1.1. Parkinson disease
|
|
|
- Emerald Blankenship
- 6 years ago
- Views:
Transcription

1 1.TREMOR

2 1.1. Parkinson disease
3 Parkinson Disease Progressive disorder: tremor, rigidity, and slowness of movements Neuronal loss of the substantia nigra Non motor features (dementia and dysautonomia), in advanced stages of the disease Orthostatic hypotension Bradykinesia Erectile dysfunction L-Dopa lack of response Evolution of the disease (years)
4 Imaging in Parkinson Disease Although neuroimaging is usually nondiagnostic in the evaluation of PD several modalities are used in its management. TC is performed to exclude specific structural abnormalities (hydrocephalus, tumor or lacunar infarcts) MR Imaging: Narrowing or disappearance of pars compacta of substantia nigra on T2 WI MR is essential in the planning of subthalamic nucleus surgery Role of transcranial ultrasound

5 Parkinson disease. Role of CT Rule out secondary causes some of them potentially reversible Drugs Wilson s disease Essential tremor Vascular parkinsonism Normal pressure hidrocephalus Trauma

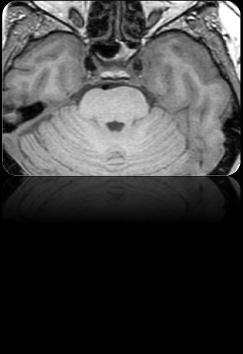
 Axial T2 WI shows hypointensity within the lentiform")
6 Parkinson disease: MR Imaging Parkinson disease. Role of MR imaging * * Axial T2 WI at midbrain level shows narrowing of the substantia nigra, pars compacta (arrow). Note the red nucleus hypointensity (*) Axial T2 WI shows hypointensity within the lentiform nuclei and mild cerebral atrophy T1 3D TFE. Coronal MPR showing bilateral gliosis due to subthalamic nucleus stimulation
7 Parkinson disease. Role of Transcranial ultrasound TCUS: Substancia nigra hiperechogenicity Hiperechogenicity of the substancia nigra: Parkinson s disease 10% healthy subjects Essential tremor Lewy dementia Corticobasal degeneration. Non hiperechogenicity of the substantia nigra: 80% healthy controls, Multiple system atrophy Progressive supranuclear palsy
8 1.2. Atypical Parkinsonian Syndromes EPIDEMIO LOGY Progressive supranuclear palsy Multiple system atrophy Corticobasal degeneration P.D. P.S.P. M.S.A. Others

9 Importance of correct diagnosis Prognosis: the prognosis for APS is worse than PD Therapeutic: APS patients respond poorly to L-Dopa Secondary effects of PD therapy: dyskinesias Atypical parkinsonism patients should not be managed by surgical means Investigation: patients with APS should not be enrolled in PD studies Is the patient in the right bowl?

10 1.2.1.Progressive supranuclear palsy
11 Progressive supranuclear palsy Also known as Steele Richardson Olszewski syndrome Vertical supranuclear palsy with downward gaze abnormalities Postural instability with unexplained falls Pseudobulbar palsy with associated dysarthria and dysphagia Frontal lobe-like dementia syndrome Course relentlessly progressive (death six years after onset)
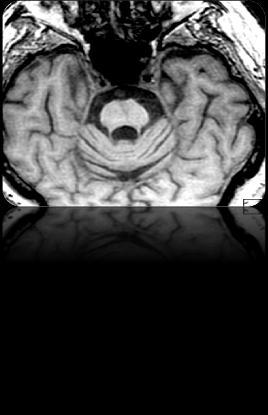
12 Progressive supranuclear palsy Atrophy of midbrain, concave profile of the midbrain forming the floor of the third ventricle: hummingbird or penguin sign Axial images show abnormal concavity of the lateral margins of midbrain tegmentum: morning glory sign Midsagital images: Midbrain axial diameter < 14mm midbrain area <70mm2 (50% normal) midbrain to pons ratio <0,15 Thinning of the superior colliculus




13 Progressive supranuclear palsy * Midbrain tegmetum atrophy: hummingbird or penguin sign





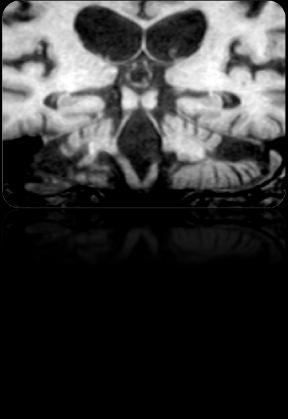
14 Progressive supranuclear palsy Mild PSP Healthy subject Morning glory flower for comparison Advanced PSP Abnormal concavity of the lateral margins of the midbrain tegmentum: mornign glory sign

15 Progressive supranuclear palsy Significantly smaller ratio of midbrain-pons area <0,15 ó <0,20
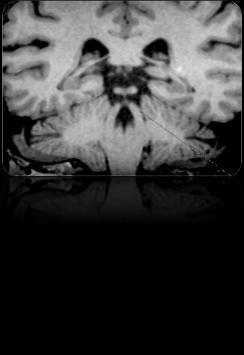
16 Progressive supranuclear palsy Thinning of the superior colliculus Healthy subject PSP
17 1.2.2.Multiple system atrophy
18 Multiple system atrophy Progressive, idiopathic, neurodegenerative process Various degrees of parkisonism, autonomic failure, cerebellar dysfunction, and pyramidal signs Glial cytoplasmic inclusions (alpha sinuclein) Insufficent or transient response to L- Dopa Orthostatic hypotension Erectile dysfunction Bradykinesia Lack of response to L-Dopa 5 10 Evolution of the disease (years)
: Asymmetrical tremor, bradykinesia, rigidity and postural instability Former striatronigral degeneration CEREBELLAR MSA-C (20%): Gait and limb ataxia, ataxic")
19 Multiple system atrophy. Subtypes PARKINSONIAN MSA-P (80%): Asymmetrical tremor, bradykinesia, rigidity and postural instability Former striatronigral degeneration CEREBELLAR MSA-C (20%): Gait and limb ataxia, ataxic dysarthria and sustained gaze evoked nystagmus Former olivoponto cerebellar atrophy MSA-P 80% MSA- C 20% Autonomic findings AUTONOMIC DISFUNCTION : Urinary dysfunction, orthostatic hypotension, erectile dysfunction, urinary incontinence Former Shy Drager Syndrome
20 MSA-P: MSA-parkinsonian - Hypointensity of the putamen in T2 weighted images that releccts iron accumulation due to striatonigral degeneration. (The hypointensity is equal to or more marked than normally seen in the pallidum, where iron accumulates during life) - A thin lateral rim of hyperintensity in the putamen relates to secondary gliosis
21 MSA-parkinsonian AMS-p. Axial T2 WI. Prominent hypointensity in the putamen and pallidus. Note also the peripheral hyperintese rim due to reactive gliosis.
22 MSA- cerebellar MSA-C: Atrophy of the brain stem and cerebellum: on sagittal iamges atrophy of the pons and medulla with flat ventral surface of the pons Atrophy of the cerebellar vermis, middle cerebellar peduncles and hemispheres Signal changes in the transverse pontine fibers ( hot cross bun sign), middle cerebellar peduncles and cerebellum





23 MSA- cerebellar Cerebellar atrophy and high signal in middle cerebellar peduncles AMS Atrophy of the pons and medulla with flat ventral surface of the pons Cruciform shape in the pons, hot cross bun sign
24 1.2.3.Corticobasal degeneration
25 Corticobasal degeneration Progressive neurodegenerative disease Presents with congitive dysfunction, asymetrical parkinson Severe focal symmetric cortical atrophy Perrolandic (posterior frontal, parietal cortex) Relative sparing of temporal, occipital regions

, axial FFE")

 Volumen")



26 Corticobasal degeneration A B C D Axial T2 (A), axial FFE T1(B), Coronal and sagittal MPR reconstructions. (C,D) Volumen rendering (E). Asimetric volume loss involving precentral and postcental giri, more strking in parasagital regions. E
27 1.3. Hereditary parkinsonism
 Former Hallervorden-Spatz Autosomal")
 Imaging: hyperintensity within a")

28 Neurodegeneration with brain iron accumulation (PKAN-2) Former Hallervorden-Spatz Autosomal recessive, mutation in the patothene kinase 2 gene (PKAN-2) Imaging: hyperintensity within a region of hypointensity in the medial globus pallidus, eye of the tiger Eye of the tiger sign

29 Wilson disease Hepatolenticular degeneration Autosomal recessive inherited copper metabolism disorder Imaging: Hyperintense signal on T2 WI, sometimes with a central core of hypointensity in the basal ganglia Face of the giant panda sign
30 1.4. Secondary parkinsonism EPIDE MIOLO GY P.D. P.S.P. M.S.A. Others Toxins (carbon monoxide, methanol) Metabolic (chronic liver failure, Wilson's disease extrapontine myelinolysis) Infections (prion disease, HIV/AIDS) Head trauma (boxing) Structural brain lesions (hydrocephalus, chronic subdural hematoma, tumor) Small vessel disease ("vascular parkinsonism") Drugs (antipsychotic agents)

31 Carbon monoxide poisoning Most common cause of accidental poisoning in Europe and North America Imaging: Globi pallidi hyperintensity on T2 WI due to necrosis Associated abnormalities: CO induced parkinsonism Axial T2 WI shows hyperintense lesion within globi pallidi

32 Methanol poisoning Axial T2 WI shows bilateral hyperintensity of the putamen and pallidal nuclei


33 Hepatic (Manganic) encephalopaty Associated with acute liver failure, portal systemic bypass and liver cirrhosis Functional, potentially reversible due to manganese accumulation A B Sagittal T1WI MR (A) and parasagittal T1WI MR (B) show hyperintense signal within lentiform nucleus extending into midbrain and pitutitary gland
34 Hepatic (Manganic) encephalopaty Coronal T2 WI. High signal along hemispheric white matter in and around corticospinal tract. DWI. High mean diffusivity In hemispheric white matter


 and in the")

35 Rapidily progressing, fatal, transmissible dementig disorder caused by a prion T2 WI: hyperintensity of basal ganglia, thalamus and cerebral cortex. DWI: hyperintense changes in striatum and cerebral cortex A C Creutzfeldt Jacob disease B D Axial FLAIR : bilateral high signal intensity in the caudate nuclei, putamina and thalami (A) and in the cingulate girus (B) Axial DWI (C,D) show hyperintense signal consistent with restricted diffusion in caudate nuclei, putamina, thalami (C) and gyriform hyperintense areas in cingulate cortex. Pulvinar and hockey stick sign
36 1.5. Essential tremor
37 Essential tremor Classical essential tremor consists of a bilateral, visible, persistent, and largely symmetrical postural and/or kinetic tremor involving the hands and forearms Radiologist must know that routine CT and MR have not shown any consistent abnormalities
38 1.6. Palatal tremor

39 Palatal tremor In patients with palatal tremor the MR imaging finding of inferior olivary nucleus hypertrophy suggests symptomatic palatal tremor Bilateral olivary hipertrophy

40 1.7. Fragile X tremor ataxia syndrome (FTAX)

 The middle cerebellar")
41 Fragile X tremor ataxia syndrome (FTAX) Genetic disorder affecting mostly men and causing tremor, ataxia, and dementia Increased T2 signal in the white matte of middle cerebellar peduncles ( the MCP sign) The middle cerebellar peduncles sign

42 2.CHOREA

43 Huntington disease Autosomal dominant Clinical triad Chorea Dementia Behavioral changes Imaging: Atrophy of caudate nucleus that leads to frontal horns enlargement Diffuse cerebral atrophy



44 Chorea-ballismus in acute non-ketotic hyperglycaemia Unilateral T1 high signal intensity, low on T2 WI and restricted DWI Reversible after treatment
45 3.HEMIFACIAL SPASM
46 Hemifacial Spasm Unilateral involuntary facial spasms Begins with orbicularis oculi spasms Tonic-clonic but becomes constant over time
47 Hemifacial Spasm Common Vascular loop syndrome, CPA-IAC Vacular loop compressing facial nerve at its root exit zone within CPA cistern Causing hemifacial spasm Hemifacial spasm offending vessel: AICA (50%), PICA (30%), VA (10%), Vein (5%) Less Common Epidermoid cyst, CPA-IAC Meningioma, CPA-IAC Aneurysm, CPA-IAC Schwannoma facial nerve, CPA-IAC Perineural tumor CN7, parotid space Hemangioma facial nerve Rare but important Multiple sclerosis Ateriovenous malformation Hemangioma IAC




 and")
48 Hemifacial spasm Axial T2 WI. Right PICA loop Axial T2 WI. Right vestibular schwannoma FLAIR and DWI. Acute (superior) and chronic (inferior) pontine infarcts

49 Can you name the signs and the diseases?




50 Hummingbird Eye of the tiger sign PKAN-2 MSA-C hot cross bun PSP Hockey stick Creuztfeldt Jakob Morning glory Giant panda sign Wilson disease
Role of Magnetic Resonance Imaging in the Diagnosis of Adult Onset Movement Disorders
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.11 March. (2018), PP 73-84 www.iosrjournals.org Role of Magnetic Resonance Imaging in
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.11 March. (2018), PP 73-84 www.iosrjournals.org Role of Magnetic Resonance Imaging in
Functional Distinctions
 Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
Lecture XIII. Brain Diseases I - Parkinsonism! Brain Diseases I!
 Lecture XIII. Brain Diseases I - Parkinsonism! Bio 3411! Wednesday!! Lecture XIII. Brain Diseases - I.! 1! Brain Diseases I! NEUROSCIENCE 5 th ed! Page!!Figure!!Feature! 408 18.9 A!!Substantia Nigra in
Lecture XIII. Brain Diseases I - Parkinsonism! Bio 3411! Wednesday!! Lecture XIII. Brain Diseases - I.! 1! Brain Diseases I! NEUROSCIENCE 5 th ed! Page!!Figure!!Feature! 408 18.9 A!!Substantia Nigra in
FDG-PET e parkinsonismi
 Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
CN V! touch! pain! Touch! P/T!
 CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
brain MRI for neuropsychiatrists: what do you need to know
 brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
SWI including phase and magnitude images
 On-line Table: MRI imaging recommendation and summary of key features Sequence Pathologies Visible Key Features T1 volumetric high-resolution whole-brain reformatted in axial, coronal, and sagittal planes
On-line Table: MRI imaging recommendation and summary of key features Sequence Pathologies Visible Key Features T1 volumetric high-resolution whole-brain reformatted in axial, coronal, and sagittal planes
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Multiple System Atrophy-Cerebellar Type (MSA-C): A Case Report Mohd Abbas Ilyas, Pramod Shaha, Kulamani Sahoo,
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Multiple System Atrophy-Cerebellar Type (MSA-C): A Case Report Mohd Abbas Ilyas, Pramod Shaha, Kulamani Sahoo,
BASAL GANGLIA. Dr JAMILA EL MEDANY
 BASAL GANGLIA Dr JAMILA EL MEDANY OBJECTIVES At the end of the lecture, the student should be able to: Define basal ganglia and enumerate its components. Enumerate parts of Corpus Striatum and their important
BASAL GANGLIA Dr JAMILA EL MEDANY OBJECTIVES At the end of the lecture, the student should be able to: Define basal ganglia and enumerate its components. Enumerate parts of Corpus Striatum and their important
Atypical parkinsonism
 Atypical parkinsonism Wassilios Meissner Service de neurologie et CMR atrophie multisystématisée, CHU de Bordeaux Institut des Maladies Neurodégénératives, Université Bordeaux 2, CNRS UMR 5293 Parkinsonism?
Atypical parkinsonism Wassilios Meissner Service de neurologie et CMR atrophie multisystématisée, CHU de Bordeaux Institut des Maladies Neurodégénératives, Université Bordeaux 2, CNRS UMR 5293 Parkinsonism?
Parts of the motor circuits
 MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
A. General features of the basal ganglia, one of our 3 major motor control centers:
 Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. April 22, 2010 THE BASAL GANGLIA Objectives: 1. What are the
Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. April 22, 2010 THE BASAL GANGLIA Objectives: 1. What are the
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Connections of basal ganglia
 Connections of basal ganglia Introduction The basal ganglia, or basal nuclei, are areas of subcortical grey matter that play a prominent role in modulating movement, as well as cognitive and emotional
Connections of basal ganglia Introduction The basal ganglia, or basal nuclei, are areas of subcortical grey matter that play a prominent role in modulating movement, as well as cognitive and emotional
A. General features of the basal ganglia, one of our 3 major motor control centers:
 Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. March 1, 2012 THE BASAL GANGLIA Objectives: 1. What are the main
Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. March 1, 2012 THE BASAL GANGLIA Objectives: 1. What are the main
Brainstem. Steven McLoon Department of Neuroscience University of Minnesota
 Brainstem Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Change in Lab Sequence Week of Oct 2 Lab 5 Week of Oct 9 Lab 4 2 Goal Today Know the regions of the brainstem. Know
Brainstem Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Change in Lab Sequence Week of Oct 2 Lab 5 Week of Oct 9 Lab 4 2 Goal Today Know the regions of the brainstem. Know
Basal ganglia Sujata Sofat, class of 2009
 Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
DISORDERS OF THE MOTOR SYSTEM. Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
Introduction to the Central Nervous System: Internal Structure
 Introduction to the Central Nervous System: Internal Structure Objective To understand, in general terms, the internal organization of the brain and spinal cord. To understand the 3-dimensional organization
Introduction to the Central Nervous System: Internal Structure Objective To understand, in general terms, the internal organization of the brain and spinal cord. To understand the 3-dimensional organization
MRI OF THE THALAMUS. Mohammed J. Zafar, MD, FAAN Kalamazoo, MI
 1 MRI OF THE THALAMUS Mohammed J. Zafar, MD, FAAN Kalamazoo, MI Objectives: The thalamic nuclei can be involved in a wide variety of conditions. A systematic imaging approach would be useful for narrowing
1 MRI OF THE THALAMUS Mohammed J. Zafar, MD, FAAN Kalamazoo, MI Objectives: The thalamic nuclei can be involved in a wide variety of conditions. A systematic imaging approach would be useful for narrowing
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Strick Lecture 4 March 29, 2006 Page 1
 Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
The motor regulator. 1) Basal ganglia/nucleus
 Basal ganglia/nucleus") The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Making Things Happen 2: Motor Disorders
 Making Things Happen 2: Motor Disorders How Your Brain Works Prof. Jan Schnupp wschnupp@cityu.edu.hk HowYourBrainWorks.net On the Menu in This Lecture In the previous lecture we saw how motor cortex and
Making Things Happen 2: Motor Disorders How Your Brain Works Prof. Jan Schnupp wschnupp@cityu.edu.hk HowYourBrainWorks.net On the Menu in This Lecture In the previous lecture we saw how motor cortex and
Cerebellum. Steven McLoon Department of Neuroscience University of Minnesota
 Cerebellum Steven McLoon Department of Neuroscience University of Minnesota 1 Anatomy of the Cerebellum The cerebellum has approximately half of all the neurons in the central nervous system. The cerebellum
Cerebellum Steven McLoon Department of Neuroscience University of Minnesota 1 Anatomy of the Cerebellum The cerebellum has approximately half of all the neurons in the central nervous system. The cerebellum
Motor System Hierarchy
 Motor Pathways Lectures Objectives Define the terms upper and lower motor neurons with examples. Describe the corticospinal (pyramidal) tract and the direct motor pathways from the cortex to the trunk
Motor Pathways Lectures Objectives Define the terms upper and lower motor neurons with examples. Describe the corticospinal (pyramidal) tract and the direct motor pathways from the cortex to the trunk
1. The cerebellum coordinates fine movement through interactions with the following motor-associated areas:
 DENT/OBHS 131 2009 Take-home test 4 Week 6: Take-home test (2/11/09 close 2/18/09) 1. The cerebellum coordinates fine movement through interactions with the following motor-associated areas: Hypothalamus
DENT/OBHS 131 2009 Take-home test 4 Week 6: Take-home test (2/11/09 close 2/18/09) 1. The cerebellum coordinates fine movement through interactions with the following motor-associated areas: Hypothalamus
Identification number: TÁMOP /1/A
 Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Basal Ganglia. Today s lecture is about Basal Ganglia and it covers:
 Basal Ganglia Motor system is complex interaction between Lower motor neurons (spinal cord and brainstem circuits) and Upper motor neurons (pyramidal and extrapyramidal tracts) plus two main regulators
Basal Ganglia Motor system is complex interaction between Lower motor neurons (spinal cord and brainstem circuits) and Upper motor neurons (pyramidal and extrapyramidal tracts) plus two main regulators
Basal Ganglia. Steven McLoon Department of Neuroscience University of Minnesota
 Basal Ganglia Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Graduate School Discussion Wednesday, Nov 1, 11:00am MoosT 2-690 with Paul Mermelstein (invite your friends)
Basal Ganglia Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Graduate School Discussion Wednesday, Nov 1, 11:00am MoosT 2-690 with Paul Mermelstein (invite your friends)
Chapter 3. Structure and Function of the Nervous System. Copyright (c) Allyn and Bacon 2004
 Allyn and Bacon 2004") Chapter 3 Structure and Function of the Nervous System 1 Basic Features of the Nervous System Neuraxis: An imaginary line drawn through the center of the length of the central nervous system, from the
Chapter 3 Structure and Function of the Nervous System 1 Basic Features of the Nervous System Neuraxis: An imaginary line drawn through the center of the length of the central nervous system, from the
BRAIN STEM AND CEREBELLUM..
 Lecture Title: BRAIN STEM AND CEREBELLUM.. (CNS Block, Radiology) Dr. Hamdy Hassan Ass.Prof. Consultant Radiology Department KKHU King Saud University Lecture Objectives.. Students at the end of the lecture
Lecture Title: BRAIN STEM AND CEREBELLUM.. (CNS Block, Radiology) Dr. Hamdy Hassan Ass.Prof. Consultant Radiology Department KKHU King Saud University Lecture Objectives.. Students at the end of the lecture
The neurvous system senses, interprets, and responds to changes in the environment. Two types of cells makes this possible:
 NERVOUS SYSTEM The neurvous system senses, interprets, and responds to changes in the environment. Two types of cells makes this possible: the neuron and the supporting cells ("glial cells"). Neuron Neurons
NERVOUS SYSTEM The neurvous system senses, interprets, and responds to changes in the environment. Two types of cells makes this possible: the neuron and the supporting cells ("glial cells"). Neuron Neurons
Damage on one side.. (Notes) Just remember: Unilateral damage to basal ganglia causes contralateral symptoms.
 Just remember: Unilateral damage to basal ganglia causes contralateral symptoms.") Lecture 20 - Basal Ganglia Basal Ganglia (Nolte 5 th Ed pp 464) Damage to the basal ganglia produces involuntary movements. Although the basal ganglia do not influence LMN directly (to cause this involuntary
Lecture 20 - Basal Ganglia Basal Ganglia (Nolte 5 th Ed pp 464) Damage to the basal ganglia produces involuntary movements. Although the basal ganglia do not influence LMN directly (to cause this involuntary
By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy
 By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy 1 By the end of the lecture, students will be able to : Distinguish the internal structure of the components of the brain stem in different levels and the specific
By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy 1 By the end of the lecture, students will be able to : Distinguish the internal structure of the components of the brain stem in different levels and the specific
Transcranial sonography in movement disorders
 Transcranial sonography in movement disorders Uwe Walter 1st Residential Training of the European Society of Neurosonology and Cerebral Hemodynamics September 7-12, 2008 Bertinoro, Italy Department of
Transcranial sonography in movement disorders Uwe Walter 1st Residential Training of the European Society of Neurosonology and Cerebral Hemodynamics September 7-12, 2008 Bertinoro, Italy Department of
MODULE 6: CEREBELLUM AND BASAL GANGLIA
 MODULE 6: CEREBELLUM AND BASAL GANGLIA This module will summarize the important neuroanatomical and key clinical concepts from Chapters 15 and 16 of the textbook for the course. The first part of this
MODULE 6: CEREBELLUM AND BASAL GANGLIA This module will summarize the important neuroanatomical and key clinical concepts from Chapters 15 and 16 of the textbook for the course. The first part of this
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology
 Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
2401 : Anatomy/Physiology
 Dr. Chris Doumen Week 7 2401 : Anatomy/Physiology The Cerebrum Central Nervous System TextBook Readings Pages 434-456 and 460-461 Make use of the figures in your textbook ; a picture is worth a thousand
Dr. Chris Doumen Week 7 2401 : Anatomy/Physiology The Cerebrum Central Nervous System TextBook Readings Pages 434-456 and 460-461 Make use of the figures in your textbook ; a picture is worth a thousand
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16
 The Brain Chapter 14 and select portions of Chapter 16") Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16 I. Introduction A. Appearance 1. physical 2. weight 3. relative weight B. Major parts of the brain 1. cerebrum 2.
Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16 I. Introduction A. Appearance 1. physical 2. weight 3. relative weight B. Major parts of the brain 1. cerebrum 2.
Brainstem. By Dr. Bhushan R. Kavimandan
 Brainstem By Dr. Bhushan R. Kavimandan Development Ventricles in brainstem Mesencephalon cerebral aqueduct Metencephalon 4 th ventricle Mylencephalon 4 th ventricle Corpus callosum Posterior commissure
Brainstem By Dr. Bhushan R. Kavimandan Development Ventricles in brainstem Mesencephalon cerebral aqueduct Metencephalon 4 th ventricle Mylencephalon 4 th ventricle Corpus callosum Posterior commissure
Nsci 2100: Human Neuroanatomy 2017 Examination 3
 Name KEY Lab Section Nsci 2100: Human Neuroanatomy 2017 Examination 3 On this page, write your name and lab section. On your bubble answer sheet, enter your name (last name, space, first name), internet
Name KEY Lab Section Nsci 2100: Human Neuroanatomy 2017 Examination 3 On this page, write your name and lab section. On your bubble answer sheet, enter your name (last name, space, first name), internet
ORIGINAL CONTRIBUTION. Brain Magnetic Resonance Imaging in Multiple-System Atrophy and Parkinson Disease
 Brain Magnetic Resonance Imaging in Multiple-System Atrophy and Parkinson Disease A Diagnostic Algorithm ORIGINAL CONTRIBUTION Kirsty Bhattacharya, MD; Daniela Saadia, MD; Barbara Eisenkraft, MD; Melvin
Brain Magnetic Resonance Imaging in Multiple-System Atrophy and Parkinson Disease A Diagnostic Algorithm ORIGINAL CONTRIBUTION Kirsty Bhattacharya, MD; Daniela Saadia, MD; Barbara Eisenkraft, MD; Melvin
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts.
 Descending Tracts I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts. III: To define the upper and the lower motor neurons. 1. The corticonuclear
Descending Tracts I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts. III: To define the upper and the lower motor neurons. 1. The corticonuclear
The Nervous System: Sensory and Motor Tracts of the Spinal Cord
 15 The Nervous System: Sensory and Motor Tracts of the Spinal Cord PowerPoint Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska Introduction Millions of sensory
15 The Nervous System: Sensory and Motor Tracts of the Spinal Cord PowerPoint Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska Introduction Millions of sensory
Basal nuclei, cerebellum and movement
 Basal nuclei, cerebellum and movement MSTN121 - Neurophysiology Session 9 Department of Myotherapy Basal Nuclei (Ganglia) Basal Nuclei (Ganglia) Role: Predict the effects of various actions, then make
Basal nuclei, cerebellum and movement MSTN121 - Neurophysiology Session 9 Department of Myotherapy Basal Nuclei (Ganglia) Basal Nuclei (Ganglia) Role: Predict the effects of various actions, then make
Dean Shibata, M.D. Department of Radiology, University of Washington. White Matter, Metabolic, and Degenerative Disease.
 White Matter, Metabolic, and Degenerative Disease UW Radiology Review 2015 Dean Shibata, M.D Neuroradiology Department of Radiology, University of Washington MS (Multiple Sclerosis) ADEM (Acute Disseminated
White Matter, Metabolic, and Degenerative Disease UW Radiology Review 2015 Dean Shibata, M.D Neuroradiology Department of Radiology, University of Washington MS (Multiple Sclerosis) ADEM (Acute Disseminated
COGNITIVE SCIENCE 107A. Motor Systems: Basal Ganglia. Jaime A. Pineda, Ph.D.
 COGNITIVE SCIENCE 107A Motor Systems: Basal Ganglia Jaime A. Pineda, Ph.D. Two major descending s Pyramidal vs. extrapyramidal Motor cortex Pyramidal system Pathway for voluntary movement Most fibers originate
COGNITIVE SCIENCE 107A Motor Systems: Basal Ganglia Jaime A. Pineda, Ph.D. Two major descending s Pyramidal vs. extrapyramidal Motor cortex Pyramidal system Pathway for voluntary movement Most fibers originate
Dr. Farah Nabil Abbas. MBChB, MSc, PhD
 Dr. Farah Nabil Abbas MBChB, MSc, PhD The Basal Ganglia *Functions in association with motor cortex and corticospinal pathways. *Regarded as accessory motor system besides cerebellum. *Receive most of
Dr. Farah Nabil Abbas MBChB, MSc, PhD The Basal Ganglia *Functions in association with motor cortex and corticospinal pathways. *Regarded as accessory motor system besides cerebellum. *Receive most of
Unit VIII Problem 5 Physiology: Cerebellum
 Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Toxic and Metabolic Disease of Nervous System
 Toxic and Metabolic Disease of Nervous System Reid R. Heffner, MD Distinguished Teaching Professor Emeritus Department of Pathology and Anatomy January 14, 2019 1 I HAVE NO CONFLICTS OF INTEREST OR DISCLOSURES
Toxic and Metabolic Disease of Nervous System Reid R. Heffner, MD Distinguished Teaching Professor Emeritus Department of Pathology and Anatomy January 14, 2019 1 I HAVE NO CONFLICTS OF INTEREST OR DISCLOSURES
Extrapyramidal Motor System. Basal Ganglia or Striatum. Basal Ganglia or Striatum 3/3/2010
 Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Voluntary Movement. Ch. 14: Supplemental Images
 Voluntary Movement Ch. 14: Supplemental Images Skeletal Motor Unit: The basics Upper motor neuron: Neurons that supply input to lower motor neurons. Lower motor neuron: neuron that innervates muscles,
Voluntary Movement Ch. 14: Supplemental Images Skeletal Motor Unit: The basics Upper motor neuron: Neurons that supply input to lower motor neurons. Lower motor neuron: neuron that innervates muscles,
Biological Bases of Behavior. 3: Structure of the Nervous System
 Biological Bases of Behavior 3: Structure of the Nervous System Neuroanatomy Terms The neuraxis is an imaginary line drawn through the spinal cord up to the front of the brain Anatomical directions are
Biological Bases of Behavior 3: Structure of the Nervous System Neuroanatomy Terms The neuraxis is an imaginary line drawn through the spinal cord up to the front of the brain Anatomical directions are
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Pietro Cortelli. IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna
 Pietro Cortelli IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna HYSTORY 1900 description of OPCA (Dejerine, Thomas) 1960 description of Shy-Drager
Pietro Cortelli IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna HYSTORY 1900 description of OPCA (Dejerine, Thomas) 1960 description of Shy-Drager
LOCALIZATION NEUROLOGY EPISODE VI HEARING LOSS AND GAIT ATAXIA
 LOCALIZATION NEUROLOGY EPISODE VI HEARING LOSS AND GAIT ATAXIA EPISODE VI HEARING LOSS APPROACH and DIAGNOSIS 2 Cochlea and Auditory nerve Pons (superior olive) lateral lemniscus Inferior colliculus Thalamus
LOCALIZATION NEUROLOGY EPISODE VI HEARING LOSS AND GAIT ATAXIA EPISODE VI HEARING LOSS APPROACH and DIAGNOSIS 2 Cochlea and Auditory nerve Pons (superior olive) lateral lemniscus Inferior colliculus Thalamus
Basal Ganglia George R. Leichnetz, Ph.D.
 Basal Ganglia George R. Leichnetz, Ph.D. OBJECTIVES 1. To understand the brain structures which constitute the basal ganglia, and their interconnections 2. To understand the consequences (clinical manifestations)
Basal Ganglia George R. Leichnetz, Ph.D. OBJECTIVES 1. To understand the brain structures which constitute the basal ganglia, and their interconnections 2. To understand the consequences (clinical manifestations)
14 - Central Nervous System. The Brain Taft College Human Physiology
 14 - Central Nervous System The Brain Taft College Human Physiology Development of the Brain The brain begins as a simple tube, a neural tube. The tube or chamber (ventricle) is filled with cerebrospinal
14 - Central Nervous System The Brain Taft College Human Physiology Development of the Brain The brain begins as a simple tube, a neural tube. The tube or chamber (ventricle) is filled with cerebrospinal
The Neuroscience of Music in Therapy
 Course Objectives The Neuroscience of Music in Therapy Unit I. Learn Basic Brain Information Unit II. Music in the Brain; Why Music Works Unit III. Considerations for Populations a. Rehabilitation b. Habilitation
Course Objectives The Neuroscience of Music in Therapy Unit I. Learn Basic Brain Information Unit II. Music in the Brain; Why Music Works Unit III. Considerations for Populations a. Rehabilitation b. Habilitation
Brainstem. Amadi O. Ihunwo, PhD School of Anatomical Sciences
 Brainstem Amadi O. Ihunwo, PhD School of Anatomical Sciences Lecture Outline Constituents Basic general internal features of brainstem External and Internal features of Midbrain Pons Medulla Constituents
Brainstem Amadi O. Ihunwo, PhD School of Anatomical Sciences Lecture Outline Constituents Basic general internal features of brainstem External and Internal features of Midbrain Pons Medulla Constituents
MULTI SYSTEM ATROPHY: REPORT OF TWO CASES Dipu Bhuyan 1, Rohit Kr. Chandak 2, Pankaj Kr. Patel 3, Sushant Agarwal 4, Debjanee Phukan 5
 MULTI SYSTEM ATROPHY: REPORT OF TWO CASES Dipu Bhuyan 1, Rohit Kr. Chandak 2, Pankaj Kr. Patel 3, Sushant Agarwal 4, Debjanee Phukan 5 HOW TO CITE THIS ARTICLE: Dipu Bhuyan, Rohit Kr. Chandak, Pankaj Kr.
MULTI SYSTEM ATROPHY: REPORT OF TWO CASES Dipu Bhuyan 1, Rohit Kr. Chandak 2, Pankaj Kr. Patel 3, Sushant Agarwal 4, Debjanee Phukan 5 HOW TO CITE THIS ARTICLE: Dipu Bhuyan, Rohit Kr. Chandak, Pankaj Kr.
Lecture 4 The BRAINSTEM Medulla Oblongata
 Lecture 4 The BRAINSTEM Medulla Oblongata Introduction to brainstem 1- Medulla oblongata 2- Pons 3- Midbrain - - - occupies the posterior cranial fossa of the skull. connects the narrow spinal cord
Lecture 4 The BRAINSTEM Medulla Oblongata Introduction to brainstem 1- Medulla oblongata 2- Pons 3- Midbrain - - - occupies the posterior cranial fossa of the skull. connects the narrow spinal cord
Biomedical Technology Research Center 2011 Workshop San Francisco, CA
 Diffusion Tensor Imaging: Parkinson s Disease and Atypical Parkinsonism David E. Vaillancourt court1@uic.edu Associate Professor at UIC Departments t of Kinesiology i and Nutrition, Bioengineering, and
Diffusion Tensor Imaging: Parkinson s Disease and Atypical Parkinsonism David E. Vaillancourt court1@uic.edu Associate Professor at UIC Departments t of Kinesiology i and Nutrition, Bioengineering, and
Medical Neuroscience Tutorial Notes
 Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
DEVELOPMENT OF BRAIN
 Ahmed Fathalla OBJECTIVES At the end of the lecture, students should: List the components of brain stem. Describe the site of brain stem. Describe the relations between components of brain stem & their
Ahmed Fathalla OBJECTIVES At the end of the lecture, students should: List the components of brain stem. Describe the site of brain stem. Describe the relations between components of brain stem & their
Biological Bases of Behavior. 8: Control of Movement
 Biological Bases of Behavior 8: Control of Movement m d Skeletal Muscle Movements of our body are accomplished by contraction of the skeletal muscles Flexion: contraction of a flexor muscle draws in a
Biological Bases of Behavior 8: Control of Movement m d Skeletal Muscle Movements of our body are accomplished by contraction of the skeletal muscles Flexion: contraction of a flexor muscle draws in a
Gross Morphology of the Brain
 Gross Morphology of the Brain Done by : Marah Marahleh & Razan Krishan *slides in bold Principal Parts of the Brain Cerebrum : largest part of the brain Diencephalon Thalamus & hypothalamus Cerebellum
Gross Morphology of the Brain Done by : Marah Marahleh & Razan Krishan *slides in bold Principal Parts of the Brain Cerebrum : largest part of the brain Diencephalon Thalamus & hypothalamus Cerebellum
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT
 Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Brain Stem and cortical control of motor function. Dr Z Akbari
 Brain Stem and cortical control of motor function Dr Z Akbari Brain stem control of movement BS nuclear groups give rise to descending motor tracts that influence motor neurons and their associated interneurons
Brain Stem and cortical control of motor function Dr Z Akbari Brain stem control of movement BS nuclear groups give rise to descending motor tracts that influence motor neurons and their associated interneurons
The Central Nervous System I. Chapter 12
 The Central Nervous System I Chapter 12 The Central Nervous System The Brain and Spinal Cord Contained within the Axial Skeleton Brain Regions and Organization Medical Scheme (4 regions) 1. Cerebral Hemispheres
The Central Nervous System I Chapter 12 The Central Nervous System The Brain and Spinal Cord Contained within the Axial Skeleton Brain Regions and Organization Medical Scheme (4 regions) 1. Cerebral Hemispheres
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Cheyenne 11/28 Neurological Disorders II. Transmissible Spongiform Encephalopathy
 Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Stanley Pruisinger 1980's
 Neuroanatomy Prion disease cerebellum chapter b/c cerebellar ataxia here as a warning for obvious reasons. Creutzfeldt - Jakob Disease (CJD) "Spongiform" (brain turns to sponge) Jews in Lybia who ate
Neuroanatomy Prion disease cerebellum chapter b/c cerebellar ataxia here as a warning for obvious reasons. Creutzfeldt - Jakob Disease (CJD) "Spongiform" (brain turns to sponge) Jews in Lybia who ate
Central nervous system (CNS): brain and spinal cord Collections of cell body and dendrites (grey matter) are called nuclei/nucleus Nucleus can also
: brain and spinal cord Collections of cell body and dendrites (grey matter) are called nuclei/nucleus Nucleus can also") Chapter 3 Part 1 Orientation Directions in the nervous system are described relatively to the neuraxis An imaginary line drawn through the center of the length of the central nervous system, from the bottom
Chapter 3 Part 1 Orientation Directions in the nervous system are described relatively to the neuraxis An imaginary line drawn through the center of the length of the central nervous system, from the bottom
SENSORY (ASCENDING) SPINAL TRACTS
 SPINAL TRACTS") SENSORY (ASCENDING) SPINAL TRACTS Dr. Jamila El-Medany Dr. Essam Eldin Salama OBJECTIVES By the end of the lecture, the student will be able to: Define the meaning of a tract. Distinguish between the different
SENSORY (ASCENDING) SPINAL TRACTS Dr. Jamila El-Medany Dr. Essam Eldin Salama OBJECTIVES By the end of the lecture, the student will be able to: Define the meaning of a tract. Distinguish between the different
PTA 106 Unit 1 Lecture 1B
 PTA 106 Unit 1 Lecture 1B Medulla Oblongata Cardiovascular Center: Regulates the rate and force of the heartbeat and the diameter of blood vessels Medullary Rhythmicity Area: adjusts the basic rhythm of
PTA 106 Unit 1 Lecture 1B Medulla Oblongata Cardiovascular Center: Regulates the rate and force of the heartbeat and the diameter of blood vessels Medullary Rhythmicity Area: adjusts the basic rhythm of
Internal Organisation of the Brainstem
 Internal Organisation of the Brainstem Major tracts and nuclei of the brainstem (Notes) The brainstem is the major pathway for tracts and houses major nuclei, that contain sensory, motor and autonomics
Internal Organisation of the Brainstem Major tracts and nuclei of the brainstem (Notes) The brainstem is the major pathway for tracts and houses major nuclei, that contain sensory, motor and autonomics
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
b. The groove between the two crests is called 2. The neural folds move toward each other & the fuse to create a
 Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Magnetic resonance imaging findings in diagnosis and prognosis of Wilson disease
 Review Article Magnetic resonance imaging findings in diagnosis and prognosis of Wilson disease Mehri Salari 1, Emad Fayyazi 1,2, Omid Mirmosayyeb 1,2 1 Isfahan Neurosciences Research Center, Alzahra Research
Review Article Magnetic resonance imaging findings in diagnosis and prognosis of Wilson disease Mehri Salari 1, Emad Fayyazi 1,2, Omid Mirmosayyeb 1,2 1 Isfahan Neurosciences Research Center, Alzahra Research
Psyc 311A, fall 2008 Conference week 3 TA: Jürgen Germann
 Psyc 311A, fall 2008 Conference week 3 TA: Jürgen Germann e-mail: jurgen.germann@mcgill.ca Overview: 1. Meninges 2. Cerebral cortex-cytoarchitecture 3. Diencephalon (thalamus/hypothalamus) (this replaces
Psyc 311A, fall 2008 Conference week 3 TA: Jürgen Germann e-mail: jurgen.germann@mcgill.ca Overview: 1. Meninges 2. Cerebral cortex-cytoarchitecture 3. Diencephalon (thalamus/hypothalamus) (this replaces
Ch 13: Central Nervous System Part 1: The Brain p 374
 Ch 13: Central Nervous System Part 1: The Brain p 374 Discuss the organization of the brain, including the major structures and how they relate to one another! Review the meninges of the spinal cord and
Ch 13: Central Nervous System Part 1: The Brain p 374 Discuss the organization of the brain, including the major structures and how they relate to one another! Review the meninges of the spinal cord and
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Basal Nuclei (Ganglia)
") Doctor said he will not go deep within these slides because we will take them in physiology, so he will explain the anatomical structures, and he will go faster in the functions sheet in yellow Basal Nuclei
Doctor said he will not go deep within these slides because we will take them in physiology, so he will explain the anatomical structures, and he will go faster in the functions sheet in yellow Basal Nuclei
PSY 302: CHAPTER 3 NOTES THE BRAIN (PART II) - 9/5/17. By: Joseline
 - 9/5/17. By: Joseline") PSY 302: CHAPTER 3 NOTES THE BRAIN (PART II) - 9/5/17 By: Joseline Left 3 MAJOR FISSURES : 2HEMISPHERES Right Lateral Ventricle Central Fissure Third Ventricle Sulcus Lateral Fissure Gyros Fissure- Fissures
PSY 302: CHAPTER 3 NOTES THE BRAIN (PART II) - 9/5/17 By: Joseline Left 3 MAJOR FISSURES : 2HEMISPHERES Right Lateral Ventricle Central Fissure Third Ventricle Sulcus Lateral Fissure Gyros Fissure- Fissures
Imaging of Hearing Loss
 Contemporary Imaging of Sensorineural Hearing Loss Imaging of Hearing Loss Discussion Outline (SNHL) Imaging Approaches Anatomic Relationships Lesions: SNHL KL Salzman, MD University of Utah School of
Contemporary Imaging of Sensorineural Hearing Loss Imaging of Hearing Loss Discussion Outline (SNHL) Imaging Approaches Anatomic Relationships Lesions: SNHL KL Salzman, MD University of Utah School of
Fig.1: A, Sagittal 110x110 mm subimage close to the midline, passing through the cingulum. Note that the fibers of the corpus callosum run at a
 Fig.1 E Fig.1:, Sagittal 110x110 mm subimage close to the midline, passing through the cingulum. Note that the fibers of the corpus callosum run at a slight angle are through the plane (blue dots with
Fig.1 E Fig.1:, Sagittal 110x110 mm subimage close to the midline, passing through the cingulum. Note that the fibers of the corpus callosum run at a slight angle are through the plane (blue dots with
Neuroanatomy. Dr. Maha ELBeltagy. Assistant Professor of Anatomy Faculty of Medicine The University of Jordan
 Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Prof Yousry 10/15/17 Types of brain fibers THE WHITE MATTER OF THE BRAIN The white matter
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Prof Yousry 10/15/17 Types of brain fibers THE WHITE MATTER OF THE BRAIN The white matter
10/3/2016. T1 Anatomical structures are clearly identified, white matter (which has a high fat content) appears bright.
 appears bright.") H2O -2 atoms of Hydrogen, 1 of Oxygen Hydrogen just has one single proton and orbited by one single electron Proton has a magnetic moment similar to the earths magnetic pole Also similar to earth in that
H2O -2 atoms of Hydrogen, 1 of Oxygen Hydrogen just has one single proton and orbited by one single electron Proton has a magnetic moment similar to the earths magnetic pole Also similar to earth in that
Objectives. Distinguishing Parkinson s disease from other parkinsonian and tremor syndromes. Characteristics. Basal Ganglia Structures
 12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships
12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships