Anesthetic Depth, Ventilation and Fluids: Too Much or Too Little
|
|
|
- Peregrine Eaton
- 6 years ago
- Views:
Transcription
1 Anesthetic Depth, Ventilation and Fluids: Too Much or Too Little Kevin K. Tremper, PhD MD Professor & Chair Department of Anesthesiology University of Michigan
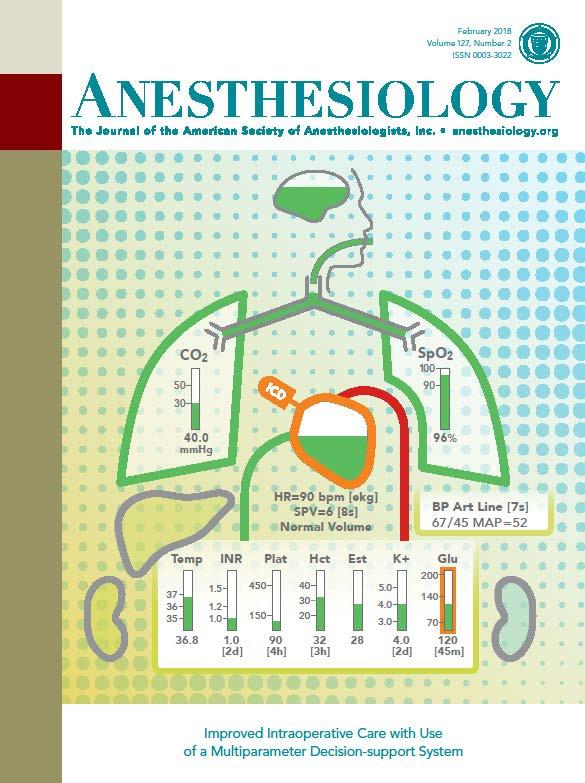
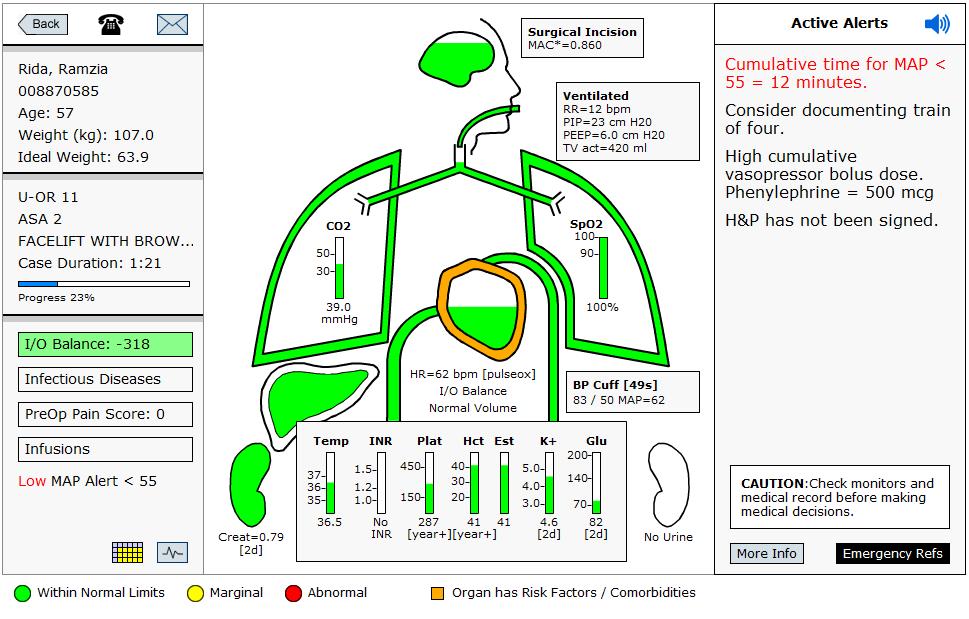
2 Disclosure COI I have several software patents granted (through the U of Michigan) regarding display technology. I am the founder, President and have an equity position in AlertWatch, a U of Michigan Startup Company (
3
4
5 AlertWatch User vs Non-User 6 yrs and 26,769 cases Process Measures: P values Hypotension < 55 mmhg <0.001 Crystalloid ml/kg/hr <0.001 Tidal Volume 6-8 ml/kg Ideal BW <0.001 Clinical Outcomes: MI 1.5% vs 2.6% vs 2.1%.. Versus no difference AKI. No difference Resource Differences: LOS 5 days vs 6 days <0.001 Hospital Charges $3,603 less for AW patients
6 History and Controversies: Goals: To be knowledgeable of the history, controversies and current thoughts regarding: 1. Anesthetic Depth/Recall 2. Ventilation 3. Fluid Management
7
8 1. Anesthetic Depth MAC vs Awareness/Recall
9 Minimum Alveolar Anesthetic Concentration, MAC: A Standard of Anesthetic Potency Edmond Eger, Lawrence Saidman and Bernard Brandstater Anesthesiology 1965
10 After 15 min of Equilibration (Inspired = Expired) 1. Tail Clamp, 30 sec 2. Electrical Stim; 10, 20 & 30 msec we found 10 to 15 volts very painful when place on our own forearms 3. Move ETT cm Flank Incision 5. Paw Clamp
11 After 15 min of Equilibration (Inspired = Expired) 1. Tail Clamp, 30 sec 2. Electrical Stim; 10, 20 & 30 msec we found 10 to 15 volts very painful when place on our own forearms 3. Move ETT cm Flank Incision 5. Paw Clamp They also varied:co2, O2,BP, Hemorrhage


12 Ether Day October 16, 1846 The First Public Demonstration W.T.G. Morton
13 Awareness/Recall First Case was Gilbert Abbott Morton s First demonstration of Postoperative Recall? Feels like my neck s been scratched
14 Incidence? Awareness vs Recall Isolated Forearm Test (IFT): Tunstall ME, BJA 1974: Awareness Tunstall ME, BJA 1980: Awareness During C-sec During C-sec requested to stay awake by hand signals to hear her baby, felt no pain. JD Pandit view: Awareness is a continuum Russell & Wang: Awareness is all or none, BJA 2015 Up to 30% of Patients will respond to Move your hand under a MAC of 1.0 or a BIS of < 60
15 Brice Questionnaire 1.What was the last thing you remember before going to sleep? 2.The First thing you remember when you wake up. 3.Do you remember anything between? 4.Did you dream?.. At 24 hrs and 30 days Brice, Hetherington and Utting Br J Anesth 1970
16 Incidence? Awareness with Recall Sebel :800 Pollard :14,560
17 Incidence? Awareness with Recall Sebel :800 Pollard :14,560 Joint Commission 2004/2008 ASA Practice Advisory 2006
18 The B-Aware Trial Randomized Double Blinded BIS vs No BIS 2463 pts: 1,225 BIS vs 1,238 No BIS Awareness 2 vs 11 P <0.02 (1:600) (1:100) Number needed to Tx 138 ($2,200/pt) Myles et al The Lancet 2004
19 B-Unaware Trial 2,000 High Risk Patients* Randomized BIS vs ETAG ( >60) (MAC< 0.7) Brice Interview at 24 hrs and 30 days Avidan et al NEJM 2008
20 B-Unaware Trial 2,000 High Risk Patients* Randomized BIS vs ETAG (>60) (MAC< 0.7) Brice Interview at 24 hrs and 30 days 2 patients in each group had Recall Avidan et al NEJM 2008
21 B-Unaware Trial 2,000 High Risk Patients* Randomized BIS vs ETAG (>60) (MAC< 0.7) Brice Interview at 24 hrs and 30 days 2 patients in each group had Recall BIS Didn't Help Avidan et al NEJM 2008
22 ASA... What to Do? BIS a Standard of Care?
23 ASA... What to Do? BIS a Standard of Care? ASA/FAER RFP $1,000,000 Jan 2008 Mike Avidan $500,000; Wash U George Mashour $500,000; U of M
24 WHERE TO START? 1. What is our incidence? (need to know to determine sample size, Power analysis) 2. How to account for Infusion anesthetics?... Propofol, Dex
25 WHERE TO START? 1. What is our incidence? (need to know to determine sample size, Power analysis) 2. How to account for Infusion anesthetics?... Propofol, Dex 3. Need a Scale?
26 WHERE TO START? 1. What is our incidence? (need to know to determine sample size, Power analysis) 2. How to account for Infusion anesthetics?... Propofol, Dex Need to develop an new MAC equation 3. Need a Scale? MACI 1 through 5 with D
27 Incidence of Self Reported Awareness/Recall A review of 116,478 post op visits Most common in MAC and Regional Case? They expected complete amnesia and we provided it 90% of the time. After GA = 1/4401 Mashour GA, et al. Anesth Analg 2009; 108(2): Esaki RK, Mashour GA. Anesth Analg 2009; 108(5):
28 A Novel Electronic Algorithm for Detecting Potentially Insufficient Anesthesia MAC Aware equation was retrospectively applied to 4 yrs of cases including 12 awareness cases MAC* < 0.5 (age adjusted) highest likelihood Mashour et al J Clin Mon & Comp; 2009
29 MAC Aware MAC (Minimum Alveolar Concentration) Formula MAC* = Propofol rate (in mcg/kg/min) / Demedetomidine adjustment + (Expired Sevoflurane / Expired Isoflurane / Expired Desflurane / Expired Nitrous / 104) x 10 ( x (age of patient 40))
30 A NOVEL CLASSIFICATION INSTRUMENT FOR INTRAOPERATIVE AWARENESS EVENTS: MACI (Michigan Awareness Classification Interment ) Class: 1 Auditory perceptions 2 Tactile perceptions 3 Pain 4 Paralysis 5 Paralysis & Pain D modifier if associated with Distress Mashour et al A & A 2010
31 3 & 4 Years later... Avidan & Mashour NEJM 2011 Mashour & Avidan Anesthesiology 2012 A total of 27,314 consented & interviewed patients
32 3 & 4 Years later... Avidan & Mashour NEJM 2011 Mashour & Avidan Anesthesiology 2012 A total of 27,314 consented & interviewed patients In both High and Normal Risk Patients Use of BIS did Not reduce the incidence of Awareness with Postop Recall
33 Incidence of Definite Awareness Avidan et al; High Risk Pts: NEJM 2011 BIS Alert = 7/2,861 (0.24%) Agent Alert = 2/2852 (0.07%) Mashour; General Pts: Anesth 2012 Over All = 19/18,836 (0.1%) BIS Alert = 0.08% Agent Alert = 0.12% No Alert = 0.38%; P< 0.006
34 Awareness Events by Class
35 Exclusion Criteria 1. All these studies excluded Pure TIVA 2. The equation does not include Ketamine * or Midazolam * BIS doesn t work with Ketamine anyway
36 1. Anesthetic Depth Conclusions: 1. Incidence about 1:1, BIS? Unless High Risk/Pure TIVA (no N2O) & Relaxant 3. Some Type of MAC Alert Helps 4. Inform Patients receiving MAC Anesthesia/Regional of Recall
37 What about Triple Low/ Double Low? Triple Low = Low BIS & BP & MAC Associate with Hospital Stay and Mortality Sessler etal Anesth 2013 Not Associated with Mortality Kertai etal Anesth 2014
38 2. Ventilation
39 Why did we/ I use 10 ml/kg tidal volumes & RR of 10 in the OR? 1963
40 A Concept of Atelectasis Declines in PaO 2 and compliance reversible with hyperinflation maneuvers PEEP had not been invented yet Bendixen et al. NEJM 1963;269:
41 Bendixen et al Conclusions: PaO2 decrease with time could be reversed by passive hyperinflation 2. Continuous use of large tidal volumes or periodic deep breaths are essential in preventing increased variable shunt 3. Large tidal volume appears to protect against falls in oxygen tension
42 Result TV = 10 ml/kg RR = 10 (whoever saw a RR of 10 on the floor?) Became a standard for 50 yrs!!! Easy to multiply
:1301-08.")
43 VENTILATION WITH LOWER TIDAL VOLUMES AS COMPARED WITH TRADITIONAL TIDAL VOLUMES FOR ACUTE LUNG INJURY AND THE ACUTE RESPIRATORY DISTRESS SYNDROME The Acute Respiratory Distress Syndrome Network. NEJM 2000;342(18):
44 ARDS Net Trial NEJM 2000 The Acute Respiratory Distress Syndrome Network. NEJM 2000;342(18):

45 ARDS Net Trial NEJM ml/kg Ideal Body Weight The Acute Respiratory Distress Syndrome Network. NEJM 2000;342(18):

46
47 TV 6-8 vs PEEP 6-8 vs 0 RM 30 for 30 every 30 Emmanuel Futier, M.D. et al, NEJM Sept 2013
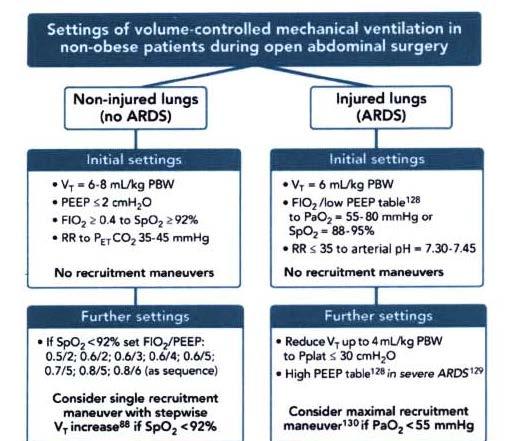
48 Lung Protective Ventilation Study A Trial of Intraoperative Low Tidal Volume Ventilation in Abdominal Surgery 400 pts ( ) TV 6-8 vs PEEP 6-8 vs 0 RM 30 cm for 30 sec every 30 min Emmanuel Futier, M.D. et al, NEJM Sept 2013
49 Lung protective ventilation study Emmanuel Futier, M.D. et al NEJM Sept % 10.5% Lots of questions/controversy To whom does this apply? etc.
50 Letter's to the Editor 1. Blum et al Control not standard of care 2. Lam et al Micro aspiration caused bad outcomes, PEEP would have prevented Mynbaev et al Open versus laparoscopic not equal in each group CO2. Blah Blah Blah.
51 Trend in median TV by quarter Bender et al A&A 2017
52
53 29,343 patient records reviewed

54 29,343 patient records reviewed Use of low intraoperative TV with minimal PEEP is associated with an increase risk of 30-day mortality.
55
56 2. Ventilation Conclusions: 1. 6 to 8 ml/kg IBW 2. PEEP 5 or Greater 3. Recruitment Helpful Is it TV, PEEP, Recruitment or all three??? This makes sense... Until further notice
57 3. Fluid Management
58 3. Fluid Management Too Much of a Good Thing 1. Blood Volume 2. I s and O s 3. Fluids 4. Goal Directed Fluid Therapy
59 Estimate Blood Volume Men = 75 ml/kg Women = 65 ml/kg Infants = 80 ml/kg Neonates = 90 ml/kg
60 Estimate Blood Volume Men = 75 ml/kg Women = 65 ml/kg Infants = 80 ml/kg Neonates = 90 ml/kg What about obese patients? Fat about 60 ml/kg? BMI Adjustment?
61 Prediction of blood volume in normal human adults 155 volunteers Angola State Prison Farm (92 men, 63 women) Ages 17 to 90 Weights 80 to 390 lbs Radio-tagged RBCs to measure EBV Nadler et al Surgery 1962
62 Prediction of blood volume in normal human adults To fit the data he used an IBM electronic digital computer... a Herculean task by any other method EBV= xH xW (for men) Nadler et al Surgery 1962
63 I s & O s: Old school IN s: Crystalloid/Colloid/Blood (accurate) OUT s: 1. Insensible losses (accurate?) 2. Urine Output (accurate) 3. EBL (not even close to accurate) 4. 3 rd Space Losses (does it exist)

64 4:2:1 Rule Santorio Santorio ( )
65 Blood Transfusion Management Transfusion Trigger & 1 to 1 to 1 (Back to Whole Blood) I m not going to Cover this
66 Crystalloid vs Colloid Crystalloid: Blood 3 to 1 Crystalloid: Colloid 3 to 1?
67 Cortés, et al. Anesthesia & Analgesia, 2015
68 3 rd Space Losses Surgical Trauma/Edema/Evaporation Low 2 ml/kg/hr Moderate 4 ml/kg/hr High 6 ml/kg/hr Seems like a lot? Miller s Anesthesia 2010
69 3 rd Space Losses Where did this come from? & Where did it go?
70 3 rd Space Losses Studies in the 1960 s using radio tagged Alb, RBCs note fluid shifts with larger abdominal surgery Shires et al Ann Surgery 1961 Moore et al N Engl J Med 1958
71 3 rd Space Losses Improved Surgical Techniques, less tissue trauma, Laparoscopic Approaches etc Doherty et al Intraoperative Fluids: How Much is Too Much. Br J Anaesth 2012
72 EBL In 42 of 140 cases EBL < ABL* If ABL < 500 ; EBL OK If ABL > 500 ; EBL underestimated * Actual Blood Loss Ram et al,chinese J of Traumatology 2014
73 Goal Directed Fluid Therapy GDT is defined as: 1. Any use of hemodynamic monitoring and therapies during the perioperative period to achieve a predetermined hemodynamic end point 2. Explicit Protocol to achieve end points Using PACs, Fluids, inotropes...
74 Goal Directed Fluid Therapy Based on original studies by Shoemaker Supranormal DO2 CCM 1988 Used PAC and Colloid Tx Replaced by noninvasive Stroke Volume techniques 1. Esophageal Doppler: 2. Pulse Contour: Thoracic Bioimpedance *


75 Several Methodologies to Estimate Stroke Volume
76 Protocols to Optimize SV 1. Induce GA 2. Measure SV 3. Place in Trendelenberg If SV increases Tx Hespan 4. Supine, Re-measure/repeat until SV does not increase NHS Department of Health (2013) Innovation Health & Wealth. Operative Fluid Management (website in handout)
77 Meta Analysis of GDT Mortality Reduced only in High Risk Group: > 20% Expected Mortality! Cecconi et al Critical Care 2013
78 More Recent Studies OPTIMISE Study Group (European Study, Multicenter) Pts Randomized GDT vs Usual Care GI Surgery 2. Study Group: LiDCOrapid to max SV with Colloid and Dopexamine Results: No Difference Conclusion: GDT did not reduce complications or 30 day mortality Pearse et al JAMA 2014
79 More Recent Studies COGUIDE: Stens et al Anaesthesia 2017 Abd Surgery: cc Nexfin Edwards
80 More Recent Studies COGUIDE: Stens et al Anaesthesia 2017 Abd Surgery: cc Nexfin Edwards Results : No difference in Outcome Complication Rate: GDT Group 46.8% Controls 44.7%

81 More Recent Studies Gomez-Izquierdo, et al. Anesthesiology 2017 Using an esophageal Doppler (DP12 Probe; Deltex Medical Ltd., UH) Randomized Control Trial Elective Lap Colorectal: Ileus 218 Pts in ERAS program; GDT did not improve postop ileus
82 Great Editorial D Murry, Anaesthesia 2017 It does work but...
83 Great Editorial D Murry, Anaesthesia 2017 It does work but... we are using the wrong statistics
84 Great Editorial D Murry, Anaesthesia 2017 It does work but... we are using the wrong statistics we are unable to prove it
85 Great Editorial D Murry, Anaesthesia 2017 It does work but... we are using the wrong statistics we are unable to prove it only as part of a bundle of care
86 Great Editorial D Murry, Anaesthesia 2017 It does work but... we are using the wrong statistics we are unable to prove it only as part of a bundle of care it is not deliverable
87 Great Editorial D Murry, Anaesthesia 2017 It does work but... we are using the wrong statistics we are unable to prove it only as part of a bundle of care it is not deliverable we need to work on how to deliver it
88 Great Editorial D Murry, Anaesthesia 2017 It does work but... we are using the wrong statistics we are unable to prove it only as part of a bundle of care it is not deliverable we need to work on how to deliver it Or maybe it just doesn t work
89 Avoid Hypotension Avoid Fluid Overload Avoid Awareness Avoid Vasopressors What s left?
90 Avoid Hypotension Avoid Fluid Overload Avoid Awareness Avoid Vasopressors What s left? The Knowns, The Unknowns and the Unknown Unknowns
91 SPV (Electronic & Manual) PPV Mathis, et al Anesthesiology, 2017
92 SPV (Electronic & Manual) PPV I Love SPV! Mathis, et al Anesthesiology, 2017
93 3. Fluid Management Conclusions: Aim for Zero Balance 1. Short, low EBL Cases: I s & O s (no 3 rd ) 2. Larger, Longer, Higher EBL: SPV & Vasopressors (Neo/Vaso/Norepi)? 3. Big Cases Central Monitoring &/TEE
94 The New Goal Directed Fluid Therapy 1. Preop euvolemia: Drink Clears up to 2 hr 2. Avoid Bowel Prep 3. Intraop zero fluid Balance 4. Objective measure for larger procedures 5. Postop oliguria OK Gupta and Gan Anaesthesia 2016
Intraoperative Fluid Management. David G Hovord BA MB BChir FRCA Clinical Assistant Professor University of Michigan
 Intraoperative Fluid Management David G Hovord BA MB BChir FRCA Clinical Assistant Professor University of Michigan Objectives Examine impact of perioperative renal failure, and discuss structure and function
Intraoperative Fluid Management David G Hovord BA MB BChir FRCA Clinical Assistant Professor University of Michigan Objectives Examine impact of perioperative renal failure, and discuss structure and function
Fluid management. Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center
 Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Hypotension after induction, corrected with 20 mg ephedrine x cc LR EBL 250cc Urine output:
 Terry C. Wicks, CRNA, MHS Catawba Valley Medical Center Hickory, North Carolina 63 y.o., 5 2, 88 kg female for hand assisted laparoscopic tranversecolectomy Co-morbidities include: Hypertension controlled
Terry C. Wicks, CRNA, MHS Catawba Valley Medical Center Hickory, North Carolina 63 y.o., 5 2, 88 kg female for hand assisted laparoscopic tranversecolectomy Co-morbidities include: Hypertension controlled
Perioperative Goal- Protocol Summary
 Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Perioperative Goal- Protocol Summary
 Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
WHICH CARDIAC OUTPUT MONITOR IN COLORECTAL ENHANCED RECOVERY? :
 WHICH CARDIAC OUTPUT MONITOR IN COLORECTAL ENHANCED RECOVERY? : RANDOMISED CONTROLLED NON-INFERIORITY TRIAL COMPARING LiDCOrapid AND OESOPHAGEAL DOPPLER MONITORS J van Dellen, S McCorkell, AB Williams
WHICH CARDIAC OUTPUT MONITOR IN COLORECTAL ENHANCED RECOVERY? : RANDOMISED CONTROLLED NON-INFERIORITY TRIAL COMPARING LiDCOrapid AND OESOPHAGEAL DOPPLER MONITORS J van Dellen, S McCorkell, AB Williams
Goal Directed Therapy
 Goal Directed Therapy Dr Maurizio Cecconi MD FRCA FFICM MD(Res) Consultant and Reader Anaesthesia and Intensive Care Medicine St George s University Hospital NHS Foundation Trust St George s University
Goal Directed Therapy Dr Maurizio Cecconi MD FRCA FFICM MD(Res) Consultant and Reader Anaesthesia and Intensive Care Medicine St George s University Hospital NHS Foundation Trust St George s University
Perioperative Fluid Management in ERPs
 Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Continuous monitoring of cardiac output: why and how
 33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
Fluid Balance in an Enhanced Recovery Pathway. Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017
 Fluid Balance in an Enhanced Recovery Pathway Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017 No Disclosures 2 Introduction The optimal intravenous fluid regimen
Fluid Balance in an Enhanced Recovery Pathway Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017 No Disclosures 2 Introduction The optimal intravenous fluid regimen
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Section 8: Accidental awareness during general anaesthesia
 Risks associated with your anaesthetic Section 8: Accidental awareness during general anaesthesia Summary This leaflet explains what accidental awareness is during an anaesthetic. During a general anaesthetic
Risks associated with your anaesthetic Section 8: Accidental awareness during general anaesthesia Summary This leaflet explains what accidental awareness is during an anaesthetic. During a general anaesthetic
SECTION 8: ACCIDENTAL AWARENESS DURING GENERAL ANAESTHESIA
 Risks associated with your anaesthetic SECTION 8: ACCIDENTAL DURING GENERAL ANAESTHESIA When you have a general anaesthetic, you become unconscious. The anaesthetist decides how much anaesthetic you need
Risks associated with your anaesthetic SECTION 8: ACCIDENTAL DURING GENERAL ANAESTHESIA When you have a general anaesthetic, you become unconscious. The anaesthetist decides how much anaesthetic you need
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
BIS Monitoring. ASSESSMENT OF DEPTH OF ANAESTHESIA. Why measure depth of anaesthesia? or how to avoid. awareness in one easy lesson
 BIS Monitoring or how to avoid www.eurosiva.org awareness in one easy lesson ASSESSMENT MONITORING ANAESTHETIC DEPTH OF DEPTH OF ANAESTHESIA Why measure depth of anaesthesia? How do the various EEG monitors
BIS Monitoring or how to avoid www.eurosiva.org awareness in one easy lesson ASSESSMENT MONITORING ANAESTHETIC DEPTH OF DEPTH OF ANAESTHESIA Why measure depth of anaesthesia? How do the various EEG monitors
Depth of Anesthesia Monitoring in Cardiac Surgery. Adam Dryden MD, FRCPC University of Ottawa Heart Institute
 Depth of Anesthesia Monitoring in Cardiac Surgery Adam Dryden MD, FRCPC University of Ottawa Heart Institute Depth of Anesthesia Monitoring in Cardiac Surgery Because it s not all about the heart. The
Depth of Anesthesia Monitoring in Cardiac Surgery Adam Dryden MD, FRCPC University of Ottawa Heart Institute Depth of Anesthesia Monitoring in Cardiac Surgery Because it s not all about the heart. The
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Edwards Critical Care Education. Perioperative Goal-Directed Therapy Protocol Summary
 Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: November 2014 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: November 2014 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Kent CD: Awareness during general anesthesia: ASA Closed Claims Database and Anesthesia Awareness Registry. ASA Newsletter 74(2): 14-16, 2010
: 14-16, 2010") Citation Kent CD: Awareness during general anesthesia: ASA Closed Claims Database and Anesthesia Awareness Registry. ASA Newsletter 74(2): 14-16, 2010 Full Text Asked repeatedly, Abbott confirmed repeatedly
Citation Kent CD: Awareness during general anesthesia: ASA Closed Claims Database and Anesthesia Awareness Registry. ASA Newsletter 74(2): 14-16, 2010 Full Text Asked repeatedly, Abbott confirmed repeatedly
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
Actualités sur le remplissage peropératoire. Philippe Van der Linden MD, PhD
 Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Perioperative Goal Directed Therapy Improving the Quality of Care for Our Surgical Patients
 Perioperative Goal Directed Therapy Improving the Quality of Care for Our Surgical Patients DESIRÉE CHAPPELL, CRNA ERAS TEAM LEAD NORTON AUDUBON HOSPITAL, LOUISVILLE, KY Disclosure Edwards Lifesciences,
Perioperative Goal Directed Therapy Improving the Quality of Care for Our Surgical Patients DESIRÉE CHAPPELL, CRNA ERAS TEAM LEAD NORTON AUDUBON HOSPITAL, LOUISVILLE, KY Disclosure Edwards Lifesciences,
PREVENT COMPLICATIONS IN MAJOR SURGERY
 PREVENT COMPLICATIONS IN MAJOR SURGERY Dept of Anesthesia and ICM (Prof. G. Della Rocca) Azienda Ospedaliero-Universitaria University of Udine. Udine, Italy CLINICAL TRIAL OF SURVIVORS CARDIORESPIRATORY
PREVENT COMPLICATIONS IN MAJOR SURGERY Dept of Anesthesia and ICM (Prof. G. Della Rocca) Azienda Ospedaliero-Universitaria University of Udine. Udine, Italy CLINICAL TRIAL OF SURVIVORS CARDIORESPIRATORY
Kinetics and Monitoring of Inhaled Anesthetics. Copyright , James H Philip, all rights reserved
 Kinetics and Monitoring of Inhaled Anesthetics Copyright 1980-2014, James H Philip, all rights reserved Ready Kinetics and Monitoring of Inhaled Anesthetics James H. Philip, M.E.(E.), M.D. Anesthesiologist
Kinetics and Monitoring of Inhaled Anesthetics Copyright 1980-2014, James H Philip, all rights reserved Ready Kinetics and Monitoring of Inhaled Anesthetics James H. Philip, M.E.(E.), M.D. Anesthesiologist
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Jan M. Headley, R.N. BS
 Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Edwards Critical Care Education. Perioperative Goal-Directed Therapy Protocol Summary
 Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: March 2013 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: March 2013 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Awareness during anesthesia: A rare but disturbing complication According to the American Society of Anesthesiologists
 ECRI Institute Perspectives Awareness during anesthesia: A rare but disturbing complication According to the American Society of Anesthesiologists (ASA), intraoperative awareness with recall occurs when
ECRI Institute Perspectives Awareness during anesthesia: A rare but disturbing complication According to the American Society of Anesthesiologists (ASA), intraoperative awareness with recall occurs when
Family Feud SPA Myron Yaster, MD
 Family Feud SPA 2014 Myron Yaster, MD Richard J Traystman Professor, Departments of Anesthesiology, Critical Care Medicine, Pediatrics, and Neurosurgery The Johns Hopkins Medical Institutions Aubrey Maze,
Family Feud SPA 2014 Myron Yaster, MD Richard J Traystman Professor, Departments of Anesthesiology, Critical Care Medicine, Pediatrics, and Neurosurgery The Johns Hopkins Medical Institutions Aubrey Maze,
Disclaimer. Improving MET-based patient care using treatment algorithms. Michael R. Pinsky, MD, Dr hc. Different Environments Demand Different Rules
 Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
BIS Technology Enabling safety and quality improvements in the cardiac operating room
 BIS Technology Enabling safety and quality improvements in the cardiac operating room BIS technology backs you up with proven brain monitoring. Using the BIS monitor has made me more of a scientist and
BIS Technology Enabling safety and quality improvements in the cardiac operating room BIS technology backs you up with proven brain monitoring. Using the BIS monitor has made me more of a scientist and
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Edwards Critical Care Education. Perioperative Goal-Directed Therapy Protocol Summary
 Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: March 2013 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: March 2013 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Hyperthermic Intra PEritoneal Chemotherapy:
 Hyperthermic Intra PEritoneal Chemotherapy: Does the anaesthesiological strategy differ from other extensive abdominal strategies? Dr V. Billard, Département d anesthésie Preoperative assessment Eligibility
Hyperthermic Intra PEritoneal Chemotherapy: Does the anaesthesiological strategy differ from other extensive abdominal strategies? Dr V. Billard, Département d anesthésie Preoperative assessment Eligibility
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
福島県立医科大学学術成果リポジトリ. Title laparoscopic adrenalectomy in patie pheochromocytoma. Midori; Iida, Hiroshi; Murakawa, Ma
 福島県立医科大学学術成果リポジトリ Examination of the usefulness of no Title variation monitoring for adjusting laparoscopic adrenalectomy in patie pheochromocytoma Isosu, Tsuyoshi; Obara, Shinju; Oha Author(s) Atsuyuki;
福島県立医科大学学術成果リポジトリ Examination of the usefulness of no Title variation monitoring for adjusting laparoscopic adrenalectomy in patie pheochromocytoma Isosu, Tsuyoshi; Obara, Shinju; Oha Author(s) Atsuyuki;
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Respiratory Depression in the Early Postoperative Period. Toby N Weingarten, MD Mayo Clinic Professor Anesthesiology
 Respiratory Depression in the Early Postoperative Period Toby N Weingarten, MD Mayo Clinic Professor Anesthesiology Conflicts of Interest Medtronic Chair of CEC Committee for PRODIGY Trial Merck Investigator
Respiratory Depression in the Early Postoperative Period Toby N Weingarten, MD Mayo Clinic Professor Anesthesiology Conflicts of Interest Medtronic Chair of CEC Committee for PRODIGY Trial Merck Investigator
Effect of peak inspiratory pressure on the development. of postoperative pulmonary complications.
 Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
If you reduce variability in volume administration, HOW. you can reduce post-surgical complications, LOS and associated costs 1-4
 A large body of clinical evidence* demonstrates If you reduce variability in volume administration, you can reduce post-surgical complications, LOS and associated costs 1-4 Complications Too Dry Too Wet
A large body of clinical evidence* demonstrates If you reduce variability in volume administration, you can reduce post-surgical complications, LOS and associated costs 1-4 Complications Too Dry Too Wet
Hemodynamic Optimization HOW TO IMPLEMENT?
 Hemodynamic Optimization HOW TO IMPLEMENT? Why Hemodynamic Optimization? Are post-surgical complications exceptions? Patients undergoing surgery may develop post-surgical complications. The morbidity rate,
Hemodynamic Optimization HOW TO IMPLEMENT? Why Hemodynamic Optimization? Are post-surgical complications exceptions? Patients undergoing surgery may develop post-surgical complications. The morbidity rate,
Inhalational Anesthesia. Munir Gharaibeh, MD, PhD, MHPE School of Medicine The University of Jordan February, 2018
 Inhalational Anesthesia School of Medicine The University of Jordan February, 2018 mgharaib@ju.edu.jo Inhalational Anesthesia n Gases or volatile liquids n Administration and Elimination is by the lungs
Inhalational Anesthesia School of Medicine The University of Jordan February, 2018 mgharaib@ju.edu.jo Inhalational Anesthesia n Gases or volatile liquids n Administration and Elimination is by the lungs
Goal-Directed Fluid Therapy: A New Way of Thinking. Ji Su Jenny Kim & Logan D. MacLean SRNA, BSN, CCRN DNP Candidates
 Goal-Directed Fluid Therapy: A New Way of Thinking Ji Su Jenny Kim & Logan D. MacLean SRNA, BSN, CCRN DNP Candidates Goal-Directed Fluid Therapy Map History of Fluid Management Significance of Fluid Management
Goal-Directed Fluid Therapy: A New Way of Thinking Ji Su Jenny Kim & Logan D. MacLean SRNA, BSN, CCRN DNP Candidates Goal-Directed Fluid Therapy Map History of Fluid Management Significance of Fluid Management
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
 Dr.Ahmad farooq") Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
W J A. World Journal of Anesthesiology. Awareness during anesthesia: Current status in Japan. Abstract INTRODUCTION MINIREVIEWS.
 W J A World Journal of Anesthesiology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5313/wja.v5.i3.62 World J Anesthesiol 2016 November 27;
W J A World Journal of Anesthesiology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5313/wja.v5.i3.62 World J Anesthesiol 2016 November 27;
Tarek M Sarhan, Assistant professor of Anesthesiology, Faculty of Medicine, Alexandria University
 7 ANALGESIA FOR TRACHEOESOPHAGEAL FISTULA REPAIR IN NEONATES : A COMPARISON OF SINGLE SHOT THORACIC PARAVERTEBRAL BLOCK AND EPIDURAL BLOCK WITH ROPIVACAINE Tarek M Sarhan, Assistant professor of Anesthesiology,
7 ANALGESIA FOR TRACHEOESOPHAGEAL FISTULA REPAIR IN NEONATES : A COMPARISON OF SINGLE SHOT THORACIC PARAVERTEBRAL BLOCK AND EPIDURAL BLOCK WITH ROPIVACAINE Tarek M Sarhan, Assistant professor of Anesthesiology,
Anesthesia for OutPatient Spine Surgery. Michael A. Kellams, D.O.
 Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
NONINVASIVE/MINIMALLY INVASIVE HEMODYNAMIC MONITORING
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
SEEING KETAMINE IN A NEW LIGHT
 SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
Can Depth of Anesthesia Monitoring Alter the Incidence of Mortality, POCD or Delirium?
 Can Depth of Anesthesia Monitoring Alter the Incidence of Mortality, POCD or Delirium? John C. Drummond, M.D., FRCPC Professor of Anesthesiology, University of California, San Diego; Staff Anesthesiologist,
Can Depth of Anesthesia Monitoring Alter the Incidence of Mortality, POCD or Delirium? John C. Drummond, M.D., FRCPC Professor of Anesthesiology, University of California, San Diego; Staff Anesthesiologist,
Role of Robotic Surgery in Endometrial Cancer: New Expensive Gadget or the Future?
 Role of Robotic Surgery in Endometrial Cancer: New Expensive Gadget or the Future? Kathleen Yang, MD, FACOG Northwest Gynecologic Oncology Willamette Valley Cancer Institute Disclosure I have nothing to
Role of Robotic Surgery in Endometrial Cancer: New Expensive Gadget or the Future? Kathleen Yang, MD, FACOG Northwest Gynecologic Oncology Willamette Valley Cancer Institute Disclosure I have nothing to
General Anesthesia. Mohamed A. Yaseen
 General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
"Gentlemen, this is no humbug" Dr John Collins Warren, 17 October : Horace Wells 1846: William T. Morton
 "Gentlemen, this is no humbug" Dr John Collins Warren, 17 October 1846 1844: Horace Wells 1846: William T. Morton Characteristic differences between anesthesia and sleep Anesthesia Sleep Onset Maintenance
"Gentlemen, this is no humbug" Dr John Collins Warren, 17 October 1846 1844: Horace Wells 1846: William T. Morton Characteristic differences between anesthesia and sleep Anesthesia Sleep Onset Maintenance
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Protecting the Lungs
 Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Awareness: Where do we stand?
 1 Awareness: Where do we stand? Peter J. Davis, M.D. Professor of Anesthesiology and Pediatrics University of Pittsburgh School of Medicine Anesthesiologist-in-Chief Children s Hospital of Pittsburgh 2
1 Awareness: Where do we stand? Peter J. Davis, M.D. Professor of Anesthesiology and Pediatrics University of Pittsburgh School of Medicine Anesthesiologist-in-Chief Children s Hospital of Pittsburgh 2
Monitoring cortical electrical activity in anesthesia for obese patient
 Monitoring cortical electrical activity in anesthesia for obese patient Gabriel M. Gurman, M.D. Division of Anesthesiology Soroka Medical Center and Faculty of Health Sciences, Ben Gurion University Beer
Monitoring cortical electrical activity in anesthesia for obese patient Gabriel M. Gurman, M.D. Division of Anesthesiology Soroka Medical Center and Faculty of Health Sciences, Ben Gurion University Beer
Neuro Quiz 25 - Monitoring
 Neuro Quiz 25 - Monitoring This quiz is being published on behalf of the Education Committee of the SNACC Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey, PA Quiz Team Shobana
Neuro Quiz 25 - Monitoring This quiz is being published on behalf of the Education Committee of the SNACC Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey, PA Quiz Team Shobana
Cricoid pressure: useful or dangerous?
 Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
The cornerstone of treating patients with hypotension,
 Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense* Paul E. Marik, MD, FCCM 1 ; Rodrigo Cavallazzi, MD 2 Background: Aim: Data Sources:
Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense* Paul E. Marik, MD, FCCM 1 ; Rodrigo Cavallazzi, MD 2 Background: Aim: Data Sources:
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL. Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
Evaluation of Postoperative Complications Occurring in Patients after Desflurane or Sevoflurane in Outpatient Anaesthesia: A Comparative Study
 Original article Evaluation of Postoperative Complications Occurring in Patients after Desflurane or Sevoflurane in Outpatient Anaesthesia: A Comparative Study Shishir Ramachandra Sonkusale 1, RajulSubhash
Original article Evaluation of Postoperative Complications Occurring in Patients after Desflurane or Sevoflurane in Outpatient Anaesthesia: A Comparative Study Shishir Ramachandra Sonkusale 1, RajulSubhash
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Anesthesia and the beach chair position
 Anesthesia and the beach chair position Paul Picton Associate Professor Senior Associate Chair of Clinical Affairs and Quality University of Michigan Medical School, Ann Arbor NIH UL1TR000433 Disclosures
Anesthesia and the beach chair position Paul Picton Associate Professor Senior Associate Chair of Clinical Affairs and Quality University of Michigan Medical School, Ann Arbor NIH UL1TR000433 Disclosures
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012
 Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Feline Anesthesia Fluid Therapy Treatment of Anesthetic Complications
 Feline Anesthesia Fluid Therapy Treatment of Anesthetic Complications Rebecca A. Krimins, DVM, MS April 29, 2018 DCVR Annual Spring Symposium Email: drkrimins@gmail.com Cat Anesthesia There is no single
Feline Anesthesia Fluid Therapy Treatment of Anesthetic Complications Rebecca A. Krimins, DVM, MS April 29, 2018 DCVR Annual Spring Symposium Email: drkrimins@gmail.com Cat Anesthesia There is no single
Bariatric Surgery. Keitha Kirkham RN, BScN
 Bariatric Surgery Keitha Kirkham RN, BScN Civic Campus BMI Obesity Definition Underweight with BMI lower than 20 Normal weight with a BMI between 20 and 25 Overweight with a BMI between 25 and 30 Obese
Bariatric Surgery Keitha Kirkham RN, BScN Civic Campus BMI Obesity Definition Underweight with BMI lower than 20 Normal weight with a BMI between 20 and 25 Overweight with a BMI between 25 and 30 Obese
Pharmacokinetics. Inhalational Agents. Uptake and Distribution
 Pharmacokinetics Inhalational Agents The pharmacokinetics of inhalational agents is divided into four phases Absorption Distribution (to the CNS Metabolism (minimal Excretion (minimal The ultimate goal
Pharmacokinetics Inhalational Agents The pharmacokinetics of inhalational agents is divided into four phases Absorption Distribution (to the CNS Metabolism (minimal Excretion (minimal The ultimate goal
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER
 SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
PiCCO based algorithms
 European Society of Anaesthesiologists Annual Meeting 12.-15. June 2010, Helsinki, Finland PiCCO based algorithms Berthold Bein, MD, PhD, DEAA Department of Anaesthesiology and Intensive Care Medicine
European Society of Anaesthesiologists Annual Meeting 12.-15. June 2010, Helsinki, Finland PiCCO based algorithms Berthold Bein, MD, PhD, DEAA Department of Anaesthesiology and Intensive Care Medicine
Intro Who should read this document 2 Key practice points 2 What is new in this version 3 Background 3 Guideline Subsection headings
 Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Inhalational Agents in Bariatric Procedures
 Inhalational Agents in Bariatric Procedures Overweight The term overweight signifies an excess body weight when compared to established standards. This weight may derive from muscle, bone, fat, and/or
Inhalational Agents in Bariatric Procedures Overweight The term overweight signifies an excess body weight when compared to established standards. This weight may derive from muscle, bone, fat, and/or
Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient
 Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient Katherine W. Arendt, M.D. Associate Professor of Anesthesiology Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient Katherine W. Arendt, M.D. Associate Professor of Anesthesiology Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Fluid responsiveness Monitoring in Surgical and Critically Ill Patients
 Fluid responsiveness Monitoring in Surgical and Critically Ill Patients Impact clinique de la Goal-directed-therapy Patrice FORGET, M.D Cliniques universitaires Saint Luc Université catholique de Louvain,
Fluid responsiveness Monitoring in Surgical and Critically Ill Patients Impact clinique de la Goal-directed-therapy Patrice FORGET, M.D Cliniques universitaires Saint Luc Université catholique de Louvain,
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2): Oxford University Press
: Oxford University Press") Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
A SAFE AND EFFECTIVE WAY TO OPTIMIZE ANESTHESIA DURING SURGERY
 Clinical Evidence Guide A SAFE AD EFFECTIVE WAY TO OPTIMIZE AESTHESIA DURIG SURGERY Bispectral Index (BIS) Complete Monitoring System This guide will help you review the clinical evidence that supports
Clinical Evidence Guide A SAFE AD EFFECTIVE WAY TO OPTIMIZE AESTHESIA DURIG SURGERY Bispectral Index (BIS) Complete Monitoring System This guide will help you review the clinical evidence that supports
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Procedural Sedation. Conscious Sedation AAP Sedation Guidelines: Disclosures. What does it mean for my practice? We have no disclosures
 2016 AAP Sedation Guidelines: What does it mean for my practice? Amber P. Rogers MD FAAP Assistant Professor of Section of Hospital Medicine and Anesthesiology Corrie E. Chumpitazi MD FAAP FACEP Assistant
2016 AAP Sedation Guidelines: What does it mean for my practice? Amber P. Rogers MD FAAP Assistant Professor of Section of Hospital Medicine and Anesthesiology Corrie E. Chumpitazi MD FAAP FACEP Assistant
Enhanced Recovery in Pediatric Surgery
 Enhanced Recovery in Pediatric Surgery Diana L Diesen, M.D., FACS Assistant Professor, Department of Surgery University of Texas Southwestern Medical Center Children s Health Dallas Dallas, Tx Disclosures
Enhanced Recovery in Pediatric Surgery Diana L Diesen, M.D., FACS Assistant Professor, Department of Surgery University of Texas Southwestern Medical Center Children s Health Dallas Dallas, Tx Disclosures
AVOIDING THE CRASH 3: RELAX, OPTIMAL POST-AIRWAY MANAGEMENT AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Full Disclosure. The case for why it matters. Goal-directed Fluid Resuscitation
 Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies