Aged Care and Health Services Research. A/Prof Kwang Lim Sep 2016
|
|
|
- Clement Parks
- 6 years ago
- Views:
Transcription
1 Aged Care and Health Services Research A/Prof Kwang Lim Sep 2016
2 Accumulating evidence 20% of health care interventions is based on hard evidence. Feasibility of doing randomised controlled trials on all interventions. Translating Practice into Research Merging service requirements and outcome evaluation.
3 Why aged care? Demographics Population aged 65 years or more, Australia - At 30 June Population change
4 Focus: hospital based interventions Using service delivery to enhance outcomes: Delivering interventions during hospitalisation Post Acute Care Preadmission
5 Orthogeriatrics Hip fracture has an in-hospital mortality that exceeds 10%. One year mortality of 30%. 50% require long term assistance with their daily activities and cannot walk unaided. 25% end up in institutional care.
6 OARS (Orthogeriatric interventions) Acute orthopaedic-geriatric co-management is the only model to demonstrate reductions in mortality 319 patients over the age of 65 years were randomly assigned to daily multidisciplinary geriatric intervention or usual care mortality was lower in patients assigned to geriatric intervention (0.6% vs 5.8%, P = 0.03) major medical complications were reduced (45.2% vs 61.7%). At 3 months more patients in the geriatric intervention group had achieved a partial recovery (57% vs 44%, P = 0.03) Vidan M, et al. Efficacy of a comprehensive geriatric intervention in older patients hospitalized for hip fracture: A randomized, controlled trial. [see comment]. Journal of the American Geriatrics Society 2005; 53:
7 Why do patients die Care is not ideal : Medical-Time to surgery, pre op and post op care Nursing-focus-prevention of pressure ulcers and delirium Physiotherapy-early mobilisation Cardiac comorbidity coronary heart disease
8 Chong et al.description of an orthopaedic-geriatric model of care in Australia with 3 years data. Geriatr Gerontol Int 2008; 8: OARS (Orthopaedic Aged Care and Rehabilitation Service) Acute co-management with dedicated medical team and multidisciplinary team including a nurse coordinator and allied health Review of outcomes over a 3 year period. 834 consecutive patients Inpatient fractured NOF mortality of 3.5% c/w state average of 5.2% 90% who died had 3 significant comorbidities 70% had a premorbid cardiac condition
9 Peri-operative Myocardial Infarction Mostly silent Occur early after surgery ECG changes non-q wave Either end of surgery or hours later Circulation 2006,Am Heart J 2007,Anesthesiology 1998
10 Cardiac Troponin I Troponin I retrospectively added onto blood ordered by unit Pre-op Days 1,2,3 post-op Tested after 30 days (mean 46 days) Architect STAT Troponin I assay (Abbott Diagnostics
11 Methods Demographic and medical data reviewed including complications and mortality 100/102 patients followed up at 1 year
12 Results 102 patients consented Mean age 79 (SD 10) 73% women 85% from home and 15% residential care Incidence of post-op troponin rise was 52.9% (54/102) Mean time to peak troponin = 2 days post-op
13 Results Mortality 21/102 (20.6%) 20 patients with a troponin rise versus 1 without (p<0.0001) Post-op troponin rise (OR 12.0,p=0.025) 50% died of cardiovascular cause
14 (a) Kaplan Meier survival curve of all patients divided into whether troponin was elevated post-operatively. Chong C P et al. Age Ageing 2009;38:
15 Findings Troponin I rise independently and significantly associated with increased mortality and cardiac events at 1 year Significant relationship between magnitude of peak troponin and one year mortality Prognostic marker for older patients undergoing emergency orthopaedic surgery Can prevention or treatment of troponin rises improve outcome?
16 Troponin elevation If elevated, patients were randomised to the intervention (cardiology care) versus standard care. Intervention: management in coronary care, telemetry for at least 24 hours, review by cardiologist within 24 hrs who made recommendations about medications, investigations outpatient follow up + functional tests if appropriate.
17 Main intervention Changes to medications as a result of a troponin elevation CC: 29 (82.9%) SC: 8 (22.9%), p<0.001 Aspirin and b-blocker use significantly different Aspirin 16 commenced CC, 2 SC(p=0.022) BBlocker 9 commenced CC, 1 SC (p=0.034) No difference with statins 12, 14 (p=0.806)
18 Intervention No patients received an inpatient coronary angiogram. All patients randomised to CC received telemetry for 24 hours. Non-sustained VT seen in 5/35 (14.3%), one dead at one year.
19 Results No difference between randomised groups 6/35 (17.1%) dead in each group (p=1.000) Cardiology care did not improve immediate outcomes nor one year mortality Treatment at discretion of cardiology unit Difficulty with follow up
20 Where to from here Intervention too late In collaboration with Department of Cardiology and Orthopaedics?RCT looking at preoperative Statins and Ivabradine
21 Adapating the lessons from orthogeriatrics Extension into elective surgery
22 Care for older patients undergoing elective surgery POPS (Proactive care of older people undergoing surgery) service at Guys Hypothesis- Multidisciplinary preoperative intervention targeting potentially modifiable risk factors will improve post-operative outcomes Harari et al. Proactive care of older people undergoing surgery ('POPS'): Designing, embedding evaluating and funding a comprehensive geriatric assessment service for older elective surgical patients Age Ageing 2007:36:190-6
 POP S Geriatrician Nurse Specialist OT Physiotherapi st Social Worker Hospital Admission Post-op consultant geriatrician/")

23 Surgical Outpatients Proactive referral of all patients aged 75 or over Patients at risk according to screening criteria Patients diagnosed as medically unfit Post Discharge Intermediate Care Links with primary care/ social care Specialist clinic follow up (falls etc) POP S Geriatrician Nurse Specialist OT Physiotherapi st Social Worker Hospital Admission Post-op consultant geriatrician/ specialist nurse intervention Therapy liaison Discharge planning Teaching/ training Pre-operative Multidisciplinary assessment, treatment and liaison with surgical and anaesthetic team Consultant assessment: Comprehensive medical management Specialist Nurse: Comprehensive assessment and patient/ carer education Physiotherapy: Domiciliary assessment, muscle strengthening (cardiovascular training and breathing exercises) OT: Home visit, equipment provision Social Care: Post-op discharge planning
24 Medical complications MR Pre-POPS Post-POPS N=54 N=54 Delirium 18.5% (10) 5.6% (3)* Pneumonia 20% (11) 4% (2)* Wound sepsis 22.2% (12) 3.7% (2)* ACS 7.4% (4) 3.7% (2) Arrhythmia 13% (7) 7.4% (4) Heart failure 3.7% (2) 0 Thrombosis 11% (6) 2% (1)
25 Multidisciplinary complications MR Pre-POPS N=54 N=54 Post-POPS Uncontrolled pain 29.6 (16) 1.9 (1)* NBM >4days 9.3 (5) 0* Catheter>4/ (11) 7.4 (4)* Constipation 29.6 (16) 16.7 (9) Dependent 14.8 (8) 0* transfers Bedridden >3days 27.8 (15) 9.3 (5)* Pressure sores 18.5 (10) 3.7 (2)*
26 Resource issues MR Pre-POPS Post-POPS N=54 N=54 Length of stay (2-80) (4-26)* Delayed discharge 70.4% (38) 24.1% (13)* - medical problems 37% (20) 13% (7) - slow rehabn. 13% (7) 7.4% (4) - wait for OT or equipment 20.4% (11) 3.7% (2)
27 PRIME (Proactive medical intervention for elective surgical patients in the CGA pre op elderly) Operative risk determined Perioperative management Case control analysis in process
28 Pilot study examining the intervention 30 patients vs 60 controls Controls recruited from previous yearsame time period and matched for procedure, age and sex.
29 Results (JAGS 2014 ) No diff in outcomes, LOS Charlson comorbidity aged adjusted: PRIME (4.8) vs Control (3.9), p= Post op cardiac complication: PRIME 0, Control 7/60, p=0.051 Notice of admission to surgery PRIME 78 days, control 132 days, p= Summary-treating sicker patients, faster with equivalent results
30 Other hospital based studies Delirium prevention study Does exercise and reorientation prevent delirium in hospital? Largest randomised controlled trial in the world (> 600 patients)- Dr Kim Jeffs and NCRC. The Ethics of cardiopulmonary resuscitation-dr Barbara Hayes PhD
31 Interface with the community The Post Acute Care Study Lim WK, Lambert SF, Gray LC. Effectiveness of case management and postacute services in older people after hospital discharge. Med J Aust :262-6.
32 Background: Definition The Victorian Post Acute Care (PAC) Program is a time limited short-term intervention designed to assist patients to fully recuperate following an acute hospital admission.
33 Post Acute Care Study The PAC study was a multicentre randomised controlled study involving four Melbourne hospitals funded by the Victorian DHS. The hypotheses was that: The PAC intervention reduces the readmission rate or the overall hospital utilisation rates in the 6 month period after discharge. The PAC intervention improves health status, quality of life and reduces continuing community service use 6 months after discharge.
34 Recruitment Patients were eligible for study enrolment if they met the following risk screening criteria: The patient was likely to have mobility and/or self care management problems OR met two or more of the following three criteria: AND The patient lived alone The patient had responsibilities for caring for others at home The patient used community services prior to their hospital admission Patient required community services on discharge.
35 Results 946 PAC eligible: Not able to recruit 266, Declined 205, Missed consented, 598 available for analysis 311 intervention, 287 controls
36 Results for readmitted patients
37 Results Improvement in Independent Living and AQoL score. Cost effective. Post Acute Care now available across the state.
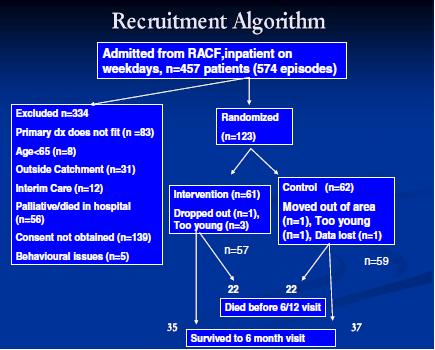
38 Interface with residential care The HARP experience
39 RECIPE Residential Care Intervention Program in the Elderly Harvey P, Storer M, Berlowitz DJ, Jackson B, Hutchinson A, Lim WK. Feasibility and impact of a post-discharge geriatric evaluation and management service for patients from residential care: the Residential Care Intervention Program in the Elderly (RECIPE). BMC Geriatrics. 2014
40 RECIPE: intervention Comprehensive (geriatric) assessment in RCF after discharge from hospital Referral to appropriate medical and allied health professionals Education and information sharing with residents, carers/family, facility staff and general practitioners ( family meetings, typed care-plan faxed on day of visit, telephone calls, liaison with hospital units) Advanced Care Planning Rapid response to intercurrent illness Hospital-in-the-facility Mobile diagnostics (radiology, pathology) Medication imprest & temporary drug chart
41
42 Baseline measures QOL-AD MMSE Barthel index Zung for depression No diff at baseline Follow-up 3 visits over 6 months
43 Baseline Characteristics n=116 Control n=52 Intervention n=51 P value Age, years, mean ± SD 86.7 ± ± Male, n (%) 24(40.7) 19 (33.3) 0.45 Hostel, n (%) 26(44.1) 27(47.4) 0.85 Australian born, n (%) 34(59.6) 38(64.4) 0.43 English speaking, n (%) 44(77.2) 45(76.3) 0.66 Index length of stay
44 Hospital Readmissions n=116 Control n=59 Intervention n=57 P value At least one readmission in 6/12 (%) Readmissions/pt, mean Acute inpatient LOS (days)/pt mean ED presentations/pt, mean Subacute LOS (days), mean Total (index,acute,subacute) LOS, mean
45 Advanced Care Planning 39/57(68.4%) of intervention group completed a written Advanced Treatment Plan 22/57(38.6%)died in intervention group and 22/59(37.2%)p=0.518 in the control group Not all who died had written Advanced Treatment Plans but all had discussions None of the control group completed Advanced Treatment Plans
46 Satisfaction -Family/patient Intervention Control n=17 P value n=19 Overall satisfaction Medical assessment 16 8 <0.01 Advice/phone contact 10 8 <0.01 Coordination of care Advanced Care Planning Family Discussion
47 Hospital treatment in residential care Lau L, Chong C, Lim WK. Hospital treatment in residential care facilities is a viable alternative to hospital admission for selected patients. Geriatrics and Gerontology International ;13:
48 Aim To determine if hospital treatment in residential care facilities, led by a geriatric team, might be a viable alternative to inpatient admission for selected patients
49 Methods Case series with a new intervention were compared with historical controls receiving the conventional treatment. Treatment in residential care facilities (TRC) by the Residential Care Intervention Program in The Elderly (RECIPE) service was compared against the conventional treatment group, aged care unit (ACU) inpatients.
50 Hospital treatment in RC
51 Conclusion Hospital treatment in residential care is viable for most patients, including those with dementia and those who need palliative care support. This model of care offers a valuable geriatric service to residents who would prefer to avoid hospital transfers, with no difference in mortality or rehospitalization rates for those treated in residential care.

52 What happened after the randomised trial
53 Methods Retrospective cohort study with 1327 patients enrolled in the RECIPE service between 2004 and RCF involved. Interrupted time series analysis. Outcomes-acute health utilisation.
54 Results Mortality-73% residents died during followup with a mean survival of 311 days. Comparison between pre and post enrolment to RECIPE, mean reduction of 0.13 admissions per patient per quarter or 0.52 admissions per patient per year (p=0.046). Average reduction in annual bed days per patient of 12 days
55 Summary A multicomponent geriatrician led outreach service to RCFs has the potential to: Reduce acute care utilisation Improve ACP and provision of Palliative care Improve patient and family satisfaction
56 The Future No shortage of research in older populations Clinical Frailty End of life care in residential care Perioperative care
57 Funding Grants Recurrent income-interface with education Future collaborations
Rehabilitation - Reducing costs and hospital stay. Dr Elizabeth Aitken Consultant Physician
 Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Care of older people in surgery (COPS)
") Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience
 Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience AA Fisher, MW Davis Department of Geriatric Medicine, The Canberra Hospital, and Australian National University
Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience AA Fisher, MW Davis Department of Geriatric Medicine, The Canberra Hospital, and Australian National University
EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY
 EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY Geriatrics, General practice, Emergency medicine, Interface medicine SUMMARY An integrated, community emergency service specifically designed for
EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY Geriatrics, General practice, Emergency medicine, Interface medicine SUMMARY An integrated, community emergency service specifically designed for
The Experience in Exeter with. hip fracture care. Data For Change
 The Experience in Exeter with hip fracture care Data For Change John Charity Associate Specialist in T&O, Lead NHFD Clinician, Royal Devon and Exeter NHS Foundation Trust Respond Deliver & Enable People
The Experience in Exeter with hip fracture care Data For Change John Charity Associate Specialist in T&O, Lead NHFD Clinician, Royal Devon and Exeter NHS Foundation Trust Respond Deliver & Enable People
Hospital at Home. Frailty and Hospital at Home. 17 th March Pam Livingstone and Gwyneth Thom
 Hospital at Home Frailty and Hospital at Home 17 th March 2016 Pam Livingstone and Gwyneth Thom National Definition of Hospital at Home December 2013 An episode of specialist care delivered at home as
Hospital at Home Frailty and Hospital at Home 17 th March 2016 Pam Livingstone and Gwyneth Thom National Definition of Hospital at Home December 2013 An episode of specialist care delivered at home as
Perioperative Infarcts: Epidemiology, predictors and post-op monitoring
 Friday Nov 3rd, 2017 1pm Perioperative Infarcts: Epidemiology, predictors and post-op monitoring Dr Carol Chong Geriatrician Northern Health, Epping, Victoria, Australia How I became interested in this
Friday Nov 3rd, 2017 1pm Perioperative Infarcts: Epidemiology, predictors and post-op monitoring Dr Carol Chong Geriatrician Northern Health, Epping, Victoria, Australia How I became interested in this
Introduction of Early Supported Discharge to Intermediate Care Pathway for Hip Fracture
 Introduction of Early Supported Discharge to Intermediate Care Pathway for Hip Fracture Neil Pendleton, Mark Brown, Heather Spence Salford Royal NHS Hospital Introduction of Early Supported Discharge to
Introduction of Early Supported Discharge to Intermediate Care Pathway for Hip Fracture Neil Pendleton, Mark Brown, Heather Spence Salford Royal NHS Hospital Introduction of Early Supported Discharge to
MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab
 MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab In response to a changing rehab landscape in which rehabilitation is offered in many different settings with variations
MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab In response to a changing rehab landscape in which rehabilitation is offered in many different settings with variations
Perioperative Care of Older People
 Perioperative Care of Older People Philip Braude, Consultant Geriatrician POPS Proactive care of Older People undergoing Surgery Guy s and St Thomas Hospital @DrPhilipBraude #AGM17conf Prevalence surgical
Perioperative Care of Older People Philip Braude, Consultant Geriatrician POPS Proactive care of Older People undergoing Surgery Guy s and St Thomas Hospital @DrPhilipBraude #AGM17conf Prevalence surgical
THE WHITE PAPER Associate Professor Peter Lipski
 A0 NEW DIRECTION FOR GERIATRIC MEDICAL SERVICES ON THE NSW CENTRAL COAST 2007 THE WHITE PAPER Associate Professor Peter Lipski 1. Traditional Acute Geriatric Medicine Models of Hospital Care. 2. Acute
A0 NEW DIRECTION FOR GERIATRIC MEDICAL SERVICES ON THE NSW CENTRAL COAST 2007 THE WHITE PAPER Associate Professor Peter Lipski 1. Traditional Acute Geriatric Medicine Models of Hospital Care. 2. Acute
COGNITIVE IMPAIRMENT IN
 COGNITIVE IMPAIRMENT IN THE HOSPITAL SETTING Professor Len Gray April 2014 Some key questions How common is cognitive impairment among hospitalised older patients? Which cognitive syndromes are associated
COGNITIVE IMPAIRMENT IN THE HOSPITAL SETTING Professor Len Gray April 2014 Some key questions How common is cognitive impairment among hospitalised older patients? Which cognitive syndromes are associated
Implementing Best Practice Rehabilitative Care for Patients with Hip Fracture & Total Joint Replacement
 Implementing Best Practice Rehabilitative Care for Patients with Hip Fracture & Total Joint Replacement A Toolkit for Implementing the RCA s TJR and Hip Fracture Best Practice Frameworks January 2018 Purpose
Implementing Best Practice Rehabilitative Care for Patients with Hip Fracture & Total Joint Replacement A Toolkit for Implementing the RCA s TJR and Hip Fracture Best Practice Frameworks January 2018 Purpose
Appendix E : Evidence table 9 Rehabilitation: Other Key Documents
 Appendix E : Evidence table 9 Rehabilitation: Other Key Documents 1. Cameron et al. Geriatric rehabilitation following following fractures in older people: a systematic review. Health Technology Assessment
Appendix E : Evidence table 9 Rehabilitation: Other Key Documents 1. Cameron et al. Geriatric rehabilitation following following fractures in older people: a systematic review. Health Technology Assessment
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Acute Care of Older Surgical Patients. Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017
 Acute Care of Older Surgical Patients Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017 NCEPOD 2010 overall care % 50 45 40 35 30 25 20 15 10 5 0 Good practice
Acute Care of Older Surgical Patients Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017 NCEPOD 2010 overall care % 50 45 40 35 30 25 20 15 10 5 0 Good practice
A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come
: What we know, what we think and what s to come") A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come The AVERT Trial Collaboration group Joshua Kwant, Blinded Assessor 17 th May 2016 NIMAST Nothing to disclose Disclosure
A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come The AVERT Trial Collaboration group Joshua Kwant, Blinded Assessor 17 th May 2016 NIMAST Nothing to disclose Disclosure
BGS Spring The Dementia and Delirium CQUIN
 The Dementia and Delirium CQUIN Dr Louise Allan Clinical Senior Lecturer in Geriatric Medicine Institute of Neuroscience Newcastle University Outline Why should it have happened? Why did it happen? How
The Dementia and Delirium CQUIN Dr Louise Allan Clinical Senior Lecturer in Geriatric Medicine Institute of Neuroscience Newcastle University Outline Why should it have happened? Why did it happen? How
Intervention and frailty: the Home-based Older People s Exercise (HOPE)Programme
Programme") #frailtywakefield Intervention and frailty: the Home-based Older People s Exercise (HOPE)Programme Andy Clegg Senior Lecturer & Consultant Geriatrician University of Leeds & Bradford Royal Infirmary Understanding
#frailtywakefield Intervention and frailty: the Home-based Older People s Exercise (HOPE)Programme Andy Clegg Senior Lecturer & Consultant Geriatrician University of Leeds & Bradford Royal Infirmary Understanding
FRAILTY PATIENT FOCUS GROUP
 FRAILTY PATIENT FOCUS GROUP Community House, Bromley 28 November 2016-10am to 12noon In attendance: 7 Patient and Healthwatch representatives: 4 CCG representatives: Dr Ruchira Paranjape went through the
FRAILTY PATIENT FOCUS GROUP Community House, Bromley 28 November 2016-10am to 12noon In attendance: 7 Patient and Healthwatch representatives: 4 CCG representatives: Dr Ruchira Paranjape went through the
Orthopaedic Therapy Service inpatient guide. Information for patients MSK Orthopaedic Inpatients (Therapy)
") Orthopaedic Therapy Service inpatient guide Information for patients MSK Orthopaedic Inpatients (Therapy) This leaflet is designed to answer any queries you may have about the Orthopaedic Therapy Service.
Orthopaedic Therapy Service inpatient guide Information for patients MSK Orthopaedic Inpatients (Therapy) This leaflet is designed to answer any queries you may have about the Orthopaedic Therapy Service.
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum
 Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
SAFE HIP FRACTURES. Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust
 SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
Professor Brian Draper
 Understanding what s different for patients with dementia in acute care hospitals coalface implications Psychiatry Professor Brian Draper UNSW & Prince of Wales Hospital, Randwick Background Previous analyses
Understanding what s different for patients with dementia in acute care hospitals coalface implications Psychiatry Professor Brian Draper UNSW & Prince of Wales Hospital, Randwick Background Previous analyses
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Pre-operative Assessment of the Frail Elderly Person at Addenbrookes Hospital. Dr Fay J Gilder Consultant Anaesthetist
 Pre-operative Assessment of the Frail Elderly Person at Addenbrookes Hospital Dr Fay J Gilder Consultant Anaesthetist Frailty Models A multidimensional state of increased vulnerability Phenotype model
Pre-operative Assessment of the Frail Elderly Person at Addenbrookes Hospital Dr Fay J Gilder Consultant Anaesthetist Frailty Models A multidimensional state of increased vulnerability Phenotype model
The Older Persons Journey: The Local Health District Perspective
 The Older Persons Journey: The Local Health District Perspective Department of Geriatric Medicine Nepean Blue Mountain LHD Dr Anita Sharma FRACP, PhD 27 th August 2015 Nepean Blue Mountains PHN Vision
The Older Persons Journey: The Local Health District Perspective Department of Geriatric Medicine Nepean Blue Mountain LHD Dr Anita Sharma FRACP, PhD 27 th August 2015 Nepean Blue Mountains PHN Vision
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Quality of Acute Care for Older Persons with Dementia
 Quality of Acute Care for Older Persons with Dementia A Hospital-Based Pilot Study Chien-Liang Liu Center for Geriatrics and Gerontology, Taipei Veterans General Hospital, Taiwan 2013/04/20 Outline Background
Quality of Acute Care for Older Persons with Dementia A Hospital-Based Pilot Study Chien-Liang Liu Center for Geriatrics and Gerontology, Taipei Veterans General Hospital, Taiwan 2013/04/20 Outline Background
Audit of perioperative management of patients with fracture neck of femur
 Audit of perioperative management of patients with fracture neck of femur *M Dissanayake 1, N Wijesuriya 2 Registrar in Anaesthesia 1, Consultant Anaesthetist 2, North Colombo Teaching Hospital, Ragama,
Audit of perioperative management of patients with fracture neck of femur *M Dissanayake 1, N Wijesuriya 2 Registrar in Anaesthesia 1, Consultant Anaesthetist 2, North Colombo Teaching Hospital, Ragama,
Department of Geriatric Govt. Medical College, Aurangabad
 Department of Geriatric Govt. Medical College, Aurangabad Recommendations: The following recommendations have been proposed : 1. There is an urgent need for developing specialized health care services
Department of Geriatric Govt. Medical College, Aurangabad Recommendations: The following recommendations have been proposed : 1. There is an urgent need for developing specialized health care services
Geriatric Medicine I) OBJECTIVES
 OBJECTIVES") Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Palliative Care and End of Life Care
 Palliative Care and End of Life Care Relevant Data and References Victorian Population 1 Total Victorian Population as at June 2016 was 6.1 million (6,179,249) Victorian 60 plus population as at June 2016
Palliative Care and End of Life Care Relevant Data and References Victorian Population 1 Total Victorian Population as at June 2016 was 6.1 million (6,179,249) Victorian 60 plus population as at June 2016
Breast cancer in the elderly - is there a role for the geriatrician?
 Breast cancer in the elderly - is there a role for the geriatrician? Workshop in Breast Cancer Surgery Aarhus 18 May 2016 Lone Winther Lietzen MD, PhD Department of Geriatrics, Geriatricians? Internal
Breast cancer in the elderly - is there a role for the geriatrician? Workshop in Breast Cancer Surgery Aarhus 18 May 2016 Lone Winther Lietzen MD, PhD Department of Geriatrics, Geriatricians? Internal
Komorbiditet og ortopædkirugi - erfaringer og viden. Benn Rønnow Duus, Ledende overlæge, Ortopædkirurgisk afdeling Bispebjerg Hospital
 Komorbiditet og ortopædkirugi - erfaringer og viden Benn Rønnow Duus, Ledende overlæge, Ortopædkirurgisk afdeling Bispebjerg Hospital Kræft og komorbiditet alle skal have del i de gode resultater 1 Kræftens
Komorbiditet og ortopædkirugi - erfaringer og viden Benn Rønnow Duus, Ledende overlæge, Ortopædkirurgisk afdeling Bispebjerg Hospital Kræft og komorbiditet alle skal have del i de gode resultater 1 Kræftens
Effect of Ortho-Geriatric Co-Management on Hip Fractures
 Effect of Ortho-Geriatric Co-Management on Hip Fractures Kenji Shigemoto Takeshi Sawaguchi Daigo Sakagoshi Kenichi Goshima Yu Hatsuchi Dept. Orthop. Surg. Toyama Municipal Hospital, Toyama, Japan Purpose
Effect of Ortho-Geriatric Co-Management on Hip Fractures Kenji Shigemoto Takeshi Sawaguchi Daigo Sakagoshi Kenichi Goshima Yu Hatsuchi Dept. Orthop. Surg. Toyama Municipal Hospital, Toyama, Japan Purpose
Early and Structured Rehabilitation Team Collaboration. David McWilliams Clinical Specialist Physiotherapist - UHB
 Early and Structured Rehabilitation Team Collaboration David McWilliams Clinical Specialist Physiotherapist - UHB Start early Moving through milestones Schweikert et al (2009) Increase frequency of higher
Early and Structured Rehabilitation Team Collaboration David McWilliams Clinical Specialist Physiotherapist - UHB Start early Moving through milestones Schweikert et al (2009) Increase frequency of higher
Acute care for older people with frailty
 Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester Worldview that will colour this talk Demography
Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester Worldview that will colour this talk Demography
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD
 HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff
 National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff Dr John Tsang MB ChB, FRCP Consultant Orthogeriatrician Lead clinician
National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff Dr John Tsang MB ChB, FRCP Consultant Orthogeriatrician Lead clinician
Quality Outcomes and Financial Benefits of Nutrition Intervention. Tracy R. Smith, PhD, RD, LD Senior Clinical Manager, Abbott Nutrition
 Quality Outcomes and Financial Benefits of Nutrition Intervention Tracy R. Smith, PhD, RD, LD Senior Clinical Manager, Abbott Nutrition January 28, 2016 SHIFTING MARKET DYNAMICS PROVIDE AN OPPORTUNITY
Quality Outcomes and Financial Benefits of Nutrition Intervention Tracy R. Smith, PhD, RD, LD Senior Clinical Manager, Abbott Nutrition January 28, 2016 SHIFTING MARKET DYNAMICS PROVIDE AN OPPORTUNITY
Management of the Frail Older Patients: What Are the Outcomes
 Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
Introduction. Peripheral arterial disease. Hospital inpatient data - 5,498 FCE (2009/10), & 530 deaths in England alone
, & 530 deaths in England alone") 1 Introduction 2 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK 500-1000/million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up
1 Introduction 2 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK 500-1000/million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Chirurgie Ziekenhuisgroep Twente Locatie Almelo. Disclosure presenter
 Disclosure presenter The effectiveness of integrated orthogeriatric treatment on 1-year outcome in frail elderly withhip fracture E. Folbert, MANP, PhD Hospital Group, Almelo-Hengelo Rotterdam, 2018 august
Disclosure presenter The effectiveness of integrated orthogeriatric treatment on 1-year outcome in frail elderly withhip fracture E. Folbert, MANP, PhD Hospital Group, Almelo-Hengelo Rotterdam, 2018 august
Scottish Standards of Care for Hip Fracture Patients
 Scottish Standards of Care for Hip Fracture Patients This document has been prepared in collaboration with Healthcare Improvement Scotland to align with the forthcoming updated Older People in Hospitals
Scottish Standards of Care for Hip Fracture Patients This document has been prepared in collaboration with Healthcare Improvement Scotland to align with the forthcoming updated Older People in Hospitals
Unnecessary hospitalisation and investigation of low risk patients presenting to hospital with chest pain
 Unnecessary hospitalisation and investigation of low risk patients presenting to hospital with chest pain Michael Perera Advanced Trainee in General and Acute Medicine Leena Aggarwal Director, Medical
Unnecessary hospitalisation and investigation of low risk patients presenting to hospital with chest pain Michael Perera Advanced Trainee in General and Acute Medicine Leena Aggarwal Director, Medical
GRADE Tables and Summary of Findings for the recommendations of Rehabilitation in health systems
 GRADE Tables and Summary of Findings for the recommendations of Rehabilitation in health systems REHABILITATION SERVICE DELIVERY For the following PICO questions, Population includes any person who requires
GRADE Tables and Summary of Findings for the recommendations of Rehabilitation in health systems REHABILITATION SERVICE DELIVERY For the following PICO questions, Population includes any person who requires
Healthcare, hospitals and the challenges of an ageing population
 Healthcare, hospitals and the challenges of an ageing population Prof David Oliver Vice President, RCP, London Past President, British Geriatrics Society Senior Visiting Fellow, King s Fund Consultant
Healthcare, hospitals and the challenges of an ageing population Prof David Oliver Vice President, RCP, London Past President, British Geriatrics Society Senior Visiting Fellow, King s Fund Consultant
The role of the Geriatrician
 Post-operative management of the older adults with cancer The role of the Geriatrician Sofia Duque Hospital Beatriz Ângelo Geriatric University Unit Faculty of Medicine of Lisbon Geriatrics Study Group
Post-operative management of the older adults with cancer The role of the Geriatrician Sofia Duque Hospital Beatriz Ângelo Geriatric University Unit Faculty of Medicine of Lisbon Geriatrics Study Group
Guidelines to standards. Orthogeriatrics How The UK Care For Fragility Fractures
 Guidelines to standards Orthogeriatrics How The UK Care For Fragility Fractures Karen Hertz-SOTN Advanced Nurse Practitioner The NHFD Project - jointly led by BOA and BGS with the involvement of the RCN
Guidelines to standards Orthogeriatrics How The UK Care For Fragility Fractures Karen Hertz-SOTN Advanced Nurse Practitioner The NHFD Project - jointly led by BOA and BGS with the involvement of the RCN
What can we learn from the AVERT trial (so far)?
?") South West Stroke Network Event, 29 th April, 2015 What can we learn from the AVERT trial (so far)? Peter Langhorne, Professor of stroke care, Glasgow University Disclosure PL was AVERT investigator and
South West Stroke Network Event, 29 th April, 2015 What can we learn from the AVERT trial (so far)? Peter Langhorne, Professor of stroke care, Glasgow University Disclosure PL was AVERT investigator and
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami
 Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Joint replacement reviews conducted by physiotherapists Bernarda Cavka Advanced Practice Physiotherapist The Royal Melbourne Hospital
 Joint replacement reviews conducted by physiotherapists Bernarda Cavka Advanced Practice Physiotherapist The Royal Melbourne Hospital 2014 The Quantum Leap The Royal Melbourne Hospital (RMH) One of two
Joint replacement reviews conducted by physiotherapists Bernarda Cavka Advanced Practice Physiotherapist The Royal Melbourne Hospital 2014 The Quantum Leap The Royal Melbourne Hospital (RMH) One of two
End of Life Care in Dementia. Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals
 End of Life Care in Dementia Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals Rosie.Lockwood@sth.nhs.uk Agenda Some facts and figures What are the challenges? What is good care? How
End of Life Care in Dementia Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals Rosie.Lockwood@sth.nhs.uk Agenda Some facts and figures What are the challenges? What is good care? How
Comprehensive Assessment of the Frail Older Patient
 Comprehensive Assessment of the Frail Older Patient Executive Summary Comprehensive geriatric assessment (CGA) is a multidimensional and usually interdisciplinary diagnostic process designed to determine
Comprehensive Assessment of the Frail Older Patient Executive Summary Comprehensive geriatric assessment (CGA) is a multidimensional and usually interdisciplinary diagnostic process designed to determine
Title: From zero to comprehensive Fracture Liaison service (FLS) within existing resources
 within existing resources") Best of Health Staff Awards 2010/11 Best of Health Awards 2013 Dr Abhaya Gupta Consultant Physician Hywel Dda Health Board Title: From zero to comprehensive Fracture Liaison service (FLS) within existing
Best of Health Staff Awards 2010/11 Best of Health Awards 2013 Dr Abhaya Gupta Consultant Physician Hywel Dda Health Board Title: From zero to comprehensive Fracture Liaison service (FLS) within existing
The Perioperative Care Chain is Only as Strong as its weakest link
 The Perioperative Care Chain is Only as Strong as its weakest link Associate Professor Kerin Fielding The University of Notre Dame, Australia School of Medicine, Sydney Outline The perioperative chain
The Perioperative Care Chain is Only as Strong as its weakest link Associate Professor Kerin Fielding The University of Notre Dame, Australia School of Medicine, Sydney Outline The perioperative chain
NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT
 NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT CONTENTS PATIENTS ADMITTED WITH HEART FAILURE...4 Demographics... 4 Trends in Symptoms... 4 Causes and Comorbidities
NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT CONTENTS PATIENTS ADMITTED WITH HEART FAILURE...4 Demographics... 4 Trends in Symptoms... 4 Causes and Comorbidities
AGED CARE alliance National Aged Care Alliance Issues Paper The Aged Care Health Care Interface
 National Aged Care Alliance Issues Paper The Aged Care Health Care Interface March 2003 Purpose and Context Progress toward a continuum of care for older people requires policies and strategies for the
National Aged Care Alliance Issues Paper The Aged Care Health Care Interface March 2003 Purpose and Context Progress toward a continuum of care for older people requires policies and strategies for the
Acute front door care of frail older people. Simon Conroy Professor of Geriatric Medicine
 Acute front door care of frail older people Simon Conroy Professor of Geriatric Medicine Why is this important for physicians? Type 1 A&E attendances 11% Total Activity (Leicester) Elective admissions
Acute front door care of frail older people Simon Conroy Professor of Geriatric Medicine Why is this important for physicians? Type 1 A&E attendances 11% Total Activity (Leicester) Elective admissions
Palliative Care Consultative Service in Acute Hospital - Impact & Challenges
 Palliative Care Consultative Service in Acute Hospital - Impact & Challenges Dr. Annie Kwok Consultant Palliative Care Unit Department of Medicine & Geriatrics Caritas Medical Centre Contents Aging population
Palliative Care Consultative Service in Acute Hospital - Impact & Challenges Dr. Annie Kwok Consultant Palliative Care Unit Department of Medicine & Geriatrics Caritas Medical Centre Contents Aging population
Health and independence Strategic Vision and Implementation Plan for the Shropshire Frail & Complex Service
 Enclosure 01 Health and independence Strategic Vision and Implementation Plan for the Shropshire Frail & Complex Service Frail &Complex Service The challenge to the local health & social care economy The
Enclosure 01 Health and independence Strategic Vision and Implementation Plan for the Shropshire Frail & Complex Service Frail &Complex Service The challenge to the local health & social care economy The
People at the centre of health and care
 People at the centre of health and care Improving Care for Older People in Acute Care F is for Frailty F is for Frailty Identification and co-ordination of care for frail older people Starting point -
People at the centre of health and care Improving Care for Older People in Acute Care F is for Frailty F is for Frailty Identification and co-ordination of care for frail older people Starting point -
Hip Fracture (HFR) Measures Document
 Measures Document") Hip Fracture (HFR) Measures Document HFR Version: 2 - covering patients discharged between 01/10/2017 and present. Programme Lead: Sam Doddridge Clinical Leads: Ms Phil Thorpe Dr John Tsang Number of Measures
Hip Fracture (HFR) Measures Document HFR Version: 2 - covering patients discharged between 01/10/2017 and present. Programme Lead: Sam Doddridge Clinical Leads: Ms Phil Thorpe Dr John Tsang Number of Measures
Integrating Medical and Social Support for Elderly System & Technology Enabled Service Innovations. Dr Christina MAW Hospital Authority, Hong Kong
 Integrating Medical and Social Support for Elderly System & Technology Enabled Service Innovations Dr Christina MAW Hospital Authority, Hong Kong Hospital Authority (HA) of Hong Kong A statutory body responsible
Integrating Medical and Social Support for Elderly System & Technology Enabled Service Innovations Dr Christina MAW Hospital Authority, Hong Kong Hospital Authority (HA) of Hong Kong A statutory body responsible
HERTS VALLEYS CCG PALLIATIVE AND END OF LIFE CARE STRATEGY FOR ADULTS AND CHILDREN
 HERTS VALLEYS CCG PALLIATIVE AND END OF LIFE CARE STRATEGY FOR ADULTS AND CHILDREN 2016-2021 1 1. Introduction Herts Valleys Palliative and End of Life Care Strategy is guided by the End of Life Care Strategic
HERTS VALLEYS CCG PALLIATIVE AND END OF LIFE CARE STRATEGY FOR ADULTS AND CHILDREN 2016-2021 1 1. Introduction Herts Valleys Palliative and End of Life Care Strategy is guided by the End of Life Care Strategic
2O18 ANNUAL REPORT SUPPLEMENTARY REPORT
 2O18 ANNUAL REPORT SUPPLEMENTARY REPORT Enhancing Outcomes for Older People ABBREVIATIONS AND DEFINITIONS For the purposes of this report, the following interpretation of terms should be used. ACT Australian
2O18 ANNUAL REPORT SUPPLEMENTARY REPORT Enhancing Outcomes for Older People ABBREVIATIONS AND DEFINITIONS For the purposes of this report, the following interpretation of terms should be used. ACT Australian
URN: Family name: Given name(s): Address: Initial Signature Print Name Role
: Address: Initial Signature Print Name Role") Do Not Write in this binding margin v5.00-02/2012 Mat. No.: 10206019 SW030b The State of Queensland (Queensland Health) 2012 Contact CIM@health.qld.gov.au ÌSW030bIÎ Facility: s Never Replace Clinical Judgement
Do Not Write in this binding margin v5.00-02/2012 Mat. No.: 10206019 SW030b The State of Queensland (Queensland Health) 2012 Contact CIM@health.qld.gov.au ÌSW030bIÎ Facility: s Never Replace Clinical Judgement
Geriatric screening in acute care wards a novel method of providing care to elderly patients
 Geriatric screening in acute care wards a novel method of providing care to elderly patients JKH Luk, T Kwok, J Woo Objective. To assess a nurse-implemented geriatric screening system. Design. Descriptive
Geriatric screening in acute care wards a novel method of providing care to elderly patients JKH Luk, T Kwok, J Woo Objective. To assess a nurse-implemented geriatric screening system. Design. Descriptive
The COLLaboration on AGEing (COLLAGE)
") The COLLaboration on AGEing (COLLAGE) Professor D. William Molloy University College Cork, Ireland. The Lessons from Europe Seminar 23-09-15 Overview Exemplars within COLLAGE: 1. What is COLLAGE? 2. The
The COLLaboration on AGEing (COLLAGE) Professor D. William Molloy University College Cork, Ireland. The Lessons from Europe Seminar 23-09-15 Overview Exemplars within COLLAGE: 1. What is COLLAGE? 2. The
MINERVA MEDICA COPYRIGHT
 Hip fracture (HF) is a common event in the geriatric population and is often associated with significant morbidity, mortality and costs for the Healthcare Systems. The growing awareness of HF consequences
Hip fracture (HF) is a common event in the geriatric population and is often associated with significant morbidity, mortality and costs for the Healthcare Systems. The growing awareness of HF consequences
Geriatric Emergency Management PLUS Program Costing Analysis at the Ottawa Hospital
 Geriatric Emergency Management PLUS Program Costing Analysis at the Ottawa Hospital Regional Geriatric Program of Eastern Ontario March 2015 Geriatric Emergency Management PLUS Program - Costing Analysis
Geriatric Emergency Management PLUS Program Costing Analysis at the Ottawa Hospital Regional Geriatric Program of Eastern Ontario March 2015 Geriatric Emergency Management PLUS Program - Costing Analysis
Hospice and Palliative Care: Value-Based Care Near the End of Life
 Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
Summary of funded Dementia Research Projects
 Summary of funded Dementia Research Projects Health Services and Delivery Research (HS&DR) Programme: HS&DR 11/2000/05 The detection and management of pain in patients with dementia in acute care settings:
Summary of funded Dementia Research Projects Health Services and Delivery Research (HS&DR) Programme: HS&DR 11/2000/05 The detection and management of pain in patients with dementia in acute care settings:
Hospice and Palliative Care: Value-Based Care Near the End of Life
 Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
Michal Boyd, 1,2,3 Joanna B Broad, 1 Xian (Tony) Zhang, 1 Ngaire Kerse, 4 and Martin J Connolly 1,3
 Zhang, 1 Ngaire Kerse, 4 and Martin J Connolly 1,3") NZACA Annual Conference - Wellington 15 October 2014 Michal Boyd, 1,2,3 Joanna B Broad, 1 Xian (Tony) Zhang, 1 Ngaire Kerse, 4 and Martin J Connolly 1,3 1 Freemasons Department of Geriatric Medicine, The
NZACA Annual Conference - Wellington 15 October 2014 Michal Boyd, 1,2,3 Joanna B Broad, 1 Xian (Tony) Zhang, 1 Ngaire Kerse, 4 and Martin J Connolly 1,3 1 Freemasons Department of Geriatric Medicine, The
Geriatric Hip Fracture Co-Management. Pannida Wattanapanom, M.D., FACP.
 Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Geriatrics in primary care, the Dutch way: eductional programs for (nursing home and family) physicians
 physicians") Geriatrics in primary care, the Dutch way: eductional programs for (nursing home and family) physicians @Wilco Achterberg Elderly care physician (ECP) Professor of elderly care medicine DEP. OF PRIMARY
Geriatrics in primary care, the Dutch way: eductional programs for (nursing home and family) physicians @Wilco Achterberg Elderly care physician (ECP) Professor of elderly care medicine DEP. OF PRIMARY
How to prevent early & unplanned hospital readmission?
 How to prevent early & unplanned hospital readmission? - after subacute care K. Singler 21th September 2017 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report. K. Singler
How to prevent early & unplanned hospital readmission? - after subacute care K. Singler 21th September 2017 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report. K. Singler
Comprehensive geriatric assessment and home-based rehabilitation for elderly people with a history of recurrent non-elective hospital admissions
 Geriatric assessment and home-based rehabilitation Age and Ageing 2006; 35: 487 491 doi:10.1093/ageing/afl049 Published electronically 13 June 2006 The Author 2006. Published by Oxford University Press
Geriatric assessment and home-based rehabilitation Age and Ageing 2006; 35: 487 491 doi:10.1093/ageing/afl049 Published electronically 13 June 2006 The Author 2006. Published by Oxford University Press
Aged Persons Mental Health Past, Present and Future
 Aged Persons Mental Health Past, Present and Future Kuruvilla George Director of Aged Persons Mental Health and Director of Medical Services, Peter James Centre and Wantirna Health, Eastern Health Deputy
Aged Persons Mental Health Past, Present and Future Kuruvilla George Director of Aged Persons Mental Health and Director of Medical Services, Peter James Centre and Wantirna Health, Eastern Health Deputy
145 overall responses (30 Respondents did not complete the survey after Q3 (no data))
)") 0 Delirium Stocktake 2017 for Health of Older People Service Level Alliance Background As part of its focus on improving the wellbeing of older people, Health of Older People Service Level Alliance (HOPSLA)
0 Delirium Stocktake 2017 for Health of Older People Service Level Alliance Background As part of its focus on improving the wellbeing of older people, Health of Older People Service Level Alliance (HOPSLA)
4/26/2012. Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012
 Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
New York City Development of the Geriatric Collaborative
 New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
2015 UK Parkinson s Audit Patient and carer report
 2015 UK Parkinson s Audit Patient and carer report Introduction This is a summary of the main findings of the 2015 UK Parkinson s Audit. This is the fifth and largest audit of Parkinson s to date. This
2015 UK Parkinson s Audit Patient and carer report Introduction This is a summary of the main findings of the 2015 UK Parkinson s Audit. This is the fifth and largest audit of Parkinson s to date. This
Acute care for older people with frailty
 Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester Why acute frailty? Demography Absence of immortality
Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester Why acute frailty? Demography Absence of immortality
12/6/2016. Objective PALLIATIVE CARE IN THE NURSING HOME. Medical Care in the US. Palliative Care
 Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Submission on the Draft National Clinical Practice Guidelines for Dementia in Australia
 Submission on the Draft National Clinical Practice Guidelines for Dementia in Australia 4 June 2015 details Name of organisation Royal Australian College of General Practitioners () Postal Address Legal
Submission on the Draft National Clinical Practice Guidelines for Dementia in Australia 4 June 2015 details Name of organisation Royal Australian College of General Practitioners () Postal Address Legal
Welcome to the RGP of Toronto network webinar!
 Welcome to the RGP of Toronto network webinar! The presentation will begin in a few moments. Here are some tips: To ask a question during the webinar, type into the Chat box A fast, wired internet connection
Welcome to the RGP of Toronto network webinar! The presentation will begin in a few moments. Here are some tips: To ask a question during the webinar, type into the Chat box A fast, wired internet connection
Medico-Social Impact of Fragility Fracture 11/2/2014. Dr David Dai Consultant Geriatrician Prince of Wales Hospital 24 th January, 2014
 Medico-Social Impact of Fragility Fracture Dr David Dai Consultant Geriatrician Prince of Wales Hospital 24 th January, 2014 2014 Policy Agenda As Hong Kong moves steadily to an ageing society (with the
Medico-Social Impact of Fragility Fracture Dr David Dai Consultant Geriatrician Prince of Wales Hospital 24 th January, 2014 2014 Policy Agenda As Hong Kong moves steadily to an ageing society (with the
Inputs from Medical Unit, Ministry of Social Security and Ministry of Health Mauritius1
 1. In your country/region, how is long-term care for older persons defined and provided for in legal and policy frameworks? What types of support and service are covered? Long term care for older persons
1. In your country/region, how is long-term care for older persons defined and provided for in legal and policy frameworks? What types of support and service are covered? Long term care for older persons
Perso An. Geri-O. Objectives: fragility fracture. AL SUPPORT. presentation.
 10 th Annual Spring Conference Arizona Geriatrics Society Perso on-centered Care: An Interprofessional Panel Ana Sanguineti, MD Geri-O Ortho Hip Fracture Consult Service Banner Univer rsity Medical Center
10 th Annual Spring Conference Arizona Geriatrics Society Perso on-centered Care: An Interprofessional Panel Ana Sanguineti, MD Geri-O Ortho Hip Fracture Consult Service Banner Univer rsity Medical Center
Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire
 Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire Introduction This document introduces South Gloucestershire Clinical Commissioning
Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire Introduction This document introduces South Gloucestershire Clinical Commissioning
Hospital Transition Management. Barbara Wood, BSN, MBA
 Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Falls Prevention Best Practice
 Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Case Review of Inpatient Rehabilitation Hospital Patients Not Suited for Intensive Therapy
 U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES OFFICE OF INSPECTOR GENERAL Case Review of Inpatient Rehabilitation Hospital Patients Not Suited for Intensive Therapy OEI-06-16-00360 DECEMBER 2016 SUZANNE MURRIN
U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES OFFICE OF INSPECTOR GENERAL Case Review of Inpatient Rehabilitation Hospital Patients Not Suited for Intensive Therapy OEI-06-16-00360 DECEMBER 2016 SUZANNE MURRIN
Sharp HealthCare Hospice and Palliative Care
 Sharp HealthCare Hospice and Palliative Care The Continuum for Advanced Illness and End Stage Disease Management (AAC) Daniel R. Hoefer, MD CMO, Outpatient Palliative Care and Hospice Suzi K. Johnson,
Sharp HealthCare Hospice and Palliative Care The Continuum for Advanced Illness and End Stage Disease Management (AAC) Daniel R. Hoefer, MD CMO, Outpatient Palliative Care and Hospice Suzi K. Johnson,