WE CAN DO BETTER: Helping People with Dementia and Their Families Live at Home with Quality of Life
|
|
|
- Sandra Kelly
- 6 years ago
- Views:
Transcription

1 WE CAN DO BETTER: Helping People with Dementia and Their Families Live at Home with Quality of Life Laura N. Gitlin, Ph.D. Professor, School of Nursing, School of Medicine Director, Center for Innovative Care in Aging Johns Hopkins University Prepared for University of Sydney March 23, 2015
2 Overview What are unmet needs of people with dementia and family caregivers living at home? How can we address these needs? Promising interventions Project COPE Tailored Activity Program Where do we go from here?
3 Funding Sources and Attributions Research funded by: NIA NIMH NINR Alzheimer s Association PA Dept. of Health, Tobacco Funds Administration on Aging No disclosures/no sources of conflict Thanks to my many collaborators and teams working with me in developing, testing and implementing behavioral interventions
 and received some helpful information from national and local chapters. Mr. Smith stopped working to care for his wife.")
4 Case Snapshot Mr. Smith cares for his wife at home. She was diagnosed with dementia 4 years ago. He learned of the Alzheimer s Association from a neighbor (by chance) and received some helpful information from national and local chapters. Mr. Smith stopped working to care for his wife. He is becoming increasingly isolated and depressed. He is having difficulty managing Mrs. Smith s increasing physical dependence and behavioral symptoms including her pacing, repetitive questioning, trying to leave home, misplacing keys, rejecting his help. He is not sure how to engage her and is concerned about her quality of life. Mr. Smith does not receive any in-home help, and Mrs. Smith s physician has put her on anticholinesterase medications that do not appear to be effective. HOW CAN WE HELP MR. AND MRS SMITH? WHAT INTERVENTIONS/TREATMENTS ARE EFFECTIVE?
5 Six Primary Goals of Dementia Care Improve and maintain quality of life Prevent, reduce/minimize, address behavioral symptoms Maintain function and engagement in activities Attend to medical management of comorbidities Support families Care coordination Callahan et al., Health Affairs, 2014; Sink, et al JAMA. 2005; Avalon et al., Arch Intern Med. 2006; Hinton et al., J. Gen Intern Med, 2007; Lingler et al., J Am Geriatr Soc
6 Unmet Needs of Persons with Dementia Living at Home (N=303) Black et al., JAGS 2013 Eval/Diagnosis Treat cognitive sx Treat neuropsych sx Behavior management Medication management Medication administration General Medical/Health care Allied Health care Safety ADL Assistance Meaningful Activities Legal Issues/ Care Planning Health Insurance Patient Education Caregiver Availability 14% 16% 21% 19% 23% 18% 25% 9% 21% 3% 35% 47% 51% 63% 90% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
7 Caregivers unmet needs (%) Caregiver education 84 Resource referral 88 Caregiver mental health 45 Caregiver medical health 24 Other

8 NPS fluctuate after Dementia Onset N=328 Cache County Study Number and severity of NPS increased over time but course was variable and episodic. Rate of change in NPS was correlated weakly, if at all, with rate of change in cognition or function. Tschanz et al, Am J Geriatr Psychiatry, 2012
9 NPS accelerate onset of severe dementia including mild NPS Rabins et al, 2013, Alzheimer s and Dementia

10 Etiologies of Behavioral Symptoms and Functional Decline Behavioral Symptoms Functional disability

11 Project COPE Care of Persons with Dementia in their Environments Gitlin et al, 2010 JAMA
12 Clinical Trajectory COPE Dyadic Focus Normal Pre- Clinical Mild Cognitive Impairment Early State Dementia Moderate Stage Dementia Severe Stage Dementia TREATMENT GOALS Treatment and Symptom Management Reduction of excess disability Prevention and management of behaviors Caregiver support and education McKhann et al., 2011, Albert et al., 2011, Sperling et al, 2011 and Jack et al., May 2011 Alzheimer's & Dementia: The Journal of the Alzheimer's Association
13 PROJECT COPE Study Desig8n (N=208) 2 weeks 72 hours Recruitment Screening Baseline Assessment (N = 272) Treatment Randomization gender/relationship 2 weeks Attention Control 4 Months Post Baseline 9 Months Post Baseline Follow-up Assessment 1 Follow-up Assessment 2 Follow-up Assessment 1 Follow-up Assessment 2
14 Profile of COPE Participants (N=239) Persons with dementia Mean = 82.4 (8.9) Female = 68.4% 27.3% African American Mean MMSE = 13.4 Medications: 95 (40.1%) on anti-depressants 77 (32.5%) on medications for behaviors 108 (45.6%) on pain medications 173 (73.3%) on memory enhancers Average # of behaviors = 6.0 High functional dependence Caregiver Mean age =62.2 Female = 89% Non-spouse = 62.2%

15 Nurse Visit to Discuss Medical Issues Provide caregiver education about: Pain Dehydration Infection Constipation Polypharmacy Discuss taking Care of self


16 Examine Individual with Dementia Nurse tests sample with Chemstrip 10 test strip: Positive outcomes cultured at lab Nurse screens for blood abnormalities Hgb, Hct., wbc, rbc, electrolytes, glucose, TSH and T4 Physical exam Laboratory results shared with caregiver
 Identification of targeted problem areas Problem solving and brainstorming strategies Implement and evaluate strategy effectiveness Knowledge")
17 Occupational Therapist Visits: Assessment Phase (session 1-3) PwD capabilities, deficits, physical function executive function CG readiness, knowledge, care challenges, risk areas Home safety and supportive features Implementation Phase (session 4-8) Identification of targeted problem areas Problem solving and brainstorming strategies Implement and evaluate strategy effectiveness Knowledge building and strategies: Communicating effectively Simplifying environment Using activities Managing their own stress and taking care of self Generalizabiltiy Phase (session 9-10) Preparing for the future Using strategies for other care challenges

18 Key Communication Strategies for Families Use 1 or 2 step simple verbal commands or demonstration Speak slowly Use brief, simple statements Eliminate questions/ comments that are abstract (vs. questions) Offer no more than 2 choices Use cueing (touch or verbal)

; provide reassurance, redirect; they may not")
19 Redirection, Go with Flow, Reassurance Behavior: My wife sometimes insists on going home when sitting in our living room. Strategy: Go along with your family member s beliefs (avoid confrontation and do not rationalize); provide reassurance, redirect; they may not recognize they are home; take a short walk


20 Verbal Cues Behavior: My husband keeps asking me the what day it is and what we will read in bible study. Strategy: Provide 1- step verbal cue to check the calendar

21 Use Written Visual Cues Behavior: My sister doesn t seem to know what to do in the morning. Strategy: Provide visual prompts - reminder notes
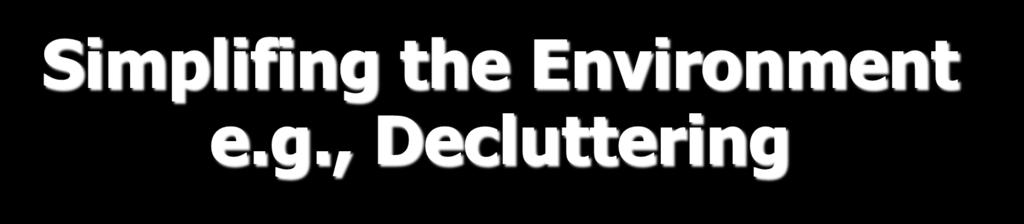
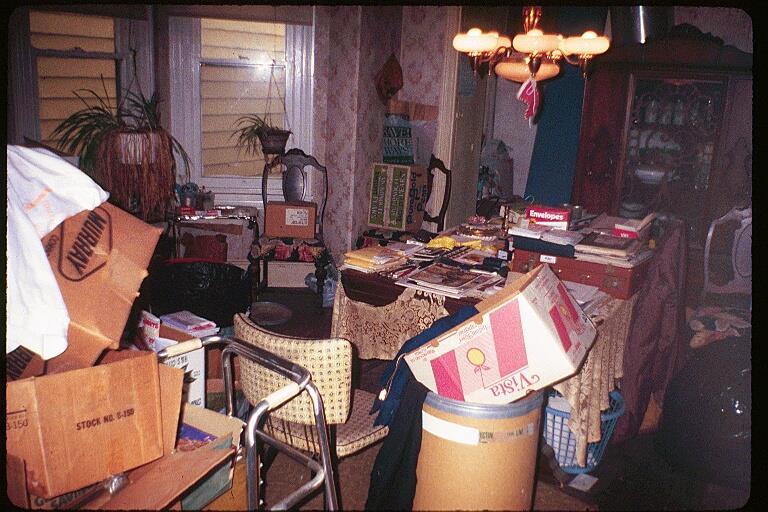

22 Simplifing the Environment e.g., Decluttering


23 Nothing to Do

24

25 Introduce Familiar Activity Behavior: Because my wife can t do anything right, I do it myself. Strategy: Lower expectations and demands; relax the rules Introduce activities that tap into previous roles
26 KEY FINDINGS
27 Prevalence of Undiagnosed Medical Undiagnosed illnesses in 40 (37.4%) patients: 3 patients (2.8%) >2 coexisting, undiagnosed medical illnesses 15% Bacteriuria 9% Anemia 5% Hyperglycemia Of 40 patients, 39 (97.5%) followed-up with physicians, 1 refused. Of 39, 1 patient was hospitalized with others treated as outpatients.
28 Comparison of COPE (n=102) and Control (n=107) Group Patients 4-months Baseline 4-Month Follow-up Control COPE Control COPE Patient Outcomes M (SD) M (SD) M (SD) M (SD) Difference of Adjusted Means 95% CI p d Overall functional dependence 2.8 (1.3) 3.0 (1.2) 3.3 (1.3) 3.7 (1.3).24.03, IADL dependence 1.8 (1.0) 1.8 (1.0) 2.5 (1.1) 2.8 (1.2).32.09, Activity engagement 2.0 (0.4) 1.9 (0.4) 1.9 (0.5) 2.0 (0.4).12.07, Quality of life 2.1 (0.5) 2.1 (0.4) 2.1 (0.5) 2.2 (0.5) ,
29 Percent Eliminating Targeted Care Challenge 70.00% 60.00% 62.7% p= % 44.9% 40.00% 30.00% COPE Control 20.00% 10.00% 0.00% Percent Eliminating Care Challenges
30 Perceived Change Scale Perceived change overall p= Control Intervention T1 Time T2
31 Confidence Scale Caregiver confidence p= Control Intervention Time
32 Percent 80 Perceived Patient Benefits at 9 Months 70 COPE Control p = p < Improved patient's life Helped you keep patient at home Response = "A great deal"

33 Tailored Activity Program Funded by NIMH #R21 MH069425;NIA Gitlin et al., 2008, 2010, American Journal of Geriatric Psychiatry; Gitlin, et al., 2010 The Gerontologist; Jutkowitz, et al., 2010 Value in Health
34 Clinical Trajectory Tailored Activity Program Normal Pre- Clinical Mild Cognitive Impairment Early State Dementia Moderate Stage Dementia Severe Stage Dementia TREATMENT GOALS Enhanced engagement Prevention and management of behaviors Caregiver support and education Reduction of objective burden (less time in care)




35 Tailored Activity Program Phase III Translation VA- TAP England TAP Australia TAP Baltimore TAP TAP-Hospital (Hopkins, Baltimore) Kentucky TAP AoA Scotland OT Home Project MIND Plus CMMI Brazil TAP Home Adult Day John Hopkins Memory Clinic and Pace Program
36 TAP STUDY DESIGN Recruitment Screening Baseline Assessment (T1) Randomization N = 60 MMSE <24 CG reports boredom, agitation, behavioral problem CG providing care > 4 hrs daily Willing to learn activities Treatment Intervention Control 4 Months Post Baseline (T2) Follow-up Assessment Follow-up Assessment Intervention 8 moths Post Baseline (T3) Follow-up
37 Intervention Characteristics 8 home/telephone sessions over 4-months by occupational therapists Phase I - Assessment: Capabilities of dementia patient using neuropsychological and structured standardized observation tools (Allen Battery) Previous roles, habits and interests Caregiver management style Physical environment Phase II Implementation Develop and introduce customized activities (Activity Prescription) Train caregivers to: Set up activity; simplify environment Communicate effectively (cueing, initiation, sequencing) Phase III Generalizability Integration of activities in daily care Use of strategies for other care challenges
38 Activity Selection Person with Dementia Environment Caregiver Interests and prior Social Roles Clinical Assessment: Cognitive funciton: Allen -Executive function Physical TUG ADL/IADL Sensory Comportment Safety Accessibility Noise Other People Readiness Stress Communication Routines Care goals Activity Prescriptions
39 Activity selection Mr. L Hollers, boredom, asking same? over and over Baseball Deacon Puppies Clinical Assessment: Allen: 3.4 MMSE: 6 TUG: 2 min 31 sec ADL/IADL: moderately to completely dependent Home Environment Busy Household Lots of people Lots of noise Great-great-grandson also has medical issues 3 Activity Prescriptions: Game of Catch Listen to Gospel Music Watch DVD of Puppies Daughter Readiness: Preparation Demanding job Cares for multiple people Communication: positive/negative

40 Play Ball

41
42 Mutual Help: activity selection Ms. H Behaviors: restless, sundowning, asking? over and over Pastor Mother of 9 Helping Clinical Assessment: Allen: 3.2 MMSE: 2 TUG: 30 sec ADL/IADL: minimal to moderate dependence Home Environment Safe Not Cluttered Quiet Daughter Readiness: Action, already trying activities Willing to listen Willing to commit time and energy Want QoL for mom 3 Activity Prescriptions: Folding Laundry Unload Dishwasher Listen to Gospel Music

43 Mutual Help: Folding the Laundry

44 Lessons Learned Initially B wanted Mom to learn new things Gear activity to where Mom is today B was raised to do household tasks properly There is no right or wrong It is stressful Stress reduction techniques used daily
45


46

47
48 TAILORED ACTIVITY PROGRAM HOSPITAL SETTINGS



49 Activity Station: Clerical Activity Station: Workbench Activity Station: Kitchen & Laundry
50 Mr. K 83 years of age Admitted to gero-psychiatric unit in acute care hospital for agitation, anxiety, and apathy Lives at home with wife (primary caregiver) Mini-mental status examination = 16 (moderate stage dementia) Previous employment chemist

51 Mr. K s Cognitive Functioning (Manual Action Level) Can handle objects, repetitive actions Eye-hand coordination Understands concrete meaning of objects Repetitive actions may not notice effect of action on object Can distinguish size, shape and color Lines objects in a row Uses short phrases
52 Mr. K
53 Mr. T
54 Mr. F 70 years of age Admitted for agitation, aggression, anxiety, delusions, hallucinations Lives at home with wife (primary caregiver) Mini-mental status examination = 15 (moderate stage dementia) Previous employment FBI agent Interests barbershop music, being outside, socializing, golf (in past) Comportment 16 (low orientation to others and socialability)
55 Mr. F s cognitive functioning ACLS 5 = 3.0 (Manual Action Level) Not able to preform self-care activities Understands concrete meaning of objects Repetitive actions may not notice effect of action on object Can distinguish size, shape and color Activities Listen and sing with barbershop music Indoor golf Dancing to music Watching golf DVD
56 Mr. F
57 Key Outcomes for Home-based Program
58 Individuals with Dementia (N=60) Mean age = % male 77% White; 23% African American 54% < H.S. education Mean MMSE = 11.6 (range ) Medications: 78.3% on cholinesterase inhibitor or memantine 32% taking psychotropic medication for behavioral symptoms 45% on antidepressants Average of 7.6 behavioral symptoms
 77% White 27.")
59 Caregiver Sample (N = 60) Mean age = 65.4 Most females (11.7% males) 77% White 27.2% <High school education Most spouses (62%)
60 4 Month Patient Outcomes (N=60) Outcomes Decline in frequency of behavioral symptoms Adjusted Mean p value Cohen s d Shadowing Repetitive question Enhanced activity engagement Enhanced pleasure
 80% 70% P=.")
61 % Reporting Improvement and Worsening of Behavioral Symptoms (4 months-baseline) 80% 70% P= % 50% 40% 30% TAP Control 20% 10% 0% Improvement Worsening

62 % Reporting Patient Agitation (N=60) Baseline 4 months TAP Control Grp P=.014; Cohen s d=.75
63 Cognitive Status and 4-month Outcomes No difference in outcomes for patients with MMSE < 10 and MMSE>10 on frequency of behavioral symptoms E.g., patients with hi or low cognitive status had reduced frequency of occurrence of behavioral symptoms compared to controls Patients with MMSE>10 in TAP also had fewer number of behavioral symptoms than patients with MMSE < 10 compared to controls
64 Mean Number of Hours Mean Number of Hours 9 Hours Caregiver Doing Things for Dementia Patient 19 Hours on Duty Control Experimental p = p =.001 Control Experimental 4 Baseline Assessment Timepoint Four Months 10 Baseline Assessment Timepoint Four Months
65 Mean Level of Mastery Mastery Control Experimental p = Baseline Assessment Timepoint Four Months
66 Mean Level of Confidence Confidence Using Activities p =.011 Control Experimental 5 Baseline Assessment Timepoint Four Months
67 Challenges Mechanisms of action How does engagement effect behavior/function/cognition Dose-response Replication, translation, implementation Who can implement these interventions? Who will pay for these interventions? Translation of knowledge into clinical tools Web-based programs for behavioral management Training of health and human service professionals

68 Translation into Practice Clinical Tools WeCare Advisor Tool for Families and health professionals to learn how to select and use non-pharmacologic strategies to address behavioral symptoms
69



70 Guide-Dementia-Activities- Strategies/dp/
WE CAN DO BETTER: Helping People with Dementia and Their Families Live at Home with Quality of Life
 WE CAN DO BETTER: Helping People with Dementia and Their Families Live at Home with Quality of Life Laura N. Gitlin, Ph.D. Professor, School of Nursing, School of Medicine Director, Center for Innovative
WE CAN DO BETTER: Helping People with Dementia and Their Families Live at Home with Quality of Life Laura N. Gitlin, Ph.D. Professor, School of Nursing, School of Medicine Director, Center for Innovative
Therapeutic Benefits of Caregiver Interventions
 Therapeutic Benefits of Caregiver Interventions Laura N. Gitlin, Ph.D. Professor, Department Community Public Health, School of Nursing Director, Center for Innovative Care in Aging Johns Hopkins University
Therapeutic Benefits of Caregiver Interventions Laura N. Gitlin, Ph.D. Professor, Department Community Public Health, School of Nursing Director, Center for Innovative Care in Aging Johns Hopkins University
Scottish Pilot of the Tailored Activity Programme Progress to date. Jenny Reid AHP Dementia Consultant NHS
 Scottish Pilot of the Tailored Activity Programme Progress to date Jenny Reid AHP Dementia Consultant NHS Lothian @JennyAHPDem Overview of seminar Setting the scene What is TAP? The National TAP pilot
Scottish Pilot of the Tailored Activity Programme Progress to date Jenny Reid AHP Dementia Consultant NHS Lothian @JennyAHPDem Overview of seminar Setting the scene What is TAP? The National TAP pilot
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION Does the Tailored Activity Program (TAP) for dementia patients reduce caregiver burden and neuropsychiatric behavior compared to a wait-list control group
CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION Does the Tailored Activity Program (TAP) for dementia patients reduce caregiver burden and neuropsychiatric behavior compared to a wait-list control group
Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego
 Dementia Skills for In-Home Care Providers Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego Objectives Familiarity with the most common
Dementia Skills for In-Home Care Providers Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego Objectives Familiarity with the most common
Support for Family Caregivers in the Context of Dementia: Promising Programs & Implications for State Medicaid Policy
 Support for Family Caregivers in the Context of Dementia: Promising Programs & Implications for State Medicaid Policy Richard H. Fortinsky, PhD Professor and Health Net Inc., Endowed Chair of Geriatrics
Support for Family Caregivers in the Context of Dementia: Promising Programs & Implications for State Medicaid Policy Richard H. Fortinsky, PhD Professor and Health Net Inc., Endowed Chair of Geriatrics
Dementia A syndrome, not a disease. Mordechai Lavi, MD Geriatric Physician
 Dementia A syndrome, not a disease Mordechai Lavi, MD Geriatric Physician Objectives 1. To improve our understanding of how we diagnose a dementia syndrome 2. Understand the workup that should be expected
Dementia A syndrome, not a disease Mordechai Lavi, MD Geriatric Physician Objectives 1. To improve our understanding of how we diagnose a dementia syndrome 2. Understand the workup that should be expected
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Session outline. Introduction to dementia Assessment of dementia Management of dementia Follow-up Review
 Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
Creating Better Lives for People with Dementia
 Creating Better Lives for People with Dementia PRESENTED BY: Kim Warchol, OTR/L Founder and President of Dementia Care Specialists LeadingAge/LALA Conference Objectives 1. Identify prevalence and characteristics
Creating Better Lives for People with Dementia PRESENTED BY: Kim Warchol, OTR/L Founder and President of Dementia Care Specialists LeadingAge/LALA Conference Objectives 1. Identify prevalence and characteristics
How Aging and Dementia Effect Resident Behaviors
 How Aging and Dementia Effect Resident Behaviors November 3, 2011 1:00 2:00 PM EST Webinar Presented by: Alfred W. Norwood, BS, MBA Education Arm of the Carmelite Sisters for the Aged and Infirm Webinar
How Aging and Dementia Effect Resident Behaviors November 3, 2011 1:00 2:00 PM EST Webinar Presented by: Alfred W. Norwood, BS, MBA Education Arm of the Carmelite Sisters for the Aged and Infirm Webinar
Staying Active with Dementia
 Moving for Health Lesson Series Facilitator s Guide Staying Active with Dementia Objective This lesson will provide information for caregivers of persons with dementia about the importance of activity
Moving for Health Lesson Series Facilitator s Guide Staying Active with Dementia Objective This lesson will provide information for caregivers of persons with dementia about the importance of activity
10/17/2017. Causes of Dementia Alzheimer's Disease Vascular Dementia Diffuse Lewy Body Disease Alcoholic Dementia Fronto-Temporal Dementia Others
 1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
Mental Health Issues in Nursing Homes. I m glad you asked.
 Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Neuropsychiatric Syndromes
 Neuropsychiatric Syndromes Susan Czapiewski,MD VAHCS December 10, 2015 Dr. Czapiewski has indicated no potential conflict of interest to this presentation. She does intend to discuss the off-label use
Neuropsychiatric Syndromes Susan Czapiewski,MD VAHCS December 10, 2015 Dr. Czapiewski has indicated no potential conflict of interest to this presentation. She does intend to discuss the off-label use
Managing Behavioral Issues
 2:45 3:45pm Caring for the Older Patient Handling Behavioral Issues Presenter Disclosure Information The following relationships exist related to this presentation: Samir Sabbag, MD, has no financial relationships
2:45 3:45pm Caring for the Older Patient Handling Behavioral Issues Presenter Disclosure Information The following relationships exist related to this presentation: Samir Sabbag, MD, has no financial relationships
WICKING DEMENTIA RESEARCH & EDUCATION CENTRE. Prof. Fran McInerney RN, BAppSci, MA, PhD Professor of Dementia Studies and Education
 WICKING DEMENTIA RESEARCH & EDUCATION CENTRE Prof. Fran McInerney RN, BAppSci, MA, PhD Professor of Dementia Studies and Education Wicking Dementia Research & Education Centre Engaging families in a palliative
WICKING DEMENTIA RESEARCH & EDUCATION CENTRE Prof. Fran McInerney RN, BAppSci, MA, PhD Professor of Dementia Studies and Education Wicking Dementia Research & Education Centre Engaging families in a palliative
End of Life with Dementia Sue Quist RN, CHPN
 End of Life with Dementia Sue Quist RN, CHPN Objectives: Describe the Medicare hospice benefit and services. Discuss the Medicare admission criteria for hospice patients with dementia due to Alzheimer
End of Life with Dementia Sue Quist RN, CHPN Objectives: Describe the Medicare hospice benefit and services. Discuss the Medicare admission criteria for hospice patients with dementia due to Alzheimer
behaviors How to respond when dementia causes unpredictable behaviors
 behaviors How to respond when dementia causes unpredictable behaviors the compassion to care, the leadership to conquer how should i handle erratic behaviors? Alzheimer's disease and related dementias
behaviors How to respond when dementia causes unpredictable behaviors the compassion to care, the leadership to conquer how should i handle erratic behaviors? Alzheimer's disease and related dementias
Jacqueline Wesson 24 May 2013
 Jacqueline Wesson 24 May 2013 Dementia is a major health care problem with prevalence to increase four-fold 1 People with dementia: twice the risk of falling & higher risk of injury than those without
Jacqueline Wesson 24 May 2013 Dementia is a major health care problem with prevalence to increase four-fold 1 People with dementia: twice the risk of falling & higher risk of injury than those without
presents Approach to Dementia Care
 presents The I m Still Here Approach to Dementia Care www.thehearth.org 888 422 CARE 1 2 I m Still Here : Activity Programming for Persons with Dementia Presented by Hearthstone Alzheimer Care I m Still
presents The I m Still Here Approach to Dementia Care www.thehearth.org 888 422 CARE 1 2 I m Still Here : Activity Programming for Persons with Dementia Presented by Hearthstone Alzheimer Care I m Still
Dementia Basics. Welcome! What to expect and how to handle a dementia diagnosis. In partnership with Scripps Health.
 Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
CARING FOR PATIENTS WITH DEMENTIA:
 CARING FOR PATIENTS WITH DEMENTIA: LESSON PLAN Lesson overview Time: One hour This lesson teaches useful ways to work with patients who suffer from dementia. Learning goals At the end of this session,
CARING FOR PATIENTS WITH DEMENTIA: LESSON PLAN Lesson overview Time: One hour This lesson teaches useful ways to work with patients who suffer from dementia. Learning goals At the end of this session,
Aims for todays session
 Aims for todays session To provide a brief overview of psychological interventions with carers of people with Dementia and to consider the existing evidence base. To explore the theoretical basis for the
Aims for todays session To provide a brief overview of psychological interventions with carers of people with Dementia and to consider the existing evidence base. To explore the theoretical basis for the
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES
 WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
Dementia Training Session for Carers. By Dr Rahul Tomar Consultant Psychiatrist
 Dementia Training Session for Carers By Dr Rahul Tomar Consultant Psychiatrist Dementia in the UK: Facts & Figures National Dementia strategy launched in 2009 800,000 people living with dementia (2012)
Dementia Training Session for Carers By Dr Rahul Tomar Consultant Psychiatrist Dementia in the UK: Facts & Figures National Dementia strategy launched in 2009 800,000 people living with dementia (2012)
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Rational Medication Use in Dementia
 Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
The Occupational Therapy Role at the Stratford Family Health Team
 The Occupational Therapy Role at the Stratford Family Health Team SKILLS FOR THE JOB OF LIVING LAURA TURNER, OT & SHELLIE BUCKLEY, RN AFHTO CONFERENCE, TORONTO OCTOBER 26, 2011 What is Occupational Therapy?
The Occupational Therapy Role at the Stratford Family Health Team SKILLS FOR THE JOB OF LIVING LAURA TURNER, OT & SHELLIE BUCKLEY, RN AFHTO CONFERENCE, TORONTO OCTOBER 26, 2011 What is Occupational Therapy?
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Managing Behaviors: Start with Yourself!
 Slide 1 Managing Behaviors: Start with Yourself! Teepa Snow, Positive Approach, LLC to be reused only with permission. Slide 2 Time Out Signal copyright - Positive Approach, LLC 2012 Slide 3 REALIZE It
Slide 1 Managing Behaviors: Start with Yourself! Teepa Snow, Positive Approach, LLC to be reused only with permission. Slide 2 Time Out Signal copyright - Positive Approach, LLC 2012 Slide 3 REALIZE It
Dementia: Rethinking our approach to behaviour
 Dementia: Rethinking our approach to behaviour Dr Kathryn Lord Research Fellow 1 A bit about me: The 3 P s! Psychology Psychiatry Person centredcare 2 Challenging behaviours in Challenging behaviours dementia
Dementia: Rethinking our approach to behaviour Dr Kathryn Lord Research Fellow 1 A bit about me: The 3 P s! Psychology Psychiatry Person centredcare 2 Challenging behaviours in Challenging behaviours dementia
Anxiety & Alzheimer s Disease
 Anxiety & Alzheimer s Disease Anxiety is a normal feeling that everyone experiences now and again. In some people, however, these feelings can be very strong and persistent. This can interfere with a person's
Anxiety & Alzheimer s Disease Anxiety is a normal feeling that everyone experiences now and again. In some people, however, these feelings can be very strong and persistent. This can interfere with a person's
How to use the CMS Hand in Hand Training for Dementia Care
 How to use the CMS Hand in Hand Training for Dementia Care How to use the CMS Hand in Hand Training for Dementia Care The purpose of Hand in Hand is to provide nursing homes with a high-quality staff training
How to use the CMS Hand in Hand Training for Dementia Care How to use the CMS Hand in Hand Training for Dementia Care The purpose of Hand in Hand is to provide nursing homes with a high-quality staff training
Forgetfulness: Knowing When to Ask for Help
 National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
Alzheimer s Disease: Behavior Management 2.0 Contact Hours Presented by: CEU Professor
 Alzheimer s Disease: Behavior Management 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Alzheimer s Disease: Behavior Management 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Behavioral and Psychological Symptoms of dementia (BPSD)
") Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
MEDICAL PROVIDERS AND COMMUNITY AGENCIES
 MEDICAL PROVIDERS AND COMMUNITY AGENCIES A GERIATRICIAN AND A COMMUNITY FAMILY CAREGIVER SPECIALIST MAKE THE CASE FOR CONSISTENT AND COORDINATED DEMENTIA CARE ANN O'SULLIVAN, OTR/L, LSW, FAOTA SOUTHERN
MEDICAL PROVIDERS AND COMMUNITY AGENCIES A GERIATRICIAN AND A COMMUNITY FAMILY CAREGIVER SPECIALIST MAKE THE CASE FOR CONSISTENT AND COORDINATED DEMENTIA CARE ANN O'SULLIVAN, OTR/L, LSW, FAOTA SOUTHERN
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
MODULE III Challenging Behaviors
 Mental Health Ombudsman Training Manual Advocacy and the Adult Home Resident MODULE III Challenging Behaviors S WEHRY 2004 Objectives: Part One Describe principles of communication Describe behavior as
Mental Health Ombudsman Training Manual Advocacy and the Adult Home Resident MODULE III Challenging Behaviors S WEHRY 2004 Objectives: Part One Describe principles of communication Describe behavior as
Non-Pharmacological Interventions for Persons With Dementia. John Erpenbach, CNP Michele Snyders, LCSW, ACHP-SW
 Non-Pharmacological Interventions for Persons With Dementia John Erpenbach, CNP Michele Snyders, LCSW, ACHP-SW Prevalence3 5.5 million people in the United States are aging with dementia and complex comorbidities
Non-Pharmacological Interventions for Persons With Dementia John Erpenbach, CNP Michele Snyders, LCSW, ACHP-SW Prevalence3 5.5 million people in the United States are aging with dementia and complex comorbidities
Alzheimer Disease and Related Dementias
 Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Delirium in Palliative care. Presentation to Volunteers 2016 David Falk
 Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
A Family Affair: Effects of Brain Injury on Family Dynamics
 A Family Affair: Effects of Brain Injury on Family Dynamics Dr. Kyle Haggerty, PhD By: Kyle Haggerty Bancroft NeuroRehab TBI Stats The Centers for Disease Control and Prevention reported that in 2010 that
A Family Affair: Effects of Brain Injury on Family Dynamics Dr. Kyle Haggerty, PhD By: Kyle Haggerty Bancroft NeuroRehab TBI Stats The Centers for Disease Control and Prevention reported that in 2010 that
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Know the 10 Signs: Early Detection Matters
 Importance of Early Detection Know the 10 Signs: Early Detection Matters If we could have had a correct diagnosis even two years earlier, it would have given us more time to plan, to do the things that
Importance of Early Detection Know the 10 Signs: Early Detection Matters If we could have had a correct diagnosis even two years earlier, it would have given us more time to plan, to do the things that
NEUROPSYCHOMETRIC TESTS
 NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
In most cases, behavioural and psychological symptoms can be successfully managed without medication.
 MEDICATION People with dementia often develop changes as their condition progresses. These include changes in their behaviour and feelings, the things they think and how they perceive the world. Collectively,
MEDICATION People with dementia often develop changes as their condition progresses. These include changes in their behaviour and feelings, the things they think and how they perceive the world. Collectively,
Know the 10 Signs: Early Detection Matters
 Know the 10 Signs: Early Detection Matters 1 Importance of Early Detection If we could have had a correct diagnosis even two years earlier, it would have given us more time to plan, to do the things that
Know the 10 Signs: Early Detection Matters 1 Importance of Early Detection If we could have had a correct diagnosis even two years earlier, it would have given us more time to plan, to do the things that
Multi-morbidity in Dementia: A 21st Century Challenge. Sube Banerjee. Professor of Dementia Brighton and Sussex Medical School
 Multi-morbidity in Dementia: A 21st Century Challenge Sube Banerjee Professor of Dementia Brighton and Sussex Medical School Most people of any age with any long term condition have multiple conditions
Multi-morbidity in Dementia: A 21st Century Challenge Sube Banerjee Professor of Dementia Brighton and Sussex Medical School Most people of any age with any long term condition have multiple conditions
Understanding and improving attention and information processing in MS
 Understanding and improving attention and information processing in MS Ben Harris Clinical Neuropsychologist Overview A follow up to previous presentation on memory strategies Aim is to provide explanation
Understanding and improving attention and information processing in MS Ben Harris Clinical Neuropsychologist Overview A follow up to previous presentation on memory strategies Aim is to provide explanation
Dementia. Presented By Jennifer L. Nanson
 Dementia Presented By Jennifer L. Nanson Dementia QuickTime and a decompressor are needed to see this picture. Dementia: Current Definition DSM-IV-TR Does not imply a prognosis Refers to a framework of
Dementia Presented By Jennifer L. Nanson Dementia QuickTime and a decompressor are needed to see this picture. Dementia: Current Definition DSM-IV-TR Does not imply a prognosis Refers to a framework of
GERIATRIC PSYCHIATRY: TREATING DEPRESSION AND ANXIETY
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC PSYCHIATRY: TREATING DEPRESSION AND ANXIETY RUTH KOHEN, MD UNIVERSITY OF WASHINGTON 9-20-2018 GENERAL
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC PSYCHIATRY: TREATING DEPRESSION AND ANXIETY RUTH KOHEN, MD UNIVERSITY OF WASHINGTON 9-20-2018 GENERAL
MANAGING DEMENTIA ACROSS THE CONTINUUM (MID TO LATE STAGE)*
*") MANAGING DEMENTIA ACROSS THE CONTINUUM (MID TO LATE STAGE)* PERSON WITH DEMENTIA CARE PARTNER Identify, Assess and Support Optimize Function and Quality of Life Manage Chronic Disease Promote Positive
MANAGING DEMENTIA ACROSS THE CONTINUUM (MID TO LATE STAGE)* PERSON WITH DEMENTIA CARE PARTNER Identify, Assess and Support Optimize Function and Quality of Life Manage Chronic Disease Promote Positive
Caregiver Mediated Intervention. Trumps Pharmacotherapy for BPSD
 Caregiver Mediated Intervention DEMENTIA RESEARCH Trumps Pharmacotherapy for BPSD Henry Brodaty and Caroline Arasaratnam Dementia Collaborative Research Centre Assessment and Better Care Collaborative
Caregiver Mediated Intervention DEMENTIA RESEARCH Trumps Pharmacotherapy for BPSD Henry Brodaty and Caroline Arasaratnam Dementia Collaborative Research Centre Assessment and Better Care Collaborative
Dementia. Memory Evaluation Center Neurology
 Dementia Memory Evaluation Center Neurology Topics Overview of dementia Stages Medications Advanced planning What is Dementia? Dementia = significant global decline in cognitive function not due to medicine
Dementia Memory Evaluation Center Neurology Topics Overview of dementia Stages Medications Advanced planning What is Dementia? Dementia = significant global decline in cognitive function not due to medicine
Outline of content of Mindfulness-based Psychoeducation Program
 Data Supplement for Chien et al. (10.1176/appi.ps.201200209) Appendix Outline of content of Mindfulness-based Psychoeducation Program Introduction The Mindfulness-based Psychoeducation Program (MBPP) consists
Data Supplement for Chien et al. (10.1176/appi.ps.201200209) Appendix Outline of content of Mindfulness-based Psychoeducation Program Introduction The Mindfulness-based Psychoeducation Program (MBPP) consists
Dementia and Driving Checklist
 6 Dementia and Driving Checklist 1. Questions to Ask the Patient and Family Patient Have you noticed any change or decreased confidence in your driving skills Have you had any accidents (or minor fender
6 Dementia and Driving Checklist 1. Questions to Ask the Patient and Family Patient Have you noticed any change or decreased confidence in your driving skills Have you had any accidents (or minor fender
Management of the Acutely Agitated Long Term Care Patient
 Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Risks of Antipsychotics use In Dementia
 AHCA/NCAL Quality Initiative for Assisted Living Webinar Series: Safely Reducing the Off-Label Use of Antipsychotics Risks of Antipsychotics use In Dementia Sanjay P. Singh, MD Chairman & Professor, Department
AHCA/NCAL Quality Initiative for Assisted Living Webinar Series: Safely Reducing the Off-Label Use of Antipsychotics Risks of Antipsychotics use In Dementia Sanjay P. Singh, MD Chairman & Professor, Department
PRACTICAL SOLUTIONS TO REHAB DEMENTIA CARE PART 1 PROMOTING EACH PERSON S BEST ABILITY TO FUNCTION
 The Dementia Problem PRACTICAL SOLUTIONS TO REHAB DEMENTIA CARE PART 1 PROMOTING EACH PERSON S BEST ABILITY TO FUNCTION Efficient, practical & compassionate service is more important than ever before Aging
The Dementia Problem PRACTICAL SOLUTIONS TO REHAB DEMENTIA CARE PART 1 PROMOTING EACH PERSON S BEST ABILITY TO FUNCTION Efficient, practical & compassionate service is more important than ever before Aging
Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital. November /20/ Safety: Falls/Cooking/Unsafe Behaviour. 2.
 How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
These conditions can have similar and overlapping symptoms, and many of them can only be diagnosed with certainty by autopsy of the brain.
 Progression MIDDLE STAGE This document is one in a five-part series on the stages of Alzheimer s disease and is written for the person with the disease, their family 1 and caregivers. The middle stage
Progression MIDDLE STAGE This document is one in a five-part series on the stages of Alzheimer s disease and is written for the person with the disease, their family 1 and caregivers. The middle stage
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care.
 Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
nicheprogram.org 2015 Annual NICHE Conference Innovation Through Leadership Background
 Wii Can Too! Using Gaming Technology with Hospital Elder Life Program Patients Megan Wheeler, MSN, RN, ACNS-BC Janice F. Moore, PhD, CFLE Background Grant Proposal Hospital Elder Life Program (HELP) proven
Wii Can Too! Using Gaming Technology with Hospital Elder Life Program Patients Megan Wheeler, MSN, RN, ACNS-BC Janice F. Moore, PhD, CFLE Background Grant Proposal Hospital Elder Life Program (HELP) proven
Session 16: Manage Your Stress
 Session 16: Manage Your Stress Stress is part of life. However, you can learn better ways to take care of yourself when faced with stress. Stress is not always bad. Some stress can make life interesting
Session 16: Manage Your Stress Stress is part of life. However, you can learn better ways to take care of yourself when faced with stress. Stress is not always bad. Some stress can make life interesting
Conducting Groups. March 2015
 Conducting Groups March 2015 Agenda Advantages of groups Members of the group Group leader Role of the leader, maximize participation, & use effective communication skills Group participants The forceful,
Conducting Groups March 2015 Agenda Advantages of groups Members of the group Group leader Role of the leader, maximize participation, & use effective communication skills Group participants The forceful,
UNDERSTANDING CAPACITY & DECISION-MAKING VIDEO TRANSCRIPT
 I m Paul Bourque, President and CEO of the Investment Funds Institute of Canada. IFIC is preparing materials to assist advisors and firms in managing effective and productive relationships with their aging
I m Paul Bourque, President and CEO of the Investment Funds Institute of Canada. IFIC is preparing materials to assist advisors and firms in managing effective and productive relationships with their aging
Delirium A guide for caregivers
 Delirium A guide for caregivers Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified health-care provider. Please consult your
Delirium A guide for caregivers Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified health-care provider. Please consult your
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) Friedmann, E., Galik, E., Thomas, S. A, Hall, P. S, Chung, S. Y., & McCune, S. (2015). Evaluation of a pet-assisted living intervention for improving functional status
CRITICALLY APPRAISED PAPER (CAP) Friedmann, E., Galik, E., Thomas, S. A, Hall, P. S, Chung, S. Y., & McCune, S. (2015). Evaluation of a pet-assisted living intervention for improving functional status
Everyday Strategies to Manage Thinking and Memory Changes Associated with MS
 Everyday Strategies to Manage Thinking and Memory Changes Associated with MS Ben Harris (MPsych, PhD) Clinical Neuropsychologist Overview Brief summary of areas of cognitive function commonly affected
Everyday Strategies to Manage Thinking and Memory Changes Associated with MS Ben Harris (MPsych, PhD) Clinical Neuropsychologist Overview Brief summary of areas of cognitive function commonly affected
CHRONIC DISEASE SELF- MANAGEMENT EDUCATION
 CHRONIC DISEASE SELF- MANAGEMENT EDUCATION People spend 99 percent of their time outside the health care system and what they do outside largely determines their quality of life. This prepares them for
CHRONIC DISEASE SELF- MANAGEMENT EDUCATION People spend 99 percent of their time outside the health care system and what they do outside largely determines their quality of life. This prepares them for
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Active Living with Arthritis Podcast #9 Being a Caregiver: Caring for Someone and Managing Your Arthritis
 Active Living with Arthritis Podcast #9 Being a Caregiver: Caring for Someone and Managing Your Arthritis Karen: Welcome to another Active Living with Arthritis podcast, presented by ENACT center at Boston
Active Living with Arthritis Podcast #9 Being a Caregiver: Caring for Someone and Managing Your Arthritis Karen: Welcome to another Active Living with Arthritis podcast, presented by ENACT center at Boston
- Impaired vision or hearing causing person to misinterpret sights and sounds. - Hallucinations.
 POSSIBLE CAUSES PHYSIOLOGICAL OR :MEDICAL CAUSES: -Fatigue at time of request, activity or event. - Disruption of sleep pattern (day and night reversal) causing sleep deprivation. - Physical discomfort,
POSSIBLE CAUSES PHYSIOLOGICAL OR :MEDICAL CAUSES: -Fatigue at time of request, activity or event. - Disruption of sleep pattern (day and night reversal) causing sleep deprivation. - Physical discomfort,
Behavioral symptoms, a core clinical feature of dementia,
 Targeting Behavioral Symptoms and Functional Decline in Dementia: A Randomized Clinical Trial Laura N. Gitlin, PhD,* Paul Arthur, PhD, OTR/L, Catherine Piersol, PhD, OTR/L, Virginia Hessels, BA, Samuel
Targeting Behavioral Symptoms and Functional Decline in Dementia: A Randomized Clinical Trial Laura N. Gitlin, PhD,* Paul Arthur, PhD, OTR/L, Catherine Piersol, PhD, OTR/L, Virginia Hessels, BA, Samuel
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE
 CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
This information explains the advice about supporting people with dementia and their carers that is set out in NICE SCIE clinical guideline 42.
 Supporting people with dementia and their carers Information for the public Published: 1 November 2006 nice.org.uk About this information NICEclinicalguidelinesadvisetheNHSoncaringforpeoplewithspe cificconditionsordiseasesandthetreatmentstheyshouldreceive.
Supporting people with dementia and their carers Information for the public Published: 1 November 2006 nice.org.uk About this information NICEclinicalguidelinesadvisetheNHSoncaringforpeoplewithspe cificconditionsordiseasesandthetreatmentstheyshouldreceive.
Organization: Sheppard Pratt Health System Solution Title: Lean Methodology: Appropriate Antipsychotic Use on an Inpatient Dementia Unit
 Organization: Sheppard Pratt Health System Solution Title: Lean Methodology: Appropriate Antipsychotic Use on an Inpatient Dementia Unit Problem: For dementia patients, antipsychotic medications are prescribed
Organization: Sheppard Pratt Health System Solution Title: Lean Methodology: Appropriate Antipsychotic Use on an Inpatient Dementia Unit Problem: For dementia patients, antipsychotic medications are prescribed
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Professor of Psychiatry Director, Program for Positive Aging
 Nonpharmaceutical Management of Professor of Psychiatry Director, Program for Positive Aging University of Michigan Acknowledgements NIMH: R01MH081070 (Antipsychotic Pharmacoepidemiology) H. Myra Kim PhD
Nonpharmaceutical Management of Professor of Psychiatry Director, Program for Positive Aging University of Michigan Acknowledgements NIMH: R01MH081070 (Antipsychotic Pharmacoepidemiology) H. Myra Kim PhD
Introduction to Dementia: Complications
 Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Psychotropic Medication. Including Role of Gradual Dose Reductions
 Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Depression in Older Adults. Key Issues
 Depression in Older Adults Key Issues Depression and Older Adults: Key Issues is an overview of important information that you should know about depression in older adults. Depression is one of the most
Depression in Older Adults Key Issues Depression and Older Adults: Key Issues is an overview of important information that you should know about depression in older adults. Depression is one of the most
Understanding and preventing delirium in older people
 Understanding and preventing delirium in older people Tips for family, whānau, and friends As people get older, especially if they are unwell or living with a dementia, they have greater risk of developing
Understanding and preventing delirium in older people Tips for family, whānau, and friends As people get older, especially if they are unwell or living with a dementia, they have greater risk of developing
Memory & Aging Clinic Questionnaire
 Memory & Aging Clinic Questionnaire The answers you give to the questions below will assist us with our evaluation. Each section is equally important so please be sure to complete the entire questionnaire.
Memory & Aging Clinic Questionnaire The answers you give to the questions below will assist us with our evaluation. Each section is equally important so please be sure to complete the entire questionnaire.
homeinstead.com Each Home Instead Senior Care franchise office is independently owned and operated Home Instead, Inc.
 Each Home Instead Senior Care franchise office is independently owned and operated. 2010 Home Instead, Inc. homeinstead.com Many of us may joke about having old timers disease, but when cognitive impairment
Each Home Instead Senior Care franchise office is independently owned and operated. 2010 Home Instead, Inc. homeinstead.com Many of us may joke about having old timers disease, but when cognitive impairment
Management of Behavioral Problems in Dementia
 Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Dealing with Distress. SUBTITLE: Coping with Challenging Behaviors. Do that Makes a Difference!
 Dealing with Distress Learning How Use Empathy & Support SUBTITLE: Coping with Challenging Behaviors It s How You Do What You Do that Makes a Difference! Changing Resistance to Care and Refusals to Participation
Dealing with Distress Learning How Use Empathy & Support SUBTITLE: Coping with Challenging Behaviors It s How You Do What You Do that Makes a Difference! Changing Resistance to Care and Refusals to Participation
CURRICULUM VITAE Part I. Year Degree Institution/Location Postdoctoral Research Johns Hopkins University School of Nursing.
 PERSONAL DATA CURRICULUM VITAE Part I Natalie G. Regier, Ph.D. Office: 525 N. Wolfe Street SON House, Room 301 21205 Phone (443) 287-4891 EDUCATION Year Degree Institution/Location 2014-2016 Postdoctoral
PERSONAL DATA CURRICULUM VITAE Part I Natalie G. Regier, Ph.D. Office: 525 N. Wolfe Street SON House, Room 301 21205 Phone (443) 287-4891 EDUCATION Year Degree Institution/Location 2014-2016 Postdoctoral
Cognitive Training Interventions for Delaying Cognitive Decline
 Cognitive Training Interventions for Delaying Cognitive Decline Jessica B. Langbaum, Ph.D. Principal Scientist, Banner Alzheimer s Institute Associate Director, Alzheimer s Prevention Initiative Disclosures
Cognitive Training Interventions for Delaying Cognitive Decline Jessica B. Langbaum, Ph.D. Principal Scientist, Banner Alzheimer s Institute Associate Director, Alzheimer s Prevention Initiative Disclosures
GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES
 FACULTY DEVELOPMENT MASTERWORKS SERIES") UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
Cognitive Impairment - Parkinson's Disease Foundation (PDF)
") Page 1 of 8 Cognitive Impairment Another troublesome symptom of Parkinson s is mild cognitive impairment. Many people with Parkinson s are surprised to find that they feel distracted or disorganized, or
Page 1 of 8 Cognitive Impairment Another troublesome symptom of Parkinson s is mild cognitive impairment. Many people with Parkinson s are surprised to find that they feel distracted or disorganized, or
section 6: transitioning away from mental illness
 section 6: transitioning away from mental illness Throughout this resource, we have emphasized the importance of a recovery perspective. One of the main achievements of the recovery model is its emphasis
section 6: transitioning away from mental illness Throughout this resource, we have emphasized the importance of a recovery perspective. One of the main achievements of the recovery model is its emphasis
The Investigation and Comparison of the underlying needs of common disruptive behaviors in patients with Alzheimer s disease
 The Investigation and Comparison of the underlying needs of common disruptive behaviors in patients with Alzheimer s disease Jing-Jy Wang Professor, Institute of Allied Health Science & Department of Nursing
The Investigation and Comparison of the underlying needs of common disruptive behaviors in patients with Alzheimer s disease Jing-Jy Wang Professor, Institute of Allied Health Science & Department of Nursing
Recognizing Signs and Symptoms of Alzheimer's Disease in Earlier Stages Can Lead to Diagnosis
 A joint publication of the Illinois Health Care Association and CE Solutions November 2015 Recognizing Signs and Symptoms of Alzheimer's Disease in Earlier Stages Can Lead to Diagnosis Early diagnosis
A joint publication of the Illinois Health Care Association and CE Solutions November 2015 Recognizing Signs and Symptoms of Alzheimer's Disease in Earlier Stages Can Lead to Diagnosis Early diagnosis
Getting Help for Patients with Dementia and their Caregivers. Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY
 Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,