Lewy Body Dementia: Diagnosis, Management and Future Directions
|
|
|
- Ronald Justin Daniels
- 6 years ago
- Views:
Transcription





1 Lewy Body Dementia: Diagnosis, Management and Future Directions Bradley F. Boeve, M.D. Divisions of Behavioral Neurology and Movement Disorders Center for Sleep Medicine Department of Neurology Mayo Clinic Rochester, Minnesota


2 Disclosures Financial/Other Investigator for clinical trials sponsored by Cephalon, Inc., Allon Pharmaceuticals, and GE Healthcare Royalties from the publication of a book entitled Behavioral Neurology Of Dementia (Cambridge Medicine, 2009) Honoraria from the American Academy of Neurology Research support from the NIA, NINDS, Alzheimer's Association, and Mangurian Foundation Off-label and/or Investigational Use Will discuss use of many medications which are not FDA-approved for the indications to be reviewed

3 Dementia with Lewy Bodies/Lewy Body Dementia Outline Nomenclature Diagnostic Features Management Options Future Directions
4 The Syndrome Dementia With Lewy Bodies Nomenclature Dementia with Lewy bodies (DLB)/Lewy body dementia (LBD) Clinically probable DLB Clinically possible DLB The Disease Lewy body disease (LBD) brainstem limbic neocortical
5 Clinical Features and Diagnostic Criteria Core features Dementia syndrome plus: Spontaneous parkinsonism (unrelated to drugs) Recurrent fully formed visual hallucinations Fluctuating arousal/cognition 2 or 3 of above = clinically probable DLB 1 of above = clinically possible DLB McKeith et al, Neurology 1996 McKeith et al, Neurology 1999 McKeith et al, Neurology 2005
6 Clinical Features and Diagnostic Criteria Suggestive features (one or more present in addition to one or more core features is sufficient for a diagnosis of probable DLB, and in the absence of any core features is sufficient for possible DLB) REM sleep behavior disorder (which may precede onset of dementia by several years) Severe neuroleptic sensitivity Abnormal (low uptake) in basal ganglia on SPECT dopamine transporter scan Boeve et al, Neurology 1998 McKeith et al, Neurology 2005
7 Clinical Features and Diagnostic Criteria Ferman et al, Neurology 2012 Core features Dementia syndrome plus: Spontaneous parkinsonism (unrelated to drugs) Recurrent fully formed visual hallucinations Fluctuating arousal/cognition RBD Any 2 of the following c/w DLB RBD plus 1 of the other features - >90% accurate

8 Video Example - RBD
9 Hypersomnia The data confirms subjective (ESS) and objective evidence of EDS (MSLT) is present in DLB and not in AD. Ferman et al, AAN 2010



10 Neuropsychiatric Features The most frequent neuropsychiatric features in DLB: Visual hallucinations Illusions Delusions (including Capgras syndrome) Depression Apathy


11 Neuropsychological Features Ferman et al, Neurology 1999 Ferman et al, Clin Neuropsych 2006 Cognitive Domains Learning & Memory Language Executive Functions Visuospatial Functions Impairment 0 to ++ 0 to + + to to +++
12 Neuropsychological Features Evaluation 2 14 AD Impaired on: Memory measures BNT and/or Cat Flu 2 0 DRS WMS- LM WMS- VR AVLT-PR BNT COWAT CAT FLU TMT-A TMT-B WAIS- DS WAIS- BD WAIS- PC REY-O Global Memory Language Attention/Executive Visuospatial Evaluation 1 DLB Impaired on: TMT, Dig Symbol WAIS-BD, -PC Rey-O CFT 0 DRS WMS-LM WMS-VR AVLT-PR BNT COWAT CAT FLU TMT-A TMT-B WAIS- DS WAIS- BD WAIS- PC Global Memory Language Attention/Executive Visuospatial REY-O Ferman et al, Neurology 1999 Ferman et al, Clin Neuropsych 2006
13 Please draw this figure: Dementia With Lewy Bodies Neuropsychological Features Please draw this figure: Draw a clock showing the time of 11:10:



14 Neuroimaging Features MRI Normal AD DLB normal hippocampi hippocampal atrophy normal hippocampi


15 Neuroimaging Features MRI VBM Whitwell et al, Brain 2007

16 Neuroimaging Features FDG-PET Normal

17 Neuroimaging Features FDG-PET Kantarci et al, Neurobiol Aging 2011 AD Posterior cingulate Temporoparietal Frontal DLB Occipital

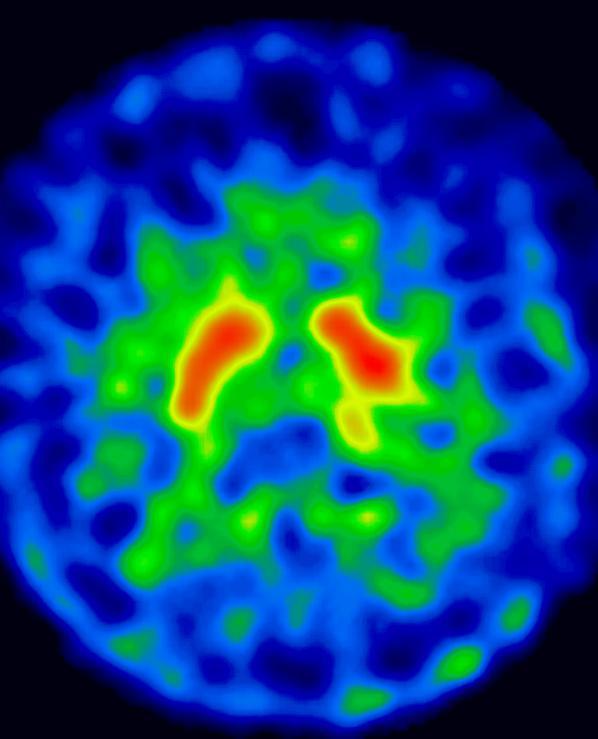
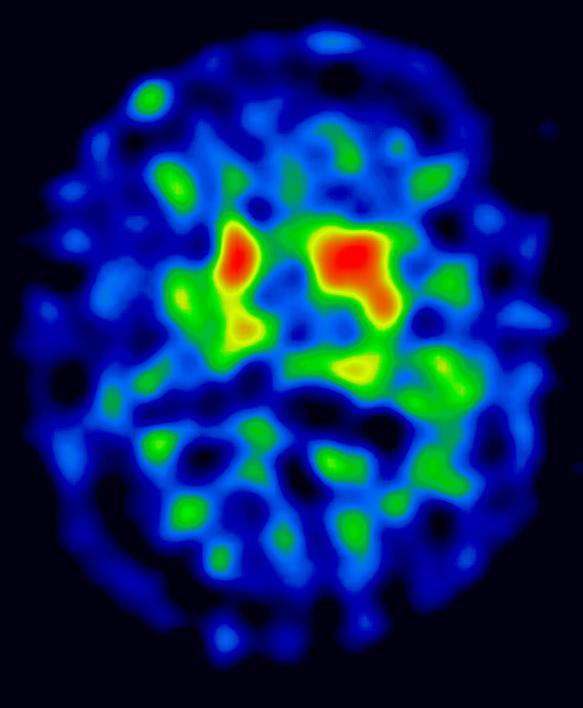
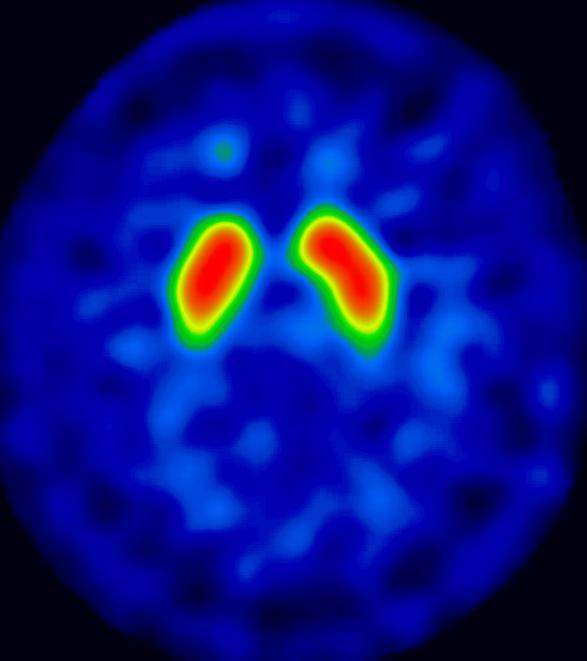
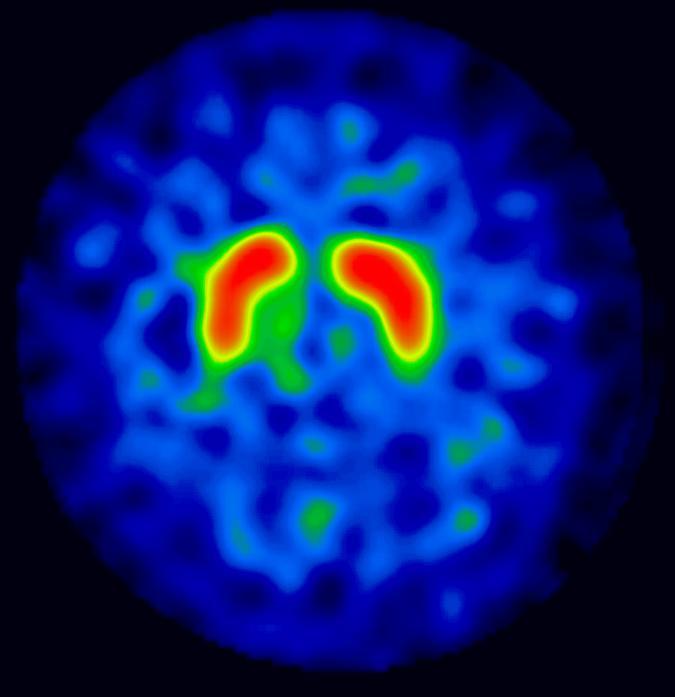
18 Neuroimaging Features - DaTscan caudate Ioflupane putamen DaTscan - meaures nigrostriatal uptake of dopamine transporter in the caudate and putamen Normal

19 Neuroimaging Features - DaTscan AD DLB


20 Neuropathologic Features A B C A Ach DA 5-HT HCT-1 Ach? (RBD) B C


21 Neuropathologic Features H&E -synuclein Photomicrographs courtesy Dennis Dickson, M.D.
22 Clinical Tools - ESS
23 Clinical Tools - MSQ 1. Have you ever seen the patient appear to act out your dreams while sleeping? (punched or flailed arms in the air; shouted or screamed) SN: 100% SP: 97% Olmsted County

24 Clinical Tools - MFS Nl AD DLB Ferman et al, Neurology 2004


25 Clinical Tools - Friedman Friedman Palate Position Friedman Tonsil Grading Friedman et al, Laryngoscope 2004;114:
26 Management Consider symptoms as they relate to: cognitive impairment neuropsychiatric features motor features sleep disorders autonomic dysfunction Ask patient/family to prioritize the most troublesome issues they seek to change Boeve BF. AAN Continuum 2004

27 Management Cognitive impairment Varying degrees of memory impairment Verbal blocking Executive dysfunction Bradyphrenia Spatial/geographic disorientation Visual misidentification Fluctuations Management Education and counseling Therapies: Aricept, Razadyne, Exelon Sinemet, Mirapex Provigil, Nuvigil, methylphenidate, Adderall
28 Cognition issues Dementia With Lewy Bodies Brain-Behavior Relationships Mainly due to reduced Ach Reductions in other brain chemicals contributes to cognitive impairment Some degree of neuron cell loss too A A B C HCT B Ach DA 5-HT C

29 Management Neuropsychiatric features Visual hallucinations Illusions Delusions Capgras syndrome Depression Anxiety Agitation/aggressive behavior Management Education and counseling Therapies: Aricept, Razadyne, Exelon SSRIs, melatonin Seroquel, Zyprexa Provigil, Nuvigil, methylphenidate, Adderall NO HALDOL
30 Brain-Behavior Relationships Neuropsychiatric issues Hallucinations and delusions related to DA imbalance Depression related to low 5-HT Apathy many causes A B C A B Ach DA 5-HT C
31 Management Motor dysfunction Tremor Bradykinesia Rigidity Myoclonus Shuffling gait Stooped posture Difficulty with fine motor skills Masked facies Sialorrhea Management Education and counseling Therapies: Sinemet Mirapex, Requip, Neupro patch (when available) Clonazepam, Neurontin
32 Motor issues Dementia With Lewy Bodies Brain-Behavior Relationships The Parkinson s disease-like features (parkinsonism) primarily relate to the reduction in DA A A B C B DA C


33 Management Sleep disorders REM sleep behavior disorder Excessive daytime somnolence Insomnia Obstructive sleep apnea Central sleep apnea Restless legs syndrome Periodic limb movement in sleep Management Education and counseling Therapies: Clonazepam, Melatonin Provigil, Nuvigil, methylphenidate, Adderall Trazodone, Ambien, chloral hydrate nasal CPAP oxygen, temazepam Mirapex, Sinemet
 relates to changes in the dorsal pons Reduced DA and 5-HT also affects sleep A A B C HCT B DA 5-HT?")
34 Sleep issues Dementia With Lewy Bodies Brain-Behavior Relationships Daytime sleepiness, insomnia, and fragmented sleep relate in part to the loss in HCT Acting out dreams (RBD) relates to changes in the dorsal pons Reduced DA and 5-HT also affects sleep A A B C HCT B DA 5-HT? C

35 Management Autonomic dysfunction Orthostatic hypotension Impotence Urinary incontinence Constipation Management Education and counseling Therapies: Midodrine, Florinef, salt Viagra, etc. Enablex, Gelnique, Sanctura Senokot, MiraLAX

36 Autonomic issues Many autonomic changes related to changes in the spinal cord and peripheral nerves in and around the: heart stomach intestines bladder sex organs Dementia With Lewy Bodies Brain-Behavior Relationships
37 Management Initial evaluation Follow-up evaluation donepezil levodopa CPAP MMSE: 21 ESS: 14 MMSE: 28 ESS: 4 Boeve BF. AAN Continuum 2004
38 Initial evaluation Dementia With Lewy Bodies Management Follow-up evaluation donepezil levodopa modafinil MMSE: 7/30 STMS: 21/38 DRS: 52/144 ESS: 15 MMSE: 25/30 STMS: 31/38 DRS: 129/144 ESS: 6

39 Future Directions

40 Future Directions Braak et al, Cell Tiss Res 2004 Boeve BF. Ann NY Acad Sci 2010
41 Functioning Dementia With Lewy Bodies Future Directions Assessment Tools RBD onset MCI MPS DLB PD Age

42 Future Directions Boot et al, Ann Neurol 2012
43 Future Directions 15/44 subjects developed MCI/PD (14 MCI, 1 PD) HR 2.2 Boot et al, Ann Neurol 2012

44 Future Directions Iranzo et al, Lancet Neurol 2011
45 Future Directions Normal RBD RBD RBD Boeve et al, unpublished data


46 Functioning Dementia With Lewy Bodies Future Directions Assessment Tools RBD onset Delay the onset and slow the course of symptoms MCI MPS DLB PD Rx Age
47 Resources Lewy Body Dementia Association Please access this website and check it at least monthly, review the newsletter
48 Resources

49 Resources




50 Collaborators/Support Ronald Petersen, PhD, MD David Knopman, MD Daniel Drubach, MD Keith Josephs, MD Laura Allen, RN, CNP Sue Kennebeck, RN Angela Lunde, MA Tanis Ferman, PhD Glenn Smith, PhD Robert Ivnik, PhD Julie Fields, PhD John Lucas, PhD Cliff Jack, Jr., MD Kejal Kantarci, MD Val Lowe, MD Jennifer Whitwell, PhD David Jones, MD Mike Silber, MBBS Erik St. Louis, MD Maja Tippmann-Peikert Mithri Junna, MD Joseph Parisi, MD Dennis Dickson, MD Departments of Neurology, Psychiatry and Psychology, Diagnostic Radiology, Pathology and Laboratory Medicine, Community Internal Medicine, and Health Sciences Research, Mayo Clinic Rochester, Mayo Clinic Jacksonvile, and Mayo Clinic Scottsdale; Neuropathology Laboratory, Mayo Clinic Jacksonville; Mayo Alzheimer s Disease Research Center, Mayo Foundation; and M.H. Udall PD Center of Excellence Grant, Mayo Foundation Supported by grants AG006786, AG016574, and AG from the NIA; Mangurian Foundation
Comprehensive Approach to DLB Management
 Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Revised criteria for the clinical diagnosis of dementia with Lewy. Dementia with Lewy bodies. (Dementia with Lewy Bodies)
") Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Parkinson s Disease Initial Clinical and Diagnostic Evaluation. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
The Spectrum of Lewy Body Disease: Dementia with Lewy Bodies and Parkinson's Disease Dementia
 Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
Assessment Toolkits for Lewy Body Dementia
 Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Assistant Professor of Neurology and Psychiatry University of Colorado Denver Goals 1) What are the most common non-motor
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Assistant Professor of Neurology and Psychiatry University of Colorado Denver Goals 1) What are the most common non-motor
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
3/7/2017. Alzheimer s and Dementia Research: An Advanced Discussion. Alzheimer s and Dementia Research: An Advanced Discussion
 Alzheimer s and Dementia Research: An Advanced Discussion Brad Boeve, MD Department of Neurology Mayo Clinic Alzheimer s and Dementia Research: An Advanced Discussion Theoretical Constructs in Aging/Dementia
Alzheimer s and Dementia Research: An Advanced Discussion Brad Boeve, MD Department of Neurology Mayo Clinic Alzheimer s and Dementia Research: An Advanced Discussion Theoretical Constructs in Aging/Dementia
NON-AD DEMENTIAS: ALPHA-SYNUCLEINOPATHIES
 NON-AD DEMENTIAS: ALPHA-SYNUCLEINOPATHIES Bradley F. Boeve, MD Professor of Neurology Mayo Clinic Rochester, Minnesota Overview With the advent of α-synuclein immunocytochemistry, some of the Parkinson-plus
NON-AD DEMENTIAS: ALPHA-SYNUCLEINOPATHIES Bradley F. Boeve, MD Professor of Neurology Mayo Clinic Rochester, Minnesota Overview With the advent of α-synuclein immunocytochemistry, some of the Parkinson-plus
Non-Motor Symptoms of Parkinson s Disease
 Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
PARKINS ON CENTER. Parkinson s Disease: Diagnosis and Management. Learning Objectives: Recognition of PD OHSU. Disclosure Information
 OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
How to Diagnose Early (Prodromal) Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.
 Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.") How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia
 Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia Bradley F. Boeve, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Alzheimer s Disease
Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia Bradley F. Boeve, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Alzheimer s Disease
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Behavioral Aspects of Parkinson s Disease
 Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Joint Session with ACOFP and Mayo Clinic. Parkinson's Disease: 5 Pearls. Jay Van Gerpen, MD
 Joint Session with ACOFP and Mayo Clinic Parkinson's Disease: 5 Pearls Jay Van Gerpen, MD Parkinson s Disease: 5 Pearls J.A. van Gerpen, MD Sections of Movement Disorders and Clinical Neurophysiology
Joint Session with ACOFP and Mayo Clinic Parkinson's Disease: 5 Pearls Jay Van Gerpen, MD Parkinson s Disease: 5 Pearls J.A. van Gerpen, MD Sections of Movement Disorders and Clinical Neurophysiology
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
ASYMMETRICAL CORTICAL DEGENERATIVE SYNDROMES
 ASYMMETRICAL CORTICAL DEGENERATIVE SYNDROMES Richard Caselli, MD Professor & Chair, Department of Neurology Mayo Clinic Arizona & Clinical Core Director, Arizona Alzheimer s Disease Center Objectives:
ASYMMETRICAL CORTICAL DEGENERATIVE SYNDROMES Richard Caselli, MD Professor & Chair, Department of Neurology Mayo Clinic Arizona & Clinical Core Director, Arizona Alzheimer s Disease Center Objectives:
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Introduction, use of imaging and current guidelines. John O Brien Professor of Old Age Psychiatry University of Cambridge
 Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE
 FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE DEE SILVER M.D MOVEMENT DISORDER SPECIALIST MEDICAL DIRECTOR -- PARKINSON ASSOCIATION OF SAN DIEGO 1980 TO PRESENT SCRIPPS MEMORIAL HOSPITAL, LA JOLLA CA.
FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE DEE SILVER M.D MOVEMENT DISORDER SPECIALIST MEDICAL DIRECTOR -- PARKINSON ASSOCIATION OF SAN DIEGO 1980 TO PRESENT SCRIPPS MEMORIAL HOSPITAL, LA JOLLA CA.
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Update on functional brain imaging in Movement Disorders
 Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Sleep disorders such as rapid eye movement (REM) sleep SCIENTIFIC INVESTIGATIONS
 sleep SCIENTIFIC INVESTIGATIONS") http://dx.doi.org/10.5664/jcsm.2670 Validation of the Mayo Sleep Questionnaire to Screen for REM Sleep Behavior Disorder in a Community-Based Sample Bradley F. Boeve, M.D., F.A.A.S.M. 1,3 ; Jennifer R.
http://dx.doi.org/10.5664/jcsm.2670 Validation of the Mayo Sleep Questionnaire to Screen for REM Sleep Behavior Disorder in a Community-Based Sample Bradley F. Boeve, M.D., F.A.A.S.M. 1,3 ; Jennifer R.
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute
 Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
CAREGIVER SUMMIT. The PD You Can't See: Dealing with Non-Motor Symptoms. Kaitlyn Roland, PhD. Sponsored by:
 CAREGIVER SUMMIT The PD You Can't See: Dealing with Non-Motor Symptoms Kaitlyn Roland, PhD Sponsored by: Cognition VS Dementia Memory Executive Function Attention Bradyphrenia Visuospatial Language Hallucinations
CAREGIVER SUMMIT The PD You Can't See: Dealing with Non-Motor Symptoms Kaitlyn Roland, PhD Sponsored by: Cognition VS Dementia Memory Executive Function Attention Bradyphrenia Visuospatial Language Hallucinations
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Diagnosing and Managing Lewy Body Dementia
 Diagnosing and Managing Lewy Body Dementia A Comprehensive Guide for Healthcare Professionals Provided by: Diagnosing and Managing Lewy Body Dementia 1 Table of contents 1. About Lewy Body Dementia...
Diagnosing and Managing Lewy Body Dementia A Comprehensive Guide for Healthcare Professionals Provided by: Diagnosing and Managing Lewy Body Dementia 1 Table of contents 1. About Lewy Body Dementia...
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Welcome and Introductions
 Parkinson s Disease Spotlight on Treatment Advances Tuesday, January 26, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing American Parkinson Disease Association 1
Parkinson s Disease Spotlight on Treatment Advances Tuesday, January 26, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing American Parkinson Disease Association 1
Extrapyramidal Motor System. Basal Ganglia or Striatum. Basal Ganglia or Striatum 3/3/2010
 Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
PACIFIC MOVEMENT DISORDERS CENTER AT PACIFIC NEUROSCIENCE INSTITUTE SM
 AT PACIFIC NEUROSCIENCE INSTITUTE SM PARKINSON S DISEASE: NON-MOTOR SYMPTOM MANAGEMENT Non-motor symptoms can have a large impact on quality of life and level of functioning in patients with PD. In some
AT PACIFIC NEUROSCIENCE INSTITUTE SM PARKINSON S DISEASE: NON-MOTOR SYMPTOM MANAGEMENT Non-motor symptoms can have a large impact on quality of life and level of functioning in patients with PD. In some
Clinical and Cognitive Features of DLB. James E. Galvin, MD, MPH Washington University School of Medicine
 Clinical and Cognitive Features of DLB James E. Galvin, MD, MPH Washington University School of Medicine James E. Galvin, MD, MPH Disclosure of Interest Research Support 1. National Institutes of Health
Clinical and Cognitive Features of DLB James E. Galvin, MD, MPH Washington University School of Medicine James E. Galvin, MD, MPH Disclosure of Interest Research Support 1. National Institutes of Health
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Update on the DLB Module. ADC Directors Meeting Baltimore, MD October 14-15, 2016
 Update on the DLB Module ADC Directors Meeting Baltimore, MD October 14-15, 2016 Committee Members James Galvin, Florida Atlantic University (Chair) James Leverenz Cleveland Clinic Brad Boeve Mayo Clinic,
Update on the DLB Module ADC Directors Meeting Baltimore, MD October 14-15, 2016 Committee Members James Galvin, Florida Atlantic University (Chair) James Leverenz Cleveland Clinic Brad Boeve Mayo Clinic,
Welcome and Introductions
 Parkinson s Disease Spotlight on Addressing Motor and Non-Motor Symptoms The Changing Landscape Wednesday, March 8, 2017 Welcome and Introductions Stephanie Paul Vice President Development and Marketing
Parkinson s Disease Spotlight on Addressing Motor and Non-Motor Symptoms The Changing Landscape Wednesday, March 8, 2017 Welcome and Introductions Stephanie Paul Vice President Development and Marketing
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Update on the DLB Module. ADC Directors Meeting Baltimore, MD October 14-15, 2016
 Update on the DLB Module ADC Directors Meeting Baltimore, MD October 14-15, 2016 Committee Members James Galvin, Florida Atlantic University Chair James Leverenz Cleveland Clinic Brad Boeve Mayo Clinic
Update on the DLB Module ADC Directors Meeting Baltimore, MD October 14-15, 2016 Committee Members James Galvin, Florida Atlantic University Chair James Leverenz Cleveland Clinic Brad Boeve Mayo Clinic
2016 Programs & Information
 Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Depression & Anxiety. What can I do? What are other possible treatments? What is this? Why does this happen? KEY POINTS
 Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
Moving Treatment Earlier Disease Modification in Early PD
 Moving Treatment Earlier Disease Modification in Early PD Ron Postuma Montreal General Hospital McGill University Disclosures: - Grants: Fonds de la Recherche en Sante Quebec, Canadian Institute of Health
Moving Treatment Earlier Disease Modification in Early PD Ron Postuma Montreal General Hospital McGill University Disclosures: - Grants: Fonds de la Recherche en Sante Quebec, Canadian Institute of Health
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases
 Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases Keith A. Josephs, MD, MST, MSc Professor of Neurology 13th Annual Mild Cognitive Impairment (MCI) Symposium: Alzheimer and Non-Alzheimer
Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases Keith A. Josephs, MD, MST, MSc Professor of Neurology 13th Annual Mild Cognitive Impairment (MCI) Symposium: Alzheimer and Non-Alzheimer
Multiple choice questions: ANSWERS
 Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What is Parkinson s Disease?
 2018 Update in Parkinson s Disease: Treatments and Future Plans Arita McCoy, MSN, CRNP Johns Hopkins Parkinson s Disease and Movement Disorder Center A National Parkinson Foundation Center of Excellence
2018 Update in Parkinson s Disease: Treatments and Future Plans Arita McCoy, MSN, CRNP Johns Hopkins Parkinson s Disease and Movement Disorder Center A National Parkinson Foundation Center of Excellence
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Imaging biomarkers for Parkinson s disease
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 6 MDS-ES/EAN: Neuroimaging in movement disorders - Level 2 Imaging biomarkers for Parkinson
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 6 MDS-ES/EAN: Neuroimaging in movement disorders - Level 2 Imaging biomarkers for Parkinson
Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University
 Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University Design of trials in DLB and PDD What has been learnt from previous trials in these indications and other dementias? Overview
Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University Design of trials in DLB and PDD What has been learnt from previous trials in these indications and other dementias? Overview
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Parkinson s Disease Update
 Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
2/20/18. History of Parkinson s. What is happening in the brain? DOPAMINE! Epidemiology. Parkinson s Disease. It s much more than tremor
 Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
Patterns of Cognitive Impairment in Dementia
 Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Any interventions, where RCTs in PD are not available, are not included in the tables.
 Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Patterns of Cognitive Impairment in Dementia
 Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Parkinsonian Disorders with Dementia
 Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
What s new for diagnosing and treating Parkinson s Disease?
 What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
Key Concepts and Issues in Parkinson s Disease in 2016
 Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
FDG-PET e parkinsonismi
 Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Enhanced Primary Care Pathway: Parkinson s Disease
 Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
DEMENTIA IN PARKINSON`S DISEASE. DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD
 Director-Parkinson`s Disease Service for the Older Person HNELHD") DEMENTIA IN PARKINSON`S DISEASE DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD DEMENTIA IN PD The concept of Non Motor Symptoms in PD Dementia in Parkinson`s
DEMENTIA IN PARKINSON`S DISEASE DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD DEMENTIA IN PD The concept of Non Motor Symptoms in PD Dementia in Parkinson`s
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1)
") 475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
Brain imaging for the diagnosis of people with suspected dementia
 Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
An old man with hallucination
 An old man with hallucination Inter-hospital Geriatric Meeting 30 March 2012 Speaker: Dr Siu Chun Yue Chairman: Dr Leung Chi Shing Caritas Medical Center History Admission 4/2011 75/M Premorbid: ADLI,
An old man with hallucination Inter-hospital Geriatric Meeting 30 March 2012 Speaker: Dr Siu Chun Yue Chairman: Dr Leung Chi Shing Caritas Medical Center History Admission 4/2011 75/M Premorbid: ADLI,
18F-FDG PET in Posterior Cortical Atrophy and Dementia with Lewy Bodies
 Journal of Nuclear Medicine, published on September 29, 2016 as doi:10.2967/jnumed.116.179903 1 18F-FDG PET in Posterior Cortical Atrophy and Dementia with Lewy Bodies 1 Jennifer L. Whitwell, PhD; 2 Jonathan
Journal of Nuclear Medicine, published on September 29, 2016 as doi:10.2967/jnumed.116.179903 1 18F-FDG PET in Posterior Cortical Atrophy and Dementia with Lewy Bodies 1 Jennifer L. Whitwell, PhD; 2 Jonathan
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Multiple System Atrophy
 Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
Date of Referral: Enhanced Primary Care Pathway: Parkinson s Disease
 Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
DIFFUSE LEWY BODY DISEASE (DLBD)
") CASE #2 Mr. S is a 62 years old male who was hospitalized in the dept. of psychogeriatrics after a suicide attempt (tried to jump from his balcony on the second floor). After a few days it was clear that
CASE #2 Mr. S is a 62 years old male who was hospitalized in the dept. of psychogeriatrics after a suicide attempt (tried to jump from his balcony on the second floor). After a few days it was clear that
UPDATE ON RESEARCH IN PARKINSON S DISEASE
 UPDATE ON RESEARCH IN PARKINSON S DISEASE Charles H. Adler, M.D., Ph.D. Professor of Neurology Mayo Clinic College of Medicine Co-Principal Investigator Arizona Parkinson s Disease Consortium Arizona Study
UPDATE ON RESEARCH IN PARKINSON S DISEASE Charles H. Adler, M.D., Ph.D. Professor of Neurology Mayo Clinic College of Medicine Co-Principal Investigator Arizona Parkinson s Disease Consortium Arizona Study
LEWY BODY DEMENTIA. Information for Patients, Families, and Professionals. LEARN ABOUT: Dementia with Lewy bodies Parkinson s disease dementia
 LEWY BODY DEMENTIA Information for Patients, Families, and Professionals LEARN ABOUT: Dementia with Lewy bodies Parkinson s disease dementia National Institute on Aging National Institute of Neurological
LEWY BODY DEMENTIA Information for Patients, Families, and Professionals LEARN ABOUT: Dementia with Lewy bodies Parkinson s disease dementia National Institute on Aging National Institute of Neurological
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
Quantifying the risk of neurodegenerative disease in idiopathic REM sleep behavior disorder
 Published Ahead of Print on January 7, 2009 as 10.1212/01.wnl.0000340980.19702.6e Quantifying the risk of neurodegenerative disease in idiopathic REM sleep behavior disorder R.B. Postuma, MD J.F. Gagnon,
Published Ahead of Print on January 7, 2009 as 10.1212/01.wnl.0000340980.19702.6e Quantifying the risk of neurodegenerative disease in idiopathic REM sleep behavior disorder R.B. Postuma, MD J.F. Gagnon,
Objectives. Distinguishing Parkinson s disease from other parkinsonian and tremor syndromes. Characteristics. Basal Ganglia Structures
 12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships
12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships