Osteoporosis. The Silent Killer. Joseph B. Hawkins, Jr., MD, FACE Sierra Endocrine Associates Fresno, California
|
|
|
- Gary Jefferson
- 5 years ago
- Views:
Transcription


1 Osteoporosis The Silent Killer Joseph B. Hawkins, Jr., MD, FACE Sierra Endocrine Associates Fresno, California
2 Disclosures Speakers Bureau Amgen
 September")
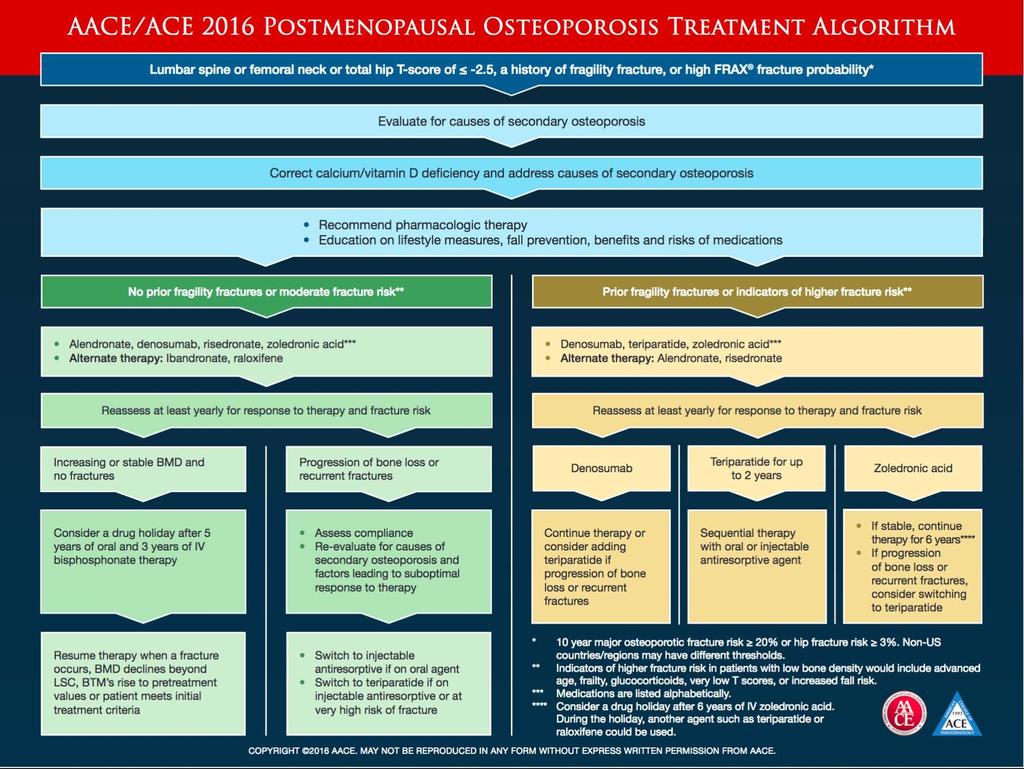
3 AACE/ACE Guidilines American Association of Clinical Endocrinologist and American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis Endocrine Practice Vol 22 (Suppl 4) September 2016
4 Osteoporosis Q1 How to assess fracture risk and diagnose Osteoporosis Q2 What is the appropriate evaluation? Q3 Fundamental measures for bone health? Q4 Who needs pharmacologic therapy? Q5 What medication should be used to treat Osteoporosis? Q6 How is treatment Monitored? Q7 What is successful treatment of Osteoporosis? Endocrine Practice Vol 22 (Suppl 4) September 2016
5 Osteoporosis Q8 How lone should patients be treated? Q9 What is the role for combination treatment? Q10 Should sequential use of agents be considered? Q11 Should vertebral augmentation be considered? Q12 When to refer to Osteoporosis specialist? Endocrine Practice Vol 22 (Suppl 4) September 2016



6 Osteoporosis: A Major Public Health Issue IS 2-million-2 Many? 5,500 Fractures Daily National Bone Health Alliance
7 Osteoporosis is a Common Condition in Women in the U.S. Number or Events Annually 2,000,000 2,000, ,500,000 1,000, , , , , , , Osteoporotic Fracture Heart Attack Stroke Breast Cancer Uterine Cancer Ovarian Cancer




8 What are the Consequences of Underdiagnosing and Undertreating Osteoporosis? In women with hip fracture: Fracture begets future fracture Deteriorated quality of life Long-term care admission Mortality 40% had prior fracture 1 40% need assistance walking 2 18% enter LTC 3 23% die within 1 year 4 Lifetime risk of hip fracture in women >50 is 12.1% 5 1. Hajcsar EE, et al. CMAJ 2000, 163: ; 2. Cooper C. Am J Med. 1997:103:12S-19S; 3. Jean et al. JBMR 2012 On-line September Ioannidis G, et al. CMAJ 2009;181: Hopkins et al Osteo Intl 2012; 23:







9 Osteoporosis :Microscopic Structure Normal Moderate Severe Normal Trabecula Thinning of Trabecula Perforation of Trabecula Osteoporosis is a systemic disease characterized by low bone mass & micro-architectural deterioration with a consequent increase in bone fragility and susceptibility to fracture
10 Osteoporosis Q1 How is fracture risk assessed?

11 Osteoporosis Compromises Bone Strength Increases Risk of Fracture Bone Quality Bone Strength + Bone Density + Fall Risk 1. Architecture 2. Turnover 3. Damage Accumulation 4. Mineralization 5. Collagen quality abmd = g/cm 2 vbmd = g/cm 3 Fracture Risk 1. LE Strength 2. Balance 3. Joint Flexibility 4. Vision Adapted from NIH Consensus Development Panel on Osteoporosis. JAMA 2001
12 Evaluation for Osteoprosis Evaluation all post menopausal women > age 50 for Osteoporosis risk Bone Quality Age, Sex, Family History Architecture, Geometry & Turnover Prior History of Fracture Steroids, Smoking or Alcohol Vitamin D Deficiency Calcium &/or nutrient Malabsorption Bone Density BMD in all > 65 BMD earlier if risk factors present
13 Osteoporosis should be diagnosed if : 1. In the presence of a fragility fracture in the absence of other metabolic bone disorders 2. BMD T-Score is 2.5 or lower in any single ROI : Lumbar Spine, Femoral Neck, total hip or 33% radius even in the absence of prevalent fracture 3. Osteoporosis may also be diagnosed in patients with low bone mass (T-Score -1.0 to -2.4, Osteopenia ) who are at increased fracture risk using FRAX Country Specific thresholds US Thresholds are: Global fractrure risk of 20% or greater or hip fracture risk 3% or greater
14 Fracture Risk Assessment How do we Combine these Risks into a usable Fracture Risk Assessment? WHO FRAX tool GARVAN Institute
15 FRAX Fracture Risk Calculator

16 FRAX Fracture Risk Calculator
17 FRAX Fracture Risk Calculator Limitations of FRAX Underestimates future risk as it only reports risk for hip and major fractures which comprise only half of all fractures Underestimates the risk in patients with multiple prior osteoporosis related fractures Underestimates the risk in patients with lumbar spine BMD lower than the femoral neck Underestimates the risk in patients secondary osteoporosis Underestimates the risk in patients in those at high risk of falling Estimates risk of those who are drug naive

18 Fracture Risk Determines Need for Treatment HIGH RISK FOR FRACTURE CONSIDER FOR TREATMENT IF: 1. Already Fractured 2. Low BMD T-score < -2.5 at any measured site 3. FRAX Global risk > 20% 4. FRAX Hip Risk > 3% 5. Reassess in 1-2 years CONSIDER PREVENTIVE THERAPY IF: 1. Other risk factors present 2. Patient is worried about fracture 3. Lifetime risk considered to be high 4. Reassess in 2-3 years NO NEED FOR PREVENTIVE THERAPY 1. May choose Hormone Therapy for other reasons 2. Reassess in 3-5 years 3. Lifestyle Modification Treat Lifestyl e Lifestyle Modification Treat
19 Top 5 Reasons to Consider Treatment in the Moderate Risk Patient: 1. Lumbar spine T-score << femoral neck T-score (by >2 T-scores) 2. Concurrent high risk disorder or medications, including: Hypogonadism or premature menopause (age <45 yr) Primary hyperparathyroidism Hyperthyroidism Rheumatoid arthritis Glucocorticoids (long-term or repeated use) Aromatase inhibitor therapy Diabetes Mellitus 3. Falls ( 2 in the past year) 4. Patient preference to be treated Steering Group Communications. Feb 9 th, Based on Osteoporosis Canada Guidelines: Papaioannou A, et al. CMAJ. 2010;182:
20 Q2 : Evaluation for Secondary Causes of Osteoporosis Evaluate for prevalent fractures Height loss, Lateral spine x-rays or VFA Many vertebral fractures go undetected Routine tests include: Consider baseline bone turnover markers Serum Ctx, BSAP o P1NP Complete blood cell count (CBC), Serum calcium, PTH, Creatinine, Albumin, PO4, 25 OH Vitamin D, Alkaline Phosphatase Urinary Calcium: Creatinine Ratio Additional tests may be appropriate: WHEN TO CONSIDER VFA Women > 70 Height loss of 1.5 inches Self reported fracture or undocumented back pain Chronic Steroid therapy Thyroid-Stimulating Hormone (TSH), Urinary cortisol, Testosterone in Men, Protein electrophoresis (SPEP/UPEP)
21 Q3 Fundamental measures for bone health Avoid Excess alcohol intake limit to two drinks a day or less Counsel patients to stop or avoid smoking Counsel patients to maintain an active lifestyle including weight-bearing, balance and resistance exercises Improve strength, balance & coordination, Reduce risk of falling Improve joint mobility & flexibility Counsel on fall prevention including a Safe environment: Bathroom safety, Rugs and night lights Avoid sedatives, hypotensive agents Walking aids (cane, walker) Consider referral to physical therapy
22 Calcium Intake Goal is to get as much as possible form dietary sources, supplementing to achieve the daily goal if necessary. Recommended daily intake: Age mg/day Age mg/day Age > mg/dl FOOD CALCIUM FOOD CALCIUM Turnip Greens, ½ cup 100 Plain Yogurt, 8 oz 400 Kale cooked 1 cup 100 Cheese, solid 1.5 oz 300 Cabbage, 1 cup 75 Sardines, 3 oz 325 Bread Slice 75 Milk, 8 oz 300 Tortilla, corn & flower 45 Tofu ½ cup 250 Broccoli ½ cup 25 Cottage Cheese 1 cup 140 Office of Dietary Supplements, National Institute of Health
23 Calcium Intake The optimal intake and utility of calcium supplements is controversial A Swedish study found both dietary and supplement calcium intake of > 1500 mg per day was associated with an increased mortality A Canadian study of 0ver 9,000 subjects found an increased survival advantage to those taking supplements Studies suggest dietary calcium may be prefered over supplements. Total calicum intake should not exceed 1500 mg per day Office of Dietary Supplements, National Institute of Health
24 Vitamin D Recommendations There is considerable disagreement among experts as the optimal and safe upper doses FOOD Vit D Goal Blood Levels of Vit D Ng/dl Cod Liver Oil 1 Tbs 1360 Deficiency <15 Swordfish, 3 oz 566 Insufficiency Salmon, 3 oz 447 Adequate Tuna, 3 oz 154 High Milk, 8 oz 120 Potentially Harmful >150 Egg yoke, 1 40 Institute of Medicine: Age < units/day Age > units/day Safe Maximum dose: 4,000 u/d Maintain 25-OH D levels at least ng/ml Office of Dietary Supplements, National Institute of Health
25 Other Supplements Magnesium may be beneficial in those using proton pump inhibitors or diuretics long term Vitamin A, K and phytoestrogen Excessive vitamin A, > 10,000 iu/d, should be avioded as it has been shown to have detremental effects on bone Data on Vitamin K is inconclusive not recommended Phytoestrogens/ isoflavones No evidence of benefit NOT recommended Caffeine high intake associated with increase fractures Protein Adequate protein intake of ~ 0.8 g/kg /day Office of Dietary Supplements, National Institute of Health
26 AACE Osteoporosis Practice Guidelines-2016 Q4: Who needs treatment for Osteoporosis? 1. Patients with low bone mass and a history of fragility fracture of the hip or spine 2. Patients with a T-score of 2.5 or lower in the spine, femoral neck, total hip or 33% radius 3. Patients with a T-Score between-1.0 and 2.5 if the FRAX 10 year probabliity for major osteoporotic fracture is > 20%, or the hip fracture risk is > 3%. (US country specific recommendations)
27 Q5 What Osteoporosis Medications should be used? 1. Approved agents with efficacy to reduce hip, non-vertebral and spine fractures 1. Alendronate, Residronate, Zolendronate, & Denosumab are appropriate as initial therapy 2. Teriparatide, Denosumab, or zolendronate should be considered for patients unable to use oral therapy as initial therapy 3. Denosumab is the agent of choice for patients with CKD 4. Raloxifene or ibandronate may be appropriate in some cases where patients requiring drugs with spine-specific efficacy 5. Calcitonin (increases cancers) and Strontium ( increased CV risk) therefore their use is not recommended 6. Estrogen use for non skeletal benefits will also serve to help prevent postmenopausal bone loss
 Bone Formation Therapy Teriparatide Vertebral Hip - - Nonvertebral - * Based on GRADE A evidence as assessed in the Osteoporosis Canada 2010")
28 Anti-fracture Efficacy of Current Therapies Type of Fracture Therapeutic Options for Fracture Prevention in PMO Women 1 * Alendronate Bisphosphonates Risedronate Antiresorptive Therapy Zoledronic Acid Denosumab Raloxifene Estrogen * (Hormone Therapy) Bone Formation Therapy Teriparatide Vertebral Hip - - Nonvertebral - * Based on GRADE A evidence as assessed in the Osteoporosis Canada 2010 Clinical Practice Guidelines for the Diagnosis and Management of Osteoporosis in Canada For postmenopausal women, indicates first line therapies and Grade A recommendation. Hormone therapy (estrogen) can be used as first-line therapy in women with menopausal symptoms. In Clinical trials, non-vertebral fractures are a composite endpoint including hip, femur, pelvis, tibia, humerus, radius, and clavicle. 1. Papaioannou A, et al. CMAJ. 2010;182:










29 Mechanism of Action of Available Osteoporosis Therapies Osteoclast Precursors Estrogen therapy Selective estrogen receptor modulators Hormones Multinucleated Osteoclast RANKL RANK Bisphosphonates Binds to bone; inhibits osteoclasts Teriparatide PTH analog Denosumab RANK Ligand inhibitor Osteoblast Osteoclast Adapted from: Boyle WJ et al. Nature 2003; 423:
30 * Correct with adequate calcium & Vitamin D intake prior to initiating therapy. Rarely, oral bisphosphonates have been associated with severe esophageal events. Uncommon; mostly with cancer patients and/or dental procedures. Consider risk/benefit balance for women with a history of stroke or risk factors for stroke or venous thromoboembolism. Urinary calcium monitoring should be considered for patients with active urolithiasis and hypercalciuria. ** Recommended that all patients have their renal function assessed prior to treatment. Refer to respective Product Monographs for full Prescribing Information. Safety and Tolerability of Available Treatments Bisphosphonates Denosumab Raloxifene Teriparatide Hypocalcemia* Hypocalcemia* Vasodilation Transient orthostatic hypotension GI symptoms Postmarketing reports of musculoskeletal pain Infections (serious events 4.1% vs. 3.4% placebo) Dermal events (10.8% vs. 8.2% placebo) Osteonecrosis of jaw Osteonecrosis of jaw Stroke Venous thromboembolism ( risk vs. placebo) Lipid and triglyceride monitoring Osteosarcoma (only observed in animal trials, not clinical trials) Urolithiasis Atypical Fracture (rare) Atypical Fracture (rare) Renal impairment ** Atrial fibrillation (2.5% vs. 1.9% placebo) Suppression of bone turnover

31 Osteonecrosis of the Jaw (ONJ) Bisphosphonate-Related Osteonecrosis of the Jaw Frequency: 1:1,700 to 1:20,000 Risk factors: Dentoalveolar surgery Steroid therapy Chemotherapy High dose Bisphosphonate Duration of therapy Treatatment Avoid surgical manipulation Antibiotics


32 Atypical Subtrochanteric Femur Fracture Ask about new thigh or pelvic pain Plain X-ray of the femur best screening tool Discontinue antiresorptive Consider prophylactic rodding Some recommending teriparatide therapy
33 Is your patient afraid to take their medication? Help put patient concerns in perspective Fatal motor vehicle accidents 8.4/100,000 person/year 1 Murder 1.8/100,000 person/year 2 ONJ* <1/100,000 pts/year 3 Atypical fracture** 2/100,000 pts on 2 yrs BPs 113.3/100,000 pts on 8 yrs BPs 4 For every 100 hip fractures prevented there is 1 atypical femur fracture 5 *The risk of ONJ is higher among cancer patients treated with high doses anti-resorptives 6 **Reports of AFF have also been documented with other osteoporosis therapies 7-8 and in patients who have never received BP therapy 9 1. Transportation Canada Casualty Rates Statistics Canada Homicide Rate Khan A, et al.j Rheumatol. 2011;38: Dell R, et al. JBMR (12): Wang et al JBMR 2011; 26: Khosla S et al. JBMR 2007:22: Kim SY et al. JBMR. 26(5): Amgen, data on file. 9. Shane E et al. JBMR 2010; 25:
34 AACE Osteoporosis Practice Guidelines-2016 Q7: What is successful treatment? Successful treatment is defined as stable or increasing BMD with no evidence of new fractures For patients taking antiresorptive agents target for success is Bone turnover at or below median value for PM women Consider alternative therapy or reassessment for secondary causes in those who have recurrent fractures or significant bone loss
35 AACE Osteoporosis Practice Guidelines-2016 Q8: How long should patients be treated Treatment with teriparatide should be limited to 2 years For Oral bisphosphonates, consider a bisphosphonate holiday after 5 years of stability in moderate risk patients For oral bisphosphonates, consider a bisphosphonate holiday after 6-10 years of stability in higher risk patients For IV zolendronic acid, consider a drug holiday after 3 annual doses and in moderate risk patients, and after 6 doses in higher risk patients Teriparatide or raloxifene may be considered during bisphosphonate holidays A holiday is NOT recommended with Denosumab Resume therapy in those at high risk for fracture after two years of Drug Holiday
36 BMD Efficacy of Long-term Treatment* In long term trials, BMD continues to increase or remains stable Medication Pivotal Study Extended Treatment Duration (yrs) # of Participants % Change Lumbar Spine BMD Ŧ % Change Total Hip BMD Ŧ Risedronate 1 VERT-MN Alendronate 2 FLEX Zoledronic Acid 3 Denosumab 4 HORIZON ( Analysis of 9 year study) FREEDOM (Analysis 10 year study) 7/ * Not head to head analyses: Results cannot be compared due to differing study populations and methodologies. Ŧ Represents % change from BL of Pivotal Trial. Represents 10 mg dose only. 1. Mellstrom D et al. Calcif Tissue Int 2004;75: Bone HG et al. N Engl J Med 2004;350: Black DM, et al. J Bone Miner Res. 2012; 27(2): Brown JP, et al ACR Annual Meeting. Presentation L8
37 Yearly Incidence of New Vertebral Fractures Through 6 Years: Continued Prolia (denosumab) Yearly Crude Incidence (%) Placebo Denosumab Pivotal Phase 3 Fracture Study Open-label Extension 3.1% 3.1% 2.2% 1.4% 1.3% 1.1% 1.1% 0.9% 0.7% /5* 6 7/8 Years of Treatment Exposure Fracture incidence was not evaluated as an efficacy endpoint in the extension study. 1. Adapted from Brown JP, et al. Presented at: ACR; November 5-9, 2011; Chicago, Ill. 2. Data on file, Amgen. 37
38 HORIZON Recurrent Fracture Trial: NEJM 2007,Sept 18: Rapid Publication online 28% Risk of Death
39 AACE Osteoporosis Practice Guidelines-2016 Q9: What About Combination Therapy? AACE does not recommend combination therapy Estrogen given for menopausal symptoms or raloxifene for prevention of breast cancer may bed used with other agents Combined Denosumab and teriparatide achieves greater BMD increases but no fracture data is available
40 AACE Osteoporosis Practice Guidelines-2016 Q10: Should sequential Therapy be considered? Treatment with teriparatide should always be followed by anti-resorptive agents to prevent BMD decline
41 AACE Osteoporosis Practice Guidelines-2016 Q11: Should Vertebral Augmentation be considered for Compression Fracture? Vertebroplasty and kyphoplasty are NOT recommended as first line treatment of vertebral fractures given the unclear benefit on oveal pain and the potential increased risk of vertebral fractures in adjacent vertebrae

42 AACE Osteoporosis Practice Guidelines-2016 Q12: When to refer to an Osteoporosis Specialist? When patient with normal BMD fractures Recurrent fractures despite receiving appropriate therapy When osteoporosis is unexpectedly severe Patients who experience fragility fracture may benefit form specialist care When the patient has conditions complicating therapy CKD, hyperparathyroid, hyperthyroid When osteoporosis is unexpectedly severe
43 Osteoporosis: A Major Public Health Issue Osteoporosis is a major health problem Patients at risk can be identified Safe and effective therapy is available 2-million-2 is too Many!
44
45 Questions
Osteoporosis. A Silent Killer. David A. Chappell, MD Endocrinology Private Practice Petaluma, California
 Osteoporosis A Silent Killer David A. Chappell, MD Endocrinology Private Practice Petaluma, California Relevant Disclosures Speakers Bureau Astra Zeneca Boehringer Ingelheim AACE/ACE Guidelines American
Osteoporosis A Silent Killer David A. Chappell, MD Endocrinology Private Practice Petaluma, California Relevant Disclosures Speakers Bureau Astra Zeneca Boehringer Ingelheim AACE/ACE Guidelines American
Osteoporosis Case Studies
 2019 Endocrine and Diabetes Symposium for Primary Care Providers Osteoporosis Case Studies Joseph B Hawkins, Jr., MD, FACE Assistant Clinical Professor of Medicine, UCSF Founder, Sierra Endocrine Associates
2019 Endocrine and Diabetes Symposium for Primary Care Providers Osteoporosis Case Studies Joseph B Hawkins, Jr., MD, FACE Assistant Clinical Professor of Medicine, UCSF Founder, Sierra Endocrine Associates
Osteoporosis Management in Older Adults
 Osteoporosis Management in Older Adults Angela M Cheung, MD, PhD, FRCPC, CCD Professor of Medicine, University of Toronto Disclosures Relationship with Commercial Entities: Honoraria from: Amgen, Eli Lilly,
Osteoporosis Management in Older Adults Angela M Cheung, MD, PhD, FRCPC, CCD Professor of Medicine, University of Toronto Disclosures Relationship with Commercial Entities: Honoraria from: Amgen, Eli Lilly,
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays. Suzanne Morin MD FRCP FACP McGill University May 2014
 Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Etiology. Presenter Disclosure Information. Epidemiology.
 12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis Update. Greg Summers Consultant Rheumatologist
 Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
SpongeBone Menopants*
 SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
Fracture=Bone Attack:
 Fracture=Bone Attack: Linking Hip Fractures to Osteoporosis Care Angela M. Cheung, MD, PhD, FRCPC Professor of Medicine, University of Toronto Potential Conflicts of Interests Industry Grants (to UHN)
Fracture=Bone Attack: Linking Hip Fractures to Osteoporosis Care Angela M. Cheung, MD, PhD, FRCPC Professor of Medicine, University of Toronto Potential Conflicts of Interests Industry Grants (to UHN)
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Osteoporosis Agents Drug Class Prior Authorization Protocol
 Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
Kristen M. Nebel, DO PENN/ LGHP Geriatrics. Temple Family Medicine Review
 Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
An Update on Osteoporosis Treatments
 An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
Monitoring Osteoporosis Therapy
 Monitoring Osteoporosis Therapy SUZANNE MORIN DEPT OF MEDICINE, DIVISION OF GENERAL INTERNAL MEDICINE, MUHC CENTRE FOR OUTCOMES RESEARCH AND EVALUATION, RI MUHC November 2017 Conflict of Interest Disclosures
Monitoring Osteoporosis Therapy SUZANNE MORIN DEPT OF MEDICINE, DIVISION OF GENERAL INTERNAL MEDICINE, MUHC CENTRE FOR OUTCOMES RESEARCH AND EVALUATION, RI MUHC November 2017 Conflict of Interest Disclosures
Page 1. Updates in Osteoporosis. I have no conflicts of interest. What is osteoporosis? What s New in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Osteoporosis Management
 Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Disclosures. Diagnostic Challenges in Osteoporosis: Whom To Treat 9/25/2014
 Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
Update on Osteoporosis 2016
 WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Assessment and Treatment of Osteoporosis Professor T.Masud
 Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Definition. Presenter Disclosure Information.
 4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment. William D. Leslie, MD MSc FRCPC
 Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
The Bare Bones of Osteoporosis. Wendy Rosenthal, PharmD
 The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Hot Topics in Osteoporosis and Fracture Prevention
 Hot Topics in Osteoporosis and Fracture Prevention Sid Feldman, MD CCFP (COE) FCFP Sandra Kim, MD, FRCPC November 15, 2018 Family Medicine Forum, Toronto Faculty/Presenter Disclosure Faculty: Sid Feldman
Hot Topics in Osteoporosis and Fracture Prevention Sid Feldman, MD CCFP (COE) FCFP Sandra Kim, MD, FRCPC November 15, 2018 Family Medicine Forum, Toronto Faculty/Presenter Disclosure Faculty: Sid Feldman
Osteoporosis. Treatment of a Silently Developing Disease
 Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Osteoporosis Update. Case 2. Case 1: Monday morning, 8:15
 Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017
 Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
Page 1. Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Updates in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Men and Osteoporosis So you think that it can t happen to you
 Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Screening Guidelines: Women
 The Situation 1 in 2 postmenopausal women and 1 in 5 older men will have an osteoporosis-related fracture in their lifetimes Osteoporosis Definition NIH Consensus Conference A skeletal disorder characterized
The Situation 1 in 2 postmenopausal women and 1 in 5 older men will have an osteoporosis-related fracture in their lifetimes Osteoporosis Definition NIH Consensus Conference A skeletal disorder characterized
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital
 Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
A Review of Bone Health Issues in Oncology
 A Review of Bone Health Issues in Oncology David L. Kendler MD FRCPC CCD Professor of Medicine (Endocrinology) University of British Columbia Vancouver Canada Disclosures David Kendler has received research
A Review of Bone Health Issues in Oncology David L. Kendler MD FRCPC CCD Professor of Medicine (Endocrinology) University of British Columbia Vancouver Canada Disclosures David Kendler has received research
Osteoporosis Treatment Overview. Colton Larson RFUMS October 26, 2018
 Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in ? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Overview. Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases. People Centred Positive Compassion Excellence
 Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Osteoporosis update. Dr. Claire Vandevelde Consultant Rheumatologist, LTHT
 Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
Osteoporosis in Men. CME Away India & Sri Lanka March 23 - April 7, 2018
 Osteoporosis in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Osteoporosis in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Chau Nguyen, D.O. Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences
 Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
Pharmacy Management Drug Policy
 Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Osteoporosis in Men Wendy Rosenthal PharmD. This program has been brought to you by PharmCon
 Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
Breast Cancer and Bone Loss. One in seven women will develop breast cancer during a lifetime
 Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Advanced medicine conference. Monday 20 Tuesday 21 June 2016
 Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
8/6/2018. Glucocorticoid induced osteoporosis: overlooked and undertreated? Disclosure. Objectives. Overview
 Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
11/4/2018. Osteoporosis Update. ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East. No disclosures.
 Osteoporosis Update ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East No disclosures. 1 Goals Review screening recommendations and workup of secondary causes
Osteoporosis Update ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East No disclosures. 1 Goals Review screening recommendations and workup of secondary causes
Using the FRAX Tool. Osteoporosis Definition
 How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
Differentiating Pharmacological Therapies for Osteoporosis
 Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
AACE/ACE Osteoporosis Treatment Decision Tool
 AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
Osteoporosis - New Guidelines. Michelle Glass B.Sc. (Pharm) June 15, 2011
 June 15, 2011") Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Page 1. New Developments in Osteoporosis. What s New in Osteoporosis
 New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
2017 Santa Fe Bone Symposium McClung
 217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
BREAST CANCER AND BONE HEALTH
 BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
Practical Management Of Osteoporosis
 Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Guideline for the investigation and management of osteoporosis. for hospitals and General Practice
 Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Page 1. Current and Emerging Strategies What s New in Osteoporosis. Osteoporosis. What is Osteoporosis? Traditional Risk Factors for Fracture
 Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Objectives: What is Osteoporosis 10/8/2015. Bone Health/ Osteoporosis: BASICS OF SCREENING, INTERPRETING, AND TREATING
 Bone Health/ Osteoporosis: BASICS OF SCREENING, INTERPRETING, AND TREATING TIFFANY PAUL, APN, CNP, CCD Objectives: Review the diagnosis of Osteoporosis Describe the basics of a bone density exam Identify
Bone Health/ Osteoporosis: BASICS OF SCREENING, INTERPRETING, AND TREATING TIFFANY PAUL, APN, CNP, CCD Objectives: Review the diagnosis of Osteoporosis Describe the basics of a bone density exam Identify
Beyond the Break. After Breast Cancer: Osteoporosis in Survivorship. Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO
 FCFP Regional Primary Care Lead CCO") Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
Bone Densitometry Pathway
 Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Fragile Bones and how to recognise them. Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey
 Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
OSTEOPOROSIS AND WHAT TO DO AFTER A VERTEBRAL FRACTURE. Lydia Au Geriatrics Ng Teng Fong Hospital
 OSTEOPOROSIS AND WHAT TO DO AFTER A VERTEBRAL FRACTURE Lydia Au Geriatrics Ng Teng Fong Hospital LET S START WITH WHAT YOU WANT TO KNOW AND DO WITH A VERT FRACTURE Vertebral fractures Most common (550K
OSTEOPOROSIS AND WHAT TO DO AFTER A VERTEBRAL FRACTURE Lydia Au Geriatrics Ng Teng Fong Hospital LET S START WITH WHAT YOU WANT TO KNOW AND DO WITH A VERT FRACTURE Vertebral fractures Most common (550K
ACP Colorado-Evidence Based Management of Osteoporosis
 ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
Skeletal Manifestations
 Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
NEW HORIZONS IN OSTEOPOROSIS THERAPY. Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN
 NEW HORIZONS IN OSTEOPOROSIS THERAPY Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN DISCLOSURES SUNDEEP KHOSLA, M.D. Investigator-initiated grant Merck No non-fda approved recommendations RISK ASSESSMENT
NEW HORIZONS IN OSTEOPOROSIS THERAPY Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN DISCLOSURES SUNDEEP KHOSLA, M.D. Investigator-initiated grant Merck No non-fda approved recommendations RISK ASSESSMENT
Optimizing Osteoporosis Management Dr. Philip A. Baer Seacourses Asia CME December 2017
 Optimizing Osteoporosis Management Dr. Philip A. Baer Seacourses Asia CME December 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Optimizing Osteoporosis Management Dr. Philip A. Baer Seacourses Asia CME December 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
DISCLAIMER DO NOT DISTRIBUTE
 DISCLAIMER The information contained in this presentation is not intended as a substitute for professional medical advice, diagnosis, or treatment. It is provided for educational purposes only. You assume
DISCLAIMER The information contained in this presentation is not intended as a substitute for professional medical advice, diagnosis, or treatment. It is provided for educational purposes only. You assume
Osteoporosis Clinical Guideline. Rheumatology January 2017
 Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
nogg Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK
 nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
Aromatase Inhibitors & Osteoporosis
 Aromatase Inhibitors & Osteoporosis Miss Sarah Horn Consultant Oncoplastic Breast Surgeon April 2018 Aims Role of Aromatase Inhibitors (AI) in breast cancer treatment AI s effects on bone health Bone health
Aromatase Inhibitors & Osteoporosis Miss Sarah Horn Consultant Oncoplastic Breast Surgeon April 2018 Aims Role of Aromatase Inhibitors (AI) in breast cancer treatment AI s effects on bone health Bone health
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
Long-term Osteoporosis Therapy What To Do After 5 Years?
 Long-term Osteoporosis Therapy What To Do After 5 Years? Developing a Long-term Management Plan North American Menopause Society Philadelphia, PA October 11, 2017 Michael R. McClung, MD, FACP Institute
Long-term Osteoporosis Therapy What To Do After 5 Years? Developing a Long-term Management Plan North American Menopause Society Philadelphia, PA October 11, 2017 Michael R. McClung, MD, FACP Institute
Osteoporosis. When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of.
 Osteoporosis When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of. Osteoblasts by definition are those cells present in the bone and are involved
Osteoporosis When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of. Osteoblasts by definition are those cells present in the bone and are involved
OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT
 AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT Dolores Shoback, MD Professor of Medicine, UCSF San Francisco VA Medical Center July 16, 21 ~ QUESTIONS ~ Who should receive therapy to prevent fractures?
AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT Dolores Shoback, MD Professor of Medicine, UCSF San Francisco VA Medical Center July 16, 21 ~ QUESTIONS ~ Who should receive therapy to prevent fractures?
Talking to patients with osteoporosis about initiating therapy
 Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Bone Health for Women: Current Research, Initiatives and Recommendations
 Page 1 BONE HEALTH FOR WOMEN: CURRENT RESEARCH, INITIATIVES AND RECOMMENDATIONS Dr. Melissa Kagarise This program has been brought to you by PharmCon PharmCon is accredited by the Accreditation Council
Page 1 BONE HEALTH FOR WOMEN: CURRENT RESEARCH, INITIATIVES AND RECOMMENDATIONS Dr. Melissa Kagarise This program has been brought to you by PharmCon PharmCon is accredited by the Accreditation Council
Osteoporosis. Open Access. John A. Kanis. Diseases, University of Sheffield, UK
 Journal of Medical Sciences (2010); 3(3): 00-00 Review Article Osteoporosis Open Access John A. Kanis WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK incorporated into
Journal of Medical Sciences (2010); 3(3): 00-00 Review Article Osteoporosis Open Access John A. Kanis WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK incorporated into
Calcium, Vitamin D and Bisphosphonates: Disclosures. Benefits, Risks and Drug Holiday. Calcium YES or NO? Calcium Bad News!!
 Calcium, Vitamin D and Bisphosphonates: Benefits, Risks and Drug Holiday Disclosures I am disclosing financial relationships as follows: Global Advisory Boards: Amgen, Lilly, Merck, Novartis Research grants:
Calcium, Vitamin D and Bisphosphonates: Benefits, Risks and Drug Holiday Disclosures I am disclosing financial relationships as follows: Global Advisory Boards: Amgen, Lilly, Merck, Novartis Research grants:
Prevention And Treatment. References. Vertebral Fracture Management KEY POINTS
 OSTEOPOROSISLoren M. Wilkerson, MD; Kenneth W. Lyles, MD, AGSF Key Points Epidemiology And Impact Bone Remodeling And Bone Loss.. Pathogenesis Diagnosis And Prediction Of Fr.. Prevention And Treatment
OSTEOPOROSISLoren M. Wilkerson, MD; Kenneth W. Lyles, MD, AGSF Key Points Epidemiology And Impact Bone Remodeling And Bone Loss.. Pathogenesis Diagnosis And Prediction Of Fr.. Prevention And Treatment
Name of Policy: Zoledronic Acid (Reclast ) Injection
 Injection") Name of Policy: Zoledronic Acid (Reclast ) Injection Policy #: 355 Latest Review Date: May 2011 Category: Pharmacy Policy Grade: Active Policy but no longer scheduled for regular literature reviews and
Name of Policy: Zoledronic Acid (Reclast ) Injection Policy #: 355 Latest Review Date: May 2011 Category: Pharmacy Policy Grade: Active Policy but no longer scheduled for regular literature reviews and