Disclosure / Conflict of Interest. None
|
|
|
- Candace Charles
- 5 years ago
- Views:
Transcription




1
2 Disclosure / Conflict of Interest None
3 Objectives Epidemiology and demographics of injury and emergency surgery in the elderly Anatomic and physiology changes in the context of surgical disease in the elderly Discuss management paradigm Clinical decision making Outcomes
4 Aging Populace Increased population Baby Boomer generation Increased life expectancy Better living conditions Income Nutition Preventative medicine Health promotion Improved diagnostics and therapeutics


5 Baby Boomers Desire for normalcy after 16 years of depression and war. Confidence that the future would be one of comfort and prosperity
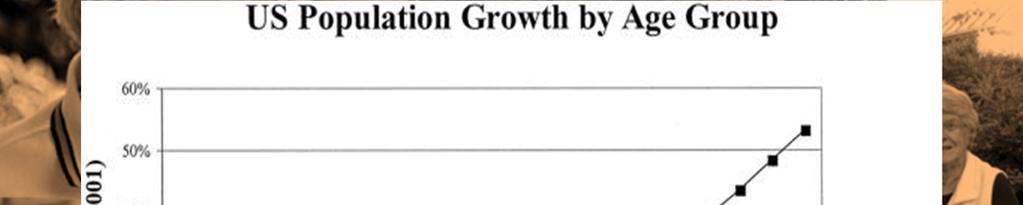
6 Population Growth Age Demographic
7 Elderly Population Growth 80 Increase in the Number of Persons Aged 65+ Years in the United States 72 (20%) Population (4%) 4 (4%) Number (millions) Percent of population 5 (5%) 7 (5%) 9 (7%) 12 (8%) 17 (9%) (10%) 26 (11%) 31 (13%) 35 (12%) 40 (13%) 55 (17%) Year Etzioni: Ann Surg 2003; 238:



8 Aging in America



9 Aging in America
10 TRAUMA
11 CDC Injury Demographics
12 Biomechanics & Epidemiology of Injury in Elderly Progressive decline in central nervous system function associated with loss of proprioception, balance, and motor coordination. Incidence of falls and the severity of associated injury increases with advancing age. Medications for comorbid disease may mask physiologic signs / exacerbate injury sequelae. After age 44, death from cancer and heart disease overtakes injury as leading cause of death.
13 Major Trauma Outcome Study Geriatric Subanalysis Major Trauma Outcome Study (MTOS) by ACS Analysis of 46,613 major trauma patients admitted to 120 Trauma Centers over 4 years Geriatric subanalysis n=4,098 Age, mechanism of injury, outcome, length of stay, complications vitals signs, Glasgow coma score, Trauma Score, AIS Data used to establish age-dependent mortality rates Champion: Am J Pub Health 1989;79:
14 Major Trauma Outcome Study Geriatric Subanalysis Elderly mortality double that of mortality in the younger group (27% vs. 14%). Markedly higher complication rate Pulmonary (14/100 vs. 6.1/1100) Infectious complications (4.6/100 vs. 0.7/100). Length of stay was twice as long for the older patients (14 days vs. 7 days). Champion: Am J Pub Health 1989;79:
15 Elderly Injury Survival Probability of fatal outcome increases linearly with age by 1% per year over 65 Factors associated with poor prognosis Severe head injury-gcs Hypotension Prolonged ventilation Pneumonia Early, cardiac dysfunction limits survival in elderly Osler: Am J Surg156:537 Dec
16 Long Term Survival Trauma Patients Retrospective cohort study of 124,421 injured adult patients Goal: Determine the long-term mortality of patients following trauma admission 7243 died before hospital discharge and 21,045 died following hospital discharge Patients who were older and those who were discharged to a skilled nursing facility had the highest risk of death Davidson: Long term survival of adult trauma patients.jama Mar 9;305(10):
17 Elderly Falls Most common injury - 40% elderly trauma 25% who fall sustain serious injury Falls M=F but females are more likely to be injured Anatomic / physiologic basis: Decreased vision and hearing Slower reflexes Impaired balance and motor/cognitive function Decreased bone density & muscle mass/ strength Less joint flexibility
18 Ground Level Falls (GLF) Retrospective review NTDB 32,320 elderly GLF (>70 y/o) Mortality 4.4% GCS <15 significantly predicts mortality Five fold risk death from GLF than younger population Spaniolas, J.Trauma 2010; 69:
")
19 Injury Incidents Age / Gender NTDB (ACS COT) Report 2013

 Report")
20 Case Fatality Rate ISS / Age NTDB (ACS COT) Report 2013

 Report")
21 Case Fatality Age / Gender NTDB (ACS COT) Report 2013


22 Injuries Mechanism and Age

")
23 Weighted Estimates Age / Admisssion Year NTDB (ACS COT) Report 2013
24 Physiologic Reserve Definition: The Individual's Ability To Tolerate Injury Function of factors: Age Gender Preexisting disease Immunocompetence
25 Outcome Physiologic Reserve & Injury Severity Physiologic Reserve High ISS Physiologic Exhaustion / Death Moderate ISS Time
26 Occult Shock in Elderly Trauma Patient Several studies suggest that geriatric patients may suffer from occult hypoperfusion Normal vital signs give inadequate assessment tissue perfusion Identifying these patients using modalities other than physical examination and vital signs critical for optimizing their resuscitation Martin : Normal vital signs belie occult hypoperfusion in geriatric trauma patients. The American Surgeon, 76(1), Schulman: Predictors of Patients Who Will Develop Prolonged Occult Hypoperfusion following Blunt Trauma. J Trauma 57(4),
27 Diagnosing Shock in Elderly Trauma Patient Lactate and base deficit have been identified as one risk stratification tool Callaway: Serum Lactate and Base Deficit as Predictors of Mortality in Normotensive Elderly Blunt Trauma Patients. The Journal of Trauma: Injury, Infection, and Critical Care, 66(4), Jansen: Early Lactate-Guided Therapy in Intensive Care Unit Patients: A Multicenter, Open-Label, Randomized Controlled Trial. American Journal of Respiratory and Critical Care Medicine, 182(6), Neville: Mortality risk stratification in elderly trauma patients based on initial arterial lactate and base deficit levels. The American Surgeon, 77(10),
28 SBP vs Mortality All Patients (n=870,634) % Mortality Base Deficit % Mortality Base Deficit Systolic Blood Pressure in ED Eastridge: Hypotension Begins at 110 mmhg: Redefining Hypotension with Data. J Trauma, 63: , 2007
29 Age vs Mortality Age vs Mortality 8 % Mortality Age (years) Age vsmortality Stratified by Gender Male Female SBP vs Mortality Stratified by Young /Old % Mortality Age < 43 Age >= Systolic Blood Pressure in the ED % Mortality Age (years) Eastridge: Hypotension Begins at 110 mmhg: Redefining Hypotension with Data. J Trauma, 63: , 2007
30 Risk of Undertriagein Geriatric Trauma Chang et al. 2008: 10 year retrospective review in Maryland 25,565 patients Risk of under-triage in age group 65 was significantly greater than younger group (independent risk factor) 49.9% vs. 17.8% Chang: Undertriage of elderly trauma patients. Arch Surg. 2008;143
31 Geriatric ATLS AMPLE history A - Airway with C-spine protection B -Breathing C - Circulation with hemorrhage control D -Disability E - Exposure / Environment
32 AMPLE History Allergies Medications (particularly those with effect on hemodynamics or coagulation) Anticoagulants Antiplatelets Beta blockers Antihypertensives Past medical history Cardiac disease Neurologic disease Prior surgery Pacemaker / defibrillator Last meal High risk complications of aspiration Events (non-traumatic events that may have precipitated injury) Acute coronary syndrome Hypovolemia Sepsis /pneumonia Stroke Syncopal episode
33 Airway Inspect oral cavity Poorly fitting, loose dental appliances Airway protection Shock Chest trauma Mental status changes Pitfalls Loss of kyphotic curve, spondylolysis, arthritis Spinal canal stenosis, decrease cervical spine mobility RSI-elderly Increase sensitivity opioids, benzos, sedatives
34 Breathing Aging effects on pulmonary function Osteoporosis Decreased rib durability Increased incidence rib/sternal fxs Pulmonary contusion even from low energy trauma Weakened respiratory muscles/degenerative changes Decrease chest wall compliance Decrease pulmonary function-vc, FRC, I and E force Limited ability to compensate Blunted responses to hypoxia and hypercarbia and acidosis Delay onset clinically apparent signs impending distress Adjunct ABG/lactate
35 Chest Wall Injury Very common injury in elderly- due to brittle rib cage Compared to younger patients Same chest AIS Increased mortality, ICU days, LOS, vent days. Mortality increased at 5 ribs fxs. (35% vs 10%) Mortality decreased with epidural use. J. Trauma 2000: 48(6) p 1040
36 Rib Fractures in the Elderly o Retrospective review of 277 with rib fractures patients admitted to Level 1 Trauma Center o Study population o Age > 64 o Matched Controls o Age o Severity of Injury o Mean chest AIS: 3.0 vs. 3.0 o Mean ISS: 20.7 vs o Mean Rib fx: 3.6 vs. 4.0 Bulger: Rib fractures in the elderly. J Trauma Jun;48(6):1040-6
37 Rib Fractures in the Elderly o Ventilator days: o 4.3 vs. 3.1 o ICU LOS: o 6.1 vs. 4.0 o Hospital LOS o 15.4 vs o Mortality: o 22% vs. 10% (p < 0.01). o Each additional rib fracture: o Increases Mortality 19% o Risk of pneumonia 27% Bulger: Rib fractures in the elderly. J Trauma Jun;48(6): J Trauma. 2000; 48:
38 Circulation/Resuscitation Normal BP- occult shock Judicious fluids, blood and blood products Adjunct: ABG/lactate/base deficit Serial evaluation in triage and resuscitation Base deficit marker of severe injury / mortality Base deficit -5 meq/l or higher less than 23% mortality Base deficit -6 meq/l or worse 60% mortality
39 Disability GCS TBI Precipitating neurologic event Highly correlated with outcome Lateralizing signs Incidence spine / spinal cord injury
40 Traumatic Brain Injury(TBI) Brain injury risk factors Cerebral atrophy / concommitantincrease intracranial space Delayed presentation extra axial hemorrhage More susceptible traumatic tears bridging veins (subdural hematoma) >65 y/o 2-5x mortality of younger groups with matched GCS/intra-cranial pathology Early diagnosis and management central to improve outcomes
41 Management Coagulopathy Elderly patients who were taking medications for systemic anticoagulation before their injury Assessment of their coagulation profile as soon as possible after admission. Expeditious head CT
42 Coagulopathy Management Coagulopathy after injury if the elderly population is associated with worse outcomes than similar injury in other age strata. Patients receiving warfarin with a posttraumatic intracranial hemorrhage should receive therapy to correct their international normalized ratio (INR) within 2 hours of admission.
43 Coagulopathy Management TEG / platelet mapping assay Specific therapy Warfarin (factor repletion) FFP Profilnine (Factor II, VII, IX, X) Anti-platelet (most not reversible) Transfuse platelets Serial assessment residual platelet activity
44 Geriatric Brain Injury Outcomes Highly correlated with recovery from brain injury Elderly patients with severe traumatic brain injury (GCS 8) At least 80% mortality or long term placement disposition Justifies discussion regarding goals of care after resuscitation Futility Advance directives LeBlanc: Comparison of functional outcome following acute care in young, middleaged and elderly patients with traumatic brain injury. Brain Inj. 2006;20:
45 Exposure Elderly trauma risks for hypothermia and pressure ulceration Poor nutrition / loss of lean muscle mass Microvascular changes Blunted hypothalamic function Rectal temperature and rewarming methods Reduce incidence of hypothermia associated coagulopathy Off back board, clear cervical collar, spine ASAP
46 Dedicated Geriatric Care G-60 Model Dedicated intensive geriatric injury care management programs compared to standard trauma programs Decreased mortality Decreased ICU length of stay and decreased hospital length of stay Decreased time to OR Diminished rate of pulmonary complications Mangram:, J.Trauma 2012;72:
47 Geriatric Consultation Geriatric consultation Comprehensive Geriatric Assessment (CGA) Multi-disciplinary diagnostic instrument Data on medical, psychological, functional capabilities and limitation in geriatric patients Develops treatment and follow-up plans 22 randomized trials / > 10,000 patients Outcomes Increased survival and likelihood to be home at 1 year Fewer episodes of delirium Decrease in-patient falls Decreased length of stay Decreased complication
48 EAST CPG Management Injury in Elderly Elderly trauma patients should be treated at centers that have appropriate resources TBI with warfarin-induced coagulopathy, the coagulation profile should be immediately assessed and corrected as necessary Base deficit > 5mEq/L should be used as a marker for severe injury and admission to ICU GCS 8, persistent after 72 hrswarrants discussion regarding goals / endpoints of care
49 Factors Predictive Post-Hospitalization Functional Decline and Poor Quality of Life Pre-Operative Age > 70 years Comorbid conditions Diabetes, CHF, neoplasia Functional Impairment in > 2 ADLs Cognitive impairment (dementia) Low level social activity (mobility or depression) Post-Operative Poorly controlled pain Delirium Arora: J Am Geriatr Soc 2007; 55: ; Manku and Leung Anesth Analg 2003; 96:
50 Conclusion Rapid assessment / clinical and radiographic (Head CT especially important) Correction of coagulopathy with extraaxiallesion and anticoagulants GCS < 8 associated with poor outcome Realistic expectation outcomes Communication with families Multidisciplinary team and treatment plan to reduce complications and improve outcome
51 Conclusion Elderly population (>65) majority of trauma admissions over the next three decades Elderly trauma patients Anatomic/physiologic differencs Limited physiologic reserve High index suspicion Occult shock Base deficit assessment Low threshold ICU admission Consider triage to designated trauma centers
52 CE NUMBER
Trauma resuscitation in the Elderlyfrom a physiological perspective
 6 November 2017 Trauma resuscitation in the Elderlyfrom a physiological perspective Joseph Mathew Consultant, Emergency/ 6 November 2017 2 http://www.who.int/ageing/publications/global_health.pdf 6 November
6 November 2017 Trauma resuscitation in the Elderlyfrom a physiological perspective Joseph Mathew Consultant, Emergency/ 6 November 2017 2 http://www.who.int/ageing/publications/global_health.pdf 6 November
Goals. Geriatric Trauma. What s the impact Erlanger Trauma Symposium
 Geriatric Trauma William S. Havron III MD Assistant Professor of Surgery University of Oklahoma Goals Realize the impact of injuries in the ageing population Identify the pitfalls associated with geriatric
Geriatric Trauma William S. Havron III MD Assistant Professor of Surgery University of Oklahoma Goals Realize the impact of injuries in the ageing population Identify the pitfalls associated with geriatric
Multidisciplinary Geriatric Trauma Care Guideline
 Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Improving Healthcare Utilization in Injured Older Adults
 Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Chapter 39 Trauma in the Elderly
 Chapter 39 Trauma in the Elderly Episode Overview 1) 5 Risk Factors for falls in the elderly? 2) What anatomic and physiologic changes in the elderly patient are important for the management of trauma
Chapter 39 Trauma in the Elderly Episode Overview 1) 5 Risk Factors for falls in the elderly? 2) What anatomic and physiologic changes in the elderly patient are important for the management of trauma
Geriatric (Orthopaedic) Trauma
 Trauma") Geriatric (Orthopaedic) Trauma Brian Buck, DO March 3, 2017 31st Annual Geriatric Conference Pearls of Geriatric Care Do not regret growing older. It is a privilege denied to most Overview East Guidelines
Geriatric (Orthopaedic) Trauma Brian Buck, DO March 3, 2017 31st Annual Geriatric Conference Pearls of Geriatric Care Do not regret growing older. It is a privilege denied to most Overview East Guidelines
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Geriatric Trauma Resuscitation: Lessons from a Geriatric Trauma Surgeon
 Geriatric Trauma Resuscitation: Lessons from a Geriatric Trauma Surgeon Aurelio Rodriguez, M.D., FACS Conemaugh Memorial Medical Center Trauma Center Johnstown, PA Demographics The fastest growing age
Geriatric Trauma Resuscitation: Lessons from a Geriatric Trauma Surgeon Aurelio Rodriguez, M.D., FACS Conemaugh Memorial Medical Center Trauma Center Johnstown, PA Demographics The fastest growing age
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami
 Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Saman Arbabi M.D., M.P.H., F.A.C.S. Kathleen O'Connell M.D. Bryce Robinson M.D., M.S., F.A.C.S., F.C.C.M
 Form "EAST Multicenter Study Proposal" Study Title Primary investigator / Senior researcher Email of Primary investigator / Senior researcher Co-primary investigator Are you a current member of EAST? If
Form "EAST Multicenter Study Proposal" Study Title Primary investigator / Senior researcher Email of Primary investigator / Senior researcher Co-primary investigator Are you a current member of EAST? If
EAST MULTICENTER STUDY DATA DICTIONARY
 EAST MULTICENTER STUDY DATA DICTIONARY Does the Addition of Daily Aspirin to Standard Deep Venous Thrombosis Prophylaxis Reduce the Rate of Venous Thromboembolic Events? Data Entry Points and appropriate
EAST MULTICENTER STUDY DATA DICTIONARY Does the Addition of Daily Aspirin to Standard Deep Venous Thrombosis Prophylaxis Reduce the Rate of Venous Thromboembolic Events? Data Entry Points and appropriate
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Chapter 2 Triage. Introduction. The Trauma Team
 Chapter 2 Triage Chapter 2 Triage Introduction Existing trauma courses focus on a vertical or horizontal approach to the ABCDE assessment of an injured patient: A - Airway B - Breathing C - Circulation
Chapter 2 Triage Chapter 2 Triage Introduction Existing trauma courses focus on a vertical or horizontal approach to the ABCDE assessment of an injured patient: A - Airway B - Breathing C - Circulation
Cases from the Streets. Kelly Buchanan MD, ATC/L EMS Fellow December, 2011
 Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
TRAUMA ALERT: THE OLDER ADULT TRAUMA PATIENT - FIX ME QUICK
 TRAUMA ALERT: THE OLDER ADULT TRAUMA PATIENT - FIX ME QUICK Alicia Mangram, MD, FACS HonorHealth John C. Lincoln Medical Center Learning Objectives: Prevalence of geriatric trauma. New management strategies.
TRAUMA ALERT: THE OLDER ADULT TRAUMA PATIENT - FIX ME QUICK Alicia Mangram, MD, FACS HonorHealth John C. Lincoln Medical Center Learning Objectives: Prevalence of geriatric trauma. New management strategies.
TRAUMA AND THE GERIATRIC PATIENT. Janine Clift, RN Geriatric Emergency Nurse University Hospital Emergency Department, LHSC April 28, 2011
 TRAUMA AND THE GERIATRIC PATIENT Janine Clift, RN Geriatric Emergency Nurse University Hospital Emergency Department, LHSC April 28, 2011 ELDERLY PATIENT ARE NOT JUST OLDER ADULTS Fraility is like pornography,
TRAUMA AND THE GERIATRIC PATIENT Janine Clift, RN Geriatric Emergency Nurse University Hospital Emergency Department, LHSC April 28, 2011 ELDERLY PATIENT ARE NOT JUST OLDER ADULTS Fraility is like pornography,
Under Triage and Anticoagulants in the Geriatric Trauma Population Fragile Must be Italian. Barry McKenzie, MD St. Vincent Healthcare
 Under Triage and Anticoagulants in the Geriatric Trauma Population Fragile Must be Italian Barry McKenzie, MD St. Vincent Healthcare Objectives Describe the increasing frequency of trauma patients being
Under Triage and Anticoagulants in the Geriatric Trauma Population Fragile Must be Italian Barry McKenzie, MD St. Vincent Healthcare Objectives Describe the increasing frequency of trauma patients being
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
CRACKCast E181 Approach to the Geriatric Patient
 CRACKCast E181 Approach to the Geriatric Patient Italicized text refers to passages quoted from Rosen s Emergency Medicine (9 th Ed). Key concepts: We are in the midst of a silver tsunami, with 10,000
CRACKCast E181 Approach to the Geriatric Patient Italicized text refers to passages quoted from Rosen s Emergency Medicine (9 th Ed). Key concepts: We are in the midst of a silver tsunami, with 10,000
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
The research questions are presented in priority order, and are further elaborated with lay summaries and three-part questions where applicable.
 Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Chapter Goal. Learning Objectives 9/12/2012. Chapter 36. Geriatrics. Use assessment findings to formulate management plan for geriatric patients
 Chapter 36 Geriatrics Chapter Goal Use assessment findings to formulate management plan for geriatric patients Learning Objectives Describe dependent & independent living environments Identify local resources
Chapter 36 Geriatrics Chapter Goal Use assessment findings to formulate management plan for geriatric patients Learning Objectives Describe dependent & independent living environments Identify local resources
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool
 Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Geriatric Emergencies. Lesson Goal. Lesson Objectives 9/10/2012. Introduce ways geriatric patients differ from other patients
 Geriatric Emergencies Lesson Goal Introduce ways geriatric patients differ from other patients Physiologic changes of aging Communication issues Effects of medications Common fears of elderly patients
Geriatric Emergencies Lesson Goal Introduce ways geriatric patients differ from other patients Physiologic changes of aging Communication issues Effects of medications Common fears of elderly patients
Episode 66 Backboard and Collar Nightmares from EMU Conference. The Risks Associated with Backboard & Collar
 However, backboards and collars are not without risk: Episode 66 Backboard and Collar Nightmares from EMU Conference With Dr. Kylie Bosman Prepared by Dr., edited by Dr. Kylie Bosman & Anton Helman, May
However, backboards and collars are not without risk: Episode 66 Backboard and Collar Nightmares from EMU Conference With Dr. Kylie Bosman Prepared by Dr., edited by Dr. Kylie Bosman & Anton Helman, May
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD
 ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department
 Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Critical care resources are often provided to the too well and as well as. to the too sick. The former include the patients admitted to an ICU
 Literature Review Critical care resources are often provided to the too well and as well as to the too sick. The former include the patients admitted to an ICU following major elective surgery for overnight
Literature Review Critical care resources are often provided to the too well and as well as to the too sick. The former include the patients admitted to an ICU following major elective surgery for overnight
Epidural analgesia improves outcome after multiple rib fractures
 Epidural analgesia improves outcome after multiple rib fractures Eileen M. Bulger, MD, Thomas Edwards, PhD, MD, Patricia Klotz, RN, and Gregory J. Jurkovich, MD, Seattle, Wash Background. Rib fractures
Epidural analgesia improves outcome after multiple rib fractures Eileen M. Bulger, MD, Thomas Edwards, PhD, MD, Patricia Klotz, RN, and Gregory J. Jurkovich, MD, Seattle, Wash Background. Rib fractures
EAST MULTICENTER STUDY DATA COLLECTION TOOL
 EAST MULTICENTER STUDY DATA COLLECTION TOOL Multicenter Study: Effect of Regional Anesthesia on Delirium in Geriatric Trauma Patients with Multiple Rib Fractures Enrolling Center: Enrolling Co-investigators:
EAST MULTICENTER STUDY DATA COLLECTION TOOL Multicenter Study: Effect of Regional Anesthesia on Delirium in Geriatric Trauma Patients with Multiple Rib Fractures Enrolling Center: Enrolling Co-investigators:
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank
 Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank Michelle Shroyer, MPH, Russell Griffin, PhD, Vincent Mortellaro, MD, and Rob Russell MD, MPH Introduction Hemorrhage is
Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank Michelle Shroyer, MPH, Russell Griffin, PhD, Vincent Mortellaro, MD, and Rob Russell MD, MPH Introduction Hemorrhage is
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
HYPOTHERMIA IN TRAUMA. Kevin Palmer EMT-P, DiMM
 HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
Factors Contributing to Fatal Outcome of Traumatic Brain Injury: A Pilot Case Control Study
 Factors Contributing to Fatal Outcome of Traumatic Brain Injury: A Pilot Case Control Study D. HENZLER, D. J. COOPER, K. MASON Intensive Care Department, The Alfred Hospital, Melbourne, VICTORIA ABSTRACT
Factors Contributing to Fatal Outcome of Traumatic Brain Injury: A Pilot Case Control Study D. HENZLER, D. J. COOPER, K. MASON Intensive Care Department, The Alfred Hospital, Melbourne, VICTORIA ABSTRACT
9/29/2014. Geriatric Trauma: Case Presentation. Sam Arbabi, MD, MPH, FACS Professor of Surgery. Objectives. Please Define Geriatric. Geriatrics?
 Geriatric Trauma: Case Presentation Sam Arbabi, MD, MPH, FACS Professor of Surgery Geriatrics? Objectives Geriatric Trauma Cases Current accepted management Future? Please Define Geriatric Age: Higher
Geriatric Trauma: Case Presentation Sam Arbabi, MD, MPH, FACS Professor of Surgery Geriatrics? Objectives Geriatric Trauma Cases Current accepted management Future? Please Define Geriatric Age: Higher
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Effect of post-intubation hypotension on outcomes in major trauma patients
 Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES
 PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
Ron D. Robertson, MD FACS Professor of Surgery Director of Trauma, Critical Care, and Acute Care Surgery UAMS
 Ron D. Robertson, MD FACS Professor of Surgery Director of Trauma, Critical Care, and Acute Care Surgery UAMS Unknown Geriatric population Age 65 and older? Problem 1 Definition of Geriatric depends on
Ron D. Robertson, MD FACS Professor of Surgery Director of Trauma, Critical Care, and Acute Care Surgery UAMS Unknown Geriatric population Age 65 and older? Problem 1 Definition of Geriatric depends on
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
EMS Subspecialty Certification Review Course. Learning Objectives. Geriatric Patients and EMS Systems
 EMS Subspecialty Certification Review Course Challenges in Geriatric Patient Care 1.4.6 Geriatric Issues Version: 2017 Learning Objectives Upon the completion of this program participants will be able
EMS Subspecialty Certification Review Course Challenges in Geriatric Patient Care 1.4.6 Geriatric Issues Version: 2017 Learning Objectives Upon the completion of this program participants will be able
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Fall Prevention and hip protectors
 Presenter Disclosure Information Edgar Pierluissi Division of Geriatrics Edgar Pierluissi, MD Medical Director, Acute Care for Elders Unit, San Francisco General Hospital and Trauma Center Fall Prevention
Presenter Disclosure Information Edgar Pierluissi Division of Geriatrics Edgar Pierluissi, MD Medical Director, Acute Care for Elders Unit, San Francisco General Hospital and Trauma Center Fall Prevention
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
vel 2 Level 2 3,034 c-spine evaluations with CSR Level 3 detected injury only 53% of the time. Level 3 False (-) rate 47%
 rate 47%") Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Complex evaluation of polytrauma in intensive care with multiple severity scores
 UNIVERSITY OF MEDICINE AND PHARMACY CRAIOVA DOCTORAL SCHOOL PhD THESIS Complex evaluation of polytrauma in intensive care with multiple severity scores Superviser Coordinator Prof. Univ. Dr. Florea Purcaru
UNIVERSITY OF MEDICINE AND PHARMACY CRAIOVA DOCTORAL SCHOOL PhD THESIS Complex evaluation of polytrauma in intensive care with multiple severity scores Superviser Coordinator Prof. Univ. Dr. Florea Purcaru
Canon of Medicine in IL Nascher in > ALE:48. IOM 2008: Woefully Inadequate. Quality of Life (and Death) Patient Advocacy
 Patient Advocacy") Canon of Medicine in 1025 IL Nascher in 1909 -> ALE:48 IOM 2008: Woefully Inadequate Quality of Life (and Death) Patient Advocacy Changes in physiology due to aging. Chronic, progressive disease processes.
Canon of Medicine in 1025 IL Nascher in 1909 -> ALE:48 IOM 2008: Woefully Inadequate Quality of Life (and Death) Patient Advocacy Changes in physiology due to aging. Chronic, progressive disease processes.
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
APPLYING THE CTAS to Appropriately Prioritize the Elderly
 APPLYING THE CTAS to Appropriately Prioritize the Elderly Presenter: Michael J Bullard MD Professor, Department of Emergency Medicine, University of Alberta, Past Co-Chair and current member CTAS NWG Faculty/Presenter
APPLYING THE CTAS to Appropriately Prioritize the Elderly Presenter: Michael J Bullard MD Professor, Department of Emergency Medicine, University of Alberta, Past Co-Chair and current member CTAS NWG Faculty/Presenter
Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017
 patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017") Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017 CONTENT WHO is the critically ill elderly (geriatric) patient? WHY look at the critically
Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017 CONTENT WHO is the critically ill elderly (geriatric) patient? WHY look at the critically
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Correlation of D-Dimer level with outcome in traumatic brain injury
 2014; 17 (1) Original Article Correlation of D-Dimer level with outcome in traumatic brain injury Pradip Prasad Subedi 1, Sushil Krishna Shilpakar 2 Email: Abstract Introduction immense. The major determinant
2014; 17 (1) Original Article Correlation of D-Dimer level with outcome in traumatic brain injury Pradip Prasad Subedi 1, Sushil Krishna Shilpakar 2 Email: Abstract Introduction immense. The major determinant
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL
 HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL Gaylan Rockswold, MD, PhD, Principal Investigator William Barsan, MD, Principal Investigator, CCC, SIREN Byron
HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL Gaylan Rockswold, MD, PhD, Principal Investigator William Barsan, MD, Principal Investigator, CCC, SIREN Byron
Screening and Management of Blunt Cereberovascular Injuries (BCVI)
") Grady Memorial Hospital Trauma Service Guidelines Screening and Management of Blunt Cereberovascular Injuries (BCVI) BACKGROUND Blunt injury to the carotid or vertebral vessels (blunt cerebrovascular injury
Grady Memorial Hospital Trauma Service Guidelines Screening and Management of Blunt Cereberovascular Injuries (BCVI) BACKGROUND Blunt injury to the carotid or vertebral vessels (blunt cerebrovascular injury
TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines
 TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines DATE: 11 April 2014 CONTEXT AND POLICY ISSUES Traumatic brain
TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines DATE: 11 April 2014 CONTEXT AND POLICY ISSUES Traumatic brain
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
INDEX&NEUROTRAUMA&(INCLUDING&SPINAL&CORD&INJURIES)&!!
&!!") 1 INDEX&NEUROTRAUMA&(INCLUDING&SPINAL&CORD&INJURIES)& Prehospital,care,in,patients,with,severe,traumatic,brain,injury:,does,the,level,of,prehospital, care,influence,mortality?,...,3 Contralateral,extraaxial,hematomas,after,urgent,neurosurgery,of,a,mass,lesion,in,patients,
1 INDEX&NEUROTRAUMA&(INCLUDING&SPINAL&CORD&INJURIES)& Prehospital,care,in,patients,with,severe,traumatic,brain,injury:,does,the,level,of,prehospital, care,influence,mortality?,...,3 Contralateral,extraaxial,hematomas,after,urgent,neurosurgery,of,a,mass,lesion,in,patients,
4. Which survey program does your facility use to get your program designated by the state?
 TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
2. To provide an ethical, moral and practical framework for decision-making during a public health emergency.
 November 2010 TABLE TOP EXERCISE PARTICIPANT GUIDE When Routine Critical Care Resources Are Not Available Time expectations for each session: SECTION ACTIVITY TIME I Introduction 5 minutes II Exercise
November 2010 TABLE TOP EXERCISE PARTICIPANT GUIDE When Routine Critical Care Resources Are Not Available Time expectations for each session: SECTION ACTIVITY TIME I Introduction 5 minutes II Exercise
ARTICLES THAT HAVE CHANGED MY INPATIENT PRACTICE OF MEDICINE
 ARTICLES THAT HAVE CHANGED MY INPATIENT PRACTICE OF MEDICINE 2016 17 Melissa (Moe) Hagman, MD, FACP Associate Professor, Internal Medicine/Palliative Medicine mhagman@uw.edu SYNCOPE 72 year old otherwise
ARTICLES THAT HAVE CHANGED MY INPATIENT PRACTICE OF MEDICINE 2016 17 Melissa (Moe) Hagman, MD, FACP Associate Professor, Internal Medicine/Palliative Medicine mhagman@uw.edu SYNCOPE 72 year old otherwise
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Guideline for Treatment of Head Injury in the Anticoagulated Patient
 Guideline for Treatment of Head Injury in the Anticoagulated Patient GUIDELINE: GUIDELINE FOR TREATMENT OF HEAD INJURY IN THE ANTICOAGULATED PATIENT BACKGROUND: Chronic anticoagulation therapy is used
Guideline for Treatment of Head Injury in the Anticoagulated Patient GUIDELINE: GUIDELINE FOR TREATMENT OF HEAD INJURY IN THE ANTICOAGULATED PATIENT BACKGROUND: Chronic anticoagulation therapy is used
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA?
 WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
Use of CT in minor traumatic brain injury. Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD
 Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders. William L. Bograkos, MA, DO, FACOEP
 Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders Toxic Brain Disorders William L. Bograkos, MA, DO, FACOEP TBI: Traumatic Brain Injury / Toxic Brain Injury (Trauma and Substance
Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders Toxic Brain Disorders William L. Bograkos, MA, DO, FACOEP TBI: Traumatic Brain Injury / Toxic Brain Injury (Trauma and Substance
Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma
 Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma Abbas PI 1,2, Carpenter K 2, Sheikh F 1,2, Peterson ML 1,2, Kljajic M 1, Naik-Mathuria B 1,2 1 Texas Children s Hospital
Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma Abbas PI 1,2, Carpenter K 2, Sheikh F 1,2, Peterson ML 1,2, Kljajic M 1, Naik-Mathuria B 1,2 1 Texas Children s Hospital
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,