive of interactions due to persecutory delusions and another hyper-interactive, demanding but with limited verbal range. The group was diverse in severity of symptoms and the duration since onset of schizophrenia varied between 4 to 23 years when the study commenced. Design and data sources The premise for the study was to use ABT as an adjunct to reduce symptom severity. A total of 51 weeks of ABT sessions were spread out from September 2013 to April 2015, equally divided between the Pilot phase (12 weeks) followed by 3 phases of intervention (13 weeks each). PANSS is a medical scale used to measure symptom severity; a 30-item, 7-point rating instrument that gives representation of positive and negative symptoms at increasing levels of psychopathology, where 1 = absent, and 7 = extreme (PANSS Institute, Kay et al 1987). The PANSS is widely used for strong psychometric properties in terms of reliability, validity and sensitivity (Leucht et al 2005) and was selected for its accessibility and familiarity. SAA clinicians rated PANSS for participants once at the beginning of the ABT pilot project in September 2013 (AS1) and 4 more times during the next phases (AS2 AS5), at an interval of 3 to 6 months. Studies confirm that most PANSS items are either very good or good at assessing the overall severity, particularly items within the Negative Symptom subscale (Santor et al. 2007). The criterion of schizophrenia remission, where a score of mild or less (less than 3) in case of the 8 selected criteria in PANSS for a minimum period of 6 months indicates remission (Andreasen et al. 2005, p. 447) have been recently in discussion. Remission is a new research outcome indicating wellness (Yeomans et al. 2010, p. 86), and thus these sub-items have been analyzed separately. The clinicians also rated a Checklist of 8 items on Attention: here and now and Interpersonal Engagement. Higher scores under Checklist reflect better attention and interpersonal engagement. ~ 66 ~
67 A 5-point Rating Scale was modified from WCCL Foundation s earlier study (Daniel et al 2013b) and was rated 4 times during the intervention period by the ABT Practitioner. It is a holistic scale that records responses and behaviours in the sub-domains of Body, Attention, Group Interaction, Cognitive, Narrative Capability, Expressive Capability. The rating statements are positive indicators of well-being and, higher scores reflect better response. Qualitative Observations of responses and interactions within every ABT session were also recorded by the ABT Practitioner and by neutral observers. Table 3: ABT Techniques for Attention Singing or prayers at the beginning and closure; memorizing them Name ritual: acknowledging and greeting self and others in a particular pattern Stimulation of attention through observations of objects e.g. bell (auditory), incense (visual, olfactory); of people e.g. clothes, colours, styles; of weather and seasons etc. Short sections of concentration on an object: e.g. focus on trees, on breath Ritual to be light: letting go and mentally/physically throwing away unwanted materials, thoughts and distractions Mindfulness ritual for coming back here and now: reminders accepted from group and facilitator for this Sharing stories: listening to stories, recalling stories, narrating stories (participants and facilitator) Drawing with crayons: free drawing and colouring, theme based drawings, occasion specific drawings Breathing and relaxation Table 4: ABT Techniques for Attention & Interaction Ball throw and ball juggle with partners, triads and the entire group Vocal warm-ups and voice exercises Physical warm-up and movement with music Games and group-work e.g. working with partners on embodiment activities, games structured around movement, attention and interaction Dramatic improvisations: Making interactive theme based scenarios and developing them, e.g. at the seashore, waking up and the beginning of the day, guests at school, visiting a restaurant etc. Narratives and Images: Verbal / physical work with images identifying images, expressing them. Joining images into narratives or stories, using toys, clay, puppets to create ~ 67 ~
68 narratives Enactments: Scenes from a story enacted, playing with roles and dialogue Song-circles: Recalling series of songs on a particular theme and singing them together in group, e.g. season, journey, morning, nationalism, fearlessness, picnic songs, A. R. Rahman songs, light, lightness etc. Exploring variety of percussions, playing them with songs Planning and visualising: Listing activities planned for an ideal day, articulating personal intent for the year Creative conversations: Discussions about picnics and travels, about pets and animals, about friends and friendships Person in focus: Exploring metaohors for each group member s special qualities, observations from the group about what can each one improve done with extensive process and permission from each member Apart from client-specific therapeutic goals, key concepts non-measurable positive aspiration for the participant group are an important aspect of ABT intervention. At SAA, the quality of generosity was the key concept, where the idea of giving and sharing was woven as a subtext for all sessions. This key concept is a vital step in mind training; it is also a logical progression towards harmonious, compassionate and successful social interaction. This key intent was integrated in all phases of intervention, and regular specific exercises were designed for it (table 5). Table 5: Exercises based on Key Concept Acknowledgement: Thanking every time someone does something for us; acknowledging others for their presence. Thanking everyone with eye contact at the closure of each session Awareness: List of who gives us what? what in oneself troubles others? what gives joy to others? Discussing significance of small acts Aspiration (Giving): If we have the means or imagination for it - what will you give to those in need? Imagination of how much of food water shelter and goodies can one give and keep on giving, to whom all? What and how much can I give to the group members here? Articulating creatively (even through songs) what it means to want good for others Action: Making an intent for oneself, making greeting cards for loved ones and giving it to them, making action plan for days or week and following that plan RESULTS Overall, there is remarkable difference between the scores on negative and general pathology sub-scales when comparing September 2013 and March 2015 scores in PANSS. The correlations between PANSS, the Checklist and Rating Scale are notable, however the changes in the scores in the Rating Scale and Checklist would not be considered statistically significant. The statistical findings should be interpreted in conjunction with the qualitative ~ 68 ~
69 observations and limitations, discussed later. Mean Differences T-tests were conducted to check if participants did indeed show significant changes in symptom severity and wellbeing after having participated in different phases of ABT from September 2013 to April The changes on the ABT Rating Scale and the Checklist scores cannot be considered statistically significant, but there was a substantial difference seen on the scores for the PANSS. While the mean score in September 2013 was (SD = 6.7), the mean score in March 2015 was (SD = 18.78). In spite of unequal variance, this difference was found to be statistically significant in favour of improved health [t (7.504) = 3.316; p < 0.05]. This difference was further explored to reveal not all aspects of PANSS showed the same amount of change. While overall scores showed a distinct move towards better mental health, it was only the scores for negative symptoms and general pathology that showed a statistically significant improvement. While the group experienced a mean score of (SD = 4.649) on negative symptoms in September 2013, this mean score had come to (SD = 8.63) by March Again, this difference achieved statistical significance in spite of unequal variance [t (9.213) = 2.815; p<0.05]. Similarly, while the group showed an average score of (SD = 3.98) on general pathology in September 2013, the mean score on March 2015 was 33 (SD = 10.01). This reduction in score was statistically significant although the variance was very different [t (7.856) = 2.77; p<0.05]. Both, the scores for positive symptoms and the composite score show a distinct improvement across the group; but these differences did not reach accepted levels of statistical significance. There is a serious increase in the variance in scores between the initial and final testing. This suggests wide variation in the performance of the participants on different scales and test items towards the end of the testing period. Since there was far lesser variability in scores at the beginning of the data collection process, it could indicate that some participants benefitted from ABT more than others. Correlations Correlations were computed across different instruments used to collect data. It was seen that all the sub-scores on the four subscales of ABT Rating Scale significantly correlate to each other; suggesting there are some common factors that govern the extent to which participants demonstrate bodily awareness, interaction with the group, cognitive ability and narrative and expressive capacity. All the sub-scores on the Rating Scale significantly correlate to the Attention sub-score on the Checklist. Logically this makes sense, since attention to the here and now is an important factor associated with awareness of one s own body, the ability to interact with each other, and with expressing thoughts and ideas, and explaining them to others. On the other hand, only the group interaction score in the Rating Scale seems to share a significant relationship with Interpersonal Engagement sub-score from the Checklist - which is the only sub-score that it shares a meaning with. It is rather intuitive that better interpersonal interaction would be associated with enhanced engagement within the group. From among the ABT Rating Scale sub-scores, PANSS as a whole reflects negative correlation with bodily awareness and narrative capacity. The relationship with group interaction and cognitive ability sub-scales while strong and in the expected direction fell just short of statistical significance. As participants do better on Rating Scale items, they report fewer and lower intensity of clinical symptoms in PANSS. This finding is reassuring, since it suggests as participants start having fewer issues, they also start experiencing improved wellbeing. Although, as expected, while the values of the correlations are strong and negative, PANSS did not share statistically significant relationships with either of the Checklist sub-scale. This suggests that better performance on the Checklist is associated with somewhat fewer clinical symptoms; and the relationship may need to be explored with a larger ~ 69 ~
70 group to make sense of it. What makes these trends heartening is they represent an interesting shift from the type of relationships seen among scores at the beginning of the testing period. Before ABT was introduced, all sub-scores on the Rating Scale and on the Checklist shared significant positive relationships; but none of these scores shared either a significant or a strong relationship with PANSS. But as some of the participants started showing improvements, these relationships started to become evident. Self-awareness and expression in particular, seem to improve as symptoms go down. To a lesser degree, attention, aspects of social interaction and cognitive process also seem to improve when clinical symptoms are lower. PANSS Remission Items When the scores on the eight remission items are looked at specifically, out of the 7 participants 5 show reduction in symptom intensity, while 2 did not benefit across the testing sessions. For some participants in particular sub-items the initial scores were low and continue to stay low. For others, there is reduction in scores for some items, but not in others. Table 6: PANSS scores on 8 Remission Items AS1: Sep 2013AS2: Mar 2014 AS3:August 2014 AS4: Nov 2014 AS5: Apr 2015 Avinash Arti Madhu Nikash Pratiksha Reena Vikas The chart for the same data ~ 70 ~
71 Graph 1: PANSS Remission Items PANSS Severe Items The impact of ABT becomes a little clearer when we identify items in the PANSS that had severe rating in September 2013, and isolate them from the others. For some participants, there were many such items, while others had a severe score on only a handful of items. The scores for all these items were tracked separately across different data collection sessions. For ease in comparison, the scores across all tracked items were aggregated for every participant during each data collection session. This was done so that the number of items being tracked would not confound the trends being explored. As observed from Table 7, there is a distinct trend towards severity reduction as time progresses for most participants. Table 7: Average Scores on PANSS Severe Items AS1: Sep 2013 AS2: April 2014 AS3: July 2014 AS4: Dec 2014AS5: Apr 2015 Avinash Arti Madhu Nikash Pratiksh a Reena Vikas This trend is better understood through the following graph. ~ 71 ~
72 Graph 2: PANSS Severe Items The observations by neutral observers and ABT Practitioner correlate with the statistical data. They reflect reduced symptomatic behaviours and an increase in the instances of attentive engagement with the here and now and others. Qualitative notes for two participants are included here. Notes for Avinash Diagnosed with disorganized schizophrenia in 1985, and living with it the longest from within the group. Avinash was of 50 years of age when ABT started. He is married and has a daughter. In the initial period, Avinash never established eye contact or participated in any activity, and never responded verbally to any suggestions or instructions. He did not maintain hygiene, was lost in talking and laughing, engaged with auditory and visual hallucinations. His past treatment included ECTs at some point. Therapeutic goals for Avinash were set as bringing attention to here and now and being participative in ABT sessions. Initially during the sessions, Avinash would be pacing about, mumbling, abruptly leaving the room. These observations recur through the entire first phase. It took 6 months to make the first eye contact, first physical participation and first coherent response within the session. Another 6 months later leaving or pacing was observed only once during the entire third cycle. ABT invited his attention and Avinash began to interact, sample this: Sitting in his typical head bowed down position and mumbling, nodding, hallucinating. The facilitator called him out to join-in. He shook his head and said no. The facilitator persuaded, he looked-up, said yes. The facilitator sat in front of him and threw a ball at him, he reached out for the ball. A game of catch-throw ensued. Another ball was added, two balls simultaneously, Avinash smiled as he juggled the balls notes the observer. Subsequent sessions build on this further Avinash played ball juggle with Pratiksha - he was alert, catching all the time, without dropping ball. He then invited the facilitator (who was on the side) to join-in. They played ball juggle, 3 persons, 3 balls simultaneously. Eventually this moves on to spontaneous interaction in another session, played a long rally of balloon pass with the facilitator. Avinash, smiling gave a hi-five to the facilitator, then played in a triad with Nikash too. Avinash started participating in the ritual of greeting each person by name and making eye contact without being prompted to do so. It is also noted that he reminded Nikash or Pratiksha to fold hands and greet! His reluctance continued, like a habitual response, but it gave way with a bit of insistence. There was some newfound inquisitiveness. Once as the facilitator arrived Avinash waved and smiled and started a conversation of his own accord, asking the facilitator questions. In the session during a concentration exercise, he added his own observations to the group s, I see bluish colour in the smoke of incense, the incense stick is brown. He was coherent in speech ~ 72 ~
73 and neater than before. Observations recur to note that he participated in prayer without prompt and did voice exercises on prompt or that he smiled in response to a joke, not hallucinatory smile. In one of the activities making drawings and intent for the year, Avinash declared I will participate in activities here! These notes coincide with PANSS scores the sub-scale of 8 remission items show a notable decline in symptom severity (Table 5, Graph 1). While the symptom severity lessens, the Attention and Interpersonal Engagement Checklist indicates marginal increase in average scores. The Rating Scale also shows a gradual positive incline in the overall scores, indicating a tilt towards wellness. Consistent bettering in all scores coincides with period when Avinash did not miss a single ABT session (AR1 and AR2). There is a marginal fall in the last phase (AR3), during this period he had missed almost 40% of the sessions. The effect of this absence was noted in observations as well, Avinash came today after 4 weeks. Said hello, smiled, but seemed inside his own world again. This suggests a connection between regularity in ABT sessions and response level, and thereby the therapeutic effect. During one exercise in which each person named their own or others extraordinary quality, the facilitator turned to Avinash and teasingly asked as you will not speak, may be we should assign you something - a high quality stubbornness.shall we say?' He promptly replied no and pointed to his ears, tapped on them and said, listening, listening. Everyone in the group saw and heard this, and laughed and agreed. In another session he explained a drawing meaningfully this is a lotus, and it grows out of the mud. In these instances, his worlds, his tune and ours came close together. Notes for Madhu Madhu, age 32, experienced a sudden onset of obsessive thoughts and hallucinations 4 years earlier. She is the most recently diagnosed within the group. Her IQ was recorded as borderline. Her parents are supportive, but she felt tremendous guilt for past violent outbursts towards them. She sometimes laughed uncontrollably and experienced sharp intense anger. She would mumble to herself, give instructions to herself, and suddenly retreat into her shell. The therapeutic goals for Madhu were set as appropriate emotional expression and building interpersonal skills. She was enthusiastic in the ABT sessions right from the outset and enjoyed movement exercises, singing songs, drawing, and other artistic exercises. Early on, the observer notes that she was attentive herself, and urging others to pay attention as well. Yet suddenly she would be adrift, mumbling, lost. Took time to orient herself. During one of the ABT sessions, she said am feeling very angry, like hitting someone. This turned into an activity of imaginary boxing game, moved on to body movements with music. The ABT sessions opened opportunities to express what was difficult otherwise. During an improvisation exercise around the theme of guests, Madhu said, there's a presence. she competes with me all the time. Whenever I want to do anything, the other one comes and takes space. She does all that I would like to do; I am upset because of this. She spoke haltingly, grappling for words, records the observer. A conversation about being alert, and about handling wanted and unwanted guests ensued. In another session, with a drawing, she managed to define things that she wanted to throw away forever in a black hole: she explained them as her moods, negative thoughts, anger and the surrounding chaotic lines as fear and difficulty around me. In ABT, the art-loving Madhu seemed to find a way to clarify and express her experience. Madhu was sincere and she took to heart the various artistic rituals created to keep alert, to say stop to obsessions and telling the hallucinatory presence to go. She reported I have been using the stop and go, especially when I get very angry, and it was useful. She was always enthusiastic to narrate stories or enact them. Once, as she started telling one story of Birbal and his khichdi, mix of rice and pulses, she mixed the narrative with another story, and continued, and further mixed it up with yet another story. Everyone just listened. At the end of her narrative she quipped, I made khichdi (mix-up) of 3 different stories together! Another time the group was working with a Marathi folktale. Apparently it is a children s tale, with rhyme and chants, about an old woman who is accosted by predators on her journey to her daughter s place. She is going there to ~ 73 ~
74 rest and recover her health. On her way back, she gives a slip to the predators by hiding inside a pumpkin. Madhu was the first one in the group to identify it as a children s tale heard in childhood!. Others caught on and memories of the tale were discussed. Madhu added her reflections I think it s a story about protection, when we are not well, to take care. This was appreciated by the group and the facilitator. She spontaneously substituted the story s rhyme with a ditty of her own chal re mana aplya gava (O mind, let's go to our true home). This was applauded by all. As the discussion went round from person to person, Madhu came back with another understanding, I think there is no pumpkin. When the old woman recovers from illness, she is a changed person. She is well-fed and her health is restored, so she has become large, like the pumpkin. On this, much laughter ensued, but the myriad meanings were not lost. Here was someone, riding on the back of traditional tale, uncovering an insight. The PANSS scores corroborate these shifts in the sub-scale of 8 remission items, all items except one show stable low or consistent decline to below severity scores. PANSS sub-items that were severe for Madhu in September 2013, all without exception, declined, showing remission sustained for period of 6 months in subsequent assessments (Table 6). The Checklist and Rating Scale correlate, where the latter shows a positive jump in expressive capability and attention. Many recurring observations note how enthusiastically Madhu sang songs and how they changed from sharp, shaky notes to more measured and accurate expression. She expressed happiness in dance movement, was alert in ball throw and made meanings in the stories the observations note. Commenting on the African folktale of the Greedy Hyena and the Great Tree, she had the last word in the group the thoughts that trouble, like the hyena in the story, must be deleted forever. DISCUSSION Limitations Statistical techniques were employed in a bid to analyze the objective trends seen among participant scores. Although the findings suggest changes, it is necessary to interpret them in context. The sample size was extremely limited (n = 7); and the data collection for PANSS in different stages was done by 2 different clinicians - a factor that may have confounded the more subjective scores. It is important to remember that the group was heterogeneous to begin with, many participants were also on medication, and that this data does not reflect any special circumstances that could have confounded the scores at any of the testing sessions. The researchers accept that these factors reduce the value of the statistical findings; but nevertheless we have chosen to explore said findings as one part of a larger analysis. The study is also constrained by limitations of time and resources, and lack of availability of a matching control group. Reflections This project has been one of its kind long-term interventions within India. It has explored the capacity of the artistic within the Indian paradigm to be helpful to those with mental health issues in an institutional setting. ABT is uniquely situated; addressing personalized therapeutic needs, within the context of local patterns and possibilities of healing and rehabilitation. It works in complementation (not confrontation) with other therapeutic work that may be going on. Given that ABT engages the participant in artistic and expressive modes, it is almost intuitive that it has had a remarkable change in negative symptoms and general psychopathology as measured on PANSS. Yet, studying carefully each participant s scores and notes, it is clear that actually for this particular group at SAA, the maximum severe items were on the negative scale followed by general psychopathology in PANSS, and those are being addressed through ABT. ABT systematically focused on, and therefore dovetailed with the therapeutic needs of the participants. We can therefore safely assert that ABT positively impacts the therapeutic needs of a participant. This is supported by initial observations of a second ongoing group of participants at SAA for a period of 6 months in 2015 that reported reduction in severity despite dissimilar symptoms than the earlier group. ~ 74 ~
75 The unique methods and approach of ABT create an artistic atmosphere. The sessions are fun, there is ease and laughter, and it relaxes the participants. ABT works with what one can do, what is intact. A reassuring contact with artistic rituals, the known and unknown music, movements and paintings is possible. Participants can choose to relate or retreat as much as they want. The individual s safeguard s are protected, but prodded playfully. It was not burdensome to be persistent and make contact with Avinash because of this underlying understanding, and also because it was essentially a playful, arts-based persistence. It is recognized that the participants are unceasingly coping with the situation they find themselves in, and their coping is to be aided with appropriate modes and tools. In the sessions each one would make and shape experiences with voice, images, narratives, rhythms or tunes. This world there was manageable, even malleable. Getting a hold over an experience can give a sense of charge over it. Madhu mixed-up narratives while telling her story, but navigated herself in that mix-up (others and she, herself, listened), and she did playfully quip that she made a mix-up! The process created opportunities to express, examine and evolve the coping energy into practical and useful explorations. The flexibility and rich variety of tools and techniques of multiple art forms enabled an eclectic, fittingly personalized approach. ABT worked with a person rather than his/her diagnosis in the true sense. No matter how severe the symptoms or how difficult a person might seem, we strove to open a dialogue with the experience of the person. After 23 years of being increasingly locked-up inside his world, Avinash seemed to eventually trust, not the words or the show of respect, but the actual experience of an alternative space. His smiles and contact with us indicated a refreshing change. Madhu could listen or tell stories and eventually arrive at insights on her own despite the label of borderline intelligence. Such potential is there in every session and each participant, all through. Each small step took us to common, shared ground. Madhu enjoyed working with colourful clay, and then she told narratives about it, attention and appreciation from others encouraged her. Avinash was amused with ball-juggle and balloon-pass, and that got him to interact. His drawing of a lotus in mud said something. In successive sessions, attention rested for one moment, briefly, or longer, as per person in the here and now, leading to acknowledgement of self and others, and interaction. It cannot be emphasized enough that trained ABT Practitioners don t approach mental health with merely a bag of artistic tools and techniques, but are informed with study of mind and training in compassion as a the preliminary mode of relating. ABT is not mere art activity ; it works with a decided and dedicated therapeutic framework. As a complementary therapy, it doesn t deny the role of other therapies and approaches. It works extremely well in suitable organizational and institutional environment. This particular study is just a beginning of a journey. A plea for more trained ABT Practitioners is a plea for a systematic approach in the arts, informed with appropriate theoretical framework and culture-specific models of intervention. Considering holistic support, care and therapeutic work for those experiencing mental illness is an urgent and forcefully growing need. There is also need for more systematic long-term studies with larger sample size and in-depth qualitative and quantitative measures to underline and extend the mere notes of this present study into well-formed score of therapeutic work. References Andreasen, N. C., Carpenter, W.T, Jr, Kane. J.M., Lasser, R. A., Marder, S. R., Weinberger, D. R. (2005) Remission in schizophrenia: proposed criteria and rationale for consensus, American Journal of Psychiatry. 162: ~ 75 ~
76 Balsara, Z., Chabukswar, A., Daniel, D. (2013) ABT Manual: Artistic Skills and Structures (3rd edition). Pune: WCCL Foundation. Chabukswar, A., and Daniel, D. (2009) Real World: ABT for Children with Disabilities. Pune: WCCL Foundation. Chabukswar, A. (2013) Review of ABT Projects in Adult Mental Health Settings in India. Pune, WCCL Foundation Daniel, D., Balsara Z., Pillai-Balsara, A., Chabukswar, A, Kulkarni, S., Gohil, P. (2013b) Best Practices in ABT: An Action Research Study with Adults in a Deaddiction Centre, Pune: WCCL Foundation. Davar, B. and Lohokare, M. (2009) Recovering from Psychosocial Traumas: the Place of Dargahs in Maharashtra, Economic and Political Weekly. Vol. 44, No.16: Evers, N. (2008) Shamanic Perspectives on Mental Illness in The Icarus Project. Online HTTP. < (accessed July 10, 2013). Jablensky, A. and Sartorius, N. (2008) What Did the WHO Studies Really Find? in Schizophrenia Bulletin, vol. 34 no. 2: Kay, S. Flszbeln, A. and QpJer, L. (1987) The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia, Schizophrenia Bulletin. Vol. 13, No. 2: Kumar, A. (2004) History of mental health services in India, Journal of Personality and Clinical Studies. March- September, Vol. 20, Number 1-2: , New Delhi: Association of Clinical Psychologists. Leucht, S., Kane, J., Kissling, W., Hamann, J., Etschel, E., and Engel, R. (2005) What does the PANSS mean? Schizophrenia Research 79, pp Padma T. (2014) The Outcomes Paradox, Nature, Vol. 508: S14-S15 PANSS Institute, The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Online. HTTP < (accessed July 30, 2013). Pillai-Balsara, A. (2013) Subtle Energy Guide (3rd edition). Pune: WCCL Foundation Santor, D. A., Ascher-Svanum, H., Lindenmayer, J.-P., & Obenchain, R. L. (2007). Item response analysis of the Positive and Negative Syndrome Scale. BMC Psychiatry, 7:66. Online. Simoes, M. (2002) Reflections of a psychiatrist on Ayurvedic medicine in Salema, A. (ed.) Ayurveda at the Crossroads of Care and Cure, pp , Lisbon: Centro de Historia de Alem-Mar, Universidade Nova de Lisboa. Spearing, M. (1999) An Overview of Schizophrenia. Publication No , Bethesda (USA): National Institute of Mental Health. Thirunavukarasu, M. and Thirunavukarasu, P. (2010) Training and National deficit of psychiatrists in India a critical analysis, Indian Journal of Psychiatry. 52, Suppl. S3: Weinberger, D. (1998) Schizophrenia: The Cancer of Mental Illness paper presented at NIMH conference, Discovering Our Selves: The Science of Emotion. Library of Congress: Washington. Online. Available HTTP ~ 76 ~
77 < (accessed September 28, 2013). WHO. (2001) Mental health: New Understanding, New Hope, The World health report Geneva: World Health Organisation, pp WHO (2010) Country Project of support to people with Schizophrenia - INDIA: SUPPORT TO PEOPLE WITH SCHIZOPHRENIA, Geneva: World health Organisation. Online. Available HTTP (accessed September 8, 2013). Yeomans, D., Taylor, M., Currie, A., Whale, R., Ford, k., Fear, C., Hynes, J., Sullivan, G., Moore, B. and Burns, T (2010) Resolution and remission in schizophrenia: getting well and staying well Advances in Psychiatric Treatment, Vol. 16, Online. HTTP: <apt.bp > (accessed 3 October 2015). ACKNOWLEDGEMENTS Many visible-invisible hands shape WCCL Foundation s ABT action research and training and we owe deep gratitude to all of them. Especially for the project Notes in Tune at SAA, we sincerely thank the funding support that came forth from many sources the Praj Foundation, Terragni Consultancy, Mr. Srikrishna Bharambe, Mr. Sunil Chavan, Ms. Sulabha Mahajan, Ms. Shaheen Colombowala for the trust they posited in us. The entire SAA team Mr. Amrit Bakshy, Mr. Gurudutt Kundpurkar for their support, Ms. Neelima Bapat and staff, the clinical psychologists Sarika, Kadambari, Tushar for the support in data collection and assessments. Ms. Gauri Sarda helped with her time and effort without any qualms, analyzing, encouraging and helping with the statistical data. Without her help, the writing wouldn t have been possible. Thanks to Amruta and Kumud for painstakingly reading the draft and for the suggestions. Dr. Bhargavi Davar contributed with her critical and timely comments. My family and team at WCCL Zubin because of him the systematic path of action research is diligently followed, Asha who as the leader constantly eggs us on into huge vision and refined action, Deborah, whose support and insights are always valued, and Anisha for her invisible work. To them, I cannot thank ever enough. Last but not the least, to those members of SAA who have participated in and have continued with ABT sessions. May the highest possible benefit of healing and wellness come to them. Bhavatau sarva mangalam ~ 77 ~
78 Better Eating and Recovery: Addressing Food Insecurity at an urban Community Mental Health Center Marydale DeBor JD Lecturer, Yale School of Medicine, Department of Psychiatry Chef Anne Gallagher Consulting Chef, Connecticut Mental Health Center Francine Blinten MS, Consulting Nutritionist, Connecticut Mental Health Center Michael Sernyak MD Professor of Psychiatry, Yale University Department of Psychiatry and Chief Executive Officer, Connecticut Mental Health Center Robert Cole MHSA Lecturer, Yale University Department of Psychiatry and Chief Operating Officer, Connecticut Mental Health Center Steve Olsen Peer Facilitator, Connecticut Mental Health Center Annie Harper PhD Associate Research Scientist, Yale University Department of Psychiatry Citation: Debor M, Gallagher A, Blinten F, Sernyak M, Cole R, Olsen S, & Harper A. (2016) Better Eating and Recovery: Addressing Food Insecurity at an urban Community Mental Health Center. International Journal of Psychosocial Rehabilitation. Vol 20 (1) ~ 78 ~
79 Corresponding Author: Annie Harper, 58 Anderson st, New Haven, CT Acklowledgements: The authors wish to acknowledge the support of Ann Joy, Director of Out Patient Rehabilitation at CMHC whose department added occupational therapy expertise in curriculum development and pilot implementation. Research Associate Cara Donovan (MPH/MS candidate Yale School of Public Health/Yale School of Forestry and Environmental Science, 2017) assisted with documentation of the sessions and research support. Also contributing to the effort were Better Eaters Club alumnae and co- facilitators Serena Spruill and Robert Forlano. Abstract This article describes a pilot program to improve diet and nutrition among low-income clients of an urban mental health center, including efforts to transform the overall food delivery system and culture, and the Better Eaters Club, a recovery oriented, hands-on intervention directly targeting clients with group based and one-on-one nutritional counseling. The article outlines the complexity involved in full-scale transformation of an institutional food delivery system and culture, and describes initial, promising results of the Better Eaters Club and one-on-one nutritional counseling, based on anecdotal reports from participants. This pilot project has laid an important foundation for a transformed food delivery system, and the institutionalization of a cooking and nutrition program designed specifically for low-income people with mental illness, including a finances and budgeting component. Future steps will incorporate more rigorous evaluation mechanisms tracking health indicators, knowledge of nutritional issues, cooking skills, and food security. Keywords: Food Insecurity; Nutrition; Cooking; Chronic Disease and Mental Health Introduction: A recovery-oriented approach to mental illness is based on the premise that a good life with the illness is possible, rather than putting life on hold while attempting to recover from symptoms of the illness. The essence of recovery is a renewed sense of self as a whole person, despite or incorporating ones illness, along with a redefinition of one s illness as only one aspect of a multidimensional self (Davidson, 2003). Within this approach, person-centered services and supports that help people lead a good life where they are able to take maximum control over decisions that affect their life are essential, alongside efforts to reduce distressing psychiatric symptoms. (Substance Abuse and Mental Health Services Administration, 2004). Diet and nutrition are key building blocks for both good physical and mental health. People with mental illness often struggle to eat a healthy diet and are more likely than the general population to be obese and suffer from diabetes and other diet-sensitive diseases (De Hert et al., 2011). This may in some cases be due to side effects of medications and/or sedentary lifestyles (Allison et al., 1999; Compton, Daumit, & Druss, 2006; Dipasquale et al., 2013; McCreadie & Scottish Schizophrenia Lifestyle Group, 2003). There is also evidence that there may be a causal relationship between poor nutrition and mental disorders including depression and anxiety (Melanson, 2007). In addition to the biological effects of an improved diet, the experience of taking control of one s diet and taking care of one s physical and mental health through that diet may support the recovery process; the development of self-efficacy a sense of a competent and agentive self has been shown to play a key role in recovery (Mancini, 2007). Poverty and related food insecurity are also important factors in the connection between mental illness and poor diet (Compton & Shim, 2015; Compton et al., 2006) (Wunderlich & Norwood, 2006). People who are poor struggle to access and afford low energy density food that has a high content of vitamins and minerals, such as whole grains, ~ 79 ~
80 lean meats, fish and fresh fruit and vegetables (Darmon & Drewnowski, 2008). People with mental illness are more likely than others to be poor and unemployed, with income from social security benefits for those unable to work leaving many recipients living below the federal poverty line (McDonald, Conroy, Morris, & Jennings, 2015). A higher percentage of people with disabilities than those without are homeless, which compounds difficulties in maintaining a healthy diet (Folsom et al., 2005) The Setting: Connecticut Mental Health Center, New Haven, CT. Connecticut Mental Health Center (CMHC), founded in 1966, is one of the oldest community mental health centers in the United States. An enduring collaboration between the State of Connecticut Department of Mental Health & Addiction Services and the Yale University Department of Psychiatry, CMHC provides mental health services for 5,000 people in the Greater New Haven area each year. It is also a center for scientific advancement in the understanding and treatment of mental health and substance abuse disorders. CMHC, is a major training site for psychiatrists and psychologists from the Yale Department of Psychiatry and welcomes trainees from a variety of other disciplines including nursing, social work, and chaplaincy. Most if not all patients served live on low or very low incomes. CMHC aspires to follow a recovery-oriented model of care, and takes seriously the social determinants of health that affect many of its clients. Recognizing the value of a healthy diet and the multiple barriers faced by people with mental illness in achieving a healthy diet particularly given poverty-related constraints, CMHC began in recent years to actively consider how to better incorporate diet and nutrition into care. In 2010, CMHC leadership arranged for a farmers market to operate on site on a weekly basis between July and October. The market is made accessible to clients not simply through proximity and convenience, but also through an arrangement whereby SNAP benefits (food stamps) can be doubled when purchasing produce ($2 of produce for every $1 of SNAP paid), and also through integrating distribution of farmers market vouchers into existing incentive programs at the Center. Building on this first step in establishing its commitment to helping clients access healthy and affordable food and desiring to change its inpatient and retail cafeteria food service, CMHC leadership then hired a consulting firm, Fresh Advantage LLC to develop an institutional food policy and a multi-faceted master plan to guide the change process. The master plan recommended redesign of the existing on-site retail cafeteria and dining space, including construction of a full scale commercial kitchen that would also be used for onsite preparation and serving of meals for the small inpatient unit (this unit had up until that point had meal service provided by the general hospital located across the street). The plan also provided for a competitive procurement process to bring a qualified food service management company to manage the entire operation. The master plan also recommended providing educational, programmatic and clinical activities to address the nutritional needs of CMHC patients, including the creation of an onsite culinary garden and a community garden close to the center, with opportunities for patients to explore and learn in both spaces. In 2013, after the plan had been finalized, members of the Fresh Advantage team, including a project leader, consulting chef and nutritionist, were hired to put the plan into practice. In order to promote the cultural change needed to fully realize the food systems transformation, the project team began by hosting a series of food tasting and educational activities on site for clients, staff and faculty. Symposia (e.g., Hunger as a Health Issue ) and lectures by prominent authors were organized, including Michael Moss, author of Salt, Sugar, Fat (Moss, 2013); Daphne Miller MD, author of The Jungle Effect and Farmacology (Miller, 2009; Miller, 2013), and Drew Ramsey, MD, author of The Happiness Diet and 50 Shades of Kale (Drew, 2013; Graham & Drew, 2012). In 2014, while construction and the procurement process were underway, work began on realizing CMHC s longterm goal of providing individual nutritional counseling to every patient at CMHC who desired it. Given resource constraints CMHC leadership and the project team decided to pilot an individual nutritional counseling program as a service of the on-site Wellness Center (a primary care clinic of a local federally qualified health center that CMHC ~ 80 ~
81 clients may choose to use for co-occurring medical needs). While this decision limited the numbers of ambulatory patients who could participate in the pilot, it housed the service where clients were receiving their primary care, ensuring strong linkage to treatment for their physical health conditions and tracking of outcomes. Oversight by the supervising physician (boarded in internal medicine and psychiatry) provided additional support to the nutritionist and primary care provider. Once referral, medical records, logistical and other administrative systems were put place the project team nutritionist was able to coordinate client care with the APRN/primary care provider and supervising physician, and to access laboratory data and client medical records. The referral process enabled the primary care provider to identify patients with diet-sensitive medical conditions that could be better managed with nutritional counseling and improved diet and then offer the nutritional counseling to them. Referral, screening and assessment forms were developed collaboratively with the primary care center staff, supervising physician-nutritionist and project leader, then submitted and approved to the medical records committee. The assessment forms include screening for food insecurity using two USDA validated questions. Cooking and food shopping habits along with food dairies were also assessed. Peer health navigators in the clinic supported clients with respect to scheduling and keeping of appointments with the nutritionist. Within a short time, the nutritional counseling sessions revealed low to very low food security (as defined by the USDA), lack of basic cooking skills and equipment, erratic patterns of meal consumption and significant barriers to accessing nutritious and affordable foods due to poverty. This combination of features of life circumstances made it difficult, if not impossible, for clients receiving the counseling to act on the learning gained in their sessions. It also gave rise to the second additional component of the comprehensive food system initiative plan: the Better Eaters Club. Better Eaters Club Program The Better Eaters Club was designed consistent with the Community Support Programs ( CSP ) model originally developed in 1977 by the National Institute for Mental Health for individuals with persistent and serious psychiatric illness (Turner J, 1978). Consistent with the CSP principles of rehabilitation, recovery, and integration into the community, the curriculum was also informed by the prior experience of the consulting chef and Project Leader in developing food learning curricula for at risk youth and their families and cancer survivors who are also nutritionally deficient due to their specific life circumstances. Importantly, as a skill-building program, the service is a Medicaid billable activity. With the consulting chef taking the lead, a six-session curriculum was developed through an interdisciplinary process that included input from occupational therapists in the outpatient rehabilitation department at CMHC, a social anthropologist in the Department of Psychiatry with expertise in promoting financial health and skill building among CMHC clients living in poverty, and peers involved in the nutritional counseling program. The curriculum takes into account the environments in which people live, including local access to affordable, healthy food ingredients, income constraints, and access to cooking facilities and equipment. The Better Eaters club was piloted in early 2015 with a cohort of six clients who had been referred by the nutritionist and were receiving ongoing individual nutritional counseling from her. The approach is highly interactive, offering a group learning experience with the goal of empowering clients living in the community to meet their basic nutritional needs and to experience the psycho-social benefits that can accompany preparation of and sharing meals. The format of each session is consistent, with preparation and sharing of a recipe/meal forming the core of the session. Each session includes the following components: i) sign in/set up, including overview of session, tasks and prep, discussion of group and individual goals; ii) preparation of food item; teaching of culinary skills and the simple equipment necessary (knife, vegetable peeler, cutting board) to prepare the item; discussion of topic of the day using the food item prepared as a guide; and iii) debrief, the take away of the day, discussion of what was done best as a group, what can we improve, and establishing a goal for the next session. Many recipes prepared are taken from the Good and Cheap: Eat Well on $4 a Day cookbook by Leanne ~ 81 ~
82 Brown (Brown, 2015). Each participant is provided with a copy of the cookbook, along with a backpack for food shopping, and notebooks for keeping handouts and notes. The topic order of the six-week series is as follows, with each session being a complete learning experience in and of itself, not conditional upon participation at each preceding session although attendance at all is strongly encouraged and optimal: Better Eaters Club 1.0 curriculum Session One: The Best Snacks: Make simple to prepare, delicious and nutrient dense foods that are fulfilling and help counteract hunger surges associated with psychoactive medications. Session Two: How to Build Your Pantry: What, how, when and where to buy key staple items to create multiple meals with a limited variety of high quality foods. Session Three: Create your Food Budget: Use monthly income, benefits and community resources to meet dietary needs. Session Four: Community Shopping Field Trip: Find the best places for quality foods at affordable prices, and recognize the value of a shopping list Session Five: Food Safety: What labels and expiration dates really mean. Prepare a meal from the mock pantry to facilitate understanding of food safety practices for animal proteins, fish and dairy. Save scraps and avoid food waste. Session Six: Celebratory meal: Prepare and enjoy a meal together, with participants their choice of menu. Raffle of special culinary gift basket, an incentive announced at the outset of the series. Better Eaters Club Experiences to Date While the Better Eaters club as an element of the organization wide food transformation initiative is a work in progress, many benefits have already been observed. Participants were extremely enthusiastic and excited about the class, both in anticipation of what they would learn, and after learning it. As one client put it after one class, you two [the chef and the nutritionist] were like a big sink of water and we were the sponges. She said of the chef Chef Anne didn t just go to cooking school, she has a gift. During the sessions, particularly when they were actively engaged in food preparation and cooking, the atmosphere was one of joy and serenity. The clients said that when they were engaged in the task at hand, their minds were at rest. One client said to the chef, as she chopped carrots my voices are telling me that they like you. There was a strong sense of community, of belonging, and of coming together on a joint endeavor. The staff involved in the program not only teach cooking skills, but also help participants overcome fears or other anxieties associated with food and its preparation. During the sessions, participants expressed these doubts and fears. Some were nervous about using the knife, others expressed a lack of confidence about experimenting with recipes, and some were concerned about particular ingredients. When participants expressed their concerns, staff reassured them, and also took the opportunity to use the moment to discuss broader food issues. For example, one participant expressed concern about the amount of salt she saw going into the food, worrying that it might be unhealthy. The chef reassured her that she was using a healthy quantity of salt that would heighten the flavors of the dish, making it more balanced and delicious, and that they would feel more satisfied after they had finished eating. She then took the opportunity to start a conversation about fast food, explaining that the amount of salt she was adding was minimal compared to the amount of salt in processed or fast food, which surprised all the participants present. Over time, clients noted that they were beginning to apply what they were learning at home eating smaller portions, ~ 82 ~
83 choosing healthier ingredients, and exercising more. The confidence they gained in the teaching kitchen was translated into their daily lives where they began to experiment with new foods and coached their peers in food matters. One participant said, My eating habits have changed. Rather than a daily bagel I have only had 2 or 3 since I last met with [the nutritionist]. Another explained I eat when I m hungry, more quality foods, and I always cook my food so I know what is in it. One participant said that he was not eating at night so frequently, a problem that had plagued him as a result of his medication. They also spoke of purchasing ingredients they had never bought before, based on what they had learned in class, starting to grow fresh herbs at home, and shopping at farmers markets. One client told us, When I was working at Wendy s, kale was just a decoration on the salad bar, a garnish. Now I can t get enough of it. Yet another client exclaimed, I never knew something without meat could taste so good. The mix of facilitators was well received by participants. They appreciated the nutritionist s detailed knowledge about the chemical make up of food, and the chef s skill, carrying the lessons they learned from her to their own kitchens. As one participant put it, I hear Chef Anne s voice while I m cooking, instructing me or telling me not to do something! One participant said You all bring your own perspective to the group, you are all very supportive. Integrating discussions about finances into the sessions was helpful, especially when coupled with use of the mock pantry so clients could learn how to get through the month using inexpensive kitchen staples. Participants were happy to share their own specific financial situations, and shared experiences and strategies that they used to afford groceries on very limited budgets. The chef and the financial health specialist worked together to ensure that the recipes being taught were within the financial constraints of most participants (most rely on food stamps, a total of approximately $190 per month, or $6 a day). The need for food to be affordable was a theme running through all the sessions; in discussions about balanced meals, for example, the chef would explain that even a small portion of a high quality protein such as fish was worth preparing, alongside large portions of vegetables to fill the stomach. During the shopping trip there was an emphasis on affordability, with participants comparing the cost of different items at different stores. Many were surprised that many items were cheaper at a health food store, rather than from the supermarket that they usually shopped at. One client said I didn t know I could eat healthy on my budget, now I know it s possible. A number of participants organized one-on-one financial counseling sessions separately from the Better Eaters Club meetings upon hearing that the financial specialist offered such counseling, to follow up on financial issues discussed during the class. One participant took advantage of those financial counseling sessions to support her realization of a long-held dream of becoming a chef, by starting a savings plan to enroll in culinary school. There is currently no process in place for formal evaluation of the Better Eaters Club, since the pilot was developed to first develop and test the organizational logistics associated with offering and sustaining the program within CMHC and the appeal and ease of delivery of the curriculum, given reliance on institutional resources (space, transportation to venues for certain sessions, peer support to facilitate attendance). However, all clients participating in the Better Eaters Club pilot to date are also participating in one-on-one counseling, and their health data is tracked as part of the counseling process. The profile below in figure one demonstrates the impact that the interventions in combination can have on individuals who are able to participate in both consistently. Figure One: A Client Profile: Impact of Combined Individual Nutritional Counseling and the Better Eaters Club Joe, a 49 year-old male client of the CMHC Wellness Center was referred in October 2014 by his primary care provider to the nutritionist with several conditions that could be improved with counseling, including: GERD Hyperlipidemia Pre-diabetes ~ 83 ~
84 Sleep Apnea Dermatitis The nutritionist provided a food prescription to the client including changes to his current diet, educated him regarding portion sizes and referred him to the Better Eaters Club. He was asked to revisit the nutritionist every 2 months, in addition to informal check-ins at the Better Eaters club (when the nutritionist was present at the sessions). The client continued to meet regularly with the nutritionist and over a period of nine months, lost 21 pounds and sustained reductions in his blood sugar non-fasting, cholesterol and A (1) C laboratory test values. He also reported improvements in his GERD sleep apnea and dermatitis symptoms As the client put it, regarding his new diet Don t call it a diet because that is something you go off; this is the way I am going to eat for the rest of my life. He then went on to become a peer facilitator in the future sessions of the Better Eaters Club. At the final celebratory session, the first cohort of clients themselves then insisted that a second six-week series be developed, entitled Better Eaters Club 2.0. With their input, the consulting chef and team created a second curriculum and all clients who participated in the 1.0 series participated in six more sessions addressing the following topics: Better Eaters Club 2.0 curriculum Session One: The Five Tastes: Explore your palate, and understand why a balanced plate is important. Address cravings and achieve healthy satiety. Session Two: Virtual Shopping Using the Mock Pantry: The importance of meal planning and preparation, using shopping lists, budgeting, and prioritizing nutritious foods. Session Three: Recipe Reading: Improvise, find healthier alternatives, and how to use seasonings. Use recipes as suggestions. Session Four: Food Myths and Common Misconceptions: Understand the difference between good and bad sugars, and the impact of sugar on physiology. Understand what natural foods are. Address personal food fears. Manage cholesterol and diabetes. Session Five: Meal Planning and Shopping Trip: Plan and shop for meal to be Prepared Following Week. Review food storage, food safety, and product shelf life. Session Six: Celebratory Community Lunch: Prepare and eat a meal together, with menu items reflective of all five tastes. Challenges and Plans for Better Eaters Club Expansion The Better Eaters club has not been without its challenges. The ideal space for the class would be a teaching kitchen, but no such space existed in the Center. The chef brought portable burners with her to class, but it was not easy to find a space at the Center where these burners could be safely used. This situation will be remedied in 2016 since funds have now been secured to renovate an underutilized kitchen space on the transitional living patient floor into a full-scale teaching kitchen. While the Better Eaters Club is targeted specifically at low-income people, limited finances remain a problem for some clients. As one client explained, when she was asked if she had ever eaten hummus (the class had prepared ~ 84 ~
85 home-made hummus that day, using a food processor), I don t do all that cause I don t got the machines. The same client also mentioned that she did not currently have a working freezer at home, and needed to replace her refrigerator. Another client mentioned how exhausted she got carrying her grocery bags full of shopping to her home. Clients told use that they found the prices to be higher at grocery stores at the beginning of the month, right when they need to replenish their supplies (we have no evidence that this is indeed the case, but clients clearly find it difficult and stressful to afford to buy the ingredients they need). Attendance became a problem when Better Eaters Club 1.0 was offered for the second time, to a new group of Wellness Center clients referred by the nutritionist. The initial group of students remained extremely enthusiastic, having advocated for Better Eaters Club 2.0, and taking on peer worker positions for the subsequent class series to support the facilitators. The second cohort was more difficult to recruit, partly due to a fairly onerous referral process, and an inadequate marketing strategy. Those who did join the group did not always attend regularly. Recognizing the complex lives of many clients, the facilitators worked to support their regular attendance. A peer led reminder system was established, whereby a peer worker would call participants the day before to remind them about class and check that they planned to attend. The Center is committed to continuing the classes, and is opening the Better Eaters Club to all CMHC ambulatory clients (not just those receiving care in the Wellness Center) by working directly with the clinical teams that provide mental health care and creating a simple referral process. The club is also developing a marketing and communications strategy with support from those CMHC departments to ensure that all clients and clinicians know about the benefits and enjoyment that can be gained from participation in the Better Eaters Club. An evaluation mechanism that builds upon the qualitative data gathered to date will be put in place, tracking not only participants health indicators (for those who agree to provide this information) but also their subjective perceptions of how participation in the club may have affected their knowledge of food issues, and their cooking and eating habits. As the program develops, we will continue to learn from our experiences, and adapt and innovate accordingly to ensure that we are reaching as wide a group of clients as possible with an effective and meaningful program. Conclusion We know that people with mental health problems struggle more than others to achieve good physical health, we know there is a connection between physical health and diet, and we know that people who are poor are more likely to have unhealthy diets. The Better Eaters Club targets all of these inter-related problems, by providing low-income people with mental illness with hands-on education about nutrition and food preparation that takes into consideration the financial constraints within which they live. Importantly, the changes that the Better Eaters Club aims to effect are supported by the wider clinical context in which the classes take place. Throughout CMHC there is a visible and explicit recognition of the importance of healthy food and nutrition, in the form of the well-appointed, professionally run cafeteria that serves healthy meal options, the weekly farmers market, the onsite culinary garden, and regular events relating to food, nutrition and the wider food system. All of these components of CMHC s food transformation plan buttress one another, as part of the overall mission of providing truly holistic mental health care. Funding and Support The CMHC Food System Transformation initiative is funded by the State of Connecticut Department of Mental Health and Addiction Services and the CMHC Foundation, which provides support for innovative pilot programs at CMHC. The Wellness Center at CMHC is funded by a grant from the Health and Human Services Administration/SAMHSA. ~ 85 ~
86 References Allison, D. B., Mentore, J. L., Heo, M., Chandler, L. P., Cappelleri, J. C., Infante, M. C., & Weiden, P. J. (1999). Antipsychoticinduced weight gain: A comprehensive research synthesis. The American Journal of Psychiatry, 156(11), doi: /ajp [doi] Brown, L. (2015). Good and cheap. eat well on $4 a day Workman Publishing Company. Compton, M. T., & Shim, R. S. (Eds.). (2015). The social determinants of mental health. Washington DC, London England.: American Psychiatric Publishing. Compton, M. T., Daumit, G. L., & Druss, B. G. (2006). Cigarette smoking and overweight/obesity among individuals with serious mental illnesses: A preventive perspective. Harvard Review of Psychiatry, 14(4) Retrieved from Darmon, N., & Drewnowski, A. (2008). Does social class predict diet quality? The American Journal of Clinical Nutrition, 87(5), Davidson, L. (2003). Eliciting narratives. In L. Davidson (Ed.), Living outside mental illness: Qualitative studies of recovery in schizophrenia (qualitative studies in psychology series) (pp ). New York: NYU Press. De Hert, M., Cohen, D., Bobes, J., Cetkovich-Bakmas, M., Leucht, S., Ndetei, D. M.,... Correll, C. U. (2011). Physical illness in patients with severe mental disorders. II. barriers to care, monitoring and treatment guidelines, plus recommendations at the system and individual level. World Psychiatry : Official Journal of the World Psychiatric Association (WPA), 10(2), Dipasquale, S., Pariante, C. M., Dazzan, P., Aguglia, E., McGuire, P., & Mondelli, V. (2013). The dietary pattern of patients with schizophrenia: A systematic review. Journal of Psychiatric Research, 47(2), doi: /j.jpsychires [doi] Drew, R. (2013). Fifty shades of kale: 50 fresh and satisfying recipes that are bound to please Harper Wave. Folsom, D. P., Hawthorne, W., Lindamer, L., Gilmer, T., Bailey, A., Golshan, S.,... Jeste, D. V. (2005). Prevalence and risk factors for homelessness and utilization of mental health services among 10,340 patients with serious mental illness in a large public mental health system. The American Journal of Psychiatry, 162(2), doi:162/2/370 [pii] Graham, T., & Drew, R. (2012). The happiness diet: A nutritional prescription for a sharp brain, balanced mood, and lean, energized body Rodale. Mancini, M. A. (2007). The role of self efficacy in recovery from serious psychiatric disabilities: A qualitative study with fifteen psychiatric survivors. Qualitative Social Work, 6(1), doi: / McCreadie, R. G., & Scottish Schizophrenia Lifestyle Group. (2003). Diet, smoking and cardiovascular risk in people with schizophrenia: Descriptive study. The British Journal of Psychiatry : The Journal of Mental Science, 183, McDonald, K. E., Conroy, N., E., Morris, M., & Jennings, E. (2015). Banking status and financial behaviors of adults with disabilities; findings from the 2013 FDIC national survey of unbanked and underbanked households. ().National Disability Institute. Melanson, K. J. (2007). Nutrition review: Relationships of nutrition with depression and anxiety. American Journal of Lifestyle Medicine, 1(3), doi: / Miller, D. (2009). The jungle effect. the healthiest diets from around the world; why they work and how to make them work for you William Morrow Paperbacks. Miller, D. (2013). Farmacology. total health from the ground up William Morrow Publishing. ~ 86 ~
87 Moss, M. (2013). Salt, sugar, fat: How the food giants hooked us (1st ed.). New York: Random House. Substance Abuse and Mental Health Services Administration. (2004). US department of health and human services; National consensus statement on mental health recovery. Rockville, MD. Retrieved from Turner J, T. W. (1978). The NIMH community support program: Pilot approach to a needed social reform. Schizophrenia Bulletin, 4, Wunderlich, G. S., & Norwood, J. L. (Eds.). (2006). Food insecurity and hunger in the united states: An assessment of the measure, panel to review the U.S. department of agriculture s measurement of food insecurity and hunger. Washington, D.C.: The National Academies Press. ~ 87 ~
88 Adherence issues to antipsychotic medication in schizophrenia: results from a Hong Kong survey targeted for psychiatrists and case managers Dr. Ki-Yan Mak1, MBBS, DPM, MHA, MD, FHKCPsy, FRCPsy, FHKAM(Psy) Dr. William Tak-Lam Lo2, MBBS, FRCPsy, FHKCPsy, FHKAM(Psy) Dr. Wai-Song Yeung3, MBBS, MPhil, MRCPsy, FHKAM(Psy) Dr. Michael Wong4, MBBS, MRCPsy, FHKCPsy Dr. Dicky Wai-Sau Chung5, MBChB, MSocSc, MRCPsy, FHKCPsy, FHKAM(Psy) Dr. Eileena Chui4, MBBS, FHKCPsy, FHKAM(Psy) Dr. Ka-Lok Tam6, FHKCPsy, FHKAM(Psy) Ms. Jolene Mui7, MSc, RN(Psy), RMN, CPN, CFT Ms. Oi-Wah Chan8, BSc (Hons), MSc (LSHTM), RMN Mr. Kwong-Lui Wong4, MSc (Counselling) 1 Room 704, Alliance Building, Hong Kong 2 Kwai Chung Hospital, Kwai Chung, Hong Kong 3 Department of Psychiatry, Pamela Youde Nethersole Eastern Hospital, Hong Kong 4 Department of Psychiatry, Queen Mary Hospital, Hong Kong 5 Tai Po Hospital, Hong Kong 6 Department of Psychiatry, United Christian Hospital, Hong Kong 7 Castle Peak Hospital, Hong Kong 8 Hong Kong Hospital Authority, Hong Kong Citation: Mak K, Lo W, Yeung W, Wong M, Chung D, Chui E, Tam K, Mui J, Chan O, & Wong K. (2016) Adherence issues to antipsychotic medication in schizophrenia: results from a Hong Kong survey targeted for psychiatrists and case managers International Journal of Psychosocial Rehabilitation. Vol 20 (1) Corresponding Author: Ki-Yan Mak, Room 704, Alliance Building, Connaught Road Central, Hong Kong. danielkymak@gmail.com Abstract Objective: The overall level of adherence of Hong Kong patients with schizophrenia is relatively unknown, and this report therefore aims to investigate the attitude of local patients towards antipsychotics, to hopefully assist future development of ~ 88 ~
89 potential strategies to address adherence problems. Methods: A survey consisting of adherence-related questions in schizophrenia was given to 71 psychiatrists and 143 case managers in Hong Kong. Survey results were summarised descriptively, and percentages for each multiple choice answer picked for each question were calculated. Results: Over half of the surveyees estimated that their patients were either partially or non-adherent with their antipsychotic medication during the past month. The three major barriers to patient recovery and improved functioning were medication non-adherence (93%), followed by loss of insight into illness (85%), and lack of integrated psychosocial support (45%). A large proportion of patients did not understand the risk of relapse due to non-adherence and showed lack of insight into illness. Conclusion: Our findings provide a glimpse of the adherence issues and perceptions of local healthcare providers regarding medication taking behaviours of local patients with schizophrenia. Further studies are required to examine the factors behind treatment non-adherence. Keywords: Schizophrenia, adherence, antipsychotics, psychiatrists, case managers, survey, Hong Kong Introduction: Non-adherence is a major issue in the management of schizophrenia (Masand, Roca, Turner, & Kane, 2009). It has been estimated that about 40% of patients with schizophrenia are non-adherent to antipsychotic medication (Freudenreich & Cather, 2012), and according to the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study, about three-fourths of schizophrenic patients had discontinued medication within 18 months (Higashi et al., 2013). Non-adherence to treatment can have a negative impact on clinical outcome due to prolonged time to remission, and increase in the risk of relapse, hospitalisation and attempted suicide (Higashi et al., 2013). Reports estimated that the risk of relapse due to non-adherence could be increased by a factor of three to ten, and the risk of suicide and hospitalisation is nearly four times higher in those who are poorly adherent (Gibson, Brand, Burt, Boden, & Benson, 2013, Potkin, Bera, Zubek, & Lau, 2013). Furthermore, non-adherence can aggravate patients social and occupational functioning, resulting in reduced quality of life and increased use of healthcare resources of the society (Dilla, Ciudad, & Álvarez, 2013). A study demonstrated that the 6-month direct cost of care for relapsed patients with schizophrenia was four times higher than for those without relapse (Munro et al., 2011), indicating that non-adherence can have significant economic consequences since it is strongly associated with relapse of schizophrenia (Dilla et al., 2013). Reasons for non-adherence are complex, including personal factors such as poor insight, health beliefs such as refusal of medication, and drug factors such as poor efficacy, drug-related side effects, medication interference with life goals, complicated treatment regimen, as well as social factors such as embarrassment/stigma over illness and lack of social support (Potkin et al., 2013, Smeraldi et al., 2013). Identifying determinants and risk factors of non-adherence in schizophrenia helps address the adherence issues, and is essential in improving patient welfare and reducing utilisation of social resources and cost of care. In Hong Kong, patient attitude towards antipsychotics and the overall level of adherence are rarely reported, and these topics therefore warrant investigation in order to provide insights on how to improve the overall management of schizophrenia. In view of this, the Hong Kong Association of Psychosocial Rehabilitation (HKAPR) conducted a survey to gather opinions from local healthcare professionals (HCPs) including psychiatrists and case managers regarding the adherence issues in the local management of schizophrenia. The survey was based on the one developed by the Spanish Adherencia Terapéutica en la Esquizofrenia (ADHES) program (translated as: therapeutic adherence in schizophrenia), which was first conducted in Spain, and was later adopted in the rest of Europe, Middle East and Africa (Olivares et al., 2013). The goal of the current study was to make use of the survey results to advise a list of follow-up actions in order to improve local services for patients with schizophrenia. ~ 89 ~
90 Method Sampling ADHES (Activities, Delivering Hope, Empowerment & Success) is a large international initiative to assess patients adherence to treatment, with an aim to raise awareness of partial/non-adherence issues in treating mental illness (Olivares et al., 2013). The current study adopted the ADHES survey but was modified for the local context. In brief, the ADHES survey targets HCPs and consists of questions relating to their perceptions of reasons/factors that affect the level of adherence of their patients (Olivares et al., 2013). The survey together with a letter explaining its objectives was handed out individually to local psychiatrists and case managers in Hong Kong through convenient sampling during January to April 2014, and each completed survey was collected later for data analysis. Data collection and analysis The completion of the survey was anonymous and voluntary. All raw data collected were kept confidential and patients personal information was not collected. The survey consisted of one question regarding the professional qualification of the surveyee (Table 1; Q1), and 9 multiple choice questions related to the adherence issues of schizophrenia (Table 1; Q2-Q10). Level of adherence of patients was assessed by estimating the percentage of prescribed doses that they took during the past month: adherent, partially adherent, and non-adherent was defined as taking 90% of prescribed doses, taking 30 to <90% of prescribed doses, and taking <30% of prescribed doses respectively (Olivares et al., 2013). Regarding factors contributing to partial or non-adherence, surveyees were instructed to estimate some responses based on the percentage of patients falling into each of three groupings (i.e. <20%, 20% 50%, and >50% of patients) (Olivares et al., 2013). After collection of the completed surveys, the survey response data were summarised descriptively, and percentages for each multiple choice answer picked for each question were calculated. No other statistical testing was performed, and the data were not weighted. Results A total of 71 psychiatrists and 143 case managers completed and returned the survey, representing a sizeable proportion of overall personnel in the field of psychiatry in Hong Kong. According to the responses from psychiatrists, the three major barriers to patient recovery and improved functioning were medication non-adherence (93%), followed by loss of insight into illness (85%), and lack of integrated psychosocial support (45%). Although case managers also agreed with the aforementioned three factors as major barriers (81%, 72% and 34%, respectively), they also considered stigma and cultural attitudes as one of the major barriers to clinical outcome (34%). On the other hand, 13% of psychiatrists agreed that stigma and cultural attitudes was impeding clinical outcome (Figure 1). ~ 90 ~
91 The difference in valuing stigma and cultural attitudes between psychiatrists and case managers may be due to the notion that patients are more willing to share their daily experience with case managers, allowing case managers to have a better grasp of patients attitude and thoughts towards their illness. Nonetheless, further studies are required to elucidate the major barriers to patient recovery and improved functioning. Respectively, over half of the surveyees (Psychiatrists: 60%; Case managers: 52%) estimated that their patients with schizophrenia were either partially (took at least 30% but no more than 90% of prescribed doses) or nonadherent (took <30% of prescribed doses) with their antipsychotic medication during the past month (Figure 2). Adherence remains an important issue that needs to be addressed in the management of schizophrenia. HCPs are advised to emphasise the importance of adherence to their patients. For assessing medication adherence, most surveyees adopted the direct inquiry method such as ask the patient explicitly (Psychiatrists: 76%; Case managers: 61%) or ask an informant (e.g. relative, friend, caregiver) (Psychiatrists: 19%; Case managers: 24%). Results reflected that up to about two thirds of surveyees had adopted objective approaches such as drug plasma levels or pill counting to assess adherence (Figure 3), but these objective approaches were not as frequently used as compared with subjective approaches. While pill counting represented the most used objective approach for case managers (10%), only 1% of psychiatrists frequently adopted this method to assess adherence. ~ 91 ~
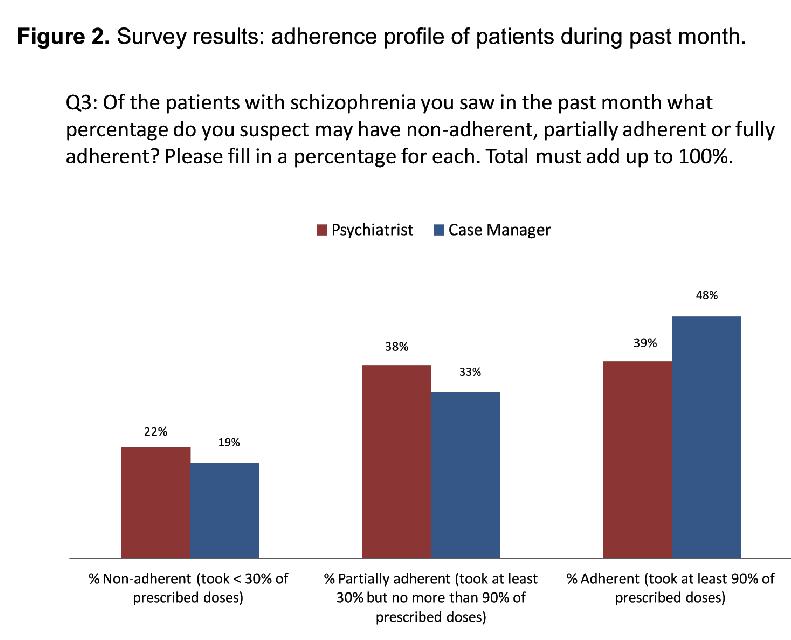
92 ~ 92 ~

93 The more frequent use of pill counting by case managers suggests that they rely on practical means to assess adherence, as they may not be as experienced/knowledgeable as psychiatrists who can depend on other means to assess adherence. Ninety two percent of psychiatrists versus 66% of case managers assessed adherence at every visit, while 27% of case managers versus 6% of psychiatrists assessed adherence every 2-3 visits (Figure 4). More than half of the surveyees (Psychiatrists: 58%; Case managers: 51%) spent 10-25% of their time staying with patients on reminding/ensuring them to take their medication as prescribed (Figure 5). Adherence is assessed in almost all patients although the frequency of assessment can vary among HCPs. HCPs should be reminded that not all patients show great insight into their illness, and therefore it is necessary for them to spend more time to remind their patients to take medication. ~ 93 ~
94 At least two thirds of the surveyees (66-77%) reported that 50% of their patients understood the risk of relapse if they failed to take their medication regularly. On the other hand, a larger portion of psychiatrists as compared with case managers (34% vs. 21% respectively) believed that >50% of patients understood the po- ~ 94 ~
95 tential risk (Figure 6). A large proportion of patients do not understand the risk of relapse due to non-adherence. HCPs may need to spend more time explaining the harm of non-adherence to their patients. The difference in percentage (34% vs. 21%) may suggest that psychiatrists are more aware of patients understanding of their illness. About 70% of the surveyees noticed that 50% of their patients showed some lack of insight into their illness during the past month, while the proportion of surveyees markedly reduced to about 30% for those who found that >50% of patients showing lack of insight. No apparent difference in opinions between psychiatrists and case managers can be found in terms of assessing patients insight (Figure 7). A large proportion of patients (about one third) show lack of insight which may affect their medication taking behaviours and their recovery. HCPs need to explain the nature of the illness including diagnosis, treatment and prevention to their patients. More patient education programmes are needed in the community, and it is a long path for patients with schizophrenia to fully understand their illness. A survey targeted for patients may be needed to further elucidate their medication taking behaviours. ~ 95 ~
96 Approximately 40-50% of surveyees reflected that <20%/between 20-50% of their patients stopped taking their medication when feeling better. It is noteworthy that the proportion of psychiatrists was more than double the proportion of case managers in feeling that their patients stopped taking their medication upon feeling better (Figure 8). There are still patients who do not take medications as prescribed. HCPs need to be aware of those who stop their medication prematurely, as their risk of relapse may increase as a result. ~ 96 ~
97 Almost all psychiatrists (98%) believed that 50% of their patients stopped taking their medication due to undesirable side effects in the past month, compared to 90% of case managers having the same thought (Figure 9). Side effects may not be the main reason of non-adherence. HCPs are advised to explore the main reasons behind non-adherence in order to improve adherence rate. Nonetheless, the percentage of overall patients who stopped taking their medication needs to be factored before making any conclusion. In addition, some patients may not completely stop their medication (i.e. become partially adherent) after experiencing side effects, and this situation also needs to be considered. Lastly, how HCPs determine the true adherence rate remains to be questioned. ~ 97 ~
98 Discussion The current study adopted the ADHES schizophrenia survey to gain insights into the general medication adherence issues in schizophrenia in Hong Kong, including the scope and causes of non-adherence, as well as the methods of assessing adherence by HCPs. The survey was distributed to local psychiatrists and case managers including nurses. The two professional sectors are considered different in terms of educational background, practice habits and clinical experience. The demographics such as the sex and age of surveyees were also not recorded. Indeed, there was a discrepancy of opinions between psychiatrists and case managers, suggesting a difference in their understanding of adherence issues in schizophrenia. The most noticeable discrepancy included the belief of case managers that stigma was a top three barrier to patient recovery and improved functioning but not psychiatrists. The use of objective approaches to assess adherence (such as pill counting, drug plasma level measurement, adherence assessment scales) was also more frequently adopted by case managers than by psychiatrists, and psychiatrists appeared to assess adherence more regularly when compared with case managers. Whether the differences in practice habits between psychiatrists and case managers induce a difference in patients clinical outcome remain of interest and may require further investigation. Nonetheless, there are some major issues relating to the local management of schizophrenia that can be derived from the survey, and the details are discussed below. Lack of treatment adherence Between 52-60% of surveyees considered that their patients with schizophrenia were partially/non-adherent to their antipsychotic medication in the past month, and these results were consistent in a previous ADHES schizophrenia survey conducted in Asia Pacific countries, which found that 56% of patients with schizophrenia were partially or non-adherent to their medication (Olivares et al., 2013). The relatively high rate of poor adherence reported in this survey is alarming and needs to be addressed, as treatment adherence is essential for patients to achieve clinical remission (Masand et al., 2009). It is also noteworthy that adherence assessment by clinical judgment often results in underestimated rates (Olivares et al., 2013), and so partial/non-adherence in local patients remains a tough problem to tackle. The survey results indicated that the top barrier to patient recovery and improved functioning was medication non-adherence, followed by loss of insight into illness ~ 98 ~
99 and lack of integrated psychosocial support. In particular, medication non-adherence and loss of insight into illness can be considered as major factors as over 50% of surveyees (both psychiatrists and case managers) thought that these 2 factors impeded patient recovery. Over 90% of psychiatrists believed that not adhering to treatment has a major impact on achieving remission. Since non-adherence sign According to previous reports, using a combination of assertive community treatment, family involvement and social skills training (Barkhof, Meijer, de Sonneville, Linszen, & de Haan, 2012), as well as long-acting injectable atypical antipsychotics (LAIs) with fewer side effects as opposed to conventional antipsychotics can be possible solutions to address the problem of poor adherence (Kaplan, Casoy, & Zummo, 2013, Smeraldi et al., 2013). In particular, LAIs can promote face-to-face contact time between HCPs and patients, as injection is required to be administered at the clinics/hospitals (Smeraldi et al., 2013). The increased contact time may contribute to improved therapeutic alliance that may help enhance treatment adherence and symptom control (Johansen, Iversen, Melle, & Hestad, 2013). Indeed, it has been reported that patients on LAIs were at least twice as likely to stay on their treatment courses as compared with those on oral antipsychotics (Kaplan et al., 2013). Lack of insight Denial and lack of insight into illness was also considered a major barrier to remission. To address the conceptual issue of insight, accurate and up-to-date information regarding the nature and management of schizophrenia need to be provided for patients. Compliance therapy may also be considered as an effective intervention in improving insight and attitudes to illness (Chakraborty & Basu, 2010). The lack of integrated psychosocial support as noted by the surveyees suggested that it is important to explore ways to improve psychotherapy services in order to help patients overcome dysfunction and regain their lives and abilities. For instance, supportive therapy can be beneficial to patients by providing positive advice and efforts to minimise stress (Penn et al., 2004). Caregivers (such as family members and friends) and peer groups are also recommended to provide support and encouragement to those with schizophrenia. Indeed, recent evidence advocated the concept of an enhanced team-oriented approach to manage patients with schizophrenia in order to improve clinical outcome (Shuler, 2014). It is interesting to note that about one third of case managers believed that stigma and cultural attitudes are major barriers to patient recovery and improved functioning, as opposed to only 13% of psychiatrists who had this belief. Reasons behind this difference in opinions are unknown, but the results implied that positive attitudes towards mental illness are important in promoting patient recovery. Difference in assessing adherence The most common approach in assessing adherence was by using subjective methods, such as asking the patient or informant directly. However, subjective approaches are often not validated, and are susceptible to error, misinterpretation, or distortion (Velligan et al., 2006). For example, patients may overestimate the extent of adherence in order to avoid queries from their doctors or case managers (Birnbaum & Sharif, 2008). Cognitive dysfunction could also impair patients ability to recall their actions, prohibiting them from providing accurate information regarding their medication taking behaviour (Barkhof et al., 2012). It is noteworthy that while psychiatrists did not prefer the use of objective approaches such as pill count (1%) and drug plasma level measurement (1%), 10% of case managers regarded pill count as the most used approach in assessing adherence. This reflects the different working habits between psychiatrists and case managers. Nonetheless, the survey indicated that objective approaches using drug plasma concentrations, pharmacy records and pill counts were not popular in local practice. To improve the accuracy of adherence assessment, it has been suggested in a clinical review to include at least 2 measures of adherence and at least 1 of these be a direct or objective measure such as pill count, urine analysis, blood analysis, electronic monitoring, pharmacy refill records, or the examination of tracer substances in blood or urine (Velligan et al., 2006). A local validated practical adherence assessment scale which is lacking now may also be helpful. Compared with case managers (66%), more psychiatrists (92%) assessed adherence level during each visit ~ 99 ~
100 with patients. On the other hand, more than one fourth of case managers (27%) reported assessing adherence every 2-3 visits. These results implied that case managers may not be fully aware of the importance of medication adherence, and they should be encouraged to assess adherence more frequently since adherence has a direct impact on patient outcome (Masand et al., 2009). More than half of the surveyees spent 25% of their time staying with patients on reminding/ensuring them to take medication as prescribed. However, as patients seldom fully adhere to treatment (Masand et al., 2009), it is advised that HCPs spend more time and become more proactive in promoting the importance of medication adherence to patients in relation to the risk of relapse. Training manuals may be required to increase the awareness of HCPs in adherence issues and instruct them on how to address such issues with patients. Poor understanding of the consequences of not adhering to treatment In the current study, it was generally agreed by the surveyees that a proportion of their patients showed some lack of insight into their illness and did not understand the risk of relapse if they failed to take their medication regularly. Accurate, up-to-date patient education programmes are recommended to inform patients on the consequences of non-adherence. HCPs should also encourage patients to learn coping skills to help them accept their illness that may in turn help enhance their adherence to treatment (Aldebot & Weisman de Mamani, 2009). Peer group sharing may also be helpful so that patients can learn from others psychotic experiences. Approximately 40% of the surveyees reflected that 20-50% of their patients stopped taking their medication in the past month, either due to improved condition or drug side effects. These findings further suggested that there was still a significant portion of patients who do not understand the importance of taking medication on a consistent basis. To encourage patients to continually take their medicines, psychiatrists could consider prescribing drugs with fewer side effects (such as atypical antipsychotics), especially for late stage patients, in order to further reduce the rate of treatment discontinuation. Limitations of the study Our findings on the antipsychotic adherence issues are based on the clinical experience of a small proportion of local HCPs (~20% of all psychiatrists and case managers in Hong Kong) during their everyday practice, and therefore it is unknown whether the survey results are representative of all HCPs in the field of mental health in Hong Kong. Another limitation of the study is that the demographic characteristics of the surveyees such as age, years of clinical experience, and practice setting were not recorded in details. Nevertheless, our findings provide a glimpse of the prevalence of partial/non-adherence and perceptions of local HCPs regarding the factors that affect medication taking behaviours of patients with schizophrenia. To further understand the implications of non-adherence in the management of schizophrenia, future studies could be conducted to examine other factors affecting adherence (e.g. severity of positive/negative symptoms, attitudes of caregivers such as expressed emotions, financial situation of patients, substance abuse, cultural and religious beliefs, etc.), as well as the usage rate of potential strategies to address adherence problems such as the use of LAIs, cognitive-behavioural therapy, compliance therapy, cognitive adaptation, and psychoeducation (Velligan et al., 2009). Conflict of interest: None. ~ 100 ~
101 References Aldebot, S., & Weisman, de Mamani A. (2009). Denial and acceptance coping styles and medication adherence in schizophrenia. Journal of Nervous and Mental Disease, 197, Barkhof, E., Meijer, C.J., de Sonneville, L.M., Linszen, D.H., & de Haan, L. (2012). Interventions to improve adherence to antipsychotic medication in patients with schizophrenia--a review of the past decade. European Psychiatry, 27, Birnbaum, M., & Sharif, Z. (2008). Medication adherence in schizophrenia: patient perspectives and the clinical utility of paliperidone ER. Patient Preference and Adherence, 2, Chakraborty, K., & Basu, D. (2010). Insight in schizophrenia a comprehensive update. German Journal of Psychiatry, 13, Dilla, T., Ciudad, A., & Álvarez, M. (2013). Systematic review of the economic aspects of nonadherence to antipsychotic medication in patients with schizophrenia. Patient Preference and Adherence, 7, Freudenreich, O., & Cather, C. (2012). Antipsychotic medication nonadherence: risk factors and remedies. Focus (Other), X(2), Gibson, S., Brand, S.L., Burt, S., Boden, Z.V.R., & Benson, O. (2013). Understanding treatment non-adherence in schizophrenia and bipolar disorder: a survey of what service users do and why. BMC Psychiatry, 13, 153. Higashi, K., Medic, G., Littlewood, K.J., Diez, T., Granström, O., & De Hert, M. (2013). Medication adherence in schizophrenia: factors influencing adherence and consequences of nonadherence, a systematic literature review. Therapeutic Advances in Psychopharmacology, 3, Johansen, R., Iversen, V.C., Melle, I., & Hestad, K.A. (2013). Therapeutic alliance in early schizophrenia spectrum disorders: a cross-sectional study. Annals of General Psychiatry, 12, 14. Kaplan, G., Casoy, J., & Zummo, J. (2013). Impact of long-acting injectable antipsychotics on medication adherence and clinical, functional, and economic outcomes of schizophrenia. Patient Preference and Adherence, 7, Masand, P.S., Roca, M., Turner, M.S., & Kane, J.M. (2009). Partial adherence to antipsychotic medication impacts the course of illness in patients with schizophrenia: a review. Primary Care Companion to The Journal of Clinical Psychiatry, 11, Munro, J., Osborne, S., Dearden, L., Pascoe, K., Gauthier, A., & Price, M. (2011). Hospital treatment and management in relapse of schizophrenia in the UK: associated costs. Psychiatric Bulletin, 35, Olivares, J.M., Thirunavukarasu, M., Kulkarni, J., Zhang, H.Y., Zhang, M., & Zhang, F. (2013). Psychiatrists awareness of partial and nonadherence to antipsychotic medication in schizophrenia: results from an Asia-Pacific survey. Neuropsychiatric Disease and Treatment, 9, Penn, D.L., Mueser, K.T., Tarrier, N., Gloege, A., Cather, C., Serrano, D., & Otto, M.W. (2004). Supportive therapy for schizophrenia: possible mechanisms and implications for adjunctive psychosocial treatments. Schizophrenia Bulletin, 30, Potkin, S., Bera, R., Zubek, D., & Lau, G. (2013). Patient and prescriber perspectives on long-acting injectable (LAI) antipsychotics and analysis of in-office discussion regarding LAI treatment for schizophrenia. BMC Psychiatry, 13, 261. Shuler, K.M. (2014). Approaches to improve adherence to pharmacotherapy in patients with schizophrenia. Patient Preference and Adherence, 8, Smeraldi, E., Cavallaro, R., Folnegovic-Šmalc, V., Bidzan, L., Ceylan, M.E., & Schreiner, A. (2013). Long-term remission ~ 101 ~
102 in schizophrenia and schizoaffective disorder: results from the risperidone long-acting injectable versus quetiapine relapse prevention trial (ConstaTRE). Therapeutic Advances in Psychopharmacology, 3, Velligan, D.I., Lam, Y.W., Glahn, D.C., Barrett, J.A., Maples, N.J., Ereshefsky, L., & Miller, A.L. (2006). Defining and assessing adherence to oral antipsychotics: a review of the literature. Schizophrenia Bulletin, 32, Velligan, D.I., Weiden, P.J., Sajatovic, M., Scott, J., Carpenter, D., Ross, R., Docherty, J.P.; Expert Consensus Panel on Adherence Problems in Serious and Persistent Mental Illness. (2009). The expert consensus guideline series: adherence problems in patients with serious and persistent mental illness. Journal of Clinical Psychiatry, 70 Suppl 4, ~ 102 ~

103 Table 1. Survey questions adopted in the current study targeted for local psychiatrists and case managers. ~ 103 ~
104 ~ 104 ~
105 Perceived burden and quality of life in Chinese caregivers of people with serious mental illness: A path analysis Yingchun Zeng1 Ying Zhou2 Jiankui Lin3 1Department of Obstetrics and Gynecology, The Third Affiliated Hospital of Guangzhou Meidcal University, Guangzhou, China. 2School of Nursing, Guangzhou Medical University, Guangzhou, China 3Department of Nursing, Guangzhou Brian Hospital, Guangzhou, China) Citation: Zeng Y, Zhou Y, & Lin J.(2016) Perceived burden and quality of life in Chinese caregivers of people with serious mental illness: A path analysis. International Journal of Psychosocial Rehabilitation. Vol 20 (1) Corresponding Author: Yingchun Zeng, Department of Obstetrics and Gynecology, The Third Affiliated Hospital of Guangzhou Meidcal University No 63 DuoBao Road, Liwan District, Guangzhou, Guangdong Province, China, (chloezengyc@hotmail.co.uk). Abstract Background: In China, family members take on the major responsibility of caring for people with serious mental illness (SMI). Caring for a family member with SMI can result in numerous consequences for the caregiver. The aims of this study were to investigate perceived caregiver burden and quality of life (QOL) among Chinese family caregivers for people with, to assess the role of social support as a mediator between caregiving and QOL, and to test whether the proposed conceptual model can explain the pathway of how caregiving influencing perceived burden and QOL. Methods: In the current cross-sectional study, 231 family caregivers were recruited and independently interviewed using the Chinese version of the WHOQOL-BREF, Hospital Anxiety and Depression Scale, Social Support Rating Scale, and Family Burden Interview Schedule as outcome measures. Results: The path analysis model provided a good fit for the data (χ2 [7] = 13.96, p = 0.052, CFI = 0.910, TLI = 0.875, IFI = 0.912, RMSEA = 0.068), with all individual paths significant at p < Caregiving time spent in SMI patients was re- ~ 105 ~
106 lated directly with family burden. Caregivers depressive symptoms were related directly levels of family burden and QOL. All other significant variables were related indirectly with family burden and QOL, social support plays the role of mediating effects. Conclusions: Study findings show that social support can be regarded not only as a protective factor in reducing the caregiving burden for family caregivers, but also in promoting caregivers QOL. Keywords: Family caregivers; Serious mental illness; Caregiver burden; Quality of life; Path analysis Introduction: Caring for a family member with SMI can result in numerous consequences for the caregiver [1,2]. Caregivers may experience considerable adverse effects on their quality of life (QOL), as well as adverse health effects such as distress [1]. Caregivers could also experience a range of negative emotions, impacting both their physical and mental health [2]. This impact of caregiving has been conceptualized as caregiver burden [2]. Caregiver burden has been associated with caregivers depressive symptoms and inadequate social support [3,4]. Previous research found that insufficient social support was the most significant predictor of caregiver depression, followed by caregiver burden [5]. Chan [6] indicated that social support appears to be an important protective factor in caregiver burden in diverse cultures. This study investigated the mediating role of social support as a major protecting factor, determining the influence of caregiving on caregivers perceived burden and quality of life (QOL). The conceptual model guided this study is illustrated in Fig. 1. The aims of this study were to investigate perceived caregiver burden and QOL among Chinese family caregivers for people with SMI, to assess the role of social support as a mediator between caregiving and QOL, and to test whether the proposed conceptual model can explain the pathway of how caregiving influencing perceived burden and QOL. Methods Subjects The SMI patients who met the following inclusion criteria were invited to participate in the study upon their planned discharge: (1) Chinese adults ages 18 to 65, (2) suffering from schizophrenia and/or other psychotic disorders, using the consensus diagnosis according to DSM-5, and (3) voluntary consent. Eligible family caregivers were recruited on the day of SMI patients discharge from hospital. Caregivers who were interested in participating signed up for the study. Inclusion criteria included (1) caregivers who have spent two hours or more each day looking after the discharged patients; (2) one caregiver per patient; and (3) age 18 or above. Measures Measures included in this study consist of five parts: 1) The Socio-demographic sheet was used to collect participants age, gender, relationship with the patient, marital status, employment status, education level, monthly income, health status, length of time as a caregiver, and average number of hours per week spent caring for the discharged patient; 2) The World Health Organization Quality of Life Brief Form (WHOQOL-BREF) ~ 106 ~
107 (Chinese version) was used to measure the quality of life in subjects; 3) The Hospital Anxiety and Depression Scale (HADS) was used to measure the psychological health of subjects; 4) The Social Support Rating Scale (SSRS) was used to measure social support of subjects; and 5) The Family Burden Interview Schedule (FBIS) was used to assess caregiver burden of subjects. Data collection and analysis This study was approved by studied hospitals Ethics Committee. Written consent was obtained from participants before data collection. Data were collected from May - July Trained research nurses collected the data in face-to-face interviews, on the day of patients discharge from hospital. Data were analyzed using SPSS and AMOS for Windows, version 20. Statistical significance was set at The findings would be summarized by descriptive statistics, correlation and path analysis. Results Subject characteristics A total of 231 family caregivers were recruited in this. Most patients were suffering from schizophrenia or schizophrenia spectrum disorder, while the remaining subjects were experiencing psychotic disorders or major depressive disorders. Participants ages ranged from 18 to 73, with a mean age of (SD=13.18). The detailed characteristics of family caregivers were listed in Table 1. Means of measurement outcomes ~ 107 ~

108 Means of measurement outcomes was listed in Table 2. With regards to QOL by WHOQOL-BREF, caregivers indicated a higher perceived QOL in the domains of environmental and physical health, than in the areas of psychological health and social relationships. Concerning symptom severity by HADS, family caregivers had more severe psychological symptoms of depression, than anxiety-related symptoms. In terms of social support by SSRS, caregivers perceived better subjective support than objective support and support use degree. In terms of a sense of care burden, the most common burden perceived by caregivers was financial. Testing the research model by path analysis Relevant correlation and regression analyses were conducted before performing the path analysis. Only significant ones were kept in the path analysis. As shown in Fig. 2, the model (Fig. 2) provided a good fit for the data (χ2 [7] = 13.96, p = 0.052, CFI = 0.910, TLI = 0.875, IFI = 0.912, RMSEA = 0.068), with all individual paths significant at p < Caregiving time spent in SMI patients was related directly with family burden. Caregivers depressive symptoms were related directly levels of family burden and QOL. All other significant variables were related indirectly with family burden and QOL, social support plays the role of mediating effects. In other words, caregivers age, health status, education levels and anxiety symptoms had no direct relations to family burden and QOL, and social support mediated the effect of caregiving on family burden and QOL. ~ 108 ~

109 Discussion By the path analysis, the severity of depression was negatively associated with caregivers QOL. Previous research reported that Chinese caregivers of people with schizophrenia with higher psychological distress were found to have a higher caregiving burden [7]. Hence, relevant interventions to promote Chinese family caregivers psychological health are urgently required. Additionally, education levels had indirect relation to QOL. Among Chinese community, obtaining a high level of education is valued. To some degree, individuals with an increased education level may often have a greater financial income and better working opportunity. Thus, higher education levels were associated with better QOL among Chinese family caregivers. Another significant indirect relation was weekly hours spent caring for the family member with SMI associated with caregiver burden. Longer hours spent caring for the SMI patient indicate a perception of higher levels of burden, especially for employed caregivers dealing with both work-related issues and providing care for a family member with SMI. Previous research found that many family caregivers had to quit their job or retire early in order to take care of family members with mental illness [8]. Thus, unemployment or early retirement could result in financial difficulties for these family caregivers. Furthermore, health status had indirect effects in family burden and QOL. One would expect that having good health when providing care for a family member with SMI would lead caregivers to experience a lighter burden. Obviously, greater objective demand burden requires family caregivers to put more effort into performing daily assistance activities, supervising patients behaviour and providing financial assistance in caring for SMI patients. In consequence, the QOL of caregivers was significantly affected. Similar to previous research, social support is one of the protective factors when providing care for a family member with schizophrenia [3,6]. This study also found that social support can be regarded not only as a protective factor in reducing the caregiving burden for family caregivers, but also in promoting caregivers QOL. Several study limitations should be taken into account. First, the convenience sampling method limits the generalizability of study findings. Further studies, at multiple sites and across regions, should be conducted. ~ 109 ~
110 Second, this study only recruited stabilized SMI patients, so replications of the current findings among family caregivers for acutely ill and ambulatory SMI patients is necessary. Finally, the current study only reported and assessed study outcomes at a single point in time. In consequence, the causality of relationships between social-demographic variables, caregiver burden and QOL could not be explored. However, this study is ongoing, with a year follow-up to be conducted with these family caregivers for people with SMI. Although this study has several limitations, its findings have important practice implications. Lower levels of social support were a significant protecting factor for higher caregiver burden and lower levels of QOL among Chinese family caregivers of people with SMI. Hence, providing caregiver support (e.g. support from friends or other family members) might prove beneficial. In addition, providing caregivers with knowledge about SMI is essential, since an increase in knowledge about SMI might help reduce caregivers sense of burden [9]. Furthermore, caregivers experienced high levels of depressive symptoms, which negatively influenced their QOL. More services, such as family psycho-education, support groups and individual counselling should be developed, with the goal of improving caregivers psychological health and QOL [7]. Implications for future research include the potential for developing and implementing effective intervention strategies to reduce caregiver burden and improve caregivers QOL. For example, intervention strategies to improve communication between mental health service providers and families should be developed. Health policy makers should provide relevant resources, such as financial assistance with care for family caregivers, and it is important that health policy fully recognizes the role of family caregivers as a healthcare resource in caring for people with SMI [10]. Conclusions Study findings show that social support can be regarded not only as a protective factor in reducing the caregiving burden for family caregivers, but also in promoting caregivers QOL. Source of funding This study was funded by Guangzhou Medical University Fund for Overseas Returners (No.2013C57). References 1. Möller-Leimkühler AM, Wiesheu A: Caregiver burden in chronic mental illness: the role of patient and caregiver characteristics. Eur Arch Psychiatry Clin Neurosci 2012, 262: Vella SL Pai N: The measurement of burden of care in serious mental illness: A qualitative review. Aust N Z J Psychiatry 2013, 47: Chien WT, Chan WC, Morrissey J: The perceived burden among Chinese family caregivers of people with schizophrenia. J Clin Nurs 2007, 16: Perlick DA, Miklowitz DJ, Link BG, Struening E, Kaczynski R, Gonzalez J, Manning LN, Wolff N, Rosenheck RA: Perceived stigma and depression among caregivers of patients with bipolar disorder. Br J Psychiatry 2007, 190: Saunders JC: Families living with severe mental illness: a literature review. Issues Ment Health Nurs 2003, 24: Chan SW: Global Perspective of Burden of Family Caregivers for Persons With Schizophrenia. Arch Psychiatr Nurs 2011, 25: Lam PCW, Ng P, Tori C: Burdens and psychological health of family caregivers of people with schizophrenia in two Chinese metropolitan cities: Hong Kong and Guangzhou. Community Ment Health J 2013, 49: Tsang HWH, Tam PKC, Chan F, Chang WM: Sources of burdens on families of individuals with mental illness. Int J ~ 110 ~
111 Rehabil Res 2003, 26: Li J, Lambert CE, Lambert VA. Predictors of family caregivers burden and quality of life when providing care for a family member with schizophrenia in the People s Republic of China. Nurs Health Sci 2007, 9: MacCourt P: Family Caregivers Advisory Committee, Mental Health Commission of Canada. National Guidelines for a Comprehensive Service System to Support Family Caregivers of Adults with Mental Health Problems and Illnesses. Calgary, AB: Mental Health Commission of Canada; Retrieved from: ~ 111 ~
112 Assessing the Suitability of Clinical Programs for Implementation Tom Bartholomew Joe Birkmann Rutgers University Citation: Bartholomew T & Birkman J. (2016) Assessing the Suitability of Clinical Programs for Implementation International Journal of Psychosocial Rehabilitation. Vol 20 (1) Abstract Mental health organizations looking to implement new clinical programs are faced with an ever-increasing number of options to choose from. Determining which program(s) to implement is often based on a fondness for pet programs and factors such as the availability of vender packages that may have little bearing on the appropriateness of a given program. A nine-dimension rubric is proposed as a way of measuring a program s suitability for implementation. This rubric involves an assessment of a program s: objective(s), efficacy, generalizability, cost benefit profile, opportunity cost(s), fidelity measurement, outcome assessment, feasibility, and three factors related to implementation. These dimensions of suitability are presented as score-able criteria to offer organizations a means to compare and contrast various clinical programs. Programs are scored, ideally first by venders or program advocates, then individually by those charged with making a decision about implementation. Lastly, consensus is sought on scores across the nine-dimension rubric using the measurable anchors. Limitations of this approach are discussed. Future work in this area is recommended. The authors have no financial disclosures or conflicts to report. Introduction: Mental health organizations are charged with evaluating and implementing effective clinical programs for the benefit of their clients. The suitability of programs for implementation is often a complex, context dependent match between programs, organizational characteristics and client s needs (Blase & Fixsen, 2013; Fixsen et al., 2005). Organizations must actively manage their clinical formulary in order to maximize the effective use of limited resources. Historically organizational leadership may have exercised a deferential attitude toward professional degrees and titles, opting for what was essentially the product of a private practice model of service delivery. In this approach practitioners could exercise their professional judgment regarding the interventions that they chose to use (Drake, Merrens & Lynde, 2005) without necessarily considering the organization s needs. This can lead to what Carol Mowbrey (2003) has called black box outcomes in which a professional does something which may or may not have an effect but what was done remains unknown. The consequence ~ 112 ~
113 of this lack of transparency and accountability is that outcomes can be unreliable and clients can and do suffer unnecessary treatment failures. The PORT studies (Leman et al., 2004: Dixon et al., 2010) demonstrate that the majority of mental health organizations in the United States are failing to use practices that have demonstrable effectiveness in favor of private practice approaches that are largely based, not on evidence, but on practitioner preferences. The need for accountability in the provision of programming is becoming more important as payers demand an evidence based clinical formulary in order provide reimbursement (Fox, 2005). In order to assist organizations and practitioners in assessing the suitability of programs for implementation a score-able nine-dimension rubric has been developed. The nine-dimension rubric (see appendix 1) allows for the assessment of a clinical program s suitability for implementation using an anchored five point scale (1 to 5), allowing for a program scoring range of between 9 and 45. Higher scores indicate greater program suitability. The intent of the rubric is not to achieve an absolute measure of program suitability. Instead the goal is to promote the development of consensus across multiple raters (see scoring grid at the bottom of appendix 1). In this way important aspects of the decision-making regarding program suitability require a focused and informed discussion focused on achieving a collective scoring decision. Multiple staff can compare multiple programs across the same nine dimensions. Another effective way to use the rubric is to have venders or program supporters score the rubric and to provide the necessary information required to score the rubric. In this way the burden of demonstrating the suitability of the program for a given organization at a given time falls on the proponent of the program. The information presented by the program s advocate is then confirmed or rejected by consensus of the larger agency group. The scoring rubric assesses a program s: objective(s), efficacy, generalizability, cost benefit profile, opportunity cost(s), fidelity measurement, outcome assessment, feasibility, and three factors related to implementation. An other dimension can be added and scored in the event that there are idiosyncratic factors that affect the suitability of a particular program and can leverage an otherwise low or high score. The first item on the rubric scores the suitability of the objective(s) of a clinical program (Blase & Fixson, 2013). Agencies define their clinical mission to include who they are going to serve, in what way, for how long and by what approach. Aroma therapy may have demonstrable effectiveness for reducing behavioral disturbances in in patients with dementia (Smallwood et al., 2001), but it is unlikely to teach an individual with severe mental illness daily living skills. The question for this first rubric item involves whether the program being rated is consistent with the clinical mission, when considering the agency s current clinical formulary. A clinical formulary can be understood much like a medication formulary, constituting the range of interventions or programs provided by an organization. The range of programs may include clinical strategies designed to meet the core aspects of particular conditions. Programs may also address more generic issues common to many clients, or programs may be primarily recreational. What is important is that an agency s clinical formulary is sufficient to meet the clinical mission of the agency. Aroma therapy may make good sense as an elective adjunct to other possibly more core strategies, or it may be considered a core strategy for use in accomplishing the agency s mission. The second rubric item is efficacy. The idea of rating efficacy is to determine the strength of the causal inference that the program was the cause of a change in an important criterion variable (important outcome) in the face of other possible explanations for the result (Shadish, Cook & Campbell, 2009). Efficacy can sometimes, though this is not required, be quantified by calculating the effect size of an intervention. One of the most common calculations of effect size is Cohen s d (1977). This effect size calculation can be done by subtracting the mean of the dependent variable of the control group from the mean of the dependent variable of the experimental group and then dividing by the standard deviation of the control group. This calculation can be combined across many similar studies to form a very stable meta-analytic measure of the program s efficacy. Short of this, raters can simply rate the known level of evidence of the program from low to high. It is important to note that not all evidence is equal and raters should understand how to assess the strength of the evidence for a program (Guyatt et al., 2004). ~ 113 ~
114 Generalizability is the third rubric dimension and it involves the confidence that a program s efficacy referred to in rubric item #2 is transferable to the population and setting of interest. This can be assessed by determining if the research demonstrating the program efficacy was done in a similar setting with a similar population under similar conditions. The fourth dimension of the rubric is an estimate of the cost of the program compared to the probable benefits. This is understandably a subjective assessment and reliable only at the extremes of a very good or very poor cost benefit ratio. Some clinical programs such as aroma therapy could reach virtually all clients and be relatively inexpensive (Low Cost). This same program, however, may have only a moderate impact on the agencies clinical mission (Low Benefit). Another program, dialectical behavior therapy, may reach few clients and be very costly. This program may potentially have a large impact on the clinical mission of the agency (high cost / high benefit). The importance of this dimension is to achieve consensus about the relative cost to benefit ratio of various programs in a given setting in the face of limited resources. The fifth dimension is opportunity cost. This is related to the cost/ benefit dimension but focuses on the program s value in relation to other possibly more efficacious programs. This rating assumes that the implementation of a given program is mutually exclusive of the implementation of another program and that the benefit(s) of the excluded program will not be realized. This rating requires that the rater(s) have an understanding of the range of similar available programs and their relative benefits. For this reason this dimension, while a critical consideration, is likely the most difficult and least reliable of all the item scores. The sixth rubric score involves the availability of a fidelity or treatment adherence scale for the program being considered. Fidelity or treatment adherence involves the ability of practitioners and administrators to have objective feedback based on a clinical or programmatic audit of the degree that a program s critical ingredients have been implemented effectively. This can be accomplished by measuring the fidelity of the program implementation. Fidelity is the degree of adherence to the critical ingredients of a program model (Bond et al, 2000). Programs can fail to produce desired outcomes because of a failure to maintain fidelity to important aspects of the model that were assessed in rubric item #2 and that are thought to produce positive outcomes. The seventh and related score on the rubric involves the ability to determine the outcome(s) of the intervention. Outcome assessment serves two purposes. The first is to be able to assess, in conjunction with a measure of fidelity if the program is effective at meeting its objectives. The second is to offer practitioners feedback about their efforts and the need to make corrections or adaptations in their approach. The eighth rubric score involves the feasibility of an organization to implement a given program. Also know as organizational readiness, feasibility can be broken into structural and psychological readiness (Weiner, 2009). Structural readiness is a measure of whether the organization has sufficient resources, time, money, space, staff expertise, etc. The second level of readiness can be thought of as psychological readiness and involves the leadership and staff s level of motivation, support, and buy in to implementation of the program. There are many ways to measure organizational readiness in an organization. One simple way is to describe the program using the rubric and ask how staff and clients feel about implementing it. Organizational readiness is not a static state and can be increased or decreased depending on actions of agency leadership and local conditions. It is important to note that both forms of organizational readiness will vary according to the program being considered. The ninth and last rubric item involves the plan for implementation of the program. Implementation necessarily involves more than training. Training programs that lack direct observation of staff behavior do not allow for staff to receive constructive feedback (Bandura, 1989, Kirkpatrick, 1979). This can result in staff believing they are skilled when they are not or can result in staff simply ignoring the training recommendations (Miller ~ 114 ~
115 & Mount 2001). The inclusion of consultation and supervision provide the best chance of the program being implemented to high fidelity and producing the desired outcomes. Without supervision, even programs that start out with high fidelity can suffer from a condition called practitioner drift in which the practitioner gradually reverts to a preferred, possibly ineffective, clinical approach (Bond et al, 2000). Discussion The assessment of the suitability of clinical programs for implementation is not an exact science nor should it be uninformed guesswork. Limited resources as well as the responsibility to provide effective interventions requires that conflicting priorities be reconciled. The implementation of pet projects or programs that are familiar to staff but are ineffective should not take precedence over programs that are likely to provide greater benefits (i.e. have a higher rubric score) in a given setting. The value in assessing and seeking consensus regarding the suitability of programs for implementation is that it allows for the triaging of an implementation decision. This enables agency staff and leadership to determine whether enough is known about the program to move it to the next phase of consideration. After the use of the rubric, it is recommended that a more detailed examination of implementation issues be undertaken. For a guideline to a more in-depth process see SAMHSA (2014). Conclusion The program assessment rubric (PAR) offers organizations a means of quickly assessing and comparing the suitability of programs for implementation in a given setting. The PAR is not intended as an absolute measure of program suitability. Instead, the intention of the PAR is to promote an examination of important aspects of program implementation and to allow the building of consensus across staff. A second purpose of the PAR is to arm staff with the ability to present dissenting opinions about program suitability in the face of pet projects or familiar programs that are unlikely to produce an agency s desired outcomes. Once programs have been vetted through consensus scoring using the PAR, it is recommended that additional work be done in order to prepare for implementation. Lastly the PAR can be used in a retrospective way to assess programs for exnovation (discontinuation) or to assess the reason(s) that programs failed or were abandoned. Program venders and sponsors can be asked to score the rubric and to provide the information and evidence needed to score the PAR. Limitations of the PAR begin with the lack of inter-rater reliability. The PAR is not intended as an absolute measure of program suitability, and as such, differences in scores of the rubric factors are expected and suggest the need for more information and or discussion in order to achieve consensus. The final decision about implementation is necessarily context dependent and may, in the end, be based on idiosyncratic factors. An additional limitation is the lack of weighting of the rubric items. Some rubric dimensions are likely to be more predictive of suitability than others. The value of rubric scoring may be in its simplicity. Future research into the assessment of program suitability for implementation should seek to determine which of the rubric dimensions are most predictive of successful implementation and under what conditions. Additional work in this area might also attempt to refine the behavioral anchors in an effort to improve inter-rater reliability. References Blase, K., Fixsen, D. (2013). Stages of Implementation Analysis: Where are we Now? National Implementation Research Network. Bond, G. R., Evans, L., Salyers, M. P., Williams, J., Kim, H. W., & Bond. (2000). Measurement of fidelity in psychiatric rehabilitation. Mental Health Services Research, 2(2), Retrieved from Cohen, J. (1977). Statistical power analysis for the behavioral sciences (rev). Lawrence Erlbaum Associates, Inc. ~ 115 ~
116 Dixon, L. B., Dickerson, F., Bellack, A. S., Bennett, M., Dickinson, D., Goldberg, W., Goldberg, R. W. (2010). The 2009 schizophrenia PORT psychosocial treatment recommendations and summary statements. Schizophrenia Bulletin, 36(1), doi: /schbul/sbp115 Drake, R. E., Goldman, H. H., Leff, H. S., Lehman, a F., Dixon, L., Mueser, K. T., & Torrey, W. C. (2001). Implementing evidence-based practices in routine mental health service settings. Psychiatric Services (Washington, D.C.), 52(2), Retrieved from Fixsen, D. L., Naoom, S. F., Blase, K. A., Friedman, R. M. & Wallace, F. (2005). Implementation Research: A Synthesis of the Literature. Tampa, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute, The National Implementation Research Network (FMHI Publication #231). Fox, D. (2005). Evidence of evidence-based health policy: the politics of systematic reviews in coverage decisions. Health Affairs, 24(1), Guyatt, G. H., Oxman, A. D., Vist, G. E., Kunz, R., Falck-Ytter, Y., Alonso-Coello, P., & Schünemann, H. J. (2008). GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ (Clinical Research Ed.), 336(7650), doi: /bmj ad Lehman, A. F., Kreyenbuhl, J., Buchanan, R. W., Dickerson, F. B., Dixon, L. B., Goldberg, R., Steinwachs, D. M. (2004). The Schizophrenia Patient Outcomes Research Team (PORT): updated treatment recommendations Schizophrenia Bulletin, 30(2), Retrieved from Mowbray, C. (2003). Fidelity Criteria: Development, Measurement, and Validation. The American Journal of Evaluation, 24(3), doi: /s (03) SAMHSA (2014). NREEP, SAMHSA, National Registry of Evidence-based Practices Programs and Practices. Retrieved from : Smallwood, J., Brown, R., Coulter, F., Irvine, E., & Copland, C. (2001). Aromatherapy and behaviour disturbances in dementia: a randomized controlled trial. International Journal of Geriatric Psychiatry, 16(10), Weiner, B. J. (2009). A theory of organizational readiness for change. Implementation Science : IS, 4, 67. doi: / Weiner, B. J., Amick, H., & Lee, S.-Y. D. (2008). Conceptualization and measurement of organizational readiness for change: a review of the literature in health services research and other fields. Medical care research and review : MCRR (Vol. 65, pp ). doi: / ~ 116 ~
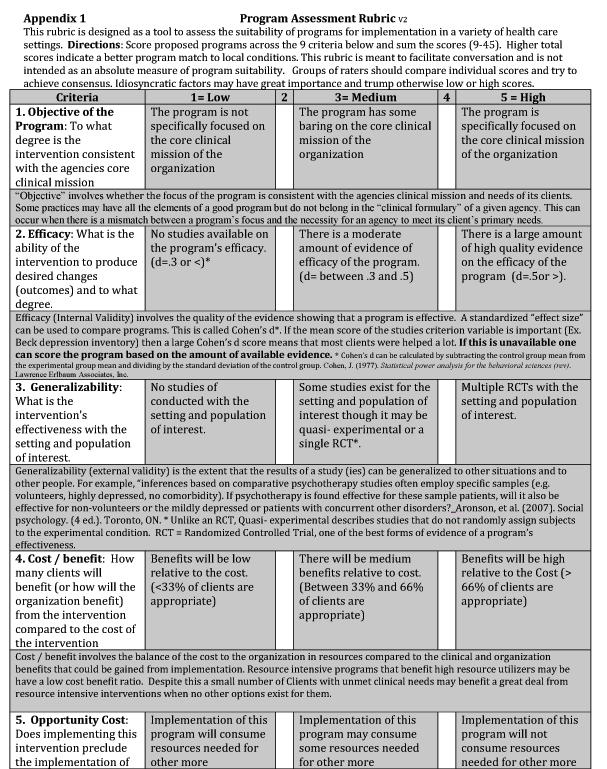
117 ~ 117 ~
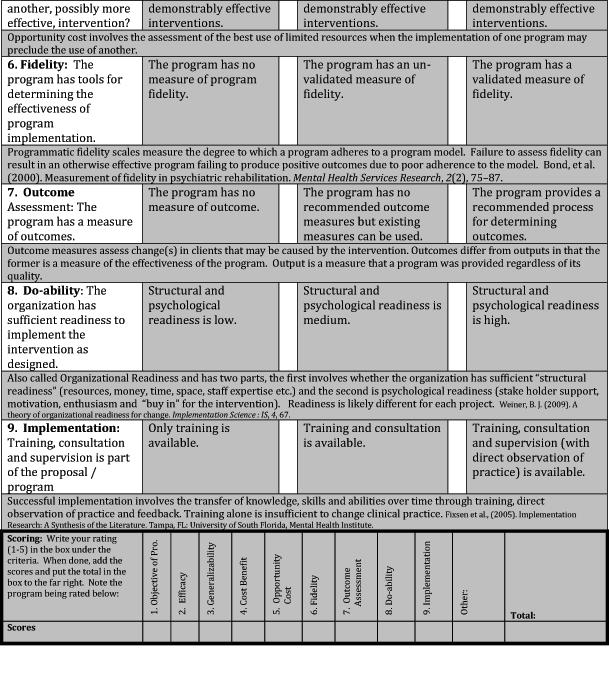
118 ~ 118 ~
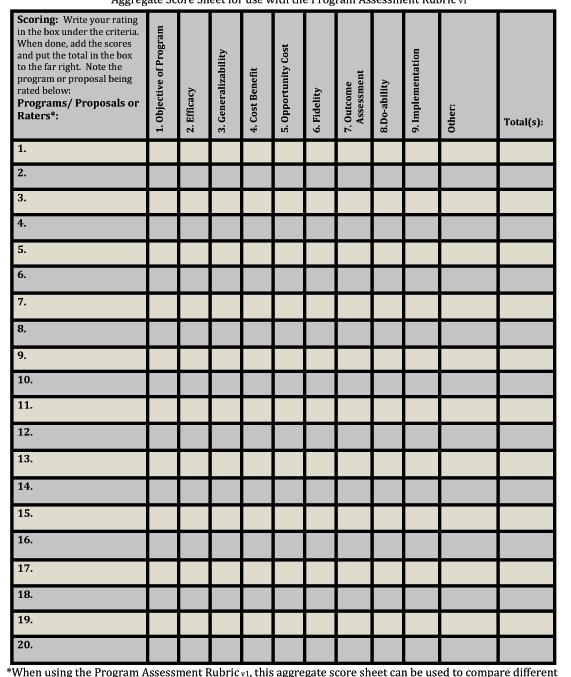
119 ~ 119 ~
120 Comparing quality of life, stress perception and quality of social networks in a community-based brain injury program Barbara Prudhomme White, Ph.D., OTR/L Associate Professor, College of Health and Human Services, University of New Hampshire 514C Conant Hall, UNH Durham, NH bpwhite@unh.edu (Corresponding Author) John Wilcox OTD, MS, OTR/L Clinical Assistant Professor, Occupational Therapy Department, University of New Hampshire 113 Hewitt Hall, UNH Durham, NH john.wilcox@unh.edu Barbara P. Kresge, MS, OTR/L, CBIS Program Director, Krempels Center, Portsmouth, NH Lisa Couture, MSW Executive Director, Krempels Center, Portsmouth, NH Citation: Prudhomme BP, Wilcox JW, Kresge BP, & Couture L.(2016) Comparing quality of life, stress perception and quality of social networks in a community-based brain injury program. International Journal of Psychosocial Rehabilitation. Vol 20 (1) Acknowledgements: The authors wish to thank all of the participants from Krempels Center who made the extra effort to share with us their personal perspectives, and to Krempels Center staff for their assistance in collecting the information critical to this study. We also thank those within the community living with brain injury who took the time to anonymously contribute information. Additional thanks are extended to the University of New Hampshire, College of Health and Human Services for ongoing support of this project as well as to Krempels Center Board of Directors. And the authors are especially grateful to Jeanne O Sullivan, M.S., Clinical Associate Professor of Communication Sciences and Disorders at UNH, and Melissa Wells, Ph.D., Associate Professor of Social Work at UNH, both of who were so generous with their expertise. ~ 120 ~
121 Abstract Objective: To study perceptions of quality of life, stress, and social networks/social connectedness in persons living with acquired brain injury. Design: This was a two-group comparative survey study, analyzing results from a common questionnaire. Participants: 83 adults with chronic brain injury, between the ages of 23-80, living within the community, were placed in one of two groups depending on whether they attended Krempels Center, a community-based center offering day programming for chronic brain injury. Main Outcome Measures: An outcomes questionnaire was compiled from other assessments used in the field, in order to identify individual perception on several psychosocial variables. Results: Several significant differences were found between groups, suggesting that Krempels Center members of at least 6 months duration were less stressed overall, had stronger perceptions of social connectedness, and had higher quality of life perception than did the community sample participants. Conclusion: Individuals with acquired brain injury are faced with daily challenges related to quality of life, management of stress, and social connectedness and opportunities to engage in the community around them. Applying a group-based approach and individualized/family support, offers an effective best-practice model for community based services post-rehabilitation. Keywords: acquired brain injury, community integration, community programs, stress perception, quality of life, social connectedness. Introduction: An acquired brain injury (ABI) includes all types of brain injuries not related to a congenital or a degenerative disease, including brain injury caused by: external trauma (traumatic brain injury), cerebral vascular accidents after birth (commonly known as stroke), loss of oxygen to the brain (hypoxic brain injury), infections of the brain, toxic exposure, fluid build- up in the brain, and tumors ( About Brain Injury, 2012). Recent statistics suggest that traumatic brain injuries (TBI) are a public health concern, with yearly cases diagnosed in the millions (Coronado et al., 2012). In a report to Congress from the CDC regarding traumatic brain injury and the need for evidence-based rehabilitation options, it was noted that an alarming 138 people die from injuries that include TBI in the United States daily (CDC, 2014). Falls account for the greatest number of emergency department visits and hospitalizations for brain injuries, reflecting an aging population. Moreover, 235,046 members of the armed forces in the US were diagnosed with TBI s from (CDC, 2014). In addition, nearly 795,000 US citizens experience strokes yearly, with strokes occurring approximately every 40 seconds in the U.S. Ischemic strokes, characterized by lack of blood flow to the brain, account for 87% of these occurrences. Lost productivity, medications, and health care services resulting from these occurrences cost the nation a staggering 34 billion annually (CDC, 2015). A 2015 update from the American Heart Association identified that 6.6 million US citizens 20 years old are living with complications from a previous stroke, and projections of stroke prevalence from 2012 to 2030 show a 20.5% increase as an additional 3.4 million adults are expected to incur a cerebral vascular accident in this country (Mozaffarian et al., 2015). Acquired brain injury has the potential to negatively impact all aspects of daily living, depending on the method, location, and severity of the injury; it is the major cause of long-term activity limitations in the United States, leaving many people with physical and cognitive impairments (Powell, Temkin, Machamer & Dikmen, 2015; Williams, Rapport, Millis, & Hanks, 2014). In a study by Dahm & Pondsford (2015) regarding long-term outcomes after traumatic injury, persons with TBI ~ 121 ~
122 reported poor physical quality of life, increased fatigue, and increased pain severity. While some of the impacts of ABI, such as physical impairments, are highly visible, many- including quality of life perception, stress perception, and social connectedness-may be less obvious and/or invisible to others. The invisibility of many of these challenges exacerbates their impact (Mahar & Fraser, 2011). The major impediments to successful community integration following brain injury are rarely just medical or physical; rather, most community isolation is a result of deficits in meaningful social conversations and relationships (Rath, Hennessy, & Diller, 2003). Social isolation contributes to feelings of decreased competence, low self-esteem, and mood disturbances, including depression and high perceived stress (Coronado et al., 2012; Strom & Kosciulek, 2007). An increase in reported psychiatric disorders, including perceptions of high stress, generalized anxiety disorder, and post-traumatic stress disorder, has been identified in self-reports of persons who have survived traumatic brain injuries (Gibson & Purdy, 2015). High stress perception is often long lasting, pervasive, and can affect health. Chronic stress is linked to negative health impacts including changes in one s immune system and greater susceptibility to illness (McEwen, 2002; Sapolsky, Romer, & Munck, 2000; Segerstrom & Miller, 2004; Tafet & Bernadini, 2003). In an extensive systematic review, researchers found that stress-related mental health disorders were associated with unusually higher or lower patterns of cortisol, the primary human stress hormone associated with enduring psychological stress (Staufenbiel, Penninx, Spijke, Elzinga, & van Rossum, 2013). Further, strong associations have been identified between cortisol elevations and health complaints in chronically stressed caregivers (De Andrés-García, Moya-Albiol, González- Bono, 2012; Bella, Garcia, & Spadari- Bratfisch, 2011). Dysregulation of cortisol levels related to stress responses in the body has also been shown to play a role in development of depression and depressive symptoms (Tafet & Bernadini, 2003; Schulze, Laudenslager, & Coussons-Read, 2009). Further, cortisol has been found to reduce the number of natural killer cells in the body leading to susceptability to various forms of cancer (Segerstrom & Miller, 2004). Thus, various sources of evidence suggest that chronic stress serves as a significant mediating factor in health. Further, social capital, referring to the presence of social relationships and connectedness, also has been linked to overall health (Gilbert, Quinn, Goodman, Butler, & Wallace, 2013). Brain injury tends to isolate people. Indeed, a particularly debilitating and common long-term effect of brain injury is decreased social participation and interaction (Jacobsson, Westerberg, & Lexes, 2012). Milders, Fuchs, and Crawford (2003) stated that a brain injury can produce debilitating changes in emotional and social behavior, with increased of feelings of neglect and loneliness. Furthermore, compared with their lives before injury, people with ABI have fewer community outings, fewer social contacts, and fewer work and school social engagement opportunities. Social isolation, loss of intimacy and failure of friendships have been identified as pertinent issues through questionnaires regarding perception of long term quality of life for persons with a brain injury (Hawthorne, Gruen, & Kaye, 2009). Lack of employment contributes further to social isolation and lower quality of life perception, and has been connected to degree of cognitive deficit residuals in brain injury survivors (Bellamkonda & Zollman, 2014). Along with perceptions of stress and social connectedness, quality of life perceptions are important indicators for persons living with an acquired brain injury. Jacobsson and Lexell (2013) identified this perception of lower life satisfaction in self-reports 6-15 years after a person had experienced a TBI, when compared to persons not living with deficits related to brain injury. Higher perceptions of life satisfaction, however, were linked to those participants who had increased opportunities for social interactions such as partner relationships and vocational endeavors. Factors that can influence quality of life for a person living with a brain injury, such as happiness and symptoms of depression, can have a direct correlation to the quality of life perception of their caregivers as well (Vogler, Klein, & Bender, 2014). Although the quality of life perception in a person who has sustained a brain injury may be influenced by contextual barriers and challenges, internal strengths associated with self-efficacy and coping skills can predict longterm quality of life perceptions and should be considered when establishing effective programming (Brands, Köhler, Stapert, Wade, & van Heugten, 2014). ~ 122 ~
123 The research described in this paper studies the perceived quality of social connections, quality of life, and stress perception in adults with acquired brain injury (ABI). Our questions focused on comparing data from adults living with ABI who participate in a community day program, Krempels Center, and those who are not attending any similar program. Our hypotheses included that persons who attended Krempels Center would have overall higher quality of life perception, lower stress perception, and higher perceived supportive social networks when compared to persons living with brain injury who did not attend a community program similar to Krempels Center. Methods Participants A total of 83 individuals with ABI living within the NH, MA, ME, New England area participated in the study. See Table 1 for participant characteristics. For the purposes of this study BIAUSA s (2012) definition of ABI was utilized and no distinction was made between persons living with traumatic brain injury and stroke or other forms of chronic ABI. Our experiences servicing individuals who are post-rehabilitation and living with chronic ABI inform us that they share similar experiences including many common psychosocial sequelae and lifestyle changes. All study participants were eligible if they had sustained a traumatic brain injury or fit the BIAUSA s description of acquired brain injury as described earlier (e.g. stroke), had completed rehabilitation services, and were living in the community. Krempels Center members were eligible to participate if they had been attending Krempels Center for at least 6 months (n = 59). The comparison group (n = 24) by self-report, did not attend any community day program, but had sustained a brain injury in the past and were living in the community. Table 1 Participant Characteristics Total Sample N = 83 (96% white) Age X = 51 (12.9) Range years Sex Female = 29 (35%) Education level Completed high School Some college College degree or above Income level Male = 54 (65%) Krempels Center members with ABI (n = 59) X = 51.5 (14) Range years 20 (34%) 39 (66%) 31 (53.5%) 14 (24%) 11 (19%) Community members with ABI (n = 24) X = 51 (12.9) Range years 9 (37%) 15 (63%) ~ 123 ~
124 < $35, 000 per year > $36, 000 per year Martial status Married/partnered Single Divorced 37 (69.8%) 21 (30.2) 15 (26.3%) 28 (49.1%) 12 (21.3%) Recruitment for the Krempels Center sample was done by signed consent. The community sample was acquired from local state brain injury association support groups and healthcare providers who were given a web link to an online consent and questionnaire to share with eligible participants. Responses from community individuals living with ABI were collected anonymously, and consent was given by completing the online questionnaire or mailing the paper questionnaire back to the researchers. Participants were not aware of overall study intentions and were encouraged to answer questions truthfully; this was especially important for long term Krempels Center members in order to avoid any bias in reporting. Additional demographic information about participants was available for Krempels Center members only. Work-study students not associated with the project entered into the database any paper copies mailed to the university. Members at Krempels Center were provided with assistance in completing the questionnaire as needed. The study received Institutional Review Board approval for human participation in research from the University of New Hampshire. Measure: Krempels Center-OET This survey study was designed as a result of team collaboration between Krempels Center staff and university partners. Once the target areas for outcomes assessment were identified, the team researched options for a simple but comprehensive questionnaire that addressed quality of life, perceived stress, and social connectedness/social capital. This process resulted in the Krempels Center Outcomes Evaluation Tool (Krempels Center-OET), which is comprised of two well-known assessments: 1) the WHOQOL-BREF (1997) and the PSS- Perceived Stress Scale (Cohen, Kamarck, & Memmelstein, 1983). Permission was granted from the World Health Organization to use the WHOQOL- BREF, and the PSS is openaccess. A third assessment component was a set of questions about social connectedness drawn from the Occupational Self-Assessment (Baron, Kielhofner, Lyenger, Goldhammer, & Wolenski, 2006). In addition, a question was added about individual self-assessment of functional level. The final questionnaire was piloted on a small sample of existing Krempels Center members, and was found to be short, user-friendly, and easy to assist in completing for those unable to do so independently. Results Data were analyzed with SPSS (2013) using group comparison and descriptive statistics. Twelve dependent variables were analyzed as follows: a) The WHOQOL-BREF (1997) standardized scores were computed according to the manual in 5 areas: ~ 124 ~
125 1. Overall Quality of Life (2 questions) 2. Domain 1: Physical Health (7 questions) 3. Domain 2: Psychological Health (6 questions) 4. Domain 3: Social Relationships (3 questions) 5. Domain 4: Environment (8 questions) b) Perceived Stress Scale (1983), composite score of 10 questions (4 reverse scored). c) Six questions from the Occupational Self Assessment (2006), as well as follow-up questions regarding whether members believed Krempels Center had helped them in each area. 1. I have people who support and encourage me 2. I have people who do things with me 3. I have opportunities to do the things I value and like 4. I have places I can go and enjoy myself 5. I can express myself to others 6. I get along with others In order to address study hypotheses, we first compared the two groups using descriptive statistics to identify any potential differences among them on two independent variables, age and sex. No significant differences between groups were found on either variable, suggesting that both groups were similar for comparison on the dependent variables of interest. To address whether the two groups differed on perceptions of stress, quality of life, and social connectedness we ran a one-way ANOVA to test differences between means on the dependent variables. See Table 2 for results. Several significant differences were found between the groups, suggesting that Krempels Center members were less stressed overall, had stronger perceptions of social connectedness, and had higher quality of life perception than did the community sample participants. Table 2 ANOVA Comparison between groups Krempels Center members with ABI (n = 59) Community members with ABI (n = 24) Effect size ~ 125 ~
126 Perceived Stress X = (7.83) X = (6.87).64 F = p =.001 WHOQOL-BREF: Overall Quality of Life X = 7.65 (1.67) X = 5.83 (1.16).11 F = p =.001 WHOQOL-BREF: Physical Health X= (16.94) X = (1553).51 F = 4.13 p =.05 WHOQOL-BREF: X= (15.59) X = (11.63) 1.68 F = p =.001 Psychological Health WHOQOL-BREF: X= (21.12) X = (14.52) 1.61 F = p =.001 Social WHOQOL-BREF: X= (17.45) X = (16.76) 2.20 F = p =.001 Environment Support/Encouragement X= 3.43 (.77) X =2.58 (.77).05 F = p =.001 Have people who do things with me X= 2.91 (1.03) X =2.20 (.72).04 F = 9.31 p =.003 Have opportunities to do things I like X= 3.01 (.94) X = 2.37 (.92).04 F = 7.93 p =.006 Have places I can go for enjoyment X= 2.77 (1.0) X = 2.33 (.91).03 F = 3.43 p =.07 Can express myself to others X= 3.26 (.79) X = 3.60 (.78).04 F = 3.14 p =.08 Get along with others X= 3.72 (.58) X = 3.75 (.67).002 F =.03 p =.86 Total N = 83 p value (α) =.05 Power (1 β) =.95 ~ 126 ~
127 Stress perception levels were similar to values reported in a national sample of healthy similar-aged individuals without brain injury histories and lower than other studies of individuals with brain injury using the same measure (Cohen, 1988; Strom & Kosciulek, 2007; Bay, Hagerty, Williams, Kirsch, & Gillespie, 2002). See Figure 1 for data comparisons. While not statistically significant in that Krempels Center members scores fall within the 1 SD range of the other two ABI studies, the means and range show meaningful differences and are more similar to the noninjured sample reported by Cohen (1988). Further, a number of social connectedness markers suggested that the Krempels Center members perceived that they had stronger social networks than the comparison group. Significant differences were found on three social connectedness variables: a) support and encouragement b) people do things with me, and c) opportunities to do things I value and like. Two variables about having places to go and enjoy myself approached significance, and no difference was found regarding participants perceptions of getting along with other people. Quality of life scores on the WHOQOL-BREF suggested that Krempels Center members had a significantly different outlook than did their comparison peers (Table 2). Further, Krempels Center members were found to have similar quality of life perceptions to well adults in two other studies. See Table 3. Table 3 WHOQOL-BREF: Comparison of Krempels Center members and other research Sample Characteristics Participants WHOQOL-BREF Standard Score (SD) KC Individuals with ABI Age range years N = 59 (35.5% female) Social Physical Health Environmental (21.12) (16.94) (17.45) ~ 127 ~
128 Psychological (15.59) Well adults N = 1328 Social (20.67) (Skevington et al., 2011) Age range not specified Physical Health Environmental Psychological (16.19) (13.81) (15.56) Well adults N = 866 Social (18.20) (Hawthorne, Herrman & Murphy, 2006) Age range years (56% female) Physical Health Environmental Psychological (18.10) (13.00) (14.00) Finally, in order to verify that Krempels Center was an influencing factor on members perceptions of social connectedness we asked members whether they believed that Krempels Center had helped or supported them in each of the social connectedness areas. Table 4 presents percentages of Krempels Center members stating that the center had a positive influencing effect. The high percentages indicate that Krempels Center had markedly helped members in making social connections and participating in activities that they enjoyed. Table 4: Percent members reporting that Krempels Center influenced their perceptions (N = 57 members) My participation at Krempels Center has helped or supported me in this area of my life I have people who support and encourage me I have people who do things with me I have opportunities to do things I value and like Yes No Yes No Yes No 96% 4% 91% 9% 95% 5% ~ 128 ~
129 I have places I can go and enjoy myself. I can express myself to others I get along with others Yes No Yes No Yes No 89% 11% 89% 11% 93% 7% Discussion The results of this study support our hypotheses that Krempels Center participants would have lower stress perception, stronger perceptions of social connectedness, and higher quality of life perception than persons living with chronic brain injury who were not participating in any community program. In fact, even though we had a relatively small sample, we found strong statistical differences between the two groups on all but three dependent variables. We believed we would see such differences because Krempels Center whose mission is to improve the lives of people living with (acquired) brain injury intentionally focuses programming on overall quality of life for acquired brain injury survivors reintegrating into the community post-rehab, with targeted attention to psychological health (encompassing stress perception) and social connectivity. It has been suggested that once the individual has made it through the acute phase of rehabilitation, community integration may be the ultimate goal (Salter, Foley, Jutal, Bayley, & Teasell, 2008; Ritchie, Wright-St Clair, Keogh, & Gray, 2014). Tate, Wakim, & Gender (2014) identified the importance of focused and sustained programming for individuals with brain injury that is goal-driven, structured, and which embraces aspects of leisure skills in influencing community reintegration and quality of life. Further, others have suggested that programs serving individuals with brain injury should include support and stress management interventions, especially since this population tends to have a higher risk for depression and anxiety disorders (Rath et al., 2003). Krempels Center provides individuals opportunities to not only learn stress management strategies, but to also build skills for increased community integration, and bolster the confidence needed to set and attain personal goals for increased quality of life in various facets and contexts. This self-efficacious behavior can result in higher QOL and better social participation (Brands et al., 2014). Limitations of the study include the relatively small sample size of 83 participants, the majority of whom have been participants at Krempels Center, and were not selected randomly. To minimize response bias, the researchers did not make the intentions of this research explicitly known to members; however, it is possible that their responses are biased in favor of the program. In addition, all participants were from the same geographical area of the U.S. encompassing states within the New England Region only. Further, in order to obtain responses from persons living with chronic brain injury within the community we were cautioned to keep the online questionnaire short. As a result, we did not collect as many descriptive characteristics from the community sample as we desired. Future research is needed to include larger sample sizes that capture more demographics within the United States and internationally. Data from other community-based programs offering services to persons living with an acquired brain injury would also assist in program comparisons to identify threads of effective programming that may be consistently effective across age, sex, race, and other demographics. Conclusion: ~ 129 ~
130 The aim of this study was to expand the literature regarding the perceptions of quality of life, perceived stress, and social connectedness in persons living with chronic acquired brain injury, with intentions of using this information to guide community based programming and interventions. The data from this research suggest that several significant differences in stress perception, quality of life, and feelings of social connectedness were identified between individuals who were participating in a community program and those who were not. In summary, our findings suggest that the Krempels Center model, applying a group-based approach and individualized/family support, offers an effective best-practice program for community-based services post-rehabilitation. Declaration of Interest The authors report no declarations of interest. References Baron, K., Kielhofner, G., Lyenger, A., Goldhammer,V., & Wolenski, J. (2006). Occupational Self Assessment, Version 2.2. Chicago, IL: University of Chicago. Bay, E., Hagerty, B.M., Williams, R..A., Kirsch, N., & Gillespie, B. (2002). Chronic stress, sense of belonging, and depression among survivors of traumatic brain injury. Journal of Nursing Scholarship, 34(3), Bella, G.P., Garcia, M.C., & Spadari-Bratfisch, R.C. (2011). Salivary cortisol, stress, and health in primary caregivers (mothers) of children with cerebral palsy. Psychoneuroendocrinology, 36(6), Bellamkonda, E. & Zollman, F. (2014). Relationship between employment status and sexual functioning after traumatic brain injury. Brain Injury, 28(8), BIAUSA. (2012). Available from: Accessed 2015 Aug 13. Brands, I., Köhler, S., Stapert, S., Wade, D.T., & van Heugten, C.M. (2014). Influence of Self- Efficacy and Coping on Quality of Life and Social Participation After Acquired Brain Injury: A 1-Year Follow-Up Study. Archives of Physical Medicine and Rehabilitation, 95(12), Centers for Disease Control and Prevention [Internet]. (2014). [cited 2015 Aug 13]; Available from: Centers for Disease Control. Heart Disease Fact Sheet [Internet]. (2015). [cited 2015 Aug 13]; Available from: Cohen, S., Kamarck, T., & Memmelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, Cohen, S. (1988). Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S, (Eds). The Social Psychology of Health (pp ). Thousand Oaks, CA US: Sage Publications, Inc. Coronado, V. G., McGuire, L. C., Sarmiento, K., Bell, J., Lionbarger, M. R., Jones, C. D.,... Xu, L. (2012). Trends in Traumatic Brain Injury in the U.S. and the public health response: Journal of Safety Research, 43 (4), Dahm, J. & Ponsford, J. (2015). Comparison of long-term outcomes following traumatic injury: What is the unique experience for those with brain injury compared with orthopaedic injury? Injury, 46(1), ~ 130 ~
131 De Andrés-García, S., Moya-Albiol, L. & González-Bono, E. (2012). Salivary cortisol and immunoglobulin A: Responses to stress as predictors of health complaints reported by caregivers of offspring with autistic spectrum disorder. Hormones and Behavior, 62(4), Gibson, R. & Purdy, S.C. (2015). Mental health disorders after traumatic brain injury in a New Zealand caseload. Brain Injury, 29(3), Gilbert, K.L., Quinn, S.C., Goodman, R.M., Butler, J. & Wallace, J. (2013). A meta-analysis of social capital and health: A case for needed research. Journal of Health Psychology, 18(11), Hawthorne, G., Gruen, R.L. & Kaye, A.H. (2009). Traumatic brain injury and long-term quality of life: Findings from an Australian study. Journal of Neurotrauma, 26(10), IBM Corporation. (2013). IBM SPSS Statistics for Windows, Version Armonk, NY Jacobsson, L. & Lexell, J. (2013). Life satisfaction 6-15 years after a traumatic brain injury. Journal of Rehabilitation Medicine, 45(10), Jacobsson, L., Westerberg, M. & Lexes, J. (2012). Health-related quality-of-life and life satisfaction 6-11 years after traumatic brain injuries in northern Sweden. Brain Injury, 24(9), Mahar, C. & Fraser, K. (2011). Strategies to facilitate successful community reintegration following acquired brain injury (ABI). International Journal of Disability Management, 6, McEwen, B. (2002). The End of Stress As We Know It. Washington, DC: Joseph Henry Press. Milders, M., Fuchs, S. & Crawford, J.R. (2003). Neuropsychological impairments and changes in emotional and social behavior following severe traumatic brain injury. Journal of Clinical & Experimental Neuropsychology, 25, Mozaffarian, D.B., Go, E.J., Arnett, A.S., Blaha, D.K., Cushman, M.J., de Ferranti, M., Després, S., Fullerton, J.P., Howard, H.J., Huffman, V.J., et al. (2014). Heart Disease and Stroke Statistics 2015 Update: A report from the American Heart Association. Available from: Powell, J.M., Temkin, N.R., Machamer, J.E. & Dikmen, S.S. (2007). Gaining insight into patients perspectives on participation in home management activities after traumatic brain injury. American Journal of Occupational Therapy, 61, Rath, J.F., Hennessy, J.J. & Diller, L. (2003). Social problem solving and community integration in postacute rehabilitation outpatients with traumatic brain injury. Rehabilitation Psychology, 48, Sapolsky, R.M., Romero, L.M. & Munck, A.U. (2000). How do glucocorticoids influence stress responses? Integrating permissive, suppressive, stimulatory, and preparatory actions. Endocrine Reviews, 21, Schulze, E., Laudenslager, M. & Coussons-Read, M. (2009). An exploration of the relationship between depressive symptoms and cortisol rhythms in Colorado ranchers. Journal of Rural Health, 25(1), Segerstrom, S.C. & Miller, G.E. (2004). Psychological stress and the human immune system: A meta-analytic study of 30 years of inquiry. Psychological Bulletin, 130(4), Staufenbiel, S.M., Penninx, B.W., Spijker, A.T., Elzinga, B.M. & van Rossum, E.F. (2013). Hair cortisol, stress exposure, and mental health in humans: A systematic review. Psychoneuroendocrinology, 38(8), Strom, T.Q. & Kosciulek, J. (2007). Stress, appraisal and coping following mild traumatic brain injury. Brain Injury, 21(11), ~ 131 ~
132 Tafet, G.E. & Bernadini, R. (2003). Psychoneuroendocrinological links between chronic stress and depression. Progress in Neuro- Psychopharmacology & Biological Psychiatry, 27, ~ 132 ~

133 Volume 20, Number 2 July 2016 December 2016 IJPR Volume 20, Number 2 Feature Articles Page Disability in person with schizophrenia: A study from north east India -Lyngdoh & Ali 3-10 We Need Each Other! : Adapting the Tavistock Method for Large Group Therapy for Adults with Severe Mental Illness -Czochara, Hazell, Semmelhack & Ende Human Rights of Mentally Ill Clients Sheth Integration of mental and psychomotor training in vocational rehabilitation for persons with mental illness improves employment -Knapen, Myszta & Moriën Experiences of otherness among students diagnosed with depression and/or anxiety disorder. -Appelqvist-Schmidlechner, Wessman, Tuulio-Henriksson, & Luoma Inpatient Psychiatric Rehabilitation: An Alternative to Bringing Back the Asylum Dawn - Reinhart-Wood & Kinter TEACH: A Framework for Recovery-Oriented Education and Training -Rudnick Internet-delivered interventions in mental health rehabilitation: A recovery-oriented online service platform -Klutch, Libling, Benyamini, Lachman & Katz Stress reaction and Post-traumatic stress disorder among flood victims of Lahore- Pakistan and role of community (ROC) -Nasar, Zulqarnain, Inayat & Khan The Rise and Fall of the Mental Health Recovery Model Field & Reed Psycho-emotional characteristics that facilitate smoking cessation David, Ramos, Freire, Batista & Ramos Individual Perspectives on the Wellness Recovery Action Plan (W.R.A.P.) as an Intervention in Mental Health Care - Horan & Fox Copyright ADG, S.A. All Rights Reserved. ~ 1 ~
134 Volume 20, Number 2 July 2016 December 2016 Feature Articles ~ 2 ~
135 Volume 20, Number 2 July 2016 December 2016 Topic: Disability in person with schizophrenia: A study from north east India Lavinia A.M Lyngdoh 1 Arif Ali M. Phil trainee, Department of Psychiatric Social Work, LGB Regional Institute of Mental Health, Tezpur Assam. 2. Assistant Professor, Department of Psychiatric Social Work, LGB Regional Institute of Mental Health, Tezpur Assam. Citation: Lyngdoth L & Ali A. (2016) Topic: Disability in person with schizophrenia: A study from north east India. International Journal of Psychosocial Rehabilitation. Vol 20 (2) 3-10 Corresponding Author: Dr. Arif Ali Department of Psychiatric Social Work, LGB Regional Institute of Mental Health, Tezpur, Assam India Abstract Schizophrenia is a significantly disabling disease that affects social.family psychological, vocational and occupational functioning. The present study aim to find the level of disability in person with schizophrenia.the research setting was at the Outpatient Department, LGB Regional Institute of Mental Health, Tezpur, Assam. Based on purposive sampling technique, samples of 60 subjects with diagnosis of schizophrenia were selected. Patients attending Outpatient Department for follow up in the age range between 18 to 60 years of both the gender were included. Patients with any organic involvement, who have any significant physical illness and with co morbid disorder were excluded.socio-demographic and clinical data sheet, Positive and Negative Syndrome Scale [PANSS], Indian Disability Evaluation Assessment Scale [IDEAS]. In the present study it was found that majority of the respondents are having moderate level of disability [43%], while 40% are having mild level of disability, 15% are having severe level of disability and 1.7% of the respondents are having profound disability. Schizophrenia required a diverse range of interventions. Beside pharmacological intervention there is an equally vital psychosocial intervention are required in promoting independence, decreasing disability and enhancing quality of life in person with schizophrenia. Key words: Disability, Schizophrenia, Positive and Negative Symptoms ~ 3 ~
136 Volume 20, Number 2 July 2016 December 2016 Introduction: Schizophrenia is a significantly disabling disease that affects all major areas of life. It causes disability leading to restrictions on many domains of social, family, psychological, vocational and occupational life. Schizophrenia usually starts during young age and is frequently associated with deterioration from the previous level of functioning and they are reported to have multiple psychological and physical impairment [King and Nazareth, 1996].Disability associated with mental illness is a major contributor to the global burden of disease. Schizophrenia is still ranked among the top ten leading causes of disease-related disability in the world [Tandon et al., 2008]. Disability is a complex bio-psycho-social phenomenon that results from interplay of illness-related factors and the overall socio-environmental context in which the person lives [World Health Organization, 2001]. As per the Census of India, 2001 there are an estimated 2,263,821 [for a population of 1,028,610,328] people suffering from disability due to mental illness in the country. Mental disorders rank third among the five leading contributors to disability in India [Census of India-Data on Disability, 2001]. However, a recent community-based study in India found mental disability to be the most common type of disability accounting for 36.7% of total disability [Ganesh et al., 2008]. People with psychiatric disabilities experience numerous limitations in everyday functioning, some of which include difficulties in interpersonal situations, have problems coping with stress, difficulty in concentrating, lack of energy or initiative and negative impact on quality of life. There is a lack of comprehensive synthesis of research findings on the full extent of psychosocial difficulties experienced by people living with schizophrenia. To initiate and plan for rehabilitation, there must be an adequate understanding of the individual person in the context of his or her specific environment.to help disabled persons identify their personal goals, disability assessment is required. It is important to identify the individuals personal costs and benefits associated with the needs for their rehabilitation. Thus the present study aims to assess disability in person with schizophrenia. Objectives: To find the level of disability in person with schizophrenia Material and Method The research setting was at the Outpatient Department, LGB Regional Institute of Mental Health, Tezpur, Assam. Based on purposive sampling technique, samples of 100 subjects with diagnosis of schizophrenia were selected. All the patients were diagnosed by a psychiatrist in accordance to the DCR-ICD-10 criteria at the time of their entry into the hospital. Patients attending Outpatient Department for follow up in the age range between 18 to 60 years of both the gender with diagnosis of schizophrenia were included. Patients with any organic involvement, who have any significant physical illness and with co morbid disorder were excluded. Assessment tools: 1. Socio-demographic and Clinical Data Sheet: It is semi-structured Performa especially designed for this study. It contained information about social demographic variables like age, sex, education, marital status, religion, employment status, domicile background etc. In clinical data sheet it contains variables like, age of onset, total duration of illness, precipitating factors, mode of onset etc. 2. Positive and Negative Syndrome Scale [PANSS] [Kay & Linden Mayer, 1987]. The PANSS is a medical scale used for a measuring symptom severity of patients with Schizophrenia. It was published by in 1987 by Stanley Kay, Levis Opler and Abraham Fiszbein which is administered to the patients for assessment of symptomatology. The patient is rated on from 1 to 7 on 30 different symptoms. ~ 4 ~
137 Volume 20, Number 2 July 2016 December Indian Disability Evaluation and Assessment Scale [IDEAS] [The Rehabilitation Committee of the Indian Psychiatric Society, 2002]: It assesses disability under four domains: Self-care, interpersonal activities [social relationships], communication and understanding, and work. Each item is scored between 0 and 4, i.e., from no to profound disability, adding scores on 4 items gives the total disability score. Global disability score is calculated by adding the total disability score and MI 2Y score [Months Ill in 2 years- a score ranging between 1 and 4, depending on the number of months in the last 2 years the patient exhibited symptoms]. Global disability score of 0 corresponds to no disability, a score between 1 and 7 corresponds to mild disability, and a score of 8-13 corresponds to moderate disability, a score between 14 and 19 corresponds to severe disability, and a score of 20 corresponds to profound disability. Indian Disability Evaluation and Assessment Scale [IDEAS] is a well-validated instrument and is being used across the country for disability evaluation in psychiatric disorders. The alpha value for the scale has been found to be , indicating good internal consistency between the items. Ethical issues: The respondents were assured confidentiality; informed consent was taken from the respondents. The participants were clearly explained the purpose of the study and samples were selected on voluntary basis. Procedure Patient was identified on the basis of DCR ICD-10 diagnosis criteria. Informed consent was taken from the patient as well as from the informant before eliciting relevant information and the nature and purpose of the study was explained. All the subjects who were selected for the present study were interviewed and then assessed with the help of semi-structured socio demographic and clinical data sheet.thereafter Indian Disability Evaluation and Assessment Scale [IDEAS] was administered to know the severity level of disability. Data analysis The collected data was analyzed using descriptive and inferential statistics in Statistical Package for Social Science [SPSS] 16 version. Results Table 1: Socio demographic details of the participants N=60 Variable Frequency Percentage Age Gender Male Female Education Illiterate ~ 5 ~
138 Volume 20, Number 2 July 2016 December 2016 Primary Secondary Graduate Other Marital status Un Married Married Separated 6 10 Hindu Muslim Religion Christian 3 5 Ethnicity Tribal Non-Tribal Assamese Community Bengali House wife 3 5 Professional 3 5 Self Employed 3 5 Agriculture Occupation Govt Job Un employed Residence Urban Semi Urban Rural Family Type Nuclear ~ 6 ~
139 Volume 20, Number 2 July 2016 December 2016 Joint Extended Socio economic details Low Upper Low Lower Middle Upper Middle Upper The above table shows that the majority of the respondents were in the age range of 31-40[40%], followed by in the age range of 42-50[36%], while 18% were in age range of and 5% were in age range of The majority of the respondents were male [66.7%] whereas 33.3% were female participants. The majority of the respondents are educated up to secondary [40%], married [51.7%], Hindus by religion [73.3%], non tribal [ 86.7%]and belongs to the Assamese community[35%].in occupation majority of the population which constitutes to 30% are employed in the government sector whereas 28.3 works in the agricultural sector and 26% are unemployed.further majority of the respondents resides in urban[47%] where 18% resides in rural and 35% resides in semi urban. Majority of the respondents stays in a nuclear family [43.3], 37% are a joint family and 20% belongs to a extended family. In the present study 33.3% belongs to the lower economic background, 26.7% belongs to the upper economic background and only 1.7 % belong the low economic background. Table 2: Clinical Profile of the participants N=60 Variable Mean SD Age of Onset of Illness Total duration of Illness Variables N [%] Precipitating factors Present 35[58.3] Absent 25[41.7] Mode of onset Acute 3[5] Abrupt 6[10] Insidious 51[85] Course Continuous 53[88.3] ~ 7 ~
140 Volume 20, Number 2 July 2016 December 2016 Episodic with Progressive deficit Episodic with stable deficit Incomplete remission 4[6.7] 2[3.3] 1[1.7] Family history of illness Present 14[23.3] Absent 46[76.7] No of Hospitalization[admission Not admitted 26[43.30] One time 18[30.0] Two times 9[15.0] Three times 4[6.7] Four times 2[3.30] Six times 19[1.7] The above table shows that the mean age of onset of illness was 27.5± 8.36, while the mean duration of illness was 9.91 ± In the present study majority of the respondents [58.3%] has precipitating for the cause of mental illness, while [41.7%] do not have any precipitating factor. Further Majority of the respondents [85%] mode of onset was insidious, 88.3% have continuous course of illness, 76.7% respondents family history of mental illness is absent and majority of the respondents [43.3%] were never admitted in hospitals [table 2] Table 3: Disability Assessment in Schizophrenia N=60 Variable Frequency Percent Mild Disability Moderate Disability Severe Disability Profound Disability In the Indian Disability Evaluation and Assessment Scale majority of the respondents are having moderate level of disability [43%], while 43% are having mild level of disability, 15% are having severe level of disability and 1.7% of the respondents are having Profound Disability ~ 8 ~
141 Volume 20, Number 2 July 2016 December 2016 Table 4: Person correlation between Global disability score and positive symptoms, Negative symptoms, General Symptoms N=60 Variable Positive Symptoms Negative Symptoms General Symptoms Disability **.148 **p 0.01 The above table shows that the global disability score has a significant s positive correlation with Negative symptoms [r=.632, p 0.01], while positive correlation was found with positive symptoms [r=.127] and General Symptoms [r=.148]. Table 5: Person correlation between Age of Onset, Total duration of Illness, Global disability score N=60 Variable Age of Onset Total duration of Illness Global disability score ** **p 0.01 The above table shows that the total global score of disability has a significant positive correlation total duration of illness [r=.403, p 0.01] and negative correlation was found with age of onset of illness [r= ] Discussion In the present study it was found that majority of the respondents are having moderate level of disability [43], while 43% are having mild level of disability, 15 %are having severe level of disability and 1.7% of the respondents are having profound disability.various researchers have also reported that that majority of the respondents have mild to moderate level of disability (Ali, 2009; Kumar et al. 2008; Sihabuddeen, Ismail, Chandran Mohan &Moosabba,2012].In the study it was found the global disability score has a significant s positive correlation with Negative symptoms [r=.632, p 0.01], while positive correlation was found with positive symptoms [r=.127] and General Symptoms [r=.148].further it was found that total global score of disability has a significant positive correlation total duration of illness [r=.403, p 0.01] and negative correlation was found with age of onset of illness [r= -.175]. Shankar et al. [1995] reported that negative symptoms predominated among the factors associated with global disability in both sexes. Grover et al. [2014] reported that the total and global disability score correlated with positive, negative and general psychopathology scores of PANSS, though the relation was strongest with negative symptom score. Thara and Joseph [1995] found that the socio-demographic and clinical variables like gender, age of onset, mode of onset, duration of illness and premorbid functioning which are related to course and outcome have also been reported to have an effect on disability. Further, Ali [2009] also reports that age of onset, duration of illness have an effect on disability [Ali, 2009]. ~ 9 ~
142 Volume 20, Number 2 July 2016 December 2016 Limitations The sample size was relatively smaller and the study, Gender comparisons was not done. It was cross sectional hospital based study and cannot be generalized. Follow up study need to be conducted. Conclusion Schizophrenia required a diverse range of interventions. Beside pharmacological intervention there is an equally vital psychosocial intervention are required in promoting independence decreasing disability and enhancing quality of life in person with schizophrenia. No rehabilitation effort will be complete without taking into consideration the disability of the patients in the execution of rehabilitative measures. References 1. Ali A. [2009]. Disability in schizophrenia and its relationship with duration of illness and age of onset. International Journal of Psychosocial Rehabilitation,14, Census of India-Data on Disability (2001). Office of the Registrar General of India. 3. Ganesh KS, Das A, Shashi JS. (2008).Epidemiology of disability in a rural community of Karnataka. Indian J Public Health. 52, Grover S, Shah R, Kulhara P, Malhotra R. (2014) Internal consistency & validity of Indian disability evaluation and assessment scale [IDEAS] in patients with schizophrenia. Indian J Med Res. Nov; 140; 5, Shihabuddeen Ismail, Chandran M, Moosabba (2012).Disability in persons with Schizophrenia correlated to family burden and family distress among their caregivers.delhi Psychiatry 15;2, Kay SR, Opler A, Fisbein A (1987). Positive and Negative syndrome Scale (PANSS) for schizophrenia.schizophr Bull, 2, King M and Nazareth. (1996). Community care of patients with schizophrenia, the role of the primary health care team. British Journal of General Practice, 46, Kumar S, Kulhara P, Grover S, Malhotra R. (2006). Preliminary experiences with use of disability assessment scales at mental disability clinic, PGIMER, Chandigarh. J Mental Health Hum Behav, 11: Shankar R, Kamath S, Joseph AA.. (1995).Gender differences in disability: A comparison of married patients with schizophrenia. Schizophr Res, 16, Thara R, Joseph A A(1995). Gender difference in symptoms and course of schizophrenia. Indian J Psychiatry, 37: The Rehabilitation Committee of the Indian Psychiatric Society (2002). IDEAS (Indian Disability Evaluation and Assessment Scale) - A scale for measuring and quantifying disability in mental disorders. Indian Psychiatric Society. 12. Tandon R, Keshavan MS, Nasrallah HA. (2008).Schizophrenia, just the facts what we know in Epidemiology and etiology. Schizophrenia Research, 102, World Health Organization (2001).Geneva: World Health Organization; International classification of functioning, disability and health: ICF. ~ 10 ~
143 Volume 20, Number 2 July 2016 December 2016 We Need Each Other! : Adapting the Tavistock Method for Large Group Therapy for Adults with Severe Mental Illness Bradford Czochara, Psy.D., LPC, CGP Neurobehavioral Medicine Consultants, Ltd. Trinity Services, Inc Exeter Ct. Orland Park, Il bczochara58@midwestern.edu Clive Hazell, Ph.D. Professor The Art Institute/Author/Private Practice Diana Semmelhack, Psy.D., ABPP Professor Midwestern University, Downers Grove, IL Larry Ende, Ph.D., MSW Citation: Czochara B, Hazell C, Semmelhack D & Ende L..(2016) We Need Each Other! : Adapting the Tavistock Method for Large Group Therapy for Adults with Severe Mental Illness. International Journal of Psychosocial Rehabilitation. Vol 20 (2) Abstract Wilfred Bion (1954) proposed a model of group theory known as a group-as-a-whole approach or the Tavistock method. This approach to group therapy emphasizes the unconscious, group-as-a-whole dynamics versus any individual member s process. As a means for individuals to deflect discussing their own idiosyncratic trauma history and allowing for a general discussion of trauma, this approach helps members feel safe to risk addressing painful issues in the present moment (Semmelhack, Ende, & Hazell, 2013). We hypothesize that this is the case because the Tavistock method creates, among other things, a deep sense of psychological safety (Hazell, 2005) There are a limited number of research studies examining the applicability, efficacy, and general impact of the Tavistock model on individuals diagnosed with a severe mental illness (Semmelhack, Ende & Hazell, 2013). Additionally, research studies examining the Tavistock model, and its application to group work, focus on small group settings instead of large group settings. This focus on small groups has perhaps resulted ~ 11 ~
144 Volume 20, Number 2 July 2016 December 2016 from widespread assumptions regarding the tendency for large groups to cause regression and depersonalization in members. This study will highlight on-going research conducted over a six month period of time utilizing a modified Tavistock approach (Semmelhack, Ende & Hazell, 2013) extending the application of the modified Tavistock method to large group work for adults with severe mental illness. It was hypothesized that group members would exhibit increased comfort and cohesiveness in the large group and reduced anxiety regarding engaging in a large group. It was also hypothesized that there would be improvements in other group dynamics such as a stable group size and the understanding of group norms. By this we mean that the group would be well attended by at least a core set of members and that a relatively stable set of growth-promoting norms such as listening and openness to experience would be understood and promulgated by group participants. The authors conducted monthly large group sessions in the style of an adapted Tavistock method (Semmelhack, Ende & Hazell, 2013). Unlike the small groups described in the 2013 study, these large groups included members. All groups consisted of members diagnosed with severe mental illness (e.g., Bipolar Spectrum Disorder, Schizophrenia Spectrum) residing in a long-term skilled nursing home facility. Qualitative and quantitative data, in the form of questionnaires, were collected and compiled after the completion of each group session. Data were collected after the first group session and subsequently for six total sessions. Results indicated increases in group comfort/cohesion (as defined as a desire to attend group sessions and willingness to share; Yalom, 2005), insight, emotional expression, enjoyment, and participation. It was also found that members preferred the large group size overall; however, this change in group size preference gradually increased based on the number of group sessions the member attended. Conclusions from this pilot study suggest the effectiveness of a novel application of the Tavistock method to large group work with a population of individuals with severe mental illness (Semmelhack, Ende & Hazell, 2013). Further research on large Tavistock style groups could focus on the use of the large group in the formation of a community setting in a long-term care institution and the dynamics of residing in a long-term facility. This study furthers research in group work, treatment approaches for individuals with severe mental illness, and treatments for individuals residing in a nursing home facility. Keywords: Group Psychotherapy, Tavistock Group, Long-term Care, Severe Mental Illness Introduction: The current study investigates the efficacy of a large group setting for a Tavistock method group for residents diagnosed with a Severe Mental Illness (SMI) living in a Skilled Nursing/Long Term Care (SNF/LTC) facility. We examined 15 group process variables over the course of six months. Using a questionnaire developed specifically for the study, the variables examined included: group comfort pre and post group sessions, group cohesion, comfort with expressing thoughts and feelings during sessions, consultant work, personal insight, enjoyment, comfort with group size, amount of participation, desire for the group sessions to continue, perceived consultant support, group size preference, and perceived lack of attention from consultants. We hypothesized that the modified Tavistock group approach in a large setting would produce statistically significant increases in scores on the 15 variables based on results from the questionnaire created for the study. Specifically, we hypothesized increases in scores related to group cohesion, participants personal insight, group size preference, and desire for the large group to continue. In addition we were very curious as to the themes and group process that would emerge over the course of time. We thus took detailed process notes after each session and content analyzed them on an ongoing basis for six months to determine identify major themes. Thus, for example, after a member of the institution had died, much group time was spent mourning this individual. When state funding was likely to be eliminated, this created considerable anxiety in the group. Such themes were identified and recalled before the following meeting to alert consultants to possible issues that might still be emotionally significant. This study is interesting and novel in several ways. First, it explores the use of modified Tavistock groups as a means of providing psychotherapy in a residential setting. Tavistock groups are typically not used for therapy but as a means for learning about group dynamics. Semmelhack, Ende, and Hazell (2013) demonstrate that this ~ 12 ~
145 Volume 20, Number 2 July 2016 December 2016 approach is feasible for various group settings (i.e., prison settings, skilled nursing, long-term care). Secondly, Tavistock groups are not typically recommended as fitting for persons with the severe spectrum of diagnoses. This is because the Tavistock technique addresses unconscious material. Such an approach is assumed to be too stressful on individuals who, theoretically, have compromised reality testing. Thirdly, this study seeks to explore and demonstrate the potential therapeutic utility of a large group. There is very little research and literature on the use of large group psychotherapy. Certain organizations claim to provide therapeutic benefit in the form of large group experiences (Bry, 1984) but there is very little, if any, systematic research on the benefits of large group work, especially Tavistock approaches, with individuals diagnosed with SMI. In addition, these large group formats operate from the precepts of what might be broadly called existential/humanistic assumptions. The Tavistock approach being explored here differs in significant ways from these approaches. Assumptions about large groups lead to conclusion that they would not be advisable for those with severe diagnoses. Kreeger (2012) argues that large groups have the effect of bringing about regression in the members. Freud (1922/1990) argues along similar lines, citing, The Crowd, of LeBon (1895/2002) and positing that the large group induces a regressive identification with the group and with the leader, thus weakening the egos of the members. When one works in conferences in the Tavistock tradition (Colman & Geller, 1985), it is a commonly held assumption that far more regressive and psychotic like phenomena will be evidenced in the large group experience as this induces depersonalization, de-individuation and thus, in turn activates the litany of primitive defense mechanisms characteristic of the large group projection, projective identification, splitting and denial. In addition, it is usually assumed that the member of a large group usually experiences some form of narcissistic insult owing to the frustrating dynamics and that this can lead to the eruption of intense hatred (de Mare, 2011). For these reasons alone, it is usually deemed inadvisable for persons who theoretically exhibit weak egos and fragile self-esteem to be placed in the potentially ego-weakening context of a large group. The Tavistock group comes in a variety of forms but it shares certain characteristics. First, there is a focus on the group-as-a-whole. Consultations are usually aimed at the entire group, not at any specific individual. Second, there is a focus on the latent content of the group s process. Latent content involves the symbolic or unconscious material the group contains, while manifest content includes conscious or overt material expressed during the group. Thus, the group might be discussing dangerous neighborhoods in the city. This would be considered manifest content. However, a consultant might interpret this to have the latent content meaning of the group discussing the relative safety of the group in the here and now. While the consultations are aimed at different layers of the unconscious, ranging from the relatively superficial hidden agendas to the deeper layers that may invoke addressing the profound layers of impulse and image found in an array of theories, they usually (nearly always) look beyond the manifest content of the group. These attributes of Tavistock groups suggest that frequently they lead members to examine fantasies and possibilities that are not part of the consciously experienced current reality in the group. With patients where ego building and reality testing are often seen as being the order of the day such interventions that will be initially experienced as ego alien and experience distant might not be seen as meeting these ends. Since Tavistock or group-as-a-whole groups are not among the most common of group styles as compared to psychosocial or skill building group styles utilized with this population, (for example Hill (1971,1977) notes that a more passive/reactive, highly structured approach is commonly employed when working with the severely mentally ill) we believe that several examples of interventions that were made by consultants might give the reader a more concrete idea of what occurred in the groups. This list is not complete but gives a beginning idea of the approach. Readers who are interested in reading further are directed to Colman and Geller (1985) Hazell (2005), Semmelhack, Hazell and Ende (2013,2015). 1) Derivatives: Consultations that come from this perspective take the manifest content of the group discussion and reframe it as a commentary on the underlying dynamics of the group-as-a-whole. For ~ 13 ~
146 Volume 20, Number 2 July 2016 December 2016 example, when several members spoke of the infrequency of visits from relatives and their sense of loneliness and isolation, the consultation, The group is concerned about the lack of contact between members in the group. In this simple example, a conversation that is on the surface about, there and then events is taken to be a commentary on the, here and now situation. 2) Symptoms: When working with the severely mentally ill it is not unusual for a member to hear voices, get up and walk out of the room, break into song, have an accident or perhaps develop a psychosomatic reaction. In the group-as-a-whole approach, these events are treated as communications about the unconscious dynamics of the group. They are decoded and fed back to the group in a less metaphorical form. For example, when a member repeatedly sang the nursery rhyme, Rockabye Baby, the interpretation that group members were feeling anxious and insecurely held in the group was offered. When a member twice spilled coffee, the interpretation that the group was overflowing with emotion was offered. When a member got up to leave, the consultation that the member was reacting to an unacknowledged rise in group anxiety was offered. These interpretations are not generated in a formulaic, lock step fashion. There has to be supporting data from other aspects of the group. In addition, the consultant waits to see if the group, through its speech and actions, affirms or negates the validity of the consultation. 3) Context: Prior to each group meeting, consultants and observers would meet for 30 minutes to discuss events that occurred in the institution and its context that might affect the community. More often than not, these events would surface explicitly in the ensuing session which then offered a means of processing these events. For example, if a member of the nursing home died, the effect of this would reverberate through the social network triggering feelings of loss, sadness and anxiety. It would also trigger memories in group members of other losses. In addition, at times the political climate at the state level would make it seem that the institution might be closed down. This would be brought up by members in the ensuing group and would be discussed. Usually these anxieties were based on the real concern that the institution might be shut down. These anxieties would also trigger anxious memories in the group for the many members that had experienced homelessness or had been foster-children. 4) Roles in the Group: At times certain individuals in the group would emerge and take up roles, often leadership roles, which seemed to serve very specific functions for the group. Quite frequently these would be consulted to, the consultant always pointing out that there was an unconscious agreement, a collusion, between the entire group and the member that they should perform this role. For example, one member would usually start each group with a speech that was rather like a sermon. This seemed to serve several functions for the group it gave the image of there being a kindly wise father; it uplifted the moral tone of the group and seemed to have a calming effect on one and all, even the consultants. Such a mechanism can be interpreted. As another example, another member took up the role of political representative to outside groups, politicians and interest groups when it appeared the survival of the institution was under threat. Other members took up roles of visionary, or spokespersons for gratitude or love and kindness. Each of these roles can be seen as instances of repository where one member or a subgroup is asked unconsciously by the group to hold and carry an affect, idea or fantasy for the group-as-a-whole. Insofar as these dynamics involve projective identification, they are worthy topics for consultation. 5) Boundaries of the Group: The boundaries of a median group, such as the ones in this study, are more porous than the typical Tavistock group. For example, people would come and go from the group. Sometimes individuals would show up at the community meeting thinking it was the church group. Usually there were several individuals who wandered back and forth just outside of the boundary of the group. Usually there would be an announcement over the loudspeaker. Consultants would pay attention to these events at the boundary of the group and weave them into consultations. For ex- ~ 14 ~
147 Volume 20, Number 2 July 2016 December 2016 ample, the members circling just outside the group might be thought of as containing some thoughts or feelings that the group had some difficulty containing or perhaps the member who showed up in the wrong room represented something that was seen to be missing from the group and yet desired. 6) Subjective state of the Consultant: It is common for the consultant to have reactions during such groups. These reactions might involve memories, emotions, loose associations, physical responses and defensive reactions. While many of these will reflect the individual mind of the consultant, some might indicate the underlying dynamics of the group. One way to tell if this is likely is to scan the group for supportive data. Thus, for example, at the outset of a group one consultant felt deep feelings of warmth and gratitude at being in the group, intermingled with anxiety at these tender feelings. At the same time, the group was discussing upcoming plans and hopes and anxieties for Thanksgiving. The way seemed clear for the consultant to offer the hunch that the group was pleased to reconvene, felt grateful for the riches in the group, but at the same time was anxious about possible disappointment. Such subjective responses can tip the consultant off to members roles. For example the role of sermonizer mentioned before became apparent when a consultant recognized how comforted and secure he felt whenever the selected member held forth with his philosophical homilies for several minutes. This is an incomplete list, to be sure, and it certainly falls far short of offering the reader a clear set of how to instructions. We hope it stimulates interest in exploring an approach which, we believe is of enormous benefit to a wide array of consumers. Our experience, described in Semmelhack, Ende and Hazell (2013, 2015) and Hazell (2005), lead us to question these assumptions. In these texts, some 21 years of research is cited where small Tavistock groups are shown to have a beneficial impact on the mental health of the severely mentally ill participants using a variety of standard measures (e.g., BDI-II, BAI). The individuals participating in these groups were quite capable of integrating and using group-as-a-whole interpretations and would show significant benefits from such experiences. In addition, we believe that the large group format offers significant opportunities for the experiencing of community. The Open Dialogues approach in Finland (Seikkula and Arnkil, 2006) demonstrates the potency of an approach that utilizes such social networks in the treatment of the severely mentally ill. We posit, along with Nancy (1991), that this need for community is equivalent to the drives posited by many other psychologists (drives such as: sex, aggression, self esteem, love and belongingness, social interest, interpersonal security etc.) and, that if this drive is frustrated many untoward symptoms emerge (Sullivan, 1968). Thus, providing for an opportunity for community experiencing, we are providing an experience that will alleviate mental suffering. In this, we follow Jones (2013), Edelson (1970), Nancy (1991), Blanchot (1988), and de Mare (2011). We are also influenced by the psychodynamically inclined anthropologists who argue cogently for the spelling out of articulations between individual personality and culture: Devereux (1980), Roheim (1971), Kardiner (1939), and Erikson (1993). We thus decided to conduct a series of large groups following modified Tavistock procedures and to monitor and record the results with questionnaires, interviews and process notes. We believed that individuals diagnosed with SMI would gain benefits and experience the group in a therapeutic fashion. This paper demonstrates that such a large group is feasible and beneficial for a population of severely mentally ill individuals. This paper also describes themes that emerged in the large group and managerial issues (that were the responsibility of the consultant team) involved in conducting such a group. These themes might be of use to other practitioners conducting large groups in similar settings. At the end of our discussion, we will posit several hypotheses and formats for future research. ~ 15 ~
148 Volume 20, Number 2 July 2016 December 2016 The groups were conducted on one Sunday afternoon a month for six months at a skilled nursing/long-term care facility (SNF/LTC) located in the suburbs of a metropolitan center in the Midwest of the USA. Attendance was entirely voluntary. The membership averaged 24 members per group (SD = 1.79), and the average composition of the groups was as follows: 8.5 males per group (SD = 1.6; 36%), 15.5 females per group (SD = 1.05; 64%), 24 members average attendance per group (SD = 1.79), and average age of the members was 60 (SD = 10.5). Members and consultants conducted the group session in a large circular arrangement. This deviation from traditional Tavistock procedure, where members sit in concentric circles or spirals, for example, was chosen for two reasons (Colman and Geller, 1985). First, we believed that this arrangement is less provocative, since it allows for more face to face contact and does not, by virtue of spatial arrangement, stimulate issues of "front seat/ back seat" or "in group/out group." Since we were experimenting, we wanted to introduce such novelties in a stepped fashion. This structure is consistent also with the recommendations of de Mare (2011). We anticipate using other arrangements in upcoming groups. Second, several members in this group utilized wheelchairs and walkers and access to chairs was greatly facilitated with the circle arrangement. Methods: Large Group Session Procedure Residents living at this facility were privy to the overall facility schedule of activities for that specific Sunday. The large group, however, was not listed on the facility activities list in order to protect confidentiality of the group members. Therefore, the research team reminded the residents participating in the large group session two days prior to the actual session in their respective small group sessions. They were also reminded of the large group the day of the session. Attendance to the large group was entirely voluntary for the residents. Each participant expressed verbal consent to the study and provided written consent for the study. Also, the participants were verbally explained the structure and nature of the group sessions, but they were not explained the research hypothesis. The information regarding the research hypothesis was omitted in order to minimize any bias and/or perceptions that might skew the data. The consultants provided no incentive or reward for attending the large group session. Merely one verbal encouragement or prompt was initiated to recruit members to the large group. This prompt was given by one member of the consultant team to potential members (e.g., Would you like to come to the large group session? ). Due to mobility issues of some participants, researchers and student observers notified participants 15 minutes or more prior to the start of the session. Mobility issues ranged from psychomotor retardation, use of wheelchairs or walkers, Parkinson s Disease, and shuffling gait due to various neurological and physical difficulties. During this time, the consultants, participants, and observers gathered in a large open room typically used as a dining and common area. Student observers were allowed to view the group from outside the group circle. The residents were familiar with the students and allowed them to observe the group and collect questionnaire data immediately after the group session. The area where the consultants and researchers conducted the group was sufficient for the size of the group. The setting was a large dining room where a holding environment and emotionally safe atmosphere could be created and contained (Winnicott, 1971/2009). This common room was already known to participants as a comfortable location in the facility and welcoming area. Prior to the start of the group session, researchers arranged 30 chairs, plus three additional chairs for the consultants, into a large circle. While a large circle formation of chairs is not typical of the Tavistock method (de Mare, 2011), this set-up was utilized to reduce anxiety of the group due to the participants severity of symptoms as well as accommodate for participants mobility issues. This circle arrangement also is more compatible with cohesive interactions, more calming, consistent with previously conducted small group settings, and familiar to residents. De Mare (2011) posits that this circle arrangement is more conducive to the sense of dialogue that is crucial in the positive psychosocial matrix of a group having between members. Members of the group chose their placement in the group during the session. The participants requiring assistance or exhibiting mobility issues were located near the entrance ~ 16 ~
149 Volume 20, Number 2 July 2016 December 2016 of the group circle. Researchers removed from the group circle all wheelchairs and other assistive devices for walking in order to minimize distractions during the group session. Therefore, all members were seated in chairs. At the start of the session, staff closed the doors to the room where the sessions were held. Researchers asked all residents who did not participate in the group study to remain outside of the room during the group session. Several members who utilized wheelchairs and walkers were helped by certified nursing assistants (CNAs) to obtain placement in chairs located around the group circle. The group session started with the sounding of a Tibetan bell. This auditory cue signaled the beginning and completion of each group session. The residents of the facility are familiar with the auditory cue and recognize it as the start of a Tavistock group since it was used as a signal in the pre-existing small groups. After the cue, the group session convened for 50 minutes without a break in the session. Group sessions included three primary consultants trained in both the traditional and modified Tavistock models. These consultants were licensed psychologists and conducted previous Tavistock groups (Semmelhack, Ende, & Hazell, 2013). Consultants adhered to the modified (Semmelhack, Ende, & Hazell, 2013) Tavistock model as closely as possible. At the completion of the session, the consultants provided a 15 to 30 minute period of time as a trauma reduction period where members could discuss issues linked with heightened anxiety either due to the group or some other factor (2008). Adhering to the traditional style of the Tavistock model, consultants refrained from providing the residents with a specific topic for discussion at the onset of each large group session (Bion, 1954; Colman & Geller, 1985). Consultants refrained from prompting residents during the group to discuss specific topics even during times of excessive silence. At the completion of the large group sessions, researchers collected data regarding participant experiences through questionnaires derived from previous studies (Semmelhack, Ende, & Hazell, 2013) and generated specifically for this study. Researchers and graduate level students administered the 15 question questionnaire. This questionnaire assessed data regarding the participants personal experience during the group session. At the end of the questionnaire, participants could provide additional comments/opinions regarding the group experiences. Graduate students and researchers collected the data after the completion of the group session and the group processing session. Structure of the Group Session The structure of the large group session reflected that of small group sessions held at the facility and based on a modified Tavistock model. The large group session followed the modified Tavistock model (Semmelhack, Ende, & Hazell, 2013; de Mare, 2011). Consultants conducted a 50 minute session with no breaks during the session. Three primary consultants positioned themselves around the group circle interspersed between the participants of the group during the session. Participants discussed any topic they chose to discuss without any overt or explicit influence from the consultants. Consultants provided interpretations and comments when they felt it was appropriate for the group members. However, consultant roles fell into various orientations including: providing descriptions of group interactions and processes, commenting on thematic developments, and interpretations of comments. The roles of the consultants were not assigned and consultants changed between roles depending on the needs of the group. Additional considerations were given to contextual influences on the group including facility events, time based boundaries, and general emotional tone of the group. Consultants and student observers would meet for 30 minutes prior to each large group session to share their personal process as it related to their work in the group, to recall the themes of the previous group, to assess any events that had occurred in the immediate and even wider context of the group and to examine their own internal dynamics as a team. ~ 17 ~
150 Volume 20, Number 2 July 2016 December 2016 Consultants to the group reduced the structure of the group sessions to 50 minute duration in order to encourage a flowing group. This open structure also allowed for group processes and themes to emerge and participants not be influenced by consultants or facility members. However, during the first large group session, consultants introduced and explained the purpose of meeting in a large group and explained the general procedure of the group (i.e., how long the group will run, that the group is open to anyone, the group is voluntary). At the completion of the group session, consultants and researchers provided time for the group to debrief and process the group session. This ten minute period of time allowed for the participants to ask questions, provide comments, and share experiences with other members and consultants. The debrief time was not an extension of the therapeutic Tavistock group. Rather, this time was unstructured and participants would choose to engage in the discussion or leave the room during this time. Group Participants Residents living at a long-term care nursing home located in the Midwest participated in the group sessions. Participants of the group ranged in age from 42 to 75 years old. The group was comprised of both males and females diagnosed with severe mental illness (e.g., Bipolar Spectrum, Schizophrenia Spectrum). In most group sessions, more females (M = 15.33) compared to males (M = 8.67) participated in the group session. The participants resided at the facility for a minimum of one year. However, most participants resided at the facility for more than three years. Table 1 Demographics of Participants Questionnaires Completed per Group Participants of the large group also previously attended small group versions of the modified Tavistock sessions that other consultants conducted on a different day of the week. These small groups were comprised of 15 members or less, but the groups drew on the same set of residents. The membership of the large group sessions ranged from 21 to 26 participants. The groups were also comprised of mainly Caucasian individuals (98%) with one African American male attending a group session and one African American female attending a different session. Most participants also were diagnosed with various medical diagnoses (e.g., Type 2 diabetes, Tay Sachs, Mild Intellectual Disability) in addition to their mental illness diagnosis. Schedule of the Group Session Researchers of the study conducted the large group sessions on one Sunday each month. Due to scheduling of activities in the facility, Sunday afternoons provided to best time for the group to be conducted with little interference. Keeping a consistent time for the group sessions provided the residents structure and a predictable time for the group in order to promote a routine to avoid confusion and/or anxiety regarding timing of the group. Researchers conducted the group sessions from 1:30pm to 2:20pm including the time for set-up, session, and debriefing. Assessments Used in the Study Mean SD % Age Attendance in Group Gender Males per Group Gender Females per Group ~ 18 ~
151 Volume 20, Number 2 July 2016 December 2016 To determine any effects from the group session, the researchers recorded and examined major themes from the group sessions using a qualitative/thematic analysis and provided a non-standardized questionnaire specific for the study to the participants. The data collected for this study is qualitative and should be reviewed as such. There are few standardized assessments available to adequately assess the Tavistock model, especially for a large group design. Therefore, it was determined to be more valuable to collect qualitative data (i.e., anecdotal data, transcripts from sessions), behavioral observations, conduct a thematic analysis, and collect questionnaire data to determine the effects of the study on group participants. During the group sessions, graduate student observers recorded behavioral observations, comments, and consultant interpretations. After the group session ended, researchers examined the observations and determined major themes occurring during the sessions. Participants also were allowed to provide any additional comments to the observers and consultants at the end of a session. The data from the behavioral observations and the anecdotal evidence is beneficial since it provides a real account of the experiences of participants that may not be captured using standardized assessments. This study also utilized a non-standardized questionnaire to assess the participants reactions and experiences. This 15-question non-standardized questionnaire provided additional objective data from the sessions. This questionnaire was designed for this study due to a lack of specific assessments assessing the variables in the study and is derived from the Current Status of Group Cohesion Scale (Treadwell, Lavertue, Kumar & Veeraraghavan, 2001) and previously used assessments (Semmelhack, Ende, & Hazell, 2013). Using a combination of items from other assessments (e.g., group cohesion scales) and novel items, the questionnaire was constructed and adapted for the long-term care residents diagnosed with severe mental illness. Participants were provided the option to answer the questionnaire on their own or with the assistance of graduate students. These accommodations were needed for some participants due to physical disabilities, verbal comprehension, and/or medical issues. Graduate level psychology students verbally administered the participants the questions on the questionnaire. Participants were then allowed to include additional comments about the group session and rate their answers using a Likert scale range. The questionnaire questions used a 5-point Likert scale with a range of 0 to 4. The questions focused on topics relevant to group dynamics and Tavistock research. For example, these topics included level of group comfort, self-reflection and insight, group size preference, and group cohesion. Together, these two forms of assessments allow for the researchers to identify major themes and events prevalent in the sessions. Also, the anecdotal evidence provided subjective evidence for the participants experience of the group. Thus, the data collected examined the objective and subjective experiences of the group members to the best of their ability. For the behavioral observations, graduate student observers recorded various overt behaviors. Shifts in facial expressions, the frequency of responses, and/or the rate of responding were some behaviors observed and collected for the study. Group participant attendance, participant drop out during the session, and changes in seating are additional factors that were observed and collected. Results: After the completion of six consistent group sessions, researchers compiled questionnaire results and examined the collected data. Due to the nature of the design of the study, only the questionnaire data can be examined quantitatively. Therefore, a discussion of the results from the questionnaires will be included in this section. Please refer to later sections for thematic and process qualitative data. Questionnaire Results ~ 19 ~
152 Volume 20, Number 2 July 2016 December 2016 Researchers surveyed participants of the groups directly after the completion of each group session. In order for data from the questionnaires to be included in the data analysis, participants needed to complete at least five of the six possible questionnaires. A total of 42 participants completed at least one questionnaire. However, after six group sessions, a total of 14 participants completed at least five of six questionnaires. This small sample of participants resulted from external factors (i.e., inconsistent group attendance, change in health status, refusal to complete a questionnaire, death). Table 2 Questionnaire Results Variable Mean F p value Pre-group Comfort * Post-group Comfort Level of Connection Desire to Express Feelings Desire to Express Thoughts Consultants Provided New Ways of Thinking Insight * Enjoyment * Group Size Comfort * Listened to by Consultants Participation Desire for Continuation of Large Group * Consultant Support Group Size Preference Feeling Ignored *p<.05 A repeated measures analysis of variance (ANOVA) was conducted examining the 15 variables of the questionnaires at three separate time intervals. From the analysis, five variables were statistically significant. These variables included: Pre-group Comfort (F = 4.371, p<.05), Insight (F = 6.207; p<.05), Enjoyment (F = 5.945, p<.05), Group Size Comfort (F = 5.198, p<.05), Desire for Continuation of Large Group (F = 6.203, p<.05). These results indicate that there were significant increases in ratings on these variables over the course of six months. As for the other variables examined, there were also increases in ratings; yet, these changes did not meet statistical significance. Results indicated that there were significant differences between the scores of five variables. After six sessions, the group members reported increased comfort, insight, enjoyment, and a desire for the group to continue. Topics Covered In The Group During the group sessions, common themes based on the residents emotional states, common experiences, and facility events emerged. Some of these themes emerged and explored frequently including themes of power, ~ 20 ~
153 Volume 20, Number 2 July 2016 December 2016 loss, anxieties, and hopes for the future. Many of the group themes that occurred were greatly influenced by the context of the group, recent events at the facility, and time of the year. Therefore, the second portion of the study examined the frequency of the most common themes during the group discussion. The most frequent themes that emerged over the course of the time of the group included Intense Emotions (i.e., Anxiety, Hostility, Depression), Interpersonal Relationships, Coping Skills, Human Contact, Interpersonal Roles, Existential Themes, and Suffering/Struggles. Additional themes were present. However, these themes of control, authority, and power did not emerge until later sessions. Table 3 Common Themes Theme Frequency % Communication 3 50 Human Contact 4 66 Interpersonal Relationships/Interactions 5 83 Interpersonal Roles 4 66 Intense Emotions (i.e., Anxiety, Hostility, Depression) Existential Themes 4 66 Community 2 33 Safety 2 33 Power/Authority 2 33 Suffering/Struggles 4 66 Group Roles 2 33 Coping Skills 5 83 Trauma/Negative Life Events 1 17 Trust/Faith 3 50 Religious Themes 2 33 Helplessness vs. Hopefulness 2 33 Sense of Self/Self Themes 2 33 Goals 1 17 Control 0 0 Change 0 0 Discussion: This study examined the effects of a modified Tavistock approach (i.e., large group application, circle formation) on a group of individuals residing in a long term skilled nursing care facility and diagnosed with severe mental illness. This study utilized a 15 question non-standardized questionnaire to assess the participants reactions and experiences to the group process and additional objective data from the sessions. This questionnaire was designed for this study due to a paucity of specific assessments assessing the variables in the study ~ 21 ~
154 Volume 20, Number 2 July 2016 December 2016 and was derived utilizing items from other assessments (e.g., group cohesion scales) and novel items. Furthermore, the questionnaire was constructed and adapted for the long-term care residents diagnosed with severe mental illness. As hypothesized, participants reported increased ratings on the variables assessed by the custom questionnaire. However, only five of the 15 variables appeared to achieve statistically significant increases. From the questionnaire results, the large group adaptation resulted in increased enjoyment in the group, insight, group size comfort, pre-group comfort, and a desire for the group to continue. From the thematic analysis, common themes included intense emotions (i.e., Anxiety, Hostility, Depression), interpersonal relationships, coping skills, human contact, interpersonal roles, existential themes, and suffering/struggles. This study has several weaknesses. There is no control group and the measures may be biased by respondents giving subjective evaluations. It must also be recalled that the participants were exposed to and experienced in the Tavistock modality in small group format having participated in such events for several years previously. However, the data of these group processes is experiential and gives other practitioners ideas as to what to expect when running such groups themselves. If it is recalled that the study is only intended to demonstrate that such a group is possible and desirable in at least one instance, then the findings are positive. These individuals with severe diagnoses were able to function and derive benefit from participating in a large Tavistock group for over a year. This is consonant with the expectations found in the writings of de Mare (2011) for example. This study demonstrates the potential utility of large Tavistock groups as a treatment modality for patients with severe diagnoses to such an extent that further studies with better controls and measures would be worthwhile. Conclusions: This study furthers research on both Tavistock group approach and group therapy in long-term care facilities. Due to the nature of long-term care facilities, the study illustrates that residents in long-term care facilities experience intense emotions, concerns about existential issues, and interpersonal issues. Therefore, group approaches such as the style used in the study may be effective and beneficial for residents by providing an outlet to address some of these common themes. It should be noted that as the group sessions progressed, additional themes focusing on power, authority, community, and sense of self were beginning to develop. While this study utilized both a questionnaire and thematic analysis as the basis for collecting data, the use of more formal assessments and analyses would be prudent. For example, future studies could include assessing levels of anxiety and/or depression before and after the completion of the adapted Tavistock group. Additionally, future studies may wish to examine the impact of community and community development in long-term care facilities using Tavistock group approaches. Financial Disclosures: Dr. Diana Semmelhack is the on staff psychologist employed at the location where this study was conducted. There were no other financial incentives, grants, or donations for the study. All participation was voluntary and no outside or private incentives were used during the study. References Bion, W.R. (1954). Group dynamics: A re-view. In M. Klein, P. Heimann & R.E. Money-Kyrle (Eds.), New directions in psycho-analysis (pp ). New York: Basic Books. Blanchot, M. (1988). The unavowable community. Station Hill Press. ~ 22 ~
155 Volume 20, Number 2 July 2016 December 2016 Bry, A. (1984). Est: Erhard seminars training: 60 hours that transform your life. Avon Books. Colman, A.D. & Geller, W. H. (eds) (1985). Group relations reader 2. Washington, DC, A. K. Rice Institute. de Mare, P. (2011). Koinonia: From hate through dialogue to culture in the larger group. London: Karnac Books. Devereux, G. (1980). Basic problems of ethnopsychiatry. University of Chicago Press. Edelson, M. (1970). Sociotherapy and psychotherapy. University of Chicago Press. Erikson, E. (1993). Childhood and society. W.W. Norton. Freud, S. (1922/1990). Group psychology and the analysis of the ego. W.W. Norton. Hazell, C. (2005). Imaginary groups. Bloomington, Indiana: Authorhouse. Jaques, E. (1954). Social systems as defense against persecutory and depressive anxiety. In M. Klein, P. Heimann & R.E. Money-Kyrle (Eds.), New directions in psycho-analysis (pp ). New York: Basic Books. Jones, M. (2013). Social psychiatry: A study of therapeutic communities. Routledge. Kardiner, A. (1939). The individual and his society. New York, Columbia University Press. Kreeger, L. (2012). The large group: Dynamics and therapy. London, Karnac Books. LeBon, G. (1895/2002). The crowd: A study of the popular mind. Dover. Nancy, J-L. (1991). The inoperative community. University of Minnesota Press. Roheim, G. (1971). The origin and function of culture. Anchor Books. Seikkula, J. and Arnkil, T.E. (2006). Dialogical meetings in social networks. London: Karnac. Semmelhack, D., Ende, L. & Hazell, C. (2013). Group therapy for adults with severe mental illness: Adapting the Tavistock method. New York, NY: Routledge. Semmelhack, D., Ende, L., & Hazell, C. (2015). The interactive world of severe mental illness: Case studies of the U.S. mental health system. New York, NY: Routledge. Sullivan, H. S. (1968) The interpersonal theory of psychiatry. New York, NY: Norton. Treadwell, T., Lavertue, N., Kumer, V.K., & Veeraraghavan, V. (2001). The group cohesion scale-revised: Reliability and validity. International Journal of Action Methods, Psychodrama, Skill Training, and Role Playing, 54, Winnicott, D.W. (2009). Playing and Reality. New York, NY: Routledge. ~ 23 ~
156 Volume 20, Number 2 July 2016 December 2016 Yalom, I. D. & Leszcz, M. (2005). The theory and practice of group psychotherapy, 5th edition. New York, NY: Basic Books. ~ 24 ~
157 Volume 20, Number 2 July 2016 December 2016 Human Rights of Mentally Ill Clients Dr Hitesh Sheth Superintendent and Psychiatrist Hospital for Mental Health Vikas Gruh Road, Jamnagar,Gujarat, India Citation: Sheth H.(2016) Human Rights of Mentally Ill Clients. International Journal of Psychosocial Rehabilitation. Vol 20 (2) Abstract Human rights are important for all strata, classes and races of the society. But it assumes special significance for mentally ill clients, who because of their vulnerability due to illness, often fail to prevent violation of their rights. Often the violation of rights occurs right from the admission in mental hospital, until discharge from the hospital. Frequently, the same violations of the rights of the mentally ills also occur in prisons, shelter homes and streets. Often the very efforts to protect the rights of mentally ill clients lead to violation of the rights. The group, which is marginalized, discriminated and stigmatized by the society, can only be helped by the society. The society can help the mentally ill clients by enacting laws favorable for them, by providing proper facilities for community based treatment, protecting their rights at mental hospitals and by rehabilitating them in society after discharge from the hospital. KeyWords: Human right violations, Mental Illness, Stigma, Mental Hospitals, Restraint of Mentally Ill Introduction: The human rights of mentally ill clients are very important because, unlike other aggrieved groups, they are unaware of their rights most of the time, hence do not stand up and fight for them. People suffering from mental illness are among the most disadvantaged groups in society. Further, they suffer severe personal distress and they are stigmatized, discriminated against, marginalized and often left vulnerable. [1] The protection of rights becomes more pertinent in a mental hospital because the moment a client enters into the hospital, he cannot venture outside the hospital premise on his own volition, unless a doctor certifies that he is fit to do so. Once in the institute his moments, if not restricted are not as free as they are in the outside world and his daily activities are likely to be scheduled according to the hospital rules. Everyone has the basic human rights, including those who are mentally ill. Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, and housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other ~ 25 ~
158 Volume 20, Number 2 July 2016 December 2016 lack of livelihood in circumstances beyond his control. [2] People with mental illness commonly experience violations of rights, including their economic and social rights. One of the reason for ill treatment of the clients may be due to decreased or absent contribution in the economic field by mentally ill clients unlike the clients having medical illness. [3] The Mental Health Act (MHA), 1987, came into force in It repealed the much-criticized the Indian Lunacy Act, The aim of the act was to protect the human rights of mentally ill people, but many people involved in the field feel that the law has too many lacunae and needs urgent attention. The findings of the recent study concluded that the human rights of people with mental illness were not protected influencing their reintegration into the community.[4] World Health Organization (WHO) states that we are facing a global human rights emergency in mental health as many countries lack the basic legal framework to protect those with a disability.[5] Human rights at Mental Hospitals: As nations have flags as their symbols of patriotism, so humanity has unreformed mental hospitals as symbols of human right violations. When one undertakes a task to improvise facilities at the mental hospital, one should not lose sight of the fact that one is improvising the facilities of a prison like structure which, even if turned into gold would still retain its original character of a prison. The condition in mental hospitals is often grim in absence of cleanliness, hygiene, entertainment facilities, restricted freedom to move at will and poor staff to client ratio. Often the hospital lacks psychiatrists, good paramedic support, psychiatric social workers, clinical psychologists or occupational therapists on board to fulfill the requisite angles of the treatment being meted out. [6][7] The study conducted in the tertiary care institute in India concluded that the human rights of people with mental illness were not protected that influenced their reintegration into the community. [8] Many a time, even when clients get cured his or her guardians don t turn up and such clients are forced to languish in mental hospitals, despite being fully fit to be discharged. Twenty percent of all clients in mental hospitals in Kolkata are fully fit to resume their normal life, but because of lack of rehabilitation facilities and post-care treatment, these people are condemned to languish in the hospitals that are no more than jails. [9] The other consequence of this development is overcrowding of the hospitals because of which deserving clients do not get proper treatment at the institute. [10] Many a time hospital staff witnesses a condition in which a cured client becomes aggressive because he or she cannot be sent home due to various reasons and the client may develop suicidal wishes or a wish to escape from the hospital. In an ideal Utopian world, facilities like adequate and hygienic space, air-conditioning, heaters, privacy, means of entertainment, gainful employment, etc., should be available to inmates of custodial homes like mental hospitals, jails, juvenile homes, etc. The same facilities should be available to inmates of shelter homes, halfway homes, quarter way homes, beggar's home, daycare shelters and rehabilitation centers. However, the truth is the significant number of the population of the world lacks even basic needs like food and shelter. Due to recession and other factors, government over the world is pulling out their hands from social spending. New York a city of developed country famous for glitz, glamour and billionaires is having a dubious record of 60,000 people, who are homeless. [11] The governments world over with poor resources is in dilemma to provide the home to poor people first or to mentally ill first. Such a situation necessitates judicious use of available resources as well as a sustained effort with government for allocation of required resources. Violation of Human Rights at Mental Hospitals: There are certain sets of problems, which one is more likely to witness in mental hospitals than in any other hospitals. The reasons are, the other hospitals are under the direct vigil of the public, which makes hospital staff and authorities alert to the clients problems. The second is, in other hospitals, client themselves are alert for their rights, which makes staff and administration sensitive to clients requirements, while in case of mentally ill clients they are completely at the mercy of the hospital staff.[12] Perhaps, the first violation of human rights occurs when a client is admitted in unreformed mental hospital. Human right is violated when a cured ~ 26 ~
159 Volume 20, Number 2 July 2016 December 2016 mentally ill and well-fed client yearns for freedom in a mental hospital. The scene frequently repeated in the mental hospital is client cured, half cured or uncured, yearns for discharge from the hospital and his relatives or caretakers unwilling to take him back at home. The psychiatrist working in the institute becomes an unwilling judge in the battle of wills. The psychiatrist again becomes unwilling judge when he has to choose whether the interest of the client is paramount or interest of his relative. He becomes unwilling judge when he has to choose between the safety of his psychiatric practice and interest of a paranoid and potentially litigious client. Similarly, human right is violated when a wandering mentally ill yearns for shelter and food on the streets. Human right is violated, when a cured client cannot be sent back home because either his relatives are unwilling to take him back or he doesn't have a home where he can be sent back. Human right is violated, when the valid anger or aggression of a cured client who wants discharge from the hospital, is controlled with involuntary admission of drugs. Human right is violated, when a mental hospital is established without rehabilitation centers in its vicinity. Human right is violated, when past history of mental illness is invoked to; intimate the client, control him or coerce his normal behavior. Human right is violated, when admission in a mental hospital is used as a pretext to control the property of the client. Human right is violated when a client lives in constant fear that he would be admitted in the hospital for the vested interest of his relatives, e.g. for a purpose of divorce or to usurp his property. Human right is violated when a client is made to work against his will in a mental hospital for fear of being punished or for a petty reward like cigarette or tobacco. Human right is violated when the client doesn t receive evidence based treatment. Human right is violated when clients are used for clinical trials without their consent. Human right is violated when the administrative authorities of mental hospital are not vested with adequate power and protection against the delinquent staff working at the institute. Human right is violated when the adequate and hygienic space, privacy, means of entertainment, gainful employment, etc., are not available to inmates of mental hospitals. Human right is violated when a client feels more comfortable in hospital than at home due to economic circumstances. Human right is violated when a prisoner develops mental illness in a prison. Human right is violated when a person is imprisoned, even when he breaks a law in a state of mental illness. Human rights are violated of both, a doctor and a client, when the former cannot give adequate time to the client due to work overload and the later cannot get proper attention for the same reason. Human rights are violated when mental health care is not geographically accessible according to WHO(World Health Organization) guidelines.[13] Human right is violated when an evolving science of psychiatry is used to label a person with revolutionary thoughts as lunatic to force him into conformity. Human right is violated; when a doctor short of time uses a nascent science of psychiatry, in haste, to label the client with psychiatric illness, the criteria of which changes from time to time. Human Rights and Restraint of mentally ill: Physical restraints of people with mental illness have a long and infamous history that starts with a period of ancient Greece, where mentally ills were chained, to the dark period of Bedlam hospital, wherein shackled clients were put on display for the price of a penny. [14] In Indonesia, there is a practice known aspasung, in which people with mental illness are chained, tied, confined in small rooms or sheds, or have their legs in wooden stocks. [15] The process of freeing the people from physical restraints was started by Philippe Pinel and Jean-Baptiste Pussin who are credited with releasing the mentally ill from the chains at the Bicêtre and the Salpêtrière hospitals in Paris at the end of the 18th century. [16] The same process of releasing clients from the restraint continues today with a goal of releasing clients not only from the physical restraints but also from the unnecessary chemical restraints. In ideal conditions of a Utopian world, no mentally ill human being should be physically restrained or kept in isolation. Some would say the ideal thing would be the use of chemical restraints not physical restraints during hospitalization. But whether we restrain client's hands by mechanical restraints or client's brain cells by unnecessary chemical restraints (neuroleptics means grasping the neurons), it is the same thing. The latter thing may be aesthetically more pleasant, but is more damaging to the human soul and mind than the former thing. The unnecessary chemical restraints may not show outer scars on the body, but it definitely causes neuronal ~ 27 ~
160 Volume 20, Number 2 July 2016 December 2016 scars, which manifest eventually as tardive dyskinesia and other adverse effects. Desire for freedom: A Core of Human Rights: The desire for freedom, is a linchpin of human rights, which forms core not only of the human beings but also of the animal beings. The ancient Indian civilization has advocated four goals for human life namely dharma (righteous conducts), artha (material and social needs), kama (sense pleasures) and moksha (freedom). The Supreme Court of India, while delivering one landmark verdict gave paramount importance to personal liberty and said that no one will ever barter his liberties for all the teas of China, all the pearls of the seas and all the stars of the sky.[17] The freedom also includes the freedom from a stigmatizing diagnosis. Often, the process of diagnosing the clients itself is a stigmatizing process, producing mental scars which are difficult to be hidden, even if one applies a makeup of Destigmatizing Campaign. A diagnosis of psychiatric illness hinges on a base of reality testing. However, according to Albert Einstein, reality is an illusion albeit a very persistent one. [18] So to diagnose the mental illness solely on a base of reality testing becomes a tad unscientific, unless it is done with humility that the diagnosis one putting is a temporary construct about the condition one know very little. Instead of diagnosing the clients with stigmatizing diagnosis like schizophrenia that denotes that unlike normal people, only the people suffering from mental illness are in two minds; one can use Japanese terminology like Integration Disorder, which may better reflect the true nature of an underlying disorder. [19][20] It is not difficult to imagine the plight of wandering homeless mentally ill client, who has been admitted in mental hospital and cured subsequently. The client cannot be sent home as he or she is without a home. The condition becomes poignant when the client does not want to go in shelter home or rehabilitation home. Moreover, it is not legally or morally appropriate for hospital authorities to release the client on the road from a custodial care hospital. Similarly, it is not appropriate to see the cured client languishing and thus suffering in mental hospital. The paternalistic role of welfare state directs to take care of wandering mentally ill person and put him or her into some institution, but what if some person is happier wandering like a fakir or mendicant than being confined to a mental hospital or other custodial care institution. What if some person writes in his advance directive that should he develop mental illness in the future, he should be left alone as wandering ill and ill-fed rather than be confined to some custodial institution and be fed well. In such a situation should state take away the freedom it provided to the person on the bases of which he chose freedom or should it renege on its promise to provide freedom. Human rights: More emphasis leads to more violation: Everything in excesses is bad and it may be true with the advocacy of human rights as well. Ideally, there should be no overcrowding in mental hospitals, but if rules be followed strictly without adequate numbers of mental hospitals in the country, then it may lead to overcrowding of mentally ill clients on the streets and in prisons. [21][22] When the institutions that cater to the needs of mentally ill clients, are under excessive legal or public scrutiny, they become defensive in response to challenges thrown by the mental health field. They may order the unnecessary investigations for clients to avoid blame in case of any eventuality. This may not only increase the overall cost of treatment, but also cause mental harassment to clients and their relatives and the indirect violation of human rights. Excessive scrutiny may avert an incident of a major human right violation, but the resultant sum-total of minor human rights violation that would ensue because of such scrutiny would far exceed the total number of gross human right violations. Ideally the mentally ill clients should be investigated thoroughly (including CT Scans and MRI Scans) before he receives the diagnosis of mental illness. However, this would amount to a colossal waste of already meager resources. The 18th century English philosopher formulated what came to be known as 'felicific calculus': a means by which to gauge how to ensure the greatest amount of happiness for the greatest number. Therefore, according to this principle, there is little harm in skipping certain procedures, if re- ~ 28 ~
161 Volume 20, Number 2 July 2016 December 2016 sources are scarce and the benefits that would accrue from such money saving steps would far outweigh the possible harms. However, such omission should be legally protected as it is done in New Zealand. [23] The excessive scrutiny may lead mental health professional to defensive practice. The defensive practice can be defined as ordering of treatments, tests and procedures for the purpose of protecting the doctor from criticism rather than diagnosing or treating the client. [24] Defensive medicine takes place when doctors prescribe unnecessary tests, procedures or specialist visits (positive defensive medicine), or avoid high risk clients or procedures (negative defensive medicine). [25] These types of practice occur whenever a practitioner gives a higher priority to self-protection from blame than to the best interests of the client. A large number of legal initiatives taken by clients have induced many doctors to adopt a defensive strategy to avoid jeopardizing their careers. Controversies in mental health, and occasional tragedies, are often the subject of close media attention and reporting which may be inflammatory. [23] A mail survey of physicians in Pennsylvania concluded that nearly all (93%) reported practicing defensive medicine. [26] The study conducted in England concluded that almost three quarters of the psychiatrists who responded had practiced defensively within the last month of the survey.[27] Therefore, No blame and learning culture, is essential for the delivery of quality health care services.[28] The same trend of defensive practice also seeps in the management of custodial setup. Ideally, one should give more freedom to clients by building the setup of mental hospital in such a way that it doesn t appear like a prison or a jail. However, from such setup if client escapes, then it leads to a kind of inquiry. The other option to employ more staff who can keep watch over clients in such setups often violates the privacy of the client and escalates the cost of maintenance of the hospital. Therefore, because of this fear, hospital staff restricts the movement of the client and thus violates human rights. In many mental hospitals in India, the death of the inmate is investigated by police and death audit committee. Similarly, in western countries, critical incidents, such as suicides, homicides, and deaths while detained under the Mental Health Act are investigated by both trust and coroner s inquest. The investigations may be followed by negligence claims from the relatives. These investigations may provide the source of incentives to act defensively. When the professionals feel that their each and every action they take or action they avoid are under scrutiny and are liable to be dissected by a group of people, they may choose a field in which a risk of litigation is less. The net result would be a shortfall of professionals in such institutes or if the professionals are available there are chances that they are not the best in their field. No wonder Bombay high court recently opined that the conditions of mental hospitals were deplorable and no psychologists or psychiatrists were available at any of the hospitals and none of the hospital had a rehabilitation program. [29] Still, surveillance and the inquiry of untoward incidents are necessary, but it should be in such a way that it doesn t cause violation of human rights, intentionally or unintentionally, it intends to protect. Role of Mental Hospital in Protection of Human Rights: Until the better option of mental hospitals is found, mental hospitals still have some role to play in the treatment of mentally ill clients. Clients in some state mental hospitals were poorly treated, mistreated, or maltreated in the past does not mandate that a new public mental hospital system would do so. Opponents of reinvigorating the public mental hospital system argue for community programs. Community programs are important, but serve a different purpose in the continuum of care for the severely mentally ill. [30] If we don t provide a safe institutional environment for aggressive and violent clients, more psychiatric hospitals will close leading to those clients being secluded and restraint in the non-therapeutic environments of prisons and jails. [31] Therefore, this approach of treating the client solely in community, leads to undesirable consequences like: utter neglect of the client by his relatives; frequent contact with criminal justice system and more people in beggar homes, shelters, streets and jails instead of mental hospitals.[32] Another benefit of a ~ 29 ~
162 Volume 20, Number 2 July 2016 December 2016 psychiatric institution is that it can provide centralized, coordinated care for an individual with severe mental illness, when the available psychiatric services in the community are fragmented and are poorly coordinated. [33] individual, regardless of whether or not they have been assigned a psychiatric diagnosis, is expected to undergo some experience that limits the harm they can generate. [34] If we consider parents insistence on sending a reluctant child to school as human right violation, then the whole world would soon revert to a stone age where there would be no human rights whatsoever. When the normal people exhibit the violent behavior, they should be counseled and may be needed to be sent to the jail; same way violent behavior in mentally ill client needs to be controlled first by psychotherapy and antipsychotic drugs and lastly by temporarily confining him or her to a mental hospital.[35] Therefore, violent and uncontrollable behaviors need to be controlled by temporary hospitalization. However, while admitting the client in the mental hospital, one should be aware that it is a temporary measure to treat the client, until he is transferred to halfway home, quarter way home, and shelter home or rehabilitated in society. It is always desirable that all long-term admissions of more than six months should be evaluated by a team comprising, a member of the judiciary, an expert of the social science department and a psychiatrist, with an aim of transferring the clients from inside the hospital. The other important issue is human rights of mentally ill prisoners. The recent study in India showed that 33% of the convicted prisoners were suffering from psychiatric illness. [36] If after giving sufficient treatment a mentally ill prisoner doesn t improve, he may be sent to another institution for treatment and if three or more institutions after giving sufficient treatment, certify that client is not likely to improve then the client may be given a bail to prevent further deterioration of his condition and to minimize overcrowding of the jails and hospitals. The reason for sending a mentally ill prisoner in three or more institutes is to make sure that prisoner gets sufficient treatment by different psychiatrist that would prevent him from subverting the system by faking symptoms of mental illness. Alternatively, if after giving sufficient treatment, if mentally ill prisoner doesn t improve and at the same time if he is not fit to be discharged from the hospital, then he may be converted into a non criminal inmate, which would increase his freedom at the institute and consequently increases the chances of recovery. The treatment in a mental hospital would become useless, if mentally ill prisoner is going to develop symptoms of institutionalization instead of being cured of his illness. Steps to Protect Human Rights: The first step to protect the human rights of the mentally ill client is not to admit him in the institution unless absolutely necessary; instead he should be provided with community based treatment and rehabilitation services. If at all, admission is necessary, he should be ideally admitted in an open ward with relatives for a short duration of time. Admission with relatives would prevent anxiety in a client who is admitted in an unfamiliar place. He should be provided an evidence based treatment during admission. In addition, as soon as he is manageable he should be handed over to his relatives. However, in absence of relatives he should be rehabilitated in halfway homes or a quarter way homes. To admit the client in unreformed institute and then protecting his human rights are like inflicting a wound on a person and then treating it. So the judicious use of available resources would be helpful in protecting the right of mentally ill clients. While dealing with agitated client, the first thing should be employed is verbal de-escalation with or without oral medication. Verbal de-escalation techniques, undertaken with genuine commitment have the potential to decrease agitation and reduce the potential for associated violence, more often than previously thought possible. [37] As far as possible, physical restraints, seclusion and chemical restraints should be used as a last resort while following the guidelines of the institution the client is admitted. While admitting the client, one should be ~ 30 ~
163 Volume 20, Number 2 July 2016 December 2016 aware that it is a stop-gate arrangement, until the client is rehabilitated in society or in some rehabilitation home, which permits more freedom to the client. Conclusion: We have progressed a great deal in protection of human rights of mentally ill; from the past when they were physically restrained brazenly to a recent period, when even the chemical restraints are used cautiously. We have to walk on tightrope to protect human rights because, many a time our very effort to protect human rights by increasing vigilance leads to violation of human rights. Still, more needs to be done in the field that would require multiple strategies that start from judicious use of antipsychotics to increase in awareness in clients and their caregivers. The changes in the nomenclature of disease that stigmatizes the clients may also help in this direction. The Human Right Commissions, civil society organizations, and health professionals and health service provision agencies all have important roles to play in the protection of human rights. [38] Psychiatrists can promote human rights through scrutinizing the admissions in mental hospitals, providing evidence-based medicine, ensuring a short stay of clients in a mental hospital, and actively participating in the rehabilitation of clients in society. References 1. Johnstone MJ. Stigma, social justice and rights of mentally ill: challenging the status quo. Australian and New Zealand Journal of Mental Health Nursing 2001; 10: Universal Declaration of Human Rights, adopted and proclaimed by the United Nations General Assembly by resolution 217A (III) on 10 December Available from: [Last accessed on 2015, Aug 15]. 3. Theodore DD. Human rights in India; Mental health perspectives. Souvenir; human rights in mental health nursing Oct 2009: Poreddi V, Ramachandra, Reddemma K, Math SB. People with mental illness and human rights: A developing countries perspective. Indian Journal of Psychiatry 2013; 55(2): doi: / WHO. Mental health, human rights and legislation: A global human rights emergency in mental health. Available from: [Last accessed on 2015, Aug 25]. 6. Kapur M. Available from: [Last accessed on 2015, April 29] 7. Tasman A.Too few psychiatrist for too many. Psychiatric Times. April 16, Available from: GUID=D7BE0FA8-937A-4FEF E9F45FC1CB1&rememberme=1&ts= [Last accessed on 2015, Aug 25]. 8. Vijayalakshmi P, Ramachandra, Konduru R, Bada Math S, Indian J Psychiatry Apr-Jun; 55(2): ~ 31 ~
164 Volume 20, Number 2 July 2016 December Kumara SV. Oh, for a new law. The Telegraph. Apr 25, Available from: com/ /asp/opinion/story_ asp. [ Last Accessed on 2015, May 1] 10. Nagaraja D, Murthy P, editors. New Delhi: National Human Rights Commission (NHRC) and the National Institute of Mental Health and Neuro-Sciences (NIMHANS). Mental Health Care and Human Rights.2008: Homeless reaches record 60,000 in New York. Times of India. Feb 4, Available from: York/articleshow/ cms.[ Last assessed on 2015, Aug 26] 12. Sheth, HC. Management of the Mental Hospital. International Journal of Psychosocial Rehabilitation 2013; Vol 17(2): Mental Health Legislation & Human Rights: Denied Citizens: Including the Excluded.Mental Health and Prisons. Geneva, World Health Organization and International Committee of the Red Cross, Available from: accessed Feb 21, 2015] 14. Foerschner AM. The History of Mental Illness: From 'Skull Drills' to 'Happy Pills. Student Pulse 2010; 2(9). Available from: Last assessed on 2015, Aug 29] 15. Minas H, Diatri H: Pasung: Physical restraint and confinement of the mentally ill in the community 16. Schuster J-P, Hoertel N, Limsin F:The man behind Philippe Pinel: Jean-Baptiste Pussin ( ).Br J Psychiatry 2011;198: Mahapatra D.SC stays Teesta Setalvad s arrest, promises anticipatory bail. Times of India. Feb 20, Available from: [ Last Accessed on 2015, May 6] 18. Alice C. The Quotable Einstein. Princeton University Press; Available from: [Last accessed on 2015 July 15] 19. SATO M. Renaming schizophrenia: a Japanese perspective. World Psychiatry 2006; 5(1): Sheth HC. Schizophrenia and yogic concepts. Int J Yoga - Philosop Psychol Parapsychol 2013;1: Sheth HC. Deinstitutionalization or Disowning Responsibility. International Journal of Psychosocial Rehabilitation 2009; 13(2): Thakker Y., Gandhi Z., Sheth H., Vankar G.K., & Shroff S. Psychiatry Morbidity Among Inmates of the 'Beggar Home International Journal of Psychosocial Rehabilitation 2007;11(2): Richard Mullen, Anita Admiraal, Judy Trevena. Defensive practice in mental health. Newzealand Medical Journal 2008; 121: McQuade JS. The medical malpractice crisis reflections on the alleged causes and proposed cures: discussion paper. J R Soc Med 1991;84: ~ 32 ~
165 Volume 20, Number 2 July 2016 December Catino M. Why do doctors practice defensive medicine, the side effects of medical litigation. Safety Sci Monit. 2011;15: Studdert DM, Mello MM, Sage WM, et al. Defensive Medicine Among High-Risk Specialist Physicians in a Volatile Malpractice Environment. JAMA. 2005;293(21): Passmore K, Leung W. Defensive practice among psychiatrists: a questionnaire survey. Postgraduate Medical Journal 2002;78(925): doi: /pmj Halligan A, Donaldson LJ. Implementing clinical governance: turning vision into reality.bmj 2001;322: Bombay HC suggests privatisation of state-run mental hospital in Maharastra. DNA INDIA. April 13, Available from: [Last accessed on 2015 July 15] 30. Kramer DA. If It Were Physical Pain, It Would Be Called Torture: A Story of Two Young Men. Psychiatric Times. March 25, Available from: physical-pain-it-would-be-called-torture-story-two-young-men?guid=d7be0fa8-937a-4fef e9f45fc1cb1&rememberme=1&ts= [ Last Accessed on 2015, May 6] 31. Moosa MYH, Jeenah FY. The use of restraints in psychiatric clients. South African Journal of Psychiatry 2009; 15(3). 32. Sheth HC. Deinstitutionalization or Disowning Responsibility, International Journal of Psychosocial Rehabilitation 2009;13(2); Pratt, C. W., Gill, K. J., Barrett, N. M., & Roberts, M. M.Psychiatric rehabilitation (2nd ed.). Burlington, MA: Elsevier Academic Press; Martz E & Newbill W. The Rehabilitation of a Hospital: The Transformation of a State Psychiatric Hospital. International Journal of Psychosocial Rehabilitation 2014; 18(2) Sheth HC. Schizophrenia and yogic concepts. Int J Yoga - Philosop Psychol Parapsychol 2013;1: Kumar V, Daria U. Psychiatric morbidity in prisoners. Indian Journal of Psychiatry. 2013;55(4): doi: / Richmond JS, Berlin JS, Fishkind AB, et al. Verbal de-escalation of the agitated client: consensus statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup. West J Emerg Med. 2011;13: Irmansyah I, Prasetyo YA, Minas H: Human rights of persons with mental illness in Indonesia: more than legislation is needed. Int j ment health Syst 2009, 3(1):14. ~ 33 ~
166 Volume 20, Number 2 July 2016 December 2016 Integration of mental and psychomotor training in vocational rehabilitation for persons with mental illness improves employment Jan Knapen, PhD1,2 Annick Myszta, MSc1 Yves Moriën, MSc1 1. AZERTIE, Boddenveldweg 11, 3520 Zonhoven, Belgium 2. Department of Rehabilitation Sciences, KU Leuven, Tervuursevest, 101, 3001 Leuven, Belgium Citation: Knapen, Myszta & Moriën.(2016) Integration of mental and psychomotor training in vocational rehabilitation for persons with mental illness improves employment. International Journal of Psychosocial Rehabilitation. Vol 20 (2) *Corresponding author: Jan Knapen, AZERTIE Boddenveldweg 11, 3520 Zonhoven, Belgium address: jan.knapen@faber.kuleuven.be Abstract Common mental health problems, such as depression, burnout, personality disorders, anxiety- and somatoform disorders are often associated with unemployment. Employment is for many people with a mental vulnerability not only a source of financial income, but employment also determines their social status and inclusion, identity and self-image. In order to increase the employment rate of people with a mental vulnerability a centre for vocational rehabilitation in Belgium (AZERTIE) developed the I Care program. The I Care program, a combination of psychomotor and mental training, resulted in a employment over than 50% of people with a mental vulnerability. After at least one year employment 90% was still at work. When we compare the employment rate (over than 50%) with the rate of the period before the start-up of the I Care program (10%), we can conclude that the I Care program increased the employment of this vulnerable group five-fold. Keywords: vocational rehabilitation, mental and psychomotor training Introduction: An analysis of data from the National Co-morbidity Survey Replication, a US nationally representative household survey, found that overall impairment was significantly higher for mental disorders than for chronic medical disorders (Druss et al., 2009). Severe functional impairment was reported by 42% persons with mental dis- ~ 34 ~
167 Volume 20, Number 2 July 2016 December 2016 orders and 24% with chronic medical disorders. Mental illnesses increase the risk of decreased workplace productivity and absenteeism resulting in lowered income, unemployment and social exclusion. Common mental health problems, such as depression, burnout, personality disorders, anxiety- and somatoform disorders (physical symptoms caused by mental or emotional factors) are often associated with work absenteeism. In Belgium, mental illnesses are the leading cause of work absenteeism, namely in 46.99% of cases (Rijksinstituut voor ziekte- en invaliditeitsverzekering, 2013). The percentages of unemployed disabled as consequence of disorders of the musculoskeletal system (28.75%) and cardiovascular disease (6.67%) follow in the second and third place. Employment is for many people not only a source of financial income, but employment also determines their social status and inclusion, identity and self-image. For people with a mental vulnerability this is no exception. However, to find and retain employment is for them not an easy task (Knaeps, 2015; Reme et al., 2015). In the Belgian healthcare sector, there is little attention to reintegrating former patients into the labour market. While resuming work right can contribute to the recovery. After all, to many people with mental vulnerabilities, the participation in the labour market is seen as a sign of recovery. People with a mental vulnerability are typically characterized by low self-esteem, depression and anxiety symptoms, and decreased physical and mental resilience (Michon, 2006). This target group has more often than not somatic health problems, primary or secondary associated to the psychological vulnerability (De Hert et al., 2011). Many people with mental vulnerability experience a weak physical fitness, low exercise tolerance, fatigue and a reduced ability to focus, a reduced task tension and stress resistance and increased irritability. In these patients, a weak physical fitness and a low physical self-concept, combined with other barriers to participation in exercise, such as deficient self-motivation and self-enhancement strategies, psychosomatic complaints, lack of any internal locus of control concerning their health, deficit of energy, and general fatigue may lead to a vicious cycle of loss of self-confidence, decreased self-esteem, an increased avoidance of physical activity, and a general physical de-conditioning (Knapen et al., 2015). This downward spiral handicaps their working abilities and employment opportunities. Moreover, personal issues such as family and parenting problems, limited social skills, a low education level, loneliness, social isolation, transport and housing problems, and stigmatization complicate their re-integration into the labour market (Michon, 2006). Success factors and impeding factors in the vocational rehabilitation. The Centre for Research and Consultancy in Care of the KU Leuven (Belgium) carried out research on the vocational rehabilitation of individuals with psychological vulnerability (Knaeps, 2015). The researcher interviewed 24 work counsellors to their vision of the impeding factors and the success factors in vocational rehabilitation. As impeding factors mentioned the work counsellors low motivation, a limited self insight, lack of proper attitudes, serious psychological problems, lack of proper housing and transportation problems, while work readiness, adequate work attitude, self-insight, self-management skills, a good physical health and fitness, and a solid social network right contribute to success in vocational rehabilitation. The I Care concept: integration of psychomotor and mental training in vocational rehabilitation AZERTIE, a centre for vocational rehabilitation in Belgium, guides for over 30 years individuals with a work disability to various attendant functions such as general clerking, networking, administrating or programming. The past 5 years AZERTIE noticed a strong increase in the number of individuals with a mental vulnerability. Initially the dropout of this target group was very high, over than 50% (20% for clients without psychological ~ 35 ~
168 Volume 20, Number 2 July 2016 December 2016 vulnerability), and the employment rate very low, approximately 10% (60% for clients without psychological vulnerability). In order to reduce the dropout and to increase the overall employment rate of this vulnerable group, the director and company doctor of AZERTIE developed the I CARE program. This program is intended for job-seekers with mental disorders, often associated with somatic diseases, that are after a long period of inactivity attempting to reintegrate into the formal labour circuit. From the start the I Care concept was based on the scientific evidence of psychomotor and mental training on the mental and somatic health of this very vulnerable group, under the maxim doing what works" (Cooney et al., 2013; Knapen & Vancampfort, 2014; Silveira et al., 2013). The integration of psychomotor and mental training in the vocational rehabilitation of people with mental vulnerability is an example of good clinical practice for a structural collaboration between the work rehabilitation and the mental health care in Belgium. The I Care team aspires to an efficient and sustainable reintegration in the labour market. Evidence-based approach with the focus on the success factors in the vocational rehabilitation The I Care program strongly focuses on the most important personal success factors in the vocational rehabilitation of people with a mental vulnerability namely, work readiness, the work attitude, the mental and physical resilience, the self image and self efficacy, the severity of symptoms, an internal locus of control, and selfmanagement skills (Knaeps, 2015; Michon, 2006; Reme et al., 2015). The eclectic I Care concept integrates the basic principles of the vocational rehabilitation, the recovery-oriented care, cognitive behavioural therapy, psychomotor therapy, and solution-oriented therapy. Interdisciplinary collaboration and method The interdisciplinary I Care team consists of the director of AZERTIE (clinical psychologist), a company doctor who is responsible for the inclusion of the clients, the medical follow-up and contacts with the treating physicians, and a psychomotor therapist/physical therapist and a clinical psychologist who are respectively responsible for the psychomotor and mental training. The I Care team members work closely with the job counsellors who accompany the clients during their training, internship and employment. The participants of the I Care program follow during their training and accompaniment three sessions per week mental training (1 h 30) and psychomotor training (1 h 30) over a period of 10 weeks. Psychomotor training includes individually adapted fitness training, stretching, yoga exercises and breathing exercises, education around dealing with pain and fatigue complaints, desk gymnastics and ergonomic advice. The mental training consists of various relaxation and stress management techniques, assertiveness training, coping skills with crisis situations, goal setting, verbal and non-verbal communication skills, job skills, and relapse prevention (Reme et al., 2015). The basic philosophy is 'a healthy mind in a healthy body'. Objectives The objectives of the I Care program are to increase and improve the work readiness, the labour attitude, the mental and physical resilience, self image, confidence, target and solution-oriented action, and social skills. Research objectives The primary objective of the study was to investigate the effectiveness of the I Care program on the inflow and maintained employment of people with a psychological vulnerability into the regular labour market. The secondary objective was to evaluate the effectiveness of the I Care program on a number of psychological and physical variables. ~ 36 ~
169 Volume 20, Number 2 July 2016 December 2016 Subjects During the period from May 2010 until present 141 clients participated in the study. The group consisted of people with mood and anxiety disorders, burnout, autism spectrum syndrome, personality problems, psychosomatic disorders such as chronic fatigue and fibromyalgia. Fourteen clients suffered from psychotic disorders. However, these persons were stabilized. Most participants had somatic health problems as well, mainly musculoskeletal diseases and chronic pain. In a number of patients the psychological vulnerability was secondary related to a severe somatic pathology such as cancer. Written informed consent was obtained from all participants before entering the study. Results During the 10 weeks I Care program 27 of the 141 (19.15%) participants dropped out. Immediately after the I Care program 8 of the clients (7.02%) found a suitable job. The remaining 106 clients followed after the I Care program additional training at AZERTIE of which 49 (46.23%) were employed within the year. Currently 24 clients are in training, of which 3 (12.50%) have a perspective on work. Thirty-three participants (23.40%) ended the training without any perspective on paid work. At a follow up after at least one year employment 90% of the clients was still at work. After the 10 week program the participants improved on the variables depression, anxiety disposition, selfesteem, coping style, cardio-respiratory fitness, and fatigue and pain perception. These results will be published elsewhere. Conclusion The integration of psychomotor and mental training in vocational rehabilitation of people with psychological vulnerability resulted in a total employment over than 50%. After at least one year employment 90% of the clients was still at work. The major limitation of the study is the lack of a no-treatment control group. Therefore the results should be interpreted cautiously. Nevertheless, when we compare the total employment rate (over than 50%) with the rate of the period before the start-up of the I Care program (10%), we can conclude that the I Care program increased the employment of this vulnerable group five-fold. Moreover the dropout rate (19.15%) is significantly lower than before (> 50%). The dropout is even significantly lower than those of a global psychiatric-epidemiological study of the World Health Organization (n = 63678) which reports that nearly a third (31.7%) of all people with mental illness stop their treatment preliminary to the intends of the provider (Wells et al., 2013). The team strives to optimize the I Care program by a systematic satisfaction survey and feedback from clients and a continuous internal evaluation by the team members. References Cooney, G., Dwan, K., Greig, C., Lawlor, D., Rimer, J., Waugh, F., McMurdo, M., & Mead, G. (2013). Exercise for depression. Cochrane Database of Systematic Reviews, Issue 9. Oxford: Cochrane Collaboration. De Hert, M., Correll, C., Bobes, J., Cetkovich-Bakmas, M., Cohen, D., Asai, I., et al. (2011). Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry, 10, Druss, B., Hwang, I., Petukhova, M., Sampson, N., Wang, P., & Kessler, R. (2009). Impairment in role functioning in mental and chronic medical disorders in the United States: results from the National Comorbidity ~ 37 ~
170 Volume 20, Number 2 July 2016 December 2016 Survey Replication. Molecular Psychiatry, 14, Knaeps, J. (2015). Vocational rehabilitation: people with mental health problems, vocational rehabilitation counselors, mental health practitioners. Doctoral dissertation. Leuven: KU Leuven. Knapen, J., & Vancampfort, D. (2014). Exercise for depression and anxiety: an evidence based approach and recommendations for clinical practice. In: M. Probst, & A. Carraro (Eds.), Physical activity and mental health in a practice oriented perspective (pp ). Milan: Edi.Ermes. Knapen, J., Vancampfort, D., Moriën, Y., & Marchal, Y. (2015). Exercise therapy improves both mental and physical health in patients with major depression. Disability and Rehabilitation, 37(16), Michon, H. (2006). Personal characteristics in vocational rehabilitation for people with severe mental illness. Doctoral dissertation. Utrecht: Trimbos Instituut. Reme, S., Grasdal, A., Løvvik, C., Lie, S., & Øverland, S. (2015). Work-focused cognitive behavioural therapy and individual job support to increase work participation in common mental disorders: a randomised controlled multicentre trial. Occupational & Environmental Medicine, 72, Rijksinstituut voor ziekte- en invaliditeitsverzekering (2013). Jaarverslag Vijfde deel statistische gegevens (Annual report 2013-part five statistical data). Silveira, H., Moraes, H., Oliveira, N., Coutinho, E., Laks, J., & Deslandes, A. (2013). Physical exercise and clinically depressed patients: a systematic review and meta-analysis. Neuropsychobiology, 67(2), Wells, J., Oakley, M., Browne, M., Aguilar-Gaxiola, S., Al-Hamzawi, A., Alonso, J., et al. (2013). Dropout from out-patient mental healthcare in the World Health Organization s World Mental Health Survey initiative. British Journal of Psychiatry, 202, ~ 38 ~
171 Volume 20, Number 2 July 2016 December 2016 Experiences of otherness among students diagnosed with depression and/or anxiety disorder Kaija Appelqvist-Schmidlechner Senior researcher, Ph.D National Institute for Health and Welfare. Mental Health Unit P.O. Box 30, FI Helsinki, Finland kaija.appelqvist@thl.fi Jenni Wessman Researcher, M.soc.Sc National Institute for Health and Welfare, Equality and Inclusion Unit P.O. Box 30, FI Helsinki, Finland jenni.wessman@thl.fi Annamari Tuulio-Henriksson Research professor, Ph.D Social Insurance Institution, Research department PL 450, Helsinki, Finland annamari.tuulio-henriksson@kela.fi Minna-Liisa Luoma Research manager, Ph.D National Institute for Health and Welfare, Ageing, Disability and Functioning Unit P.O. Box 30, FI Helsinki, Finland minna-liisa.luoma@thl.fi Appelqvist-Schmidlechner K, Wessman J, Tuulio-Henriksson J, & Luoma ML.(2016) Experiences of otherness among students diagnosed with depression and/or anxiety disorder. International Journal of Psychosocial Rehabilitation. Vol 20 (2) Corresponding author: Kaija Appelqvist-Schmidlechner, PhD, Senior researcher National Institute for Health and Welfare P.O. Box 30, FI Helsinki, Finland kaija.appelqvist@thl.fi ~ 39 ~
172 Volume 20, Number 2 July 2016 December 2016 Conflicts of interest: The authors declare that they have no conflict of interest. Funding: The study was funded by the Social Insurance Institution of Finland Abstract Introduction. People with mental disorders sometimes experience that they are perceived as abnormal or different. Aim. The study aimed at investigating the experiences of otherness among students diagnosed with depression and/or anxiety disorder who participated in a psychosocial rehabilitation program. Method. The data were gathered with focus groups by interviewing eight groups of students (n=47) aged years diagnosed with depression and/or anxiety disorder who participated in a rehabilitation program during Results. Seven themes were discovered related to the sense of otherness: 1) Carnival of depression, 2) Stereotypes, 3) Shame, 4) Ethos of self management, 5) Overabundance of help, 6) Minimisation and lack of understanding, and 7) Power of peer support. Conclusion. Sense of otherness is related to stigma experiences which may carry both negative and positive meanings. Health care professionals should be aware of the power of peer support and humour among young adults with mental disorders. KEYWORDS: depression, young people, otherness, stigma, peer support Introduction: Depression in adolescence or in young adulthood may severely impair psychological, social and occupational development indicating a broad, lasting tendency toward psychosocial problems in later life (Kessler et al. 1995).The prevalence of depression increases significantly during the transition from childhood to adolescence (Lewinsohn et al. 1994, Hankin 2009), with the highest incidence at ages 15 to18 (Hankin et al. 1998). The continuity to adulthood is very common (Hankin et al. 1998; Kessler et al. 2012). Lifetime prevalence of major depressive disorder of children in early adulthood varies between follow-up studies of community samples from 23 to 43 per cent (Merikangas et al. 2009). In the WHO Mental Health Survey, the average 12-month prevalence of major depressive episode in developed countries was 7 % among young adults (18 34 years) and of these, only 48 % reported receiving some kind of treatment (Kessler et al. 2010). Individuals suffering from mental disorders are sometimes affected by the experience of being perceived as abnormal or different (Leavey 2005; Moses 2009). The term "otherness" is well established and central to sociological analyses of how majority and minority identities are constructed. The dictionary defines "otherness" as "being or feeling different in appearance or character from what is familiar, expected, or generally accepted (Cambridge Advanced Learner s Dictionary & Thesaurus Cambridge University Press). According to Bauman (1990), the notion of otherness is central to the way in which societies establish identity categories. These social categories shape our ideas about who we think we are and the groups to which we belong. They represent an established social order - hierarchy where certain groups are established as being superior to other groups. Ideas of similarity or difference are central to the way in which we achieve a sense of identity and social belonging. In the view of Bauman, identities are set up as dichotomies, for example, illness represents the opposite of the norm or the ideal of health. (Bauman 1990.) In health sciences, the term otherness has been applied rarely. The focus of research interest has rather been on stigma and stigma experiences, which can be seen as a marker of otherness. Stigma is a social construction that defines individuals in terms of a distinguishing characteristic of mark and, as a consequence, devalues them ~ 40 ~
173 Volume 20, Number 2 July 2016 December 2016 (Crocker et al. 1998). Goffman (1963) describes stigma as a process by which the reaction of others spoils normal identity. The concept of stigma is a power-dependent phenomenon which consists of labeling, stereotyping, cognitive separation, emotional reactions, loss of status and discrimination (Link & Phelan 2001). Due to this process, stigma can be seen as a meaningful indicator of otherness. Stigma and its effects are commonly distinguished into two forms: public and self-stigma (Corrigan & Watson 2002). Public stigma refers to stigmatizing perceptions among the general population whereas self-stigma occurs when people with mental illness self-label themselves as someone who is socially unacceptable. According to Corrigan et al. (2009), self-stigma comprises three steps: awareness of the stereotype, agreement with it, and applying it to themselves. As a result of this process, people suffer reduced self-esteem and self-efficacy. Label avoidance has been seen as a third level of stigma (Ben-Zeev et al. 2010). This is the case when people with mental health problems avoid seeking help from mental health services because they do not want to be categorized as a "mentally ill person" or they do not want to face the prejudice and discrimination that the label entails. Stigma is one of the main reasons why individuals with mental illnesses hesitate in seeking mental health services (Chen-Fang et al. 2005, Schomerus & Angermeyer 2008, Bowers et al. 2013). Studies have shown that only about half of young people with mental health problems had used mental health services (Aalto-Setälä et al. 2002; Sourander et al. 2004; Biddle et al. 2006; Kessler et al. 2010). Self-stigmatization, particularly, has been seen as an important mechanism decreasing the willingness to seek psychiatric help (Corrigan 2004; Cheng-Fang et al. 2005; Schomerus et al. 2009). Moreover, fear of negative attitudes among peers towards people with mental disorder in general may hinder young people with mental problems to seek help (Rose et al. 2007). Stigma has also been seen as a barrier to recovery from mental illness (Link et al. 2001) as it may harm self-esteem among individuals with mental health challenges. Secrecy, shame and limited social interaction are often related with having mental health problems among adults (Link et al. 1989). However, less is known about experiences of otherness among young adults diagnosed with a psychiatric diagnosis. Knowledge on this area is crucial as these aspects have an impact on the quality of life, help seeking behavior and recovery (Link et al. 2001; Ceng-Fang et al. 2005; Schomerus et al. 2009; Ben-Zeev et al. 2010; Bowers et al. 2013). In this study, we set out to investigate the experiences of otherness among young adults with depression and/or anxiety disorder. Study participants were students with these diagnoses who participated in a psychosocial rehabilitation program. Materials and methods Study design This study was a part of a larger evaluation study in which feasibility, perceived impact and benefits of the OPI rehabilitation program for students with depression and/or anxiety disorder were investigated (Appelqvist-Schmidlechner et al. 2015). The project was implemented and funded by the Social Insurance Institution of Finland (Kela) and the study was conducted by the National Institute for Health and Welfare, in co-operation with Kela. The OPI program is an outpatient group rehabilitation program that enables young people to attend psychiatric rehabilitation alongside vocational education. The target group comprised students aged years studying in vocational schools who had a diagnosis of depression and/or anxiety disorder. The rehabilitation program represented a recovery based approach (Anthony 1993) to support students with mental health challenges to cope with their life situation and to accomplish their studies. The program consisted of 18 group sessions and 6 one-to-one sessions. The length of the program was 18 months including a 6 month follow up period. The program was cognitive-behavioral-therapy -oriented with solution-focused approach and led by two counselors. Two service providers offered altogether 8 courses during , each course had a maximum number of ~ 41 ~
174 Volume 20, Number 2 July 2016 December participants. Referrals to the program were mostly made by the school health service, school social workers or community health services. Collaboration with the school - particularly with school social worker and school health service - played an important role in the OPI program. Besides screening for potential participants, they served as a link between the school and rehabilitation providing dialog and consultation between these two parties, in collaboration with the client. (Appelqvist-Schmidlechner et al ) In investigating the program, both quantitative and qualitative research methods were used. The study on the feasibility and outcomes of the OPI program showed positive outcomes in quality of life, learning capacities and severity of depression among program participants (Appelqvist-Schmidlechner et al. 2015) The present study is based on the qualitative data collected in focus groups of program participants. Focus group was chosen as a method as it enables the uncovering of the unique cultural beliefs, values and motivations that affect one's health behavior and well-being (Krueger & Casey 2000). Recruitment and participant selection Altogether 80 students participated in the OPI program and were invited to participate in the OPI evaluation study that has been described in detail previously (Appelqvist-Schmidlechner et al. 2015). Written informed consent and obtained parental consent - in the cases of participants under 18 years old - was received from 70 participant. All of them were invited to take part in one focus group session to be organized in the end of the rehabilitation. Information about the study and the purpose of the focus group was provided. Of the 70 participants, 23 did not attend the focus group for various reasons. According to the program providers, some participants had dropped out the program earlier, some had personal reasons not to attend the session in this particular day and some were reluctant to participate in the focus group. Altogether 47 students (38 females and 9 males) participated in the focus group (5-7 participants in each focus group). All study participants were students in two different vocational schools in Finland (16-26 years, mean age 19, SD 2,15), all with diagnosed depression and/or anxiety disorder. The anonymity of the participants was ensured for ethical reason. As a result, name, age or demographic data about those who participated in the focus group could not be collected. Data collection Eight groups of students aged years diagnosed with depression and/or anxiety disorder who participated in the OPI program were interviewed during The focus groups took place on the premises of the service providers during the last group session. Each focus group was facilitated by two female researchers (the first and second author); one leading the interview and the other supporting the facilitator by specifying questions about important issues, ensuring that all questions were exhaustively discussed and making notes if necessary. All interviews followed a similar structure with a primary focus to collect experiences on participating in the OPI program. The structure was developed by the first and second author and discussed within a project team (including professionals from Kela and the National Institute for Health and Welfare) providing support for the study. The interview started with the clarification of the purpose of the focus group, asking for permission to tape the interview, and then posing questions based on the interview guide. Interviews were semistructured with following themes: Experiences of participating in the program, feelings about starting the program and about telling other people about it, perceived benefits and feasibility of the program, and experiences of integrating rehabilitation and school. In spite of the structured interview guide, the facilitators wanted to ensure the natural flow of the discussion and to avoid controlling the discussion too strictly. Consequently, despite of the fact that the primary focus of the group discussion was not the sense of otherness, this theme was very present and dominant in every group session, thus providing interesting data related to the subject of the present study. The length of each focus group interview was from 40 minutes to 2 hours, typically minutes. Following ~ 42 ~
175 Volume 20, Number 2 July 2016 December 2016 informed consent procedures, the interviews were recorded with the permission of the respondents and transcribed. The length of the recording was altogether 9 hours and 25 minutes (transcribed in 159 pages, single line spacing, font Times New Roman 12). To ensure confidentiality, all identifying information was removed and participants were assigned pseudonyms. Ethical issues The ethical approval for the study was granted by the ethics committee of The Hospital District of Helsinki and Uusimaa and the National Institute for Health and Welfare. Written informed consent was received from all study participants or their parents if the participant was under 18 years. Information about the study and the purpose of the focus group interview was provided. Both researchers that facilitated the focus groups were working at the National Institute for Health and Welfare in Finland as researchers and had previous experiences with this study method and interviewing young people. The researchers were not involved with planning or providing the program. The anonymity of participants was ensured for ethical reason. Data analysis and reporting Thematic content analysis (Braun & Clarke 2006) using an inductive approach was used to analyze the transcripts. The purpose was to identify, analyze and report patterns within the phenomenon of being labeled with a psychiatric diagnosis. Relevant expressions (sentences/paragraphs) for the aim of the study (sense of otherness) were identified and divided into meaning units. The procedure included the following steps: 1) data familiarization, 2) generation of initial codes, 3) searching for themes, 4) reviewing themes, and 5) defining and naming the themes. The raw data were systematized by the first author into different themes following the verification of the themes by the second author. The authors discussed then the themes until they reached agreement. The themes and examples of data extracts are presented in Table 1 and quotes illustrating the themes in the text. As the students participated in the focus group anonymously, the quotes are presented without detailed labels specifying, for example, the age of the participant at the end of each quotations. Results The data analysis discovered seven themes which were named as 1) Carnival of depression, 2) Stereotypes, 3) Shame, 4) Ethos of self management, 5) Overabundance of help, 6) Minimisation and lack of understanding, and 7) Power of peer support. Carnival of depression Humor was used as a method to deal with the condition of mental illness and to cope with public stigma. The expressions related to this was named as "Carnival of depression". A peer group with individuals in similar condition set frames for this "carnival". Students were joking about depression or depressed people in general, but they were also laughing a lot at themselves, as the following citations from the interview show: Participant 1: I was a little bit afraid to come in, in the middle of the session, I thought fuck, there are at least ten totally strange people and I have to come in. I am brought out there. Hey, here you have a new one. And then they get one more weirdo. [snickering] Participant 2: Yippee! We got one depressed more! [laughing] Participant 1: Straight from Transylvania! [laughing one s head of] ~ 43 ~
176 Volume 20, Number 2 July 2016 December 2016 Participant 3: Let s put all the depressed here together, in the headquarters of depression. Participant 2: Let s dump them all there [laughing] (Focus group 4) Stereotypes The study participants very often saw mental illness and treatment of mental disorders through culturally mediated stereotypes. Messages in the media and in the television influenced their attitudes. Themes in this category reflect how young people with a mental illness find psychiatric rehabilitation and, more generally, people with mental disorders. The study participants did not exactly know what rehabilitation actually means. Images about mental health problems and rehabilitation came from stereotypes presented in films and media. However, they could not relate themselves with these stereotypes, as illustrated in the following quotes and examples of discussion: "As I heard the word psychiatric rehabilitation I thought a while what it means and how it sounds and I thought I will be locked up in a hospital and I will be there in a room with soft walls with five other people wearing a straitjacket. And I told her (school health nurse) that I don t know if I want to participate in this rehabilitation program. Because it felt like I am going to sit in a closed ward and have to explain why I feel myself a little bit depressed." (Female, focus group 6) Participant 1: I think the word psychiatric rehabilitation is totally wrong to use. For people in our age it sounds like you are about to be locked up in a closed ward... Participant 2: For me, all drug addicts and alcoholics came to mind. (Focus group 4) Participant 1: And I thought, hmmmm... rehabilitation...well well..., Participant 2: You will be banded in your bed... Participant 3: Look at these pictures, what do they tell to you...? Participant 1. Do you hear voices? Do you feel something wringing your head? [laughing] (Focus group 4) Shame Students were often concerned with the attitudes of peers or relatives about their condition. Many of them were ashamed and felt embarrassed about having mental health problems and participating in the rehabilitation. Worries about the reaction of peers were common. Telling about their participation in a rehabilitation program was difficult for most of the participants. It seemed that they protected their self-esteem by not disclosing their illness to others. "Well, I still worry that they think I m weird because I have this diagnosis and attend this kind of program..." (Female, focus group 1) "..and my friends could talk something like, what kind of a fucking whacko she is, or something like that." (Female, focus group 8) Some rather kept it as a secret, as illustrated in the quotation below. ~ 44 ~
177 Volume 20, Number 2 July 2016 December 2016 "I definitely won t tell to my friends that I participate in a psychiatric rehabilitation program, that I m in this kind of club for depressed people." (Female, focus group 7) Some of the students were afraid they would disappoint their parents by telling about their condition. An example of discussion below describes the feelings of some study participants. Participant 1: It s a little bit difficult to tell to your parents, suddenly you have to tell them that your child is depressed. Well, what? Participant 2: It feels like you disappoint them Participant 3: Yes, I felt the same (Focus group 4) However, some study participants reported being able to talk openly about their illness with peers and relatives. These students had often relatives who had a history of mental illness, which normalized their condition. Ethos of self management Many study participants had a strong ethos of self management. This is not surprising considering the age of the study participants, being in the middle of the transition phase to adulthood and independence. As most of them lived no longer with their parents, they had the possibility to conceal their condition. Some of them did not want to burden their parents with their problems, as is shown in the following citation: "This is my problem. They don t have to stress about it." (Female, focus group 4) Many did not want to burden their friends and class mates with their mental health challenges, either. Many had this uncomfortable feeling like they would only ruin other's mood by telling about own bad feelings. Consequently, some of them tried to hide their bad feelings behind a "fake happy face". Participant 1: That terrible embarrassment among other people if they heard about such problems. Participant 2: Depression is still a kind of taboo...(focus group 2) Overabundance of help Themes coded as "Overabundance of help " include negative perceptions directed toward peers and friends who were too keen to offer help. Many had faced overabundance of help, which was experienced as annoying by some study participants. The following are illustrations of these themes. "So many think they are like Jesus... I can heal you. Just talk to me". (Female, focus group 4) "One friend of mine talked to me like I was 5 years old. That was so annoying." (Female, focus group 4) Students didn t want to be treated as special cases by friends or teachers because of fear of stigma. "And then somebody in the class, in front of the class, asked me if I m ok and if I manage. And by doing that she made me look even more weirdo ". (Female, focus group 7) Students didn t want other people to pity them. They wanted to be handled like other students, despite their diagnosis. They wanted teachers to take their diagnosis into account, but they didn t want to be treated as a special case. "I have sent my teacher an and told that I want you to take this into account, but I don t want any special treatment or pity. I don t want to turn this into a big issue." (Female, focus group 2) Minimisation and lack of understanding Despite of the overabundance of help experienced by some study participants, many reported experiences of ~ 45 ~
178 Volume 20, Number 2 July 2016 December 2016 other people minimizing their condition, or lack of being understood by others. They reported having been misunderstood by teachers and peers, as well as by professionals. Some felt, that even mental health professionals did not take their condition seriously. The following citations present experiences with the public health care. "I got this feeling that they minimised my condition. Then I started to cry uncontrollably and yelled them that fuck, I feel bad!" (Female, focus group 4) "They told me that my condition is too good. Should I have a rope around my neck before they understand? I m not suicidal and I don t want to be like that. I just want to have somebody to talk with. When I m sitting all day long alone in my apartment staring at walls, well, it can t be that normal. (Female, focus group 4) Due to numerous professionals providing help in the past, some of the study participants were tired to explain their condition and tell their story over and over again. They felt that peers, teachers and even psychiatric and mental health nurses could not really understand them despite their education and many years of working experience. Some of the study participants had a strong feeling of being misunderstood by all without the same condition. "And then as I talked with a nurse, I don t think she really understood, even though she had studied this for ten years and more. But I think she can t REALLY understand me." (female, focus group 6) Power of peer support This theme reflects how the students with mental disorder felt a sense of belonging when interacting with others with similar condition. Group members were bonded through sharing a common problem. It was a relief for many to realize that others experience the same problems and are struggling, too. They felt connected, sharing a common problem and getting peer support. One main benefit of the group-based rehabilitation was the opportunity to laugh and cry together. Nobody needed to hide their bad feelings, but everybody had also the permission to laugh. "It s so cool that even if we talk about rough things and cry together and something like that, but after a coffee break we can have fun and laugh together. I mean, you don t have to be sad all day, even if you...if you have just handled very deep stuff and talked about rough issues." (Female, focus group 2) In groups with a good group cohesion, students had the experience of being understood by others, they were able to talk confidentially and openly. They felt more connected and less alone, reducing feelings of isolation. "And also...you are not alone with this issue. And...well...it has been so good to talk with these people. They understand how you feel." (female, focus group 1) ~ 46 ~
179 Volume 20, Number 2 July 2016 December 2016 Table 1. Themes Themes Coded for Examples of data extract Carnivalisation of depression Joking about depression in general Joking about depressed people "Also my uncle is a nutcase" "...Let s put all the depressed here together, in the headquarters of depression..." Joking about oneself as a depressed person Joking about taking part in a rehabilitation program "...Straight from Transylvania..." "... And then they get one more weirdo..." Stereotypes Stereotypic images of depression and depressed people Stereotypic images of psychiatric rehabilitation "...They (people with mental health problems) walk in the street and mutter..." "For people in our age it sounds like you are about to be locked up in a closed ward...". Shame Shame in telling about one's depression Fear to disappoint the parents Worries about the reaction and attitudes of peers "I definitely won t tell to my friends that I participate in a psychiatric rehabilitation program, that I m in this kind of club for depressed people." "It feels like you disappoint them (parents)" "...I have the feeling that my brother may think, that what...is my sister ok? Is she allowed to be among the people? Should she be locked up somewhere?" Ethos of self management Unwillingness to burden other (parents, friends) Willingness to manage alone "They (friends) get embarrassed when I talk about my problems or about issues we are talking here. Then I got this feeling, I don't want to bother them..."otherwise the feeling of others will be ruined." " This is my problem. They don t have to stress about it." ~ 47 ~
180 Volume 20, Number 2 July 2016 December 2016 Overabundance of help "One friend of mine talked to me like I was 5 years old. That was so annoying." "All this fuss over me, I sit there alone with all these people, parents, school nurses and nearly the school Annoying friends offering help cooks, too. Then you get the feeling, that well...here you are..." Too many parties offering help Turning one's condition to an too big issue "And then somebody in the class, in front of the class, asked me if I m ok and if I manage. And by doing that she made me look even more weirdo ". Minimisation and lack of understanding Lack of understanding Minimisation of symptoms by others Exhaustion to explain one's condition "But I think she can t REALLY understand me." "...they minimised my condition." "I am so tired to explain everybody about all this.."..." It's so tiring." Power of peer support Feeling of being understood Sharing a common problem Sharing different feelings "They understand how you feel..." "...you are not alone with this issue." "It s so cool that even if we talk about rough things and cry together and something like that, but after a coffee break we can have fun and laugh together Discussion The study aimed to synthesize qualitative evidence related to experiences of otherness among students diagnosed with depression and/or anxiety disorder who participated in a psychosocial rehabilitation program. The themes described here highlight and explain how study participants experienced their illness, the reactions of other people to their condition and taking part in a rehabilitation program with peers in similar condition. The present study showed that the sense of otherness due to a psychiatric diagnosis is related to stigma experiences, which may carry both negative and positive meanings (Link & Phelan 2010). The study participants had faced sense of shame, minimisation of their condition, lack of being understood by others and inappropriate way of providing support. On the other hand, in groups with peers with the same condition, they had experienced the possibility to share common thoughts and problems, to laugh and to make fun of themselves and to ~ 48 ~
181 Volume 20, Number 2 July 2016 December 2016 get peer support. The findings of the present study were in line with those of the study by Kranke and Floersch (2009), who interviewed adolescents with a mental health diagnosis and described their experiences of stigma in schools, finding both negative and positive meanings of stigma experiences. In the present study, the presence of self stigma and label avoidance was particularly remarkable. Fear of social stigma strongly affected the student's willingness to participate in the rehabilitation program. Many felt embarrassed about having a mental health problem and they were worried about other people's reactions. During adolescence and young adulthood, concerns about opinions of others are common also among those without mental health challenges. It is understandable that young people with mental health problems experience these concerns even stronger. Young people with mental health problems commonly feel stigmatized and labeled experiencing multiple losses of identity, family, career choices, and educational and social standing at worst (Leavey 2005; Moses 2009). It is also known that they commonly are stigmatized by peers without mental health problems (O'Driscoll 2012). Despite of the dominant presence of stigma experiences among study participants, not every student in this study experienced fear of stigma. Some study participants did not have difficulties to talk openly about their illness with peers and relatives. Previous studies have shown that stigma experiences among young people with mental disorders are not necessarily that common. In the study of Moses (2009), relatively low levels of stigma among adolescent recipients of mental health treatment was shown. The authors stated this to be related to the commonality of mental health symptoms during this age period or increased knowledge about mental health problems and the treatability of these problems. In the present study, those with previous experiences with mental health problems in the family seemed to face fewer difficulties with telling other people about their condition. The diagnosis of depression / anxiety disorder formed a bond between the study participants, providing connection with others in similar condition, sense of belonging and being understood as well as peer support. Shared experiences of otherness deepened the social cohesion. The strategy of forming friendships with others in similar condition is called positive stigma avoidance strategy (Kranke & Floersch 2009). This is a strategy of managing stigma by producing a sense of belonging as well as normalizing behavior, feeling and experience. Group-based interventions - like the OPI program - have the opportunity to foster the group identity and to normalize the illness, reducing stress and self-stigma and supporting the recovery (Corrigan & Wassel 2005; Newbold et al. 2013). Further, group-based interventions have the possibility to provide opportunities to create and maintain friendships with individuals in similar condition. This is important as in this age period young people commonly choose friends based on similarity (Abound & Mendelson 1996). The study participants used humor as a method in dealing with their mental illness. They were making fun of themselves and the peer group set frames for that. The "carnivalisation of depression" was perceived in using stereotypes, playing the fool and in lots of laugh with peers in similar condition. Previous studies have shown that the use of humor is a common method in coping with stress and it can be seen as a coping strategy, as a method to escape and/or avoid the reality (Crawford & Caltabiano 2011; Wu & Chan 2013). The term "Carnivalisation" is not found in the literature related to mental health issues, but it describes the phenomenon observed in this study better than the common term "humour" as it includes a stronger social aspect provided by the peer group. It also includes elements like atmosphere through humour and chaos, parody and personal satire, as described by Bakhtin (1968). The study also showed up that the students did not have adequate information about mental disorders or psychiatric rehabilitation. Young people do not necessarily understand the meaning of the terms used by health care professionals or these terms may be experienced as stigmatizing. The perceptions were formed by stereotypic pictures from the media and television. It is known that media messages very often influence perceptions and form stigmatizing attitudes toward people with mental problems (Cutcliffe & Hannigan 2001; Kranke et al. ~ 49 ~
182 Volume 20, Number 2 July 2016 December ). Strengths and limitations There are strengths but also several limitations of the study that have to be taken into account. The method used in this study fits for the purpose of the study. Qualitative research has the possibility to lend relevant insight into experiences of otherness as a young person with mental disorder. Group settings can trigger people to talk about things that they may not necessary talk about in individual interviews, enriching the data with group experiences and interpretations. Focus groups are seen as an ideal method for exploring people's own meanings and understandings of health and illness (Wilkinson 1998). However, as the sample was small, the results can not be generalized. One challenge in facilitating focus groups is to get every participant to open up and engage in the discussion. Some were more dominant while other needed encouragement to speak. On the whole, the atmosphere during every focus group was open and friendly. Some groups were more talkative than the others. This impression was confirmed also by the counselors providing the program. One weakness of the study is the small number of males among the study participants. Participants of the OPI program were mainly females and the voice of male students is underrepresented in the study. It is also to note, that not every participating in the feasibility study participated in the focus group interview. It is difficult to estimate, how this might have biased the results as the reasons for nonparticipating were various. Further, it has to be taken into consideration that the study participants were taking part in a group rehabilitation program. This has most likely had an influence on the themes that came up in the analysis, especially highlighting the meaning of peer support. The experiences of otherness among those without the possibility to participate in this kind of group-based rehabilitation program or those not having any kind of treatment would differ from these findings. This could be an interesting aim for future studies. Implications for practice The present study highlighted many interesting and important aspects for health care practitioners. First, as young people are known to be reluctant to seek help for their mental health problems, it is important to avoid minimisation of symptoms when dealing with a young person with a mental health concern. On the other hand, young people do not want to be handled like a person with a disability. Health care professionals can contribute to the positive experiences among young patients with mental illness with a person-centered approach, where the patients and their concerns are taken seriously. Young people with mental health problems want to be heard and respected like any other people. Second, young people do not necessarily understand the terms used by the health care system. Service providers and mental health professionals have to pay more attention on how to reach those young people in need for help and how to lower the threshold for seeking help. Young people with mental disorders should be provided with adequate information about services that are supplied. Besides oral and written information, also an opportunity to visit the venue and professionals providing the service is recommended. Within the OPI program, this opportunity lowered the threshold to take part in the program. Third, service providers should also be aware of the power of peer support in planning and developing mental health services for young people with mental illness. Connection with peers with similar condition has the opportunity to normalize the experience of the illness. This can have a positive impact on recovery. Further, young people with mental disorders should be used as experts by experience and be engaged in planning and developing mental health programs for their own age group. ~ 50 ~
183 Volume 20, Number 2 July 2016 December 2016 Conclusions The findings of the present study showed that the experiences of otherness among young people with depression and/or anxiety disorder are related to stigma experiences, which may carry both negative and positive meanings. Negative meanings were related, most of all, to shame and worries about the reaction of peers and relatives as well as to the lack of being understood by others. The positive feelings came out in interacting with peers in similar condition providing support, understanding and sense of belonging. Humor was used as a coping method of dealing with mental illness. The present study provides a better understanding of the social identity of young people receiving support for mental health challenges, and it helps service providers to pay more attention on how to reach those in need of help, how to lower the threshold for seeking help and how young people with mental disorders should be supported. Acknowledgements. We express our appreciation to Noora Sipilä and Ulla Salmelainen for assisting with the interviews. References Aalto-Setälä, T., Marttunen, M., Tuulio-Henriksson, A., Poikolainen, K. & Lönnqvist, J. (2002). Psychiatric treatment seeking and psychosocial impairment among young adults with depression. Journal of Affective Disorders, 70, Abound, F. & Mendelson, M. (1996). Determinants of friendship selection and quality Developmental perspectives. In: Bukowski, W., Newcomb, A. & Hartup, W. (Eds.) The company they keep: Friendship in childhood and adolescence (pp ). New York: Cambridge University Press. Anthony, W. (1993). Recovery from mental illness: The guiding vision of the mental health service system in the 1990 s. Psychosocial Rehabilitation Journal, 16(4), Appelqvist-Schmidlechner, K., Wessman, J., Salmelainen, U., Henriksson, A. & Luoma, M-L. (2015). Rehabilitation for students diagnosed with depression and/or anxiety disorder - Feasibility and perceived impact of the OPI group rehabilitation program. International Journal of Psychosocial Rehabilitation, 19(1), Bakhtin, M. (1968). Rabelais and His World. Trans. Helene Iswolsky. Cambridge, Mass.: MIT Press. Bauman, Z. (1990). Thinking sociologically. Blackwell: Oxford. Ben-Zeev, D., Young, M. & Corrigan P. (2010). DSM-IV and the stigma of mental illness. Journal of Mental Health, 19 (4), Biddle, L., Gunnel, D., Donovan, J. & Sharp, D. (2006). Young adults' reluctance to seek help and use medications for mental distress. Journal of Epidemiology and Community Health, 60, 426 Bowers, H., Manion, I., Papadopoulos, D. & Gauvreau, E. (2013). Stigma in school-based mental health: perceptions of young people and service providers. Child and Adolescent Mental Health, 18(3), Braun, V. & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3, Cheng-Fang, Y., Cheng-Chun, C., Lee, Y., Tang, T., Yen, J. & Ko C. (2005). Self-Stigma and its correlates ~ 51 ~
184 Volume 20, Number 2 July 2016 December 2016 among outpatients with depressive disorders. Psychiatric Services, 56 (5), Corrigan, P. (2004). How Stigma Interferes With Mental Health Care. American Psychologist, 59 (7), Corrigan, P., Larson, J. & Ruesch, N. (2009). Self-stigma and the "why try" effect: impact o life goals and evidence-based practices. World Psychiatry, 8, Corrigan, P. & Wassel, A. (2008). Understanding and influencing the stigma of mental illness. Journal of Psychosocial Nursing and Mental Health Services, 46 (1), Corrigan, P. & Watson, A. (2002). Understanding the impact of stigma on people with mental illness. World Psychiatry, 1, Crawford, S. & Caltabiano, N. (2011). Promoting emotional well-being through the use of humour. Journal of Positive Psychology 6(3), Crocker, J., Major, B. & Steele, C. (1998). Social stigma. In: Handbook of Social Psychology, Vol. 2 (4th edn) (eds D. Gilbert, S. Fiske & G. Lindzey), pp Boston: McGraw-Hill. Cutcliffe, J. & Hannigan, B. (2001). Mass media, "monsters" and mental health clients: the need for increased lobbying. Journal of psychiatric and Mental Health Nursing 8, Goffman, E. (1963) Stigma: Notes on the Management of Spoiled Identity. Prentice-Hall. Hankin, B. (2009). Development of sex differences in depressive and co-occurring anxious symptoms during adolescence: Descriptive trajectories and potential explanations in a multi-wave prospective study. Journal of Clinical Child and Adolescence Psychology 38, Hankin, B., Abramson, L., Moffit, T., Silva, P, McGee, R. & Angell, K. (1998). Development of depression from preadolescence to young adulthood: emerging gender differences in a 10- year longitudinal study. Journal of Abnormal Child Psychology 107, Kessler, R., Avenevoli, S., Costello, J., Georgiades, K., Green, J., Gruber, M., He, J., Koretz, D., McLaughlin, K., Petukhova, M., Sampson, N., Zaslavsky, A. & Merikangas, K. (2012). Prevalence, persistence, and sociodemographic correlates of DSM-IV disorders in the National Comorbidity Survey Replication Adolescent Supplement. Archives of General Psychiatry 69 (4), Kessler, R., Birnbaum, H., Shahly, V., Bromet, E., Hwang, I., McLaughlin, K., Sampson, N., Andrade, L., de Girolamo, G., Demyttenaere, K., Haro, J., Karam, A., Kostyuchenko, S., Kovess, V., Lara, C., Levinson, D., Matschinger, H., Nakane, Y., Browne, M., Ormel, J., Posada-Villa, J., Sagar, R. & Stein, D. (2010). Age differences in the prevalence and comorbidity of DSM-IV major depressive episodes: Results from the WHO World Mental health Survey Initiative. Depression and Anxiety. 27 (4), Kessler, R., Foster, C., Saunders, W. & Stang, P. (1995). Social consequences of psychiatric disorders, I: Educational attainment. American Journal of Psychiatry 152, Kranke, D. & Floersch, J. (2009). Mental health stigma among adolescents: Implications for school social workers. School Social Work Journal 34(1), Kranke, D., Guada, J., Kranke, B. & Floersch, J. (2014). What do African American youth with a mental ill- ~ 52 ~
185 Volume 20, Number 2 July 2016 December 2016 ness think about help-seeking and psychiatric medication? Origins of stigmatizing attitudes. Social Work in Mental Health 10, Krueger, R. & Casey, M. (2000). Focus Groups: A Practical Guide for Applied Research, 3rd ed. Sage Publications, Thousand Oaks, CA. Leavey, J. (2005). Youth experiences of living with mental health problems: emergence, loss, adaptation and recovery (ELAR). Canadian Journal of Community Mental health 24 (2), Lewinsohn, P., Clarke, G., Seeley J. & Rohde, P. (1994). Major depression in community adolescents: age at onset, episode duration, and time to recurrence. American Academy of Child and adolescents Psychiatry 33, Link, B., Cullen, F., Struening, E., Shrout, P. & Dohrenwend, B. (1989). A modified labeling theory approach to mental disorders: An empirical assessment. American Sociological Review 54, Link, B. & Phelan, J. (2001). Conceptualizing stigma. Annual Review of Sociology 27, Link, B. & Phelan, J. (2010). Labeling and stigma. In: Scheid, T. & Brown, T. (Eds) A handbook for the study of mental health: Social contexts, theories and systems (pp ). New York: Cambridge University Press. Link, B., Struening, E. & Neese-Todd, S., Asmussen, S. & Phelan, J. (2001). Stigma as a Barrier to Recovery: The Consequences of Stigma for the Self-Esteem of People with Mental Illnesses. Psychiatric Services 52 (12), Merikangas, K., Nakamura, E. & Kessler, R. (2009). Epidemiology of mental disorders in children and adolescents. Dialogues in Clinical Neuroscience 11(1), Newbold, A., Hardy, G. & Byng, R. (2013). Staff and patient experience of improving access to psychological therapy group interventions for anxiety and depression. Journal of Mental Health 22 (5), Moses, T. (2009). Stigma and self-concept among adolescents receiving mental health treatment. American Journal of Orthopsychiatry 79(2), O'Driscoll, C., Heary, C., Hennessy, E. & McKeague, L. (2012). Explicit and implicit stigma towards peers with mental health problems in childhood and adolescence. Journal of Child Psychology and Psychiatry 53(10), Raitasalo, R. (2007). Mielialakysely. Suomen oloihin Beckin lyhyen depressiokyselyn pohjalta kehitetty masennusoireilun ja itsetunnon kysely. Kela, Sosiaali- ja terveysturvan tutkimuksia 86. Helsinki. Rose, D., Thornicroft, G., Pinfold, V. & Kassam, A. (2007). 250 labels used to stigmatize people with mental illness. BMC Health Services Research 7, 97. Schomerus, G. & Angermeyer, M. (2008). Stigma and its impact on help-seeking for mental disorders: what do we know? Epidemiologia e psichiatria sociale 17(1), Schomerus, G., Matschinger, H. & Angermeyer, M. (2009). The stigma of psychiatric treatment and help-seeking intentions for depression. European Archives of Psychiatry and Clinical Neurosciences 259, ~ 53 ~
186 Volume 20, Number 2 July 2016 December 2016 Sourander, A., Multimäki, P., Santalahti, P., Parkkola, K., Haavisto, A., Helenius, H., Nikolakaros, G., Piha, J., Tamminen, T., Moilanen, I., Kumpulainen, K., Aronen, E., Linna, S-L., Puura, K. & Almqvist, F.. (2004). Mental health service use among 18-year-old adolescent boys: A prospective 10-year follow-up study. Journal of the American Academy of Child and Adolescent Psychiatry 43 (10), Wilkinson, S. (1998). Focus groups in health research. Journal of Health Psychology 3(3), Wu, J. & Chan, R. (2013). Chinese teachers use of humour in coping with stress. International Journal of Psychology 48(6), ~ 54 ~
187 Volume 20, Number 2 July 2016 December 2016 Inpatient Psychiatric Rehabilitation: An Alternative to Bringing Back the Asylum Dawn L. Reinhardt- Wood Kenneth T. Kinter Rutgers University Department of Psychiatric Rehabilitation and Counseling Professions, Rutgers University, Scotch Plains, NJ. Citation: Reinhart-Wood L & Kinter KT.(2016) Inpatient Psychiatric Rehabilitation: An Alternative to Bringing Back the Asylum Dawn. International Journal of Psychosocial Rehabilitation. Vol 20 (2) Acknowledgment We acknowledge the inspirational individuals who demonstrate that recovery is possible despite the challenge of mental illness. We thank Thomas Bartholomew, Joseph Birkmann, and Dr. Kenneth Gill, Department of Psychiatric Rehabilitation and Counseling Professions, Rutgers University, Scotch Plains, NJ for their feedback on early drafts. Corresponding Author Dawn L. Reinhardt-Wood, MA, CPRP, Department of Psychiatric Rehabilitation and Counseling Professions, Rutgers University, 1776 Raritan Road, Scotch Plains, NJ (dawn.reinhardtwood@rutgers.edu). Abstract Recent recommendations by medical ethicists advocate for the return of asylums to improve long-term psychiatric care for individuals who have treatment refractory psychiatric conditions. Long-term inpatient psychiatric hospital environments are not conducive to learning tenancy and recovery skills necessary for optimal community integration. Psychiatric rehabilitation and alternative community interventions provide greater opportunities for learning practical and recovery-oriented skills. Increasing evidence-based psychiatric rehabilitation interventions in the inpatient setting while adequately funding community-based service options is a better alternative. Returning to the asylum-model of long-term psychiatric treatment will harm advances made in the field of psychiatric rehabilitation and the reduction of stigma. Keywords: Psychiatric rehabilitation, recovery, hospitals, severe and persistent mental illness, medical ethics Introduction: ~ 55 ~
188 Volume 20, Number 2 July 2016 December 2016 Sisti, Segal, and Emanuel (2015) asserted that long-term institutionalization is the optimal course of treatment for individuals diagnosed with treatment refractory severe and persistent mental illness. Their opinion was offered despite long-standing contradictory evidence. In a 32-year longitudinal study of long-stay patients, researchers found that 50-75% of participants achieved considerable improvement or recovery following discharge (Harding, Brooks, Ashikaga, Strauss, & Breier, 1987). Rather than press for the return to newer versions of the asylums of old, a more ethical approach would be to advocate for the increase in funding and support for evidence-based practices (EBPs), including psychiatric rehabilitation, in the least restrictive community setting. In some cases, inpatient hospitalization may serve as the least restrictive community setting for periods of time for individuals with significant psychosocial impairment. Therefore, such settings must increase their provision of interventions aimed at restoring or improving upon previous skills individuals require to live fully integrated lives in the community. We agree with Sisti, et al, (2015) on one point: inpatient institutional settings should be safe and modern. They should also utilize scientifically proven interventions to improve individualized outcomes. State psychiatric hospitals are a vital component in the continuum of psychiatric services. These hospitals serve individuals during periods when they cannot otherwise remain in the community due to dangerousness to self or others. However, psychiatric inpatient facilities often do not provide an environment in which individuals living with psychiatric disorders can best learn and practice the skills necessary to improving community integration. State psychiatric hospital services should be further integrated within a continuum of community services in order that persons can be served in the community wherever possible and appropriate (National Association of Mental Health Program Directors, 2014). Integration begins by psychiatric rehabilitation practitioners being increasingly included into the hospitals staffing, bringing with them the ability to inspire the change from a culture of stabilization and maintenance to one of action and improvement. For far too long, psychiatric rehabilitation has been emphasized in the community-based setting alone. Increasing psychiatric rehabilitative interventions in the inpatient setting may contribute to the paradigm shift our aging institutions urgently require. Large psychiatric hospitals frequently lack high-fidelity evidence based treatment interventions and practices. These settings are large and change happens slowly. It is imperative for any initiative to be championed by and monitored by leadership. For EBPs to be effective, they must be delivered with fidelity to intended clinical standards. Without adequate clinical supervision within institutions, it is difficult to achieve delivery of high-fidelity EBPs. Until clinical service settings can administer EBPs as they are developed and studied, the problem of the imperfect and inadequate application of research to clinical practice will persist (Dixon, L.B., Dickerson, F., Bellack, A.S., Bennett, M., Dickerson, D., Goldberg, R.W., Lehman, A., Tenhula, W.N., Calmes, C., Pasillas, R.M., Peer, J., & Kreyenbuhl, J., 2009). Hospital executive administrators and senior state governmental leaders must be supportive of the human and financial resources required to effectively implement EBPs. It is our role as psychiatric rehabilitation practitioners to advocate to these stakeholders. There are benefits for the service participants and long-term cost-savings to communities when individuals recover and require shorter and less frequent hospitalizations. An institution is not a home. In accordance with the Olmstead v. L.C. United States Supreme Court decision, States are required to place persons with mental disabilities in community settings rather than in institutions when they have determined that community placement is appropriate, the transfer from institutional care to a less restrictive setting is not opposed by the affected individual, and the placement can be reasonably accommodated, taking into account the resources available to the State and the needs of others with mental disabilities (Olmstead v. LC, 1999). Advocating for the long-term institutionalization, without also emphasizing the need for efficacious interventions, violates the spirit and intent of the Olmstead legislation. Withholding an individual s right to take risks that may allow them to grow and flourish inside and outside of the inpatient environment seems inconsistent with the traditional medical model value to do no harm. Psychiatric recovery is ~ 56 ~
189 Volume 20, Number 2 July 2016 December 2016 not a linear process and individuals may experience periods of sustained wellness interrupted by instances of symptom relapse. The learning that occurs along the way, during either period, is essential to one s personal recovery process. This learning can occur in the inpatient setting if rehabilitative programs are implemented effectively and receive ongoing administrative and organizational support. Psychosocial factors other than symptoms severity contribute to an individual s successful community tenure. Factors regarded as important for recovery include empowerment, hope, optimism, knowledge about illness and services, life satisfaction, increased self-esteem, self-respect, improved self-control over symptoms and stress, social connectedness, social relationships, and social support (van Gestel-Timmermans, Brouwers, Bongers, van Assen, & van Nieuwenhuizen, 2011). Recovery is possible despite the presence of manageable psychiatric symptoms. The findings by van Gestel- Timmermans, et al. (2011), indicate the need for increasing opportunities for individuals to strengthen their occupational and tenancy skills while hospitalized. Individuals may require acute intensive services when they experience a recurrence of distressing symptoms, however, by aiding individuals in building support networks and developing skills necessary to life after the hospital, individuals can learn techniques to manage symptoms distress and strengthen their roles as citizens in the community of their choice. Traditional long-term institutionalization should not be the only option. Psychiatric hospitalization, when offering psychiatric rehabilitative services, should be among the evidence-based offerings in a well-integrated continuum of behavioral healthcare services available to service participants. Pratt, Gill, Barrett, and Roberts (2014) present several brief alternatives to long-term institutionalization for individuals experiencing significant psychiatric symptoms. These approaches include crisis residences, peer-delivered crisis services, partial and day programs, in-home crisis services, and early intervention teams (Pratt, et al.). At an intermediate level of care, short-term care units can further stabilize individuals who are unable to be stabilized in a less structured community or voluntary inpatient setting. This reduces the need for admission to state psychiatric hospitals and provides local communities with more intensive treatment alternatives. Short-term care units are often accessed via a psychiatric screening commitment when an individual has been deemed a danger to self or others. This option keeps the individual in their community and does not disrupt connection to local mental health providers, social services, and natural supports. We do not consider hospital confinement, as it exists today, the optimal course of treatment for practically any other group of medical conditions other than severe and persistent mental illnesses. Individuals make decisions on a daily basis that may hasten negative consequences of chronic illnesses such as diabetes, hypertension, and hyperlipidemia. Are these individuals not contributing to a possible early demise by being non-compliant with treatment recommendations? They may even be contributing to increased healthcare costs for the nation due to the secondary conditions brought on by poor management of their primary health conditions. Couldn t the poorly managed diet of the individual with diabetes cause a fluctuation in blood sugar, loss of consciousness, and a traffic accident (when that individual is behind the wheel) jeopardizing the safety and welfare of the public? If that sounds ridiculous, it is meant to be. Let s remember that we are not talking about persistently dangerous people. We are talking about a minority of the individuals diagnosed with severe and persistent mental illness who, episodically, exhibit behavior that is deemed unsafe. If we say that we desire mental health care parity with traditional primary health care, we must enforce parity on both sides. Equality for individuals living with mental illness will only come when the providers and leaders in this field walk their own talk. This change will not occur without psychiatric rehabilitation practitioners advocating for a change to inpatient settings. In 1963, President Kennedy promised people with severe and persistent mental illness that they would be treated in the community and funds once used for psychiatric incarceration would follow them into the com- ~ 57 ~
190 Volume 20, Number 2 July 2016 December 2016 munity. We find it unethical and counter- therapeutic to break that promise and revert to a system that didn t work the first time. References Dixon, L.B., Dickerson, F., Bellack, A.S., Bennett, M., Dickerson, D., Goldberg, R.W., Lehman, A., Tenhula, W.N., Calmes, C., Pasillas, R.M., Peer, J., & Kreyenbuhl, J. (2009). The 2009 Schizophrenia PORT psychosocial treatment recommendations and summary statement. Schizophrenia Bulletin, 36(1), Harding, C.M., Brooks, G.W., Ashikaga, T., Strauss, J.S., & Breier, A. (1987). The Vermont longitudinal study of persons with severe mental illness, I: Methodology, study sample, and overall status 32 years later. American Journal of Psychiatry, 144(6), Irmiter, C., McCarthy, J.F., Barry, K.L., Soliman, S., & Blow, F.C. (2007). Reinstitutionalization following psychiatric discharge among VA patients with serious mental illness: A national longitudinal study. Psychiatric Quarterly, 78(4), DOI: /s y. National Association of Mental Health Program Directors. (2014). The vital role of state psychiatric hospitals. Alexandria, VA: National Association of Mental Health Program Directors. Olmstead v. L.C. 527 U.S (1999). (Supreme Court) Pratt, C.W., Gill, K.J., Barrett, N.M., & Roberts, M.M. (2014). Psychiatric Rehabilitation (3rd Edition). New York: Academic Press. Schmutte, T., Dunn, C.L, & Sledge, W.H. (2010). Predicting time to readmission in patients with recent histories of recurrent psychiatric hospitalization: A matched- control survival analysis. Journal of Nervous and Mental Disease, 198(12), ,.DOI: /NMD.0b013e3181fe726b. Sisti, D.A., Segal, A.G, & Emanuel, E.J. (2015). Improving long-term psychiatric care: Bring back the asylum. Journal of the American Medical Association, 313(3), DOI: /jama van Gestel-Timmermans, J.A., Brouwers, E.P., Bongers, I.L., van Assen, M.A., & van Nieuwenhuizen, C. (2011). Profiles of individually defined recovery of people with major psychiatric problems. International Journal of Social Psychiatry, 58(5), DOI: / ~ 58 ~
191 Volume 20, Number 2 July 2016 December 2016 TEACH: A Framework for Recovery-Oriented Education and Training Abraham Rudnick Professor, Department of Psychiatry and Behavioural Neurosciences McMaster University, Hamilton, Ontario, Canada harudnick@hotmail.com Citation: Rudnick A.(2016) TEACH: A Framework for Recovery-Oriented Education and Training. International Journal of Psychosocial Rehabilitation. Vol 20 (2) Abstract Recovery-oriented services for people with mental illness are best practices, yet related education and training is not well developed. This article highlights an approach TEACH (Theory, Evidence, Action in Care for Health) to facilitate recovery-oriented education and training. Research about TEACH and other recovery-oriented education and training approaches is needed. Introduction: Providing recovery-oriented services assumes that providers are educated and trained appropriately. Such education and training in relation to recovery and related services requires teachers to be recovery-oriented in the education and training they provide to learners. There is no generally accepted framework to guide such education and training. In this paper, I report an education and training framework TEACH (Theory, Evidence, Action in Care for Health) that I have developed, and its application to recovery-oriented education and training. Sound education and training uses theory, empirical evidence and practice (action) iteratively and contextually. Thus, all three TEACH components should be used by recovery-oriented teachers. In relation to theory, recovery-oriented teachers can use theories of psychiatric rehabilitation (among other theories), such as Anthony et al s formulation of environments of choice (Anthony, Cohen, Farkas, & Gagne, 2002). In relation to evidence, recovery-oriented teachers can use evidence such as facts about recovery-oriented systems and services (Nelson, Kloos, & Ornelas, 2014). In relation to action, recovery-oriented teachers can use practice such as exercises for person-centered care planning (Tondora, Miller, Slade, & Davidson, 2014). This is about the content the what of education. What about the process the how of education? As noted above, sound education and training is iterative. In relation to TEACH, this means that theory, evidence and action inform each other and are taught in stages and in cycles (or perhaps using a better visual analogy, in spirals), so that after basic theory, evidence and action are addressed, often focusing on awareness and ~ 59 ~
192 Volume 20, Number 2 July 2016 December 2016 knowledge (Knowles, Holton and Swanson 2011), more advanced level theory, evidence and action are addressed, often focusing on skills and attitudes (Ibid). The order of theory, evidence and action may change, although starting with theory, proceeding to evidence, and continuing with action may make most sense in many situations. For example, learning about theoretical aspects of recovery (Rudnick, 2012) and about evidence related to person-centered care for people with serious mental illness (Rudnick & Roe, 2011) is conducive to and hence may best precede learning person-centered care planning (Tondora, Miller, Slade, & Davidson, 2014). That being said, learning style intellectual, experiential or other may determine this order. And teaching style which is often ignored may also contribute to this determination; for an overview of some teaching styles and a measure to assess them, see the teaching perspectives inventory ( which addresses five teaching styles that each teacher exhibits to a smaller or larger extent 1. transmission, which is knowledge focused; 2. apprenticeship, which is skills focused; 3. developmental, which is reasoning focused; 4. nurturing, which is support focused; and 5. social reform, which is values focused. Sound education and training is also contextual. In relation to TEACH, that means that relevance or pertinence of theory, evidence and action is imperative. For example, Anthony and colleagues use theory from physical rehabilitation to teach psychiatric rehabilitation (Anthony, Cohen, Farkas, & Gagne, 2002). And although the conventional biomedical model of care is foreign to a recovery-oriented approach, clinical communication practice that was developed for medical education purposes can be useful in recovery-oriented education and training, as in the teaching of structured empathic communication (Buckman, 2010). An illustration of TEACH based on some of my psychiatric rehabilitation education and training innovation (Rudnick & Eastwood, 2013) may be relevant and helpful. For example, when teaching psychiatric rehabilitation to obtain and maintain success and satisfaction in social environments of choice, basic theory can be related to social behavior and to stigma and advanced theory can be related to social cognition and to structural inequalities in society; basic evidence can be related to effects of social skills training and to stigma reduction and advanced evidence can be related to effects of social cognition remediation and to advocacy; and basic practice can be related to social skills training and to stigma reduction while advanced practice can be related to social cognition remediation training and to advocacy training. Applying TEACH facilitates staging and otherwise individualizing such education and training, so that teachers can help learners customize such education and training, using a fairly structured and reasoned approach. Thus, an intellectually oriented learner who has no knowledge of this area of psychiatric rehabilitation would likely need to start with learning about social behavior and stigma, and then proceed to learn about and practice social skills training and stigma reduction. An experientially oriented learner who has already learned social skills training would likely benefit from social cognition remediation training and advocacy training. In summary, TEACH is a framework that is applicable to recovery-oriented education and training. Research about, as well as further development and attempted implementation of, TEACH and other frameworks for recovery-oriented education and training are needed. References Anthony, W.A., Cohen, M., Farkas, M., & Gagne, C. (2002). Psychiatric Rehabilitation, 2nd edition. Boston: Boston University, Center for Psychiatric Rehabilitation. Buckman, R. (2010). Practical Plans for Difficult Conversations in Medicine: Strategies that Work in Breaking Bad News. Baltimore: Johns Hopkins University Press. Knowles, M.S., Holton, E.F., & Swanson, R.A. (2011). The Adult Learner: The Definitive Classic in Adult Education and Human Resource Development, 7th edition. Amsterdam: Elsevier. Nelson, G., Kloos, G., & Ornelas, J. (eds.) (2014). Community Psychology and Community Mental Health: Towards ~ 60 ~
193 Volume 20, Number 2 July 2016 December 2016 Transformative Change. Oxford: Oxford University Press. Rudnick, A. (ed.) (2012). Recovery of People with Mental Illness: Philosophical and Related Perspectives. Oxford: Oxford University Press. Rudnick, A., & Roe, D. (eds.) (2011). Serious Mental Illness: Person-Centered Approaches. London: Radcliffe. Rudnick, A., & Eastwood, D. (2013). Psychiatric rehabilitation education for physicians. Psychiatric Rehabilitation Journal, 36(2), Tondora, J., Miller, R., Slade, M., & Davidson, L. (2014). Partnering for Recovery in Mental Health: A Practical Guide to Person-Centered Planning. Chichester, West Sussex: Wiley. ~ 61 ~
194 Volume 20, Number 2 July 2016 December 2016 Internet-delivered interventions in mental health rehabilitation: A recovery-oriented online service platform Eitan Ben Itzhak Klutch, MA Makshivim-Net, eitan@makshivim.com Liat Libling, MPH Makshivim-Net, liat@makshivim.net Nirit Benyamini, MSW Makshivim-Net, nirit@makshivim.net Max Lachman, Ph.D Senior Lecture, Community Mental Health Department, Haifa University, lachman55@gmail.com Ayala Friedlander Katz, BSW, MA Israel Psychiatric Rehabilitation Association (ISPRA) ayajavi@hotmail.com Citation: Klutch EBI, Libling L, Benyamini N, Lachman M & Katz AF.(2016) Internet-delivered interventions in mental health rehabilitation: A recovery-oriented online service platform. International Journal of Psychosocial Rehabilitation. Vol 20 (2) Authors' note The programs presented in this article are supported in part by the Israeli Ministry of Health, Department of mental health services; the JDC Israel non-profit organization; and the Israel Institution for Social security. The first three authors are staff members in the programs presented in this article. All authors guarantee their sufficient participation in this manuscript. Corresponding author: Liat libling, Hashoftim 27/4, Tel Aviv, Israel. liat@makshivim.net Abstract Objective: The purpose of this article is to present an online service platform applied in Israel, which comprises various technological tools aimed at assisting recovery-oriented psychiatric rehabilitation processes. Method: We describe the technological tools and preliminary results of the e-social and e-occupational programs, developed as part of national initiatives in Israel. Descriptive data, satisfaction evaluation results, survey results of reasons for participation and perceived contributions are presented. Findings: Within e-social programs, peer-led social groups showed high satisfaction rates among clients. Reported contributions in- ~ 62 ~
195 Volume 20, Number 2 July 2016 December 2016 cluded finding friends, emotional, vocational, and self-confidence improvements, acquiring knowledge and helping others. "Safety net" social project has been reported to be beneficial in increasing the sense of security during national emergencies. An e-vocational service for professionals with psychiatric disabilities showed high rates of placement. Conclusions and Implications: Makshivim-Net offers an online assistance for recovery-goals promotion, with preliminary positive results. Rigorous research with standardized measures is needed. Key-words: Mental health; Rehabilitation; Internet intervention; Online-recovery-assistance; Peer-support. Introduction: The use of the internet as a rehabilitation tool carries unique potential advantages unavailable in traditional rehabilitation services. A majority of mental health (MH) consumers use internet and Smartphone communication for diverse purposes, such as , text message communication, employment, medical information search, and social networks participation (Carras, Mojtabai, Furr-Holden, Eaton, & Cullen, 2014). In this paper we aim to address existing knowledge of internet technology as a form of intervention with MH consumers and then focus on our experience in developing and implementing internet-based technologies to advance consumers' rehabilitation and recovery processes. Advantages of internet-delivered interventions in mental health A large body of research supports the use of internet as a form of delivering therapy for common mental disorders (Andersson & Titov, 2014; Cunningham, Gulliver, Farrer, Bennett, & Carron-Arthur, 2014), addressing its advantages compared to face-to-face delivery forms. Internet interventions increase accessibility to professional assistance for people who seek to remain anonymous (Christensen & Griffiths, 2002), enable to deliver help for people who did not approach services previously (Ybarra & Eaton, 2005), and to provide availability of services for people living in remote areas (Farrell, & McKinnon, 2003). Other advantages include high frequency of contact and quick response, allowing effective collaborative interactions (Andersson & Titov, 2014), with low economical costs for clients (Ybarra & Eaton, 2005) and relatively high cost-effectiveness compared to other forms of service delivery (Donker et al., 2015). Organizationally, internet interventions allow efficiency at work settings as the focus during work shifts from time of work to outcomes; decreased costs and increased profits; service delivery improvement; and reduction of environmental damage with the decreased need for transportation (Cascio, 2000). In addition to these advantages, the literature shows positive clinical outcomes of internet and Smartphone interventions for psychiatric disorders, and positive potential for relapse prevention (Alleman, 2002; Ybarra & Eaton, 2005). Most research assessed internet- delivered interventions for mood and anxiety disorders. For example, Andersson and colleagues (Andersson et al., 2013) compared internet-cbt with face-to face CBT for depression and found equivalent outcomes with long-term sustained gains. Richards and colleagues (Richards et al., 2015) presented a randomized controlled trial of a weekly internet-delivered CBT treatment for depression, compared to waiting list control group. Their results showed positive outcomes in depressive symptoms and maintained gains at 6- month follow-up. Zabinski and colleagues (Zabinski et al., 2001) evaluated an 8-week internet treatment for eating disorders among 60 women, delivering different intervention tools each week, such as text use, video, group discussion, and self-behavior assessment. A 3- months follow-up showed a significant decrease in participants' will to lose weight, and an enhanced body image. Lange and colleagues (Lange, van de Ven, Schrieken, Bredeweg, & Emmelkamp, 2000) explored internet CBT treatment for 24 participants diagnosed with PTSD. Their results demonstrated significant decreases in anxiety, depression, somatization, and sleeping problems following a 5- week intervention, as well as at 6-month follow-up. Most participants reported anonymity of internet-based treatment as an advantage, and this group showed the ~ 63 ~
196 Volume 20, Number 2 July 2016 December 2016 most symptom relief. Yet, 40% noted the lack of in-person contact as a disadvantage. Generally, symptom relief was reported as similar to that of patients who received traditional treatment. The accumulated findings led researchers to suggest that internet treatment could serve as an alternative for people who are reluctant towards in-person therapy (Lange et al., 2000) or as an initial step that encourages people to later approach face-to-face treatment (Metanoia, 2001). This suggests the need for an integrated approach to practice, considering internet and in-person treatments as complementary services (Andersson & Titov, 2014; Ybarra & Eaton, 2005). Internet-delivered interventions in psychiatric rehabilitation Much less research has been conducted to explore internet use within the field of psychiatric- rehabilitation. Haslett and colleagues (Haslett, McHugo, Bond, & Drake, 2014) studied a tablet-based intervention and showed its' contribution to increased involvement in supported employment compared to a control group. Another occupational project (Nilsson & Lodestad Misa, 2014) assessed the effectiveness of shifting from in-person meetings to internet chat between clients and supported employment experts. Results showed that internet coaching was perceived as a good complementing form of communication, though not as an exclusive one. Both clients and employment experts experienced internet coaching as useful for the purpose of practical and informative communication, and as a good way to save clients' time, energy, and money. Yet, both clients and experts identified difficulty in reading personal moods and responses via internet chat. Ben-Zeev and colleagues (Ben-Zeev et al., 2013) described a development and usability testing process of a Smartphone system for illness self-management for people with schizophrenia. This project involved clients diagnosed with schizophrenia-spectrum or schizoaffective disorders, and practitioners in a community rehab agency: First, surveys collected interests and expectations from 904 clients and 8 practitioners, concerning the use of mobile intervention; then a multidisciplinary team incorporated consumer and practitioner input, and eventually provided design principles for the development of mobile intervention. Next, 12 consumers participated in laboratory usability sessions, performing tasks involved in operating the new system. They provided feedback about their needs and preferences, and usability ratings. As a result, the designed system is focused on five dimensions of self- management: medication adherence; mood regulation; sleep; social functioning; and coping with symptoms. This inspiring process demonstrates a way to involve clients and practitioners in a shared process of learning and creating, leading to a shared intervention- product. Such processes and outcomes seem to put into practice principles of mutual partnership, empowerment, self-determination and hope in recovery-oriented services (Farkas, 2007), and further demonstrate the adoption of a co-productive practice, addressed to in other recovery-oriented interventions (e.g. Tew et al. 2015; Thorneycroft & Dobel-Ober, 2015). This project illuminates the potential of mobile technologies to assist illness self- management, yet need for systemic evaluation in real-world conditions (Ben-Zeev et al., 2013). Challenges in using internet-delivered interventions in mental health Several challenges arise while using internet technologies in MH therapy and rehabilitation. Anonymity, which might be an advantage to some, may cause difficulties for practitioners to identify the person with whom they are interacting, and to control accessibility of people with negative intentions. With the growing ability for online anonymity, new problems emerge, such as cyber-bullying, gossip, or shaming. These phenomena may lead to depression, and even suicide. Furthermore, clients' and providers' concerns about documentation and information confidentiality in technological systems, give rise to the need for clear guidelines for online interventions (Richards et al., 2016; Ybarra & Eaton, 2005). Several researchers addressed difficulties in interpreting vague messages or identifying authentic moods online, with the absence of non-verbal cues, usually integral to therapeutic discourse (Andersson & Titov, 2014; Ybarra & Eaton, 2005). Additionally, high availability of electronic communication opens possible expectations for immediate response, which may not suite practitioner's working hours. This might expose relationships between clients and practitioners to increased occupation with ~ 64 ~
197 Volume 20, Number 2 July 2016 December 2016 boundaries issues, when it becomes hard to ignore clients' repeated requests, questions, or comments. Additionally, technology assimilation may be challenging for professional teams used to traditional work, demanding adjustment of their professional practice. Moreover, online or mobile communication is usually preformed while a worker is alone, which may cause lack of interaction with colleagues, as their working hours may not overlap (Cascio, 2000; Sucala et al., 2012). Makshivim-Net: A technological-professional platform for online rehabilitation services Makshivim-Net (MN) is a platform for rehabilitation services delivered through Internet and mobile communications, combined with some face-to-face work. This platform has been developed and applied since 2005, in a shared collaborative process with clients (Ben-Itzhak- Klutch, 2008). This collaborative process included focus-group discussions aimed at clarifying participants' needs and specified expectations regarding features and information to be placed on site platforms. Participants' involvement also included choosing a name and logo for the project by vote. MN provides a range of online programs, offering support services targeting two main goals- domains: employment, and social networks. Additionally, two other services, which will not be presented in the current paper, include virtual supported education and virtual mentoring/coaching, both function in initial phases to date, and delivered as private services. The platform offers varied online tools to assist recovery-goals achievement for each of these domains. These services have been assimilated within the national mental health rehabilitation system in Israel and function as part of the "Mental health rehabilitation basket" under the ministry of health, in compliance with the "Community rehabilitation for people with mental disabilities" law (Aviram, Ginath, & Roe, 2012). Makshivim-Net system was developed with high standards of security and privacy protection, using different updated technologies. Staff is trained to use these tools, learn about their advantages and limitations. Supervision is provided online, both individually and in a group, and face-to-face staff meetings and workshops provide training and discussion opportunities. Assessment of clients' needs and preferences is preformed face-to-face (in occupational services) or online (in social services), aimed at getting to know each other, discussing and choosing relevant service\s for each individual. Assessment and intervention planning consider the preferred combination of virtual and face-to-face encounters, and preferred individual and\or group supports. We next describe the main service programs and tools offered to clients on this platform. Despite lacking empirical academic research, much can be learnt through examination of existing data and accumulated experience among staff and clients. Each of the services to be presented provides regular reports to the ministry of health, or other formal partners, including number of participants and outcomes. Additionally, the services are regularly inspected as part of the procedural measure of quality performance in rehabilitation services by the ministry of health. Other data includes participants' responses to satisfaction surveys conducted by the ministry of health, and other measures used as part of organizational developmental learning. Assistive Rehabilitation Technologies: ARTech, ARChat, ARContact, and ARPackage AR Technologies include four software functions designed to assist the rehabilitation process, used by client and worker to manage the rehabilitation process and follow-up goals achievement: ARTech: A monitoring system to follow and assist in managing the online recovery process. This tool is equivalent to "client file" where information is collected and a personal rehabilitation plan is created ~ 65 ~
198 Volume 20, Number 2 July 2016 December 2016 and modified. The system allows building a process plan, that contains all the information gathered by client and practitioner, from intake interview, to rehabilitation goals and preferences, and following gradual steps, in accordance with the determined recovery goal. The collected data may be displayed according to authorization determined by client and worker, deciding who can access the system, and which information will be presented (either partial (e.g. occupational), or full ARTech information). The system was developed to provide accessibility for clients with various disabilities within a framework of positive reinforcement, where accomplished tasks are marked graphically. It is designed as a user friendly site, enabling independent operation and self-management of the rehabilitation plan, aimed for increased use of the system over time; ARChat: A Chat program for both individuals and groups on website or Smartphone App. This program provides a space for personal private conversations between client and worker, and serves as a platform for group discussions. It allows participants to receive supportive response from their worker or peers. ARContact: A monitoring external system that serves to receive data from the participant's support community, such as employers, family, or teachers. It allows receiving (but not exporting) input from others involved in the rehabilitation process, in order to integrate important information and feedback into the shared process of client and worker. This input can be used for discussion and consideration in decision making processes. ARPackage: A system that incorporates all of the applications and their data that is collected in realtime. The system can supply observations on individual clients in each of the services which they are using, and thus provide a detailed large picture of the individual rehabilitation progress at all relevant goal-domains. In addition, ARPackage can provide a wider, bird s eye view observation on the system's different programs, while incorporating several client-files and\or services hence allowing to examine overall success in goal achievement. Thus, MN is a large format which contains four system-ingredients which serve as tools to assist personal rehabilitation processes in the e-social and e-occupational domains, which we detail next. e-social rehabilitation services Two services are offered to clients who wish to focus on social goals: Peer-led mixed-online and face-to-face group intervention; and "Safety Net" for improved community resilience. (1) Peer-led social online groups combined with face-to-face monthly meetings: This service, opened in 2005, aimed to meet clients' needs for connectedness to peers and enhancement of social networks. Group participation requires accessibility to the technology in use, so that practitioners need to ensure that a client who joins a group is connected and equipped with the technological tools and the knowledge necessary to use it. Groups vary in their nature - from general social groups to specified-content groups (e.g. healthy life-style). Group coordinators (all consumers-providers) facilitate the group, and also arrange special guest- talks occasionally, who join the chat in order to present specific topics of interest. For example: government officials guest talks, addressing disability rights and benefits; a Clubhouse representative guest, presenting the Clubhouse principles and activities; and many more. The first step in joining a group is by creating a "personal profile" as a way to present oneself to group members. Group chats eventually lead to "real-world" face-to-face group meetings, planned and organized by group participants with coordinator. ~ 66 ~
 initiated by the ministry of health during 2007 (conducted by peerpollsters as part of a national evaluation project) showed high rates of satisfaction with staff, with group contents,")
199 Volume 20, Number 2 July 2016 December 2016 A satisfaction survey (Dereh Halev. 2007) initiated by the ministry of health during 2007 (conducted by peerpollsters as part of a national evaluation project) showed high rates of satisfaction with staff, with group contents, activities and atmosphere, and with activity time schedule. In January 2009 an anonymous "Project efficiency survey" (Makshivim-Net, 2009) was sent by the agency s professional management to all groups' participants (N=129) in order to assess their reasons for joining the group, the expected areas of improvement as a result of participation, and their perceived actual progress in those areas. Thirty-nine participants responded, and expressed their consent to answer the survey questions without providing any personal details. Participants revealed varied reasons for participation in social- groups. Finding friends, improving wellbeing, and hope to find a spouse, were prominent reasons. Table 1 shows reasons for joining groups, expected areas of contribution and perceived actual contribution of group participation. Table 1 shows that most participants (82%, n=32) joined a group for the purpose of friendship, while 68% reported actual progress in achieving this purpose. 76% of those who expected to improve their mental wellbeing reported actual improvement, though only 17% reported actual perceived progress in their hope to find a spouse. Nonetheless, one couple of group members who met in the project is getting married and two other ~ 67 ~
200 Volume 20, Number 2 July 2016 December 2016 couples are now living together. (2) "Safety Net": Improving community resilience: This service was initiated together with the JDC Israel non-profit organization, as a response to the stressful times followed by a military operation in southern Israel during During that time, people were not allowed to gather in large groups or be far away from a bomb shelter. They could not go to work, school or other everyday activities. Obviously, stress levels are raised when missiles and sirens become a daily experience, which in some may trigger more severe symptoms, while having fewer opportunities for social support. Thus, "Safety Net" offered online group meetings, scheduled in advance, and with higher frequency during emergency events. Additionally, a professional worker was available at all times, and participants were given the option to speak to him over the phone or meet face-to-face. This project now continues to function as a general community support for regular times. Participants experiences in this program were assessed using a self-report questionnaire designed for this purpose (Makshivim-Net, 2015). Participants were informed about the purpose of the survey and twenty provided their consent and completed the survey online, anonymously. Two-thirds (66%) of participants reported that group members were helpful to them and contributed to their sense of security. From this group, 88.89% reported that using the chat service with peers was helpful in providing relief during real-time emergency events % reported that the group was "very helpful" during those times. Furthermore, fewer participants reported turning to the professional support compared to using group peer- support during stressful times. Nevertheless, one third (33%) of participants did not consider the group chat as helpful in feeling more secure. The positive feedback from participants in this program led to expanding it to all people with disabilities, with the opening of the "online center for independent living" model, providing virtual tools for independent living and social integration, not exclusively for times of crises, but rather at all times. This new project is consistent with the principal of peer-led intervention, employing group coordinators with different types of disabilities. e-occupational rehabilitation services MN platforms offer two vocational assistive programs: (1) Online supported employment: This program is supported by the Israeli Social Security Institution and open to all people with disabilities who wish to receive supported employment services online, as an alternative to such services provided traditionally. This service adopted supported employment model principles (Bond, Drake, & Becker, 2012), while shifting communication between client and practitioner to MN technology platform, allowing on-going follow up of goals achievement in a collaborative relationship. The service is available to all people with disabilities as a pilot program opened in January A research conducted to evaluate the program's effectiveness will collect data over two years, and initial results are expected by the end of ~ 68 ~

201 Volume 20, Number 2 July 2016 December 2016 (2) Figure 1 - Occupational characteristics summarizing 12 months during 2015 (N=80) (2) Online supported employment for academics and professionals with psychiatric disabilities: This program combines internet communication and face-to-face meetings aimed to assist professionals with psychiatric disabilities to overcome barriers to competitive employment within their professional field. This program provides personal coaching, focusing on structured stages leading to work placement. These stages include preferences definition, job search, and interview preparation, follow up communication and ongoing support. Initial statistics among 80 participants, preformed as part of a service documentation, reported to the ministry of health (Ben-Itzhak Klutch, Benyamini, & Libling, 2015) showed high placement rates 82% during 2015 (13% higher than 2014) of which 58% worked over 6 months. Age characteristics in this sample show higher placement rates for those aged Two thirds (67%) of placements were within client's professional expertise, while one third were working in non-professional jobs. This data is presented in Figure 1: Emerging challenges and difficulties through implementation of MN Through the years of developing and assimilating MN, challenges and difficulties emerged and search for solutions ~ 69 ~
202 Volume 20, Number 2 July 2016 December 2016 influenced the programs' design and development. As in literature, sometimes workers find it difficult to interpret participants' partial or unclear messages (Andersson & Titov, 2014). Boundaries of working hours are also challenged, as technological communication's availability is unlimited (Ybarra & Eaton, 2005). Such issues are discussed during supervision, in search of individualized solutions for different situations. Confidentiality of medical and other private information is another challenge, as technology allows keeping group discussions on personal computers' and mobile phone's memory. While social media such as WhatsApp can serve as a platform for interesting and important discussions, it also exposes personal identifiable details of participants. For this reason, rehabilitation interventions need other platforms, which allow confidentiality. MN solved this issue by developing the chat platform (ARChat) software that prevents exposure of all information systems, open only to clients and practitioners in the program. Providing online support for people with mental illness may bring about professional dilemmas for practitioners. For example, when clients argue about personal issues and reveal personal details in group, or when clients express extreme emotional states, such as anxiety, depression, or suicidal thoughts, to either online group or practitioner. In such situations, practitioners might feel helpless, and program's policy should consider and address ways to handle them. Training and supervision are highly important as a space for discussion about emerging dilemmas, challenging situations with clients, feelings of loneliness in this unique work environment, or difficulties in keeping professional boundaries (Cascio, 2000). In MN, daily communication between staff members allows continuous online contact, which seems to strengthen workers' sense of belonging in spite of little face-to-face contact. Nevertheless, individual and group supervision also take place, online and face-to-face, as well as staff meetings in both forms. Discussion The varied programs described above allow a range of technological tools to support rehabilitation processes, adjusted to individual needs. In order to use these tools effectively it is necessary to understand each technology, the type of intervention that it may provide, and how it may (or may not) fit specific goals in rehabilitation processes. The services presented above differ in their goal focus, format (individual or group), and balance of virtual vs. face- toface communication. These differences should be considered while tailoring a rehabilitation plan. For example, when the client's goal is focused on enlarging their social network, and enhancing the quality of their relationships, group interventions may be better suited - either general peer-facilitated support groups, or topic-specified groups. Group interventions provide additional value where clients may find the group of equals as a source for support and encouragement in goal pursuit. Real-world meetings offered in facilitated groups may further contribute to enhancement of social integration, while relationships among group members are encouraged to continue and develop beyond facilitated sessions. Thus, for some goals, group online interventions may have advantages over individual intervention. For others, personal relationships conducted online can meet the need for an individualized process and the high availability of the practitioner assists their personal recovery. For example, in our experience, occupational processes would usually benefit from a personal individualized process. More generally, considering dynamic changes in client's goals may lead to the recommendation of using individual intervention first, and then shifting to group intervention as client's goals evolve. Thus, our experience indicates that choosing an individualized combination of group and individual supports can bring about better rehabilitation outcomes. Another important consideration is the balance of online and face-to-face encounters, following each individual's rehabilitation plan. The process of planning with each client emphasizes the combination of possibilities in both forms of meeting online and face-to- face. Following an initial face-to-face meeting, client and practitioner discuss the best form of communication along their relationship process. Yet, most of the time the online communication dominates, which makes the helping relationship more intense and frequent compared to traditional therapy. This seems to increase clients' involvement, catalyze task performance, and thus enhance self-agency and advance goals ~ 70 ~
203 Volume 20, Number 2 July 2016 December 2016 achievement. Variations in use of online versus face-to-face communications may also be related to the program s main target social, occupational, educational, etc. Thus, the possibility to combine both forms of communication (online and face-to-face), either individually or in a group, enables individual adjustments of the intervention plan throughout the process, in accordance with personal changed priorities, preferences, or needs (Alleman, 2002; Andersson & Titov, 2014). This is a unique aspect of MN that provides clients with the possibility to receive both individual and group support, both online and face- to-face, allowing a wide range of individualized intervention plans. Recently, Richards and colleagues (Richards et al., 2016) suggested guiding elements for quality online interventions delivered by MH professionals. These include the use of empirically valid contents, ensuring that technologies are strong, secure, engaging and responsive, and that MH professionals' input shape these technologies. Moreover, technological tools' development and design should employ client-centered principles, and focus on desired clinical outcomes. Such technologies should rely on effectiveness evaluation and research, and employ well-established implementation methods (Richards et al., 2016). These guidelines support the efforts made during the gradual development of MN over the last decade, to ensure effective and secure service delivery of mixed-online and direct interventions in psychiatric rehabilitation. Furthermore, employing consumers-providers in MN programs and providing online peer-support interventions is consistent with recovery- oriented practice (Farkas & Anthony, 2010; Kaplan, Salzer, Solomon, Brusilovskiy, & Cousounis, 2011). This approach may as well contribute to a variety of work opportunities for people in recovery from mental illness as peer-specialists. Strengths and limitations This paper presented a well-implemented yet still-developing service platform, which demonstrates an online practice model applied in the field of psychiatric rehabilitation. Initial results from ongoing documentation, formal reports and evaluations suggest positive potential of the assessed services to assist recovery processes among MH consumers. Nonetheless, the existing data is partial and more investigation is required with more rigorous methodologies in order to clarify rehabilitation outcomes and understand more deeply the value of internet services for people in recovery. Future research may contribute to further development, towards realizing the positive potential of such tools through assimilation into MH systems. Acknowledgment: The service programs presented in this article are supported in part by the Israeli ministry of health, department of mental health services; the JDC Israel non-profit organization; and the Israel Institution for Social security. We acknowledge their financial and professional contributions to delivering and evaluating these services. ~ 71 ~
204 Volume 20, Number 2 July 2016 December 2016 References Alleman, J. R. (2002). Online counseling: The internet and mental health treatment. Psychotherapy: Theory,Research, Practice, Training, 39(2), doi: // Andersson, G., Hesser, H., Veilord, A., Svedling, L., Andersson, F., Sleman, Amminen,. (2 1 ). Randomised controlled non-inferiority trial with -year follow-up of internet-delivered versus face-to-face group cognitive behavioural therapy for depression. Journal of affective disorders, 1 1( ), Andersson, G., & Titov, N. (2014). Advantages and limitations of internet-based interventions for common mental disorders. World Psychiatry 13(1), Aviram, U., Ginath, Y., & Roe, D. (2012). Mental health reforms in Europe: Israel's rehabilitation in the community of persons with mental disabilities law: challenges and opportunities. Psychiatric ervices, (2), Ben-Zeev, D., Kaiser, S. M., Brenner, C. J., Begale, M., Duffecy, J., & Mohr, D. C. (2013). Development and usability testing of FOCUS: A smartphone system for self-management of schizophrenia. Psychiatric Rehabilitation Journal. 36(4), doi: /prj Ben-Itzhak Klutch, E. (2008). Makshivim An online project to promote recovery and social inclusion of persons with psychiatric disabilities. International News, 1, Ben-Itzhak Klutch, E., Benyamini, N., & Libling, L. (2015). "Occupational greenhouse" occupational rehabilitation via internet: Annual report to the ministry of health. (Hebrew). Bond, G. R., Drake, R. E., & ecker,. R. (2 12). enerali ability of the Individual Placement and upport (IP ) model of supported employment outside the. orld Psychiatry, 11(1), 2-9. Carras, M. C., Mojtabai, R., Furr-Holden, C. D., Eaton, W. & Cullen, B. A.M. (2014). Use of mobile phones, computers and internet among clients of an inner-city community psychiatric clinic. Journal of Psychiatric Practice, 20(2), Cascio, W. (2000). Managing a virtual workplace. The Academy of Management Executive, 14(3), Christensen, H., & Griffiths, K. M. (2002). The prevention of depression using the Internet. Medical Journal of Australia, 7,S122 S125. Cunningham, J. A., Gulliver, A., Farrer, L., Bennett, K., & Carron-Arthur, B. (2014). Internet interventions for mental health and addictions: urrent findings and future directions. urrent psychiatry reports, 1 (12), 1-. Dereh Halev. (2007), Satisfaction survey findings for participants in social club: Final report. (Hebrew). Donker, T., Blankers, M., Hedman, E., Ljótsson, B., Petrie, K., & Christensen, H. (2015). Economic evaluations of Internet interventions for mental health: A systematic review. Psychological medicine, 45(16), Farkas, M. (2007). The vision of recovery today: What it is and what it means for services. World Psychiatry, 6(2), Farkas, M., & Anthony, W.A. (2010). Psychiatric rehabilitation interventions: A review. International Review of Psychiatry, 22(2), Farrell, S. P., & McKinnon, C. R. (2003). Technology and rural mental health. Archives in Psychiatric Nursing, 17, Haslett, W. R., McHugo, G. J., Bond, G. R., & Drake, R. E. (2014). Use of software for tablet computers to promote engagement with supported employment: Results from an RCT. Psychiatric Services, 65(7), ~ 72 ~
205 Volume 20, Number 2 July 2016 December 2016 Kaplan, K., Salzer, M. S., Solomon, P., Brusilovskiy, E., & Cousounis, P. (2011). Internet peer support for individuals with psychiatric disabilities: A randomized controlled trial. Social Science & Medicine, 72, Lange, A., van de Ven, J. -P., Schrieken, B. A. L., Bredeweg, B., & Emmelkamp, P. M. G. (2000). Internet-mediated, protocol-driven treatment of psychological dysfunction. Journal of Telemedicine and Telecare, 6, Makshivim-Net. (2009). Organizational clients survey report for social groups. (Hebrew). Makshivim-Net. (2015). Safety- Net: Summary of a pilot program. (Hebrew). Metanoia, (2001). E-therapy history and survey. Retrieved from Nilsson, E., & Lodestad Misa, S. (2014). Web coaching: An alternative and complementary form of meeting. Journal of Vocational Rehabilitation 41, doi: /jvr Richards,., Timulak,., Vigano, N., rien, E., oherty,., harry,., & Hayes,. (2015). A randomized controlled trial of an internet-delivered treatment: It's potential as a low-intensity community intervention for adults with symptoms of depression. Behaviour Research and Therapy 75, Richards,., Vigano, N., allaghan,.., rien, E., ooney,., & onner,. (2 1 ). Towards a gold standard for internet-delivered programs in behavioural and mental health. European Psychiatry, 33, S610. Sucala, M., Schnur, J. B., Constantino, M. J., Miller, S. J., Brackman, E. H., & Montgomery, G. H. (2012). The therapeutic relationship in e-therapy for mental health: A systematic review. Journal of Medical Internet Research, 14(4), e110, doi: /jmir Tew, J., Larsen, J., Hamilton, S., Manthorpe, J., Clewett, N., Pinfold, V., & Szymczynska, P. (2 1 ). And the stuff that I m able to achieve now is really ama ing : The potential of personal budgets as a mechanism for supporting recovery in mental health. British Journal of Social Work, 45, Supplement 1, i79 i97. Thorneycroft, J., & Dobel-Ober, D. (2015). Exploratory evaluation of co-produced groups in a community psychiatry organization in England. Journal of Psychosocial Rehabilitation in Mental Health, 2(1), doi /s Ybarra, M. L., & Eaton, W. W. (2005). Internet-based mental health interventions. Mental Health Services Research, 7(2), Zabinski, M. F., Wilfley, D. E., Pung, M. A., Winzelberg, A., Eldredge, K., & Taylor, C. B. (2001). An interactive Internet-based intervention for women at risk of eating disorders: A pilot study. International Journal of Eating Disorders, 30, ~ 73 ~
206 Volume 20, Number 2 July 2016 December 2016 Stress reaction and Post-traumatic stress disorder among flood victims of Lahore- Pakistan and role of community (ROC) Dr Amina Nasar MBBS, FCPS (Psychiatry) Child and General Adult Psychiatrist, Lahore Pakistan Ms Sadaf Inayat MS Clinical Psychology Clinical Psychologist working with Dr. Amina Nasar Dr Ali Zulqarnain MBBS, FCPS (Psychiatry) General Adult Psychiatrist Assistant Professor of Psychiatry, Sargodha Medical and Dental College, Sargodha Pakistan. Dr. Muhammad Nasar Sayeed Khan MBBS, FCPS (Psychiatry) Associate Professor of Psychiatry, Division of Developmental Disabilities, Department of Psychiatry, Queens University, Kingston Ontario, Canada Citation: Nasar A, Zulqarnain S, Inayat A, & Khan MNS. (2016) Stress reaction and Post-traumatic stress disorder among flood victims of Lahore- Pakistan and role of community (ROC) Vol 20 (2) Abstract Aims and Objectives: The present study investigated the relationship between stress reaction, Post-Traumatic Stress Disorder (PTSD) and Role of community (ROC) among flood victims. Sample: The stratified random sampling was used to collect total sample of 130; consisted of 100 flood victims with the age range of 18 to 40 years (M=1.52, SD=3.9) and 30 community relief group workers with the age range from most flood affected areas of district Lahore. Material and Method: Kessler stress reaction Scale and The Impact Event Scale-Revised were used to measure the stress reaction and Post-Traumatic Stress Disorder (PTSD) among flood victims after translating into Urdu language. Results and Conclusion: The study found that there was a significant positive relationship between stress reaction and Post-Traumatic Stress Disorder. Moreover Post Traumatic Stress Disorder and Education emerged as significant predictors of stress reaction. Key words: Stress reaction, Post-traumatic stress disorder, role of community flood victims, Lahore ~ 74 ~
207 Volume 20, Number 2 July 2016 December 2016 Introduction: A disaster is defined as a basic disruption of the social context within which individuals and groups function (Fritz, 1961). Among all the natural disasters floods are the most distressing and disturbing which result in various physical and psychological effects on individual life in terms of personal and daily functioning. It results in a lot of personal and public harm in term of their possessions, properties, well-being, strength and loss of employment and income. These all contribute as a major risk factor for effecting the behavior, thoughts and overall well-being of people affected by it. Various emotional problems are caused by increased apprehensions, terror, anxiety and miseries related with the disaster. Among these depression and anxiety are frequently reported among flood victims. After flood like disaster the rise in water level, lack of proper awareness and less time for precautionary and defensive measures may cause anxiety symptoms among the victims. The various factors that serve an important function in determining the nature and severity of the problem are their coping strategies, flexibility, age, gender, type of family system and their socioeconomic status (Agnieszka et al., 2007;Noris et al., 2002). The effect of the particular disaster depends on the coping mechanism used by the victim which predisposes him or her toward stress disorder which further results in more extreme psychological problem (Green & Lindy 1994, Stab et al., 1999). Stress reaction is characterized by unpleasant emotional states such as tension, depression, worthlessness and irritability (Barlow & Durand, 2005). These all result in reduction of resilience; lack of emotional wellbeing, disability to cope with pain, dissatisfaction and depression. Stress reaction starts with experiencing decreased wellbeing then moving towards distress and various times affecting individual s whole life (Horwitz & Scheid,1999). Stress reaction emerges when there is a negative relationship between the individual and his or her environment (Lazarus, 1966; Lazarus & Folkman, 1984). Depression results in short-term experience of sadness or a temporary or permanent loss. Anxiety is an innate and natural instinct or character for the purpose of saving from emotional shock, panic and fear of damage. Concerns regarding disaster result in unpleasant experience as the environmental factors are perceived life threatening. The effect of this is long lasting, permanent and sometimes remains up to a lifetime. The things that can stimulate fear and stress among the individuals will cause concern them to deal with the situation (Calvin, 1979). Stress reaction is predisposed by various environmental, psychological, environmental and personal variables and emotional distress among the individual. According to Norris (2005) among the various effects of natural disaster the main include depression, anxiety, stress reaction, cognitive misjudgments errors, terror and various health related difficulties. According to National Disaster Management Authority (2003), the natural disasters lead to major breakdowns and stress which may result in symptoms such as increased anxiety levels and depressive symptoms that may be long lasting and prolonged. These psychological characteristics can impair the vulnerabilities and sometimes restore the recovery efforts. Sanaand Khattak (2013) conducted a research with the aim to assess the psychological status of the people suffering from flood victims and the level of well-being in individuals suffering from Post-Traumatic Stress Disorder (PTSD) and their gender effects. For this people from Banda Sheikh Ismail was asked about the experience of the disaster and how they perceived it. The results revealed that there are no effects with respect to their age, gender and the level of education level. This study reveals that most people who suffer from various catastrophic events like floods have increased risk of developing PTSD symptoms and need specialized mental health services in order to manage their symptoms. Otto, Boos, Dalbert, Schops and Hoyer (2006) conducted a research on the symptoms of PTSD, depression and ~ 75 ~
208 Volume 20, Number 2 July 2016 December 2016 anxiety among the flood victims. This study focused on the investigation of the Belief in a Just World (BJW) on the overall mental health and well-being of the flood victims. The results revealed symptoms of PTSD and stress reaction among flood victims and they also studied relationship of these two clusters with BJW. It was concluded that Belief in Just world was negatively associated with the stress reaction among flood victims. Also, the BJW did not reveal any relationship with PTSD symptoms. In conclusion, the results revealed that BJW buffers mental health and psychological wellbeing. Neria, Nandiand Galea (2007) conducted a research on the Post-traumatic stress disorder (PTSD) after the disaster. The research aimed at assessing the indication about Post-traumatic stress disorder (PTSD). The results indicated that the disasters were classified in various categories such as human-made disasters, technological disasters and natural disasters. It suggested the fact that the burden of Post-traumatic stress disorder (PTSD) among persons exposed to disasters is extensive and associated with various social, demographic and background factors. Liu et al. (2006) conducted a study to assess the incidence and factors of posttraumatic stress disorder (PTSD) in flood victims of Hunan, China. The results indicated that among the people experiencing the disaster most of them had symptoms of posttraumatic stress disorder (PTSD). The factors, which were more prone to developing the symptoms, were gender, old age and the nature and severity of the flood. Ahern, Kovats, Wilkinson, Fewand Matthies (2005) conducted a study to assess the global health impacts of flood victim. They concluded that floods are associated with many physiological and psychological conditions and remedies for such condition should be contingent before and after disasters. Stanke, Murray, Amlot, Nurse and Williams (2012) studied the effects of the floods on the mental health of the individuals. The results indicated that all most people of all the age groups are prone to developing various mental health problems associated with the floods. The study also put great emphasis on the effect of various primary and secondary stressors on people affected by floods. Psychological support plays a very important role that is provided through close relationships such as families, friends and community help. Gibbs and Montagnino (2001) conducted a study aimed at determining the psychological perspective of disasters and the mental health hazards. They reported that more stress reaction the individuals suffers the more chances is that he or she will suffer from various emotional consequences. In order to control the effects of emotional as well as stress reaction various efforts by the psychologists are needed to help the victims and sufferers of the disasters. There is a constant need of various intervention techniques and therapies in order to help the disaster victims. Rationale of the Study In regions of Lahore flood effects almost after every two or three year on average so the perceptions of flood victims and community have changed regarding disaster management through period of the time. The findings of the study will highlight the role of community in providing relief and support and its effect on the level of stress reaction and Post-Traumatic Stress Disorder (PTSD) present in flood victims. The study will help in monitoring the level of stress reaction and symptoms of Post-Traumatic Stress Disorder (PTSD). Remediation and prevention of stress reaction and associated psychological problems present among flood victims. Psycho education will be provided regarding promotion and maintenance of mental health among victims after floods. Awareness regarding service provision and wellbeing of individuals will also be raised with the help of this study. It also includes the evaluation of the contribution of contingency plan and disaster management by Government and awareness campaigns by the Media. Hypothesis The hypotheses of the study are as follows: ~ 76 ~
209 Volume 20, Number 2 July 2016 December There will be a positive relationship between stress reaction and Post Traumatic Stress Disorder (PTSD) among flood victims 2. There will be a negative relationship between Role of Community, Psychological, Distress and Post Traumatic Stress Disorder (PTSD) among flood victims. Method The nature of study is Correlational as it is aimed to find the relationship between stress reaction, Post -Traumatic stress disorder (PTSD) and role of community among flood victims of Lahore. An Ex post facto research design was used because people were already prone towards flood. The research was carried out in two phases. In the first phase translation of the Kessler stress reaction Scale (K-10) and the Impact of Event Scale (IES-R) was done to use it in the present study. Originally the scale was in English language which was not comprehendible for the population of research study so it was translated into Urdu language and its psychometric properties were also explored and the phase two was comprised of the main study. Sample: Stratified Random Sampling was used to select the 100 flood victims (96 men and 34 women, age range year, M = 1.52, SD =.61) belonging to different areas of Lahore. Measures The following measures were used in the current study: 1. Kessler stress reaction Scale (Kessler, 2002). It consisted of a total of 10 items which contained various symptoms of anxiety and depression. All the 10 items are summed together to get a total score. It ranges from 10 to 50 where 10 indicates low risk of anxiety or depressive and 50 indicates high risk of anxiety or depressive disorder. The cut off scores for the level of anxiety and depression are: 10 to 15 indicate low or no risk, 16 to 29 indicate medium risk and 30 to 50 indicate high risk. The alpha reliability scores ranged from 0.42 to 0.74 which indicated that the scale is a moderately reliable. The alpha value of the translated version is.88, which is considered reliable. 2. The Impact Event Scale (Weiss, 2007) The Urdu version of the Impact Event Scale (TES-R) was used to measure the Post-Traumatic Stress Disorder (PTSD) symptoms. The Impact Event Scale (TES-R) consisted of 22 items. It consists of three subscales i.e. Intrusion subscale, Avoidance subscale and hyper arousal sub scale. For all the scales the scores range from o to 40. It can be used with healthy as well as older adults exposed to any form of traumatic life event. The alpha reliability or the English version of the Impact Event Scale (IES-R)was.80, which is highly reliable. The scale for translated into Urdu the alpha reliability for the Urdu version is Demographic Questionnaire. Demographic questionnaire was developed based on literature review which was used to get details like gender of the participant, age, profession, education, and marital status, number of family members, family system and monthly income. Information related to damage due to flood, profession after flood, precautionary measures and the role of community in helping flood victims were also mentioned in the questionnaire. 4. Informed Consent Form. All research participants were debriefed about the objectives and purpose of the study before administration of the research protocol. They were assured that whole information sought from them would be kept confidential and used for academic purposes. Moreover a written consent was taken from them. ~ 77 ~
210 Volume 20, Number 2 July 2016 December 2016 Methodology: The permission was sought from the Flood Fighting Department of Lahore and they were also briefed about the purpose of conducting this research. A list of flood affected arears was taken from them and population of the Lahore affected areas was divided into eight strata s and research participants were selected randomly in each stratum. The Impact Event Scale and Kessler stress reaction scale was translated into Urdu language for use in the present study. The sample consisted of flood victims so brief counseling sessions were also planned with the victims in order to ease their distress regarding flood. Permissions were also sought from the original authors of the scales. Results Table 1 Pearson Product Moment Correlation between stress reaction and Post Traumatic Stress Disorder (N=100) Variables Total PD Total PTSD INT AVO HYP M SD Total PD **.70 **.54 **.53 ** Total PTSD **.89 **.88 ** INT **.76 ** AVO ** HYP Note. PD= stress reaction, PTSD=Post-Traumatic Stress Disorder, INT= Introversion, AVO= Avoidance, HYP= Hyperarousal **p<.01 The table showed that the there is significant relationship between stress reaction and Post Traumatic Stress Disorder (r=.66, p<.01). This indicates the fact that the stress reaction and Post Traumatic Stress Disorder (PTSD) and its subscales as Introversion (r=.93, p<.01), Avoidance (r=.89, p<.01) and Hyperarousal (r=.88, p<.01) were strongly correlated with each other. So the hypothesis was accepted as if the stress reaction increases the symptoms of PTSD will also likely to be increased. ~ 78 ~
211 Volume 20, Number 2 July 2016 December 2016 Table 2 Predictors of stress reaction stress reaction Model 2 Variable Model 1β β 95% CI Constant 6.01** 10.45** [6.79, 14.11] Total PTSD.31**.31** [.25,.39] Education.58** [-2.99, -.68] R² F 73.67** 45.19** R². 05 F 9.93 Note. N=100, CI= Confidence Interval. ** p<.01 The table demonstrated the regression analysis of stress reaction and the clusters. In the regression model, Total PTSD and Education emerged significant predictors of stress reaction. According to model 2, the values obtained for PTSD was (p<.01, t=9.06) and Education was (p<.05, t=-3.15). This indicated that PTSD and education emerged as significant predictors of stress reaction. According to model 2, the value of R² indicated that Post-Traumatic Stress Disorder (PTSD) and education accounted for 49% variance in stress reaction among flood victims. Table 3 Linear Regression Analysis of stress reaction and Post Traumatic Stress Disorder (PTSD) stress reaction B SE Β t P 95% CI Constant [3.78, 8.50] AVO [-1.17,-.19] HYP [-1.38,-.24] PTSD [.48, 1.06] R.70 ΔR².40 ~ 79 ~
212 Volume 20, Number 2 July 2016 December 2016 Note. AVO=Avoidance, HYP=Hyper arousal, PTSD= Post Traumatic Stress Disorder, B= unstandardized beta. The table demonstrated the regression analysis of stress reaction and the clusters of Post-Traumatic Stress Disorder (PTSD) Psychology. A total of four variables i.e. Total Post-Traumatic Stress Disorder (PTSD), Introversion, Avoidance and Hyperarousal were entered in the model. The values obtained for sub scales of Hyperarousal was (p<.05, t=-2.83) and the subscale of Avoidance was (p<.05, t=-2.77).also, the values obtained for total Post Traumatic Stress Disorder (PTSD) was (p<.05, t= 5.20). This indicated the fact individuals belonging to the sub scales of Hyper arousal and Avoidance had significant stress reaction. The value of R² indicated that Post-Traumatic Stress Disorder (PTSD) accounted for 77% variance in stress reaction among flood victims. Table 4 One-Way Analysis of Variance stress reaction and Post-Traumatic Stress Disorder (PTSD) among flood victims Variables Source MS F p stress reaction Early adulthood Middle adulthood Late adulthood Post Traumatic Stress Disorder Early adulthood Middle adulthood Late adulthood Note. M=Mean SD=Standard Deviation. P>.05 The table showed that there were three age ranges of the participants i.e. Early, middle and late adulthood which acted as the independent variables and stress reaction served as a dependent variable. The results of Analysis of Variance (ANOVA) were found to be insignificant (p>.05). This means that there was a no significant difference on stress reaction among the three age ranges of the participants i.e. Early, middle and late adulthood. On the other hand, the results of Analysis of Variance (ANOVA) were found to be significant (p<.05).this means that there was a significant difference on Post-traumatic Stress Disorder (PTSD) among the three age ranges of the participants i.e. Early, middle and late adulthood. Table 5 ~ 80 ~
213 Volume 20, Number 2 July 2016 December 2016 Mean differences of Males and Females on stress reaction F 9 Male emale 5% CI M SD M SD T Df P LL UL Cohen s Variable d PD PTSD Note. M=Mean SD=Standard Deviation, df=degree of freedom, CI=Confidence Interval, PD= stress reaction, PTSD= Post traumatic stress disorder The table showed that slight differences were found between the mean scores of males and females that indicated that there is no significant difference present between the two categories (i.e. males and females) based stress reaction. The significance level was (p>0.5) which indicated that there was no significant difference on stress reaction among males and females. This means that both males and females were equally prone towards stress reaction. Discussion The results indicated that there was a significant relationship among stress reaction and posttraumatic stress disorder (PTSD) among flood victims. Asad (2011) investigated the relationship between psychopathology, clinical symptoms and their demographic correlated among female adolescent flood affectees of district Muzzafargarh. The results showed that most common disorder found among them was Posttraumatic Stress Disorder (PTSD) followed by Generalized Anxiety Disorder and Major depressive Disorder. Also clinical symptoms of Posttraumatic Stress Disorder (PTSD) and Generalized Anxiety Disorder such as emotional and stress reaction, depression and anxiety were also present among the participants. It was also hypothesized that Post-traumatic stress disorder (PTSD) is likely to be a predictor of stress reaction among flood victims. This hypothesis was accepted that Post-traumatic stress disorder (PTSD) emerged as a significant predictor of stress reaction among the flood victims. Manguno-Mire, Sautter, Lyons,Meyers, Perry, Sherman, Glynn and Sullivan (2007) investigated the relationship between stress reaction and burden among female partners of combat veterans with Post Traumatic Stress Disorder (PTSD).The results indicated that partners of veterans with combat-related Post Traumatic Stress Disorder (PTSD) experienced significant level of emotional distress. stress reaction and partner burden each was associated with associated with others predictors have distinct correlates and implications within the family environment. Results of our study indicated that a significant difference was not found on stress reaction among adults in middle and late adulthood as compared to early adulthood.this can be related to the fact that irrespective of their age groups all the three sub group i.e. early, middle and late adulthood are equally prone to developing stress reaction as they are residing within the same flood effected community and sharing the same resources. The results indicated that adults in middle and late adulthood had increased level Post-traumatic stress disorder (PTSD) than people in early adulthood. Telles, Singh and Joshi (2009) explored the risk of developing Post Traumatic Stress Disorder and Depression in the survivors of the Bihar floods. The results indicated that the ~ 81 ~
214 Volume 20, Number 2 July 2016 December 2016 people which were above the age of 60 years had significantly higher level of Post-Traumatic Stress Disorder (PTSD) as well as depression when compared with the others groups. This means the people in old age are more prone to developing Post Traumatic Stress Disorder (PTSD) depression which must be taken into account by the relief organizations. This study showed that the people belonging to low socioeconomic status were not prone to developing stress reaction as well as symptoms of Post-Traumatic Stress Disorder (PTSD). This can be due to the fact the people living in the community sample had approximately the same level of income annually so no distinction could be made in their income status. It was hypothesized that there would be gender differences on stress reaction among flood victims of Lahore. Surprisingly the hypothesis was rejected as there was no gender differences were found on stress reaction among flood victims of Lahore. This can be related to the fact that the number of males and females was not equal and females were far less prevalent than males. Also, the females failed to give their consent and were reluctant to give any kind of information which can be traced to their educational level and lack of exposure. A significant difference was found among gender differences on posttraumatic stress disorder among the flood victims. A research was conducted by Tahira (2011) investigated the role of social support in predicting the amount of psychological wellbeing and Quality of life among the flood victims of Muzzaffargarh. Results revealed that Social Support had an impact on Quality of Life a. The results revealed that on the basis of gender difference, males had a better level of social support, psychological wellbeing and quality of life as compared to females. This reveals the fact the females are more prone towards developing psychological symptoms and ailments like Post Traumatic Stress Disorder (PTSD). Implications A number of implications are generated from the current study. This study will help to understand the role of community to lessen the impact of flood disaster on mental health of victims. Based on this research the government, mental health professional and vulnerability of mental health problems among victims. The findings provided us broader spectrum about all those factors contributed in prevalence of psychological issues among flood victims such as less role of community including government, media, and people living nearby flood affected areas. Limitations There were a number of limitations based on individual, government and media level. First of all, the flood victims who were approached were mostly illiterate so even after proper psycho education they could not comprehend the questions asked and information sought properly. As the fieldwork was done on individual basis and the flood victims were approached on door to door basis so it consumed a lot of time and effort. Equal number of males and females could not be included in the study as the females were more introverts and shy so they failed to give their consent for data collection. There was also a contradiction between the information given by the government and the flood effected people. Recommendations Government should play an active role in managing the practical issue of disaster other than only calculating and proposing solution. Mental health issues such as stress reaction among flood victims and maintain proper monitoring system on the aid sent to the flood affected areas should be kept on preference. Also, during the flood they should play a major role in controlling physical illnesses and stress reaction by managing all disaster related issue on pre hand. The flood victims were passive in seeking aid for their damages, so media agencies should approach the government and NGO S in order to help them. Volunteer work, relief aid projects and early contingency plans should be made and implemented by the government along with help of nearby educated people. The teachings of appropriate coping skills to deal with aftermaths of disaster i.e. both ~ 82 ~
215 Volume 20, Number 2 July 2016 December 2016 physiological and psychological should be done with the individuals. These coping skills will help flood victims to cope with their stress reaction and trauma related issues and there will be less probability of developing stress reaction and post-traumatic stress disorder among flood victims in an area where floods are common. References Ahern, M., Kovats, R.S., Wilkinson,P., Few,R., & Matthies, F.(2005). Global health impacts of floods: epidemiologic evidence. Journal of Epidemiological Revolution, 27, American Psychiatric Association.(2013). Diagnostic and statistical manual of mental disorders (5th ed.).arlington, VA: American Psychiatric Publishing. Amstadter, A.B.(2008).Emotion regulation and anxiety disorders. Journal of Anxiety Disorders,22(2), doi: /s Barlow, D.,& Durand,V.(2005). Abnormal psychology: An integrative approach. Belmont, CA: Thomson Wadsworth Publishers. Beck, A.T.(1967). Depression: Clinical, experimental, and theoretical aspects. New York: Harper & Row Publishers. Becker, M. H., & Rosenstock, I. M. (1984). Compliance with medical advice.health care and human behavior, Bruhn, J. G. (2005). The sociology of community connections. New York: Springer Publications. Calvin, S.H.(1979). A Primer of Freudian Psychology: A Mentor Book. Pennsylvania State University: New American Library. Chou, F.H., Chou, P., Su, T.T, Ou-Yung.W.C., Chein, I.C., Lu, M.K.,&Huang, M.W.(2004).Survey of quality of life and related risk factors for a Taiwanese village population 21 months after an earthquake. Australian Journal of Psychiatry,38, doi : /j Crabtree, A. (2012). Climate change and mental health following flood disasters in developing countries, A review of the epidemiological literature: What do we know, what is being recommended?. The Australasian Journal of Disaster and Trauma Studies, 1, Retrieved from Dunmore, E., Clark, D. M., & Ehlers, A. (2001). A prospective investigation of the role of cognitive factors in persistent posttraumatic stress disorder (PTSD) after physical or sexual assault. Behavior Research and Therapy, 39(9), doi: /S (00) Durkin,M.E.( 1993).Major depression and post-traumatic stress disorder following the Coalinga (California) and Chile earthquake: A cross sectional comparison. In R. Allen (Ed.), Handbook of disaster intervention. New York: Springer Publications. Ehlers, A. & Clark, D.M. (2000). A cognitive model of Post-Traumatic Stress Disorder. Journal of Behavior Research and Therapy, 38, doi: S (99)00123 Fistein, E., Bhamani, A., Sobani, Z.A., Baqir, M., Bham, N.S. & Beg, M.A. (2012). Mental health in the wake of flooding in Pakistan: An ongoing humanitarian crisis Journal of the College of Physicians and Surgeons Pakistan, 22(1), Retrieved from Food and Agriculture Organization of the United Nations. (2003).Non-Human Antimicrobial Usage and Antimicrobial Resistance:Scientific assessment. Retrieved from int/foodsafety/publications/micro/en/amr.pdf Fritz, C. E. (1961).Contemporary social problems:an introduction to the sociology deviant behavior and social disorganization. New York: Harcout. Green, B. L., & Lindy, J. D. (1994). Post-traumatic stress disorder in victims of disasters. Psychiatric Clinics of North America. Retrieved from Hidalgo, R. B., & Davidson, J. R. (2000). Posttraumatic stress disorder: epidemiology and health-related considerations. Journal of Clinical Psychiatry. Retrieved from ~ 83 ~
216 Volume 20, Number 2 July 2016 December 2016 Horwitz, A.V & Scheid, T.L. (1999) Approaches to mental health and illness: Conflicting definitions and emphases: Handbook for the study of mental health. New York: Cambridge University Press. Johari, J. & Marzuki, N.A. (2013).Relating Stress, Anxiety and Depression among Flood Victims Quality of Life in Malaysia: A Theoretical Perspective. International Journal of Social Science and Humanity, 3(6), doi: /IJSSH.2013.V3. Kaplan, H.B.(1980).Psychological Stress: Trend in Theory and Research. NY:Academic Press Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and ageof-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), Retrieved from Khattak, S. R., & Khattak, S. U.(2014). Prevalence of Post-Traumatic Stress Disorder in Flood Affected Population of Banda Sheikh Ismail, District Nowshera. Journal of Postgraduate Medical Institute (Peshawar-Pakistan), 28(1). Retrieved from mi.org.pk/index.php/jpmi/article/vie w/1443/1440 Lazarus, P. J., Jimerson, S. R., & Brock, S. E. (2003). Responding to natural disasters: Helping children and families. National Association of School Psychologists. Retrieved from Liu, A., Tan, H., Zhou, J., Li, S., Yang, T., Wang, J., Liu, J.,&.. Wen, S.W. (2006).An epidemiologic study of posttraumatic stress disorder in flood victims in Hunan China.Canadian Journal of Psychiatry, 51(6), PMID: Mandler, G. & Watson, D.L. (1996).Anxiety and the intruption of behaviour.in C.D. Spielberger (Ed) Anxiety and behavior. New York:Academic Press. Meyer, H., Taiminen, T., Vuori, T., Äijälä, A., & Helenius, H. (1999). Posttraumatic stress disorder symptoms related to psychosis and involuntary hospitalization in schizophrenic and delusional patients. The Journal of Nervous and Mental Disease, 187(6), Retrieved from Meyer, M. A. (2013). Social capital and collective efficacy for disaster resilience: Connecting individuals with communities and vulnerability with resilience in Hurricane-prone Communities in Florida (Unpublished doctoral dissertation), Colorado State University. Mirowsky,J. & Ross,C.E. (2013).Social Causes of stress reaction. New York: Walter de Gruyter.Inc. Nasir, R., Zainah, A.Z.,& Khairudin, R.(2012).Psychological Effects on Victims of the Johor Flood 2006/2007.Journal of Asia Social Science, 8(8).doi: /ass.v8 n8p126 National Mental Health Association-NMHA. (2003).Post- Traumatic Stress Disorder. Retrieved from Neria, Y., Nandi, A., & Galea, S. (2008). Post-traumatic stress disorder following disasters: a systematic review. Psychological Medicine, 38(04), doi: /s National Disaster Management Authority-NDMA. (2013).Flooding and its management plans. Retrieved from Norris, F.H., Friedman, M, J., Watson, P.J., Byrne. C.M.,Diaz, E., & Kaniasty, K.(2002).6000 disaster victims speak- Part 1:An empirical review of the empirical literature, journal of Psychiatry, doi: /psyc Otto, K., Boos, A., Dalbert, C., Schöps, D., & Hoyer, J. (2006). Posttraumatic symptoms, depression, and anxiety of flood victims: The impact of the belief in a just world. Personality and Individual Differences, 40(5), doi: /j.paid Stanke, C., Murray, V., Amlôt, R., Nurse, J., & Williams, R. (2012). The effects of flooding on mental health: Outcomes and recommendations from a review of the literature. PLoS currents. PMCID: PMC Stępień, A., Małyszczak, K., Piotrowski, P., & Kiejna, A. (2007). Picture of posttraumatic stress disorder among flood victims correlated to scale of sustained loss. Archives of Psychiatry and Psychotherapy, 4, Retrieved from app.nazwa.pl/uploads /images/2007 ~ 84 ~
217 Volume 20, Number 2 July 2016 December 2016 Strongman, K.T.(1995).Theory of anxiety.new Zealand Journal of Psychology, 77, Retrieved from Stuart, M (2004). Understanding depression following a disaster. (Unpublished Master Thesis) Cooperative Extension, College of Agriculture and Life Sciences, the University of Arizona. Tapsell, S.M., Tunstall, S.M.,Penning-Rosell, E.C.,& Handmer, J.W.(1999). The health effects of the 1998 easter flooding in Banbury and Kidlington. Flood Hazard Research Centre, Middlesex University. Thayer, J.F & Lane, R.D.(2000). A model of neurovisceral integration in emotion regulation and dysregulation. Journal of Affective Disorders, 61(3), doi: /S (00) The Rapid Response Plan. (2011). Flooding in Pakistan. Retrieved from Plan.pdf The World Bank Group. (2010). Response to Pakistan s Floods: Evaluative Lessons and Opportunity. Retrieved from Wahlstrom, L., Michelson, H., Schulman,A. & Backheden, M.(2008).Different type of exposure to the 2004 Tsunami are associated with different levels of stress reaction and post-traumatic stress. Journal of Traumatic Stress.21(5), Retrieved from Wang, X., Gao, L., Shinfuku, N., Zhang,H., Zhao, C.,& Shen,Y.(2000). Longitudinal study of earthquake related PTSD in a randomly selected community sample in in North China. American Journal of Psychiatry, 57, doi: /appi.ajp ~ 85 ~
218 Volume 20, Number 2 July 2016 December 2016 The Rise and Fall of the Mental Health Recovery Model Brian I Field B.A, PG Cert (mental health and addictions), PG Cert (clinical rehabilitation), PG Dip (social sector evaluation research), M.A. (applied) (social science research), M.A. (applied) (social work) Doctor of Health Science Student Auckland University of Technology New Zealand Kirk Reed DHSc, MOT, Dip OT, NZROT Senior Lecturer Department of Occupational Science and Therapy School of Clinical Sciences Auckland University of Technology New Zealand Citation: Field, BI & Reed, K. (2016) The Rise and Fall of the Mental Health Recovery Model. (ROC) The International Journal of Psychosocial Rehabilitation. Vol 20 (2) Abstract The recovery model in mental health was the result of a number of coinciding events that include economic issues, social movements and consumer rights. This led to a new approach to mental health treatment. However the economic issues led to a new political agenda arising. Neo liberalism saw the decline in mental health consumers gaining empowerment and an equal share for the responsibility of their own treatment. This paper looks at a number of reasons why this model was introduced, the history behind it being introduced and why it has been largely ineffective in becoming a dominant model within mental health practice. Keywords: Neo liberalism, Mental health recovery model, Deinstitutionalisation ~ 86 ~
219 Volume 20, Number 2 July 2016 December 2016 Introduction: The Mental health recovery has been a part of the mental health landscape for over forty years but has failed to be effective in improving outcomes for service users of mental health. This paper looks at a number of reasons why this model was introduced, the history behind it being introduced and why it has been largely ineffective in becoming a dominant model within mental health practice, including Neo liberal policies and economic necessities. History Psychiatric institutionalisation within Aotearoa / New Zealand had been seen as a failure, yet at it's peak, in 1972, thirteen public and three private psychiatric hospitals provided 10,000 psychiatric beds (Department of Health,1972). At this time, psychiatric hospitals were expected to handle the majority of psychiatric patients for the foreseeable future (Department of Health, 1969). Yet the purpose and success of psychiatric hospitals was slowly being challenged, evidenced by the apparent decision in 1963 to plan to build no more psychiatric institutions (Brunton, 2012). A national survey at this time recommended that 26 per cent of all patients with a psychiatric diagnosis be considered for placement in a range of accommodation settings outside psychiatric hospitals (Jeffery & Booth, 1974). To counteract the move away from psychiatric inpatient services, from the early 1970's, psychiatric services began to concentrate on outpatient care, community-based treatment and the development of modern facilities (Brunton, 2012). This move was partly due to economic factors, the advent of psychotropic drugs and the counter-culture movements of the era, such as the anti war movement, woman's rights movement, anti racist movements, environmental movements and equal rights movements which included psychiatric patients (Boyd, 2016; Knapp, Beecham, McDaid, Matosevic & Smith, 2011; Hirsch, Kett &Trefil, 1993). Economic Reasons Economically Aotearoa / New Zealand suffered when Britain finally joined the European Economic Community in At this time Aotearoa/ New Zealand s exports to the Mother Country had fallen to less than 30% of all the countries exports. This occurred around the time of the first oil crisis when the cost of oil rose from US $3 a barrel to nearly US $20 a barrel. In turn this led to higher petrol prices which escalated to higher freight costs, higher costs for goods, higher wage rates and inevitably higher retail prices (Ministry for Culture and Heritage, 2012). As a result the Government needed to reduce its spending. Prior to this period the escalating expenditure on health and the inequity of health provision had become a source of economic concern for governments and the health sector. These issues were highlighted by a series of reviews from the 1950's beginning with the Barrowclough Committee (1953), The Department of Health review (1969), The Royal Commission on social security (1972) and 'A health service for New Zealand' (1975) (New Zealand Parliament, 2009). Social Movements Added to these challenges were the social movements of the 1960's and 1970's. The culture of this period was distinct from the post World War Two conservative lifestyle of the 1950's and there was a revolution of thought and a radical shift within the framework in most western cultures. Within this period there was a focus on the rights of individuals with both the civil rights movement and the feminist movement attacking beliefs and values that oppressed and limited groups within the population (Goodwin & Bradley, 2005). This generation was also shaped by powerful events including the war in Vietnam, the civil rights movements, the hippie movement, a newly emerging environmental movement, gay rights movements and populous music and drug use (Goodwin & Bradley, 2005; Dixon & Goldman, 2003). Consumer Influences ~ 87 ~
220 Volume 20, Number 2 July 2016 December 2016 The 1960's saw the establishment of the consumer/survivor/ex-patient movements (Morrison, 2005). This group was a diverse association of individuals who either were currently accessing mental health services (known as consumers or service users) (Morrison, 2005), or who were survivors of interventions by psychiatry, or who were ex-patients of mental health services (Corrigan, Roe &Tsang, 2011). From within the movement arose the recovery model - which sought to overturn therapeutic pessimism and to support sufferers to forge their own personal journal towards the life they wanted to live (Everett, 1994). Health Professionals Influences Within mental health a number of professionals also sort changes, including psychiatry, nursing and social work. Within psychiatry a movement arose which came to be referred to as the anti-psychiatry movement (Berlim, Fleck, Shorter, 2003). Anti-psychiatry was foremost a social movement that questioned not only the legal privilege of psychiatrists to detain and treat individuals with mental disorders, especially in a compulsory manner, but also the increasing medicalisation of madness. Anti-psychiatry also questioned the very existence of mental illness itself (Berlim, Fleck, Shorter, 2003). In conjunction with the anti psychiatric movement, in the 1960s, saw changes continue between nursing and social work (Jones, 1963), with the formation of the New Zealand Association of Social Work in 1964 (Beddoe & Deeney, 2012). This was important as social work in health care in New Zealand had from its inception added the holistic dimension to health care (Auslander, 2001). Auslander's review of 100 years of health social work documents the move from the disease paradigm (biomedical) to the social model of health (psychosocial) which takes into consideration social, psychological, spiritual, cultural and ecological factors of health (Auslander, 2001). This holistic approach of care was important for the recovery model as it conceptualises illness (and mental illness) as a complex interaction between the environment and the physical, behavioural, psychological, cultural and social factors which impact on health (Bracht, 1978; Bywaters, 1986; Lindau, Laumann, Levinson, & Waite, 2003). Bywaters adds that social work can assert the value of care as well as cure (1986, p 670). The Recovery Model Within mental health the new model of recovery has a number of definitions, and has two main streams of thought. One definition is derived from the medical model and is described clinically and understood to be the return of the patient s former state of health. This is normally obtained by hospitalisation and medication (Petersen, Friis, Haxholm, Nielsen & Wind, 2015). Other definitions of recovery come from within the consumer/user/survivor movements of mental health and does not require, or focus on symptom remission or a return to normal functioning, as does the medical model. Within these definitions, recovery is expressed as a process of personal growth and development which can lead to regaining control of one's life, having personal fulfilment and a meaningful life (Davidson, O'Connell, Tondora & Evans, 2005). Another consumer/user/survivor definition describes recovery as being client-centred and having a client-directed focus, with the client deciding how their recovery is defined (Lukens & Solomon, 2013). From a holistic perspective Lapsley, Waimarie & Black (2002 p2) describe recovery as, knowing who you are, and where you come from, and reintegrating yourself with your own people in your own way. Recovery became recognised and a practised theory within mental health systems in a number of countries which included; United States of America, England, Ireland, Australia and Aotearoa / New Zealand (Schrank & Slade, 2007). Within Aotearoa/ New Zealand the recovery model was first introduced and promoted in 1998 through the Blueprint for mental health in New Zealand-how things need to be and quickly became a main model of practice (O Hagan, Reynolds & Smith, 2012). The Blueprint for Mental Health Services in New Zealand; how things need to be set out the need to remodel ~ 88 ~
221 Volume 20, Number 2 July 2016 December 2016 the mental health services to allow mental health consumers to be more actively involved in their treatment. Aotearoa / New Zealand led the way in introducing such services as peer support programmes and peer led agencies, consumer support staff and family support staff within mental health inpatient units and was becoming a consumer focused and driven mental health service. However within a a few short years Aotearoa / New Zealand has traversed back to a medical driven mental health service with only a few remaining relics of these initiatives left in place and are only symbolic with little impact (O Hagan, Reynolds & Smith, 2012). Which led O Hagan Reynolds & Smith (2012) to state that since the mid 2000's the recovery model concepts has been on the decline within Aotearoa / New Zealand. Yet this is disputed by the Ministry of Health (2014) who states that they are currently supporting recovery model practices. The impact of the recovery model With mental health in a flux of change, the degradation of service delivery and the move towards deinstitutionalisation, new models of care were being examined and saw the drive towards the recovery model (Mental Health Commission, 2001). The recovery model has been described as the first genuinely post-institutional service philosophy (Mental Health Advocacy Coalition, 2008) with Aotearoa / New Zealand being attributed as being the first country in the world to formalise recovery as a national policy (Mental Health Commission, 2007). The recovery model requires mental health service providers to enable service users to identify and develop their own strengths and resources and service users taking an active role in improving their lives and service delivery focused on making this possible (Martindale & Phillips, 2010; Mental Health Commission, 2001). The recovery model has had an international impact on treatment for mental health with different countries introducing the model of care. Since 1998 all mental health services in Aotearoa / New Zealand have been required by government policy to use a recovery approach (O Hagan, 2004; Jacobson & Greenley, 2001). In the United States recovery was primarily initiated by the Presidents Freedom Commission Report (Commissioner of Mental Health 2003). In Ireland the Mental Health Commission (2008) released 'A Recovery Approach within the Irish Mental Health Services. A Framework for Development' which introduced mental health recovery approaches after a four year review of the international evidence. The Australian government released it's 'National framework for recovery-oriented mental health services: Policy and theory' in 2013 (Commonwealth of Australia, 2013). This Australian national policy eventuated after including recovery in the National Mental Health Plan ( ), but not as a national document as there was variation in service delivery between States and Territories (Rickwood, 2004). In the United Kingdom the National Institute for Mental Health (NIMHE) formally endorsed the principles of recovery in 2005, (National Institute for Mental Health, 2005). However there is currently no national government strategy or policy on recovery in mental health in the United Kingdom and the fundamental reason for NIMHE supporting the principles of recovery is because that is what service users want, as it has the potential to provide patients with an enhanced experience of mental health services, to improve the quality of those services and to improve the outcomes of people who use those services (Boardman, Goddard, Henderson, et al, 2010 p6). In Canada the 'Toward Recovery and Well- Being: A Framework for a Mental Health Strategy for Canada' was published and was first produced by the Mental Health Commission in 2009, and outlined a vision with broad goals for transforming the mental health system. This was followed by the same organisation in 2012 with 'Changing Directions, Changing Lives: The Mental Health Strategy for Canada' with the aim of presenting a way of understanding mental health, mental illness, recovery, and well-being that underpins the recommendations set out in ''Toward Recovery and Well- Being: A Framework for a Mental Health Strategy for Canada' and enhances the use of a recovery model within mental health (Mental Health Commission of Canada, 2012). However there is also no Federal policy on re- ~ 89 ~
222 Volume 20, Number 2 July 2016 December 2016 covery-oriented services or policies within Canada, but Ontario has adopted a recovery focused approach to mental health (Canadian Mental Health Association, 2016). All of these nations have based these mental health policy changes on the United Nations development on international human right obligations. Of relevance to this framework are the following international agreements; The United Nations universal declaration of human rights (1948), The United Nations Principles for the protection of persons with mental illness and for the improvement of mental health care (1991) and the United Nations Convention on the rights of persons with disability (2006) (Australia Government Department of Health, 2013). The decline in the recovery model Neo Liberalism On a international scale the introduction of Neo liberalism was one of the major drivers of power and the shift away from Keynesian economic policies - which supported a welfare state supported by Government interventions (Palley, 2004). Historically Neo liberalism has been the overarching political driver since the 1970s with Margaret Thatcher (United Kingdom) and Ronald Regan (United States) instigating these policies which are now dominant within most western societies (Wynne, 2004). Neo liberal political policies, are based on neoclassical theories of economics, or the Washington consensus'. The key elements of this consensus is on the privatisation of assets, outsourcing any services previously (or elsewhere) provided directly by government (Carpenter, 2000; Hartman, 2000). This model of governance relegates the state to setting policy goals and providing funding for services tendered-out to private sector providers, whether the service is for a minority population (like welfare or mental health care) or all citizens (such as local government refuse collection). Along with greater reliance on personal responsibility and civil society (such as non-government volunteer services), these measures remove the state from responsibility for service delivery and focuses on deregulation and tax reform which seeks to maximise the role of the private sector in determining the political and economic priorities of the state (Carney, 2008; Heywood, 2007; Kelsey, 1995). Aotearoa / New Zealand Aotearoa / New Zealand embraced Neo liberalism in 1984 with the election of the fourth Labour Government and commenced policies which included a large portion of state assets being privatised and those which remained in State control were expected to act as businesses within the private sector and produce maximum profits (Kelsey, 1995). Social services was further effected as Neo liberal ideas in Aotearoa / New Zealand brought considerable changes to the way society viewed social security (O'Brien, 2008; Roper, 2005; St John & Rankin, 2002; Kelsey, 1995, 1993). Social services and welfare provision were seen as reducing choice, creating disincentives to work, not supporting tax revenue and adding to the countries debt problems as successive governments borrowed to maintain social spending (Green, 1996). People who received or supported state funding of social services and welfare were portrayed as contributing to the moral decay and social breakdown (Green,1996). This change in societal attitude saw a return of the old individual moral argument to explain why poverty, crime and other social ills occurred which was seen in early colonial times. The welfare state which had enjoyed many years of widespread social and government support came under serious attack and despite considerable evidence based research which warned of the dangers of cutting welfare provisions and social services (Gustafson, 1986; Oliver, 1977) Aotearoa / New Zealand faced a return to the residual model of welfare seen prior to 1938 (McDonald, 1998). This residual model of welfare, with its clear approaches to personal responsibility and moral order was directed by the state, and heavily influenced social services with its new ideas for success and failure, which included new models for social service provision (McDonald, 1998; Barretta-Herman, 1994). As a result the 1980s were characterised by strong tensions, both within and outside of Aotearoa / New Zealand between the calls for social justice and social action. Therefore Neo liberalism has not helped ~ 90 ~
223 Volume 20, Number 2 July 2016 December 2016 the recovery model as it has encouraged stigmatisation of the mentally unwell (Nash, 2007). Yet despite these failings in 2015 the National Party led New Zealand Government announced plans to introduce 'Social Bonds' into Aotearoa / New Zealand and do so in mental health. The basis behind social bonds is to allow the Government to contract out services and funding to non-government or private organisations, with agreed targets and time frames, and if the targets are met, Government will pay back the investors, and also pays a return on their investment. The return to the investors depends on the level of results, up to an agreed maximum (Davison, 2015). Reducing Services Under funding and reducing services within mental health recovery models of care can reduce the challenge to traditional notions of professional power and expertise by preventing the break down of the conventional demarcation between consumers and staff that acknowledges and explores the power differences in the therapeutic relationship and their possible impacts (Australian Health Ministers Advisory Council, 2013). Therefore some organisations have seen the introduction of recovery based services as a way of reducing services and saving money (Slade et al. 2014). One way that the gradual reduction in contact with formal mental health services is undertaken is by contracting our service delivery and then applying funding cuts to organisations that provide these community services which were previously commissioned patient recovery (Slade et al. 2014). The reduction of services are often claimed by Neo liberals as removing ineffective services that need to be replaced or amalgamated with other service providers, but the reduction in services cannot be justified based on meeting the goal of being supportive of recovery as they reduce the power of consumers (Slade et al. 2014). Conclusion The recovery model in mental health has generally failed to provide better outcomes for patients and has failed to become a more inclusive and empowering model through the strong influences of Neo liberal policies. While western cultures, including Aotearoa / New Zealand continue to follow Neo liberal policies, mental health and mental health patients will continue to suffer, just as they have throughout history. References Auslander, G. (2001). Social work in health care: What have we achieved? Journal of Social Work alues and Ethics, 1(2), Australia Government Department of Health. (2013). A national framework for recovery-oriented mental health services: Policy and theory. Canberra Australia: Department of Health and Ageing. Australian Health Ministers Advisory Council. (2013). A national framework for recovery-oriented mental health services: Guide for practitioners and providers. Canberra Australia: Department of Health and Ageing. Barretta-Herman, A. (1994 ). Welfare state to welfare society: Restructuring New Zealand's social services. New York, United States of America: Garland Publishing. Beddoe, L., & Deeney, C. (2012). Discovering health social work in New Zealand in its published work: Implications for the profession. Aotearoa New Zealand Social Work, 24(1), Berlim, M. T., Fleck, M. P. A., & Shorter, E. (2003 ). Notes on antipsychiatry. European Archives of Psychiatry and Clinical Neuroscience, 253(2), doi: doi: Boardman, J., Goddard, C., Henderson, C., McCarthy, J., McInerny, T., Cohen, A.,... Whicher, E. (2010 ). ~ 91 ~
224 Volume 20, Number 2 July 2016 December 2016 Recovery is for All. Hope, Agency and Opportunity in Psychiatry. A Position Statement by Consultant Psychiatrists London England. Boyd, N. (2016). Deinstitutionalization Movement of the 1960s and Other Mental Health Issues. Retrieved February 17, 2016, from Bracht, N. (1978). Scope of social work and its contribution to health care. In N. Bracht (Ed.), Social work in health care: A guide to professional practice (pp. 3-33).. New York America: Haworth Press. Brunton.W. (2012). Mental health services - Closing the hospitals, 1960s to 1990s. Retrieved February 17, 2016, from Bywaters, P. (1986). Social work and the medical profession: Arguments against unconditional collaboration British Journal of Social Work, 16(6), Canadian Mental Health Association. (2016). Recovery rediscovered: Implications for the Ontario mental health system. Retrieved April 5, 2016, from Carney, T. (2008). The mental health service crisis of neoliberalism An antipodean perspective. International Journal of Law and Psychiatry, 31, Carpenter, M. (2000 ). 'It's a small world : Mental health policy under welfare capitalism since Sociology of Health and Illness, 22(5), Commissioner of Mental Health. (2003). President's New Freedom Commission on Mental Health. Achieving the Promise: Transforming Mental Health Care in America. Retrieved April 4, 2016, from Commonwealth of Australia. (2013). A National framework for recovery-oriented mental health services: Policy and theory. Canberra Australia: Department of Health and Ageing Retrieved from /$File/recovpol.pdf. Corrigan, P., Roe, D., & Tsang, H. W. H. (2011). Challenging the Stigma of Mental Illness: Lessons for Therapists and Advocates. New York, United States of America: John Wiley and Sons. Davidson, L., O'Connell, M. J., Tondora, J., Lawless, M., & Evans, A. C. (2005 ). Recovery in serious mental illness: a new wine or just a new bottle?. Professional Psychology: Research and Practice, 36(March 20), Davison, I. (2015). Government announces plans for social bonds for mental health services, New Zealand Herald. Retrieved from Department of Health. (1969). A Review of Hospital and Related Services. Wellington: Department of Health. Department of Health. (1972). Submission to the Royal Commission of Inquiry into Hospital and Related Services - Stage II, Psychiatric Services exclude psychopaedic hospitals (Vol. 2): Department of Health. ~ 92 ~
225 Volume 20, Number 2 July 2016 December 2016 Dixon, L. B., & Goldman, H. H. (2003 ). Forty years of progress in community mental health: the role of evidence-based practices Australian & New Zealand Journal of Psychiatry, 37(6 ), Everett, B. (1994). Something is happening: the contemporary consumer and psychiatric survivor movement in historical context Journal of Mind and Behavior, 15: (55-7). Goodwin, S., & Bradley, B. (2005 ). American Cultural History, The Kingwood College Library. Green, D. (1996 ). From welfare state to civil society Wellington New Zealand Business Roundtable. Gustafson, B. (1986 ). From the cradle to the grave. Auckland Reed Methuen. Hartman, R. (2000). Adolescent autonomy: Clarifying an ageless conundrum Hastings Law Journal, 51, Heywood, A. (2007 ). Political ideologies: An introduction (4th ed.). London, England: Palgrave Macmillan. Hirsch, J. E. D., Kett, J., F., & Trefil, J. S. (1993). The Dictionary of Cultural Literacy (Second ed.). Boston, Massachusetts, United States: Houghton Mifflin Harcourt Jacobson. N, & Greenley, D. (2001). What is recovery? A conceptual model and explication Psychiatric Services, 52 (4 ), doi: /appi.ps Jeffery, I. J., & Booth, J. M. (1974). Survey of Patients in Psychiatric Hospitals (Vol. Special Report pp. 4). Wellingon: Department of Health, Wellington. Jones, A. (1963 ). The contribution of medical social work programme to nursing services New Zealand Nursing Journal, 56(2), Kelsey, J. (1993). Rolling back the State : Privatisation of power in Aotearoa/New Zealand. Wellington: Bridget Williams Books. Kelsey, J. (1995 ). The New Zealand experiment : A world model for structural adjustment?. Auckland Auckland University Press with Bridget Williams Books. Knapp, M., Beecham, J., McDaid, D., Matosevic, T., & Smith, M. (2011). The economic consequences of deinstitutionalisation of mental health services: lessons from a systematic review of European experience. Health and Social Care in the Community, 19(2), doi: /j x Lapsley, H., Waimarie, L. N., & Black, R. (2002). Kia Mauri Tau! Narratives of Recovery from Disabling Mental Health Problems Wellington: Mental Health Commission. Lindau, S. T., Lauman, E. O., Levinson, W., & Waite, L. J. (2003). Synthesis of scientific disciplines in pursuit of health: The interactive biopsychosocial model. Perspectives in Biology and Medicine, 46(3), S74-S86. Luken, J. M., & Solomon, P. (2013). Thinking through recovery: Resolving ethical challenges and promoting social work values in mental health services Journal of Social Work Values and Ethics, 10, Martindale, K., & Phillips, R. (2010). Applying quality of life in mental health social work practice. Aotearoa New Zealand Social Work, 22(1). ~ 93 ~
226 Volume 20, Number 2 July 2016 December 2016 McDonald, D. (1998 ). Social work in Aotearoa New Zealand: An introduction. Auckland Addison Wesley Longman New Zealand Limited. Mental Health Advocacy Coalition. (2008). Destination: Recovery Te Unga ki Uta, Te Oranga. Auckland: Mental Health Foundation of New Zealand. Mental Health Commission. (2001). Recovery competencies for New Zealand mental health workers Wellington Mental Health Commission. Mental Health Commission. (2007). Te harerenga mo te whakaoranga : The journey of recovery for the New Zealand mental health sector Wellington: Mental Health Commission. Mental Health Commission. (2008). A Recovery Approach within the Irish Mental Health Services. A Framework for Development. Retrieved April 4, 2016, from Mental Health Commission of Canada. (2012). Changing directions, changing lives: The mental health strategy for Canada. Calgary Canada: Mental Health Commission of Canada. Ministry for Culture and Heritage. (2012) key events. Retrieved February 18, 2016, from Ministry of Health. (2014). Recovery approach to mental illness Like Minds, Like Mine project. Retrieved March 6, 2016, from Morrison, L. J. (2005). Talking Back to Psychiatry: The Psychiatric Consumer/Survivor/Ex-Patient Movement (New Approaches in Sociology). New York United States of America: Routledge. Nash. M. (2007). History of ANZASW: The New Zealand Association of Social Workers: Origins and early years. Retrieved February 26, 2016, from National Institute for Mental Health. (2005). NIMHE Guiding Statement on Recovery. Retrieved April 5, 2016, from New Zealand Parliament. (2009). New Zealand Health System Reforms. Retrieved February 18, 2016, from O Hagan, M. (2004). Recovery in New Zealand: lessons for Australia?. Australian e-journal for the Advancement of Mental Health, 3, 1-3. O'Brien, M. (2008). Poverty, policy and the state: The changing face of social security Bristol, England: The Policy Press. O'Hagan, M., Reynolds, P., & Smith, C. (2012). Recovery in New Zealand: An evolving concept?. International Review of Psychiatry, 24(February 1), Oliver, W. (1977). Origin and growth of the welfare state. In A. D. Trilin (Ed.), Social welfare and New Zealand society Wellington Methuen. ~ 94 ~
227 Volume 20, Number 2 July 2016 December 2016 Palley, T. I. (2004). From Keynesianism to Neoliberalism: Shifting Paradigms in Economics Retrieved May 4, 2016, from Petersen, K. S., Friis, V. S., Haxholm, B. L., Nielsen, C. V., & Wind, G. (2015 ). Recovery from Mental Illness: A Service User Perspective on Facilitators and Barriers. Community Ment Health Journal, 5, doi: /s Rickwood, D. (2004). Recovery in Australia: slowly but surely. Australian e-journal for the Advancement of Mental Health, 3(1), 1-3. Roper, B. (2005). Prosperity for all? Economic, social and political change in New Zealand since 1935 Melbourne, Australia: Thomson. Schrank, B., & Slade, M. (2007). Recovery in psychiatry. Psychiatric Bulletin, 31, Slade, M., Amering, M., Farkas, M., Hamilton, B., O'Hagan, M., Panther, G.,... Whitley, R. (2014). Uses and abuses of recovery: implementing recovery-oriented practices in mental health systems. World Psychiatry, 13, St John, S., & Rankin, K. (2002). Entrenching the welfare mess (Vol. Series 24): Department of Economics: Policy Discussion Paper Wynne, A. (2004). Public Sector Accounting Democratic Accountability or Market Rules?. Public Money & Management, 24(1), 5-7. doi: /j x ~ 95 ~
228 Volume 20, Number 2 July 2016 December 2016 Psycho-emotional characteristics that facilitate smoking cessation Renata M. David 1Laboratory of Studies of Mucus-Secreting Apparatus (LEAMS) Master's Degree Program in Physiotherapy Department of Physiotherapy Faculty of Science and Technology / São Paulo State University - FCT / UNESP Rua Roberto Simonsen, nº 305. Presidente Prudente, São Paulo, Brasil CEP renatamdavid@hotmail.com Dionei Ramos 2Professor of Physiotherapy course and post-graduation in Physiotherapy Faculty of Science and Technology / São Paulo State University - FCT / UNESP Rua Roberto Simonsen, nº 305. Presidente Prudente, São Paulo, Brasil CEP dionei-ramos@bol.com.br Ana Paula C. F. Freire 1Laboratory of Studies of Mucus-Secreting Apparatus (LEAMS) Master's Degree Program in Physiotherapy Department of Physiotherapy Faculty of Science and Technology / São Paulo State University - FCT / UNESP Rua Roberto Simonsen, nº 305. Presidente Prudente, São Paulo, Brasil CEP anapcff@hotmail.com Ana Luiza P. Batista 3Department of Psychology Faculty of Science and Technology / São Paulo State University - FCT / UNESP Rua Roberto Simonsen, nº 305. Presidente Prudente, São Paulo, Brasil CEP analuizab@uol.com.br Ercy M. C. Ramos 2Professor of Physiotherapy course and post-graduation in Physiotherapy Faculty of Science and Technology / São Paulo State University - FCT / UNESP Rua Roberto Simonsen, nº 305. Presidente Prudente, São Paulo, Brasil CEP ercy@bol.com.br Citation: David RM, Ramos D, Freire ACPF, Batista ALP & Ramos EMV. (2016) Psycho-emotional characteristics that facilitate smoking cessation. The International Journal of Psychosocial Rehabilitation. Vol 20 (2) ~ 96 ~
229 Volume 20, Number 2 July 2016 December 2016 Corresponding Author: Renata Marques David Rua Roberto Simonsen, nº 305. CEP Presidente Prudente, São Paulo, Brasil. renatamdavid@hotmail.com Abstract Objectives: To investigate and clarify which psycho-emotional factors are related to success in smoking cessation. Results: Of the 65 individuals who participated in the study, 36 were successful in smoking cessation. There was an association between the level of addiction to nicotine and an unsuccessful outcome in smoking cessation (p = 0.009). It was also observed that failure in smoking cessation was associated with both the presence of depressive episodes (p = 0.037) but also of severe psycho-emotional disorders (p <.001). In the binary logistic regression analysis for the psycho-emotional disorders and relapse chances in Group Success there was no statistical significance (p> 0.05) in all the variables studied. Conclusion: Among the factors related to failure in smoking cessation, the presence of severe psycho-emotional and current untreated alcoholism should be highlighted. The factors related to successful cessation were the absence of alcoholism and lower levels of dependence on nicotine. Key-words: Smoking, Affective Disorders Psychotic, Smoking Cessation, Health Public. Introduction: It is known that smoking is a worldwide public health problem and the leading cause of preventable death in the world as a result of tobacco-related diseases. 1 Therefore, various measures to combat smoking are being carried out in order to promote the prevention and treatment of this disease, defined by the World Health Organization as "a mental and behavioral disorder due to nicotine dependency syndrome", which is included in the International Classification of Diseases (ICD) in the section for mental and behavioral disorders due to psychoactive substance use (ICD- F.17). 2 In Brazil, anti-smoking actions are intense, with regulatory policies, 3,4 socio-educational campaigns 5,6 and smoking cessation programs. 7,8 Among these interventions, the latter have been developed in most health care centers, however, there is still no consensus on the success rate in smoking cessation due to the methodological diversity adopted by cessation programs. Freire et al., 9 presented a model of a smoking cessation program which demonstrated high success rates when compared to those found in the literature, 7,8,10-13 with the implementation of new procedures such as: intensification of the frequency of meetings (from once to twice a week), including a specific date of termination of tobacco and participation of former smokers in the treatment. It is worth noting that one of the factors that interferes with successful smoking cessation is nicotine abstinence syndrome, which is characterized by the manifestation of a set of symptoms such as: bradycardia, gastrointestinal discomfort, increased appetite, weight gain, anxiety, dysphoria, depression, insomnia, irritability, nervousness, fatigue and difficulty concentrating. 14,15 On the one hand, such symptoms frequently lead to smoking and on the other hand, the great difficulty in dealing with these symptoms increases the likelihood of relapse, particularly during the critical period of abstinence (less than six months of cessation) since the intensity and frequency of symptoms varies from individual to individual. 16 In addition, other factors that can also influence non-adherence to anti-smoking treatment and smoking cessation are high levels of anxiety and depression, living with other smokers, a high degree of nicotine dependence and low motivation to participate in anti-smoking therapies. 17,18 There is a clear association between smoking and psycho-emotional disorders such as depression, anxiety, at- ~ 97 ~
230 Volume 20, Number 2 July 2016 December 2016 tention deficit, panic syndrome and psychiatric disorders, 18 however; it is not yet well established in the literature which psycho-emotional characteristics are determinant in success in smoking cessation and continued abstinence. The psycho-emotional disorders are related to mood swings, behavioral changes and emotional instability, however, during tobacco abstinence these factors are intensified, such as depression, the individual present no interest in the outside world, there is the feeling of intense sadness and long-lasting, which undermines the social, emotional and especially professional life and these negative influences make it difficult to achieve success in smoking cessation. 19 According to the study Zvolensky et al. (2015), 20 former smokers with a history of depression, are likely to have relapse to smoking even after 10 years of abstinence compared to former smokers with no history of the disorder. Moreover, the chances of relapse to smoking further increase over time in cases withdrawal of current depression and / or applicant and such relapse is associated with symptoms such intensity. 21 Given the above, this study aimed to investigate and clarify which psycho-emotional factors are related to success in smoking cessation. Methods Study design and sample selection This was a prospective, descriptive study conducted at the Faculty of Science and Technology - FCT / UNESP of Presidente Prudente/SP, to understand how some participants in a smoking cessation program even with some personal characteristics that initially suggest the failure in the smoking cessation process managed to get the success, ie, they managed to remain for at least six months without smoking. The study was approved by the Research Ethics Committee of this institution under protocol no. 245/2008. The study sample consisted of 65 participants of both sexes, female predominance (68%) divided into two groups: Relapse group (n = 29), characterized by those who did not stop smoking and the Success group (n = 36) characterized by successful smoking cessation for at least six months. We included in the study individuals of both sexes, aged between 35 and 65, that participated of at least three meetings before the date of smoking cessation proposed by the health care team and who remained abstinent for at least six months. We excluded individuals who abandoned the program. PROCAT uses an intensive approach with cognitive behavioral therapy (CBT) associated with drug therapies and nicotine replacement. The therapy is performed in groups through structured sessions which take place twice a week, each session lasting 60 minutes. The first five sessions consist of socio-educational classes, after which begins the so-called "Stopping Day" (pre-established date for cessation) that occurs after the presentation and discussion of all educational classes on the themes proposed by National Cancer Institute - INCA. Individual reports in group meetings begin from the sixth therapy session. 9 For monitoring the withdrawal situation of each individual, an abstinence control sheet was completed which included the presence or absence of relapses, at all meetings after the proposed date of cessation. During the PROCAT admission phase, all participants underwent an initial evaluation, at which information was collected on personal data, anthropometric measurements (weight and height) and smoking history (number of cigarettes smoked per day; duration of smoking in years), education level and socioeconomic classification according to the Brazilian Association of Research Companies ABEP The motivational stage for change in behavior according to the Prochaska and DiClemente stages 23 was also evaluated, adapted for the Brazilian population. 24 In addition, the degree of dependence on nicotine was evaluated through the Fagerström Test, which consists of a scale of six items and scoring from 0 to 10. The classification of nicotine dependence encompasses five levels: very low (0-2 points); low (3-4 points); moderate (5 points); high (6-7 points); and very high (8-10 points). 25 Individuals who present a score of over 6 points are more likely to have greater diffi- ~ 98 ~
231 Volume 20, Number 2 July 2016 December 2016 culty in stopping smoking due to abstinence syndrome. 26 Subsequently, a psychological assessment was performed in order to verify the psych-emotional state of the participants who would be subjected to the withdrawal process and investigate possible psycho-emotional disorders that could influence this process. It should be emphasized that the identification of psycho-emotional disorders was conducted through self reporting by the participants, and some presented the prescription drugs that they frequently used. This evaluation followed the schematic plan presented below (Figure 1). Figure 1 A psycho-emotional disorder was considered as something which provoked significant changes in the psychological and emotional area of the individual, reflected in individual behavior in social life, in the context of work or family. After the psychological evaluation, the following psycho-emotional disorders were identified: alcoholism, anxiety, depressive episodes, severe disorders (characterized by: panic disorder, bipolar disorder ~ 99 ~
232 Volume 20, Number 2 July 2016 December 2016 and deep/recurrent depression), critical moment of life (characterized by situations of emotional instability for the following reasons: loss of loved-ones, financial problems, marital crisis/separation and family conflict). In severe disorders and critical life categorie when the individuals were classified if they had at least one of the subclasses. If the individual present more than one category of psycho-emotional disorders, it was considered for classification only the category of most serious disorder. Statistical Analysis Data were analyzed using the statistical software Statistical Package for Social Sciences (SPSS), version Data normality was assumed or rejected by the Shapiro-Wilk test. Numerical variables were expressed as mean and standard deviation, and categorical variables were described in absolute and percentage values. For comparison between groups the independent t test was used for parametric data and the Mann-Whitney test for nonparametric data. The chi-square test was used to analyze categorical data. Was used Spearman correlation test to check the relationship between variables. In addition we performed a regression test Binary Logistic to check the chances of relapse according to the classification of psycho-emotional disorders. Adopted the statistical significance level of p <0.05. Results The sample was predominantly female in both groups (83% in the Relapse group and 56% in Success group) and presented homogeneity as there were no statistical differences in relation to demographic or smoking-related data. (Table 1). Table 1. Profile of the studied sample. Data expressed as mean and standard deviation. Characteristics Relapse Group (n=29) Success Group (n=36) p-value M/F 5/24 16/ Age (years) ± ± Weight (kg) 66.41± ± Height (m) 1.60± ± BMI (kg/m²) 25.82± ± Cig/Day (unit) 21.63± ± Pack-years 31.16± ± Fagerström 6.07± ± Legend: M/F = male / female; BMI = body mass index; kg/m² = kilograms per meter squared; Cig/Day (units) = cigarette units consumed per day; pack-years = ratio of time and smoking load; Fagerström: average nicotine dependence. *Difference significant= p<0.05. In this study it was observed that the majority of individuals from both groups were in the contemplation stage, i.e., they were aware that smoking was a problem and seriously planned to change their behavior (Table 2). In addition, Table 2 presents the association between the nicotine addiction level and failure in smoking cessation (p = 0.009), as the majority of members of the group of smokers who failed to quit smoking presented higher nicotine dependence (very high level) when compared with the group that stopped smoking. It was further not- ~ 100 ~
233 Volume 20, Number 2 July 2016 December 2016 ed that there was a marginal difference (p = 0.054) between the groups in relation to socioeconomic classification. Additionally, there was a negative correlation between success in smoking cessation and socio-economic level (r = ; p = 0.002), which suggested that the higher the socioeconomic status of the individual the smaller the chance of succeeding in smoking cessation. Table 2. Descriptive analysis of the sample with respect to the Prochaska and DiClemente stage, Fagerström, Educational level and Socio-Economic Class Characteristics Relapse Group (n=29) N (%) Success Group (n=36) N (%) p-value (χ²) Prochaska and Di- Clemente stage Pre-contemplation 6(20.7) 9 (25.0) Contemplation 23 (79.3) 27 (75.0) Preparation 0 (0) 0 (0) Action 0 (0) 0 (0) Maintenance 0 (0) 0 (0) Fagerström 0.009* Very low 2 (6.9) 2 (5.6) Low 6 (20.7) 8 (22.2) Average 3 (10.3) 3 (8.3) High 8 (27.6) 22 (61.1) Very high 10 (34.5) 1 (2.8) Educational Level Higher education Complete College Complete/ Higher education Incomplete Secondary Complete/ College Incomplete Primary Complete/ Secondary Incomplete 6 (20.7) 8 (22.2) 12 (41.4) 12 (33.3) 3 (10.3) 3 (8.3) 6 (20.7) 11 (30.6) Illiterate/ Primary 2 (6.9) 2 (5.6) ~ 101 ~
234 Volume 20, Number 2 July 2016 December 2016 Incomplete Socioeconomic a Class A1 0 (0) 0 (0) Class A2 1 (3.45) 1 (2.8) Class B1 2 (6.9) 8 (22.2) Class B2 6 (20.7) 15 (41.7) Class C1 10 (34.5) 9 (25.0) Class C2 9 (31.0) 3 (8.3) Class D and E 1 (3.45) 0 (0) Legend: a = Socioeconomic classification according to the Brazilian Association of Research Companies - ABEP Data presented in absolute values (n) and percentage of occurrence (%) χ²= Chi-square test. *Difference significant= p<0.05. Table 3 demonstrates that failure in smoking cessation was associated with both the presence of depressive episodes (p = 0.037) and the presence of severe psycho-emotional disorders such as: Panic Disorder, Bipolar Disorder and Deep/Recurrent Depression (p <.001). In addition, it was noted that although not statistically significant, there was a marginal difference between the groups in relation to treatment for alcoholism, which allowed us to assume that alcoholism, when treated, greatly increases the chances of success in smoking cessation. Figure 2 is a graphical representation of the prevalence of psycho-emotional disorders according to the relapse and success groups. Among the individuals who demonstrated some kind of psycho-emotional disorder, 13 were attending psychological and/or psychiatric counseling, representing 28% in the relapse group and 14% in the success group. Table 3. Association between the psycho-emotional characteristics and success in smoking cessation according to the group: Relapse Group (RG) and Success Group (SG). Psycho-emotional Characteristics RG (n= 29) N (%) SG (n=36) N (%) p-value Presence/Absence 24/5 26/ Treatment for alcoholism 0 (0) 4 (11.1) Not treated for alcoholism 2 (6.7) 0 (0) Anxiety 6 (20.7) 6 (16.7) Depressive Episodes 0 (0) 5 (13.9) 0.037* Serious Disorders 11 (37.9) 0 (0) 0.000* Critical Life Moments 5 (17.2) 11 (30.5) ~ 102 ~
235 Volume 20, Number 2 July 2016 December 2016 Legend: Serious disorders= Panic Disorder, Bipolar Disorder and Deep and/or Recurrent Depressio; Critical Life Moments = characterized by situations of mourning, financial problems, marital crisis/separation, family conflict. Data presented in absolute values (n) and percentage of occurrence (%). Chi-square test. * *Difference significant= p<0.05. Figure 2 Logistic regression analysis (Table 4) shows that the psycho-emotional disorders except treated alcoholism, adversely impacted the chances of success Group to remain abstinent, because untreated alcoholism, depressive episodes and serious disorders have 100% relapse chance. Already treated alcoholism, anxiety and critical life time have 29%, 41% and 50% chance of relapse respectively. However, for all variables there was no statistical significance (p> 0.05). ~ 103 ~
 with 37.9% and anxiety with 20.7%.")
236 Volume 20, Number 2 July 2016 December 2016 Discussion In the present study it was found that the psycho-emotional characteristics with higher prevalence in the relapse group were serious disorders (Panic Disorder, Bipolar Disorder and Deep/Recurrent Depression) with 37.9% and anxiety with 20.7%. What is interesting is that these serious disorders, even when being monitored, are directly associated with failure in smoking cessation, however, this could be justified by the exacerbation of psycho-emotional symptoms during the period of abstinence, which greatly increases the risk of relapses during treatment. 27 In addition, high levels of nicotine dependence are significantly associated with level of depression and low rates of success 11,28 this corroborates the findings of the present study, which also found an association between high levels of nicotine dependence and failure in smoking cessation. Considering that the sample was predominantly female, this prevalence may be related to gender. According to Silva et al. (2012), 29 female smokers; present more intense and frequent depressive disorders than male smokers; have more difficulty enduring and controlling the symptoms of withdrawal syndrome according to the phase of the menstrual cycle; and receive less cessation support than men, which makes them more susceptible to relapses. Male smokers more commonly present the symptom of anxiety than depression. 30 Although anxiety did not present statistical significance in the present study, it can be considered one of the complicating factors in the cessation process, since the relationship between smoking and anxiety is a kind of vicious circle, on the one hand there are patients who smoke to alleviate the feeling of anxiety and on the other hand, there are those that compulsively smoke because they are very anxious. 17,31 It is important to point out that the difference between healthy and pathological anxiety is very subtle. However, anxiety becomes ~ 104 ~
Trauma-Informed Approaches. The Nelson Trust women s residential treatment service
 Trauma-Informed Approaches The Nelson Trust women s residential treatment service The Nelson Trust The Nelson Trust is a Gloucestershire based charity. We were established in 1985 to provide residential
Trauma-Informed Approaches The Nelson Trust women s residential treatment service The Nelson Trust The Nelson Trust is a Gloucestershire based charity. We were established in 1985 to provide residential
Practitioner Guidelines for Enhanced IMR for COD Handout #10: Getting Your Needs Met in the Mental Health System
 Chapter X Practitioner Guidelines for Enhanced IMR for COD Handout #10: Getting Your Needs Met in the Mental Health System Introduction This module provides an overview of the mental health system, including
Chapter X Practitioner Guidelines for Enhanced IMR for COD Handout #10: Getting Your Needs Met in the Mental Health System Introduction This module provides an overview of the mental health system, including
Practitioner Guidelines for Enhanced IMR for COD Handout #2: Practical Facts About Mental Illness
 Chapter II Practitioner Guidelines for Enhanced IMR for COD Handout #2: Practical Facts About Mental Illness There are four handouts to choose from, depending on the client and his or her diagnosis: 2A:
Chapter II Practitioner Guidelines for Enhanced IMR for COD Handout #2: Practical Facts About Mental Illness There are four handouts to choose from, depending on the client and his or her diagnosis: 2A:
TOUGH TALK HOW TO HAVE THE DIFFICULT CONVERSATION ABOUT HOARDING
 TOUGH TALK HOW TO HAVE THE DIFFICULT CONVERSATION ABOUT HOARDING Denise Burningham and Leslie Shapiro HOARDING DISORDER: THE BASICS Hallmarks of HD Difficulty Discarding Clutter Distress Excessive Acquisition
TOUGH TALK HOW TO HAVE THE DIFFICULT CONVERSATION ABOUT HOARDING Denise Burningham and Leslie Shapiro HOARDING DISORDER: THE BASICS Hallmarks of HD Difficulty Discarding Clutter Distress Excessive Acquisition
1) What kind of home do you live in? Who else lives there with you?
 What kind of home do you live in? Who else lives there with you?") Hoarding Interview Client initials: Date: 1) What kind of home do you live in? Who else lives there with you? 2) Let s talk about the rooms in your home. [Use the Clutter Image Rating pictures to determine
Hoarding Interview Client initials: Date: 1) What kind of home do you live in? Who else lives there with you? 2) Let s talk about the rooms in your home. [Use the Clutter Image Rating pictures to determine
CAMHS. Your guide to Child and Adolescent Mental Health Services
 CAMHS Your guide to Child and Adolescent Mental Health Services The support I received from CAHMS was invaluable and I do not know where I would be now without it. I now study Health and Social Care and
CAMHS Your guide to Child and Adolescent Mental Health Services The support I received from CAHMS was invaluable and I do not know where I would be now without it. I now study Health and Social Care and
Not sure if a talking therapy is for you?
 South Tyneside NHS Foundation Trust Primary Care Mental Health Service Not sure if a talking therapy is for you? Take a look at the different types of therapy we have available to find out more about them.
South Tyneside NHS Foundation Trust Primary Care Mental Health Service Not sure if a talking therapy is for you? Take a look at the different types of therapy we have available to find out more about them.
Peer Support. Introduction. What is Peer Support?
 Peer Support Introduction We are all social beings by nature connectedness and community are necessary if not vital to our wellbeing. The very existence of positive social relationships can be a source
Peer Support Introduction We are all social beings by nature connectedness and community are necessary if not vital to our wellbeing. The very existence of positive social relationships can be a source
Centre for Specialist Psychological Treatments of Anxiety and Related Problems
 Centre for Specialist Psychological Treatments of Anxiety and Related Problems Information for people interested in accessing treatment at the Centre and those who already have a referral Welcome Welcome
Centre for Specialist Psychological Treatments of Anxiety and Related Problems Information for people interested in accessing treatment at the Centre and those who already have a referral Welcome Welcome
Workforce Analysis: Children and Young People s Mental Health and Wellbeing Wider system
 Workforce Analysis: Children and Young People s Mental Health and Wellbeing Wider system This questionnaire is aimed at any member of the workforce supporting the mental health and wellbeing for children
Workforce Analysis: Children and Young People s Mental Health and Wellbeing Wider system This questionnaire is aimed at any member of the workforce supporting the mental health and wellbeing for children
Cluster 1 Common Mental Health Problems (mild)
") Cluster 1 Common Mental Health Problems (mild) You have recently sought help for the first time. You have experienced depression and/or anxiety. This may cause distraction or minor disruption to you as
Cluster 1 Common Mental Health Problems (mild) You have recently sought help for the first time. You have experienced depression and/or anxiety. This may cause distraction or minor disruption to you as
Healthy Parent Carers Project - Meeting 6. 06/05/2015 South Cloisters
 Healthy Parent Carers Project - Meeting 6 06/05/2015 South Cloisters Family Faculty: Annette, Ursula, Mary, Mirtha, Ruth, Jen, Julia, Lynn, Kirsty, John, Tricia, Maureen, Maria, Harriet; PenCRU: Chris,
Healthy Parent Carers Project - Meeting 6 06/05/2015 South Cloisters Family Faculty: Annette, Ursula, Mary, Mirtha, Ruth, Jen, Julia, Lynn, Kirsty, John, Tricia, Maureen, Maria, Harriet; PenCRU: Chris,
Improving Access to Psychological Therapies. Guidance for faith and community groups
 Improving Access to Psychological Therapies Guidance for faith and community groups 1 The aims of this resource This document aims to improve faith communities understanding of the professional treatments
Improving Access to Psychological Therapies Guidance for faith and community groups 1 The aims of this resource This document aims to improve faith communities understanding of the professional treatments
Emotional Health and ADHD
 Emotional Health and ADHD Dr Jo Steer, Chartered Clinical Psychologist & Head of the Emotional Health Service (EHS) & Dr Amrita Basu, Chartered Counselling Psychologist & Clinical Specialist Objectives
Emotional Health and ADHD Dr Jo Steer, Chartered Clinical Psychologist & Head of the Emotional Health Service (EHS) & Dr Amrita Basu, Chartered Counselling Psychologist & Clinical Specialist Objectives
Hoarding Behavior in Elders
 Hoarding Behavior in Elders Presented by: Emily B. Saltz, LICSW Elder Resources www.eldres.com NAPGCM Webinar January 11, 2012 Definition of Hoarding* 1) The acquisition of, and failure to discard a large
Hoarding Behavior in Elders Presented by: Emily B. Saltz, LICSW Elder Resources www.eldres.com NAPGCM Webinar January 11, 2012 Definition of Hoarding* 1) The acquisition of, and failure to discard a large
Assessment and management of selfharm
 Assessment and management of selfharm procedure Version: 1.1 Consultation Approved by: Medical Director, CAMHS Director, Director of Quality, Patient Experience and Adult services Medical Director Date
Assessment and management of selfharm procedure Version: 1.1 Consultation Approved by: Medical Director, CAMHS Director, Director of Quality, Patient Experience and Adult services Medical Director Date
Private Young People s Services
 www.priorygroup.com Private Young People s Services Understanding mental health in young people Supporting young people Priory Group is the leading provider of mental health and behavioural care services
www.priorygroup.com Private Young People s Services Understanding mental health in young people Supporting young people Priory Group is the leading provider of mental health and behavioural care services
Dialectical Behaviour Therapy in Secure Services Calverton Hill & Priory Hospital East Midlands Priory Group
 Context Our Dialectical Behaviour Therapy (DBT) team is a large multi-site team offering a standard DBT programme to patients who present with complex, severe, and enduring mental illness, personality
Context Our Dialectical Behaviour Therapy (DBT) team is a large multi-site team offering a standard DBT programme to patients who present with complex, severe, and enduring mental illness, personality
Engaging individuals in dealing with their hoarding
 Engaging individuals in dealing with their hoarding generic ppt slide Satwant Singh Nurse Consultant in CBT & MH Newham, London, UK copyright Satwant Singh MHASF Nov 2014 1 Aims for today To understand
Engaging individuals in dealing with their hoarding generic ppt slide Satwant Singh Nurse Consultant in CBT & MH Newham, London, UK copyright Satwant Singh MHASF Nov 2014 1 Aims for today To understand
CASY Counselling Services for Schools
 CASY Counselling Services for Schools Registered Charity Number 1092938 A Company Limited by Guarantee in England and Wales. Registered number 4310724 16 London Rd, Newark, Nottinghamshire NG24 1TW T:
CASY Counselling Services for Schools Registered Charity Number 1092938 A Company Limited by Guarantee in England and Wales. Registered number 4310724 16 London Rd, Newark, Nottinghamshire NG24 1TW T:
section 6: transitioning away from mental illness
 section 6: transitioning away from mental illness Throughout this resource, we have emphasized the importance of a recovery perspective. One of the main achievements of the recovery model is its emphasis
section 6: transitioning away from mental illness Throughout this resource, we have emphasized the importance of a recovery perspective. One of the main achievements of the recovery model is its emphasis
BASIC VOLUME. Elements of Drug Dependence Treatment
 BASIC VOLUME Elements of Drug Dependence Treatment BASIC VOLUME MODULE 1 Drug dependence concept and principles of drug treatment MODULE 2 Motivating clients for treatment and addressing resistance MODULE
BASIC VOLUME Elements of Drug Dependence Treatment BASIC VOLUME MODULE 1 Drug dependence concept and principles of drug treatment MODULE 2 Motivating clients for treatment and addressing resistance MODULE
SECOND AUSTRALIAN CHILD AND ADOLESCENT SURVEY OF MENTAL HEALTH AND WELLBEING HIGHLIGHTS
 The Mental Health of Children and Adolescents 3 SECOND AUSTRALIAN CHILD AND ADOLESCENT SURVEY OF MENTAL HEALTH AND WELLBEING HIGHLIGHTS A second national survey of the mental health and wellbeing of Australian
The Mental Health of Children and Adolescents 3 SECOND AUSTRALIAN CHILD AND ADOLESCENT SURVEY OF MENTAL HEALTH AND WELLBEING HIGHLIGHTS A second national survey of the mental health and wellbeing of Australian
Kaiser Telecare Program for Intensive Community Support Intensive Case Management Exclusively for Members within a Managed Care System
 Kaiser Telecare Program for Intensive Community Support Intensive Case Management Exclusively for Members within a Managed Care System 12-Month Customer Report, January to December, 2007 We exist to help
Kaiser Telecare Program for Intensive Community Support Intensive Case Management Exclusively for Members within a Managed Care System 12-Month Customer Report, January to December, 2007 We exist to help
Rosebank House A supported step towards independence
 A supported step towards independence 2 Our service at a glance Rosebank House in Caversham near Reading is an independent hospital providing recoveryfocused 24-hour care and support for men and women
A supported step towards independence 2 Our service at a glance Rosebank House in Caversham near Reading is an independent hospital providing recoveryfocused 24-hour care and support for men and women
WHAT CAN I DO TO HELP MYSELF WITH ANXIETY?
 WHAT CAN I DO TO HELP MYSELF WITH ANXIETY? Self help strategies for mild anxiety latrobe.edu.au WHAT CAN I DO TO HELP MYSELF WITH ANXIETY? This guide offers some effective self-help strategies that you
WHAT CAN I DO TO HELP MYSELF WITH ANXIETY? Self help strategies for mild anxiety latrobe.edu.au WHAT CAN I DO TO HELP MYSELF WITH ANXIETY? This guide offers some effective self-help strategies that you
Priory Hospital Glasgow
 www.priorygroup.com GLASGOW Priory Hospital Glasgow Addiction Treatment Programme Take the first step to recovery A real and lasting difference for everyone we support We believe that anyone who is struggling
www.priorygroup.com GLASGOW Priory Hospital Glasgow Addiction Treatment Programme Take the first step to recovery A real and lasting difference for everyone we support We believe that anyone who is struggling
The science of the mind: investigating mental health Treating addiction
 The science of the mind: investigating mental health Treating addiction : is a Consultant Addiction Psychiatrist. She works in a drug and alcohol clinic which treats clients from an area of London with
The science of the mind: investigating mental health Treating addiction : is a Consultant Addiction Psychiatrist. She works in a drug and alcohol clinic which treats clients from an area of London with
The Great Gatsby J. Gatsby
 Case Study in Therapeutic Recreation for The Great Gatsby J. Gatsby Introduction and Global Assessment/Social History: I diagnosed J. Gatsby from the movie The Great Gatsby. Using the Global Assessment
Case Study in Therapeutic Recreation for The Great Gatsby J. Gatsby Introduction and Global Assessment/Social History: I diagnosed J. Gatsby from the movie The Great Gatsby. Using the Global Assessment
Online Resources, Community Resources and You
 Online Resources, Community Resources and You If your child is in distress or having difficulties there s a lot that you can learn that might prove of help to him or her. Where might you do this learning?
Online Resources, Community Resources and You If your child is in distress or having difficulties there s a lot that you can learn that might prove of help to him or her. Where might you do this learning?
Taking Care of Yourself and Your Family After Self-Harm or Suicidal Thoughts A Family Guide
 It is devastating to have a suicidal family member and to live with the feelings that go with this kind of traumatic anxiety. That is why this guide is developed for you. It will give you some important
It is devastating to have a suicidal family member and to live with the feelings that go with this kind of traumatic anxiety. That is why this guide is developed for you. It will give you some important
How to Choose a Counsellor
 How to Choose a Counsellor Many survivors of sexual assault, sexual abuse, or other forms of violence find counselling to be a helpful part of their recovery process. Counselling can accelerate the relief
How to Choose a Counsellor Many survivors of sexual assault, sexual abuse, or other forms of violence find counselling to be a helpful part of their recovery process. Counselling can accelerate the relief
Healing Trauma Evaluation Year 1 Findings
 2551 Galena Avenue #1774 Simi Valley, CA 93065 310-801-8996 Envisioning Justice Solutions, Inc. Determining the Programs, Policies, and Services Needed to Rebuild the Lives of Criminal Justice Involved
2551 Galena Avenue #1774 Simi Valley, CA 93065 310-801-8996 Envisioning Justice Solutions, Inc. Determining the Programs, Policies, and Services Needed to Rebuild the Lives of Criminal Justice Involved
HOARDING: The Problem Behind Closed Doors. Thursday, June 7, th Annual Supportive Housing Network of NY Conference. Rebuilding Lives Together
 HOARDING: The Problem Behind Closed Doors Thursday, June 7, 2012 12 th Annual Supportive Housing Network of NY Conference June 18, 2012 Rebuilding Lives Together OUR DISTINGUISHED PANELIST Moderator: Michael
HOARDING: The Problem Behind Closed Doors Thursday, June 7, 2012 12 th Annual Supportive Housing Network of NY Conference June 18, 2012 Rebuilding Lives Together OUR DISTINGUISHED PANELIST Moderator: Michael
Post-Traumatic Stress Disorder
 Post-Traumatic Stress Disorder Teena Jain 2017 Post-Traumatic Stress Disorder What is post-traumatic stress disorder, or PTSD? PTSD is a disorder that some people develop after experiencing a shocking,
Post-Traumatic Stress Disorder Teena Jain 2017 Post-Traumatic Stress Disorder What is post-traumatic stress disorder, or PTSD? PTSD is a disorder that some people develop after experiencing a shocking,
IDDT Fidelity Action Planning Guidelines
 1a. Multidisciplinary Team IDDT Fidelity Action Planning Guidelines Definition: All clients targeted for IDDT receive care from a multidisciplinary team. A multi-disciplinary team consists of, in addition
1a. Multidisciplinary Team IDDT Fidelity Action Planning Guidelines Definition: All clients targeted for IDDT receive care from a multidisciplinary team. A multi-disciplinary team consists of, in addition
What? Who? Why? Where? When? College Statement: Restricted Activity of Psychosocial Intervention
 College Statement: Restricted Activity of Psychosocial Intervention What? Who? Why? Where? When? Registered Dietitians no longer require authorization from the College to work with clients/patients with
College Statement: Restricted Activity of Psychosocial Intervention What? Who? Why? Where? When? Registered Dietitians no longer require authorization from the College to work with clients/patients with
The Role of the Psychologist in an Early Intervention in Psychosis Team Dr Janice Harper, Consultant Clinical Psychologist Esteem, Glasgow, UK.
 The Role of the Psychologist in an Early Intervention in Psychosis Team Dr Janice Harper, Consultant Clinical Psychologist Esteem, Glasgow, UK. Ferrara, Italy, 5 th May 2017 Overview Essential Components
The Role of the Psychologist in an Early Intervention in Psychosis Team Dr Janice Harper, Consultant Clinical Psychologist Esteem, Glasgow, UK. Ferrara, Italy, 5 th May 2017 Overview Essential Components
a guide to cognitivebehavioural (cbt)
") a guide to cognitivebehavioural therapy (cbt) Cognitive-behavioural aims to help you to change the way that you think, feel and behave. It is used as a treatment for various mental health and physical
a guide to cognitivebehavioural therapy (cbt) Cognitive-behavioural aims to help you to change the way that you think, feel and behave. It is used as a treatment for various mental health and physical
Core Competencies for Peer Workers in Behavioral Health Services
 BRINGING RECOVERY SUPPORTS TO SCALE Technical Assistance Center Strategy (BRSS TACS) Core Competencies for Peer Workers in Behavioral Health Services OVERVIEW In 2015, SAMHSA led an effort to identify
BRINGING RECOVERY SUPPORTS TO SCALE Technical Assistance Center Strategy (BRSS TACS) Core Competencies for Peer Workers in Behavioral Health Services OVERVIEW In 2015, SAMHSA led an effort to identify
1996: Cognitive behavioral model paper
 Randy Frost, PhD April 26, 2012 14 th Annual Conference on Hoarding and Cluttering 1947: Collyer brothers 1947 1993: Virtually nothing 1993: First systematic study Frost & Gross (1993). The hoarding of
Randy Frost, PhD April 26, 2012 14 th Annual Conference on Hoarding and Cluttering 1947: Collyer brothers 1947 1993: Virtually nothing 1993: First systematic study Frost & Gross (1993). The hoarding of
NCFE Level 2 Certificate in Awareness of Mental Health Problems SAMPLE. Part A
 NCFE Level 2 Certificate in Awareness of Mental Health Problems Part A Certificate in Awareness of Mental Health Problems Welcome to this Level 2 Certificate in Awareness of Mental Health Problems. We
NCFE Level 2 Certificate in Awareness of Mental Health Problems Part A Certificate in Awareness of Mental Health Problems Welcome to this Level 2 Certificate in Awareness of Mental Health Problems. We
Focus of Today s Presentation. Partners in Healing Model. Partners in Healing: Background. Data Collection Tools. Research Design
 Exploring the Impact of Delivering Mental Health Services in NYC After-School Programs Gerald Landsberg, DSW, MPA Stephanie-Smith Waterman, MSW, MS Ana Maria Pinter, M.A. Focus of Today s Presentation
Exploring the Impact of Delivering Mental Health Services in NYC After-School Programs Gerald Landsberg, DSW, MPA Stephanie-Smith Waterman, MSW, MS Ana Maria Pinter, M.A. Focus of Today s Presentation
Case Study. Salus. May 2010
 Case Study Salus May 2010 Background Based within Coatbridge, Salus consists of one of the largest NHS based multidisciplinary teams in Scotland. Through its various services Salus Case Management Services
Case Study Salus May 2010 Background Based within Coatbridge, Salus consists of one of the largest NHS based multidisciplinary teams in Scotland. Through its various services Salus Case Management Services
Young People s Therapy Services
 Young People s Therapy Services A REAL AND LASTING DIFFERENCE FOR EVERYONE WE SUPPORT Supporting young people with their mental health The Priory Group is the leading provider of mental health and behavioural
Young People s Therapy Services A REAL AND LASTING DIFFERENCE FOR EVERYONE WE SUPPORT Supporting young people with their mental health The Priory Group is the leading provider of mental health and behavioural
6/23/2015. Disclosures. Overview. Learning Objectives
 Disclosures The speakers have no known or real conflicts of interest to declare 16th Annual Canadian Collaborative Mental Health care Conference June 18-20, 2015 Murli Soni, Bounce Back Program Manager
Disclosures The speakers have no known or real conflicts of interest to declare 16th Annual Canadian Collaborative Mental Health care Conference June 18-20, 2015 Murli Soni, Bounce Back Program Manager
Living well with and beyond cancer Information, support and practical advice to help you through treatment and beyond
 Living well with and beyond cancer Information, support and practical advice to help you through treatment and beyond Exceptional healthcare, personally delivered Introduction to this booklet Receiving
Living well with and beyond cancer Information, support and practical advice to help you through treatment and beyond Exceptional healthcare, personally delivered Introduction to this booklet Receiving
Recovery Oriented Prescribing Why take any medication?
 Recovery Oriented Prescribing Why take any medication? June 15, 2012 University of Wisconsin Department of Psychiatry Medical Director, Journey Mental Health Center of Dane County Consultant, Wisconsin
Recovery Oriented Prescribing Why take any medication? June 15, 2012 University of Wisconsin Department of Psychiatry Medical Director, Journey Mental Health Center of Dane County Consultant, Wisconsin
HERTFORDSHIRE PARTNERSHIP UNIVERSITY NHS FOUNDATION TRUST. Referral Criteria for Specialist Tier 3 CAMHS
 Referral Criteria for Specialist Tier 3 CAMHS Specialist CAMHS provides mental health support, advice and guidance and treatment for Children and Young People with moderate or severe mental health difficulties,
Referral Criteria for Specialist Tier 3 CAMHS Specialist CAMHS provides mental health support, advice and guidance and treatment for Children and Young People with moderate or severe mental health difficulties,
Choosing Life: empowerment, Action, Results! CLEAR Menu Sessions. Adherence 1: Understanding My Medications and Adherence
 Choosing Life: empowerment, Action, Results! CLEAR Menu Sessions Adherence 1: Understanding My Medications and Adherence This page intentionally left blank. Understanding My Medications and Adherence Session
Choosing Life: empowerment, Action, Results! CLEAR Menu Sessions Adherence 1: Understanding My Medications and Adherence This page intentionally left blank. Understanding My Medications and Adherence Session
9/10/2018. Hoarding Digging to the Bottom of the Problem. Hoarding Is Not A Messy Desk. Marilyn A Halpern MSW
 Hoarding Digging to the Bottom of the Problem Marilyn A Halpern MSW Professional Guardian Client/Patient Advocate Medical Social Worker End-of-Life Doula Marilyn Halpern, LSW Hoarding Is Not A Messy Desk
Hoarding Digging to the Bottom of the Problem Marilyn A Halpern MSW Professional Guardian Client/Patient Advocate Medical Social Worker End-of-Life Doula Marilyn Halpern, LSW Hoarding Is Not A Messy Desk
Doncaster Improving Access to Psychological Therapies (IAPT) Nurse Target September 2018 Dennis Convery
 Nurse Target September 2018 Dennis Convery") Doncaster Improving Access to Psychological Therapies (IAPT) Nurse Target September 2018 Dennis Convery Aims of the session To introduce the role and function of Doncaster IAPT (improving access to psychological
Doncaster Improving Access to Psychological Therapies (IAPT) Nurse Target September 2018 Dennis Convery Aims of the session To introduce the role and function of Doncaster IAPT (improving access to psychological
The acquisition of, and failure to discard, a large number of possessions that appear to be useless or of limited value. Living spaces sufficiently
 Sandra McMillan The acquisition of, and failure to discard, a large number of possessions that appear to be useless or of limited value. Living spaces sufficiently cluttered so as to preclude activities
Sandra McMillan The acquisition of, and failure to discard, a large number of possessions that appear to be useless or of limited value. Living spaces sufficiently cluttered so as to preclude activities
Assertive Community Treatment Team
 Assertive Community Treatment Team Badri Daneshamouz December, 2014 About CMHA Founded in 1918, CMHA is one of the oldest voluntary health organizations National office, provincial divisions, local branches
Assertive Community Treatment Team Badri Daneshamouz December, 2014 About CMHA Founded in 1918, CMHA is one of the oldest voluntary health organizations National office, provincial divisions, local branches
Targeted interventions for asylum seeking and refugee young carers and their families
 Practice example Targeted interventions for asylum seeking and refugee young carers and their families What is the initiative? CareFree Asylum Seeking, Refugee and Newly Arrived Young Carers Project Who
Practice example Targeted interventions for asylum seeking and refugee young carers and their families What is the initiative? CareFree Asylum Seeking, Refugee and Newly Arrived Young Carers Project Who
A new scale for the assessment of competences in Cognitive and Behavioural Therapy. Anthony D. Roth. University College London, UK
 A new scale for the assessment of competences in Cognitive and Behavioural Therapy Anthony D. Roth University College London, UK Abstract Background: Scales for assessing competence in CBT make an important
A new scale for the assessment of competences in Cognitive and Behavioural Therapy Anthony D. Roth University College London, UK Abstract Background: Scales for assessing competence in CBT make an important
A major feature of hoarding is the large amount of disorganized clutter that creates chaos in the home. Such as:
 Articles on Compulsive Hoarding # 1 OCD Foundation What is hoarding, and how does it differ from collecting? Two behaviors characterize hoarding: acquiring too many possessions and difficulty discarding
Articles on Compulsive Hoarding # 1 OCD Foundation What is hoarding, and how does it differ from collecting? Two behaviors characterize hoarding: acquiring too many possessions and difficulty discarding
ADHD clinic for adults Feedback on services for attention deficit hyperactivity disorder
 ADHD clinic for adults Feedback on services for attention deficit hyperactivity disorder Healthwatch Islington Healthwatch Islington is an independent organisation led by volunteers from the local community.
ADHD clinic for adults Feedback on services for attention deficit hyperactivity disorder Healthwatch Islington Healthwatch Islington is an independent organisation led by volunteers from the local community.
Caring for someone who has self-harmed or had suicidal thoughts. A family guide
 Caring for someone who has self-harmed or had suicidal thoughts A family guide This booklet is aimed at the families/carers of people who have self-harmed or had suicidal thoughts. It will be provided
Caring for someone who has self-harmed or had suicidal thoughts A family guide This booklet is aimed at the families/carers of people who have self-harmed or had suicidal thoughts. It will be provided
HELPING A PERSON WITH SCHIZOPHRENIA
 HELPING A PERSON WITH SCHIZOPHRENIA OVERCOMING CHALLENGES WHILE TAKING CARE OF YOURSELF The love and support of family plays an important role in schizophrenia treatment and recovery. If someone close
HELPING A PERSON WITH SCHIZOPHRENIA OVERCOMING CHALLENGES WHILE TAKING CARE OF YOURSELF The love and support of family plays an important role in schizophrenia treatment and recovery. If someone close
Interviewing, or MI. Bear in mind that this is an introductory training. As
 Motivational Interviewing Module 2 Slide Transcript Slide 1 In this module, you will be introduced to the basics of Motivational Interviewing, or MI. Bear in mind that this is an introductory training.
Motivational Interviewing Module 2 Slide Transcript Slide 1 In this module, you will be introduced to the basics of Motivational Interviewing, or MI. Bear in mind that this is an introductory training.
Basic Flow diagram of Life Coaching
 TUTOR TALK: Key Learning Points 1. Life Coaching is the combination of therapeutic techniques and training the client in new skills and knowledge. 2. You must not give direct advice unless qualified in
TUTOR TALK: Key Learning Points 1. Life Coaching is the combination of therapeutic techniques and training the client in new skills and knowledge. 2. You must not give direct advice unless qualified in
Understanding Hoarding
 Understanding Hoarding Dr. David Orr Self-Neglect and Hoarding Conference Ipswich, 6th November 2018 Hoarding: Why Now? 1. Policy Developments Included in recognised forms of abuse and neglect: Self-neglect
Understanding Hoarding Dr. David Orr Self-Neglect and Hoarding Conference Ipswich, 6th November 2018 Hoarding: Why Now? 1. Policy Developments Included in recognised forms of abuse and neglect: Self-neglect
The Priory Hospital Hayes Grove Addiction Treatment Programme
 The Priory Hospital Hayes Grove Addiction Treatment Programme Take the first step to recovery A REAL AND LASTING DIFFERENCE FOR EVERYONE WE SUPPORT We believe that anyone struggling with addictive behaviours
The Priory Hospital Hayes Grove Addiction Treatment Programme Take the first step to recovery A REAL AND LASTING DIFFERENCE FOR EVERYONE WE SUPPORT We believe that anyone struggling with addictive behaviours
Eating Disorder Support Services
 Eating Disorder Support Services Counselling Information Sheet Every year in the UK and globally, millions of people struggle with eating disorders. Furthermore, many of these sufferers and their families
Eating Disorder Support Services Counselling Information Sheet Every year in the UK and globally, millions of people struggle with eating disorders. Furthermore, many of these sufferers and their families
CSD Level 2 from $57,170 $62,811 pa (Pro Rata) Dependent on skills and experience
 Dependent on skills and experience") Position Description August 17 Position Description Peer Support Worker Section A: Position details Position title: Employment Status: Classification and Salary: Location: Hours: Peer Support Worker Part-Time
Position Description August 17 Position Description Peer Support Worker Section A: Position details Position title: Employment Status: Classification and Salary: Location: Hours: Peer Support Worker Part-Time
Let s Talk About Treatment
 What Doesn t Work Let s Talk About Treatment Lisa R. Terry, LPC What we ve tried Talk therapy- You can t talk you way out of a medical disorder Play Therapy Family Therapy Psychoanalysis While these are
What Doesn t Work Let s Talk About Treatment Lisa R. Terry, LPC What we ve tried Talk therapy- You can t talk you way out of a medical disorder Play Therapy Family Therapy Psychoanalysis While these are
Coach on Call. Please give me a call if you have more questions about this or other topics.
 Coach on Call It was great to talk with you. Thank you for your interest in. I hope you find this tip sheet helpful. Please give me a call if you have more questions about this or other topics. As your
Coach on Call It was great to talk with you. Thank you for your interest in. I hope you find this tip sheet helpful. Please give me a call if you have more questions about this or other topics. As your
COMMUNICATION- FOCUSED THERAPY (CFT) FOR OCD
 FOR OCD") COMMUNICATION- FOCUSED THERAPY (CFT) FOR OCD Dr., M.D. Communication-Focused Therapy (CFT) is a psychotherapy developed by the author, which can be applied to a number of mental health conditions, including
COMMUNICATION- FOCUSED THERAPY (CFT) FOR OCD Dr., M.D. Communication-Focused Therapy (CFT) is a psychotherapy developed by the author, which can be applied to a number of mental health conditions, including
Psychotherapy Services
 Psychotherapy Services Available now Free mental health services for people in Ontario experiencing mild to moderate depression and anxiety Funded by the Government of Ontario Meet Sarah. Sarah is 30
Psychotherapy Services Available now Free mental health services for people in Ontario experiencing mild to moderate depression and anxiety Funded by the Government of Ontario Meet Sarah. Sarah is 30
VA Recovery Transformation & Local Recovery Coordinators
 VA Recovery Transformation & Local Recovery Coordinators David Carroll, Ph.D. Director, Recovery Services Office of Mental Health Services Department of Veterans Affairs David.Carroll@va.gov April 27,
VA Recovery Transformation & Local Recovery Coordinators David Carroll, Ph.D. Director, Recovery Services Office of Mental Health Services Department of Veterans Affairs David.Carroll@va.gov April 27,
Module 10: Challenging Maladaptive Thoughts and Beliefs
 Module 10: Challenging Maladaptive Thoughts and Beliefs Objectives To learn techniques for addressing dysfunctional thoughts and beliefs To understand and manage potential difficulties using thought records
Module 10: Challenging Maladaptive Thoughts and Beliefs Objectives To learn techniques for addressing dysfunctional thoughts and beliefs To understand and manage potential difficulties using thought records
My name is Todd Elliott and I graduated from the University of Toronto, Factor- Inwentash Faculty of Social Work, in 1999.
 Profiles in Social Work Episode 32 Todd Elliott Intro - Hi, I m Charmaine Williams, Associate Professor and Associate Dean, Academic, for the University of Toronto, Factor-Inwentash Faculty of Social Work.
Profiles in Social Work Episode 32 Todd Elliott Intro - Hi, I m Charmaine Williams, Associate Professor and Associate Dean, Academic, for the University of Toronto, Factor-Inwentash Faculty of Social Work.
An Evaluation of the Sonas Freedom Programme September- December January 2012 Researcher: Paula McGovern
 An Evaluation of the Sonas Freedom Programme September- December 2011 January 2012 Researcher: Paula McGovern Introduction This evaluation examines the efficacy of the Sonas Housing Freedom Programme as
An Evaluation of the Sonas Freedom Programme September- December 2011 January 2012 Researcher: Paula McGovern Introduction This evaluation examines the efficacy of the Sonas Housing Freedom Programme as
Schizophrenia is a serious mental health condition that affects
 Schizophrenia Schizophrenia is a serious mental health condition that affects a person s thoughts, feelings and behaviours. Whilst it is serious, schizophrenia is both treatable and manageable, and we
Schizophrenia Schizophrenia is a serious mental health condition that affects a person s thoughts, feelings and behaviours. Whilst it is serious, schizophrenia is both treatable and manageable, and we
Catherine Madigan Clinical Psychologist 365 Burwood Road, Hawthorn,
 Catherine Madigan Clinical Psychologist 365 Burwood Road, Hawthorn, 3122 0419 104284 anxietyaustralia.com.au@gmail.com What Makes A Hoarder? Psychological Issues Behind Hoarding Picture of a Hoarder Bob
Catherine Madigan Clinical Psychologist 365 Burwood Road, Hawthorn, 3122 0419 104284 anxietyaustralia.com.au@gmail.com What Makes A Hoarder? Psychological Issues Behind Hoarding Picture of a Hoarder Bob
Problem Solving
 www.working-minds.org.uk Problem Solving Problem Solving The psychological importance of effective problem solving is very underestimated and is often taken for granted. As human beings, we assume that
www.working-minds.org.uk Problem Solving Problem Solving The psychological importance of effective problem solving is very underestimated and is often taken for granted. As human beings, we assume that
Management of depression
 Primary Management of depression care in General Principles Most adults with depression present with mild depression and can be treated in primary care. The goal of treatment is to achieve remission of
Primary Management of depression care in General Principles Most adults with depression present with mild depression and can be treated in primary care. The goal of treatment is to achieve remission of
A new scale (SES) to measure engagement with community mental health services
 to measure engagement with community mental health services") Title A new scale (SES) to measure engagement with community mental health services Service engagement scale LYNDA TAIT 1, MAX BIRCHWOOD 2 & PETER TROWER 1 2 Early Intervention Service, Northern Birmingham
Title A new scale (SES) to measure engagement with community mental health services Service engagement scale LYNDA TAIT 1, MAX BIRCHWOOD 2 & PETER TROWER 1 2 Early Intervention Service, Northern Birmingham
The Co-Occurring Disorders Treatment Program
 G R O U P D E S C R I P T I O N S The Co-Occurring Disorders Treatment Program is designed to provide a continuum of services to the substance abusing and dually diagnosed populations. These services include
G R O U P D E S C R I P T I O N S The Co-Occurring Disorders Treatment Program is designed to provide a continuum of services to the substance abusing and dually diagnosed populations. These services include
Honest, Open, Proud. To Erase the Stigma of Mental Health Challenges. Sue McKenzie, MA Sarah Reed, PhD WISE
 Honest, Open, Proud To Erase the Stigma of Mental Health Challenges Sue McKenzie, MA Sarah Reed, PhD WISE Honest, Open, Proud High School Small group program for youth (8 th -college) who have faced mental
Honest, Open, Proud To Erase the Stigma of Mental Health Challenges Sue McKenzie, MA Sarah Reed, PhD WISE Honest, Open, Proud High School Small group program for youth (8 th -college) who have faced mental
maintaining gains and relapse prevention
 maintaining gains and relapse prevention Tips for preventing a future increase in symptoms 3 If you do experience an increase in symptoms 8 What to do if you become pregnant again 9 2013 BC Reproductive
maintaining gains and relapse prevention Tips for preventing a future increase in symptoms 3 If you do experience an increase in symptoms 8 What to do if you become pregnant again 9 2013 BC Reproductive
Hearing Voices Group. Introduction. And. Background information. David DddddFreemanvvvvvvvvv
 Hearing Voices Group Introduction And Background information David DddddFreemanvvvvvvvvv Contents Hearing Voices Group Rationale Inclusion criteria for hearing voices group Structure of Group Process The
Hearing Voices Group Introduction And Background information David DddddFreemanvvvvvvvvv Contents Hearing Voices Group Rationale Inclusion criteria for hearing voices group Structure of Group Process The
I think women coming together and speaking is really great. Hearing other women s stories was very inspiring. To hear what they have been through and
 I think women coming together and speaking is really great. Hearing other women s stories was very inspiring. To hear what they have been through and come out the other side confident and strong in themselves.
I think women coming together and speaking is really great. Hearing other women s stories was very inspiring. To hear what they have been through and come out the other side confident and strong in themselves.
Reviewing Peer Working A New Way of Working in Mental Health
 Reviewing Peer Working A New Way of Working in Mental Health A paper in the Experts by Experience series Scottish Recovery Network: July 2013 Introduction The Scottish Government s Mental Health Strategy
Reviewing Peer Working A New Way of Working in Mental Health A paper in the Experts by Experience series Scottish Recovery Network: July 2013 Introduction The Scottish Government s Mental Health Strategy
Awareness of Borderline Personality Disorder
 Borderline Personality Disorder 1 Awareness of Borderline Personality Disorder Virginia Ann Smith Written Communication Sarah Noreen, Instructor November 13, 2013 Borderline Personality Disorder 2 Awareness
Borderline Personality Disorder 1 Awareness of Borderline Personality Disorder Virginia Ann Smith Written Communication Sarah Noreen, Instructor November 13, 2013 Borderline Personality Disorder 2 Awareness
Chronic Fatigue Syndrome (CFS) / Myalgic Encephalomyelitis/Encephalopathy (ME)
 / Myalgic Encephalomyelitis/Encephalopathy (ME)") Chronic Fatigue Syndrome (CFS) / Myalgic Encephalomyelitis/Encephalopathy (ME) This intervention (and hence this listing of competences) assumes that practitioners are familiar with, and able to deploy,
Chronic Fatigue Syndrome (CFS) / Myalgic Encephalomyelitis/Encephalopathy (ME) This intervention (and hence this listing of competences) assumes that practitioners are familiar with, and able to deploy,
Chapter 4. Lessons. Managing Mental and Emotional Health. Managing Mental and Emotional Health
 Managing Mental and Emotional Health Managing Mental and Emotional Health Lessons Lesson 1 Emotions Lesson 2 Understanding Emotions Lesson 3 Expressing Emotions Lesson 4 Coping with Emotions Lesson 5 Mental
Managing Mental and Emotional Health Managing Mental and Emotional Health Lessons Lesson 1 Emotions Lesson 2 Understanding Emotions Lesson 3 Expressing Emotions Lesson 4 Coping with Emotions Lesson 5 Mental
Information about PSYCHOTHERAPY
 Information om psykoterapi For adults Information about PSYCHOTHERAPY Psykiatri og Social psykinfomidt.dk CONTENTS 03 What is psychotherapy? 03 What is cognitive therapy? 04 Who can get cognitive therapy?
Information om psykoterapi For adults Information about PSYCHOTHERAPY Psykiatri og Social psykinfomidt.dk CONTENTS 03 What is psychotherapy? 03 What is cognitive therapy? 04 Who can get cognitive therapy?
Understanding the Stages of Change in the Recovery Process
 Understanding the s of Change in the Recovery Process STAGES OF CHANGE Pre- Contemplation Contemplation PERSON WHO HAS DEVELOPED AN EATING DISORDER The person does not believe they have a problem. Refusal
Understanding the s of Change in the Recovery Process STAGES OF CHANGE Pre- Contemplation Contemplation PERSON WHO HAS DEVELOPED AN EATING DISORDER The person does not believe they have a problem. Refusal
The Needs of Young People who have lost a Sibling or Parent to Cancer.
 This research focussed on exploring the psychosocial needs and psychological health of young people (aged 12-24) who have been impacted by the death of a parent or a brother or sister from cancer. The
This research focussed on exploring the psychosocial needs and psychological health of young people (aged 12-24) who have been impacted by the death of a parent or a brother or sister from cancer. The
Welcome to Pathways. - Auckland - Information about Pathways services in the Auckland region.
 Welcome to Pathways - Auckland - Information about Pathways services in the Auckland region. Alongside you in your recovery journey Welcome to Pathways. We re here to support you in your journey to being
Welcome to Pathways - Auckland - Information about Pathways services in the Auckland region. Alongside you in your recovery journey Welcome to Pathways. We re here to support you in your journey to being
HOARDING BEHAVIOR: Treatment and Research Results. Stephanie Yamin, PhD Clinical Psychology Assistant Professor, Saint-Paul University
 HOARDING BEHAVIOR: Treatment and Research Results Stephanie Yamin, PhD Clinical Psychology Assistant Professor, Saint-Paul University PERSONAL BELONGINGS EXERCISE Who has brought something precious or
HOARDING BEHAVIOR: Treatment and Research Results Stephanie Yamin, PhD Clinical Psychology Assistant Professor, Saint-Paul University PERSONAL BELONGINGS EXERCISE Who has brought something precious or
MATCP When the Severity of Symptoms Interferes with Progress
 MATCP 2017 When the Severity of Symptoms Interferes with Progress 1 Overview Stages of Change, or Readiness for Change Changing Behavior Medication Adherence Disruptive Behaviors Level of Care Tools including
MATCP 2017 When the Severity of Symptoms Interferes with Progress 1 Overview Stages of Change, or Readiness for Change Changing Behavior Medication Adherence Disruptive Behaviors Level of Care Tools including
SFHPT02 Develop a formulation and treatment plan with the client in cognitive and behavioural therapy
 Develop a formulation and treatment plan with the client in cognitive Overview This standard shows how the cognitive and behavioural therapist works collaboratively with the client to help them understand
Develop a formulation and treatment plan with the client in cognitive Overview This standard shows how the cognitive and behavioural therapist works collaboratively with the client to help them understand
A fact sheet produced by the Mental Health Information Service
 Anxiety what is it? A fact sheet produced by the Mental Health Information Service Anxiety is a natural reaction that everyone experiences - part of our fight or flight response - which helps us to be
Anxiety what is it? A fact sheet produced by the Mental Health Information Service Anxiety is a natural reaction that everyone experiences - part of our fight or flight response - which helps us to be
Depression: what you should know
 Depression: what you should know If you think you, or someone you know, might be suffering from depression, read on. What is depression? Depression is an illness characterized by persistent sadness and
Depression: what you should know If you think you, or someone you know, might be suffering from depression, read on. What is depression? Depression is an illness characterized by persistent sadness and
A guide to Getting an ADHD Assessment as an adult in Scotland
 A guide to Getting an ADHD Assessment as an adult in Scotland This is a guide for adults living in Scotland who think they may have ADHD and have not been diagnosed before. It explains: Things you may
A guide to Getting an ADHD Assessment as an adult in Scotland This is a guide for adults living in Scotland who think they may have ADHD and have not been diagnosed before. It explains: Things you may
Mood Disorders Society of Canada Mental Health Care System Study Summary Report
 Mood Disorders Society of Canada Mental Health Care System Study Summary Report July 2015 Prepared for the Mood Disorders Society of Canada by: Objectives and Methodology 2 The primary objective of the
Mood Disorders Society of Canada Mental Health Care System Study Summary Report July 2015 Prepared for the Mood Disorders Society of Canada by: Objectives and Methodology 2 The primary objective of the
HOARDING BEHAVIOR: Treatment and Research Results. Stephanie Yamin, PhD Clinical Psychology Assistant Professor, Saint-Paul University
 HOARDING BEHAVIOR: Treatment and Research Results Stephanie Yamin, PhD Clinical Psychology Assistant Professor, Saint-Paul University PERSONAL BELONGINGS EXERCISE Who has brought something precious or
HOARDING BEHAVIOR: Treatment and Research Results Stephanie Yamin, PhD Clinical Psychology Assistant Professor, Saint-Paul University PERSONAL BELONGINGS EXERCISE Who has brought something precious or