Osteoporosis Update: Review of Current Guidelines, Controversies, and Common Questions
|
|
|
- Mabel Montgomery
- 6 years ago
- Views:
Transcription

1 Osteoporosis Update: Review of Current Guidelines, Controversies, and Common Questions Holly Hofkamp, MD OHSU Family Medicine, Assistant Professor 4/25/14
2 No disclosures
3 Goals/Objectives Highlight current guidelines (NOF, USPSTF, AACE) to guide diagnosis and management of osteoporosis Use case based approach to address common issues that arise when diagnosing and treating osteoporosis. Plan to address issues of screening, prevention, and treatment
4 Scope of the Problem
5 Triple Aim Improve access: Improve access to appropriate screening Improve outcomes: Appropriate screening will identify those at risk for osteoporotic fractures and allow treatment to decrease overall fracture burden Decrease cost: Detecting and treating those at risk for osteoporotic fracture will decrease cost by reducing hospitalizations, long term care placement, etc.
6 A quick review: Definitions Normal T score at -1 and above Low bone mass T score between -1 and Osteoporosis T score at or below -2.5
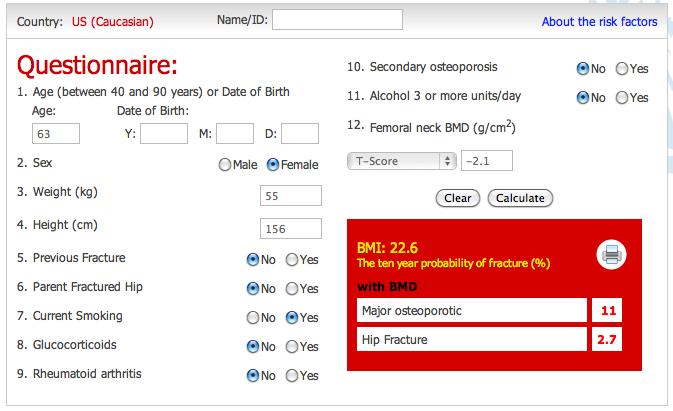
7 Case 1 63 yo woman with PMH of moderate macular degeneration, HTN, HLD, and RLS presents for her well woman exam. She notes that she had a bone density test in 2005 that showed osteopenia with femoral neck T score of -1.8 and wonders if she needs a repeat DXA. Meds: Atenolol, Niacin, Mirapex SH: smoker (1 ppd x 30 years) Wt 55 kg, Ht 156 cm; BMI 22.6 What is the next step? A. Calculate FRAX to determine if repeat DXA should be ordered today B. Decline repeat DXA until age 65; Counsel on calcium/vitamin D, smoking cessation, and weight bearing exercise C. Start a bisphosphonate D. Perform a vertebral fracture assessment
8 National Osteoporosis Foundation (NOF) Screening Recommendations Recommended modality: DXA Women age 65 and men age 70 Based on risk factor profile for postmenopausal women and men (if FRAX 10 year risk score is 9.3%) Adults who have had fracture (without trauma) after age 50 Adults with condition (eg RA) or taking a medication (eg steroids) associated with osteoporosis
9 USPSTF Recommendations The USPSTF recommends (DXA) Screening for osteoporosis in women aged 65 years or older Screening for younger women whose fracture risk is equal to or greater than that of a 65-year-old white woman who has no additional risk factors. (Frax 9.3%) Grade B Insufficient evidence to assess the balance of benefits and harms of screening for osteoporosis in men (Grade I)
10 FRAX Fracture risk can be determined by using FRAX calculator Only for postmenopausal women and men 50 FRAX not validated in patients currently or previously treated
11 FRAX Risk Calculator
12 Case 1 63 yo woman with PMH of moderate macular degeneration, HTN, HLD, and RLS presents for her well woman exam. She notes that she had a bone density test in 2005 that showed osteopenia with a femoral neck T score of -1.8 and wonders if she needs a repeat DXA. Meds: Atenolol, Niacin, Trazodone, Mirapex SH: smoker (1 ppd x 30 years) Wt 55 kg, Ht 156 cm; BMI 22.6 What is the next step? A. Calculate FRAX to determine if repeat DXA should be ordered today B. Decline repeat DXA until age 65; Counsel on calcium/vitamin D, smoking cessation, and weight bearing exercise C. Start a bisphosphonate D. Perform a vertebral fracture assessment
13 Vertebral Imaging 2 methods Lateral thoracic and lumbar spine x-ray Lateral vertebral fracture assessment (available on most DXA machines) Radiographically confirmed vertebral fractures Sufficient to make the diagnosis of osteoporosis Automatically makes the patient a candidate for treatment Increases risk of future vertebral fractures 5-fold and the risk of hip and other fractures 2- to 3- fold
14 Vertebral Imaging NOF recommendations Consider for: All women 70 and all men 80 if T score at the spine, total hip or femoral neck is -1.0 Women between and men between if T score at spine, total hip or femoral neck is -1.5 Postmenopausal woman and men with specific risk factors: Low trauma fracture Patient report of height loss of 4 cm Measured height loss of 2 cm Recent or ongoing long-term glucocorticoid treatment
15 Screening Interval Optimal screening interval would allow detection of low BMD/osteoporosis before the onset of a fragility fracture Common practice to screen every 2 years National Osteoporosis Foundation Unclear if patients have normal initial screen or in upper low bone mass range and don t have major risk factors USPSTF No Recommendation

16 Screening Interval AACE, 2010
17

18 1 year 4.6 years ~17 years

19 Conclusion: For untreated men and women with a mean age of 75, repeating DXA after 4 years did not improve fracture risk prediction
20 What does Medicare cover? DXA once every 24 months (more often if medically necessary ) No limit on number of total tests Goal is to find the correct interval to improve quality of care and contain cost This data suggests that q 2 years may be too frequent for most clinical scenarios
21 Bottom lines for screening and interval Screen women age 65 and men 70 Screen younger patients if FRAX 10 year risk score is 9.3%) Consider screening adults who have had low trauma fracture after age 50, and those with medical conditions or medications associated with osteoporosis Screening interval is unclear, but every 2 years is likely too often for some patients Consider baseline BMD and age when considering screening interval
22 Case 1 (continued) Repeat DXA shows a femoral neck T score of -2.1 Additional history reveals patient is not taking any supplements, but has 1-2 servings of calcium daily. She is sedentary. Which of the following treatments are indicated at this time to prevent falls and fracture risk? A. Start alendronate 10 mg PO daily B. Counsel on adequate calcium/vitamin D intake C. Home safety eval and exercise program D. Start alendronate 70 mg PO weekly
23 Who should I Treat? Hip or vertebral fracture in absence of major trauma T score -2.5 at femoral neck, total hip, or lumbar spine Low bone mass/osteopenia (T score between -1 and -2.5) if 10 year hip fracture risk is > 3% or if 10 year major osteoporotic fracture risk is >20% using FRAX
24
25 Prevention NOF recommendations Weight bearing and strengthening exercises Fall risk assessment and risk modification Adequate calcium and vitamin D Tobacco cessation Identify and treat alcoholism Measure height annually
26 Fall Prevention/Exercise 2012 Cochrane review 159 trials; 80,000 subjects Group and home exercise programs reduced risk of falling as well as risk of fall related fractures Home safety evaluations/interventions reduced rate and risk of falls. More effective when delivered by an occupational therapist. Vitamin D supplementation did not prevent falls* 2012 USPSTF Recommends exercise or physical therapy (B) Recommends vitamin D supplementation (B)
27 NOF recommendations Calcium 1200 mg daily for women > 50 and men > mg daily for men Vitamin D IU daily Consider check levels in those at risk for deficiency and supplementing as necessary If adequate dietary calcium cannot be obtained, dietary supplementation is indicated up to the recommended daily intake.
28 Prevention: Calcium/Vitamin D USPSTF, 2013 Recommend against daily supplementation with 400 IU or less of vitamin D and 1000 mg or less of calcium for the primary prevention of fractures in non-institutionalized postmenopausal women. (D) Insufficient evidence to assess the balance of the benefits and harms of combined vitamin D and calcium supplementation for the primary prevention of fractures in premenopausal women or in men. (I) Insufficient evidence to assess the balance of the benefits and harms of daily supplementation with greater than 400 IU of vitamin D3 and greater than 1000 mg calcium for the primary prevention of fractures in noninstitutionalized postmenopausal women. (I)
29 Bottom Line: Calcium/Vitamin D Highly controversial area of ongoing research Advocate for getting RDI of calcium/d through food Not great evidence for prevention of osteoporosis/fractures with supplements, but good studies are limited Risk of CVD is not compelling, but modest increase in urinary tract stones
30 Case 2 70 year old postmenopausal woman with PMH of GERD, hypothyroidism, and depression has a routine DXA as part of a well woman assessment. Her chronic medical conditions are well controlled, though she is due for a TSH. Her T score at the femoral neck is -2.7 and -3.2 at the L spine. She has no history of fractures. BMI 24.1 Meds: omeprazole 20 mg daily, levothyroxine 100 mcg daily, and citalopram 10 mg daily Which of the following statements is true? A. Bisphosphonates are contraindicated because of her h/o GERD B. All of the medications this patient takes can adversely affect bone health. C. Vertebral imaging would help to guide your management of this patient. D. The first line therapy for this patient would be estrogen.

31
32 Case 2 (revisit) 70 year old postmenopausal woman with PMH of GERD, hypothyroidism, and depression has a routine DXA with T score at the femoral neck is -2.7 and -3.2 at the L spine. She has no history of fractures. Her TSH is normal. BMI 24.1 Meds: omeprazole 20 mg daily, levothyroxine 100 mcg daily, and citalopram 10 mg daily What class of medication should we start? A. Calcitonin B. HRT C. Bisphosphonate D. Teriparatide

33 Have demonstrated decreased vertebral, nonvertebral, and hip fractures when compared to placebo
34 Bisphosphonates (BPs) Alendronate* Reduced vertebral and hip fractures by ~ 50 % over 3 years Risendronate Reduced vertebral fractures by 41-49%; Reduced other fractures by 36% over 3 years Ibandronate Reduced vertebral fractures by ~ 50% over 3 years; no effect on non-vertebral fractures Zoledronic acid Reduced vertebral fractures by 70%; Reduced hip fractures by 41%; other fracture reduction 25% over 3 years
35 Bisphosphonates Side effects: difficulty swallowing, esophageal erosions/inflammation, gastric ulcer, bone/joint pain, osteonecrosis of jaw, hypocalcemia, low trauma atypical femur fracture Can have flu like syndrome after IV infusions Can affect renal function check creatinine/gfr first Not recommended if GFR < 30
36 Bisphosphonates Empty stomach First thing in the morning Stay upright for minutes 8 oz water Can pretreat with acetominophen before IV meds
37 Osteonecrosis of the Jaw Risk very small in those treated for osteoporosis to 0.1% risk with oral BPs % risk with high dose IV BPs for > 2 year Risk increases with treatment duration and higher doses Oral exam with xrays indicated to evaluate jaw heaviness, tingling, pain, loose teeth or oral ulceration
38 Atypical femur fractures Absolute risk is low ( cases per 100,000 patient years) Miniscule when compared to risk of osteoporotic fractures Risk increases with treatment duration Usually precipitated by pain in groin/thigh Check xrays, MRI, bone scan if suspected
39 Other FDA Approved Therapies Calcitonin Estrogen Agonist/Antagonist: Raloxifene Parathyroid hormone: Teriparatide RANKL/RANKL inhibitor: Denosumab
40 Teriparatide Synthetic parathyroid hormone stimulates osteoblasts to form bone (anabolic), increases calcium absorption Reduces risk of vertebral fractures by 65%; nonvertebral fractures by 53% over 18 months Daily SQ injection Side effects: leg cramps, nausea, dizziness, increased osteosarcoma in rats Only approved for use for 2 years, usually followed by a bisphosphonate
41 Denosumab Monoclonal Ab that prevents Receptor Activator of Nuclear Factor kappa-b (RANK) and RANK ligand from interfacing RANK/RANKL interaction critical for osteoclast function Reduces vertebral fractures 68%, hip fractures 40%, and other fracture 20% over 3 years SQ injection q 6 months Side effects: hypocalcemia, skin rash and infection, osteonecrosis of jaw, atypical femur fractures
42 Monitoring treatment Repeating DXA sooner than 2 years is not likely to show significant change Stability of or increase in BMD is considered a good response Even those with decreased BMD show fracture risk reduction Good evidence on the utility of DXA for monitoring is lacking, controversial area Looking for non-responders and noncompliance
43 Monitoring treatment NOF guidelines: Clinical assessment: review med side effects and compliance, risk factors, fall prevention measures, calcium/vitamin d intake, exercise 1-2 years after starting therapy, the q 2 years thereafter Vertebral imaging only repeat if ht loss, new back pain Bone Turnover Markers AACE Repeat DXA every 1-2 years until BMD is stable, then reduce testing frequency NIH, UK, and Canada do not offer recommendation
44 Case 2 (continued) The patient asks she will have to take a bisphosphonate for the rest of her life? How do you counsel her? A. Lifelong treatment is warranted B. 1-2 years of treatment C. 3-5 years of treatment D. 10 years of treatment
45 Duration of treatment FLEX study, 2006 Demonstrated that taking alendronate > 5 years did not provide additional fracture protection for nonvertebral fractures Did lower clinical vertebral fracture risk FLEX 2, 2010 Alendronate for > 5 years may be beneficial in those women with femoral neck T -2.5, unlikely to be beneficial in those with 2 Reassess risk after 3-5 years Interval fracture history, new meds/conditions, height measurement, BMD, and vertebral imaging (if there has been documented height loss 2 cm) If low risk of fracture: Consider stopping oral therapy after 5 years Consider stopping IV therapy (zoledronic acid) after 3 years No consensus on how to monitor after treatment is stopped and if you should restart meds
46 Bottom Line for Treatment Bisphosphonates are first line Monitoring is controversial, but generally check for response 2 years after initiating treatment Consider contributing causes/secondary work up if patient isn t responding as expected Consider stopping treatment after 3-5 years
47 Take Home Points: Screening Screen women 65 and and men 70 Screen younger patients if FRAX 10 year risk score is 9.3% Consider screening adults who have had low trauma fracture after age 50, and those with medical conditions or medications associated with osteoporosis Consider baseline BMD and age when considering screening interval
48 Take Home Points: Prevention Fall Prevention: Group or home exercise programs/physical therapy Home safety evaluations Consider vitamin D Calcium and Vitamin D Controversial Best through food
49 Take Home Points: Treatment Bisphosphonates are first line Monitoring is controversial, but generally check for response 2 years after initiating treatment Consider contributing causes/secondary work up if patient isn t responding as expected Consider stopping treatment after 3-5 years
50 Questions/Comments???
51 References Nelson HD, Haney EM, Dana T, Bougatsos C, Chou R. Screening for osteoporosis: an update for the U.S. Preventive Services Task Force. Ann Intern Med 2010; 153: [PMID: ] National Osteoporosis Foundation. Clinicians Guide to Prevention and Treatment of Osteoporosis Available online. Watts NB, Bilezikian JP, Camacho PM, et al; AACE Osteoporosis Task Force. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the diagnosis and treatment of postmenopausal osteoporosis. Endocr Pract. 2010;16 Suppl 3:1-37 Gourlay ML, Fine JP, et al. Study of Osteoporotic Fracture Reasearch Group. Bone-density testing interval and transition to osteoporosis in older women. N Eng J Med 2012; 366: Frost SA, Nguyen ND, et all. Timing of repeat BMD measurements: Development of an absolute risk-based prognostic model. J Bone Miner Res 2009; 24: Hillier TA, Stone KL, Bauer DC, et al. Evaluating the Value of Repeat Bone Mineral Density Measurement and Prediction of Fractures in Older Women: The Study of Osteoporotic Fractures. Arch Intern Med. 2007;167(2): Berry SD, Samelson EJ, Pencina MJ, et al. Repeat Bone Mineral Density Screening and Prediction of Hip and Major Osteoporotic Fracture. JAMA. 2013;310(12): Bandiralia M, et al. Dose absorption in lumbar and femoral dual energy X-ray absorptiometry examinations using three different scan modalities: an anthropomorphic phantom study. J Clin Densitom Jul-Sep;16(3): doi: /j.jocd Epub 2013 Mar 25 Virginia A. Moyer, on behalf of the U.S. Preventive Services Task Force*; Vitamin D and Calcium Supplementation to Prevent Fractures in Adults: U.S. Preventive Services Task Force Recommendation Statement. Annals of Internal Medicine May;158(9): Chung M, Lee J, Terasawa T, Lau J, Trikalinos TA. Vitamin D with or without calcium supplementation for prevention of cancer and fractures: an updated meta-analysis for the U.S. Preventive Services Task Force. Ann Intern Med. 2011; 155: Prentice RL, Pettinger RD, et al. Health risks and benefits from calcium and vitamin D supplementation: Women's Health Initiative clinical trial and cohort study. Osteoporosis International. Feb 2013; 24 (2):
52 References Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR (2011) Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the Women s Health Initiative limited dataset and metaanalysis. BMJ 342:d2040. doi: /bmj.d2040 Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C, Gates S, Clemson LM, Lamb SE. Interventions for preventing falls in older people living in the community. Cochrane Database of Systematic Reviews 2012, Issue 9. Art. No.: CD DOI: / CD pub3. Davidge Pitts CJ, et al.. Update on medications with adverse skeletal effects. Mayo Clin Proc Apr; 86(4): quiz 343. doi: /mcp Epub 2001 Mar 9. Das S, Crockett JC. Osteoporosis a current view of pharmacological prevention and treatment. Drug Des Devel Ther May 31;7: doi: /dddt.s Print Curtis JR et al. RisedronatE and ALendronate Intervention over Three Years (REALITY): Minimal Differences in Fracture Risk Reduction Os Int June ; 20(6): doi: /s Emkey R, et al. Efficacy and tolerability of once-monthly oral ibandronate (150 mg) and once-weekly oral alendronate (70 mg): additional results from the Monthly Oral Therapy With Ibandronate For Osteoporosis Intervention (MOTION). Clin Ther Apr;31(4): doi: /j.clinthera Jansen JP, et al. The efficacy of bisphosphonates in the prevention of vertebral, hip, and nonvertebralnonhip fractures in osteoporosis: a network meta-analysis. Semin Arthritis Rheum Feb;40(4): e1-2. doi: /j.semarthrit Epub 2010 Sep 9.
53 References Reid DM, Hosking D, et al. A comparison of the effect of alendronate and risedronate on bone mineral density in postmenopausal women with osteoporosis: 24-month results from FACTS-International. Int J Clin Pract Apr;62(4): doi: /j x. Downs RW, Bell NH, et al. Comparison of alendronate and intranasal calcitonin for treatment of osteoporosis in postmenopausal women. J Clin Endocrinol Metab May;85(5): Bilezikian JP. Efficacy of bisphosphonates in reducing fracture risk in postmenopausal osteoporosis. Am J Med Feb;122(2 Suppl):S doi: /j.amjmed Saag K, Lindsay R, Kriegman A, Beamer E, Zhou W. A single zoledronic acid infusion reduces bone resorption markers more rapidly than weekly oral alendronate in postmenopausal women with low bone mineral density. Bone. 2007;40(5): McClung M, Recker R, Miller P, et al. Intravenous zoledronic acid 5 mg in the treatment of postmenopausal women with low bone density previously treated with alendronate. Bone. 2007;41(1): Hadji P, Gamerdinger D, et al. Rapid Onset and Sustained Efficacy (ROSE) study: results of a randomised, multicentre trial comparing the effect of zoledronic acid or alendronate on bone metabolism in postmenopausal women with low bone mass. Osteoporos Int Feb;23(2): doi: /s Epub 2011 Mar 26. Levis S, Theodore G. Summary of AHRQ's comparative effectiveness review of treatment to prevent fractures in men and women with low bone density or osteoporosis: update of the 2007 report. J Manag Care Pharm May;18(4 Suppl B):S1-15; discussion S13. Lin T, Yan SG, et al. Alendronate versus Raloxifene for Postmenopausal Women: A Meta-Analysis of Seven Head-to-Head Randomized Controlled Trials. Int J Endocrinol. 2014;2014: Epub 2014 Jan 5.
54 Reference Pharmacist s Letter. PL Detail-Document # November Safety of Long-Term Bisphosphonate Therapy. Pharmacist s Letter. PL Detail-Document # July Optimal Duration of Bisphosphonate Therapy. Shane E, Burr D, et al. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone Miner Res Jan;29(1):1-23. doi: /jbmr Epub 2013 Oct 1. Black DM, Schwartz AV, et al. Flex Research Group. Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. JAMA Dec 27;296(24): Schwartz AV, Bauer, DC, et al. Efficacy of continued alendronate for fractures in women with and without prevalent vertebral fracture: the FLEX trial. J Bone Miner Res May;25(5): doi: /jbmr.11. Laster AJ. Dual-energy x-ray absorptiometry: overused, neglected, or just misunderstood? N C Med J Mar-Apr;75(2): Bell KJ, Hayen A, Macaskill P, et al. Value of routine monitoring of bone mineral density after starting bisphosphonate treatment: secondary analysis of trial data. BMJ. 2009;338:b2266. Watts NB, Lewiecki EM, Bonnick SL, et al. Clinical value of monitoring BMD in patients treated with bisphosphonates for osteoporosis. J Bone Miner Res. 2009;24(10): Lewiecki EM, Watts NV. Assessing response to osteoporosis therapy. Osteoporos Int Oct;19(10): doi: /s Epub 2008 Jun 11.
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Etiology. Presenter Disclosure Information. Epidemiology.
 12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Page 1. Updates in Osteoporosis. I have no conflicts of interest. What is osteoporosis? What s New in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Pharmacy Management Drug Policy
 Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Definition. Presenter Disclosure Information.
 4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
Page 1. Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in ? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Page 1. New Developments in Osteoporosis. What s New in Osteoporosis
 New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Page 1. Current and Emerging Strategies What s New in Osteoporosis. Osteoporosis. What is Osteoporosis? Traditional Risk Factors for Fracture
 Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Updates in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
Osteoporosis Update. Greg Summers Consultant Rheumatologist
 Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment. William D. Leslie, MD MSc FRCPC
 Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Chau Nguyen, D.O. Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences
 Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Page 1. Current and Emerging Strategies for Osteoporosis. Osteoporosis Warm-Up: Which of the Following is True?
 Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
Osteoporosis Treatment Overview. Colton Larson RFUMS October 26, 2018
 Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Current and Emerging Approaches for Osteoporosis
 Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
AACE/ACE Osteoporosis Treatment Decision Tool
 AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
Kristen M. Nebel, DO PENN/ LGHP Geriatrics. Temple Family Medicine Review
 Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
Assessment and Treatment of Osteoporosis Professor T.Masud
 Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
ACP Colorado-Evidence Based Management of Osteoporosis
 ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
SpongeBone Menopants*
 SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
Advanced medicine conference. Monday 20 Tuesday 21 June 2016
 Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Osteoporosis Management
 Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Current Issues in Osteoporosis
 Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
11/4/2018. Osteoporosis Update. ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East. No disclosures.
 Osteoporosis Update ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East No disclosures. 1 Goals Review screening recommendations and workup of secondary causes
Osteoporosis Update ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East No disclosures. 1 Goals Review screening recommendations and workup of secondary causes
Healthy Bones: Osteoporosis Management. Laurel Short, MSN, FNP-C
 Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
The Bare Bones of Osteoporosis. Wendy Rosenthal, PharmD
 The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
Osteoporosis Update. Case 2. Case 1: Monday morning, 8:15
 Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Disclosures. Diagnostic Challenges in Osteoporosis: Whom To Treat 9/25/2014
 Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Screening Guidelines: Women
 The Situation 1 in 2 postmenopausal women and 1 in 5 older men will have an osteoporosis-related fracture in their lifetimes Osteoporosis Definition NIH Consensus Conference A skeletal disorder characterized
The Situation 1 in 2 postmenopausal women and 1 in 5 older men will have an osteoporosis-related fracture in their lifetimes Osteoporosis Definition NIH Consensus Conference A skeletal disorder characterized
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital
 Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
An Update on Osteoporosis Treatments
 An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
Bisphosphonate treatment break
 Bulletin 110 December 2015 Bisphosphonate treatment break Bisphosphonates have been widely used in the treatment of osteoporosis with robust data demonstrating efficacy in fracture risk reduction over
Bulletin 110 December 2015 Bisphosphonate treatment break Bisphosphonates have been widely used in the treatment of osteoporosis with robust data demonstrating efficacy in fracture risk reduction over
Osteoporosis Clinical Guideline. Rheumatology January 2017
 Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Controversies in Osteoporosis Management
 Controversies in Osteoporosis Management 2018 Northwest Rheumatism Society Meeting Portland, OR April 28, 2018 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Institute
Controversies in Osteoporosis Management 2018 Northwest Rheumatism Society Meeting Portland, OR April 28, 2018 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Institute
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays. Suzanne Morin MD FRCP FACP McGill University May 2014
 Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Horizon Scanning Technology Briefing. Zoledronic Acid (Aclasta) once yearly treatment for postmenopausal. National Horizon Scanning Centre
 once yearly treatment for postmenopausal. National Horizon Scanning Centre") Horizon Scanning Technology Briefing National Horizon Scanning Centre Zoledronic Acid (Aclasta) once yearly treatment for postmenopausal osteoporosis December 2006 This technology summary is based on information
Horizon Scanning Technology Briefing National Horizon Scanning Centre Zoledronic Acid (Aclasta) once yearly treatment for postmenopausal osteoporosis December 2006 This technology summary is based on information
Osteoporosis Agents Drug Class Prior Authorization Protocol
 Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis: current treatment and future prospects. Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus
 Osteoporosis: current treatment and future prospects Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus Disclosures Consultancy and speaking fees for Gilead, related to development
Osteoporosis: current treatment and future prospects Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus Disclosures Consultancy and speaking fees for Gilead, related to development
sad EFFECTIVE DATE: POLICY LAST UPDATED:
 Medical Coverage Policy Bone Mineral Density Studies sad EFFECTIVE DATE: 06 07 2011 POLICY LAST UPDATED: 11 06 2018 OVERVIEW Bone density studies can be used to identify individuals with osteoporosis and
Medical Coverage Policy Bone Mineral Density Studies sad EFFECTIVE DATE: 06 07 2011 POLICY LAST UPDATED: 11 06 2018 OVERVIEW Bone density studies can be used to identify individuals with osteoporosis and
Drug Intervals (Holidays) with Oral Bisphosphonates
 with Oral Bisphosphonates") Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017
 Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Calcium, Vitamin D and Bisphosphonates: Disclosures. Benefits, Risks and Drug Holiday. Calcium YES or NO? Calcium Bad News!!
 Calcium, Vitamin D and Bisphosphonates: Benefits, Risks and Drug Holiday Disclosures I am disclosing financial relationships as follows: Global Advisory Boards: Amgen, Lilly, Merck, Novartis Research grants:
Calcium, Vitamin D and Bisphosphonates: Benefits, Risks and Drug Holiday Disclosures I am disclosing financial relationships as follows: Global Advisory Boards: Amgen, Lilly, Merck, Novartis Research grants:
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary
 Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Guideline for the investigation and management of osteoporosis. for hospitals and General Practice
 Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Osteoporosis Medications: A Case-Based Discussion. Laila S. Tabatabai, MD August 5, 2017
 Osteoporosis Medications: A Case-Based Discussion Laila S. Tabatabai, MD August 5, 2017 Disclosures Eli Lilly Radius Objectives Determine which patients with low bone density require treatment, along with
Osteoporosis Medications: A Case-Based Discussion Laila S. Tabatabai, MD August 5, 2017 Disclosures Eli Lilly Radius Objectives Determine which patients with low bone density require treatment, along with
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
Pathway from Fracture or Risk Factor to Treatment
 Appendix 6A - Guidance on Diagnosis and Management of Osteoporosis Pathway from Fracture or Risk Factor to Treatment Fragility Fracture = fracture sustained from a low energy fall from standing height
Appendix 6A - Guidance on Diagnosis and Management of Osteoporosis Pathway from Fracture or Risk Factor to Treatment Fragility Fracture = fracture sustained from a low energy fall from standing height
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Session 4: New Evidence-Based Clinical Prac ce Guidelines B: Management of Osteoporosis in Post-Menopausal Women 4:15pm - 5:15pm
 January 20-22, 2012 Des Moines Marrio, 700 Grand Avenue, Des Moines, IA Session 4: New Evidence-Based Clinical Prac ce Guidelines B: Management of Osteoporosis in Post-Menopausal Women 4:15pm - 5:15pm
January 20-22, 2012 Des Moines Marrio, 700 Grand Avenue, Des Moines, IA Session 4: New Evidence-Based Clinical Prac ce Guidelines B: Management of Osteoporosis in Post-Menopausal Women 4:15pm - 5:15pm
Update on Osteoporosis 2016
 WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 21 July 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 21 July 2010 ACTONEL 5 mg, film-coated tablet B/14 (CIP code: 354 362-3) ACTONEL 30 mg, film-coated tablet B/28 (CIP
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 21 July 2010 ACTONEL 5 mg, film-coated tablet B/14 (CIP code: 354 362-3) ACTONEL 30 mg, film-coated tablet B/28 (CIP
Osteoporosis in Men Wendy Rosenthal PharmD. This program has been brought to you by PharmCon
 Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Interpreting DEXA Scan and. the New Fracture Risk. Assessment. Algorithm
 Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Page 1. Osteoporosis Warm-Up: Which of the Following is True? Diagnosis and Treatment of Osteoporosis: What is New in What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What is New in 2017 Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis
Diagnosis and Treatment of Osteoporosis: What is New in 2017 Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis
Tymlos (abaloparatide)
") Tymlos (abaloparatide) Policy Number: 5.01.638 Last Review: 11/2018 Origination: 10/2017 Next Review: 11/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Tymlos
Tymlos (abaloparatide) Policy Number: 5.01.638 Last Review: 11/2018 Origination: 10/2017 Next Review: 11/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Tymlos
Effective Health Care
 Number 12 Effective Health Care Comparative Effectiveness of Treatments To Prevent Fractures in Men and Women With Low Bone Density or Osteoporosis Executive Summary Background Osteoporosis is a systemic
Number 12 Effective Health Care Comparative Effectiveness of Treatments To Prevent Fractures in Men and Women With Low Bone Density or Osteoporosis Executive Summary Background Osteoporosis is a systemic
nogg Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK
 nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
Disclosures. Osteoporosis and Fracture Prevention. Objectives. Objectives. Osteoporosis Overview. Advisory Board: Hologic Advisory Board: LabCorp
 Disclosures Osteoporosis and Fracture Prevention Advisory Board: Hologic Advisory Board: LabCorp Nancy R. Berman MSN, ANP-BC, NCMP, FAANP Adult Nurse Practitioner/Colposcopist Certified Menopause Practitioner
Disclosures Osteoporosis and Fracture Prevention Advisory Board: Hologic Advisory Board: LabCorp Nancy R. Berman MSN, ANP-BC, NCMP, FAANP Adult Nurse Practitioner/Colposcopist Certified Menopause Practitioner
Misuse of Bisphosphonates. Dr Rukhsana Parvin Associate Professor Department of Medicine Enam Medical College & Hospital
 Misuse of Bisphosphonates Dr Rukhsana Parvin Associate Professor Department of Medicine Enam Medical College & Hospital Introduction Bisphosphonates are chemically stable analogues of pyrophosphate compounds.
Misuse of Bisphosphonates Dr Rukhsana Parvin Associate Professor Department of Medicine Enam Medical College & Hospital Introduction Bisphosphonates are chemically stable analogues of pyrophosphate compounds.
Focusing on the Patient: Diagnosis and Management of Osteoporosis
 Focusing on the Patient: Diagnosis and Management of Osteoporosis Learning Objectives After participating in this educational activity, participants should be able to: 1. Apply updated guidelines to assess
Focusing on the Patient: Diagnosis and Management of Osteoporosis Learning Objectives After participating in this educational activity, participants should be able to: 1. Apply updated guidelines to assess
NAMS Practice Pearl. Use of Drug Holidays in Women Taking Bisphosphonates. Released April 1, 2013
 NAMS Practice Pearl Use of Drug Holidays in Women Taking Bisphosphonates Released April 1, 2013 Dima L. Diab, MD 1, and Nelson B. Watts, MD 2 ( 1 Cincinnati VA Medical Center, Cincinnati, OH, 2 Mercy Health
NAMS Practice Pearl Use of Drug Holidays in Women Taking Bisphosphonates Released April 1, 2013 Dima L. Diab, MD 1, and Nelson B. Watts, MD 2 ( 1 Cincinnati VA Medical Center, Cincinnati, OH, 2 Mercy Health
S H A R E D C A R E G U I D E L I N E Drug: Denosumab 60mg injection Indication: treatment of osteoporosis in postmenopausal women
 S H A R E D C A R E G U I D E L I N E Drug: Denosumab 60mg injection Indication: treatment of osteoporosis in postmenopausal women Introduction Indication: Denosumab (Prolia ) is recommended in NICE TA204
S H A R E D C A R E G U I D E L I N E Drug: Denosumab 60mg injection Indication: treatment of osteoporosis in postmenopausal women Introduction Indication: Denosumab (Prolia ) is recommended in NICE TA204
Monitoring Osteoporosis Therapy
 Monitoring Osteoporosis Therapy SUZANNE MORIN DEPT OF MEDICINE, DIVISION OF GENERAL INTERNAL MEDICINE, MUHC CENTRE FOR OUTCOMES RESEARCH AND EVALUATION, RI MUHC November 2017 Conflict of Interest Disclosures
Monitoring Osteoporosis Therapy SUZANNE MORIN DEPT OF MEDICINE, DIVISION OF GENERAL INTERNAL MEDICINE, MUHC CENTRE FOR OUTCOMES RESEARCH AND EVALUATION, RI MUHC November 2017 Conflict of Interest Disclosures
Outline. Switching treatment. Evidence from randomized trials. The effects of switching 7/8/2016. When and for whom? Steven Cummings, MD
 Outline Switching treatment When and for whom? Steven Cummings, MD Focus on switching from alendronate or risedronate Evidence about the effects of switching on BMD Purposes of switching Symptoms Poor
Outline Switching treatment When and for whom? Steven Cummings, MD Focus on switching from alendronate or risedronate Evidence about the effects of switching on BMD Purposes of switching Symptoms Poor
Osteoporosis update. Dr. Claire Vandevelde Consultant Rheumatologist, LTHT
 Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Osteoporosis - New Guidelines. Michelle Glass B.Sc. (Pharm) June 15, 2011
 June 15, 2011") Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
9/9/2015 OSTEOPOROSIS WHAT S NEW AND ON THE HORIZON IN SCREENING, DRUG HOLIDAYS, SUPPLEMENTS, CONSERVATIVE THERAPY DISCLOSURES
 OSTEOPOROSIS WHAT S NEW AND ON THE HORIZON IN SCREENING, DRUG HOLIDAYS, SUPPLEMENTS, CONSERVATIVE THERAPY Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Stock options/holdings,
OSTEOPOROSIS WHAT S NEW AND ON THE HORIZON IN SCREENING, DRUG HOLIDAYS, SUPPLEMENTS, CONSERVATIVE THERAPY Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Stock options/holdings,
8/6/2018. Glucocorticoid induced osteoporosis: overlooked and undertreated? Disclosure. Objectives. Overview
 Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
From Fragile to Firm. Monika Starosta MD. Advocate Medical Group
 From Fragile to Firm Monika Starosta MD Advocate Medical Group Bone Remodeling 10% remodeled each year Calcium homoeostasis Maintain Mechanical strength Replace Osteocytes Release Growth Factors Bone remodeling
From Fragile to Firm Monika Starosta MD Advocate Medical Group Bone Remodeling 10% remodeled each year Calcium homoeostasis Maintain Mechanical strength Replace Osteocytes Release Growth Factors Bone remodeling
This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only.
 This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only. INJECTABLE OSTEOPOSIS AGENTS SUBJECT Pharmacologic Agents: Bisphosphonates: Boniva IV (ibandronate) Reclast (zoledronic
This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only. INJECTABLE OSTEOPOSIS AGENTS SUBJECT Pharmacologic Agents: Bisphosphonates: Boniva IV (ibandronate) Reclast (zoledronic
Beyond the Break. After Breast Cancer: Osteoporosis in Survivorship. Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO
 FCFP Regional Primary Care Lead CCO") Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
Fragile Bones and how to recognise them. Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey
 Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Coordinator of Post Professional Programs Texas Woman's University 1
 OSTEOPOROSIS Update 2007-2008 April 26, 2008 How much of our BMD is under our control (vs. genetics)? 1 2 Genetic effects on bone loss: longitudinal twin study (Makovey, 2007) Peak BMD is under genetic
OSTEOPOROSIS Update 2007-2008 April 26, 2008 How much of our BMD is under our control (vs. genetics)? 1 2 Genetic effects on bone loss: longitudinal twin study (Makovey, 2007) Peak BMD is under genetic
Clinical Specialist Statement Template
 Clinical Specialist Statement Template Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can
Clinical Specialist Statement Template Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can
Using the FRAX Tool. Osteoporosis Definition
 How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
Fracture=Bone Attack:
 Fracture=Bone Attack: Linking Hip Fractures to Osteoporosis Care Angela M. Cheung, MD, PhD, FRCPC Professor of Medicine, University of Toronto Potential Conflicts of Interests Industry Grants (to UHN)
Fracture=Bone Attack: Linking Hip Fractures to Osteoporosis Care Angela M. Cheung, MD, PhD, FRCPC Professor of Medicine, University of Toronto Potential Conflicts of Interests Industry Grants (to UHN)