Diagnosis and treatment of dementia
|
|
|
- Britton Quinn
- 5 years ago
- Views:
Transcription

 Study")
1 Diagnosis and treatment of dementia Nathaniel Chin, MD, Assistant Professor (CHS) of Medicine Division of Geriatrics, UW School of Medicine and Public Health Director of Medical Services, Wisconsin Alzheimer s Disease Research Center Medical Director, Wisconsin Registry for Alzheimer s Prevention (WRAP) Study Madison, Wisconsin
2 Learning Objectives Overview of neurodegenerative diseases Clinical evaluation of memory complaint Discuss staging and disease course
3 Disclosures None
4 Misunderstanding in the community Confusion due to terminology I don t have dementia, I have Alzheimer s disease I have Alzheimer s, but at least I don t have dementia I don t have Alzheimer s, I was diagnosed with MCI
5 NIA & AA Diagnostic Criteria for Dementia Problems with thinking and daily function Cognitive symptoms that: Represent a decline from previous level Affect at least 2 thinking abilities on cognitive testing Interfere with usual functional abilities Are not explained by other medical or psychiatric illness Dementia due to AD Memory is the primary complaint & ruled out other causes Gradually progressive and with a documented decline Genetic testing or biomarkers

6 Dementia is a syndrome not a disease Rule out: Underlying medical disease Psychiatric disease Medications Progressive decline Alzheimer s Disease Vascular cognitive impairment Lewy Body dementia HIV, Alcohol, CJD Frontotemporal Dementia Parkinson s disease dementia Mixed pathologies
7 There are many causes of dementia Alzheimer s disease Vascular cognitive impairment Frontotemporal dementia Parkinson's disease Other Lewy Body dementia Frontotemporal dementia Lewy body disease Alzheimer's disease alone Parkinson disease dementia Vascular Mixed pathology Mixed pathology
8 Vascular Cognitive Impairment
9 Changes in definition Vascular Dementia NINDS AIREN (1993) 1. Memory impairment + at least one other domain 2. IADL impairment 3. Evidence of CVD 4. Causal relationship between dementia & CVD (onset within 3 months of stroke and/or acute onset) Vascular Dementia AHA/ASA (2011) 1. Evidence of stroke or subclinical vascular injury 2. 2 cognitive domains + IADL impairment PROBABLE VAD: IMAGING EVIDENCE TEMPORAL RELATIONSHIP OR RELATIONSHIP IN SEVERITY/PATTERN OF IMPAIRMENT AND PRESENCE OF DIFFUSE, SUBCORTICAL CVD NO GRADUALLY PROGRESSIVE DEFICITS BEFORE OR AFTER STROKE Major vascular neurocognitive disorder DSM 5 (2013) 1. Major neurocognitive disorder criteria met 2. Onset of deficits temporally related to cerebrovascular event OR Evidence for decline prominent in complex attention (including processing speed) and frontalexecutive dysfunction 3. Evidence of CVD from history, physical exam, and/or neuroimaging sufficient to account for neurocognitive deficits PROBABLE VAD: AT LEAST ONE OF 3 FEATURES Both clinical and genetic evidence of CVD is present

10 Vascular Cognitive Impairment subtypes Vascular impairment of cognition classification consensus study (VICCCS; Skroot, 2017) Proposed mechanisms of cause: Cerebral amyloid angiopathy Mixed dementia White matter hyperintensities Microbleeds/microhemorrhages Microinfarcts Arteritis/vasculitis

11 Lewy body disease
12 Dementia with Lewy Bodies (DLB) 4 th consensus report of the DLB consortium (McKeith et al, 2017) CORE CLINICAL FEATURES Fluctuating cognition with pronounced variations in attention and alertness. Recurrent visual hallucinations that are typically well formed and detailed. REM sleep behavior disorder, which may precede cognitive decline. One or more spontaneous cardinal features of parkinsonism: these are bradykinesia (defined as slowness of movement and decrement in amplitude or speed), rest tremor, or rigidity. SUPPORTING CLINICAL FEATURES Severe sensitivity to antipsychotic agents Postural instability; repeated falls; syncope or other transient episodes of unresponsiveness Severe autonomic dysfunction, e.g., constipation, orthostatic hypotension, urinary incontinence Hypersomnia; hyposmia Hallucinations in other modalities; systematized delusions; apathy, anxiety, and depression *(1) Reduced dopamine transporter uptake in basal ganglia demonstrated by SPECT or PET. (2) Abnormal (low uptake) 123iodine MIBG myocardial scintigraphy. (3) Polysomnographic confirmation of REM sleep without atonia. Probable DLB: 2 or more core clinical features 1 core clinical feature + 1 indicative biomarker* Possible DLB: 1 core clinical feature or 1 indicative biomarker* is present
13 Parkinson s disease dementia Development of Parkinson s motor symptoms first Motor symptoms precede cognitive symptoms by at least 1 year but often it is 6 8 years Population based studies 37% of patients whose PD began after 70yo had dementia 9% of patients whose PD began before 70yo Prevalence of dementia was 42% 4 years after PD diagnosis and 78% 8 years after diagnosis Possible association with APOE4 Galvin JE et al. "Current Issues in LBD Diagnosis, Treatment and Research" May 2008.
14 Frontotemporal disease
 Primary progressive")
: 2456 77.")
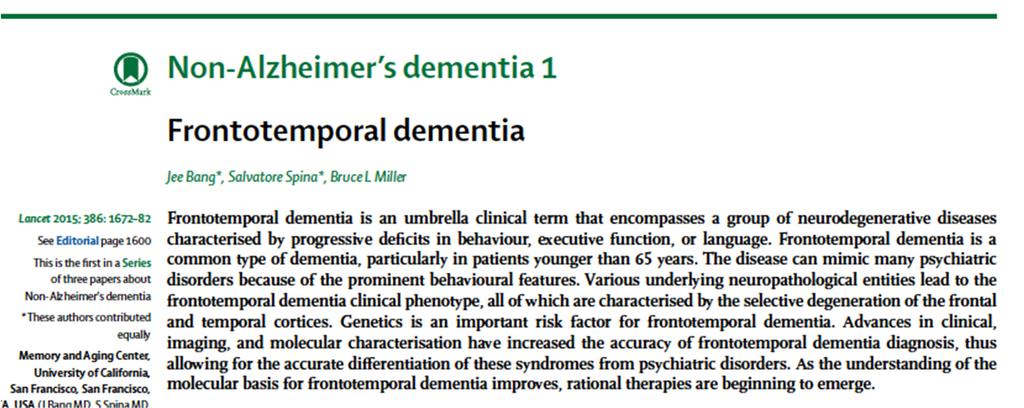
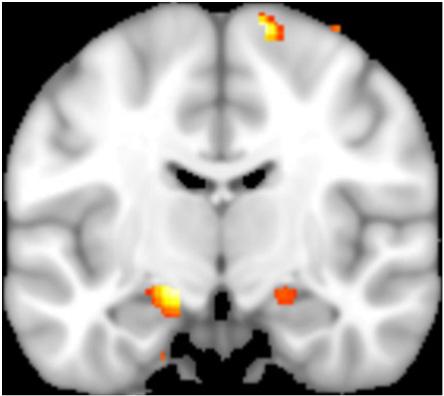
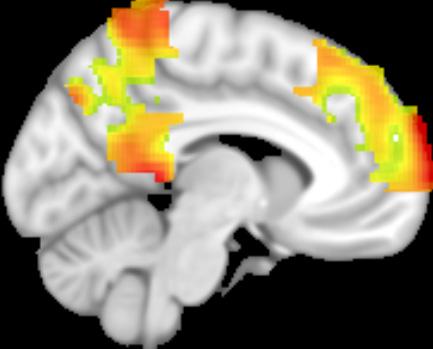
15 Frontotemporal dementia Normal Behavioral variant FTD (bvftd) Primary progressive aphasia (PPA) Rascovsky K et al. Brain Sep, 134(pt9): Epub 2011 Aug 2.
16 Behavioral variant FTD Early behavioral disinhibition, apathy, loss of empathy Early perseverative, stereotyped, compulsive/ritualistic behavior Hyperorality and/or dietary changes Neuropsychological profile: deficits in executive tasks, but relative sparing of memory and visuospatial skills Rascovsky K et al. Brain Sep, 134(pt9): Epub 2011 Aug 2.
17 Primary progressive aphasia Difficulty with language is most prominent clinical feature Language deficits are principal cause for impaired function Aphasia should be most prominent deficit at symptom onset Mesulam MM. Ann Neurol 2001;49:

18 Alzheimer s disease is not dementia AD can cause MCI and dementia MCI and dementia can be caused by other diseases AD is an abnormal process in the brain Amyloid builds up and plaques form Deposits of excess amyloid Amyloid not cleared from the brain Neurofibrillary tangles develop within cells Exposure of tau protein, become hyperphosphorylated Inflammation Develops after amyloid and tangles May be involved in development of amyloid
 Kapasi, DeCarli, Schneider, 2017; Acta")
19 Mixed pathologies are more common than single pathology In persons with probable AD, vascular disease is present in approximately 90% and other degenerative diseases in about 65% N=1078 autopsied subjects from the Religious Orders Study and Memory & Aging Project (Rush) Kapasi, DeCarli, Schneider, 2017; Acta Neuropathologica
20 To provide help the patient has to be seen and diagnosed Less than 50% of persons with AD are diagnosed Reasons to be evaluated Rule out reversible causes Take advantage of early treatments Participate in support programs Participate in research, public awareness & advocacy Advanced care planning Prince M et al. Alzheimer s Disease International World Alzheimer Report The benefits of early diagnosis and intervention, King s College London, UK.
21 Other benefits of early diagnosis Identify MCI in addition to dementia More research is focusing on MCI Lifestyle interventions that may modify disease course
22 Risk factors for Alzheimer s disease Age Family history of AD Apolipoprotein E4 (APOE4) genetic risk Low educational level Head trauma with loss of consciousness Vascular risk factors Inflammation Insulin resistance & metabolic risk factors Depression
23 Vascular risk factors associated with Alzheimer s Elevated blood pressure in midlife Obesity Diabetes Obstructive sleep apnea Physical inactivity Smoking

24 Addressing modifiable risk factors may impact disease course Physical activity Diet Stress reduction Sleep Cognitive activity Social activity Hearing/Vision Smoking cessation
25 Finnish Geriatric (FINGER) study to Prevent Cognitive Impairment 2 year study 1260 adults ages yrs Multi domain intervention: Diet Exercise Cognitive training Vascular risk monitoring Improved cognitive performance Ngandu et al. Lancet 2015; 385:

26 Cardiorespiratory fitness strengthens our brain

27 Among individuals with higher amyloid, higher physical fitness was associated with better memory performance Shultz et al., 2015, Journal of the International Neuropsychological Society
.")
28 The MIND diet keeps your brain younger Brain healthy food groups: Green leafy vegetables Other vegetables Nuts Berries Beans Whole grains Fish Poultry Olive oil Unhealthy groups are: Red meats Butter and stick margarine Cheese Pastries and sweets Fried or fast food Morris, M. C., Tangney, C. C., Wang, Y., Sacks, F. M., Barnes, L. L., Bennett, D. A., & Aggarwal, N. T. (2015). MIND diet slows cognitive decline with aging. Alzheimer's & dementia, 11(9),

29 MIND diet associated with reduced development of Alzheimer s disease 2 nd Tertile Hazard Ratio = 0.65 Highest Tertile Hazard Ratio = 0.47 Mediterranean Diet Hazard Ratio = 0.46 DASH Diet = 0.61 Alzheimers Dement Sep;11(9):
30 Stress can affect our brain and its function High cortisol associated with Worse memory and visual perception Lower total brain volume, occipital and frontal gray matter volume Microstructural change in areas connecting parts of the brain More evident in women No relationship to APOE4
31 Perceived stress can affect our brain function Increasing levels of perceived stress associated with Lower initial cognitive testing scores Faster rate of cognitive decline Present in both black and white adults % greater risk of MCI Alzheimer Dis Assoc Disord Apr Jun;30(2):93 8.

32 Sleep & AD 3 subjective sleep measures Worse sleep quality Sleep related problems Daytime somnolence Worse subjective sleep measures associated with greater AD pathology CSF AB, t tau, p tau


33 Sleep & AD Less adequate sleep, more sleep problems, and greater somnolence on questionnaires associated with greater amyloid burden on PET scan Amyloid burden not related to sleep amount, trouble falling asleep, and Epworth Sleepiness scale

34 Evaluation of suspected dementia
35 What can be done in a non memory clinic? Ask the patient if they re worried about their memory Then ask a family member Be on the look out for functional changes (IADLs primarily) Missing appointments Making mistakes on medications Multiple ER or urgent care visits Driving accidents Unkempt on exam Weight loss in elderly (are they eating?) Perform a cognitive screener
36 Cognitive screening tests are helpful but do not provide the diagnosis Perform when patient, family member, or provider are worried about memory/thinking changes Takes time: minutes Can be done by a medical assistant, RN, APP, PhD, MD Recommended screeners Mini Cog SLUMS MOCA
37 Initial work up Assess reversible causes Medications Mood Sleep apnea Thyroid Obtain memory labs or confirm labs within the past 12 months Complete metabolic panel: Na, Cr/BUN, Ca, LFTs Complete blood count, including MCV TSH, HgbA1c, Lipid panel Vitamin B1, B6, B12, Vitamin D, Folate Obtain or confirm structural brain imaging Image obtained during the time period of cognitive symptoms MRI provides best picture but CT is adequate in most cases


38 The hippocampus shrinks in AD Scheltens et al. Lancet Neurol 2002;1:13 20.

39 Metabolism decreases on FDG PET Less glucose use Scheltens et al. Lancet Neurol 2002;1:13 20.
40 Making the diagnosis takes time Detailed interview with patient and family Cognitive, functional, behavioral/psychiatric history Physical exam Full neurological exam Cognitive testing RBANS, Cognistat = 1 hour Lab testing if needed HIV, RPR, Vitamin levels Brain scans if needed CT or MRI Advanced brain scans FDG PET DAT scan Education and feedback Referral to appropriate resources Advanced care planning
41 What are the reversible forms of cognitive impairment? Non reversible = neurodegeneration AD, FTD, LBD, PDD, VCI Reversible = treat the underlying problem and cognition improves Medication induced Hypothyroidism/Hyperthyroidism Vitamin deficiency: Vit B1, B6, B12, D, Folate Chronic infection: Syphilis, Lyme disease Sleep apnea Mood disorders: depression, anxiety, bipolar, schizophrenia Delirium
42 Once diagnosed Things to get done immediately HC POA Financial POA Advanced directive Eventually Advanced Care Planning Discuss health values Discuss living environments Safety issues Support services
43 Stages of Dementia No two cases of dementia are the same May have symptoms from several stages at one time Typical course duration is 8 10 years from diagnosis Most have symptoms years prior to diagnosis 3 stage model & 7 stage model Confusing terminology Not comprehensive Do not discuss abilities that remain
44 3 Stage Model Often used for dementia due to Alzheimer s disease Mild dementia Early stage Moderate dementia Middle stage Severe dementia Late stage
45 7Stage Model Stage 1: No cognitive impairment Stage 2: Very mild cognitive decline Mild cognitive changes Stage 3: Mild cognitive impairment Cognitive impairment on testing Stage 4: Moderate cognitive decline Early stage dementia Stage 5: Moderately severe cognitive decline Mid stage dementia Impaired ADLs Stage 6: Severe cognitive decline Moderately severe dementia or middle stage Assistance for all ADLs Stage 7: Very severe cognitive decline Late stage dementia
46 Stage 1 Mild dementia Early Stage Cognition Mild memory loss of recent events Forgets what was just done, loses items Word finding difficulties Trouble remembering names Trouble planning or organizing Function Can still care for self, but takes longer to do perform ADLs or IADLs Psychological function and behavior Mood or personality changes Irritable, less initiative (apathy)
47 Stage 2 Moderate dementia Middle Stage Cognition Moderate memory loss & confusion Forgetful of events and/or personal history Difficulty expressing thoughts Cannot calculate, judge, plan Disoriented to time, place, date Function Needs more assistance with daily tasks & hygiene Urinary and stool incontinence Psychological function and behavior Sleep pattern disruption Irritable, moody, focused on self Withdrawn, wandering at times
48 Stage 3 Severe dementia Late Stage Cognition Severe memory and cognitive impairment Appears to not understand surroundings Cannot recognize family or self Minimal to no speech Function Bedridden requiring 24 hour assistance Physical impairments: coordination, walk, sit up, transfer, swallowing, smile Psychological function and behavior May have delusions, paranoia, hallucinations

49 FAST Scale Life Your Health/Hospice Palliative Scales Part I
50 Develop community allies Refer patients to: Alzheimer s Association Alzheimer s and Dementia Alliance of WI Aging and Disability Resource Center Provide information on home health services
51 Optimize care by working with the caregiver Establish routines Sleep wake cycles Timing of medications, location of medications Routine daily tasks Utilize calendars, sticky notes, white board Address safety Involve Physical Therapy for falling, weakness, ambulation Involve Occupational Therapy for ADLS/IADLs, home environment Involve Speech Therapy for communication and swallow issues
52 We must address the caregiver Compared with non caregiver controls matched by age, gender, race and marital status, caregivers of persons with AD or related disorders require 46% more physician visits 71% more prescribed medications Higher diastolic blood pressure Hyper coagulable state Higher plasma norepinephrine 60% rate stress as high or very high 40% suffer from depression Haley WE, Levine EG, Brown SL et al. Am J Geriatr Soc. 1987(May); 35(5): Shaw et al. J Psychosom Res 2003; 54: VonKanel et al. Am J of Cardiol 2001(June);87: Grant I; Psychosom Med 1999; 51:
 Rivastigmine (Exelon) Galantamine (Razadyne) N methyl D aspartate (NMDA) Receptor Antagonists Memantine")
53 FDA approved treatments for AD treat symptoms and not the disease Acetylcholinesterase inhibitors Donepezil (Aricept) Rivastigmine (Exelon) Galantamine (Razadyne) N methyl D aspartate (NMDA) Receptor Antagonists Memantine (Namenda)
54 The benefits of cholinesterase inhibitors can be meaningful improved cognition: but difficult to detect clinically small treatment effects improved global performance improved ADLs and possibly QOL decreased caregiver burden delayed nursing home placement Cummings Am J Geri Psychiatry 2003; Schneider Lancet 2004
55 The side effects of cholinesterase inhibitors can be meaningful and costly Most common side effects GI: nausea, vomiting, diarrhea CNS: insomnia, abnormal dreams Cardiac: bradycardia, syncope Other: muscle cramps, fatigue, weight loss Start low, go slow; meals may help with GI side effects May worsen frontotemporal dementia

56 NMDA antagonist: memantine Glutamate, the main excitatory neurotransmitter in the brain, acts at NMDA receptors Memantine blocks NMDA receptors and so may reduce the negative effects of glutamate (excitotoxicity and cell death)
57 The benefits of memantine can be meaningful later in the course of disease FDA approved for moderate-to-severe Alzheimer s disease Has been shown to slow the progression of cognitive changes May delay nursing home placement Provides an alternative for patients who cannot tolerate cholinesterase inhibitors Very few side effects relative to placebo Tariot et al JAMA 2004; Lopez et al J Neurol Neurosurg Psychiatry 2009
58 The treatment of other dementias look similar Cholinesterase inhibitors can be used in: Lewy body disease Parkinson disease dementia (rivastigmine) Vascular cognitive impairment (galantamine) Selective serotonin reuptake inhibitors (SSRIs) are used in: Frontotemporal dementia
59 Other related treatments Antidepressants Selective serotonin reuptake inhibitors (SSRIs) Anxiolytics No benzodiazepines SSRI Buspirone, wellbutrin, gabapentin Sleep aides Trazodone & mirtazapine Psychotropics (not FDA approved for dementia) First utilize DICE approach Quetiapine, risperidone, olanzapine Avoid haldol in lewy body dementia
60 Research studies Diagnostic studies Imaging techniques PET scan for amyloid, tau, synapses MRI scans CSF studies Different markers Blood based biomarkers Intervention trials Drug trials Lifestyle interventions Disclosure of amyloid status
61 Resources NIA Alzheimer s Disease Education & Referral (ADEAR) Center Alzheimer s Association Alzheimer s & Dementia Alliance Wisconsin Department of Health Services caregiver training.htm Wisconsin Alzheimer s Institute Wisconsin Alzheimer s Research Center (ADRC)

62 Dementia Matters is a podcast about Alzheimer s disease research, news, and resources. Targets a general audience 10 to 15 minutes long New episode every other week Two ways to listen: adrc.wisc.edu/dementia matters Subscribe through itunes, Stitcher, or Google Play
11/7/2018. Learning Objectives. Diagnosis and treatment of dementia. Disclosures. Misunderstanding in the community
 Learning Objectives Diagnosis and treatment of dementia Overview of neurodegenerative diseases Clinical evaluation of memory complaint Discuss staging and disease course Nathaniel Chin, MD, Assistant Professor
Learning Objectives Diagnosis and treatment of dementia Overview of neurodegenerative diseases Clinical evaluation of memory complaint Discuss staging and disease course Nathaniel Chin, MD, Assistant Professor
11/12/2018. Acknowledgements. Risk factors for Alzheimer s disease
 Is it Possible to Reduce My Risk for Alzheimer's Disease? An Overview of Current Risk Reduction Strategies Dorothy Farrar Edwards PhD, Professor of Medicine and Kinesiology Core Leader: Outreach, Recruitment
Is it Possible to Reduce My Risk for Alzheimer's Disease? An Overview of Current Risk Reduction Strategies Dorothy Farrar Edwards PhD, Professor of Medicine and Kinesiology Core Leader: Outreach, Recruitment
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Patterns of Cognitive Impairment in Dementia
 Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia
 Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Dementia is not normal aging!
 The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
How to Diagnose Early (Prodromal) Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.
 Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.") How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
100 billion neurons!
 100 billion neurons! Where s my car parked? Normal Memory Changes with Age Memory changes start even before 30 Harder to store new memories Sensory inputs aren't as sharp hear, see, taste Multi-tasking
100 billion neurons! Where s my car parked? Normal Memory Changes with Age Memory changes start even before 30 Harder to store new memories Sensory inputs aren't as sharp hear, see, taste Multi-tasking
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Introduction, use of imaging and current guidelines. John O Brien Professor of Old Age Psychiatry University of Cambridge
 Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University
 Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University Design of trials in DLB and PDD What has been learnt from previous trials in these indications and other dementias? Overview
Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University Design of trials in DLB and PDD What has been learnt from previous trials in these indications and other dementias? Overview
Evaluation and Treatment of Dementia
 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center
 Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
10 Facts We All Need to Know About Dementia (MNCD) in Old Age
 in Old Age") 10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
ALZHEIMER S DISEASE OVERVIEW. Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health
 ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
Comprehensive Approach to DLB Management
 Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status. Case 1 4/7/11. Which of the following evaluations is your next step?
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Resources: Types of dementia
 1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
September 26 28, 2013 Westin Tampa Harbour Island. Co-sponsored by
 September 26 28, 2013 Westin Tampa Harbour Island Co-sponsored by From Brains at Risk to Cognitive Dysfunction: The Role of Vascular Pathology Ralph Sacco, MD, MS, FAHA, FAAN Miller School of Medicine
September 26 28, 2013 Westin Tampa Harbour Island Co-sponsored by From Brains at Risk to Cognitive Dysfunction: The Role of Vascular Pathology Ralph Sacco, MD, MS, FAHA, FAAN Miller School of Medicine
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Understanding Dementia
 Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Neurocognitive Disorders Research to Emerging Therapies
 Neurocognitive Disorders Research to Emerging Therapies Edward Huey, MD Assistant Professor of Psychiatry and Neurology The Taub Institute for Research on Alzheimer s Disease and the Aging Brain Columbia
Neurocognitive Disorders Research to Emerging Therapies Edward Huey, MD Assistant Professor of Psychiatry and Neurology The Taub Institute for Research on Alzheimer s Disease and the Aging Brain Columbia
3/6/2019 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING FINANCIAL DISCLOSURES LEARNING OBJECTIVES
 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
Dementia Diagnosis Guidelines Primary Care
 Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
Dementia NICE Guidelines Update. Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018
 26 September 2018") Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
Objectives. Objectives continued: 3/24/2012. Copyright Do not distribute or replicate without permission 1
 Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
EARLY DEMENTIA. University of Hawaii Geriatric Medicine Department
 EARLY DEMENTIA University of Hawaii Geriatric Medicine Department INTRODUCTION Dementia is very prevalent Screening and early diagnosis is important Evaluation Dementia Management DEMENTIA IS VERY PREVALENT
EARLY DEMENTIA University of Hawaii Geriatric Medicine Department INTRODUCTION Dementia is very prevalent Screening and early diagnosis is important Evaluation Dementia Management DEMENTIA IS VERY PREVALENT
The Spectrum of Lewy Body Disease: Dementia with Lewy Bodies and Parkinson's Disease Dementia
 Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Medications and Non-Pharma Approaches to Treatment. David J. Irwin, MD Penn Frontotemporal Degeneration Center
 Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Alzheimer s Disease Update: From Treatment to Prevention
 Alzheimer s Disease Update: From Treatment to Prevention Jeffrey M. Burns, MD Edward H. Hashinger Professor of Medicine Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science
Alzheimer s Disease Update: From Treatment to Prevention Jeffrey M. Burns, MD Edward H. Hashinger Professor of Medicine Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
The Aging Brain The Aging Brain
 The Aging Brain The Aging Brain R. Scott Turner, MD, PhD Director, Memory Disorders Program Professor, Department of Neurology Georgetown University Washington, DC memory.georgetown.edu rst36@georgetown.edu
The Aging Brain The Aging Brain R. Scott Turner, MD, PhD Director, Memory Disorders Program Professor, Department of Neurology Georgetown University Washington, DC memory.georgetown.edu rst36@georgetown.edu
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
Alzheimer s Disease. Fact Sheet. Fact Sheet. Fact Sheet. What Causes AD?
 2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
Memory Matters: Learning Objectives: Synapses, Age, and Health. Neuronal Synapses DISCLOSURE DECLARATION. Cognition and Normal Aging
 Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Differentiating Dementia Diagnoses
 Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Part 2: Early detection, assessment and treatment in relation to the new guidelines. Christopher Patterson McMaster University
 Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Alzheimer s Disease - Dementia
 - Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
- Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
Alzheimer s disease is an
 Alzheimer s Disease FACT SHEET Alzheimer s disease is an irreversible, progressive brain disease that slowly destroys memory and thinking skills, and eventually even the ability to carry out the simplest
Alzheimer s Disease FACT SHEET Alzheimer s disease is an irreversible, progressive brain disease that slowly destroys memory and thinking skills, and eventually even the ability to carry out the simplest
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Assessment Toolkits for Lewy Body Dementia
 Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Moving Targets: An Update on Diagnosing Dementia in the Clinic
 Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018
 From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
What is dementia? Symptoms of dementia. Memory problems
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
Dementia the A,B,Cs. Dr. Frank Molnar. Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital
 Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
If you have dementia, you may have some or all of the following symptoms.
 About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
Multiple choice questions: ANSWERS
 Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Approach to Cognitive Disorders in Primary Care
 Approach to Cognitive Disorders in Primary Care What can reasonably be done in an office visit? What about screening for cognitive disorders? USPSTF (2014) doesn t recommend screening: magnitude of clinically
Approach to Cognitive Disorders in Primary Care What can reasonably be done in an office visit? What about screening for cognitive disorders? USPSTF (2014) doesn t recommend screening: magnitude of clinically
Understanding Alzheimer s Disease
 Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease
 Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Vascular Dementia. Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center
 Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
As a general cognitive screening tool or as part of an annual exam (Medicare Annual Wellness Visit).
.") EMR DECISION SUPPORT TOOLS FOR ALZHEIMER S AND RELATED DEMENTIAS 1. Screening Tool Criteria For When to Use: As a general cognitive screening tool or as part of an annual exam (Medicare Annual Wellness
EMR DECISION SUPPORT TOOLS FOR ALZHEIMER S AND RELATED DEMENTIAS 1. Screening Tool Criteria For When to Use: As a general cognitive screening tool or as part of an annual exam (Medicare Annual Wellness
8/14/2018. The Evolving Concept of Alzheimer s Disease. Epochs of AD Research. Diagnostic schemes have evolved with the research
 The Evolving Concept of Alzheimer s Disease David S. Geldmacher, MD, FACP Warren Family Endowed Chair in Neurology Department of Neurology UAB School of Medicine Epochs of AD Research Epoch Years Key Event
The Evolving Concept of Alzheimer s Disease David S. Geldmacher, MD, FACP Warren Family Endowed Chair in Neurology Department of Neurology UAB School of Medicine Epochs of AD Research Epoch Years Key Event
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia and cognitive decline
 Dementia and cognitive decline Expert Briefing Su Ray and Dr Susan Davidson Research Department Together, we can help everyone to love later life 01 Brain basics Normal ageing, cognitive impairment and
Dementia and cognitive decline Expert Briefing Su Ray and Dr Susan Davidson Research Department Together, we can help everyone to love later life 01 Brain basics Normal ageing, cognitive impairment and
8/24/18. Dementia. Risk of Dementia Following Traumatic Brain Injury: A Review of the Literature. Media Presence. Media Presence
 Risk of Dementia Following Traumatic Brain Injury: A Review of the Literature Media Presence Carlos Marquez de la Plata, Ph.D. & Jeff Schaffert, M.S. Media Presence Dementia What is dementia? Dementia
Risk of Dementia Following Traumatic Brain Injury: A Review of the Literature Media Presence Carlos Marquez de la Plata, Ph.D. & Jeff Schaffert, M.S. Media Presence Dementia What is dementia? Dementia
Forgetfulness: Knowing When to Ask for Help
 National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
Mild Cognitive Impairment
 Mild Cognitive Impairment The Role of the Family Physicians McGill Refresher Course December 2018 Fadi Massoud MD FRCPC, Internist-Geriatrician Centre Hospitalier Charles LeMoyne & Institut Universitaire
Mild Cognitive Impairment The Role of the Family Physicians McGill Refresher Course December 2018 Fadi Massoud MD FRCPC, Internist-Geriatrician Centre Hospitalier Charles LeMoyne & Institut Universitaire
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask. Presented By: Tuesday, March 22, 2011 at 1:00 PM ET
 PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA
 BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of