EPIDEMIOLOGY AND CLASSIFICATION OF MOVEMENT DISORDERS
|
|
|
- Arron Hall
- 6 years ago
- Views:
Transcription
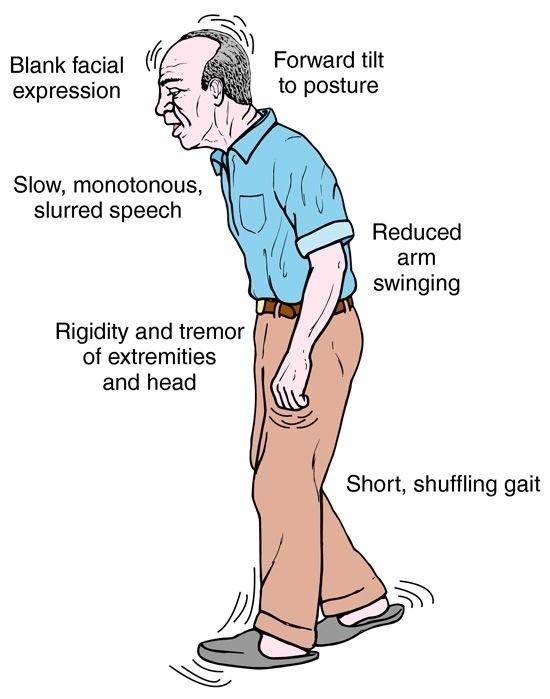
1 EPIDEMIOLOGY AND CLASSIFICATION OF MOVEMENT DISORDERS Njideka U. Okubadejo Professor & Consultant Neurologist College of Medicine, University of Lagos & Lagos University Teaching Hospital, Lagos State, Nigeria Chairperson Task Force on Africa & Africa Section Steering Committee, International Parkinson Disease and Movement Disorders Society (MDS)

2 To disseminate knowledge and promote research to advance the field of Movement Disorders
3 No fee* Waived dues membership Specifically designed to enable those on a lower income to join the Society. All member benefits except the print version of the journal Movement Disorders. Apply every 3 years to renew membership. Task Force on Africa krudolph@movementdisorders.org

4 MDS Outreach Education Programs
5 Asynchronous Consultation for Movement Disorders (ACMD) Project Improve patient care in regions with limited access to specialists. Provide education on movement disorders for local physicians. Bring together doctors across different timezones, with different levels of access to participate. Contact:
6 No fee* Waived dues membership Specifically designed to enable those on a lower income to join the Society. Individuals who reside in countries classified as lowincome, lower-middle-income or upper-middleincome economies by the World Bank are eliguble. * Benefits include all member benefits except the print journal Movement Disorders. Waived Dues Members need to apply every 3 years in order to renew their membership.
7 Learning Objectives To briefly describe the epidemiology of movement disorders from a global and African perspective To describe the current classification of movement disorders in general To describe the current classification of common movement disorders
8 Outline Definition of movement disorders Epidemiology (Global data; Africa data) Parkinson disease Essential tremor Classification Broad subtypes Parkinsonism Dystonia Tremor Ataxias
9 What are movement disorders? Previously referred to as extrapyramidal disorders BUT.. basal ganglia is not entirely extrapyramidal: intimate connections with pyramidal tract other extrapyramidal non-basal ganglia tracts exist e.g. descending vestibulospinal and reticulospinal pathways some disorders of abnormal movement are not associated with basal ganglia function (e.g. ataxia, myoclonus) Preferred term is that based on clinical phenomenology rather than anatomic location Coined by Stanley Fahn and Lewis P. Rowland in 1968.
10 Definition Neurological syndromes in which there is EITHER an excess of movement OR a paucity of voluntary and automatic movements, unrelated to weakness or spasticity
11 EPIDEMIOLOGY
12 Epidemiology: Global Common neurological disorders Availability of population-based data for all movement disorders is hampered by the broad spectrum of conditions Most prevalence data refer to specific movement disorders Hospital-based data provide insight into more disabling MDs
13 Disorder Prevalence of movement disorders Prevalence rate per 100,000 population RLS 9800 (age 65 83) Essential tremor 415 Parkinson disease 187 Tourette syndrome /2990 Primary torsion dystonia 33 Hemifacial spasm Blepharospasm 13.3 Hereditary ataxia 6 Huntington disease 6 Wilson disease 3 PSP MSA 4.4 Fahn S, Jankovic J. Principles and Practice of Movement Disorders, 2007: page 5
14 Percentage Hospital-based frequency of MD Adapted from Fahn & Jancovic; data from 2 large MD clinics in USA 1996
15 Hospital-based frequency of MD: Africa ~5 15% of outpatient neurology consultations (Bower JH et al, Ethiopia, 2005; Tegueu et al, Cameroon, 2013) Hypokinesias 55.4%; Hyperkinesias 44.6% (Okubadejo et al, 2012) Most common Parkinsonism/Parkinson disease Predominant forms: (similar to global MD clinic reports) parkinsonism other tremors dystonia
16 Okubadejo NU et al. Spectrum of movement disorders at the premier Lagos Movement Disorders Clinic in Nigeria: First year s experience(2012), Poster Presentations. Mov. Disord., 27: S1 S523. doi: /mds.25051
17 PARKINSON DISEASE One of the most frequent (top 10) neurological diseases encountered in primary care globally, including in Africa. PD frequency in specialist care: 4 th major neurological disease encountered in specialist care (46.2%) overall, 18.8% (6 th in Africa) and 66.7% (4 th in SE Asia). Burden (population) of PD from 2015 to 2030 Developing countries: 2.37 mill (39.7%) to 3.08 mill(42.5%) Developed countries: 3.60 mill (60.3%) to 4.16 ml (57.5%)
18 Proportion (%) of PD in emerging and developed countries: 2015 to Emerging countries Developed countries Year 2015 Year 2030

19 Dorsey ER, et al. Projected number of people with Parkinson disease in the most populous nations, 2005 through Neurology. 2007;68(5):384-6.
20 PD epidemiology ii Affects ~ 1% population yrs; 4.3% >85 yrs Prevalence rates vary widely: methodological, geographic, genetic, environmental differences In metanalysis, steady increased prevalence with age Age-standardized DALY rates rank (Global Burden of Disease Study 2015) for all neurologic dx (14 categories) Global: 11 th North, central SSA, western SSA: 11 th Eastern SSA: 12 th Southern SSA: 10 th

. Movement Disorders.")
21 Prevalence per 100, Global prevalence of PD > 80 Age category (years) Based on data from systematic review by Pringsheim T. et al (2014). Movement Disorders. 29(13):
22 Movement Disorders. 2006;21(12):
23 PD epidemiology iii: incidence Based on most recent systematic review and metanalysis (Hirsch L, et al. Neuroepidemiologu 2016;46: ) Overall incidence (females >40): per 100,000 person-years Overall incidence (males > 40): per 100,000 personyears Increased incidence with age in both sexes
24 BMC Neurology 2010;10:1 (doi: / Descriptive study of General Neurology Clinic based PD cases: parkinsonism 98 (79.0% PD) and 26 (21.0% others) Mean time from onset to diagnosis: 24.6 months (median 12 mo) Severity at presentation (Hoehn and Yahr stage 2)
25 PD: environmental risk factors Variable evidence for specific risk factors Rural living, agricultural occupation, well water consumption Pesticides paraquat, rotenone, organochlorines, organophosphates, permethrin, benomyl Solvents Polychlorinated biphenyls Mild to moderate head injury Toxins: MPTP Behavioural risk factors (reduced risk): caffeine and cigarette smoking
26 PD: genetic factors Monogenic causes of PD/parkinsonism Classic PD: PARK-SNCA, PARK-LRRK2, PARK-VPS35 (all autosomal dominant) Early onset PD: PARK-parkin, PARK-PINK1, PARK-DJ1 (all autosomal recessive) Parkinsonism: PARK-ATP13A2, PARK-FBX07, PARK- DNAJC6, PARK-SYNJ1 Genetic risk variants (GWAS): > 26 genetic risk variants consistently associated

27 ESSENTIAL TREMOR Most common tremor Worldwide prevalence: per 1000 Highest prevalence >60: per 1000 Prevalence in Lagos: 23.8 per 1000 (age-adjusted to WHO New world population) Consistent increase in prevalence with advancing age
28 CLASSIFICATION
29 Broad subtypes of MD Hypokinesias Hyperkinesias
30 Hypokinesias 1.Parkinsonism (Akinesia/bradykinesia) 2. Apraxia 3. Cataplexy and drop attacks 4. Freezing 5. Rigidity 6. Blocking (holding) tics 7. Catatonia, psychomotor depression, and obsessional slowness 8. Hesitant gaits 9. Hypothyroid slowness 10. Stiff muscles
31 Hyperkinesias 1. Tremors 2. Dystonia 3. Chorea/Athetosis/ Ballism 4. Ataxia/dysmetria 5. Myoclonus 6. Hemifacial spasm 7. Tics 8. Hyperekplexia 9. RBD 10. Myokymia and synkinesis 11. Restless legs 12. Moving toes/fingers 13. Paroxysmal dyskinesia 14. Abdominal dyskinesias 15. Akathisia 16. Hypnogenic dyskinesias 17. Jumpy stumps 18. Myorhythmia 19. Stereotypy
32 PARKINSONISM
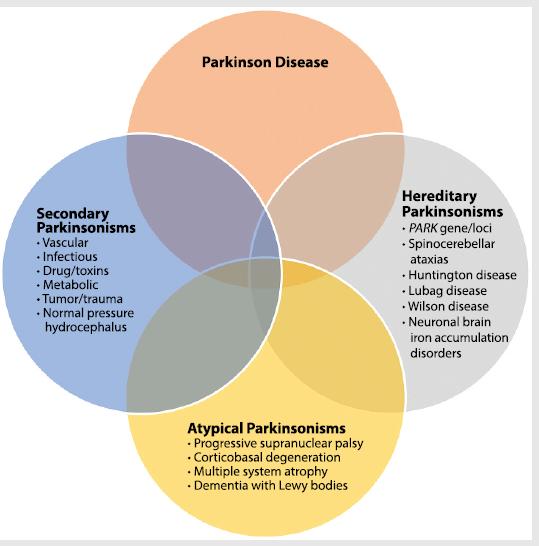
33 Parkinsonism: classification I. Primary (Parkinson disease, idiopathic PK) II. Atypical parkinsonism: MSA, PSP, CBD, parkinsonism with dementia III. Heredodegenerative disorders I. Secondary: infections, toxins, drugs, tumor, trauma, vascular, metabolic
34 Continuum. 2016;22(4):
35 Classification of PD (motor subtypes) i. Tremor dominant ii. Postural impairment and gait disturbance (PIGD)
36 Multiple system atrophy (subtypes) i. MSA - cerebellar ii. MSA parkinsonian
37 Progressive supranuclear palsy subtypes/phenotypes Classic PSP (Richardson disease) PSP parkinsonism PSP pure akinesia with freezing of gait PSP corticobasal syndrome PSP behavioural variant of frontotemporal dementia PSP cerebellar ataxia PSP primary lateral sclerosis
38 Corticobasal degeneration (CBD) subtypes/phenotypes Corticobasal syndrome (classic CBD) CBS frontal behavioural variant CBS posterior cortical atrophy syndrome CBS progressive non-fluent /agrammatic aphasia CBS PSP syndrome
39 DYSTONIA
40 Dystonia Axis I: Clinical characteristics Age at onset Infancy (birth 2 years) Childhood (3 12 years) Adolescence (13 20 years) Early adulthood (21 40 yrs) Late adulthood (> 40 years) Body distribution Focal Segmental Multifocal Generalized (with or without leg involvement) Hemidystonia Temporal pattern Disease course: Static or Progressive Variability: persistent, actionspecific, diurnal, paroxysmal Coexistence of other movement disorders Isolated dystonia (±tremor) Combined (with another MD e.g. myoclonus, park) Other neurological manifestations (complex) Other systemic features Movement Disorders, Vol. 28, No. 7, 2013
41 Dystonia Axis II: Aetiology Nervous system pathology Evidence of degeneration Evidence of structural (often static) lesion No evidence of degeneration or structural lesion Inherited or acquired Inherited: AD, AR, X-linked recessive, Mitochondrial Acquired: Perinatal brain injury, infection, drug, toxic, vascular, neoplastic, brai injury, psychogenic Idiopathic: Sporadic, Familial Movement Disorders, Vol. 28, No. 7, 2013
42 TREMOR
43 Tremor: classification by phenomenology A) Rest tremor B) Action tremor i. Postural tremor i. Position-independent postural tremor ii. Position-dependent postural tremor ii. Kinetic tremor a) Simple (non goal directed) b) Target-directed (intention) iii. Task-specific kinetic tremor iv. Isometric tremor
44 Tremor: syndromic classification a) Physiologic tremor b) Enhanced physiologic tremor c) Essential tremor d) Dystonic tremor e) Parkinsonian tremor g) Holmes tremor h) Palatal tremor i) Drug/ Toxin-induced j) Tremor in periph. neuropathy k) Psychogenic tremor l) Unclassified f) Cerebellar tremor
45 ATAXIAS
46 Classification Age of onset Time course: acute, subacute, chronic, episodic Anatomic involvement Distribution: focal or generalized/symmetrical Cause: acquired or inherited or sporadic
47 Hereditary ataxias Autosomal dominant: Spinocerebellar ataxias (SCAs), DRPLA, episodic ataxias 1 & 2 Autosomal recessive: e.g. Friedreich ataxia, Ataxia telangiectasia X-linked Mitochondrial e.g. MERRF, MELAS

48 Systematic Approach to Diagnosis of Movement Disorders Abdo WF, et al. Nat. Rev. Neurol. 2010
49 References Fahn S. Classification of movement disorders. Movement Disorders. 2011;26(6): World Health Organization. Neurological disorders: public health challenges World Health Organization. Atlas: country resources for neurological disorders Patel V, et al. Advisory Group of the Movement for Global Mental Health. The Lancet s Series on Global Mental Health: 1 year on. Lancet. 2008; 372: Obeso JA et al. Past, Present, and Future of Parkinson s Disease: A Special Essay on the 200th Anniversary of the Shaking Palsy. Movement Disorders, Vol. 32, No. 9, 2017




50
Shake It Off: Recognizing & Treating Movement Disorders
 Ooi Phaik Yee Annual scientific meeting College of Medicine, Academy of Medicine of Malaysia 12 th November 2017 Shake It Off: Recognizing & Treating Movement Disorders MOVEMENT DISORDER A group of symptoms
Ooi Phaik Yee Annual scientific meeting College of Medicine, Academy of Medicine of Malaysia 12 th November 2017 Shake It Off: Recognizing & Treating Movement Disorders MOVEMENT DISORDER A group of symptoms
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Phenomenology of Movement Disorders
 Phenomenology of Movement Disorders Raja Mehanna MD Anatomical reasoning Anatomical reasoning Phenomenological reasoning Abnormal movement Hypokinetic Hyperkinetic Ataxia Video 1 But there is a tremor!
Phenomenology of Movement Disorders Raja Mehanna MD Anatomical reasoning Anatomical reasoning Phenomenological reasoning Abnormal movement Hypokinetic Hyperkinetic Ataxia Video 1 But there is a tremor!
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Table of Contents. Preface... xi. Part I: Introduction to Movement Disorders
 Table of Contents Visit www.healthreferenceseries.com to view A Contents Guide to the Health Reference Series, a listing of more than 14,000 topics and the volumes in which they are covered. Preface...
Table of Contents Visit www.healthreferenceseries.com to view A Contents Guide to the Health Reference Series, a listing of more than 14,000 topics and the volumes in which they are covered. Preface...
GENETICS AND TREATMENT OF DYSTONIA
 GENETICS AND TREATMENT OF DYSTONIA Oksana Suchowersky, M.D., FRCPC, FCCMG Professor of Medicine, Medical Genetics, and Psychiatry Toupin Research Chair in Neurology DYSTONIA Definition: abnormal sustained
GENETICS AND TREATMENT OF DYSTONIA Oksana Suchowersky, M.D., FRCPC, FCCMG Professor of Medicine, Medical Genetics, and Psychiatry Toupin Research Chair in Neurology DYSTONIA Definition: abnormal sustained
An Approach to Patients with Movement Disorders
 An Approach to Patients with Movement Disorders Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon EDUCATIONAL TOOLS MDS video library
An Approach to Patients with Movement Disorders Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon EDUCATIONAL TOOLS MDS video library
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Diagnosis and treatment of dystonia
 Diagnosis and treatment of dystonia Professor Tom Warner, Reta Lila Weston Institute of Neurological Studies UCL Institute of Neurology National Hospital for Neurology and Neurosurgery Queen Square What
Diagnosis and treatment of dystonia Professor Tom Warner, Reta Lila Weston Institute of Neurological Studies UCL Institute of Neurology National Hospital for Neurology and Neurosurgery Queen Square What
Diagnosis and treatment of dystonia
 Diagnosis and treatment of dystonia Professor Tom Warner, Reta Lila Weston Institute of Neurological Studies UCL Institute of Neurology National Hospital for Neurology and Neurosurgery Queen Square What
Diagnosis and treatment of dystonia Professor Tom Warner, Reta Lila Weston Institute of Neurological Studies UCL Institute of Neurology National Hospital for Neurology and Neurosurgery Queen Square What
Disorders of gait and balance
 Disorders of gait and balance clinical assessment and classification Evžen Růžička Charles University in Prague 1st Medical Faculty and General University Hospital handout additional videos and photos
Disorders of gait and balance clinical assessment and classification Evžen Růžička Charles University in Prague 1st Medical Faculty and General University Hospital handout additional videos and photos
An approach to movement disorders. Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London
 An approach to movement disorders Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London Neurology Diagnosis Two main questions: What parts of the nervous
An approach to movement disorders Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London Neurology Diagnosis Two main questions: What parts of the nervous
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y
 Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Department of Neurology, Rigshospitalet, 9 Blegdamsvej, PAULSON, O.B. Involuntary Movements. Tohoku J. Exp. Med., 1990, 161,
 Tohoku J. Exp. Med., 1990, 161, Suppl., 21-27 Involuntary Movements OLAF B. PAULSON Department of Neurology, Rigshospitalet, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark PAULSON, O.B. Involuntary Movements.
Tohoku J. Exp. Med., 1990, 161, Suppl., 21-27 Involuntary Movements OLAF B. PAULSON Department of Neurology, Rigshospitalet, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark PAULSON, O.B. Involuntary Movements.
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Movement disorders. Dr Rick Leventer Royal Children s Hospital
 Movement disorders Dr Rick Leventer Royal Children s Hospital richard.leventer@rch.org.au Movement disorders! conditions that affect the speed, fluency, quality, and ease of movement! usually affect TONE
Movement disorders Dr Rick Leventer Royal Children s Hospital richard.leventer@rch.org.au Movement disorders! conditions that affect the speed, fluency, quality, and ease of movement! usually affect TONE
Update on Parkinson s disease and other Movement Disorders October 2018
 Update on Parkinson s disease and other Movement Disorders October 2018 DR. JONATHAN EVANS CONSULTANT IN NEUROLOGY QUEEN S MEDICAL CENTRE NOTTINGHAM Disclosures: Honoraria UCB, Britannia, Allergan, AbbVie
Update on Parkinson s disease and other Movement Disorders October 2018 DR. JONATHAN EVANS CONSULTANT IN NEUROLOGY QUEEN S MEDICAL CENTRE NOTTINGHAM Disclosures: Honoraria UCB, Britannia, Allergan, AbbVie
I do not have any disclosures
 Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Movement disorders in childhood: assessment and diagnosis. Lucinda Carr
 Movement disorders in childhood: assessment and diagnosis Lucinda Carr Movement disorders in childhood: Assessment Classification Causes Diagnosis Presentation of movement disorders in childhood: Concerns
Movement disorders in childhood: assessment and diagnosis Lucinda Carr Movement disorders in childhood: Assessment Classification Causes Diagnosis Presentation of movement disorders in childhood: Concerns
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Objectives. RAIN Difficult Diagnosis 2014: A 75 year old woman with falls. Case History: First visit. Case History: First Visit
 Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
MAXIMIZING FUNCTION IN PARKINSON S DISEASE
 1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE
 FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE DEE SILVER M.D MOVEMENT DISORDER SPECIALIST MEDICAL DIRECTOR -- PARKINSON ASSOCIATION OF SAN DIEGO 1980 TO PRESENT SCRIPPS MEMORIAL HOSPITAL, LA JOLLA CA.
FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE DEE SILVER M.D MOVEMENT DISORDER SPECIALIST MEDICAL DIRECTOR -- PARKINSON ASSOCIATION OF SAN DIEGO 1980 TO PRESENT SCRIPPS MEMORIAL HOSPITAL, LA JOLLA CA.
STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS)
") STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS) Karen M. Thomas D.O. Diplomate, ABPN Director of Movement Disorders Program Director of Comprehensive Parkinson s Disease Program Sentara
STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS) Karen M. Thomas D.O. Diplomate, ABPN Director of Movement Disorders Program Director of Comprehensive Parkinson s Disease Program Sentara
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Imaging biomarkers for Parkinson s disease
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 6 MDS-ES/EAN: Neuroimaging in movement disorders - Level 2 Imaging biomarkers for Parkinson
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 6 MDS-ES/EAN: Neuroimaging in movement disorders - Level 2 Imaging biomarkers for Parkinson
DISORDERS OF THE MOTOR SYSTEM. Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology
 Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Movement Disorders- Parkinson s Disease. Fahed Saada, MD March 8 th, th Family Medicine Refresher Course St.
 Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
! slow, progressive, permanent loss of neurologic function.
 UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
Initial symptom or syndrome: (1) FOCAL WEAKNESS OR NUMBNESS
 FOCAL WEAKNESS OR NUMBNESS") View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
Atypical parkinsonism
 Atypical parkinsonism Wassilios Meissner Service de neurologie et CMR atrophie multisystématisée, CHU de Bordeaux Institut des Maladies Neurodégénératives, Université Bordeaux 2, CNRS UMR 5293 Parkinsonism?
Atypical parkinsonism Wassilios Meissner Service de neurologie et CMR atrophie multisystématisée, CHU de Bordeaux Institut des Maladies Neurodégénératives, Université Bordeaux 2, CNRS UMR 5293 Parkinsonism?
MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS
 MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS There are a wide variety of Neurologic and Musculoskeletal disorders which can impact driving safety. Impairment may be the result of altered muscular, skeletal,
MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS There are a wide variety of Neurologic and Musculoskeletal disorders which can impact driving safety. Impairment may be the result of altered muscular, skeletal,
Dystonia: Title. A real pain in the neck. in All the Wrong Places
 Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Update on the Genetics of Ataxia. Vicki Wheelock MD UC Davis Department of Neurology GHPP Clinic
 Update on the Genetics of Ataxia Vicki Wheelock MD UC Davis Department of Neurology GHPP Clinic Outline Definitions Review of genetics Autosomal Dominant cerebellar ataxias Autosomal Recessive cerebellar
Update on the Genetics of Ataxia Vicki Wheelock MD UC Davis Department of Neurology GHPP Clinic Outline Definitions Review of genetics Autosomal Dominant cerebellar ataxias Autosomal Recessive cerebellar
USING PRECISION MEDICINE TO HELP PATIENTS WITH PARKINSON S DISEASE. The Michael J. Fox Foundation for Parkinson s Research
 USING PRECISION MEDICINE TO HELP PATIENTS WITH PARKINSON S DISEASE The Michael J. Fox Foundation for Parkinson s Research MJFF IS THE WORLD S LARGEST NONPROFIT FUNDER OF PD RESEARCH Our Mission We are
USING PRECISION MEDICINE TO HELP PATIENTS WITH PARKINSON S DISEASE The Michael J. Fox Foundation for Parkinson s Research MJFF IS THE WORLD S LARGEST NONPROFIT FUNDER OF PD RESEARCH Our Mission We are
Non-Genetic Ataxia Susan L. Perlman, M.D. Clinical Professor of Neurology David Geffen School of Medicine at UCLA Director, Ataxia Clinic
 Non-Genetic Ataxia Susan L. Perlman, M.D. Clinical Professor of Neurology David Geffen School of Medicine at UCLA Director, Ataxia Clinic Is Anything Non-Genetic? 1,212,000 references in PubMed under genetics
Non-Genetic Ataxia Susan L. Perlman, M.D. Clinical Professor of Neurology David Geffen School of Medicine at UCLA Director, Ataxia Clinic Is Anything Non-Genetic? 1,212,000 references in PubMed under genetics
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer
 The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
Objectives. Distinguishing Parkinson s disease from other parkinsonian and tremor syndromes. Characteristics. Basal Ganglia Structures
 12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships
12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships
10/13/2017. Disclosures. Deep Brain Stimulation in the Treatment of Movement Disorders. Deep Brain Stimulation: Objectives.
 Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Phenotypic Variability in ALS
 Phenotypic Variability in ALS Michael A. Elliott, MD, FAAN Medical Director, ALS Clinic Swedish Neuroscience Institute 1 Outline ALS Background Description Typical Presentation Clinical Phenotype Motor
Phenotypic Variability in ALS Michael A. Elliott, MD, FAAN Medical Director, ALS Clinic Swedish Neuroscience Institute 1 Outline ALS Background Description Typical Presentation Clinical Phenotype Motor
FTD basics! Etienne de Villers-Sidani, MD!
 FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
2016 Programs & Information
 Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
MOVEMENT DISORDERS UPDATE H. MURRAY TODD, M.D., F.A.A.N.
 MOVEMENT DISORDERS UPDATE H. MURRAY TODD, M.D., F.A.A.N. Movement Disorders Hypokinesia : decreased voluntary and automatic movements Hyperkinesia : excessive movements HYPOKINESIAS Parkinson s disease
MOVEMENT DISORDERS UPDATE H. MURRAY TODD, M.D., F.A.A.N. Movement Disorders Hypokinesia : decreased voluntary and automatic movements Hyperkinesia : excessive movements HYPOKINESIAS Parkinson s disease
Hubert H. Fernandez, MD
 Hubert H. Fernandez, MD Associate Professor Co-Director, Movement Disorders Center Director, Clinical Trials for Movement Disorders Program Director, Neurology Residency and Movement Disorders Fellowship
Hubert H. Fernandez, MD Associate Professor Co-Director, Movement Disorders Center Director, Clinical Trials for Movement Disorders Program Director, Neurology Residency and Movement Disorders Fellowship
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Differential Diagnosis of Movement Disorders in Clinical Practice
 Differential Diagnosis of Movement Disorders in Clinical Practice Abdul Qayyum Rana Peter Hedera Differential Diagnosis of Movement Disorders in Clinical Practice Abdul Qayyum Rana Parkinson's Clinic
Differential Diagnosis of Movement Disorders in Clinical Practice Abdul Qayyum Rana Peter Hedera Differential Diagnosis of Movement Disorders in Clinical Practice Abdul Qayyum Rana Parkinson's Clinic
This is a free sample of content from Parkinson's Disease. Click here for more information or to buy the book.
 A AADC. See Aromatic amino acid decarboxylase AAV. See Adeno-associated virus Acetylcholine (ACh), functional imaging, 174 175 ACh. See Acetylcholine Adaptive immune system central nervous system, 381
A AADC. See Aromatic amino acid decarboxylase AAV. See Adeno-associated virus Acetylcholine (ACh), functional imaging, 174 175 ACh. See Acetylcholine Adaptive immune system central nervous system, 381
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Hypokinetic Movement Disorders
 Hypokinetic Movement Disorders Ariane Park, MD, MPH Assistant Professor-Clinical Division of Neurology The Ohio State University Wexner Medical Center Hypokinetic movement disorders Diminished voluntary
Hypokinetic Movement Disorders Ariane Park, MD, MPH Assistant Professor-Clinical Division of Neurology The Ohio State University Wexner Medical Center Hypokinetic movement disorders Diminished voluntary
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
HEREDITARY ATAXIAS (HA)
") HEREDITARY ATAXIAS (HA) Elison Sarapura-Castro January 11, 2018 OUTLINE Background Causes of ataxia and classification of HA SCAs Diagnostic workup Final Remarks BACKGROUND 25 years ago, ATAXIA: Abscense
HEREDITARY ATAXIAS (HA) Elison Sarapura-Castro January 11, 2018 OUTLINE Background Causes of ataxia and classification of HA SCAs Diagnostic workup Final Remarks BACKGROUND 25 years ago, ATAXIA: Abscense
Parkinson s Disease and other related movement disorders a video guide to diagnosis
 Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
Moving fast or moving slow: an overview of Movement Disorders
 Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Enhanced Primary Care Pathway: Parkinson s Disease
 Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Deep Brain Stimulation: Patient selection
 Deep Brain Stimulation: Patient selection Halim Fadil, MD Movement Disorders Neurologist Kane Hall Barry Neurology Bedford/Keller, TX 1991: Thalamic (Vim) DBS for tremor Benabid AL, et al. Lancet. 1991;337(8738):403-406.
Deep Brain Stimulation: Patient selection Halim Fadil, MD Movement Disorders Neurologist Kane Hall Barry Neurology Bedford/Keller, TX 1991: Thalamic (Vim) DBS for tremor Benabid AL, et al. Lancet. 1991;337(8738):403-406.
LOCALIZATION NEUROLOGY EPISODE VI HEARING LOSS AND GAIT ATAXIA
 LOCALIZATION NEUROLOGY EPISODE VI HEARING LOSS AND GAIT ATAXIA EPISODE VI HEARING LOSS APPROACH and DIAGNOSIS 2 Cochlea and Auditory nerve Pons (superior olive) lateral lemniscus Inferior colliculus Thalamus
LOCALIZATION NEUROLOGY EPISODE VI HEARING LOSS AND GAIT ATAXIA EPISODE VI HEARING LOSS APPROACH and DIAGNOSIS 2 Cochlea and Auditory nerve Pons (superior olive) lateral lemniscus Inferior colliculus Thalamus
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Tremor. Mario Zappia. Università degli Studi di Catania
 Tremor Mario Zappia Università degli Studi di Catania Tremor: Definition Rhythmical, Involuntary, Oscillatory movement of a body part Classification of Dyskinesias Based on Rhythmicity Rhythmical Dyskinesias:
Tremor Mario Zappia Università degli Studi di Catania Tremor: Definition Rhythmical, Involuntary, Oscillatory movement of a body part Classification of Dyskinesias Based on Rhythmicity Rhythmical Dyskinesias:
2/18/ yo man with history of mild developmental delay and chorea of unclear etiology, with new complaints of speech difficulty
 18 yo man with history of mild developmental delay and chorea of unclear etiology, with new complaints of speech difficulty Audrey Foster-Barber UCSF Child Neurology February 18, 2011 Several years of
18 yo man with history of mild developmental delay and chorea of unclear etiology, with new complaints of speech difficulty Audrey Foster-Barber UCSF Child Neurology February 18, 2011 Several years of
Evolution of a concept: Apraxia/higher level gait disorder. ataxia v. apraxia gait = limb apraxia. low, middle, high gait disturbance levels
 Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Multiple System Atrophy
 Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Clinical Spectrum and Genetic Mechanism of GLUT1-DS. Yasushi ITO (Tokyo Women s Medical University, Japan)
") Clinical Spectrum and Genetic Mechanism of GLUT1-DS Yasushi ITO (Tokyo Women s Medical University, Japan) Glucose transporter type 1 (GLUT1) deficiency syndrome Mutation in the SLC2A1 / GLUT1 gene Deficiency
Clinical Spectrum and Genetic Mechanism of GLUT1-DS Yasushi ITO (Tokyo Women s Medical University, Japan) Glucose transporter type 1 (GLUT1) deficiency syndrome Mutation in the SLC2A1 / GLUT1 gene Deficiency
Transcranial sonography in movement disorders
 Transcranial sonography in movement disorders Uwe Walter 1st Residential Training of the European Society of Neurosonology and Cerebral Hemodynamics September 7-12, 2008 Bertinoro, Italy Department of
Transcranial sonography in movement disorders Uwe Walter 1st Residential Training of the European Society of Neurosonology and Cerebral Hemodynamics September 7-12, 2008 Bertinoro, Italy Department of
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
Functional Distinctions
 Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Parkinson s Disease Update
 Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else?
 Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
Types of involuntary movements
 Tremor Types of involuntary movements Dystonia Chorea Myoclonus Tics Tremor Rhythmic shaking of muscles that produces an oscillating movement Parkinsonian tremor Rest tremor > posture > kinetic Re-emergent
Tremor Types of involuntary movements Dystonia Chorea Myoclonus Tics Tremor Rhythmic shaking of muscles that produces an oscillating movement Parkinsonian tremor Rest tremor > posture > kinetic Re-emergent
CN V! touch! pain! Touch! P/T!
 CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
Martin A. Samuels, M.D. MOVEMENT DISORDERS
 Martin A. Samuels, M.D. MOVEMENT DISORDERS I. Nomenclature of Movement Disorders A. Too Little Movement 1. Paralysis (paresis) 2. Rigidity a. spasticity (pyramidal) b. "lead pipe" (extra pyramidal) c.
Martin A. Samuels, M.D. MOVEMENT DISORDERS I. Nomenclature of Movement Disorders A. Too Little Movement 1. Paralysis (paresis) 2. Rigidity a. spasticity (pyramidal) b. "lead pipe" (extra pyramidal) c.
Motor Fluctuations in Parkinson s Disease
 Motor Fluctuations in Parkinson s Disease Saeed Bohlega, MD, FRCPC Senior Distinguished Consultant Department of Neurosciences King Faisal Specialist Hospital & Research Centre Outline Type of fluctuations
Motor Fluctuations in Parkinson s Disease Saeed Bohlega, MD, FRCPC Senior Distinguished Consultant Department of Neurosciences King Faisal Specialist Hospital & Research Centre Outline Type of fluctuations
Genetics of parkinsonian and dystonic syndromes
 Genetics of parkinsonian and dystonic syndromes Enza Maria Valente CSS-Mendel Institute, Rome University of Salerno Genetic forms of Parkinson disease 2 polymorphisms (++ in autosomal dominant PD genes:
Genetics of parkinsonian and dystonic syndromes Enza Maria Valente CSS-Mendel Institute, Rome University of Salerno Genetic forms of Parkinson disease 2 polymorphisms (++ in autosomal dominant PD genes:
Examination of lalopathy and cognitive function in Parkinson's disease-associated diseases
 Examination of lalopathy and cognitive function in Parkinson's disease-associated diseases Nana Miyata, S.T. #1, Yuri Taniguchi, S.T. #1, Kumiko Kawamichi, S.T. #1, Toshio Inui, M.D. #2, Yoshiharu Arii,
Examination of lalopathy and cognitive function in Parkinson's disease-associated diseases Nana Miyata, S.T. #1, Yuri Taniguchi, S.T. #1, Kumiko Kawamichi, S.T. #1, Toshio Inui, M.D. #2, Yoshiharu Arii,
Basal ganglia Sujata Sofat, class of 2009
 Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Form A3: Subject Family History
 Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
Index. Springer-Verlag Wien 2017 C. Falup-Pecurariu et al. (eds.), Movement Disorders Curricula, DOI /
, Movement Disorders Curricula, DOI /") A Abetalipoproteinemia (ALP), 441 Acanthocytosis ALP, 441 HDL2, 441 Acquired dystonias, 261 Action tremor, 304 ADHD. See Attention-deficit hyperactivity disorder (ADHD) Aetiological epidemiology induction
A Abetalipoproteinemia (ALP), 441 Acanthocytosis ALP, 441 HDL2, 441 Acquired dystonias, 261 Action tremor, 304 ADHD. See Attention-deficit hyperactivity disorder (ADHD) Aetiological epidemiology induction
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
Update on functional brain imaging in Movement Disorders
 Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
DOWNLOAD OR READ : ON CHOREA AND OTHER ALLIED MOVEMENT DISORDERS OF EARLY LIFE PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : ON CHOREA AND OTHER ALLIED MOVEMENT DISORDERS OF EARLY LIFE PDF EBOOK EPUB MOBI Page 1 Page 2 on chorea and other allied movement disorders of early life on chorea and other pdf on chorea
DOWNLOAD OR READ : ON CHOREA AND OTHER ALLIED MOVEMENT DISORDERS OF EARLY LIFE PDF EBOOK EPUB MOBI Page 1 Page 2 on chorea and other allied movement disorders of early life on chorea and other pdf on chorea
Proposal form for the evaluation of a genetic test for NHS Service Gene Dossier
 Proposal form for the evaluation of a genetic test for NHS Service Gene Dossier Test Disease Population Triad Disease name Parkinson disease 8, automsomal dominant OMIM number for disease 607060 Disease
Proposal form for the evaluation of a genetic test for NHS Service Gene Dossier Test Disease Population Triad Disease name Parkinson disease 8, automsomal dominant OMIM number for disease 607060 Disease
Basal ganglia motor circuit
 Parkinson s Disease Basal ganglia motor circuit 1 Direct pathway (gas pedal) 2 Indirect pathway (brake) To release or augment the tonic inhibition of GPi on thalamus Direct pathway There is a tonic inhibition
Parkinson s Disease Basal ganglia motor circuit 1 Direct pathway (gas pedal) 2 Indirect pathway (brake) To release or augment the tonic inhibition of GPi on thalamus Direct pathway There is a tonic inhibition
Rarer causes of dementia
 Rarer causes of dementia Factsheet 442LP March 2015 Alzheimer s disease is the most common cause of dementia, but there are many rarer diseases and conditions that can lead to dementia, dementialike symptoms
Rarer causes of dementia Factsheet 442LP March 2015 Alzheimer s disease is the most common cause of dementia, but there are many rarer diseases and conditions that can lead to dementia, dementialike symptoms