PD PEARLS. Ezra Hazzan MD November 19, 2014
|
|
|
- Jonas Hubbard
- 6 years ago
- Views:
Transcription
1 PD PEARLS Ezra Hazzan MD November 19, 2014
2 Case study 43 year old female, DM and now needs to start dialysis. Works full Ime, highly moivated and good support system. 65 year old male, Spanish speaking, unemployed, recent immigrant with spouse at home. 50 year old male, obese, on HD with an IJ permacath (failed fistula) and inquiring about PD. 20 year old male who drinks a lot of fluid >1.5liters, and loves eaing fruit( tons of potassium).
3 Peritoneal Dialysis MisconcepIons The prevalence of infecions is much higher in PD than HD PaIent survival is less on PD PD takes too much of the paient s Ime PaIents do not want PD PD requires high levels of understanding and educaion PD requires a companion at home to help with therapy

4 Reality of PD InfecIons
5
6
7
8 The prevalence of infecions is much higher in PD than in HD NOT TRUE
9
10
11 PaIents survive less Ime on PD NOT TRUE
12 PD takes too much of the paient s Ime o On CAPD 4 exchanges x 30 minutes = 2 hours (14 hours a week) o On CCPD : Seang up machine, min, connecion/disconnecion 5 min. Plus day Ime exchange 45 min = 1 hr 10/15 min. Total weekly set up Ime: 8-9 hr + sleep Ime. o On HD: HD Ime 4 hours plus on/off Ime, about ½ hour. WaiIng /travel Ime 1 treatment Total weekly Ime: 16 ½ hr (without resing aier HD) Courtesy of Karen Kelley, Baxter
13 PD takes too much of the paient s Ime, when compared with HD NOT TRUE

14
15
16 PaIent raings of dialysis care with PD or HD Rubin et al JAMA 291: ,2004 Cross- secional survey at enrollment of paients who recently started dialysis at 37 dialysis centers in 14 states paricipaing in the CHOICE Study. A paient administered quesionnaire included 20 items raing specific aspects of dialysis care, and 3 overall dialysis care raings. Of 736 enrolled paients, 656 (89%) returned the quesionnaire aier an average of 7 weeks on dialysis.

17
18 SaIsfacIon with renal replacement therapy and educaion: the American AssociaIon of Kidney PaIents Survey Fadem et al. CJASN 2011 This was an open invitaion on the AAKP website + nearly 9000 paients received the invitaion to complete the survey. The survey consisted of 46 quesions to measure paient saisfacion with their RRT modality. SaIsfacIon was measured on a 1 (extremely dissaisfied) to 7 (extremely saisfied) scale.
19
20 Requirements for PD FuncIoning PD catheter Dialyzer: funcioning peritoneum Ability and interest in learning home dialysis on part of paient or support person
21 PaIents need to understand that there are two types of PD CAPD con%nuous ambulatory peritoneal dialysis, done 2-4 %mes per day. APD or CCPD done at night using a machine called a cycler. From the pa+ent perspec+ve these are not the same. 21

22 CAPD: coninuous ambulatory peritoneal dialysis Each exchange takes about 30 minutes. Number of exchanges depends on residual kidney funcion 22

23
 20 minutes.")
24 APD: automated peritoneal dialysis At bedtime the patient places bags on In the morning, the paient cycler and attaches catheter to cycler tubing, disconnects and discards used pushes button to start the cycler. Takes about tubing. (takes <5 min) 20 minutes. 24
25 Deciding on modality Cycler PD In center HD Nightly, while sleeping 3 Imes per week Done by paient Done by staff Private In center PD catheter TDC/Grai/fistula No needles Two needles 3 x wk Risk of peritoniis Risk of bacteremia
 flexibility (2) convenience (3) night- Ime dialysis Adapted from Wuerth et al PDI")
26 Why do paients choose PD- - Issues of autonomy and control were important for 95% of paients choosing PD. Other reasons for choosing PD: (1) flexibility (2) convenience (3) night- Ime dialysis Adapted from Wuerth et al PDI 2002; 22:
27 Other notes on PD selecion Non adherence is common on in center HD. If PD is the paient choice, paient may be more compliant with PD than HD. Most paients can learn PD with a good trainer who tailors the therapy to the individual. 27
28 Your paient has chosen PD. What now? 28


29 Schedule PD catheter placement 29
30 The PD catheter can be placed as same day surgery. Very important to chose operator to place the PD catheter who will work with you. Can be surgeon, nephrologist, radiologist. Leave exit site covered with clean dressing unil training begins; do not allow paient to get this wet. 30
31 Urgent start PD PD catheter can be used the same day or the next day. This is now called urgent start dialysis. Appropriate if dialysis needed sooner. PD should be supine with low volumes. Generally used when paient hospitalized. 31

32 PD training We believe one- on- one training is best. Nurse doing the training must be trained in not only PD but how to teach PD. Training best individualized to the paient. Training covers theory, basics of the procedure, recogniion of peritoniis. Test is given at the compleion of training to ensure knowledge. 32

33 Dialysis fluid contains Dextrose 1.5, 2.5, 4.25 Na and Cl Lactate Ca Mg sterile water ph low Efluent is the spent (dwelled) dialysate 33
34 Obtain a clearance early in the course of PD. Kt/V is used but described as per week. Obtained by collecing effluent for one day, measuring urea nitrogen to calculate Kt and divided by V. This is then muliplied by 7 to get weekly value. Renal clearance is added into this, when present. Minimum: 1.7 per week. 34




35 PeritoniIs causes pain, hospitaliza%on, peritoneal membrane damage and some%mes death. 35
36 PeritoniIs may contribute to death AUSNZ registry: examined 1316 PD pts who died on PD or within 30 days of transfer to HD 19% of PD pt who died had peritonifs in the preceding 30 days Even though only 6% coded as having died from peritoniis. Boudville et al JASN 2012: 23: 1-8
37 InfecFons are the second leading cause of death in the dialysis pafents HD and PD both have associated infecions but different types: HD pa%ents get bacteremia and pneumonia PD pa%ents get peritoni%s 37
 GU")
38 Think about what causes peritoniis ContaminaIon Enteric sources Catheter related: exit site or slime related Bacteremia (rare) GU sources (rare)
39 PrevenIng peritoniis from contaminaion: the nurse is all- important in training the PD paient Do not assume a nurse who knows PD, knows how to teach PD. ISPD web site has a secion on Training the Trainer Found at ispd.org


40 GI sources of peritoniis Transmural migraion Bowel ischemia DiverIculiIs ColiIs CholecysIIs PerforaIon of an organ AppendiciIs GI procedures Ischemic bowel CholecysFFs
41 Procedures can lead to peritoniis Extensive dental work (streptococcus) Colonoscopy/proctoscopy (enteric) Lap cholecystectomy (enteric) Percutaneous gastrostomy (enteric/fungal) Endometrial biopsy/hysteroscopy (streptococcus, funal, anaerobes)

42 PrevenIng peritoniis from ESI: Double blinded muli- center RCT of exit site gentamicin vs mupirocin 0.6 Exit site infections in episodes per year at risk other fungal P aeruginsos S aureus mupirocin gentamicin Bernardini.Piraino JASN 2005: 16:







43

44 PeritoniIs due to biofilm Biofilm can lead to refractory, relapsing or repeat peritonifs Nessim et al PDI 2012 Canadian study, POET data base: 181 paients had 2 episodes peritoniis with same organism - Coag neg staph caused 2/3-1 st episode coag neg staph peritoniis vs other organisms had odds raio of 2.1 of another episode within one year - ½ occurred within 6 months of 1 st episodes
45 Topics to be Discussed The impact of increased intra- abdominal pressure Hernias Abdominal and Genital Leaks Hydrothorax Colored dialysis effluent Psychosocial issues EncapsulaIng Peritoneal Sclerosis Metabolic changes secondary to PD

46
47 Increased Intra- abdominal Pressure Hernias: Incisional Umbilical Ventral DiaphragmaIc Leaks Pericatheter Leaks: Abdominal wall or Genital Abdominal swelling or bogginess or scrotal or labial edema Diagnosis: physical exam, Radiological studies CT scan, TechneIum scan

48
49 Management Hernias: Repair Leaks: Use low pressure PD (eg APD with low volumes with paient lying and a dry day ). Temporary HD to allow healing.

50 Hydrothorax The presence of peritoneal dialysis fluid in the pleural cavity. PD fluid moves through congenital or acquired defects in the diaphragm. Diagnosis: a. Pleural tap with fluid analysis b. TechniIum scan, CT scan c. Stop and restart PD with monitoring of extent of pleural effusion. Treatment: temporary respite from PD pleurodesis, pleuroscopic repair (diaphragmaic defects idenified and patched or sutured)
51 Metabolic Problems of the CKD PaIent General for CKD paients Thyroid dysfuncion Metabolic syndrome AbnormaliIes of sex hormones Lipid abnormaliies Glucose intolerance Mineral metabolism Insulin resistance PD Specific Dextrose exposure Weight gain Metabolic syndrome Specific lipid related issues Insulin resistance Others: LepIn, AdinoponecIn, Ghrelin Protein losses
52 Lipid Changes Aier the Start of PD Pennell Clin Nephrol 62:35, 2004 A significant increase in total cholesterol, LDL, cholesterol, triglyceride, and VLDL levels occur aier start of PD. No change in HDL levels These changes can be ameliorated with appropriate management protocols.
53 Metabolic Syndrome and the PD PaIent Jhang et al : Blood PurificaIon, 26:423, 2008 Increased risk in PD paients (c. 50% of prevalent PD paients, 20% HD paients, 30% CKD paients. The driving forces for the development of Metabolic Syndrome in Pd paients are clearly related to glucose absorpion. 195 non- diabeic paients maintained on PD 22% of paients met criteria for MS* at iniiaion of PD Aier mean of 34 months (range months), 69% met criteria for MS Development of MS was correlated with dextrose exposure and duraion of PD. * Defined with NaIonal Cholesterol EducaIon Adult Treatment Panel III criteria.

54
55 Conclusion There are a variety of non- infecious problems that are specific to peritoneal dialysis. With increasing experience, the impact of these problems may be manageable The largest problem relates to chronic dextrose exposure, which in turn results in changes in transport characterisics, damage to the peritoneal membrane and various metabolic issues.
56 RecommendaIons LimiIng dextrose exposure must be a cornerstone of PD management Liberal use of icodextrin and high dose furosemide therapy (in those paients with residual funcion) to minimize dextrose exposure is criically important. TargeIng Kt/V algorithms to achieve levels of should be the standard; there is no benefit of targeing higher doses.
57 What is important when prescribing PD? Clearance targets. Adequate ultrafiltraion to control volume. Avoiding excess glucose exposure. Cost of prescripion.
58 What is important when prescribing PD? But this is the era of paient centered care and we need paient centered PD so PaIent symptoms PaIent lifestyle
59 INTRODUCTION Achieving high solute clearance in PD is a whole lot easier since the Ademex Study and the consequent reducion in K/DOQI targets. A target Kt/V of 1.7 per week for all paients CAPD and APD, high and low transporters.
60 Clearance on PD determinants 1. Residual renal funcion. 2. Body size. 3. Peritoneal transport status. 4. PD prescripion
61 Present Kt/V Targets Easy to reach if paients have residual renal funcion. Typically, 60-70% do and it is oien substanial due to earlier start on dialysis. Each ml/min urea clearance equals about 0.25 Kt/V per week so 4 mls/min = 1.0 Kt/V
62 Increasing Clearance in CAPD Three opions: Increase dwell volume Increase number of exchanges Increase dialysate tonicity
63 Increasing Dwell Volume Most cost effecive way to increase clearance. Diffusion gradient lasts longer EquilibraIon for 2.5L is only slightly less than with standard 2L volumes. Raised intraperitoneal pressure is limiing factor mechanical side effects.
64 Strategies to Achieve Targets CAPD In CAPD, many smaller paients will achieve pkt/v 1.7 on 4 x 2L daily. Larger paients will require 4 x 2.5L Few will need 4 x 3L or 5 x 2L or switch to APD
65

66

67

68

69

70 Thank you.
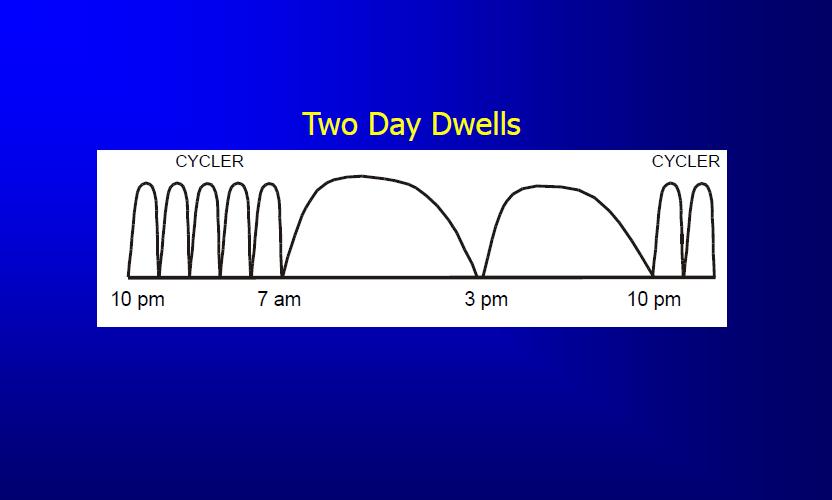
71 APD PrescripIon Cycler Related: Number of cycles Day Dwell Related: No cf Day dwells Dwell volume Dwell volume Cycler Ime Dwell duraion Tonicity Tonicity
72 Day Dwells Single most effecive way to raise clearance in a day. Dry APD paient is to add a day dwell raises Kt/V 30 40% If already has a day dwell, the most effecive intervenion is a second day dwell raises Kt/V c 20%. Should be at least 4 hours duraion to get full benefit in Kt/V
73 Day Dwells POINTS TO REMEMBER The larger the dwell volume the greater the clearance i.e. 2.5v 2v 1.5L Day dwells can be done more simply and less expensively using cycler tubing and large volume bags. Adding a second day dwell creates more work for the paient or caregiver.
74 Day Dwells POINTS TO REMEMBER Longer glucose based day dwells may lead to net fluid resorpion and so may actually decrease clearance as well as UF. There are a number of strategies to deal with this.
75 Day Dwell OpIons for Be{er UF Go day dry an opion if there is lots of residual funcion. Do 2 day dwells drain and refill maximizes clearance. Shorten day dwell by draining and remaining dry part of the day. Use Icodextrin for day dwell increasingly popular.
76 Increasing Cycler Clearance Longer Ime raises clearance but > 9 hrs is not acceptable to most paients. What about dwell volume? Is 4 x 2.5 L cycles be{er than 5 x 2L? What about cycle frequency? Is 7 x 2L be{er than 5 x 2L? Is 9 x 2L be{er than 7 x 2L?
77 OpImal Cycle Frequency There is confusion about whether or not increasing the number of cycles raises clearance significantly. Concern is that more Ime is spent draining and filling (down Ime) and less actually dialyzing. However, frequent cycling keeps blood to dialysate gradient high and so promotes more diffuse clearance.
78 OpImal Cycle Frequency Study Perez et al (PDI 2000) 18 paients at 2 centers 4 different prescripions for 7 days each Measurement of clearances, UF, Na, K+, and protein losses and glucose absorpion on days 5-7 on each prescripion. Clearance due to residual renal funcion and day dwells was ignored.
79 OpImal Cycle Frequency Study 4 prescripions 1. 5 x 2L over 9 hours 2. 7 x 2L over 9 hours 3. 9 x 2L over 9 hours 4. 15L TPD (50%) using 1L + 14 x 1L over 9 hours
80 OpImal Cycle Frequency Study Perez et al (PDI 2000) 9 x 2L was the best in 12 of the 18 (in 9 by > 10%) 7 x 2L was the best in 3, TPD in 2 Advantage of 9 x 2L was greatest for Kt/V Advantage was seen in both low and high transporters for both Kt/V and Cr Cl UF was be{er in 7 x 2L and 9 x 2L versus 5 x 2L.
81 OpImal Cycle Frequency Study Conclusion More cycles raise clearance significantly in most paients. 4 5 cycles per 9 hours under- uses clearance potenial of APD. But cost was 27% greater for 15L vs. 10L and 54% for 18L vs. 10L so adding day dwells is more cost effecive but also more work for paient.
82 Incremental Dialysis Idea that full dialysis dose need not be prescribed iniially in paients with substanial residual renal funcion. In HD twice weekly treatments. In PD 3 dwells daily in CAPD or day dry in APD

83
84 Incremental Dialysis London Approach All elecive starts do day dry APD. Quarterly measurements of pkt/v and rkt/v as well as clinical assessment. ConInue without day dwell as long as paient well and Kt/V > 1.7 Some cycle < 7 nights a week.
85 Incremental PD DefiniIon Total weekly Kt/V reaching target of > 1.7 with peritoneal Kt/V < 1.7. PLUS A day dry or < 7 nights/ week schedule for APD paients. OR < 8L/ day schedule for CAPD paients.

86

87
UW MEDICINE PATIENT EDUCATION. Peritoneal Dialysis. A treatment option for kidney disease. There are 2 types of PD: continuous ambulatory
 UW MEDICINE PATIENT EDUCATION Peritoneal Dialysis A treatment option for kidney disease Class Goals 1. Understand the purpose and basic principles of continuous ambulatory peritoneal dialysis (CAPD). 2.
UW MEDICINE PATIENT EDUCATION Peritoneal Dialysis A treatment option for kidney disease Class Goals 1. Understand the purpose and basic principles of continuous ambulatory peritoneal dialysis (CAPD). 2.
Objectives. Peritoneal Dialysis vs. Hemodialysis 02/27/2018. Peritoneal Dialysis Prescription and Adequacy Monitoring
 Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Your Kidney Health. Your Choices. Chronic Kidney Disease
 Your Kidney Health Your Choices Your doctor may have told you that you have chronic kidney disease (CKD or advanced kidney disease; or, you may be in kidney failure, and may have to make a decision about
Your Kidney Health Your Choices Your doctor may have told you that you have chronic kidney disease (CKD or advanced kidney disease; or, you may be in kidney failure, and may have to make a decision about
Fistula First? Vascular Symposium 4/28/18
 Fistula First? Vascular Symposium 4/28/18 Disclosure I have no financial interest to disclose connected to any of the information presented in this discussion Objectives Scope of Problem Benefits of PD
Fistula First? Vascular Symposium 4/28/18 Disclosure I have no financial interest to disclose connected to any of the information presented in this discussion Objectives Scope of Problem Benefits of PD
Select the dialysis treatment option that is best for you and your family.
 PEP CONNECT PEP Talk Outline P a t i e n t E d u c a t i o n P r o g r a m Your Treatment Options Part 1 Peritoneal Dialysis Select the dialysis treatment option that is best for you and your family. This
PEP CONNECT PEP Talk Outline P a t i e n t E d u c a t i o n P r o g r a m Your Treatment Options Part 1 Peritoneal Dialysis Select the dialysis treatment option that is best for you and your family. This
KIDNEY FAILURE TREATMENT OPTIONS Choosing What s Best For You
 KIDNEY FAILURE TREATMENT OPTIONS Choosing What s Best For You What Kidneys Do The kidneys are a pair of bean shaped organs located below your ribcage near the middle of your back. Kidneys play a vital
KIDNEY FAILURE TREATMENT OPTIONS Choosing What s Best For You What Kidneys Do The kidneys are a pair of bean shaped organs located below your ribcage near the middle of your back. Kidneys play a vital
You can sleep while I dialyze
 You can sleep while I dialyze Nocturnal Peritoneal Dialysis Dr. Suneet Singh Medical Director, PD, VGH Division of Nephrology University of British Columbia Acknowledgements Melissa Etheridge You can sleep
You can sleep while I dialyze Nocturnal Peritoneal Dialysis Dr. Suneet Singh Medical Director, PD, VGH Division of Nephrology University of British Columbia Acknowledgements Melissa Etheridge You can sleep
Peritoneal Dialysis. Choosing your logo. V2.0 logos. information. you can trust. Certified Member. The Information Standard
 Use of The Information Standard s Member Logos Peritoneal Dialysis Patient Information Choosing your logo The Information Standard has four logo versions for its members. They are designed to fit neatly
Use of The Information Standard s Member Logos Peritoneal Dialysis Patient Information Choosing your logo The Information Standard has four logo versions for its members. They are designed to fit neatly
PD In Acute Kidney Injury. February 7 th -9 th, 2013
 PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
What is a PET? Although there are many types of pets, we will be discussing the Peritoneal Equilibration Test
 1 2 3 What is a PET? Although there are many types of pets, we will be discussing the Peritoneal Equilibration Test 4 Background information about the PET 1983 Dr. Twardowski and colleagues began measuring
1 2 3 What is a PET? Although there are many types of pets, we will be discussing the Peritoneal Equilibration Test 4 Background information about the PET 1983 Dr. Twardowski and colleagues began measuring
PERITONEAL EQUILIBRATION TEST. AR. Merrikhi. MD. Isfahan University of Medical Sciences
 PERITONEAL EQUILIBRATION TEST AR. Merrikhi. MD. Isfahan University of Medical Sciences INTRODUCTION The peritoneal equilibration test (PET) is a semiquantitative assessment of peritoneal membrane transport
PERITONEAL EQUILIBRATION TEST AR. Merrikhi. MD. Isfahan University of Medical Sciences INTRODUCTION The peritoneal equilibration test (PET) is a semiquantitative assessment of peritoneal membrane transport
Peritoneal Dialysis Program King Campus 2757 King Street East Hamilton, Ontario ext
 Peritoneal Dialysis Program King Campus 2757 King Street East Hamilton, Ontario 905-522-1155 ext. 38275 1 Table of Contents Page What is peritoneal dialysis? 1 How does this happen? 1 What are the types
Peritoneal Dialysis Program King Campus 2757 King Street East Hamilton, Ontario 905-522-1155 ext. 38275 1 Table of Contents Page What is peritoneal dialysis? 1 How does this happen? 1 What are the types
Smart APD prescription. Prof. Wai Kei Lo Tung Wah Hospital The University of Hong Kong
 Smart APD prescription Prof. Wai Kei Lo Tung Wah Hospital The University of Hong Kong Costing Comparison of Different Modes of RRT in Hong Kong in 2011 (Per Year) HK$300,000 HK$250,000 HK$200,000 HK$150,000
Smart APD prescription Prof. Wai Kei Lo Tung Wah Hospital The University of Hong Kong Costing Comparison of Different Modes of RRT in Hong Kong in 2011 (Per Year) HK$300,000 HK$250,000 HK$200,000 HK$150,000
Peritoneal Dialysis Prescriptions: A Primer for Nurses
 Peritoneal Dialysis Prescriptions: A Primer for Nurses A Primer ABCs of PD R x Betty Kelman RN-EC MEd CNeph (C) Toronto General Hospital University Health Network Toronto, Ontario, Canada A moment to remember
Peritoneal Dialysis Prescriptions: A Primer for Nurses A Primer ABCs of PD R x Betty Kelman RN-EC MEd CNeph (C) Toronto General Hospital University Health Network Toronto, Ontario, Canada A moment to remember
Imad Ahmed MD. Renal Associates of West Michigan
 Imad Ahmed MD Renal Associates of West Michigan ESRD Facts: - Medicare funded program - Cost - Significant mortality and morbidity - Reduced quality of life - Shrinking donor pool ESRD CAUSES - DM - Hypertension
Imad Ahmed MD Renal Associates of West Michigan ESRD Facts: - Medicare funded program - Cost - Significant mortality and morbidity - Reduced quality of life - Shrinking donor pool ESRD CAUSES - DM - Hypertension
Choices. Patient Education. Making the treatment decision. Overview. How do you define quality of life?
 Patient Education (KEEP) Chapter 6 Making the treatment decision Objectives: 1. List the 3 main options to supplement or replace failing kidney function. 2. Review steps for each of the main kidney replacement
Patient Education (KEEP) Chapter 6 Making the treatment decision Objectives: 1. List the 3 main options to supplement or replace failing kidney function. 2. Review steps for each of the main kidney replacement
Patient Education Programme. Kidney Options Guiding you when kidneys fail
 Patient Education Programme Kidney Options Guiding you when kidneys fail About the kidneys What do healthy kidneys do? Your two kidneys work more than you realise. The kidneys remove excess body water
Patient Education Programme Kidney Options Guiding you when kidneys fail About the kidneys What do healthy kidneys do? Your two kidneys work more than you realise. The kidneys remove excess body water
Understanding Your Hemodialysis Access Options UNDERSTANDING YOUR PERITONEAL DIALYSIS OPTIONS
 Understanding Your Hemodialysis Access Options UNDERSTANDING YOUR PERITONEAL DIALYSIS OPTIONS HOW THE KIDNEYS WORK Inside each nephron, a special blood vessel called a glomerulus works like a strainer
Understanding Your Hemodialysis Access Options UNDERSTANDING YOUR PERITONEAL DIALYSIS OPTIONS HOW THE KIDNEYS WORK Inside each nephron, a special blood vessel called a glomerulus works like a strainer
Peritoneal dialysis. Overview. Preparing for dialysis. Links to sections in topic Other topics available on website
 Peritoneal dialysis This infokid topic is for parents and carers about children s kidney conditions. Visit www.infokid.org.uk to find more topics about conditions, tests & diagnosis, treatments and supporting
Peritoneal dialysis This infokid topic is for parents and carers about children s kidney conditions. Visit www.infokid.org.uk to find more topics about conditions, tests & diagnosis, treatments and supporting
3/21/2017. Solute Clearance and Adequacy Targets in Peritoneal Dialysis. Peritoneal Membrane. Peritoneal Membrane
 3/21/2017 Solute Clearance and Adequacy Targets in Peritoneal Dialysis Steven Guest MD Director, Medical Consulting Services Baxter Healthcare Corporation Deerfield, IL, USA Peritoneal Membrane Image courtesy
3/21/2017 Solute Clearance and Adequacy Targets in Peritoneal Dialysis Steven Guest MD Director, Medical Consulting Services Baxter Healthcare Corporation Deerfield, IL, USA Peritoneal Membrane Image courtesy
PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT GUIDE
 PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT GUIDE TABLE OF CONTENTS Introduction.... 3 SECTION 1: FUNDAMENTALS OF THE PRESCRIPTION.... 4 Getting Started: Patient Pathway to First Prescription.... 5 Volume
PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT GUIDE TABLE OF CONTENTS Introduction.... 3 SECTION 1: FUNDAMENTALS OF THE PRESCRIPTION.... 4 Getting Started: Patient Pathway to First Prescription.... 5 Volume
UW MEDICINE PATIENT EDUCATION. Making your treatment decision. How do you define quality of life?
 UW MEDICINE PATIENT EDUCATION Choices Making your treatment decision Class Goals 1. List the 3 main options to supplement or replace kidney function. 2. Review steps for each of the main kidney replacement
UW MEDICINE PATIENT EDUCATION Choices Making your treatment decision Class Goals 1. List the 3 main options to supplement or replace kidney function. 2. Review steps for each of the main kidney replacement
Oxford Kidney Unit. Treatment options for chronic kidney disease A brief overview
 Oxford Kidney Unit Treatment options for chronic kidney disease A brief overview You may feel well at the moment and may not have any symptoms from your kidney disease, but it is important that you understand
Oxford Kidney Unit Treatment options for chronic kidney disease A brief overview You may feel well at the moment and may not have any symptoms from your kidney disease, but it is important that you understand
Kidney Patients with Chronic Kidney Disease
 Cheshire and Merseyside Kidney Care Services Renal Replacement Therapy Options for Kidney Patients with Chronic Kidney Disease Stage 5 Renal Replacement Therapy Options for Kidney Patients with Chronic
Cheshire and Merseyside Kidney Care Services Renal Replacement Therapy Options for Kidney Patients with Chronic Kidney Disease Stage 5 Renal Replacement Therapy Options for Kidney Patients with Chronic
Renal Self Learning Package INTRODUCTION TO PERITONEAL DIALYSIS
 Renal Self Learning Package INTRODUCTION TO PERITONEAL DIALYSIS St George Hospital Renal Department, reviewed 2017 St George Hospital Renal Department RENAL SELF LEARNING PACKAGE INTRODUCTION TO PERITONEAL
Renal Self Learning Package INTRODUCTION TO PERITONEAL DIALYSIS St George Hospital Renal Department, reviewed 2017 St George Hospital Renal Department RENAL SELF LEARNING PACKAGE INTRODUCTION TO PERITONEAL
Kidney Decisions Aid
 Kidney Decisions Aid A G U I D E F O R P E O P L E W H O H A V E, O R K N O W S O M E O N E, W I T H C H R O N I C K I D N E Y D I S E A S E, A N D T O A I D I N T H E D E C I S I O N A B O U T W H I C
Kidney Decisions Aid A G U I D E F O R P E O P L E W H O H A V E, O R K N O W S O M E O N E, W I T H C H R O N I C K I D N E Y D I S E A S E, A N D T O A I D I N T H E D E C I S I O N A B O U T W H I C
Getting Knowledge About Kidney Disease
 Last Reviewed Getting Knowledge About Kidney Disease Have you been told that you have late stage kidney disease? Choose Your Lifestyle On Dialysis There are two kinds of dialysis. Dialysis can be done
Last Reviewed Getting Knowledge About Kidney Disease Have you been told that you have late stage kidney disease? Choose Your Lifestyle On Dialysis There are two kinds of dialysis. Dialysis can be done
Treatment choices for someone with Stage 5 kidney disease are:
 Information for patients about advanced kidney disease Dialysis and non-dialysis treatments DOCUMENT PREPARED FOR This information is to help you understand some key issues about dialysis; it is designed
Information for patients about advanced kidney disease Dialysis and non-dialysis treatments DOCUMENT PREPARED FOR This information is to help you understand some key issues about dialysis; it is designed
Know The Facts About Home Dialysis Choices
 Know The Facts About Home Dialysis Choices Fact Sheet www.esrdncc.org Table of Contents What are my choices for dialysis at home?...3 Why consider home hemodialysis?...4 What are the different types of
Know The Facts About Home Dialysis Choices Fact Sheet www.esrdncc.org Table of Contents What are my choices for dialysis at home?...3 Why consider home hemodialysis?...4 What are the different types of
It is important upfront to realize and believe that, like many adults,
 Kids With Kidney Disease Can Realize Their Dreams and Live Long, Normal, Productive Lives By Gordon Lore It is important upfront to realize and believe that, like many adults, children with kidney failure
Kids With Kidney Disease Can Realize Their Dreams and Live Long, Normal, Productive Lives By Gordon Lore It is important upfront to realize and believe that, like many adults, children with kidney failure
Volume Management 2/25/2017. Disclosures statement: Objectives. To discuss evaluation of hypervolemia in peritoneal dialysis patients
 Volume Management Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 14, 2017 Disclosures statement: Consultant: Allena, Becker Professional Education Grant
Volume Management Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 14, 2017 Disclosures statement: Consultant: Allena, Becker Professional Education Grant
Talking with Patients About Home Therapies
 Talking with Patients About Home Therapies Sherri L. Bresn BS, BSN, RN, CNN 1 This presentation is not intended to replace the medical diagnosis, and/or prescription for therapy as determined by a practicing
Talking with Patients About Home Therapies Sherri L. Bresn BS, BSN, RN, CNN 1 This presentation is not intended to replace the medical diagnosis, and/or prescription for therapy as determined by a practicing
HEALTHYSTART TRAINING MANUAL. Living well with Kidney Disease
 HEALTHYSTART TRAINING MANUAL Living well with Kidney Disease KIDNEY DISEASE CAN AFFECT ANYONE! 1 HEALTHYSTART PROGRAMME HEALTHYSTART is a lifestyle management programme to assist you to remain healthy
HEALTHYSTART TRAINING MANUAL Living well with Kidney Disease KIDNEY DISEASE CAN AFFECT ANYONE! 1 HEALTHYSTART PROGRAMME HEALTHYSTART is a lifestyle management programme to assist you to remain healthy
Chapter 2 Peritoneal Equilibration Testing and Application
 Chapter 2 Peritoneal Equilibration Testing and Application Francisco J. Cano Case Presentation FW, a recently diagnosed patient with CKD Stage 5, is a 6-year-old boy who has been recommended to initiate
Chapter 2 Peritoneal Equilibration Testing and Application Francisco J. Cano Case Presentation FW, a recently diagnosed patient with CKD Stage 5, is a 6-year-old boy who has been recommended to initiate
Treatment Options Not Not access
 Treatment Options Treatment options for Chronic Kidney Disease (CKD) CKD is a permanent condition. Treatment will: Help the patient feel better Not cure the disease Not make the kidneys start working again
Treatment Options Treatment options for Chronic Kidney Disease (CKD) CKD is a permanent condition. Treatment will: Help the patient feel better Not cure the disease Not make the kidneys start working again
Home Dialysis. Peritoneal Dialysis. Home Hemodialysis
 Home Dialysis The information provided is not intended to be a substitute for professional medical advice. A licensed healthcare professional should be consulted for diagnosis and treatment of any and
Home Dialysis The information provided is not intended to be a substitute for professional medical advice. A licensed healthcare professional should be consulted for diagnosis and treatment of any and
02/21/2017. Assessment of the Peritoneal Membrane: Practice Workshop. Objectives. Review of Physiology. Marina Villano, MSN, RN, CNN
 Assessment of the Peritoneal Membrane: Practice Workshop Marina Villano, MSN, RN, CNN marina.villano@fmc-na.com Objectives Briefly review normal peritoneal physiology including the three pore model. Compare
Assessment of the Peritoneal Membrane: Practice Workshop Marina Villano, MSN, RN, CNN marina.villano@fmc-na.com Objectives Briefly review normal peritoneal physiology including the three pore model. Compare
Ana Paula Bernardo. CHP Hospital de Santo António ICBAS/ Universidade do Porto
 Ana Paula Bernardo CHP Hospital de Santo António ICBAS/ Universidade do Porto Clinical relevance of hyperphosphatemia Phosphate handling in dialysis patients Phosphate kinetics in PD peritoneal phosphate
Ana Paula Bernardo CHP Hospital de Santo António ICBAS/ Universidade do Porto Clinical relevance of hyperphosphatemia Phosphate handling in dialysis patients Phosphate kinetics in PD peritoneal phosphate
The Physiology of Peritoneal Dialysis As Related To Drug Removal
 The Physiology of Peritoneal Dialysis As Related To Drug Removal Thomas A. Golper, MD, FACP, FASN Vanderbilt University Medical Center Nashville, TN thomas.golper@vanderbilt.edu Clearance By Dialysis Clearance
The Physiology of Peritoneal Dialysis As Related To Drug Removal Thomas A. Golper, MD, FACP, FASN Vanderbilt University Medical Center Nashville, TN thomas.golper@vanderbilt.edu Clearance By Dialysis Clearance
Peritoneal Dialysis: An Overview Budapest Nephrology School 2013
 Peritoneal Dialysis: An Overview Budapest Nephrology School 2013 Joanne M Bargman MD FRCPC Director, Home Peritoneal Dialysis Unit University Health Network, Toronto The Peritoneal-Vascular Interface dialysate
Peritoneal Dialysis: An Overview Budapest Nephrology School 2013 Joanne M Bargman MD FRCPC Director, Home Peritoneal Dialysis Unit University Health Network, Toronto The Peritoneal-Vascular Interface dialysate
From Peritoneal Dialysis to Hemodialysis How could we improve the transition? Th Lobbedez CHU de Caen Self Dialysis Meeting 22 May 2014
 From Peritoneal Dialysis to Hemodialysis How could we improve the transition? Th Lobbedez CHU de Caen Self Dialysis Meeting 22 May 2014 Deux grands principes concernant la DP La dialyse péritonéale doit
From Peritoneal Dialysis to Hemodialysis How could we improve the transition? Th Lobbedez CHU de Caen Self Dialysis Meeting 22 May 2014 Deux grands principes concernant la DP La dialyse péritonéale doit
Kidney Disease Treatment Options
 Page 1 Fact sheet The kidneys play a number of important roles in your body such as: extracting excess water to make urine (wee) controlling your blood pressure filtering waste products and toxins from
Page 1 Fact sheet The kidneys play a number of important roles in your body such as: extracting excess water to make urine (wee) controlling your blood pressure filtering waste products and toxins from
PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT QUICK REFERENCE GUIDE
 PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT QUICK REFERENCE GUIDE This quick reference guide will help serve as a reference tool for clinicians setting a patient s Peritoneal Dialysis (PD) prescription.
PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT QUICK REFERENCE GUIDE This quick reference guide will help serve as a reference tool for clinicians setting a patient s Peritoneal Dialysis (PD) prescription.
The CARI Guidelines Caring for Australians with Renal Impairment. Monitoring patients on peritoneal dialysis GUIDELINES
 Date written: August 2004 Final submission: July 2005 Monitoring patients on peritoneal dialysis GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Date written: August 2004 Final submission: July 2005 Monitoring patients on peritoneal dialysis GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Continuous Ambulatory Peritoneal Dialysis and Automated Peritoneal Dialysis: What, Who, Why, and How? Review and Case Study
 Advances in Peritoneal Dialysis, Vol. 33, 2017 Kunal Malhotra, Ramesh Khanna Continuous Ambulatory Peritoneal Dialysis and Automated Peritoneal Dialysis: What, Who, Why, and How? Review and Case Study
Advances in Peritoneal Dialysis, Vol. 33, 2017 Kunal Malhotra, Ramesh Khanna Continuous Ambulatory Peritoneal Dialysis and Automated Peritoneal Dialysis: What, Who, Why, and How? Review and Case Study
Who is a Candidate for Home Dialysis? Why We Chose Home Dialysis. Midwest Kidney Network September 2016
 Who is a Candidate for Home Dialysis? Why We Chose Home Dialysis Midwest Kidney Network September 2016 Goals of This Presentation Identify common misconceptions about patient candidacy for home dialysis
Who is a Candidate for Home Dialysis? Why We Chose Home Dialysis Midwest Kidney Network September 2016 Goals of This Presentation Identify common misconceptions about patient candidacy for home dialysis
Chapter 12 PERITONEAL DIALYSIS
 Chapter 12 PERITONEAL DIALYSIS B. Sunita A/P V. Bavanandan Anita Bhajan Manocha Lily Binti Mushahar Mohamad Zaimi Bin Abdul Wahab Sudhaharan Sivathasan PERITONEAL DIALYSIS 22nd Report of the SECTION 12.1:
Chapter 12 PERITONEAL DIALYSIS B. Sunita A/P V. Bavanandan Anita Bhajan Manocha Lily Binti Mushahar Mohamad Zaimi Bin Abdul Wahab Sudhaharan Sivathasan PERITONEAL DIALYSIS 22nd Report of the SECTION 12.1:
Drivers have GPS. Dialysis Patients have. Making possible personal.
 Drivers have GPS Dialysis Patients have with The Amia System with Sharesource Connectivity Platform. For step-by-step navigation of home peritoneal dialysis. Please see indications for use on the back
Drivers have GPS Dialysis Patients have with The Amia System with Sharesource Connectivity Platform. For step-by-step navigation of home peritoneal dialysis. Please see indications for use on the back
Shared Decision Making established kidney failure dialysis. Deciding what type of dialysis to choose for established kidney failure
 Shared Decision Making established kidney failure Next clinical review date March 2018 Deciding what type of to choose for established kidney failure This short decision aid is to help you decide what
Shared Decision Making established kidney failure Next clinical review date March 2018 Deciding what type of to choose for established kidney failure This short decision aid is to help you decide what
A VIDEO SERIES. living WELL. with kidney failure WHAT IS KIDNEY FAILURE?
 A VIDEO SERIES living WELL with kidney failure WHAT IS KIDNEY FAILURE? Contents 2 Introduction 11 What is a kidney transplant? 3 What will I learn? 12 What role do diet and medi- 5 Who is on my 7 healthcare
A VIDEO SERIES living WELL with kidney failure WHAT IS KIDNEY FAILURE? Contents 2 Introduction 11 What is a kidney transplant? 3 What will I learn? 12 What role do diet and medi- 5 Who is on my 7 healthcare
Starting Peritoneal Dialysis
 PD Education Booklet 1 Starting Peritoneal Dialysis What you will learn: What your kidneys do Uremia (kidney disease) and its symptoms How Peritoneal Dialysis (PD) helps The two types of PD: Automated
PD Education Booklet 1 Starting Peritoneal Dialysis What you will learn: What your kidneys do Uremia (kidney disease) and its symptoms How Peritoneal Dialysis (PD) helps The two types of PD: Automated
LLL Session - Nutritional support in renal disease
 ESPEN Congress Leipzig 2013 LLL Session - Nutritional support in renal disease Peritoneal dialysis D. Teta (CH) Nutrition Support in Patients undergoing Peritoneal Dialysis (PD) Congress ESPEN, Leipzig
ESPEN Congress Leipzig 2013 LLL Session - Nutritional support in renal disease Peritoneal dialysis D. Teta (CH) Nutrition Support in Patients undergoing Peritoneal Dialysis (PD) Congress ESPEN, Leipzig
What are my pre-dialysis options and what does this mean for me?
 What are my pre-dialysis options and what does this mean for me? Gabby Hadley CKD Community Support Team Lead Nurse Queen Elizabeth Hospital Birmingham ADPKD Information Day 18/11/17 Where do I go from
What are my pre-dialysis options and what does this mean for me? Gabby Hadley CKD Community Support Team Lead Nurse Queen Elizabeth Hospital Birmingham ADPKD Information Day 18/11/17 Where do I go from
THERE S A BIG DIFFERENCE BETWEEN SIMPLY SURVIVING AND REALLY LIVING.
 THERE S A BIG DIFFERENCE BETWEEN SIMPLY SURVIVING AND REALLY LIVING. IT S CALLED PD. Peritoneal dialysis, or PD, is a different kind of dialysis. PD is a choice that could help you feel like you re living,
THERE S A BIG DIFFERENCE BETWEEN SIMPLY SURVIVING AND REALLY LIVING. IT S CALLED PD. Peritoneal dialysis, or PD, is a different kind of dialysis. PD is a choice that could help you feel like you re living,
STARTING PERITONEAL DIALYSIS
 STARTING PERITONEAL DIALYSIS What you will learn: What your kidneys do What uremia (kidney disease) is and what the symptoms are How Peritoneal Dialysis (PD) helps What the two types of PD are: automated
STARTING PERITONEAL DIALYSIS What you will learn: What your kidneys do What uremia (kidney disease) is and what the symptoms are How Peritoneal Dialysis (PD) helps What the two types of PD are: automated
PREDICTORS OF PERITONITIS AMONG CANADIAN PERITONEAL DIALYSIS PATIENTS
 PREDICTORS OF PERITONITIS AMONG CANADIAN PERITONEAL DIALYSIS PATIENTS By Sharon J. Nessim, MD A thesis submitted in conformity with the requirements for the degree of Master of Science Graduate Department
PREDICTORS OF PERITONITIS AMONG CANADIAN PERITONEAL DIALYSIS PATIENTS By Sharon J. Nessim, MD A thesis submitted in conformity with the requirements for the degree of Master of Science Graduate Department
Drug Use in Dialysis
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
(Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
PERITONEAL DIALYSIS ADEQUACY: The KDOQI Guidelines and Beyond
 PERITONEAL DIALYSIS ADEQUACY: The KDOQI Guidelines and Beyond John Burkart, M.D. Wake Forest University Baptist Medical Center CMO Health Systems Management 8/2014 John M. Burkart, MD Educational Grants
PERITONEAL DIALYSIS ADEQUACY: The KDOQI Guidelines and Beyond John Burkart, M.D. Wake Forest University Baptist Medical Center CMO Health Systems Management 8/2014 John M. Burkart, MD Educational Grants
Immediate Start Peritoneal Dialysis Is It Really an option? Gerry Endall PD Nurse Specialist 16 TH March 2016
 4/12/2016 Page 1 Immediate Start Peritoneal Dialysis Is It Really an option? Gerry Endall PD Nurse Specialist 16 TH March 2016 4/12/2016 Page 2 Do we really need that option? Peritoneal Dialysis is a well
4/12/2016 Page 1 Immediate Start Peritoneal Dialysis Is It Really an option? Gerry Endall PD Nurse Specialist 16 TH March 2016 4/12/2016 Page 2 Do we really need that option? Peritoneal Dialysis is a well
Medical Emergencies in Dialysis Patients
 Medical Emergencies in Dialysis Patients John Anderton Consultant Renal Physician Lancashire Teaching Hospitals NHS Foundation Trust Talk Plan A Flavour of Dialysis patients Emergencies in HD patients
Medical Emergencies in Dialysis Patients John Anderton Consultant Renal Physician Lancashire Teaching Hospitals NHS Foundation Trust Talk Plan A Flavour of Dialysis patients Emergencies in HD patients
Introduction To The Peritoneal Dialysis Outcomes and Practice Pattern Study
 Introduction To The Peritoneal Dialysis Outcomes and Practice Pattern Study Western Canada PD Days Friday February 8, 2013 Vancouver, British Columbia Jeffrey Perl MD SM FRCP(C) Division of Nephrology
Introduction To The Peritoneal Dialysis Outcomes and Practice Pattern Study Western Canada PD Days Friday February 8, 2013 Vancouver, British Columbia Jeffrey Perl MD SM FRCP(C) Division of Nephrology
PD prescribing for all. QUESTION: Which approach? One size fits all or haute couture? (1) or (2)? The patient 18/03/2014.
 or (2)? The patient 18/03/2014.") PD prescribing for all Pr Max Dratwa Honorary consultant, Nephrology-Dialysis CHU Brugmann Université Libre de Bruxelles BSN 22 March 2014 QUESTION: Which approach? One size fits all or haute couture?
PD prescribing for all Pr Max Dratwa Honorary consultant, Nephrology-Dialysis CHU Brugmann Université Libre de Bruxelles BSN 22 March 2014 QUESTION: Which approach? One size fits all or haute couture?
Life Goes On. After Your Kidneys Stop Working. Put the Dialysis and Transplant Puzzle Together and Learn to Make Smart Choices About Your Care
 Life Goes On After Your Kidneys Stop Working Put the Dialysis and Transplant Puzzle Together and Learn to Make Smart Choices About Your Care Your Important Phone Numbers Doctor: Dialysis Unit: Dialysis
Life Goes On After Your Kidneys Stop Working Put the Dialysis and Transplant Puzzle Together and Learn to Make Smart Choices About Your Care Your Important Phone Numbers Doctor: Dialysis Unit: Dialysis
CHAPTER 6 PERITONEAL DIALYSIS. Neil Boudville. Hannah Dent. Stephen McDonald. Kylie Hurst. Philip Clayton Annual Report - 36th Edition
 CHAPTER 6 Neil Boudville Hannah Dent Stephen McDonald Kylie Hurst Philip Clayton 213 Annual Report - 36th Edition ANZDATA Registry 213 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis was used to treat
CHAPTER 6 Neil Boudville Hannah Dent Stephen McDonald Kylie Hurst Philip Clayton 213 Annual Report - 36th Edition ANZDATA Registry 213 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis was used to treat
Experts in all modalities The Expanding Role of PD Trends and Advances That Have Increased the Viability and Utilization of Peritoneal Dialysis
 Experts in all modalities The Expanding Role of PD Trends and Advances That Have Increased the Viability and Utilization of Peritoneal Dialysis Todd W.B. Gehr, M.D. Professor and Chairman, Division of
Experts in all modalities The Expanding Role of PD Trends and Advances That Have Increased the Viability and Utilization of Peritoneal Dialysis Todd W.B. Gehr, M.D. Professor and Chairman, Division of
Prescription Management: The Tough Cases
 Prescription Management: The Tough Cases Western Canada PD Days JOANNE M BARGMAN MD, FRCPC DIRECTOR OF THE PERITONEAL DIALYSIS PROGRAM UNIVERSITY HEALTH NETWORK A review of ancient history my recruitment
Prescription Management: The Tough Cases Western Canada PD Days JOANNE M BARGMAN MD, FRCPC DIRECTOR OF THE PERITONEAL DIALYSIS PROGRAM UNIVERSITY HEALTH NETWORK A review of ancient history my recruitment
Your life will need to change, however, and you have some big decisions to make concerning your treatment options.
 Project: Dialysis Center Educational Video Assignment: In conjunction with CAPA Production, develop a script to educate newly diagnosed kidney disease patients about their treatment options. The technical
Project: Dialysis Center Educational Video Assignment: In conjunction with CAPA Production, develop a script to educate newly diagnosed kidney disease patients about their treatment options. The technical
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
About Your Dialysis Treatment
 PATIENT & CAREGIVER EDUCATION About Your Dialysis Treatment This information explains dialysis at Memorial Sloan Kettering (MSK). Your Kidneys and Their Functions Your kidneys are 2 bean-shaped organs
PATIENT & CAREGIVER EDUCATION About Your Dialysis Treatment This information explains dialysis at Memorial Sloan Kettering (MSK). Your Kidneys and Their Functions Your kidneys are 2 bean-shaped organs
ad e quate adjective \ˈa-di-kwət\
 PD Prescriptions and Adequacy Monitoring: The Basics Fundamentals of Dialysis in Children Seattle, Washington February 27th, 2016 Colin White Steve Alexander Brad Warady Alicia Neu Franz Schaefer Bruce
PD Prescriptions and Adequacy Monitoring: The Basics Fundamentals of Dialysis in Children Seattle, Washington February 27th, 2016 Colin White Steve Alexander Brad Warady Alicia Neu Franz Schaefer Bruce
Update in Peritoneal dialysis
 Update in Peritoneal dialysis Matthew Jose MBBS, FRACP, PhD, FASN, AFRACMA Royal Hobart Hospital FACULTY OF HEALTH I pay my respects to the traditional owners of this land, the Larrakia people, and to
Update in Peritoneal dialysis Matthew Jose MBBS, FRACP, PhD, FASN, AFRACMA Royal Hobart Hospital FACULTY OF HEALTH I pay my respects to the traditional owners of this land, the Larrakia people, and to
A PATIENT S GUIDE. Author: Dr. A. Patel. Editor: Dr. A. Kadri
 A PATIENT S GUIDE Author: Dr. A. Patel Editor: Dr. A. Kadri 1 ACKNOWLEDGMENT I would like to thank all of those individuals involved in producing this educational book for patients. The printing of this
A PATIENT S GUIDE Author: Dr. A. Patel Editor: Dr. A. Kadri 1 ACKNOWLEDGMENT I would like to thank all of those individuals involved in producing this educational book for patients. The printing of this
Utopia Health Career Center, LLC. Do not distribute without permission.
 Introduction What is dialysis and a brief history. What laws govern dialysis treatments. How to ensure high quality care for patients. How to behave in a professional way. How to become certified. We don
Introduction What is dialysis and a brief history. What laws govern dialysis treatments. How to ensure high quality care for patients. How to behave in a professional way. How to become certified. We don
Strategies to Preserve the Peritoneal Membrane. Reusz GS Ist Dept of Pediatrics Semmelweis University, Budapest
 Strategies to Preserve the Peritoneal Membrane Reusz GS Ist Dept of Pediatrics Semmelweis University, Budapest Outline 1. Structure of the peritoneal membrane 2. Mechanisms of peritoneal injury 3. Signs
Strategies to Preserve the Peritoneal Membrane Reusz GS Ist Dept of Pediatrics Semmelweis University, Budapest Outline 1. Structure of the peritoneal membrane 2. Mechanisms of peritoneal injury 3. Signs
Physiology of Blood Purification: Dialysis & Apheresis. Outline. Solute Removal Mechanisms in RRT
 Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
Objectives. Certification Review Course. Peritoneal Dialysis. Peritoneal Membrane. 010e Certification Review Course: Peritoneal Dialysis - Kennedy
 Certification Review Course Peritoneal Dialysis Ray Agnello, MSN, RN, CNN Quality Management Specialist Saint Joseph s Regional Medical Center Paterson, New Jersey To provide attendees with a summarized
Certification Review Course Peritoneal Dialysis Ray Agnello, MSN, RN, CNN Quality Management Specialist Saint Joseph s Regional Medical Center Paterson, New Jersey To provide attendees with a summarized
Urgent start PD: Putting the person first
 Urgent start PD: Putting the person first Arsh Jain MD, FRCPC, MSc ADC 2019 Who can we target with urgent start PD? Late or not referred Early referral Urgent dialysis start HD catheter Facility HD Who
Urgent start PD: Putting the person first Arsh Jain MD, FRCPC, MSc ADC 2019 Who can we target with urgent start PD? Late or not referred Early referral Urgent dialysis start HD catheter Facility HD Who
Options in Renal Replacement Therapy: When, whom, which? Prof Dr. Serhan Tuğlular Marmara University Medical School Division of Nephrology
 Options in Renal Replacement Therapy: When, whom, which? Prof Dr. Serhan Tuğlular Marmara University Medical School Division of Nephrology CKD Classification Stage Description GFR (ml/min/1.73.m2) 1 Kidney
Options in Renal Replacement Therapy: When, whom, which? Prof Dr. Serhan Tuğlular Marmara University Medical School Division of Nephrology CKD Classification Stage Description GFR (ml/min/1.73.m2) 1 Kidney
St George & Sutherland Hospitals PERITONEAL DIALYSIS UNIT RENAL DEPARTMENT Workplace Instruction (Renal_SGH_WPI_097)
") PERITONEAL DIALYSIS (PD) PERITONEAL EQUILIBRATION TEST (PET) Cross references NSW Health PD2007_036 - Infection Control Policy SGH-TSH CLIN027 - Aseptic Technique - Competency and Education Requirements
PERITONEAL DIALYSIS (PD) PERITONEAL EQUILIBRATION TEST (PET) Cross references NSW Health PD2007_036 - Infection Control Policy SGH-TSH CLIN027 - Aseptic Technique - Competency and Education Requirements
THERAPEUTIC INTERVENTIONS TO PRESERVE RESIDUAL KIDNEY FUNCTION. Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle
 THERAPEUTIC INTERVENTIONS TO PRESERVE RESIDUAL KIDNEY FUNCTION Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle 1 2 Outline of Presentation Refinements in our understanding
THERAPEUTIC INTERVENTIONS TO PRESERVE RESIDUAL KIDNEY FUNCTION Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle 1 2 Outline of Presentation Refinements in our understanding
Clinical Grand Rounds BY AL ETINGER AUGUST 2015
 Clinical Grand Rounds BY AL ETINGER AUGUST 2015 The Case 51M with a PMHx of ESRD secondary to DM on peritoneal dialysis, type 1 DM, CAD s/p CABG, HFrEF s/p ICD, HTN presents with substernal chest pain.
Clinical Grand Rounds BY AL ETINGER AUGUST 2015 The Case 51M with a PMHx of ESRD secondary to DM on peritoneal dialysis, type 1 DM, CAD s/p CABG, HFrEF s/p ICD, HTN presents with substernal chest pain.
YOUR KIDNEYS AREN T WORKING PROPERLY.
 When you re born, everything works perfectly. Then something goes wrong and you ask: YOUR KIDNEYS AREN T WORKING PROPERLY. What does this mean? How can you stay healthy? HOW DO I DEAL WITH THIS? WHAT ROLE
When you re born, everything works perfectly. Then something goes wrong and you ask: YOUR KIDNEYS AREN T WORKING PROPERLY. What does this mean? How can you stay healthy? HOW DO I DEAL WITH THIS? WHAT ROLE
University Journal of Medicine and Medical Sciences
 ISSN 2455-2852 Volume 2 Issue 6 2016 Pleuroperitoneal leak (PPL) - A diagnostic dilemma resolved by peritoneal scintigraphy in a patient on continuous ambulatory peritoneal dialysis (CAPD) - A case report
ISSN 2455-2852 Volume 2 Issue 6 2016 Pleuroperitoneal leak (PPL) - A diagnostic dilemma resolved by peritoneal scintigraphy in a patient on continuous ambulatory peritoneal dialysis (CAPD) - A case report
Andrea Pizutti, LCSW Gayle Hall, BSN, RN, CNN Regional Operations Director Area Director Davita NxStage Kidney Care
 Andrea Pizutti, LCSW Regional Operations Director Davita Gayle Hall, BSN, RN, CNN Area Director NxStage Kidney Care 1 Compare and contrast Home Dialysis Therapies Describe the End Stage Renal Disease patient
Andrea Pizutti, LCSW Regional Operations Director Davita Gayle Hall, BSN, RN, CNN Area Director NxStage Kidney Care 1 Compare and contrast Home Dialysis Therapies Describe the End Stage Renal Disease patient
UW MEDICINE PATIENT EDUCATION. Hemodialysis. A treatment option for kidney disease. Treatment Options for Kidney Disease
 UW MEDICINE PATIENT EDUCATION Hemodialysis A treatment option for kidney disease Class Goals 1. Understand the purpose and care of blood access. 2. Understand the purpose and basic principles of hemodialysis.
UW MEDICINE PATIENT EDUCATION Hemodialysis A treatment option for kidney disease Class Goals 1. Understand the purpose and care of blood access. 2. Understand the purpose and basic principles of hemodialysis.
CHAPTER 12. Peritoneal Dialysis
 23rd Report of the PERITONEAL DIALYSIS CHAPTER 12 Peritoneal Dialysis Sunita Bavanandan Anita Bhajan Manocha Lily Mushahar Mohamad Zaimi Bin Abdul Wahab PERITONEAL DIALYSIS 23rd Report of the SECTION 12.1:
23rd Report of the PERITONEAL DIALYSIS CHAPTER 12 Peritoneal Dialysis Sunita Bavanandan Anita Bhajan Manocha Lily Mushahar Mohamad Zaimi Bin Abdul Wahab PERITONEAL DIALYSIS 23rd Report of the SECTION 12.1:
Abbreviated Prescribing Information
 Abbreviated Prescribing Information balance 1.5% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 2.3% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 4.25%
Abbreviated Prescribing Information balance 1.5% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 2.3% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 4.25%
NATIONAL QUALITY FORUM Renal EM Submitted Measures
 NATIONAL QUALITY FORUM Renal EM Submitted Measures Measure ID/ Title Measure Description Measure Steward Topic Area #1662 Percentage of patients aged 18 years and older with a diagnosis of CKD ACE/ARB
NATIONAL QUALITY FORUM Renal EM Submitted Measures Measure ID/ Title Measure Description Measure Steward Topic Area #1662 Percentage of patients aged 18 years and older with a diagnosis of CKD ACE/ARB
Peritoneal Dialysis. Sonia M. Astle PREREQUISITE NURSING KNOWLEDGE PROCEDURE
 PROCEDURE 121 Peritoneal Dialysis Sonia M. Astle PURPOSE: Peritoneal dialysis (PD) is used for the removal of fl uid and toxins, the regulation of electrolytes, and the management of azotemia. PREREQUISITE
PROCEDURE 121 Peritoneal Dialysis Sonia M. Astle PURPOSE: Peritoneal dialysis (PD) is used for the removal of fl uid and toxins, the regulation of electrolytes, and the management of azotemia. PREREQUISITE
Patients and Machines. NANT Annual National Symposium Wednesday March 9 th, 2011
 Patients and Machines John A Sweeny John A. Sweeny NANT Annual National Symposium Wednesday March 9 th, 2011 Caroline Helm Caroline Helm was the first homepatient in the United States. She was a patient
Patients and Machines John A Sweeny John A. Sweeny NANT Annual National Symposium Wednesday March 9 th, 2011 Caroline Helm Caroline Helm was the first homepatient in the United States. She was a patient
Disclosures. History. Case. Using the peritoneal cavity for dialysis. Background 2/4/2015 ASDIN PD in the Acute Setting- Myth or Reality?
 PD in the Acute Setting- Myth or Reality? ASDIN Scientific Meeting February 15, 2015 Disclosures Investigator: BARD, Otsuka, Shire, Gilead Grants: Amgen Consultant: Covidien, Deltanoid No disclosures for
PD in the Acute Setting- Myth or Reality? ASDIN Scientific Meeting February 15, 2015 Disclosures Investigator: BARD, Otsuka, Shire, Gilead Grants: Amgen Consultant: Covidien, Deltanoid No disclosures for
Treatment Options for Kidney Failure Living with End-Stage Renal Disease
 Treatment Options for Kidney Failure Dialysis Center Living with End-Stage Renal Disease 1887_FMech_1601.indd 25 12/29/15 10:56 AM Facing Kidney Failure Your doctor has told you that you have kidney failure,
Treatment Options for Kidney Failure Dialysis Center Living with End-Stage Renal Disease 1887_FMech_1601.indd 25 12/29/15 10:56 AM Facing Kidney Failure Your doctor has told you that you have kidney failure,
The peritoneal dialysis catheter
 The peritoneal dialysis catheter Department of Renal Medicine Patient Information Leaflet Introduction The information contained in this booklet is for: Patients who have renal failure and need a peritoneal
The peritoneal dialysis catheter Department of Renal Medicine Patient Information Leaflet Introduction The information contained in this booklet is for: Patients who have renal failure and need a peritoneal
BONE AND MINERAL METABOLISM in the PD PATIENT
 BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
Abbreviated Prescribing Information
 Abbreviated Prescribing Information balance 1.5% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 2.3% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 4.25%
Abbreviated Prescribing Information balance 1.5% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 2.3% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 4.25%
Peritoneal transport testing
 THOROUGH CRITICAL APPRAISAL www.sin-italy.org/jnonline www.jnephrol.com Peritoneal transport testing Vincenzo La Milia Nephrology and Dialysis Department, A. Manzoni Hospital, Lecco - Italy Ab s t r a
THOROUGH CRITICAL APPRAISAL www.sin-italy.org/jnonline www.jnephrol.com Peritoneal transport testing Vincenzo La Milia Nephrology and Dialysis Department, A. Manzoni Hospital, Lecco - Italy Ab s t r a
Who? Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011
 Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate
 Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate Summary. The urea reduction ratio (URR) has been rising year on year but now appears to have reached a plateau.. The URR increases the longer
Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate Summary. The urea reduction ratio (URR) has been rising year on year but now appears to have reached a plateau.. The URR increases the longer
02/27/2018. About half million people in the US with ESRD. HD is currently more prevalent than PD
 Anil S. Paramesh, MD, FACS Professor of Surgery, Urology and Pediatrics Tulane University School of Medicine Transplant Advisor, ESRD Network 13 First described in the 1920s Chronic PD initiated in 1960s
Anil S. Paramesh, MD, FACS Professor of Surgery, Urology and Pediatrics Tulane University School of Medicine Transplant Advisor, ESRD Network 13 First described in the 1920s Chronic PD initiated in 1960s