TRAILS & Tribulations
|
|
|
- George Harrison
- 6 years ago
- Views:
Transcription
1 TRAILS & Tribulations Choosing between common fitness-to-drive office-based screening tests Dr. Frank Molnar CanDRIVE ( ) Co-Chair, Champlain Dementia Network ( ) Medical Director, Regional Geriatric Program of Eastern Ontario ( ) Associate Professor of Medicine, University of Ottawa and Staff Geriatrician, Division of Geriatric Medicine, The Ottawa Hospital
2 Conflict of interests None No Pharmaceutical Industry support More relevant to driving No Automotive Insurance Industry support
3 Objectives To highlight the complexity of the assessment of fitness to drive To compare commonly promoted screening tests (MMSE, Clock, MOCA, Trails B, SIMARD) To provide a practical approach to assessing fitness to drive in dementia
4 Projections Projected Change in Collisions by Driver Age ( ) Projected Increase in Casualty Crashes by Age ( ) Projected Percent Increase < Projected INCREASE Fatalities Injuries < Age Range AGE Source: L Écuyer et al. (2006). Transport Canada
5 A Major Public Health Concern When involved in a crash, seniors are over 4 times more likely to be seriously injured and hospitalized than are drivers years of age. Treatment of injuries to seniors is more costly, recovery slower, less complete. Majority of crash-injured seniors were driving the vehicle. Most (3 of 4) crashes involving older drivers are multiple vehicle crashes (e.g. merging into traffic, left hand turns across oncoming traffic).
6 Assessment of Fitness-to-Drive The Complexity of the Medical Driving Evaluation
7 It is Not Age Medical conditions and medications are the primary cause of declines in older driver competence. Can make even the best of drivers unsafe to drive. Can affect drivers of any age: Increasingly likely as we age due to the cumulative effect of multiple diseases. Not merely the presence but severity and/or instability of conditions +/- high doses and/or changing doses of medications Medical community best placed to first recognize possibly impairing medical conditions / medications.
8 Medical conditions that when severe, poorly controlled or changing rapidly can impact on driving 3Ds: Dementia / Delirium / Depression Diabetes vision and hearing cardiac disease Stroke Parkinson s Arthritis Sleep apnea etc
9 Medications / substances that can affect driving during dose changes (period of acclimatization) or at high doses (above threshold at which one can acclimatize) Benzodiazepines Narcotics Anticholinergic medications e.g.: tricyclic antidepressants, antipsychotics, oxybutynin, detrol, gravol Antihistamines Seizure meds e.g.: phenytoin, phnobarbital, Gabapentin / pregabalin, clobazam Parkinson s meds (Sinemet ) Alcohol Cannabis etc
10 Effects of Medical Conditions and Medications Multiple Domains can be affected: Physical: weakness; slow / limited movement Sensory: vision loss; limited feeling in limbs Cognitive/Perceptual: slowed thinking; decreased attention Emotional: anxiety, panic reactions
11 Effect of Behavior
12 Realistic Conclusions No screening or assessment protocol will ever predict 100% of risk of Motor Vehicle Crash (MVC) Only test stable intrinsic features operational > tactical, strategic Miss new or fluctuating illness, or behavior in non-testing real life situations Cannot predict extrinsic factors weather, other drivers, road conditions, car malfunction Full complexity cannot be fully addressed with time available in front-line clinical settings Therefore objective is to improve not to perfect the assessment of fitness to drive
13 Let s focus on Dementia
14 Estimated Numbers of Drivers with Dementia in Ontario , ,803 14,909 30,642 24,083 32,373 34, from Hopkins, et al., (2004)
15 Conclusions of Consensus Guidelines regarding Driving and Dementia Recognize limitations of data those with moderate to severe dementia should not drive Canadian Medical Association: Moderate = 1 ADL or 2 iadls impaired due to cognition (CMA guidelines currently being revised) individual assessment for those with mild dementia What does this really mean?? gold standard is comprehensive on-road assessment Ministry on road
16 Individualized Assessment Based on expert opinion recommend tests such as MMSE, Clock Drawing, Trails B Lack of operating instructions (i.e. lack of guidance regarding how to interpret the results of the tests) Do not provide guidance regarding HOW physicians are to apply such tests (e.g. how to respond to different scores, what cut-offs to use, which errors = automatic failure )




17 Screening (detection of a potential problem); MoCA In this corner MMSE
18 MMSE vs. MOCA Folstein Mini-Mental State Exam (MMSE) Limited sensitivity - misses cases of mild dementia or Mild Cognitive Impairment. Higher False Negative Rate Good specificity less likely to label people with normal cognition as impaired Copyrighted (we should be paying to use it) Large body of supportive literature Does not test Executive function Montreal Cognitive Assessment Test (MOCA) Great website see Great sensitivity picks up cases of mild dementia or Mild Cognitive Impairment. Limited specificity Labels some people with normal cognition as impaired (Higher False Positive Rate) Copyrighted but do not charge to use Limited body of supporting literature and validation studies flawed.
19 Lack of evidence-based cut-offs Clinical Utility of Office-Based Cognitive Predictors of Fitness to Drive in Persons with Dementia: A Systematic Review. (Molnar, Marshall, Man-Son-Hing et al., JAGS 2006; 54: ) No cognitive tests that could potentially be used in an office-setting had cut-off scores validated in persons with dementia! That does NOT mean the tests cannot be useful BUT haven t cut-offs been recommended for Trails B????
20 TRAILS B Work of Dr. Mononita Roy, Geriatric Fellow University of Ottawa Presented at Canadian Geriatrics Society national meeting April 2011
21 Trails A
22 Trails B
23 Trails B: 180 second cut-off? A time of over 180 sec for completion of Trails B is often recommended as a cut-off for intervention. The origin of this 180 sec cut-off comes from the following non driving-related studies: Fals-Stewart 1992 Franzen 1996 Tombaugh 2004
24 Tombaugh, T. Trail Making Test A and B: Normative data stratified by age and education. Archives of Clinical Neuropsychology 19(2004) Presented normative data for Trails A and B for 911 communitydwelling individuals aged years. Performance on both Trails A and B decreased with increasing age and lower levels of education. Q? Do people get more time to stop a car just because they are older? Q? If not, does being within the boundaries of normative data really mean someone is safe to drive? Based on these results, the norms were stratified for age (11 groups) and education levels (2 groups 0-12 years and 12+ years).
25 Tombaugh 2004: Normative Data for Trails A and B Method Convenience sample Subjects were selected from participants in other studies. These may be individuals who are more willing to participate, more confident etc. May not be a representative sample, thus introducing bias. Is this truly a disease-free sample? Self-reported medical and psychiatric hx. Medical hx and dx of absence of cognitive impairment may not be up-to-date as done when recruiting for previous studies. All subjects had MMSE >23 (mean 28.6, SD 1.5) and GDS <14 (mean 4.1, SD 3.4) with fairly tight confidence intervals. But, MMSE does not test executive function. At lower end of MMSE score and GDS, could still have some subjects with mild cognitive impairment or depressive sx who were included in the study.
26 Normative Data for Trails A and B Scores on Trails A and B increased with increasing age and fewer years of education. All mean times for Trails B were under 180 seconds, so it seems that the 3 minute cut off does mean something.


27 Table 3: Percentiles for Trails A and B scores for each normative group Even as age increases, most people still are able to complete Trails B in <180 sec, with the lowest percentiles taking longer than 180 sec. Again, suggests 180 sec as a threshold? Our job is to identify these individuals who are outliers and forward them on for further neuropsychology testing or on road driving evaluation.
28 Our conclusions from Tombaugh 2004 article This convenience sample may not have been representative of completely healthy, cognitively intact individuals. Many groups had small sample sizes, so use caution in interpreting these scores (especially age group 85-89). Mean time to complete Trails B is under 180 seconds for all age groups, so this may indicate that this is a meaningful threshold. However, even if these are true norms for healthy people, being in a normative range may not necessarily mean the patient is safe to drive. As age increases, outliers in the lowest percentiles take longer than 180 seconds to complete Trails B Our job is to identify these individuals and refer them on for further testing.
29 Trails B and Driving Trails B Number of studies 31 out of total 32 Positive association (p<0.05) = 20 studies No association (p>0.05) = 11 studies - True negatives + false Negatives (due to small sample size) Cut-off scores Very sparse evidence based support. Ball seconds Staplin seconds Mazer 1998 < 3 errors Cut-offs reported (justification unclear) Marottoli seconds Wang seconds
30 Trails B and Driving This does not mean Trails B is useless As performance progressively worsens with longer and longer times and / or more errors (not due to language or education) then clinicians can become increasingly comfortable stating a patient has a functional impairment that may increase risk of crash E.g. 10 minutes and 10 errors unlikely any MD would allow such a person to drive. This follows the principle of the Ontario Highway Traffic Act where MDs must report drivers who have findings that may indicate lack of fitness to drive. Where to set the borderline cut-off (3 minutes and 3 errors?) requires further research and discussion.
31
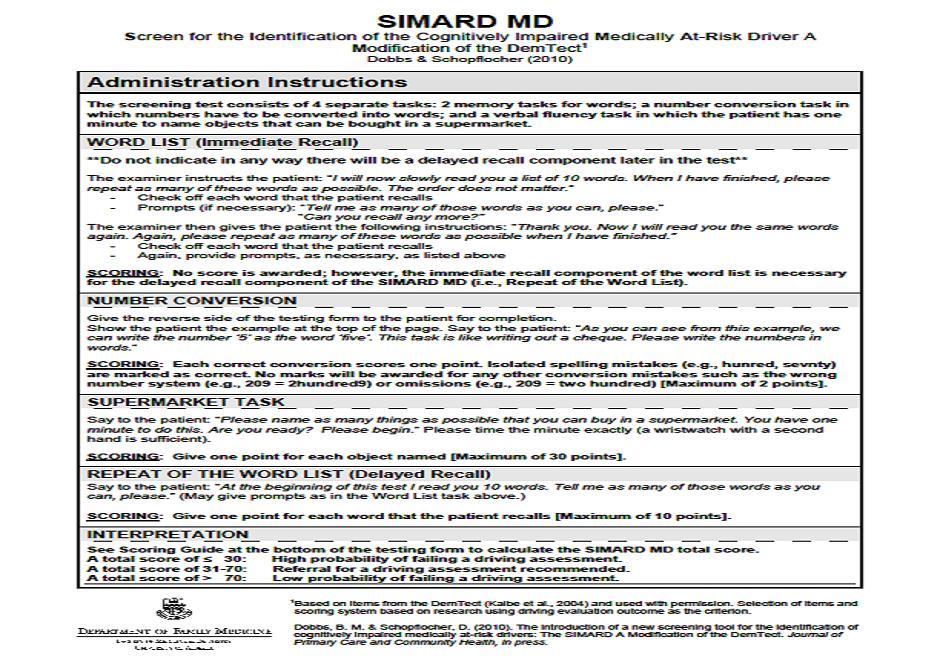
32 SIMARD Cut-offs were 30 and 70 Those who scored 30 or less 85.7% failed the on-road test 14.3% passed on-road Those who scored 31 to % failed on-road test 55.1% passed on-road test Those who scored 70 or more 16.1% failed on-road test 83.7% passed on-road test

33 THE FUTURE CanDRIVE Prospective Cohort Study older drivers followed for 5 years to attempt to derive better screening and assessment tests for fitnessto-drive Will look at MMSE, Clock, MOCA, Trails, SIMARD + develop new tests
34 Using Tests Intelligently The MMSE, Clock, MOCA, Trails B and SIMARD can provide a rough framework for assessing driving safety. Like any screening tool they can generate false results if not applied appropriately The information obtained from them can also be optimized through intelligent application
35 Is the Test result consistent with other evidence? Are the results of the test consistent with (what you would expect to find given) History provided by patient, caregiver, family Other tests Do the results fit with other tests done? OR is this single test an outlier and possibly not reflective of the patient s true functional ability
36 Make certain you know what you are really measuring Make certain low scores are not due to confounding variables: language barrier low education performance anxiety sensory deficits
37 Consider TRAJECTORY Consider whether the patient s function is: Expected to improve; Delirium, recent head injury, recent stroke etc. Expected to remain stable; stable head injury, stable stroke etc. Expected to decline; Dementia, Parkinson's, recurrent delirium etc.
38 Understand your role The role of Health Care Professionals is NOT to determine fitness-to-drive The role is to report drivers who have clinical findings that may indicate lack of fitness to drive. Ontario Highway Traffic Act The Ministry of Transportation makes the decision regarding fitness-to-drive in part based on accurate, fair and timely information from Health Care Professionals

39 Use common sense Sometimes it is obvious a patient is not safe to drive Very low valid test scores Very dangerous behaviours Very significant physical limitations Very significant functional impairment


40 Understand cut-off scores For many health care measures, there is significant overlap between the scores of normals vs. the scores of those who are impaired This makes reliance on a single cut-off score challenging if not impossible.
41 % Overlapping Cognitive Scores (Dichotomization ) Unsafe drivers scores single cut-off Safe drivers scores % Trichotomization Fail uncertain, needs further testing Pass Fail Pass Cognitive score Cognitiv e score
42 Applying Trichotomization Given the results of the cognitive test would you get in the car with the patient driving? Would you let a loved one get in a car with the patient driving? Would you want to be crossing a street (or have a loved one cross a street) in front of a car with the patient driving? These questions help you get off the fence. 3 answers are possible Yes (no concerns to trigger further testing) Uncertain (need more testing) Absolutely not (risk is clear)

43 Putting it all together the approach
44 Use Tests in the context of a more detailed approach (i.e. tests do not stand alone) Health Care Practitioners Resources Safety and Security Driving The Driving and Dementia Toolkit for Health Professionals ( ) Right click and Open Hyperlink Dr. Anna Byszewski et al (Toolkit overall) Dr. Bill Dalziel (10 step approach)
45 The Driving and Dementia Toolkit for Health Professionals 1. Dementia Type Generally, Lewy body dementia (fluctuations, hallucinations, visuospatial problems) and frontotemporal dementias (if associated behaviour or judgment issues) are unsafe. 2. Functional Impact of the Dementia - According to CMA guidelines, unsafe if: Impairment of >1 IADL due to cognition (IADLs mnemonic = SHAFT: Shopping, Housework/Hobbies, Accounting [banking, bills, taxes], Food preparation, Telephone / Tools / Transportation [driving]) OR impairment of 1 or more personal ADLs due to cognition (ADLs mnemonic = DEATH: Dressing, Eating, Ambulation, Toileting, Transfers, Hygiene) 3. Family Concerns (Ask in a room separate from the patient) Family feels safe/unsafe (make sure family has recently been in the car with the person driving). The granddaughter question Would you feel it was safe if a 5-year-old granddaughter was in the car alone with the person driving? (Often different response from family s answer to previous question) Generally if the family feels the person is unsafe to drive, they are unsafe. If the family feels the person is safe to drive, they may still be unsafe as family may be unaware or may be protecting the patient. 4. Visuospatial Issues (Intersecting pentagons/clock-drawing test) If major abnormalities, likely unsafe. 5. Physical Inability to Operate a Car (Often a physical reason is better accepted) Medical/physical concerns such as musculoskeletal problems, weakness/multiple medical conditions (neckturn, problems in the use of steering wheel/pedals), cardiac/neurological problems (episodic spells ).
46 The Driving and Dementia Toolkit for Health Professionals 6. Vision/Visual Fields Significant problems including visual acuity, field of vision. 7. Drugs (If associated with side effects drowsiness, slow reaction time, lack of focus) Alcohol, benzodiazepines, narcotics, neuroleptics, sedatives, Anticholinergic antiparkinsonian drugs, muscle relaxants, tricyclics, antihistamine (OTC), antiemetics, antipruritics, antispasmodics, others 8. Trail Making A and B (available at ). Trail Making A: Unsafe = >2 minutes or 2 or more errors Trail Making B: Safe = <2 minutes and <2 errors (0 or 1 error) Unsure = 2 3 minutes or 2 errors (consider qualitative dynamic information regarding how the test was performed slowness, hesitation, anxiety or panic attacks, impulsive or perseverative behaviour, lack of focus, multiple corrections, forgetting instructions, inability to understand test, etc.) Unsafe = >3 minutes or 3 or more errors 9. Ruler Drop Reaction Time Test (Accident Analysis and Prevention 2007;39: ) The bottom end of a 12 inch (30-cm) ruler is placed between thumb and index finger (1/2 inch [1 cm] apart) - let go and person tries to catch ruler (normal = 6-9 inches (15 22 cm); abnormal = 2 failed trials) 10.Judgment/Insight (Ask the person): What would you do if you were driving and saw a ball roll out on the street ahead of you? With your diagnosis of dementia, do you think at some time you will need to stop driving?
![YOUR HOMEWORK!!!! (Right click and Open Hyperlink) [1] Link to and review the Dementia and Driving Toolkit (http://www.rgpeo.](/docs-images/72/66279357/images/47-0.jpg "com/en/health-carepractitioners/resources/driving.aspx ) [2] Read about another approach based on Dr.")

47 YOUR HOMEWORK!!!! (Right click and Open Hyperlink) [1] Link to and review the Dementia and Driving Toolkit ( ) [2] Read about another approach based on Dr. Dalziel s 10 steps Approach to assessing fitness to drive in patients with cardiac and cognitive conditions ( Canadian Family Physician 2010;56:1123-9) 11/1123.full.pdf+html?sid=78 c25ba8-3cd8-4e80-94a0-26a92130d55b [3] Go to Alzheimer Knowledge Exchange ( x ) Dementia and Driving Resources hys Module
Driving & Cognitive Impairment: When to Suspect, How to Test, What to do?
 Driving & Cognitive Impairment: When to Suspect, How to Test, What to do? Dr. W.B. Dalziel Professor, Division of Geriatric Medicine University of Ottawa Regional Geriatric Program of Eastern Ontario Toronto
Driving & Cognitive Impairment: When to Suspect, How to Test, What to do? Dr. W.B. Dalziel Professor, Division of Geriatric Medicine University of Ottawa Regional Geriatric Program of Eastern Ontario Toronto
Would you let Granpa drive?
 Would you let Granpa drive? Driving and Cognitive Impairment When to suspect and how to test. What to do? Dr. Greg Thomson Family Physician Medical Program Lead Rehabilitation and Geriatrics Halton Healthcare
Would you let Granpa drive? Driving and Cognitive Impairment When to suspect and how to test. What to do? Dr. Greg Thomson Family Physician Medical Program Lead Rehabilitation and Geriatrics Halton Healthcare
Dementia and Driving Checklist
 6 Dementia and Driving Checklist 1. Questions to Ask the Patient and Family Patient Have you noticed any change or decreased confidence in your driving skills Have you had any accidents (or minor fender
6 Dementia and Driving Checklist 1. Questions to Ask the Patient and Family Patient Have you noticed any change or decreased confidence in your driving skills Have you had any accidents (or minor fender
Driving and Dementia Practical Tips for the Family Physician
 Driving and Dementia Practical Tips for the Family Physician L. Lee, MD, MClSc, CCFP, FCFP 2015 Canadian Medical Association. Determining fitness to operate motor vehicles: CMA Driver s Guide, 7th ed.
Driving and Dementia Practical Tips for the Family Physician L. Lee, MD, MClSc, CCFP, FCFP 2015 Canadian Medical Association. Determining fitness to operate motor vehicles: CMA Driver s Guide, 7th ed.
Driving and Dementia Practical Tips for the Family Physician. L. Lee, MD, MClSc, CCFP, FCFP 2014
 Driving and Dementia Practical Tips for the Family Physician L. Lee, MD, MClSc, CCFP, FCFP 2014 Medico-legal problems related to fitness to drive CMPA experience, 2005-2009: 67 medico-legal cases Half
Driving and Dementia Practical Tips for the Family Physician L. Lee, MD, MClSc, CCFP, FCFP 2014 Medico-legal problems related to fitness to drive CMPA experience, 2005-2009: 67 medico-legal cases Half
TO DRIVE OR NOT TO DRIVE: THAT IS THE QUESTION
 TO DRIVE OR NOT TO DRIVE: THAT IS THE QUESTION Gary Naglie, MD, FRCPC, FGSA Department of Medicine, Baycrest Geriatric Health Care Centre & University of Toronto Scientist, Rotman Research Institute, Baycrest
TO DRIVE OR NOT TO DRIVE: THAT IS THE QUESTION Gary Naglie, MD, FRCPC, FGSA Department of Medicine, Baycrest Geriatric Health Care Centre & University of Toronto Scientist, Rotman Research Institute, Baycrest
TO DRIVE OR NOT TO DRIVE: THAT IS THE QUESTION
 TO DRIVE OR NOT TO DRIVE: THAT IS THE QUESTION Gary Naglie, MD, FRCPC, FGSA Department of Medicine, Baycrest & University of Toronto Scientist, Rotman Research Institute, Baycrest & Toronto Rehabilitation
TO DRIVE OR NOT TO DRIVE: THAT IS THE QUESTION Gary Naglie, MD, FRCPC, FGSA Department of Medicine, Baycrest & University of Toronto Scientist, Rotman Research Institute, Baycrest & Toronto Rehabilitation
Driving and Dementia Practical Tips for the Family Physician
 Driving and Dementia Practical Tips for the Family Physician L. Lee, MClSc (FM), MD, CCFP(COE), FCFP 2017 Canadian Medical Association. Determining fitness to operate motor vehicles: CMA Driver s Guide,
Driving and Dementia Practical Tips for the Family Physician L. Lee, MClSc (FM), MD, CCFP(COE), FCFP 2017 Canadian Medical Association. Determining fitness to operate motor vehicles: CMA Driver s Guide,
Driving in Dementia. Tel Aviv University Spring 2016 Mark Rapoport, MD, FRCPC Associate Professor, Dep t of Psychiatry
 Driving in Dementia Tel Aviv University Spring 2016 Mark Rapoport, MD, FRCPC Associate Professor, Dep t of Psychiatry With appreciation Disclosures CIHR Alzheimer Society of Canada Brain Canada/Chagnon
Driving in Dementia Tel Aviv University Spring 2016 Mark Rapoport, MD, FRCPC Associate Professor, Dep t of Psychiatry With appreciation Disclosures CIHR Alzheimer Society of Canada Brain Canada/Chagnon
Objectives. The Problem. The Problem. The Problem. Assessing the Older Driver
 Assessing the Older Driver Objectives Practical office evaluation. Testing and reporting Dementia and driving Strategies for counseling On-line resources Amelia Gennari, MD Director of Ambulatory Care
Assessing the Older Driver Objectives Practical office evaluation. Testing and reporting Dementia and driving Strategies for counseling On-line resources Amelia Gennari, MD Director of Ambulatory Care
Driving and Dementia Case Study
 Driving and Dementia Case Study Review the following case study one section at a time, responding to the questions posed following the information provided. Expert opinion about how to respond to the case
Driving and Dementia Case Study Review the following case study one section at a time, responding to the questions posed following the information provided. Expert opinion about how to respond to the case
The Road Map. Collisions and aging Function, skill and driving Licensing and assessment The future
 Senior Licensing 7th International Conference on Urban Traffic Safety Edmonton, AB April, 2015 C.T. (Chip) Scialfa University of Calgary scialfa@ucalgary.ca The Road Map Collisions and aging Function,
Senior Licensing 7th International Conference on Urban Traffic Safety Edmonton, AB April, 2015 C.T. (Chip) Scialfa University of Calgary scialfa@ucalgary.ca The Road Map Collisions and aging Function,
The role of memory on patients with mild cognitive impairment. Sophia Vardaki, PhD National Technical University of Athens
 The role of memory on patients with mild cognitive impairment Sophia Vardaki, PhD National Technical University of Athens Athens, 26 June 2015 Objective-Presentation Structure Objective To explore the
The role of memory on patients with mild cognitive impairment Sophia Vardaki, PhD National Technical University of Athens Athens, 26 June 2015 Objective-Presentation Structure Objective To explore the
HEART INTERVENTIONS IN OLDER PATIENTS. FILTERING FOR FRAILTY.
 HEART INTERVENTIONS IN OLDER PATIENTS. FILTERING FOR FRAILTY. December 8, 2017 Allen R. Huang, MDCM, FRCPC, FACP 1 Faculty Disclosure Faculty: Allen Huang MDCM, FRCPC, FACP Associate Professor, University
HEART INTERVENTIONS IN OLDER PATIENTS. FILTERING FOR FRAILTY. December 8, 2017 Allen R. Huang, MDCM, FRCPC, FACP 1 Faculty Disclosure Faculty: Allen Huang MDCM, FRCPC, FACP Associate Professor, University
Michel Bédard, PhD Canada Research Chair in Aging and Health Director, Centre for Research on Safe Driving Scientific Director, St.
 Michel Bédard, PhD Canada Research Chair in Aging and Health Director, Centre for Research on Safe Driving Scientific Director, St. Joseph s Care Group CRSD mandate Our mandate is to contribute to the
Michel Bédard, PhD Canada Research Chair in Aging and Health Director, Centre for Research on Safe Driving Scientific Director, St. Joseph s Care Group CRSD mandate Our mandate is to contribute to the
Recognizing Dementia can be Tricky
 Dementia Abstract Recognizing Dementia can be Tricky Dementia is characterized by multiple cognitive impairments that cause significant functional decline. Based on this brief definition, the initial expectation
Dementia Abstract Recognizing Dementia can be Tricky Dementia is characterized by multiple cognitive impairments that cause significant functional decline. Based on this brief definition, the initial expectation
Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes
 Town Hall Forum Making a Plan: The Smart Approach to Alzheimer s Care Needs May 25, 2017 Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes Daniel D. Sewell,
Town Hall Forum Making a Plan: The Smart Approach to Alzheimer s Care Needs May 25, 2017 Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes Daniel D. Sewell,
DEMENTIA NEWSLETTER FOR PHYSICIANS
 Vol. 1, No. 3 DEMENTIA NEWSLETTER FOR PHYSICIANS A Publication of the Ontario Dementia Network Fall 2011 In This Issue... Dementia Interview Guide - Dr. W. B. Dalziel Editorial Committee Dr. Andrew R.
Vol. 1, No. 3 DEMENTIA NEWSLETTER FOR PHYSICIANS A Publication of the Ontario Dementia Network Fall 2011 In This Issue... Dementia Interview Guide - Dr. W. B. Dalziel Editorial Committee Dr. Andrew R.
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Objectives. My Patient: The story 10/6/2017
 Objectives Our Grey Matter Matters: A Case in Point Vivien Brown MDCM, CCFP,FCFP, NCMP Assistant Professor, University of Toronto Vice President, Medical Affairs, Medisys Healthy Group Past President,
Objectives Our Grey Matter Matters: A Case in Point Vivien Brown MDCM, CCFP,FCFP, NCMP Assistant Professor, University of Toronto Vice President, Medical Affairs, Medisys Healthy Group Past President,
Assessing Fitness to Drive. DriveSafe DriveAware. A valid cognitive fitness to drive screening test for medical practice? 8/10/2015.
 DriveSafe DriveAware A valid cognitive fitness to drive screening test for medical practice? Presented by Beth Cheal Faculty of Health Sciences, School of Occupational Therapy, USyd / Pearson The University
DriveSafe DriveAware A valid cognitive fitness to drive screening test for medical practice? Presented by Beth Cheal Faculty of Health Sciences, School of Occupational Therapy, USyd / Pearson The University
Cognitive Evaluation in Primary Care. Scott T. Larson, MD Clinical Assistant Professor University of Iowa
 Cognitive Evaluation in Primary Care Scott T. Larson, MD Clinical Assistant Professor University of Iowa scott-larson@uiowa.edu Objectives Understand the subtypes of dementia, and the DSM-5 categorization
Cognitive Evaluation in Primary Care Scott T. Larson, MD Clinical Assistant Professor University of Iowa scott-larson@uiowa.edu Objectives Understand the subtypes of dementia, and the DSM-5 categorization
Case Presentation. Cognition: changes with Normal Aging? Synonyms
 Case Presentation 78 yr old new patient presenting for new PCP after discharge from hospital stay Discharged 3 days ago Summary : admitted with new atrial fibrillation, with history of DM, CHF. In hospital,
Case Presentation 78 yr old new patient presenting for new PCP after discharge from hospital stay Discharged 3 days ago Summary : admitted with new atrial fibrillation, with history of DM, CHF. In hospital,
UNDERSTANDING CAPACITY & DECISION-MAKING VIDEO TRANSCRIPT
 I m Paul Bourque, President and CEO of the Investment Funds Institute of Canada. IFIC is preparing materials to assist advisors and firms in managing effective and productive relationships with their aging
I m Paul Bourque, President and CEO of the Investment Funds Institute of Canada. IFIC is preparing materials to assist advisors and firms in managing effective and productive relationships with their aging
Optimizing Functional Ability in Driving
 Optimizing Functional Ability in Driving Cherie P. Brunker, MD Chief of Geriatrics, Intermountain Healthcare Associate Professor, Division of Geriatrics, UU Medical Director, Mission at Hillside Rehabilitation
Optimizing Functional Ability in Driving Cherie P. Brunker, MD Chief of Geriatrics, Intermountain Healthcare Associate Professor, Division of Geriatrics, UU Medical Director, Mission at Hillside Rehabilitation
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Table 5.11 Stroke Rehabilitation Assessment Tools For Pre-Driving Screening Canadian Best Practice Recommendations for Stroke Care Update
 Table 5.11 Stroke Rehabilitation Assessment Tools For Pre-Driving Canadian Best Practice Recommendations for Stroke Care 2011- Update Last Updated: June 19, Assessment Tools for Pre-Driving Developed by
Table 5.11 Stroke Rehabilitation Assessment Tools For Pre-Driving Canadian Best Practice Recommendations for Stroke Care 2011- Update Last Updated: June 19, Assessment Tools for Pre-Driving Developed by
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Assessment Toolkits for Lewy Body Dementia
 Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
DEMENTIA NEWSLETTER for PHYSICIANS
 DEMENTIA NEWSLETTER for PHYSICIANS Vol. 6, No. 4 OTTAWA AND RENFREW COUNTY Winter 2008 In This Issue... Mild Cognitive Impairment Monitoring Patient Response to Cognitive Enhancers CDN Diagnostic Assessment
DEMENTIA NEWSLETTER for PHYSICIANS Vol. 6, No. 4 OTTAWA AND RENFREW COUNTY Winter 2008 In This Issue... Mild Cognitive Impairment Monitoring Patient Response to Cognitive Enhancers CDN Diagnostic Assessment
Identifying Medically At-Risk Drivers
 Identifying Medically At-Risk Drivers Brian R. Ott, MD Director, Alzheimer s Disease & Memory Disorders Center Rhode Island Hospital Professor of Neurology, Alpert Medical School of Brown University Providence,
Identifying Medically At-Risk Drivers Brian R. Ott, MD Director, Alzheimer s Disease & Memory Disorders Center Rhode Island Hospital Professor of Neurology, Alpert Medical School of Brown University Providence,
Cognitive Assessment 4/29/2015. Learning Objectives To be able to:
 Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Older Driver at Risk: What do I do?
 2018 TZD Annual Statewide Conference, Mankato, MN Older Driver at Risk: What do I do? Panelists: Catherine Sullivan (St. Catherine University). Alan Ainsworth (AARP), Jennifer Fischer (Courage Kenny),
2018 TZD Annual Statewide Conference, Mankato, MN Older Driver at Risk: What do I do? Panelists: Catherine Sullivan (St. Catherine University). Alan Ainsworth (AARP), Jennifer Fischer (Courage Kenny),
Physical and Medical Impairments in Elderly Drivers
 Physical and Medical Impairments in Elderly Drivers Kam Hunter, MD PhD AzGS Summer Interdisciplinary Conference August 3 rd, 2011 Physiology Pertinent Systems Affected by Aging Visual Decreased central
Physical and Medical Impairments in Elderly Drivers Kam Hunter, MD PhD AzGS Summer Interdisciplinary Conference August 3 rd, 2011 Physiology Pertinent Systems Affected by Aging Visual Decreased central
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Frequently Asked Questions About Dementia
 Frequently Asked Questions About Dementia Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified healthcare provider. Please consult
Frequently Asked Questions About Dementia Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified healthcare provider. Please consult
Early Recognition of Cognitive Impairment:
 Early Recognition of Cognitive Impairment: If you do not ask they will not tell Temple Family Practice Review Course Leon S. Kraybill, MD, CMD Geriatrics, Lancaster General Hospital Physicians Division
Early Recognition of Cognitive Impairment: If you do not ask they will not tell Temple Family Practice Review Course Leon S. Kraybill, MD, CMD Geriatrics, Lancaster General Hospital Physicians Division
Note: These are abbreviated slides with graphics and other protected content removed for electronic posting purposes with NAPSA.
 Note: These are abbreviated slides with graphics and other protected content removed for electronic posting purposes with NAPSA. Please attend the presentation for the full slideshow and information. Attendees
Note: These are abbreviated slides with graphics and other protected content removed for electronic posting purposes with NAPSA. Please attend the presentation for the full slideshow and information. Attendees
Cognitive Screening in Risk Assessment. Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University.
 Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
Assessing cognition in ELDERLY drivers
 Assessing cognition in ELDERLY s Alexandra Economou Assistant Professor Department of Psychology University of Athens 18 October 2013 Athens Overview ability in the older ability in the older The older
Assessing cognition in ELDERLY s Alexandra Economou Assistant Professor Department of Psychology University of Athens 18 October 2013 Athens Overview ability in the older ability in the older The older
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
DriveWise Driving Evaluation. Ann M. Hollis OTR/L
 DriveWise Driving Evaluation Ann M. Hollis OTR/L DriveWise Objective assessment of driving safety with support for patient/family Hospital based, Multidisciplinary team approach ClinicalEvaluation, Research
DriveWise Driving Evaluation Ann M. Hollis OTR/L DriveWise Objective assessment of driving safety with support for patient/family Hospital based, Multidisciplinary team approach ClinicalEvaluation, Research
Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes
 Town Hall Forum Making a Plan: The Smart Approach to Alzheimer s Care Needs May 25, 2017 Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes Daniel D. Sewell,
Town Hall Forum Making a Plan: The Smart Approach to Alzheimer s Care Needs May 25, 2017 Understanding the Progression of Alzheimer s and Related Dementias And Planning for Future Changes Daniel D. Sewell,
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Multifactorial risk assessments and evidence-based interventions to address falls in primary care. Objectives. Importance
 Multifactorial risk assessments and evidence-based interventions to address falls in primary care Sarah Ross, DO, MS Assistant Professor Internal Medicine, Geriatrics Nicoleta Bugnariu, PT, PhD Associate
Multifactorial risk assessments and evidence-based interventions to address falls in primary care Sarah Ross, DO, MS Assistant Professor Internal Medicine, Geriatrics Nicoleta Bugnariu, PT, PhD Associate
Appendix 2 (continued): Recommendations for the management of mild to moderate dementia, dementia with a cerebrovascular component, and for addressing
: Recommendations for the management of mild to moderate dementia, dementia with a cerebrovascular component, and for addressing") a cerebrovascular component, and for addressing ethical issues in dementia (page 1 of 7) Mild to moderate dementia 1. Most patients with dementia can be assessed and managed adequately by their primary
a cerebrovascular component, and for addressing ethical issues in dementia (page 1 of 7) Mild to moderate dementia 1. Most patients with dementia can be assessed and managed adequately by their primary
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
OBJECTIVES. 1. Become familiar with common classes of psychotropic medications, indications for their use, and side effects.
 OBJECTIVES 1. Become familiar with common classes of psychotropic medications, indications for their use, and side effects. 2. Use familiar conditions, as drawn from current caseloads, to evaluate the
OBJECTIVES 1. Become familiar with common classes of psychotropic medications, indications for their use, and side effects. 2. Use familiar conditions, as drawn from current caseloads, to evaluate the
Transportation and Healthy Aging: Issues and Ideas for an Aging Society
 COUNCIL ON HEALTHY AGING Agenda Transportation and Healthy Aging: Issues and Ideas for an Aging Society April 30 and May 1, 2015 Toronto, Ontario The Old Mill Hotel http://www.oldmilltoronto.com/ Transportation
COUNCIL ON HEALTHY AGING Agenda Transportation and Healthy Aging: Issues and Ideas for an Aging Society April 30 and May 1, 2015 Toronto, Ontario The Old Mill Hotel http://www.oldmilltoronto.com/ Transportation
The Medically At-Risk Driver Cognitive Impairment Leads the Way
 The Medically At-Risk Driver Cognitive Impairment Leads the Way Bonnie M. Dobbs, PhD* and Allen R. Dobbs, PhD * University of Alberta, Edmonton, Canada DriveABLE Assessment Centres Inc. Paper presented
The Medically At-Risk Driver Cognitive Impairment Leads the Way Bonnie M. Dobbs, PhD* and Allen R. Dobbs, PhD * University of Alberta, Edmonton, Canada DriveABLE Assessment Centres Inc. Paper presented
Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives, friends
 ASSESSING COMPETENCE Michael A Hill MD UNC Psychiatry 2008 Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives,
ASSESSING COMPETENCE Michael A Hill MD UNC Psychiatry 2008 Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives,
Introduction to Dementia: Diagnosis & Evaluation. Created in March 2005 Duration: about 15 minutes
 Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Managing Behavioral Issues
 2:45 3:45pm Caring for the Older Patient Handling Behavioral Issues Presenter Disclosure Information The following relationships exist related to this presentation: Samir Sabbag, MD, has no financial relationships
2:45 3:45pm Caring for the Older Patient Handling Behavioral Issues Presenter Disclosure Information The following relationships exist related to this presentation: Samir Sabbag, MD, has no financial relationships
For primary care clinicians, one of the most challenging aspects
 Driving and dementia Efficient approach to driving safety concerns in family practice Clinical Review Linda Lee MD MClSc(FM) CCFP (COE) FCFP Frank Molnar MSc MD CM FRCPC Abstract Objective To provide primary
Driving and dementia Efficient approach to driving safety concerns in family practice Clinical Review Linda Lee MD MClSc(FM) CCFP (COE) FCFP Frank Molnar MSc MD CM FRCPC Abstract Objective To provide primary
Lori Grismore, OTR/L, Occupational Therapist USF Health Byrd Alzheimer s Center and Research Institute
 Lori Grismore, OTR/L, Occupational Therapist USF Health Byrd Alzheimer s Center and Research Institute To identify the diagnoses and clinical symptoms that may warrant a referral for a driving evaluation.
Lori Grismore, OTR/L, Occupational Therapist USF Health Byrd Alzheimer s Center and Research Institute To identify the diagnoses and clinical symptoms that may warrant a referral for a driving evaluation.
MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS
 MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS There are a wide variety of Neurologic and Musculoskeletal disorders which can impact driving safety. Impairment may be the result of altered muscular, skeletal,
MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS There are a wide variety of Neurologic and Musculoskeletal disorders which can impact driving safety. Impairment may be the result of altered muscular, skeletal,
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Key Points For Physicians To Review With Adolescents and Adults Who Have ADHD
 SUPPORTING DOCUMENT 6C ADHD AND DRIVING Key Points For Physicians To Review With Adolescents and Adults Who Have ADHD Risk Data: a) Clinical studies indicate that young drivers with untreated or sub-optimally
SUPPORTING DOCUMENT 6C ADHD AND DRIVING Key Points For Physicians To Review With Adolescents and Adults Who Have ADHD Risk Data: a) Clinical studies indicate that young drivers with untreated or sub-optimally
Senior Drivers: The Clinician s Role in Maintaining Independence and Assessing Capabilities for Driving Safely.
 Senior Drivers: The Clinician s Role in Maintaining Independence and Assessing Capabilities for Driving Safely. Daniel K. Onion, MD, MPH Prof of Community and Family Medicine Geisel School of Medicine
Senior Drivers: The Clinician s Role in Maintaining Independence and Assessing Capabilities for Driving Safely. Daniel K. Onion, MD, MPH Prof of Community and Family Medicine Geisel School of Medicine
Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital. November /20/ Safety: Falls/Cooking/Unsafe Behaviour. 2.
 How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
Dementia and Primary Care. A Structured Team Approach UNE/MGEC Conference June 2014
 Dementia and Primary Care A Structured Team Approach UNE/MGEC Conference June 2014 First Proviso I have no actual or potential conflict of interest in relation to this program or presentation. Second Proviso
Dementia and Primary Care A Structured Team Approach UNE/MGEC Conference June 2014 First Proviso I have no actual or potential conflict of interest in relation to this program or presentation. Second Proviso
8/26/2013 DMV UCSD CHP. Presenters. Law Enforcement s Identification and Referral of Medically Impaired Older Drivers. NHTSA Priority.
 Presenters Law Enforcement s Identification and Referral of Medically Impaired Older Drivers Linda Hill, MD, MPH Department of Family and Preventive Medicine University of California, San Diego D. R. Ike
Presenters Law Enforcement s Identification and Referral of Medically Impaired Older Drivers Linda Hill, MD, MPH Department of Family and Preventive Medicine University of California, San Diego D. R. Ike
CHRONIC PAIN & OPIOID PRESCRIBING GUIDELINES
 CHRONIC PAIN & OPIOID PRESCRIBING GUIDELINES The following guidelines have been reviewed and endorsed by the New Brunswick Medical Society July 2004 Chronic pain can be due to cancer or noncancer conditions.
CHRONIC PAIN & OPIOID PRESCRIBING GUIDELINES The following guidelines have been reviewed and endorsed by the New Brunswick Medical Society July 2004 Chronic pain can be due to cancer or noncancer conditions.
David A Scott Lis Evered. Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne
 David A Scott Lis Evered Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne This talk will include live polling so please be sure to have the meeting
David A Scott Lis Evered Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne This talk will include live polling so please be sure to have the meeting
13/09/2018. Syncope & Driving. Risk Syncope during Driving. Risk of Recurrence Syncope
 Risk Syncope during Driving & Motor Vehicle Crash (MVC) Syncope & Driving Declan Whelan FRCPI; FFOM RCPI. March 2018 Danish Cohort Study: JAMA Intern. Med. 2016: 176(4):503-510. 41,039patients with 1 st
Risk Syncope during Driving & Motor Vehicle Crash (MVC) Syncope & Driving Declan Whelan FRCPI; FFOM RCPI. March 2018 Danish Cohort Study: JAMA Intern. Med. 2016: 176(4):503-510. 41,039patients with 1 st
Managing Behaviors: Start with Yourself!
 Slide 1 Managing Behaviors: Start with Yourself! Teepa Snow, Positive Approach, LLC to be reused only with permission. Slide 2 Time Out Signal copyright - Positive Approach, LLC 2012 Slide 3 REALIZE It
Slide 1 Managing Behaviors: Start with Yourself! Teepa Snow, Positive Approach, LLC to be reused only with permission. Slide 2 Time Out Signal copyright - Positive Approach, LLC 2012 Slide 3 REALIZE It
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Practical Functional Assessment of Elderly Persons: A Primary- Care Approach
 Practical Functional Assessment of Elderly Persons: A Primary- Care Approach The following is abstracted from: Fleming KC, Evans JM, Weber DC and Chutka DS. Practical Functional Assessment of Elderly Persons:
Practical Functional Assessment of Elderly Persons: A Primary- Care Approach The following is abstracted from: Fleming KC, Evans JM, Weber DC and Chutka DS. Practical Functional Assessment of Elderly Persons:
Supporting Persons with Dementia Face the Decision and Effects of Hanging up the Keys
 TEAM TITLE List Team Members Supporting Persons with Dementia Face the Decision and Effects of Hanging up the Keys CCNA Team 16: Driving and Dementia Team Leaders: G. Naglie & M. Rapoport www.ccna-ccnv.ca
TEAM TITLE List Team Members Supporting Persons with Dementia Face the Decision and Effects of Hanging up the Keys CCNA Team 16: Driving and Dementia Team Leaders: G. Naglie & M. Rapoport www.ccna-ccnv.ca
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE
 CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
Paying for Dementia Care. Mary Ann Forciea MD Clinical Professor of Medicine Division of Geriatric Medicine University of Pennsylvania Health System
 Paying for Dementia Care Mary Ann Forciea MD Clinical Professor of Medicine Division of Geriatric Medicine University of Pennsylvania Health System Audience: Possible concerns about dementia care in my
Paying for Dementia Care Mary Ann Forciea MD Clinical Professor of Medicine Division of Geriatric Medicine University of Pennsylvania Health System Audience: Possible concerns about dementia care in my
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Parkinson s Disease and Driving
 Parkinson s Disease and Driving Virginia Mason Mary Muszynski Occupational Therapist Arin Sumerwell Occupational Therapist 2 Driving and Parkinson s From Parkinson s Foundation website: The ability to
Parkinson s Disease and Driving Virginia Mason Mary Muszynski Occupational Therapist Arin Sumerwell Occupational Therapist 2 Driving and Parkinson s From Parkinson s Foundation website: The ability to
ADRC Dementia Care Training. Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium
 ADRC Dementia Care Training Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium 1 Federal definition: Ages 18 and older Serious Mental Illness
ADRC Dementia Care Training Module 10: Supporting People with Serious Mental Illness and Dementia: Bipolar Disorders, Dementia, and Delirium 1 Federal definition: Ages 18 and older Serious Mental Illness
Toolkit for Detection of Dementia. And. Safe DR(ive)
") Toolkit for Detection of Dementia And Safe DR(ive) Sudbury, Ontario October, 2007 Dr. J.K. Le Clair Tools to Promote Common Language and Approach Physical: 5D s 1. Delirium 2. Disease 3. Drugs 4. Discomfort
Toolkit for Detection of Dementia And Safe DR(ive) Sudbury, Ontario October, 2007 Dr. J.K. Le Clair Tools to Promote Common Language and Approach Physical: 5D s 1. Delirium 2. Disease 3. Drugs 4. Discomfort
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
Memory & Aging Clinic Questionnaire
 Memory & Aging Clinic Questionnaire The answers you give to the questions below will assist us with our evaluation. Each section is equally important so please be sure to complete the entire questionnaire.
Memory & Aging Clinic Questionnaire The answers you give to the questions below will assist us with our evaluation. Each section is equally important so please be sure to complete the entire questionnaire.
Behavioral Aspects of Parkinson s Disease
 Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Onanong Jitkritsadakul 1 and Roongroj Bhidayasiri 1,2*
 Jitkritsadakul and Bhidayasiri Journal of Clinical Movement Disorders (2016) 3:14 DOI 10.1186/s40734-016-0043-x REVIEW Open Access Physicians role in the determination of fitness to drive in patients with
Jitkritsadakul and Bhidayasiri Journal of Clinical Movement Disorders (2016) 3:14 DOI 10.1186/s40734-016-0043-x REVIEW Open Access Physicians role in the determination of fitness to drive in patients with
Research ALZHEIMER S DISEASE AND RISK FACTORS
 Research ALZHEIMER S DISEASE AND RISK FACTORS What is Alzheimer s disease? Alzheimer s disease is the most common of a large group of disorders known as dementias. It is an irreversible disease of the
Research ALZHEIMER S DISEASE AND RISK FACTORS What is Alzheimer s disease? Alzheimer s disease is the most common of a large group of disorders known as dementias. It is an irreversible disease of the
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Vocally Disruptive Behaviours
 Vol. 8, No. 1 Fall 2009 A Publication of the Champlain Dementia Network In This Issue... Vocally Disruptive Behaviours Office Assessment of Dementia: A Guide to Scheduling and Billing for Family Physicians
Vol. 8, No. 1 Fall 2009 A Publication of the Champlain Dementia Network In This Issue... Vocally Disruptive Behaviours Office Assessment of Dementia: A Guide to Scheduling and Billing for Family Physicians
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Active Learning Strategies for Mastering Geriatric Assessment Tools
 Active Learning Strategies for Mastering Geriatric Assessment Tools Sara McCumber, MS, RN, CNP, CNS Family Nurse Practitioner & Adult-Gerontological Primary Care NP The College of St. Scholastica Nursing
Active Learning Strategies for Mastering Geriatric Assessment Tools Sara McCumber, MS, RN, CNP, CNS Family Nurse Practitioner & Adult-Gerontological Primary Care NP The College of St. Scholastica Nursing
Providing Driving Recomendations to Older Adults and Patients with Dementia
 Providing Driving Recomendations to Older Adults and Patients with Dementia Mark A. Reger, Ph.D. Department of Psychology, Madigan Army Medical Center Department of Psychiatry and Behavioral Sciences,
Providing Driving Recomendations to Older Adults and Patients with Dementia Mark A. Reger, Ph.D. Department of Psychology, Madigan Army Medical Center Department of Psychiatry and Behavioral Sciences,
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Dementia the A,B,Cs. Dr. Frank Molnar. Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital
 Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Evaluations. Alzheimer s Disease A Public Health Response. Viewer Call-In. July 19, Guest Speakers. Thanks to our Sponsors:
 Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received