Strategic Framework for Kidney Care in Cheshire and Merseyside:
|
|
|
- Lenard Hicks
- 5 years ago
- Views:
Transcription
1 Cheshire and Merseyside Kidney Care Network Strategic Framework for Kidney Care in Cheshire and Merseyside: July 2008 FINAL VERSION Approved by Cheshire & Merseyside DoCs 19 th September 2008
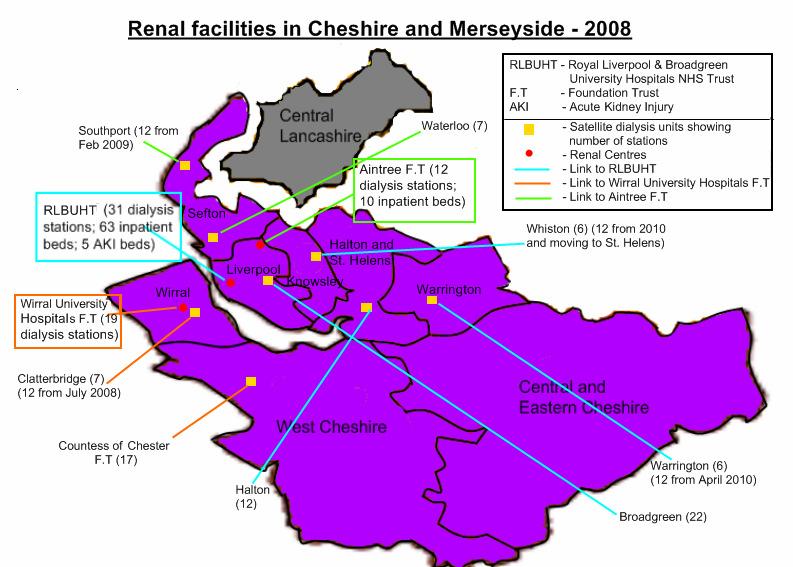
2 CONTENTS Foreword Executive Summary The Next Five Years: A Patients Perspective Renal Facilities in Cheshire and Merseyside 2008 Page i ii iv v SECTION 1 SECTION Guiding Principles and Scope of the Framework What is kidney failure? What services are involved in renal care? Renal service descriptions Principles of commissioning National drivers, guidelines and policies Renal National Service Framework Local drivers Chronic Kidney Disease (CKD) and General Nephrology Transplantation Acute Kidney Injury (Acute Renal failure) Dialysis access surgery Dialysis Active Renal Supportive Care Health needs assessment and demography Demography Patient Acceptance (Incidence) and Prevalence rates Current renal facilities Patient and carer involvement in planning Renal Services Monitoring of the service Chronic kidney disease (CKD) and general nephrology Anaemia management Outpatient services Psychological and social support General Nephrology Transplantation Transplant waiting list Organ donation rates and registered donors Innovations in transplantation The transplantation laboratory Post transplant care Transplantation demand forecast Acute Kidney Injury (acute renal failure) Dialysis Access Surgery Establishing and maintaining dialysis access Dialysis Development of home haemodialysis and peritoneal dialysis services 31
3 SECTION Expansion of haemodialysis capacity Innovations in dialysis Services for patients with blood borne viruses (BBVs) Renal transport Dialysis demand forecast Rationale for future capacity planning Haemodialysis capacity plan ( ) Satellite dialysis unit developments beyond April Active Renal Supportive care (conservative management, palliative care and end of life care) The next steps Summary Key reference documents Acknowledgements Glossary of terms 49 Page SECTION 4: APPENDICES 1 Kidney Care Network: Terms of reference and membership 51 2 Renal NSF Part 1 Standards and Markers of Good Practice 55 3 Renal NSF Part 2 Quality Requirements and Markers of Good Practice 57 4 Renal Services descriptions for non renal specialists 59 5 National initiatives and key strategies impacting on renal services 61 6 Further information and resources 64
4 FOREWORD Renal dialysis and transplantation services across Cheshire and Merseyside have been developing over the past few years in response to inevitable pressures facing the service. These pressures include an increasingly older renal patient population with more comorbidities, such as diabetes and coronary heart disease, and the need to enhance the choices available to renal patients in the care they receive. Equity of access and consistency in quality are two of the key drivers in this document. The Renal National Service Framework (NSF) 1 provides a clear guide on standards and is therefore the basis for all service developments across Cheshire and Merseyside and the North West Strategic Health Authority. This Strategic Framework for Kidney Care in Cheshire and Merseyside is a five year plan that builds on the existing strategy and uses the NSF Standards in reviewing local service delivery and in developing a clear improvement plan to take the service through to the end of the NSF implementation timescales. The Cheshire and Merseyside Kidney Care Network (Appendix 1) has a clear vision for renal care. A fundamental aspect of this is the commitment to place the patient and their carers at the centre of all service planning, in order that the quality of care will be focussed on patient outcome. This Strategic Framework outlines the key issues facing renal services and identifies actions for addressing these concerns. It is recognised that all health care sectors need to be involved to provide a high quality pathway of renal care; in primary care where early diagnosis, management and prompt referral to secondary or tertiary care impacts on outcome; in secondary and tertiary care where the joint management of chronic kidney disease, co-morbidities, and all aspects of established renal disease are crucially important in providing good quality of care; and finally end of life care which requires close collaboration across the healthcare sectors, and the involvement of other agencies. The Framework is population based for each provider, and includes in and out flows to and from the area to account for patients who receive their care in a location other than that in which they live. Work with healthcare professionals and patients in Cheshire and Merseyside will be undertaken as part of the process of implementation. The Framework includes core principles for the commissioning of renal services; the projected growth in the number of patients on renal replacement therapy programmes based on a health needs assessment; and the planning assumptions which will deliver those programmes necessary to provide a quality service for patients. The Kidney Care Network is totally committed to improving patient care and fully supports the aspiration of making the provision of renal care in the North West a world class service. This document aims to outline clearly the national requirements for renal services together with the local response required to meet these standards. On behalf of the Cheshire and Merseyside Renal Network, we look forward to working with the North West Specialised Commissioning Team, local Primary Care Trusts (PCTs), providers of primary, secondary and tertiary care and patient representatives, to ensure local services are responsive, effective and above all provide the best possible care for people with kidney disease. Helen Bellairs Chair Kidney Care Network i
5 EXECUTIVE SUMMARY Overview Chronic Kidney Disease (CKD) is common, harmful and treatable. Using research statistics, there are potentially more than 650,000 people within the catchment population of Cheshire and Merseyside renal services living with some form of renal impairment. This also means there is the potential to delay progression of renal disease in more than 450,000 people by managing their disease in primary care to prevent development of established renal disease. The Renal National Service Framework (NSF) 1 is a ten year plan going through to 2014 and provides a clear guide on standards. This Strategic Framework for Kidney Care in Cheshire and Merseyside is a five year plan and uses the NSF Standards in reviewing local service delivery and in developing a clear improvement plan to take the service through to near the end of the NSF implementation timescales. This Strategic Framework for kidney Care in Cheshire and Merseyside includes core principles for the commissioning of renal services; the projected growth in the number of patients on renal replacement therapy programmes based on a health needs assessment; and the planning assumptions which will deliver those programmes necessary to provide a quality service for patients. Patients and their carers are the focus of this document and they remain at the centre of planning renal services in Cheshire and Merseyside. Kidney Function and Disease Progression Kidneys have five main functions. Removing toxic waste from the blood and excess water from the body: helping to control blood pressure and the manufacture of red blood cells: and helping to keep bones strong and healthy by maintaining the balance of calcium and phosphate. With kidney damage all these functions are either temporarily or permanently compromised. Most people may only start to feel unwell when their kidney function is reduced to less than 30% of normal levels. By 15% the point they begin to be very symptomatic, much of the damage done to the kidneys is irreversible. The only options available to patients with established renal disease are dialysis, either peritoneal dialysis or haemodialysis, transplantation, or active renal supportive care (palliative care / conservative management and end of life care). Key issues facing local services The number of patients in Cheshire and Merseyside requiring dialysis is projected to increase by more than 300 in the next 5 years. The local challenges will involve provision of quality care for these patients by ensuring the timely opening of the planned new dialysis units, increasing patient choice, increasing the number of transplants and liaising with primary care to identify patients earlier in their disease pathway. ii
6 Key Priorities for Action The importance of strengthening links with primary care to manage effectively the projected increase in the number of renal patients is unmistakably recognised. Transplantation is the best form of renal replacement therapy for those patients who are clinically suitable. The case for increasing the number of transplants is indisputable. Local implementation of the recommendations from Organs for Transplant: A Report from the Organ Donation Taskforce 2 will be critical to the success of increasing the number of transplants and they are fully supported by this Strategic Framework. Further work will be essential to ensure there is capacity to cope with the projected increase in the number of transplants and for the local followup of transplanted patients. Accreditation of the Transplantation Laboratory Service must be achieved without delay. A significant number of patients are receiving suboptimal haemodialysis care due to constraints on the existing facilities. Plans are in place to provide 53 more haemodialysis station to address this quality of care issue. It will be essential to ensure progress of these plans and to monitor future requirements. There is a need to progress high quality peritoneal dialysis and home haemodialysis as options for patient choice. Reliable and effective patient transport for renal haemodialysis patients is essential to their overall well being. Work will be done to improve current systems. It is essential to develop active renal supportive care for patients with established renal disease who choose not to receive dialysis (which may include some patients whose transplanted organs are failing), or for those patients currently receiving treatment who wish to stop and for those for whom it is no longer clinically appropriate. The Next Steps Work with healthcare professionals and patients in Cheshire and Merseyside will be undertaken as part of the process of implementing the recommendations from this document. An agreed programme of reviews on different aspects of the service will be developed, to ensure progress is being made and that the plans being implemented are bringing the desired improvement. Data collection systems will be established to constantly monitor developments and national statistics and information will be examined on a regular basis to check progress. There will be regular reporting to the Directors of Commissioning and the North West Specialised Commissioning Group. iii
7 THE NEXT FIVE YEARS: A PATIENTS PERSPECTIVE On behalf of the patients, families and carers whom we represent, we welcome this opportunity to express our thoughts about the future direction of the renal service in the North West. For more than a decade, (starting with the reorganisation of renal services in Greater Manchester, right through to the ongoing ISTC programme to increase haemodialysis capacity in Cheshire & Merseyside), we have had real, as opposed to rhetorical, patient involvement in planning and monitoring the regional renal service. Such involvement carries with it a responsibility on our part to act in a committed and professional manner, and it automatically raises expectations in the patient community, (sometimes unrealistically) as to what can be achieved. Whilst recognising the realities of limited available resources, be they financial, workforce or otherwise, we believe strongly that we should set challenging targets for the next five years, and examine different and innovative ways of delivering the service. It should never be forgotten that the overall strategy will be judged by patients on their individual experience of what is provided, especially when it affects their quality of life. Being a renal patient is much more than a clinical experience; it impacts on all aspects of the lives of not only the patients themselves, but also their immediate family and those who care for them. Hours wasted waiting for transport, an inability to access the full range of multidisciplinary staff, a lack of spare capacity to enable patients to dialyse away from home for employment, family, or holiday purposes, and so on, matter as much as clinical excellence to those directly affected. From a patients perspective there is nothing to disagree with in the contents of this strategy document. Given its endpoint almost coincides with the date by which the implementation of all the standards and markers of good practice contained in the renal National Service Framework should be met, we believe that ensuring such implementation is achieved must be a priority. Linked to that, increased capacity to be able to offer all suitable modalities of treatment to all patients throughout the region has to be accomplished. That should include developing the availability of treatments such as daily haemodialysis, implementing the recommendations contained in the recent Organ Donor Task Force report 2, building on the primary care renal Quality Outcomes Framework (QOF) to reduce further the number of patients crash landing into the system, and providing comprehensive and appropriate end of life care for patients and their loved ones. We do not doubt the enormity of the challenge we face, but take heart from the very real progress made in recent years, and will do what we can to help meet and overcome the difficulties that lie ahead. Dennis Crane North Region Advocacy Officer National Kidney Federation iv
8 v
9 SECTION 1 Section 1 sets out the background to the document explaining about renal disease, the current position both nationally and locally, the drivers for improvement in renal care and the involvement of patients and carers in the planning and delivery of the service. 1.1 GUIDING PRINCIPLES AND SCOPE OF THE FRAMEWORK The guiding principles in developing renal and transplant care across Cheshire and Merseyside and the North West are that: patients and their carers will be the focus, and be at the centre, of all service planning. there will be equity of access to services for all patients. wherever possible, and appropriate, services will be developed close to the patient s home. patients will have choices in the care they receive unless clinically contraindicated, and such choices may change over time due to changing circumstances. there will be equitable standards of care provided by all renal service providers. the standards and markers of good practice outlined within the Renal National Service Framework 1, together with other relevant guidance, (eg Operating Framework 2008/09, NICE guidelines) will form the basis of all future plans for the service. the care provided for patients will be holistic, personalised, effective and safe. This Framework is based upon the catchment population of the Cheshire and Merseyside adult renal service providers as detailed in section Some Central and Eastern Cheshire residents receive their care through the Greater Manchester Renal Network and the strategic developments for that area are addressed in a separate document. The performance monitoring and review of equity of access to renal care will be undertaken by the North West Specialised Commissioning Team on behalf of the PCTs. This Framework does however highlight the needs of the inflow population into Cheshire and Merseyside including patients from the West Lancashire area, the Isle of Man and parts of North Wales. The Framework is a five year plan, taking the service through to the end of the timescales for implementation of the standards, quality requirements and markers of good practice in the Renal National Service Framework 1 (NSF), and sets out the key planning assumptions for the recommendations made and will be reviewed on an annual basis in the light of actual service changes and other relevant factors. Renal services for children will be addressed within the North West Paediatric Partnership Board and are therefore not detailed within this document. However, the transition of children into the adult service crosses both areas of work and is covered in the Renal NSF 1. A forthcoming report from two Renal Action Learning Sets will deal with this topic and recommendations are made at the end of this document with regard to liaison between paediatric and adult renal services. 1
10 1.2 WHAT IS KIDNEY FAILURE? Kidney failure can occur for several reasons some patients develop kidney failure from hypertension, diabetes, autoimmune or genetic abnormalities; some from early damage to the kidneys in childhood; and others due to sudden damage, perhaps as a result of trauma, but in many cases the cause is not known. Figure 1 identifies the primary renal diagnosis in new patients across England and Wales in 2005 (Source: UK Renal Registry 3 ). Figure 1: Percentage distribution of primary renal diagnosis in 2005 incident cohort Polycystic kidney 6.1% Hypertension 4.8% Reno-vascular Disease 7.6% Other 15.2% Diabetes 19.8% Unknown Aetiology 28.0% Glomerulonephritis 10.3% Pyelonephritis 8.2% Unknown Aetiology Glomerulonephritis Pyelonephritis Diabetes Reno-vascular Disease Hypertension Polycystic kidney Other Kidneys have five main functions. They are responsible for removing toxic waste from the blood and excess water from the body, both via urine. The kidneys also help to control blood pressure: help to control the manufacture of red blood cells by making erythropoietin (EPO): and help to keep bones strong and healthy by maintaining the balance of calcium and phosphate. With kidney damage all these functions are either temporarily or permanently compromised. Patients with progressive renal disease may feel perfectly well for months or years without knowing they have any problems. However, relatively simple urine analysis and laboratory tests would indicate that their kidney function was deteriorating with a decrease in, for example, their egfr (estimated Glomerular Filtration Rate). Referral based on the stage of chronic kidney disease (CKD) is now thought to be most appropriate. These stages are shown in the table below using egfr as the clinical indicator of kidney disease: Table 1: UK Prevalence of Chronic Kidney Disease (CKD) Stage egfr (ml / min) UK prevalence from NeoErica study* 1 >90 (normal GFR) 3.31% (mild impairment) 14.43% (moderate 7.39% impairment) (severe 0.29% impairment) 5 <15 (established renal failure) 0.04% n.b. 5 indicating end stage renal disease. *Ref: PE Stevens et al 4 egfr = estimated Glomerular Filtration Rate this indicates how well the kidneys are functioning with Stage Most people may only start to feel unwell when their kidney function is reduced to less than 30% of normal levels. By 15% the point they begin to be very symptomatic, much of the damage done to the kidneys is irreversible. 2
11 The only options available to patients with established renal disease are dialysis and transplantation, (jointly referred to as renal replacement therapy) or active renal supportive care (palliative care / conservative management and end of life care). Using the percentage figures from Table1 and the catchment population figures from Table 4 (p17), there are potentially more than 650,000 people within the Cheshire and Merseyside catchment population of renal services living with some form of renal impairment. This also means there is the potential to delay progression of renal disease in more than 450,000 people by managing their disease in primary care to prevent development of established renal disease. Others patients will, regrettably, have a continued decline in kidney function until further treatment options will need to be considered. Figure 2 illustrates prevalence of patients nationally with CKD stage 3-5 by age group and highlights that renal disease is most common amongst older people many of whom will have co-morbidities. It is also known that CKD is approximately four times more prevalent in the Asian and Afro-Caribbean populations. Figure 2: Prevalence of CKD 3-5 in UK from NeoErica study Percentage of population Males w ith CKD 3-5 Females w ith CKD Overall Age groups 1.3 WHAT SERVICES ARE INVOLVED IN RENAL CARE? Renal care spans many professional groups and healthcare sectors, with different members of the multi-professional team treating various stages of the patient journey. At primary care level, GPs, dieticians, nurses and other professionals have a crucial role to play in screening for early stages of Chronic Kidney Disease (CKD). Primary care staff are also crucial in identifying those patients at risk of renal disease as early as possible and, where appropriate, referring them into specialist nephrology services for diagnosis. The recent Department of Health initiative to screen people between the ages of for vascular disease will concurrently highlight those at risk of renal disease (see section 1.8). Secondary care also enables patients to be cared for in their District General Hospitals. Some elements of chronic kidney disease management such as blood pressure control and cardio vascular risk factor management can be undertaken mainly in primary care. Other 3
12 complications of CKD such as anaemia, bone disease and acidosis and also preparation for dialysis or transplantation will occur in the secondary care sector. Issues such as end of life care may be shared across both primary and secondary health and social care and voluntary, (e.g. hospice care), sectors. Links with other clinical specialities such as diabetes and cardiac services are also essential in the provision of holistic care. In specialist renal services, a wide range of professionals are involved in providing care including medical staff, nurses, pharmacists, dieticians, renal technicians, managers, social workers, occupational therapists, physiotherapists and psychologists. Figure 3, adapted from the Renal NSF 1, illustrates the renal patient pathway through services and outlines the options available to patients once they reach established renal failure and require renal replacement therapy (dialysis or transplantation). Figure 3: The care pathway for renal replacement therapy Patient Important at all stages of the care pathway: Unplanned or emergency presentation Planned referral from primary care Planned referral from other specialty (eg cardiology, elderly, diabetes) Quality of life Nephrology assessment and review Shared information Pre- renal replacement therapy programme with multidisciplinary review Choice for patients Renal replacement therapy treatment choices Continuing education Peritoneal access surgery Vascular access surgery Preemptive transplant Clinical care Nutritional support Medicines management Peritoneal or Haemodialysis Transplantation Treatment with respect and dignity Active renal supportive care and end of life care Failing transplant Psychological and social support for patients and carers 4
13 Early identification of kidney disease can greatly increase the success of managing the disease and slowing (or even stopping) the progression to established renal disease. The introduction of CKD into the Quality Outcomes Framework (QOF) in 2006 has facilitated the identification and management of CKD patients in primary care. Many patients with CKD will not develop progressive renal failure and may never be referred to a renal unit. Established renal disease is a long term condition like diabetes, and many patients within renal services also have other medical conditions. The challenge in this framework is not only to identify renal specific issues but also to address the need for synergy with other key service areas, particularly coronary heart disease and diabetes care. This interaction may include the linking of IT systems and registers, shared care plans, an integrated workforce and clinical targets. In addition, there is a direct link with non NHS agencies such as social services, transport providers, hospices etc, who provide essential services to renal patients throughout the care pathway. One way to improve the synergy and interaction between other service areas and non NHS agencies would be to consider migrating the renal care pathway into the Map of Medicine The map is a web-based visual representation of evidencebased patient care journeys currently covering 28 medical specialties and 390 pathways. As healthcare provision becomes much more specialised the need to plan and then benchmark clinical practice against national standards whilst incorporating local intricacies is key. The Map provides a visual framework for clinical knowledge that can be customised to meet local needs. All NHS staff in England and Wales can now access the Map of Medicine s national care pathways and quickly view the latest evidence, including NICE guidelines. Currently nephrologists in Wales, for example, are using the map as a way of delivering clinical information to primary care in order to reduce the number of people presenting to secondary care with late stages of chronic kidney disease. The Map of Medicine clinical pathways have now been made available to patients via the NHS Choices website Renal Service Descriptions For those patients who do progress to CKD stage 5, they will need renal replacement therapy (RRT) in the form of dialysis (either peritoneal dialysis or haemodialysis) or transplantation. Some patients will choose not to have RRT and these patients will need active renal supportive care and eventually end of life palliative care. Transplantation is the best form of RRT for those patients who are clinically suitable (approximately 40%), and a pre-emptive transplant (ie, one carried out before dialysis is required) is considered the optimum. Organs can be donated from a living or deceased donor. It is important to recognise that transplants may fail, even after many years, and these patients will need to return to dialysis. Patients may receive a kidney or, for some patients with diabetes, a kidney and pancreas. Pancreatic transplants will cure diabetes which may be the cause of the renal failure. By doing a simultaneous kidney and pancreas transplant both the diabetes and the renal disease can be treated. Dialysis can be provided either as peritoneal dialysis (PD) or haemodialysis. 5
. Both of these forms of treatment can be performed by the patient at home and involve draining bags of special fluid into and out of the peritoneal cavity.")
14 Peritoneal dialysis is carried out through a catheter inserted into the patient s peritoneal cavity and can be in the form of continuous ambulatory peritoneal dialysis (CAPD) or automated peritoneal dialysis (APD). Both of these forms of treatment can be performed by the patient at home and involve draining bags of special fluid into and out of the peritoneal cavity. These exchanges of bags are carried out 3-4 times a day in the case of CAPD or 3-4 times overnight for APD using a machine whilst the patient is asleep. Automated peritoneal dialysis can be organised as an assisted process (AAPD) for patients who do not have the dexterity to manipulate the machine. Haemodialysis purifies the blood outside the body by passing it through a filter called the dialyser. The dialyser is fitted to a machine which pumps the patient s blood through the filter and controls the whole process. A haemodialysis session will normally last for 3-5 hours and in most cases takes place 3 times a week. Patients who are clinically stable can dialyse in a satellite dialysis unit away from the renal centre, usually closer to where they live, or at home. Those patients who require extra care will need to dialyse in the renal centre. Dialysis access surgery is needed by both PD and haemodialysis patients in preparation for treatment. This will involve insertion of the catheter for PD or formation of a fistula for haemodialysis. Both of these procedures need to be performed in a timely fashion negating the requirement for any temporary access which increases morbidity and chances of infection. Active renal supportive care, previously referred to as conservative management, palliative care and end of life care, will be needed by patients who choose not to have RRT, or who cannot continue it for clinical reasons. It is important to stress that this does not mean no treatment but supportive treatment and will mostly be carried out in primary care with close liaison between renal staff and primary care staff. The crucial factor in the care pathway is that patients should be allowed to make an informed choice of treatment that can be reviewed at any time. 1.4 PRINCIPLES OF COMMISSIONING The development of commissioners as leaders of change has been progressing over a number of years. The core components of commissioning are illustrated in Figure 4: The National Review of Commissioning Arrangements for Specialised Services (Carter Report) 5 May 2006, looked at Figure 4: Core components of commissioning ways to improve the commissioning of specialised services to make the arrangements more robust and consistent and to ensure a good fit with the wider NHS system reform programme, the new organisational infrastructure for commissioning by the NHS and the changing role of the Department of Health (DH). 6
15 The Report made 32 recommendations including the establishing of a National Specialised Commissioning Group (formerly NSCAG) and 10 Specialised Commissioning Groups coterminous with the SHAs and supported by dedicated specialised commissioning teams (SCTs). The North West Specialised Commissioning Team (NWSCT) has delegated authority to act on behalf of 24 North West PCTs and commissions all 35+ specialised services including renal and transplant care. The NWSCT has a lead commissioner for renal services who will play an active role on the Kidney Care Network Group. The NWSCT will also be working closely with PCT commissioners in developing effective commissioning strategies across the patient pathway particularly focussed on vascular risk assessment and early kidney disease management. 1.5 NATIONAL DRIVERS, GUIDELINES AND POLICIES Over the past few years, the profile of renal services has been raised significantly and renal care is designated as one of eight national priorities within specialised services. Renal care is a relatively young discipline and only began to be provided as a mainstream service in the late 1960s. Since this time, significant advances have been made in the care that can be offered. As long ago as 1991, a National Renal Review was commissioned and this highlighted the fact that there were major gaps in renal service provision. It was noted that there was a significant shortfall in renal services and those services which did exist were patchy and uneven. Referral of patients was often late in their renal disease thereby reducing the options for treatment. There was also little patient choice in the modality of care received or in the location and timing of dialysis. Disappointingly, these issues are still relevant today. The findings of the National Renal Review, together with an ever-increasing number of patients presenting with established renal disease, have resulted in several key national initiatives being developed. These are described in Appendix 5 together with other key strategies, policies and guidelines which will impact upon renal services. Of particular importance is the Renal National Service Framework 1 (see 1.6 below), The Operating Framework for the NHS in England 2008/09 and the Report from the Organ Donor Taskforce The Operating Framework for 2008/09 states in commissioning for world-class health services, Specialised Commissioning Groups (SCGs) should pay particular attention to areas where significant increases in demand are likely to lead to pressure on services. For example, demand for renal replacement therapy (dialysis and transplantation) is projected to rise by around 5% per year until at least SCGs will wish to consider options for expanding the provision of satellite dialysis centres and offering more people the option of home dialysis as well as expanding main acute dialysis units. We know that demand for haemodialysis (as opposed to overall renal replacement therapy) is increasing at the even higher rate of 6-8% per annum. 7
16 The Report from the Organ Donor Taskforce 2 is discussed in more detail in section 2.2 but it makes 14 recommendations that are fully supported by this document and the Kidney Care Network. The Cheshire and Merseyside Kidney Care Network also recognises the importance of the new report from the North West Strategic Health Authority Healthier Horizons for the North West 6. The publication of this report in May 2008 marked the beginning of a three month period of discussion and engagement regarding the report s recommendations and commitments. The Cheshire and Merseyside Kidney Care Network fully supports the report and there is nothing in this Framework that conflicts with Healthier Horizons for the North West. 1.6 RENAL NATIONAL SERVICE FRAMEWORK 1 Renal services have become the focus of national attention in recent years with the publication of the Renal National Service Framework 1 (NSF). The NSF was published in two parts in January 2004 and February The Standards, Quality Requirements and Markers of Good Practice are detailed in Appendices 2 and 3. Part One of the NSF sets five standards and identifies 30 Markers of Good Practice and deals with Dialysis and Transplantation. Part One of the NSF had five actions to be achieved by Table 2 shows the current position with regards to these five actions in Cheshire and Merseyside. Table 2: Actions required from Part One of the NSF and current status for Cheshire and Merseyside Action to be achieved Use national data to support planning and to identify local priorities including the needs of black and minority ethnic (BME) groups. Continue to expand haemodialysis capacity Join the UK Renal Registry (RR) of the Renal Association and take part in national comparative audit. Implement NICE appraisal: assessment for home haemodialysis Implement NICE appraisal: immunosuppressive therapy Current position This Strategy uses national (e.g. Renal Registry, ONS) and local data to plan future services and accounts for the needs of BME groups Capacity has expanded over recent years and is an on going process. The renal centres in the conurbation submit data to the RR but this is not complete. Home haemodialysis is provided in the area and forms part of this planning document. The transplant unit has implemented the NICE guidelines. Part Two of the NSF sets out four Quality Requirements and 27 Markers of Good Practice dealing with chronic kidney disease, acute renal failure and end of life care (Appendix 3). Whilst the second part of the NSF does not have any specific actions to be achieved, the Quality Requirements and Markers of Good Practice are used in this document for planning purposes. 8
17 1.7 LOCAL DRIVERS Renal services within Cheshire and Merseyside have been one of the leaders in the development of renal satellite dialysis care. Effective relationships with private sector providers in the 1980s and 1990s have continued with the inclusion of Cheshire and Merseyside in the first national tender for independent sector provision of haemodialysis which was awarded to Fresenius Medical Care. This has meant that the provision of haemodialysis across the zone has been extensive and future plans are in place for new and refurbished units over the next two years. This has also meant that new patient acceptance rates are relatively good across Cheshire and Merseyside. The Transplant Unit takes patients from North Wales and the Isle of Man as well as from across Cheshire and Merseyside. Patients who need a pancreas transplant currently have to travel to Manchester, Birmingham or Oxford. The local drivers for improvements to the services are summarised below Chronic Kidney Disease (CKD) and General Nephrology A key theme running through the NSF is the importance of enhancing primary care in the early identification of renal patients, early referral to delay the progression of renal failure, and in the commissioning of integrated care across the patient pathway. Management of patients in primary care is at an early stage of development in Cheshire and Merseyside. Progressing this development will need education, training and closer liaison between primary and secondary care staff. There are insufficient specialist outpatient clinics in local District General Hospitals including transplant clinics and multi-professional low clearance clinics. Many patients have to travel into renal centres for outpatient appointments. The provision of psychological and social support to kidney patients and their carers is fundamental in a patient centred service. Patients often need access to advice on their benefit entitlement, support in psychological adjustment to their treatment options and regimes and help in taking control back in their lives whilst living with a chronic condition. Many patients suffer from depression and appropriate psychological support can greatly benefit them in managing their condition. Anaemia management (both the prescribing of iron and erythropoietin - EPO) is a key quality issue for renal patients who are often anaemic and is fundamental to the service. (The more familiar term, EPO, has been used in this document to represent all the Erythropoiesis Stimulating Agents now referred to as ESAs). Renal information systems must evolve and develop in line with the service expansion. In particular, it is a requirement of the NSF that units submit full data reports to the Renal Registry. Integrated IT systems enable comparative data to be collected but also facilitate the multi-professional way of working across the renal team. There is a need to ensure the Renal Registry submissions are accurate, reliable, timely and completed by all renal service providers and data used for monitoring and audit and comparison with national performance. The national Renal Services Information Implementation Strategy 7 was published in January 2004 and gives guidance on how the implementation of its recommendations will help deliver the NSF targets. 9
18 1.7.2 Transplantation Transplantation is the best form of renal replacement therapy for those patients who are clinically suitable. The procedure not only significantly increases the patients quality of life but is also highly cost effective. The case for increasing the number of transplants is indisputable. Raising the number of transplants can be achieved in a number of ways including the development of antibody incompatible transplants, a non-heart beating donor programme and increasing the number of live donor transplants. Expansion of the donor retrieval programme and increasing organ donation rates is essential if national targets are to be met and the number of transplants increased. Additional work is required to increase the number of registered organ donors across the whole of the North West. This work will need to address sensitive issues such as the high rates of relative refusals to organ donation and closer interaction with Intensive Care Unit (ICU) staff. Organs for Transplant: A Report from the Organ Donation Taskforce 2 deals with the points above and the recommendations from this report will be fully supported by this Cheshire and Merseyside Strategic Framework document. The Renal NSF 1 section on transplantation recommends that patients are placed on the transplant list at least six months before dialysis is due to commence. It also highlights the importance of giving patients information regarding transplantation in order for them to make informed choices and to ensure that the infrastructure of the service is sufficient to meet key quality standards. Tissue typing is a fundamental element of the transplant service as this ensures the transplant recipient receives the best-matched organ, thereby reducing the potential for organ rejection. Serious concerns have been raised regarding the transplantation laboratory service in Cheshire and Merseyside which is not accredited. This situation is not sustainable and the recent appointment of a consultant clinical scientist should be followed up to ensure accreditation is achieved without delay. Development of local transplant outpatient clinics closer to patients homes would ensure patients could be followed up on a regular basis, including a comprehensive annual review, which may in turn improve rates of compliance with the treatment regimen. Good IT links with the Transplant Centre would facilitate this expansion. The data from the UK Transplant Allocation Review has raised a number of points that are relevant to the transplant unit. The issues raised by the review, need to be followed up and monitored. Following the implementation of the Human Tissue Act, a national paired-donation scheme now exists. It is likely this will have an impact on the living donor programme, and has a major impact on the demands made on the transplantation laboratory. The transplant unit does not run a non heart-beating donor programme. This may be essential to increase the number of transplants undertaken if the new allocation scheme does not favour the Liverpool unit. 10
19 1.7.3 Acute Kidney Injury (Acute Renal Failure) Acute kidney injury is an abrupt decline in kidney function (within 48 hours) resulting from an injury causing a functional or structural change in the kidney. At present there is no specific therapy for AKI and the cornerstone of treatment is renal replacement therapy Dialysis Access Surgery Standard 3 in Part One of the Renal NSF 1 (Appendix 2) highlights the importance of good access surgery to support the dialysis programme. Haemodialysis patients who require vascular access should have this established six months before commencing dialysis and peritoneal dialysis patients have their catheters inserted four weeks before dialysis. A national dialysis access survey carried out by the UK Renal Registry 3 in 2005, showed that in reports from 62 of 72 renal centres only 31% of haemodialysis patients commenced treatment with definitive access. It is known that temporary access leads to increased morbidity and mortality, increased numbers of inpatient episodes, increased risk of infection and poorer outcomes. The Renal NSF 1 recommends that patients are prepared for dialysis for around one year. This requires patients to be prepared for dialysis access well in advance of the need for surgery in order to meet European standards for establishing permanent access prior to dialysis. The number of patients with arterio-venous fistulas should be around 80% and this is the case in a number of European countries (Germany 84%, Spain 82%). The UK has a rate of 66%. The rate in Cheshire and Merseyside is 90%. Vascular access surgery may be undertaken by vascular surgeons or transplant surgeons or for some procedures, by specialist nurses. If sufficient procedures are to be undertaken to meet future need, new ways of working may need to be considered. Once access is established, the maintenance of the fistula or catheter site through use of clinical surveillance and regular monitoring is crucial so that problems can be detected early and action taken to preserve the access. Interventional radiology is fundamental to this process and the necessary radiological expertise is essential at each renal centre Dialysis There is a need to ensure high quality hospital haemodialysis can be provided 3 times weekly, local to the patient where clinically appropriate, and at a regular time to suit the patient. Many patients are currently receiving sub-optimal care. The new expansion programme should alleviate this situation but will need constant monitoring over the five year period of this plan. There is a need to maintain high quality peritoneal dialysis and home haemodialysis as options for patient choice and expand services as required. 11
20 Renal facilities for patients with blood borne viruses need to be reviewed and developed in the light of the Dept of Health guidance 8. This guidance sets out recommendations for managing the care of infected renal patients, particularly those with Hepatitis B, Hepatitis C and HIV. Transport for haemodialysis patients to and from their treatment venues is a key consideration for the service. Implementing the recommendations from the Cheshire and Merseyside Transport Action Learning Set will form part of this strategic plan Active Renal Supportive Care The term active renal supportive care is used in this document to cover all aspects of conservative management, palliative care and end of life care. The term active renal supportive care for patients opting not to have, or who are not suitable for, or who have to withdraw from, dialysis therapies is considered more appropriate, as choosing not to have dialysis does not mean no treatment but active treatment in the form of anaemia management, biochemical management, dietary management etc. There is a need to develop this active renal supportive care for patients with established renal disease who choose not to receive dialysis (which may include some patients whose transplanted organs are failing), or for those patients currently receiving treatment who wish to stop and for those for whom it is no longer clinically appropriate. 1.8 HEALTH NEEDS ASSESSMENT AND DEMOGRAPHY The key factors affecting the incidence of renal disease are age and ethnicity. Additional factors include co-morbidities and, to some extent, socio-economic deprivation. In order to plan for the needs of this population, it is important to understand the underlying pathology and its progression, the effects of co-morbid and associated conditions, as well as the complex interactions of patients, care providers, and service constraints. Renal disease is strongly linked to vascular disease and diabetes. These two conditions play a major role in the development of renal disease, and in the long-term prognosis of patients with renal failure. Like kidney disease, coronary heart disease, diabetes and stroke are forms of circulatory disease that relate to some extent to blood vessels or vascular disease. In July 2006, the Department of Health (DH) Renal Team was integrated into the DH s Vascular Programme, ensuring stronger policy links with colleagues working on heart disease, stroke and diabetes to address a set of shared issues such as prevention, early detection and risk management. More recently (April 2008) it has been announced that approval has been given to transform the National Diabetes Support Team into the National Diabetes and Kidney Support Team. This is seen as an opportunity to create a structure of support mechanisms to implement kidney care improvement across England. In the report Putting prevention first vascular checks: risk assessment and management 9 The link between kidney disease and other vascular diseases is highlighted. The majority of patients with early chronic kidney disease (CKD) do not progress to established renal disease (ERD) but do have increased risk of cardiovascular disease. 12
21 Optimal management of the risk factors for cardiovascular disease also reduces the risk of progression from early CKD to ERD. Late referral to specialist renal services of patients with ERD requiring renal replacement therapy is known to be associated with significant costs and poor clinical outcomes. Guidelines have been developed jointly by the Royal College of Physicians and the Renal Association on the identification, management, and referral of patients with CKD. These guidelines have been issued to GPs in the form of an information leaflet (September 2007) and there is already evidence that more patients are being referred in good time. The Vascular Programme Renal Disease Diabetes Shared Vascular Agenda: prevention, screening, managing risk Heart Disease Stroke Treatment for established renal disease (ERD) by dialysis or transplantation is very expensive costing over 2% of the total NHS budget. The numbers of patients requiring renal replacement therapy (RRT) is rising and unlikely to reach steady state within the next 20 years. Any improvement in the cost effective treatment of early renal disease is therefore highly desirable. There has been a significant rise in the number of patients treated with RRT in England over the last 10 years. It is likely, however, that as this rate is still below that of many similar developed countries, there is a persistent unmet need for RRT in the UK as a result of an under-provision of renal services. Section 1.8.2, shows a number of areas of the North West including Cheshire and Merseyside have an under-provision compared with other areas of England. The impact of demographic change, particularly the ageing of the ethnic minority population who have higher rates of renal disease and the increase in Type 2 diabetes may have contributed to the rise and will continue to affect demand. The modalities of RRT therapy have changed due to falling numbers of deceased donor kidneys with consequent growth in dialysis, particularly haemodialysis in satellite units. 13
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care
 SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
Specialised renal services and QIPP
 Specialised renal services and QIPP Contents 1. Executive summary 2. Background 2.1 QIPP 2.2 Specialised renal services 3. Main themes 3.1 Need 3.2 Diagnosis 3.3 Commissioning 3.4 Treatment 3.5 Care 4.
Specialised renal services and QIPP Contents 1. Executive summary 2. Background 2.1 QIPP 2.2 Specialised renal services 3. Main themes 3.1 Need 3.2 Diagnosis 3.3 Commissioning 3.4 Treatment 3.5 Care 4.
DESIGNED TO TACKLE RENAL DISEASE IN WALES DRAFT 2 nd STRATEGIC FRAMEWORK for
 DESIGNED TO TACKLE RENAL DISEASE IN WALES DRAFT 2 nd STRATEGIC FRAMEWORK for 2008-11 1. Aims, Outcomes and Outputs The National Service Framework Designed to Tackle Renal Disease in Wales sets standards
DESIGNED TO TACKLE RENAL DISEASE IN WALES DRAFT 2 nd STRATEGIC FRAMEWORK for 2008-11 1. Aims, Outcomes and Outputs The National Service Framework Designed to Tackle Renal Disease in Wales sets standards
Kidney Patients with Chronic Kidney Disease
 Cheshire and Merseyside Kidney Care Services Renal Replacement Therapy Options for Kidney Patients with Chronic Kidney Disease Stage 5 Renal Replacement Therapy Options for Kidney Patients with Chronic
Cheshire and Merseyside Kidney Care Services Renal Replacement Therapy Options for Kidney Patients with Chronic Kidney Disease Stage 5 Renal Replacement Therapy Options for Kidney Patients with Chronic
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic kidney disease: early identification and management of adults with chronic kidney disease in primary and secondary
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic kidney disease: early identification and management of adults with chronic kidney disease in primary and secondary
. Time to transplant listing is dependent on. . In 2003, 9.1% of all prevalent transplant. . Patients with diabetes mellitus are less
 Chapter 5: Joint Analyses with UK Transplant in England and Wales; Access to the Renal Transplant Waiting List, Time to Listing, Diabetic Access to Transplantation and the Influence of Social Deprivation
Chapter 5: Joint Analyses with UK Transplant in England and Wales; Access to the Renal Transplant Waiting List, Time to Listing, Diabetic Access to Transplantation and the Influence of Social Deprivation
National Chronic Kidney Disease Audit
 National Chronic Kidney Disease Audit // National Report: Part 2 December 2017 Commissioned by: Delivered by: // Foreword by Fiona Loud And if, as part of good, patient-centred care, a record of your condition(s),
National Chronic Kidney Disease Audit // National Report: Part 2 December 2017 Commissioned by: Delivered by: // Foreword by Fiona Loud And if, as part of good, patient-centred care, a record of your condition(s),
The Health Problem: Guidelines: NHS Priority:
 PRIORITY BRIEFING The purpose of this briefing paper is to aid Stakeholders in prioritising topics to be taken further by PenCLAHRC as the basis for a specific evaluation or implementation research project.
PRIORITY BRIEFING The purpose of this briefing paper is to aid Stakeholders in prioritising topics to be taken further by PenCLAHRC as the basis for a specific evaluation or implementation research project.
Treatment choices for someone with Stage 5 kidney disease are:
 Information for patients about advanced kidney disease Dialysis and non-dialysis treatments DOCUMENT PREPARED FOR This information is to help you understand some key issues about dialysis; it is designed
Information for patients about advanced kidney disease Dialysis and non-dialysis treatments DOCUMENT PREPARED FOR This information is to help you understand some key issues about dialysis; it is designed
Chapter 3: National Renal Review 2002: summary report on adult and paediatric renal services
 Chapter 3: National Renal Review : summary report on adult and paediatric renal services Summary The total annual acceptance rate of new patients for Renal Replacement Therapy (RRT) in the UK was 103.0
Chapter 3: National Renal Review : summary report on adult and paediatric renal services Summary The total annual acceptance rate of new patients for Renal Replacement Therapy (RRT) in the UK was 103.0
AUTISM ACTION PLAN FOR THE ROYAL BOROUGH OF GREENWICH
 AUTISM ACTION PLAN FOR THE ROYAL BOROUGH OF GREENWICH NATIONAL CONTEXT Fulfilling and Rewarding Lives (2010) is the Government s strategy for adults with Autistic Spectrum Disorders. It sets out the Government
AUTISM ACTION PLAN FOR THE ROYAL BOROUGH OF GREENWICH NATIONAL CONTEXT Fulfilling and Rewarding Lives (2010) is the Government s strategy for adults with Autistic Spectrum Disorders. It sets out the Government
The next steps
 Greater Manchester Hepatitis C Strategy The next steps 2010-2013 Endorsed by GM Director of Public Health group January 2011 Hepatitis Greater Manchester Hepatitis C Strategy 1. Introduction The Greater
Greater Manchester Hepatitis C Strategy The next steps 2010-2013 Endorsed by GM Director of Public Health group January 2011 Hepatitis Greater Manchester Hepatitis C Strategy 1. Introduction The Greater
North Somerset Autism Strategy
 North Somerset Autism Strategy Approved by: Ratification date: Review date: September 2017 1 Contents 1 Introduction and background... 3 2 Defining Autism...Error! Bookmark not defined. 3 National and
North Somerset Autism Strategy Approved by: Ratification date: Review date: September 2017 1 Contents 1 Introduction and background... 3 2 Defining Autism...Error! Bookmark not defined. 3 National and
The NHS Cancer Plan: A Progress Report
 DEPARTMENT OF HEALTH The NHS Cancer Plan: A Progress Report LONDON: The Stationery Office 9.25 Ordered by the House of Commons to be printed on 7 March 2005 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL
DEPARTMENT OF HEALTH The NHS Cancer Plan: A Progress Report LONDON: The Stationery Office 9.25 Ordered by the House of Commons to be printed on 7 March 2005 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL
Young onset dementia service Doncaster
 Young onset dementia service Doncaster RDaSH Older People s Mental Health Services Introduction The following procedures and protocols will govern the operational working and function of the Doncaster
Young onset dementia service Doncaster RDaSH Older People s Mental Health Services Introduction The following procedures and protocols will govern the operational working and function of the Doncaster
HERTS VALLEYS CCG PALLIATIVE AND END OF LIFE CARE STRATEGY FOR ADULTS AND CHILDREN
 HERTS VALLEYS CCG PALLIATIVE AND END OF LIFE CARE STRATEGY FOR ADULTS AND CHILDREN 2016-2021 1 1. Introduction Herts Valleys Palliative and End of Life Care Strategy is guided by the End of Life Care Strategic
HERTS VALLEYS CCG PALLIATIVE AND END OF LIFE CARE STRATEGY FOR ADULTS AND CHILDREN 2016-2021 1 1. Introduction Herts Valleys Palliative and End of Life Care Strategy is guided by the End of Life Care Strategic
Acceptance onto dialysis guidelines: St George Hospital
 Acceptance onto dialysis guidelines: St George Hospital The following information is a guideline to support clinicians in decision making regarding acceptance onto dialysis. A review of international guidelines
Acceptance onto dialysis guidelines: St George Hospital The following information is a guideline to support clinicians in decision making regarding acceptance onto dialysis. A review of international guidelines
ROLE SPECIFICATION FOR MACMILLAN GPs
 ROLE SPECIFICATION FOR MACMILLAN GPs November 2010 History of Macmillan GPs Macmillan Cancer Support has funded GP positions from the early 1990 s, following the success of our investment in supporting
ROLE SPECIFICATION FOR MACMILLAN GPs November 2010 History of Macmillan GPs Macmillan Cancer Support has funded GP positions from the early 1990 s, following the success of our investment in supporting
Sheffield s Emotional Wellbeing and Mental Health Strategy for Children and Young People
 Sheffield s Emotional Wellbeing and Mental Health Strategy for Children and Young People The Sheffield Vision In Sheffield we want every child and young person to have access to early help in supporting
Sheffield s Emotional Wellbeing and Mental Health Strategy for Children and Young People The Sheffield Vision In Sheffield we want every child and young person to have access to early help in supporting
Kirklees Safeguarding Children Board. Annual Report. January 2011 March Executive Summary.
 Kirklees Safeguarding Children Board Annual Report January 2011 March 2012 Executive Summary www.kirkleessafeguardingchildren.com Foreword As the Chair of Kirklees Safeguarding Children s Board, I am pleased
Kirklees Safeguarding Children Board Annual Report January 2011 March 2012 Executive Summary www.kirkleessafeguardingchildren.com Foreword As the Chair of Kirklees Safeguarding Children s Board, I am pleased
SOLIHULL BEREAVEMENT COUNSELLING SERVICE (SBCS)
") SOLIHULL BEREAVEMENT COUNSELLING SERVICE (SBCS) REVIEW AND DEVELOPMENT PLAN 2013 2016 1 EXECUTIVE SUMMARY Solihull Bereavement Counselling Service (SBCS) is a charity which provides specialist bereavement
SOLIHULL BEREAVEMENT COUNSELLING SERVICE (SBCS) REVIEW AND DEVELOPMENT PLAN 2013 2016 1 EXECUTIVE SUMMARY Solihull Bereavement Counselling Service (SBCS) is a charity which provides specialist bereavement
Regional differences in the provision of adult renal dialysis services in the UK
 Q J Med 2005; 98:183 190 doi:10.1093/qjmed/hci023 Original papers Regional differences in the provision of adult renal dialysis services in the UK L. BLANK 1, J. PETERS 1, A. LUMSDON 2, D.J. O DONOGHUE
Q J Med 2005; 98:183 190 doi:10.1093/qjmed/hci023 Original papers Regional differences in the provision of adult renal dialysis services in the UK L. BLANK 1, J. PETERS 1, A. LUMSDON 2, D.J. O DONOGHUE
GOVERNING BODY REPORT
 GOVERNING BODY REPORT DATE OF MEETING: 20th September 2012 TITLE OF REPORT: KEY MESSAGES: NHS West Cheshire Clinical Commissioning Group has identified heart disease as one of its six strategic clinical
GOVERNING BODY REPORT DATE OF MEETING: 20th September 2012 TITLE OF REPORT: KEY MESSAGES: NHS West Cheshire Clinical Commissioning Group has identified heart disease as one of its six strategic clinical
Urban Village Medical Practice Service Review An integrated model for high quality healthcare for homeless people in Manchester
 An integrated model for high quality healthcare for homeless people in Manchester Urban Village Medical Practice Urban Village Medical Practice (UVMP) is a GP practice based at Ancoats Primary Care Centre
An integrated model for high quality healthcare for homeless people in Manchester Urban Village Medical Practice Urban Village Medical Practice (UVMP) is a GP practice based at Ancoats Primary Care Centre
in North East Lincolnshire Care Trust Plus Implementation Plan Executive Summary
 North East Lincolnshire Care Trust Plus Living Well with Dementia in North East Lincolnshire Implementation Plan 2011-2014 Executive Summary Our vision is for all Individuals with Dementia and their carers
North East Lincolnshire Care Trust Plus Living Well with Dementia in North East Lincolnshire Implementation Plan 2011-2014 Executive Summary Our vision is for all Individuals with Dementia and their carers
02/GMS/0030 ADULT EPILEPSY SERVICE CCP for General Medical and Surgical POOLE HOSPITAL NHS FOUNDATION TRUST
 Service Specification No. Service Commissioner Leads 02/GMS/0030 ADULT EPILEPSY SERVICE CCP for General Medical and Surgical Provider Lead POOLE HOSPITAL NHS FOUNDATION TRUST Period 1 April 2013 to 31
Service Specification No. Service Commissioner Leads 02/GMS/0030 ADULT EPILEPSY SERVICE CCP for General Medical and Surgical Provider Lead POOLE HOSPITAL NHS FOUNDATION TRUST Period 1 April 2013 to 31
GOVERNING BODY MEETING in Public 22 February 2017 Agenda Item 3.4
 GOVERNING BODY MEETING in Public 22 February 2017 Paper Title Purpose of paper Redesign of Services for Frail Older People in Eastern Cheshire To seek approval from Governing Body for the redesign of services
GOVERNING BODY MEETING in Public 22 February 2017 Paper Title Purpose of paper Redesign of Services for Frail Older People in Eastern Cheshire To seek approval from Governing Body for the redesign of services
A06/S(HSS)b Ex-vivo partial nephrectomy service (Adult)
b Ex-vivo partial nephrectomy service (Adult)") A06/S(HSS)b 2013/14 NHS STANDARD CONTRACT FOR EX-VIVO PARTIAL NEPHRECTOMY SERVICE (ADULT) PARTICULARS, SCHEDULE 2 THE SERVICES, A - SERVICE SPECIFICATION Service Specification No. Service Commissioner
A06/S(HSS)b 2013/14 NHS STANDARD CONTRACT FOR EX-VIVO PARTIAL NEPHRECTOMY SERVICE (ADULT) PARTICULARS, SCHEDULE 2 THE SERVICES, A - SERVICE SPECIFICATION Service Specification No. Service Commissioner
Draft Falls Prevention Strategy
 Cheshire West & Chester Council Draft Falls Prevention Strategy 2017-2020 Visit: cheshirewestandchester.gov.uk Visit: cheshirewestandchester.gov.uk 02 Cheshire West and Chester Council Draft Falls Prevention
Cheshire West & Chester Council Draft Falls Prevention Strategy 2017-2020 Visit: cheshirewestandchester.gov.uk Visit: cheshirewestandchester.gov.uk 02 Cheshire West and Chester Council Draft Falls Prevention
Kidney Disease Treatment Options
 Page 1 Fact sheet The kidneys play a number of important roles in your body such as: extracting excess water to make urine (wee) controlling your blood pressure filtering waste products and toxins from
Page 1 Fact sheet The kidneys play a number of important roles in your body such as: extracting excess water to make urine (wee) controlling your blood pressure filtering waste products and toxins from
Palliative and End of Life Care in End Stage Renal Disease
 Palliative and End of Life Care in End Stage Renal Disease Palliative and End of Life Care Priority for Action Regional Consensus Workshop 30.06.2010 Neal Morgan Consultant Nephrologist SHSCT Outline Introduction
Palliative and End of Life Care in End Stage Renal Disease Palliative and End of Life Care Priority for Action Regional Consensus Workshop 30.06.2010 Neal Morgan Consultant Nephrologist SHSCT Outline Introduction
People in Norfolk and Waveney with Autistic Spectrum Disorder
 People in Norfolk and Waveney with Autistic Spectrum Disorder Linda Hillman Public Health Consultant, March 2011 The national strategy to improve the lives of adults with Autism, Fulfilling and Rewarding
People in Norfolk and Waveney with Autistic Spectrum Disorder Linda Hillman Public Health Consultant, March 2011 The national strategy to improve the lives of adults with Autism, Fulfilling and Rewarding
British Association of Stroke Physicians Strategy 2017 to 2020
 British Association of Stroke Physicians Strategy 2017 to 2020 1 P age Contents Introduction 3 1. Developing and influencing local and national policy for stroke 5 2. Providing expert advice on all aspects
British Association of Stroke Physicians Strategy 2017 to 2020 1 P age Contents Introduction 3 1. Developing and influencing local and national policy for stroke 5 2. Providing expert advice on all aspects
A. Service Specification
 A. Service Specification Service Specification No: 1767 Service Adult Highly Specialist Pain Management Services Commissioner Lead For local completion Lead For local completion 1. Scope 1.1 Prescribed
A. Service Specification Service Specification No: 1767 Service Adult Highly Specialist Pain Management Services Commissioner Lead For local completion Lead For local completion 1. Scope 1.1 Prescribed
Beyond the Diagnosis. Young Onset Dementia and the Patient Experience
 Beyond the Diagnosis Young Onset Dementia and the Patient Experience November 2017 1 Contents Executive Summary... 4 Recommendations... 4 1. Introduction... 6 2. Background & Rationale... 6 3. Methodology...
Beyond the Diagnosis Young Onset Dementia and the Patient Experience November 2017 1 Contents Executive Summary... 4 Recommendations... 4 1. Introduction... 6 2. Background & Rationale... 6 3. Methodology...
Implementing NICE clinical guidelines on Parkinson s disease
 ORIGINAL PAPERS Clinical Medicine 2009, Vol 9, No 5: 436 40 Implementing NICE clinical guidelines on Parkinson s disease Beverly A Ryton and B Jane Liddle ABSTRACT Implementing national guidance such as
ORIGINAL PAPERS Clinical Medicine 2009, Vol 9, No 5: 436 40 Implementing NICE clinical guidelines on Parkinson s disease Beverly A Ryton and B Jane Liddle ABSTRACT Implementing national guidance such as
Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire
 Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire Introduction This document introduces South Gloucestershire Clinical Commissioning
Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire Introduction This document introduces South Gloucestershire Clinical Commissioning
From Better to Best: Improving the availability of organs for transplant
 From Better to Best: Improving the availability of organs for transplant Elisabeth Buggins CBE Strategy Oversight Group Chair Presentation outline Progress 2004-2014 Strategy and work underway Outcomes
From Better to Best: Improving the availability of organs for transplant Elisabeth Buggins CBE Strategy Oversight Group Chair Presentation outline Progress 2004-2014 Strategy and work underway Outcomes
CABINET PROCURING A SUBSTANCE MISUSE & COMMUNITY TREATMENT SERVICE IN RUTLAND
 CABINET Report No: 105/2017 PUBLIC REPORT 16 May 2017 PROCURING A SUBSTANCE MISUSE & COMMUNITY TREATMENT SERVICE IN RUTLAND Report of the Director of Public Health Strategic Aim: Safeguarding Key Decision:
CABINET Report No: 105/2017 PUBLIC REPORT 16 May 2017 PROCURING A SUBSTANCE MISUSE & COMMUNITY TREATMENT SERVICE IN RUTLAND Report of the Director of Public Health Strategic Aim: Safeguarding Key Decision:
Report by the Comptroller and. SesSIon January Improving Dementia Services in England an Interim Report
 Report by the Comptroller and Auditor General HC 82 SesSIon 2009 2010 14 January 2010 Improving Dementia Services in England an Interim Report 4 Summary Improving Dementia Services in England an Interim
Report by the Comptroller and Auditor General HC 82 SesSIon 2009 2010 14 January 2010 Improving Dementia Services in England an Interim Report 4 Summary Improving Dementia Services in England an Interim
Nephrology. 2. To facilitate a trainee to acquire the knowledge, clinical skills, procedural competence and professional attributes in Nephrology.
 Nephrology I) OBJECTIVES 1. To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Nephrology. 2. To
Nephrology I) OBJECTIVES 1. To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Nephrology. 2. To
The Ayrshire Hospice
 Strategy 2010-2015 Welcome... The Ayrshire Hospice : Strategy 2010-2015 Index 05 06 08 09 10 12 15 17 19 Foreword Our vision and purpose Our guiding principles Our achievements 1989-2010 Our priorities
Strategy 2010-2015 Welcome... The Ayrshire Hospice : Strategy 2010-2015 Index 05 06 08 09 10 12 15 17 19 Foreword Our vision and purpose Our guiding principles Our achievements 1989-2010 Our priorities
Community alcohol detoxification in primary care
 Community alcohol detoxification in primary care 1. Purpose The purpose of this primary care enhanced service is to improve the health and quality of life of people whose health may be compromised by their
Community alcohol detoxification in primary care 1. Purpose The purpose of this primary care enhanced service is to improve the health and quality of life of people whose health may be compromised by their
Victorian Paediatric Oncology Situational Analysis & Workforce Requirements
 - Victorian Paediatric Oncology Situational Analysis & Workforce Requirements 2012-2026 SUMMARY REPORT May 2013 1 Contents Executive summary...3 1. Introduction...6 2. Project method...8 2.1 Estimating
- Victorian Paediatric Oncology Situational Analysis & Workforce Requirements 2012-2026 SUMMARY REPORT May 2013 1 Contents Executive summary...3 1. Introduction...6 2. Project method...8 2.1 Estimating
Commissioning Living with and Beyond Cancer in Yorkshire and Humber; an Overview.
 Commissioning Living with and Beyond Cancer in Yorkshire and Humber; an Overview. Document Title An Overview of Commissioning Living with and Beyond Cancer in Yorkshire and Humber Version number: 1 First
Commissioning Living with and Beyond Cancer in Yorkshire and Humber; an Overview. Document Title An Overview of Commissioning Living with and Beyond Cancer in Yorkshire and Humber Version number: 1 First
Project Initiation Document:
 Project Initiation Document: Lancashire Support Services for Children, Young People, Families and Carers Affected by Autistic Spectrum Disorder (ASD) and Diagnosis 1. Background The Children and Young
Project Initiation Document: Lancashire Support Services for Children, Young People, Families and Carers Affected by Autistic Spectrum Disorder (ASD) and Diagnosis 1. Background The Children and Young
Renal Service Plan for the Midland Region
 Renal Service Plan for the Midland Region Part Two Recommendations Options and Opportunities Prepared by: Jan Barber, Midland Regional Service Planner Date: December 2004 Acknowledgements: A number of
Renal Service Plan for the Midland Region Part Two Recommendations Options and Opportunities Prepared by: Jan Barber, Midland Regional Service Planner Date: December 2004 Acknowledgements: A number of
Foreword 3. Introduction 5. Standard 1 - Care for All 15. Module 1: Care for Children and Young People 25 Children s Standards 1-10
 Contents Foreword 3 Designed to Tackle Renal Disease in Wales: A National Service Framework Introduction 5 Standard 1 - Care for All 15 Page Module 1: Care for Children and Young People 25 Children s Standards
Contents Foreword 3 Designed to Tackle Renal Disease in Wales: A National Service Framework Introduction 5 Standard 1 - Care for All 15 Page Module 1: Care for Children and Young People 25 Children s Standards
KIDNEY FAILURE TREATMENT OPTIONS Choosing What s Best For You
 KIDNEY FAILURE TREATMENT OPTIONS Choosing What s Best For You What Kidneys Do The kidneys are a pair of bean shaped organs located below your ribcage near the middle of your back. Kidneys play a vital
KIDNEY FAILURE TREATMENT OPTIONS Choosing What s Best For You What Kidneys Do The kidneys are a pair of bean shaped organs located below your ribcage near the middle of your back. Kidneys play a vital
The Vision. The Objectives
 The Vision Older people participate to their fullest ability in decisions about their health and wellbeing and in family, whānau and community life. They are supported in this by co-ordinated and responsive
The Vision Older people participate to their fullest ability in decisions about their health and wellbeing and in family, whānau and community life. They are supported in this by co-ordinated and responsive
Cardiovascular disease profile
 Cardiovascular disease profile Kidney disease Background This chapter of the Cardiovascular disease profiles focuses on kidney disease and is produced by the National Cardiovascular Intelligence Network
Cardiovascular disease profile Kidney disease Background This chapter of the Cardiovascular disease profiles focuses on kidney disease and is produced by the National Cardiovascular Intelligence Network
The role of cancer networks in the new NHS
 The role of cancer networks in the new NHS October 2012 UK Office, 89 Albert Embankment, London SE1 7UQ Questions about cancer? Call the Macmillan Support Line free on 0808 808 00 00 or visit macmillan.org.uk
The role of cancer networks in the new NHS October 2012 UK Office, 89 Albert Embankment, London SE1 7UQ Questions about cancer? Call the Macmillan Support Line free on 0808 808 00 00 or visit macmillan.org.uk
Core Standard 24. Cass Sandmann Emergency Planning Officer. Pat Fields Executive Director for Pandemic Flu Planning
 Trust Board Meeting Agenda Item 7 Date: 30 September 2009 Title of Report Recommendations (please outline the purpose of the report and the key issues for consideration/decision) Progress with Pandemic
Trust Board Meeting Agenda Item 7 Date: 30 September 2009 Title of Report Recommendations (please outline the purpose of the report and the key issues for consideration/decision) Progress with Pandemic
TRANSFORM CANCER SERVICES
 WORKING TOGETHER to TRANSFORM CANCER SERVICES in SOUTH EAST WALES 1 Understanding the context Cancer survival rates are increasing. But the number of people getting cancer is increasing too. At Velindre
WORKING TOGETHER to TRANSFORM CANCER SERVICES in SOUTH EAST WALES 1 Understanding the context Cancer survival rates are increasing. But the number of people getting cancer is increasing too. At Velindre
Dorset Health Scrutiny Committee
 Dorset Health Scrutiny Committee Date of Meeting 15 June 2018 Officer/Author Diane Bardwell, Dementia Services Review Project Manager, NHS Dorset Clinical Commissioning Group Subject of Report Dementia
Dorset Health Scrutiny Committee Date of Meeting 15 June 2018 Officer/Author Diane Bardwell, Dementia Services Review Project Manager, NHS Dorset Clinical Commissioning Group Subject of Report Dementia
National Diabetes Treatment and Care Programme
 National Diabetes Treatment and Care Programme Introduction to and supporting documentation for VALUE BASED TRANSFORMATION FUNDING SITE SELECTION December 2016 1 Introduction and Contents The Planning
National Diabetes Treatment and Care Programme Introduction to and supporting documentation for VALUE BASED TRANSFORMATION FUNDING SITE SELECTION December 2016 1 Introduction and Contents The Planning
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE SCOPE. Dementia: the management of dementia, including the use of antipsychotic medication in older people
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Dementia: the management of dementia, including the use of antipsychotic medication in older people 1.1 Short title Dementia 2 Background
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Dementia: the management of dementia, including the use of antipsychotic medication in older people 1.1 Short title Dementia 2 Background
FINANCE COMMITTEE DEMOGRAPHIC CHANGE AND AGEING POPULATION INQUIRY SUBMISSION FROM NATIONAL OSTEOPOROSIS SOCIETY
 FINANCE COMMITTEE DEMOGRAPHIC CHANGE AND AGEING POPULATION INQUIRY SUBMISSION FROM NATIONAL OSTEOPOROSIS SOCIETY What is your view of the effects of the demographic change and an ageing population on the
FINANCE COMMITTEE DEMOGRAPHIC CHANGE AND AGEING POPULATION INQUIRY SUBMISSION FROM NATIONAL OSTEOPOROSIS SOCIETY What is your view of the effects of the demographic change and an ageing population on the
TRANSPLANT ACTIVITY IN THE UK
 Activity Report 2010/11 TRANSPLANT ACTIVITY IN THE UK www.nhsbt.nhs.uk PREFACE This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report
Activity Report 2010/11 TRANSPLANT ACTIVITY IN THE UK www.nhsbt.nhs.uk PREFACE This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report
CORPORATE PLANS FOR CHILD PROTECTION AND LOOKED ATER CHILDREN AND YOUNG PEOPLE
 NHS Highland Board 28 March 2017 Item 4.11 CORPORATE PLANS FOR CHILD PROTECTION AND LOOKED ATER CHILDREN AND YOUNG PEOPLE Report by Dr Stephanie Govenden Lead Doctor Child Protection and Looked After Children
NHS Highland Board 28 March 2017 Item 4.11 CORPORATE PLANS FOR CHILD PROTECTION AND LOOKED ATER CHILDREN AND YOUNG PEOPLE Report by Dr Stephanie Govenden Lead Doctor Child Protection and Looked After Children
The Constitution of the British Association for Chronic Fatigue Syndrome/ME (BACME) CONTENTS. Name of the Organisation. 2. Aims and Objectives
 CONTENTS. Name of the Organisation. 2. Aims and Objectives") The Constitution of the British Association for Chronic Fatigue Syndrome/ME (BACME) October 2013 CONTENTS Name of the Organisation 1. History 2. Aims and Objectives 3. Membership of BACME 4. BACME executive
The Constitution of the British Association for Chronic Fatigue Syndrome/ME (BACME) October 2013 CONTENTS Name of the Organisation 1. History 2. Aims and Objectives 3. Membership of BACME 4. BACME executive
A Suite of Enhanced Services for. Prudent Structured Care for Adults with Type 2 Diabetes
 An Enhanced Service for Prudent Structured Care for Adults with Type 2 Diabetes Page 1 A Suite of Enhanced Services for Prudent Structured Care for Adults with Type 2 Diabetes 1. Introduction All practices
An Enhanced Service for Prudent Structured Care for Adults with Type 2 Diabetes Page 1 A Suite of Enhanced Services for Prudent Structured Care for Adults with Type 2 Diabetes 1. Introduction All practices
REPORT TO CLINICAL COMMISSIONING GROUP
 REPORT TO CLINICAL COMMISSIONING GROUP 12th December 2012 Agenda No. 6.2 Title of Document: Report Author/s: Lead Director/ Clinical Lead: Contact details: Commissioning Model for Dementia Care Dr Aryan
REPORT TO CLINICAL COMMISSIONING GROUP 12th December 2012 Agenda No. 6.2 Title of Document: Report Author/s: Lead Director/ Clinical Lead: Contact details: Commissioning Model for Dementia Care Dr Aryan
TESTING TIMES TO COME? AN EVALUATION OF PATHOLOGY CAPACITY IN NORTHERN IRELAND NOVEMBER 2016
 TESTING TIMES TO COME? AN EVALUATION OF PATHOLOGY CAPACITY IN NORTHERN IRELAND NOVEMBER 2016 EXECUTIVE SUMMARY Whilst cancer survival is at its highest ever level, our health services are under considerable
TESTING TIMES TO COME? AN EVALUATION OF PATHOLOGY CAPACITY IN NORTHERN IRELAND NOVEMBER 2016 EXECUTIVE SUMMARY Whilst cancer survival is at its highest ever level, our health services are under considerable
It is important upfront to realize and believe that, like many adults,
 Kids With Kidney Disease Can Realize Their Dreams and Live Long, Normal, Productive Lives By Gordon Lore It is important upfront to realize and believe that, like many adults, children with kidney failure
Kids With Kidney Disease Can Realize Their Dreams and Live Long, Normal, Productive Lives By Gordon Lore It is important upfront to realize and believe that, like many adults, children with kidney failure
Primary Health Networks
 Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 Hunter New England & Central Coast Please note: This Activity Work Plan was developed in response to the HNECC PHN
Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 Hunter New England & Central Coast Please note: This Activity Work Plan was developed in response to the HNECC PHN
GMS Contract in Wales Enhanced Service for Homeless Patients Specification
 Doc 4 GMS Contract in Wales 2008-09 Enhanced Service for Homeless Patients Specification Introduction The purpose of this paper is to provide an enhanced service specification for Local Health Boards when
Doc 4 GMS Contract in Wales 2008-09 Enhanced Service for Homeless Patients Specification Introduction The purpose of this paper is to provide an enhanced service specification for Local Health Boards when
Arrhythmia Care in the DGH What Still Needs to be Done? Dr. Sundeep Puri Consultant Cardiologist
 Arrhythmia Care in the DGH What Still Needs to be Done? Dr. Sundeep Puri Consultant Cardiologist LOTS!!! This presentation confines itself to the situation in the North West. The views expressed are my
Arrhythmia Care in the DGH What Still Needs to be Done? Dr. Sundeep Puri Consultant Cardiologist LOTS!!! This presentation confines itself to the situation in the North West. The views expressed are my
Revised Standards. S 1a: The service routinely collects data on age, gender and ethnicity for each person referred for psychological therapy.
 Revised Standards S 1a: The service routinely collects data on age, gender and ethnicity for each person referred for psychological therapy. S1b: People starting treatment with psychological therapy are
Revised Standards S 1a: The service routinely collects data on age, gender and ethnicity for each person referred for psychological therapy. S1b: People starting treatment with psychological therapy are
Palliative & End of Life Care Plan
 Palliative & End of Life Care Plan 2018-2023 Contents 1. Palliative Care Definition Page 1 2. Our Vision Page 2 3. Key Aims Page 2 4. Planned Actions Page 3-5 5. Priorities Page 6-7 6. Appendix 1 HSCP
Palliative & End of Life Care Plan 2018-2023 Contents 1. Palliative Care Definition Page 1 2. Our Vision Page 2 3. Key Aims Page 2 4. Planned Actions Page 3-5 5. Priorities Page 6-7 6. Appendix 1 HSCP
Patient Decision Aid. Kidney Failure Treatment Options. Patient Information. Sussex Kidney Unit
 Patient Decision Aid Kidney Failure Treatment Options Sussex Kidney Unit Patient Information Contents Page Do I want Renal Replacement Therapy? 3 Established Kidney Failure (EKF) 4 Why do I need to make
Patient Decision Aid Kidney Failure Treatment Options Sussex Kidney Unit Patient Information Contents Page Do I want Renal Replacement Therapy? 3 Established Kidney Failure (EKF) 4 Why do I need to make
National Service Framework for Diabetes: Delivery Strategy
 National Service Framework for Diabetes: Delivery Strategy National Service Framework for Diabetes: Delivery Strategy Contents Foreword 1 Executive summary 2 1 Introduction 3 2 Building Capacity: Organisational
National Service Framework for Diabetes: Delivery Strategy National Service Framework for Diabetes: Delivery Strategy Contents Foreword 1 Executive summary 2 1 Introduction 3 2 Building Capacity: Organisational
BETTER CANCER CARE AND THE FUTURE PROVISION OF CANCER CARE IN NHS LANARKSHIRE
 NHS Lanarkshire Board Meeting Wednesday 23rd November Boardroom, Kirklands Corporate HQ NHS Lanarkshire Headquarters, Kirklands Fallside Road, Bothwell G71 8BB www.nhslanarkshire.co.uk BETTER CANCER CARE
NHS Lanarkshire Board Meeting Wednesday 23rd November Boardroom, Kirklands Corporate HQ NHS Lanarkshire Headquarters, Kirklands Fallside Road, Bothwell G71 8BB www.nhslanarkshire.co.uk BETTER CANCER CARE
The Hepatitis C Action Plan for Scotland: Draft Guidelines for Hepatitis C Care Networks
 The Hepatitis C Action Plan for Scotland: Draft Guidelines for Hepatitis C Care Networks Royal College of Physicians of Edinburgh Friday 12 October 2007 CONTENTS 1.0 ACCOUNTABILITY AND ORGANISATION 2.0
The Hepatitis C Action Plan for Scotland: Draft Guidelines for Hepatitis C Care Networks Royal College of Physicians of Edinburgh Friday 12 October 2007 CONTENTS 1.0 ACCOUNTABILITY AND ORGANISATION 2.0
PRIMARY CARE CO-COMMISSIONING COMMITTEE 8 SEPTEMBER 2015
 Part 1 Part 2 PRIMARY CARE CO-COMMISSIONING COMMITTEE 8 SEPTEMBER 2015 Title of Report Trafford Palliative care Quality Premium Scheme 2015/16 Purpose of the Report The purpose of the report is to detail
Part 1 Part 2 PRIMARY CARE CO-COMMISSIONING COMMITTEE 8 SEPTEMBER 2015 Title of Report Trafford Palliative care Quality Premium Scheme 2015/16 Purpose of the Report The purpose of the report is to detail
Item No: 6. Meeting Date: Tuesday 12 th December Glasgow City Integration Joint Board Performance Scrutiny Committee
 Item No: 6 Meeting Date: Tuesday 12 th December 2017 Glasgow City Integration Joint Board Performance Scrutiny Committee Report By: Susanne Millar, Chief Officer, Strategy & Operations / Chief Social Work
Item No: 6 Meeting Date: Tuesday 12 th December 2017 Glasgow City Integration Joint Board Performance Scrutiny Committee Report By: Susanne Millar, Chief Officer, Strategy & Operations / Chief Social Work
Oxford Kidney Unit. Treatment options for chronic kidney disease A brief overview
 Oxford Kidney Unit Treatment options for chronic kidney disease A brief overview You may feel well at the moment and may not have any symptoms from your kidney disease, but it is important that you understand
Oxford Kidney Unit Treatment options for chronic kidney disease A brief overview You may feel well at the moment and may not have any symptoms from your kidney disease, but it is important that you understand
INTRODUCTION TO HAEMODIALYSIS
 INTRODUCTION TO HAEMODIALYSIS Why do I need dialysis? What is dialysis? How does haemodialysis work? Where will I have my treatment? Will dialysis cure my kidney failure? Will dialysis keep me well? I
INTRODUCTION TO HAEMODIALYSIS Why do I need dialysis? What is dialysis? How does haemodialysis work? Where will I have my treatment? Will dialysis cure my kidney failure? Will dialysis keep me well? I
Influencing planning to improve the quality of Parkinson s care in Scotland
 Influencing planning to improve the quality of Parkinson s care in Scotland This short guide enables you to influence commissioning by making the case for high quality, cost-effective care for people affected
Influencing planning to improve the quality of Parkinson s care in Scotland This short guide enables you to influence commissioning by making the case for high quality, cost-effective care for people affected
We need to talk about Palliative Care COSLA
 Introduction We need to talk about Palliative Care COSLA 1. Local government recognises the importance of high quality palliative and end of life care if we are to give people greater control over how
Introduction We need to talk about Palliative Care COSLA 1. Local government recognises the importance of high quality palliative and end of life care if we are to give people greater control over how
London Strategic Clinical Networks. Quality Standard. Version 1.0 (2015)
") London Strategic Clinical Networks Quality Standard Version 1.0 (2015) Supporting the delivery of equitable, high quality AKI care through collaboration www.londonaki.net @LondonAKI Overview The management
London Strategic Clinical Networks Quality Standard Version 1.0 (2015) Supporting the delivery of equitable, high quality AKI care through collaboration www.londonaki.net @LondonAKI Overview The management
Peritoneal Dialysis. Choosing your logo. V2.0 logos. information. you can trust. Certified Member. The Information Standard
 Use of The Information Standard s Member Logos Peritoneal Dialysis Patient Information Choosing your logo The Information Standard has four logo versions for its members. They are designed to fit neatly
Use of The Information Standard s Member Logos Peritoneal Dialysis Patient Information Choosing your logo The Information Standard has four logo versions for its members. They are designed to fit neatly
Appendix 1. Cognitive Impairment and Dementia Service Elm Lodge 4a Marley Close Greenford Middlesex UB6 9UG
 Appendix 1 Mr Dwight McKenzie Scrutiny Review Officer Legal and Democratic Services Ealing Council Perceval House 14 16 Uxbridge Road Ealing London W5 2HL Cognitive Impairment and Dementia Service Elm
Appendix 1 Mr Dwight McKenzie Scrutiny Review Officer Legal and Democratic Services Ealing Council Perceval House 14 16 Uxbridge Road Ealing London W5 2HL Cognitive Impairment and Dementia Service Elm
Together for Health A Diabetes Delivery Plan
 Welsh Government Together for Health A Diabetes Delivery Plan A Delivery Plan up to 2016 for NHS Wales and its partners Digital ISBN 978 1 4734 0291 1 Crown copyright 2013 WG19785 CONTENTS Foreword by
Welsh Government Together for Health A Diabetes Delivery Plan A Delivery Plan up to 2016 for NHS Wales and its partners Digital ISBN 978 1 4734 0291 1 Crown copyright 2013 WG19785 CONTENTS Foreword by
Waterloo Wellington Regional Renal Program. Renal Plan
 Waterloo Wellington Regional Renal Program Renal Plan 2015-2019 A message from the Regional Director and the Chief of Nephrology Peter Varga and Dr. Gerald Rosenstein Each year, our region experiences
Waterloo Wellington Regional Renal Program Renal Plan 2015-2019 A message from the Regional Director and the Chief of Nephrology Peter Varga and Dr. Gerald Rosenstein Each year, our region experiences
Transforming educational provision for children and young people with autism using the Autism Education Trust Materials and Training Programme
 Transforming educational provision for children and young people with autism using the Autism Education Trust Materials and Training Programme Pam Simpson and the Communication and Autism Team, Birmingham,
Transforming educational provision for children and young people with autism using the Autism Education Trust Materials and Training Programme Pam Simpson and the Communication and Autism Team, Birmingham,
Northamptonshire Hospice Charities Strategy
 Northamptonshire Hospice Charities Strategy Please note that sections in italics are comments related to the main statement above it. Introduction This document sets out how the hospice charities in Northamptonshire
Northamptonshire Hospice Charities Strategy Please note that sections in italics are comments related to the main statement above it. Introduction This document sets out how the hospice charities in Northamptonshire
Building on Success. Driving improvements in clinical outcomes through a Greater Manchester Cancer Alliance. May 2015
 Building on Success Driving improvements in clinical outcomes through a Greater Manchester Cancer Alliance May 2015 Introduction Cancer care in Greater Manchester has seen significant improvements in recent
Building on Success Driving improvements in clinical outcomes through a Greater Manchester Cancer Alliance May 2015 Introduction Cancer care in Greater Manchester has seen significant improvements in recent
Your Kidney Health. Your Choices. Chronic Kidney Disease
 Your Kidney Health Your Choices Your doctor may have told you that you have chronic kidney disease (CKD or advanced kidney disease; or, you may be in kidney failure, and may have to make a decision about
Your Kidney Health Your Choices Your doctor may have told you that you have chronic kidney disease (CKD or advanced kidney disease; or, you may be in kidney failure, and may have to make a decision about
Yorkshire and the Humber Strategic Clinical Networks
 1. Welcome & Introduction Yorkshire and the Humber Strategic Clinical Networks Yorkshire and the Humber Kidney Care Conservative Care Forum Tuesday 25 th February 2014 1300-1630 Notes Welcome and Introduction
1. Welcome & Introduction Yorkshire and the Humber Strategic Clinical Networks Yorkshire and the Humber Kidney Care Conservative Care Forum Tuesday 25 th February 2014 1300-1630 Notes Welcome and Introduction
NHS Sheffield Community Pharmacy Seasonal Flu Vaccination Programme for hard to reach at risk groups (and catch up campaign for over 65s)
") NHS Sheffield Community Pharmacy Seasonal Flu Vaccination Programme for hard to reach at risk groups 2012-13 (and catch up campaign for over 65s) Service Evaluation! Supported by Sheffield!Local!Pharmaceutical!Committee!
NHS Sheffield Community Pharmacy Seasonal Flu Vaccination Programme for hard to reach at risk groups 2012-13 (and catch up campaign for over 65s) Service Evaluation! Supported by Sheffield!Local!Pharmaceutical!Committee!
Sandwell & West Birmingham integrated community care diabetes model (DICE) the future of diabetes services?
 the future of diabetes services?") Sandwell & West Birmingham integrated community care diabetes model (DICE) the future of diabetes services? Dr PARIJAT DE DUK Clinical Champion Clinical Lead for Diabetes & Endocrinology, Sandwell & West
Sandwell & West Birmingham integrated community care diabetes model (DICE) the future of diabetes services? Dr PARIJAT DE DUK Clinical Champion Clinical Lead for Diabetes & Endocrinology, Sandwell & West
Strategic Clinical Network for Yorkshire and the Humber
 Strategic Clinical Network for Yorkshire and the Humber SCN-CVD-Nephrology-AKI John Stoves Park Plaza, Leeds 16 th June 2014 2 Strategic Clinical Networks SCNs operate as engines for change across complex
Strategic Clinical Network for Yorkshire and the Humber SCN-CVD-Nephrology-AKI John Stoves Park Plaza, Leeds 16 th June 2014 2 Strategic Clinical Networks SCNs operate as engines for change across complex
The Burden of Kidney Disease in Rural & Northern Ontario
 Ontario Branch The Burden of Kidney Disease in Rural & Northern Ontario Contact: Janet Bick Director, Policy & Programs The Kidney Foundation of Canada Ontario Branch Tel: 905-278-3003/1.800-387-4474 ext.4970
Ontario Branch The Burden of Kidney Disease in Rural & Northern Ontario Contact: Janet Bick Director, Policy & Programs The Kidney Foundation of Canada Ontario Branch Tel: 905-278-3003/1.800-387-4474 ext.4970
From the Permanent Secretary and HSC Chief Executive
 From the Permanent Secretary and HSC Chief Executive Dr Andrew Murrison MP Chair, N. Ireland Affairs Committee Committee Office House of Commons LONDON SW1A 0AA northircom@parliament.uk Castle Buildings
From the Permanent Secretary and HSC Chief Executive Dr Andrew Murrison MP Chair, N. Ireland Affairs Committee Committee Office House of Commons LONDON SW1A 0AA northircom@parliament.uk Castle Buildings
Patient Education Programme. Kidney Options Guiding you when kidneys fail
 Patient Education Programme Kidney Options Guiding you when kidneys fail About the kidneys What do healthy kidneys do? Your two kidneys work more than you realise. The kidneys remove excess body water
Patient Education Programme Kidney Options Guiding you when kidneys fail About the kidneys What do healthy kidneys do? Your two kidneys work more than you realise. The kidneys remove excess body water
THE WORLD MEDICAL ASSOCIATION, INC. WMA STATEMENT ON ORGAN AND TISSUE DONATION
 THE WORLD MEDICAL ASSOCIATION, INC. WMA STATEMENT ON ORGAN AND TISSUE DONATION Adopted by the 63rd WMA General Assembly, Bangkok, Thailand, October 2012 PREAMBLE Advances in medical sciences, especially
THE WORLD MEDICAL ASSOCIATION, INC. WMA STATEMENT ON ORGAN AND TISSUE DONATION Adopted by the 63rd WMA General Assembly, Bangkok, Thailand, October 2012 PREAMBLE Advances in medical sciences, especially
Vision 2025: Summary
 Vision 2025: Summary At the Royal Berkshire NHS Foundation Trust our vision is: Working together to provide outstanding care for our community We have a rich history of providing healthcare to the people
Vision 2025: Summary At the Royal Berkshire NHS Foundation Trust our vision is: Working together to provide outstanding care for our community We have a rich history of providing healthcare to the people
The Way Ahead Our Three Year Strategic Plan EVERY MOMENT MATTERS
 The Way Ahead Our Three Year Strategic Plan 2017-2020 EVERY MOMENT MATTERS Every moment matters - that s what our logo says right next to our name John Taylor Hospice and for us the two are inseparable.
The Way Ahead Our Three Year Strategic Plan 2017-2020 EVERY MOMENT MATTERS Every moment matters - that s what our logo says right next to our name John Taylor Hospice and for us the two are inseparable.