Do Prognostic Models Matter in Neurocritical Care?
|
|
|
- Cory Sharp
- 6 years ago
- Views:
Transcription

1 Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical Care Medicine Université Laval Quebec City, Quebec, Canada Scientific Director Cochrane Canada Francophone Deputy Director Population Health and Optimal Health Practices Unit, CHU de Quebec Université Laval Research Centre Canada Critical Care Forum November 2, 2016



2 Disclosures 2
3 Objectives Discuss the importance of neuroprognostication and prognostic models in critically ill TBI patients Discuss some of the gaps in the current knowledge Present Canadian data on prognosis, withdrawal of life-sustaining therapies (WLST) and outcomes in critically ill TBI patients 3
4 What do you think this patient s prognosis will be at one year? One week ago, you admitted a previously healthy 26 year-old man with severe TBI after a MVC. The patient was intubated at the scene and immediately transferred to the ED of your hospital. After adequate stabilization, his GCS is 6 (eye = 2, verbal = 1, motor = 3). Pupils are sluggish but equal and reactive. A head CT scan performed on arrival reveals diffuse edema. The patient has no other injuries. An intracranial monitor was installed and the ICP was 15 mmhg. The patient was not intoxicated and remained hemodynamically stable, as well as with an ICP below 20 mmhg during his ICU stay. A repeat CT scan showed diffuse edema with no sign of herniation. The family is very concerned about long-term neurological deficits and requests more information on prognosis from you. Based on the GOSe, what do you think his prognosis will be at one year? 4
5 Is TBI really a problem? 60% of all trauma cases are associated with a traumatic brain injury Main cause of death Main cause of permanent impairment Most healthcare resource utilization Altered quality of life 5
6 Why are neuroprognostication and prognostic models so important? High incidence of withdrawal of life-sustaining therapies O Callahan et al. Crit Care Med 1995 Rocker et al. Can J Anesth 2006 Appropriate decisions? Mayer et al. Neurol 1999 Becker et al. Neurol 2001 New programs of organ donation following cardiocirculatory arrest 6

7 Public awareness 7
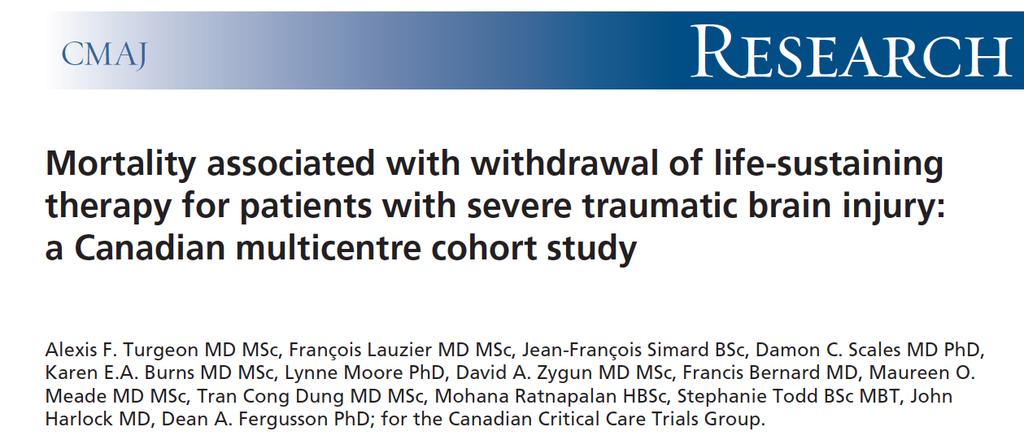

8 CMAJ

9 Hospital mortality 9

10 Hospital mortality following WLST 10
11 11
12 Could differences in the management of patients be responsible for such results? Maas et al. J Neurotrauma
13 What can explain these variations in mortality? Differences in mortality between centres may be partly due to variation in physicians perceptions of long-term prognosis and physicians' practice patterns for recommending WLST 13
14 Clinical scenario One week ago, you admitted a previously healthy 26 year-old man with severe TBI after a MVC. The patient was intubated at the scene and immediately transferred to the ED of your hospital. After adequate stabilization, his GCS is 6 (eye = 2, verbal = 1, motor = 3). Pupils are sluggish but equal and reactive. A head CT scan performed on arrival reveals diffuse edema. The patient has no other injuries. An intracranial monitor was installed and the ICP was 15 mmhg. The patient was not intoxicated and remained hemodynamically stable, as well as with an ICP below 20 mmhg during his ICU stay. A repeat CT scan showed diffuse edema with no sign of herniation. Based on the GOSe, what do you think his prognosis will be at one year? 1) favourable (GOSe 5-8) lower moderate disability, upper moderate disability, lower good recovery, upper good recovery 2) neutral on the matter 3) unfavourable (GOSe 1-4) death, vegetative state, lower severe disability, upper severe disability 14



15 Turgeon et al. Crit Care Med 2013 Targeted population Canadian Intensivists, Neurosurgeons an Neurologists caring for TBI Identified through Trauma Coordinators of each Level 1 Trauma centers all across Canada Questionnaire validated in multiple steps Sensibility testing Face validity, content validity, test-retest reliability, feasibility, ease of administration Web and regular mail-based survey Response rate 64% (455/712) 15
16 How can we better assess prognosis? Many known/potential predictive factors of prognosis Event-related characteristics Patients characteristics Clinical exam Radiological imaging Electrophysiological tests Tissue biomarkers 16
17 Percentages of respondents When evaluating neurological PROGNOSIS in patients with SEVERE TRAUMATIC BRAIN INJURY, HOW USEFUL do you consider the followings and HOW FREQUENTLY do you use them? 100% Monitoring Clinical Exam Imaging Neuro Tests Biomarkers 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Probably or definitely useful Often or always use Vital signs ICP CPP SjO2 pbto2 (LycoxTM) Pupillary reaction to light Corneal reflex Motor response GCS Spontaneous breathing effort CT scan CT-Angio MRI PET scan and/or SPECT EEG (Intermittent measures) EEG (Continuous measure) SSEP BSAEP micro-dialysis Biological markers Turgeon et al. Crit Care Med
18 What factors may be associated with prognosis? Event-related characteristics Transfer time Cardiorespiratory arrest Patients characteristics Age Co-morbidities Clinical exam Level of consciousness following stabilization GCS Motor score Pupillary reactivity Episodes of hypotension Episodes of hypoxemia Clinical measures Increased ICP Decreased brain tissue oxygenation 18
19 What factors may be associated with prognosis? Radiological imaging CT scan MRI Electrophysiological tests EEG SSEP Tissue biomarkers Serum CSF 19
20 Brain oxygen monitoring PbtO 2 Value < 15 mmhg associated with unfavourable outcome Valadka et al Bullock et al. J Neurotrauma 2007 Nangunoori et al. Neuro Crit Care 2011 Brain oxygen saturation NIRS Limited data available and reliability/validity 20
21 Neuroimaging-CT CT scan Type of lesion intra-parenchymal hematoma > sub-dural > epidural Basal cistern Compression or absence (OR 2.45 [ ]) Medial shift > 5 mm (OR 2.2 [ ]) Sub-arachnoid hemorrhage Extended t-sah (OR 2.64 [ ]) Marshall score Score III and IV (OR 2.5, OR 3.0) Unfavourable prognosis at 6 months (GOS 1-3) Marshall et al. J Neurosurg 1991 Rovlias et al. J Neurotrauma 2004 Mass et al. (IMPACT)J Neurotrauma
22 Neuroimaging-MRI Magnetic Resonance Imaging SWI susceptibility weighted imaging Lesions Corpus callosum Mesencephalon Basal ganglia 40 studies (the largest with ~100 patients) Mainly 1.5 Tesla MRI Variable periods following admission 7 to 21 days Wedekind et al. J Trauma 1999 Mannion et al. J Neurotrauma 2007 Weiss et al. J Neurol
23 Neuroimaging-MRI Diffusion Tensor Imaging (DTI) MRI MRI-spectroscopy Functional MRI (fmri) Limited access and few data to support its clinical use Tollard et al. Crit Care Med
 Robinson et al. Crit Care Med 2003 www.ulaval.ca 24")
24 Electrophysiological tests-ssep SomatoSensory Evoked Potentials Systematic review Observational studies SSEP - coma - prognosis Median nerve, N20 > 4 patients/study 41 studies 14 studies only on TBI (adults/teenagers) Robinson et al. Crit Care Med
25 Electrophysiological tests-ssep Robinson et al. Crit Care Med 2003 Robinson et al. Crit Care Med

 www.")
26 Single center prospective study (n=81) Median nerve SSEP day 1, 3 and 7 6-point scoring system Houlden et al. Crit Care Med 2010 One-year outcome (GOS, Barthel, Rivermead, General health questionnaire, attention) 26
27 Electrophysiological tests-eeg Electroencephalogram Continuous EEG Absence of variability (alpha) Mean 3 day PAV GOS 1-3 at 6 months Gutling et al. Neurol 1995 Vespa et al. J Neurosurg 2002 Hebb et al. J Neurotrauma 2007 Nenadovic et al. J Neurotrauma
28 Tissue biomarkers Many serum proteins identified S100-ß Neuron Specific Enolase (NSE) GFAP UCH-L1 > 100 small cohort studies Association observed Unknown thresholds for clinical significance Mussack et al. Crit Care Med 2002 Woertgen et al. Brain Inj 2002 Stalnacke et al. J Rehab Med 2005 Haqqani et al. J Neurotrauma 2007 Korfias et al. Int Care Med

29 Mercier et al. BMJ
30 Other tissue biomarkers Brain microdialysis Lactate/pyruvate ratio > 25 Glucose, glycerol, glutamate ph Unfavourable prognosis at 6 months (GOS 1-3) Few data from small cohort studies Stahl et al. Anesth Scand 2001 Clauen et al. J Neurosurg 2005 Karathanou et al. Crit Care 2006 Karathanou et al. J Neurosurg Sc 2011 Timofeev et al. J Cerebral Blood flow met
31 Which factors are the most important ones for prognostic evaluation? 1. Age 2. GCS motor score 3. Pupillary response to light Murray et al. J Neurotrauma Lesion compatible with DAI Lesions in the white matter Brain stem Hemisphere Corpus callosum 31
32 How can we determine prognosis? Many known/potential predictive factors of prognosis Event-related characteristics Patients characteristics Clinical exam Radiological imaging Electrophysiological tests Biological markers None of these predictive factors contains sufficient prognostic information for clinical decision making 32
33 Systematic reviews of prognostic models Three systematic reviews Multiple methodological flaws Single center studies Retrospective Limited number of predictors Bias by indication (tests) None of the models can be used in clinical practice Perel et al 2006, Turgeon et al. 2007, Mushkudiani et al
34 Two recent prognostic models using large databases CRASH database Data from the CRASH RCT on steroids in moderate and severe TBI N=1008 patients Validation in IMPACT database IMPACT database Perel et al. BMJ 2008 Database from Phase III neuroprotection trials N=9205 patients Validation in CRASH database Steyerberg et al. Plos


35 Most recent models 35 Steyenberg et al. PlosMed 2008 CRASH study investigators. BMJ 2008
36 Most recent models Excellent for baseline risk assessment Improve trial design and risk adjustment Clinical audit Certainly not optimal for clinical decisionmaking Mainly derived from admission data Do not consider secondary cerebral injury Do not consider most prognostic tests used Limited ability for accurate prognostic assessment 36

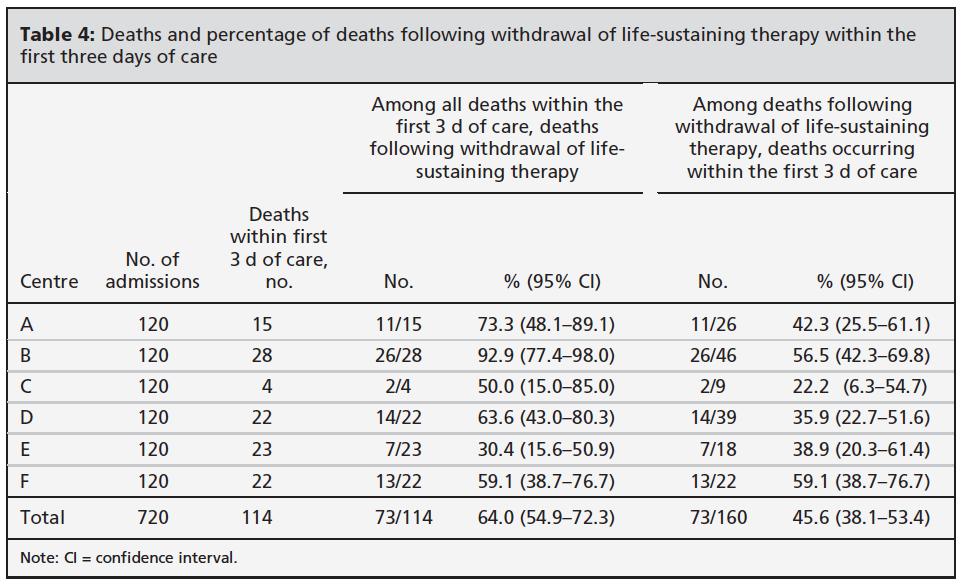
37 TBI-Prognosis Program of Research 37

38 TBI-Prognosis Study schematic
39 What can we say about prognosis then? No perfect test, no perfect model Major improvement over the last decade Multimodal approach required Perfect determination of long-term prognosis is not possible However, better prognostic information through prognostic models is required for both clinicians and families in order to give the most appropriate cares in a predominantly young healthy population 39
40 We must go beyond opinion-based medicine One week ago, you admitted a previously healthy 26 year-old man with severe TBI after a MVC. The patient was intubated at the scene and immediately transferred to the ED of your hospital. After adequate stabilization, his GCS is 6 (eye = 2, verbal = 1, motor = 3). Pupils are sluggish but equal and reactive. A head CT scan performed on arrival reveals diffuse edema. The patient has no other injuries. An intracranial monitor was installed and the ICP was 15 mmhg. The patient was not intoxicated and remained hemodynamically stable, as well as with an ICP below 20 mmhg during his ICU stay. A repeat CT scan showed diffuse edema with no sign of herniation. The family is very concerned about long-term neurological deficits and requests more information on prognosis from you. Based on the GOSe, what do you think his prognosis will be at one year? 40
41 What is the role of prognostic models then? Provide prognostic information as objective as possible Balance prognosis and patient s wishes Obtain informed consent for care Decision for agressive care require the same consent as for the limitation of care Concept often mistaken 41
42
How should clinical trials in brain injury be designed
 How should clinical trials in brain injury be designed Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
How should clinical trials in brain injury be designed Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
Multimodal monitoring to individualize care in TBI
 Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN (865) LABEL
 LABEL") 1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS
 GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
Neuroprognostication after cardiac arrest
 Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
Changing Demographics in Death After Devastating Brain Injury
 Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Neurological Prognosis after Cardiac Arrest Guideline
 Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
THREE HUNDRED AND ten TBI patients with a
 Acute Medicine & Surgery 2014; 1: 31 36 doi: 10.1002/ams2.5 Original Article Outcome prediction model for severe traumatic brain injury Jiro Iba, 1 Osamu Tasaki, 2 Tomohito Hirao, 2 Tomoyoshi Mohri, 3
Acute Medicine & Surgery 2014; 1: 31 36 doi: 10.1002/ams2.5 Original Article Outcome prediction model for severe traumatic brain injury Jiro Iba, 1 Osamu Tasaki, 2 Tomohito Hirao, 2 Tomoyoshi Mohri, 3
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Deceased Organ Donation Requires Timely Not Early Referral To An Organ Donation Organization
 Deceased Organ Donation Requires Timely Not Early Referral To An Organ Donation Organization Andreas H. Kramer MD MSc FRCPC Clinical Associate Professor Departments of Critical Care Medicine & Clinical
Deceased Organ Donation Requires Timely Not Early Referral To An Organ Donation Organization Andreas H. Kramer MD MSc FRCPC Clinical Associate Professor Departments of Critical Care Medicine & Clinical
Ancillary Testing in Death
 Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN
 Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
FORENSIC SCIENCE NEWSLETTER Forensic Pathology and Neuropathology. William A. Cox, M.D., FCAP.
 NEUROPATHOLOGY FORENSIC SCIENCE NEWSLETTER Forensic Pathology and Neuropathology William A. Cox, M.D., FCAP www.forensicjournals.cm May 15, 2016 This issue of the Forensic Science Newsletter will address
NEUROPATHOLOGY FORENSIC SCIENCE NEWSLETTER Forensic Pathology and Neuropathology William A. Cox, M.D., FCAP www.forensicjournals.cm May 15, 2016 This issue of the Forensic Science Newsletter will address
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Positron Emission Tomography Imaging in Brain Injured Patients
 Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines
 TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines DATE: 11 April 2014 CONTEXT AND POLICY ISSUES Traumatic brain
TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines DATE: 11 April 2014 CONTEXT AND POLICY ISSUES Traumatic brain
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Outcomes after severe traumatic brain injury (TBI)
") CLINICAL ARTICLE J Neurosurg 129:234 240, 2018 Clinical characteristics and temporal profile of recovery in patients with favorable outcomes at 6 months after severe traumatic brain injury Aditya Vedantam,
CLINICAL ARTICLE J Neurosurg 129:234 240, 2018 Clinical characteristics and temporal profile of recovery in patients with favorable outcomes at 6 months after severe traumatic brain injury Aditya Vedantam,
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
9/16/2018. Recognizing & Managing Seizures in Pediatric TBI. Objectives. Definitions and Epidemiology
 Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Mild TBI (Concussion) Not Just Less Severe But Different
 Not Just Less Severe But Different") Mild TBI (Concussion) Not Just Less Severe But Different Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Mild TBI (Concussion) Not Just Less Severe But Different Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Use of CT in minor traumatic brain injury. Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD
 Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
PSEUDO-SUBARACHNOID HEMORRHAGE AFTER INADVERTENT DURAL PUNCTURE DURING CERVICAL EPIDURAL STEROID INJECTION
 PSEUDO-SUBARACHNOID HEMORRHAGE AFTER INADVERTENT DURAL PUNCTURE DURING CERVICAL EPIDURAL STEROID INJECTION HAI NGUYEN, DO, MPH Anesthesiology Resident (University of Kansas Wichita) JOEL CAVAZOS, MD Pain
PSEUDO-SUBARACHNOID HEMORRHAGE AFTER INADVERTENT DURAL PUNCTURE DURING CERVICAL EPIDURAL STEROID INJECTION HAI NGUYEN, DO, MPH Anesthesiology Resident (University of Kansas Wichita) JOEL CAVAZOS, MD Pain
Serum biomarkers for predicting outcome after TBI
 Józef Opara, Andrzej Małecki, Elżbieta Małecka Serum biomarkers for predicting outcome after TBI Jerzy Kukuczka Academy of Physical Education in Katowice TBI biomarkers A biomarker, or biological marker,
Józef Opara, Andrzej Małecki, Elżbieta Małecka Serum biomarkers for predicting outcome after TBI Jerzy Kukuczka Academy of Physical Education in Katowice TBI biomarkers A biomarker, or biological marker,
What is elevated ICP?
 What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
SPECIALIZED UNITS: DO THEY SAVE LIVES? NEUROCRITICAL CARE
 SPECIALIZED UNITS: DO THEY SAVE LIVES? NEUROCRITICAL CARE David Zygun MD MSc FRCPC Zone Clinical Department Head Critical Care Medicine, Edmonton Zone Professor and Director Division of Critical Care Medicine
SPECIALIZED UNITS: DO THEY SAVE LIVES? NEUROCRITICAL CARE David Zygun MD MSc FRCPC Zone Clinical Department Head Critical Care Medicine, Edmonton Zone Professor and Director Division of Critical Care Medicine
BMJ Open. For peer review only - Journal: BMJ Open. Manuscript ID bmjopen
 Feasibility of a prospective multi-center prognostication study in critically ill patients with severe traumatic brain injury: The TBI-Prognosis pilot study Journal: Manuscript ID bmjopen-0-0 Article Type:
Feasibility of a prospective multi-center prognostication study in critically ill patients with severe traumatic brain injury: The TBI-Prognosis pilot study Journal: Manuscript ID bmjopen-0-0 Article Type:
ALS 713: Prognostication in Normothermia
 ALS 713: Prognostication in Normothermia TFQO: Clifton Callaway (COI #214) EVREVs: Claudio Sandroni (COI #134); Tobias Cronberg (COI #35) Taskforce: ALS COI Disclosure (specific to this systematic review)
ALS 713: Prognostication in Normothermia TFQO: Clifton Callaway (COI #214) EVREVs: Claudio Sandroni (COI #134); Tobias Cronberg (COI #35) Taskforce: ALS COI Disclosure (specific to this systematic review)
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL
 HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL Gaylan Rockswold, MD, PhD, Principal Investigator William Barsan, MD, Principal Investigator, CCC, SIREN Byron
HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL Gaylan Rockswold, MD, PhD, Principal Investigator William Barsan, MD, Principal Investigator, CCC, SIREN Byron
A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary Hospital of South India
 International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
PREDICTION OF PROGNOSIS IN PATIENTS OF DIFFUSE BRAIN INJURY USING PROGNOSTIC PREDICTIVE MODEL DEVELOPED BY NIMHANS
 PREDICTION OF PROGNOSIS IN PATIENTS OF DIFFUSE BRAIN INJURY USING PROGNOSTIC PREDICTIVE MODEL DEVELOPED BY NIMHANS Devendra Singh Dhaker, Yogendra Singh Bhakuni, Ashish Kumar Dwivedi, A. K. Chaurasia,
PREDICTION OF PROGNOSIS IN PATIENTS OF DIFFUSE BRAIN INJURY USING PROGNOSTIC PREDICTIVE MODEL DEVELOPED BY NIMHANS Devendra Singh Dhaker, Yogendra Singh Bhakuni, Ashish Kumar Dwivedi, A. K. Chaurasia,
Congenital Heart Disease and Critical Neurological Injury: Do Our Patients Belong in a Neurocritical Care Unit?
 Congenital Heart Disease and Critical Neurological Injury: Do Our Patients Belong in a Neurocritical Care Unit? Shriprasad R Deshpande, MBBS MS Assistant Professor of Pediatrics Medical Director, Mechanical
Congenital Heart Disease and Critical Neurological Injury: Do Our Patients Belong in a Neurocritical Care Unit? Shriprasad R Deshpande, MBBS MS Assistant Professor of Pediatrics Medical Director, Mechanical
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center
 Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center Financial Disclosure None 1 Introduction Each year, 356,000 Americans are treated by EMS
Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center Financial Disclosure None 1 Introduction Each year, 356,000 Americans are treated by EMS
1st Turku Traumatic Brain Injury Symposium Turku, Finland, January 2014
 The TBIcare decision support tool aid for the clinician Jyrki Lötjönen & Jussi Mattila, VTT Technical Research Centre of Finland Validation of the decision support tool Ari Katila University of Turku 1st
The TBIcare decision support tool aid for the clinician Jyrki Lötjönen & Jussi Mattila, VTT Technical Research Centre of Finland Validation of the decision support tool Ari Katila University of Turku 1st
Multimodal monitoring to prognosticate in anoxic brain injury
 Multimodal monitoring to prognosticate in anoxic brain injury Eyal Golan, MD FRCPC PhD(c) Critical Care & Neurosciences Critical Care Medicine Interdepartmental Division of Critical Care and Department
Multimodal monitoring to prognosticate in anoxic brain injury Eyal Golan, MD FRCPC PhD(c) Critical Care & Neurosciences Critical Care Medicine Interdepartmental Division of Critical Care and Department
Extubation Failure & Delay in Brain-Injured Patients
 Extubation Failure & Delay in Brain-Injured Patients Niall D. Ferguson, MD, FRCPC, MSc Director, Critical Care Medicine University Health Network & Mount Sinai Hospital Associate Professor of Medicine
Extubation Failure & Delay in Brain-Injured Patients Niall D. Ferguson, MD, FRCPC, MSc Director, Critical Care Medicine University Health Network & Mount Sinai Hospital Associate Professor of Medicine
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Prognostic indicators of childhood acute viral encephalitis
 ecommons@aku Community Health Sciences Department of Community Health Sciences December 1999 Prognostic indicators of childhood acute viral encephalitis E Bhutto Aga Khan University M Naim Aga Khan University
ecommons@aku Community Health Sciences Department of Community Health Sciences December 1999 Prognostic indicators of childhood acute viral encephalitis E Bhutto Aga Khan University M Naim Aga Khan University
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
INDEX&NEUROTRAUMA&(INCLUDING&SPINAL&CORD&INJURIES)&!!
&!!") 1 INDEX&NEUROTRAUMA&(INCLUDING&SPINAL&CORD&INJURIES)& Prehospital,care,in,patients,with,severe,traumatic,brain,injury:,does,the,level,of,prehospital, care,influence,mortality?,...,3 Contralateral,extraaxial,hematomas,after,urgent,neurosurgery,of,a,mass,lesion,in,patients,
1 INDEX&NEUROTRAUMA&(INCLUDING&SPINAL&CORD&INJURIES)& Prehospital,care,in,patients,with,severe,traumatic,brain,injury:,does,the,level,of,prehospital, care,influence,mortality?,...,3 Contralateral,extraaxial,hematomas,after,urgent,neurosurgery,of,a,mass,lesion,in,patients,
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017
 Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017 Peter E. Ricci, M.D. Staff Neuroradiologist Radiology Imaging Associates OBJECTIVES 1. Understand
Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017 Peter E. Ricci, M.D. Staff Neuroradiologist Radiology Imaging Associates OBJECTIVES 1. Understand
Imaging Biomarkers Significance S100B NSE. Admitted within 6 hours of injury and CT scan occurred after initial examination. N = 1,064 CT+ N = 50 4.
 Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators Supplemental Content 7 Evidence Table. Included Studies For Key Question 4 Imaging and Biomarker Publications Medium Potential for
Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators Supplemental Content 7 Evidence Table. Included Studies For Key Question 4 Imaging and Biomarker Publications Medium Potential for
Head Injury: Classification Most Severe to Least Severe
 Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Therapeutic Hypothermia
 Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
ICP (Intracranial Pressure) Monitoring Brain Tissue Oxygen Monitoring Jugular Venous Bulb Oximetry
 Monitoring Brain Tissue Oxygen Monitoring Jugular Venous Bulb Oximetry") ICP (Intracranial Pressure) Monitoring Secondary brain injury may be a direct consequence of intracranial hypertension. Therefore monitoring of ICP and cerebral perfusion pressure (CPP) are immediate priority
ICP (Intracranial Pressure) Monitoring Secondary brain injury may be a direct consequence of intracranial hypertension. Therefore monitoring of ICP and cerebral perfusion pressure (CPP) are immediate priority
Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality
 Original articles Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality J. A. MYBURGH*, S. B. LEWIS *Intensive Care Unit, Royal Adelaide Hospital, Adelaide, SOUTH
Original articles Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality J. A. MYBURGH*, S. B. LEWIS *Intensive Care Unit, Royal Adelaide Hospital, Adelaide, SOUTH
SUPPLEMENTARY FIG. S2. (A) Risk of bias and applicability concerns graph by marker. Review authors judgments about each domain presented as
 Risk of bias and applicability concerns graph by marker. Review authors judgments about each domain presented as") Supplementary Data SUPPLEMENTARY FIG. S1. Graphical depiction of (A) influence and (B) outlier detection analyses of S100 calcium binding protein B (S100B) 0.10 0.11lg/L cutoff value studies. (C) Summary
Supplementary Data SUPPLEMENTARY FIG. S1. Graphical depiction of (A) influence and (B) outlier detection analyses of S100 calcium binding protein B (S100B) 0.10 0.11lg/L cutoff value studies. (C) Summary
N E W T O N. Hänggi D, Etminan N, Macdonald RL, Steiger HJ, Mayer SA, Aldrich F, Diringer MN, Hoh BJ, Mocco J, Strange P, Faleck HJ, Miller M
 N E W T O N Nimodipine microparticles to Enhance recovery While reducing TOxicity after subarachnoid hemorrhage Phase 1/2a Multicenter, Controlled, Randomized, Open Label, Dose Escalation, Safety, Tolerability,
N E W T O N Nimodipine microparticles to Enhance recovery While reducing TOxicity after subarachnoid hemorrhage Phase 1/2a Multicenter, Controlled, Randomized, Open Label, Dose Escalation, Safety, Tolerability,
11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome?
 11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome? Critical levels of CPP, ICP and PRx Percentage of patients in outcome
11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome? Critical levels of CPP, ICP and PRx Percentage of patients in outcome
Post-resuscitation care for adults. Jerry Nolan Royal United Hospital Bath
 Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
Report of the Welsh Neuroscience External Expert Review Group. All Wales Recommendations
 Report of the Welsh Neuroscience External Expert Review Group All Wales Recommendations Main Recommendations 1. The workforce delivering all aspects of care to people with acute and long term neurological
Report of the Welsh Neuroscience External Expert Review Group All Wales Recommendations Main Recommendations 1. The workforce delivering all aspects of care to people with acute and long term neurological
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
Med 536 Communicating About Prognosis Workshop. Case 2
 Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Neurological examination of the neurosurgical patient. Dániel Bereczki SU Department of Neurology
 Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES
 PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
APP Placement of ICP Monitors. Sanjay Patra, MD
 APP Placement of ICP Monitors Sanjay Patra, MD Can midlevel providers place external ventricular drains safely and accurately? Sanjay Patra MD MSc Director Epilepsy Surgery Director Brain Trauma Spectrum
APP Placement of ICP Monitors Sanjay Patra, MD Can midlevel providers place external ventricular drains safely and accurately? Sanjay Patra MD MSc Director Epilepsy Surgery Director Brain Trauma Spectrum
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision
 Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
PEDIATRIC MILD TRAUMATIC HEAD INJURY
 PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
Pituitary Complications in Traumatic Brain Injury
 Pituitary Complications in Traumatic Brain Injury François Lauzier, MD, MSc, FRCPC Assistant Professor Division of Critical Care Medicine Department of Anesthesiology and Critical Care Medicine Department
Pituitary Complications in Traumatic Brain Injury François Lauzier, MD, MSc, FRCPC Assistant Professor Division of Critical Care Medicine Department of Anesthesiology and Critical Care Medicine Department
Optimum sodium levels in children with brain injury. Professor Sunit Singhi, Head, Department of Pediatrics, Head, Pediatric
 India Optimum sodium levels in children with brain injury Professor Sunit Singhi, Head, Department of Pediatrics, Head, Pediatric Sodium and brain Sodium - the major extracellular cation and most important
India Optimum sodium levels in children with brain injury Professor Sunit Singhi, Head, Department of Pediatrics, Head, Pediatric Sodium and brain Sodium - the major extracellular cation and most important
Continuous cerebral autoregulation monitoring
 Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Instructional Course #34. Review of Neuropharmacology in Pediatric Brain Injury. John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD
 Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
Surgical Management & Clinical Outcome of Severe Brain Trauma due to Acute Subdural Hematoma.
 International Journal of Sciences: Basic and Applied Research (IJSBAR) ISSN 2307-4531 (Print & Online) http://gssrr.org/index.php?journal=journalofbasicandapplied ----------------------------------------------------------------------------------------------------------------
International Journal of Sciences: Basic and Applied Research (IJSBAR) ISSN 2307-4531 (Print & Online) http://gssrr.org/index.php?journal=journalofbasicandapplied ----------------------------------------------------------------------------------------------------------------
Comparison of outcome of etiological factors for non-traumatic coma in geriatric population in India
 Original article: Comparison of outcome of etiological factors for non-traumatic coma in geriatric population in India 1 DrAmit Suresh Bhate, 2 DrSatishNirhale, 3 DrPrajwalRao, 4 DrShubangi A Kanitkar
Original article: Comparison of outcome of etiological factors for non-traumatic coma in geriatric population in India 1 DrAmit Suresh Bhate, 2 DrSatishNirhale, 3 DrPrajwalRao, 4 DrShubangi A Kanitkar
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Outcome of severe traumatic brain injury at a critical care unit: a review of 87 patients
 Original Article Outcome of severe traumatic brain injury at a critical care unit: a review of 87 patients E.A. Opondo, MBChB, MMed (Surg), General surgeon, North Kinangop Mission Hospital, Surgery Department
Original Article Outcome of severe traumatic brain injury at a critical care unit: a review of 87 patients E.A. Opondo, MBChB, MMed (Surg), General surgeon, North Kinangop Mission Hospital, Surgery Department
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Cosa chiedo alla PtO 2
 Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Traumatic Brain Injury (1.2.3) Management of severe TBI ( ) Learning Objectives
 Management of severe TBI ( ) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management