The IMPACT Model. Delivering Effective Depression Treatment in the Primary Care Setting
|
|
|
- Anthony Pierce
- 6 years ago
- Views:
Transcription





1 The IMPACT Model Delivering Effective Depression Treatment in the Primary Care Setting
2 Presenters Jürgen Unützer, MD, MPH, MA Professor & Vice-Chair Psychiatry and Behavioral Sciences, UW Rita Haverkamp, MSN, PMHCNS-BC, CNS Clinical Nurse Specialist Kaiser Permanente Southern California Marty Adelman, MA, CPRP Mental Health Program Coordinator San Diego Council of Community Clinics

3 University of Washington Building on 25 years of Research and Practice in Integrated Mental Health Care
4 Overview Integrated Mental Health Care The IMPACT Model Existing programs with lessons for implementation

5 66% of PCPs Report Poor Access to Mental Health Care for Their Patients Cunningham PJ, Health Affairs 2009;28(3)


6 Mental Disorders are Rarely the Only Health Problem Chronic Physical Pain Cancer 10-20% 25-50% Smoking, Obesity, Physical Inactivity Mental Health / Substance Abuse Neurologic Disorders 10-20% 40-70% Heart Disease 10-30% Diabetes 10-30%
 Expensive 50-100% higher health care costs (ED, inpatient, outpatient, pharmacy) Deadly Over 30,000 suicides /")
7 Improving Care for Depression Common 10% in primary care, more common in patients with chronic medical illnesses Disabling #2 cause of disability (WHO) Expensive % higher health care costs (ED, inpatient, outpatient, pharmacy) Deadly Over 30,000 suicides / year
8 Evidence for Collaborative Care for Depression Metaanalysis by Gilbody S. et al, Archives of Internal Medicine; Dec trials of collaborative care for depression in primary care (US and Europe) CC consistently more effective than usual care



9 IMPACT Study Effective Collaboration PCP supported by Behavioral Health Care Manager Practice Support Informed, Active Patient Measurement Caseload-focused psychiatric consultation Training
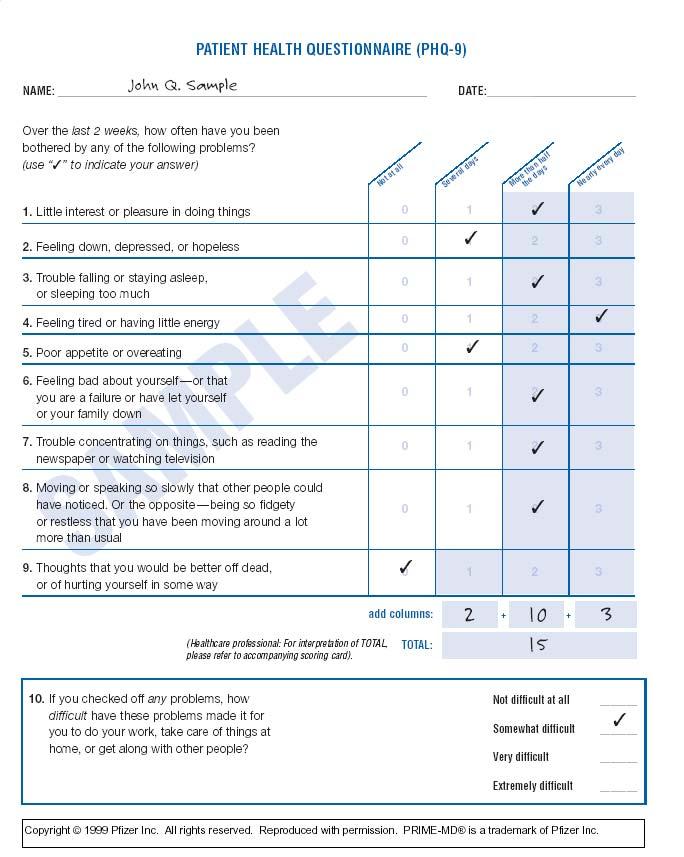
10 IMPACT Team Care Model TWO PROCESSES 1. Systematic diagnosis and outcomes tracking PHQ-9 to facilitate diagnosis and track depression outcomes 2. Stepped Care a) Change treatment according to evidence-based algorithm if patient is not improving b) Relapse prevention once patient is improved TWO NEW TEAM MEMBERS Care Manager - Patient education / self management support - Close follow-up to make sure pts don t fall through the cracks - Support anti-depressant Rx by PCP - Brief counseling (behavioral activation, PST-PC, CBT, IPT) - Facilitate treatment change / referral to mental health - Relapse prevention Consulting Psychiatrist - Caseload consultation for care manager and PCP (population-based) - Diagnostic consultation on difficult cases - Consultation focused on patients not improving as expected - Recommendations for additional treatment / referral according to evidence-based guidelines
11
12 Improved Satisfaction with Depression Care (% Excellent, Very Good) percent Usual Care IMPACT month Unützer et al, JAMA 2002; 288:
13 IMPACT Doubles Effectiveness of Care for Depression 50 % or greater improvement in depression at 12 months % Usual Care IMPACT Unutzer et al, Psych Clin NA 2004 Participating Organizations

14 Better Physical Function SF-12 Physical Function Component Summary Score (PCS-12) P<0.01 P<0.01 P<0.01 P= Usual Care IMPACT Baseline 3 mos 6 mos 12 mos Callahan et al, JAGS 2005; 53:
15 Long-Term Cost Savings Cost Category 4-year costs in $ Intervention group cost in $ Usual care group cost in $ Difference in $ IMPACT program cost Outpatient mental health costs Savings Pharmacy costs 7,284 6,942 7, Other outpatient costs 14,306 14,160 14, Inpatient medical costs 8,452 7,179 9, Inpatient mental health / substance abuse costs Total health care cost 31,082 29,422 32,785 -$3363 Unützer et al. Am J Managed Care 2008.

16 Endorsements IOM Report Presidents New Freedom Commission on Mental Health National Business Group on Health AHRQ CDC Consensus Panel SAMHSA National Registry of Evidence-Based Programs & Practices (NREPP)
17 IMPACT Replication Studies Patient Population (Study Name) Target Clinical Conditions Reference Adult primary care patients (Pathways) Diabetes and depression Katon et al., 2004 Adult patients in safety net clinics (Project Dulce; Latinos) Adult patients in safety net clinics (Latino patients) Diabetes and depression Gilmer et al., 2008 Diabetes and depression Ell et al., 2010 Public sector oncology clinic (Latino patients) Cancer and depression Dwight-Johnson et al., 2005 Ell et al., 2008 HMO patients Depression in primary care Grypma et al., 2006 Adolescents in primary care Adolescent depression Richardson et al., 2009 Older adults Arthritis and depression Unützer et al., 2008 Acute coronary syndrome patients (COPES) Coronary events and depression Davidson et al., 2010


18 Over 4,000 providers trained in IMPACT Care Clinicians Trained Over 500 clinics 500 0
19 Washington State Mental Health Integration Program (MHIP)

20

21 MHIP across Washington State
22 MHIP Best Practice Clinic Example Population Mean baseline PHQ-9 depressi on score (0-27) Followup (%) Mean number of contacts %with psych consultat ion % with significant clinical improveme nt Disabled % % 50 % Uninsured % % 53 % Older Adults % % 54 %

23 Integrated Care Team Building Process
24 Program Staffing in Diverse Clinic Settings Clinic Population (mental health needs) % of clinic population with need for care management Typical caseload size for 1 FTE Care Manager # of unique primary care clinic patients to justify 1 FTE CM FTE Care Manager Low need (e.g., insured, employed) 2% Typical personnel requirement for 1,000 unique primary care patients FTE Psychiatrist** 0.05 (2 hrs / week) Medium need (e.g., comorbid medical needs / chronic pain / substance abuse) 5% High need (e.g, safety-net population)* 15% (3 hrs / week) 0.3 (12 hrs / week)
25 Summary: Effective Integrated Care Programs Effective multidisciplinary practice Efficient use of limited specialty mental health resources Population focus Proactive care for a defined population of patients instead of behavioral health urgent care Registry to prevent people from falling through the cracks Measurement-based stepped care Outcome measurement guides systematic application of evidence-based treatments Treatment to target
26 Rita Haverkamp, MSN, PMHCNS-BC, CNS Clinical Nurse Specialist Kaiser Permanente Southern California
27 IMPACT Dissemination at KPSC in IMPACT Study Kaiser Permanente (~ 280 participants in 1 clinic) KPSC in San Diego after IMPACT (2 clinics; Grypma et al, 2006) KPSC Depression Initiative (Dreskin) 13 regional medical centers serving 3 million members
28 Kaiser Permanente of Southern California Pilot Study Compare 284 clients in adapted program with 140 usual care patients and 140 intervention patients in the IMPACT study (Grypma L, Haverkamp R, Little S, Unützer J, General Hospital Psychiatry, 2006) Dissemination Implemented core components of program in 13 regional medical centers
29 Program Adaptations Adults of all ages Expanded team (medical assistant) Added steps ( depression class ) Psychiatric supervision by telephone
30 KPSC San Diego After IMPACT Fewer care manager contacts 18.9 IMPACT Study Post-Study Total contacts Clinic visits Phone calls Grypma L, Haverkamp R, Little S, Unützer J, General Hospital Psychiatry, 2006.
31 IMPACT Remains Effective >= 50 % drop in PHQ-9 depression scores 66% 68% 64% 68% At 3 months IMPACT Post-Study At 6 months Grypma L, Haverkamp R, Little S, Unützer J, General Hospital Psychiatry, 2006.
32 Lower Total Health Care Costs $8,800 $ / year $8,400 $8,000 $7,600 $7,200 $8,588 $7,949 $7,471 Study Usual Care Study IMPACT Post Study IMPACT $6,800 Grypma L, Haverkamp R, Little S, Unützer J, General Hospital Psychiatry, 2006.
33 Kaiser Southern California Depression Program Dissemination Implementing program at 13 regional medical centers in KPSC (over 3 million members) Screening of all CVD, diabetic, COPD and patients Adding other patients with chronic conditions to this process over time

34 Complete Care Depression Program YTD Screening Results Categorized by Score January 1, 2009 December 31, 2009

35 PHQ-9 Initial Screening Results for Patients Scoring 10 or More

36 Complete Care Depression Program Treatment Outcomes January 1, 2009 December 31, 2009 * 36.3% 29.3% 31.6% 2.8% * Patients started the program any time in 2009, so some patients still receiving treatment after these results.
37 Marty Adelman, MA, CPRP Mental Health Program Coordinator San Diego Council of Community Clinics
38 Mental Health and Primary Care Integration Project CCC represents and supports 16 community clinic organizations operating over 100 sites in San Diego, Imperial and Riverside Counties. Funding originates from Mental Health Services Act (prop 63) thru County of San Diego to Council of Community Clinics (CCC). CCC subcontracts with 9 clinic organizations to provide mental health services at 16 sites. Services first provided in February of 2007, with the majority of clinics initiating services in May of 2007.
39 Project Services Target population: Individuals with SMI/SED who are unfunded for mental health services: Three Age Groups Children and Youth (ages 0-17) Adults (ages 18-59) Older Adults (ages 60 and over) Two Treatment Models Specialty Pool Services (SPS) IMPACT Challenges serving kids and older adults Outreach Component Senior Peer Promotora Program
40 Specialty Pool Services Traditional model - therapy provided by mental health professional. Medication management provided by psychiatrist Maximum 13 visits for children and youth Maximum 12 visits for adults/older adults Medications for up to 90 days, then pharmacy assistance programs (PAPs) Short Term Treatment Model one year, those needing additional treatment are transitioned to County Mental Health providers Achieves Colocation but not necessarily integration
41 IMPACT services Up to 16 visits with a Depression Care Manager Up to 4 visits with the PCP to prescribe and monitor medication Treatment period of one year Medication for a period of one year Consulting psychiatry services provided by dually board certified psychiatrist/fp physician Inherently integrated Model Consulting Psychiatrist is built-in Safety Net
42 Essential Elements of IMPACT 1. Collaborative Care; DCM-PCP, DCM-psychiatrist 2. Depression Care Manager; treats, educates, monitors 3. Consulting Psychiatrist; consults primarily on those not who are not improving 4. Outcome Measurement; PHQ-9 administered at every visit 5. Stepped Care; treatment adjusted based on clinical outcomes
43 PHQ-9 scores IMPACT Client's PHQ-9 Scores PHQ-9 Score Session Number N= IMPACT clients complete PHQ-9 at each visit. Graph represents PHQ-9 scores for 947 A & OA s. The average score at enrollment was By session six, the average score was below 10. N indicates the number of clients in treatment at each session.
44 Cross Training DCM s Cross-training DCM s to support PCPs in encouraging clients to make the necessary behavioral changes. Psychotropic Medications Diabetes Chronic pain Maternal Depression CVD/Heart Disease Link between Physical and Mental Health
45 Clients Served February 1, 2007 December 31,2010 Clients Served by Age Range Clients Served by Treatment Model 1191 Youth Adult Older Adult SPS IMPACT ,135 3,587 unduplicated clients served to date
46 Senior Peer Promotora Program Specifically designed for Older Adults who are: Less likely to seek services on their own Less likely to identify their symptoms as depression More likely to isolate More likely to commit suicide Promotoras Coordinators and Promotoras provide outreach, education and engagement activities to assist older adults and their families to access mental health and primary care services and stay in treatment
47 Meeting the DMH mandate 58.9% of clients who were approved for services by CCC (January 1, 2007 to June 30, 2010) had not been seen previously in the County Mental Health System. 30.4% of clients report that Spanish is their language preference compared to 16% of County clients. 43.7% of clients identify as Hispanic/Latino compared to 21% of County clients. Meeting the expectation that Counties identify unserved and underserved populations
48 What it does Limitations The project has successfully provided services to a population which is typically underserved due to the stigma associated with seeking and accepting MH services The project has likely made less impact on the morbidity disparity for those with SMI as only a small portion of those with SMI are seen in PC thru this project
49 The Projects Two projects achieving integration using differing approaches MH clinician Primary Care NCM Mental Health Program MHSA SAMHSA
50 Primary and Behavioral Healthcare Integration Project (PBHI) Four year project funded by SAMHSA One of initial 13 demonstration projects funded across the US Nurse Care Managers (NCMs) embedded in MH programs, screening for; Diabetes Hypertension Hyperlipidemia (high cholesterol) Obesity Smoking
51 PBHCI outcomes Between February 1 and September 29, 2010 NCM s have screened 444 individuals Gender: male (176); female (268) Age:18-24 years (18); years (163); years (243); 65+ (20) Income: <100% of FPL (378); % FPL (49); >200% FPL (11) Insurance Status: Medicaid/Medicare (177); Uninsured (263)
52 PBHCIS Screening Results positive screens Diabetes 357/ % Hypertension 436/ % Hyperlipidemia 353/ % Obesity 436/ % Smoking 433/ % Reaching those most at risk for premature illness and death


53 Thank You James D. Ralston
54 Q: How are the providers incentivized to adopt this model of integrated care? do they bill differently for this care? If so, how? Please advise. Thank you! This varies. In some cases, health plan or county / state contracts pay for the care manager / consulting psychiatrist s services in primary care. In some cases, licensed care managers bill for the patient contacts. In some cases, the care management activities are incorporated in care management fees in the context of a Patient Centered Medical Home. Q: How often do primary care physician and psychiatrist communicate about the patients' care? Is there an ideal ratio of psychiatrist to primary care physician? What is the good patient panel size? Most of the communication between PCP and Psychiatrist is conducted through the care manager who is based in primary care (a weekly scheduled review of all active cases and recommendations from the psychiatrist to the PCP), but PCPs and Psychiatrists do talk directly on occasion. Q: Any advice on how to implement the IMPACT model to a large population? Kaiser Permanente s approach (outlined by Rita) is a fine example or the MHIP program ( or the DIAMOND program in Minnesota (see Q: What would be the key components of your program that has engaged the PCP's in the program? Care management and psychiatry support makes their jobs easier. PCP visits become more productive / shorter. See Levine et al for a paper on PCP satisfaction with the program: Levine S, Unützer J, Yip JY, Hoffing M, Leung M, Fan MY, Lin EHB, Grypma L, Katon W, Harpole LH, Langston CA. Physician satisfaction with a collaborative disease management program for late-life depression in primary care. General Hospital Psychiatry. 2005; 27: Q: Wondering if any type of CEUs credits are given. Yes. We have given CEUs in various on-line or in person training activities. See training sections of AIMS ( or IMPACT websites ( Q: is there any data using this model within dialysis facilities? Not that I am aware of.
55 Q: 1) Has there been any studies to see if the results at 12 months is maintained at 24 months? YES. The results were largely maintained. See Hunkeler et al, BMJ: Hunkeler EM, Katon W, Tang L, Williams JW, Kroenke K, Lin EHB, Harpole LH, Areán PA, Levine S, Grypma LM, Hargreaves WA, Unützer J. Long term outcomes from the IMPACT randomised trial for depressed elderly patients in primary care. British Medical Journal. 2006; 332(7536): ) What is the SF-12? Is this the same as VR-12? SF-12 is a population health measure used in health services research ( 3) Please define "older adults". In the original IMPACT trial, we included patients age 60 and older. Q: What specific backgrounds do the case managers have? as far as mental health, etc. We do not use the term case manager but rather care manager because the individual is involved in providing care. The background varies. Mental health background is helpful but not absolutely required if adequate training and psychiatry support is available to support the care managers. We have trained nurses, social workers, licensed counselors and psychologists in the role of care manager. Some organizations have used Medical Assistants partnered with licensed professionals in this role.
University of Washington
 Integrated Mental Health Care: closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Professor & Vice-Chair Psychiatry and Behavioral Sciences University of Washington unutzer@uw.edu
Integrated Mental Health Care: closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Professor & Vice-Chair Psychiatry and Behavioral Sciences University of Washington unutzer@uw.edu
Integrating Behavioral Health into Primary Care: Collaborative-Care Models
 Integrating Behavioral Health into Primary Care: Collaborative-Care Models Presented at the National Health Policy Forum September 17 th, 2013 Marc Avery, MD Clinical Associate Professor Associate Director
Integrating Behavioral Health into Primary Care: Collaborative-Care Models Presented at the National Health Policy Forum September 17 th, 2013 Marc Avery, MD Clinical Associate Professor Associate Director
Integrating Behavioral Health and Primary Care. Jürgen Unützer, MD, MPH, MA University of Washington November 13, 2013
 Integrating Behavioral Health and Primary Care Jürgen Unützer, MD, MPH, MA University of Washington November 13, 2013 Jürgen Unützer, MD, MPH, MA Disclosures Employment: University of Washington Professor
Integrating Behavioral Health and Primary Care Jürgen Unützer, MD, MPH, MA University of Washington November 13, 2013 Jürgen Unützer, MD, MPH, MA Disclosures Employment: University of Washington Professor
New York State Collaborative Care Initiative Thursday, January 24, 2013
 New York State Collaborative Care Initiative Thursday, January 24, 2013 Lloyd Sederer, MD Medical Director New York State Office of Mental Health Key Components of Collaborative Care Jürgen Unützer, MD,
New York State Collaborative Care Initiative Thursday, January 24, 2013 Lloyd Sederer, MD Medical Director New York State Office of Mental Health Key Components of Collaborative Care Jürgen Unützer, MD,
IMPACT Improving Mood Promoting Access to Collaborative Treatment
 IMPACT Improving Mood Promoting Access to Collaborative Treatment for Late-Life Depression Funded by John A. Hartford Foundation, California HealthCare Foundation, Robert Wood Johnson Foundation, Hogg
IMPACT Improving Mood Promoting Access to Collaborative Treatment for Late-Life Depression Funded by John A. Hartford Foundation, California HealthCare Foundation, Robert Wood Johnson Foundation, Hogg
Making an IMPACT on late-life depression. Partnering with primary care providers can double the effect of treatment
 University of Massachusetts Boston From the SelectedWorks of Steven D Vannoy Fall September, 2006 Making an IMPACT on late-life depression. Partnering with primary care providers can double the effect
University of Massachusetts Boston From the SelectedWorks of Steven D Vannoy Fall September, 2006 Making an IMPACT on late-life depression. Partnering with primary care providers can double the effect
Time Topic / Activity Presenter(s)
") Social Innovation Fund Pre-Launch Training Agenda September 14, 2013 Time Topic / Activity Presenter(s) 8:00 REGISTRATION 8:30 Welcome - JAHF and AIMS Center Introductions 8:50 Agenda & Materials Review
Social Innovation Fund Pre-Launch Training Agenda September 14, 2013 Time Topic / Activity Presenter(s) 8:00 REGISTRATION 8:30 Welcome - JAHF and AIMS Center Introductions 8:50 Agenda & Materials Review
Treating Depression in Disadvantaged Women: What is the evidence?
 Treating Depression in Disadvantaged Women: What is the evidence? Megan Dwight Johnson, MD MPH Associate Professor Medical Director, UWMC Inpatient Psychiatry Department of Psychiatry and Behavioral Sciences
Treating Depression in Disadvantaged Women: What is the evidence? Megan Dwight Johnson, MD MPH Associate Professor Medical Director, UWMC Inpatient Psychiatry Department of Psychiatry and Behavioral Sciences
IMPACT: Evidence-based depression treatment in primary care. Rita Haverkamp, MSN, CNS-BC Virna Little, PsyD, LCSW-R, SAP
 IMPACT: Evidence-based depression treatment in primary care Rita Haverkamp, MSN, CNS-BC Virna Little, PsyD, LCSW-R, SAP IMPACT: A Practical Approach to Team Based Depression Care What is Depression? Common:
IMPACT: Evidence-based depression treatment in primary care Rita Haverkamp, MSN, CNS-BC Virna Little, PsyD, LCSW-R, SAP IMPACT: A Practical Approach to Team Based Depression Care What is Depression? Common:
Integrated Mental Health Care
 Integrated Mental Health Care Jürgen Unützer, MD, M.P.H., M.A. This brief overview will summarize the case for providing behavioral health services in primary care, review core components of evidence-based
Integrated Mental Health Care Jürgen Unützer, MD, M.P.H., M.A. This brief overview will summarize the case for providing behavioral health services in primary care, review core components of evidence-based
Featured Industry Partner
 Featured Industry Partner Concurrent Strategy Session October 7, 2015: 3:15-4:30 Making it Work: Integrating Mental Health Panel: Jürgen Unützer, MD, MPH, MA, Professor and Chair, Department of Psychiatry
Featured Industry Partner Concurrent Strategy Session October 7, 2015: 3:15-4:30 Making it Work: Integrating Mental Health Panel: Jürgen Unützer, MD, MPH, MA, Professor and Chair, Department of Psychiatry
Closing the Gap: Implementing Evidence-based Behavioral Health Practices for Older Americans
 Closing the Gap: Implementing Evidence-based Behavioral Health Practices for Older Americans Steve Bartels MD, MS Professor of Psychiatry, Community and Family Medicine, and The Dartmouth Institute Geisel
Closing the Gap: Implementing Evidence-based Behavioral Health Practices for Older Americans Steve Bartels MD, MS Professor of Psychiatry, Community and Family Medicine, and The Dartmouth Institute Geisel
Behavioral Health Treatment in a Primary Care Setting
 Behavioral Health Treatment in a Primary Care Setting Andrew J. McLean, MD, MPH Medical Director, ND DHS Chair, Psychiatry and Behavioral Science, UNDSMHS ajmclean@nd.gov Objectives Understand the importance
Behavioral Health Treatment in a Primary Care Setting Andrew J. McLean, MD, MPH Medical Director, ND DHS Chair, Psychiatry and Behavioral Science, UNDSMHS ajmclean@nd.gov Objectives Understand the importance
Depression in Late Life Initiative
 Depression in Late Life Initiative made possible by the Archstone Foundation Depression in Late Life Request for Proposals (RFP) Care Partners: Bridging Families, Clinics, and Communities to Advance Late
Depression in Late Life Initiative made possible by the Archstone Foundation Depression in Late Life Request for Proposals (RFP) Care Partners: Bridging Families, Clinics, and Communities to Advance Late
Care Team Training. Key Components of Collaborative Care. Collaborative Team Approach 4/21/2014 PCP. Core Program. New Roles. Psychiatric Consultant
 Team Training Key Components of Collaborative Collaborative Team Approach Patient PCP Manager New Roles Core Program Psychiatric Consultant Behavioral Health Clinicians Additional Clinic Resources Substance,
Team Training Key Components of Collaborative Collaborative Team Approach Patient PCP Manager New Roles Core Program Psychiatric Consultant Behavioral Health Clinicians Additional Clinic Resources Substance,
Include Substance Use Disorder Services in New Hampshire Medicaid Managed Care
 Include Substance Use Disorder Services in New Hampshire Medicaid Managed Care New Futures mission is to advocate, educate, and collaborate to reduce alcohol and other drug problems in New Hampshire. Expanding
Include Substance Use Disorder Services in New Hampshire Medicaid Managed Care New Futures mission is to advocate, educate, and collaborate to reduce alcohol and other drug problems in New Hampshire. Expanding
The Value of Providing Collaborative Care Models For Treating Employees with Depression
 The Value of Providing Collaborative Care Models For Treating Employees with Depression Summary Depression is one of the costliest health issues for employers because of its high prevalence and co-morbidity
The Value of Providing Collaborative Care Models For Treating Employees with Depression Summary Depression is one of the costliest health issues for employers because of its high prevalence and co-morbidity
Integrating Care for the Whole Person: Collaborative Teams for Behavioral Health and Medical Conditions
 Integrating Care for the Whole Person: Collaborative Teams for Behavioral Health and Medical Conditions February 16, 2016 Presented by Dr. Paul Ciechanowski 2/25/2017 1 Opening Remarks Purpose Welcoming
Integrating Care for the Whole Person: Collaborative Teams for Behavioral Health and Medical Conditions February 16, 2016 Presented by Dr. Paul Ciechanowski 2/25/2017 1 Opening Remarks Purpose Welcoming
Quality Improvement With Pay-for-Performance Incentives in Integrated Behavioral Health Care
 Quality Improvement With Pay-for-Performance Incentives in Integrated Behavioral Health Care Jürgen Unützer, MD, MPH, MA, Ya-Fen Chan, PhD, Erin Hafer, MPH, Jessica Knaster, MPH, Anne Shields, RN, MPH,
Quality Improvement With Pay-for-Performance Incentives in Integrated Behavioral Health Care Jürgen Unützer, MD, MPH, MA, Ya-Fen Chan, PhD, Erin Hafer, MPH, Jessica Knaster, MPH, Anne Shields, RN, MPH,
2/28/2012. Roles for State Title V Programs in Building Systems of Care for CYSHCN- ASD & Other DD: Lessons Learned in NJ
 Roles for State Title V Programs in Building Systems of Care for CYSHCN- ASD & Other DD: Lessons Learned in NJ Presented by Diana MTK Autin, Executive Co-Director, Statewide Parent Advocacy Network 35
Roles for State Title V Programs in Building Systems of Care for CYSHCN- ASD & Other DD: Lessons Learned in NJ Presented by Diana MTK Autin, Executive Co-Director, Statewide Parent Advocacy Network 35
Disorder. Objectives. Under Recognition/ Undertreatment. Making a Diagnosis
 Care Partners Primary Care Provider Lunch & Learn: Why PCPs Love Collaborative Care Presenter: Wayne Bentham, MD The advantage of the collaborative care model of depression management in primary care is
Care Partners Primary Care Provider Lunch & Learn: Why PCPs Love Collaborative Care Presenter: Wayne Bentham, MD The advantage of the collaborative care model of depression management in primary care is
CENTER OF EXCELLENCE MATERNAL AND CHILD MENTAL HEALTH (MCMH)
") CENTER OF EXCELLENCE MATERNAL AND CHILD MENTAL HEALTH (MCMH) The infant and young child should experience a warm, intimate, and continuous relationship with his mother in which both find satisfaction and
CENTER OF EXCELLENCE MATERNAL AND CHILD MENTAL HEALTH (MCMH) The infant and young child should experience a warm, intimate, and continuous relationship with his mother in which both find satisfaction and
Psychiatry in a Collaborative System-Level and Practice-Level
 Psychiatry in a Collaborative System-Level and Practice-Level Robin M. Reed, MD, MPH Presentation for the North Carolina Psychiatric Association October 2 nd 2015 Disclosures I have no relevant financial
Psychiatry in a Collaborative System-Level and Practice-Level Robin M. Reed, MD, MPH Presentation for the North Carolina Psychiatric Association October 2 nd 2015 Disclosures I have no relevant financial
Peer Support Services Improve Clinical Outcomes by Fostering Recovery and Promoting Empowerment
 Peer Support Services Improve Clinical Outcomes by Fostering Recovery and Promoting Empowerment Optum has recognized the role of peer support services as an integral part of state Medicaid plans and has
Peer Support Services Improve Clinical Outcomes by Fostering Recovery and Promoting Empowerment Optum has recognized the role of peer support services as an integral part of state Medicaid plans and has
2) Percentage of adult patients (aged 18 years or older) with a diagnosis of major depression or dysthymia and an
 Percentage of adult patients (aged 18 years or older) with a diagnosis of major depression or dysthymia and an") Quality ID #370 (NQF 0710): Depression Remission at Twelve Months National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Prevention, Treatment, and Management of Mental Health
Quality ID #370 (NQF 0710): Depression Remission at Twelve Months National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Prevention, Treatment, and Management of Mental Health
City of Berkeley CSS Plan Revised Budget Narratives. Full Service Partnership Integrated Services Expansion for TAY, Adults and Older Adults
 City of Berkeley CSS Plan Revised Budget Narratives The additional funds provided by the CSS expansion have been added into the previously approved 07/08 budgets. What follows are the revised budget narratives
City of Berkeley CSS Plan Revised Budget Narratives The additional funds provided by the CSS expansion have been added into the previously approved 07/08 budgets. What follows are the revised budget narratives
Integrating MH/SA Treatment in Primary Care Firm Clinics: The Behavioral Health Clinic
 Integrating MH/SA Treatment in Primary Care Firm Clinics: The Behavioral Health Clinic John D. Dingell VA Medical Center VISN 11 - Detroit, MI Objectives Upon completion of this session, participants will
Integrating MH/SA Treatment in Primary Care Firm Clinics: The Behavioral Health Clinic John D. Dingell VA Medical Center VISN 11 - Detroit, MI Objectives Upon completion of this session, participants will
Reverse Integration Project at Lehigh Valley Health Network
 Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Reverse Integration Project at Lehigh Valley Health Network Barbara Gouzouasis MBA Lehigh Valley Health Network, Barbara.Gouzouasis@lvhn.org
Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Reverse Integration Project at Lehigh Valley Health Network Barbara Gouzouasis MBA Lehigh Valley Health Network, Barbara.Gouzouasis@lvhn.org
Relapse Prevention Webinar Agenda Relapse Prevention Planning
 Relapse Prevention Webinar Agenda Relapse Prevention Planning Rita Haverkamp, MSN, PMHCNS BC, CNS Expert Care Manager and AIMS Trainer By the end of the webinar you will be able to Describe what a RPP
Relapse Prevention Webinar Agenda Relapse Prevention Planning Rita Haverkamp, MSN, PMHCNS BC, CNS Expert Care Manager and AIMS Trainer By the end of the webinar you will be able to Describe what a RPP
Preparing for New Hampshire Behavioral Health Summit December 3, 2015
 Preparing for 2016 New Hampshire Behavioral Health Summit December 3, 2015 9.3 million more Americans have insurance Uninsured rate down to 11.9% Health spending historically low growth rate 3.7% 27
Preparing for 2016 New Hampshire Behavioral Health Summit December 3, 2015 9.3 million more Americans have insurance Uninsured rate down to 11.9% Health spending historically low growth rate 3.7% 27
Integrating Behavioral Health. Deborah J. Cohen, PhD Oregon Health & Science University
 Integrating Behavioral Health and Primary Care Deborah J. Cohen, PhD Oregon Health & Science University Presentation Goals Provide evidence based rationale for behavior health primary care integration
Integrating Behavioral Health and Primary Care Deborah J. Cohen, PhD Oregon Health & Science University Presentation Goals Provide evidence based rationale for behavior health primary care integration
How to Integrate Peer Support & Navigation into Care Delivery
 How to Integrate Peer Support & Navigation into Care Delivery Andrew Bertagnolli, PhD Care Management Institute Why Integrate Peer Support into the Care Delivery Pathway? Improved health Increased feelings
How to Integrate Peer Support & Navigation into Care Delivery Andrew Bertagnolli, PhD Care Management Institute Why Integrate Peer Support into the Care Delivery Pathway? Improved health Increased feelings
7/20/2010. Cherokee Health Systems Cherokee Health Systems
 The Implementation of SBIRT: Screening and Treatment of Substance Use Disorders in an Integrated dpi Primary Care Setting Suzanne Bailey, Psy.D. Behavioral Health Consultant Intensive Outpatient alcohol
The Implementation of SBIRT: Screening and Treatment of Substance Use Disorders in an Integrated dpi Primary Care Setting Suzanne Bailey, Psy.D. Behavioral Health Consultant Intensive Outpatient alcohol
Quality ID #411 (NQF 0711): Depression Remission at Six Months National Quality Strategy Domain: Effective Clinical Care
: Depression Remission at Six Months National Quality Strategy Domain: Effective Clinical Care") Quality ID #411 (NQF 0711): Depression Remission at Six Months National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #411 (NQF 0711): Depression Remission at Six Months National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Implementing a Community- Based Initiative for Early Treatment of Psychosis: From RAISE Connection to OnTrackNY
 Implementing a Community- Based Initiative for Early Treatment of Psychosis: From RAISE Connection to OnTrackNY Lisa Dixon, M.D., M.P.H. Director, Center for Practice Innovations, NYSPI Columbia University
Implementing a Community- Based Initiative for Early Treatment of Psychosis: From RAISE Connection to OnTrackNY Lisa Dixon, M.D., M.P.H. Director, Center for Practice Innovations, NYSPI Columbia University
Unmanaged Behavioral Health Puts Your Company At Risk. Presented by: Dr. Sam Mayhugh Integrated Behavioral Health
 Unmanaged Behavioral Health Puts Your Company At Risk Presented by: Dr. Sam Mayhugh Integrated Behavioral Health Behavioral Health Management Webinar Overview History of BH management Prevalence of behavioral
Unmanaged Behavioral Health Puts Your Company At Risk Presented by: Dr. Sam Mayhugh Integrated Behavioral Health Behavioral Health Management Webinar Overview History of BH management Prevalence of behavioral
Wednesday, June 22, 2016
 Wednesday, June 22, 2016 8:00 a.m. 4:00 p.m. Toftrees 1 Country Club Lane State College, PA 16803 Sponsored by the Center for Excellence in Rural Public Psychiatry, part of Western Psychiatric Institute
Wednesday, June 22, 2016 8:00 a.m. 4:00 p.m. Toftrees 1 Country Club Lane State College, PA 16803 Sponsored by the Center for Excellence in Rural Public Psychiatry, part of Western Psychiatric Institute
Patient and Family Engagement and Retention. Care Manager Role. Who is on the recruitment/engagement team? General Recruitment Challenges
 Patient and Family Engagement and Retention Announcement from Archstone Foundation Rita Haverkamp, MSN, PMHCNS BC, CNS Expert Care Manager and AIMS Center Trainer Collaborative Care Team Approach Care
Patient and Family Engagement and Retention Announcement from Archstone Foundation Rita Haverkamp, MSN, PMHCNS BC, CNS Expert Care Manager and AIMS Center Trainer Collaborative Care Team Approach Care
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Depression & Diabetes: Pathways and TeamCare Studies
 Depression & Diabetes: Pathways and TeamCare Studies Wayne Katon, MD 1 Mike VonKorff, ScD 2 Elizabeth Lin, MD, MPH 2 Paul Ciechanowski, MD, MPH 1 Evette Ludman, PhD 2 Joan Russo, PhD 1 Carolyn Rutter,
Depression & Diabetes: Pathways and TeamCare Studies Wayne Katon, MD 1 Mike VonKorff, ScD 2 Elizabeth Lin, MD, MPH 2 Paul Ciechanowski, MD, MPH 1 Evette Ludman, PhD 2 Joan Russo, PhD 1 Carolyn Rutter,
APNA 26th Annual Conference Session 1012: November 7, 2012
 Fighting Stigma Through Social Inclusion and a Whole Person Approach to Wellness American Psychiatric Nurses Association 26 th Annual Conference Pittsburgh, PA November 9, 2012 Wilma Townsend, M.S.W. Acting
Fighting Stigma Through Social Inclusion and a Whole Person Approach to Wellness American Psychiatric Nurses Association 26 th Annual Conference Pittsburgh, PA November 9, 2012 Wilma Townsend, M.S.W. Acting
An Alternative Payment Model Concept for Office-based Treatment of Opioid Use Disorder
 An Alternative Payment Model Concept for Office-based Treatment of Opioid Use Disorder CONTENTS I. Need for an Alternative Payment Model for Opioid Use Disorder and Addiction... 2 A. Improving Services
An Alternative Payment Model Concept for Office-based Treatment of Opioid Use Disorder CONTENTS I. Need for an Alternative Payment Model for Opioid Use Disorder and Addiction... 2 A. Improving Services
Brenda Schmitthenner, MPA
 Brenda Schmitthenner, MPA 1 San Diego s ADRC implemented Care Transitions Intervention (CTI) in August 2010 Evidence based Coleman Model to coach, not do, using Four Pillars Establish and maintain a PHR
Brenda Schmitthenner, MPA 1 San Diego s ADRC implemented Care Transitions Intervention (CTI) in August 2010 Evidence based Coleman Model to coach, not do, using Four Pillars Establish and maintain a PHR
Community Health Needs Assessment: Implementation Plan
 Community Health Needs Assessment: Implementation Plan Community Health Needs Assessment (CHNA) California Senate Bill 697, the Patient Protection and Affordable Care Act (PPACA) (HR3590), and Internal
Community Health Needs Assessment: Implementation Plan Community Health Needs Assessment (CHNA) California Senate Bill 697, the Patient Protection and Affordable Care Act (PPACA) (HR3590), and Internal
2016 Community Service Plan & Community Health Improvement Plan
 2016 Community Service Plan & Community Health Improvement Plan A.O. Fox Memorial Hospital The Mary Imogene Bassett Hospital (dba: Bassett Medical Center) & Otsego County Health Department Service Area:
2016 Community Service Plan & Community Health Improvement Plan A.O. Fox Memorial Hospital The Mary Imogene Bassett Hospital (dba: Bassett Medical Center) & Otsego County Health Department Service Area:
Telephone Cognitive Behavioral Therapy for Rural Latinos: A Randomized Pilot Study
 Telephone Cognitive Behavioral Therapy for Rural Latinos: A Randomized Pilot Study Gino Aisenberg, PhD UW School of Social Work Megan Dwight Johnson, MD MPH RAND Corporation Daniela Golinelli,, PhD RAND
Telephone Cognitive Behavioral Therapy for Rural Latinos: A Randomized Pilot Study Gino Aisenberg, PhD UW School of Social Work Megan Dwight Johnson, MD MPH RAND Corporation Daniela Golinelli,, PhD RAND
Violence Prevention: Rethinking the Standard of Care for Family Planning
 Violence Prevention: Rethinking the Standard of Care for Family Planning Policy Brief For more than a decade, public health policies have been enacted to reduce health disparities in communities of color.
Violence Prevention: Rethinking the Standard of Care for Family Planning Policy Brief For more than a decade, public health policies have been enacted to reduce health disparities in communities of color.
TYPE IN THE CHAT. Please type your name, organization, and city/state into the chat.
 TYPE IN THE CHAT Please type your name, organization, and city/state into the chat. 1 EDC. 2017 All Rights Reserved. Data-Driven Quality Improvement in Zero Suicide May 2, 2017 2 Funding and Disclaimer
TYPE IN THE CHAT Please type your name, organization, and city/state into the chat. 1 EDC. 2017 All Rights Reserved. Data-Driven Quality Improvement in Zero Suicide May 2, 2017 2 Funding and Disclaimer
5/12/11. Educational Objectives. Goals
 Educational Objectives Learn: steps for initial depression screening and management in primary care when to refer to mental health providers tools for providers and patients principles of collaborative
Educational Objectives Learn: steps for initial depression screening and management in primary care when to refer to mental health providers tools for providers and patients principles of collaborative
Organization: NAMI Minnesota Request ID: Program Title: Reducing Smoking Among People with Mental Illnesses
 Organization: NAMI Minnesota Request ID: 16872475 Program Title: Reducing Smoking Among People with Mental Illnesses 1. Overall Goal & Objectives The overall goal of this project is to reduce the rate
Organization: NAMI Minnesota Request ID: 16872475 Program Title: Reducing Smoking Among People with Mental Illnesses 1. Overall Goal & Objectives The overall goal of this project is to reduce the rate
Integrated Care for Depression, Anxiety and PTSD. Introduction: Overview of Clinical Roles and Ideas
 Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
Clinical Inertia. The Promise of Collaborative Care for Treating Behavioral Health and Chronic Medical Conditions. Study: 161,697 Patients 4/12/17
 The Promise of Collaborative Care for Treating Behavioral Health and Chronic Medical Conditions Paul Ciechanowski, MD, MPH Clinical Associate Professor, University of Washington Chief Medical Officer,
The Promise of Collaborative Care for Treating Behavioral Health and Chronic Medical Conditions Paul Ciechanowski, MD, MPH Clinical Associate Professor, University of Washington Chief Medical Officer,
PCORI s Role in Supporting CER
 PCORI s Role in Supporting CER Ayodola Anise, MHS Program Officer, Addressing Disparities Program December 8, 2014 1 Objectives Background on PCORI Our national priorities and research PCORI supports Focus
PCORI s Role in Supporting CER Ayodola Anise, MHS Program Officer, Addressing Disparities Program December 8, 2014 1 Objectives Background on PCORI Our national priorities and research PCORI supports Focus
Taking Care: Child and Youth Mental Health TREATMENT OPTIONS
 Taking Care: Child and Youth Mental Health TREATMENT OPTIONS Open Learning Agency 2004 TREATMENT OPTIONS With appropriate treatment, more than 80% of people with depression get full relief from their symptoms
Taking Care: Child and Youth Mental Health TREATMENT OPTIONS Open Learning Agency 2004 TREATMENT OPTIONS With appropriate treatment, more than 80% of people with depression get full relief from their symptoms
COLLABORATIVE CARE: DELIVERING TEAM-BASED MENTAL HEALTH IN PRIMARY CARE SETTINGS
 COLLABORATIVE CARE: DELIVERING TEAM-BASED MENTAL HEALTH IN PRIMARY CARE SETTINGS ANNA RATZLIFF, MD,PHD ASSOCIATE PROFESSOR DIRECTOR OF INTEGRATED CARE TRAINING PROGRAM Behavioral Health Care in Washington
COLLABORATIVE CARE: DELIVERING TEAM-BASED MENTAL HEALTH IN PRIMARY CARE SETTINGS ANNA RATZLIFF, MD,PHD ASSOCIATE PROFESSOR DIRECTOR OF INTEGRATED CARE TRAINING PROGRAM Behavioral Health Care in Washington
The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles
 The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles Linda M. Siminerio, RN, PhD, CDE Professor of Medicine University of Pittsburgh School of Medicine & Nursing Objectives
The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles Linda M. Siminerio, RN, PhD, CDE Professor of Medicine University of Pittsburgh School of Medicine & Nursing Objectives
Webinar Agenda. Terminology. What Is It? How this fits for depression. Social Innovation Fund. Relapse Prevention Planning. Relapse Prevention
 SIF Webinar: Relapse Prevention 3/11/15 Webinar Agenda Relapse Prevention Social Innovation Fund Relapse Prevention Planning Rita Haverkamp Lori Higa What it is Why it s important Common and best practices
SIF Webinar: Relapse Prevention 3/11/15 Webinar Agenda Relapse Prevention Social Innovation Fund Relapse Prevention Planning Rita Haverkamp Lori Higa What it is Why it s important Common and best practices
ZERO SUICIDE WORKFORCE SURVEY
 ZERO SUICIDE WORKFORCE SURVEY The Zero Suicide Workforce Survey is a tool to assess staff knowledge, practices, and confidence. This survey is part of our organizational mission to adopt a system-wide
ZERO SUICIDE WORKFORCE SURVEY The Zero Suicide Workforce Survey is a tool to assess staff knowledge, practices, and confidence. This survey is part of our organizational mission to adopt a system-wide
DMAS UPDATE ON GAP PROGRAM. Cindi B. Jones, Director, DMAS House Appropriations Committee September 18, 2017
 DMAS UPDATE ON GAP PROGRAM Cindi B. Jones, Director, DMAS House Appropriations Committee September 18, 2017 Bridging the Mental Health Coverage GAP GAP s Inception The Governor s Access Plan 1 of a 10
DMAS UPDATE ON GAP PROGRAM Cindi B. Jones, Director, DMAS House Appropriations Committee September 18, 2017 Bridging the Mental Health Coverage GAP GAP s Inception The Governor s Access Plan 1 of a 10
Sample Report for Zero Suicide Workforce Survey
 Sample Report for Zero Suicide Workforce Survey Zero Suicide Workforce Survey Zero Suicide Workforce Survey Results This reports presents results from the Zero Suicide Workforce Survey that was implemented
Sample Report for Zero Suicide Workforce Survey Zero Suicide Workforce Survey Zero Suicide Workforce Survey Results This reports presents results from the Zero Suicide Workforce Survey that was implemented
Implementing and Improving Depression Screenings in the Primary Care Setting. Janet Tennison, PhD, MSW, LCSW Behavioral Health Project Manager
 Implementing and Improving Depression Screenings in the Primary Care Setting Janet Tennison, PhD, MSW, LCSW Behavioral Health Project Manager Today s Objectives Participants will: Increase understanding
Implementing and Improving Depression Screenings in the Primary Care Setting Janet Tennison, PhD, MSW, LCSW Behavioral Health Project Manager Today s Objectives Participants will: Increase understanding
HHSC LAR Request. Substance Abuse Disorder Coalition. Contact Person: Will Francis Members:
 HHSC LAR Request Substance Abuse Disorder Coalition Contact Person: Will Francis wfrancis.naswtx@socialworkers.org Members: NAMI Texas Children s Defense Fund Texas Communities for Recovery National Association
HHSC LAR Request Substance Abuse Disorder Coalition Contact Person: Will Francis wfrancis.naswtx@socialworkers.org Members: NAMI Texas Children s Defense Fund Texas Communities for Recovery National Association
WELLNESS CENTERS: A Coordinated Model to Support Students Physical & Emotional Health and Well-being in TUHSD High Schools
 WELLNESS CENTERS: A Coordinated Model to Support Students Physical & Emotional Health and Well-being in TUHSD High Schools Jessica Colvin, MSW, MPH, PPSC Wellness Director Tamalpais Union High School District
WELLNESS CENTERS: A Coordinated Model to Support Students Physical & Emotional Health and Well-being in TUHSD High Schools Jessica Colvin, MSW, MPH, PPSC Wellness Director Tamalpais Union High School District
517 Individuals 23 Families
 LATINO COMMUNITY CONNECTION Program Overview is a multi-layered program to provide behavioral health outreach, engagement, and prevention services in the Latino community. Canal Alliance, a trusted multi-service
LATINO COMMUNITY CONNECTION Program Overview is a multi-layered program to provide behavioral health outreach, engagement, and prevention services in the Latino community. Canal Alliance, a trusted multi-service
A Depression Management Program for Elderly Adults
 Program to Encourage Active, Rewarding Lives for Seniors (PEARLS) A Depression Management Program for Elderly Adults Illinois Governor s Conference on Aging Chicago, IL December 13, 2012 Amanda Timm Planning
Program to Encourage Active, Rewarding Lives for Seniors (PEARLS) A Depression Management Program for Elderly Adults Illinois Governor s Conference on Aging Chicago, IL December 13, 2012 Amanda Timm Planning
Suicide Prevention Strategic Plan
 Suicide Prevention Strategic Plan 2019 For more information visit dphhs.mt.gov/suicideprevention 2 Vision Zero suicide in the Big Sky State Mission Our Reduce suicide in Montana through a comprehensive,
Suicide Prevention Strategic Plan 2019 For more information visit dphhs.mt.gov/suicideprevention 2 Vision Zero suicide in the Big Sky State Mission Our Reduce suicide in Montana through a comprehensive,
2016 American Academy of Neurology
 2016 American Academy of Neurology PCSS-O is a collaborative effort led by American Academy of Addiction Psychiatry (AAAP) in partnership with: Addiction Technology Transfer Center (ATTC), American Academy
2016 American Academy of Neurology PCSS-O is a collaborative effort led by American Academy of Addiction Psychiatry (AAAP) in partnership with: Addiction Technology Transfer Center (ATTC), American Academy
Enhanced Substance Abuse Management in Higher Risk Populations
 Enhanced Substance Abuse Management in Higher Risk Populations Pano Yeracaris, MD, MPH Vice President & Chief Medical Officer, Network Health Annual Community Health Institute May 9-11, 2012 Resort & Conference
Enhanced Substance Abuse Management in Higher Risk Populations Pano Yeracaris, MD, MPH Vice President & Chief Medical Officer, Network Health Annual Community Health Institute May 9-11, 2012 Resort & Conference
CHI Franciscan. Matt Levi Director Virtual Health Services. March 31, 2015
 CHI Franciscan Matt Levi Director Virtual Health Services March 31, 2015 Reflection / 2 Agenda Introduction and background Matt Levi Director of Franciscan Health System Virtual Health Katie Farrell Manager
CHI Franciscan Matt Levi Director Virtual Health Services March 31, 2015 Reflection / 2 Agenda Introduction and background Matt Levi Director of Franciscan Health System Virtual Health Katie Farrell Manager
The Need for an Inter-Professional Approach for Working with Older Persons
 The Need for an Inter-Professional Approach for Working with Older Persons Linda K. Shumaker, R.N.- BC, M.A. Lynne Nessel, LCSW Pennsylvania Behavioral Health and Aging Coalition Effective and adequate
The Need for an Inter-Professional Approach for Working with Older Persons Linda K. Shumaker, R.N.- BC, M.A. Lynne Nessel, LCSW Pennsylvania Behavioral Health and Aging Coalition Effective and adequate
Implementation Strategy
 Implementation Strategy Analyzing primary data collected from surveys and focus groups as well as available data from secondary sources allowed the CNHA committee to prioritize the health needs for each
Implementation Strategy Analyzing primary data collected from surveys and focus groups as well as available data from secondary sources allowed the CNHA committee to prioritize the health needs for each
Case Management and Care Coordination: Two Successful Models
 Case Management and Care Coordination: Two Successful Models Asthma Educator Sharing Day October 17, 2011 Karen Meyerson, MSN, RN, FNP-C, AE-C Asthma Network of West Michigan Jan Roberts, RN, BSN, AE-C
Case Management and Care Coordination: Two Successful Models Asthma Educator Sharing Day October 17, 2011 Karen Meyerson, MSN, RN, FNP-C, AE-C Asthma Network of West Michigan Jan Roberts, RN, BSN, AE-C
DUPLICATION DISTRIBUTION PROHIBBITED AND. Utilizing Economic and Clinical Outcomes to Eliminate Health Disparities and Improve Health Equity
 General Session IV Utilizing Economic and Clinical Outcomes to Eliminate Health Disparities and Improve Health Equity Accreditation UAN 0024-0000-12-012-L04-P Participation in this activity earns 2.0 contact
General Session IV Utilizing Economic and Clinical Outcomes to Eliminate Health Disparities and Improve Health Equity Accreditation UAN 0024-0000-12-012-L04-P Participation in this activity earns 2.0 contact
The Bypassing the Blues Trial: Telephone-Delivered Collaborative Care for Treating Post-CABG Depression
 The Bypassing the Blues Trial: Telephone-Delivered Collaborative Care for Treating Post-CABG Depression www.bypassingtheblues.pitt.edu Bruce L. Rollman, MD, MPH Professor of Medicine, Psychiatry, and Clinical
The Bypassing the Blues Trial: Telephone-Delivered Collaborative Care for Treating Post-CABG Depression www.bypassingtheblues.pitt.edu Bruce L. Rollman, MD, MPH Professor of Medicine, Psychiatry, and Clinical
Integrating Mental Health and Primary Care (why would we want to do that?)
") Integrating Mental Health and Primary Care (why would we want to do that?) Andrew S. Pomerantz, MD National Mental Health Director, Integrated Services Veterans Health Administration Associate Professor
Integrating Mental Health and Primary Care (why would we want to do that?) Andrew S. Pomerantz, MD National Mental Health Director, Integrated Services Veterans Health Administration Associate Professor
Thank you for joining today, please wait while others sign in.
 Webinar Instructions Thank you for joining today, please wait while others sign in. The audio portion of this call will be heard through your computer speakers. Please make sure your speakers are on and
Webinar Instructions Thank you for joining today, please wait while others sign in. The audio portion of this call will be heard through your computer speakers. Please make sure your speakers are on and
You Can Make a Difference!
 You Can Make a Difference! How to help your clients become tobacco free What Does Smoking Cost Us? One study estimates that cost savings of between $1,142 and $1,358 per pregnancy can be achieved for each
You Can Make a Difference! How to help your clients become tobacco free What Does Smoking Cost Us? One study estimates that cost savings of between $1,142 and $1,358 per pregnancy can be achieved for each
NORTH CAROLINA CARDIOVASCULAR STATE PLAN I N T R O D U C T I O N S, G O A L S, O B J E C T I V E S A N D S T R A T E G I E S
 NORTH CAROLINA CARDIOVASCULAR STATE PLAN 2011-2016 I N T R O D U C T I O N S, G O A L S, O B J E C T I V E S A N D S T R A T E G I E S PRIMARY PREVENTION OF CARDIOVASCULAR DISEASE THROUGH HEALTHY LIVING
NORTH CAROLINA CARDIOVASCULAR STATE PLAN 2011-2016 I N T R O D U C T I O N S, G O A L S, O B J E C T I V E S A N D S T R A T E G I E S PRIMARY PREVENTION OF CARDIOVASCULAR DISEASE THROUGH HEALTHY LIVING
MHMR: Services in the Community. Susan Garnett, MSW Chief Executive Officer
 MHMR: Services in the Community Susan Garnett, MSW Chief Executive Officer Background 1969: The Texas system of community-based services was established as a state-local partnership delivering care to
MHMR: Services in the Community Susan Garnett, MSW Chief Executive Officer Background 1969: The Texas system of community-based services was established as a state-local partnership delivering care to
A Community Wide Approach to Innovating Outreach, Crisis Intervention, and Community Education for Youth affected by Mental Health Challenges
 Waukesha County Health and Human Services A Community Wide Approach to Innovating Outreach, Crisis Intervention, and Community Education for Youth affected by Mental Health Challenges Quick Review of the
Waukesha County Health and Human Services A Community Wide Approach to Innovating Outreach, Crisis Intervention, and Community Education for Youth affected by Mental Health Challenges Quick Review of the
Curriculum Outline for Advanced Level Training for Geriatric Mental Health Certificate
 Curriculum Outline for Advanced Level Training for Geriatric Mental Health Certificate The Geriatric Certificate Training Program shall address the following goals: Reduce stigma Increase knowledge about
Curriculum Outline for Advanced Level Training for Geriatric Mental Health Certificate The Geriatric Certificate Training Program shall address the following goals: Reduce stigma Increase knowledge about
Evidence Based Collaborative Care. Natasha Cunningham, MD Duke Department of Psychiatry and Behavioral Health Psychiatry Grand Rounds 9/24/15
 Evidence Based Collaborative Care Natasha Cunningham, MD Duke Department of Psychiatry and Behavioral Health Psychiatry Grand Rounds 9/24/15 Objectives Identify three components of evidence based collaborative
Evidence Based Collaborative Care Natasha Cunningham, MD Duke Department of Psychiatry and Behavioral Health Psychiatry Grand Rounds 9/24/15 Objectives Identify three components of evidence based collaborative
Psychiatry and Psychology Continuing Education 2018 Offerings
 Mayo Clinic School of Continuous Professional Development Psychiatry and Psychology Continuing Education 2018 Offerings Sarasota, FL Chicago, IL Santa Fe, NM Washington, DC Rochester, MN Psychiatry in
Mayo Clinic School of Continuous Professional Development Psychiatry and Psychology Continuing Education 2018 Offerings Sarasota, FL Chicago, IL Santa Fe, NM Washington, DC Rochester, MN Psychiatry in
ATTUD APPLICATION FORM FOR WEBSITE LISTING (PHASE 1): TOBACCO TREATMENT SPECIALIST (TTS) TRAINING PROGRAM PROGRAM INFORMATION & OVERVIEW
: TOBACCO TREATMENT SPECIALIST (TTS) TRAINING PROGRAM PROGRAM INFORMATION & OVERVIEW") ATTUD APPLICATION FORM FOR WEBSITE LISTING (PHASE 1): TOBACCO TREATMENT SPECIALIST (TTS) TRAINING PROGRAM APPLICATION NUMBER: TTS 2010_2_0011 PROGRAM INFORMATION & OVERVIEW Date of this Application 2/01/10
ATTUD APPLICATION FORM FOR WEBSITE LISTING (PHASE 1): TOBACCO TREATMENT SPECIALIST (TTS) TRAINING PROGRAM APPLICATION NUMBER: TTS 2010_2_0011 PROGRAM INFORMATION & OVERVIEW Date of this Application 2/01/10
Petaluma Sober Circle
 Petaluma Sober Circle NATIONAL HEALTH CARE FOR THE HOMELESS WASHINGTON D.C. JUNE 2017 Annie Nicol, FNP, and Randy Clay Outreach Lead Petaluma Sober Circle Petaluma, California The Petaluma Sober Circle
Petaluma Sober Circle NATIONAL HEALTH CARE FOR THE HOMELESS WASHINGTON D.C. JUNE 2017 Annie Nicol, FNP, and Randy Clay Outreach Lead Petaluma Sober Circle Petaluma, California The Petaluma Sober Circle
Identifying Adult Mental Disorders with Existing Data Sources
 Identifying Adult Mental Disorders with Existing Data Sources Mark Olfson, M.D., M.P.H. New York State Psychiatric Institute Columbia University New York, New York Everything that can be counted does not
Identifying Adult Mental Disorders with Existing Data Sources Mark Olfson, M.D., M.P.H. New York State Psychiatric Institute Columbia University New York, New York Everything that can be counted does not
and Independence PROVIDING RESIDENTIAL AND OUTPATIENT TREATMENT FOR ADOLESCENTS WITH BEHAVIORAL, EMOTIONAL AND SUBSTANCE ABUSE PROBLEMS
 The Center for Success and Independence PROVIDING RESIDENTIAL AND OUTPATIENT TREATMENT FOR ADOLESCENTS WITH BEHAVIORAL, EMOTIONAL AND SUBSTANCE ABUSE PROBLEMS THE CENTER FOR SUCCESS AND INDEPENDENCE 3722
The Center for Success and Independence PROVIDING RESIDENTIAL AND OUTPATIENT TREATMENT FOR ADOLESCENTS WITH BEHAVIORAL, EMOTIONAL AND SUBSTANCE ABUSE PROBLEMS THE CENTER FOR SUCCESS AND INDEPENDENCE 3722
at Kaiser Permanente, Southern California April 2017
 Complete Care at Kaiser Permanente, Southern California April 2017 Tim Ho, MD, MPH Regional Assistant Medical Director, Quality & Complete Care Southern California Permanente Medical Group Session Objectives
Complete Care at Kaiser Permanente, Southern California April 2017 Tim Ho, MD, MPH Regional Assistant Medical Director, Quality & Complete Care Southern California Permanente Medical Group Session Objectives
Adolescent Coping with Depression (CWD-A)
") This program description was created for SAMHSA s National Registry for Evidence-based Programs and Practices (NREPP). Please note that SAMHSA has discontinued the NREPP program and these program descriptions
This program description was created for SAMHSA s National Registry for Evidence-based Programs and Practices (NREPP). Please note that SAMHSA has discontinued the NREPP program and these program descriptions
Making Diabetes Prevention a Reality: The National Diabetes Prevention Program
 Making Diabetes Prevention a Reality: The National Diabetes Prevention Program Ann Albright, PhD, RD Director, Division of Diabetes Translation Centers for Disease Control and Prevention National Center
Making Diabetes Prevention a Reality: The National Diabetes Prevention Program Ann Albright, PhD, RD Director, Division of Diabetes Translation Centers for Disease Control and Prevention National Center
Exhibit I-1 Performance Measures. Numerator (general description only)
") # Priority Type Performance Measure Core Measures (implement 9/1/09) 1 C OE Hospital readmissions within 7, 30 and 90 days postdischarge 2 C OE Percent of Members prescribed redundant or duplicated antipsychotic
# Priority Type Performance Measure Core Measures (implement 9/1/09) 1 C OE Hospital readmissions within 7, 30 and 90 days postdischarge 2 C OE Percent of Members prescribed redundant or duplicated antipsychotic
Primary Care Mental Health. Primary Care Mental Health. Ms. Jones. Big picture: need, strategies Collaborative care model Implementing Barriers
 Big picture: need, strategies Collaborative care model Implementing Barriers Ms. Jones New patient to you 45 year old with depression & anxiety Several prior antidepressant trials Primary Care Mental Health
Big picture: need, strategies Collaborative care model Implementing Barriers Ms. Jones New patient to you 45 year old with depression & anxiety Several prior antidepressant trials Primary Care Mental Health
Substance Abuse. Among current drinkers, men in nonmetro areas consume 5 or more drinks in one day than those in metro areas (56% vs.
 Framing the Issue Substance Abuse Among current drinkers, men in nonmetro areas consume 5 or more drinks in one day than those in metro areas (56% vs. 48-52%) Periodic heavy drinking more common among
Framing the Issue Substance Abuse Among current drinkers, men in nonmetro areas consume 5 or more drinks in one day than those in metro areas (56% vs. 48-52%) Periodic heavy drinking more common among
Program Summary. The CT Early Detection and Prevention Program
 Program Summary The CT Early Detection and Prevention Program 1 The CT Early Detection and Prevention Program is part of the Center for Disease Control and Prevention s (CDC) National Breast and Cervical
Program Summary The CT Early Detection and Prevention Program 1 The CT Early Detection and Prevention Program is part of the Center for Disease Control and Prevention s (CDC) National Breast and Cervical
16 th Annual IHA Stakeholders Meeting Session 2C
 16 th Annual IHA Stakeholders Meeting Session 2C September 19, 2017 Hilton Los Angeles Airport Thank you to our Content Partner: Medication Adherence AppleCare Pharmacy Programs Confidential and proprietary.
16 th Annual IHA Stakeholders Meeting Session 2C September 19, 2017 Hilton Los Angeles Airport Thank you to our Content Partner: Medication Adherence AppleCare Pharmacy Programs Confidential and proprietary.
GUIDELINES FOR POST PEDIATRICS PORTAL PROGRAM
 GUIDELINES FOR POST PEDIATRICS PORTAL PROGRAM Psychiatry is a medical specialty that is focused on the prevention, diagnosis, and treatment of mental, addictive, and emotional disorders throughout the
GUIDELINES FOR POST PEDIATRICS PORTAL PROGRAM Psychiatry is a medical specialty that is focused on the prevention, diagnosis, and treatment of mental, addictive, and emotional disorders throughout the
How pharmacy and retail health can support health and wellness. Nancy Gagliano Chief Medical Officer, MC September, 2014
 How pharmacy and retail health can support health and wellness Nancy Gagliano Chief Medical Officer, MC September, 2014 2 An important decision for public health Current Health Care Challenges The State
How pharmacy and retail health can support health and wellness Nancy Gagliano Chief Medical Officer, MC September, 2014 2 An important decision for public health Current Health Care Challenges The State
Mentors on Discharge
 Mentors on Discharge Repeated psychiatric hospitalizations are costly, impede recovery and are demoralizing to individuals, families, and clinicians. Between 40 to 50 percent of patients with a history
Mentors on Discharge Repeated psychiatric hospitalizations are costly, impede recovery and are demoralizing to individuals, families, and clinicians. Between 40 to 50 percent of patients with a history
Pathway to Care. Rationale. Organization of the Pathway. Education about the Suicide Safe Care Pathway
 Pathway to Care Goal 7: Individuals assessed to be at risk will receive care in accordance with the Suicide Safe Care Pathway. Agencies will use quality management tools to monitor adherence to the Suicide
Pathway to Care Goal 7: Individuals assessed to be at risk will receive care in accordance with the Suicide Safe Care Pathway. Agencies will use quality management tools to monitor adherence to the Suicide