An Update on Prevention and Treatment of Glucocorticoid-Induced Osteoporosis
|
|
|
- Luke Marsh
- 6 years ago
- Views:
Transcription
1 An Update on Prevention and Treatment of Glucocorticoid-Induced Osteoporosis Joseph Flood, MD, FACR, CCD President, Musculoskeletal Medical Specialists, Inc. Clinical Assistant Professor of Internal Medicine The Ohio State University College of Medicine and Public Health

 of Musculoskeletal Disorders and Center")
2 New Strategies in the Management of Glucocorticoid-Induced Osteoporosis (GIOP) Kenneth G. Saag, M.D., M.Sc. Jane Knight Lowe Professor of Medicine Division of Clinical Immunology and Rheumatology Director, Center for Education and Research on Therapeutics (CERTs) of Musculoskeletal Disorders and Center for Outcomes, Effectiveness Research, and Education (COERE) THE UNIVERSITY OF ALABAMA AT BIRMINGHAM
3 2010 ACR Recommendations for the Prevention and Treatment of Glucocorticoid Induced Osteoporosis (GIOP) Arthritis Care & Research Vol. 62, No. 11, November 2010, pp
4 GIOP 2011 New Treatment Strategies How is osteoporosis risk best assessed? What can be done to prevent and treat GIOP? What is being done? How can we improve quality?
5 GIOP Pathophysiology Glucocorticoids BONE OSTEOCYTE Function Apoptosis OSTEOBLAST Differentiation Function Apoptosis bone formation Bone Quality Bone Mass Increased risk of fracture Canalis E. Osteoporosis Int 2007;18:1319
6 GIOP Pathophysiology Glucocorticoids BONE RANKL OSTEOCYTE OSTEOBLAST OSTEOCLAST CSF Function Differentiation Genesis Apoptosis Function Apoptosis Apoptosis bone formation bone resorption Bone Quality Bone Mass Increased risk of fracture Canalis E. Osteoporosis Int 2007;18:1319
7 GIOP Pathophysiology Glucocorticoids BONE Neuroendocrine Calcium Metabolism RANKL OSTEOCYTE OSTEOBLAST OSTEOCLAST CSF Function Differentiation Genesis Apoptosis Function Apoptosis GH/ IGF-I Apoptosis sex steroids intestinal absorption Renal excretion bone formation bone resorption Negative calcium balance Bone Quality Bone Mass Increased risk of fracture Canalis E. Osteoporosis Int 2007;18:1319
8 GIOP Pathophysiology Glucocorticoids BONE Neuroendocrine Calcium Metabolism Muscle RANKL OSTEOCYTES OSTEOBLASTS OSTEOCLASTS CSF Function Differentiation Genesis Apoptosis Function Apoptosis GH/ IGF-I Apoptosis sex steroids intestinal absorption Renal excretion Proteolysis of myofibrils Fibrils bone formation bone resorption Negative calcium balance Bone Quality Bone Mass Myopathy Increased risk of fracture risk of falls Muscle weakness Canalis E. Osteoporosis Int 2007;18:1319
9 Adjusted Relative Rate of Non-vertebral fracture van Staa et al, Rheum, 2000
10 Fracture Risk by Spine BMD is Different in Post Menopausal Oral Glucocorticoid Users 56 postmenopausal patients in PBO arm of Risedronate GIO trials comp. to 1899 post menopausal women from PMO trials for fracture incidence at 1 year at specific BMDs (RR=5.67) vs Non-Users Fracture Incidence (%) PMO GI O Lumbar Spine T-Score Van Staa et al. Arthritis Rheum 2003; 48:3224-9

11 Steroids alter the BMD Fracture Threshold Steroid users Nonusers % Fractures Lumbar spine BMD van Staa. Arth Rheum 2003; 48: Femoral neck BMD
12 Prevalence and the RR of fracture for age, sex, risk factors in GIOP (not included in 2001 recommendations) Risk Factor Age (for each 10 years of age) Prevalence Clinical osteoporotic fracture RR (95%CI) 1.63 ( ) 1.66) Sex, Male 39.8% 0.51 ( ) 0.54) BMI <20 4.8% 1.48 ( ) 1.62) BMI > % 0.84 ( ) 0.89) History of fall in prior 6 m 1.6% 2.57 ( ) 2.86) Van Staa, Q J Med, 2005
13 Screening by bone mass measurement and prescription of non-estrogen therapies for the prevention of GIOP in Curtis JR et al. Arthritis Rheum Vol.52, 8:
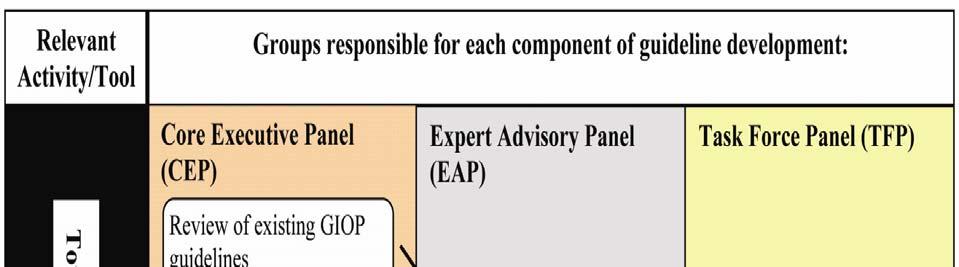
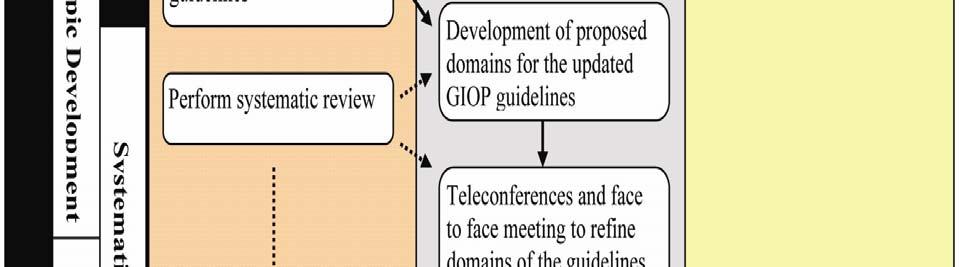
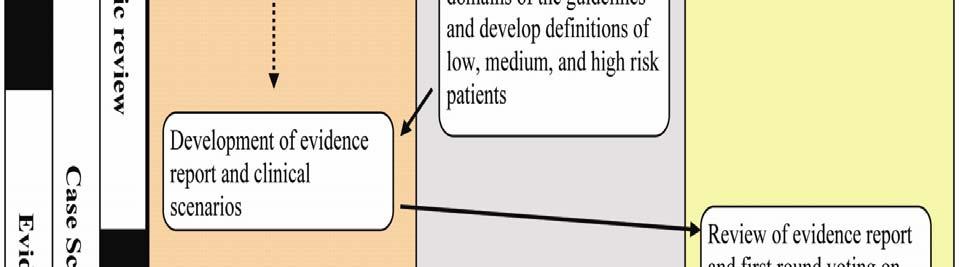
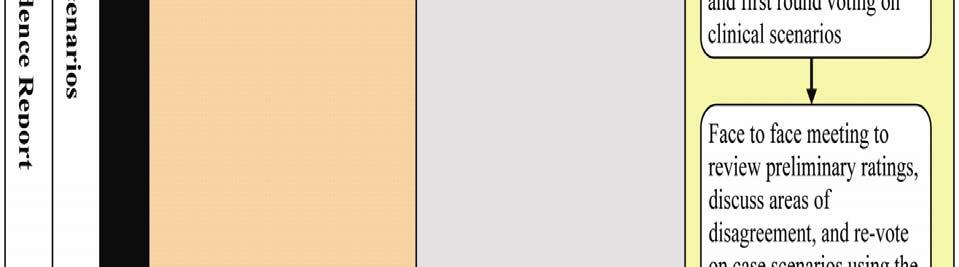
14 Updating the Recommendations Systematically developed statements to assist both practitioners and patients decisions about appropriate health care for specific clinical situations. This was an update to the prior 2001 recommendations from the ACR Since 2001 New osteoporosis medications Expanded data on existing therapies New methodology of fracture risk assessment Refined methodology of developing guidelines
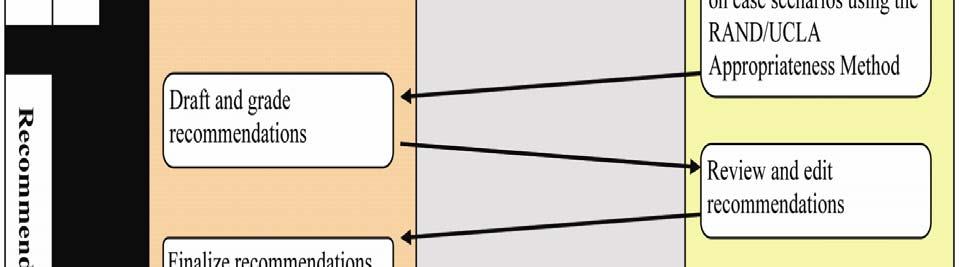
15
16 Core Executive Panel UCLA Jennifer Grossman, MD Daniel E. Furst, MD Rebecca Gordon, MD Maureen McMahon, MD Veena Ranganath, MD Elizabeth Volkmann, MD Weiling Chen, MA Diane Tan, BA Rikke Ogawa UAB/U of Colorado Kenneth Saag MD, MSc Jeffrey Curtis MD, MPH Nivedita Patkar MD, MSPH Kathy Parham Liron Caplan, MD
17 Expert Advisory Panel Marc Hochberg, MD Nancy Lane, MD Johannes Bijlsma, MD Willem Lems, MD Chad Deal, MD Catherine MacLean, MD, PhD
18 Task Force Panel Ted Hahn, MD Robert Adler, MD Cathleen Colon-Emeric, MD Michael Maricic, MD Anthony Sebba, MD Stuart Silverman, MD Gary Bryant, MD Chad Deal, MD Joseph Flood, MD Amye Leong
19 Refining the Scope No childhood GIOP No transplant GIOP No inhaled steroids only No IV pulse steroids only Limited to medications approved by FDA, Canada, or EU used to treat osteoporosis Refine scope of project given number of variables that can affect fracture risk
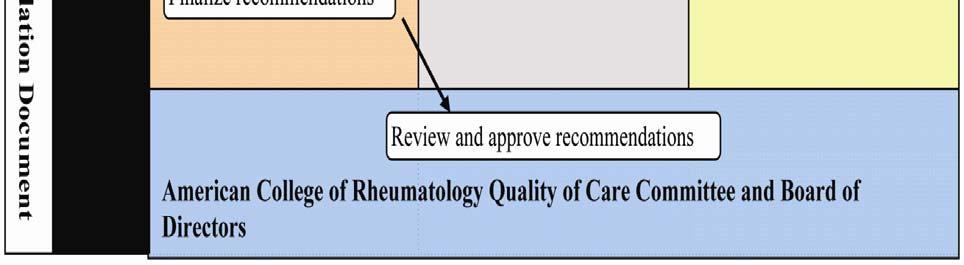
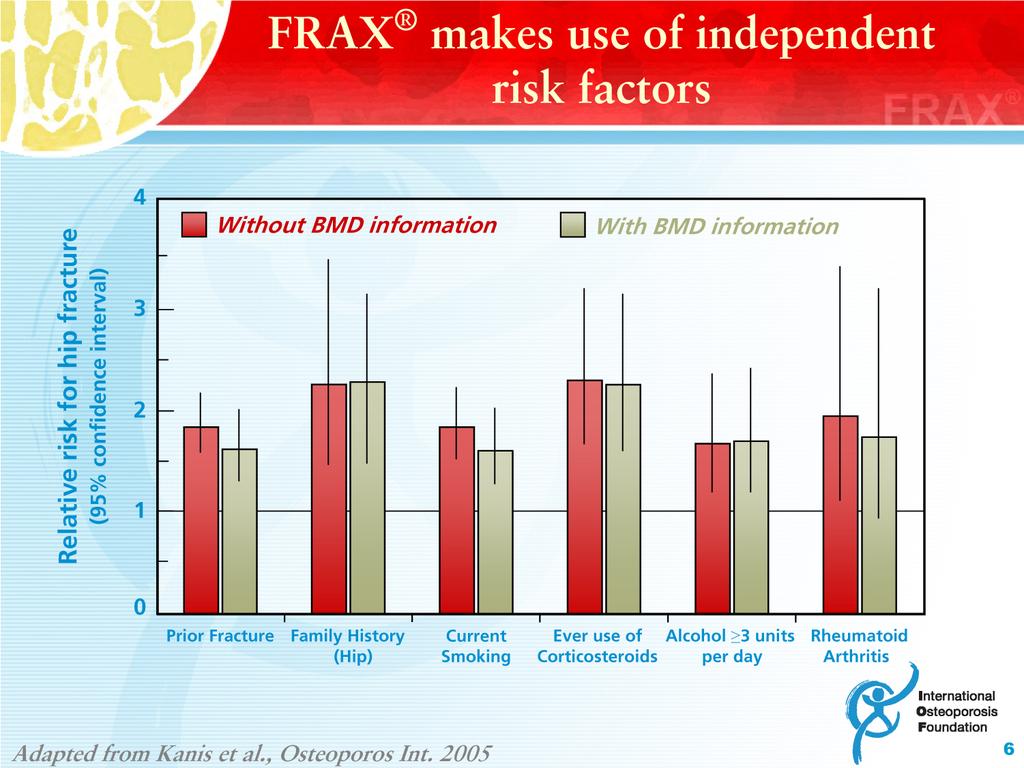
20 What is FRAX A tool to calculate 10-year probability of fracture hip fracture major osteoporotic fracture clinical spine, hip, forearm, humerus Uses patient derived intuitive clinical risk factors Can calculate with or without femoral neck BMD Intended to provide information to clinicians and patients on fracture risk that adds to that provided by BMD alone
21
22
23 T-Score Caucasian Women Age Low Risk- FRAX <10% for 10 yr major OP fracture Medium Risk-FRAX 10-20% for 10 yr major OP fracture High Risk-FRAX >20% for 10 yr major OP fracture Major OP fractures are hip, clinical spine, wrist and humerus fractures
24 Limitations of Frax Does not incorporate all known risk factors (ie falls) Lacks dose response effects (corticosteroids, tobacco, alcohol, severity of rheumatoid arthritis, number of previous fractures) Uses only BMD of the hip Does not account for non-hip fractures in parents Relevant only for untreated patients
25 How Good is FRAX In Accounting for Steroid Use? Average Dose Captured by FRAX is ~2.5 to 7.5 mg/day prednisone Fracture probability under-estimated estimated if prednisone dose > 7.5 mg/d and over- estimated if < 2.5 mg/d Frequent intermittent high dose steroids increases fracture risk; FRAX can not capture this FRAX may underestimate fracture risk in users of high dose inhaled steroids Appropriate glucocorticoid replacement in individuals with adrenal insufficiency should not be included in FRAX Leib E, JCD, 2011
 < 50 yr 60 yr 70 yr > 80 yr High")

26 Recommended Adjustment to FRAX Based on Glucocorticoid Dose Adjustment Of FRAX By Age (%) < 50 yr 60 yr 70 yr > 80 yr High Dose > 7.5 mg Low Dose < 2.5 mg McCloskey E. OI 2011:22;809 Green = Hip Fracture Adjustment Pink = Major Osteoporosis Fracture Adjustment
27 GIOP 2011 New Treatment Strategies How is osteoporosis risk best assessed? What can be done to prevent and treat GIOP? What is being done? How can we improve quality?
28 Alendronate GIOP Prevention and Treatment % Change (Mean + SE) Spine 10 mg*** 5 mg*** PBO % Change (Mean + SE) Trochanter 10 mg** 5 mg** PBO Weeks Weeks 2 1 % Change (Mean 0 + SE) -1-2 Femoral Neck 5 mg** 10 mg** PBO** * ** P < ** P 0.01 Saag KG. NEJM 1998; 339: Weeks
29 Effect of Risedronate on BMD in Patients on Long-Term Corticosteroid Therapy % Change in BMD From Baseline 1.0 at 12 Months 0.0 Control Risedronate 2.5 mg Risedronate 5 mg * * * * Lumbar Spine Femoral Neck Trochanter Reid DM. J BMR 2000; 15: 1006 *P < 0.05 vs control.
30 Zoledronic Acid vs. Risedronate in GIO Lumbar Spine BMD Treatment sub-population Risedronate Zoledronic acid Prevention sub-population % Change From Baseline 5 [1.04*] [1.36*] Time (months) N = 249 N = 275 % Change From Baseline [1.72*] Time (months) [1.96*] N = 129 N = 136 * p-value < 0.01 Reid D, Lancet 2009; 373: 1253
31 Raloxifene for GIOP (n = 117 PM Women) Mok CC. Ann Rheum Dis :778
32 Teriparatide vs. ALN: Lumbar Spine BMD Percent Change in BMD Mean ± SE * Endpoint Months Alendronate n= Teriparatide n= % 3.8% Teriparatide 9.8% 5.2% Alendronate 11.0% 5.3% Saag K, NEJM 2007;357:2 Saag K. Arth Rheum, % 4.2% * P<0.05; P<0.001 Teriparatide vs. Alendronate BMD = bone mineral density, g/cm 2
33 Teriparatide vs. ALN New Vertebral Fractures Vertebral radiographic Alendronate (n=169)* Teriparatide (n=173)* P-value 13 (7.7%) 3 (1.7%) Clinical vertebral** 4 (2.4%) *Number (%) of patients with paired baseline and post-baseline spinal radiographs **Radiographically confirmed vertebral fracture(s) associated with symptoms such as back pain; vertebrae graded individually for compression deformity using semiquantitative criteria
 Note: Percentages reflect the %-change from baseline, from the MMRM")
34 TPTD vs. Risedronate in GIOP Change in vbmd in Men ( n= 77) * * p=0.004 for the between treatment comparison (MMRM model) Note: Percentages reflect the %-change from baseline, from the MMRM model. Glüer CC et al. ASBMR 2011 (Plenary Poster FR0413)

")
35 TPTD vs. Risedronate Finite Element Analysis - Strength * * * Anterior Bending Axial Compression Axial Torsion * P for the between treatment comparison (MMRM model) Glüer CC et al. ASBMR 2011 (Plenary Poster FR0413)
36 Risk Category Modifiers Higher daily dose of glucocorticoids Higher cumulative dose of glucocorticoids Declining bone mineral density Low body mass Parental history of hip fracture Current smoking More than 2 alcoholic drinks daily A diagnosis of rheumatoid arthritis Secondary osteoporosis (other than GIOP) If using risk charts and not calculating the actual FRAX score
37 Recommendations -Counseling weight bearing activities smoking cessation avoidance of excessive alcohol intake > 2 drinks per day nutritional counseling on calcium and vitamin D intake
38 Recommendations -Counseling weight bearing activities smoking cessation avoidance of excessive alcohol intake > 2 drinks per day nutritional counseling on calcium and vitamin D intake fall risk assessment baseline DXA serum 25-OH vitamin D level baseline height
39 Recommendations -Counseling weight bearing activities smoking cessation avoidance of excessive alcohol intake > 2 drinks per day nutritional counseling on calcium and vitamin D intake fall risk assessment baseline DXA serum 25-OH vitamin D level baseline height assessment of prevalent fragility fractures Vitamin D supplementation Calcium intake (supplement plus oral intake) of mg daily Consider radiographic imaging of the spine or VFA
40 Vertebral Fracture Assessment (VFA) Prevalent vertebral fractures (VF) predict future risk The relative risk associated with a history of fractures was (95% CI ) for clinical osteoporotic fracture, 1.68 (95% CI ) 1.87) for femur/hip fracture 2.04 (95% CI ) for clinical vertebral fracture (Van Staa et al) Only approximately 25-33% of all VF are clinically apparent Many patients with VF have T scores that would not be in the osteoporosis range and might not be offered therapy Can be done using DXA scan. Grade 2 and 3 have good specificity for vertebral fracture while more research is needed to improve the specificity of grade 1 fractures



41 X-ray T12 Fracture X-ray VFA
42 Height Measurement Historical height loss (HHL) (the patient s s tallest recalled height minus the current measured height) exceeding 4 cm has been associated with: an odds ratio for VF of 2.8 (95% CI ) in the Study of Osteoporotic Fractures 2.9 (95% CI ) for women who screened for the Fracture Intervention Trial In the placebo arm of the Vertebral Efficacy with Risedronate Therapy studies, height loss over three years of > 4.0 cm (1.57 inches) had an odds ratio of 20.6 for incident vertebral fractures (95% CI 9, 45.8) while >2 cm (~0.8 inch) height loss had sensitivity of 35.5% for picking up new VF and specificity of 93.6%. Ettinger et al. JBMR 1992; Vogt et al Mayo Clin Proc 2000; Siminoski Osteoporos Int 2005


43 Meta-Analysis Effect of Calcium Supplementation on Myocardial Infarction Bolland M J et al. BMJ 2010; by British Medical Journal Publishing Group
44 Recommendations -Monitoring Consider serial bone mineral density testing Consider annual serum 25OH vitamin D measurements Assessment of incident fragility fracture Annual height measurement Assessment of medication compliance
45 LOW RISK Postmenopausal women and men 50 years: Pharmacologic Recommendations alendronate for 7.5 mg or more prednisone daily OR risedronate for 7.5 mg or more prednisone daily OR Zoledronic acid for 7.5 mg or more prednisone daily starting glucocorticoid therapy with an anticipated duration of 3 3 months OR prevalent glucocorticoid therapy of 3 months duration Low risk -FRAX 10 year major osteoporotic fracture risk <10%
46 MEDIUM RISK Postmenopausal women and men 50 years Pharmacologic Recommendations alendronate for any dose of glucocorticoids OR risedronate for any dose of glucocorticoids OR zoledronic acid for 7.5mg or more prednisone daily starting glucocorticoid therapy with an anticipated duration of 3 3 months OR prevalent glucocorticoid therapy of 3 months duration Medium risk -FRAX 10 year major osteoporotic fracture risk 10-20%
47 HIGH RISK Postmenopausal women and men 50 years Pharmacologic Recommendations alendronate for any dose of glucocorticoids risedronate for any dose of glucocorticoids zoledronic acid for any dose of glucocorticoids teriparatide for any dose of glucocorticoids duration > 1 month For high risk patients- any anticipated duration justifies initiating prescription therapy; for prednisone duration < 1 month, teriparatide recommended for 5 mg daily and higher High risk -FRAX 10 year major osteoporotic fracture risk >20% or prevalent fracture
48 Premenopausal Patients The panel felt that there was limited data on premenopausal patients Following recommendations are for those with a history of prevalent fracture Absence of recommendation does not equal no treatment for this population
49 Premenopausal non-child child-bearing potential women and men <50 years with history of fragility fracture Anticipated duration glucocorticoid >1 month and < 3 months alendronate if prednisone 5 mg daily or more risedronate if prednisone 5 mg daily or more zoledronic acid if prednisone 7.5 mg daily or more Anticipated duration glucocorticoid 3 months alendronate risedronate zoledronic acid teriparatide
50 Premenopausal women of child bearing potential with prior fragility fracture For those with an anticipated duration of >3 months or 3 months of prevalent glucocorticoid use alendronate if prednisone 7.5 mg daily or more OR risedronate if prednisone 7.5 mg daily or more OR teriparatide if prednisone 7.5 mg daily or more
51 Teriparatide or Alendronate in Glucocorticoid Induced Osteoporosis 428 men and women age (ave 57 yr) 80% women, 70% Caucasian Randomized to 20 mcg daily teriparatide or alendronate 10 mg daily Prednisone 5 mg/d for at least 3 months immediately prior to the start of the study (median dose about 7.5/duration years) T score of -2.0 at hip or spine or T-1.0 T and a fragility fracture 75% with rheumatologic disorders, 14% with respiratory Saag KG et al. NengJMed 2007;357:
52 Percent Change in Mean Bone Mineral Density at the Lumbar Spine and Total Hip from Baseline to 18 Months or the Last Measurement At 18 months. 10 new VF in the ALN arm vs 1 in the Teriparatide (p=0.004) Saag KG et al. N Engl J Med 2007;357:
53 Zoledronic acid and risedronate in the prevention and treatment of glucocorticoid-induced osteoporosis (HORIZON) 833 men and women 7.5 mg daily of prednisolone with anticipated duration of at least 12 months Treatment (n=545) and prevention subgroups (n=288) 68% female (approx 66% postmenopausal) BMD treatment group T -1.37, prevention T-0.93T Mostly rheumatologic disorders (41% RA)
54 Zoledronic acid vs Risedronate Reid et al; Lancet 2009
55 Bone Resorption is Dependent on RANK Ligand, the Primary Mediator of Osteoclast Activity RANK Ligand is Essential for Osteoclast Formation, Function and Survival CFU-M RANKL RANK Pre-Fusion Osteoclast Growth Factors Hormones Cytokines Osteoblast Multinucleated Osteoclast Activated Osteoclast Bone Adapted from Boyle WJ, et al. Nature. 2003;423: CFU-M = colony forming unit macrophage


56 Proposed Mechanism of Action for Denosumab RANKL RANK OPG denosumab CFU-M Pre-Fusion Osteoclast Growth Factors Hormones Cytokines Multinucleated Osteoclast Osteoclast Osteoblast Lineage Bone CFU-M = colony forming unit macrophage
57 Percent Changes in Bone Mineral Density Cummings SR et al. N Engl J Med 2009;361:

58 Adverse Events Cummings SR et al. N Engl J Med 2009;361:
59 Differences from 2001 to 2010 Expanded recommendations for counseling and monitoring Updated pharmacologic recommendations Delineated for postmenopausal women and men over age 50 years, premenopausal women not of childbearing potential and men under the age of 50 years with a history of a fragility fracture, and premenopausal women of childbearing potential with a history of a fragility fracture. The newer therapies zoledronic acid and teriparatide are now recommended along with alendronate and risedronate for the treatment of GIOP, while the previously included therapies estrogen replacement and testosterone are no longer endorsed. Recommendations now guided by patient s s overall clinical risk instead of T-scores T alone
60 Counsel and assess risk factors those those starting or on prevalent glucocorticoid therapy (table 2) * For low and medium risk patients recommendations are for an anticipated or prevalent duration of 3 months glucocorticoids Determine Patient Risk Category (figure 1a-d and table 1) Low Risk*- Alendronate, Risedronate or Zoledronic acid for those on 7.5 mg daily glucocorticoids Medium Risk*- Alendronate and risedronate for any dose glucocorticoids and zoledronic acid for 7.5 mg daily glucocorticoids High Risk- Alendronate, risedronate, zoledronic acid for any dose or duration of glucocorticoids, and teriparatide for 5 mg or more prednisone daily duration 1 month or less and for any dose of glucocorticoids with a duration greater than 1 month Monitor patients on prevalent glucocorticoid therapy (table 3)
61 Approach to premenopausal women and men under age 50 years starting or on glucocorticoid therapy
62
63 GIOP The Data-free Zone Indications for Therapy Premenopausal women? Children? Surveillance Frequency of DXA? Utility of bone biomarkers? Duration of therapy Rx after teriparatide? Persistence of Rx after steroid discontinued? Drug Holidays?
64 PERSPECTIVE JBMR Uncertainties in the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis Professional Practice Committee of the American Society for Bone and Mineral Research We discuss several patient scenarios for which the new treatment [2010 ACR] guidelines do not apply, or for which our committee interprets existing literature differently and suggests an alternative approach. Karen E Hansen, H Alexander Wilson, Carol Zapalowski, Howard A Fink, Salvatore Minisola, and Robert A Adler Journal of Bone and Mineral Research, Vol. 26, No. 9, September 2011, pp
65 Treatment of Postmenopausal Women and Men Over Age 50 ASBMR PPC: Low risk Medium risk High risk Prednisone <7.5 mg/d: If no therapy given, monitor closely for prevalent fracture and decline in BMD Prednisone 7.5 mg/day: Bisphosphonates Bisphosphonate Bisphosphonate or teriparatide COMPARISON to ACR: Agreement JBMR: 26 (9), ACR recommended zoledronate only in patients taking 7.5 mg of prednisone daily ACR recommended teriparatide only in patients taking glucocorticoids >1 month, or 5 mg daily for <1 month
66 Treatment of Premenopausal Infertile Women and Men Under Age 50 ASBMR PPC: Prevalent fracture No prevalent fracture Consider therapy if Z-score 2.0 or significant decline in BMD related to glucocorticoid therapy Prednisone 3 months Bisphosphonate Prednisone >3 months Bisphosphonate or teriparatide COMPARISON to ACR: ACR committee found inadequate data for this subgroup ACR committee recommended zoledronate only if prednisone dose 7.5 mg/d Agreement JBMR: 26 (9),
67 Treatment of Premenopausal Fertile Women ASBMR PPC: Prevalent fracture No prevalent fracture Consider therapy if Z-score 2.0 or lower, or significant decline in BMD related to ongoing glucocorticoid therapy COMPARISON to ACR: ACR committee found inadequate data for this subgroup Prednisone 3 months Little data to support therapy Agreement Prednisone >3 months Preference for shortacting drugs like teriparatide or denosumab instead of bisphosphonates No consensus if prednisone dose <7.5 mg/d; alendronate, risedronate, or zoledronate (not teriparatide) if prednisone dose 7.5 mg/d JBMR: 26 (9),
68 GIOP 2011 New Treatment Strategies How is osteoporosis risk best assessed? What can be done to prevent and treat GIOP? What is being done? How can we improve quality?
69 Rate of treatment Changing Patterns of GIOP Rx- US 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% HRT + Bone Rx among New Glucocorticoid Users (n = 5,471) p < 0.01 for all comparisons % 41% 33% 23% 14% 9% Men Women < 50 Women 50+ Curtis JR. Arth Rheum 2005;52:2485
70 GIOP Treatment Rates by Specialist MEDCO (n = 106K steroid users) Treatment Prescriber Specialty N (%) OR (95% CI) Internal Medicine 5,053 (25.1) Referent Rheumatology 7,726 (32.1) 1.61 ( ) Gastroenterology 685 (18.4) 1.15 ( ) Nephrology 578 (20.1) 1.36 ( ) Pulmonology 1,351 (27.7) 1.35 ( ) Other 5,710 (17.4) 0.78 ( ) Outman R. ASBMR, 2010
71 GIOP 2011 New Treatment Strategies What effects do glucocorticoid patterns of use have on osteoporosis risk? How is osteoporosis risk best assessed? What can be done to prevent and treat GIOP? What is being done? How can we improve quality?
72 UAB GIOP Group RCT Study Design Aetna U.S. Healthcare Population Doctors Prescribing Steroids High-risk Steroid Users Control Arm (n = 75) Unrelated CME Module Intervention Arm (n = 75) Internet GIOP Intervention Baseline DXA Screening and Rx Rate Follow up DXA Screening and Rx Rate Curtis, JR, Arch Int Med 2007; 167:591
73 GIOP Internet Intervention Access via e Tailored presentation Case-based interactive learning Personal data feedback using Achievable Benchmark of Care (ABC ) Improvement toolbox Printable CME certificate Continued exposure to combat decay Kiefe C. JAMA 285(22): , 2001.
74 GIOP Group RCT Results Intent-To-Treat Intervention (n = 76 docs) % Receipt Control (n = 73 docs) p-value BMD NS Prescription Rx NS Per Protocol* (n = 27 (n = 18 docs) p-value docs) BMD BisphosphonateRx BMD or Rx * Completed all 3 modules Curtis, JR, Arch Int Med 2007; 167:591
,")
75 Self Scheduling of DXAs Results From Kaiser NW Warriner A, ASBMR (Plenary Poster FR0325), 2011
 Risedronate (n = 314) 0.2 0.0 0 180 360 540 720 900 1080 Days of Filled Bisphosphonate Rx Curtis J.")
76 Poor Adherence to Bisphosphonates Among Glucocorticoid Users 1.0 % Remaining on Therapy Alendronate (n = 609) Risedronate (n = 314) Days of Filled Bisphosphonate Rx Curtis J. Osteoporosis Int, 2006; 17:126
77 Sclerostin is a protein Sclerostin produced by osteocytes and functions to inhibit bone formation by b binding to LRP5 and inhibiting Wnt signaling Sclerosteosis is an autosomal recessive trait resulting from a deficiency of sclerostin which is an inhibitor of Wnt signaling heterozygous carriers have increased bone mass with few sequalae Homozygous individuals have high bone mass Z-scores often >+7.0. In a study of a monoclonal antibody against sclerostin given to cynomolgus monkeys Increased BMD Increased osteoblast mediated bone formation Doubled skeletal strength Ominsky et al. JBMR 2010
78 Odanacatib Cathepsin K inhibitor CatK, a cysteine protease, is expressed primarily in osteoclasts degrades type I collagen- Inhibits matrix dissolution but not viability of the osteoclast 2 year phase IIb study of 399 subjects randomized to placebo or one of 4 doses The 50 mg dose was associated with 5.7% increase in LS spine and 4.1% increase in total hip compared to placebo Safety profile similar to placebo Bone et al. JBMR 2010
 with attempts to disassociate properties- Selected Glucocorticoid Receptors Agonists (SEGRAs) Bledsoe RK, Cell 110:93,2002 Dissociated Glucocorticoid Receptor Agonists")
79 Building Designer Steroids Crystal structure of GR ligand binding domain discovered Trans-activation toxicity Trans-repression antiinflammatory effects Glucocorticoid Mimetics (GCM) with attempts to disassociate properties- Selected Glucocorticoid Receptors Agonists (SEGRAs) Bledsoe RK, Cell 110:93,2002 Dissociated Glucocorticoid Receptor Agonists (DAGR)
8/6/2018. Glucocorticoid induced osteoporosis: overlooked and undertreated? Disclosure. Objectives. Overview
 Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
Advanced medicine conference. Monday 20 Tuesday 21 June 2016
 Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment. William D. Leslie, MD MSc FRCPC
 Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
An Update on Osteoporosis Treatments
 An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Page 1. Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in ? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Osteoporosis: current treatment and future prospects. Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus
 Osteoporosis: current treatment and future prospects Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus Disclosures Consultancy and speaking fees for Gilead, related to development
Osteoporosis: current treatment and future prospects Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus Disclosures Consultancy and speaking fees for Gilead, related to development
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Etiology. Presenter Disclosure Information. Epidemiology.
 12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
Osteoporosis Physician Performance Measurement Set. October 2006
 American Academy of Family Physicians/American Academy of Orthopaedic Surgeons/American Association of Clinical Endocrinologists/American College of Rheumatology/The Endocrine Society/Physician Consortium
American Academy of Family Physicians/American Academy of Orthopaedic Surgeons/American Association of Clinical Endocrinologists/American College of Rheumatology/The Endocrine Society/Physician Consortium
Page 1. Updates in Osteoporosis. I have no conflicts of interest. What is osteoporosis? What s New in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
SpongeBone Menopants*
 SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
Updates in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Osteoporosis Update. Greg Summers Consultant Rheumatologist
 Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Clinical Specialist Statement Template
 Clinical Specialist Statement Template Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can
Clinical Specialist Statement Template Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can
Healthy Bones: Osteoporosis Management. Laurel Short, MSN, FNP-C
 Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays. Suzanne Morin MD FRCP FACP McGill University May 2014
 Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Using the FRAX Tool. Osteoporosis Definition
 How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
Page 1. Current and Emerging Strategies What s New in Osteoporosis. Osteoporosis. What is Osteoporosis? Traditional Risk Factors for Fracture
 Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Disclosures. Diagnostic Challenges in Osteoporosis: Whom To Treat 9/25/2014
 Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Page 1. New Developments in Osteoporosis. What s New in Osteoporosis
 New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
FRAX Based Lebanese Osteoporosis Guidelines Second Update for Lebanese Guidelines for Osteoporosis Assessment and Treatment
 These guidelines are endorsed by the following Lebanese Scientific Societies and Associations: Lebanese Society of Endocrinology Diabetes and Lipids, Lebanese Society of Rheumatology, Lebanese Society
These guidelines are endorsed by the following Lebanese Scientific Societies and Associations: Lebanese Society of Endocrinology Diabetes and Lipids, Lebanese Society of Rheumatology, Lebanese Society
Assessment and Treatment of Osteoporosis Professor T.Masud
 Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
Hot Topics in Bone Disease in 2017: Building Better Bones Breaking News in Osteoporosis
 Hot Topics in Bone Disease in 2017: Building Better Bones Breaking News in Osteoporosis Aromatase Inhibitor-Induced Bone Loss in Early Breast Cancer Rachel Pessah-Pollack, M.D., F.A.C.E. Mount Sinai School
Hot Topics in Bone Disease in 2017: Building Better Bones Breaking News in Osteoporosis Aromatase Inhibitor-Induced Bone Loss in Early Breast Cancer Rachel Pessah-Pollack, M.D., F.A.C.E. Mount Sinai School
Osteoporosis update. Dr. Claire Vandevelde Consultant Rheumatologist, LTHT
 Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Controversies in Osteoporosis Management
 Controversies in Osteoporosis Management 2018 Northwest Rheumatism Society Meeting Portland, OR April 28, 2018 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Institute
Controversies in Osteoporosis Management 2018 Northwest Rheumatism Society Meeting Portland, OR April 28, 2018 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Institute
Current and Emerging Approaches for Osteoporosis
 Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Current Issues in Osteoporosis
 Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017
 Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Assessment and management of glucocorticoid-induced osteoporosis
 PRESCRIBING IN PRACTICE n Assessment and management of glucocorticoid-induced osteoporosis Gerald Tracey and Tehseen Ahmed Glucocorticoid-induced osteoporosis (GIO) is the most prevalent form of secondary
PRESCRIBING IN PRACTICE n Assessment and management of glucocorticoid-induced osteoporosis Gerald Tracey and Tehseen Ahmed Glucocorticoid-induced osteoporosis (GIO) is the most prevalent form of secondary
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Horizon Scanning Centre March Denosumab for glucocorticoidinduced SUMMARY NIHR HSC ID: 6329
 Horizon Scanning Centre March 2014 Denosumab for glucocorticoidinduced osteoporosis SUMMARY NIHR HSC ID: 6329 This briefing is based on information available at the time of research and a limited literature
Horizon Scanning Centre March 2014 Denosumab for glucocorticoidinduced osteoporosis SUMMARY NIHR HSC ID: 6329 This briefing is based on information available at the time of research and a limited literature
Osteoporosis Physician Performance Measurement Set. October 2006 Coding Reviewed and Updated November 2009
 American Academy of Family Physicians/American Academy of Orthopaedic Surgeons/American Association of Clinical Endocrinologists/American College of Rheumatology/The Endocrine Society/Physician Consortium
American Academy of Family Physicians/American Academy of Orthopaedic Surgeons/American Association of Clinical Endocrinologists/American College of Rheumatology/The Endocrine Society/Physician Consortium
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Biochemical Markers of Bone Turnover: Definitions and Recommendations for Monitoring Therapy Learning Objectives for Biochemical
Annual Rheumatology & Therapeutics Review for Organizations & Societies Biochemical Markers of Bone Turnover: Definitions and Recommendations for Monitoring Therapy Learning Objectives for Biochemical
Chau Nguyen, D.O. Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences
 Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Osteoporosis Screening and Treatment in Type 2 Diabetes
 Osteoporosis Screening and Treatment in Type 2 Diabetes Ann Schwartz, PhD! Dept. of Epidemiology and Biostatistics! University of California San Francisco! October 2011! Presenter Disclosure Information
Osteoporosis Screening and Treatment in Type 2 Diabetes Ann Schwartz, PhD! Dept. of Epidemiology and Biostatistics! University of California San Francisco! October 2011! Presenter Disclosure Information
Osteoporosis Management
 Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
Osteoporosis as a Focus for Practice Improvement
 Osteoporosis as a Focus for Practice Improvement Karen E. Hansen, M.D. Assistant Professor of Medicine Rheumatology and Endocrine Sections University of Wisconsin Madison, WI Postmenopausal Osteoporosis
Osteoporosis as a Focus for Practice Improvement Karen E. Hansen, M.D. Assistant Professor of Medicine Rheumatology and Endocrine Sections University of Wisconsin Madison, WI Postmenopausal Osteoporosis
NEW HORIZONS IN OSTEOPOROSIS THERAPY. Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN
 NEW HORIZONS IN OSTEOPOROSIS THERAPY Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN DISCLOSURES SUNDEEP KHOSLA, M.D. Investigator-initiated grant Merck No non-fda approved recommendations RISK ASSESSMENT
NEW HORIZONS IN OSTEOPOROSIS THERAPY Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN DISCLOSURES SUNDEEP KHOSLA, M.D. Investigator-initiated grant Merck No non-fda approved recommendations RISK ASSESSMENT
Page 1. Current and Emerging Strategies for Osteoporosis. Osteoporosis Warm-Up: Which of the Following is True?
 Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
2017 Santa Fe Bone Symposium McClung
 217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Upcoming Agents for Osteoporosis
 Upcoming Agents for Osteoporosis May 5, 2017 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Professorial Fellow, Institute of Health and Ageing Australian Catholic
Upcoming Agents for Osteoporosis May 5, 2017 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Professorial Fellow, Institute of Health and Ageing Australian Catholic
nogg Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK
 nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Definition. Presenter Disclosure Information.
 4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
Osteoporosis Treatment Overview. Colton Larson RFUMS October 26, 2018
 Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis 2017 Breaking News. Julie L. Carkin, MD The Seattle Arthritis Clinic
 Osteoporosis 2017 Breaking News Julie L. Carkin, MD The Seattle Arthritis Clinic 1 Yes, Hopefully & No Anabolic Teriparatide Abaloparatide Romosozumab blosozumab Anti-catabolic Bisphosphonates Denosumab
Osteoporosis 2017 Breaking News Julie L. Carkin, MD The Seattle Arthritis Clinic 1 Yes, Hopefully & No Anabolic Teriparatide Abaloparatide Romosozumab blosozumab Anti-catabolic Bisphosphonates Denosumab
BAD TO THE BONE. Peter Jones, Rheumatologist QE Health, Rotorua. GP CME Conference Rotorua, June 2008
 BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
Executive Summary- Lebanese FRAX-Based Osteoporosis Guidelines 2013
 Executive Summary- Lebanese FRAX-Based Osteoporosis Guidelines 2013 Marlene Chakhtoura, MD, Rafic Baddoura, MD, MPH and Ghada El-Hajj Fuleihan, MD, MPH. On behalf of National Task Force for Osteoporosis
Executive Summary- Lebanese FRAX-Based Osteoporosis Guidelines 2013 Marlene Chakhtoura, MD, Rafic Baddoura, MD, MPH and Ghada El-Hajj Fuleihan, MD, MPH. On behalf of National Task Force for Osteoporosis
A KL/R / AN A K/O / P O G G
 Outline and New Treatments on the Horizon Steven R. Cummings, MD CPMC and UCSF San Francisco Coordinating Center Support from Lilly and Amgen New treatments, new mechanisms of action Cathepsin K inhibition
Outline and New Treatments on the Horizon Steven R. Cummings, MD CPMC and UCSF San Francisco Coordinating Center Support from Lilly and Amgen New treatments, new mechanisms of action Cathepsin K inhibition
BAD for the Bones Skeletal Woes from Commonly Prescribed Medications
 BAD for the Bones Skeletal Woes from Commonly Prescribed Medications A Case of Skeletal Cruelty Phenobarbitol Arimidex Heparin Jonathan Graf, MD Asst. Professor Medicine, UCSF Div. Rheumatology, SFGH Prednisone
BAD for the Bones Skeletal Woes from Commonly Prescribed Medications A Case of Skeletal Cruelty Phenobarbitol Arimidex Heparin Jonathan Graf, MD Asst. Professor Medicine, UCSF Div. Rheumatology, SFGH Prednisone
Osteoporosis Clinical Guideline. Rheumatology January 2017
 Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Osteoporosis - Pathophysiology and diagnosis. Bente L Langdahl Department of Endocrinology Aarhus University Hospital Aarhus, Denmark
 Osteoporosis - Pathophysiology and diagnosis Bente L Langdahl Department of Endocrinology Aarhus University Hospital Aarhus, Denmark Objective General knowledge about osteoporosis Optimise your protocols
Osteoporosis - Pathophysiology and diagnosis Bente L Langdahl Department of Endocrinology Aarhus University Hospital Aarhus, Denmark Objective General knowledge about osteoporosis Optimise your protocols
New Therapeutic Directions: Osteoanabolic and Antiresorptive Therapy in Combination Therapy and in Sequence
 New Therapeutic Directions: Osteoanabolic and Antiresorptive Therapy in Combination Therapy and in Sequence John P. Bilezikian, MD, PhD(hon), MACE Silberberg Professor of Medicine Vice-Chair for International
New Therapeutic Directions: Osteoanabolic and Antiresorptive Therapy in Combination Therapy and in Sequence John P. Bilezikian, MD, PhD(hon), MACE Silberberg Professor of Medicine Vice-Chair for International
Osteoporosis Management in Older Adults
 Osteoporosis Management in Older Adults Angela M Cheung, MD, PhD, FRCPC, CCD Professor of Medicine, University of Toronto Disclosures Relationship with Commercial Entities: Honoraria from: Amgen, Eli Lilly,
Osteoporosis Management in Older Adults Angela M Cheung, MD, PhD, FRCPC, CCD Professor of Medicine, University of Toronto Disclosures Relationship with Commercial Entities: Honoraria from: Amgen, Eli Lilly,
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
BREAST CANCER AND BONE HEALTH
 BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
Pharmacy Management Drug Policy
 Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Bone Mass Measurement BONE MASS MEASUREMENT HS-042. Policy Number: HS-042. Original Effective Date: 8/25/2008
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Drug Intervals (Holidays) with Oral Bisphosphonates
 with Oral Bisphosphonates") Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Meta-analysis: analysis:
 1 Diabetes and TZDs: Risk Factors for Fracture Ann Schwartz, PhD Dept. of Epidemiology and Biostatistics University of California San Francisco July 2010 Osteoporosis CME Presenter Disclosure Information
1 Diabetes and TZDs: Risk Factors for Fracture Ann Schwartz, PhD Dept. of Epidemiology and Biostatistics University of California San Francisco July 2010 Osteoporosis CME Presenter Disclosure Information
Effective Health Care
 Number 12 Effective Health Care Comparative Effectiveness of Treatments To Prevent Fractures in Men and Women With Low Bone Density or Osteoporosis Executive Summary Background Osteoporosis is a systemic
Number 12 Effective Health Care Comparative Effectiveness of Treatments To Prevent Fractures in Men and Women With Low Bone Density or Osteoporosis Executive Summary Background Osteoporosis is a systemic
Differentiating Pharmacological Therapies for Osteoporosis
 Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Pathophysiology of Postmenopausal & Glucocorticoid Induced Osteoporosis. March 15, 2016 Bone ECHO Kate T Queen, MD
 Pathophysiology of Postmenopausal & Glucocorticoid Induced Osteoporosis March 15, 2016 Bone ECHO Kate T Queen, MD Review: normal bone formation Bone Modeling Remodeling Peak Bone Mass Maximum bone mass
Pathophysiology of Postmenopausal & Glucocorticoid Induced Osteoporosis March 15, 2016 Bone ECHO Kate T Queen, MD Review: normal bone formation Bone Modeling Remodeling Peak Bone Mass Maximum bone mass
HRT and Risedronate Combined Anabolic and Antiresorptive Therapy
 Optimizing Combined and Sequential Osteoanabolic and Antiresorptive Therapy Benjamin Leder, M.D. Endocrine Unit Massachusetts General Hospital Boston, MA Antiresorptive and Osteoanabolic Therapies Increase
Optimizing Combined and Sequential Osteoanabolic and Antiresorptive Therapy Benjamin Leder, M.D. Endocrine Unit Massachusetts General Hospital Boston, MA Antiresorptive and Osteoanabolic Therapies Increase
7/5/2016. We need drugs that. Disclosures. New Osteoporosis Treatments. What we have today. Maintain or promote bone formation
 New Osteoporosis Treatments Disclosures Mary L. Bouxsein, PhD Department of Orthopedic Surgery Harvard Medical School, Boston, MA Advisory Board: Research funding: Merck, Eli Lilly, Radius Merck, Amgen
New Osteoporosis Treatments Disclosures Mary L. Bouxsein, PhD Department of Orthopedic Surgery Harvard Medical School, Boston, MA Advisory Board: Research funding: Merck, Eli Lilly, Radius Merck, Amgen
Treatment of Osteoporosis: IHFD 6 th March 2015
 Treatment of Osteoporosis: IHFD 6 th March 2015 Dr. John J. Carey, MB, MS, FACR, FRCPI, CCD. Consultant Physician Galway University Hospitals Associate Professor in Medicine, NUIG, Galway Vice-President
Treatment of Osteoporosis: IHFD 6 th March 2015 Dr. John J. Carey, MB, MS, FACR, FRCPI, CCD. Consultant Physician Galway University Hospitals Associate Professor in Medicine, NUIG, Galway Vice-President
Update on Osteoporosis 2016
 WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
Outline. Switching treatment. Evidence from randomized trials. The effects of switching 7/8/2016. When and for whom? Steven Cummings, MD
 Outline Switching treatment When and for whom? Steven Cummings, MD Focus on switching from alendronate or risedronate Evidence about the effects of switching on BMD Purposes of switching Symptoms Poor
Outline Switching treatment When and for whom? Steven Cummings, MD Focus on switching from alendronate or risedronate Evidence about the effects of switching on BMD Purposes of switching Symptoms Poor
Use of DXA / Bone Density in the Care of Your Patients. Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist
 Use of DXA / Bone Density in the Care of Your Patients Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist Important Websites Resources for Clinicians and Patients www.nof.org www.iofbonehealth.org
Use of DXA / Bone Density in the Care of Your Patients Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist Important Websites Resources for Clinicians and Patients www.nof.org www.iofbonehealth.org
Osteoporosis Update. Case 2. Case 1: Monday morning, 8:15
 Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Osteoporosis. Treatment of a Silently Developing Disease
 Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary
 Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
Osteoporosis - New Guidelines. Michelle Glass B.Sc. (Pharm) June 15, 2011
 June 15, 2011") Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
Bisphosphonate treatment break
 Bulletin 110 December 2015 Bisphosphonate treatment break Bisphosphonates have been widely used in the treatment of osteoporosis with robust data demonstrating efficacy in fracture risk reduction over
Bulletin 110 December 2015 Bisphosphonate treatment break Bisphosphonates have been widely used in the treatment of osteoporosis with robust data demonstrating efficacy in fracture risk reduction over
AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents
 AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents Injectable Osteoporosis Agents Forteo (teriparatide); zoledronic acid Prolia (denosumab)] Authorization guidelines For
AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents Injectable Osteoporosis Agents Forteo (teriparatide); zoledronic acid Prolia (denosumab)] Authorization guidelines For
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Calcium, Vitamin D and Bisphosphonates: Disclosures. Benefits, Risks and Drug Holiday. Calcium YES or NO? Calcium Bad News!!
 Calcium, Vitamin D and Bisphosphonates: Benefits, Risks and Drug Holiday Disclosures I am disclosing financial relationships as follows: Global Advisory Boards: Amgen, Lilly, Merck, Novartis Research grants:
Calcium, Vitamin D and Bisphosphonates: Benefits, Risks and Drug Holiday Disclosures I am disclosing financial relationships as follows: Global Advisory Boards: Amgen, Lilly, Merck, Novartis Research grants:
Men and Osteoporosis So you think that it can t happen to you
 Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Fragile Bones and how to recognise them. Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey
 Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Disclosures D. Black. Bisphosphonates: Background, Efficacy and Recent Controversies. Page 1. Research Funding: Novartis, Merck
 Bisphosphonates: Background, Efficacy and Recent Controversies Disclosures D. Black Research Funding: Novartis, Merck Dennis M. Black, PhD Consulting: Amgen, Lilly, Zosano, Nycomed Dept. of Epidemiology
Bisphosphonates: Background, Efficacy and Recent Controversies Disclosures D. Black Research Funding: Novartis, Merck Dennis M. Black, PhD Consulting: Amgen, Lilly, Zosano, Nycomed Dept. of Epidemiology
Osteoporosis and Lupus. Andrew Ruthberg, MD University Rheumatologists
 Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don