Restoring function in community dwelling older adults: Balancing risk, frailty and medical complexity
|
|
|
- Daniel Ramsey
- 6 years ago
- Views:
Transcription

1 Restoring function in community dwelling older adults: Balancing risk, frailty and medical complexity Dr. Jo-Anne Clarke Geriatrician, North East Specialized Geriatric Services
2 Disclosure Faculty: Jo- Anne Clarke Relationships with commercial interests: No Grants/Research Support Speakers Bureau/Honoraria: none from pharmaceutical interests in 2 years Consulting Fees: None Other: None Disclosure of commercial support This program has not received any financial or in- kind support. Potential for conflict of interest: There is no conflict of interest

3 Courtesy Dr. S. Sinha, with permission
4 1) Steep Downward Slant Trajectory Health Wellness Heart Attack / Car Accident Few of us will die in this manner Illness Death Function Time Diagnosis Death Courtesy, Dr. J McElhaney
5 2) Gradual Slant Trajectory Health Wellness MS / ALS Illness Death Function Diagnosis Time Death Courtesy, Dr. J McElhaney
6 3) Peaks and Valleys Trajectory Health Wellness Chronic Heart and Lung Failure Illness Death Function Diagnosis Time Death Courtesy, Dr. J McElhaney
7 4) Gradual Descending Plateaus Trajectory Health Wellness Function Illness Death Diagnosis Time Frailty and Dementia Dwindling Over Time Death Courtesy, Dr. J McElhaney
8 Chronic disease burden Rapoport et al, 1999; National Population Health Survey, Chronic Dis Canda 2004 Older persons accumulate chronic illness as they age Age Number of chronic conditions % 30% 14% 12% % 25% 25% 30% % 24% 22% 41% Heckman, With Permission
9 Disability Gilmour & Park, Suppl Health Reports, Stats Can Canadian Community Health Survey adults > 65, are women Age Basic ADL Instrumental ADL Men Women Men Women % 4% 9% 18% % 9% 21% 36% % 23% 46% 65% Heckman, With Permission
10 Frailty Impairments in multiple systems that lead to a decline in homeostatic reserve and resiliency Comorbidity Two or more medical conditions Disability Difficulty or dependency in daily living (ADL/IADL)
11 Frailty A medical syndrome with multiple causes and contributors that is characterized by diminished strength, endurance, and reduced physiologic function that increases an individual s vulnerability for developing increased dependency and/or death 1 Is a result of deficit accumulation Is a predictor of poor outcomes Functional decline Falls Health service utilization Caregiver fatigue and stress Death Institutionalization 1. Morley et al JAMDA 14 (2013)
12 Frailty and Functional Decline are geriatric syndromes Inouye, 2007
13 HRS Study - Association btw disease, geriatric syndromes, and disability Condition Number of geriatric conditions Stroke Diabetes Heart disease Cancer RR of disability Ann Intern Med 2007;147: Heckman, With Permission
14 Geriatric syndromes As prevalent as chronic disease In the HRS, 50 % of people > 65 had 1 or more geriatric conditions Commonly co- occur with chronic disease more than 25% of older adults with chronic disease have at least one geriatric syndrome Strongly associated with functional decline and disability More likely than stroke to cause disability Top 3 predictors of why cannot go home from hospital (mobility, incontinence, cognitive impairment) Incontinence Pressure ulcers Falls Frailty Delirium Cognitive impairment.
15 Frailty: Is a changeable state Frailty is dynamic, characterized by frequent transitions between frailty states over time 57.6 % had at least one transition Transitions to states of greater frailty (up to 43.3%) was more common than states of lesser frailty (23.0%). Gill et al. Arch Intern Med 2006;166:
16 ADL Disability also dynamic Transitions were common The frail, when compared to the non- frail were less likely to stay independent - > (20% vs 47%, p< 0.001) Had higher absolute numbers of transitions Had higher rates of transition to more disability Had longer durations of disability Severe disability episodes resulting in recovery tended to be very short (ie. less than 1 month) Hardy et al Am J Epidemiol 2005;161:575-84
17 Mobility Disability also dynamic Mobility disability highly dynamic Rates of transition over 5yrs 74.3 /1000 person mo. walking 51.7/1000 person mo. climbing Transitions to states of greater disability correlated with age, frailty, sex (women) Most had at least one episode (intermittent disability) lasted on average six months, highest transition rate (to no disability) Gill et al. JAGS 2006; 54:
18 Disability can occur insidiously Not physically frail Physically frail Physical frailty was the only factor that was associated significantly with the development of insidious disability, OR 2.1 (95%CI: 1.2 to 3.8) Gill. Am J Med. 2004;117:484
19 Disabled patients recover 80% recover But it can be short lasting Type of Recovery Disability 2 mo Recovery 6 mo Any 79% 57% Persistent 64% 40% Chronic 57% 33% Even with chronic disability (> 3months) > 60% recovered Hardy et al JAMA 2004
20 Hospitalizations and illnesses leading to restricted activity are important sources of disability Factors associated to development of disability Factor COPD 1.09 Depression 1.32 Cognitive impairment 1.23 CHF 1.66 Stroke 1.66 Frailty 2.09 New Intervening event Hospitalization 59.8 Restricted activity 5.11 Hazard Ratio Most common reason for disability post hospitalization was cardiac, but: Injurious falls most POTENT, conferring the highest risk of disability 79.4% of admissions for a fall- related injury led to any disability, 45.2% to persistent disability, 58.8% to disability with nursing home admission. Gill T et al JAMA 2004, JAMA 2010
21 Risk factors for functional decline community dwelling (Stuck 1999 soc sci med.) Risk Factors Syndrome Intervention Cognitive impairment Depression High Disease burden High and low BMI LE functional limitation Low frequency of social contacts Low level of physical activity Polypharmacy Poor self perceived health Smoking Vision impairment FUNCTIONAL DECLINE Modify reversible factors Asses and treat Co- manage Healthy diet, exercise Exercise and physio Social engagement Exercise and physio Medication review? Smoking cessation Assess and treat
 Risk Factors Syndrome Intervention Cognitive impairment Depression HighDisease burden High and low BMI LE functional limitation Low frequency of social contacts Low level of physical activity")
22 Risk factors for functional decline community dwelling (Stuck 1999 soc sci med.) Risk Factors Syndrome Intervention Cognitive impairment Depression HighDisease burden High and low BMI LE functional limitation Low frequency of social contacts Low level of physical activity Polypharmacy Poor self perceived health Smoking Vision impairment FUNCTIONAL DECLINE Modify reversible factors Asses and treat Co- manage Healthy diet, exercise Exercise and physio Social engagement Exercise and physio Medication review? Smoking cessation Assess and treat
23 Interventions work to reduce functional decline in frail older adults Exercise works in the frail 1-2, even in LTC 3, in the cognitively impaired 4-5 and in those with geriatric syndromes 6 to reduce functional decline and falls Home OT with exercise improves function and reduced mortality 7 Medication Review improves function, reduces falls and mortality 8-9 Comprehensive Geriatric Assessment Leads to better prescribing, better function, improved cognition, less institutionalization, less hospitalization, lower mortality Gill NEJM 2002;347: Pahor J Gerontol A biol Sci Med Sci 2006: Fiaterone N Engl J Med 1994; Vreugdenhil Scand J Caring Sci ;26:12 5. Pitkala. JAMA Intern Med. 2013;173: Kim, Arch Gerontol Geriatr :99 7. Gitlin et al. JAGS 2009;57: Garfinkel et al Isr Med Assoc2007;9:430-4, 9. Hill et al. Drugs Aging 2012;29: Stuck, Lancet NZHTA Report 2004, 12.Schmader Am J Med Beswick Lancet 2008, 14.Challis 2004.
24 Comprehensive assessment An individualized approach to risk factor modification Medication Review Optimize Communication (vision, hearing) Dehydration/Orthostatic BP Mood Cognition Function Balance Gait Aids, Environmental modification Formal and informal supports Interdisciplinary With timely access and open communication with home care /community support services
25 Evaluation of New Disability or Decline in Function Community Transitions ED interrai Hospital Identify function Characterize disabilities and threats to independence Establish risk CGA Identify impairments / syndromes Identify health conditions Identify resources Clinical assessment Data gathering A multidimensional, interdisciplinary process that determines a frail older person s medical, psychological, functional and environmental capacity, and creates an overall plan for treatment and follow- up Goal setting, priorities, prognostication 2. Improve health and capacity for self care 3. Reduce task demand What is modifiable or requires support? Action Collaboration with primary care Family & support education Integrated care and chronic disease management Ongoing re- evaluation of treatment plan Anticipatory guidance Risk optimization Advanced care planning Adapted with permission from Functional Decline in Older Adults, September 15, 2013, Vol 88, No 6, American Family Physician Copyright 2013 American Academy of Family Physicians. All Rights Reserved 1 and Molnar, 2015
26 Evaluation of New Disability or Decline in Function Characterize disabilities and threats to independence CGA Identify impairments / syndromes Cognition / Delirium Mood Pain Nutrition Identify health conditions Cardio / Resp disease MSK conditions Mood / cognitive disorders Identify resources Social supports Financial Environmental Personality traits Clinical assessment Data gathering Medication review Mobility / Falls Neurological conditions Vision / Hearing Sleep Bowel / Bladder Incontinence Metabolic disorders Caregiver Burden Adapted with permission from Functional Decline in Older Adults, September 15, 2013, Vol 88, No 6, American Family Physician Copyright 2013 American Academy of Family Physicians. All Rights Reserved 1 and Molnar, 2015
27 Evaluation of New Disability or Decline in Function What is modifiable or requires support? CGA 1. Goal setting, priorities, prognostication 2. Improve health and capacity for self care Re- evaluate need for ongoing test/procedures/treatments Medication changes Surgical options Nutritional strategies Devices Exercise / Rehabilitation Counselling 3. Reduce task demand Supports / Environment Environmental modification Devices Human resources Caregiver support Action Adapted with permission from Functional Decline in Older Adults, September 15, 2013, Vol 88, No 6, American Family Physician Copyright 2013 American Academy of Family Physicians. All Rights Reserved 1 and Molnar, 2015
28 Evaluation of New Disability or Decline in Function Communit y Transitions ED Hospital Identify function loss Characterize disabilities and threats to independence interrai Establish risk CGA Identify impairments / syndromes Identify health conditions Identify resources Clinical assessment Data gathering Goal setting, priorities, prognostication A multidimensional, interdisciplinary process that determines a frail older person s medical, psychological, functional and environmental capacity, and creates an overall plan for treatment and follow- up. 2 Improve health and capacity for self care Reduce task demand Action What is modifiable or requires support? Collaboration with primary care Integrated care and chronic disease management Family & support education Ongoing re- evaluation of treatment plan Anticipatory guidance Risk optimization Advanced care planning Adapted with permission from Functional Decline in Older Adults, September 15, 2013, Vol 88, No 6, American Family Physician Copyright 2013 American Academy of Family Physicians. All Rights Reserved 1 and Molnar, 2015
29 inpatient Ellis G et al. Comprehensive Geriatric Assessment for older adults admitted to hospital : meta analysis of randomized controlled trial. BMJ 2011;343 Baztan JJ, Suarez- Garcia FM, Lopez- Arrieta J et al. Effectiveness of acute geriatric units on functional decline, living at home and case fatality among older patients admitted to hospital or acute medical disordes: Meta Analysis. BMJ 2009;338:b50. Van Craen K, Braes T, Wellens N et al. The effectiveness of inpatient geriatric evaluation and management units; a systematic review and meta- analysis. J Am Geriatr Soc 2010;58: Deschodt M et al. Impact of geriatric consultation teams on clinical outcomes in acute hospitals: a systematic review and meta- analaysis. BMC Med 2013;11:48 Stuck AE. Comprehensive geriatric assessment: a meta analysis of controlled trials. Lancet 1993;342:
30 Ambulatory Ekdahl AW, Wiren AB, Alwin J et al.costs and Effects of an Ambulatory Geriatric Unit (the Age- FIT Study): a Randomized Controlled Trial. JAMDA xxx(2015) 1-7 Article in Press. Elkan R, Kendrick K, Dewey M et al. Effectiveness of homes based support for older people. Systematic review and meta- analysis BMJ 2001; 323: Huss A, Stuck AE, Rubenstein LZ et al. Multidimentional preventive home visit programs for community dwelling older aldults. A systematic review and meta- analysis of randomized controlled trial. J Gerontol A Biol Sci Med Sci 2008;63: Lihavainen K, Sipila S, Rantanen T et al. Effects of comprehensive geriatric assessment and targeted intervention on mobility in persons aged 75 years and over: a randomized controlled trial. Clin Rehabil 2012;26 (4): Tikkanen P, Lonnroos E, Sipila S et al. Effects of comprehensive geriatric assessment- based individually targeted iinterventions on mobility of pre- frail and frail community- dwelling older people. Geriatr Gerontol Int 2015;15: Fairhall N, Sherrington C, Kurrle SE. Effect of multifactorial interdisciplinary intervention on mobility- related disability in frail older people: a randomized controlled trial. BMC Med 2012;10 (120):1-13. Challis et al The value of specialist clinical assessment of older people prior to entry to care homes. Age Agein 2004; 33:25-34 Beswick et al Complex interventions to improve physical function and maintain independent living in elderly people: a systematic review and meta- analysis. Lancet 2008; 371: Caplan et al A Randomized, Controlled Trial of Comprehensive Geriatric Assessment and Multidisciplinary Intervention After Discharge of Elderly from the Emergency Department - The DEED II StudyJ Am Geriatr Soc 52: , 2004.
31 Outpatient CGA Based Care AGe- FIT Study Community dwelling pts 75 who had received inpatient care 3 x or more in the last year and 3 medical diagnosis Randomized CGA based care at ambulatory unit (n=208) vs usual care (n=174), followed for 24 months, municipal setting RN, geriatrician, manager, OT, PT, dietician, admin assistant, access to psychologist, dental, pharmacist. CGA was standardized, then an individually tailored program and follow up. Home visit, telephone calls, as needed. All reassessed at 1 yr by RN clinician, and subsequent follow up tailored. If hospitalized, team members visited, facilitated care and assisted with discharge Ekdahl AW et al. JAMDA xxx (2015):1-7, in Press.
32 Outpatient CGA Based Care Age- FIT Study Number hospitalizations did not differ between groups Number of inpatients days during 24 month period was smaller in the intervention group (11.1 vs 15.2, p=0.035). Cost of health care did not differ Intervention group had higher ambulatory costs, which were offset by reduced inpatient days Trend towards fewer days in nursing home (29 vs 36 days) and lower nursing home admittance (12.5% vs 18.9%, NS p= 0.065) Intervention group used 25% more hours of home help services (NS) Sense of security of care was higher in the intervention group (p <0.001) Ekdahl AW et al. JAMDA xxx (2015):1-7, in Press.
33 Partcipants in the intervention group lived an average of 30.9 days longer Kaplan Meier mortality curves from the time of study inclusion. Intention to treat. HR 1.51, 95% CI , p =0.057* *per protocol analysis (exl. 11 who never participated). Mortality was lower in the intervention group: HR 1.60 ( , p=.035)
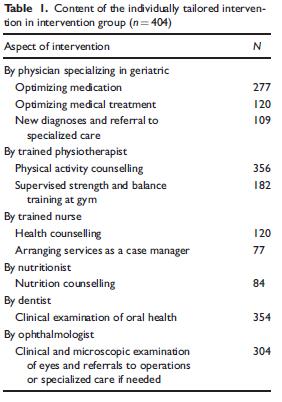
34 Oupatient CGS Based Care - GeMS study Finnish persons aged years were randomized to CGA with multifactorial intervention (n=404) or usual care (n=377). Community dwelling and assisted living facilities. The intervention included individualized referrals, recommendations, physical activity counselling and supervised resistance training, follow up = 2 years. Measurements: Perceived limitation in walking 400m was gathered annually during the intervention and at the one- year post- intervention follow- up. Lihavainen et al. Clin Rehabil 2012;26:
35
36 Proportion of participants reporting mobility limitation in the IG and CG at baseline, during study, and at follow up. Control Intervention 77% without mobility limitation in IG maintained vs 69% CG (p<0.001) Proportion who had or developed mobility limitation during the study were 13% in IG vs 25% in the CG (p < 0.001) NNT to prevent or recoover mobility limitation was 12.
37 Effect of the intervention on mobility was greater among persons with MSK pain, the frail or pre- frail. Whole sample With pain Without pain MobilityLimitation
38 Effect of the intervention on mobility was greater among persons with MSK pain, the frail or pre- frail. Intervention Control Intervention Non- Frail Control Pre- Frail and Frail Tikkanen et al. Geriatr Gerontol Int 2015;15:80-88
39 Oupatient CGS Based Care FiT study RCT with 241 frail community- dwelling older people in Sydney, Participants were classified as frail using the Cardiovascular Health Study definition, did not have severe cognitive impairment (MMSE as low as 18) and were recently discharged from an aged care and rehabilitation service. Intervention was complex begins with a Comprehensive Geriatric evaluation followed by a 12 month multifactorial, interdisciplinary intervention targeting identified frailty components The intervention was individualized, both in relation to the problem s cause and to the goals of participants and family members 1. Cameron et al BMC Medicine 2013,11:65 2. Fairhall et al BMC Medicine 2012,10:120
40 Interventions Based on Targeting Frailty components If weight loss - > dietician, home delivered meals If BMI < 18.5kg/m2 - > nutritional supplementation Exhaustion, high GDS - > psychiatrist or psychologist Socially isolated - > options for social engagement, volunteer phone calls Up to 10 homebased, 45- to 60- minute physiotherapy sessions over 12 months. Front- end loaded, with five sessions in the first three months. Weight Bearing for Better Balance, tailored to pts individual impairments, prescribed 3-4x/week, reviewed regularly 2 physiotherapy sessions targeted the pts mobility goal OT / community exercise as indicated Case management and care coordination by physiotherapist, and regular case conferences with PT, geriatrician, rehab physicians, RN, dietician to coordinate intervention Additional interventions based on CGA (pain, chronic disease, incontinence) 1. Cameron et al BMC Medicine 2013,11:65 2. Fairhall et al BMC Medicine 2012,10:120
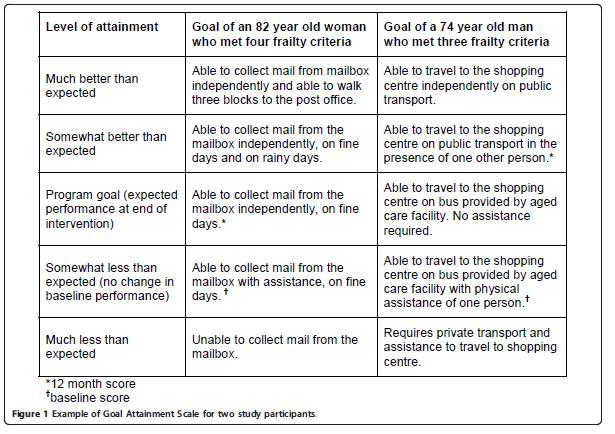
41 Outcomes Primary outcomes 1 : Frailty and mobility Frailty CHS criteria (3 or more of slow gait speed, weak grip strength, exhaustion, low energy expenditure, and weight loss) Mobility SPPB Ability to stand feet side by side, tandem and semi- tandem Time to walk 4 meters Time to rise from chair and return to seated position 5 times Secondary Outcomes1: Hospitalizations, NH, disability, QOL Mobility related disability2 Participation restriction Goal attainments scaling to measure achievement of mobility related participation goals set in the home or community The Life Space Assessment to quantify mobility (distance, frequency and degree of independence Activity limitation Walking speed using 4 m walk test Self report measures 1. Cameron et al BMC Medicine 2013,11:65 2. Fairhall et al BMC Medicine 2012,10:120
42
43 What did the intervention look like Women 68%, age 83.3 years, mean frailty score 3.4 Well matched at baseline, control group had slightly better Mobility score (SPPB) and lower extremity score Adherence was 0% for 16 (13%), Median adherence overall was 26 to 50% Average of 10 face to face sessions with a physio, incl. 8 sessions to teach the WEBB program Average of 4 telephone calls to each participant (and 4 to other parties) WEBB program was delivered to 93% of intervention group Dietician assessment and intervention 50% Medical specialist (geriatrician or rehabilitation physician) 24% Psychologist or psychiatrist 3%
44 CGA based - multidisciplinary intervention reduces frailty, improves mobility - FiT Trial At 12 months : Frailty was lower in the intervention group: Absolute difference : 14.7% (95% CI 2.4 to 2.07%) p = 0.02 NNT = 6.8 Mobility remained stable in the intervention group, declined in control group SPPB score increased in IG by 0.52 (SD 2.47) and declined in CG by 0.98 (SD 2.3) Similar results for mobility as assessed by LE strength No differences in secondary outcomes Stronger adherence was significantly associated with improved outcomes No change seen at 3 months Outcome Intervention Control P- value Death 12 (10%) 10 (8.26%) 0.64 Hospitalization NH admission Cameron et al BMC Medicine 2013;11:65
45 CGA based - multidisciplinary intervention reduced Mobility related disability FiT Trial Had better scores on the Goal Attainment Scale OR 2.1; 95% CI 1.3 to 3.3, P = 0.004) Had Better scores on the Life Space Assessment (4.68 points, 95% CI 1.4 to 9.9, P = 0.005). Walked 0.05 m/s faster over 4 m (95% CI to 0.1, P = 0.048), Scored higher on the Activity Measure for Post Acute Care (P < 0.001). Fairhall et al BMC Medicine 2012;10:120
46 Heterogeneity is the new normal This population is by definition complex, and heterogeneous One approach will not fit all older adults Cannot use a simple tool, simple model No guideline exists for the management of complexity BGS Best Practice Guideline recommends CGA as the gold standard for managing frailty 1 Approach with most likelihood of success tends to be multi- dimentional / mutli- disciplinary/ multi- organizational in approach Mantra of geriatrics it depends Dementia - - is it a predictor of poor outcome for rehab? Apathy 2 1. Turner G, Clegg A Age and Ageing 2014;43: Clarke D et al Int Psychogeriatr 2010;22:819-29
47 Predicting restorative potential is complicated Patterns of Functional Decline at the end of life is highly variable Frail patients 8x more likely than elders who have sudden death to be ADL dependent at end of life; organ failure patients 3x more likely 1 Determining expected trajectory is challenging 2 easier to predict if acute or subacute change Approach should be determined by the comprehensive clinical assessment What components have led or are contributing to the functional decline, and what is reversible/modifiable. Need to ask the question why 1. Lunney JAMA 2003; Gill et al NEJM 2010;362:
48
49 High Yield aspects of CGA Those targeting persons at highest risk Those providing a higher intensity intervention Those with longer follow up periods Individualized interventions (rather than standardized protocols) Mulit- component /Interdisciplinary intervention Individualized Plan Integration with primary and palliative care, goals of care being at the fore front Rubenstein JAMDA 2015 Rockwood BMC Medicine :121
50 System issues Frail, complex older adults have different needs Multiple chronic diseases, daily symptoms, vulnerable to small stressors Require difference services from different practitioners in home, hospital, outpatient, community, telemedicine Functional Disability is the most influential determinant of cost, utilization, complexity Mobility related disability, in particular, is the result of multiple impairments Complex problems require complex responses 1 Episodic visits, short visits, do not allow for early identification and prevention of functional decline Multiple visits, assessments, result Require coordination of care, chronic disease management, and integration of functional status and prognosis in to care planning Reduced acute care use, better patient outcomes, lower costs Beswick et al Lancet 2008; 371: Eklund K Health and Social Care in the Community 17: Johri M,. International Journal of Geriatric Psychiatry 18:
51 An Effective Assess and Restore Strategy Will Appreciate the complexity and heterogeneity of this population Understand that functional decline is a geriatric syndrome, which is a complicated clinical problem requiring specialty care Emphasize the need for timely and effective geriatric assessment that includes a multidisciplinary approach, specialized services, and intervention Minimize red tape and multiple assessments as barriers to timely and effective intervention Creates capacity in the system to support a pre- hab, re- hab and post- hab approach
52

53 Freestyle Centenarian Mieko Nagaoka, 100 yr woman first centenarian to complete 1500 m freestyle swim, 20 years after she took up the sport
54 Beautiful young people are accidents of nature, but beautiful old people are works of art. - Eleanor Roosevelt (maybe)
PREVENTION AND MANAGEMENT OF FRAILTY. Christopher Patterson John Feightner for the Canadian Initiative on frailty and Aging 2006
 PREVENTION AND MANAGEMENT OF FRAILTY Christopher Patterson John Feightner for the Canadian Initiative on frailty and Aging 2006 Prevention & management Avoidance of definition of frailty SER of RCTs addressing
PREVENTION AND MANAGEMENT OF FRAILTY Christopher Patterson John Feightner for the Canadian Initiative on frailty and Aging 2006 Prevention & management Avoidance of definition of frailty SER of RCTs addressing
Ageing Well. Avoiding falls in older people. Prof Martin Vernon NCD Older People. Find Recognise Assess Intervene Long-term.
 Ageing Well Avoiding falls in older people Prof Martin Vernon NCD Older People 21 October 2016 1 Its not how old we are, but how we are old 2 Key points 1. Demography 2. Frailty & falls 3. Routine frailty
Ageing Well Avoiding falls in older people Prof Martin Vernon NCD Older People 21 October 2016 1 Its not how old we are, but how we are old 2 Key points 1. Demography 2. Frailty & falls 3. Routine frailty
Functional Decline in Community Dwelling Older Adults
 Functional Decline in Community Dwelling Older Adults An Update from the Frail Senior/Medically Complex Task Group Rehabilitative Care Alliance Dr. Jo-Anne Clarke Geriatrician North East Specialized Geriatric
Functional Decline in Community Dwelling Older Adults An Update from the Frail Senior/Medically Complex Task Group Rehabilitative Care Alliance Dr. Jo-Anne Clarke Geriatrician North East Specialized Geriatric
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum
 Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Integrating Geriatrics into Oncology Care
 Integrating Geriatrics into Oncology Care William Dale, MD, PhD Chief, Geriatrics & Palliative Medicine Director, Specialized Oncology Care & Research in the Elderly (SOCARE) Clinic University of Chicago
Integrating Geriatrics into Oncology Care William Dale, MD, PhD Chief, Geriatrics & Palliative Medicine Director, Specialized Oncology Care & Research in the Elderly (SOCARE) Clinic University of Chicago
public health crisis! Understanding frailty at population level!
 Frailty as an emerging public health crisis! Understanding frailty at population level! Dr Rónán O Caoimh, MB, MRCPI, MSc, PhD Senior Lecturer in Geriatric Medicine 08/03/2017 A brief history of frailty...
Frailty as an emerging public health crisis! Understanding frailty at population level! Dr Rónán O Caoimh, MB, MRCPI, MSc, PhD Senior Lecturer in Geriatric Medicine 08/03/2017 A brief history of frailty...
Outcomes in GEM models of geriatric care: How do we measure success? Disclosure. Objectives. Geriatric Grand Rounds
 Geriatric Grand Rounds Tuesday, October 7, 2008 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital Outcomes in GEM models of geriatric care: How do we measure success? In keeping with
Geriatric Grand Rounds Tuesday, October 7, 2008 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital Outcomes in GEM models of geriatric care: How do we measure success? In keeping with
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
INTEGRATED GERIATRIC AND PRIMARY CARE MANAGEMENT OF FRAIL OLDER ADULTS IN THE COMMUNITY
 INTEGRATED GERIATRIC AND PRIMARY CARE MANAGEMENT OF FRAIL OLDER ADULTS IN THE COMMUNITY LM Pérez (1), P Burbano (1), M Hernandez (1), N Gual (1,2), G Liesa (1), E Martin (3), L Tobella (3), MB Enfedaque
INTEGRATED GERIATRIC AND PRIMARY CARE MANAGEMENT OF FRAIL OLDER ADULTS IN THE COMMUNITY LM Pérez (1), P Burbano (1), M Hernandez (1), N Gual (1,2), G Liesa (1), E Martin (3), L Tobella (3), MB Enfedaque
Comprehensive geriatric assessment (CGA)
") Comprehensive geriatric assessment (CGA) Mieke Deschodt, RN, PhD Lucky you, getting older in Europe - Multiplier event IC Dien Oostduinkerke, 5 June 2018 @mieke_deschodt 2 Outline Comprehensive geriatric
Comprehensive geriatric assessment (CGA) Mieke Deschodt, RN, PhD Lucky you, getting older in Europe - Multiplier event IC Dien Oostduinkerke, 5 June 2018 @mieke_deschodt 2 Outline Comprehensive geriatric
Frailty: Challenges and Possible Solutions
 Frailty: Challenges and Possible Solutions EMA Workshop: Ensuring safe and effective medicines for an ageing population Niccolò Marchionni Professor of Geriatrics University of Florence, Italy 22-23 March
Frailty: Challenges and Possible Solutions EMA Workshop: Ensuring safe and effective medicines for an ageing population Niccolò Marchionni Professor of Geriatrics University of Florence, Italy 22-23 March
4/26/2012. Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012
 Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Pre- Cardiac intervention. Dr. Victor Sim 26 th Sept 2014
 Pre- Cardiac intervention Frailty assessment Dr. Victor Sim 26 th Sept 2014 Defining frailty Lacks consensus (Rockwood CMAJ 2005;173(5):489-95 Introduction) Some consider symptoms, signs, diseases and
Pre- Cardiac intervention Frailty assessment Dr. Victor Sim 26 th Sept 2014 Defining frailty Lacks consensus (Rockwood CMAJ 2005;173(5):489-95 Introduction) Some consider symptoms, signs, diseases and
Changing care systems for people with frailty. John Young
 Changing care systems for people with frailty John Young Geriatrician, Bradford Hospitals Trust, UK National Clinical Director for Integration & the Frail Elderly, NHS England (john.young@bthft.nhs.uk)
Changing care systems for people with frailty John Young Geriatrician, Bradford Hospitals Trust, UK National Clinical Director for Integration & the Frail Elderly, NHS England (john.young@bthft.nhs.uk)
Developing an Integrated System of Care for Frail Seniors in the WWLHIN
 Developing an Integrated System of Care for Frail Seniors in the WWLHIN George Heckman MD MSc FRCPC HTCP-1 RIA-UW Schlegel Research Chair in Geriatric Medicine Associate Professor, School of Public Health
Developing an Integrated System of Care for Frail Seniors in the WWLHIN George Heckman MD MSc FRCPC HTCP-1 RIA-UW Schlegel Research Chair in Geriatric Medicine Associate Professor, School of Public Health
Improving the Survivorship of Older Adults with Cancer Using Geriatric Assessment
 Improving the Survivorship of Older Adults with Cancer Using Geriatric Assessment Deborah Bacon, RN,BSN Geriatric Oncology Clinical Nurse Coordinator James P Wilmot Cancer Institute Outline Geriatric assessment
Improving the Survivorship of Older Adults with Cancer Using Geriatric Assessment Deborah Bacon, RN,BSN Geriatric Oncology Clinical Nurse Coordinator James P Wilmot Cancer Institute Outline Geriatric assessment
Evaluating Functional Status in Hospitalized Geriatric Patients. UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series
 Evaluating Functional Status in Hospitalized Geriatric Patients UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series Case 88 y.o. woman was admitted for a fall onto her hip. She is having trouble
Evaluating Functional Status in Hospitalized Geriatric Patients UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series Case 88 y.o. woman was admitted for a fall onto her hip. She is having trouble
Pre- Cardiac intervention. Dr. Victor Sim 16 th Oct 2014
 Pre- Cardiac intervention Frailty assessment Dr. Victor Sim 16 th Oct 2014 Topics to cover Defining frailty Pathophysiology of frailty Are current pre-cardiac surgery assessment tools adequate? Why do
Pre- Cardiac intervention Frailty assessment Dr. Victor Sim 16 th Oct 2014 Topics to cover Defining frailty Pathophysiology of frailty Are current pre-cardiac surgery assessment tools adequate? Why do
Services for Frailty or Services for Dementia? Dr Gill Turner Lymington New Forest
 Services for Frailty or Services for Dementia? Dr Gill Turner Lymington New Forest Hospital gill.turner1@nhs.net @turner_gill Do we have to decide? How Common are they? Frailty up to 25% of those over
Services for Frailty or Services for Dementia? Dr Gill Turner Lymington New Forest Hospital gill.turner1@nhs.net @turner_gill Do we have to decide? How Common are they? Frailty up to 25% of those over
Ageing Well. The challenge of our ageing population. Martin Vernon NCD Older People. Find Recognise Assess Intervene Long-term.
 Ageing Well The challenge of our ageing population Martin Vernon NCD Older People 7 th June 2017 1 Projected UK age structure Foresight, 2016 2 Ageing impacts 15 million live with a long term condition
Ageing Well The challenge of our ageing population Martin Vernon NCD Older People 7 th June 2017 1 Projected UK age structure Foresight, 2016 2 Ageing impacts 15 million live with a long term condition
Geriatric screening tools in older patients with cancer
 Geriatric screening tools in older patients with cancer Pr. Elena Paillaud Henri Mondor hospital, Créteil, France University Paris-Est Créteil CONFLICT OF INTEREST DISCLOSURE I have the following potential
Geriatric screening tools in older patients with cancer Pr. Elena Paillaud Henri Mondor hospital, Créteil, France University Paris-Est Créteil CONFLICT OF INTEREST DISCLOSURE I have the following potential
Frailty Assessment: Simplifying the Complex
 Frailty Assessment: Simplifying the Complex Natalie Sanders, DO Internal Medicine, Geriatrics Rocky Mountain Geriatrics Conference 2017 U N I V E R S I T Y O F U T A H H E A L T H, 2 0 1 7 OBJECTIVES Define
Frailty Assessment: Simplifying the Complex Natalie Sanders, DO Internal Medicine, Geriatrics Rocky Mountain Geriatrics Conference 2017 U N I V E R S I T Y O F U T A H H E A L T H, 2 0 1 7 OBJECTIVES Define
Understanding and Assessing for Frailty
 Understanding and Assessing for Frailty Dr Gloria Yu Clinical Head of Bexley Integrated Care Consultant Physician in Elderly, General and Stroke Medicine 8 July 2015 Learning objectives What is frailty?
Understanding and Assessing for Frailty Dr Gloria Yu Clinical Head of Bexley Integrated Care Consultant Physician in Elderly, General and Stroke Medicine 8 July 2015 Learning objectives What is frailty?
Geriatric Medicine I) OBJECTIVES
 OBJECTIVES") Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Comprehensive Assessment of the Frail Older Patient
 Comprehensive Assessment of the Frail Older Patient Executive Summary Comprehensive geriatric assessment (CGA) is a multidimensional and usually interdisciplinary diagnostic process designed to determine
Comprehensive Assessment of the Frail Older Patient Executive Summary Comprehensive geriatric assessment (CGA) is a multidimensional and usually interdisciplinary diagnostic process designed to determine
Management of the Frail Older Patients: What Are the Outcomes
 Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
Rehabilitation - Reducing costs and hospital stay. Dr Elizabeth Aitken Consultant Physician
 Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Interprofessional Care for Elders through 48/5
 Interprofessional Care for Elders through 48/5 Janet E. McElhaney, MD, FRCPC, FACP HSN Volunteer Association Chair in Geriatric Research Professor of Medicine, Northern Ontario School of Medicine Health
Interprofessional Care for Elders through 48/5 Janet E. McElhaney, MD, FRCPC, FACP HSN Volunteer Association Chair in Geriatric Research Professor of Medicine, Northern Ontario School of Medicine Health
What is Frailty? National Background and Local Pathways
 What is Frailty? National Background and Local Pathways Learning Outcomes At the end of the session you will be able to :Know where to go to look at key national resources on frailty. Define frailty. Screen
What is Frailty? National Background and Local Pathways Learning Outcomes At the end of the session you will be able to :Know where to go to look at key national resources on frailty. Define frailty. Screen
Frailty. Nicholas Butler MD, MBA Department of Family Medicine University of Iowa
 Frailty Nicholas Butler MD, MBA Department of Family Medicine University of Iowa Doris 84 yo female who comes into your clinic with her daughter. She complains of feeling increasingly fatigued and just
Frailty Nicholas Butler MD, MBA Department of Family Medicine University of Iowa Doris 84 yo female who comes into your clinic with her daughter. She complains of feeling increasingly fatigued and just
Hospitalization- Associated Disability
 Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
ACEing Age Old Issues in the Care of Older Canadians
 ACEing Age Old Issues in the Care of Older Canadians Dr. Samir K. Sinha MD, DPhil, FRCPC Peter and Shelagh Godsoe Chair in Geriatrics and Director of Geriatrics Sinai Health System and the University Health
ACEing Age Old Issues in the Care of Older Canadians Dr. Samir K. Sinha MD, DPhil, FRCPC Peter and Shelagh Godsoe Chair in Geriatrics and Director of Geriatrics Sinai Health System and the University Health
Breast cancer in the elderly - is there a role for the geriatrician?
 Breast cancer in the elderly - is there a role for the geriatrician? Workshop in Breast Cancer Surgery Aarhus 18 May 2016 Lone Winther Lietzen MD, PhD Department of Geriatrics, Geriatricians? Internal
Breast cancer in the elderly - is there a role for the geriatrician? Workshop in Breast Cancer Surgery Aarhus 18 May 2016 Lone Winther Lietzen MD, PhD Department of Geriatrics, Geriatricians? Internal
Integration; Frailty; and efi
 Integration; Frailty; and efi John Young Geriatrician, Bradford Hospitals Trust, UK National Clinical Director for Integration & the Frail Elderly, NHS England (john.young@bthft.nhs.uk) NHS England Older
Integration; Frailty; and efi John Young Geriatrician, Bradford Hospitals Trust, UK National Clinical Director for Integration & the Frail Elderly, NHS England (john.young@bthft.nhs.uk) NHS England Older
Living well with frailty. JOHN YOUNG National Clinical Director for the Frail Elderly & Integration, NHS England
 Living well with frailty JOHN YOUNG National Clinical Director for the Frail Elderly & Integration, NHS England A LTC rarely travels alone Kent Whole Population Dataset: Interim Report 2014 The burden
Living well with frailty JOHN YOUNG National Clinical Director for the Frail Elderly & Integration, NHS England A LTC rarely travels alone Kent Whole Population Dataset: Interim Report 2014 The burden
Quality of Acute Care for Older Persons with Dementia
 Quality of Acute Care for Older Persons with Dementia A Hospital-Based Pilot Study Chien-Liang Liu Center for Geriatrics and Gerontology, Taipei Veterans General Hospital, Taiwan 2013/04/20 Outline Background
Quality of Acute Care for Older Persons with Dementia A Hospital-Based Pilot Study Chien-Liang Liu Center for Geriatrics and Gerontology, Taipei Veterans General Hospital, Taiwan 2013/04/20 Outline Background
Biological theory for the construct of intrinsic capacity to be used in clinical settings Matteo Cesari, MD, PhD
 Biological theory for the construct of intrinsic capacity to be used in clinical settings Matteo Cesari, MD, PhD World Health Organization Geneva (Switzerland) December 1, 2016 World Health Organization.
Biological theory for the construct of intrinsic capacity to be used in clinical settings Matteo Cesari, MD, PhD World Health Organization Geneva (Switzerland) December 1, 2016 World Health Organization.
Healthcare, hospitals and the challenges of an ageing population
 Healthcare, hospitals and the challenges of an ageing population Prof David Oliver Vice President, RCP, London Past President, British Geriatrics Society Senior Visiting Fellow, King s Fund Consultant
Healthcare, hospitals and the challenges of an ageing population Prof David Oliver Vice President, RCP, London Past President, British Geriatrics Society Senior Visiting Fellow, King s Fund Consultant
Identifying and Understanding Frailty
 Identifying and Understanding Frailty Dr Dawn Moody Associate National Clinical Director for Older People and Integrated Person-Centred Care, NHS England GPSI Care of Older People, Derbyshire The North
Identifying and Understanding Frailty Dr Dawn Moody Associate National Clinical Director for Older People and Integrated Person-Centred Care, NHS England GPSI Care of Older People, Derbyshire The North
Global ACE Forum 2017
 1 It s broke! Fix it! Challenging the status quo of geriatrics in acute care George A Heckman MD MSc FRCPC HTCP-1 Schlegel Research Chair in Geriatric Medicine Associate Professor, University of Waterloo
1 It s broke! Fix it! Challenging the status quo of geriatrics in acute care George A Heckman MD MSc FRCPC HTCP-1 Schlegel Research Chair in Geriatric Medicine Associate Professor, University of Waterloo
Improving Healthcare Utilization in Injured Older Adults
 Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Frailty and Aging Managing from a Community Perspective. Dr. John Puxty
 Frailty and Aging Managing from a Community Perspective Dr. John Puxty puxtyj@providencecare.ca Presenter Disclosure No commercial support received or potential conflicts Learning Objectives The participant
Frailty and Aging Managing from a Community Perspective Dr. John Puxty puxtyj@providencecare.ca Presenter Disclosure No commercial support received or potential conflicts Learning Objectives The participant
FRAILTY SYNDROME. dr. Rose Dinda Martini, Sp.PD, K-Ger
 FRAILTY SYNDROME dr. Rose Dinda Martini, Sp.PD, K-Ger Geriatric Division, Internal Medicine Department M. Djamil Hospital Padang Faculty of Medicine, Andalas University, 2018 Medical syndrome Multiple
FRAILTY SYNDROME dr. Rose Dinda Martini, Sp.PD, K-Ger Geriatric Division, Internal Medicine Department M. Djamil Hospital Padang Faculty of Medicine, Andalas University, 2018 Medical syndrome Multiple
Update on Falls Prevention Research
 Update on Falls Prevention Research Jasmine Menant NSW Falls Prevention Network Rural Forum 26 th March 2015 Acknowledgments: Prof Stephen Lord Recent falls risk factor studies Vascular disease 38.6% of
Update on Falls Prevention Research Jasmine Menant NSW Falls Prevention Network Rural Forum 26 th March 2015 Acknowledgments: Prof Stephen Lord Recent falls risk factor studies Vascular disease 38.6% of
People living with frailty: View from NHS England. John Young
 People living with frailty: View from NHS England John Young Geriatrician, Bradford Hospitals Trust, UK National Clinical Director for Integration & the Frail Elderly, NHS England (john.young@bthft.nhs.uk)
People living with frailty: View from NHS England John Young Geriatrician, Bradford Hospitals Trust, UK National Clinical Director for Integration & the Frail Elderly, NHS England (john.young@bthft.nhs.uk)
Assess & Restore February 2015
 Assess & Restore February 2015 Objective of Presentation Provide an update on the Rehabilitative Care Alliance s (RCA) priority process and standardized tools for delivering rehabilitative care to frail
Assess & Restore February 2015 Objective of Presentation Provide an update on the Rehabilitative Care Alliance s (RCA) priority process and standardized tools for delivering rehabilitative care to frail
Frailty in Older Adults
 Frailty in Older Adults John Puxty puxtyj@providencecare Geriatrics 20/20: Bringing Current Issues into Perspective Session Overview Definition of Frailty Strategies for identifying frail older adults
Frailty in Older Adults John Puxty puxtyj@providencecare Geriatrics 20/20: Bringing Current Issues into Perspective Session Overview Definition of Frailty Strategies for identifying frail older adults
Care & Support Planning/Advanced Care Planning for people living with frailty John Young
 Care & Support Planning/Advanced Care Planning for people living with frailty John Young Geriatrician, Bradford Hospitals Trust National Clinical Director for Integration & Frail Elderly, NHS England (john.young@bthft.nhs.uk)
Care & Support Planning/Advanced Care Planning for people living with frailty John Young Geriatrician, Bradford Hospitals Trust National Clinical Director for Integration & Frail Elderly, NHS England (john.young@bthft.nhs.uk)
Edith Haage, PT, GCS NewCourtland Senior Services 10/26/2016. NEWCOURTLAND.org
 Edith Haage, PT, GCS NewCourtland Senior Services 10/26/2016 NEWCOURTLAND.org 1-888-530-4913 Edith Haage has disclosed she has no financial relationships. 1. Define frailty in geriatric clientele, including
Edith Haage, PT, GCS NewCourtland Senior Services 10/26/2016 NEWCOURTLAND.org 1-888-530-4913 Edith Haage has disclosed she has no financial relationships. 1. Define frailty in geriatric clientele, including
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Frailty: what s it all about?
 Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
The Community Assessment of Risk and Treatment Strategies (CARTS) Project. Professor D. William Molloy COLLAGE University College Cork, Ireland.
 Project. Professor D. William Molloy COLLAGE University College Cork, Ireland.") The Community Assessment of Risk and Treatment Strategies (CARTS) Project Professor D. William Molloy COLLAGE University College Cork, Ireland. Centre for Gerontology and Rehabilitation A time of limited
The Community Assessment of Risk and Treatment Strategies (CARTS) Project Professor D. William Molloy COLLAGE University College Cork, Ireland. Centre for Gerontology and Rehabilitation A time of limited
Update on Falls Prevention Research
 Update on Falls Prevention Research Dr Jasmine Menant NSW Falls Prevention Network Rural Forum 17 th October 2014 Acknowledgement: Prof Stephen Lord Recent falls risk factor studies Vascular disease 38.6%
Update on Falls Prevention Research Dr Jasmine Menant NSW Falls Prevention Network Rural Forum 17 th October 2014 Acknowledgement: Prof Stephen Lord Recent falls risk factor studies Vascular disease 38.6%
Multifactorial risk assessments and evidence-based interventions to address falls in primary care. Objectives. Importance
 Multifactorial risk assessments and evidence-based interventions to address falls in primary care Sarah Ross, DO, MS Assistant Professor Internal Medicine, Geriatrics Nicoleta Bugnariu, PT, PhD Associate
Multifactorial risk assessments and evidence-based interventions to address falls in primary care Sarah Ross, DO, MS Assistant Professor Internal Medicine, Geriatrics Nicoleta Bugnariu, PT, PhD Associate
Economics of Frailty. Eamon O Shea
 Economics of Frailty Eamon O Shea Patient Complexity Framework Demography Mutimorbidity Mental health Frailty Social capital Resource utilisation WHO and Frailty Progressive age-related decline in physiological
Economics of Frailty Eamon O Shea Patient Complexity Framework Demography Mutimorbidity Mental health Frailty Social capital Resource utilisation WHO and Frailty Progressive age-related decline in physiological
Primary Screening and Ongoing Assessment, Diagnosis and Interventions
 Primary Screening and Ongoing Assessment, Diagnosis and Interventions Vicky Scott, RN, PhD Clinical Professor, School of Population and Public Health Faculty of Medicine, University of British Columbia
Primary Screening and Ongoing Assessment, Diagnosis and Interventions Vicky Scott, RN, PhD Clinical Professor, School of Population and Public Health Faculty of Medicine, University of British Columbia
Acute care for older people with frailty
 Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester Worldview that will colour this talk Demography
Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester Worldview that will colour this talk Demography
Falls and Mobility. Katherine Berg, PhD, PT and Arielle Berger, MD. Presented by: Ontario s Geriatric Steering Committee
 Falls and Mobility Katherine Berg, PhD, PT and Arielle Berger, MD Key Learnings Arielle Berger, MD Key Learnings Learn approaches to falls assessment Understand inter-relationship between promoting safe
Falls and Mobility Katherine Berg, PhD, PT and Arielle Berger, MD Key Learnings Arielle Berger, MD Key Learnings Learn approaches to falls assessment Understand inter-relationship between promoting safe
Quality Care for the Hospitalized Older Adult
 Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
7/12/2016. Presenter Disclosure Information. The Other Half of the Fracture Equation: Fall Prevention and Management. Presentation Outline
 Presenter Disclosure Information Edgar Pierluissi Division of Geriatrics Edgar Pierluissi, MD Acute Care for Elders Unit Zuckerberg San Francisco General Hospital July 21, 2016 OSTEOPOROSIS NEW INSIGHTS
Presenter Disclosure Information Edgar Pierluissi Division of Geriatrics Edgar Pierluissi, MD Acute Care for Elders Unit Zuckerberg San Francisco General Hospital July 21, 2016 OSTEOPOROSIS NEW INSIGHTS
What is frailty and why it is important
 What is frailty and why it is important Tony Moran North West Knowledge and Intelligence Team Cancer Outcomes Conference 2013 Contents Definitions of frail and frailty Prevalence and measurement Use in
What is frailty and why it is important Tony Moran North West Knowledge and Intelligence Team Cancer Outcomes Conference 2013 Contents Definitions of frail and frailty Prevalence and measurement Use in
Comprehensive Geriatric Assessment: what s it all about? Deborah Mayne, City Hospitals Sunderland Clinical Lead for Frailty
 Comprehensive Geriatric Assessment: what s it all about? Deborah Mayne, City Hospitals Sunderland Clinical Lead for Frailty What is Comprehensive Geriatric Assessment (CGA)? Gold standard for management
Comprehensive Geriatric Assessment: what s it all about? Deborah Mayne, City Hospitals Sunderland Clinical Lead for Frailty What is Comprehensive Geriatric Assessment (CGA)? Gold standard for management
Welcome to the Routine frailty identification in the GP contract webinar presented by Dawn Moody
 Welcome to the Routine frailty identification in the GP contract webinar presented by Dawn Moody The presentation will begin at 12.00pm. Attendees will be muted during the presentation to avoid interference.
Welcome to the Routine frailty identification in the GP contract webinar presented by Dawn Moody The presentation will begin at 12.00pm. Attendees will be muted during the presentation to avoid interference.
Implementing Best Practice Rehabilitative Care for Patients with Hip Fracture & Total Joint Replacement
 Implementing Best Practice Rehabilitative Care for Patients with Hip Fracture & Total Joint Replacement A Toolkit for Implementing the RCA s TJR and Hip Fracture Best Practice Frameworks January 2018 Purpose
Implementing Best Practice Rehabilitative Care for Patients with Hip Fracture & Total Joint Replacement A Toolkit for Implementing the RCA s TJR and Hip Fracture Best Practice Frameworks January 2018 Purpose
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
ASSESS & RESTORE SHARED PROVINCIAL INDICATORS AND TECHNICAL SPECIFICATIONS
 Shared Provincial s & ASSESS & RESTORE SHARED PROVINCIAL INDICATORS AND TECHNICAL SPECIFICATIONS January 2018 0 P a g e J a n u a r y 2 0 1 8 Shared Provincial s & BACKGROUND To evaluate the impact of
Shared Provincial s & ASSESS & RESTORE SHARED PROVINCIAL INDICATORS AND TECHNICAL SPECIFICATIONS January 2018 0 P a g e J a n u a r y 2 0 1 8 Shared Provincial s & BACKGROUND To evaluate the impact of
Care of older people in surgery (COPS)
") Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Lorraine Montoya, BSN, MAdEd APN / Coordinator TAVI Program. 7 April
 Using Frailty Measurement to Assist With Patient Assessment and Discharge Planning in Patients Undergoing Transcatheter Aortic Valve Implant Results of a Pilot Project Lorraine Montoya, BSN, MAdEd APN
Using Frailty Measurement to Assist With Patient Assessment and Discharge Planning in Patients Undergoing Transcatheter Aortic Valve Implant Results of a Pilot Project Lorraine Montoya, BSN, MAdEd APN
Medico-Social Impact of Fragility Fracture 11/2/2014. Dr David Dai Consultant Geriatrician Prince of Wales Hospital 24 th January, 2014
 Medico-Social Impact of Fragility Fracture Dr David Dai Consultant Geriatrician Prince of Wales Hospital 24 th January, 2014 2014 Policy Agenda As Hong Kong moves steadily to an ageing society (with the
Medico-Social Impact of Fragility Fracture Dr David Dai Consultant Geriatrician Prince of Wales Hospital 24 th January, 2014 2014 Policy Agenda As Hong Kong moves steadily to an ageing society (with the
The SOCARE Model of Cancer Care for Older Adults: Building Infrastructure and Policies for Truly Personalized Cancer Care for an Aging Society
 The SOCARE Model of Cancer Care for Older Adults: Building Infrastructure and Policies for Truly Personalized Cancer Care for an Aging Society William Dale, MD, PhD Michael M Davis Lecture Series University
The SOCARE Model of Cancer Care for Older Adults: Building Infrastructure and Policies for Truly Personalized Cancer Care for an Aging Society William Dale, MD, PhD Michael M Davis Lecture Series University
March 13, :00 11:00 a.m. CST. Jane F. Potter, MD
 University of Nebraska Medical Center CAPTURE Collaboration and Proactive Teamwork Used to Reduce Falls March 13, 2012 10:00 11:00 a.m. CST Jane F. Potter, MD Harris Professor of Geriatric Medicine Chief,
University of Nebraska Medical Center CAPTURE Collaboration and Proactive Teamwork Used to Reduce Falls March 13, 2012 10:00 11:00 a.m. CST Jane F. Potter, MD Harris Professor of Geriatric Medicine Chief,
Dementia and Primary Care. A Structured Team Approach UNE/MGEC Conference June 2014
 Dementia and Primary Care A Structured Team Approach UNE/MGEC Conference June 2014 First Proviso I have no actual or potential conflict of interest in relation to this program or presentation. Second Proviso
Dementia and Primary Care A Structured Team Approach UNE/MGEC Conference June 2014 First Proviso I have no actual or potential conflict of interest in relation to this program or presentation. Second Proviso
Frailty: from Academic Definition to Clinical Applicability
 Frailty: from Academic Definition to Clinical Applicability Associate Professor Ruth E. Hubbard October 26 th 2018 Objectives 1. Describe the development of frailty as a concept 2. Provide an overview
Frailty: from Academic Definition to Clinical Applicability Associate Professor Ruth E. Hubbard October 26 th 2018 Objectives 1. Describe the development of frailty as a concept 2. Provide an overview
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
after acute care (inc. ED)?
?") How to prevent early & unplanned hospital admission after acute care (inc. ED)? Luis Mieiro @luismieiro Consultant Geriatrician Forest Assessment Unit - Older People s Services Whipps Cross University
How to prevent early & unplanned hospital admission after acute care (inc. ED)? Luis Mieiro @luismieiro Consultant Geriatrician Forest Assessment Unit - Older People s Services Whipps Cross University
NATIONAL REHABILITATION HOSPITAL (NRH) THE SPINAL CORD SYSTEM OF CARE (SCSC) PROGRAMME INPATIENT SCOPE OF SERVICE
 THE SPINAL CORD SYSTEM OF CARE (SCSC) PROGRAMME INPATIENT SCOPE OF SERVICE") NATIONAL REHABILITATION HOSPITAL (NRH) THE SPINAL CORD SYSTEM OF CARE (SCSC) PROGRAMME INPATIENT SCOPE OF SERVICE NATIONAL REHABILITATION HOSPITAL SCOPE OF SERVICE FOR THE SPINAL CORD SYSTEM OF CARE PROGRAMME
NATIONAL REHABILITATION HOSPITAL (NRH) THE SPINAL CORD SYSTEM OF CARE (SCSC) PROGRAMME INPATIENT SCOPE OF SERVICE NATIONAL REHABILITATION HOSPITAL SCOPE OF SERVICE FOR THE SPINAL CORD SYSTEM OF CARE PROGRAMME
The Role of Physiatry in the Care of Adults and Children with Hydrocephalus
 The Role of Physiatry in the Care of Adults and Children with Hydrocephalus Scott E. Brown, MD Chairman Department of Physical Medicine and Rehabilitation Sinai Hospital of Baltimore Who Are We? PHYSICAL
The Role of Physiatry in the Care of Adults and Children with Hydrocephalus Scott E. Brown, MD Chairman Department of Physical Medicine and Rehabilitation Sinai Hospital of Baltimore Who Are We? PHYSICAL
EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY
 EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY Geriatrics, General practice, Emergency medicine, Interface medicine SUMMARY An integrated, community emergency service specifically designed for
EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY Geriatrics, General practice, Emergency medicine, Interface medicine SUMMARY An integrated, community emergency service specifically designed for
The COLLaboration on AGEing (COLLAGE)
") The COLLaboration on AGEing (COLLAGE) Professor D. William Molloy University College Cork, Ireland. The Lessons from Europe Seminar 23-09-15 Overview Exemplars within COLLAGE: 1. What is COLLAGE? 2. The
The COLLaboration on AGEing (COLLAGE) Professor D. William Molloy University College Cork, Ireland. The Lessons from Europe Seminar 23-09-15 Overview Exemplars within COLLAGE: 1. What is COLLAGE? 2. The
Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire
 Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire Introduction This document introduces South Gloucestershire Clinical Commissioning
Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire Introduction This document introduces South Gloucestershire Clinical Commissioning
Department of Geriatrics. Annual Report Larry Lawhorne, M.D. Professor and Chair
 Department of Geriatrics Annual Report 2016 Larry Lawhorne, M.D. Professor and Chair For the period including January 1, 2016 December 31, 2016 1Statement from the Chair The Department of Geriatrics was
Department of Geriatrics Annual Report 2016 Larry Lawhorne, M.D. Professor and Chair For the period including January 1, 2016 December 31, 2016 1Statement from the Chair The Department of Geriatrics was
Polymedication in nursing home. Graziano Onder Centro Medicina dell Invecchiamento Università Cattolica del Sacro Cuore Rome - Italy
 Polymedication in nursing home Graziano Onder Centro Medicina dell Invecchiamento Università Cattolica del Sacro Cuore Rome - Italy Services and Health for Elderly in Long TERm care (SHELTER) 4156 residents
Polymedication in nursing home Graziano Onder Centro Medicina dell Invecchiamento Università Cattolica del Sacro Cuore Rome - Italy Services and Health for Elderly in Long TERm care (SHELTER) 4156 residents
Ageing as a game-changer for acute and general medicine and wider systems in which we practice
 Ageing as a game-changer for acute and general medicine and wider systems in which we practice Acute and General Medicine Conference October 23 2017 David Oliver RCP London Clinical Vice President To Cover
Ageing as a game-changer for acute and general medicine and wider systems in which we practice Acute and General Medicine Conference October 23 2017 David Oliver RCP London Clinical Vice President To Cover
Talking the same language for effective care of older people
 Introducing the interrai Home Care Talking the same language for effective care of older people interrai has developed an entire range of instruments and screeners to support assessment in a wide array
Introducing the interrai Home Care Talking the same language for effective care of older people interrai has developed an entire range of instruments and screeners to support assessment in a wide array
Table to Demonstrate a method of working through Triggered CAPs.
 CAP Problem Goals Triggers Guidelines Physical Activities increase hours of exercises Reports less than 2 hours Personal choice Promotion and physical activity activity in last 3 days Instrumental Activities
CAP Problem Goals Triggers Guidelines Physical Activities increase hours of exercises Reports less than 2 hours Personal choice Promotion and physical activity activity in last 3 days Instrumental Activities
GRACE Team Care A New Model of Integrated Medical and Social Care for Older Persons
 GRACE Team Care A New Model of Integrated Medical and Social Care for Older Persons Steven R. Counsell, MD Mary Elizabeth Mitchell Professor and Director, Scientist, IU Center for Aging Research E-mail:
GRACE Team Care A New Model of Integrated Medical and Social Care for Older Persons Steven R. Counsell, MD Mary Elizabeth Mitchell Professor and Director, Scientist, IU Center for Aging Research E-mail:
Community Actions & Resources Empowering Seniors (CARES)
") Community Actions & Resources Empowering Seniors (CARES) Proactively Preventing Frailty in At Risk Seniors June 13, 2017 @cfhi_fcass Welcome With us today: Christine Quinn Annette Garm Dr. Grace Park Dr.
Community Actions & Resources Empowering Seniors (CARES) Proactively Preventing Frailty in At Risk Seniors June 13, 2017 @cfhi_fcass Welcome With us today: Christine Quinn Annette Garm Dr. Grace Park Dr.
Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial
 Dr Kyra Neubauer Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial assessment Understand what are potential
Dr Kyra Neubauer Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial assessment Understand what are potential
Update on Frailty. Stephanie Studenski Longitudinal Studies Section Intramural Research Program National Institute on Aging
 Update on Frailty Stephanie Studenski Longitudinal Studies Section Intramural Research Program National Institute on Aging Agenda What is frailty? Overlap with sarcopenia, slow walking and multimorbidity
Update on Frailty Stephanie Studenski Longitudinal Studies Section Intramural Research Program National Institute on Aging Agenda What is frailty? Overlap with sarcopenia, slow walking and multimorbidity
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Thank You to Our Sponsors: Evaluations & CE Credits. Featured Speakers. Conflict of Interest & Disclosure Statements 10/18/2016
 Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
GERIATRIC DAY HOSPITAL
 GERIATRIC DAY HOSPITAL MISSION To provide interdisciplinary assessment, consultation and rehabilitation services to community dwelling older adults and their families. To optimize their health and functional
GERIATRIC DAY HOSPITAL MISSION To provide interdisciplinary assessment, consultation and rehabilitation services to community dwelling older adults and their families. To optimize their health and functional
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
The Long-term Prognosis of Delirium
 The Long-term Prognosis of Jane McCusker, MD, DrPH, Professor, Epidemiology and Biostatistics, McGill University; Head, Clinical Epidemiology and Community Studies, St. Mary s Hospital, Montreal, QC. Nine
The Long-term Prognosis of Jane McCusker, MD, DrPH, Professor, Epidemiology and Biostatistics, McGill University; Head, Clinical Epidemiology and Community Studies, St. Mary s Hospital, Montreal, QC. Nine
MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab
 MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab In response to a changing rehab landscape in which rehabilitation is offered in many different settings with variations
MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab In response to a changing rehab landscape in which rehabilitation is offered in many different settings with variations
Frailty in Older Adults. Farshad Sharifi, MD, MPH Elderly Health Research Center
 Frailty in Older Adults Farshad Sharifi, MD, MPH Elderly Health Research Center 1 Outlines Definition of frailty Significance of frailty Conceptual Frailty Models Pathogenesis of frailty Management of
Frailty in Older Adults Farshad Sharifi, MD, MPH Elderly Health Research Center 1 Outlines Definition of frailty Significance of frailty Conceptual Frailty Models Pathogenesis of frailty Management of
WHAT IS THE ROLE OF EXERCISE IN PREVENTING FALLS AND FRACTURES IN LONG-TERM CARE?
 WHAT IS THE ROLE OF EXERCISE IN PREVENTING FALLS AND FRACTURES IN LONG-TERM CARE? CAITLIN MCARTHUR, PHD, MScPT, BSc(KIN) POST-DOCTORAL FELLOW GERAS CENTRE FOR AGING RESEARCH MCMASTER UNIVERSITY ABOUT ME...
WHAT IS THE ROLE OF EXERCISE IN PREVENTING FALLS AND FRACTURES IN LONG-TERM CARE? CAITLIN MCARTHUR, PHD, MScPT, BSc(KIN) POST-DOCTORAL FELLOW GERAS CENTRE FOR AGING RESEARCH MCMASTER UNIVERSITY ABOUT ME...
End of Life Care in Dementia. Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals
 End of Life Care in Dementia Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals Rosie.Lockwood@sth.nhs.uk Agenda Some facts and figures What are the challenges? What is good care? How
End of Life Care in Dementia Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals Rosie.Lockwood@sth.nhs.uk Agenda Some facts and figures What are the challenges? What is good care? How
Significance of Walking Speed. Maggie Benson Virginia Commonwealth University Department of Physical Therapy
 Significance of Walking Speed Maggie Benson Virginia Commonwealth University Department of Physical Therapy The 6 th Vital Sign Walking speed is considered the 6 th vital sign A valid and reliable measure
Significance of Walking Speed Maggie Benson Virginia Commonwealth University Department of Physical Therapy The 6 th Vital Sign Walking speed is considered the 6 th vital sign A valid and reliable measure
FALL PREVENTION AND OLDER ADULTS BURDEN. February 2, 2016
 February 2, 2016 FALL PREVENTION AND OLDER ADULTS Each year in Winnipeg, one in three adults over 65 years of age will experience a fall. 1 Approximately one third of people 65 years of age and older and
February 2, 2016 FALL PREVENTION AND OLDER ADULTS Each year in Winnipeg, one in three adults over 65 years of age will experience a fall. 1 Approximately one third of people 65 years of age and older and