MANAGEMENT OF PATIENT WITH DEMENTIA SSA PERSPECTIVE
|
|
|
- Austin Cunningham
- 6 years ago
- Views:
Transcription
1 MANAGEMENT OF PATIENT WITH DEMENTIA SSA PERSPECTIVE Njideka U. Okubadejo, MBChB, FMCP Associate Professor & Consultant Neurologist College of Medicine, University of Lagos, & Lagos University Teaching Hospital Lagos, Nigeria
2 OUTLINE Background Approach to management History taking Physical education Cognitive testing Laboratory investigations Neuroimaging Treatment: Pharmacological/Non-pharmacological Issues in management in SSA
3 BACKGROUND Chronic, typically progressive neurologic disorder. Adversely affects higher cortical functions including memory, thinking and orientation. Most common cause is Alzheimer s disease. Significantly impairs quality of life. Associated with disability, mortality, significant psychosocial and economic consequences for individual affected, their families, communities and nations.
4 Case history Mrs. OL, a 75 year old retired primary school teacher is brought to the clinic, accompanied by her daughter, who complains that her previously meticulous mother is increasingly forgetful, missing appointments, misplacing her handbag and money, and less wellkempt than before. She thinks this has been going on for about a year, and recently has difficulty recalling the date and month. She seems more withdrawn, and avoids coming out of her room when there are guests in the house. She also started wandering about aimlessly and formed a habit of keeping her unwashed underwear under her pillow. She often insists that she has had a bath, and resists being assisted to bathe in the mornings. There have been a few episodes of bedwetting at night. She prefers to wear the same clothes repeatedly despite a drawer full of new clothe bought by her daughter. About a week ago, her daughter relocated her to her home, and since then she appears more confused, often losing her way within the house. Mrs. OL is of the opinion that nothing is wrong and her daughter has brought her to you for a normal checkup.
5 Questions o Do you think the daughter is overly concerned and there is nothing wrong as the patient asserts? o What will your approach be to establishing a diagnosis? o Who will you focus management on: mother or daughter?
6 Approach to management Thorough history Physical examination Cognitive testing Laboratory investigations Neuroimaging Patient and caregiver education Nonpharmacologic treatment Pharmacologic treatment Follow-up visits
7 History taking Establish reason(s) for consultation Allow patient account and caregiver account Explore aspects of cognitive functioning (memory, language use, etc) and effect on activities of daily living Ask about behavioural changes withdrawal, aggressiveness, sexual disinhibition, wandering, etc. Enquire concerning mode of onset, duration, progression of symptoms, other neurologic symptoms (including depression), general medical history. Specifically ask about: diabetes, hypertension, cigarette smoking, alcohol use, nutrition, family history.
8 Physical examination Be gentle and explain what you want to do to the patient General physical examination: look out for anemia, clues to malnutrition, general hygiene Neurologic examination: examine for focal lesions (especially cranial nerves and muscle power), asymmetry, deep tendon reflexes, primitive reflexes Examine the cardiovascular system: pulse, blood pressure, praecordium
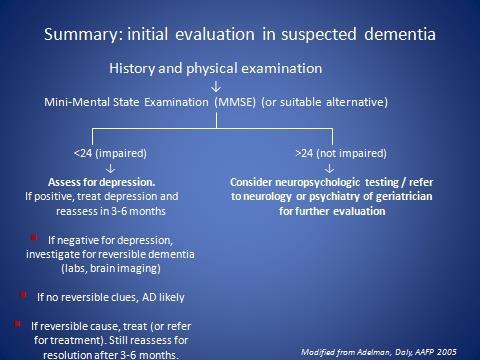
9 Cognitive testing Perform a bedside cognitive test MMSE most widely used Some local translations available Be aware that educational level may affect responses. May use alternative tests that are less affected by education/literacy. Learn to interpret the findings in conjunction with history and other features (not in isolation)
10 Cognitive testing ii Severity of cognitive impairment using MMSE Normal cognitive function: MMSE Mild cognitive impairment: MMSE Moderate cognitive impairment : MMSE Severe cognitive impairment : MMSE <10 Reference: NICE, UK
11 Laboratory investigations Baseline (to exclude reversible causes of dementia) Full blood count (Hb, WBC, differentials, platelets) Serum electrolytes, BUN, creatinine Blood glucose Lipid profile Serology (HIV) may be done Serum B12 levels (urine MMA) if available Liver function tests Thyroid function tests May be indicated: EEG, Lumbar puncture
12 Neuroimaging To exclude structural cause of dementia To explore for other forms of dementia: vascular, normal pressure hydrocephalus Brain CT scan Brain MRI scan
 Coronal MRIs.")

13 AD MRI brain scan Normal Alzheimer's disease (advanced) Coronal MRIs. In AD, widened sulci, enlarged ventricles and gaping temporal horns, reflecting cortical and hippocampal atrophy.
14
15 Treatment of reversible dementia Treat any reversible cause found (e.g. hypothyroidism) May be a co-morbidity rather than actual cause of cognitive decline Reassess cognitive function after a reasonable period following treatment of potentially reversible cause Reassessment after 3 6 months reasonable If still impaired, consider Alzheimer's or other irreversible dementia
16 TREATMENT OF ALZHEIMER S DEMENTIA
17 Goals of treatment Maintain / improve quality of life Improve / maximize functioning Slow decline in cognition (if feasible) Treat/control/modify co-morbid mood, behavioural and medical conditions Ease caregiver burden
18 Patient and caregiver education Key to successful management May require separate encounters. Obtain consent from patient where feasible Identify responsible family member(s) to communicate diagnosis and care plan Empathetically convey prognosis/expected progression Emphasize importance of general care, safety, assistance, social support Discuss treatment options /expected responses (including cost implications)
19 APPROACH TO TREATMENT Multidisciplinary approach!!! Neurologist/Geriatrician/Psychiatrist/Physician with special interest in dementia/geriatrics/neurology Nurse/nurse specialists Neuropsychologist/clinical psychologist Physical therapists Occupational therapists Social worker Others.
20 Pharmacologic treatment Applicable to: treatment of cognitive symptoms treatment of co-morbid mood / behavioural problems treatment of any co-morbid disease (e.g. hypertension or diabetes)
21 Pharmacologic Tx: cognitive symptoms Based on cholinergic hypothesis of memory impairment: cognitive and behavioural changes in AD are due to cholinergic deficits Medication may slow decline in functioning; does not restore lost function. May not work in some. NOT A CURE FOR DEMENTIA! Cholinesterase inhibitors: Useful when impairments affect functioning Indicated for mild to moderate AD. S/E: nausea, diarrhea, dizziness Donepezil 5-10 mg/day Galantamine 4 8 mg BD (16-24 mg/d) Rivastigmine mg BD (6-12 mg/d) Antiglutamate: Indicated for severe dementia. S/E: dizziness, worsen aggression, confusion Memantine: start dose: 5 mg/d, increasing gradually to 10 mg BD
22 Cholinesterase inhibitors should be considered in mild to moderate AD, although studies suggest a small average degree of benefit Vitamin E (1000 IU po BID) should be considered in an attempt to slow progression of AD Insufficient evidence to support use of other antioxidants, antiinflammatories, or other putative disease-modifying agents to treat AD Neurology 2001;56:
23 Pharmacologic Tx: behavioural symptoms Antipsychotic medication used when environmental manipulation fails to control agitation, combativeness, or psychosis Atypical antipsychotics (e.g. risperidone) preferred to traditional agents (e.g. haloperidol) Antidepressant medication to treat depression in patients with dementia SSRI s preferred. Selected MAO-B inhibitors and tricyclic antidepressants may be used.
24 Non-pharmacologic treatment Regular exercise: within reason; tailored; walking; dance Regular routine: limit disruptions and changes Sleep: regular hours; daytime naps may cause insomnia Meals: regular, avoid heavy meals at night Dressing, grooming and bathing: supervise, assist, guide Toileting: prompted voiding; post-prandial voiding; adult diapers Music (esp during meals, bathing), religious activities Photo albums, familiar company, happy memories Regular brain stimulation: Ludo, cards, Sudoku, Scrabble Home/environmental modification: safety, familiarity
25 Caregivers / Family members Patience with repetitive behaviours Behaviours are not intentional and may not be amenable to counseling/advice/scolding Speak slowly; simple ideas; simple instructions Avoid reacting to emotional outbursts and suspicion Engage by distraction, change of scene, walks Ask for help/support take a break; get help/support Psychosocial interventions: (e.g. education, support, respite care) improve caregiver QoL and emotional well-being.
26 Family involvement Plan for the future Plan early while patient can still contribute Address: living conditions/arrangements finances healthcare decision making? Identification of responsible next of kin
27 MANAGEMENT ISSUES IN SSA Delayed diagnosis, no diagnosis and misdiagnosis Access to trained professional care Patient education Caregiver education Caregiver burden: social support Access to pharmacologic therapy: out-of-pocket cost Support services: daycare, nursing homes, rehabilitation services Cultural barriers to care Economic barriers to care
If you have dementia, you may have some or all of the following symptoms.
 About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center
 Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
Forgetfulness: Knowing When to Ask for Help
 National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Session outline. Introduction to dementia Assessment of dementia Management of dementia Follow-up Review
 Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
To help you prepare for your doctor's visit, the Alzheimer Society has developed the following list:
 The Alzheimer Society has a tool kit to help you prepare for a conversation with your doctor or health provider about your concerns and questions about a possible dementia diagnosis. Symptoms of dementia
The Alzheimer Society has a tool kit to help you prepare for a conversation with your doctor or health provider about your concerns and questions about a possible dementia diagnosis. Symptoms of dementia
Dementia Basics. Welcome! What to expect and how to handle a dementia diagnosis. In partnership with Scripps Health.
 Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Introduction to Dementia: Diagnosis & Evaluation. Created in March 2005 Duration: about 15 minutes
 Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care.
 Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Dr. Adeniyi Mofoluwake and Stacy Kramer
 Dr. Adeniyi Mofoluwake and Stacy Kramer Definition of Alzheimer s Disease Alzheimer's disease is a neurological disorder in which insidious onset of the death of brain cells causes memory loss and cognitive
Dr. Adeniyi Mofoluwake and Stacy Kramer Definition of Alzheimer s Disease Alzheimer's disease is a neurological disorder in which insidious onset of the death of brain cells causes memory loss and cognitive
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Evaluations. Alzheimer s Disease A Public Health Response. Viewer Call-In. July 19, Guest Speakers. Thanks to our Sponsors:
 Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Alzheimer s disease. The facts in brief
 Alzheimer s disease Dementia is an umbrella term used to describe various conditions which damage brain cells and lead to a loss of brain function over time. Dementia causes a progressive decline in a
Alzheimer s disease Dementia is an umbrella term used to describe various conditions which damage brain cells and lead to a loss of brain function over time. Dementia causes a progressive decline in a
4/11/2017. The impact of Alzheimer s disease. Typical changes. The impact of Alzheimer s disease. Problematic changes. Problematic changes
 The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
Dementia NICE Guidelines Update. Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018
 26 September 2018") Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
homeinstead.com Each Home Instead Senior Care franchise office is independently owned and operated Home Instead, Inc.
 Each Home Instead Senior Care franchise office is independently owned and operated. 2010 Home Instead, Inc. homeinstead.com Many of us may joke about having old timers disease, but when cognitive impairment
Each Home Instead Senior Care franchise office is independently owned and operated. 2010 Home Instead, Inc. homeinstead.com Many of us may joke about having old timers disease, but when cognitive impairment
Understanding. Alzheimer s Disease. Lora, diagnosed in 2004, with her daughter, Jill.
 Understanding Alzheimer s Disease Lora, diagnosed in 2004, with her daughter, Jill. What Is Alzheimer s Disease? Alzheimer s disease is a neurologic disorder that affects the brain. It causes dementia.
Understanding Alzheimer s Disease Lora, diagnosed in 2004, with her daughter, Jill. What Is Alzheimer s Disease? Alzheimer s disease is a neurologic disorder that affects the brain. It causes dementia.
Community Pharmacy Dementia Audit
 Community Pharmacy Dementia Audit Introduction To comply with the NHS contractual requirements associated with the Clinical Governance Essential Service, pharmacy contractors must perform an annual practice
Community Pharmacy Dementia Audit Introduction To comply with the NHS contractual requirements associated with the Clinical Governance Essential Service, pharmacy contractors must perform an annual practice
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego
 Dementia Skills for In-Home Care Providers Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego Objectives Familiarity with the most common
Dementia Skills for In-Home Care Providers Seniors Helping Seniors September 7 & 12, 2016 Amy Abrams, MSW/MPH Education & Outreach Manager Alzheimer s San Diego Objectives Familiarity with the most common
Module: Dementia. Overview. Learning objectives. Key messages DEM
 Module: Dementia Overview Learning objectives Promote respect and dignity for people with dementia. Know common presentations of dementia. Know the assessment principles of dementia. Know the management
Module: Dementia Overview Learning objectives Promote respect and dignity for people with dementia. Know common presentations of dementia. Know the assessment principles of dementia. Know the management
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Diagnosis and assessment
 PBO 930022142 NPO 049-191 Diagnosis and assessment If you are close to someone who is feeling confused, agitated or forgetful, you may like to suggest that the person see their general practitioner (GP).
PBO 930022142 NPO 049-191 Diagnosis and assessment If you are close to someone who is feeling confused, agitated or forgetful, you may like to suggest that the person see their general practitioner (GP).
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
Alzheimer Disease and Related Dementias
 Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Alzheimer Disease and Related Dementias. Alzheimer Society of Manitoba Dr. David Strang
 Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Understanding Dementia
 Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Cognitive and Behavioral Changes in ALS: A Guide for People with ALS and their Families
 Cognitive and Behavioral Changes in ALS: A Guide for People with ALS and their Families Overview If you had asked doctors about ALS 15 years ago, the majority of providers would have told you that ALS
Cognitive and Behavioral Changes in ALS: A Guide for People with ALS and their Families Overview If you had asked doctors about ALS 15 years ago, the majority of providers would have told you that ALS
Appendix K: Evidence review flow charts
 K.1 Dementia diagnosis K.1.1 Dementia diagnosis What are the most effective methods of primary assessment to decide whether a person with suspected dementia should be referred to a dementia service? What
K.1 Dementia diagnosis K.1.1 Dementia diagnosis What are the most effective methods of primary assessment to decide whether a person with suspected dementia should be referred to a dementia service? What
Resources: Types of dementia
 1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
Medications for Alzheimer s disease: are they right for you?
 Medications for Alzheimer s disease: are they right for you? There are no medications today that can cure Alzheimer s disease. But there are currently four medications approved by Health Canada which can
Medications for Alzheimer s disease: are they right for you? There are no medications today that can cure Alzheimer s disease. But there are currently four medications approved by Health Canada which can
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Donepezil, galantamine, rivastigmine and memantine for the treatment of Alzheimer's disease (Review of TA 111) Appraisal
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Donepezil, galantamine, rivastigmine and memantine for the treatment of Alzheimer's disease (Review of TA 111) Appraisal
Causes of Transient Incontinence. Geriatrics: Urinary Incontinence, Dementia, and Delirium. Classification of Established Incontinence
 Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
ALZHEIMER S DISEASE OVERVIEW. Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health
 ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
Evaluating an Apparent Unprovoked First Seizure in Adults
 Evaluating an Apparent Unprovoked First Seizure in Adults Case Presentation A 52 year old woman is brought to the emergency room after a witnessed seizure. She was shopping at the local mall when she was
Evaluating an Apparent Unprovoked First Seizure in Adults Case Presentation A 52 year old woman is brought to the emergency room after a witnessed seizure. She was shopping at the local mall when she was
Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital. November /20/ Safety: Falls/Cooking/Unsafe Behaviour. 2.
 How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
Memory & Aging Clinic Questionnaire
 Memory & Aging Clinic Questionnaire The answers you give to the questions below will assist us with our evaluation. Each section is equally important so please be sure to complete the entire questionnaire.
Memory & Aging Clinic Questionnaire The answers you give to the questions below will assist us with our evaluation. Each section is equally important so please be sure to complete the entire questionnaire.
These conditions can have similar and overlapping symptoms, and many of them can only be diagnosed with certainty by autopsy of the brain.
 Progression MIDDLE STAGE This document is one in a five-part series on the stages of Alzheimer s disease and is written for the person with the disease, their family 1 and caregivers. The middle stage
Progression MIDDLE STAGE This document is one in a five-part series on the stages of Alzheimer s disease and is written for the person with the disease, their family 1 and caregivers. The middle stage
Behavioral and Psychological Symptoms of dementia (BPSD)
") Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
WHAT S NEW IN THE FIGHT AGAINST DEMENTIA
 WHAT S NEW IN THE FIGHT AGAINST DEMENTIA KAREN FOREN LAKE, PHD, RNC, NP MICHIGAN NURSES ASSOCIATION REVISED 7/2017 DEMENTIA This Independent Study is presented by Michigan Nurses Association. 1.0 contact
WHAT S NEW IN THE FIGHT AGAINST DEMENTIA KAREN FOREN LAKE, PHD, RNC, NP MICHIGAN NURSES ASSOCIATION REVISED 7/2017 DEMENTIA This Independent Study is presented by Michigan Nurses Association. 1.0 contact
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction.
 Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Research & Policy Brief
 USM Muskie School of Public Service Maine DHHS Office of Elder Services Research & Policy Brief Caring for People with Alzheimer s Disease or Dementia in Maine A Matter of Public Health Alzheimer s disease
USM Muskie School of Public Service Maine DHHS Office of Elder Services Research & Policy Brief Caring for People with Alzheimer s Disease or Dementia in Maine A Matter of Public Health Alzheimer s disease
For the Lifespan: The Caregiver Guide Module 2 Dementia and Memory Loss
 For the Lifespan: The Caregiver Guide Module 2 Dementia and Memory Loss After completing this module, participants will be able to: Define dementia and memory loss. Recognize medical and social components
For the Lifespan: The Caregiver Guide Module 2 Dementia and Memory Loss After completing this module, participants will be able to: Define dementia and memory loss. Recognize medical and social components
In-Service Education. workbook 3. by Hartman Publishing, Inc. second edition
 In-Service Education workbook 3 second edition by Hartman Publishing, Inc. Alzheimer s Disease Dignity Diabetes Restraints and Restraint Alternatives Abuse and Neglect Death and Dying Managing Stress Perf
In-Service Education workbook 3 second edition by Hartman Publishing, Inc. Alzheimer s Disease Dignity Diabetes Restraints and Restraint Alternatives Abuse and Neglect Death and Dying Managing Stress Perf
Dementia and Delirium
 Dementia and Delirium LPT Gondar Mental Health Group www.le.ac.uk Dementia and Delirium WTINP Chapter 4.6 Introduction - areas to be covered Delirium Definition and causes Clinical features Management
Dementia and Delirium LPT Gondar Mental Health Group www.le.ac.uk Dementia and Delirium WTINP Chapter 4.6 Introduction - areas to be covered Delirium Definition and causes Clinical features Management
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
Raj C. Shah, MD Associate Professor in Family Medicine Rush Alzheimer s Disease Center Rush University Medical Center
 Raj C. Shah, MD Associate Professor in Family Medicine Rush Alzheimer s Disease Center Rush University Medical Center Raj_C_Shah@rush.edu From Legal Practice to What s Next: The Boomer-Lawyer s Guide to
Raj C. Shah, MD Associate Professor in Family Medicine Rush Alzheimer s Disease Center Rush University Medical Center Raj_C_Shah@rush.edu From Legal Practice to What s Next: The Boomer-Lawyer s Guide to
OUR BRAINS!!!!! Stroke Facts READY SET.
 HealthSouth Rehabilitation Hospital Huntington Dr. Timothy Saxe, Medical Director READY SET. OUR BRAINS!!!!! Stroke Facts 795,000 strokes each year- 600,000 new strokes 5.5 million stroke survivors Leading
HealthSouth Rehabilitation Hospital Huntington Dr. Timothy Saxe, Medical Director READY SET. OUR BRAINS!!!!! Stroke Facts 795,000 strokes each year- 600,000 new strokes 5.5 million stroke survivors Leading
How to Spot. How to Spot. the Early Signs of Alzheimer s
 How to Spot the Early Signs of Alzheimer s How to Spot the Early Signs of Alzheimer s The First Signs of Alzheimer s We all lose our keys and forget where we put our reading glasses as we get older. It
How to Spot the Early Signs of Alzheimer s How to Spot the Early Signs of Alzheimer s The First Signs of Alzheimer s We all lose our keys and forget where we put our reading glasses as we get older. It
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
This information explains the advice about supporting people with dementia and their carers that is set out in NICE SCIE clinical guideline 42.
 Supporting people with dementia and their carers Information for the public Published: 1 November 2006 nice.org.uk About this information NICEclinicalguidelinesadvisetheNHSoncaringforpeoplewithspe cificconditionsordiseasesandthetreatmentstheyshouldreceive.
Supporting people with dementia and their carers Information for the public Published: 1 November 2006 nice.org.uk About this information NICEclinicalguidelinesadvisetheNHSoncaringforpeoplewithspe cificconditionsordiseasesandthetreatmentstheyshouldreceive.
What is dementia? Symptoms of dementia. Memory problems
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
Alzheimer s disease and related disorders. Patient risks
 Alzheimer s disease and related disorders Patient risks ALZHEIMER BELGIQUE Alzheimer Belgique is a patient association founded in 1985 by families affected by the disease Some of our missions: Inform the
Alzheimer s disease and related disorders Patient risks ALZHEIMER BELGIQUE Alzheimer Belgique is a patient association founded in 1985 by families affected by the disease Some of our missions: Inform the
Medications and Non-Pharma Approaches to Treatment. David J. Irwin, MD Penn Frontotemporal Degeneration Center
 Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Introduction to Dementia: Complications
 Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia is not normal aging!
 The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE SCOPE. Dementia: the management of dementia, including the use of antipsychotic medication in older people
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Dementia: the management of dementia, including the use of antipsychotic medication in older people 1.1 Short title Dementia 2 Background
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Dementia: the management of dementia, including the use of antipsychotic medication in older people 1.1 Short title Dementia 2 Background
Alzheimer s Disease. Fact Sheet. Fact Sheet. Fact Sheet. What Causes AD?
 2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
Multiple Sclerosis. What is multiple sclerosis? What is the cause? What are the symptoms?
 What is multiple sclerosis? Multiple Sclerosis Multiple sclerosis (MS) is a disease of the central nervous system (the brain and spinal cord). Many people with multiple sclerosis are only mildly affected
What is multiple sclerosis? Multiple Sclerosis Multiple sclerosis (MS) is a disease of the central nervous system (the brain and spinal cord). Many people with multiple sclerosis are only mildly affected
Alzheimer s Disease Update: From Treatment to Prevention
 Alzheimer s Disease Update: From Treatment to Prevention Jeffrey M. Burns, MD Edward H. Hashinger Professor of Medicine Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science
Alzheimer s Disease Update: From Treatment to Prevention Jeffrey M. Burns, MD Edward H. Hashinger Professor of Medicine Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science
Dementia. Information for service users and carers. RDaSH leading the way with care
 Dementia Information for service users and carers RDaSH leading the way with care What is Dementia is a term that is used to describe the symptoms that occur when the brain is affected by specific diseases
Dementia Information for service users and carers RDaSH leading the way with care What is Dementia is a term that is used to describe the symptoms that occur when the brain is affected by specific diseases
10/17/2017. Causes of Dementia Alzheimer's Disease Vascular Dementia Diffuse Lewy Body Disease Alcoholic Dementia Fronto-Temporal Dementia Others
 1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
Alzheimer s Disease - Dementia
 - Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
- Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
Department of Geriatric Medicine
 Department of Geriatric Medicine Pre-Visit Questionnaire for Dementia Evaluation Name: MR#: Imprint Area This questionnaire is to be filled out by someone who knows you well. Name of Person completing
Department of Geriatric Medicine Pre-Visit Questionnaire for Dementia Evaluation Name: MR#: Imprint Area This questionnaire is to be filled out by someone who knows you well. Name of Person completing
What is Alzheimer s disease
 PBO 930022142 NPO 049-191 What is Alzheimer s disease Alzheimer s disease is the most common form of dementia. This information sheet outlines the symptoms and cause of Alzheimer s disease and describes
PBO 930022142 NPO 049-191 What is Alzheimer s disease Alzheimer s disease is the most common form of dementia. This information sheet outlines the symptoms and cause of Alzheimer s disease and describes
Alzheimer s disease. What is Alzheimer s disease?
 Alzheimer s disease What is Alzheimer s disease? What do we know about dementia and Alzheimer s disease? Alzheimer s disease is the most common form of dementia. Alzheimer s disease causes symptoms of
Alzheimer s disease What is Alzheimer s disease? What do we know about dementia and Alzheimer s disease? Alzheimer s disease is the most common form of dementia. Alzheimer s disease causes symptoms of
Alzheimer's Disease. Dementia
 Alzheimer's Disease Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s Disease
Alzheimer's Disease Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s Disease
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018
 Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Decline in Mental Capacity
 Decline in Mental Capacity Elder Law: Issues, Answers and Opportunities ALI-ABA, February 23-24, 2006 Robert B. Fleming 1 FLEMING & CURTI, P.L.C. 330 N. Granada Ave. Tucson, Arizona 85701 www.elder-law.com
Decline in Mental Capacity Elder Law: Issues, Answers and Opportunities ALI-ABA, February 23-24, 2006 Robert B. Fleming 1 FLEMING & CURTI, P.L.C. 330 N. Granada Ave. Tucson, Arizona 85701 www.elder-law.com
Management of Behavioral Symptoms in Dementia. Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal
 Management of Behavioral Symptoms in Dementia Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal Behavioral Symptoms Common & troubling At least one will occur in 61-92% of those with any dementia
Management of Behavioral Symptoms in Dementia Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal Behavioral Symptoms Common & troubling At least one will occur in 61-92% of those with any dementia
ASK IF NAMZARIC MAY BE RIGHT FOR THEM.
 IF YOUR LOVED ONE WITH MODERATE ALZHEIMER S IS TAKING DONEPEZIL 10 MG, ASK IF NAMZARIC MAY BE RIGHT FOR THEM. Once-daily NAMZARIC is a prescription medicine approved to treat moderate to severe Alzheimer
IF YOUR LOVED ONE WITH MODERATE ALZHEIMER S IS TAKING DONEPEZIL 10 MG, ASK IF NAMZARIC MAY BE RIGHT FOR THEM. Once-daily NAMZARIC is a prescription medicine approved to treat moderate to severe Alzheimer
Rational Medication Use in Dementia
 Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Geriatric Alterations Associated with Neurological Conditions
 Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Pharmacological Treatment of Dementia
 Pharmacological Treatment of Dementia Measure Description Percentage of patients with dementia or their caregivers with whom available guideline-appropriate pharmacological treatment options and nonpharmacological
Pharmacological Treatment of Dementia Measure Description Percentage of patients with dementia or their caregivers with whom available guideline-appropriate pharmacological treatment options and nonpharmacological
Across the Spectrum of Dementia. Keys to Understanding Behaviours & Anticipating Needs
 Across the Spectrum of Dementia Keys to Understanding Behaviours & Anticipating Needs Outline Review current predictions for dementia prevalence, & the implications for future needs Discuss retrogenesis
Across the Spectrum of Dementia Keys to Understanding Behaviours & Anticipating Needs Outline Review current predictions for dementia prevalence, & the implications for future needs Discuss retrogenesis
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
PROJECTION: Worlds dementia population is expected to triple by 2050
 DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
Dementia is an overall term for a set of symptoms that is caused by disorders affecting the brain.
 Vascular Dementia Vascular Dementia Other Dementias This information sheet provides an overview of a type of dementia known as vascular dementia. In this information sheet you will find: An overview of
Vascular Dementia Vascular Dementia Other Dementias This information sheet provides an overview of a type of dementia known as vascular dementia. In this information sheet you will find: An overview of
What is Alzheimer s disease?
 What is Alzheimer s disease? Factsheet 401LP July 2014 Alzheimer s disease is the most common cause of dementia. The word dementia describes a set of symptoms that can include memory loss and difficulties
What is Alzheimer s disease? Factsheet 401LP July 2014 Alzheimer s disease is the most common cause of dementia. The word dementia describes a set of symptoms that can include memory loss and difficulties
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Appendix 2 (continued): Recommendations for the management of mild to moderate dementia, dementia with a cerebrovascular component, and for addressing
: Recommendations for the management of mild to moderate dementia, dementia with a cerebrovascular component, and for addressing") a cerebrovascular component, and for addressing ethical issues in dementia (page 1 of 7) Mild to moderate dementia 1. Most patients with dementia can be assessed and managed adequately by their primary
a cerebrovascular component, and for addressing ethical issues in dementia (page 1 of 7) Mild to moderate dementia 1. Most patients with dementia can be assessed and managed adequately by their primary
Psychotropic Strategies Handout Package
 Psychotropic Strategies Handout Package Psychotropic Strategies Learning Objectives Utilize all clinical information available Assess the patient s overall condition this is essential Basic Principles
Psychotropic Strategies Handout Package Psychotropic Strategies Learning Objectives Utilize all clinical information available Assess the patient s overall condition this is essential Basic Principles
Dementia Chronic Brain Failure The forgotten cardiovascular disease Clare Hawley 2015
 Dementia Chronic Brain Failure The forgotten cardiovascular disease Clare Hawley 2015 MB ChB, MRCGP, PG Dip Cardiol, PG Cert Med Ed Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI Refractory
Dementia Chronic Brain Failure The forgotten cardiovascular disease Clare Hawley 2015 MB ChB, MRCGP, PG Dip Cardiol, PG Cert Med Ed Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI Refractory
ALZHEIMER S DISEASE, DEMENTIA & DEPRESSION
 ALZHEIMER S DISEASE, DEMENTIA & DEPRESSION Daily Activities/Tasks As Alzheimer's disease and dementia progresses, activities like dressing, bathing, eating, and toileting may become harder to manage. Each
ALZHEIMER S DISEASE, DEMENTIA & DEPRESSION Daily Activities/Tasks As Alzheimer's disease and dementia progresses, activities like dressing, bathing, eating, and toileting may become harder to manage. Each
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Mental Health Rotation Educational Goals & Objectives
 Mental Health Rotation Educational Goals & Objectives Mental illness is prevalent in the general population and is commonly seen and treated in the office of the primary care provider. Educational experiences
Mental Health Rotation Educational Goals & Objectives Mental illness is prevalent in the general population and is commonly seen and treated in the office of the primary care provider. Educational experiences
Functional Assessment Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico
 Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Retired - Geriatrics/Extended Care New Mexico Veterans Affairs Healthcare System Albuquerque, NM Disclosure Statement:
Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Retired - Geriatrics/Extended Care New Mexico Veterans Affairs Healthcare System Albuquerque, NM Disclosure Statement:
Significance A Busy Clinician's Guide to Seniors with Memory Loss
 Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
Dementia Diagnosis Guidelines Primary Care
 Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)