Anesthesia For The Elderly. Yasser Sakawi, M.D. Associate Professor Anesthesiology Department
|
|
|
- Deirdre Reeves
- 6 years ago
- Views:
Transcription

1 Anesthesia For The Elderly Yasser Sakawi, M.D. Associate Professor Anesthesiology Department
2 Topics of Discussion General concepts and definitions Aging and general organ function Cardiopulmonary function Hepato-renal and immune function Nervous system Anesthetic management and outcome
3 General Concepts Aging is a universal progressive degenerative changes in structure and function of organs Chronologic age versus physiologic age No clear consensus over the cutoff off age for being old Generally age 65 and older has been arbitrarily accepted to define human subjects as elderly or geriatric

4 General Concepts Advances in medical science and health care has prolonged the life expectancy of human beings, but failed to prolong the life span of our species which continues to be around years over the past 20 centuries

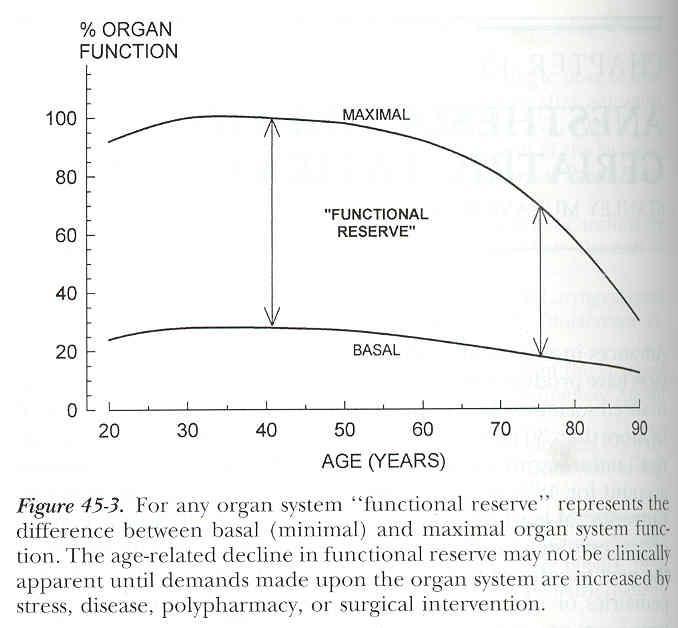
5 Aging and General Organ Function The first apparent decline in organ function usually starts around the fourth decade of life, then become more dramatic around the seventh decade of life Organ system functional reserve represent a safety margin of organ capacity to meet additional demands at times of stress
6
7

8 Cardio-pulmonary Physiology of Aging Aging usually produces progressive depression of cardiac output and index In healthy elderly this usually correlates well with the drop in metabolic demands resulting from atrophy of skeletal muscles and loss of tissue mass in major organs
9 Cardio-pulmonary Physiology of Aging Aging usually results in diastolic dysfunction, due to stiffer and less compliant myocardium Elderly patients are more dependent on sinus rhythm for proper filling of the ventricles Any modest decrease in venous return can compromise the stroke volume
10 Cardio-pulmonary Physiology of Aging Loss of elastic tissue in the lungs results in some deleterious effects on gas exchange An emphysema like picture develops over time in elderly patient The closing volume and capacity moves closer to the FRC leading to alveolar collapse even in sitting position
11 Cardio-pulmonary Physiology of Aging Elderly patients are more susceptible to the respiratory depressant effects of both narcotics and benzodiazepines Chest wall rigidity is more prevalent in elderly patients after narcotics Less sensitivity of vocal cord closure reflex results in more susceptibility to aspiration
12 Hepato-renal and Immune Function Liver tissue mass and hepatic blood flow declines about 40% by age 80 That might explain the delayed biotransformation of narcotics and other drugs Should avoid hypotention, low cardiac output states and hypothermia to prevent hepatic injury
13 Hepato-renal and Immune Function By eighth decade there is loss of 30% of renal tissue mass and renal blood flow decreases by 50% Despite compromise of renal functional reserve the creatinine level stays WNL due to declining skeletal muscle mass Diminished thirst, poor diet and use of diuretics predisposes elderly patients to intravascular and intracellular dehydration
14 Nervous System Brain mass at age 80 is 20% less than values measured postmortem in young adults Rapid reduction in gray matter tissue mass with compensatory increase in CSF after the sixth decade Aging in effect produces a form of low pressure hydrocephalus
15 Nervous System The blood-brain barrier remains intact as well as the autoregulation of the cerebrovascular resistance General knowledge base, comprehension, and long-term memory are well maintained in active and fit older adults There is decline in short-term memory, visual and auditory reaction time
16
17 Perioperative Management and Outcome Overall, perioperative mortality and major morbidity increase with advancing age However, age related disease, not aging itself, largely determines the morbidity and mortality
18
19 Perioperative Management and Outcome Morbidity and mortality are higher in elderly surgical patients because this patient population has greater incidence and severity of concurrent disease and greater exposure to invasive medical interventions
20 Perioperative Management and Outcome The high incidence of polypharmacy associated with chronic disease produces an age related increase in adverse drug reaction and complicate the perioperative management of the elderly Probability of serious pulmonary or hemodynamic complication is determined by site of surgery and physical status of pt
21 Perioperative Management and Outcome Adverse outcomes in geriatric patients show relative predominance of cardiac and hemodynamic complications Other complications like pulmonary, sepsis, and renal failure contribute significantly to morbidity in the elderly

22 Perioperative Management and Outcome Even when elderly patients are cleared for surgery by consultants they might still have mild to severe cardiopulmonary functional deficits Adequate time for diagnosis, treatment and preparation for the anesthetic plan is essential for reducing the severity of complications
23 Perioperative Management and Outcome It is not possible to determine if there is a single best anesthetic for the elderly with regards to survival and outcome All anesthetic techniques are appropriate and in widespread use From perspective of major adverse outcome and mortality, a brief intraopertive exposure to anesthesia is insignificant component of a prolonged, difficult and complex hospital course
24 Perioperative Management and Outcome Neither regional nor general anesthesia has clearly demonstrable superiority of outcome in the elderly One or the other technique may be preferred for use in specific procedures for other medical reasons
25 Perioperative Management and Outcome The use of newer intravenous agents like remifentanil and cisatracurium minimizes dependence upon organ system functional reserve for drug elimination New inhalational agents like desflurane and sevoflurane provide rapid recovery of consciousness in the elderly Well conducted GA is safe
26 Perioperative Management and Outcome Recent large scale prospective studies of outpatients showed less postoperative nausea and vomiting in elderly Sinclair DR, Anesthesiology, 1999;91:109 Prompt and complete recovery of mental function is important in elderly patients because mentation is already compromised by age related disease and drug therapy
27 Perioperative Management and Outcome After GA there is greater incidence of postoperative confusion in the elderly outpatient population Yzabar Y, Br J Anesthe, 1996;76:194 The most common cause of failure to emerge promptly from GA is simply the use of too much anesthesia and too many anesthetic agents Muravcheck S, Clin Anesthesiol, 1986;4:1035
28 Perioperative Management and Outcome Full return of cognitive function to preop levels with properly conducted uncomplicated GA, may take up to 5-10 days after prolonged GA Psychometrically defined post op cognitive dysfunction could be demonstrated for up to 3 months in 10-15% of uncomplicated surgery with HLOS 4 or more days Moller JT, Lancet 1998;351:857 The exact neurophysiologic and pharmacologic mechanism remains unknown

29 Perioperative Management and Outcome Chronic medication, drug interaction, disorientation due to sensory deprivation or the disruption of normal routine needed to maintain implicit memory may explain such high incidence of delirium in the elderly population GA or the drugs used to produce it may produce residual neurotransmitter injury
30 Perioperative Management and Outcome Local anesthesia or regional anesthesia, if can be comfortably performed without need for heavy sedation, may significantly improve postoperative mental function However, there is no evidence of any longterm benefit to this approach Chung FF, Can J Anesth, 1989;36:382 Complications of RA like nerve palsies, neuropraxias, and residual parasthesia are more common in the elderly population
31 Perioperative Management and Outcome Intraoperative management require gentle and expert routine care The aged skin is very thin, bones are fragile, joints are stiff and the range of motion is limited Proper padding, positioning and warming is important Avoid direct contact of heat with poorly perfused skin or pressure points, it can produce ischemic lesions
32 Perioperative Management and Outcome Postoperative bleeding diathesis or hypercoagulable states, and infection are more common in elderly Diastolic dysfunction results in elderly patients more prone to congestive heart failure from modest I/V rates
33 Perioperative Management and Outcome Major surgery and the resultant tissue injury produce extensive neuroendocrine and sympathoadrenal stress Suppression of excessive sympathetic activity appears to promote rewarming and healing, reduce cardiovascular and pulmonary demands
34 Perioperative Management and Outcome Ageism may influence caregivers to withhold adequate analgesia for fear of opioid side effects Untreated pain and related emotional stress may impair immune response and increase the risk of postoperative infection Esterling BA, Psychosom Med 1996;58:264
35 Perioperative Management and Outcome Therefore, a postoperative anesthetic plan than include postoperative epidural analgesia and sympathectomy or a sympathetic modulator like dexmedetomidine (precedex) may be of special value in elderly patient

36 Summary Elderly patients do not require special type of anesthetic their perioperative care simply requires the highest standards of preparation and diagnosis and control of pre-existing disease, vigilance, and meticulous execution of all details of the planned anesthetic and postoperative management
37 Questions?
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006.
 Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Chapter Goal. Learning Objectives 9/12/2012. Chapter 36. Geriatrics. Use assessment findings to formulate management plan for geriatric patients
 Chapter 36 Geriatrics Chapter Goal Use assessment findings to formulate management plan for geriatric patients Learning Objectives Describe dependent & independent living environments Identify local resources
Chapter 36 Geriatrics Chapter Goal Use assessment findings to formulate management plan for geriatric patients Learning Objectives Describe dependent & independent living environments Identify local resources
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
General surgery. Thyroid surgery. Physiological response to pneumoperitoneum. Bowel resection
 General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
General Anesthesia. Mohamed A. Yaseen
 General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
CRACKCast E181 Approach to the Geriatric Patient
 CRACKCast E181 Approach to the Geriatric Patient Italicized text refers to passages quoted from Rosen s Emergency Medicine (9 th Ed). Key concepts: We are in the midst of a silver tsunami, with 10,000
CRACKCast E181 Approach to the Geriatric Patient Italicized text refers to passages quoted from Rosen s Emergency Medicine (9 th Ed). Key concepts: We are in the midst of a silver tsunami, with 10,000
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adverse drug events, polypharmacy and perioperative considerations in elderly patients, 377 389 Age, and risk of postoperative urinary retention,
Note: Page numbers of article titles are in boldface type. A Adverse drug events, polypharmacy and perioperative considerations in elderly patients, 377 389 Age, and risk of postoperative urinary retention,
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification
 Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Chapter 25. General Anesthetics
 Chapter 25 1. Introduction General anesthetics: 1. Analgesia 2. Amnesia 3. Loss of consciousness 4. Inhibition of sensory and autonomic reflexes 5. Skeletal muscle relaxation An ideal anesthetic: 1. A
Chapter 25 1. Introduction General anesthetics: 1. Analgesia 2. Amnesia 3. Loss of consciousness 4. Inhibition of sensory and autonomic reflexes 5. Skeletal muscle relaxation An ideal anesthetic: 1. A
Preventing Postoperative Cognitive Decline in the Elderly
 Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Richard A. Beers, M.D. Professor, Anesthesiology SUNY Upstate Medical Univ VA Medical Center Syracuse, NY
 Richard A. Beers, M.D. Professor, Anesthesiology SUNY Upstate Medical Univ VA Medical Center Syracuse, NY beersr@verizon.net 2 Improvements in safety and advances in care are re-invested in older, sicker
Richard A. Beers, M.D. Professor, Anesthesiology SUNY Upstate Medical Univ VA Medical Center Syracuse, NY beersr@verizon.net 2 Improvements in safety and advances in care are re-invested in older, sicker
Remifentanil. Addressing the challenges of ambulatory orthopedic procedures 1-3
 Remifentanil Addressing the challenges of ambulatory orthopedic procedures 1-3 INDICATIONS AND IMPORTANT RISK INFORMATION INDICATIONS ULTIVA (remifentanil HCl) for Injection is indicated for intravenous
Remifentanil Addressing the challenges of ambulatory orthopedic procedures 1-3 INDICATIONS AND IMPORTANT RISK INFORMATION INDICATIONS ULTIVA (remifentanil HCl) for Injection is indicated for intravenous
General anesthesia. No single drug capable of achieving these effects both safely and effectively.
 General anesthesia General anesthesia is essential to surgical practice, because it renders patients analgesic, amnesia, and unconscious reflexes, while causing muscle relaxation and suppression of undesirable
General anesthesia General anesthesia is essential to surgical practice, because it renders patients analgesic, amnesia, and unconscious reflexes, while causing muscle relaxation and suppression of undesirable
GENERAL VERSUS SPINAL ANESTHESIA: WHICH IS A RISK FACTOR FOR OCTOGENARIAN HIP FRACTURE REPAIR PATIENTS?
 ORIGINAL ARTICLE GENERAL VERSUS SPINAL ANESTHESIA: WHICH IS A RISK FACTOR FOR OCTOGENARIAN HIP FRACTURE REPAIR PATIENTS? Yi-Ju Shih 1,2, Cheng-Hung Hsieh 1,3, Ting-Wei Kang 1, Shih-Yen Peng 1,4, Kuo-Tung
ORIGINAL ARTICLE GENERAL VERSUS SPINAL ANESTHESIA: WHICH IS A RISK FACTOR FOR OCTOGENARIAN HIP FRACTURE REPAIR PATIENTS? Yi-Ju Shih 1,2, Cheng-Hung Hsieh 1,3, Ting-Wei Kang 1, Shih-Yen Peng 1,4, Kuo-Tung
General anesthetics. Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine
 General anesthetics Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine Rationale General anesthesia is essential to surgical practice, because it renders patients analgesic,
General anesthetics Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine Rationale General anesthesia is essential to surgical practice, because it renders patients analgesic,
Cardiothoracic Fellow Expectations Division of Cardiac Anesthesia, Beth Israel Deaconess Medical Center
 The fellowship in Cardiothoracic Anesthesia at the Beth Israel Deaconess Medical Center is intended to provide the foundation for a career as either an academic cardiothoracic anesthesiologist or clinical
The fellowship in Cardiothoracic Anesthesia at the Beth Israel Deaconess Medical Center is intended to provide the foundation for a career as either an academic cardiothoracic anesthesiologist or clinical
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
ICU Management of Minimally Invasive Cardiac Surgery
 ICU Management of Minimally Invasive Cardiac Surgery Benjamin A. Kohl, MD, FCCM Chief of Critical Care, Aria-Jefferson Health Professor of Anesthesiology Thomas Jefferson University Sidney Kimmel Medical
ICU Management of Minimally Invasive Cardiac Surgery Benjamin A. Kohl, MD, FCCM Chief of Critical Care, Aria-Jefferson Health Professor of Anesthesiology Thomas Jefferson University Sidney Kimmel Medical
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Anesthesiology in advanced radical surgery. Bruno Carrara Ospedali Riuniti di Bergamo
 Anesthesiology in advanced radical surgery Bruno Carrara Ospedali Riuniti di Bergamo Anesthetic considerations Anesthesiology in advanced radical surgery Anesthesiologists's task is to minimize the contribution
Anesthesiology in advanced radical surgery Bruno Carrara Ospedali Riuniti di Bergamo Anesthetic considerations Anesthesiology in advanced radical surgery Anesthesiologists's task is to minimize the contribution
Chapter 19. Media Directory. Topical (Surface) Anesthesia. Spinal Anesthesia. Nerve-Block Anesthesia. Infiltration (Field-Block) Anesthesia
 Anesthesia. Spinal Anesthesia. Nerve-Block Anesthesia. Infiltration (Field-Block) Anesthesia") Chapter 19 Drugs for Local and General Anesthesia Slide 18 Media Directory Lidocaine Animation Upper Saddle River, New Jersey 07458 All rights reserved. Topical (Surface) Anesthesia Creams, sprays, suppositories
Chapter 19 Drugs for Local and General Anesthesia Slide 18 Media Directory Lidocaine Animation Upper Saddle River, New Jersey 07458 All rights reserved. Topical (Surface) Anesthesia Creams, sprays, suppositories
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Delirium and Dementia
 Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased
Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased
Dr Kelly Jones Anesthesiologist at Northwest Orthopedics
 Dr Kelly Jones Anesthesiologist at Northwest Orthopedics Decrease narcotic use in the immediate post operative period. Better Pain Control Less side effects then General Anesthesia Sedation Post operative
Dr Kelly Jones Anesthesiologist at Northwest Orthopedics Decrease narcotic use in the immediate post operative period. Better Pain Control Less side effects then General Anesthesia Sedation Post operative
Anaesthesia for the Over 75s. Chris Edge
 Anaesthesia for the Over 75s Chris Edge Topics to be Covered Post-operative cognitive management Morbidity and mortality General anaesthesia a good idea or not? Multiple comorbidities and assessment of
Anaesthesia for the Over 75s Chris Edge Topics to be Covered Post-operative cognitive management Morbidity and mortality General anaesthesia a good idea or not? Multiple comorbidities and assessment of
Childhood Obesity: Anesthetic Implications
 Childhood Obesity: Anesthetic Implications The Changing Practice of Anesthesia 2015 UCSF Department of Anesthesia and Perioperative Care Marla Ferschl, MD Associate Professor of Anesthesia University of
Childhood Obesity: Anesthetic Implications The Changing Practice of Anesthesia 2015 UCSF Department of Anesthesia and Perioperative Care Marla Ferschl, MD Associate Professor of Anesthesia University of
Anesthesia for OutPatient Spine Surgery. Michael A. Kellams, D.O.
 Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Preoperative Anxiety
 Alyssa Brzenski Case You are called by a parent of a child who you took care of a week and a half ago. The child, a 4 year old boy, came to IR for the first of many sclerotherapy of a Venous Malformation
Alyssa Brzenski Case You are called by a parent of a child who you took care of a week and a half ago. The child, a 4 year old boy, came to IR for the first of many sclerotherapy of a Venous Malformation
Day 1 10:50. Panel Discussions/Group Photo Coffee/Tea Break 11:15-11:30 (Networking) Different types of. Anesthesia. Day 2
 Different types of. Anesthesia. Day 2") Day 1 Evening Sessions Morning Sessions Reception/Registration 08:3009:30 General Session Time 09:3009:55 Inaugural Address 10:0010:25 Keynote/Plenary Talk 1 Least of 3 Keynote/Plenary 10:25Talks 10:50
Day 1 Evening Sessions Morning Sessions Reception/Registration 08:3009:30 General Session Time 09:3009:55 Inaugural Address 10:0010:25 Keynote/Plenary Talk 1 Least of 3 Keynote/Plenary 10:25Talks 10:50
Accidental Hypothermia
 Accidental Hypothermia Gordon G. Giesbrecht, Ph.D., Professor Health Leisure and Human Performance Research Institute University of Manitoba, Winnipeg, Manitoba, Canada, R3T 2N2 Learning Objectives: 1)
Accidental Hypothermia Gordon G. Giesbrecht, Ph.D., Professor Health Leisure and Human Performance Research Institute University of Manitoba, Winnipeg, Manitoba, Canada, R3T 2N2 Learning Objectives: 1)
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Management Of Medical Emergencies
 Management Of Medical Emergencies U.S. Aging Population 35 million people (12%) 65 years or older Number will increase by nearly 75% by year 2030 The number of people more than 85 years old will approach
Management Of Medical Emergencies U.S. Aging Population 35 million people (12%) 65 years or older Number will increase by nearly 75% by year 2030 The number of people more than 85 years old will approach
ISPUB.COM. Review Of Currently Used Inhalation Anesthetics: Part II. O Wenker SIDE EFFECTS OF INHALED ANESTHETICS CARDIOVASCULAR SYSTEM
 ISPUB.COM The Internet Journal of Anesthesiology Volume 3 Number 3 O Wenker Citation O Wenker.. The Internet Journal of Anesthesiology. 1998 Volume 3 Number 3. Abstract SIDE EFFECTS OF INHALED ANESTHETICS
ISPUB.COM The Internet Journal of Anesthesiology Volume 3 Number 3 O Wenker Citation O Wenker.. The Internet Journal of Anesthesiology. 1998 Volume 3 Number 3. Abstract SIDE EFFECTS OF INHALED ANESTHETICS
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017
 patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017") Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017 CONTENT WHO is the critically ill elderly (geriatric) patient? WHY look at the critically
Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017 CONTENT WHO is the critically ill elderly (geriatric) patient? WHY look at the critically
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Optimal Perioperative Management of the Geriatric Patient: A Best Practices Guideline from the ACS NSQIP/American Geriatrics Society
 Optimal Perioperative Management of the Geriatric Patient: A Best Practices Guideline from the ACS NSQIP/American Geriatrics Society Sanjay Mohanty, MD; Ronnie A. Rosenthal, MS,MD; Marcia M. Russell, MD;
Optimal Perioperative Management of the Geriatric Patient: A Best Practices Guideline from the ACS NSQIP/American Geriatrics Society Sanjay Mohanty, MD; Ronnie A. Rosenthal, MS,MD; Marcia M. Russell, MD;
Anatomy and Physiology of Ageing
 Anatomy and Physiology of Ageing Dr Reena Hacking, Specialist Registrar, Anaesthesia, Imperial School of Anaesthesia, U.K. Dr Dominic O Connor, Consultant Anaesthetist, Royal Perth Hospital, Western Australia
Anatomy and Physiology of Ageing Dr Reena Hacking, Specialist Registrar, Anaesthesia, Imperial School of Anaesthesia, U.K. Dr Dominic O Connor, Consultant Anaesthetist, Royal Perth Hospital, Western Australia
7/18/2014 به نام خداوند جان و خرد
 1 به نام خداوند جان و خرد NURSING CARE in GERIATRIC SURGERY A. Shahrokhi Qazvin Nursing & Midwifery School 3 Natural, progressive & irreversible alterations in aged people result in significant physiological
1 به نام خداوند جان و خرد NURSING CARE in GERIATRIC SURGERY A. Shahrokhi Qazvin Nursing & Midwifery School 3 Natural, progressive & irreversible alterations in aged people result in significant physiological
ANESTHESIA EXAM (four week rotation)
") SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
REGIONAL/LOCAL ANESTHESIA and OBESITY
 REGIONAL/LOCAL ANESTHESIA and OBESITY Jay B. Brodsky, MD Stanford University School of Medicine Jbrodsky@stanford.edu Potential Advantages Regional compared to General Anesthesia Minimal intra-operative
REGIONAL/LOCAL ANESTHESIA and OBESITY Jay B. Brodsky, MD Stanford University School of Medicine Jbrodsky@stanford.edu Potential Advantages Regional compared to General Anesthesia Minimal intra-operative
Pre-eclampsia: key issues. Robin Russell Nuffield Department of Anaesthetics John Radcliffe Hospital Oxford
 Robin Russell Nuffield Department of Anaesthetics John Radcliffe Hospital Oxford Antenatal Issues Labour Analgesia Anaesthesia for Delivery High Dependency Care Hypertension systolic >140 mmhg or diastolic
Robin Russell Nuffield Department of Anaesthetics John Radcliffe Hospital Oxford Antenatal Issues Labour Analgesia Anaesthesia for Delivery High Dependency Care Hypertension systolic >140 mmhg or diastolic
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Disclosure. Objectives 9/13/2018. NIA/NIH 1R03AG (PI-Bentov) More than Start low go slow. start low go slow
 More than Start low go slow. start low go slow") Sedation and analgesia in geriatric trauma Sept 2018 Itay Bentov MD PhD Disclosure NIA/NIH 1R03AG042353 (PI-Bentov) More than Start low go slow start low go slow Objectives List age-related physiologic
Sedation and analgesia in geriatric trauma Sept 2018 Itay Bentov MD PhD Disclosure NIA/NIH 1R03AG042353 (PI-Bentov) More than Start low go slow start low go slow Objectives List age-related physiologic
INHALATION AGENTS 2013/05/28 1
 INHALATION AGENTS 2013/05/28 1 2013/05/28 Isn t it romantic? 2 Administration 3 Physics Critical temperature Vapour vs. Gas Vapour pressure Blood Gas Partition Coefficient BGPC MAC 2013/05/28 4 Critical
INHALATION AGENTS 2013/05/28 1 2013/05/28 Isn t it romantic? 2 Administration 3 Physics Critical temperature Vapour vs. Gas Vapour pressure Blood Gas Partition Coefficient BGPC MAC 2013/05/28 4 Critical
Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy
 Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy Department of Anaesthesia University Children s Hospital Zurich Switzerland Epidemiology Herniotomy needed in
Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy Department of Anaesthesia University Children s Hospital Zurich Switzerland Epidemiology Herniotomy needed in
Subspecialty Rotation: Anesthesia
 Subspecialty Rotation: Anesthesia Faculty: John Heaton, M.D. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation. Recognize and manage upper
Subspecialty Rotation: Anesthesia Faculty: John Heaton, M.D. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation. Recognize and manage upper
Physiology and Pharmacology
 Pharmacokinetics Physiology and Pharmacology Pharmacokinetics of Local Anesthetics Uptake Oral Route Topical Route Injection Distribution Metabolism (Biotransformation) Excretion Uptake Vasoactivity Local
Pharmacokinetics Physiology and Pharmacology Pharmacokinetics of Local Anesthetics Uptake Oral Route Topical Route Injection Distribution Metabolism (Biotransformation) Excretion Uptake Vasoactivity Local
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia. RA Dyer Interlaken 2017
 The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
Anesthesia for Total Hip and Knee Arthroplasty
 Anesthesia for Total Hip and Knee Arthroplasty Typical approach Describe anesthesia technique Rather Describe issues with THA and TKA How anesthesia can modify Issues Total Hip Total Knee Blood Loss ++
Anesthesia for Total Hip and Knee Arthroplasty Typical approach Describe anesthesia technique Rather Describe issues with THA and TKA How anesthesia can modify Issues Total Hip Total Knee Blood Loss ++
Delayed Emergence After Craniotomy: No Delays Accepted Rafi Avitsian, M.D. Cleveland Clinic, Cleveland, OH
 Session: L134 Session: L253 Delayed Emergence After Craniotomy: No Delays Accepted Rafi Avitsian, M.D. Cleveland Clinic, Cleveland, OH Disclosures: This presenter has no financial relationships with commercial
Session: L134 Session: L253 Delayed Emergence After Craniotomy: No Delays Accepted Rafi Avitsian, M.D. Cleveland Clinic, Cleveland, OH Disclosures: This presenter has no financial relationships with commercial
Inhalational Anesthesia. Munir Gharaibeh, MD, PhD, MHPE School of Medicine The University of Jordan February, 2018
 Inhalational Anesthesia School of Medicine The University of Jordan February, 2018 mgharaib@ju.edu.jo Inhalational Anesthesia n Gases or volatile liquids n Administration and Elimination is by the lungs
Inhalational Anesthesia School of Medicine The University of Jordan February, 2018 mgharaib@ju.edu.jo Inhalational Anesthesia n Gases or volatile liquids n Administration and Elimination is by the lungs
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery
 Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
"Opium teaches only one thing, which is; that aside from physical suffering there is nothing real." André Malraux MAN'S FATE
 "Opium teaches only one thing, which is; that aside from physical suffering there is nothing real." André Malraux MAN'S FATE Pain Management in the Older Adult 5 TH VITAL SIGN Pain is a common problem
"Opium teaches only one thing, which is; that aside from physical suffering there is nothing real." André Malraux MAN'S FATE Pain Management in the Older Adult 5 TH VITAL SIGN Pain is a common problem
Can Depth of Anesthesia Monitoring Alter the Incidence of Mortality, POCD or Delirium?
 Can Depth of Anesthesia Monitoring Alter the Incidence of Mortality, POCD or Delirium? John C. Drummond, M.D., FRCPC Professor of Anesthesiology, University of California, San Diego; Staff Anesthesiologist,
Can Depth of Anesthesia Monitoring Alter the Incidence of Mortality, POCD or Delirium? John C. Drummond, M.D., FRCPC Professor of Anesthesiology, University of California, San Diego; Staff Anesthesiologist,
Postoperative Delirium and Sleep Apnea
 Postoperative Delirium and Sleep Apnea Sakura Kinjo, MD Clinical Professor Anesthesia Medical Director, Orthopaedic Institute University of California, San Francisco Objectives Discuss possible risk factors
Postoperative Delirium and Sleep Apnea Sakura Kinjo, MD Clinical Professor Anesthesia Medical Director, Orthopaedic Institute University of California, San Francisco Objectives Discuss possible risk factors
Geriatric (Orthopaedic) Trauma
 Trauma") Geriatric (Orthopaedic) Trauma Brian Buck, DO March 3, 2017 31st Annual Geriatric Conference Pearls of Geriatric Care Do not regret growing older. It is a privilege denied to most Overview East Guidelines
Geriatric (Orthopaedic) Trauma Brian Buck, DO March 3, 2017 31st Annual Geriatric Conference Pearls of Geriatric Care Do not regret growing older. It is a privilege denied to most Overview East Guidelines
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Guidelines on the Safe Practice of Acute Pain Management
 Page 1 of 7 Guidelines on the Safe Practice of Acute Pain Version Effective Date 1 1 MAY 1994 (Reviewed Feb 2002) 2 1 DEC 2014 Document No. HKCA P11 v2 Prepared by College Guidelines Committee Endorsed
Page 1 of 7 Guidelines on the Safe Practice of Acute Pain Version Effective Date 1 1 MAY 1994 (Reviewed Feb 2002) 2 1 DEC 2014 Document No. HKCA P11 v2 Prepared by College Guidelines Committee Endorsed
8/26/14. Disclosures. Objectives. None
 Disclosures None Objectives Understand Importance of Pediatric Obesity Impact on Physiology Preoperative Assessment Intra-operative Management PACU & the obese pediatric Patient 1 Gender specific charts
Disclosures None Objectives Understand Importance of Pediatric Obesity Impact on Physiology Preoperative Assessment Intra-operative Management PACU & the obese pediatric Patient 1 Gender specific charts
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Activated partial thromboplastin time abnormality, perioperative approach to, 104 105 Acute kidney injury, perioperative, 89 99 early
Index Note: Page numbers of article titles are in boldface type. A Activated partial thromboplastin time abnormality, perioperative approach to, 104 105 Acute kidney injury, perioperative, 89 99 early
Adolescent Substance Abuse
 Adolescent Substance Abuse WHY IT S A PROBLEM AND WHAT WE NEED TO KNOW AS ANESTHESIA PROVIDERS BRIDGET L. MULDOWNEY MD ASSISTANT PROFESSOR OF ANESTHESIOLOGY UNIVERSITY OF WISCONSIN- SCHOOL OF MEDICINE
Adolescent Substance Abuse WHY IT S A PROBLEM AND WHAT WE NEED TO KNOW AS ANESTHESIA PROVIDERS BRIDGET L. MULDOWNEY MD ASSISTANT PROFESSOR OF ANESTHESIOLOGY UNIVERSITY OF WISCONSIN- SCHOOL OF MEDICINE
POCD: What is it and do the anesthetics play a role?
 POCD: What is it and do the anesthetics play a role? Deborah J. Culley, M.D. Associate Professor Harvard Medical School Brigham & Women s Hospital Conflicts of Interest NIH/NIGMS/NIA ABA: Director ABMS:
POCD: What is it and do the anesthetics play a role? Deborah J. Culley, M.D. Associate Professor Harvard Medical School Brigham & Women s Hospital Conflicts of Interest NIH/NIGMS/NIA ABA: Director ABMS:
Death by Bedrest: The Perils of The Hospital
 Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
The Surgical Patient. Objectives:
 The Surgical Patient Objectives: 1. Discuss the effect of surgery on the body systems. 2. Explain the etiological factors, nursing assessment, and management of potential problems during the postoperative
The Surgical Patient Objectives: 1. Discuss the effect of surgery on the body systems. 2. Explain the etiological factors, nursing assessment, and management of potential problems during the postoperative
Cervical Plating Lumbar Microdiscectomy SCOLIOSIS
 SCOLIOSIS Introduction Scoliosis is the term given to abnormal lateral curvature of the spine when looked from front or back. If diagnosed early then it could be treated conservatively through bracing
SCOLIOSIS Introduction Scoliosis is the term given to abnormal lateral curvature of the spine when looked from front or back. If diagnosed early then it could be treated conservatively through bracing
Cardiovascular Responses to Exercise
 CARDIOVASCULAR PHYSIOLOGY 69 Case 13 Cardiovascular Responses to Exercise Cassandra Farias is a 34-year-old dietician at an academic medical center. She believes in the importance of a healthy lifestyle
CARDIOVASCULAR PHYSIOLOGY 69 Case 13 Cardiovascular Responses to Exercise Cassandra Farias is a 34-year-old dietician at an academic medical center. She believes in the importance of a healthy lifestyle
Obstetrical Anesthesia. Safe Pain Relief for Childbirth
 Obstetrical Anesthesia Safe Pain Relief for Childbirth Introduction Pain relief (analgesia) for labor and delivery is now safer than ever. In the United States approximately two-thirds of all women receive
Obstetrical Anesthesia Safe Pain Relief for Childbirth Introduction Pain relief (analgesia) for labor and delivery is now safer than ever. In the United States approximately two-thirds of all women receive
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Postoperative cognitive dysfunction a neverending story
 Postoperative cognitive dysfunction a neverending story Adela Hilda Onuţu, MD, PhD Cluj-Napoca, Romania adela_hilda@yahoo.com No conflict of interest Contents Postoperative cognitive dysfunction (POCD)
Postoperative cognitive dysfunction a neverending story Adela Hilda Onuţu, MD, PhD Cluj-Napoca, Romania adela_hilda@yahoo.com No conflict of interest Contents Postoperative cognitive dysfunction (POCD)
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
General OR Rotations GOALS & OBJECTIVES
 General OR Rotations GOALS & OBJECTIVES Goals At the end of the CA 1 year General OR rotations, the resident should competently manage uncomplicated ambulatory, orthopedic, maxillo-facial, ENT, gynecologic,
General OR Rotations GOALS & OBJECTIVES Goals At the end of the CA 1 year General OR rotations, the resident should competently manage uncomplicated ambulatory, orthopedic, maxillo-facial, ENT, gynecologic,
Perioperative Fluid Management in ERPs
 Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Care for patients with Neurological disorders
 King Saud University College of Nursing Medical Surgical Department Application of Adult Health Nursing Skills ( NUR 317 ) Care for patients with Neurological disorders Outline; EEG Overview. Nursing Interventions;
King Saud University College of Nursing Medical Surgical Department Application of Adult Health Nursing Skills ( NUR 317 ) Care for patients with Neurological disorders Outline; EEG Overview. Nursing Interventions;
Innovative Approaches and New Technology to Gain Access
 Innovative Approaches and New Technology to Gain Access The following is intended only for presentation to the Reimbursement and Access 2017 audience, August 17, 2017. This information is not for promotional
Innovative Approaches and New Technology to Gain Access The following is intended only for presentation to the Reimbursement and Access 2017 audience, August 17, 2017. This information is not for promotional
Peri-Operative Management: Guidelines for Inpatient Management of Children with Sickle Cell Disease
 Version 02 Approved by Interprofessional Patient Care Committee: September 16, 2016 1.0 Background Children with Sickle Cell are at risk of developing post-operative Acute Chest Syndrome. With improvements
Version 02 Approved by Interprofessional Patient Care Committee: September 16, 2016 1.0 Background Children with Sickle Cell are at risk of developing post-operative Acute Chest Syndrome. With improvements
Preoperative Pulmonary Evaluation. Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine
 Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
May 2013 Anesthetics SLOs Page 1 of 5
 May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
Cancer in the United States
 https://www.cancer.gov/aboutcancer/understanding/statistics https://www.cancer.gov/aboutcancer/understanding/statistics 09/05/2018 Anesthesia for Cancer Surgery: How we can impact survival Paul G. Tarasi
https://www.cancer.gov/aboutcancer/understanding/statistics https://www.cancer.gov/aboutcancer/understanding/statistics 09/05/2018 Anesthesia for Cancer Surgery: How we can impact survival Paul G. Tarasi
Milestone Guide. CBD Anesthesia
 Table of Contents Department of Anesthesiology Foundations 1 Airway 1 Pharmacology 1 Physiology 1 Common Uncomplicated Anesthetics Practice 2 Obstetrics 2 Pain 2 Core 3 Perioperative Medicine 3 Complex
Table of Contents Department of Anesthesiology Foundations 1 Airway 1 Pharmacology 1 Physiology 1 Common Uncomplicated Anesthetics Practice 2 Obstetrics 2 Pain 2 Core 3 Perioperative Medicine 3 Complex
Current evidence in acute pain management. Jeremy Cashman
 Current evidence in acute pain management Jeremy Cashman Optimal analgesia Best possible pain relief Lowest incidence of side effects Optimal analgesia Best possible pain relief Lowest incidence of side
Current evidence in acute pain management Jeremy Cashman Optimal analgesia Best possible pain relief Lowest incidence of side effects Optimal analgesia Best possible pain relief Lowest incidence of side
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
Anesthesia for Cardiac Patients for Non Cardiac Surgery. Kimberly Westra DNP, MSN, CRNA
 Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Enhanced Perioperative Management of Older Adults
 Enhanced Perioperative Management of Older Adults Bernardo Reyes, MD Assistant Professor of Geriatrics Charles E. Schmidt College of Medicine Disclosures None Interesting Facts Warhol was a sickly child,
Enhanced Perioperative Management of Older Adults Bernardo Reyes, MD Assistant Professor of Geriatrics Charles E. Schmidt College of Medicine Disclosures None Interesting Facts Warhol was a sickly child,
Perioperative Pain Management
 Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Geriatric Emergencies. Lesson Goal. Lesson Objectives 9/10/2012. Introduce ways geriatric patients differ from other patients
 Geriatric Emergencies Lesson Goal Introduce ways geriatric patients differ from other patients Physiologic changes of aging Communication issues Effects of medications Common fears of elderly patients
Geriatric Emergencies Lesson Goal Introduce ways geriatric patients differ from other patients Physiologic changes of aging Communication issues Effects of medications Common fears of elderly patients
MEDICAL ADVISORY COUNCIL Position Statement PREHOSPITAL PAIN MANAGEMENT
 MEDICAL ADVISORY COUNCIL Position Statement PREHOSPITAL PAIN MANAGEMENT MAC PS 2013-002 Appropriate treatment of acute pain in the prehospital arena offers an opportunity to positively impact many patients.
MEDICAL ADVISORY COUNCIL Position Statement PREHOSPITAL PAIN MANAGEMENT MAC PS 2013-002 Appropriate treatment of acute pain in the prehospital arena offers an opportunity to positively impact many patients.
University of Groningen. Acute kidney injury after cardiac surgery Loef, Berthus Gerard
 University of Groningen Acute kidney injury after cardiac surgery Loef, Berthus Gerard IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
University of Groningen Acute kidney injury after cardiac surgery Loef, Berthus Gerard IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
Pain Management in Older Adults. Mary Shelkey, PhD, ARNP
 Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Trauma resuscitation in the Elderlyfrom a physiological perspective
 6 November 2017 Trauma resuscitation in the Elderlyfrom a physiological perspective Joseph Mathew Consultant, Emergency/ 6 November 2017 2 http://www.who.int/ageing/publications/global_health.pdf 6 November
6 November 2017 Trauma resuscitation in the Elderlyfrom a physiological perspective Joseph Mathew Consultant, Emergency/ 6 November 2017 2 http://www.who.int/ageing/publications/global_health.pdf 6 November
Prevention and Treatment Patrick Levelle, MD
 Prevention and Treatment Patrick Levelle, MD LOCAL ANESTHETIC TOXICITY 1. PERIPHERAL NERVE BLOCKS 2. ROLE OF THE PERIANESTHESIA RN 3. LOCAL ANESTHETIC TOXICITY Use of Lipid Emulsion Regional and Peripheral
Prevention and Treatment Patrick Levelle, MD LOCAL ANESTHETIC TOXICITY 1. PERIPHERAL NERVE BLOCKS 2. ROLE OF THE PERIANESTHESIA RN 3. LOCAL ANESTHETIC TOXICITY Use of Lipid Emulsion Regional and Peripheral
CHAPTER 9. Shock National Safety Council
 CHAPTER 9 Shock Shock Dangerous condition: Not enough oxygen-rich blood reaching vital organs, such as brain and heart Caused by anything that significantly reduces blood flow Life-threatening emergency
CHAPTER 9 Shock Shock Dangerous condition: Not enough oxygen-rich blood reaching vital organs, such as brain and heart Caused by anything that significantly reduces blood flow Life-threatening emergency
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
INTRAVENOUS LIDOCAINE INFUSIONS AND INTRALIPID RESCUE
 INTRAVENOUS LIDOCAINE INFUSIONS AND INTRALIPID RESCUE Acute Pain Service-LHSC VH and UH sites HISTORY Lidocaine and procaine used by IV infusion in the 1950s and 1960s for general analgesia Often continued
INTRAVENOUS LIDOCAINE INFUSIONS AND INTRALIPID RESCUE Acute Pain Service-LHSC VH and UH sites HISTORY Lidocaine and procaine used by IV infusion in the 1950s and 1960s for general analgesia Often continued
Overview. Physiology of Heat Stress Causal factors Heat Disorders & Health Effects Control
 Overview Physiology of Heat Stress Causal factors Heat Disorders & Health Effects Control 1 Causal Factors Age, weight, degree of physical fitness Degree of acclimatization, metabolism Intercurrent illnesses
Overview Physiology of Heat Stress Causal factors Heat Disorders & Health Effects Control 1 Causal Factors Age, weight, degree of physical fitness Degree of acclimatization, metabolism Intercurrent illnesses
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis