Prognostication Art & Science (or just another dirty word?)
|
|
|
- Morgan Bradley
- 6 years ago
- Views:
Transcription
1 Prognostication Art & Science (or just another dirty word?) Richard Stephenson MD It s About How You Live January 28, 2011 Dick.Stephenson@hospicecarecenter.org
2 Objectives The program says Discuss the use of prognostication when working with patients and families in need of a palliative care consult Suggesting 1. How do we use prognostication to identify patients/families in need of palliative care? 2. What prognostic tools do we have available for that purpose? 3. How do we talk prognosis with patients and families?
3 Palliative Care (and hospice) Is the medical specialty focused on improving the quality of life of people facing serious illness. Emphasis is placed on pain and symptom management, communication and coordinated care. Palliative care is appropriate from the time of diagnosis and can be provided along with curative treatment. Different from Hospice Terminal illness 6 month prognosis Forego curative Prognostic tools might be somewhat different
4 Presumes Prognostication Important? Goal setting Decision making Treatment options Future planning Resource utilization Hospice referral Care-planning Hospice discharge Done poorly Burdensome Futile care Painful Stressful Done well Reduced stress Dr/Pt alliance Appropriate care Resource utilization
5 Prognostication Is it a word? Sounds bad, eh? Prognosis, n. (Greek literally fore-knowing, foreseeing) is a medical term denoting the doctor s prediction of how a patients disease will progress, and whether there is a chance of recovery. Wictionary Prognostication, n. 1 a forecast; prediction 2 the act of foretelling. WB Dictionary A prognosis is more than a best guess it is a prediction of the likelihood of a given outcome based on multiple sources of information. Sinclair
6 Just another dirty word? Not to be said in public Doctors don t like to talk about it Patients don t want to hear it A classic, therapeutic dilemma Like treating an asymptomatic condition (HBP) With expensive medications that make you feel bad Lots of challenges
7 Doctors Fear extinguishing hope Feel we lack accurate tools Time-consuming Lack Education Prognostic tools Communication Prior knowledge of the future may be very sad Hard place for lots of us to go We practice, Realism, optimism, or avoidance.
8 Do doctors want to tell? Christakis, NA. Attitude and self-reported practice regarding prognostication in a national sample of internists. Archiv Intern Med. 1998;158(21): Survey of 1311 Internists / 697 respondents How long do I have to live? 10X Withdrew/Withheld 5X; Hospice referral 5X Terminal = / weeks to live
9 Majority Really Dislike Prognostication Characteristic Freq (%) Stressful to make predictions 60.4 Difficult 58.7 Wait to be asked by patient 43.7 Believe patients expect too much certainty 80.2 Error will result in loss of patient confidence 50.2 Should avoid being specific 89.9 Inadequate training in prognostication 56.8
10 How Good Are We? Christakis, NA. Extent and determinants of error in doctors prognoses in terminally ill patients: prospective cohort study. BMJ 2000;320: At the time of hospice referral, MD asked for a Clinical Prediction of Survival (CPS) Only 20% accurate Overestimated survival by a factor of 5! (but consistently) Experience helps; relationship hinders Implications Late hospice referral, LOS 1 month (rather than 3), counterproductive choices (futile, aggressive, $$) Corrections Disinterested, second opinion
11 Prognostic Disclosure to Patients with Cancer near the End of Life. Lamont EB, Christakes NA. Ann Intern Med. 2001;134: Compared formulated and communicated diagnosis How often MDs give frank survival estimates to patients who request them? Physician telephone survey (n=326)
12 Results 23% would not communicate temporally specific prognosis 37% would 40% would communicate discrepant prognosis Median formulated Px 75 days Median communicated Px 90 days Median survival 26 days
13 More Pts with with optimistic or no Px communicated to them had shortest survival Pessimistic > the longest Older pt > franker Less functional > franker Older MDs favored (3X) no disclosure Less confident in Prognosis less disclosure More experience with hospice less frank Female MDs more pessimistic (maybe more accurate)
14 2 nd Opinion?
15 Authors Concluded Provided frank estimate only 37% Able and willing to formulate, but not communicate (even with insistent patients) Conscious and unconscious optimism Confident in Px, no more accurate, but if not confident less likely to be frank Most types of MDs avoid frank disclosure to most types of patients with cancer To be of real use to patients, the science of prognostication must be improved! Patients want accurate Px Tactful, respectful; not truth-dumping
16 Patients Views on Prognosis Communicating with realism and hope: Incurable cancer patients views on the disclosure of prognosis. Hagerty et al. J Clin Onc. 2005;23: consecutive metastatic cancer patients, 30 oncologists, Sydney, Australia A clear majority (but not all) of patients want: Individualized and realistic disclosure From a confident, collaborative, informed and supportive cancer specialist Detailed information, checking for understanding, time for questions Hope-giving approach favored
17 Additional evidence suggests Honest, ongoing communication of prognosis Reinforces trust and hope Enhances a mutually respectful doctor-patient relationship Facilitates treatment decisions that are consistent with underlying values
18 What Simple Tools Do We Have? (Pessimistic, accurate female physician)
19 How Good Are They?
20 Good Evidence-Based Medicine?
21 Tools KISS (Keep It Simple Stephenson) More complicated tools won t be generally useful Simple tools or indicators to suggest Palliative Care Consult or at least Turn our attention to a palliative plan of care Keeping PC definition in mind combined with all other medical care that is appropriate What might suggest a significant shift in focus or PC consult? And then have more sophisticated tools available
22 As I was thinking about it Boom! Ahead-of-print alert from J Palliative Medicine Identifying patients in need of a PC assessment in the hospital setting. Weissman DE & Meier DE. J Palliat Med A consensus report from CAPC Consultation Triggers Audio Conference CAPC Checklist theory
23 Criteria for a PC Assessment At the time of Admission A potential life-limiting condition and Primary Criteria (global indicators) The surprise question (SQ) You would not be surprised if the patient died within 12 months or before adulthood Frequent admissions Admission prompted by difficult-to-control symptoms Complex care requirements (home vent) Failure to thrive (function, nutrition, cognition) Secondary criteria (more-specific indicators) LTCF, chronic home O 2, hospice enrollee Elderly, cognitively impaired, acute hip fx Metastatic or locally advanced CA, out-of-hospital arrest Limited social support; absence of advance care plans
24 Criteria for a PC Assessment During each Hospital Day A potentially life limiting condition and Primary Criteria (global indicators) The surprise question Difficult-to-control symptoms ICU LOS > 7 days Lack of goals clarity Disagreements (Pt, staff, family RE Rx, CPR, PEG) Secondary criteria Transplant (awaiting, not elig), Pt/F distress or request Candidate/consult for: PEG, trach, dialysis, LVAD or AICD, LTAC discharge, BMTransplant
25 (Focus on) KISS = SQ! Are these simple Primary Criteria accurate enough to: Initiate PC Assessment and/or Consult Begin a process with patient and family Turn to more specific criteria and Apply more sophisticated prognostic tools if necessary These indicators also apply to LTCF, office or homecare settings In a systems-based way, great tool for nursing Gee, Dr. S., I was doing the checklist on Mrs. Myra Bund in Rm 201, it really wouldn t surprise me if she died this year. We need to talk to her about what she really wants.
26 SQ The Surprise Question Talked about it for years Hospices market physicians with 6-month SQ Some apply over-estimation prognostic factor of 3X and say, Would you be surprised if your patient died in the next 18 mos to 2 years? (to get patients who die in 6 mos) Applied to PC settings as the 12-month SQ Seems so simple soft science you say? Wouldn t it be nice if it was that simple? Is there hard science?
27 Predicting 6-Month Mortality for Patients on Hemodialysis Cohen, Moss, et al. Cl J Am Soc Neph 2010 Despite specific guidelines, nephrologists rarely talk about prognosis accuracy/hope This study of 512 hemodialysis patients Combined actuarial data from the record Charlson Comorbidity Index (CCI) With SQ = 6-months Would I be surprised if this patient died in the next 6 months? Came up with an integrated prognostic model Integrating SQ with significant variables
28 Charlson Comorbidity Index Beddhu et al 2000 Comorbidity Score Condition CAD, CHF, PVD, CerebroVD, Dementia, COPD, PUD, CLD, DM Hemiplegia, Mod-Sev Renal, DM with end-organ damage, any tumor, leukocytosis, lymphocytopenia Mod or severe liver disease Metastatic solid tumor, AIDS Add 1 for each decade > 40. Score > 8 had a 1-year survival of 50% (Factor in alb and (Karnofsky) perf status would help)
29 Known Major Factors Influence Prognosis Older age Nutritional status Functional status Comorbid conditions CHF, COPD, PVD, CVD, MI, DM, CA, dementia Serum albumin! In 133 studies! < 3.0 g/dl vs > 4.0 g/dl = 4.4X risk of death < 3.5 g/dl associated with 1 year mortality = 50%
30 Results No response to SQ was a statistically significant marker for worse survival Also significant Albumin, older age, presence of dementia, PVD All more significant that full CCI At the completion of the study (2 yrs) 54.9% of No group was dead vs. just 17.0% of Yes group Simpler was better, resulting in a 5-term integrated prognostic model 4 factors + Surprise Question
31 Prognostic Significance of the Surprise Question in CA Patients Moss et al JPM 2010 Not previously studied in cancer patients (well actually only in HD patients work to do) 853 consecutive cancer patients in an academic cancer center with breast, lung or colon cancer Used SQ = 12 months No had a 7X greater hazard of death than Yes Simple, feasible, and effective tool to identify cancer patients at a greatly increased risk of 1- year mortality.
32 Compare to Palliative Prognostic Score (PPS 2 ) for cancer Prognostic Factor Dyspnea Absent Present Anorexia Absent Present Karnofsky Performance Status >/= Clinical Prediction of Survival > 12 wks wks Total WBC count: Normal K High K Very High > 11K Lymphocyte percentage Normal 20-40% Low % Very low % Partial Score PPS = dyspnea score + anorexia score + KPS score + CPS score + total WBC score + lymph % score Total score = 70% of 30d = 30-70% = < 30% (of surviving 30-days)
33 Many General and Disease-Specific Tools/Indices Emerging Palliative Performance Scale (PPS) CHF COPD ESRD ALS Cancer Dementia Prognostication is no longer just another dirty word; there is science
34 Palliative Performance Scale (PPS) Developed 1996 Victoria Hospice Society, BC, Canada Designed to measure functional performance and progressive decline to: Communicate patient status Evaluate home nursing care workloads Study effects of treatment on the patient Plan visits according to patient acuity and Make discharge decisions Combines performance and extent of disease with nutritional and mental status Scores range from 0 (dead) to 100% in increments of 10 Many hospices and PCServices use PPS
35 Palliative Performance Scale (PPS) % Score Amb Activity/Evi DZ Self-care Nutr Intake Conscious 100 Full Normal; NEDz Full Normal Full 90 Full Nl; Some EDz Full Normal Full 80 Full Nl w/ effort; Sig Dz Full Nl or reduced Full 70 Reduced Unable to do Nl work; Sig Dz Full Nl or reduced Full 60 Reduced Unable to hobby; extensive Dz Occ asst nec Nl or reduced Full or confuse 50 Sit or lie Unable any work; extensive Dz Occ asst req Nl or reduced Full or confuse 40 Mstly Bed Unable to do most activities Mainly asst Nl or reduced Full, drowsy, +/- conf 30 Total Bed As above Total Care Reduced As above 20 As above As above Total Care Minimal sips As above 10 As above As above Total Care Mouth care only Drowsy or coma +/- conf 0 Death
36 Validation of PPS ½ dozen studies Most recent PC Consults in Chapel Hill! O. Olajide, Laura Hanson et al PPS correlates well with length of survival Different numbers in different populations but correlates well Previous studies in Home, NH, Hospital, and Inpatient units Not widely used in this country Can also help validate admission, plan care, plan discharge
37 PPS and Survival in Days Inpatient PC Unit adapted from Lau et al % 20% 30% 40% 50%
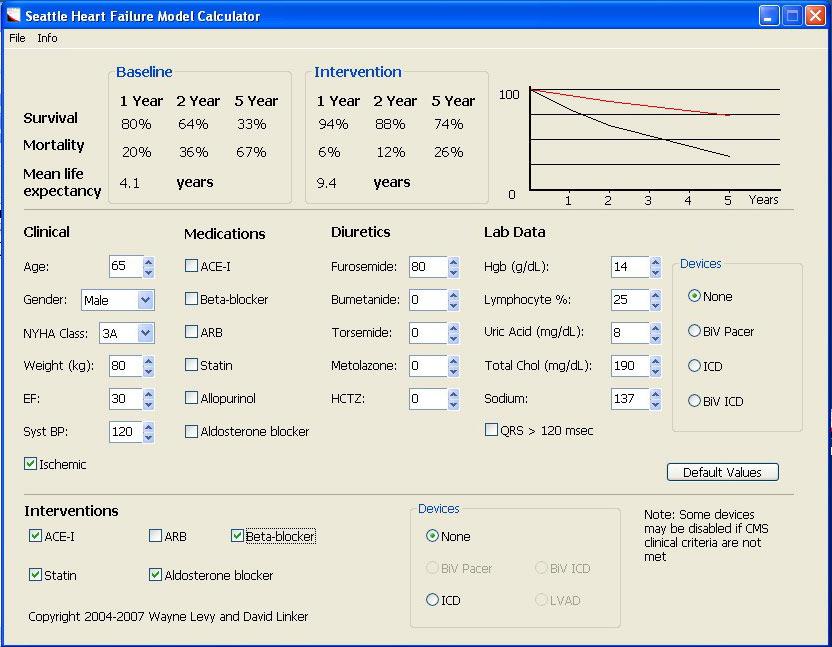
38 CHF The Seattle Heart Failure Model (SHFM) A much more sophisticated tool Web-based Combines: Clinical and lab values, HF meds, and devices Age, sex, NYHA class, EF, BP, pacer, ICD, etc. Baseline data calculates 1-, 2-, 5-years survival and mortality rate and mean life expectancy Post-intervention can be input and re-calculated
39
40 James T et al. Increasing palliative consults for HF using the SHFM. J Hosp Pall Pall Nurs. 2010; Applied tool retrospectively to 214 patients DC d with Dx of CHF Divided into 3 groups based on life expectancy < 1.5 yrs; yrs; > 5 yrs 27 fit < 1.5 yrs and 17 died within a year On average 2.8 mos and 9.6 mos shorter than predicted Most had postintervention scores that declined or did not improve 75 with > 1.5 yrs died in study period Now use SHFM < 1.5 for automatic PC referral Patients are not informed of their score
41 Mitchell SL, Miller DC, Teno JM et al. Prediction of 6-month survival of NH residents with advanced dementia using ADEPT JAMA. 2010;304(17): Used minimum data set (MDS) data To create, retrospectively validate, then re-derive and prospectively validate a bedside score a 12-item Advanced Dementia Prognostic Tool (ADEPT) Looked at 606 patients and compared with Hospice eligibility guidelines Ability to predict residents at high risk of death in 6 months was modest but better Potential for setting scores as triggers and doing further study (or PC consult or compare to SQ)
42 Table 1. ADEPT Scoring in Nursing Home Residents With Advanced Dementia (N = 606).
43 Enough with tools! Or we ll look like this
44 The Art of prognostication Part of a therapeutic alliance Maltoni et al. J Clin Onc 2005 Principles Process of prognostication should not impose an additional burden ie time-consuming, too much detail Process, probabilistic, dramatically inaccurate for some. Never lose sight of patient or their individual patient trajectory. Deeply embedded in open, flexible, patient-centered dialogue Communicate when requested (?). Right to know or not know. Ethical, religious, cultural, psychological considerations Avoid inflicting additional harm Emphasize a holistic therapeutic approach beyond time limits
45 Discussing Prognosis from Back A, Arnold R, Tulsky J: Mastering Communication with Seriously Ill Patients How much do you want to know? Normalize a range of patient interest 1. Some people want details 2. Some want to focus on the big picture 3. Some would rather not discuss it at all What would be best for you? The power of some, many, and most
46 For Patients Who Want Information 1. Negotiate the content Different ways to answer statistics, worst & best case scenario, future events What would work best for you? 2. Provide the information pause & check in 3. Acknowledge patient/family reaction It looks like the information is not what you were expecting. I wish it wasn t so I wish that there was more tell me what you re thinking 4. Check for understanding Tell me what you are taking away from this discussion. Tell me what you will tell your spouse.
47 Some Patients Maybe Relieved Patients are often the best teachers Mrs. B.
48 For Patients Who Don t 1. Try to elicit and understand why 2. Acknowledge the patient s concerns 3. Ask for permission to revisit the topic 4. Make a private assessment about whether prognosis might change the patient s current decision-making Negotiate for limited disclosure Do they want someone else to know I understand you would rather not talk about it and respect that. I also think there are some important reasons to talk about it. I think it might influence some decisions
49 How good are we? H & PC Specialist Doctors & Nurses Twomey F et al. Prediction of patient survival by healthcare professionals in a specialist PCU To compare accuracy of different professionals MDs (PC and nonpc); RNs; CNAs; ward sisters CPS in ranges (<24h;24-72h;72h-10d;10d-1m;1-3m;>3m) To identify helpful predictive variables Accurately predicted survival only ~50% Nursing and junior medical more accurate Assistants least accurate Senior medical, when in error, tended to underestimate (Ward sisters not noted in results) Independent mobility only predictive variable of LOS
50 How Good Are We? Palliative Care Teams Higginson I, Constantini M. Accuracy of prognosis estimates by four palliative care teams: a prospective cohort study. To test the accuracy of giving an estimated range of prognosis rather than a specific time Mostly nurses, a few physicians and SWs Compared minimum and maximum estimated survival with actual 42% accurate; 36% optimistic; 22% pessimistic More accurate if minimum estimate < 14 days (closer to death) horizon effect Concludes discussion is more important and if appropriate consult more experienced clinicians
51 Prognostication Competencies Are we testing ourselves? Quality Assessment and Performance Improvement Every hospice, PC Service, and unit Every admission CPS, SQ, and/or disease-specific tool Board questions about tools and conversation ACGME (Accreditation Council for Graduate Medical Education) CHPN (Certified Hospice and Palliative Nurse) More research studies it wouldn t take much to tip QAPI into research
52 Well-trained PC Super Docs and Nurses! Capable of using multiple scores & indices!
53 Summary Prognostication Simple tools beget more sophisticated tools As Donald Berwick, now Administrator of CMS, said at ACP in 1999: If you would not be surprised that your patient died in the coming months tell him. But tell him in a patient-centered empathetic way with negotiated content Let s get good at it! Let s study our ownselves!
54 References 1. Sinclair C. Communicating a prognosis in advanced cancer. Supp Onc 2006;4: Christakis, NA. Attitude and self-reported practice regarding prognostication in a national sample of internists. Archiv Intern Med. 1998;158(21): Christakis, NA. Extent and determinants of error in doctors prognoses in terminally ill patients: prospective cohort study. BMJ 2000;320: Lamont EB, Christakes NA. Prognostic Disclosure to Patients with Cancer near the End of Life. Ann Intern Med. 2001;134: Hagerty et al. Communicating with realism and hope: Incurable cancer patients views on the disclosure of prognosis. J Clin Onc. 2005;23: Weissman DE, Meier DE. Identifying patients in need of a palliative care assesment in the hospital setting. J Palliat Med. 2011;14 DOI: 10:1089/jpm
55 7. Cohen LM et al. Predicting six-month mortality for patients who are on Cl J Am Soc Neph. 2010;5: Beddhu S, Bruns FJ, Saul M, Seddon P, Zeidel ML. A simple comorbidity scale predicts clinical outcomes and costs in dialysis patients. Am J Med 2000;108: Moss AH et al. Prognostic significance of the surprise question in cancer patients. J Palliat Med 2010;13: Lamont EB and Christakis NA. Complexities in prognostication in advanced cancer. JAMA 2003;290: Back A, Arnold R, Tulsky J: Mastering Communication with Seriously Ill Patients. New York, NY: Cambridge University Press, Back A, Arnold R. Discussing prognosis: How much do you want to know? Talking to patients who are prepared for explicit information. J Clin Onc 2006;24: Back A, Arnold R. Discussing prognosis: How much do you want to know? Talking to patients who do not want information or are ambivalent. J Clin Onc 2006;24: Twomey F et al. Prediction of patient survival by healthcare professionals in a specialist palliative care inpatient unit: A prospective study. Am J Hosp Pall Care. 2008;25: Higginson IJ, Contantini M. Accuracy estimates by four palliative care teams: A prospective cohort study. BMC PC. 2002;1:1-5.
56 16. Olajide O, Hanson L, et al. Validation of the Palliative Performance Scale in the acute tertiary care hospital setting. J Pall Med 2007;10: Anderson F, Downing GM. Palliative Performance Scale (PPS): A new tool. J Pall Care 1996;12: Virik K, Glare P. Validation of the Palliative Performance Scale for inpatients admitted to a Palliative Care Unit in Sydney, Australia. J Pain S M 2002;23: Harrold J, Casarett D, et al. Is the palliative performance scale a useful predictor of mortality in a heterogenious hospice population? J Pall Med 2005;8: James T et al. Increasing palliative care consults for heart failure inpatients using the Seattle Heart Failure Model. J Hosp Pall Nurs 2010;12: Mitchell LS et al. Prediction of 6-month survival of nursing home residents with advanced dementia using ADEPT vs hospice eligibility guidelines. JAMA. 2010;304(17):
Discussing Prognosis. David Ross Russell MD ProHealth Physicians Inc.
 Discussing Prognosis David Ross Russell MD ProHealth Physicians Inc. Prognosis- peeling back the layers Not a new Science Psalm 39 LORD, make me to know mine end, and the measure of my days. Hippocrates
Discussing Prognosis David Ross Russell MD ProHealth Physicians Inc. Prognosis- peeling back the layers Not a new Science Psalm 39 LORD, make me to know mine end, and the measure of my days. Hippocrates
How Can Palliative Care Help Your Patient Get Home Sooner?
 How Can Palliative Care Help Your Patient Get Home Sooner? Annette T. Carron, D.O. Director Geriatrics and Palliative Care Botsford Hospital OMED 2014 Patient Care Issues That Can Delay Your Day/ Pain
How Can Palliative Care Help Your Patient Get Home Sooner? Annette T. Carron, D.O. Director Geriatrics and Palliative Care Botsford Hospital OMED 2014 Patient Care Issues That Can Delay Your Day/ Pain
How Long Do I Have? The Art and Science of Prognostication
 How Long Do I Have? The Art and Science of Prognostication Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Associate Program Director, Colorado
How Long Do I Have? The Art and Science of Prognostication Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Associate Program Director, Colorado
Top 3 Tips in Decision Making
 Top 3 Tips in Decision Making Jeanie Youngwerth, MD, FAAHPM University of Colorado School of Medicine Assistant Professor of Medicine, Hospitalist Associate Program Director, Colorado Palliative Medicine
Top 3 Tips in Decision Making Jeanie Youngwerth, MD, FAAHPM University of Colorado School of Medicine Assistant Professor of Medicine, Hospitalist Associate Program Director, Colorado Palliative Medicine
Evidence Based Prognostication
 Evidence Based Prognostication Christian T Sinclair, MD, FAAHPM 1 Overview Define benefits and limitations of open frequent prognostication Understand theories for accurate formulation of prognostication
Evidence Based Prognostication Christian T Sinclair, MD, FAAHPM 1 Overview Define benefits and limitations of open frequent prognostication Understand theories for accurate formulation of prognostication
Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations
 communication skills that every provider needs AND clinical triggers for PPC conversations") Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations Esmé Finlay, MD Division of Palliative Medicine University of
Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations Esmé Finlay, MD Division of Palliative Medicine University of
Prognostic Tools Compare the Models
 Prognostic Tools Compare the Models 31/07/2008 Dr Ray Viola Mark Corkum 34 Barrie St Kingston, Ontario Canada K7L 3W6 rav@queensu.ca (613) 549 6666 ext. 3223 1 Table of Contents Goal... 3 Sample Size...
Prognostic Tools Compare the Models 31/07/2008 Dr Ray Viola Mark Corkum 34 Barrie St Kingston, Ontario Canada K7L 3W6 rav@queensu.ca (613) 549 6666 ext. 3223 1 Table of Contents Goal... 3 Sample Size...
Guideline for Estimating Length of Survival in Palliative Patients
 http://pal 11 ative. into Cornelius Woelk MD, CCFP Medical Director of Palliative Care Regional Health Authority - Central Manitoba 385 Main Street Winkler, Manitoba, Canada R6W 1J2 Ph: 204-325-4312 Fax:
http://pal 11 ative. into Cornelius Woelk MD, CCFP Medical Director of Palliative Care Regional Health Authority - Central Manitoba 385 Main Street Winkler, Manitoba, Canada R6W 1J2 Ph: 204-325-4312 Fax:
THE ROLE OF PALLIATIVE CARE IN TREATMENT OF PATIENTS WITH CHRONIC, INFECTIOUS DISEASE
 THE ROLE OF PALLIATIVE CARE IN TREATMENT OF PATIENTS WITH CHRONIC, INFECTIOUS DISEASE JESSICA MCFARLIN MD ASSISTANT PROFESSOR OF NEUROLOGY DIVISION CHIEF, PALLIATIVE AND SUPPORTIVE CARE I HAVE NO COI OR
THE ROLE OF PALLIATIVE CARE IN TREATMENT OF PATIENTS WITH CHRONIC, INFECTIOUS DISEASE JESSICA MCFARLIN MD ASSISTANT PROFESSOR OF NEUROLOGY DIVISION CHIEF, PALLIATIVE AND SUPPORTIVE CARE I HAVE NO COI OR
WebEx Quick Reference
 Session 2 Drs. Alvin Moss & David Weissman WebEx Quick Reference Welcome to today s session! Please use Chat to All Raise your hand Participants for questions For technology issues only, please Chat to
Session 2 Drs. Alvin Moss & David Weissman WebEx Quick Reference Welcome to today s session! Please use Chat to All Raise your hand Participants for questions For technology issues only, please Chat to
A Practical Approach to Palliative Care in the ICU
 A Practical Approach to Palliative Care in the ICU Wendy Anderson, MD MS Critical Care Medicine and Trauma May 31, 2013 Disclosure Statement Dr. Anderson has no relevant financial relationships to disclose.
A Practical Approach to Palliative Care in the ICU Wendy Anderson, MD MS Critical Care Medicine and Trauma May 31, 2013 Disclosure Statement Dr. Anderson has no relevant financial relationships to disclose.
Palliative Care Consultative Service in Acute Hospital - Impact & Challenges
 Palliative Care Consultative Service in Acute Hospital - Impact & Challenges Dr. Annie Kwok Consultant Palliative Care Unit Department of Medicine & Geriatrics Caritas Medical Centre Contents Aging population
Palliative Care Consultative Service in Acute Hospital - Impact & Challenges Dr. Annie Kwok Consultant Palliative Care Unit Department of Medicine & Geriatrics Caritas Medical Centre Contents Aging population
Palliative Care in the Continuum of Oncologic Management
 Palliative Care in the Continuum of Oncologic Management PC in the Routine Continuum of Cancer Care Michael W. Rabow, MD Director, Symptom Management Service Helen Diller Family Comprehensive Cancer Center
Palliative Care in the Continuum of Oncologic Management PC in the Routine Continuum of Cancer Care Michael W. Rabow, MD Director, Symptom Management Service Helen Diller Family Comprehensive Cancer Center
Palliative Medicine Overview. Francine Arneson, MD Palliative Medicine
 Palliative Medicine Overview Francine Arneson, MD Palliative Medicine Palliative Medicine: Definition Palliative care: An approach that improves the quality of life of patients and their families facing
Palliative Medicine Overview Francine Arneson, MD Palliative Medicine Palliative Medicine: Definition Palliative care: An approach that improves the quality of life of patients and their families facing
USING PALLIATIVE PERFORMANCE SCALE
 USING PALLIATIVE PERFORMANCE SCALE S U A N D O K P A L L I A T I V E C A R E D A Y, J U N E 2 2 t h 2010 G. Michael Downing, MD Clin. Assoc. Prof, U of British Columbia, Fac. of Med. Adj. Ass t Prof, U
USING PALLIATIVE PERFORMANCE SCALE S U A N D O K P A L L I A T I V E C A R E D A Y, J U N E 2 2 t h 2010 G. Michael Downing, MD Clin. Assoc. Prof, U of British Columbia, Fac. of Med. Adj. Ass t Prof, U
Palliative Care in the ED:
 Palliative Care in the ED: Don t Just Do Something Stand There Eric Isaacs, MD, FACEP Attending Physician, San Francisco General Hospital and Trauma Center Professor of Emergency Medicine, University of
Palliative Care in the ED: Don t Just Do Something Stand There Eric Isaacs, MD, FACEP Attending Physician, San Francisco General Hospital and Trauma Center Professor of Emergency Medicine, University of
Palliative Care for Older Adults in the United States
 Palliative Care for Older Adults in the United States Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine Icahn School
Palliative Care for Older Adults in the United States Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine Icahn School
Palliative Medicine in Critical Care Not Just Hospice. Robin. Truth or Myth 6/11/2015. Francine Arneson, MD Palliative Medicine
 Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
There Is Something More We Can Do: An Introduction to Hospice and Palliative Care
 There Is Something More We Can Do: An Introduction to Hospice and Palliative Care presented to the Washington Patient Safety Coalition July 28, 2010 Hope Wechkin, MD Medical Director Evergreen Hospice
There Is Something More We Can Do: An Introduction to Hospice and Palliative Care presented to the Washington Patient Safety Coalition July 28, 2010 Hope Wechkin, MD Medical Director Evergreen Hospice
I want to Die a Free man : The Psycho-Social-Spiritual Issues Surrounding Death in the Prison System
 I want to Die a Free man : The Psycho-Social-Spiritual Issues Surrounding Death in the Prison System Loretta Lee Grumbles, MD Associate Professor of Medicine Director of Palliative Medicine Division Department
I want to Die a Free man : The Psycho-Social-Spiritual Issues Surrounding Death in the Prison System Loretta Lee Grumbles, MD Associate Professor of Medicine Director of Palliative Medicine Division Department
Palliative Care The Benefits of Early Intervention
 The Royal Marsden Palliative Care The Benefits of Early Intervention Dr Anna-Marie Stevens, Nurse Consultant Symptom Control and Palliative Care Team, The Royal Marsden NHS Foundation Trust, London, UK
The Royal Marsden Palliative Care The Benefits of Early Intervention Dr Anna-Marie Stevens, Nurse Consultant Symptom Control and Palliative Care Team, The Royal Marsden NHS Foundation Trust, London, UK
Hospice and Palliative Care An Essential Component of the Aging Services Network
 Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
2012 AAHPM & HPNA Annual Assembly
 in the Last 2 Weeks of Life: When is it Appropriate? When is it Not Appropriate? Disclosure No relevant financial relationships to disclose AAHPM SIG Presentation Participants Eric Prommer, MD, FAAHPM
in the Last 2 Weeks of Life: When is it Appropriate? When is it Not Appropriate? Disclosure No relevant financial relationships to disclose AAHPM SIG Presentation Participants Eric Prommer, MD, FAAHPM
CareFirst Hospice. Health care for the end of life. CareFirst
 Hospice Health care for the end of life 1 What is Hospice? Hospice is a philosophy- When a person in end stages of an illness can no longer receive, or wants to receive, life sustaining treatment, he or
Hospice Health care for the end of life 1 What is Hospice? Hospice is a philosophy- When a person in end stages of an illness can no longer receive, or wants to receive, life sustaining treatment, he or
Interprofessional Webinar Series
 Interprofessional Webinar Series Prognostication I: Improving Accuracy to Support Care and Hospice Access Pauline Lesage, MD, LLM Physician Educator MJHS Institute for Innovation in Palliative Care Disclosure
Interprofessional Webinar Series Prognostication I: Improving Accuracy to Support Care and Hospice Access Pauline Lesage, MD, LLM Physician Educator MJHS Institute for Innovation in Palliative Care Disclosure
COMMUNICATION ISSUES IN PALLIATIVE CARE
 COMMUNICATION ISSUES IN PALLIATIVE CARE Palliative Care: Communication, Communication, Communication! Key Features of Communication in Appropriate setting Permission Palliative Care Be clear about topic
COMMUNICATION ISSUES IN PALLIATIVE CARE Palliative Care: Communication, Communication, Communication! Key Features of Communication in Appropriate setting Permission Palliative Care Be clear about topic
PALLIATIVE CARE GOALS of CARE: DNR. Debra Luczkiewicz MD Kelly Denall ANP Supportive Medical Partners
 PALLIATIVE CARE GOALS of CARE: DNR Debra Luczkiewicz MD Kelly Denall ANP Supportive Medical Partners OBJECTIVES Understand the scope of palliative care. Describe the differences between Hospice and palliative
PALLIATIVE CARE GOALS of CARE: DNR Debra Luczkiewicz MD Kelly Denall ANP Supportive Medical Partners OBJECTIVES Understand the scope of palliative care. Describe the differences between Hospice and palliative
Palliative Care & Haematology: Known Unknowns or Unknown Unknowns? Working towards a better collaboration.
 Palliative Care & Haematology: Known Unknowns or Unknown Unknowns? Working towards a better collaboration. Dr Michelle Gold Director, Palliative Care Alfred Health ANZSPM Update June 2013 % Epidemiology
Palliative Care & Haematology: Known Unknowns or Unknown Unknowns? Working towards a better collaboration. Dr Michelle Gold Director, Palliative Care Alfred Health ANZSPM Update June 2013 % Epidemiology
Palliative and End of Life Care Extended Workshop: CSIM 2014 Calgary. Karen Tang, MD FRCPC General Internal Medicine University of Calgary
 Palliative and End of Life Care Extended Workshop: CSIM 2014 Calgary Karen Tang, MD FRCPC General Internal Medicine University of Calgary Drs. Brisebois, Hiebert, and I have no affiliation with pharmaceutical,
Palliative and End of Life Care Extended Workshop: CSIM 2014 Calgary Karen Tang, MD FRCPC General Internal Medicine University of Calgary Drs. Brisebois, Hiebert, and I have no affiliation with pharmaceutical,
Who, Me? Starting THE Conversation
 Who, Me? Starting THE Conversation Nancy Flowers, LCSW Social Work Manager Rainbow Hospice and Palliative Care nflowers@rainbowhospice.org 847-685-9900 Objectives Clarify the importance of advance directives
Who, Me? Starting THE Conversation Nancy Flowers, LCSW Social Work Manager Rainbow Hospice and Palliative Care nflowers@rainbowhospice.org 847-685-9900 Objectives Clarify the importance of advance directives
2018 Hospitalization Project Call
 2018 Hospitalization Project Call Date: 6/14/2018 Host: Barbara Breckler, QI Director Email: bbreckler@nw16.esrd.net Honoring Patient Wishes Palliative and Hospice Care for Patients with Late Stage Kidney
2018 Hospitalization Project Call Date: 6/14/2018 Host: Barbara Breckler, QI Director Email: bbreckler@nw16.esrd.net Honoring Patient Wishes Palliative and Hospice Care for Patients with Late Stage Kidney
Prognostication: How good or (bad) are we?
 are we?") Prognostication: How good or (bad) are we? Dr Vincent Thai MBBS, MMed (Int Med) (S), MRCP (UK), C.C.F.P (C), ABPHM (USA) Director - Palliative Care Services (UAH site) Associate Clinical i l Prof - Division
Prognostication: How good or (bad) are we? Dr Vincent Thai MBBS, MMed (Int Med) (S), MRCP (UK), C.C.F.P (C), ABPHM (USA) Director - Palliative Care Services (UAH site) Associate Clinical i l Prof - Division
Prognostication: How good or (bad) are we?
 are we?") Prognostication: How good or (bad) are we? ) Dr Vincent Thai MBBS, MMed (Int Med) (S), MRCP (UK), C.C.F.P (C), ABPHM (USA) Director - Palliative Care Services (UAH site) Associate Clinical Prof - Division
Prognostication: How good or (bad) are we? ) Dr Vincent Thai MBBS, MMed (Int Med) (S), MRCP (UK), C.C.F.P (C), ABPHM (USA) Director - Palliative Care Services (UAH site) Associate Clinical Prof - Division
Communicating with Patients with Heart Failure and their Families
 Communicating with Patients with Heart Failure and their Families Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine
Communicating with Patients with Heart Failure and their Families Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine
Matisse Meets Osler: The Art and Science of Prognostication
 Matisse Meets Osler: The Art and Science of Prognostication Timothy G. Ihrig, MD, MA Medical Director, Palliative Medicine Trinity Regional Health System ihrigtg@ihs.org Adapted From Prognostication at
Matisse Meets Osler: The Art and Science of Prognostication Timothy G. Ihrig, MD, MA Medical Director, Palliative Medicine Trinity Regional Health System ihrigtg@ihs.org Adapted From Prognostication at
Estimating and explaining survival time in metastatic breast cancer
 Estimating and explaining survival time in metastatic breast cancer Dr Belinda Kiely Medical Oncologist Concord and Campbelltown Hospitals NHMRC Clinical Trials Centre, University of Sydney Clinic this
Estimating and explaining survival time in metastatic breast cancer Dr Belinda Kiely Medical Oncologist Concord and Campbelltown Hospitals NHMRC Clinical Trials Centre, University of Sydney Clinic this
Preventing harmful treatment
 Preventing harmful treatment How can Palliative Care prevent patients receiving overzealous or futile treatment? Antwerp, November 2010 Prof Scott A Murray, St Columba s Hospice Chair of Primary Palliative
Preventing harmful treatment How can Palliative Care prevent patients receiving overzealous or futile treatment? Antwerp, November 2010 Prof Scott A Murray, St Columba s Hospice Chair of Primary Palliative
You want us to do everything?! RETHINKING COMMUNICATION AROUND GOALS OF CARE
 You want us to do everything?! RETHINKING COMMUNICATION AROUND GOALS OF CARE Michael D. Barnett, MD, MS, FAAP, FAAHPM UAB Center for Palliative & Supportive Care OBJECTIVES 1. Gauge patient/family understanding
You want us to do everything?! RETHINKING COMMUNICATION AROUND GOALS OF CARE Michael D. Barnett, MD, MS, FAAP, FAAHPM UAB Center for Palliative & Supportive Care OBJECTIVES 1. Gauge patient/family understanding
Geriatric Grand Rounds
 Geriatric Grand Rounds Tuesday, April 15, 2008 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital Visit web sites: for handouts, poster, schedule, subscription: http://www.ualberta.ca/~geriatri/ggr/.
Geriatric Grand Rounds Tuesday, April 15, 2008 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital Visit web sites: for handouts, poster, schedule, subscription: http://www.ualberta.ca/~geriatri/ggr/.
THE CONSERVATIVE CARE PATHWAY
 THE CONSERVATIVE CARE PATHWAY Dr. Gaylene Hargrove Sept. 19, 2015 Island Health Renal Program End of Life Conference Learning Objectives Describe and discuss what defines conservative care. Identify key
THE CONSERVATIVE CARE PATHWAY Dr. Gaylene Hargrove Sept. 19, 2015 Island Health Renal Program End of Life Conference Learning Objectives Describe and discuss what defines conservative care. Identify key
Palliative Care: Mission and Strategic Imperative. Sarah E. Hetue Hill, PhD Ascension Healthcare
 Palliative Care: Mission and Strategic Imperative Sarah E. Hetue Hill, PhD Ascension Healthcare Ascension Palliative Care Definition Palliative Care is person-centered, holistic care delivered by an interdisciplinary
Palliative Care: Mission and Strategic Imperative Sarah E. Hetue Hill, PhD Ascension Healthcare Ascension Palliative Care Definition Palliative Care is person-centered, holistic care delivered by an interdisciplinary
Advances in Palliative Care
 Steven Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative Care Program and Palliative Care Leadership Center Division of
Steven Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative Care Program and Palliative Care Leadership Center Division of
"Meeting Patients Where They Are": Tips on Formulating and Communicating Prognosis
 "Meeting Patients Where They Are": Tips on Formulating and Communicating Prognosis Daniel Johnson, MD, FAAHPM Care Management Institute, Kaiser Permanente Director Emeritus, Life Quality Institute U. Colorado
"Meeting Patients Where They Are": Tips on Formulating and Communicating Prognosis Daniel Johnson, MD, FAAHPM Care Management Institute, Kaiser Permanente Director Emeritus, Life Quality Institute U. Colorado
Predicting Survival with the Palliative Performance Scale in a Minority-Serving Hospice and Palliative Care Program
 642 Journal of Pain and Symptom Management Vol. 37 No. 4 April 2009 Original Article Predicting Survival with the Palliative Performance Scale in a Minority-Serving Hospice and Palliative Care Program
642 Journal of Pain and Symptom Management Vol. 37 No. 4 April 2009 Original Article Predicting Survival with the Palliative Performance Scale in a Minority-Serving Hospice and Palliative Care Program
Symptoms Assess symptoms and needs across all domains. Screen using Edmonton Symptom Assessment System (ESAS) for: Pain Nausea Depression
 for: Pain Nausea Depression") A Palliative Care Approach for Oncology Integrating a palliative care approach earlier in the disease trajectory improves the quality of living and dying, and relieves suffering for patients and families
A Palliative Care Approach for Oncology Integrating a palliative care approach earlier in the disease trajectory improves the quality of living and dying, and relieves suffering for patients and families
Supportive and Palliative care for patients with Pancreatic Cancer. Dr Holly Taylor September 2018
 Supportive and Palliative care for patients with Pancreatic Cancer Dr Holly Taylor September 2018 Aims of this session To discuss the principles of supportive and palliative care Identification of patients
Supportive and Palliative care for patients with Pancreatic Cancer Dr Holly Taylor September 2018 Aims of this session To discuss the principles of supportive and palliative care Identification of patients
Quick Guide to Prognostication Tools
 Quick Guide to Prognostication Tools 31/07/2008 Dr Ray Viola Mark Corkum 34 Barrie St. Kingston, Ontario Canada K7L 3W6 rav@queensu.ca (613) 549 6666 ext. 3223 1 Table of Contents The SUPPORT Model...
Quick Guide to Prognostication Tools 31/07/2008 Dr Ray Viola Mark Corkum 34 Barrie St. Kingston, Ontario Canada K7L 3W6 rav@queensu.ca (613) 549 6666 ext. 3223 1 Table of Contents The SUPPORT Model...
Feasibility of Implementing Advance Directive in Hong Kong Chinese Elderly People
 Asia Pacific Regional Conference in End-of-Life and Palliative Care in Long Term Care Settings Feasibility of Implementing Advance Directive in Hong Kong Chinese Elderly People Dr. Patrick CHIU MBBS (HK),
Asia Pacific Regional Conference in End-of-Life and Palliative Care in Long Term Care Settings Feasibility of Implementing Advance Directive in Hong Kong Chinese Elderly People Dr. Patrick CHIU MBBS (HK),
Can oncologists predict survival for patients with progressive disease after standard chemotherapies?
 Curr Oncol, Vol. 21, pp. 84-90; doi: http://dx.doi.org/10.3747/co.21.1743 CLINICAL PREDICTION OF SURVIVAL BY ONCOLOGISTS ORIGINAL ARTICLE Can oncologists predict survival for patients with progressive
Curr Oncol, Vol. 21, pp. 84-90; doi: http://dx.doi.org/10.3747/co.21.1743 CLINICAL PREDICTION OF SURVIVAL BY ONCOLOGISTS ORIGINAL ARTICLE Can oncologists predict survival for patients with progressive
Patient Experience Research in Malignant Hematology: describing the lived experience of illness with acute myeloid leukemia
 Patient Experience Research in Malignant Hematology: describing the lived experience of illness with acute myeloid leukemia Thomas W. LeBlanc, MD, MA, MHS, FAAHPM Associate Professor of Medicine Division
Patient Experience Research in Malignant Hematology: describing the lived experience of illness with acute myeloid leukemia Thomas W. LeBlanc, MD, MA, MHS, FAAHPM Associate Professor of Medicine Division
The Interface of Cardiology and Palliative Medicine
 The Interface of Cardiology and Palliative Medicine Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine Mount Sinai School
The Interface of Cardiology and Palliative Medicine Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine Mount Sinai School
Aspects of Communication in Quality End-of Life Care
 Aspects of Communication in Quality End-of Life Care Presented by Stephen Goldfine, MD Chief Medical Officer Samaritan Healthcare & Hospice SamaritanNJ.org Objectives To know and understand: The importance
Aspects of Communication in Quality End-of Life Care Presented by Stephen Goldfine, MD Chief Medical Officer Samaritan Healthcare & Hospice SamaritanNJ.org Objectives To know and understand: The importance
Temiskaming Hospital Hospice Palliative Care. Presented by: Dr. Don Davies January 31, 2017
 Temiskaming Hospital Hospice Palliative Care Presented by: Dr. Don Davies January 31, 2017 Objectives Talk a little about Palliative Care. In general A quick look at Temiskaming District and Hospice Model
Temiskaming Hospital Hospice Palliative Care Presented by: Dr. Don Davies January 31, 2017 Objectives Talk a little about Palliative Care. In general A quick look at Temiskaming District and Hospice Model
So let s go through each disease then and understand some of the established prognostic factors starting with COPD.
 Okay, I am Dr. David Hui from the Department of Palliative Care from The University of Texas MD Anderson Cancer Center and we are going to talk about Prognostication in Advanced Diseases, Part II. So in
Okay, I am Dr. David Hui from the Department of Palliative Care from The University of Texas MD Anderson Cancer Center and we are going to talk about Prognostication in Advanced Diseases, Part II. So in
Learning Goals: REMAP: Discussing Goals of Care. Reframe. 2. Expect emotion: respond empathically. 2. Expect emotion: respond empathically
 Practicing patient centered medicine in the 4th quarter Bob Arnold MD 2016 Learning Goals: To define the difference between goals and strategy To describe a goal focused method of talking with patients
Practicing patient centered medicine in the 4th quarter Bob Arnold MD 2016 Learning Goals: To define the difference between goals and strategy To describe a goal focused method of talking with patients
Objectives. ORC Definition. Definitions of Palliative Care. CMS and National Quality Forum Definition (2013) CAPC 9/7/2017
 CAPC 9/7/2017") Objectives General overview of palliative care Define the role of palliative care Palliative Care Management and Transition Joan Hanson, Director of WRN Palliative Care, RN, CHPCA Jennifer Martnick, Team
Objectives General overview of palliative care Define the role of palliative care Palliative Care Management and Transition Joan Hanson, Director of WRN Palliative Care, RN, CHPCA Jennifer Martnick, Team
Palliative Approach to Chronic Disease Management versus End-of-Life Care
 Palliative Approach to Chronic Disease Management versus End-of-Life Care 1 Acknowledgements Marg Poling, RN, Palliative Pain and Symptom Management Consultant North West Community Care Access Centre (Thunder
Palliative Approach to Chronic Disease Management versus End-of-Life Care 1 Acknowledgements Marg Poling, RN, Palliative Pain and Symptom Management Consultant North West Community Care Access Centre (Thunder
12/6/2016. Objective PALLIATIVE CARE IN THE NURSING HOME. Medical Care in the US. Palliative Care
 Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Palliative Care: Transforming the Care of Serious Illness
 Palliative Care: Transforming the Care of Serious Illness Diane E. Meier, MD Director, Center to Advance Palliative Care diane.meier@mssm.edu www.capc.org www.getpalliativecare.org @dianeemeier No Disclosures
Palliative Care: Transforming the Care of Serious Illness Diane E. Meier, MD Director, Center to Advance Palliative Care diane.meier@mssm.edu www.capc.org www.getpalliativecare.org @dianeemeier No Disclosures
Palliative Care & Hospice
 Palliative Care & Hospice Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor, Department of Geriatrics Florida State University College of Medicine 1 Diane Meier, MD Director, Center to Advance
Palliative Care & Hospice Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor, Department of Geriatrics Florida State University College of Medicine 1 Diane Meier, MD Director, Center to Advance
Hospice and Palliative Care: Value-Based Care Near the End of Life
 Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
Hospice and Palliative Care: Value-Based Care Near the End of Life
 Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
Hospice and Palliative Care: Value-Based Care Near the End of Life Mary Dittrich, MD, FASN Senior Medical Director, Remedy Partners Joseph W. Shega, MD National Medical Director, VITAS Healthcare 2017
ICDs - decisions at the end of life
 ICDs - decisions at the end of life James Beattie Consultant Cardiologist Heart of England NHS Foundation Trust, Birmingham, UK National Clinical Adviser, NHS Heart Improvement Heart Statement of disclosure
ICDs - decisions at the end of life James Beattie Consultant Cardiologist Heart of England NHS Foundation Trust, Birmingham, UK National Clinical Adviser, NHS Heart Improvement Heart Statement of disclosure
Transplant Dilemmas in Palliative Care
 Transplant Dilemmas in Palliative Care Stacy Schulof APRN, FNP-C DISCLOSURES No financial disclosures I am a recovering ICU nurse OBJECTIVES Identify three dilemmas Review the patient population Make the
Transplant Dilemmas in Palliative Care Stacy Schulof APRN, FNP-C DISCLOSURES No financial disclosures I am a recovering ICU nurse OBJECTIVES Identify three dilemmas Review the patient population Make the
Independent Prospective Validation of the PaP Score in Terminally Ill Patients Referred to a Hospital-Based Palliative Medicine Consultation Service
 Vol. 22 No. 5 November 2001 Journal of Pain and Symptom Management 891 Original Article Independent Prospective Validation of the PaP Score in Terminally Ill Patients Referred to a Hospital-Based Palliative
Vol. 22 No. 5 November 2001 Journal of Pain and Symptom Management 891 Original Article Independent Prospective Validation of the PaP Score in Terminally Ill Patients Referred to a Hospital-Based Palliative
Medicine (prognosis) is the science of uncertainty and the art of probability --Osler. TO KNOW BEFORE: Complexities of Prognosis in Advanced Cancer
 is the science of uncertainty and the art of probability --Osler. TO KNOW BEFORE: Complexities of Prognosis in Advanced Cancer") TO KNOW BEFORE: Complexities of Prognosis in Advanced Cancer Garrett Snipes, MD Spartanburg Regional Healthcare System The challenge: To make a prognosis talk interesting enough to hold the attention of
TO KNOW BEFORE: Complexities of Prognosis in Advanced Cancer Garrett Snipes, MD Spartanburg Regional Healthcare System The challenge: To make a prognosis talk interesting enough to hold the attention of
Mark V. Blum, MD, FAAHPM Medical Director. Dawn Lambie, RN, MSN Executive Director. Bristol Hospice, Sacramento
 Mark V. Blum, MD, FAAHPM Medical Director Bristol Hospice, Sacramento Dawn Lambie, RN, MSN Executive Director Bristol Hospice, Sacramento Mark Blum has no unresolved conflicting affiliations to disclose.
Mark V. Blum, MD, FAAHPM Medical Director Bristol Hospice, Sacramento Dawn Lambie, RN, MSN Executive Director Bristol Hospice, Sacramento Mark Blum has no unresolved conflicting affiliations to disclose.
The Role of Palliative Care in the Management of Advanced Heart Failure
 Disclosure The Role of Palliative Care in the Management of Advanced Heart Failure I have no conflict of interest to disclose. Darrell Craig MD Medical Director, Palliative Care Services St. Joseph Mercy
Disclosure The Role of Palliative Care in the Management of Advanced Heart Failure I have no conflict of interest to disclose. Darrell Craig MD Medical Director, Palliative Care Services St. Joseph Mercy
Navigating Conflict with Families
 Navigating Conflict with Families Gordon J. Wood, MD, MSCI, FAAHPM Winter Workshop, Coleman Palliative Medicine Training Program February 28, 2014 With thanks to Bob Arnold, Elizabeth Weinstein and Jonathan
Navigating Conflict with Families Gordon J. Wood, MD, MSCI, FAAHPM Winter Workshop, Coleman Palliative Medicine Training Program February 28, 2014 With thanks to Bob Arnold, Elizabeth Weinstein and Jonathan
Hospice May Prolong Life
 OBJECTIVES Shatter some myths about Hospice care Revisit difference between Hospice/PC Learn to use a Discussion Guide to clarify GOC Expand the Letterman Technique of Presentation Myths Myth # 20, Prognostic
OBJECTIVES Shatter some myths about Hospice care Revisit difference between Hospice/PC Learn to use a Discussion Guide to clarify GOC Expand the Letterman Technique of Presentation Myths Myth # 20, Prognostic
Objectives 2/11/2016 HOSPICE 101
 HOSPICE 101 Overview Hospice History and Statistics What is Hospice? Who qualifies for services? Levels of Service The Admission Process Why Not to Wait Objectives Understand how to determine hospice eligibility
HOSPICE 101 Overview Hospice History and Statistics What is Hospice? Who qualifies for services? Levels of Service The Admission Process Why Not to Wait Objectives Understand how to determine hospice eligibility
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital
 - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital") Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Understanding referrals to outpatient palliative care and goals of care discussions with individuals diagnosed with stage IV advanced cancer
 Understanding referrals to outpatient palliative care and goals of care discussions with individuals diagnosed with stage IV advanced cancer ELLIS DILLON, JINNAN LI, AMY MEEHAN, SU-YING LIANG, STEVE LAI,
Understanding referrals to outpatient palliative care and goals of care discussions with individuals diagnosed with stage IV advanced cancer ELLIS DILLON, JINNAN LI, AMY MEEHAN, SU-YING LIANG, STEVE LAI,
Pediatric Palliative Care and Having Difficult Conversations
 Pediatric Palliative Care and Having Difficult Conversations UCSF Pediatric Neurology and Palliative Care Audrey Foster-Barber, MD, PhD Pediatric Hospital Medicine Boot Camp 6/14 Palliative Care A philosophy
Pediatric Palliative Care and Having Difficult Conversations UCSF Pediatric Neurology and Palliative Care Audrey Foster-Barber, MD, PhD Pediatric Hospital Medicine Boot Camp 6/14 Palliative Care A philosophy
Prognostication: balancing certainty, science and experience
 Prognostication: balancing certainty, science and experience Christian T Sinclair, MD, FAAHPM University of Kansas Medical Center Spring 2017 csinclair@kumc.edu Objectives Identify three barriers to effective
Prognostication: balancing certainty, science and experience Christian T Sinclair, MD, FAAHPM University of Kansas Medical Center Spring 2017 csinclair@kumc.edu Objectives Identify three barriers to effective
Withholding & Withdrawing Life Sustaining Treatment: A Lifespan Approach
 Withholding & Withdrawing Life Sustaining Treatment: A Lifespan Approach Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor, Department of Geriatrics FSU College of Medicine Basic Concepts
Withholding & Withdrawing Life Sustaining Treatment: A Lifespan Approach Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor, Department of Geriatrics FSU College of Medicine Basic Concepts
Best of palliative care
 Best of palliative care Summer School Palliativmedizin 6-7.7.2016 Dr. Eve Rubli Chaire de soins palliatifs gériatriques CHUV Lausanne Geriatric Palliative Care CHUV, Lausanne Endowed professorship, supported
Best of palliative care Summer School Palliativmedizin 6-7.7.2016 Dr. Eve Rubli Chaire de soins palliatifs gériatriques CHUV Lausanne Geriatric Palliative Care CHUV, Lausanne Endowed professorship, supported
The Role of Palliative Care in Readmission Reduction Steven Z. Pantilat, MD
 The Role of Palliative Care in Readmission Reduction Steven Z. Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative Care Program
The Role of Palliative Care in Readmission Reduction Steven Z. Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative Care Program
Primary Palliative Care
 Primary Palliative Care Amanda Overstreet, DO October 20, 2017 No financial disclosures Objectives Discuss palliative care and how it differs from hospice Explore how to manage patients goals and expectations
Primary Palliative Care Amanda Overstreet, DO October 20, 2017 No financial disclosures Objectives Discuss palliative care and how it differs from hospice Explore how to manage patients goals and expectations
10/15/2013. Discussing Treatment Preferences When Patients Want Everything. Dr. Quill has no significant conflicts of interest to declare
 Discussing Treatment Preferences When Patients Want Everything Dr. Quill has no significant conflicts of interest to declare Timothy E. Quill MD University of Rochester Medical Center Rochester, NY 1 10/15/2013
Discussing Treatment Preferences When Patients Want Everything Dr. Quill has no significant conflicts of interest to declare Timothy E. Quill MD University of Rochester Medical Center Rochester, NY 1 10/15/2013
Palliative Performance Scale (PPS)
") Palliative Performance Scale (PPS) Description The Palliative Performance Scale is a reliable and valid tool used for assessing a patient s functional status. PPS was developed by Victoria Hospice Society,
Palliative Performance Scale (PPS) Description The Palliative Performance Scale is a reliable and valid tool used for assessing a patient s functional status. PPS was developed by Victoria Hospice Society,
Walking together: Palliative Care and heart failure.
 Walking together: Palliative Care and heart failure. St Paul's Hospital Heart Function Supportive Care Clinic Cindy Nordquist MN-NP(F) Objectives Review heart failure. Review palliative care/ palliative
Walking together: Palliative Care and heart failure. St Paul's Hospital Heart Function Supportive Care Clinic Cindy Nordquist MN-NP(F) Objectives Review heart failure. Review palliative care/ palliative
MiPCT Palliative Care Webinar: Leading a Family Goal Setting Meeting. David E. Weissman, MD Professor Emeritus Medical College of Wisconsin
 MiPCT Palliative Care Webinar: Leading a Family Goal Setting Meeting David E. Weissman, MD Professor Emeritus Medical College of Wisconsin Continuing Education Credit To receive continuing education credit
MiPCT Palliative Care Webinar: Leading a Family Goal Setting Meeting David E. Weissman, MD Professor Emeritus Medical College of Wisconsin Continuing Education Credit To receive continuing education credit
Palliative and End of Life Care in End Stage Renal Disease
 Palliative and End of Life Care in End Stage Renal Disease Palliative and End of Life Care Priority for Action Regional Consensus Workshop 30.06.2010 Neal Morgan Consultant Nephrologist SHSCT Outline Introduction
Palliative and End of Life Care in End Stage Renal Disease Palliative and End of Life Care Priority for Action Regional Consensus Workshop 30.06.2010 Neal Morgan Consultant Nephrologist SHSCT Outline Introduction
Easing the transition from curative care to palliative care
 Easing the transition from curative care to palliative care Manon Coulombe, RN, MSc(A), CHPCN(C) Pivot nurse in palliative care mcoulombe2.hmr@ssss.gouv.qc.ca Presentation My clinical practice Characteristics
Easing the transition from curative care to palliative care Manon Coulombe, RN, MSc(A), CHPCN(C) Pivot nurse in palliative care mcoulombe2.hmr@ssss.gouv.qc.ca Presentation My clinical practice Characteristics
Achieving earlier entry to hospice care: Issues and strategies. Sonia Lee, APN, GCNS-BC
 Achieving earlier entry to hospice care: Issues and strategies Sonia Lee, APN, GCNS-BC Objectives The learner will: Describe the benefits of hospice List at least barriers to early hospice care List at
Achieving earlier entry to hospice care: Issues and strategies Sonia Lee, APN, GCNS-BC Objectives The learner will: Describe the benefits of hospice List at least barriers to early hospice care List at
Delivering personalised care to end of life patients. Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London
 Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Bridging Palliative Care and Chronic Disease in Ontario: A Respirology and Nephrology Perspective
 Bridging Palliative Care and Chronic Disease in Ontario: A Respirology and Nephrology Perspective St. Joseph s Healthcare Hamilton Palliative Care Team Quality Hospice Palliative Care Coalition of Ontario
Bridging Palliative Care and Chronic Disease in Ontario: A Respirology and Nephrology Perspective St. Joseph s Healthcare Hamilton Palliative Care Team Quality Hospice Palliative Care Coalition of Ontario
Bring Palliative Care Into Your Office. Renee Baird, MSN, FNP-C, CHPN
 Bring Palliative Care Into Your Office Renee Baird, MSN, FNP-C, CHPN Pal-ee-uh-tiv Kair Palliative care is both a philosophy of care and an organized, highly structured system for delivering care. The
Bring Palliative Care Into Your Office Renee Baird, MSN, FNP-C, CHPN Pal-ee-uh-tiv Kair Palliative care is both a philosophy of care and an organized, highly structured system for delivering care. The
There For You. Your Compassionate Guide. World-Class Hospice Care Since 1979
 There For You Your Compassionate Guide World-Class Hospice Care Since 1979 What Is Hospice? Hospice is a type of care designed to provide support during an advanced illness. Hospice care focuses on comfort
There For You Your Compassionate Guide World-Class Hospice Care Since 1979 What Is Hospice? Hospice is a type of care designed to provide support during an advanced illness. Hospice care focuses on comfort
Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges. Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009
 Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009 Objectives Highlight the relevance of palliative/supportive care
Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009 Objectives Highlight the relevance of palliative/supportive care
Adam D. Marks, MD MPH Assistant Professor of Medicine University of Michigan Health System
 Adam D. Marks, MD MPH Assistant Professor of Medicine University of Michigan Health System The truth will set you free but first it will piss you off - Gloria Steinem Life expectancy is up dramatically
Adam D. Marks, MD MPH Assistant Professor of Medicine University of Michigan Health System The truth will set you free but first it will piss you off - Gloria Steinem Life expectancy is up dramatically
BETTER CONVERSATIONS, BETTER CARE : HOW MEANINGFUL CONVERSATIONS IMPROVE PATIENT EXPERIENCE AND QUALITY OF LIFE
 Teva Pharmaceuticals Europe BV, Piet Heinkade 107, 1019 GM Amsterdam, Netherlands Date of preparation: March 2017. HQ/ONCO/17/0001 BETTER CONVERSATIONS, BETTER CARE : HOW MEANINGFUL CONVERSATIONS IMPROVE
Teva Pharmaceuticals Europe BV, Piet Heinkade 107, 1019 GM Amsterdam, Netherlands Date of preparation: March 2017. HQ/ONCO/17/0001 BETTER CONVERSATIONS, BETTER CARE : HOW MEANINGFUL CONVERSATIONS IMPROVE
Talking to Your Oncologist & Living with Cancer
 Talking to Your Oncologist & Living with Cancer Anthony Back, M.D. University of Washington Fred Hutchinson Cancer Research Center Seattle Cancer Care Alliance Highlights? The old way doctors talked What
Talking to Your Oncologist & Living with Cancer Anthony Back, M.D. University of Washington Fred Hutchinson Cancer Research Center Seattle Cancer Care Alliance Highlights? The old way doctors talked What
Managing Conflicts Around Medical Futility
 Managing Conflicts Around Medical Futility Robert M. Taylor, MD Medical Director, OSUMC Center for Palliative Care Associate Professor of Neurology The Ohio State University James Cancer Hospital Objectives
Managing Conflicts Around Medical Futility Robert M. Taylor, MD Medical Director, OSUMC Center for Palliative Care Associate Professor of Neurology The Ohio State University James Cancer Hospital Objectives
Transplant Dilemmas in Palliative Care
 Transplant Dilemmas in Palliative Care Stacy Schulof APRN, FNP-C DISCLOSURES No financial disclosures I am a recovering ICU nurse OBJECTIVES What is the dilemma? Identify the patient population Make the
Transplant Dilemmas in Palliative Care Stacy Schulof APRN, FNP-C DISCLOSURES No financial disclosures I am a recovering ICU nurse OBJECTIVES What is the dilemma? Identify the patient population Make the
MODULE 1 PALLIATIVE NURSING CARE
 Curriculum MODULE 1 PALLIATIVE NURSING CARE Objectives Describe the role of the nurse in providing quality palliative care for patients across the lifespan. Identify the need for collaborating with interdisciplinary
Curriculum MODULE 1 PALLIATIVE NURSING CARE Objectives Describe the role of the nurse in providing quality palliative care for patients across the lifespan. Identify the need for collaborating with interdisciplinary
section 6: transitioning away from mental illness
 section 6: transitioning away from mental illness Throughout this resource, we have emphasized the importance of a recovery perspective. One of the main achievements of the recovery model is its emphasis
section 6: transitioning away from mental illness Throughout this resource, we have emphasized the importance of a recovery perspective. One of the main achievements of the recovery model is its emphasis
Palliative & End of Life Care in Frailty & Dementia. Dr Ruth Ting Palliative Care Consultant Gateshead
 Palliative & End of Life Care in Frailty & Dementia Dr Ruth Ting Palliative Care Consultant Gateshead One Chance to get it right How people die remains in the memory of those who live on Dame Cicely Saunders
Palliative & End of Life Care in Frailty & Dementia Dr Ruth Ting Palliative Care Consultant Gateshead One Chance to get it right How people die remains in the memory of those who live on Dame Cicely Saunders
Sharp HealthCare Hospice and Palliative Care
 Sharp HealthCare Hospice and Palliative Care The Continuum for Advanced Illness and End Stage Disease Management (AAC) Daniel R. Hoefer, MD CMO, Outpatient Palliative Care and Hospice Suzi K. Johnson,
Sharp HealthCare Hospice and Palliative Care The Continuum for Advanced Illness and End Stage Disease Management (AAC) Daniel R. Hoefer, MD CMO, Outpatient Palliative Care and Hospice Suzi K. Johnson,