Objectives. Overview. Why FTD and AD? FTD May Mimic AD. Introduction and Process Norman L. Foster, MD. Introduction and Process 7BS.
|
|
|
- Jacob Ira Robbins
- 6 years ago
- Views:
Transcription
1 Introduction and Process Norman L. Foster, MD 7BS.006 IMPROVING ACCURACY OF DEMENTIA DIAGNOSIS: CASE STUDIES WITH NEUROPATHOLOGY Norman L. Foster, MD University of Utah Salt Lake City, UT Edward Zamrini, MD University of Utah Salt Lake City, UT James B. Leverenz, MD University of Washington Seattle, WA 6:45 a.m. - 8:30 a.m. Friday, May 4, 2007 Breakfast Seminar Introduction and Process Norman L. Foster, M.D. Center for Alzheimer s Care, Imaging and Research Department of Neurology, University of Utah No conflicts to disclose Overview An interactive discussion of clinical cases with FDG-PET scans and autopsy diagnosis of Alzheimer s disease (AD) or frontotemporal dementia (FTD) Briefly review FDG-PET and its interpretation in dementia Briefly review the clinical criteria for AD and FTD Briefly review the histopathology of AD and FTD Cases will be presented to stimulate discussion We will ask the audience to vote on diagnosis Objectives CMS recently approved the use of FDG-PET in the evaluation of dementia to distinguish AD from FTD Neurologists need to better understand when and how to utilize this new technology Improve accuracy and confidence in clinical diagnosis of dementing illnesses Learn when and how to use molecular imaging in dementia evaluations Better apply diagnostic criteria for dementing disorders in individual situations Why FTD and AD? AD and FTD are common causes of dementia AD is the most common cause of dementia in the elderly in the US FTD is much less prevalent, but still the second most common neurodegenerative cause early-onset dementia Neither has characteristic physical findings that aid the diagnosis of other dementias Clinically difficult to distinguish FDG-PET can help this clinical decision and is CMS approved FTD May Mimic AD Behavior disturbance is common in AD Language is affected early in AD AD is sometimes asymmetric causing prominent aphasia Most FTD patients develop a significant memory disturbance Most FTD patients also meet NINCDS-ADRDA criteria for AD (Varma et al., JNNP 1999;66: ) Clinicians depend upon relative severity of symptoms; none are pathognomonic 7BS.006-1
2 Introduction and Process Norman L. Foster, MD Clinical Summaries Collected all available medical records Removed personal identifiers, imaging results, and autopsy reports Several page clinical narrative from these records summarizing the patient s entire clinical course Developed by a dementia expert unaware of diagnosis who did not serve as a rater How We Will Consider Cases Review scenario and rate, then we will discuss Review with FDG-PET and rate, then discuss with interpretation of FDG-PET Present neuropathological findings Diagnosis - AD or FTD Must decide one or the other Degree of Confidence Very confident Somewhat confident Uncertain How to Rate Cases Diagnosis - AD or FTD Must decide one or the other Degree of Confidence Very confident Somewhat confident Uncertain Rating Card Example 7BS.006-2

 FDG-PET provides")
 What Glucose Metabolism Measures Under normal conditions the brain")
3 Clinical Application of FDG-PET Imaging Norman L. Foster, MD Clinical Application of FDG-PET Imaging Norman L. Foster, M.D. Center for Alzheimer s Care, Imaging and Research Department of Neurology, University of Utah No conflicts to disclose 18-F Flurodeoxyglucose Positron Emission Tomography (FDG-PET) FDG-PET provides unique information, complementary to structural imaging Short-lived positron-labeled form of sugar that follows the early steps of glucose, but gets trapped in the cell Fluorine -18: 120 min PET scanner uses physical properties of positrons to localize relevant radioactive emissions and discards others (improved resolution) What Glucose Metabolism Measures Under normal conditions the brain uses glucose as its sole source of energy Glucose metabolism primarily reflects synaptic activity Hypometabolism may not correspond to areas with greatest changes in routine neuropathology Routine neuropathology is better at detecting loss of neuronal cell bodies than synapses It is not directly affected by intracellular or extracellular inclusions Synapses are Lost Before Neurons Die FDG-PET Image Presentation Methods Alzheimer s Disease T R A N S A X I A L S S P 7BS.006-1

4 Clinical Application of FDG-PET Imaging Norman L. Foster, MD Frontotemporal Dementia Simple Rules for FDG-PET Diagnosis in this Course Alzheimer s disease Temporoparietal cortex hypometabolism > frontal cortex Posterior cingulate cortex hypometabolic Frontotemporal dementia Frontal cortex hypometabolism > temporoparietal cortex Anterior temporal and anterior cingulate cortex hypometabolic When several areas affected, are AD or FTD regions most hypometabolic 7BS.006-2
5 Clinical Diagnostic Criteria for AD and FTD Edward Zamrini, MD CLINICAL DIAGNOSTIC CRITERIA FOR AD AND FTD Edward Zamrini M.D. Center for Alzheimer s Care Imaging and Research Department of Neurology University of Utah Overview Clinical features and diagnostic criteria for Alzheimer s disease Clinical features and diagnostic criteria for frontotemporal dementia Reasons for difficulty with diagnosis Importance of making a diagnosis No conflicts to disclose Objectives Improve accuracy and confidence in clinical diagnosis of dementing illnesses Apply diagnostic criteria for dementing disorders in individual situations Identify features that distinguish between AD and FTD Alzheimer s s Disease Insidious onset of gradual progressive dementia Memory loss usually initial and most prominent symptom No focal weakness or sensory loss Gait normal and continent until late in the illness NINCDS-ADRDA criteria validated NINCDS/ADRDA Criteria for Diagnosis of Probable AD: (a) Dementia established by clinical examination, and documented by a standard test of cognitive function, and confirmed by neuropsychological tests. (b) Significant deficiencies in two or more areas of cognition, for example, word comprehension and task-completion ability. (c) Progressive deterioration of memory and other cognitive functions. (d) No loss of consciousness. (e) Onset from age 40 to 90, typically after 65. (f) No other diseases or disorders that could account for the loss of memory and cognition. Frontotemporal Dementia Insidious onset of progressive dementia Disturbing behavior and speech problems most prominent, less evident memory loss Perseveration, decreased verbal fluency Typical behavioral changes including apathy unrestrained and inappropriate social conduct Memory loss often not prominent; AD screening tests may be insensitive May be associated with motor neuron disease 7BS.006-1
6 Clinical Diagnostic Criteria for AD and FTD Edward Zamrini, MD FTD: Clinical profile Frontotemporal dementia (FTDbv): Character change and disordered social conduct. Instrumental functions relatively well preserved. Progressive nonfluent aphasia (PA): Disorder of expressive language is the dominant feature initially and throughout the disease course. Other aspects of cognition are intact or relatively well preserved. Semantic aphasia and associative agnosia dementia (Semantic dementia, SD): impaired understanding of word meaning and/or object identity. Diagnostic features of frontotemporal dementia behavioral variant I. Core diagnostic features of FTD A. Insidious onset and gradual progression B. Early decline in social interpersonal conduct C. Early impairment of personal conduct D. Early emotional blunting E. Early loss of insight II. Supportive diagnostic features of FTD A. Behavioral disorder B. Speech and language C. Physical signs Diagnostic features progressive non-fluent aphasia I. Core diagnostic features of PA A. Insidious onset and gradual progression B. Nonfluent spontaneous speech with: agrammatism, phonemic paraphasias, anomia II. Supportive diagnostic features of PA A. Speech and language 1. Stuttering or oral apraxia 2. Impaired repetition 3. Alexia, agraphia 4. Early preservation of word meaning, 5. Late mutism B. Behavior 1. Early preservation of social skills 2. Late behavioral changes similar to FTD C. Physical signs: late contralateral primitive reflexes, akinesia, rigidity, and tremor Diagnostic features of semantic aphasia and associative agnosia I. Core diagnostic features of SD A. Insidious onset and gradual progression B. Language Disorder and/or C. Perceptual disorder D. Preserved perceptual matching and drawing reproduction E. Preserved single-word repetition F. Preserved ability to read aloud and write to dictation orthographically regular words II. Supportive diagnostic features of semantic dementia A. Speech and language B. Behavior C. Physical signs FTD May Mimic AD Alzheimer s disease is much more common than frontotemporal dementia Behavior disturbance is common in AD Language is affected early in AD AD is sometimes asymmetric causing prominent aphasia Most patients with FTD have a significant memory disturbance Most patients with FTD also meet NINCDS- ADRDA criteria for AD (Varma et al. JNNP 1999;66: ) Clinicians depend upon relative severity of symptoms; none are pathognomonic AD or FTD Does it Make a Difference? YES!!!! Drug treatment differs In FTD no evidence of a cholinergic deficiency In FTD impaired initiative is easily confused with depression In FTD amyloid strategies are inappropriate Management differs In FTD behavior less likely to respond to usual drug treatments and appear to be more spontaneous rather than responsive to environment Understanding behavior can help caregivers Prognosis and genetics differ 7BS.006-2



: NP, NFT, PB, BN /H&E: myelin, neurons, glia PTAH: glia")
7 Pathological Diagnostic Criteria: An overview of AD and FTD pathology and diagnostic criteria James B. Leverenz, M.D. Departments of Neurology and Psychiatry and Behavioral Sciences University of Washington School of Medicine and VA Northwest Network Mental Illness and Parkinson s s Disease Research, Education, and Clinical Centers Overview: Neuropathology of AD and FTD Review of AD pathology CERAD and Reagan criteria Stains for detection of NP and NFT Review of FTD pathology Pathologic subgroups Stains for detection of FTD-associated pathology Normal Brain Weight Mean Brain Weight: 1424g for men 1265g for women Stains for AD/FTD neuropathology Histologic stains (silver stain): NP, NFT, PB, BN /H&E: myelin, neurons, glia PTAH: glia (reactive, fibers) Immunohistochemistry tau: NFT, neurites in plaques, PB ubiquitin: NFT, neurites in plaques, PB, LB, ubiquitin-only inclusions and neurites neurofilament: NFT, BN Miller and Corsellis, Ann Hum Biol, 4:253-7, Dekaban and Sadowsky, Ann. Neurology, 4: , Alzheimer's Disease Pathology Alzheimer's Disease Pathology Auguste Autopsy (1906): evenly affected atrophic brain stain: fibrils arranged parallel a tangled bundle of fibrils Dispersed over the entire cortex,miliary foci Normal Alzheimer s Disease 1
 Neurofibrillary tangles are not considered in these criteria Mirra S et al, Neurology.. 1991.")

 FTD Pathology: Neuronal loss and gliosis 1892 Pick describes first case 71 y.o. man 3 yr decline including aphasia Autopsy Focal temporal lobe atrophy (Chiari( Chiari) 1911 Alzheimer describes Pick Bodies (PB) & Ballooned Neurons (BN) GFAP Normal GFAP FTD 2")
8 Alzheimer's Disease (AD) CERAD Criteria for AD Neuritic Plaques Neuritic Plaques Neurofibrillary Tangles Cortical density of neuritic plaques Infrequent Moderate Frequent Classification possible or probable Interaction of plaque stage and age (A,B,C) Neurofibrillary tangles are not considered in these criteria Mirra S et al, Neurology Braak Staging of AD Neurofibrillary tangles NIA-Reagan Criteria for AD Transentorhinal Stages (I-II) Limbic Stages (III-IV) Isocortical Stages (V-VI) Probability pathology accounts for dementia Low-Braak stage I/II, CERAD infrequent plaques Intermediate-Braak stage III/IV, CERAD intermediate plaques High-Braak stage V/VI, CERAD frequent plaques Integrates plaque and tangle pathology Braak H, Braak E. Acta Neurol Scand Suppl ;165:3-12. Neurobiol Aging Jul-Aug;18(4 Suppl):S1-2. Frontotemporal Dementia (FTD) FTD Pathology: Neuronal loss and gliosis 1892 Pick describes first case 71 y.o. man 3 yr decline including aphasia Autopsy Focal temporal lobe atrophy (Chiari( Chiari) 1911 Alzheimer describes Pick Bodies (PB) & Ballooned Neurons (BN) GFAP Normal GFAP FTD 2
 neurofilament Ballooned Neuron (BN) FTD Pathology: Neuronal")

")
,")
* Variable neuronal loss and gliosis ubiquitin-only")
 Mott et al, J Neuropath Exp Neurol, 2005 3")
9 FTD Pathology: Hippocampal sclerosis FTD Pathology: Neuronal and glial alterations DG Frontal Cortex DG PHG tau Pick Bodies (PB) neurofilament Ballooned Neuron (BN) FTD Pathology: Neuronal and glial alterations DG ubiquitin Ubiquitin-only inclusions White matter tau Tau-positive glial inclusions FTD Pathologic Classifications Pick-Type Severe neuronal loss and gliosis Tauopathy (3R) Pick bodies and ballooned neurons Corticobasal degeneration (CBD) Tauopathy (4R) NFT, neuropil threads, astrocytic plaques, coiled bodies Progressive supranuclear palsy (PSP) Tauopathy (4R) NFT, tufted astrocytes,, coiled bodies Mott et al, J Neuropath Exp Neurol, 2005 FTD Pathologic Classifications Neurofibrillary tangle dementia Tauopathy (variable tau subtype), Tau mutations Variable tau pathology (neurons and glia) Frontotemporal lobar degeneration with MND or MND- type inclusions (FTLD-MND/MNI)* Variable neuronal loss and gliosis ubiquitin-only inclusions (TDP-43 +) Dementia lacking distinctive histopathology (DLDH) Neuronal loss and gliosis without distinctive biochemical signal (e.g. tau or ubiquitin-only pathology) Mott et al, J Neuropath Exp Neurol,
10 Scenario 2026 Review Cases 1) Review Scenario and Vote 2) Review Scenario with PET and Vote 3) Pathology Scenario yo M w 3.5y h/o progressive memory impairment. Sx: occ. WFD, poor concentration, difficulty following series of directions, finances, operating power tools. Able to drive. SH: Retired billing specialist, 12y ed. FH: F w probable dementia Neuro: Slight rest and postural tremor of UEs Scenario 2026 MS: MMSE 19. Partly oriented. Trouble naming parts of objects. Impaired WORLD backwards, calculations, clock hands. 0/3 recall, 2/3 with prompting. 4y: can t read, name president, calculate, name items of clothing. 4y 9m: Can still travel. May reverse clothing, skips parts of the lawn mowing, unable to start new lawnmower. Scenario 2026 Rate Scenario y: anxiety & agitation, 5y 9m: Cannot roll down car windows, find utensils while eating. Does not speak till spoken to. Unable to speak full sentences. 6.5y: brief hallucinations. Easily distracted. Speech limited to 2-word phrases. 8y: wandering, occ striking. 9y: several falls, complete care, died. 1



11 Rate Scenario with PET Pathologic Category Scenario 2026 Scenario Frontal Cortex Brain wt 1160g Moderate frontal > temporal atrophy 2






12 Scenario Frontal Cortex Scenario Hippocampus DG Scenario Hippocampus Scenario Inf. Temporal Gyrus DG Scenario 2026 Brain wt 1160g Moderate frontal > temporal atrophy 2026 Pathologic Category Definite AD Histologic Findings Frequent neuritic plaques Braak Stage V No Lewy bodies No Strokes or other focal lesions 3

13 Scenario 2040 Scenario yo RHF w 2y h/o change in personality and memory loss. Doesn t participate in daily activities. No longer does housework or participates in conversations, preferring to sit in a chair all day. Stopped driving after becoming lost on familiar routes 1y into her illness. Very forgetful. Has purchased items she does not need, and eating more. She may laugh inappropriately or become upset, and has made statements that people are trying to dupe her. SH: Married, 8th grade educ. Homemaker FH: Unk. Scenario 2040 Exam: O x 3/3. DS 6 forward, 5 back. Current President + 4/5 past. 4/5 serial 7s, unable to calculate nickels in $1.35. Language intact. Draws clock, not cube. Recall 3/5 at 5. Affect generally flat and poor awareness of cognitive changes. Slow, deliberate gait. No primitive reflexes. At 2y 3mo: speaking less, hums frequently. C/o being tired and hungry all the time. Sleeps frequently during the day. Needs prompting to do household chores and spends most of her day watching TV. On exam, markedly apathetic. Knows date and location. Names current but not prior Presidents. recalls 1/3 after delay. Performed simple but not complex calculations. Excellent naming but occasional paraphasias. Poor comprehension with reading. Scenario y: Incontinent. Screams suddenly then starts to laugh. Hums almost constantly and wants to eat. On exam, humming almost constantly and picking at clothing in purposeless fashion. Paucity of spontaneous speech. Recall 3/4 at 5. 6y: no intelligible speech. Agitated, distracted, and may spend time simply staring at her hands. Now needs occasional encouragement to eat. near total care for personal hygiene. On exam, had constant chewing motions. Vocalized with high pitched moans. Frequently attempted to leave the examination room. Frequently clapped. Unable to respond to any commands. Gait slightly slowed and stooped. Grasp reflexes present. Patient died after 14 years of symptoms. Rate Scenario


14 2040 Rate Scenario with PET Pathologic Category Scenario 2040 Brain wt 800g Severe fronto-temporal atrophy knife-edged atrophy Scenario Frontal Cortex Scenario FC vs OC FC OC 5







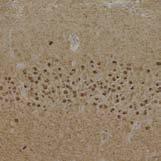

15 Scenario Frontal Cortex Scenario Frontal Cortex tau tau Scenario Hippocampus Scenario Hippocampus DG DG tau Scenario Hippocampus Scenario PHG and Striatum DG Parahippocampal Gyrus Caudate PHG tau tau PTAH 6
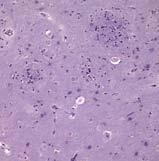
16 Scenario 2040 Brain wt 800g Severe fronto-temporal atrophy knife-edged atrophy Histopathology Severe FC/TC neuronal loss and gliosis Pick body inclusions (tau positive) 2040 Pathologic Category Frontotemporal Dementia Pick s Disease subtype Review Scenario 2162 Scenario yof w 6y h/o progressive memory loss. Got lost after taking a bus downtown. Calls D several times a day w/o realizing she had called. Able to shop and prep light meals. Signif. visual and auditory impairment and bumps into objects when walking. She can no longer read or quilt. SH: Unknown FH: Unknown MS: A+O to yr, season, and mo but not day of week. O to place, x county. Recalls 1/3 after 3. Unable to subtract 7 from 100 and only 3 letters correct when spelling WORLD backwards. No difficulty with language. Mild impairment when copying a design. Neuro: Unremarkable x for macular degeneration and auditory impairment. Scenario 2162 Rate Scenario 2162 At 6y 9m: in NH, socializes, good mood, incontinent of urine +/- stool. D/o to date & names of children & current events. Follows simple commands. 0/3 recall at 5, 2/3 w clues. Fluent. At 7y 3m: can feed self, but needs help with dressing, incontinent, calm. O to city and doctor s office. Fluent. 0/3 recall at 5. Slight stoop. At 7y 9m: wanders, paces, assists others as possible, helping them get out of restraints. Patient died after 10.5 years of symptoms. 7


17 Rate Scenario with PET Pathologic Category Scenario 2162 Scenario Frontal Cortex Brain wt 925g Severe bilateral fronto-temporal atrophy 8









18 Scenario Frontal Cortex Scenario Hippocampus DG PHG Scenario Hippocampus Scenario Dentate Gyrus PTAH ubiquitin Biel ubiquitin Scenario PHG/Insular cortex Scenario Substantia Nigra Parahippocampal Gyrus Insular Cortex 2162 SN RN SN CP Normal SN RN SN CP ubiquitin 9
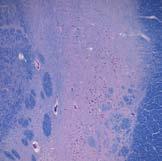
19 Scenario 2162 Brain wt 925g Severe fronto-temporal atrophy Histopathology Severe neuronal loss and gliosis, insular and temporal cortex, hippocampus ( hippocampal sclerosis, and substantia nigra Ubiquitin-only inclusions/neurities DG, superficial neocortex Frequent neuritic plaques Braak stage III 2162 Pathologic Category - FTD Frontotemporal Dementia: Motor Neuron Disease/MND-like Inclusions Subtype Intermediate Likelihood AD 10
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FTD basics! Etienne de Villers-Sidani, MD!
 FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
I do not have any disclosures
 Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Neuropathology of Neurodegenerative Disorders Prof. Jillian Kril
 Neurodegenerative disorders to be discussed Alzheimer s disease Lewy body diseases Frontotemporal dementia and other tauopathies Huntington s disease Motor Neuron Disease 2 Neuropathology of neurodegeneration
Neurodegenerative disorders to be discussed Alzheimer s disease Lewy body diseases Frontotemporal dementia and other tauopathies Huntington s disease Motor Neuron Disease 2 Neuropathology of neurodegeneration
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
DEMENTIA 9/29/16. Introduction. Introduction. Signs and Symptom. Epidemiology. Dementia. Dr. Yotin Chinvarun M.D. Ph.D.
 Introduction DEMENTIA Dr. Yotin Chinvarun M.D. Ph.D. Neurology, Pramongkutklao hospital In 1901 Auguste Deter, a woman in her early 50s, became 1 st person diagnosed with Alzheimer's disease, a form of
Introduction DEMENTIA Dr. Yotin Chinvarun M.D. Ph.D. Neurology, Pramongkutklao hospital In 1901 Auguste Deter, a woman in her early 50s, became 1 st person diagnosed with Alzheimer's disease, a form of
2016 Programs & Information
 Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Clinicopathologic and genetic aspects of hippocampal sclerosis. Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA
 Clinicopathologic and genetic aspects of hippocampal sclerosis Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA The hippocampus in health & disease A major structure of the medial temporal
Clinicopathologic and genetic aspects of hippocampal sclerosis Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA The hippocampus in health & disease A major structure of the medial temporal
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia
 Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia Bradley F. Boeve, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Alzheimer s Disease
Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia Bradley F. Boeve, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Alzheimer s Disease
Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases
 Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases Keith A. Josephs, MD, MST, MSc Professor of Neurology 13th Annual Mild Cognitive Impairment (MCI) Symposium: Alzheimer and Non-Alzheimer
Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases Keith A. Josephs, MD, MST, MSc Professor of Neurology 13th Annual Mild Cognitive Impairment (MCI) Symposium: Alzheimer and Non-Alzheimer
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Dementia. Amber Eker, MD. Assistant Professor Near East University Department of Neurology
 Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
! slow, progressive, permanent loss of neurologic function.
 UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer
 The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
FDG-PET e parkinsonismi
 Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Frontotemporal Dementia: Towards better diagnosis. Frontotemporal Dementia. John Hodges, NeuRA & University of New South Wales, Sydney.
 I.1 I.2 II.1 II.2 II.3 II.4 II.5 II.6 III.1 III.2 III.3 III.4 III.5 III.6 III.7 III.8 III.9 III.10 III.11 III.12 IV.1 IV.2 IV.3 IV.4 IV.5 Frontotemporal Dementia: Towards better diagnosis Frontotemporal
I.1 I.2 II.1 II.2 II.3 II.4 II.5 II.6 III.1 III.2 III.3 III.4 III.5 III.6 III.7 III.8 III.9 III.10 III.11 III.12 IV.1 IV.2 IV.3 IV.4 IV.5 Frontotemporal Dementia: Towards better diagnosis Frontotemporal
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Diagnosis before NIA AA The impact of FDG PET in. Diagnosis after NIA AA Neuropathology and PET image 2015/10/16
 The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
For carers and relatives of people with frontotemporal dementia and semantic dementia. Newsletter
 For carers and relatives of people with frontotemporal dementia and semantic dementia Newsletter AUGUST 2008 1 Welcome Welcome to the August edition of our CFU Support Group Newsletter. Thanks to all of
For carers and relatives of people with frontotemporal dementia and semantic dementia Newsletter AUGUST 2008 1 Welcome Welcome to the August edition of our CFU Support Group Newsletter. Thanks to all of
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction.
 Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Navigating The Cognitive Internet: Introduction. Wendy Lemere DNP, GNP-BC Gerontological Nurse Practitioner Henry Ford Health System
 Navigating The Cognitive Internet: Introduction Wendy Lemere DNP, GNP-BC Gerontological Nurse Practitioner Henry Ford Health System What s so hard about diagnosing dementia? Diagnosis relies on synthesis
Navigating The Cognitive Internet: Introduction Wendy Lemere DNP, GNP-BC Gerontological Nurse Practitioner Henry Ford Health System What s so hard about diagnosing dementia? Diagnosis relies on synthesis
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Objectives. RAIN Difficult Diagnosis 2014: A 75 year old woman with falls. Case History: First visit. Case History: First Visit
 Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
Lecture 42: Final Review. Martin Wessendorf, Ph.D.
 Lecture 42: Final Review Martin Wessendorf, Ph.D. Lecture 33 cortex Heilbronner 5 lobes of the cortex Lateral view (left side) Mid-saggital view (right side) Cellular organization of cortex White matter
Lecture 42: Final Review Martin Wessendorf, Ph.D. Lecture 33 cortex Heilbronner 5 lobes of the cortex Lateral view (left side) Mid-saggital view (right side) Cellular organization of cortex White matter
What is dementia? Symptoms of dementia. Memory problems
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Do not copy or distribute without permission. S. Weintraub, CNADC, NUFSM, 2009
 Sandra Weintraub, Ph.D. Clinical Core Director, Cognitive Neurology and Alzheimer s Disease Center Northwestern University Feinberg School of Medicine Chicago, Illinois Dementia: a condition caused by
Sandra Weintraub, Ph.D. Clinical Core Director, Cognitive Neurology and Alzheimer s Disease Center Northwestern University Feinberg School of Medicine Chicago, Illinois Dementia: a condition caused by
What is Neuropsychology?
 Alzheimer s Disease Neurological Bases and Informed Behavioral Interventions Peter T. Keenan Clinical Neuropsychologist Marshfield Clinic Minocqua Center What is Neuropsychology? Science of the relationship
Alzheimer s Disease Neurological Bases and Informed Behavioral Interventions Peter T. Keenan Clinical Neuropsychologist Marshfield Clinic Minocqua Center What is Neuropsychology? Science of the relationship
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Objectives. Objectives continued: 3/24/2012. Copyright Do not distribute or replicate without permission 1
 Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Session outline. Introduction to dementia Assessment of dementia Management of dementia Follow-up Review
 Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Confronting the Clinical Challenges of Frontotemporal Dementia
 Confronting the Clinical Challenges of Frontotemporal Dementia A look at FTD s symptoms, pathophysiology, subtypes, as well as the latest from imaging studies. By Zac Haughn, Senior Associate Editor Ask
Confronting the Clinical Challenges of Frontotemporal Dementia A look at FTD s symptoms, pathophysiology, subtypes, as well as the latest from imaging studies. By Zac Haughn, Senior Associate Editor Ask
Prof Tim Anderson. Neurologist University of Otago Christchurch
 Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
10/17/2017. Causes of Dementia Alzheimer's Disease Vascular Dementia Diffuse Lewy Body Disease Alcoholic Dementia Fronto-Temporal Dementia Others
 1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
Dementia and Healthy Ageing : is the pathology any different?
 Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
NACC Minimum Data Set (MDS) Public Data Element Dictionary
 Public Data Element Dictionary") Department of Epidemiology, School of Public Health and Community Medicine, University of Washington 4311 11 th Avenue NE #300 Seattle, WA 98105 phone: (206) 543-8637; fax: (206) 616-5927 e-mail: naccmail@u.washington.edu
Department of Epidemiology, School of Public Health and Community Medicine, University of Washington 4311 11 th Avenue NE #300 Seattle, WA 98105 phone: (206) 543-8637; fax: (206) 616-5927 e-mail: naccmail@u.washington.edu
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Brain Advance Access published February 25, doi: /brain/awu024 Brain 2014: Page 1 of 17 1
 Brain Advance Access published February 25, 2014 doi:10.1093/brain/awu024 Brain 2014: Page 1 of 17 1 BRAIN A JOURNAL OF NEUROLOGY Asymmetry and heterogeneity of Alzheimer s and frontotemporal pathology
Brain Advance Access published February 25, 2014 doi:10.1093/brain/awu024 Brain 2014: Page 1 of 17 1 BRAIN A JOURNAL OF NEUROLOGY Asymmetry and heterogeneity of Alzheimer s and frontotemporal pathology
Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre
 Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre Today Introduction to CT Introduction to MRI Introduction to nuclear medicine Imaging the dementias The Brain ~ 1.5
Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre Today Introduction to CT Introduction to MRI Introduction to nuclear medicine Imaging the dementias The Brain ~ 1.5
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
FTD/PPA Caregiver Education Conference March 11, 2011
 FTD/PPA Caregiver Education Conference March 11, 2011 Question and Answer Session Answered by Joseph Cooper, MD, Darby Morhardt, MSW, LCSW, Mary O Hara, AM, LCSW, Jaimie Robinson, MSW, LCSW, Emily Rogalski,
FTD/PPA Caregiver Education Conference March 11, 2011 Question and Answer Session Answered by Joseph Cooper, MD, Darby Morhardt, MSW, LCSW, Mary O Hara, AM, LCSW, Jaimie Robinson, MSW, LCSW, Emily Rogalski,
FDG-PET improves accuracy in distinguishing frontotemporal dementia and Alzheimer s disease
 doi:10.1093/brain/awm177 Brain (2007), 130,2616^2635 FDG-PET improves accuracy in distinguishing frontotemporal dementia and Alzheimer s disease Norman L. Foster, 1 Judith L. Heidebrink, 2,4 Christopher
doi:10.1093/brain/awm177 Brain (2007), 130,2616^2635 FDG-PET improves accuracy in distinguishing frontotemporal dementia and Alzheimer s disease Norman L. Foster, 1 Judith L. Heidebrink, 2,4 Christopher
Disorders of language and speech. Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology
 Disorders of language and speech Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology http://neurology.pote.hu major categories disorders of language and speech cortical types aphasias
Disorders of language and speech Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology http://neurology.pote.hu major categories disorders of language and speech cortical types aphasias
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
What About Dementia? Module 8, Part B (With Dr Allison Lamont)
") What About Dementia? Module 8, Part B (With Dr Allison Lamont) Slide 1 Module 8 Part B will address the question What about dementia? Several surveys of older people both in the UK and USA have shown that
What About Dementia? Module 8, Part B (With Dr Allison Lamont) Slide 1 Module 8 Part B will address the question What about dementia? Several surveys of older people both in the UK and USA have shown that
The progression of dementia
 PBO 930022142 NPO 049-191 The progression of dementia Although everyone experiences dementia in their own individual way, it can be helpful to think of the progression of dementia as a series of stages.
PBO 930022142 NPO 049-191 The progression of dementia Although everyone experiences dementia in their own individual way, it can be helpful to think of the progression of dementia as a series of stages.
The Spectrum of Age-Associated Astroglial Tauopathies. Dennis W. Dickson MD Department of Neuroscience Mayo Clinic, Jacksonville, FL
 The Spectrum of Age-Associated Astroglial Tauopathies Dennis W. Dickson MD Mayo Clinic, Jacksonville, FL Thorn-shaped astrocytes TSA were first reported by Ikeda (1995), as tau-positive astrocytes in various
The Spectrum of Age-Associated Astroglial Tauopathies Dennis W. Dickson MD Mayo Clinic, Jacksonville, FL Thorn-shaped astrocytes TSA were first reported by Ikeda (1995), as tau-positive astrocytes in various
What is. frontotemporal. address? dementia?
 What is frontotemporal address? dementia? Contents 03 What is frontotemporal dementia? 04 Symptoms 05 Diagnosis 06 Treatments Information in this booklet is for anyone who wants to know more about frontotemporal
What is frontotemporal address? dementia? Contents 03 What is frontotemporal dementia? 04 Symptoms 05 Diagnosis 06 Treatments Information in this booklet is for anyone who wants to know more about frontotemporal
NACC Neuropathology (NP) Diagnosis Coding Guidebook
 Diagnosis Coding Guidebook") Department of Epidemiology, School of Public Health and Community Medicine, University of Washington 4311 11 th Avenue NE #300 Seattle, WA 98105 phone: (206) 543-8637; fax: (206) 616-5927 e-mail: naccmail@u.washington.edu
Department of Epidemiology, School of Public Health and Community Medicine, University of Washington 4311 11 th Avenue NE #300 Seattle, WA 98105 phone: (206) 543-8637; fax: (206) 616-5927 e-mail: naccmail@u.washington.edu
To help you prepare for your doctor's visit, the Alzheimer Society has developed the following list:
 The Alzheimer Society has a tool kit to help you prepare for a conversation with your doctor or health provider about your concerns and questions about a possible dementia diagnosis. Symptoms of dementia
The Alzheimer Society has a tool kit to help you prepare for a conversation with your doctor or health provider about your concerns and questions about a possible dementia diagnosis. Symptoms of dementia
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
Introduction, use of imaging and current guidelines. John O Brien Professor of Old Age Psychiatry University of Cambridge
 Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Dementia Basics. Welcome! What to expect and how to handle a dementia diagnosis. In partnership with Scripps Health.
 Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Neuro degenerative PET image from FDG, amyloid to Tau
 Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
Title: Clinical and neuropathologic variation in neuronal intermediate filament inclusion disease (NIFID)
") Neurology/2004/048785 Title: Clinical and neuropathologic variation in neuronal intermediate filament inclusion disease (NIFID) Correspondence to: Nigel J. Cairns PhD MRCPath Center for Neurodegenerative
Neurology/2004/048785 Title: Clinical and neuropathologic variation in neuronal intermediate filament inclusion disease (NIFID) Correspondence to: Nigel J. Cairns PhD MRCPath Center for Neurodegenerative
LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION
 LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION Murray Grossman University of Pennsylvania Support from NIH (AG17586, AG15116, NS44266, NS35867, AG32953, AG38490), IARPA, ALS Association, and the
LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION Murray Grossman University of Pennsylvania Support from NIH (AG17586, AG15116, NS44266, NS35867, AG32953, AG38490), IARPA, ALS Association, and the
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative
 is a progressive neurodegenerative") ORIGINAL RESEARCH E. Matsusue S. Sugihara S. Fujii T. Kinoshita T. Nakano E. Ohama T. Ogawa Cerebral Cortical and White Matter Lesions in Amyotrophic Lateral Sclerosis with Dementia: Correlation with MR
ORIGINAL RESEARCH E. Matsusue S. Sugihara S. Fujii T. Kinoshita T. Nakano E. Ohama T. Ogawa Cerebral Cortical and White Matter Lesions in Amyotrophic Lateral Sclerosis with Dementia: Correlation with MR
DEMENTIA ANDREA BERG, MD
 DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
Frontal Behavioural Inventory (FBI)
") This is a Sample version of the Frontal Behavioural Inventory (FBI) The full version of the Frontal Behavioural Inventory (FBI) comes without sample watermark. The full complete version includes Complete
This is a Sample version of the Frontal Behavioural Inventory (FBI) The full version of the Frontal Behavioural Inventory (FBI) comes without sample watermark. The full complete version includes Complete
Chapter 2: Alzheimer s Disease and Other Dementias
 By Eun-Shim Nahm, PhD, RN Assistant Professor University of Maryland School of Nursing OUTLINE What is Alzheimer s disease? Causes of Alzheimer s disease? Cognitive Changes Behavioral, Psychiatric issues
By Eun-Shim Nahm, PhD, RN Assistant Professor University of Maryland School of Nursing OUTLINE What is Alzheimer s disease? Causes of Alzheimer s disease? Cognitive Changes Behavioral, Psychiatric issues
Frontotemporal dementia and dementia with Lewy bodies in a case-control study of Alzheimer s disease
 International Psychogeriatrics: page 1 of 8 C 2009 International Psychogeriatric Association doi:10.1017/s1041610209009454 Frontotemporal dementia and dementia with Lewy bodies in a case-control study
International Psychogeriatrics: page 1 of 8 C 2009 International Psychogeriatric Association doi:10.1017/s1041610209009454 Frontotemporal dementia and dementia with Lewy bodies in a case-control study
Aging often includes changes to vision, hearing, taste, smell, skin, hair, weight & changes to Brain:
 Aging & Cognition Ladan Ghazi Saidi, Ph.D., Assistant Professor, Department of Communication Disorders, COE, University of Nebraska at Kearney 2018 Nebraska Speech-Language-Hearing Association Fall Convention
Aging & Cognition Ladan Ghazi Saidi, Ph.D., Assistant Professor, Department of Communication Disorders, COE, University of Nebraska at Kearney 2018 Nebraska Speech-Language-Hearing Association Fall Convention
Form A3: Subject Family History
 Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Overview of the non-alzheimer Dementias
 Overview of the non-alzheimer Dementias Chiadi U. Onyike, MD, MHS FTD/Young-Onset Dementias Program Johns Hopkins Neuropsychiatry Disclaimer Dr. Onyike is a principal investigator for the Baltimore site
Overview of the non-alzheimer Dementias Chiadi U. Onyike, MD, MHS FTD/Young-Onset Dementias Program Johns Hopkins Neuropsychiatry Disclaimer Dr. Onyike is a principal investigator for the Baltimore site
ALS, Cognitive Impairment (CI) and Frontotemporal Lobar Dementia (FTLD): A Professional s Guide
 and Frontotemporal Lobar Dementia (FTLD): A Professional s Guide") ALS, Cognitive Impairment (CI) and Frontotemporal Lobar Dementia (FTLD): A Professional s Guide Overview A link between ALS and cognitive dysfunction was first noted in the late 1800 s, but only in the
ALS, Cognitive Impairment (CI) and Frontotemporal Lobar Dementia (FTLD): A Professional s Guide Overview A link between ALS and cognitive dysfunction was first noted in the late 1800 s, but only in the
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Dementia: Diagnosis and Treatment
 Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
02/04/2015. The structure of the talk. Dementia as a motor disorder. Movement, cognition & behaviour. Example 1. Example 2
 The th Annual Memory Clinic Conference Dublin, Trinity College, 27 March 1 The structure of the talk Dementia as a motor disorder Thomas H. Bak Human Cognitive Neuroscience & Centre for Clinical Brain
The th Annual Memory Clinic Conference Dublin, Trinity College, 27 March 1 The structure of the talk Dementia as a motor disorder Thomas H. Bak Human Cognitive Neuroscience & Centre for Clinical Brain
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
EARLY ONSET FRONTOTERMPORAL DEMENTIA AND ALZHEIMERS DISEASE: DIAGNOSIS, TREATMENT AND CARE
 EARLY ONSET FRONTOTERMPORAL DEMENTIA AND ALZHEIMERS DISEASE: DIAGNOSIS, TREATMENT AND CARE John Rudge, BA Hons This thesis is presented as partial requirement for the degree of Doctor of Psychology at
EARLY ONSET FRONTOTERMPORAL DEMENTIA AND ALZHEIMERS DISEASE: DIAGNOSIS, TREATMENT AND CARE John Rudge, BA Hons This thesis is presented as partial requirement for the degree of Doctor of Psychology at
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There