Navigating The Cognitive Internet: Introduction. Wendy Lemere DNP, GNP-BC Gerontological Nurse Practitioner Henry Ford Health System
|
|
|
- Philomena Welch
- 6 years ago
- Views:
Transcription
1 Navigating The Cognitive Internet: Introduction Wendy Lemere DNP, GNP-BC Gerontological Nurse Practitioner Henry Ford Health System
2 What s so hard about diagnosing dementia? Diagnosis relies on synthesis of information from many sources Time consuming Requires training / specialized skill set Multiple dementia syndromes Most dementias are mixed disorders Heterogeneity of phenotypes

3
4 Colors of the Palette History & Functional Status (aka symptoms) First symptoms, temporal evolution, functional impairments, sleep, appetite, falls etc... Medical History Cancer, autoimmune, diabetes, liver failure, medications Family History Cognitive disorders, seizures, mental retardation Cognitive Exam Deficits in memory, attention, language, visuoperceptual abilities Neurologic Exam Parkinsonism, eye movements, ataxia, dystonia Diagnostics Labs, MRI, EEG, PET,
5 Alzheimer s Disease
6 NINCDA-ARDA Criteria for AD Probable AD Dementia established by clinical examination Dementia confirmed with cognitive testing Deficits in 2 or more cognitive domains Progressive decline in memory or other areas of cognition Preserved consciousness Onset between the ages of Absence of systemic illness or other brain disease that could otherwise account for the symptoms McKhann G, Drachman D, Folstein M, et al: Clinical diagnosis of Alzheimer's disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology 1984;34:
7 AD History & Functional Status (Symptoms) Repetitions Misplacing Geographic disorientation Word Finding Delusions Ask same question, repeat same statement Lose glasses, keys, purse Lost while driving That whatchmacallit Someone stole my purse. Spouse is having an affair
8 AD History & Functional Status (Symptoms) Bill paying Forget to pay or mail bills, pay twice, can t write out checks Cooking / Appetite Leave burners on, forget well known recipes, confused with the steps of cooking, spoiled food in the refrigerator, weight loss, forgets to eat Driving Get lost, ask which way to turn Socialization Quieter in a group, wants to stay home
9 Medical History Family History By definition, medical comorbidities should not be of a sufficient magnitude to explain the dementia Increased risk with family history of A first degree relative with AD Down s syndrome
10 Cognitive Exam Memory loss Amnestic or retrieval deficit (early disease) Attention preserved or mildly reduced Visuospatial deficits proportional to memory loss Deficits in executive functioning, present but usually not prominent Planning, organizing, prioritizing, focusing attention, sustaining attention, shifting attention
11 Cerad in AD Ticket Letter Arm Grass Pole Cabin Letter Shore Engine Butter Trial 1: 2 Trial 2: 3 Trial 3: 3 Free recall: 0 Recognition: 2 Targets 10 Foils ************************ Fruits & vegetables: 6 Letter F: 8
12 AD Neuro Exam No focal abnormalities Absence of parkinsonism
13 Diagnostics MRI Temporal lobe atrophy EEG PET/SPECT Lumbar puncture Independent bitemporal slow waves. Absence of seizures. Hypometabolism in bilateral temporal/parietal lobes Tau/a-beta ratio Useful biomarker
14 Lewy Body Disease Chronic delirium
15 LBD History & Functional Status (Symptoms) Visual hallucinations Visual perceptual deficits Fluctuations Milder memory problems REM sleep disorder Word finding Delusions See animals, little people Scrape the car when backing out, can t stay in lane, Fine one moment/ bad the next. Fluctuations scale Forget why they went into a different room Kick & punch the bed, dreams seem real, walk or talk in sleep Search for word, hesitancies Complex, stereotyped
16 Medical History Autonomic Dysfunction: Supportive Feature Postural hypotension Syncope Arrythmias Temperature dysregulation There should be no other medical condition that in and of itself could explain the patient s symptoms
17 Family History Patient s with LBD have an increased incidence of a family history of dementia compared to normal controls
18 Cognitive Exam Poor attention (digits forward, digits backwards) Disproportionate deficits in executive functioning (poor letter fluency, clock drawing) Visuospatial deficits out of proportion to memory impairment
19 Cerad LBD Ticket Letter Arm Grass Pole Cabin Letter Shore Engine Butter Trial 1: 2 Trial 2: 5 Trial 3: 7 Free recall: 3 Recognition: 10 Targets 9 Foils ************************ Fruits & vegetables: 13 Letter F: 4
20 House Drawing
21 Simple Figures

22 Boston Naming Test
23 Comparison of AD to LBD Flat learning Amnestic or retrieval deficit Fairly well preserved attention Poor category fluency Anomia Visuospatial deficits in keeping with memory impairment Learning curve Retrieval or source memory deficit Poor attention Poor letter fluency Visual errors with confrontational naming Visuospatial deficits out of proportion to memory impairment
24 LBD Neuro Exam Parkinsonism Increased tone, gait changes, decreased facial expression, rest tremor, bradykinesia, bradyphrenia, hypophonia, hypoknietic dysarthria
25 Diagnostics MRI Possibly parietal/occipital atrophy EEG PET/SPECT FIRDA Parietal/occipital hypometabolism
26 Lewy Body Disease Criteria Core clinical features Fluctuating cognition with pronounced variations in alertness and attention daytime sleep greater than 2 hours, daytime lethargy, disorganized speech, staring spells Recurrent visual hallucinations that are well formed and detailed Spontaneous features of parkinsonism not solely due to medications Probable LBD: 2 or more core features Possible LBD: 1 core feature
27 Lewy Body Disease Criteria Supportive Features Repeated falls Syncope / autonomic dysfunction Neuroleptic sensitivity Complex systematized delusions Hallucinations in other modalities REM sleep disorder
28 Frontotemporal Dementia Behavior variant (bvftd) Semantic dementia (SD) Progressive nonfluent aphasia (PNFA)

29 MRI Frontal Atrophy
30 bvftd Symptoms Change in personality or behavior Compulsions Executive dysfunction Food /Eating Language impairment (less prominent than personality changes) Disinhibited Restlessness, wandering, inappropriateness, increased jocularity, sexual inappropriateness, drinking, childlike behavior, lack of empathy, remorse Apathetic Depressed, lack motivation, hypersomnolent Hyper-religiousity, gambling, pornography, purchasing multiples Perseverations, inattention, utilization behavior Gluttony, unusual food cravings, cramming food, non-edible food Word retrieval
31 Progressive nonfluent aphasia Nonfluent speech output Agrammatism Telegraphic speech Phonemic paraphasias & anomia Single word comprehension good. May have comprehension problems for complex sentences Early behavior & personality changes less common Extrapyramidal features, behavioral problems, and executive dysfunction later
32 Semantic dementia Loss of word & object knowledge Sentences of normal length (>7 words /utterance), but they don t make sense Poor comprehension at the single word level Can t recognize faces Prosopagnosia (more common with greater L temporal lobe atrophy Behavior changes (R temporal lobe atrophy)

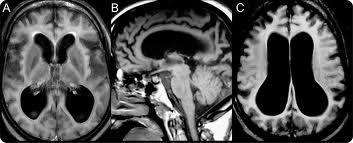
33 Normal Pressure Hydrocephalus
34
35 Ventriculomegaly Idiopathic Normal Pressure Hydrocephalus Secondary Hydrocephalus Brain surgery Infection Medical Conditions Sleep apnea Diabetes Atrophy
36 NPH Cardinal Symptoms Problems with walking and falls Bladder incontinence Memory loss Diagnostic Challenge Who will benefit from treatment Treatment Surgical
37 Corticobasal Degeneration Core features Insidious and progressive Cortical Dysfunction AEB at least one Focal or asymmetric ideomotor apraxia Alien limb Cortical sensory loss Visual or hemisensory neglect Constructional apraxia Focal or asymmetric myoclonus Apraxia of speech/non-fluent aphasia Extrapyramidal dysfunction Focal or asymmetric appendicular rigidity Focal or asymmetric appendicular dystonia
38 Mixed Neuropathology 141 community dwelling participants. Annual clinical exams and brain donation. Examined brains for neuropathology of cerebral infarctions, AD, and PD/LBD. In persons with dementia 30% had pure AD 38% had AD & infarcts 12% Vascular demetnia 12% AD & PD/LBD In person without dementia 28.6% no diagnostic abnormalities 24.2% had pure AD 17.6% brain infarctions Persons with multiple diagnoses were nearly 3 times more likely to exhibit dementia compared to those with only one pathologic process Schneider, J.A., Arvanitakis, Z., Bang, W., & Bennett, D.A. (2007). Mixed brain pathologies account for most dementia cases in communitydwelling older persons. Neurology, 69,
39 The National Alzheimer s Coordinating Center (NACC) Department of Epidemiology, School of Public Health, University of Washington, Seattle, WA Kukull, W., Phillips, L., Gill, D.,Chen, B., Wu, J., Beekly, D., Koepsell, T NACC database from >30 ADRC from autopsies

40 Normal AD LBD n=351 n=5679 n=1195 Plaques &T 14% 97% 70% Lewy bodies 5% 21% 97% Large stroke 10% 12% 8% Micro stroke 18% 18% 13% ASVD 18% 36% 30%


41 FTD VaD All n=609 n=308 n=8142 Plaques &T 26% 42% 80% Lewy bodies 8% 5% mixed Large stroke 5% 31% path Micro stroke 10% 42% ASVD 18% 58%
42 Heterogeneity of Expression Adapted from McMonagle, P., & Kertesz, A. Cognition in corticobasal degeneration and progressive supranuclear palsy. In B.L. Miller & B.F. Boeve (Eds.), The behavioral neurology of dementia. (pp ). Cambridge: Cambridge University Press. 1st bv FTD n=15 2nd CBDS n=5 2nd PPA n=10 3rd PPA n=5 3rd CBDS n=10 Path CBD (2) GSS Path CBD (2) PiD MNDI
43 Gold Standard Clinical Diagnosis? Genetic characterization? Neuropathology?
I do not have any disclosures
 Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
2016 Programs & Information
 Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
FTD basics! Etienne de Villers-Sidani, MD!
 FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Objectives. RAIN Difficult Diagnosis 2014: A 75 year old woman with falls. Case History: First visit. Case History: First Visit
 Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
Prof Tim Anderson. Neurologist University of Otago Christchurch
 Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Patterns of Cognitive Impairment in Dementia
 Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia
 Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
What is dementia? Symptoms of dementia. Memory problems
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Differentiating Dementia Diagnoses
 Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Introduction to Dementia: Diagnosis & Evaluation. Created in March 2005 Duration: about 15 minutes
 Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
Overview of the non-alzheimer Dementias
 Overview of the non-alzheimer Dementias Chiadi U. Onyike, MD, MHS FTD/Young-Onset Dementias Program Johns Hopkins Neuropsychiatry Disclaimer Dr. Onyike is a principal investigator for the Baltimore site
Overview of the non-alzheimer Dementias Chiadi U. Onyike, MD, MHS FTD/Young-Onset Dementias Program Johns Hopkins Neuropsychiatry Disclaimer Dr. Onyike is a principal investigator for the Baltimore site
Introduction, use of imaging and current guidelines. John O Brien Professor of Old Age Psychiatry University of Cambridge
 Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer
 The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
DEMENTIA ANDREA BERG, MD
 DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
02/04/2015. The structure of the talk. Dementia as a motor disorder. Movement, cognition & behaviour. Example 1. Example 2
 The th Annual Memory Clinic Conference Dublin, Trinity College, 27 March 1 The structure of the talk Dementia as a motor disorder Thomas H. Bak Human Cognitive Neuroscience & Centre for Clinical Brain
The th Annual Memory Clinic Conference Dublin, Trinity College, 27 March 1 The structure of the talk Dementia as a motor disorder Thomas H. Bak Human Cognitive Neuroscience & Centre for Clinical Brain
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Frontotemporal Dementia: Towards better diagnosis. Frontotemporal Dementia. John Hodges, NeuRA & University of New South Wales, Sydney.
 I.1 I.2 II.1 II.2 II.3 II.4 II.5 II.6 III.1 III.2 III.3 III.4 III.5 III.6 III.7 III.8 III.9 III.10 III.11 III.12 IV.1 IV.2 IV.3 IV.4 IV.5 Frontotemporal Dementia: Towards better diagnosis Frontotemporal
I.1 I.2 II.1 II.2 II.3 II.4 II.5 II.6 III.1 III.2 III.3 III.4 III.5 III.6 III.7 III.8 III.9 III.10 III.11 III.12 IV.1 IV.2 IV.3 IV.4 IV.5 Frontotemporal Dementia: Towards better diagnosis Frontotemporal
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
DEMENTIA 9/29/16. Introduction. Introduction. Signs and Symptom. Epidemiology. Dementia. Dr. Yotin Chinvarun M.D. Ph.D.
 Introduction DEMENTIA Dr. Yotin Chinvarun M.D. Ph.D. Neurology, Pramongkutklao hospital In 1901 Auguste Deter, a woman in her early 50s, became 1 st person diagnosed with Alzheimer's disease, a form of
Introduction DEMENTIA Dr. Yotin Chinvarun M.D. Ph.D. Neurology, Pramongkutklao hospital In 1901 Auguste Deter, a woman in her early 50s, became 1 st person diagnosed with Alzheimer's disease, a form of
UDS version 3 Summary of major changes to UDS form packets
 UDS version 3 Summary of major changes to UDS form packets from version 2 to VERSION 3 february 18 final Form A1: Subject demographics Updated question on principal referral source to add additional options
UDS version 3 Summary of major changes to UDS form packets from version 2 to VERSION 3 february 18 final Form A1: Subject demographics Updated question on principal referral source to add additional options
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia
 Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia Bradley F. Boeve, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Alzheimer s Disease
Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia Bradley F. Boeve, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Alzheimer s Disease
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Revised criteria for the clinical diagnosis of dementia with Lewy. Dementia with Lewy bodies. (Dementia with Lewy Bodies)
") Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Dementia. Dr Maria Foundas Consultant Physician. Training support Skills development Competency Assessment Scholarships Education
 Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
For carers and relatives of people with frontotemporal dementia and semantic dementia. Newsletter
 For carers and relatives of people with frontotemporal dementia and semantic dementia Newsletter AUGUST 2008 1 Welcome Welcome to the August edition of our CFU Support Group Newsletter. Thanks to all of
For carers and relatives of people with frontotemporal dementia and semantic dementia Newsletter AUGUST 2008 1 Welcome Welcome to the August edition of our CFU Support Group Newsletter. Thanks to all of
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
NCFE Level 2 Certificate in The Principles of Dementia Care
 The Principles of Dementia Care S A M P LE NCFE Level 2 Certificate in The Principles of Dementia Care Part A 1 These learning resources and assessment questions have been approved and endorsed by ncfe
The Principles of Dementia Care S A M P LE NCFE Level 2 Certificate in The Principles of Dementia Care Part A 1 These learning resources and assessment questions have been approved and endorsed by ncfe
Frontal Behavioural Inventory (FBI)
") This is a Sample version of the Frontal Behavioural Inventory (FBI) The full version of the Frontal Behavioural Inventory (FBI) comes without sample watermark. The full complete version includes Complete
This is a Sample version of the Frontal Behavioural Inventory (FBI) The full version of the Frontal Behavioural Inventory (FBI) comes without sample watermark. The full complete version includes Complete
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Dementia. Amber Eker, MD. Assistant Professor Near East University Department of Neurology
 Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss
 Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss Incidence of Common Neurological Diseases Incidence New Cases Disease (per 100,000) (per
Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss Incidence of Common Neurological Diseases Incidence New Cases Disease (per 100,000) (per
Evolution of a concept: Apraxia/higher level gait disorder. ataxia v. apraxia gait = limb apraxia. low, middle, high gait disturbance levels
 Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Enhanced Primary Care Pathway: Parkinson s Disease
 Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
What Difference Does it Make what Kind of Dementia it is? Strategies for Care
 What Difference Does it Make what Kind of Dementia it is? Strategies for Care Sandra Petersen, DNP, APRN, FNP-BC, GNP-C, PMHNP-BE, FAANP E-mail: spetersen@uttyler.edu What is dementia? Umbrella term Used
What Difference Does it Make what Kind of Dementia it is? Strategies for Care Sandra Petersen, DNP, APRN, FNP-BC, GNP-C, PMHNP-BE, FAANP E-mail: spetersen@uttyler.edu What is dementia? Umbrella term Used
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Non-Motor Symptoms of Parkinson s Disease
 Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Presenter Disclosure Information. I have no financial relationships to disclose:
 Sandra Weintraub, Ph.D. Cognitive Neurology and Alzheimer s Disease Center Northwestern University, Feinberg School of Medicine Chicago, Illinois http://www.brain.northwestern.edu/dementia/ppa/index.html
Sandra Weintraub, Ph.D. Cognitive Neurology and Alzheimer s Disease Center Northwestern University, Feinberg School of Medicine Chicago, Illinois http://www.brain.northwestern.edu/dementia/ppa/index.html
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Resources: Types of dementia
 1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
FTD/PPA Caregiver Education Conference March 11, 2011
 FTD/PPA Caregiver Education Conference March 11, 2011 Question and Answer Session Answered by Joseph Cooper, MD, Darby Morhardt, MSW, LCSW, Mary O Hara, AM, LCSW, Jaimie Robinson, MSW, LCSW, Emily Rogalski,
FTD/PPA Caregiver Education Conference March 11, 2011 Question and Answer Session Answered by Joseph Cooper, MD, Darby Morhardt, MSW, LCSW, Mary O Hara, AM, LCSW, Jaimie Robinson, MSW, LCSW, Emily Rogalski,
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
EARLY ONSET FRONTOTERMPORAL DEMENTIA AND ALZHEIMERS DISEASE: DIAGNOSIS, TREATMENT AND CARE
 EARLY ONSET FRONTOTERMPORAL DEMENTIA AND ALZHEIMERS DISEASE: DIAGNOSIS, TREATMENT AND CARE John Rudge, BA Hons This thesis is presented as partial requirement for the degree of Doctor of Psychology at
EARLY ONSET FRONTOTERMPORAL DEMENTIA AND ALZHEIMERS DISEASE: DIAGNOSIS, TREATMENT AND CARE John Rudge, BA Hons This thesis is presented as partial requirement for the degree of Doctor of Psychology at
Dementia. Team Members: Abdulaziz Alsalem, Khalid Al-Qahtani, Dania Alkelabi, Sarah Alshamrani
 Dementia Objectives: differentiate delirium from dementia differentiate Mild Cognitive Impairment from Dementia become familiar with common dementia syndromes, and available treatments Team Members: Abdulaziz
Dementia Objectives: differentiate delirium from dementia differentiate Mild Cognitive Impairment from Dementia become familiar with common dementia syndromes, and available treatments Team Members: Abdulaziz
Title: Clinical and neuropathologic variation in neuronal intermediate filament inclusion disease (NIFID)
") Neurology/2004/048785 Title: Clinical and neuropathologic variation in neuronal intermediate filament inclusion disease (NIFID) Correspondence to: Nigel J. Cairns PhD MRCPath Center for Neurodegenerative
Neurology/2004/048785 Title: Clinical and neuropathologic variation in neuronal intermediate filament inclusion disease (NIFID) Correspondence to: Nigel J. Cairns PhD MRCPath Center for Neurodegenerative
LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION
 LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION Murray Grossman University of Pennsylvania Support from NIH (AG17586, AG15116, NS44266, NS35867, AG32953, AG38490), IARPA, ALS Association, and the
LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION Murray Grossman University of Pennsylvania Support from NIH (AG17586, AG15116, NS44266, NS35867, AG32953, AG38490), IARPA, ALS Association, and the
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES
 WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Objectives. Overview. Why FTD and AD? FTD May Mimic AD. Introduction and Process Norman L. Foster, MD. Introduction and Process 7BS.
 Introduction and Process Norman L. Foster, MD 7BS.006 IMPROVING ACCURACY OF DEMENTIA DIAGNOSIS: CASE STUDIES WITH NEUROPATHOLOGY Norman L. Foster, MD University of Utah Salt Lake City, UT Edward Zamrini,
Introduction and Process Norman L. Foster, MD 7BS.006 IMPROVING ACCURACY OF DEMENTIA DIAGNOSIS: CASE STUDIES WITH NEUROPATHOLOGY Norman L. Foster, MD University of Utah Salt Lake City, UT Edward Zamrini,
NACC Minimum Data Set (MDS) Public Data Element Dictionary
 Public Data Element Dictionary") Department of Epidemiology, School of Public Health and Community Medicine, University of Washington 4311 11 th Avenue NE #300 Seattle, WA 98105 phone: (206) 543-8637; fax: (206) 616-5927 e-mail: naccmail@u.washington.edu
Department of Epidemiology, School of Public Health and Community Medicine, University of Washington 4311 11 th Avenue NE #300 Seattle, WA 98105 phone: (206) 543-8637; fax: (206) 616-5927 e-mail: naccmail@u.washington.edu
Biomarkers: Translating Research into Clinical Practice
 Biomarkers: Translating Research into Clinical Practice AFTD Education Conference San Diego, April 2015 Nadine Tatton, PhD Scientific Director, AFTD HelpLine 866-5507-7222 u info@theaftd.org u www.theaftd.org
Biomarkers: Translating Research into Clinical Practice AFTD Education Conference San Diego, April 2015 Nadine Tatton, PhD Scientific Director, AFTD HelpLine 866-5507-7222 u info@theaftd.org u www.theaftd.org
Do not copy or distribute without permission. S. Weintraub, CNADC, NUFSM, 2009
 Sandra Weintraub, Ph.D. Clinical Core Director, Cognitive Neurology and Alzheimer s Disease Center Northwestern University Feinberg School of Medicine Chicago, Illinois Dementia: a condition caused by
Sandra Weintraub, Ph.D. Clinical Core Director, Cognitive Neurology and Alzheimer s Disease Center Northwestern University Feinberg School of Medicine Chicago, Illinois Dementia: a condition caused by
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Dementia is not normal aging!
 The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Evaluation and Treatment of Dementia
 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
What is frontotemporal dementia?
 What is frontotemporal dementia? Introduction Information in this introductory booklet is for anyone who wants to know more about frontotemporal dementia (FTD). This includes people living with FTD, their
What is frontotemporal dementia? Introduction Information in this introductory booklet is for anyone who wants to know more about frontotemporal dementia (FTD). This includes people living with FTD, their
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Diagnosing & Dealing with Dementia
 Diagnosing & Dealing with Dementia Robert G. Arias, PhD. I have no financial disclosures or conflicts of interest to report. Robert G. Arias, PhD. 1 Today We Will Learn About: Diagnosing dementia Characteristics
Diagnosing & Dealing with Dementia Robert G. Arias, PhD. I have no financial disclosures or conflicts of interest to report. Robert G. Arias, PhD. 1 Today We Will Learn About: Diagnosing dementia Characteristics
Research on Primary Progressive Aphasia: What It Is Teaching Us About Brain Function and Progression
 Research on Primary Progressive Aphasia: What It Is Teaching Us About Brain Function and Progression Sandra Weintraub, PhD Clinical Core Leader and Professor Northwestern Cognitive Neurology and Alzheimer
Research on Primary Progressive Aphasia: What It Is Teaching Us About Brain Function and Progression Sandra Weintraub, PhD Clinical Core Leader and Professor Northwestern Cognitive Neurology and Alzheimer
The progression of dementia
 PBO 930022142 NPO 049-191 The progression of dementia Although everyone experiences dementia in their own individual way, it can be helpful to think of the progression of dementia as a series of stages.
PBO 930022142 NPO 049-191 The progression of dementia Although everyone experiences dementia in their own individual way, it can be helpful to think of the progression of dementia as a series of stages.
10/17/2017. Causes of Dementia Alzheimer's Disease Vascular Dementia Diffuse Lewy Body Disease Alcoholic Dementia Fronto-Temporal Dementia Others
 1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
1 Dementia Dementia comes from the Latin word demens, meaning out of mind. It is the permanent loss of multiple intellectual functions. It is progressive deterioration of mental powers accompanied by changes
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Dementia the A,B,Cs. Dr. Frank Molnar. Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital
 Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)