Romayne Gallagher MD, CCFP Divisions of Residential and Palliative Care Providence Health Care Vancouver, BC
|
|
|
- Arnold Cummings
- 6 years ago
- Views:
Transcription



1 Romayne Gallagher MD, CCFP Divisions of Residential and Palliative Care Providence Health Care Vancouver, BC
2 My father s memory may be gone but otherwise he is all there Daughter of 92 yr old in wheelchair, advanced dementia with anorexia and dysphagia All she needs is a little fluid and then she pops right back Family of 97 year old with advanced dementia after multiple trips to ER for rehydration
3 We need to make him eat because he has NPH insulin daily Nurse of resident with brain tumor and DM The licensing board monitors weights of the residents on a monthly basis to prevent elder abuse Dietician speaking of trying to keep weight stable in residents with advanced disease
4 She has become less responsive could it be the increase in the opioid dose? Nurse of advanced dementia resident on opioids for months for pain, open leg ulcers, temp = 39C, RR 24 Yes but are they distressed? Physician after being told that resident s respiratory rate is 44
5 Therapies to modify disease or improve function Palliative Care Presentation Therapies to relieve suffering and/or improve quality of life 6m Bereavement Care Death
6 Number of persons between ages 20 and Number of persons 20 to 64 to each person Wiener J. from US Census data

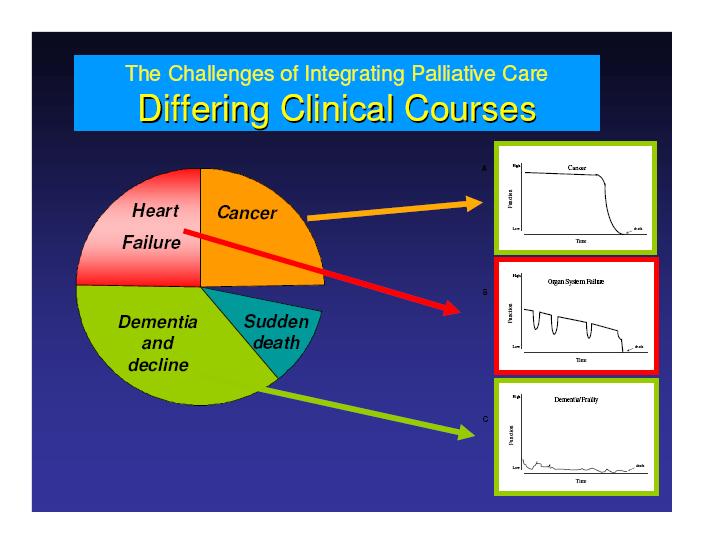
7 Prognosis often uncertain, right up to the end of life A patient with serious chronic heart failure has chance to live 6 months on the day before death Labeling some patients as palliative and others not will not work Is RAI-MDS helpful?
8
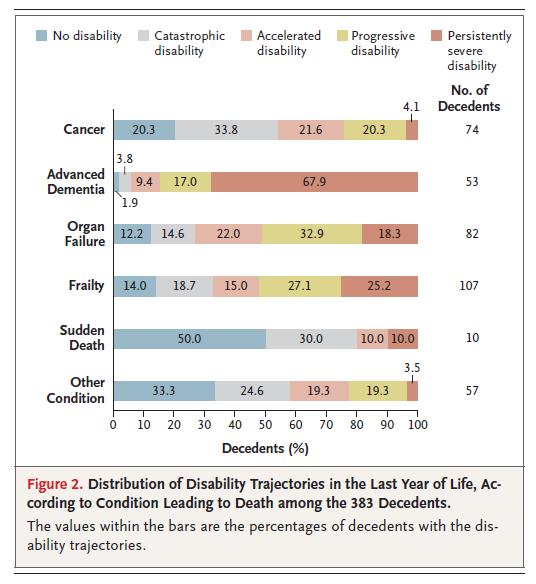
9 Gill et al. NEJM 2010
10
11 Make it part of your practice It is an approach to care combined with specific knowledge and skill set Know how to access palliative care teams and when you would need them Complex symptom management Complex family or psychosocial needs Goals of care not certain

12 Therapies to modify disease and/or improve function Residential Care Palliative Approach Presentation Therapies to relieve suffering and/or improve quality of life Death Bereavement Care
13 Symptom-based approach to care Outcomes based on resolution of symptoms rather than disease indices Understanding patient and family life goals Care for body/mind/spirit Improve quality of living
14 Prevalence exceeds 50% in residential care Antipsychotics are usual drug of choice Atypical antipsychotics associated with increased CVA and mortality Chronic pain in residential care: 50-80% prevalence Neuropathic pain common
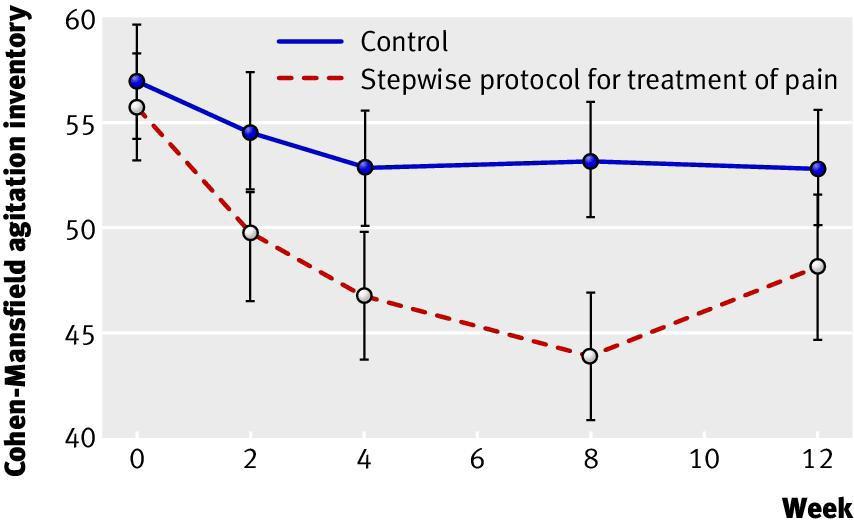
15 Cluster randomized trial of a stepwise protocol for pain and its effect on BPSD 352 moderate to severe dementia patients Randomized to stepwise pain medication vs usual care over 8 weeks Followed agitation, aggression, pain observation scales, function, cognition at baseline, during and after trial Husebo et al. BMJ 2011
16
17 Most therapy trials exclude patients over 70 due to reduced ability to complete study Most trials are based on a single disease in order to assess effect of drug/therapy The outcomes are based on disease indices rather than quality of life outcomes
18 Tight glycemic control may not improve dementia, and may worsen cognition Poor control may worsen cognition. Hyperglycemia (hyperosmolar state) and hypoglycemia can both precipitate delirium. J Am Geriatr Soc. 2003; 51(5 suppl):s265-s280 Diabetes Care 1998; 21:
19 Atypical presentation: personality change, ADL change, delirium, obtundation. Many predisposing factors: Age-related decrease in gluconeogenesis Unawareness (reduced adrenergic symptoms, underlying dementia) Under-nutrition Polypharmacy Social isolation
20 Establish patient s health goals and preferences. Help patient to prioritize treatment options for diabetes and other medical conditions consistent with patient s goals, the magnitude and time to benefit. Evaluate and manage geriatric syndromes. Estimate life expectancy within same agesex cohort by considering overall health and physical function. JAMA. 2006; 295:
21 Establish patient s health goals and preferences. Estimate life expectancy within same age-sex cohort by considering overall health and physical function. Consider intensive glycemic targets if: Lower risk of hypoglycemia Existing microvascular complications Life expectancy > 8 years Consider more conservative goals (symptom management) if : Higher risk of hypoglycemia (e.g. severe dementia) Heavy burden of medical illness Difficulty with drug adherence Significant risks from intensive management of vascular risks Short life expectancy JAMA. 2006; 295:
22 The End of the Disease Era Mary E. Tinetti, MD, Terri Fried, MD Am J. Med. 2004;116:


23
24 Acute care: 75% of decisions in patients with life-threatening illness Residential care: >70% of all decisions Find the process highly stressful 82% of SDM decision-makers in ICU life/death decisions had PTSD symptoms Azoulay E et al Crit. Care Med. 2005
25 Most surrogates feel unprepared May not know patient preferences May only know preferences for catastrophic situations Often use their own hopes, needs to inform their decisions Vig et al JAGS 2006; Fagerlin et al Health Psychol 2001; Vig et al J Gen Int Med 2007
26 Interviews with 246 SDM 55% agreed they made decision 75% wished decision to be shared with physician Asked if it was discussed: benefits (80%) risks (72%) option of no tube (67%) asked if they understood information (85%) 28-41% wanted more information Lewis et al. Patient Educ. Counseling 2006
27 728 adult outpatients attending Oregon internal medicine clinic 69% refusal of treatment 46% withdrawal of treatment 41% relief of symptoms vs length of life Education, being a health proxy correlated best Having an advance directive did not Silveira MJ et al. JAMA 2000; 284:
28 Semi-structured, in depth interviews with 30 elders with chronic disease and their caregivers Recurring factors affecting EOL decision making: Expected quality of life Emotional and financial cost of treatment Likelihood of treatment success Effect of treatment on longevity Rodriguez, Young. J Med. Ethics 2006
29 Over 1/3 of patients changed their preference s for life sustaining treatment over a 2 year period Illness, treatment and hospitalization influenced people s wishes The healthy are more likely to prefer death to disability
30 The skills to enable access, understanding and use of information for health The degree to which individuals have the capacity to obtain, process and understand information and services needed to make appropriate health decisions It requires more skill than literacy
31 48% of Canadians do not have adequate literacy (level 1 & 2) 60% of Canadians do not have the necessary skills to adequately manage their health (level 1 & 2 in health literacy assessment)
32 What are the factors associated with low health literacy?: Age (cognitive decline, disuse) Chronic Illness Stress Education Language

33 80 African Americans and 64 Whites visiting their family physician Health literacy measured Verbal description of advanced dementia followed by questions on preference for care Two minute video of advanced dementia followed by questions on preference for care Volandes et al. J Palliative Medicine 2008
34 After verbal description, low health literacy predicted those who choose more aggressive interventions OR After watching video there were no significant differences in preference for care by race or health literacy Volandes et al. J Palliative Medicine 2008
35 Decisions that are shared by healthcare provider(s) and person(s), informed by the best evidence available, weighted according to the specific charactaristics and values of the person(s)
36 Patient preferences for amount of information degree of involvement in decision-making preferences, values, goals etc Information presented by the clinician the nature of the condition treatment options including the option of no treatment or withdrawal of treatment risks and potential complications of the treatment the probability of success of the treatment options
37 The clinician makes a recommendation The patient/family/clinician decide on an option for treatment
38 Incorporates patient preferences, values, goals into clinical decision making Allows different models of decision-making e.g. patient decides, family decides, patient + family etc Multiple options, stressful situations, lack of surrogate or patient experience with decision-making
39 Clinicians need to communicate the connection between daily events (lack of appetite, poor swallowing, UTI, dyspnea etc ) with the natural course of the disease (increased infection risk with advanced dementia, lack of appetite is natural in all advanced illness) Clinicians must communicate the natural process of dying to families

40 THE BRAIN 27
41 What are we asking from the SDM? Their role is to represent the values and preferences of the patient/resident How we phrase our questions: what would your mother prefer if she were in this situation What would your father consider a good outcome in this situation?
42 Patients/residents/family (PFR) have a good understanding of the illness and how it manifests itself in daily life PFR understand their rights in the health care system PFR understand their responsibilities in the health care system
43 Healthcare providers (HCP) respect the decision-making styles of PFR HCP are aware of potential conflicts for SDM Healthcare providers give PFR an accurate picture of illness (in a way that PFR can understand) and prepare them for the future

44 HCP do not let their own values and beliefs alter what options are presented and how they are presented HCP understand their responsibility in shared decision-making i.e. making a recommendation HCP understand their role in responsible use of healthcare resources
45 YES Start early Don t miss an opportunity Everyone on the team can contribute Consistency of the message
46 Use plain language Drawings, visual models, videos Teach back method Ask Me 3: What is my main problem? What do I have to do? What is it important for me to do this?

47 1. What do you call your problem? 2. What has caused it? 3. Why do you think it started when it did? 4. What does it do to you? 5. How severe is it? 6. What do you fear most about it? 7. What are the chief problems it has caused you? 8. What kind of treatment do you think you should receive? 9. What do you hope for in the future? 10. What would be a good outcome for you?
48 Inquiry about advance care planning documents is built into the system The advance care directive has a specific place in the healthcare record There are triggers to inquire about the directive
49 Needs to start in chronic disease management and recur regularly in all health care settings The moving in assessment needs to include resident and SDM understanding of the medical situation and what the future holds
50 All family conferences should be viewed and used as an opportunity to educate the resident and SDM on: The current medical situation What the future will be like What kind of decisions may have to be made in the future
51
Artificial Nutrition and Hydration at End of Life (EOL)
") Artificial Nutrition and Hydration at End of Life (EOL) Sonali M Wilborn, MD, MBA National Medical Director Seasons Healthcare Management Seasons Hospice & Palliative Care 1 Objectives Define Artificial
Artificial Nutrition and Hydration at End of Life (EOL) Sonali M Wilborn, MD, MBA National Medical Director Seasons Healthcare Management Seasons Hospice & Palliative Care 1 Objectives Define Artificial
Palliative Care for Older Adults in the United States
 Palliative Care for Older Adults in the United States Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine Icahn School
Palliative Care for Older Adults in the United States Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine Icahn School
Update in Geriatrics: Choosing Wisely Primum Non Nocere
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations
 communication skills that every provider needs AND clinical triggers for PPC conversations") Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations Esmé Finlay, MD Division of Palliative Medicine University of
Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations Esmé Finlay, MD Division of Palliative Medicine University of
Brought to you by the Massachusetts Medical Society and its Committee on Geriatric Medicine
 Brought to you by the Massachusetts Medical Society and its Committee on Geriatric Medicine What is palliative care? Care focused on helping support and guide patients who have life limiting and serious
Brought to you by the Massachusetts Medical Society and its Committee on Geriatric Medicine What is palliative care? Care focused on helping support and guide patients who have life limiting and serious
PALLIATIVE CARE FOR THE HEART AND STROKE PATIENT December 8, 2017
 PALLIATIVE CARE FOR THE HEART AND STROKE PATIENT December 8, 2017 1 Faculty Disclosure Faculty: Jeff Myers, MD, MSEd, CCFP (PC) Associate Professor, University of Toronto Palliative Care Physician, Sinai
PALLIATIVE CARE FOR THE HEART AND STROKE PATIENT December 8, 2017 1 Faculty Disclosure Faculty: Jeff Myers, MD, MSEd, CCFP (PC) Associate Professor, University of Toronto Palliative Care Physician, Sinai
Communication with relatives of critically ill patients. Dr WAN Wing Lun Specialist in Critical Care Medicine Yan Chai Hospital
 Communication with relatives of critically ill patients Dr WAN Wing Lun Specialist in Critical Care Medicine Yan Chai Hospital Why is communication with relatives important? Relatives of ICU patients suffer
Communication with relatives of critically ill patients Dr WAN Wing Lun Specialist in Critical Care Medicine Yan Chai Hospital Why is communication with relatives important? Relatives of ICU patients suffer
9 End of life issues
 9 End of life issues In this part Key points: End of life issues 132 Palliative care 134 Grief and bereavement 136 130 131 Key points: End of life issues As a person with dementia approaches the end of
9 End of life issues In this part Key points: End of life issues 132 Palliative care 134 Grief and bereavement 136 130 131 Key points: End of life issues As a person with dementia approaches the end of
Dr. Andrea Johnson Saskatoon Health Region/Saskatoon Cancer Centre September 30, 2016
 Dr. Andrea Johnson Saskatoon Health Region/Saskatoon Cancer Centre September 30, 2016 Conflicts of Interest None... Our drugs are old and cheap (for the most part) so big pharma isn t really interested
Dr. Andrea Johnson Saskatoon Health Region/Saskatoon Cancer Centre September 30, 2016 Conflicts of Interest None... Our drugs are old and cheap (for the most part) so big pharma isn t really interested
Feasibility of Implementing Advance Directive in Hong Kong Chinese Elderly People
 Asia Pacific Regional Conference in End-of-Life and Palliative Care in Long Term Care Settings Feasibility of Implementing Advance Directive in Hong Kong Chinese Elderly People Dr. Patrick CHIU MBBS (HK),
Asia Pacific Regional Conference in End-of-Life and Palliative Care in Long Term Care Settings Feasibility of Implementing Advance Directive in Hong Kong Chinese Elderly People Dr. Patrick CHIU MBBS (HK),
Palliative Care: Communication. Edward W Martin MD MPH Home and Hospice Care of RI May 13, 2010
 Palliative Care: Communication Edward W Martin MD MPH Home and Hospice Care of RI May 13, 2010 End-of-Life Discussions You shouldn t have counseling at the end of life Senator Charles Grassley Aug 12 2009
Palliative Care: Communication Edward W Martin MD MPH Home and Hospice Care of RI May 13, 2010 End-of-Life Discussions You shouldn t have counseling at the end of life Senator Charles Grassley Aug 12 2009
NeuroPI Case Study: Palliative Care Counseling and Advance Care Planning
 Case: An 86 year-old man presents to your office after recently being diagnosed as having mild dementia due to Alzheimer s disease, accompanied by his son who now runs the family business. At baseline
Case: An 86 year-old man presents to your office after recently being diagnosed as having mild dementia due to Alzheimer s disease, accompanied by his son who now runs the family business. At baseline
How Can Palliative Care Help Your Patient Get Home Sooner?
 How Can Palliative Care Help Your Patient Get Home Sooner? Annette T. Carron, D.O. Director Geriatrics and Palliative Care Botsford Hospital OMED 2014 Patient Care Issues That Can Delay Your Day/ Pain
How Can Palliative Care Help Your Patient Get Home Sooner? Annette T. Carron, D.O. Director Geriatrics and Palliative Care Botsford Hospital OMED 2014 Patient Care Issues That Can Delay Your Day/ Pain
Call the National Dementia Helpline on
 128 Call the National Dementia Helpline on 1800 100 500 End of life issues 9 9 End of life issues In this part Key points: End of life issues 130 Palliative care 132 Grief and bereavement 134 For more
128 Call the National Dementia Helpline on 1800 100 500 End of life issues 9 9 End of life issues In this part Key points: End of life issues 130 Palliative care 132 Grief and bereavement 134 For more
End of Life Care in Dementia. Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals
 End of Life Care in Dementia Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals Rosie.Lockwood@sth.nhs.uk Agenda Some facts and figures What are the challenges? What is good care? How
End of Life Care in Dementia Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals Rosie.Lockwood@sth.nhs.uk Agenda Some facts and figures What are the challenges? What is good care? How
What You Need To Know About Palliative Care. Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director
 What You Need To Know About Palliative Care Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director None of the faculty, planners, speakers, providers, nor CME committee members
What You Need To Know About Palliative Care Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director None of the faculty, planners, speakers, providers, nor CME committee members
Advance Care Planning: not just for Geriatrics
 Advance Care Planning: not just for Geriatrics RAIsing Awareness, A Geriatric Refresher Day March 4, 2015 St. Elias Centre 750 Ridgewood Avenue, Ottawa ON K1B 6N1 Disclosure No conflicts of interest No
Advance Care Planning: not just for Geriatrics RAIsing Awareness, A Geriatric Refresher Day March 4, 2015 St. Elias Centre 750 Ridgewood Avenue, Ottawa ON K1B 6N1 Disclosure No conflicts of interest No
Deprescribing. Deprescribing. Webinar #12 Webinar #1 Developing Cultural Competency. Addressing EOL Issues Jessica Visco, PharmD, CGP
 August 24, 2016 Webinar #12 Webinar #1 Developing Cultural Competency in Deprescribing Addressing EOL Issues Jessica Visco, PharmD, CGP SeniorPharmAssist Kimberly S. Johnson MD MHS Associate Professor
August 24, 2016 Webinar #12 Webinar #1 Developing Cultural Competency in Deprescribing Addressing EOL Issues Jessica Visco, PharmD, CGP SeniorPharmAssist Kimberly S. Johnson MD MHS Associate Professor
Who, Me? Starting THE Conversation
 Who, Me? Starting THE Conversation Nancy Flowers, LCSW Social Work Manager Rainbow Hospice and Palliative Care nflowers@rainbowhospice.org 847-685-9900 Objectives Clarify the importance of advance directives
Who, Me? Starting THE Conversation Nancy Flowers, LCSW Social Work Manager Rainbow Hospice and Palliative Care nflowers@rainbowhospice.org 847-685-9900 Objectives Clarify the importance of advance directives
Communicating with Patients with Heart Failure and their Families
 Communicating with Patients with Heart Failure and their Families Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine
Communicating with Patients with Heart Failure and their Families Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine
Palliative Care: A Place on the Quality Scorecard?
 Palliative Care: A Place on the Quality Scorecard? J. Randall Curtis, MD, MPH Professor of Medicine Director, Palliative Care Center of Excellence www.uwpalliativecarecenter.com Disclosures and Funding
Palliative Care: A Place on the Quality Scorecard? J. Randall Curtis, MD, MPH Professor of Medicine Director, Palliative Care Center of Excellence www.uwpalliativecarecenter.com Disclosures and Funding
A Palliative Approach in Caring for the Person and Family Living with Dementia Hospice and Palliative Nurses Association (HPNA) Online Education
 Online Education") A Palliative Approach in Caring for the Person and Family Living with Dementia Anne Carr, GNP BC Anne Mahler, GCNS BC, ACHPN Created May 2017 Disclosures Anne Carr and Anne Mahler have no real or perceived
A Palliative Approach in Caring for the Person and Family Living with Dementia Anne Carr, GNP BC Anne Mahler, GCNS BC, ACHPN Created May 2017 Disclosures Anne Carr and Anne Mahler have no real or perceived
Pain in dementia. Prof Rowan Harwood Geriatrician, NUH. Disclaimer
 Pain in dementia Prof Rowan Harwood Geriatrician, NUH Disclaimer Pain What is pain? Pain Pain is what the patient says it is McCaffery 1968 Pain An unpleasant sensory or emotional experience associated
Pain in dementia Prof Rowan Harwood Geriatrician, NUH Disclaimer Pain What is pain? Pain Pain is what the patient says it is McCaffery 1968 Pain An unpleasant sensory or emotional experience associated
End of Life Care Communication and Advance Illness Care Planning. Gideon Sughrue MD May 18, 2013
 End of Life Care Communication and Advance Illness Care Planning Gideon Sughrue MD May 18, 2013 Objectives End of life Care Communication Describe Palliative Care Place in therapy What is hospice? What
End of Life Care Communication and Advance Illness Care Planning Gideon Sughrue MD May 18, 2013 Objectives End of life Care Communication Describe Palliative Care Place in therapy What is hospice? What
PALLIATIVE CARE IN NEW YORK STATE
 Collaborative for Palliative Care In collaboration with its partners End of Life Choices New York Finger Lakes Geriatric Education Center at the University of Rochester COLLABORATIVE FOR PALLIATIVE CARE
Collaborative for Palliative Care In collaboration with its partners End of Life Choices New York Finger Lakes Geriatric Education Center at the University of Rochester COLLABORATIVE FOR PALLIATIVE CARE
The Role of POLST in the Care of People with Dementia
 The Role of POLST in the Care of People with Dementia Kenneth Brummel-Smith, MD Charlotte Edwards Maguire Professor of Geriatrics Florida State University College of Medicine Objectives Describe the process
The Role of POLST in the Care of People with Dementia Kenneth Brummel-Smith, MD Charlotte Edwards Maguire Professor of Geriatrics Florida State University College of Medicine Objectives Describe the process
PART one. The Palliative Care Spectrum: Providing Care Across Settings
 PART one The Palliative Care Spectrum: Providing Care Across Settings Chapter 1 An Introduction to Palliative Pharmacy Care Jennifer M. Strickland To palliate means to alleviate. Palliative care, as the
PART one The Palliative Care Spectrum: Providing Care Across Settings Chapter 1 An Introduction to Palliative Pharmacy Care Jennifer M. Strickland To palliate means to alleviate. Palliative care, as the
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Maureen A. Malin, MD, PhD, MBA, EdD McLean Hospital, Geriatrics Program September 1, 2016
 Maureen A. Malin, MD, PhD, MBA, EdD McLean Hospital, Geriatrics Program September 1, 2016 Describe the demographics of aging and how this has shaped care needs Review evolving models of palliative and
Maureen A. Malin, MD, PhD, MBA, EdD McLean Hospital, Geriatrics Program September 1, 2016 Describe the demographics of aging and how this has shaped care needs Review evolving models of palliative and
Betty Black, EdS, PhD Building an Evidence Base for Education on Advance Care Planning
 Betty Black, EdS, PhD Building an Evidence Base for Education on Advance Care Planning Fall ADC Meeting, October 10, 2014 Baltimore, MD 1 Dementia is a Terminal Illness AD is 6 th leading cause of death
Betty Black, EdS, PhD Building an Evidence Base for Education on Advance Care Planning Fall ADC Meeting, October 10, 2014 Baltimore, MD 1 Dementia is a Terminal Illness AD is 6 th leading cause of death
Facilitating Advance Care Planning Conversations
 Facilitating Advance Care Planning Conversations Jeff Myers, MD, MSEd, CCFP Acting Provincial Clinical Lead, OPCN W. Gifford-Jones Professor in Pain and Palliative Care Head and Associate Professor Division
Facilitating Advance Care Planning Conversations Jeff Myers, MD, MSEd, CCFP Acting Provincial Clinical Lead, OPCN W. Gifford-Jones Professor in Pain and Palliative Care Head and Associate Professor Division
Module 1: Principles of Palliative Care. Part I: Dying Well. A Good Death Defined
 E L N E C End-of-Life Nursing Education Consortium Geriatric Curriculum Module 1: Principles of Palliative Care Part I: Dying Well A natural part of life Opportunity for growth Profoundly personal experience
E L N E C End-of-Life Nursing Education Consortium Geriatric Curriculum Module 1: Principles of Palliative Care Part I: Dying Well A natural part of life Opportunity for growth Profoundly personal experience
Palliative Care In PICU
 Palliative Care In PICU Professor Lucy Lum University Malaya Annual Scientific Meeting on Intensive Care 15 August 2015 2 Defining Palliative Care: Mistaken perception: For patients whom curative care
Palliative Care In PICU Professor Lucy Lum University Malaya Annual Scientific Meeting on Intensive Care 15 August 2015 2 Defining Palliative Care: Mistaken perception: For patients whom curative care
Symptoms Assess symptoms and needs across all domains. Screen using Edmonton Symptom Assessment System (ESAS) for: Pain Nausea Depression
 for: Pain Nausea Depression") A Palliative Care Approach for Oncology Integrating a palliative care approach earlier in the disease trajectory improves the quality of living and dying, and relieves suffering for patients and families
A Palliative Care Approach for Oncology Integrating a palliative care approach earlier in the disease trajectory improves the quality of living and dying, and relieves suffering for patients and families
Faculty/Presenter Disclosure
 Faculty/Presenter Disclosure Faculty: Dr. Anthony Kerigan Relationships with commercial interests:* Grants/Research Support: NONE Speakers Bureau/Honoraria: NONE Consulting Fees: NONE Other: NONE Meeting
Faculty/Presenter Disclosure Faculty: Dr. Anthony Kerigan Relationships with commercial interests:* Grants/Research Support: NONE Speakers Bureau/Honoraria: NONE Consulting Fees: NONE Other: NONE Meeting
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Élie AZOULAY Hôpital Saint-Louis, Service de Réanimation Médicale Université Paris-Diderot, Sorbonne Paris-Cité
 Élie AZOULAY Hôpital Saint-Louis, Service de Réanimation Médicale Université Paris-Diderot, Sorbonne Paris-Cité Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique (GRRR-OH) Thank you for
Élie AZOULAY Hôpital Saint-Louis, Service de Réanimation Médicale Université Paris-Diderot, Sorbonne Paris-Cité Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique (GRRR-OH) Thank you for
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delivering personalised care to end of life patients. Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London
 Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
End-of-Life Decision-Making
 End-of-Life Decision-Making Ian Anderson Continuing Education Program in End-of of-life Care Sense of Self and Decision-Making! Our sense of self is shaped by our families, past experiences, our sense
End-of-Life Decision-Making Ian Anderson Continuing Education Program in End-of of-life Care Sense of Self and Decision-Making! Our sense of self is shaped by our families, past experiences, our sense
Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions
 Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions Mary Tinetti, M.D. Canadian Geriatrics Society May, 2013 CFPC CoI Templates: Slide 1 Faculty/Presenter
Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions Mary Tinetti, M.D. Canadian Geriatrics Society May, 2013 CFPC CoI Templates: Slide 1 Faculty/Presenter
A Palliative Approach to Supporting Individuals and Families Living With Late and End-Stage Dementia. Dianna Drascic 2018 Alzheimer Symposium
 A Palliative Approach to Supporting Individuals and Families Living With Late and End-Stage Dementia Dianna Drascic 2018 Alzheimer Symposium Objectives Identify when a palliative approach becomes palliative
A Palliative Approach to Supporting Individuals and Families Living With Late and End-Stage Dementia Dianna Drascic 2018 Alzheimer Symposium Objectives Identify when a palliative approach becomes palliative
Paul E. Stander, MD, MBA, FACP Division of Palliative Care Geriatrics and Extended Care Phoenix VAHS
 Paul E. Stander, MD, MBA, FACP Division of Palliative Care Geriatrics and Extended Care Phoenix VAHS Objectives Define a population of patients with serious illness for whom improved communication holds
Paul E. Stander, MD, MBA, FACP Division of Palliative Care Geriatrics and Extended Care Phoenix VAHS Objectives Define a population of patients with serious illness for whom improved communication holds
Wellness along the Cancer Journey: Palliative Care Revised October 2015
 Wellness along the Cancer Journey: Palliative Care Revised October 2015 Chapter 2: Palliative Care Palliative Care Rev. 10.8.15 Page 352 Group Discussion True False Not Sure 1. Palliative care is only
Wellness along the Cancer Journey: Palliative Care Revised October 2015 Chapter 2: Palliative Care Palliative Care Rev. 10.8.15 Page 352 Group Discussion True False Not Sure 1. Palliative care is only
Conservative Care Pathway: A Client-Centred Approach
 2016 Conservative Care Pathway: A Client-Centred Approach Abbotsford Kidney Care Clinic October 7, 2016 Bobbi Preston, MSW, RCSW Jane Valcourt, RN Susan Cooper, MD, FRCP Goals of Session 1. Introduce the
2016 Conservative Care Pathway: A Client-Centred Approach Abbotsford Kidney Care Clinic October 7, 2016 Bobbi Preston, MSW, RCSW Jane Valcourt, RN Susan Cooper, MD, FRCP Goals of Session 1. Introduce the
THE CONSERVATIVE CARE PATHWAY
 THE CONSERVATIVE CARE PATHWAY Dr. Gaylene Hargrove Sept. 19, 2015 Island Health Renal Program End of Life Conference Learning Objectives Describe and discuss what defines conservative care. Identify key
THE CONSERVATIVE CARE PATHWAY Dr. Gaylene Hargrove Sept. 19, 2015 Island Health Renal Program End of Life Conference Learning Objectives Describe and discuss what defines conservative care. Identify key
Palliative Care under a Value Based Reimbursement Model. Janet Bull MD, MBA, FAAHPM CMO Four Seasons
 Palliative Care under a Value Based Reimbursement Model Janet Bull MD, MBA, FAAHPM CMO Four Seasons Objectives o Describe palliative care o Discuss benefits of palliative care o Understand differences
Palliative Care under a Value Based Reimbursement Model Janet Bull MD, MBA, FAAHPM CMO Four Seasons Objectives o Describe palliative care o Discuss benefits of palliative care o Understand differences
The Palliative Care Journey. By Sandra O Sullivan Clinical Nurse Manager 1 St Luke's home
 The Palliative Care Journey By Sandra O Sullivan Clinical Nurse Manager 1 St Luke's home Aims 1. To provide an overview of what palliative care involves. 2. Identify, at what stage should Dementia be acknowledged
The Palliative Care Journey By Sandra O Sullivan Clinical Nurse Manager 1 St Luke's home Aims 1. To provide an overview of what palliative care involves. 2. Identify, at what stage should Dementia be acknowledged
UCSF PAIN SUMMIT /8/15
 UCSF PAIN SUMMIT 2015 5/8/15 Case 3 Geriatric Pain Disclosure Statements UCSF PAIN SUMMIT 2015 Wendy Anderson Patrice Villars 5/8/15 Case 3 Geriatric Pain Pain Management in the Geriatric & End-of-Life
UCSF PAIN SUMMIT 2015 5/8/15 Case 3 Geriatric Pain Disclosure Statements UCSF PAIN SUMMIT 2015 Wendy Anderson Patrice Villars 5/8/15 Case 3 Geriatric Pain Pain Management in the Geriatric & End-of-Life
PACE Care Pathways. Initiatives to Apply Contemporary Guidelines
 PACE Care Pathways Initiatives to Apply Contemporary Guidelines to Participant Goals Stephen D Ryan, MD, MPH. Senior Medical Director for PACE/Managed Long Term Care Clinical Assistant Professor of Medicine,
PACE Care Pathways Initiatives to Apply Contemporary Guidelines to Participant Goals Stephen D Ryan, MD, MPH. Senior Medical Director for PACE/Managed Long Term Care Clinical Assistant Professor of Medicine,
CANP March 22, 2014 Conrad Rios FNP-BC, PA, MS
 Providing Palliative Care for Elderly Patients with Dementia in the ED CANP March 22, 2014 Conrad Rios FNP-BC, PA, MS Disclosures Conrad Rios FNP-BC, PA, MS has no financial relationships with commercial
Providing Palliative Care for Elderly Patients with Dementia in the ED CANP March 22, 2014 Conrad Rios FNP-BC, PA, MS Disclosures Conrad Rios FNP-BC, PA, MS has no financial relationships with commercial
We All Have It! Obvious Manifestations: Religion Ethnicity (Race?) National Origin (language) Gender
 National Origin (language) Gender") We All Have It! Obvious Manifestations: Religion Ethnicity (Race?) National Origin (language) Gender Less Obvious Manifestations: Age Education Educational Status Mobility (including handicaps) What is
We All Have It! Obvious Manifestations: Religion Ethnicity (Race?) National Origin (language) Gender Less Obvious Manifestations: Age Education Educational Status Mobility (including handicaps) What is
Death With Dignity-Albany. Sept 12 th, Judith Schwarz, PhD, RN Clinical Director End of Life Choices New York
 Death With Dignity-Albany Sept 12 th, 2018 Judith Schwarz, PhD, RN Clinical Director End of Life Choices New York I have been the Clinical Director, EOLCNY & predecessor group for more than 15 years Not-for-profit
Death With Dignity-Albany Sept 12 th, 2018 Judith Schwarz, PhD, RN Clinical Director End of Life Choices New York I have been the Clinical Director, EOLCNY & predecessor group for more than 15 years Not-for-profit
Palliative Medicine in Critical Care Not Just Hospice. Robin. Truth or Myth 6/11/2015. Francine Arneson, MD Palliative Medicine
 Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Palliative and End of Life Care Extended Workshop: CSIM 2014 Calgary. Karen Tang, MD FRCPC General Internal Medicine University of Calgary
 Palliative and End of Life Care Extended Workshop: CSIM 2014 Calgary Karen Tang, MD FRCPC General Internal Medicine University of Calgary Drs. Brisebois, Hiebert, and I have no affiliation with pharmaceutical,
Palliative and End of Life Care Extended Workshop: CSIM 2014 Calgary Karen Tang, MD FRCPC General Internal Medicine University of Calgary Drs. Brisebois, Hiebert, and I have no affiliation with pharmaceutical,
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Recent Elder Abuse Research: Implications for APS. Laura Mosqueda, M.D.
 Recent Elder Abuse Research: Implications for APS Laura Mosqueda, M.D. Aileen Wiglesworth, Ph.D. Game Plan Review some terms and concepts Incidence, prevalence Relationship, cause and effect Screening
Recent Elder Abuse Research: Implications for APS Laura Mosqueda, M.D. Aileen Wiglesworth, Ph.D. Game Plan Review some terms and concepts Incidence, prevalence Relationship, cause and effect Screening
CareFirst Hospice. Health care for the end of life. CareFirst
 Hospice Health care for the end of life 1 What is Hospice? Hospice is a philosophy- When a person in end stages of an illness can no longer receive, or wants to receive, life sustaining treatment, he or
Hospice Health care for the end of life 1 What is Hospice? Hospice is a philosophy- When a person in end stages of an illness can no longer receive, or wants to receive, life sustaining treatment, he or
Hospice and Palliative Medicine
 Hospice and Palliative Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Hospice and Palliative Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Adam D. Marks, MD MPH Assistant Professor of Medicine University of Michigan Health System
 Adam D. Marks, MD MPH Assistant Professor of Medicine University of Michigan Health System The truth will set you free but first it will piss you off - Gloria Steinem Life expectancy is up dramatically
Adam D. Marks, MD MPH Assistant Professor of Medicine University of Michigan Health System The truth will set you free but first it will piss you off - Gloria Steinem Life expectancy is up dramatically
Improving Healthcare Utilization in Injured Older Adults
 Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Hospice and Palliative Care An Essential Component of the Aging Services Network
 Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Palliative care in advanced dementia: care for families
 Palliative care in advanced dementia: care for families Jenny T. van der Steen, PhD VU University Medical Center EMGO Institute for Health and Care Research Department of General Practice & Elderly Care
Palliative care in advanced dementia: care for families Jenny T. van der Steen, PhD VU University Medical Center EMGO Institute for Health and Care Research Department of General Practice & Elderly Care
12/6/2016. Objective PALLIATIVE CARE IN THE NURSING HOME. Medical Care in the US. Palliative Care
 Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Karl Sash, MD Board Certified: Internal Medicine, Geriatrics, and Hospice and Palliative Medicine Medical Director, St Mary s Palliative Care
 Karl Sash, MD Board Certified: Internal Medicine, Geriatrics, and Hospice and Palliative Medicine Medical Director, St Mary s Palliative Care (Inpatient) Medical Director, Aseracare Hospice Evansville
Karl Sash, MD Board Certified: Internal Medicine, Geriatrics, and Hospice and Palliative Medicine Medical Director, St Mary s Palliative Care (Inpatient) Medical Director, Aseracare Hospice Evansville
Meeting the Palliative Care Needs of the Frail Elderly
 Meeting the Palliative Care Needs of the Frail Elderly 5 Days in Palliative Care 2016 Dr. A. T. Kerigan Associate Clinical Professor Department of Medicine, Mc Master University 1. What is frailty? 2.
Meeting the Palliative Care Needs of the Frail Elderly 5 Days in Palliative Care 2016 Dr. A. T. Kerigan Associate Clinical Professor Department of Medicine, Mc Master University 1. What is frailty? 2.
ICDs - decisions at the end of life
 ICDs - decisions at the end of life James Beattie Consultant Cardiologist Heart of England NHS Foundation Trust, Birmingham, UK National Clinical Adviser, NHS Heart Improvement Heart Statement of disclosure
ICDs - decisions at the end of life James Beattie Consultant Cardiologist Heart of England NHS Foundation Trust, Birmingham, UK National Clinical Adviser, NHS Heart Improvement Heart Statement of disclosure
4/26/2012. Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012
 Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
DEPARTMENT OF GERIATRIC MEDICINE GHENT UNIVERSITY HOSPITAL ADVANCE CARE PLANNING IN DEMENTIA: CLINICAL RECOMMENDATIONS
 DEPARTMENT OF GERIATRIC MEDICINE GHENT UNIVERSITY HOSPITAL ADVANCE CARE PLANNING IN DEMENTIA: CLINICAL RECOMMENDATIONS Nele Van Den Noortgate EUGMS Nice 21th September No conflict of interest to declare
DEPARTMENT OF GERIATRIC MEDICINE GHENT UNIVERSITY HOSPITAL ADVANCE CARE PLANNING IN DEMENTIA: CLINICAL RECOMMENDATIONS Nele Van Den Noortgate EUGMS Nice 21th September No conflict of interest to declare
Table to Demonstrate a method of working through Triggered CAPs.
 CAP Problem Goals Triggers Guidelines Physical Activities increase hours of exercises Reports less than 2 hours Personal choice Promotion and physical activity activity in last 3 days Instrumental Activities
CAP Problem Goals Triggers Guidelines Physical Activities increase hours of exercises Reports less than 2 hours Personal choice Promotion and physical activity activity in last 3 days Instrumental Activities
This information explains the advice about supporting people with dementia and their carers that is set out in NICE SCIE clinical guideline 42.
 Supporting people with dementia and their carers Information for the public Published: 1 November 2006 nice.org.uk About this information NICEclinicalguidelinesadvisetheNHSoncaringforpeoplewithspe cificconditionsordiseasesandthetreatmentstheyshouldreceive.
Supporting people with dementia and their carers Information for the public Published: 1 November 2006 nice.org.uk About this information NICEclinicalguidelinesadvisetheNHSoncaringforpeoplewithspe cificconditionsordiseasesandthetreatmentstheyshouldreceive.
End of Life Care in IJN Our journey. Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia
 End of Life Care in IJN Our journey Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia End of Life Dying is final part of everyone journey in life Deaths used to occur
End of Life Care in IJN Our journey Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia End of Life Dying is final part of everyone journey in life Deaths used to occur
The COLLaboration on AGEing (COLLAGE)
") The COLLaboration on AGEing (COLLAGE) Professor D. William Molloy University College Cork, Ireland. The Lessons from Europe Seminar 23-09-15 Overview Exemplars within COLLAGE: 1. What is COLLAGE? 2. The
The COLLaboration on AGEing (COLLAGE) Professor D. William Molloy University College Cork, Ireland. The Lessons from Europe Seminar 23-09-15 Overview Exemplars within COLLAGE: 1. What is COLLAGE? 2. The
Survive and Thrive: Palliative Care. Gordon J. Wood, MD, MSCI, FAAHPM September 9, 2017
 Survive and Thrive: Palliative Care Gordon J. Wood, MD, MSCI, FAAHPM September 9, 2017 Objectives Define Palliative Care Differentiate Palliative Care from Hospice Describe the history of Palliative Care
Survive and Thrive: Palliative Care Gordon J. Wood, MD, MSCI, FAAHPM September 9, 2017 Objectives Define Palliative Care Differentiate Palliative Care from Hospice Describe the history of Palliative Care
Walking together: Palliative Care and heart failure.
 Walking together: Palliative Care and heart failure. St Paul's Hospital Heart Function Supportive Care Clinic Cindy Nordquist MN-NP(F) Objectives Review heart failure. Review palliative care/ palliative
Walking together: Palliative Care and heart failure. St Paul's Hospital Heart Function Supportive Care Clinic Cindy Nordquist MN-NP(F) Objectives Review heart failure. Review palliative care/ palliative
St George Hospital Renal Supportive Care Psychosocial Day, 10 th August Michael Noel, Supportive and Palliative Care Physician, Nepean Hospital
 St George Hospital Renal Supportive Care Psychosocial Day, 10 th August 2017 Michael Noel, Supportive and Palliative Care Physician, Nepean Hospital Michael.Noel@health.nsw.gov.au Hannah Burgess, Renal
St George Hospital Renal Supportive Care Psychosocial Day, 10 th August 2017 Michael Noel, Supportive and Palliative Care Physician, Nepean Hospital Michael.Noel@health.nsw.gov.au Hannah Burgess, Renal
It Takes a Village: Caring for Veterans with Advanced Dementia
 It Takes a Village: Caring for Veterans with Advanced Dementia Eric Widera, MD Professor, Division of Geriatrics, UCSF Blog and Podcast: www.geripal.org In our village, what tasks should we be confident
It Takes a Village: Caring for Veterans with Advanced Dementia Eric Widera, MD Professor, Division of Geriatrics, UCSF Blog and Podcast: www.geripal.org In our village, what tasks should we be confident
Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol
 Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol") 483.25 Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary
483.25 Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary
11/11/2016. Disclosures. Natural history of BPSD. Objectives. Assessment of BPSD. Behavioral Management of Persons with Alzheimer s Disease
 Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
Talking the same language for effective care of older people
 Introducing the interrai Home Care Talking the same language for effective care of older people interrai has developed an entire range of instruments and screeners to support assessment in a wide array
Introducing the interrai Home Care Talking the same language for effective care of older people interrai has developed an entire range of instruments and screeners to support assessment in a wide array
Palliative Care and Hospice. Silver Linings: Reflecting on Our Past & Transitioning into our Future
 Palliative Care and Hospice Silver Linings: Reflecting on Our Past & Transitioning into our Future Objectives: 1. What is Palliative Care? What is Hospice? What is the difference? 2. What are the trending
Palliative Care and Hospice Silver Linings: Reflecting on Our Past & Transitioning into our Future Objectives: 1. What is Palliative Care? What is Hospice? What is the difference? 2. What are the trending
A Population Health Approach to Palliative Care
 A Population Health Approach to Palliative Care Steven Pantilat, MD Professor of Medicine Kates-Burnard and Hellman Distinguished Professor in Palliative Care Director, and Palliative Care Quality Network
A Population Health Approach to Palliative Care Steven Pantilat, MD Professor of Medicine Kates-Burnard and Hellman Distinguished Professor in Palliative Care Director, and Palliative Care Quality Network
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
Deciding whether a person has the capacity to make a decision the Mental Capacity Act 2005
 Deciding whether a person has the capacity to make a decision the Mental Capacity Act 2005 April 2015 Deciding whether a person has the capacity to make a decision the Mental Capacity Act 2005 The RMBI,
Deciding whether a person has the capacity to make a decision the Mental Capacity Act 2005 April 2015 Deciding whether a person has the capacity to make a decision the Mental Capacity Act 2005 The RMBI,
Associated Resources and Guidelines for Their Use
 Infusing Geropsychiatric Nursing into Curricula: Associated Resources and Guidelines for Their Use The National Institute of Mental Health predicts that by 2030, the numbers of older adults (age 65+) with
Infusing Geropsychiatric Nursing into Curricula: Associated Resources and Guidelines for Their Use The National Institute of Mental Health predicts that by 2030, the numbers of older adults (age 65+) with
Early Integration of Palliative Care
 Early Integration of Palliative Care Dr. Camilla Zimmermann Head, Palliative Care Program University Health Network Toronto November 1, 2014 www.fpon.ca Early Integration of Palliative Care: Evidence and
Early Integration of Palliative Care Dr. Camilla Zimmermann Head, Palliative Care Program University Health Network Toronto November 1, 2014 www.fpon.ca Early Integration of Palliative Care: Evidence and
Communication and Shared Decision-Making in the Absence of Terminal Disease
 Communication and Shared Decision-Making in the Absence of Terminal Disease Prema R. Menon, MD, PhD Assistant Professor of Medicine Pulmonary and Critical Care Division University of Vermont Outline Introduction:
Communication and Shared Decision-Making in the Absence of Terminal Disease Prema R. Menon, MD, PhD Assistant Professor of Medicine Pulmonary and Critical Care Division University of Vermont Outline Introduction:
Palliative and End of Life Care in End Stage Renal Disease
 Palliative and End of Life Care in End Stage Renal Disease Palliative and End of Life Care Priority for Action Regional Consensus Workshop 30.06.2010 Neal Morgan Consultant Nephrologist SHSCT Outline Introduction
Palliative and End of Life Care in End Stage Renal Disease Palliative and End of Life Care Priority for Action Regional Consensus Workshop 30.06.2010 Neal Morgan Consultant Nephrologist SHSCT Outline Introduction
Course Handouts & Disclosure
 ALS: DISEASE TRAJECTORY AND HOSPICE ELIGIBILITY Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc Hospice Education Network Inc Course Handouts & Disclosure To download presentation
ALS: DISEASE TRAJECTORY AND HOSPICE ELIGIBILITY Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc Hospice Education Network Inc Course Handouts & Disclosure To download presentation
Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges. Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009
 Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009 Objectives Highlight the relevance of palliative/supportive care
Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009 Objectives Highlight the relevance of palliative/supportive care
Skin Susceptible to injury; longer time Senses of the senses Respiratory system Decreased ability to exchange
 1 Geriatric Review 2 Geriatrics Geriatric patients are individuals older than years of age. In 2000, the geriatric population was almost 35 million. By 2020, the geriatric population is projected to be
1 Geriatric Review 2 Geriatrics Geriatric patients are individuals older than years of age. In 2000, the geriatric population was almost 35 million. By 2020, the geriatric population is projected to be
PATIENTS WHO WITHDRAW FROM DIALYSIS. Dr Katalin Urban Palliative Care Specialist Greenwich Hospital
 PATIENTS WHO WITHDRAW FROM DIALYSIS Dr Katalin Urban Palliative Care Specialist Greenwich Hospital Registrar project for FRACP Title: Patients who withdraw from dialysis in a Sydney centre with Palliative
PATIENTS WHO WITHDRAW FROM DIALYSIS Dr Katalin Urban Palliative Care Specialist Greenwich Hospital Registrar project for FRACP Title: Patients who withdraw from dialysis in a Sydney centre with Palliative
Evaluations. Featured Speakers. Thank You to Our Sponsors: 9/15/2015. Conflict of Interest & Disclosure Statements
 Evaluations Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org to fill out your evaluation and complete the post-test. Conflict of Interest & Disclosure Statements The
Evaluations Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org to fill out your evaluation and complete the post-test. Conflict of Interest & Disclosure Statements The
Understanding Dementia &
 Understanding Dementia & Care Options for Those Suffering with the Disease Paige Landry BSN Hospice Care Consultant SouthernCare New Beacon Hospice Objectives Understand Dementia Understand Common Problems
Understanding Dementia & Care Options for Those Suffering with the Disease Paige Landry BSN Hospice Care Consultant SouthernCare New Beacon Hospice Objectives Understand Dementia Understand Common Problems
Palliative care for children with Rare Diseases
 Palliative care for children with Rare Diseases Busi Nkosi International Children s Palliative Care Network Need for children s palliative care More than 21 million children need palliative care worldwide
Palliative care for children with Rare Diseases Busi Nkosi International Children s Palliative Care Network Need for children s palliative care More than 21 million children need palliative care worldwide
THE ROLE OF PALLIATIVE CARE IN TREATMENT OF PATIENTS WITH CHRONIC, INFECTIOUS DISEASE
 THE ROLE OF PALLIATIVE CARE IN TREATMENT OF PATIENTS WITH CHRONIC, INFECTIOUS DISEASE JESSICA MCFARLIN MD ASSISTANT PROFESSOR OF NEUROLOGY DIVISION CHIEF, PALLIATIVE AND SUPPORTIVE CARE I HAVE NO COI OR
THE ROLE OF PALLIATIVE CARE IN TREATMENT OF PATIENTS WITH CHRONIC, INFECTIOUS DISEASE JESSICA MCFARLIN MD ASSISTANT PROFESSOR OF NEUROLOGY DIVISION CHIEF, PALLIATIVE AND SUPPORTIVE CARE I HAVE NO COI OR
Dementia. Memory Evaluation Center Neurology
 Dementia Memory Evaluation Center Neurology Topics Overview of dementia Stages Medications Advanced planning What is Dementia? Dementia = significant global decline in cognitive function not due to medicine
Dementia Memory Evaluation Center Neurology Topics Overview of dementia Stages Medications Advanced planning What is Dementia? Dementia = significant global decline in cognitive function not due to medicine