Interdisciplinary detection of potential drug related problems in older people
|
|
|
- Cathleen Ball
- 6 years ago
- Views:
Transcription

1 Interdisciplinary detection of potential drug related problems in older people Prof. dr. Mirko Petrovic Department of Internal Medicine, Ghent University Department of Geriatrics, Ghent University Hospital, Ghent, Belgium GERIZOL, Genk, 14 October
2 Factors for ADRs in older people PHARMACOKINETICS PHARMACODYNAMICS PATIENT COMPLIANCE SKILLS ADR POLYPATHOLOGY POLYPHARMACY PRESCRIPTION MONITORING Most important factor for ADRs is the number of prescribed drugs. J Am Geriatr Soc 1996;44:194-7
3 Features of polypharmacy Medication not indicated Duplicate medications Concurrent interacting medications Contraindicated medications Inappropriate dosage Drug treatment of adverse drug reaction Improvement following discontinuance
4 Structure How should we identify subjects at risk of drug related problems (DRPs) and adverse drug reactions (ADRs)? How should we review prescribing for an older patient? Which tools and strategies can help us to reduce DRPs and ADRs? 4
5 Approaches to screen and prevent the occurrence of DRPs and ADRs Screening- identification of subjects at risk of ADR Medication review Avoiding use op potentially inappropriate medications (PIM) Computer-based prescribing systems Comprehensive geriatric assessment (CGA)
6 Case of Mrs. M. Mrs. M is an 81 years old widow, living alone in her own house. She suffers from diabetes mellitus, hypertension, ischemic heart disease, glaucoma, osteoarthritis and osteoporosis. Her weight is 46 kg and she is 160 cm tall. Because of osteoarthritis she reports slowness and reduced level of physical activity. She is currently on the following drugs: Atenolol 50 mg/day, Perindopril 5 mg/day, Pantoprazole 20 mg/day, Metformin 1000 mg/day, Hydrochlorothiazide 12.5 mg/day, Timolol eye drops (0.5%, twice daily in both eyes), ASA 100 mg/day, Diazepam 5 mg/day. Her blood pressure is 152/88 mmhg and her last HbA1c was 8.2%.
7 Variables of the GerontoNet ADR risk score Odds Ratio 95% CI Points 4 co-morbid conditions Heart failure Liver disease* No of drugs, < Previous ADR Renal failure** *transaminases > 2 x upper normal limit; ** GFR < 60 ml/min
8 Brighton Adverse Drug Reactions Risk (BADRI) Model Odds Ratio 95% CI Hyperlipidemia No of drugs Length of stay 12 days Use of anti-diabetic agents High WCC on admission Tangiisuran B et al. PLos ONE 2014; 9: e111254
9 MRS. M GerontoNet ADR risk score Mrs. M presents with multiple risk factors for ADR, including co-morbidity and polypharmacy. She screened positive on the risk of ADR based on the GerontoNet ADR risk score (score=5; 4 co-morbid conditions: 1 point and 8 drugs: 4 points), suggesting a high risk for ADR and the need for an intervention to prevent the risk of ADR.
10 Medication review An individualized assessment provided by a clinical pharmacist: during which the medication list is analyzed in a structured manner, with full access to the medical file, in order to identify drug related problems. First step: identification of all the medications that the patient is taking. Second step: the medication list is screened for drug related problems i.e. any misuse, underuse or overuse of drugs. Third step: possible solutions to the drug related problems (DRPs) are then discussed with the treating physician and, if possible, with the patient.
11 Medication review Level 3 CLINICAL MEDICATION REVIEW Level 2 TREATMENT REVIEW Face-to-face review of medicines and condition Level 1 PRESCRIPTION REVIEW Review of medicines with full patient s notes Level 0 AD-HOC Unstructured, opportunistic Technical review of list of patient s medicines
12 Reporting adverse drug reactions on a geriatric ward: spontaneous reporting vs. patient interview spontaneous reporting Patients Patients with ADRs Number of ADRs patient interview Interviewed patients (n = 56) Mean Median Range Age (years) Length of stay (days) Number of drugs patients with ADR (n=23) patients without ADR (n=33) Somers A et al. Eur Clin Pharmacol 2003;58:707-14
13 Reporting adverse drug reactions on a geriatric ward: spontaneous reporting vs. patient interview Results of the patient interview Gender Male 10 (43%) Female 13 (57%) Causality Probable 23 (72%) Possible 9 (28%) Level 1 = no change 13 (41%) 2 = stopped / dose changed 12 (37%) 3 = stopped + additional therapy 7 (22%) Severity Serious ADR 12 (38%) Non-serious ADR 20 (62%) Type Type A 32 (100%) Type B 0 (0%) Somers A et al. Eur Clin Pharmacol 2003;58:707-14

14 Impact on appropriateness of prescribing RCT, 203 patients, one acute geriatric unit, Belgium Pharmaceutical care from admission to discharge - appropriateness of prescribing (MAI, ACOVE) - 90% acceptance rate - Trend towards mortality and ED visits Spinewine A et al. J Amer Geriatr Soc 2007; 55: RCT, 400 patients 80y, 2 internal medicine wards, Sweden Pharmaceutical care from admission to discharge(+ after) - 16% hospital visits - 46% ED visits - 80% drug-related readmissions Gillespie U et al. Arch Intern Med 2009;169:

15 Impact on appropriateness of prescribing Spinewine et al. Lancet 2007;370:
16 Medication review: evidence Good evidence that collaboration with pharmacists can decrease the risk of drugrelated problems Mixed / lacking evidence for effect on: Health outcomes HR QoL Cost-effectiveness of care Chisholm-Burns Med Care. 2010;48: Spinewine et al. Drugs Aging. 2012;29:
17 Mrs. M Medication review 1. Structured pharmaceutical anamnesis: information of the GP and the community pharmacist is gathered. Specific questions on use of drugs easily forgotten (such as sleeping pills, inhaled drugs, over-the-counter drugs and supplements and drugs on an as needed basis) and on time and mode of administration are asked. 2. Structured screening for drug related problems (DRPs): drugs are assessed for indication, correct dose, choice of the appropriate treatment, frequency and time of intake. Drug-drug interactions, presence of ADRs and under prescribing are also assessed.
18 Mrs. M Medication review Potential DRPs related to the case of Mrs M are the following: Perindopril, hydrochlorothiazide, and metformin: are doses adjusted for renal function? Metformine: the HbA1C-level is not satisfactory and attempts should be made to improve glucose control, but with due regard to avoiding hypoglycaemic episodes. Diazepam: inappropriate in older adults because of increased risk of falls Calcium/vitamin D and bisphosphonate may be necessary given the diagnosis of osteoporosis Pantoprazole: no clear indication Atenolol: not the best choice for the treatment of hypertension Timolol: combined use of timolol and atenolol can increase the risk of symptomatic bradycardia and falls 3. This list is then discussed with the treating physician and a plan for implementation and evaluation is created.
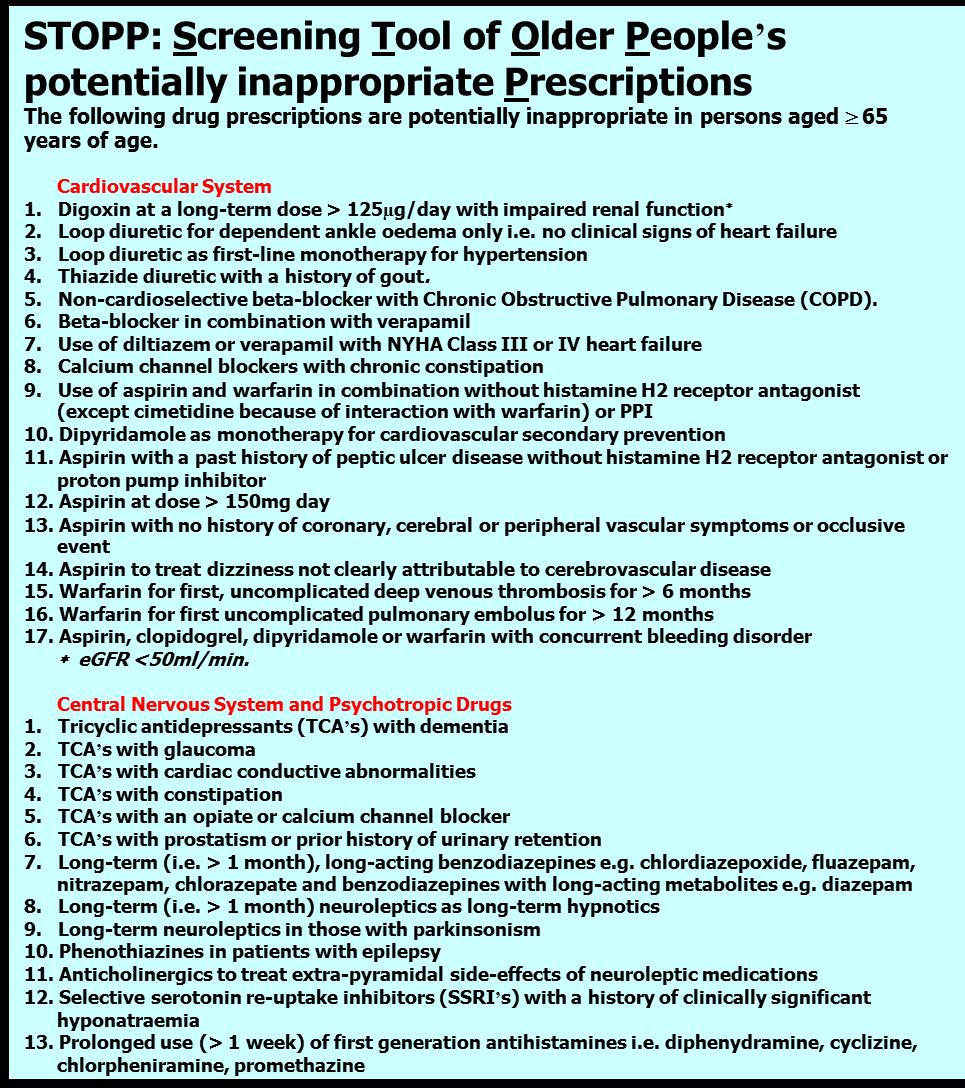
19 Avoiding use of potentially inappropriate medications (PIM) Medication Assessment Tools 1) Explicit (criteria based): drugs to avoid Beers (1991, updates 1997, 2003, 2012, 2015) McLeod (1997) ACOVE: Assessing Care of Vulnerable Elders (2001) IPET: Improved Prescribing in the Elderly Tool (2002) STOPP: Screening Tool of Older Person s Prescriptions/ START: Screening Tool to Alert doctors to Right Treatment) (2008, update 2015) 2) Implicit (judgement based): MAI: Medication Appropriateness Index (1992) GMA: Geriatric Medication Algorithm (1994) Lipton s criteria (1993)
20

21 Courtesy: Prof. B. Boland, Univ. Louvain
22 Older patients with polypharmacy 1. Systematic Review 2. Development of GheOP³S-tool 3. Validation of GheOP³S-tool 4. Observational research in communitydwelling older patients 5. Observational research in nursing home residents STEP 1 Literature search STEP 2 Selection of clinical relevant items for primary care STEP 3 Selection of feasible items for community pharmacy practice GheOP³S-tool Ghent Older People Prescriptions community Pharmacy Screening Tool 83 items / 5 parts
23 Explicit instruments Pros of using explicit criteria in our daily practice Relatively easy to remember and to detect Provide support to identify inappropriate prescribing in older people HOWEVER 23
24 Explicit instruments Cons of using explicit criteria in daily practice This is just one part of the story The patient s perspective is often not taken into consideration We should not limit our evaluation to the application of such criteria 24
25 Medication Appropriateness Index (MAI) 10 questions per drug 1. Valid indication? 2. Appropriate choice? 3. Correct dose? 4. Modalities of treatment correct? 5. Modalities of treatment practical? 6. Clinically significant drug-drug interactions? 7. Clinically significant drug-disease interactions? 8. Duplication? 9. Appropriate duration? 10.Cost? Hanlon et al. Am J Med 1996;100:
26 Original MAI index Adapted MAI index Question per drug Weight Question per drug Weight 1. Indication 3 2. Effectiveness 3 3. Dosage 2 4. Correct directions 2 5. Practical directions 1 6. Drug drug interactions 2 7. Drug disease interactions 2 8. Duplication 1 9. Duration 1 1. Indication 3 2. Right choice 3 3. Dosage 2 4. Directions 1 5. Drug drug interactions 2 6. Drug disease interactions 7. Duration 1 8. Adverse drug reactions Expense 1 Somers A et al. Am J Geriatr Pharmacother. 2012;10:
27 Implicit intruments Time consuming Knowledge-dependent Comprehensive and systematic Includes operational definitions, explicit instructions, and examples Excellent as an educational «tool» for students! Hanlon et al. Am J Med 1996;100:
28 Mrs. M Avoiding use of PIM Beers and START and STOPP criteria identified the following concerns about Mrs. M treatment: Beers 2012 criteria Diazepam: increase risk of cognitive impairment, delirium, falls, fractures, and motor vehicle accidents STOPP Diazepam: risk of prolonged sedation, confusion, impaired balance, falls. Atenolol: risk of masking hypoglycemic symptoms Pantoprazole: if full therapeutic dosage for > 8 weeks (dose reduction or earlier discontinuation indicated) START Statin therapy with a documented history of coronary, cerebral or peripheral vascular disease, where the patient s functional status remains independent for activities of daily living and life expectancy is greater than 5 years Calcium and vitamin D supplement in patients with known osteoporosis
29 Computer-based prescribing systems Clinical Decisions Support Systems (CDSS) and Computerized Prescription Support System (CPSS) are interactive softwares, designed As potentially powerful tools to prevent ADRs To support at the time of prescribing All categories of inappropriate prescribing can be addressed, if prescription data are linked to clinical data Computerized Provider Order Entry Systems (CPOE), which are based on these softwares, enable providers to enter medical orders into a computer system that is located within an inpatient or ambulatory setting. Schiff G et al. JAMA 1998; 279:
30 Complexity Translating Quality Measures into Clinical Decision Support Drugs, Dx s, Labs & Clinical Info Drugs, Dx s & Labs Drug Data Drugs & Dx s Validity
31 Computer-based prescribing Disadvantages systems Very few studies demonstrated an improvement in patient outcomes Challenging to implement Existing systems are not geriatric specific High volume of alerts: risk of unimportant warnings Some prescribers are reluctant to use Gurwitz J et al. J Am Geriatr Soc 2008; 56: Wolfstadt J et al. J Gen Inten Med 2008;23: Strom B et al; Arch Intern Med. 2010;170:
32 Mrs. M Computer-based prescribing systems The following warning messages are taken from the CPSS developed by the Istituto di Ricerche Farmacologiche Mario Negri, Milan, Italy Drug interactions: 1) Pantoprazole- Hydrochlorothiazide (moderate risk): increased risk of hypomagnesaemia in case of prolonged use of PPI 2) Perindopril- Hydrochlorothiazide (moderate risk): increased risk of hypotension at the first dose 3) Metformin- Atenolol (moderate): risk of masking hypoglycemic symptoms Inappropriate drug use: Diazepam (Beers 2003, Beers 2012, STOPP): risk of prolonged sedation, confusion, impaired balance, falls Atenolol (STOPP): risk of masking hypoglycemic symptoms Pantoprazole (STOPP): if full therapeutic dosage for > 8 weeks (dose reduction or earlier discontinuation indicated)
33 Mrs. M Computer-based prescribing systems Underuse of drugs: Statin (START): statin therapy is indicated with a documented history of coronary, cerebral or peripheral vascular disease, where the patient s functional status remains independent for activities of daily living and life expectancy is greater than 5 years Calcium and vitamin D (START): Calcium and vitamin D supplement in patients with known osteoporosis Anticholinergic Cognitive Burden (ACB scale): Atenolol=1; Diazepam=1 Total score = 2 - moderate anticholinergic effect
34 Mrs. M Computer-based prescribing systems Dose: The following drugs need dose adjustment based on creatinine clearance: Perindopril, Atenolol, Metformin, Hydrochlorothiazide GerontoNet GerontoNet ADR risk score 4, suggesting a high risk for ADR.
35 Comprehensive geriatric assessment (CGA) Medical complexity plays an important role in the onset of ADR and should always be considered before prescribing a pharmacological treatment in older people. Drugs which use is indicated in clinical guidelines should be used carefully in complex older adults since they may interact with co-existing diseases or geriatric syndromes, not be assumed correctly because of presence of cognitive deficits, disability or social problems or be useless because the health expectancy of the patient is too short to determine a beneficial effect of the drug. Tinetti M et al. N Engl J Med 2004; 351:
36 Comprehensive geriatric assessment (CGA): evidence CGA allows a complete and global assessment and management of the health care problems, including evaluation of drugs with the goal of recognizing and preventing potential drug-related problems and improve quality of prescribing. Onder G et al. Curr Drug Metab 2011; 12: CGA associated with a multidisciplinary team approach, as compared with usual care in frail older adults shows a 35% reduction in the risk of a serious ADRs and a substantial reduction in unnecessary and inappropriate drug use. Schmader K et al. Am J Med. 2004; 116:
37 Mrs. M Comprehensive geriatric assessment the CGA identifies several problematic areas of Mrs. M which may limit the use of drugs: Malnutrition The use of multiple drugs may impair appetite and reduce food intake. In particular metformin may cause anorexia and weight loss. Mrs. M is underweight (BMI < 18 kg/m2) and for this reason treatment with metformin should be reconsidered and opportunity to reduce in the overall number of drugs should be evaluated. Social problems and frailty Lack of social support and frailty may suggest potential difficulties in managing complex drug regimens and possible problems in drug adherence. In particular, applying a tight blood pressure and glycaemic control to Mrs. M may be problematic because of potential medication errors and severity and consequences of ADR may be accentuated by these factors.
38 Mrs. M Comprehensive geriatric assessment Falls Mrs. M presents several risk factors for falls, including polypharmacy, use of benzodiazepines and diuretics and functional limitations (slowness). Therefore the CGA identifies her as a person at high risk for fall. This suggests the need to reduce the number of used drugs and withdrawal from the use of benzodiazepines and diuretics. Vitamin D supplementation may be considered given its positive effects on osteoporosis and falls and its safe profile. Limited life expectancy given the presence of the malnutrition, frailty, co-morbidities and advanced age, life expectancy of Mrs. M might not be long enough to get benefit from intensive drug treatment. For example, tight glycaemic control may be unrewarding if life expectancy < 5 years.
39 THM: Conclusions None of the existing approaches shows a clear beneficial effect on patients health outcomes: available evidence on the impact of medication review, avoidance of PIM, computer-based prescribing systems and CGA is mixed and controversial. A main limitation of all the described approaches is the lack of standardization. Large differences are described in the delivery of the pharmacist-led medication review. Criteria to assess quality of prescribing vary across countries and no widely accepted gold standard exists, yet. Computer-based prescribing systems are often home-grown and they implement different types of information, tools and algorithms. Geriatric assessment and management programs are heterogeneous in terms of structural components and care processes.
40 THM: Conclusions (cont.) Most of the available research is focused on a single intervention targeting either clinical or pharmacological factors causing ADR. When these approaches were combined- as for studies assessing the efficacy of an intervention based on experienced pharmacists performing medication review in the context of a multidisciplinary team- positive effects on patients health outcomes were shown. Safe drug use goes along with global assessment of patients clinical and functional parameters and that integration of skills from different health care professionals is needed to address medical complexity of older adults. The challenge for future research is to integrate valuable information obtained by existing instruments and methodologies in a complete and global approach targeting all potential factors involved in the onset of ADR.
41 COLLABORATIVE CARE Multidisciplinary teams Geriatric medicine services/cga Collaboration with General practitioners Clinical pharmacists Nurses Collaboration with the patient Computerized support Educational approaches 42


42 Development and clinical trials of a new Software ENgine for the Assessment & Optimization of drug and non-drug Therapy in Older persons
Stronger together - optimizing pharmacotherapy on geriatric wards?
 Stronger together - optimizing pharmacotherapy on geriatric wards? Clinicamp FOD 27/4/2018 Dr. Jean-Claude Lemper ( Geriater UZ Brussel) Apr. Julie Hias (ziekenhuisapotheker UZ Leuven) Project College
Stronger together - optimizing pharmacotherapy on geriatric wards? Clinicamp FOD 27/4/2018 Dr. Jean-Claude Lemper ( Geriater UZ Brussel) Apr. Julie Hias (ziekenhuisapotheker UZ Leuven) Project College
ASPIRIN MISUSE AT HOME ACCORDING TO START AND STOPP IN FRAIL OLDER PERSONS
 ASPIRIN MISUSE AT HOME ACCORDING TO START AND STOPP IN FRAIL OLDER PERSONS O. Dalleur 1,4, B. Boland 2,3, A. Spinewine 4-5 1 Pharmacy and 2 Geriatric Medicine, St-Luc university Hospital, 3 Institute of
ASPIRIN MISUSE AT HOME ACCORDING TO START AND STOPP IN FRAIL OLDER PERSONS O. Dalleur 1,4, B. Boland 2,3, A. Spinewine 4-5 1 Pharmacy and 2 Geriatric Medicine, St-Luc university Hospital, 3 Institute of
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients
 A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients") There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Appropriateness of prescribing in older patients
 Appropriateness of prescribing in older patients Which tools should be used? Anne Spinewine MPharm, MSc, PhD Université catholique de Louvain, Belgium Louvain Drug Research Institute and CHU Mont-Godinne
Appropriateness of prescribing in older patients Which tools should be used? Anne Spinewine MPharm, MSc, PhD Université catholique de Louvain, Belgium Louvain Drug Research Institute and CHU Mont-Godinne
Presentation of a specific research project
 Presentation of a specific research project Appropriate use of medicines in care of the elderly: Factors underlying inappropriateness, and impact of the clinical pharmacist Anne Spinewine 04.10.2011 WBI-
Presentation of a specific research project Appropriate use of medicines in care of the elderly: Factors underlying inappropriateness, and impact of the clinical pharmacist Anne Spinewine 04.10.2011 WBI-
Polypharmacy. Polypharmacy. Suboptimal Prescribing in Older Adults. Kenneth Schmader, MD Professor of Medicine-Geriatrics
 Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION. Building Partnerships for Successful Aging
 MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Screening tools for elderly patients in primary care
 Screening tools for elderly patients in primary care Cristín Ryan 1 Prof. Julia Kennedy 1 Dr. Denis O Mahony 2 Dr. Stephen Byrne 1 Co-Investigator: Dr. Paul Gallagher 2 1 Pharmaceutical Care Research Group,
Screening tools for elderly patients in primary care Cristín Ryan 1 Prof. Julia Kennedy 1 Dr. Denis O Mahony 2 Dr. Stephen Byrne 1 Co-Investigator: Dr. Paul Gallagher 2 1 Pharmaceutical Care Research Group,
From medicines reconciliation to medicines review. Dr. Fatma Karapinar Hospital pharmacistepidemiologist
 From medicines reconciliation to medicines review Dr. Fatma Karapinar Hospital pharmacistepidemiologist Conflict of interest Nothing to disclose Questions Medication review is more important than medicines
From medicines reconciliation to medicines review Dr. Fatma Karapinar Hospital pharmacistepidemiologist Conflict of interest Nothing to disclose Questions Medication review is more important than medicines
Politerapia e interazioni negli anziani: possibili interventi
 LE ANALISI SULL'USO DEI FARMACI: METODI ED ESPERIENZE IN ITALIA Politerapia e interazioni negli anziani: possibili interventi Graziano Onder Centro Medicina dell Invecchiamento Università Cattolica del
LE ANALISI SULL'USO DEI FARMACI: METODI ED ESPERIENZE IN ITALIA Politerapia e interazioni negli anziani: possibili interventi Graziano Onder Centro Medicina dell Invecchiamento Università Cattolica del
Pharmacology in the Elderly
 Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy
 START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
Appropriate use of medicines in care of the elderly - Factors underlying inappropriateness, and impact of the clinical pharmacist
 Appropriate use of medicines in care of the elderly - Factors underlying inappropriateness, and impact of the clinical pharmacist Anne Spinewine PhD thesis - Public defense 8 June 2006 A spoonful of sugar,
Appropriate use of medicines in care of the elderly - Factors underlying inappropriateness, and impact of the clinical pharmacist Anne Spinewine PhD thesis - Public defense 8 June 2006 A spoonful of sugar,
National Medicines Information Centre ST. JAMES S HOSPITAL DUBLIN 8 TEL or FAX
 National Medicines Information Centre ST. JAMES S HOSPITAL DUBLIN 8 TEL 01-4730589 or 1850-727-727 FAX 01-4730596 www.nmic.ie PRESCRIBING IN THE ELDERLY INTRODUCTION According to the most recent census
National Medicines Information Centre ST. JAMES S HOSPITAL DUBLIN 8 TEL 01-4730589 or 1850-727-727 FAX 01-4730596 www.nmic.ie PRESCRIBING IN THE ELDERLY INTRODUCTION According to the most recent census
Medication Management. Medications: The Right Balance. Who are we talking about? Geriatric Syndromes 9/19/2016. Older adults are a heterogenous group!
 Medication Management Who are we talking about? Older adults are a heterogenous group! Patricia W. Slattum, PharmD, PhD Professor of Pharmacotherapy and Outcomes Science Director, Geriatric Pharmacotherapy
Medication Management Who are we talking about? Older adults are a heterogenous group! Patricia W. Slattum, PharmD, PhD Professor of Pharmacotherapy and Outcomes Science Director, Geriatric Pharmacotherapy
Pharmaceutical Care for Geriatrics
 Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Polypharmacy and Deprescribing for Older People
 Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Medication safety in vulnerable patient groups - Elderly patients -
 Woodennature/CC-BY-SA-3.0 http://theintelligence.de Medication safety in vulnerable patient groups - Elderly patients - 20th Congress of EAHP 25-27 March, 2015, Hamburg, Germany Dr. rer. nat. Beate Wickop
Woodennature/CC-BY-SA-3.0 http://theintelligence.de Medication safety in vulnerable patient groups - Elderly patients - 20th Congress of EAHP 25-27 March, 2015, Hamburg, Germany Dr. rer. nat. Beate Wickop
Polymedication in nursing home. Graziano Onder Centro Medicina dell Invecchiamento Università Cattolica del Sacro Cuore Rome - Italy
 Polymedication in nursing home Graziano Onder Centro Medicina dell Invecchiamento Università Cattolica del Sacro Cuore Rome - Italy Services and Health for Elderly in Long TERm care (SHELTER) 4156 residents
Polymedication in nursing home Graziano Onder Centro Medicina dell Invecchiamento Università Cattolica del Sacro Cuore Rome - Italy Services and Health for Elderly in Long TERm care (SHELTER) 4156 residents
Iatrogenesis in the frail elderly
 Iatrogenesis in the frail elderly Professor Michael Dooley Director of Pharmacy Alfred Health Professor of Clinical Pharmacy Centre for Medicine Use and Safety Monash University Iatrogenesis in the frail
Iatrogenesis in the frail elderly Professor Michael Dooley Director of Pharmacy Alfred Health Professor of Clinical Pharmacy Centre for Medicine Use and Safety Monash University Iatrogenesis in the frail
HA CONVENTION Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward
 Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward HA CONVENTION 2017 Candis Chang Pharmacist Department of Pharmacy Ruttonjee and Tang Shiu Kin Hospitals Background
Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward HA CONVENTION 2017 Candis Chang Pharmacist Department of Pharmacy Ruttonjee and Tang Shiu Kin Hospitals Background
THE ADVANCED MEDICATION REVIEW
 THE ADVANCED MEDICATION REVIEW PCNE WORKING SYMPOSIUM ON MEDICATION REVIEW 2009 WORKSHOP 3 Facilitator: Nina Griese n.griese@abda.aponet.de Aim of the workshop 2 To define an advanced medication review
THE ADVANCED MEDICATION REVIEW PCNE WORKING SYMPOSIUM ON MEDICATION REVIEW 2009 WORKSHOP 3 Facilitator: Nina Griese n.griese@abda.aponet.de Aim of the workshop 2 To define an advanced medication review
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Appropriate prescribing and deprescribing for older people getting it right. Alan Davis Northland District Health Board
 Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Polypharmacy and the Older Adult. Leslie Baker, PharmD, BCGP Umanga Sharma, MD
 Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
This material is the copyright of the original publisher. Unauthorised copying and distribution is prohibited.
 Terms and Conditions for Use of PDF The provision of PDFs for authors personal use is subject to the following Terms & Conditions: The PDF provided is protected by copyright. All rights not specifi cally
Terms and Conditions for Use of PDF The provision of PDFs for authors personal use is subject to the following Terms & Conditions: The PDF provided is protected by copyright. All rights not specifi cally
Update in Geriatrics: Choosing Wisely Primum Non Nocere
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016
 Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Around fifteen semi-structured interviews are going to be conducted with specialist physicians of the domains selected for the checklist.
 1 SEMI-STRUCTURED INTERVIEW GUIDE THE INTERVIEW PROCESS This interview is intended to create statements of potential interest for a prescription-screening checklist to detect potentially inappropriate
1 SEMI-STRUCTURED INTERVIEW GUIDE THE INTERVIEW PROCESS This interview is intended to create statements of potential interest for a prescription-screening checklist to detect potentially inappropriate
Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L.
 Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L. Murphy Division Clinical Assistant Professors, University of Texas/UTHSCSA
Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L. Murphy Division Clinical Assistant Professors, University of Texas/UTHSCSA
23/11/2018. Tools to stratify patients for clinical pharmacy interventions
 Tools to stratify patients for clinical pharmacy interventions Professor Mike Scott Director of the Regional Medicines Optimisation Innovation Centre (MOIC) 47 th ESCP Symposium, Belfast 24 th October
Tools to stratify patients for clinical pharmacy interventions Professor Mike Scott Director of the Regional Medicines Optimisation Innovation Centre (MOIC) 47 th ESCP Symposium, Belfast 24 th October
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Optimising Safe & Appropriate Medicines Use and Deprescribing. Katie Smith, Director, East Anglia Medicines Information Service February 2014
 Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE
 POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
A Primer on Safe Prescribing to the Elderly. Dr. John Puxty
 A Primer on Safe Prescribing to the Elderly Dr. John Puxty Learning Objectives Describe an approach to safe prescribing for older patients. Appreciate the significance and causes of Polypharmacy. Identify
A Primer on Safe Prescribing to the Elderly Dr. John Puxty Learning Objectives Describe an approach to safe prescribing for older patients. Appreciate the significance and causes of Polypharmacy. Identify
Disclosures. Use caution in the elderly: review of safe and effective medication use in older patients. Institute of Medicine. Learning Objectives
 Use caution in the elderly: review of safe and effective medication use in older patients Disclosures I have no disclosures or conflicts of interest related to this presentation John T. Holmes, PharmD,
Use caution in the elderly: review of safe and effective medication use in older patients Disclosures I have no disclosures or conflicts of interest related to this presentation John T. Holmes, PharmD,
Briefing Document on Medication use and Falls
 Briefing Document on Medication use and Falls This document is intended as a briefing document and is not to be regarded as a document offering definitive legal advice in relation to the subject matter.
Briefing Document on Medication use and Falls This document is intended as a briefing document and is not to be regarded as a document offering definitive legal advice in relation to the subject matter.
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks
 Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Strategies to Decrease Medication Errors in Elderly. Abeer Zeitoun, Pharm. D Certified in Medication Safety, MCPHS
 Strategies to Decrease Medication Errors in Elderly Abeer Zeitoun, Pharm. D Certified in Medication Safety, MCPHS Road Map..Outline 1. Introduction A. Definitions B. Geriatrics: High risk population C.
Strategies to Decrease Medication Errors in Elderly Abeer Zeitoun, Pharm. D Certified in Medication Safety, MCPHS Road Map..Outline 1. Introduction A. Definitions B. Geriatrics: High risk population C.
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Rationalizing Medications. Tan Jianming Senior Pharmacist KTPH
 Rationalizing Medications Tan Jianming Senior Pharmacist KTPH + Older patients are more likely to: 2 Have multiple co-morbid diseases Have age-related physiological changes that result in a reduced tolerance
Rationalizing Medications Tan Jianming Senior Pharmacist KTPH + Older patients are more likely to: 2 Have multiple co-morbid diseases Have age-related physiological changes that result in a reduced tolerance
Rational prescribing in the older adult. Assoc Prof Craig Whitehead
 Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Inappropriate Prescribing and Related Hospital Admissions in Frail Older Persons According to the STOPP and START Criteria
 Drugs Aging (22) 29:829 837 DOI.7/s4266-2-6- ORIGINAL RESEARCH ARTICLE Inappropriate Prescribing and Related Hospital Admissions in Frail Older Persons According to the STOPP and START Criteria Olivia
Drugs Aging (22) 29:829 837 DOI.7/s4266-2-6- ORIGINAL RESEARCH ARTICLE Inappropriate Prescribing and Related Hospital Admissions in Frail Older Persons According to the STOPP and START Criteria Olivia
A Drug-related Problem Risk Assessment Tool (DRP-RAT) for use by home care practical nurses
 for use by home care practical nurses") A Drug-related Problem Risk Assessment Tool (DRP-RAT) for use by home care practical nurses Maarit Dimitrow, PhD (Pharm) University of Helsinki Finland www.helsinki.fi/yliopisto Background The demand for
A Drug-related Problem Risk Assessment Tool (DRP-RAT) for use by home care practical nurses Maarit Dimitrow, PhD (Pharm) University of Helsinki Finland www.helsinki.fi/yliopisto Background The demand for
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks
 Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS
 ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS Philip J. Schneider, MS, FASHP The University of Arizona College of Pharmacy Learning Objectives: Describe the medication-use system and all interdependent
ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS Philip J. Schneider, MS, FASHP The University of Arizona College of Pharmacy Learning Objectives: Describe the medication-use system and all interdependent
Geriatric Pharmacology. Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center
 Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Deprescribing: A Practical Guide
 Deprescribing: A Practical Guide The information in this booklet should be used as a pragmatic decision aid, in conjunction with other relevant patient specific data. Useful resource links http://www.derbyshiremedicinesmanagement.nhs.uk/assets/clinical_guidelines/clinical_guidelines_fr
Deprescribing: A Practical Guide The information in this booklet should be used as a pragmatic decision aid, in conjunction with other relevant patient specific data. Useful resource links http://www.derbyshiremedicinesmanagement.nhs.uk/assets/clinical_guidelines/clinical_guidelines_fr
Drug use in long term care. Graziano Onder Centro Medicina Invecchiamento Università Cattolica Sacro Cuore, Rome
 Drug use in long term care Graziano Onder Centro Medicina Invecchiamento Università Cattolica Sacro Cuore, Rome Polypharmacy in nursing home (USA) Concurrent use of 9 medications was reported for 39.7%
Drug use in long term care Graziano Onder Centro Medicina Invecchiamento Università Cattolica Sacro Cuore, Rome Polypharmacy in nursing home (USA) Concurrent use of 9 medications was reported for 39.7%
Exposure to potentially inappropriate medications among long-term care residents with cognitive impairment in Ontario:
 Exposure to potentially inappropriate medications among long-term care residents with cognitive impairment in Ontario: Is there an association with frailty? Laura Maclagan, Jun Guan, Sima Gandhi, Colleen
Exposure to potentially inappropriate medications among long-term care residents with cognitive impairment in Ontario: Is there an association with frailty? Laura Maclagan, Jun Guan, Sima Gandhi, Colleen
SAFETY CONCERNS WITH MULTIPLE MEDICATIONS AND BEYOND. Sandra Brownstein, PharmD, CGP
 SAFETY CONCERNS WITH MULTIPLE MEDICATIONS AND BEYOND Sandra Brownstein, PharmD, CGP Objectives: List potential medication related problems that increase in the frail elderly with acute illness Differentiate
SAFETY CONCERNS WITH MULTIPLE MEDICATIONS AND BEYOND Sandra Brownstein, PharmD, CGP Objectives: List potential medication related problems that increase in the frail elderly with acute illness Differentiate
DEPRESCRIBING IN THE ELDERLY
 DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
A systematic approach to improving pharmacotherapy in the elderly
 A systematic approach to improving pharmacotherapy in the elderly Bergkvist, Anna 2010 Link to publication Citation for published version (APA): Bergkvist, A. (2010). A systematic approach to improving
A systematic approach to improving pharmacotherapy in the elderly Bergkvist, Anna 2010 Link to publication Citation for published version (APA): Bergkvist, A. (2010). A systematic approach to improving
Empowering Older Adults On Drug Adherence A Collaborative Service Model. Cheng Po-po, Peggy Nurse Consultant (Gerontology) Yan Chai Hospital, KWC, HA
 Yan Chai Hospital, KWC, HA") Empowering Older Adults On Drug Adherence A Collaborative Service Model Cheng Po-po, Peggy Nurse Consultant (Gerontology) Yan Chai Hospital, KWC, HA Introduction Older adults have multiple pathologies
Empowering Older Adults On Drug Adherence A Collaborative Service Model Cheng Po-po, Peggy Nurse Consultant (Gerontology) Yan Chai Hospital, KWC, HA Introduction Older adults have multiple pathologies
Prevention of Medication-Related Falls Through Appropriate Medication Use. Clay Sprouse, MEd., CPhT Piedmont Technical College
 Prevention of Medication-Related Falls Through Appropriate Medication Use Clay Sprouse, MEd., CPhT Piedmont Technical College Disclosure I have no relevant financial or nonfinancial relationships to disclose
Prevention of Medication-Related Falls Through Appropriate Medication Use Clay Sprouse, MEd., CPhT Piedmont Technical College Disclosure I have no relevant financial or nonfinancial relationships to disclose
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
Intelligent Polypharmacy. Professor Colin P Bradley Department of General Practice University College Cork
 Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Introducing ValueOptions Clinical Care Alerts
 Introducing ValueOptions Clinical Care Alerts January 2013 Agenda What are Clinical Care Alerts? How does it work? What are the benefits? Questions and Answers 2 The Issue of Poor Medication Adherence
Introducing ValueOptions Clinical Care Alerts January 2013 Agenda What are Clinical Care Alerts? How does it work? What are the benefits? Questions and Answers 2 The Issue of Poor Medication Adherence
Prevalence of Polypharmacy in Geriatric Patients in Rural Teaching Hospital
 Original Article Prevalence of Polypharmacy in Geriatric Patients in Rural Teaching Hospital Maheshkumar V.P.* and Dhanapal C.K Department of Pharmacy, Annamalai University, Chidambaram- 608002, Tamil
Original Article Prevalence of Polypharmacy in Geriatric Patients in Rural Teaching Hospital Maheshkumar V.P.* and Dhanapal C.K Department of Pharmacy, Annamalai University, Chidambaram- 608002, Tamil
Reduction of High Risk Medications Using A Quality Initiative Perspective
 Reduction of High Risk Medications Using A Quality Initiative Perspective Richard Mueller PharmD, MBA, MS, Director of Pharmacy Dianne Hempel BSN, RN Quality Improvement Coordinator Objectives Learn what
Reduction of High Risk Medications Using A Quality Initiative Perspective Richard Mueller PharmD, MBA, MS, Director of Pharmacy Dianne Hempel BSN, RN Quality Improvement Coordinator Objectives Learn what
Public Dissemination Effective: January 2018
 Board of Pharmacy Specialties Board Certified Geriatric Pharmacist (BCGP) Detailed Content Outline 1. GENERAL PRINCIPLES OF AGING (20%) A. Apply the knowledge of physiologic changes associated with aging
Board of Pharmacy Specialties Board Certified Geriatric Pharmacist (BCGP) Detailed Content Outline 1. GENERAL PRINCIPLES OF AGING (20%) A. Apply the knowledge of physiologic changes associated with aging
Disclosure. The elderly at risk: reducing medications safely to meet life s changes. Relevant financial relationships.
 The elderly at risk: reducing medications safely to meet life s changes Barbara Farrell BScPhm, PharmD, FCSHP European Society of Hospital Pharmacists Conference March 2017 Disclosure Relevant financial
The elderly at risk: reducing medications safely to meet life s changes Barbara Farrell BScPhm, PharmD, FCSHP European Society of Hospital Pharmacists Conference March 2017 Disclosure Relevant financial
2/11/2016. Managing Polypharmacy: Evidence-based Dissection of Pharmaceuticals. Disclosure. Objectives
 Managing Polypharmacy: Evidence-based Dissection of Pharmaceuticals Heather Veeder MD Medical Director VITAS Healthcare San Antonio, TX Adjunct Professor of Medicine University of Texas Health Science
Managing Polypharmacy: Evidence-based Dissection of Pharmaceuticals Heather Veeder MD Medical Director VITAS Healthcare San Antonio, TX Adjunct Professor of Medicine University of Texas Health Science
Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial
 Dr Kyra Neubauer Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial assessment Understand what are potential
Dr Kyra Neubauer Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial assessment Understand what are potential
Selecting the right patient for medication reviews
 Selecting the right patient for medication reviews Prof dr Petra Denig, Clinical Pharmacy & Pharmacology, University Medical Center Groningen, the Netherlands 2 Who is in need of medication review: can
Selecting the right patient for medication reviews Prof dr Petra Denig, Clinical Pharmacy & Pharmacology, University Medical Center Groningen, the Netherlands 2 Who is in need of medication review: can
Frailty: what s it all about?
 Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
Use caution in the elderly: review of safe and effective medication use in older patients
 Use caution in the elderly: review of safe and effective medication use in older patients John T. Holmes, PharmD, BCPS Assistant Professor of Family Medicine and Pharmacy Practice In support of improving
Use caution in the elderly: review of safe and effective medication use in older patients John T. Holmes, PharmD, BCPS Assistant Professor of Family Medicine and Pharmacy Practice In support of improving
CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS
 CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS 1. The following is an accurate description of the aging population: A. The number of older adults will reach 17 million in 2030 B. The ratio of women to
CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS 1. The following is an accurate description of the aging population: A. The number of older adults will reach 17 million in 2030 B. The ratio of women to
Association between Potentially Inappropriate Prescription (PIP) and Health Outcome Among Geriatric Home Residents
 and Health Outcome Among Geriatric Home Residents") The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (6), Page 4660-4665 Association between Potentially Inappropriate Prescription (PIP) and Health Outcome Among Geriatric Home Residents Moatassem
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (6), Page 4660-4665 Association between Potentially Inappropriate Prescription (PIP) and Health Outcome Among Geriatric Home Residents Moatassem
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
Polypharmacy in HIV and Aging. Aroonsiri Sangarlangkarn, MD, MPH, Jonathan S. Appelbaum, MD, FACP
 Polypharmacy in HIV and Aging Aroonsiri Sangarlangkarn, MD, MPH, Jonathan S. Appelbaum, MD, FACP Educational Objectives By the end of the session, learners will be able to: 1. Describe one feature that
Polypharmacy in HIV and Aging Aroonsiri Sangarlangkarn, MD, MPH, Jonathan S. Appelbaum, MD, FACP Educational Objectives By the end of the session, learners will be able to: 1. Describe one feature that
Deprescribing with Confidence Dr Sanjay Suman MD FRCP
 Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
ARIC Manuscript Proposal #2493. PC Reviewed: 2/10/15 Status: A Priority: 2 SC Reviewed: Status: Priority:
 ARIC Manuscript Proposal #2493 PC Reviewed: 2/10/15 Status: A Priority: 2 SC Reviewed: Status: Priority: 1. a. Full Title: Potentially inappropriate medication use in older people: Prevalence and outcomes.
ARIC Manuscript Proposal #2493 PC Reviewed: 2/10/15 Status: A Priority: 2 SC Reviewed: Status: Priority: 1. a. Full Title: Potentially inappropriate medication use in older people: Prevalence and outcomes.
David Dosa MD, MPH Assistant Professor of Medicine and Community Health The Warren Alpert School of Medicine, Brown University Director, Primary Care
 David Dosa MD, MPH Assistant Professor of Medicine and Community Health The Warren Alpert School of Medicine, Brown University Director, Primary Care Geriatrics Clinic- Providence VAMC VA Grand Rounds
David Dosa MD, MPH Assistant Professor of Medicine and Community Health The Warren Alpert School of Medicine, Brown University Director, Primary Care Geriatrics Clinic- Providence VAMC VA Grand Rounds
*GERIATRIC FELLOWSHIP COMPETENCY CHECKLIST EDUCATIONAL GOALS:
 *GERIATRIC FELLOWSHIP COMPETENCY CHECKLIST EDUCATIONAL GOALS: The goal of geriatric fellowship training is to prepare fellows for competency in the following core areas: Check and record date completed
*GERIATRIC FELLOWSHIP COMPETENCY CHECKLIST EDUCATIONAL GOALS: The goal of geriatric fellowship training is to prepare fellows for competency in the following core areas: Check and record date completed
The role of medication in falls risk
 The role of medication in falls risk Patrick A. Ball, Foundation Professor of Rural Pharmacy, Charles Sturt University, Wagga Wagga Lecture outline The aged are not created equal Insidious nature of onset
The role of medication in falls risk Patrick A. Ball, Foundation Professor of Rural Pharmacy, Charles Sturt University, Wagga Wagga Lecture outline The aged are not created equal Insidious nature of onset
Polypharmacy. in the Elderly. Lesley Charles, MBChB, CCFP
 Polypharmacy in the Elderly Lesley Charles, MBChB, CCFP Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine, University of Alberta March 06, 2016 1 Faculty/Presenter
Polypharmacy in the Elderly Lesley Charles, MBChB, CCFP Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine, University of Alberta March 06, 2016 1 Faculty/Presenter
XXXXXXXXX XXXXXXXXXXX. #ahacop18
 XXXXXXXXX XXXXXXXXXXX #ahacop18 Specific Objectives Education and Empowerment Qualification of counselling for the empowerment of polymedicated patients Clara Cena 3.1 Improving decision making and adherence
XXXXXXXXX XXXXXXXXXXX #ahacop18 Specific Objectives Education and Empowerment Qualification of counselling for the empowerment of polymedicated patients Clara Cena 3.1 Improving decision making and adherence
Amal AL-Anazi, BSc.(Pharm) Medication Safety Officer In Eastern Region
 Medication Safety Officer In Eastern Region") Risks Of Polypharmacy Amal AL-Anazi, BSc.(Pharm) Medication Safety Officer In Eastern Region What is Polypharmacy? Polypharmacy means many drugs. In practice, polypharmacy refers to the use of more medication
Risks Of Polypharmacy Amal AL-Anazi, BSc.(Pharm) Medication Safety Officer In Eastern Region What is Polypharmacy? Polypharmacy means many drugs. In practice, polypharmacy refers to the use of more medication
About ISMP Canada. Analysis Outputs: Safety Bulletins. Less is More: An Introduction to Deprescribing. canada.org
 Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
How to prevent iatrogenic risk with antidiabetics in older people. Prof Bourdel-Marchasson University of Bordeaux, France
 How to prevent iatrogenic risk with antidiabetics in older people Prof Bourdel-Marchasson University of Bordeaux, France CONFLICT OF INTEREST DISCLOSURE I have the following potential conflicts of interest
How to prevent iatrogenic risk with antidiabetics in older people Prof Bourdel-Marchasson University of Bordeaux, France CONFLICT OF INTEREST DISCLOSURE I have the following potential conflicts of interest
STOPP START Toolkit Supporting Medication Review in the Older Person
 STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
Division of pharmaceutical sciences, Shri Guru Ram Rai Institute of Technology & Science, Dehradun;
 Academic Sciences Asian Journal of Pharmaceutical and Clinical Research Vol 5, Suppl 4, 2012 ISSN - 0974-2441 Research Article HOME MEDICATION REVIEW- ITS STATUS AND AWARENESS AMONG GERIATRIC POPULATION
Academic Sciences Asian Journal of Pharmaceutical and Clinical Research Vol 5, Suppl 4, 2012 ISSN - 0974-2441 Research Article HOME MEDICATION REVIEW- ITS STATUS AND AWARENESS AMONG GERIATRIC POPULATION
Review of Current Literature 4/2/18 POLYPHARMACY IN ASSISTED LIVING EVIDENCE BASED APPROACH
 POLYPHARMACY IN ASSISTED LIVING A Evidence Based Approach to Management of Medication Regimen Complexity By Burton Korer, MSN, RN-BC, CPHQ EVIDENCE BASED APPROACH Evidence-based practice (EBP) is the conscientious
POLYPHARMACY IN ASSISTED LIVING A Evidence Based Approach to Management of Medication Regimen Complexity By Burton Korer, MSN, RN-BC, CPHQ EVIDENCE BASED APPROACH Evidence-based practice (EBP) is the conscientious
Supplemental materials for:
 Supplemental materials for: Wallis KA, Andrews A, Henderson M. Swimming against the tide: primary care physicians views on deprescribing in everyday practice. Ann Fam Med. 2017;15(4):341-346. General Practice
Supplemental materials for: Wallis KA, Andrews A, Henderson M. Swimming against the tide: primary care physicians views on deprescribing in everyday practice. Ann Fam Med. 2017;15(4):341-346. General Practice
Taking the harm out of Polypharmacy Step by step. Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian
 Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
NICE guideline Published: 21 September 2016 nice.org.uk/guidance/ng56
 Multimorbidity: clinical assessment and management NICE guideline Published: 21 September 2016 nice.org.uk/guidance/ng56 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Multimorbidity: clinical assessment and management NICE guideline Published: 21 September 2016 nice.org.uk/guidance/ng56 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
To Take or Not To Take?
 To Take or Not To Take? Assessment Question How do the terms adherence & compliance differ? 1. The terms are synonymous 2.Adherence assumes collaboration between patient & provider while compliance suggests
To Take or Not To Take? Assessment Question How do the terms adherence & compliance differ? 1. The terms are synonymous 2.Adherence assumes collaboration between patient & provider while compliance suggests
META-ANALYSIS Impact of strategies to reduce polypharmacy on clinically relevant endpoints: a systematic review and meta-analysis
 British Journal of Clinical Pharmacology Br J Clin Pharmacol (2016) 82 532 548 532 META-ANALYSIS Impact of strategies to reduce polypharmacy on clinically relevant endpoints: a systematic review and meta-analysis
British Journal of Clinical Pharmacology Br J Clin Pharmacol (2016) 82 532 548 532 META-ANALYSIS Impact of strategies to reduce polypharmacy on clinically relevant endpoints: a systematic review and meta-analysis
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Less is More: Introduction to Deprescribing
 Less is More: Introduction to Deprescribing 7th Annual Pharmaceutical Care Conference Muscat, Oman Feb 23, 2017 Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About
Less is More: Introduction to Deprescribing 7th Annual Pharmaceutical Care Conference Muscat, Oman Feb 23, 2017 Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About
Appraisal of the appropriateness of prescribing in community-dwelling oldest old (aged 80+)
") Faculty of Medicine and Health Sciences Heymans Institute of Pharmacology Division of Clinical Pharmacology 2018 Appraisal of the appropriateness of prescribing in community-dwelling oldest old (aged 80+)
Faculty of Medicine and Health Sciences Heymans Institute of Pharmacology Division of Clinical Pharmacology 2018 Appraisal of the appropriateness of prescribing in community-dwelling oldest old (aged 80+)
Disclosure and Acknowledgements
 Greetings from Penn Nursing SOHN 37 TH ANNUAL CONGRESS AND NURSING SYMPOSIUM POLYPHARMACY AND OLDER ADULTS: HIGH RISK MEDS, TOO MANY MEDS, AND TOO FEW MEDS Sarah H. Kagan PhD, RN University of Pennsylvania,
Greetings from Penn Nursing SOHN 37 TH ANNUAL CONGRESS AND NURSING SYMPOSIUM POLYPHARMACY AND OLDER ADULTS: HIGH RISK MEDS, TOO MANY MEDS, AND TOO FEW MEDS Sarah H. Kagan PhD, RN University of Pennsylvania,
Meds and Falls: Keep in Step with your Meds
 Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Geriatric Syndromes. Elizabeth K Keech PhD, RN Elise Pizzi MSN, GNP-BC
 Geriatric Syndromes Elizabeth K Keech PhD, RN Elise Pizzi MSN, GNP-BC What are they? Conditions, not diseases Common in the elderly Typically: Multifactorial Share risk factors Linked with functional decline,
Geriatric Syndromes Elizabeth K Keech PhD, RN Elise Pizzi MSN, GNP-BC What are they? Conditions, not diseases Common in the elderly Typically: Multifactorial Share risk factors Linked with functional decline,
Detecting inappropriate prescribing for older patients at the community pharmacy
 Detecting inappropriate prescribing for older patients at the community pharmacy Eline Tommelein, Els Mehuys, Koen Boussery Pharmaceutical Care Unit, Faculty of Pharmaceutical Sciences, Ghent University,
Detecting inappropriate prescribing for older patients at the community pharmacy Eline Tommelein, Els Mehuys, Koen Boussery Pharmaceutical Care Unit, Faculty of Pharmaceutical Sciences, Ghent University,
Danielle Pierotti RN, PhD, AOCN, CHPN Chief Nurse/Director of Clinical Practice HCI Hospice. with you at every step
 Danielle Pierotti RN, PhD, AOCN, CHPN Chief Nurse/Director of Clinical Practice HCI Hospice Objectives Review current policy and environmental issues influencing medication choices at end of life Discuss
Danielle Pierotti RN, PhD, AOCN, CHPN Chief Nurse/Director of Clinical Practice HCI Hospice Objectives Review current policy and environmental issues influencing medication choices at end of life Discuss