Secondary Stroke Prevention
|
|
|
- Albert Montgomery
- 6 years ago
- Views:
Transcription

1 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical Medicine, Director, University of Toronto Stroke Program Sunnybrook Health Sciences Centre, University of Toronto R.H.Swartz, University of Toronto.
2 Disclosures Salary support: Heart and Stroke Foundation Centre for Stroke Recovery CIHR/CSN Focus on Stroke Advisory Boards: None. Speaker s Honararia: GTA stroke conference, Ontario Stroke Day. Bristol-Myers Squibb Canada Trials: None. No stock in pharmaceutical companies rick.swartz@sunnybrook.ca R.H.Swartz, University of Toronto.
3 Objectives To review basic epidemiology of stroke and rationale for stroke prevention efforts To review secondary prevention strategies and outline an approach to the art & science of secondary prevention R.H.Swartz, University of Toronto.
4 Stroke is a brain attack sudden loss of specific brain functions from damage to one part of the brain secondary to: an interruption of that region s blood supply (ischemic ~ 85%) OR bleeding into that area of brain (hemorrhagic ~15%) R.H.Swartz, University of Toronto

5 R.H.Swartz, University of Toronto
6 Basic epidemiology of stroke 1 stroke every 10 minutes in Canada #1 leading cause of adult disability in Canada 2 nd leading cause of death worldwide Overall, ~20% fatal; 60-75% some disability ~50,000 Canadians annually have strokes resulting in death or serious disability. World Stroke Day Proclamation, Stroke 2008;39 R.H.Swartz, University of Toronto


7 Outcome of Stroke Adapted from Hacke 1998, Asplund, 1997 About 50% are either dead or disabled Prognosis of hemorrhage is worse Adapted from Stegmayr B, et al. Stroke 1997;28:
8 Stroke outcome in round numbers For every 10 stroke patients 2 will die 2 will recover 6 will be left with disability ICES data, 2001 Dr. David Gladstone, 2004
9 Basic epidemiology of stroke ~300,000 Canadian survivors live at risk for: another stroke (20% in 2 years) post-stroke dementia & post-stroke depression. < 50% survivors return to work lost income. 50% caregivers develop emotional illness within 1 year (care for the caregivers). Estimated direct and indirect costs of stroke are ~$4 BILLION annually in Canada. R.H.Swartz, University of Toronto
10 So Strokes are common (and silent strokes = 3x symptomatic!) Strokes kill and disable people. Fortunately, some of this burden is also preventable Stroke is common, serious and treatable we can make a difference R.H.Swartz, University of Toronto
11 A brief interlude for motivation We will cure more people by aggressively managing risk factors than we will EVER cure with tpa. R.H.Swartz, University of Toronto
12
13 Primary Prevention of Stroke Primary prevention means treating us modifying risk factors before symptoms or illnesses occur (individuals & populations) We treat far more people for primary prevention, and the event you re trying to prevent is rarer. Thus, treatments have to be VERY safe and effective in populations. R.H.Swartz, University of Toronto
14 Primary Prevention of Stroke (& heart disease) Blood pressure lowering Atrial fibrillation (CHADS 2 ) Smoking cessation Diabetes treatment Cholesterol treatment Weight loss / abdominal obesity / exercise Low-risk drinking guidelines Stroke. 2006;37: R.H.Swartz, University of Toronto
15 Secondary Stroke Prevention Treatment of those with prior stroke or TIA, regardless of etiology 1) Why treat? 2) When to treat? 3) Who to treat? 4) What to treat? R.H.Swartz, University of Toronto
16
17 Secondary Prevention 1) Why treat? In people with TIAs discharged from ER: 12% are readmitted to hospital within 30 days 9 12% recurrent stroke or death within 30 days! 9% for TIA with speech deficit 12% for TIA with motor deficit Also need to treat FAST Gladstone et al. CMAJ 2004 R.H.Swartz, University of Toronto

18 Secondary Prevention 2) when? Stroke After TIA Canadian Data (slide courtesy Dr. F. Silver) 9.5 % 14.5 % 21.8 %
19 When treat? Early Risk of Stroke After TIA Gladstone et al. CMAJ 2004 Half of the strokes occurred in the first 2 days (slide courtesy Dr. D. Gladstone)
20 2) When to treat? 23% of patients with ischemic stroke have had a TIA before their stroke 17% occur the day of the stroke, 9% the previous day, 43% had a TIA during the 7 days prior to the stroke. pooled analysis from population and RCT s (OXVASC, OCSP, UK-TIA and ECST). Rothwell & Warlow, Neurology, 2005;64: R.H.Swartz, University of Toronto
21 2) When to treat? EXPRESS Study Rothwell et al. Lancet 2007 Phase 1 vs day stroke risk from 10% to 2% Medications started right away Carotid endarterectomy expedited R.H.Swartz, University of Toronto
22 2) When to treat? Urgent assessments prevent stroke FASTER Kennedy et al. Lancet Neurology 2007 Fast Assessment of Stroke and TIA to prevent Early Recurrence ASA +/- clopidogrel +/- simvastatin in 24 hours Stroke risk: 10.8% vs. 7.1% in favour of ASA/clopidogrel combination (n.s.) SOS-TIA Lavallee et al. Lancet Neurol hours TIA unit had lower event rates than expected from ABCD 2 score (1.24% vs. 5.96%)
23 Secondary Prevention 3)Who to treat? Risk Stratification with ABCD2 vs. Motor or speech TIA s Age 1 point if >60 years Blood pressure 1 point if sbp >140 or dbp >90 Clinical features 2 points for unilateral weakness; 1 point speech deficit without weakness Duration 2 points if >60 min; 1 point if >10-59 min Diabetes 1 point 2-day stroke risk: 1% (0-3 points), 4% (4-5 points), 8% (6-7 points) 90-day stroke risk up to 25% Johnston, Rothwell, et al. Lancet 2007; 369:283-92
24 Who to treat? The problem with ABCD s It isn t always as simple as the ABC s For example: 61 y.o. woman with mild HTN and diet controlled DM, who had >2 hours of dizziness 58 y.o. man without diabetes or hypertension but had a 15 minute episode of right face, arm and leg weakness, with speaking gibberish and not understanding speech. Gladstone et al. CMAJ 2004 R.H.Swartz, University of Toronto
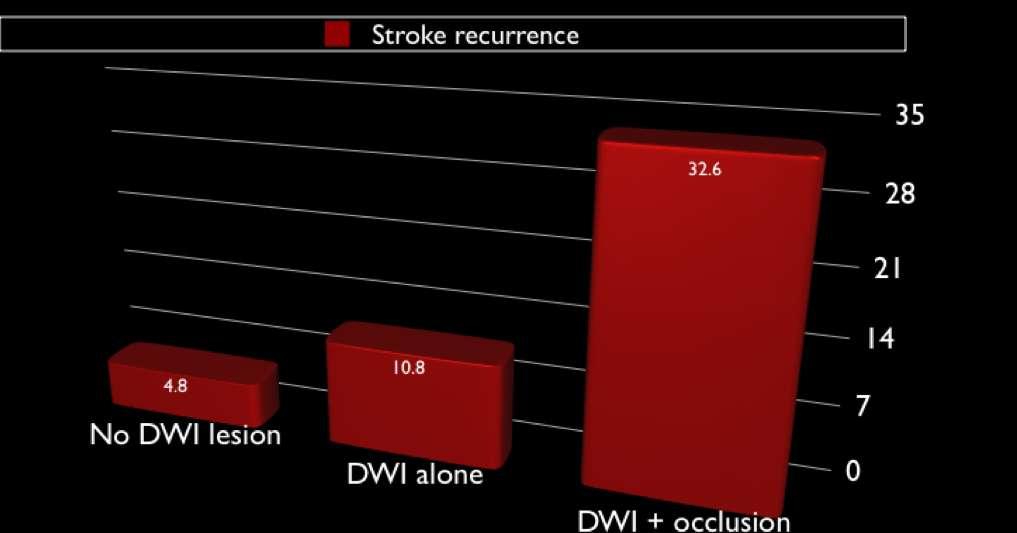
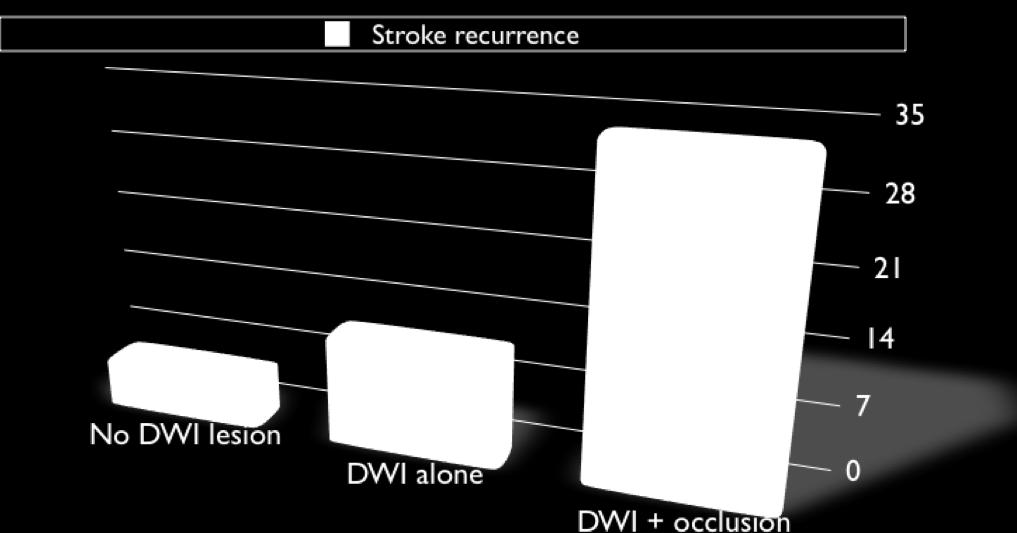
25 3) Who to treat? Defining high risk. ABCD2 + MRI (DWI / intracranial vessel occlusions) Coutts et al., Int J. Stroke 2008; AnnNeurol 2005 R.H.Swartz, University of Toronto
26


27 The future of TIA Triaging?
28 Secondary Prevention 4) What to treat? 1) Look at the intracranial vessels: atherosclerosis, moya-moya, inflammatory diseases 2) Look at the neck: Carotid stenosis, dissections 3) Look at the heart: Atrial fibrillation (+/- valve etc.) 4) Look at the blood: Platelet, APLA etc. 5) Look at the patient: risk factor modification (hypertension, high cholesterol, diabetes, smoking, drinking, diet/exercise, social situation) R.H.Swartz, University of Toronto
29 Percentage 3-Month Stroke Risk According to Etiological Subtype Lovett et al. Neurology 2004: meta-analysis, n= small vessel unknown cardiac large vessel TOAST Classification (slide courtesy Dr. D. Gladstone)
30 What to treat: A) Symptomatic Carotid Stenosis Severe stenosis (70-99%) surgery highly beneficial (NNT=3*) Moderate stenosis (50-69%) surgery beneficial (NNT=7*) Mild stenosis (<50%) No surgery (slide courtesy Dr. D. Gladstone)

31 Timing of Carotid Surgery Rothwell et al. Lancet 2004 NNT to prevent one stroke at 5 years: NNT = 5 if surgery within 2 weeks NNT = 125 if surgery delayed >3 months! (slide courtesy Dr. D. Gladstone)
32 Management of Surgical Carotid Disease 2008 Canadian Best Practice Recommendations TIA or non-disabling stroke and ipsilateral 70% 99% ICA stenosis should be offered carotid endarterectomy within 2 weeks unless contraindicated Appropriate antiplatelet therapy depends on timing: Surgery in 24 hours: consider ASA Surgery in 1-2 weeks: consider combination ASA + clopidogrel Ensure optimal management of vascular risk factors * CMAJ 2008;179(12 Suppl):S1-S25.
33 What to treat? B) Atrial Fibrillation Atrial fibrillation (CHADS 2 ): Atrial fibrillation increases stroke risk 3-5x Higher risks: CHF, HTN, Age, DM, prior stroke/tia (2) CHADS Score Risk Stroke Rate / yr Recommendation 0 low <2 % ASA mg/d 1 low-mod <2 % warfarin INR 2-3 OR ASA 2 mod 4 % warfarin INR high 5.9 % warfarin INR v. high 8 18 % warfarin INR 2-3 Gage et al, JAMA 2001;285(22): R.H.Swartz, University of Toronto

34 Stroke Prevention R.H.Swartz, University of Toronto
35 Prevalence (%) Strokes Attributable to Atrial Fibrillation AF prevalence Strokes attributable to AF Age (years) Wolf, Stroke 1991;22:983-8 (slide courtesy Dr. F. Silver)
36 Warfarin: RRR in Stroke 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% SPINAF CAFA BAATAF SPAF I AFASK All Patients Hart RG Ann Intern Med 131: , 1999

37 Gladstone et al, Stroke 2009
38 4) What to treat? C) Vascular risks Blood pressure: Common. >2/3 of adults >65 The most important modifiable risk factor (2-5 x) Ischemic, bleeding, silent strokes Contributes to: Large-vessel atherosclerotic disease Small-vessel (lacunar) disease LV dysfunction and Afib Untreated HTN increases stroke risk 3-4 times. Treatment can reduce stroke risk and fatalities ~40%. Most patients require 2 or more agents CHEP guidelines <140/90 (or if diabetes <130/80) Stroke. 2006;37: R.H.Swartz, University of Toronto
39 4) What to treat? C) Vascular risks Diabetes: ~2x increased risk of stroke. Highly correlated w/ HTN, high cholesterol, weight and sedentary lifestyles. Target HbA1c <0.07. Treatment reduces microvascular complications > macrovascular. Cholesterol: 2x increased risk of stroke. Risk for CAD (which independently also increases stroke risk). SPARCL (NNT = 50) Stroke. 2006;37: R.H.Swartz, University of Toronto
40 4) What to treat? C) Vascular risks Smoking: 2 6 x risk (2x with second hand smoke only); normalizes >5 yrs, independent of age one-time advice from physician results in 2% of smokers quitting for >1 yr Weight loss, exercise, abdominal obesity: 2-6x increased stroke risk with obesity. Treatments: lowcalorie, low-fat, low-sodium diet, minutes of moderate exercise most days R.H.Swartz, University of Toronto
41 4) What to treat? C) Vascular risks Anti-platelets (Aspirin (ASA), Clopidogrel (Plavix), ASA/ER-dipyridimol (Aggrenox)): Low-dose ASA 1 o prevention in people at risk increases GI bleed & hemorrhagic stroke risk mg daily as effective as higher doses. Stroke. 2006;37: R.H.Swartz, University of Toronto
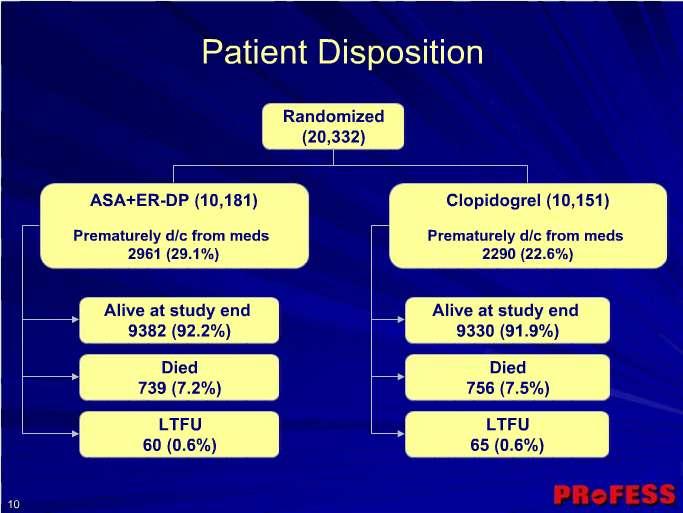
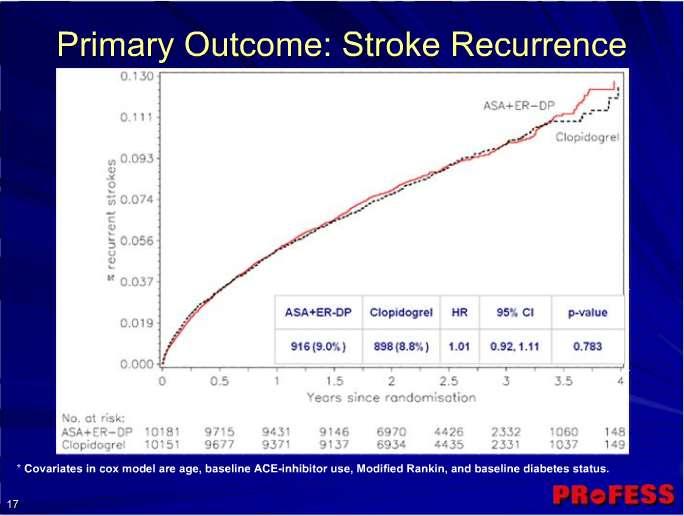
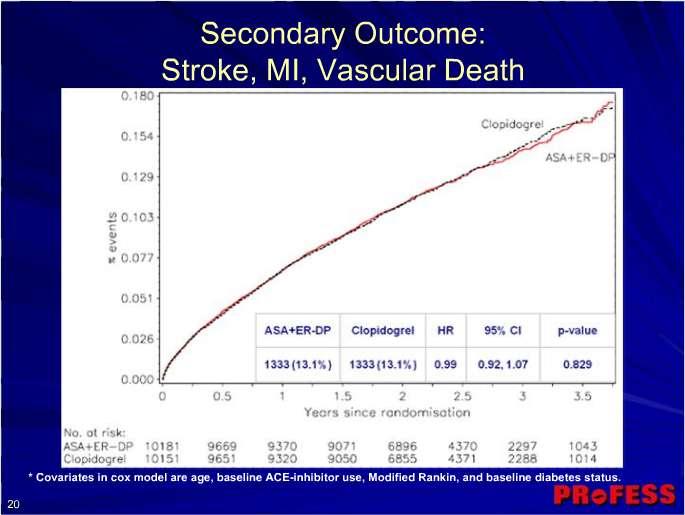
42 4) What to treat? C) Vascular risks Deciding between anti-platelets?! CAPRIE (ASA vs. Plavix), CURE (Plavix/ASA vs placebo/asa post-acs), ESPS2 and ESPRIT (ASA plus ER dipyridamole vs. ASA) MATCH (Plavix vs. ASA/plavix): bleeding higher w/ combined ASA/Plavix (risk increases with long-term use) PROFESS: no decisions between Plavix and Aggrenox Stroke. 2006;37: R.H.Swartz, University of Toronto

43
44
45
46
47 Smoking cessation: Stroke Prevention 2 6 x increased risk (2x with second hand smoke); normalizes 5 yrs after quitting, independent of age one-time advice from physician results in 2% of smokers quitting for >1 yr Weight loss, exercise, abdominal obesity: 2-6x increased stroke risk with obesity. Treatments: lowcalorie, low-fat, low-sodium diet, minutes of moderate exercise most days R.H.Swartz, University of Toronto
48 Stroke Prevention We will cure more people by aggressively managing risk factors than we will EVER cure with tpa. R.H.Swartz, University of Toronto
49 Secondary Prevention: What to treat? 1) Look at the intracranial vessels: atherosclerosis, moya-moya, inflammatory diseases 2) Look at the neck: Carotid stenosis, dissections 3) Look at the heart: Atrial fibrillation (+/- valve etc.) 4) Look at the blood: Platelet, APLA etc. 5) Look at the patient: risk factor modification (hypertension, high cholesterol, diabetes, smoking, drinking, diet/exercise, social situation) R.H.Swartz, University of Toronto
50 Summary: Stroke Prevention Strokes are common and serious We can identify high risk patients We have effective stroke prevention therapies But current management is often suboptimal Primary prevention: do the things we should do anyway Secondary prevention: Look at the brain vessels, neck, heart, blood and patient Treat TIA s early and aggressively Expedite surgery for symptomatic carotid artery disease Anticoagulate patients with atrial fibrillation Anti-platelets and other risk reduction for everyone else!
51
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
TRANSIENT ISCHEMIC ATTACK (TIA)
") TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin?
 MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE
 KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Disclosures. An Update on TIA and Minor Stroke. The Agenda PROGNOSIS PATHOPHYSIOLOGY GUIDELINES AND PROVEN MANAGEMENT STRATEGIES AGGRESSIVE TREATMENT
 Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
44TH ANNUAL RECENT ADVANCES IN NEUROLOGY
 Presenter Disclosure Information J. Donald Easton, MD Clinical Professor of Neurology February 17, 2011 44TH ANNUAL RECENT ADVANCES IN NEUROLOGY TIA: Definition, Evaluation, and Treatment J. Donald Easton,
Presenter Disclosure Information J. Donald Easton, MD Clinical Professor of Neurology February 17, 2011 44TH ANNUAL RECENT ADVANCES IN NEUROLOGY TIA: Definition, Evaluation, and Treatment J. Donald Easton,
Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia
 GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
Stroke and TIA. Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne
 Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne Global burden of stroke 20 million strokes each year 2 nd leading cause of
Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne Global burden of stroke 20 million strokes each year 2 nd leading cause of
Understanding Risk Factors for Stroke
 MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Understanding Risk Factors for Stroke About This Kit Risk factors have been identified that can predict who is most
MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Understanding Risk Factors for Stroke About This Kit Risk factors have been identified that can predict who is most
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE OR TIA December 8, 2017
 KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE OR TIA December 8, 2017 1 Faculty Disclosure Faculty: Grant Stotts MD, FRCPC Assistant Professor, uottawa Brain and Mind Institute
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE OR TIA December 8, 2017 1 Faculty Disclosure Faculty: Grant Stotts MD, FRCPC Assistant Professor, uottawa Brain and Mind Institute
Stroke secondary prevention. Gill Cluckie Stroke Nurse Consultant St. George s Hospital
 Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Strokes , The Patient Education Institute, Inc. hp Last reviewed: 11/11/2017 1
 Strokes Introduction A stroke or a brain attack is a very serious condition that can result in death and significant disability. This disease is ranked as the third leading cause of death in the United
Strokes Introduction A stroke or a brain attack is a very serious condition that can result in death and significant disability. This disease is ranked as the third leading cause of death in the United
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Asymptomatic Carotid Stenosis To Do or Not To Do
 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Stroke Support Group
 Mercy Walworth Hospital and Medical Center Stroke Support Group Angie Schnobel, MS, CCC-SLP Hannah Herland, MOTR/L Karen Graham, LPTA MercyWalworthStrokeSupport.org Meeting second Tuesday of the month
Mercy Walworth Hospital and Medical Center Stroke Support Group Angie Schnobel, MS, CCC-SLP Hannah Herland, MOTR/L Karen Graham, LPTA MercyWalworthStrokeSupport.org Meeting second Tuesday of the month
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Long-Term Care Updates
 Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Speakers. 2015, American Heart Association 1
 Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS?
 IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS? J.Y. LE HEUZEY Georges Pompidou Hospital, René Descartes University, Paris H E G P Munich, August 27, 2012 Disclosure Consultant / Conferences / Advisory
IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS? J.Y. LE HEUZEY Georges Pompidou Hospital, René Descartes University, Paris H E G P Munich, August 27, 2012 Disclosure Consultant / Conferences / Advisory
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
La terapia antiaggregante nel paziente con stroke
 La terapia antiaggregante nel paziente con stroke Paolo Gresele Dipartimento di Medicina, Sez. Medicina Interna e Cardiovascolare Università di Perugia XXVII Congresso Nazionale FCSA Milano, 20-22 Ottobre
La terapia antiaggregante nel paziente con stroke Paolo Gresele Dipartimento di Medicina, Sez. Medicina Interna e Cardiovascolare Università di Perugia XXVII Congresso Nazionale FCSA Milano, 20-22 Ottobre
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology
 Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Subject Expert. Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO
 Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
TIA triage in Not all that glitters is gold
 TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
Luisa Vinciguerra. Ictus recidivanti
 Luisa Vinciguerra Ictus recidivanti Recurrent Strokes DEFINITION Population-based studies exclude strokes: - within 28 or 21 days of the incident event - events in the same vascular territory as the original
Luisa Vinciguerra Ictus recidivanti Recurrent Strokes DEFINITION Population-based studies exclude strokes: - within 28 or 21 days of the incident event - events in the same vascular territory as the original
Ischemic stroke: management, prevention and follow up. Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute
 Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Steps Against Recurrent Stroke (STARS)
") Steps Against Recurrent Stroke (STARS) Take steps against recurrent stroke by making the necessary changes in your life. Your Guide to Ischemic What happened to me? You had a stroke. The stroke you had
Steps Against Recurrent Stroke (STARS) Take steps against recurrent stroke by making the necessary changes in your life. Your Guide to Ischemic What happened to me? You had a stroke. The stroke you had
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Cryptogenic Stroke: What Don t We Know. Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare
 Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
WHAT IS A STROKE? What causes a stroke? What disabilities can result from a stroke?
 Know Stroke Stroke is the third leading cause of death in the United States and a leading cause of serious, long-term disability in adults. About 600,000 new strokes are reported in the U.S. each year.
Know Stroke Stroke is the third leading cause of death in the United States and a leading cause of serious, long-term disability in adults. About 600,000 new strokes are reported in the U.S. each year.
Epidemiology and Prevention of Stroke
 Copyright Information Copyright protected material has been deleted from this presentation. References to the deleted material are provided for each slide. Epidemiology and Prevention of Stroke Larry B.
Copyright Information Copyright protected material has been deleted from this presentation. References to the deleted material are provided for each slide. Epidemiology and Prevention of Stroke Larry B.
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Liping Liu Dpet. of Neurology and Stroke Center Beijing Tiantan Hospital Capital Medical University
 Liping Liu Dpet. of Neurology and Stroke Center Beijing Tiantan Hospital Capital Medical University Disclosures Conflict of interest disclosures: No Disclosures Funding The CHANCE trial is funded by the
Liping Liu Dpet. of Neurology and Stroke Center Beijing Tiantan Hospital Capital Medical University Disclosures Conflict of interest disclosures: No Disclosures Funding The CHANCE trial is funded by the
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen
 What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
TREATMENT OF STROKE PATIENTS THAT ARE TAKING NOVEL ANTICOAGULANTS. Jesse Weinberger, MD The Icahn School of Medicine at Mount Sinai
 TREATMENT OF STROKE PATIENTS THAT ARE TAKING NOVEL ANTICOAGULANTS Jesse Weinberger, MD The Icahn School of Medicine at Mount Sinai Acknowledgement Many of the slides for this presentation were obtained
TREATMENT OF STROKE PATIENTS THAT ARE TAKING NOVEL ANTICOAGULANTS Jesse Weinberger, MD The Icahn School of Medicine at Mount Sinai Acknowledgement Many of the slides for this presentation were obtained
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Conflicts of Interest: None. Aspirin, primary prevention and USPSTF. Primary prevention of ASCVD is important
 Aspirin, primary prevention and USPSTF Presented by: Craig Williams, PharmD., BCPS., FNLA; February 2017 Conflicts of Interest: None Primary prevention of ASCVD is important Myocardial Infarction Incidence
Aspirin, primary prevention and USPSTF Presented by: Craig Williams, PharmD., BCPS., FNLA; February 2017 Conflicts of Interest: None Primary prevention of ASCVD is important Myocardial Infarction Incidence
Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham
 New Guidelines for SPAF Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham Stroke prevention and atrial fibrillation Epidemiology of atrial fibrillation How common is it?
New Guidelines for SPAF Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham Stroke prevention and atrial fibrillation Epidemiology of atrial fibrillation How common is it?
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Section Editor Scott E Kasner, MD
 1 of 6 9/29/2013 6:55 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
1 of 6 9/29/2013 6:55 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
Atrial Fibrillation. 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018
 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
E X P L A I N I N G STROKE
 EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Update in the Literature 2012
 Update in the Literature 2012 Mel L. Anderson, MD, FACP Chief, Hospital Medicine Section Associate Chief, Medical Service Denver VA Medical Center Associate Professor of Medicine University of Colorado
Update in the Literature 2012 Mel L. Anderson, MD, FACP Chief, Hospital Medicine Section Associate Chief, Medical Service Denver VA Medical Center Associate Professor of Medicine University of Colorado
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Game Strategy: High Intensity Statin in Stroke. K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018
 Game Strategy: High Intensity Statin in Stroke K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018 No Disclosures Are you Mind Full or Mindful? Objectives 1. Discuss the correlation between
Game Strategy: High Intensity Statin in Stroke K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018 No Disclosures Are you Mind Full or Mindful? Objectives 1. Discuss the correlation between
Consequences of stroke and AF
 Consequences of stroke and AF Lorenzo G Mantovani Center of Pharmacoeconomics University of Naples Center for Public Health Research University of Milan Bicocca Questions Is stroke frequent? Is stroke
Consequences of stroke and AF Lorenzo G Mantovani Center of Pharmacoeconomics University of Naples Center for Public Health Research University of Milan Bicocca Questions Is stroke frequent? Is stroke
Document Title: The Management of Acute Ischemic Stroke & TIA
 Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis?
 for stroke prevention in patients with asymptomatic carotid stenosis?") How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis? Dorothee Saur Department of Neurology University of Leipzig Disclosure for Dorothee
How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis? Dorothee Saur Department of Neurology University of Leipzig Disclosure for Dorothee
Understanding transient ischaemic attack
 chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Stroke Quality Measures. Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed: May, 2012 Most recently updated: December 2012
 1 Stroke Quality Measures Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed: May, 2012 Most recently updated: December 2012 2 Application of the Stroke Measure Set The stroke
1 Stroke Quality Measures Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed: May, 2012 Most recently updated: December 2012 2 Application of the Stroke Measure Set The stroke
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015
 in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015") Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to
 It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK
 Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
How do we assess risk in TIA?
 How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
Preoperative Management of Patients Receiving Antithrombotics
 Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
AF stroke prevention in the Canadian context
 AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor
 Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor What is TIA? TIA vs CVA, does it matter? Who needs the hospital? What is the ABCD 2
Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor What is TIA? TIA vs CVA, does it matter? Who needs the hospital? What is the ABCD 2
Peripheral Arterial Disease Medical Approach and Management
 Peripheral Arterial Disease Medical Approach and Management April 2, 2016 Michael F. Hagerty, MD FACC PAD: Classic and New Concepts Let s take a look at what s new and what s old or classic in 2016. PAD:
Peripheral Arterial Disease Medical Approach and Management April 2, 2016 Michael F. Hagerty, MD FACC PAD: Classic and New Concepts Let s take a look at what s new and what s old or classic in 2016. PAD:
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
NORTH MISSISSIPPI MEDICAL CENTER MEDICAL CENTER. Stroke: Are you at risk? A guide to stroke risk factors & resources at ACUTE STROKE UNIT
 North Mississippi Medical Center Acute Stroke Unit 830 South Gloster Street Tupelo, MS 38801 (662) 377-3000 or 1-800-THE DESK (1-800-843-3375) www.nmhs.net Stroke: Are you at risk? A guide to stroke risk
North Mississippi Medical Center Acute Stroke Unit 830 South Gloster Street Tupelo, MS 38801 (662) 377-3000 or 1-800-THE DESK (1-800-843-3375) www.nmhs.net Stroke: Are you at risk? A guide to stroke risk
The Impact of Smoking on Acute Ischemic Stroke
 Smoking The Impact of Smoking on Acute Ischemic Stroke Wei-Chieh Weng, M.D. Department of Neurology, Chang-Gung Memorial Hospital, Kee-Lung, Taiwan Smoking related mortality Atherosclerotic vascular disease
Smoking The Impact of Smoking on Acute Ischemic Stroke Wei-Chieh Weng, M.D. Department of Neurology, Chang-Gung Memorial Hospital, Kee-Lung, Taiwan Smoking related mortality Atherosclerotic vascular disease