Antipsychotic Medications in the Treatment of Dementia with Behavior Disturbance
|
|
|
- Avice Shelton
- 6 years ago
- Views:
Transcription
1 Antipsychotic Medications in the Treatment of Dementia with Behavior Disturbance American Association for Geriatric Psychiatry Los Angeles, CA March 2013
2 Maureen C. Nash, MD, MS, FAPA Medical Director, Tuality Center for Geriatric Psychiatry CoChair, Clinical Practice Committee, American Association for Geriatric Psychiatry Affiliate Assistant Professor of Psychiatry, Oregon Health and Sciences University Diplomate, American Board of Internal Medicine Diplomate, American Board of Psychiatry and Neurology
3 Disclosures Off label use of medications will be discussed
4 But, I thought dementia was a cognitive disorder?
5 Dr Alzheimer's Case Auguste D. 1901, 51 year old female at the Frankfurt Asylum Hx of progressive cognitive impairments, and Reason for admission: Hallucinations, delusions and psychosocial incompetence Example of one of Dr. Alzheimer s notes: During physical examination she cooperates and is not anxious. Auditory Hallucinations: Just now a child called, is he there? Delusions that she was going to be raped Maurer K et al: Lancet 349: , 1997

6 First Case of Alzheimers Auguste D. She died in 1906 Case and autopsy findings presented at 37 th Conference of Southwest German Psychiatrists Tubingen
7 What is Behavior Disturbance in Dementia?

8 Neuropsychiatric Inventory (NPI) Symptom Anytime during illness Shown in last month Delusions 50% 35% Hallucinations Agitation/Aggression Depression Anxiety Apathy Craig D et al: Am J Geriatr Psych 13:460-8, 2005
9 Neuropsychiatric Inventory (NPI) Symptom Anytime during illness Shown in last month Euphoria Irritability Aberrant Motor Behaviors Sleep Disturbance Appetite Craig D et al: Am J Geriatr Psych 13:460-8, 2005
10 Why this topic? Dementia is common and the number of people suffering from it is increasing -AND- Behavior disturbance that often accompanies dementia is very common -BUT- Behavior disturbance that often accompanies dementia is TREATABLE! -BUT- All treatments have risks and benefits -AND- Some pharmacological treatments are under attack
11 OBRA 1987 Formalized nursing home reform Legislation based on IOM report Inadequate care in NH Inadequate assessment, poor QOL, violations of basic rights, failure to recognize and treat reversible causes of physical and functional decline Application of standards still problematic
12 CMS announces partnership to improve dementia care in nursing homes Hand in hand training series with an emphasis on non-pharmacological interventions Person centered care Prevention of abuse High quality care Stated goal of reducing antipsychotic use by 15% Publish every Nursing Home s antipsychotic use
13 Staff (and family members) are in danger Aggression towards staff 138 nursing assistants at 6 Nursing Homes 59% assaulted once per week 16% assaulted daily Gates DM, Fitzwater E, Meyer U. Violence against caregivers in nursing homes. Expected, tolerated, and accepted. J Gerontol Nurs. 25: 12-22, 1999
14 Quotes from Family: I don t want my Mom s last days filled with fear and terror because of the delusion that someone is trying to hurt her or steal her money. I don t want Mom to hurt anyone. If my Dad knew what he was doing, he would be so embarrassed. I m afraid Dad is going to kill my Mom.
15 Select look at severe NH aggression May yo M kills 84yo M in MI Mar yo M kills 80yo M in IL Feb yo M kills 70yo M in PA (2 staff injured) Dec yo F kills 100 yo F in MA
16 Therapeutic Approach to Dementia Care adapted from I-ADAPT Identify/ Assess Causes of Behavior Unmet Physical Needs Unmet Psychological Needs Environmental Causes Psychiatric Symptoms Key Stage for Assessments of Cognitive and Functional Abilities Behavioral Rating Scales Select Interventions based on assessments Apply Interventions Caregiving Approaches Adapt Environment Evidence Based Interventions (sensory, activity, communication) Staff Training Monitor Outcomes Behavior Rating Scales Continued staff training Individualize interventions based on preference and positive outcomes
17 Psychiatric Symptoms often amenable to treatment with medications Sometimes depression Paranoia and delusions Hallucinations Sometimes anxiety Pain
18 Symptoms not usually amenable to medications Wandering Calling out (not related to pain) Repetitive questions Anxiety related to having memory loss Psychomotor agitation?agitation
19 Informed Consent for all treatments including pharmacological Discussion and documentation of discussion with patient, family or surrogate decision-maker of: Risks Benefits Alternatives (including the risks of no treatment) Common risks of no treatment for moderate or severe psychosis and aggression: patient or peers injured, staff injured, loss of place to live, social isolation by being avoided by peers and staff, increased neuropsychiatric symptoms, decreased quality of life, increased institutionalization
20 Comparison of Risk of Hospitalization and Mortality in 4 medicine classes 10,900 Nursing Home patients in Canada Risks of conventional AP, antidepressants & bzd vs risks of Atypical AP (risk of 1) Risk of death: Conventional AP and antidepressants 1.47 Risk of femur fracture: Conventional 1.61, Antidepressant 1.29 Users of BZD Risk of death 1.8, Heart Fail 1.54, Pneumonia 1.85 Huybrechts K F et al. CMAJ 2011;183:E411-E419
21 Kaplan Meier estimate of the probability of no events over time Huybrechts K F et al. CMAJ 2011;183:E411-E by Canadian Medical Association
22

23 Huybrechts K F et al. Comparison of risks in 4 classes of medications
24 Are antidepressants safe in older adults? Cohort (observational) study GP practices in UK age 65 to ,746 patients in 570 practices No mention of dementia status Risks that were monitored Falls, hyponatremia, mortality, attempted suicide/self harm, stroke/transient ischaemic attack, fracture, and epilepsy/seizures Coupland C, et al. Antidepressant use and risk of adverse outcomes in older people: population based cohort study. BMJ 2011;343:d4551
25 Highest adjusted hazard ratios compared to non-antidepressant use SSRI falls 1.66 hyponatraemia 1.52 Other antidepressants (like mirtazapine, trazodone, venlafaxine) all cause mortality 1.66 attempted suicide/self harm 5.16 stroke/transient ischaemic attack 1.37 fracture (1.64), and epilepsy/seizures (2.24) Tricyclic antidepressants did not have the highest hazard ratio for any of the outcomes. Absolute risks over 1 year for all cause mortality were 7.04% for patients while not taking antidepressants, 8.12% for TCA, 10.61% for SSRI 11.43% for other antidepressants Coupland C, et al. Antidepressant use and risk of adverse outcomes in older people: population based cohort study. BMJ 2011;343:d4551
26 Antipsychotic Medications: Treating Psychosis - delusions and hallucinations the newer anti-psychotics: RIS, OLZ, QTP, ZPS and ARP Be careful of dosage, however. For example, in demented patients using RIS for psychosis and agitation, 1 mg/day was associated with a decreased risk of falls, but 2 mg/day increased the risk of falls RIS and Haloperidol were compared in dementia patients with behavioral disturbances, risperidone worked better with fewer side effects Very few studies have used ZPS or ARP Katz IR et al, Am J Geriatr Psychiatry 12:499-08, 2004 Suh G, et al, Am J Geriatr Psychiatry 12:509-16, 2004
27 Pharmacological strategies Antipsychotics for agitation Despite evidence that these drugs can help; other studies cast doubt on the effectiveness for these drugs as anti-agitation drugs in dementia. (64 sites), prospective study of 500 patients with Dementia patients who had psychosis and associated behaviors RIS, OLZ and Placebo were compared Results: placebo and drug treatment groups improved Reasons: inadequate dose (doubtful) temporary phenomena (possible) patient selection (possible) agitation is not a single symptom (probable) Deberdt WG et al: Am J Geriatr Psychiatry 13:722-30, 2005
28 De Deyn et al compared Risperidone to haloperidol to placebo in 1999 for treating behavioral symptoms in dementia Haloperidol Dose 0.5-4mg/day Mean dose 1.2 Risperidone Dose 0.5-4mg/day Mean Dose 1.1 Haloperidol more motor side effects Risperidone more effective at controlling aggression
29 Antipsychotics And more. Risperidone vs. placebo 473 patients, randomized mg/day vs placebo Used BEHAVE-AD and CGI-C Both groups improved! The more severe the dementia, the more likely someone was to benefit from risperidone Mintzer J et al. AJGP 14(3):280-91, 2006
30 Antipsychotics in treatment of behavior disturbance in dementia Haldol is effective but there is a high level of acute and chronic side effects Trouble swallowing Stooped posture Trouble ambulating Tremor/stiffness Falls Lonergan et al Cochrane Database Syst Rev Dolder et al Biol Psychiatry. 53: , 2003
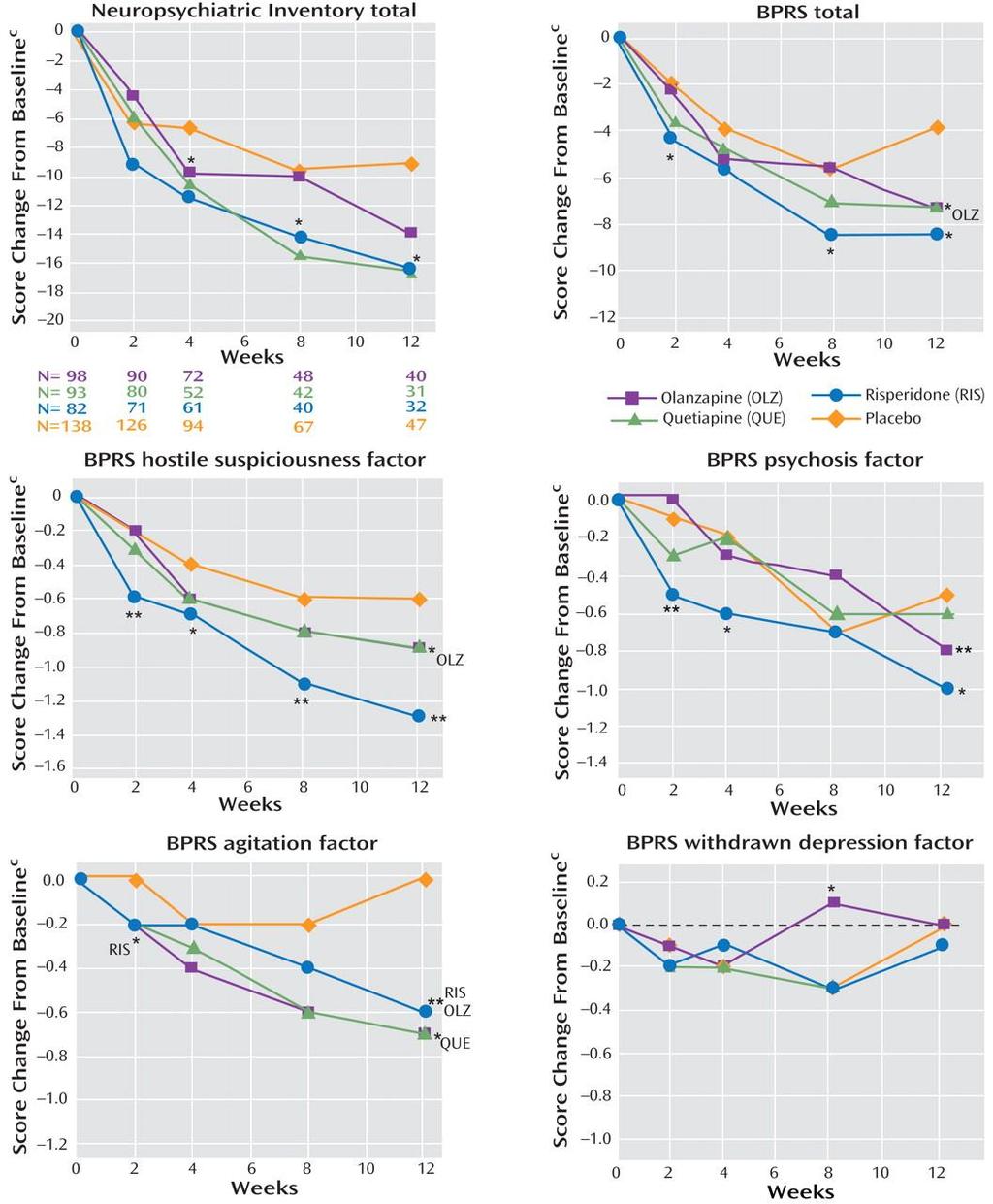
31 What about CATIE-AD? Initial publication did not look at efficacy of treating the symptoms! Reanalysis in 2008 did. OLZ, RIS, QTP, Placebo Response on NPI and CGIC after 12 weeks no different (range 21-32%), p=.22 Patients were more likely to stop placebo due to lack of effectiveness and stop drug because of side effects. If patient tolerated the medicine and stayed on it, there was improvement in anger, aggression and paranoia. But care needs, functioning did not improve. Schneider et al. NEJM 155(15): , 2006 Sultzer et al. AJP 165:844-54, 2008
32
33 FDA Boxed Warning FDA in 2005 added a boxed warning on all atypicals - Risperidone, Clozapine, Olanzapine, Ziprasidone, Aripiprazole and Quetiapine. The warning is for increased mortality with the off-label use of antipsychotics in the elderly/dementia population Data upon which warning was based: average age 85 Medications not prescribed for psychosis causes of mortality were varied People who were dying not excluded
34 Effect of FDA warning Within one year of 2005 warning, 19% decreased use of atypical antipsychotics among those with dementia By 2008, 50% decrease in use of atypical antipsychotics among those with dementia Use of atypical antipsychotics decreased for everyone, not just those with dementia Dorsey et al Arch Int Med 2010
35 Discussion with Dr Laughren and Dr Matthis of the FDA March 29, 2012 We don t understand the signal Meta-analysis of data collected prior to 2005 Data NOT for treatment of those with psychosis or aggression but a mix of behavior disturbance without any definition of what this is Age where risk most notable: 85 and older!!! Causes of death all over the map -no clear physiological etiology Risk highest at start of treatment, Dr Laughren theorizes that increased risk is due to excess sedation (though EPS causing swallowing problems seems much more likely to me) The boxed warning is not a contraindication to using these medications. Phone conference between Dr Nash and FDA Psychiatric Director and Assistant
36 FDA Boxed Warnings Later, for unstated reasons, FDA recognized that typical antipsychotics are dangerous Based on a study in 2007, FDA added the boxed warning on typical or first generation antipsychotics The warning is for increased mortality with the off-label use of antipsychotics in the elderly/dementia population
37 Typicals have more risk Typical antipsychotics are riskier 2 year period in patients older than 65 receiving Haloperidol (299) versus OLZ (1,254), 21.4% died in the Haloperidol group, 4.75% in the OLZ group. In another large retrospective study, with 649 cases and 2962 controls the use of older antipsychotics in the elderly was associated with nearly a 2-fold increased risk of hospitalization due to Ventricular arrhythmias or cardiac arrest no increased risk was found with the atypicals. Nasarallah HA et al: Am J Geriatr Psych 12:437-9, 2004 Liperoti R et al: Arch Intern Med 165: , 2005
38 Typicals have more risk Mortality ratio for risperidone 1.3 Mortality ratio haldol 2.14 CV or infectious causes were the major reasons for death, and could not be directly associated with the drugs. Highest period of risk within 40 days of starting prescription Schneeweiss S, et al CMAJ 176:627-32, 2007 Gill SS et al Ann Int Med 146:775-86, 2007
39 Typicals have more risk Wang et al did retrospective of nearly 23,000 patients over 65 years old in Pennsylvania who received conventional or atypical antipsychotics from Conventional/Typicals were associated with a significantly higher risk of death than atypicals in all subgroups. Highest risk was early in therapy and at higher doses. Wang PS et al: NEJM 353: , 2005
40 Evidence of risk? There s more evidence about antipsychotics: Another large retrospective study: 1,130 cases with 3,658 case controls NH patients, using either typicals or atypicals. No increased risk for stroke for any group or particular drug Trend for OLZ to increase risk of CVA, but not statistically significant Liperoti et al. J Clin Psychiatry, 66(9): , 2005
41 Quantity or quality of life? Quality of Life (QOL) None of these studies (FDA or others) looked at Quality of Life (QOL) issues for the patients and caregivers Improving behavioral symptoms (as noted on the NPI) through medications has been shown to improve QOL measures for both patients and CG Given all this information, I strongly recommend the continued careful use of atypicals for psychotic symptoms and life threatening aggression with informed consent for this population when and if necessary Il-Seon S et al: Am J Geriatr Psychiatry 13:469-74, 2005
42 Risks of use of BZD and atypical antipsychotics (Ellul et al 2007)
43 Personal Thoughts on Ellul study This study did not control for why these medications were prescribed. Does the presence of hallucinations, delusions and other psychotic symptoms indicate someone is nearing end of life? Does agitation or aggression severe enough that clinician s prescribe an antipsychotic predict nearing the end of life in some or even most patients with end-stage dementia? Do psychotic symptoms represent unrecognized delirium in patients with dementia (delirium has a very high mortality rate in older patients with dementia)?
44 Title of a LTE that I wrote Death is Not a Question of If
45 2/14/2013 Larry Tune, M.D. Professor, Department of Psychiatry and Behavioral Sciences and Neurology Emory University School of Medicine Pharmaceutical Trials Expatriate Associate Medical Director for Psychiatric Services at 4 nursing facilities Otherwise nothing The absence of proof is not proof of absence Some dementia psychopathology responds to antipsychotics..and they may need to stay on their antipsychotics Anger, aggression, paranoia Sultzer, et al, 2008; Devanand, et al, 2012 And some symptoms don t.. Wandering, calling out, repetitive questions, anxiety, agitation Huybrechts, et al,
46 2/14/2013 Announced in 2005, by 2008 there was a 50% reduction in the use of atypicals Did make us think (and worry) for that we should be grateful Antipsychotics aren t entirely safe physicians and families of patients need to be informed Special concerns: Subsyndromal delirium sedation is one area of concern Swallowing difficulties Due to sedation Or independent motor side effect No. Any questions? Well, not very many of them and perhaps they shouldn t be. 2
47 2/14/2013 Best results coming from a true culture change Interdisciplinary approach involving nurses, CNA s??expanded role for psychiatry consultants Energize the milieu U Pittsburgh U Iowa Mclean Hospital Teepa Snow! We are not immune We NEED TO STUDY THEM AS MUCH AS THEY STUDY US. 3

48 2/14/2013 Start low, go slow. Restore the biopsychosocial approach KNOW your patients Support/get to know/collaborate with your local Alzheimer s Association The absence of proof is not proof of absence. 4
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias. Aaron H. Kaufman, MD
 Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychosis and Agitation in Dementia
 Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
The place for treatments of associated neuropsychiatric and other symptoms
 The place for treatments of associated neuropsychiatric and other symptoms Luca Pani dg@aifa.gov.it London, 25 th November 2014 Workshop on Alzheimer s Disease European Medicines Agency London, UK Public
The place for treatments of associated neuropsychiatric and other symptoms Luca Pani dg@aifa.gov.it London, 25 th November 2014 Workshop on Alzheimer s Disease European Medicines Agency London, UK Public
Disclosure. Speaker Bureaus. Grant Support. Pfizer Forest Norvartis. Pan American Health Organization/WHO NIA HRSA
 Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
11/11/2016. Disclosures. Natural history of BPSD. Objectives. Assessment of BPSD. Behavioral Management of Persons with Alzheimer s Disease
 Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
Risks of Antipsychotics use In Dementia
 AHCA/NCAL Quality Initiative for Assisted Living Webinar Series: Safely Reducing the Off-Label Use of Antipsychotics Risks of Antipsychotics use In Dementia Sanjay P. Singh, MD Chairman & Professor, Department
AHCA/NCAL Quality Initiative for Assisted Living Webinar Series: Safely Reducing the Off-Label Use of Antipsychotics Risks of Antipsychotics use In Dementia Sanjay P. Singh, MD Chairman & Professor, Department
Management of Behavioral Problems in Dementia
 Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Pharmacological Treatment of Aggression in the Elderly
 Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches
 Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches Andrea Iaboni, MD, DPhil, FRCPC Toronto Rehab Institute, UHN Learning objectives Recognize
Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches Andrea Iaboni, MD, DPhil, FRCPC Toronto Rehab Institute, UHN Learning objectives Recognize
Organization: Sheppard Pratt Health System Solution Title: Lean Methodology: Appropriate Antipsychotic Use on an Inpatient Dementia Unit
 Organization: Sheppard Pratt Health System Solution Title: Lean Methodology: Appropriate Antipsychotic Use on an Inpatient Dementia Unit Problem: For dementia patients, antipsychotic medications are prescribed
Organization: Sheppard Pratt Health System Solution Title: Lean Methodology: Appropriate Antipsychotic Use on an Inpatient Dementia Unit Problem: For dementia patients, antipsychotic medications are prescribed
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
MORTALITY ASSOCIATED WITH USE OF ANTIPSYCHOTICS IN DEMENTIA: REVIEWING THE EVIDENCE
 MORTALITY ASSOCIATED WITH USE OF ANTIPSYCHOTICS IN DEMENTIA: REVIEWING THE EVIDENCE KRISTA L. LANCTÔT, PHD PROFESSOR OF PSYCHIATRY AND PHARMACOLOGY, UNIVERSITY OF TORONTO; SENIOR SCIENTIST, HURVITZ BRAIN
MORTALITY ASSOCIATED WITH USE OF ANTIPSYCHOTICS IN DEMENTIA: REVIEWING THE EVIDENCE KRISTA L. LANCTÔT, PHD PROFESSOR OF PSYCHIATRY AND PHARMACOLOGY, UNIVERSITY OF TORONTO; SENIOR SCIENTIST, HURVITZ BRAIN
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Management of Agitation in Dementia. Kimberly Triplett Ferguson, MS4
 Management of Agitation in Dementia Kimberly Triplett Ferguson, MS4 Objectives 1. Review recommended evaluation of agitated patients with dementia. 2. Discuss evidence concerning nonpharmacologic management.
Management of Agitation in Dementia Kimberly Triplett Ferguson, MS4 Objectives 1. Review recommended evaluation of agitated patients with dementia. 2. Discuss evidence concerning nonpharmacologic management.
USING ANTIPSYCHOTICS TO TREAT THE BEHAVIORAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA (BPSD)- WHAT IS THE EVIDENCE?
- WHAT IS THE EVIDENCE?") USING ANTIPSYCHOTICS TO TREAT THE BEHAVIORAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA (BPSD)- WHAT IS THE EVIDENCE? Mugdha Thakur, MD Associate Professor of Psychiatry and Behavioral Sciences Duke University
USING ANTIPSYCHOTICS TO TREAT THE BEHAVIORAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA (BPSD)- WHAT IS THE EVIDENCE? Mugdha Thakur, MD Associate Professor of Psychiatry and Behavioral Sciences Duke University
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist. HMS Training Webinar January 27, 2017
 Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
MANAGEMENT OF NEUROPSYCHIATRIC SYMPTOMS OF DEMENTIA
 MANAGEMENT OF NEUROPSYCHIATRIC SYMPTOMS OF DEMENTIA Dr. Dallas Seitz MD PhD FRCPC Associate Professor and Division Chair, Division of Geriatric Psychiatry Department of Psychiatry, Queen s University President,
MANAGEMENT OF NEUROPSYCHIATRIC SYMPTOMS OF DEMENTIA Dr. Dallas Seitz MD PhD FRCPC Associate Professor and Division Chair, Division of Geriatric Psychiatry Department of Psychiatry, Queen s University President,
9/11/2012. Clare I. Hays, MD, CMD
 Clare I. Hays, MD, CMD Review regulatory background for current CMS emphasis on antipsychotics Understand the risks and (limited) benefits of antipsychotic medications Review non-pharmacologic management
Clare I. Hays, MD, CMD Review regulatory background for current CMS emphasis on antipsychotics Understand the risks and (limited) benefits of antipsychotic medications Review non-pharmacologic management
The Place for Treatments of Associated Neuropsychiatric and Other Symptoms in Alzheimer s Disease and Other Dementias
 The Place for Treatments of Associated Neuropsychiatric and Other Symptoms in Alzheimer s Disease and Other Dementias The Patient and Carers Perspective Mary-Frances Morris, Trustee, Alzheimer Scotland.
The Place for Treatments of Associated Neuropsychiatric and Other Symptoms in Alzheimer s Disease and Other Dementias The Patient and Carers Perspective Mary-Frances Morris, Trustee, Alzheimer Scotland.
Management of the Acutely Agitated Long Term Care Patient
 Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good?
 ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good? STEPHANIE M. OZALAS, PHARMD, BCPS, BCGP VA MARYLAND HEALTH CARE SYSTEM BALTIMORE, MD DISCLOSURES Off-label use of medications will be
ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good? STEPHANIE M. OZALAS, PHARMD, BCPS, BCGP VA MARYLAND HEALTH CARE SYSTEM BALTIMORE, MD DISCLOSURES Off-label use of medications will be
Psychotropic Medication Use in Dementia
 Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Neuropsychiatric Syndromes
 Neuropsychiatric Syndromes Susan Czapiewski,MD VAHCS December 10, 2015 Dr. Czapiewski has indicated no potential conflict of interest to this presentation. She does intend to discuss the off-label use
Neuropsychiatric Syndromes Susan Czapiewski,MD VAHCS December 10, 2015 Dr. Czapiewski has indicated no potential conflict of interest to this presentation. She does intend to discuss the off-label use
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
MEDICATIONS IN MANAGING DIFFICULT BEHAVIORS
 MEDICATIONS IN MANAGING DIFFICULT BEHAVIORS A REALITY CHECK reality check Noun informal an occasion on which one is reminded of the state of things in the real world. ROBERT LACOSTE, MD MEDICAL DIRECTOR,
MEDICATIONS IN MANAGING DIFFICULT BEHAVIORS A REALITY CHECK reality check Noun informal an occasion on which one is reminded of the state of things in the real world. ROBERT LACOSTE, MD MEDICAL DIRECTOR,
Coordinating Care Between Neurology and Psychiatry to Improve the Diagnosis and Treatment of Parkinson s Disease Psychosis
 Coordinating Care Between Neurology and Psychiatry to Improve the Diagnosis and Treatment of Parkinson s Disease Psychosis Jeff Gelblum, MD Senior Attending Neurologist Mt. Sinai Medical Center Miami,
Coordinating Care Between Neurology and Psychiatry to Improve the Diagnosis and Treatment of Parkinson s Disease Psychosis Jeff Gelblum, MD Senior Attending Neurologist Mt. Sinai Medical Center Miami,
Antipsychotic use in dementia: a systematic review of benefits and risks from metaanalyses
 658463TAJ0010.1177/2040622316658463Therapeutic Advances in Chronic DiseaseRR Tampi, DJ Tampi research-article2016 Therapeutic Advances in Chronic Disease Original Research Antipsychotic use in dementia:
658463TAJ0010.1177/2040622316658463Therapeutic Advances in Chronic DiseaseRR Tampi, DJ Tampi research-article2016 Therapeutic Advances in Chronic Disease Original Research Antipsychotic use in dementia:
Clinical Trial Designs for RCTs focussing on the Treatment of Agitation in people with Alzheimer s disease
 Clinical Trial Designs for RCTs focussing on the Treatment of Agitation in people with Alzheimer s disease Professor Clive Ballard Dr Byron Creese University of Exeter, UK Guardian guide for 2018: Top
Clinical Trial Designs for RCTs focussing on the Treatment of Agitation in people with Alzheimer s disease Professor Clive Ballard Dr Byron Creese University of Exeter, UK Guardian guide for 2018: Top
Please Join Us. International Psychogeriatric Association. Dependency Ratio. Geriatric Psychiatry in the 21st Century: A Global Perspective
 International Psychogeriatric Association Please Join Us Geriatric Psychiatry in the 21st Century: A Global Perspective Jacobo Mintzer M.D. Executive Director Roper Saint Frances Clinical and Biotechnology
International Psychogeriatric Association Please Join Us Geriatric Psychiatry in the 21st Century: A Global Perspective Jacobo Mintzer M.D. Executive Director Roper Saint Frances Clinical and Biotechnology
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care
 Summary document for Primary Care") Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA
 BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
Antipsychotic Medication in Dementia; The good, the bad and the ugly! Anthony Bainbridge Deputy Director of Nursing Sheffield Health and Social Care
 Antipsychotic Medication in Dementia; The good, the bad and the ugly! Anthony Bainbridge Deputy Director of Nursing Sheffield Health and Social Care Different types of antipsychotic medication Antipsychotic
Antipsychotic Medication in Dementia; The good, the bad and the ugly! Anthony Bainbridge Deputy Director of Nursing Sheffield Health and Social Care Different types of antipsychotic medication Antipsychotic
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A
 Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Managing agitation in dementia using non-pharmacological therapies
 Managing agitation in dementia using non-pharmacological therapies Gill Livingston Lynsey Kelly, Elanor Lewis-Holmes, Gianluca Baio, Rumana Omar, Stephen Morris, Nishma Patel, Cornelius Katona, Claudia
Managing agitation in dementia using non-pharmacological therapies Gill Livingston Lynsey Kelly, Elanor Lewis-Holmes, Gianluca Baio, Rumana Omar, Stephen Morris, Nishma Patel, Cornelius Katona, Claudia
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Psychotropic Medication. Including Role of Gradual Dose Reductions
 Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A
 Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Is Depression management getting you down? G. Michael Allan Director Programs and Practice Support, CFPC Professor, Family Med, U of A Faculty/Presenter Disclosures Faculty: Mike Allan Salary: College
Medication Treatment of Cognitive and Behavioral Symptoms in Dementia
 Medication Treatment of Cognitive and Behavioral Symptoms in Dementia Cary J. Kohlenberg, M.D. Medical Director, IPC Research and Independent Psychiatric Consultants Environmental interventions directly
Medication Treatment of Cognitive and Behavioral Symptoms in Dementia Cary J. Kohlenberg, M.D. Medical Director, IPC Research and Independent Psychiatric Consultants Environmental interventions directly
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
9/24/2012. Amer M Burhan, MBChB, FRCP(C)
") Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
Mental Health Issues in Nursing Homes. I m glad you asked.
 Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
I received help from Bosch Health Care
 John Kasckow, MD, PhD VA Pittsburgh Health Care System Western Psychiatric Institute and Clinic, UPMC VA Pittsburgh Health Care System I received help from Bosch Health Care 1 Diagnoses of Interest Early
John Kasckow, MD, PhD VA Pittsburgh Health Care System Western Psychiatric Institute and Clinic, UPMC VA Pittsburgh Health Care System I received help from Bosch Health Care 1 Diagnoses of Interest Early
Objectives. Antipsychotics 7/25/2016. LeadingAge Florida 53rd Annual Convention & Exposition
 Reducing the Use of Antipsychotics in Long Term Care Communities Alan W. Obringer RPh, CPh, CGP Executive Director Senior Care Pharmacy Objectives Recognize the clinical evidence for the need to change
Reducing the Use of Antipsychotics in Long Term Care Communities Alan W. Obringer RPh, CPh, CGP Executive Director Senior Care Pharmacy Objectives Recognize the clinical evidence for the need to change
From Neurodevelopment to Neurodegeneration: Behavioral Issues
 From Neurodevelopment to Neurodegeneration: Behavioral Issues Amer M. Burhan, MBChB, FRCPC Associate Professor and Chair Geriatric Psychiatry at Western U Objectives Discuss factors that contribute to
From Neurodevelopment to Neurodegeneration: Behavioral Issues Amer M. Burhan, MBChB, FRCPC Associate Professor and Chair Geriatric Psychiatry at Western U Objectives Discuss factors that contribute to
Restrained use of antipsychotic medications:
 Balanced information for better care Restrained use of antipsychotic medications: Rational management of irrationality These drugs are commonly prescribed in conditions for which there is little evidence
Balanced information for better care Restrained use of antipsychotic medications: Rational management of irrationality These drugs are commonly prescribed in conditions for which there is little evidence
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Older People Mental Health - new directorate/new plans. Dr Adrian Treloar Clinical director
 Older People Mental Health - new directorate/new plans Dr Adrian Treloar Clinical director Dementia 700,000 people in the UK currently have dementia; this number is set to double by 2038 1/3 of people
Older People Mental Health - new directorate/new plans Dr Adrian Treloar Clinical director Dementia 700,000 people in the UK currently have dementia; this number is set to double by 2038 1/3 of people
Choosing Wisely Psychiatry s Top Priorities for Appropriate Primary Care
 Choosing Wisely Psychiatry s Top Priorities for Appropriate Primary Care JASON BEAMAN D.O., M.S., FAPA ASSISTANT CLINICAL PROFESSOR CHAIR, DEPARTMENT OF PSYCHIATRY AND BEHAVIORAL SCIENCES OKLAHOMA STATE
Choosing Wisely Psychiatry s Top Priorities for Appropriate Primary Care JASON BEAMAN D.O., M.S., FAPA ASSISTANT CLINICAL PROFESSOR CHAIR, DEPARTMENT OF PSYCHIATRY AND BEHAVIORAL SCIENCES OKLAHOMA STATE
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018
 Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Treatment of behavioral and psychological symptoms of dementia: a systematic review
 Psychiatr. Pol. 2016; 50(4): 679 715 PL ISSN 0033-2674 (PRINT), ISSN 2391-5854 (ONLINE) www.psychiatriapolska.pl DOI: http://dx.doi.org/10.12740/pp/64477 Treatment of behavioral and psychological symptoms
Psychiatr. Pol. 2016; 50(4): 679 715 PL ISSN 0033-2674 (PRINT), ISSN 2391-5854 (ONLINE) www.psychiatriapolska.pl DOI: http://dx.doi.org/10.12740/pp/64477 Treatment of behavioral and psychological symptoms
Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD
 Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD Define BPSD and review the spectrum of associated symptoms Review pharmacologic and non-pharmacologic treatments for BPSD Evaluate
Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD Define BPSD and review the spectrum of associated symptoms Review pharmacologic and non-pharmacologic treatments for BPSD Evaluate
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Dementia: Managing Difficult Behaviors. No conflicts of interest. Off-label medication use will be discussed during this talk.
 Dementia: Managing Difficult Behaviors No conflicts of interest. Off-label medication use will be discussed during this talk. 1 Types of Neurocognitive Disorder Alzheimer s Disease Vascular Frontotemporal
Dementia: Managing Difficult Behaviors No conflicts of interest. Off-label medication use will be discussed during this talk. 1 Types of Neurocognitive Disorder Alzheimer s Disease Vascular Frontotemporal
Behavioural Problems and Patterns of Psychopharmacological Treatment given in Elderly Patients with Dementia
 The International Journal of Indian Psychology ISSN 2348-5396 (e) ISSN: 2349-3429 (p) Volume 6, Issue 4, DIP: 18.01.090/20180604 DOI: 10.25215/0604.090 http://www.ijip.in October-December, 2018 Research
The International Journal of Indian Psychology ISSN 2348-5396 (e) ISSN: 2349-3429 (p) Volume 6, Issue 4, DIP: 18.01.090/20180604 DOI: 10.25215/0604.090 http://www.ijip.in October-December, 2018 Research
Lewy Body Disease. Dementia Education for the First Responder July 27, 2017
 Lewy Body Disease Dementia Education for the First Responder July 27, 2017 Dylan Wint, M.D. NV Energy Chair for Brain Health Education Cleveland Clinic Lou Ruvo Center for Brain Health OUTLINE Lewy body
Lewy Body Disease Dementia Education for the First Responder July 27, 2017 Dylan Wint, M.D. NV Energy Chair for Brain Health Education Cleveland Clinic Lou Ruvo Center for Brain Health OUTLINE Lewy body
NeuroPharmac Journal ISSN: Alzheimer s Disease: Pharmacotherapy of noncognitive symptoms Aslam Pathan; Abdulrahman M.
 ISSNISSN ISSN: 2456-3927 NeuroPharmac Journal Alzheimer s Disease: Pharmacotherapy of noncognitive symptoms Aslam Pathan; Abdulrahman M. Alshahrani www. neuropharmac.com Jan-April 2018, Volume 3, Issue
ISSNISSN ISSN: 2456-3927 NeuroPharmac Journal Alzheimer s Disease: Pharmacotherapy of noncognitive symptoms Aslam Pathan; Abdulrahman M. Alshahrani www. neuropharmac.com Jan-April 2018, Volume 3, Issue
Psychiatry in Primary Care: What is the Role of Pharmacist?
 Psychiatry in Primary Care: What is the Role of Pharmacist? Benjamin Chavez, PharmD, BCPP, BCACP Clinical Associate Professor Director of Behavioral Health Pharmacy Services January 12, 2019 Disclosure
Psychiatry in Primary Care: What is the Role of Pharmacist? Benjamin Chavez, PharmD, BCPP, BCACP Clinical Associate Professor Director of Behavioral Health Pharmacy Services January 12, 2019 Disclosure
Behavioral Issues in Dementia. March 27, 2014 Dylan Wint, M.D.
 Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Appendix 2017UEMS031
 Appendix 2017UEMS031 PREVENTION Clinical checklist This checklist should be completed for each person with dementia. Keep this chart with the person s corresponding paperwork. General symptoms Include
Appendix 2017UEMS031 PREVENTION Clinical checklist This checklist should be completed for each person with dementia. Keep this chart with the person s corresponding paperwork. General symptoms Include
EARLY ONSET SCHIZOPHRENIA
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences EARLY ONSET SCHIZOPHRENIA JON MCCLELLAN CHILD STUDY AND TREATMENT CENTER GENERAL DISCLOSURES The University of Washington
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences EARLY ONSET SCHIZOPHRENIA JON MCCLELLAN CHILD STUDY AND TREATMENT CENTER GENERAL DISCLOSURES The University of Washington
Depression in Late Life
 Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Medications for Anxiety & Behavior in Williams Syndrome. Disclosure of Potential Conflicts. None 9/22/2016. Evaluation
 Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Burden of behavioral and psychiatric symptoms in people screened positive for dementia in primary care results of the DelpHi-study René Thyrian
 Burden of behavioral and psychiatric symptoms in people screened positive for dementia in primary care results of the DelpHi-study René Thyrian German Center for Neurodegenerative Diseases (DZNE), site
Burden of behavioral and psychiatric symptoms in people screened positive for dementia in primary care results of the DelpHi-study René Thyrian German Center for Neurodegenerative Diseases (DZNE), site
Pharmacological Treatment of Behavioural and Psychological Symptoms of Dementia (BPSD) Gurdeep K Major St. Charles Hospital
 Gurdeep K Major St. Charles Hospital") Pharmacological Treatment of Behavioural and Psychological Symptoms of Dementia (BPSD) Gurdeep K Major St. Charles Hospital with thanks to Jonathan Cavan for his input Aims Define BPSD and common symptoms
Pharmacological Treatment of Behavioural and Psychological Symptoms of Dementia (BPSD) Gurdeep K Major St. Charles Hospital with thanks to Jonathan Cavan for his input Aims Define BPSD and common symptoms
OBJECTIVES. Achieving Success in Reducing Inappropriate Use of Antipsychotic Medication in Patients with Dementia
 Achieving Success in Reducing Inappropriate Use of Antipsychotic Medication in Patients with Dementia Amy J. Osborn, NHA, PMP Executive Director, Health Services Advisory Group (HSAG) Rick Foley, PharmD,
Achieving Success in Reducing Inappropriate Use of Antipsychotic Medication in Patients with Dementia Amy J. Osborn, NHA, PMP Executive Director, Health Services Advisory Group (HSAG) Rick Foley, PharmD,
Whose Problem Is It? Mental Health & Illness in Long-term Care
 Whose Problem Is It? Mental Health & Illness in Long-term Care Revised by M. Smith (2005) from M. Smith & K.C. Buckwalter (1993), Whose Problem Is It? Mental Health & Illness in Long-term Care, The Geriatric
Whose Problem Is It? Mental Health & Illness in Long-term Care Revised by M. Smith (2005) from M. Smith & K.C. Buckwalter (1993), Whose Problem Is It? Mental Health & Illness in Long-term Care, The Geriatric
Cognitive enhancers PINCH ME. Anticholinergic burden BPSD. Agitation, Aggression and antipsychotics
 Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Drugs used to relieve behavioural and psychological symptoms in dementia
 alzheimers.org.uk Drugs used to relieve behavioural and psychological symptoms in dementia People with dementia may develop behavioural and psychological symptoms including restlessness, aggression, delusions,
alzheimers.org.uk Drugs used to relieve behavioural and psychological symptoms in dementia People with dementia may develop behavioural and psychological symptoms including restlessness, aggression, delusions,
October 28, Geriatrics Update Course. Lesley Wiesenfeld, MD, MHCM, FRCPC. Managing BPSD. Geriatric Psychiatrist, Mount Sinai Hospital
 October 28, 2016 Geriatrics Update Course Managing BPSD Lesley Wiesenfeld, MD, MHCM, FRCPC Geriatric Psychiatrist, Mount Sinai Hospital Disclosures ~No Pharmaceutical or Industry Support ~ No Health Without
October 28, 2016 Geriatrics Update Course Managing BPSD Lesley Wiesenfeld, MD, MHCM, FRCPC Geriatric Psychiatrist, Mount Sinai Hospital Disclosures ~No Pharmaceutical or Industry Support ~ No Health Without
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #283: Dementia Associated Behavioral and Psychiatric Symptoms Screening and Management National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #283: Dementia Associated Behavioral and Psychiatric Symptoms Screening and Management National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together. Presented by
 WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together Presented by Our agenda for today Understanding behavioral symptoms in people living with dementia Briefly review key strategies
WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together Presented by Our agenda for today Understanding behavioral symptoms in people living with dementia Briefly review key strategies
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Reducing Antipsychotic Drug Use in Long Term Care
 Reducing Antipsychotic Drug Use in Long Term Care Janice S. Ceriotti, RPh, CGP Director of Clinical Services Omnicare Pharmacies / Eastern MO Goals and Objectives Understand the history of Antipsychotics
Reducing Antipsychotic Drug Use in Long Term Care Janice S. Ceriotti, RPh, CGP Director of Clinical Services Omnicare Pharmacies / Eastern MO Goals and Objectives Understand the history of Antipsychotics
Behavioral Interventions
 Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
CHCS. Multimorbidity Pattern Analyses and Clinical Opportunities: Dementia. Center for Health Care Strategies, Inc. FACES OF MEDICAID DATA SERIES
 CHCS Center for Health Care Strategies, Inc. FACES OF MEDICAID DATA SERIES Multimorbidity Pattern Analyses and Clinical Opportunities: Dementia December 2010 Cynthia Boyd, MD, MPH* Bruce Leff, MD* Carlos
CHCS Center for Health Care Strategies, Inc. FACES OF MEDICAID DATA SERIES Multimorbidity Pattern Analyses and Clinical Opportunities: Dementia December 2010 Cynthia Boyd, MD, MPH* Bruce Leff, MD* Carlos
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Abbreviated Class Review: Long-Acting Injectable Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Abbreviated Class Review: Long-Acting Injectable Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
What Can Geriatrics Teach Us About the Care of Vulnerable Patients?
 What Can Geriatrics Teach Us About the Care of Vulnerable Patients? Helen Kao MD Associate Professor Medical Director, UCSF Geriatrics Clinical Programs UCSF March 11, 2016 Objectives 1. Define vulnerabilities
What Can Geriatrics Teach Us About the Care of Vulnerable Patients? Helen Kao MD Associate Professor Medical Director, UCSF Geriatrics Clinical Programs UCSF March 11, 2016 Objectives 1. Define vulnerabilities
Behavioral and Psychological Symptoms of dementia (BPSD)
") Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Screening and Management of Behavioral and Psychiatric Symptoms Associated with Dementia
 Screening and Management of Behavioral and Psychiatric Symptoms Associated with Dementia Measure Description Percentage of patients with dementia for whom there was a documented screening* for behavioral
Screening and Management of Behavioral and Psychiatric Symptoms Associated with Dementia Measure Description Percentage of patients with dementia for whom there was a documented screening* for behavioral
Effective Health Care Program
 Comparative Effectiveness Review Number 43 Effective Health Care Program Off-Label Use of Atypical Antipsychotics: An Update Executive Summary Background Antipsychotics medications are approved by the
Comparative Effectiveness Review Number 43 Effective Health Care Program Off-Label Use of Atypical Antipsychotics: An Update Executive Summary Background Antipsychotics medications are approved by the
Depression in Older Adults. Paul Boulware, MD Arizona Neurological Institute April 22, 2012
 Depression in Older Adults Paul Boulware, MD Arizona Neurological Institute April 22, 2012 What is it? Major depressive disorder is a syndrome, a collection of symptoms Presentation is variable among individuals
Depression in Older Adults Paul Boulware, MD Arizona Neurological Institute April 22, 2012 What is it? Major depressive disorder is a syndrome, a collection of symptoms Presentation is variable among individuals
Silvia Duong, 1,2 Kam-Tong Yeung, 1 and Feng Chang 1,3. 1. Introduction
 Aging Research Volume 2015, Article ID 570410, 6 pages http://dx.doi.org/10.1155/2015/570410 Research Article Intramuscular Olanzapine in the Management of Behavioral and Psychological Symptoms in Hospitalized
Aging Research Volume 2015, Article ID 570410, 6 pages http://dx.doi.org/10.1155/2015/570410 Research Article Intramuscular Olanzapine in the Management of Behavioral and Psychological Symptoms in Hospitalized
BPSD%What&to&do?&& Geriatric&Refresher&Day&& 11:30#12:30,&Wed&March&4 th,&2015& St&Elias&Centre,&OCawa&Ontario& &
 RGPEO% Regional&Geriatric&Program&of&Eastern&Ontario& BPSD%What&to&do?&& Geriatric&Refresher&Day&& 11:30#12:30,&Wed&March&4 th,&2015& St&Elias&Centre,&OCawa&Ontario& & Behavioural&and& Psychological& Symptoms&&
RGPEO% Regional&Geriatric&Program&of&Eastern&Ontario& BPSD%What&to&do?&& Geriatric&Refresher&Day&& 11:30#12:30,&Wed&March&4 th,&2015& St&Elias&Centre,&OCawa&Ontario& & Behavioural&and& Psychological& Symptoms&&
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Negative Symptoms of Schizophrenia: Treatments
 Negative Symptoms of Schizophrenia: Treatments Nowadays we tend to think of the various symptoms of schizophrenia as falling into two groups. There are the positive symptoms such as delusions and hallucinations
Negative Symptoms of Schizophrenia: Treatments Nowadays we tend to think of the various symptoms of schizophrenia as falling into two groups. There are the positive symptoms such as delusions and hallucinations
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
How I Treat Aggression in Outpatients With Dementia. C. Omelan MD, FRCP(C)
") How I Treat Aggression in Outpatients With Dementia C. Omelan MD, FRCP(C) Conflict of Interest I have no potential conflicts of interest to declare Overview Outline the prevalence of aggression Review
How I Treat Aggression in Outpatients With Dementia C. Omelan MD, FRCP(C) Conflict of Interest I have no potential conflicts of interest to declare Overview Outline the prevalence of aggression Review
Rational Medication Use in Dementia
 Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
TRANSPARENCY COMMITTEE Opinion 19 February 2014
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 19 February 2014 RISPERDAL 1 mg, scored film-coated tablet B/60 (CIP: 34009 338 948 7 0) RISPERDAL 2 mg, scored film-coated
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 19 February 2014 RISPERDAL 1 mg, scored film-coated tablet B/60 (CIP: 34009 338 948 7 0) RISPERDAL 2 mg, scored film-coated
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
PDFlib PLOP: PDF Linearization, Optimization, Protection. Page inserted by evaluation version
 PDFlib PLOP: PDF Linearization, Optimization, Protection Page inserted by evaluation version www.pdflib.com sales@pdflib.com doi:10.1111/j.1479-8301.2007.00215.x PSYCHOGERIATRICS 2008; 8: 32 37 REVIEW
PDFlib PLOP: PDF Linearization, Optimization, Protection Page inserted by evaluation version www.pdflib.com sales@pdflib.com doi:10.1111/j.1479-8301.2007.00215.x PSYCHOGERIATRICS 2008; 8: 32 37 REVIEW
Corporate Presentation August 6, 2015
 Corporate Presentation August 6, 2015 Creating the Next Generation of CNS Drugs Forward-Looking Statement This presentation contains forward-looking statements. These statements relate to future events
Corporate Presentation August 6, 2015 Creating the Next Generation of CNS Drugs Forward-Looking Statement This presentation contains forward-looking statements. These statements relate to future events