ABCDEF Bundle Breakout
|
|
|
- Mercy Parker
- 6 years ago
- Views:
Transcription
1 ABCDEF Bundle Breakout Andrew Masica, MD, MSCI VP, Chief Clinical Effectiveness Officer Baylor Scott & White Health
2 Disclosures/Funding Support Grant R18-HS from the Agency for Healthcare Research and Quality (AHRQ) funded portions of this work. The findings and conclusions in this program are those of the author, who is responsible for its content, and do not necessarily represent the views of AHRQ. Baylor Scott & White Research institute holds research grants from the following companies on which Dr. Masica is an investigator: Pfizer, Mallinckrodt, Medtronic. These research grants are unrelated to the presentation content. No commercial products or services will be referenced. 2
3 Learning Objectives 1. Articulate ABCDEF bundle care processes, eligibility criteria, and safety parameters 2. Delineate specific EHR workflows to facilitate ABCDEF Bundle adoption and reliable use by front-line staff 3. Interpret and apply ABCDEF reports to help guide ICU quality improvement efforts 3

 trial Choice to")



4 ABCDEF: A Bundle of Best Practices A B C D E Assess for, prevent, and manage pain Both spontaneous awakening trial (SAT) and spontaneous breathing (SBT) trial Choice to use (and of) analgesia and sedation ABCD Bundle Delirium assessment, prevention, Delirium and assessment, prevention, and management management ABCD Bundle which will be deployed across Intermountain Healthcare ABCDE Bundle Early activity and mobility F=Family Engagement
5 Synergy of the ABCDEF Bundle 5

6 ABCDEF Bundle Safety Parameters Adapted from Girard TD et al, Lancet 2008
7 Bundle Eligibility Inclusion Criteria 18 years of age or older ICU admission lasting >24 hours On the ventilator for >48 hours and <14 days Exclusion Criteria On comfort/hospice care Pending transfer to non-icu bed Never on the ventilator Physician opt-out Bundle currently used across all ICU-types/specialties 7
8 ABCDEF Bundle Implementation Tactics Adoption Program Component Time to Completion Activate Nurse/ Physician Champions and secure clinical staff conceptual buy-in Assess current state (workflow, performance) Development of supportive EHR Documentation and order set with incorporation into production (live use) environment Training Sessions a. Train the trainer b. Frontline staff c. E-learning modules Use of daily rounding tool Standardized Performance Reporting (hospital and unit levels) Optimization/EHR refinement/standing meetings Accountability as a system critical care goal 1-2 months (based on hospital size) 1-month 9-12 months 4-6 month cycle to launch each unit; multiple reinforcement sessions required months 4 months after completion of EHR workflow tools Ongoing 3 months after standardized reporting 8

9 Maynard G, SHM VTE QI Resource Room, 9
10 Interdisciplinary Effort Identify Stakeholders Collaborative Patient Care Team VP of Medical Affairs/ CMO Hospital and Unit Directors Nursing Physicians RT PT/OT Pharmacy IT Quality Improvement Patient Safety Nursing Pharmacists Respiratory PT/OT Physicians 10 10
11 Automated Bundle Activation (Opt-Out Order Set) 11

12 12

13 Assess for, Prevent and Manage Pain CPOT for intubated patients Pain Intensity Scale for verbal patients Assessments every 2 hours for ICU level care 13

14 Sedation Vacation-Structured Note 5 14
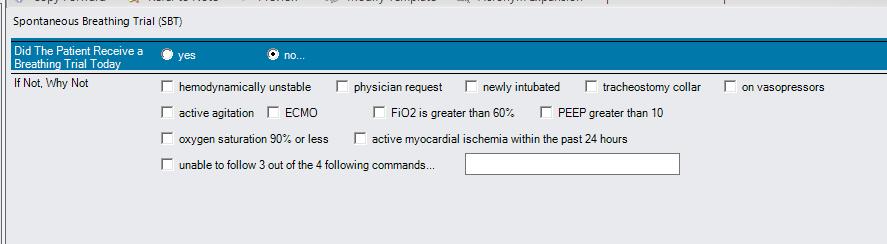
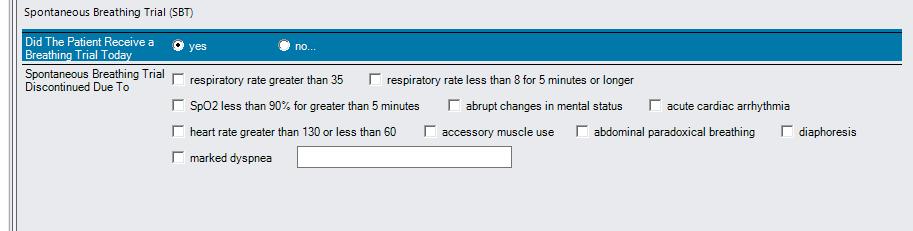
15 Breathing Trial-Structured Note 15

16 Choice to use (and of) Analgesia and Sedation Sample ICU Cohort CONFIDENTIAL - Internal Use Only 16
17 Opioid Related ADEs: Surgical Patients (N=135,000) ORADE Descriptions Severity ICD9 Codes N (%) Respiratory 9,437 (49%) Pulmonary congestion & hypostasis Mild (2%) Pulmonary insufficiency following surgery and trauma Respiratory complications Moderate 518.5X 997.3X 1,386 (15%) Other pulmonary insufficiency, not elsewhere classified Bradypnea Moderate (3%) Acute respiratory failure Severe ,897 (20%) Hypoxemia Moderate Hypoxia ,151 (13%) Mechanical ventilator Severe 96.7X 4,530 (48%) Central Nervous System 1,431 (7%) Delirium Altered mental status Confusion classified otherwise Moderate xx 1,426 (99%) Nervousness Mild 799.2X 4 (<1%) Dizziness/vertigo Mild (<1%) Baylor Scott & White Health Proprietary and Confidential Document 17
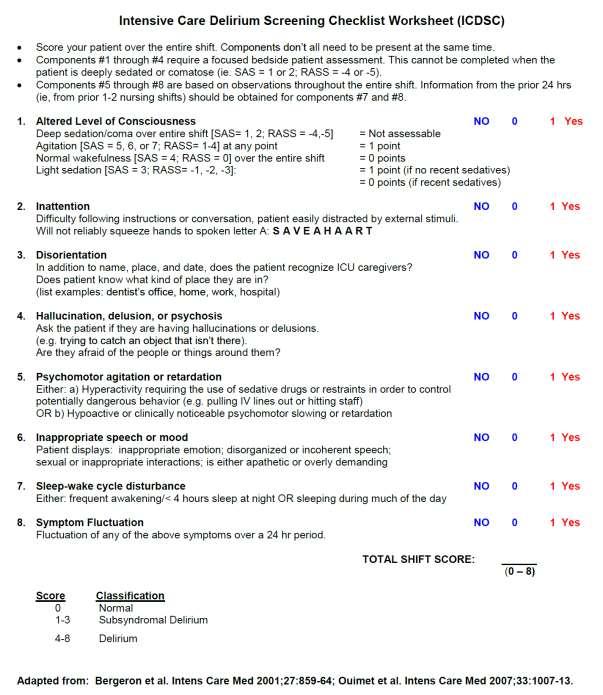
18 Tests to Detect Delirium-ICU Test Description Performance Confusion Assessment Method (Long Form) Confusion Assessment Method- Intensive Care Unit (CAM-ICU) Generally used in research Bedside clinical application Adapted for Non-verbal patients Gold Standard Sensitivity-80% Specificity-96% Intensive Care Unit Delirium Screening Checklist (ICSDC) Point scoring system Sensitivity-74% Specificity-89% Gusmao-Flores D et al. The confusion assessment method for the intensive care unit (CAM-ICU) and intensive care delirium screening checklist (ICDSC) for the diagnosis of delirium: a systematic review and meta-analysis of clinical studies. Critical Care :R
19 Other Delirium Tests Test Description Performance Confusion Assessment Method (Long Form) Confusion Assessment Method (Short Form) Ultrabrief Screening 3D Confusion Assessment Method Generally used in research First 4 items of full CAM Bedside clinical application Should be scored with cognitive screen 2 questions Months of year backwards What is the day of the week? Short CAM + embedded cognitive screen 3D=3 minutes, diagnostic Gold Standard Sensitivity-94% Specificity-89% Sensitivity-93% Specificity-64% Sensitivity-95% Specificity-94% Fick et al, Preliminary Development of an Ultrabrief Two-Item Bedside Test for Delirium, J Hosp Med 2015 Kuczmarka et al, Detection of Delirium in Hospitalized Older General Medicine Patients: A Comparison of the 3D-CAMand CAM-ICU, J Gen Intern Med


20 Sedation and Delirium Assessment CAM-ICU 20
21 21

22 CAM-ICU Decision Support 22
23 Exercise/Mobility Documentation 23

24 It s All About Family 24

25 Real-Time Reporting for Measure-Vention 25

26 Bundle Inclusion in Team Rounds/Unit Huddles 26
27 Training/Education Super-trainer course: Capability of teaching peers in CAM-ICU (including teach-back) High degree of acumen with EHR changes Case studies Basic course for frontline staff: Understand components of the ABCDE bundle and ways to incorporate those processes into routine clinical care Identify potential barriers and facilitators to implementation of the ABCDE bundle Become comfortable with bundle related changes in the EHR Development of e-learning modules 27
28 Provider Accountability Goal: For ICU patients with acute respiratory failure requiring mechanical ventilation for 24 hours, adherence to specific components of the ventilator management bundle (daily awakening trials, spontaneous breathing trials, delirium screening, early mobility). The denominator will be based on the # of observations for which the patient is eligible (i.e. had an appropriate indication and met safety criteria to receive that process) on a daily basis. Observations after > 14 days on mechanical ventilation will be excluded. Points assigned for process performance levels and added cumulatively. Performance Targets: A Daily Awakening Trial: 60-70% (1 point); 71-80% (2 points), above 80% (3 points) Breathing Trials: 60-70% (1 point); 71-80% (2 points); above 80% (3 points) B D Delirium Screening: 70-80% (1 point), 81-90% (2 points); above 90% (3 points) Exercise/Mobility: 50-60% (1 point); 61-70% (2 points); above 70% (3 points) E Composite Bundle: 50-60% (1 point), 61-70% (2 points), above 70% (3 points) 28

29 Reporting: SAT and SBT 29

30 Reporting: Delirium Metrics 30

31 Reporting: Mobility 31
32 Reporting: Mobility Detail 32

33 Reporting: Composite Bundle 33
34 Interrater Reliability of CAM-ICU Performance of CAM-ICU in Eligible Patients Inter-rater Reliability of CAM-ICU Pre Post Pre Post Patients with documented CAM-ICU Patients with documented CAM-ICU Paired cases N Kappa Coefficient (95% CI) Paired cases N Kappa Coefficient (95% CI) (%) (%) Tertiary Hospital 65 84* ( ) ( ) Community 70 85* Hospital ( ) Combined 66 84* ( ) *P-value <0.05 ( ) ( ) 34
35 Composite Bundle Uptake by Intervention Group Maintaining at > 90% Apr-15 35
36 Individual Bundle Element Adherence Trends 36
37 Baseline Population Characteristics (by Bundle Adherence Level) 25-50% N=1004 Adherence Level 50-75% N= % N=1317 p-value Age, mean (SD) (15.21) (15.47) (15.64) Gender (male), n (%) 460 (51) 523 (58) 504 (55) * Race, n (%) White 605 (67) 926 (66) 877 (71) * Black 252 (28) 418 (30) 308 (25) Other 50 (6) 60 (5) 54 (5) Hispanic n (%) 127 (14) 108 (11) 114 (13) Insurance, n (%) Private 111 (12) 205 (15) 182 (15) Medicare 501 (55) 742 (53) 612 (49) Medicaid 51 (6) 72 (5) 61 (5) Other 244 (26) 385 (26) 386 (27) APACHE Score, mean (SD) (6.73) (6.29) (6.43) * Charlson Comorbidity Index, mean (SD) 5.06 (2.86) 4.70 (2.75) 4.51 (2.78) <.0001* APR DRG Severity, n (%) 3 68 (8) 162 (12) 192 (15) <.0001* (92) 1233 (88) 1026 (83) APR-DRG Mortality Risk, n (%) (14) 308 (22) 359 (29) <.0001* (84) 1057 (75) 838 (68) Surgical, n (%) 94 (10) 166 (18) 161 (18) <.0001* Dementia, n (%) 70 (8) 63 (7) 61 (7) Alcohol, n (%) 21 (2) 23 (2) 17 (2) Current Smoker, n (%) 172 (19) 187 (21) 193 (21)
38 Impact on Delirium and Coma Outcomes (Risk Adjusted for Illness Severity): Comparison Group: 25%-50% Composite Bundle Adherence Medium Adherence 50-75% (n = 1337) High Adherence % (n = 869) Risk-adjusted Outcomes Estimate CI Estimate CI Incidence of delirium (OR) 1.49* (1.21, 1.84) 1.73* (1.37, 2.18) Duration of delirium (days) a 0.10 (-0.08, 0.29) 0.23 (-0.04, 0.50) Incidence of coma (OR) 0.67* (0.51, 0.88) 0.53* (0.40, 0.71) Duration of coma (days) b -0.32* (-0.37, -0.27) -0.52* (-0.72, -0.33) % Coma/delirium free days 0.18* (0.13, 0.23) 0.23* (0.13, 0.33) a For patients diagnosed with delirium b For patients diagnosed with coma *p <
39 Impact on Additional Clinical Outcomes (Risk Adjusted for Illness Severity): Comparison Group: 25%-50% Composite Bundle Adherence Medium Adherence 50-75% (n = 1337) High Adherence % (n = 869) Risk-adjusted Outcomes Estimate CI Estimate CI ICU Length of Stay a 0.03 (-0.05, 0.11) 0.04 (-0.05, 0.12) Hospital Length of Stay a 0.00 (-0.04, 0.03) (-0.08, 0.03) Ventilator days (-0.14, 0.03) -0.20* (-0.36, -0.05) Mobilized out of bed (OR) 2.49* (1.97, 3.15) 3.97* (3.05, 5.16) Discharged home (OR) 1.76* (1.41, 2.21) 2.16* (1.69, 2.75) Inpatient mortality (OR) 0.39* (0.31, 0.48) 0.25* (0.19, 0.31) a Patients who died during ICU stay were excluded from LOS calculations *p <
40 Bundle Program Clinical Implications Higher use of the ABCDEF bundle across a real-world setting (multiple hospitals in a heterogeneous delivery organization) was associated with improvements in several patient-centered outcomes. Deployment of the bundle likely unmasks cases of hidden ICU delirium rather than a true incidence increase; % of days awake without delirium increased with higher adherence levels. We have observed ongoing opportunities to improve physician response to recognized cases of delirium and with mobilization. The bundle is gaining momentum as a patient safety practice; several collaboratives to promote adoption are underway. The financial savings may accrue more from reduced post-acute care cost reduction (i.e. 90-day costs rather than inpatient stay) 40

41 Questions/Discussion 41
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation
 Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Wake up and Breathe: A journey in quality improvement and unintended benefits
 Wake up and Breathe: A journey in quality improvement and unintended benefits Jeffrey Singh MD FRCPC MSc Toronto Western Hospital Interdepartmental Division of Critical Care University of Toronto Disclosures
Wake up and Breathe: A journey in quality improvement and unintended benefits Jeffrey Singh MD FRCPC MSc Toronto Western Hospital Interdepartmental Division of Critical Care University of Toronto Disclosures
VENTILATOR ACQUIRED DELIRIUM CREATED BY JOSHUA VRONA COHP 450
 VENTILATOR ACQUIRED DELIRIUM CREATED BY JOSHUA VRONA COHP 450 INTRODUCTION: Delirium is defined as An acute change in mental status or a fluctuating course, impaired attention, and disorganized thinking.
VENTILATOR ACQUIRED DELIRIUM CREATED BY JOSHUA VRONA COHP 450 INTRODUCTION: Delirium is defined as An acute change in mental status or a fluctuating course, impaired attention, and disorganized thinking.
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
PREVENTING VENTILATORASSOCIATED EVENTS >>> >>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>> 2018 UPDATE
 2018 UPDATE PREVENTING VENTILATORASSOCIATED EVENTS >>> PREVENTING VENTILATOR-ASSOCIATED EVENTS CHANGE PACKAGE ii >>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>> ACKNOWLEDGEMENTS The analyses upon
2018 UPDATE PREVENTING VENTILATORASSOCIATED EVENTS >>> PREVENTING VENTILATOR-ASSOCIATED EVENTS CHANGE PACKAGE ii >>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>> ACKNOWLEDGEMENTS The analyses upon
Early and Structured Rehabilitation Team Collaboration. David McWilliams Clinical Specialist Physiotherapist - UHB
 Early and Structured Rehabilitation Team Collaboration David McWilliams Clinical Specialist Physiotherapist - UHB Start early Moving through milestones Schweikert et al (2009) Increase frequency of higher
Early and Structured Rehabilitation Team Collaboration David McWilliams Clinical Specialist Physiotherapist - UHB Start early Moving through milestones Schweikert et al (2009) Increase frequency of higher
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Reducing COPD Exacerbation Readmissions in a Community-Based Teaching Hospital
 Reducing COPD Exacerbation Readmissions in a Community-Based Teaching Hospital Dawn Waddell, PharmD, BCPS Clinical Pharmacy Manager Lisa Kingdon, PharmD, BCPS Clinical Pharmacy Specialist Dawn Waddell
Reducing COPD Exacerbation Readmissions in a Community-Based Teaching Hospital Dawn Waddell, PharmD, BCPS Clinical Pharmacy Manager Lisa Kingdon, PharmD, BCPS Clinical Pharmacy Specialist Dawn Waddell
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
Diabetes Care begins with Diabetes Prevention. Neha Sachdev, MD Janet Williams, MA
 Diabetes Care begins with Diabetes Prevention Neha Sachdev, MD Janet Williams, MA Objectives Describe the clinical practice burden and trends in type 2 diabetes Review evidence for diabetes prevention
Diabetes Care begins with Diabetes Prevention Neha Sachdev, MD Janet Williams, MA Objectives Describe the clinical practice burden and trends in type 2 diabetes Review evidence for diabetes prevention
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
William Osler Health System
 William Osler Health System Implementation of a Standardized approach to Delirium Assessment, Prevention & Management Cohort 1: Stephanie Jarvis, CNS, Seniors Health System Kuldeep Chahal, ELS, Hospital
William Osler Health System Implementation of a Standardized approach to Delirium Assessment, Prevention & Management Cohort 1: Stephanie Jarvis, CNS, Seniors Health System Kuldeep Chahal, ELS, Hospital
Hospital Transition Management. Barbara Wood, BSN, MBA
 Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Diabetes Quality Improvement Initiative
 Diabetes Quality Improvement Initiative Community Care of North Carolina 2300 Rexwoods Drive, Ste. 100 Raleigh, NC 27607 (919) 745-2350 www.communitycarenc.org 2007 Background The Clinical Directors of
Diabetes Quality Improvement Initiative Community Care of North Carolina 2300 Rexwoods Drive, Ste. 100 Raleigh, NC 27607 (919) 745-2350 www.communitycarenc.org 2007 Background The Clinical Directors of
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care
 Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care Charles G Macias MD, MPH Chief Clinical Systems Integration Officer Director of Evidence-Based Outcomes
Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care Charles G Macias MD, MPH Chief Clinical Systems Integration Officer Director of Evidence-Based Outcomes
Approved Care Model for Project 3gi: Integration of Palliative Care into the PCMH Model
 1 Approved Care Model for Project 3gi: Integration of Palliative Care into the PCMH Model OneCity Health Webinar January 13, 2016 Overview of presentation 2 Approach to care model development Project overview
1 Approved Care Model for Project 3gi: Integration of Palliative Care into the PCMH Model OneCity Health Webinar January 13, 2016 Overview of presentation 2 Approach to care model development Project overview
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
NYSPFP HIIN: VAE/Delirium Prevention. Operationalizing the Pain, Agitation and Delirium Assessments
 NYSPFP HIIN: VAE/Delirium Prevention Operationalizing the Pain, Agitation and Delirium Assessments March 28, 2017 1 Agenda Topic Welcome and Introductions A Guide for Success: Implementing the Confusion
NYSPFP HIIN: VAE/Delirium Prevention Operationalizing the Pain, Agitation and Delirium Assessments March 28, 2017 1 Agenda Topic Welcome and Introductions A Guide for Success: Implementing the Confusion
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
Asthma: Evaluate and Improve Your Practice
 Potential Barriers and Suggested Ideas for Change Key Activity: Initial assessment and management Rationale: The history and physical examination obtained from the patient and family interviews form the
Potential Barriers and Suggested Ideas for Change Key Activity: Initial assessment and management Rationale: The history and physical examination obtained from the patient and family interviews form the
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
Buprenorphine Order Set and Rapid Access Referral. Copyright 2017, CAMH
 2 Buprenorphine Order Set and Rapid Access Referral 1 Agenda Problem Identification / Identification Importance / Importance Baseline Workflow Baseline Workflow Baseline Data Baseline Data Objectives Solution
2 Buprenorphine Order Set and Rapid Access Referral 1 Agenda Problem Identification / Identification Importance / Importance Baseline Workflow Baseline Workflow Baseline Data Baseline Data Objectives Solution
Category Code Procedure description
 Supplemental Table 1: ICD-9 codes for procedures/surgeries Category Code Procedure description Cesarean 74 Cesarean Section And Removal Of Fetus Cesarean 74.0 Classical cesarean section Cesarean 74.1 Low
Supplemental Table 1: ICD-9 codes for procedures/surgeries Category Code Procedure description Cesarean 74 Cesarean Section And Removal Of Fetus Cesarean 74.0 Classical cesarean section Cesarean 74.1 Low
Ensuring Safety of Anticoagulation Therapy
 Ensuring Safety of Anticoagulation Therapy Abha Agrawal, MD, FACP Chief Medical Officer Kings County Hospital Clinical Associate Dean SUNY Downstate College of Medicine Brooklyn, NY NYACP Webinar April
Ensuring Safety of Anticoagulation Therapy Abha Agrawal, MD, FACP Chief Medical Officer Kings County Hospital Clinical Associate Dean SUNY Downstate College of Medicine Brooklyn, NY NYACP Webinar April
What are Appropriate End-points for Delirium Prevention/Treatment Studies
 What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University
 Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University Crit Care Med. 2004;32(4):955 62. BMJ. 2015;350:h2538. Background Delirium, defined as acute brain
Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University Crit Care Med. 2004;32(4):955 62. BMJ. 2015;350:h2538. Background Delirium, defined as acute brain
Cambia Palliative Care Metrics: Where are we and where are we going?
 Cambia Palliative Care Metrics: Where are we and where are we going? J. Randall Curtis, MD, MPH Director, Cambia Palliative Care Center of Excellence www.uwpalliativecarecenter.com Overview of System-Wide
Cambia Palliative Care Metrics: Where are we and where are we going? J. Randall Curtis, MD, MPH Director, Cambia Palliative Care Center of Excellence www.uwpalliativecarecenter.com Overview of System-Wide
In each hospital-year, we calculated a 30-day unplanned. readmission rate among patients who survived at least 30 days
 Romley JA, Goldman DP, Sood N. US hospitals experienced substantial productivity growth during 2002 11. Health Aff (Millwood). 2015;34(3). Published online February 11, 2015. Appendix Adjusting hospital
Romley JA, Goldman DP, Sood N. US hospitals experienced substantial productivity growth during 2002 11. Health Aff (Millwood). 2015;34(3). Published online February 11, 2015. Appendix Adjusting hospital
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
EFFECT OF ABCDE BUNDLE IMPLEMENTATION DELIRIUM IN INTENSIVE CARE UNIT PATIENTS ON PREVALENCE OF. Delirium Assessment. 1.0 Hour
 Delirium Assessment EFFECT OF ABCDE BUNDLE IMPLEMENTATION ON PREVALENCE OF DELIRIUM IN INTENSIVE CARE UNIT PATIENTS By Mandy Bounds, RN, MSN, CCRN, Stacey Kram, RN-BC, DNP, PCCN, CCRN, Karen Gabel Speroni,
Delirium Assessment EFFECT OF ABCDE BUNDLE IMPLEMENTATION ON PREVALENCE OF DELIRIUM IN INTENSIVE CARE UNIT PATIENTS By Mandy Bounds, RN, MSN, CCRN, Stacey Kram, RN-BC, DNP, PCCN, CCRN, Karen Gabel Speroni,
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Geriatric Medicine I) OBJECTIVES
 OBJECTIVES") Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Kress, J.P. (2009). Early physical and occupational therapy in mechanically
CRITICALLY APPRAISED PAPER (CAP) Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Kress, J.P. (2009). Early physical and occupational therapy in mechanically
16 th Annual IHA Stakeholders Meeting Session 2C
 16 th Annual IHA Stakeholders Meeting Session 2C September 19, 2017 Hilton Los Angeles Airport Thank you to our Content Partner: Medication Adherence AppleCare Pharmacy Programs Confidential and proprietary.
16 th Annual IHA Stakeholders Meeting Session 2C September 19, 2017 Hilton Los Angeles Airport Thank you to our Content Partner: Medication Adherence AppleCare Pharmacy Programs Confidential and proprietary.
CUSP 4 MVP-VAP Patient Care Bundle
 Spontaneous Awakening and Spontaneous Breathing Trials, Literature Synopsis CUSP 4 MVP-VAP Patient Care Bundle Spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT) reduce the length
Spontaneous Awakening and Spontaneous Breathing Trials, Literature Synopsis CUSP 4 MVP-VAP Patient Care Bundle Spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT) reduce the length
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
CARE OF THE ADULT COPD PATIENT
 CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
The Severe Illness Management System (SIMS) Platform: Initial Implementation in Western Uganda
 Platform: Initial Implementation in Western Uganda") The Severe Illness Management System (SIMS) Platform: Initial Implementation in Western Uganda J. Lucian Davis, MD, MAS Epidemiology of Microbial Diseases Pulmonary, Critical Care, & Sleep Medicine Lucian.Davis@yale.edu
The Severe Illness Management System (SIMS) Platform: Initial Implementation in Western Uganda J. Lucian Davis, MD, MAS Epidemiology of Microbial Diseases Pulmonary, Critical Care, & Sleep Medicine Lucian.Davis@yale.edu
Delirium Assessment and the assessment of people at risk
 Assessment and the assessment of people at risk Tracey Mc Erlain Burns RGN, Dip N (lond), MBA, Chief Nurse The Rotherham NHS Foundation Trust What is delirium? Historically seen as a person who is confused/
Assessment and the assessment of people at risk Tracey Mc Erlain Burns RGN, Dip N (lond), MBA, Chief Nurse The Rotherham NHS Foundation Trust What is delirium? Historically seen as a person who is confused/
NYSPFP HIIN: VAE/Delirium Prevention. Operationalizing Prevention Strategies in the ICU
 NYSPFP HIIN: VAE/Delirium Prevention Operationalizing Prevention Strategies in the ICU 1 Agenda Time Topic Speakers 9:00 a.m.-9:10 a.m. Welcome & Introductions NYSPFP Staff 9:10 a.m.-10:40 am Why Prevent
NYSPFP HIIN: VAE/Delirium Prevention Operationalizing Prevention Strategies in the ICU 1 Agenda Time Topic Speakers 9:00 a.m.-9:10 a.m. Welcome & Introductions NYSPFP Staff 9:10 a.m.-10:40 am Why Prevent
Diabetes Care begins with Diabetes Prevention. Neha Sachdev, MD Janet Williams, MA
 Diabetes Care begins with Diabetes Prevention Neha Sachdev, MD Janet Williams, MA Objectives Describe the clinical practice burden and trends in type 2 diabetes Review evidence for diabetes prevention
Diabetes Care begins with Diabetes Prevention Neha Sachdev, MD Janet Williams, MA Objectives Describe the clinical practice burden and trends in type 2 diabetes Review evidence for diabetes prevention
Development of Guidelines to Manage Geriatric Trauma Patients. Kelly Czarnecki MS,FNP
 Development of Guidelines to Manage Geriatric Trauma Patients Kelly Czarnecki MS,FNP No Disclosures Disclosures Project Introduction According to best practice recommendations the geriatric trauma population
Development of Guidelines to Manage Geriatric Trauma Patients Kelly Czarnecki MS,FNP No Disclosures Disclosures Project Introduction According to best practice recommendations the geriatric trauma population
The Cost Burden of Worsening Heart Failure in the Medicare Fee For Service Population: An Actuarial Analysis
 Client Report Milliman Client Report The Cost Burden of Worsening Heart Failure in the Medicare Fee For Service Population: An Actuarial Analysis Prepared by Kathryn Fitch, RN, MEd Principal and Healthcare
Client Report Milliman Client Report The Cost Burden of Worsening Heart Failure in the Medicare Fee For Service Population: An Actuarial Analysis Prepared by Kathryn Fitch, RN, MEd Principal and Healthcare
The Pain of a Fractured Neck of Femur. Ms Fiona Nielsen- Project Lead
 The Pain of a Fractured Neck of Femur - Project Lead Our health service 75,000 in-patients 165,000 out-patients 900 beds 6,200 staff 70,000 emergency attendances #NOF Presentations 2010-2011- 262 2011-2012-
The Pain of a Fractured Neck of Femur - Project Lead Our health service 75,000 in-patients 165,000 out-patients 900 beds 6,200 staff 70,000 emergency attendances #NOF Presentations 2010-2011- 262 2011-2012-
Longitudinal Care Management. September 2016
 Longitudinal Care Management September 2016 Risk Score Assignment of Longitudinal CM Other C M Referral sources Screening: Need CM? Clinical Assessment tools Program Services Integrated Care Management
Longitudinal Care Management September 2016 Risk Score Assignment of Longitudinal CM Other C M Referral sources Screening: Need CM? Clinical Assessment tools Program Services Integrated Care Management
Pain Management and Safe use of opioids in hospitals. Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN
 Pain Management and Safe use of opioids in hospitals Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN Bronx Care Health System Bronx Lebanon Hospital Concourse/ Fulton division, Nursing
Pain Management and Safe use of opioids in hospitals Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN Bronx Care Health System Bronx Lebanon Hospital Concourse/ Fulton division, Nursing
Antithrombotics: Percent of patients with an ischemic stroke or TIA prescribed antithrombotic therapy at discharge. Corresponding
 Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
It Takes A Village to Curb the Prescription Opioid Epidemic: Supply healthcare providers with resources to improve patient safety
 Session L6 This presenter has nothing to disclose It Takes A Village to Curb the Prescription Opioid Epidemic: CDC Efforts Jan Losby, PhD Team Lead, Overdose Prevention Health Systems Team Division of
Session L6 This presenter has nothing to disclose It Takes A Village to Curb the Prescription Opioid Epidemic: CDC Efforts Jan Losby, PhD Team Lead, Overdose Prevention Health Systems Team Division of
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Suicide Prevention in New York State: Zero Suicide Initiative. Ann Sullivan, MD, OMH Commissioner NASMHPD Annual Commissioners Meeting August 7, 2016
 Suicide Prevention in New York State: Zero Suicide Initiative Ann Sullivan, MD, OMH Commissioner NASMHPD Annual Commissioners Meeting August 7, 2016 2 Community Based Suicide Prevention Schools: Sources
Suicide Prevention in New York State: Zero Suicide Initiative Ann Sullivan, MD, OMH Commissioner NASMHPD Annual Commissioners Meeting August 7, 2016 2 Community Based Suicide Prevention Schools: Sources
Complex evaluation of polytrauma in intensive care with multiple severity scores
 UNIVERSITY OF MEDICINE AND PHARMACY CRAIOVA DOCTORAL SCHOOL PhD THESIS Complex evaluation of polytrauma in intensive care with multiple severity scores Superviser Coordinator Prof. Univ. Dr. Florea Purcaru
UNIVERSITY OF MEDICINE AND PHARMACY CRAIOVA DOCTORAL SCHOOL PhD THESIS Complex evaluation of polytrauma in intensive care with multiple severity scores Superviser Coordinator Prof. Univ. Dr. Florea Purcaru
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Integration of Specialty Care into ACOs: Considering JMAP and Beyond
 Integration of Specialty Care into ACOs: Considering JMAP and Beyond The Seventh National Accountable Care Organization Summit Scott A. Berkowitz MD MBA Senior Medical Director, Accountable Care, Johns
Integration of Specialty Care into ACOs: Considering JMAP and Beyond The Seventh National Accountable Care Organization Summit Scott A. Berkowitz MD MBA Senior Medical Director, Accountable Care, Johns
Re-Admit It! Transitions of Care for Heart Failure PPA Annual Conference October 2018 Christopher Tanski PharmD, BCPS Cardiology Pharmacist SOCRATIVE
 Re-Admit It! Transitions of Care for Heart Failure PPA Annual Conference October 2018 Christopher Tanski PharmD, BCPS Cardiology Pharmacist SOCRATIVE ROOM CODE: SOC-36515031 Disclosures: I have no financial
Re-Admit It! Transitions of Care for Heart Failure PPA Annual Conference October 2018 Christopher Tanski PharmD, BCPS Cardiology Pharmacist SOCRATIVE ROOM CODE: SOC-36515031 Disclosures: I have no financial
Implementing Rapid Response Teams (RRT) National Call September 13, 2007
 National Call September 13, 2007") Implementing Rapid Response Teams (RRT) National Call September 13, 2007 Purpose By the end of this call, participants will have: Heard successes and learnings from Improvement Teams Updated information
Implementing Rapid Response Teams (RRT) National Call September 13, 2007 Purpose By the end of this call, participants will have: Heard successes and learnings from Improvement Teams Updated information
Risk Mitigation in Bundled Payment
 Risk Mitigation in Bundled Payment When to Hold Them and When To Fold Them Lily Pazand, MPH NYU Langone Medical Center Jonathan Pearce, MBA, CPA, FHFMA Singletrack Analytics Jessica Walradt, MS Association
Risk Mitigation in Bundled Payment When to Hold Them and When To Fold Them Lily Pazand, MPH NYU Langone Medical Center Jonathan Pearce, MBA, CPA, FHFMA Singletrack Analytics Jessica Walradt, MS Association
TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS
 TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS Challenges and Opportunities Providing Medication Assisted Treatment (Buprenorphine) August 18, 2016 SPEAKERS TODAY Nilesh Kalyanaraman, MD, Chief Health
TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS Challenges and Opportunities Providing Medication Assisted Treatment (Buprenorphine) August 18, 2016 SPEAKERS TODAY Nilesh Kalyanaraman, MD, Chief Health
Treating Emergency Room Opioid Withdrawal with Buprenorphine
 Treating Emergency Room Opioid Withdrawal with Buprenorphine Monday, February 11th (3:45pm 4:30pm) Room W314B Christine Bucago, Advanced Practice Clinical Leader (Nursing), CAMH Jane Paterson, Director,
Treating Emergency Room Opioid Withdrawal with Buprenorphine Monday, February 11th (3:45pm 4:30pm) Room W314B Christine Bucago, Advanced Practice Clinical Leader (Nursing), CAMH Jane Paterson, Director,
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program. Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN
 Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN Challenge, Journey, Evolution Everest is 29, 035 ft. 5 ½
Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN Challenge, Journey, Evolution Everest is 29, 035 ft. 5 ½
Fall Risk Assessment Content Review Questions
 Fall Risk Assessment Content Review Questions 1. What percentage of inpatient falls results in a serious injury? A. 10% B. 15% C. 30% D. Less than 1% 2. When an elderly person falls, they psychologically
Fall Risk Assessment Content Review Questions 1. What percentage of inpatient falls results in a serious injury? A. 10% B. 15% C. 30% D. Less than 1% 2. When an elderly person falls, they psychologically
Supplementary Online Content
 Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
Systematic Improvement of Diabetes Care in the Inpatient Setting
 Success Story Systematic Improvement of Diabetes Care in the Inpatient Setting EXECUTIVE SUMMARY Texas Children s Hospital is improving the care delivery of its patients with diabetes, one of the most
Success Story Systematic Improvement of Diabetes Care in the Inpatient Setting EXECUTIVE SUMMARY Texas Children s Hospital is improving the care delivery of its patients with diabetes, one of the most
Palliative Care: A Business Analysis of the Pros and Cons of Establishing a Palliative Care Program
 1 Palliative Care: A Business Analysis of the Pros and Cons of Establishing a Palliative Care Program Daniel Maison, MD Larry Oberst, CPA Spectrum Health 2 Faculty Information Daniel Maison, MD FAAHPM
1 Palliative Care: A Business Analysis of the Pros and Cons of Establishing a Palliative Care Program Daniel Maison, MD Larry Oberst, CPA Spectrum Health 2 Faculty Information Daniel Maison, MD FAAHPM
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Falls Risk Screening, Assessment, and Referral
 Falls Risk Screening, Assessment, and Referral Kady Reese, MPH, CPHQ Lana Comstock, MSN, RN Iowa Fall Symposium July 13, 2017 Goals Identify risk assessment tools for varied patient populations Recite
Falls Risk Screening, Assessment, and Referral Kady Reese, MPH, CPHQ Lana Comstock, MSN, RN Iowa Fall Symposium July 13, 2017 Goals Identify risk assessment tools for varied patient populations Recite
Patricia Bax, RN, MS August 17, Reaching New York State Tobacco Users through Opt-to-Quit
 Patricia Bax, RN, MS August 17, 2015 Reaching New York State Tobacco Users through Opt-to-Quit Good Afternoon! Welcome Roswell Park Cessation Services and Opt-to-Quit Overview Featured Site: Stony Brook
Patricia Bax, RN, MS August 17, 2015 Reaching New York State Tobacco Users through Opt-to-Quit Good Afternoon! Welcome Roswell Park Cessation Services and Opt-to-Quit Overview Featured Site: Stony Brook
Health Services & High Risk Admissions Registries. David Carnahan, MD MSCE DHA CEI Branch Chief 12 June 2014
 Health Services & High Risk Admissions Registries David Carnahan, MD MSCE DHA CEI Branch Chief 12 June 2014 Introduction Background Information Variables of Interest (potential markers) ACG Use case Readmissions
Health Services & High Risk Admissions Registries David Carnahan, MD MSCE DHA CEI Branch Chief 12 June 2014 Introduction Background Information Variables of Interest (potential markers) ACG Use case Readmissions
Stop Delirium! A complex intervention for delirium in care homes for older people
 Stop Delirium! A complex intervention for delirium in care homes for older people Final report Summary September 2009 1 Contents Abstract...3 Lay Summary...4 1. Background...6 2. Objectives...6 3. Methods...7
Stop Delirium! A complex intervention for delirium in care homes for older people Final report Summary September 2009 1 Contents Abstract...3 Lay Summary...4 1. Background...6 2. Objectives...6 3. Methods...7
Dana L. Gilbert Chief Operating Officer Sharon Rudnick Vice President Outpatient Care Management
 Ambulatory Sensitive Admissions Dana L. Gilbert Chief Operating Officer Sharon Rudnick Vice President Outpatient Care Management 1 Sites Of Care Advocate Health Care 12 Hospitals 10 acute care hospitals
Ambulatory Sensitive Admissions Dana L. Gilbert Chief Operating Officer Sharon Rudnick Vice President Outpatient Care Management 1 Sites Of Care Advocate Health Care 12 Hospitals 10 acute care hospitals
Knowledge to Practice; Applying New Skills
 Knowledge to Practice; Applying New Skills Linda R. Greene, RN, BS, MPS,CIC UR Highland Hospital Rochester, NY linda_greene@urmc.rochester.edu Kim M. Delahanty, RN, BSN, PHN,MBA/HCM,CIC UCSD Health System
Knowledge to Practice; Applying New Skills Linda R. Greene, RN, BS, MPS,CIC UR Highland Hospital Rochester, NY linda_greene@urmc.rochester.edu Kim M. Delahanty, RN, BSN, PHN,MBA/HCM,CIC UCSD Health System
SmartIX EMPI Taking It to the Next Level
 SmartIX EMPI Taking It to the Next Level Theresa Mendoza Director of Quality, BI, and Data Services Dallas-Fort Worth Education and Research Foundation Agenda Welcome Introduction History Next Level of
SmartIX EMPI Taking It to the Next Level Theresa Mendoza Director of Quality, BI, and Data Services Dallas-Fort Worth Education and Research Foundation Agenda Welcome Introduction History Next Level of
FINANCES OF PALLIATIVE CARE
 FINANCES OF PALLIATIVE CARE Andrew Molosky, MBA Vice President of Operations Seasons Hospice & Palliative Care Learning Objectives: Distinguish and identify the unique needs of one's organization as it
FINANCES OF PALLIATIVE CARE Andrew Molosky, MBA Vice President of Operations Seasons Hospice & Palliative Care Learning Objectives: Distinguish and identify the unique needs of one's organization as it
AdvaMed Medtech Value Assessment Framework in Practice
 AdvaMed Medtech Value Assessment Framework in Practice Application of the Medtech Value Assessment Framework to Cymedica s e-vive System Value Framework Overview In response to the growing need to demonstrate
AdvaMed Medtech Value Assessment Framework in Practice Application of the Medtech Value Assessment Framework to Cymedica s e-vive System Value Framework Overview In response to the growing need to demonstrate
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Delirium Undetected: The impact of allied health care professional documentation on delirium detection in hospitalized elders
 Delirium Undetected: The impact of allied health care professional documentation on delirium detection in hospitalized elders Sheryl Hodgson Canadian Geriatrics Society April 20, 2018 Disclosure Presenter:
Delirium Undetected: The impact of allied health care professional documentation on delirium detection in hospitalized elders Sheryl Hodgson Canadian Geriatrics Society April 20, 2018 Disclosure Presenter:
Rapid Response Teams. January 17, Safe Table Webinar
 Rapid Response Teams January 17, 2017 Safe Table Webinar Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project
Rapid Response Teams January 17, 2017 Safe Table Webinar Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project
Integrating delirium measurement into your research. Edward R. Marcantonio, M.D., S.M. CEDARTREE Bootcamp November 8, 2016.
 Integrating delirium measurement into your research Edward R. Marcantonio, M.D., S.M. CEDARTREE Bootcamp November 8, 2016 Outline Selection of an appropriate measure Training of delirium assessors Ongoing
Integrating delirium measurement into your research Edward R. Marcantonio, M.D., S.M. CEDARTREE Bootcamp November 8, 2016 Outline Selection of an appropriate measure Training of delirium assessors Ongoing
NoCVA Preventing Avoidable Readmissions Collaborative. Pre-work: Assessing Risk April 21, 2014
 NoCVA Preventing Avoidable Readmissions Collaborative Pre-work: Assessing Risk April 21, 2014 Agenda Context Collaborative Overview Setting up to succeed Why assess risk of readmission Methods to assess
NoCVA Preventing Avoidable Readmissions Collaborative Pre-work: Assessing Risk April 21, 2014 Agenda Context Collaborative Overview Setting up to succeed Why assess risk of readmission Methods to assess
TACKLING COPD READMISSIONS. Wendy Presley RN
 TACKLING COPD READMISSIONS Wendy Presley RN WHY START WITH COPD? HIGH VOLUME PROBLEM PRONE COSTLY And you just can t resist a challenge Chronic Obstructive Pulmonary Disease (COPD) is a preventable and
TACKLING COPD READMISSIONS Wendy Presley RN WHY START WITH COPD? HIGH VOLUME PROBLEM PRONE COSTLY And you just can t resist a challenge Chronic Obstructive Pulmonary Disease (COPD) is a preventable and
Respiratory Failure & Pneumonia Definitions Workgroup
 Respiratory Failure & Pneumonia Definitions Workgroup Purpose To develop standard clinical definitions on select diagnoses & categories to be used consistently across all hospitals in Maryland Definitions
Respiratory Failure & Pneumonia Definitions Workgroup Purpose To develop standard clinical definitions on select diagnoses & categories to be used consistently across all hospitals in Maryland Definitions
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Pulmonary and Critical Care
 Pulmonary and Critical Care 2015-2016 DRAFT REPORT FOR COMMENT April 21, 2016 This report is funded by the Department of Health and Human Services under contract HHSM-500-2012-00009I Task Order HHSM-500-T0000
Pulmonary and Critical Care 2015-2016 DRAFT REPORT FOR COMMENT April 21, 2016 This report is funded by the Department of Health and Human Services under contract HHSM-500-2012-00009I Task Order HHSM-500-T0000
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
Strategies for Enhancing Sepsis Survivorship
 Strategies for Enhancing Sepsis Survivorship Hallie Prescott, MD, MSc Ohio Hospital Association August 16, 2016 Disclosures I have no relevant financial conflicts of interest Key Funding NIH/NIGMS American
Strategies for Enhancing Sepsis Survivorship Hallie Prescott, MD, MSc Ohio Hospital Association August 16, 2016 Disclosures I have no relevant financial conflicts of interest Key Funding NIH/NIGMS American
MULTICARE Health System Care of the Adult Chronic Obstructive Pulmonary Disease (COPD) Patient
 Patient") Clinical Guideline Ver. 2.0 MULTICARE Health System Care of the Adult Chronic Obstructive Pulmonary Disease (COPD) Patient Target Audience: The target audience for this clinical guideline is all MHS providers
Clinical Guideline Ver. 2.0 MULTICARE Health System Care of the Adult Chronic Obstructive Pulmonary Disease (COPD) Patient Target Audience: The target audience for this clinical guideline is all MHS providers