Metastatic Spinal Cord Compression
|
|
|
- Maximilian Rice
- 6 years ago
- Views:
Transcription

1 Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK
2 Introduction 2-5% of cancer patients have an episode of MSCC Initial presentation in 8% cancer patients, sometimes of unknown primary 10% of patients diagnosed with MSCC may have a second episode

3 Modes of compression Diagram from Cancer and its Management Souhami & Tobias
4 Location 60-80% thoracic* 15-30% lumbosacral <10% cervical Up to 50% have > 1 area involved *Due to natural kyphosis and the spinal cord occupying most of the intrathecal cross section
5 First symptom Pain 95% Weakness 5% Ataxia 1% Sensory loss 1%
6 Pain May be mild to begin with Lasts for more than 1-2 weeks Pain may feel like a 'band' around the chest or abdomen (radicular) Can radiate over the lower back, into the buttocks or legs
7 Motor weakness Weakness: 60-85% Tends to be symmetrical Severity greatest with thoracic mets At or above conus medularis Extensors of the upper extremities Above the thoracic spine Weakness from corticospinal dysfunction Affects flexors in the lower extremities Patients may be hyper reflexic below the lesion and have extensor plantars Greenberg, HS, Kim, JH, Posner, JB. Epidural spinal cord compression from metastatic tumor: Results with a new treatment protocol. Ann Neurol 1980; 8:361.
8 Sensory disturbance Less common than motor findings Still present in majority of cases Ascending numbness and paraesthesias Feeling unsteady on feet, having difficulty with walking, or legs giving way Numbness or 'pins and needles' in toes and fingers or over the buttocks Sensory level Saddle anaesthesia
9 Sphincter function Loss of function is late finding Problems passing urine may include difficulty controlling bladder function passing very little urine or passing none at all Constipation or problems controlling bowels Autonomic neuropathy presents usually as urinary retention Rarely sole finding
10 Impending cord compression is an oncological emergency - it may be too late if its established Need to diagnose before neurology alerts you Be alert to radicular back pain Don t wait for sensory level Low threshold for MRI Outcome related to walking at time of treatment
11
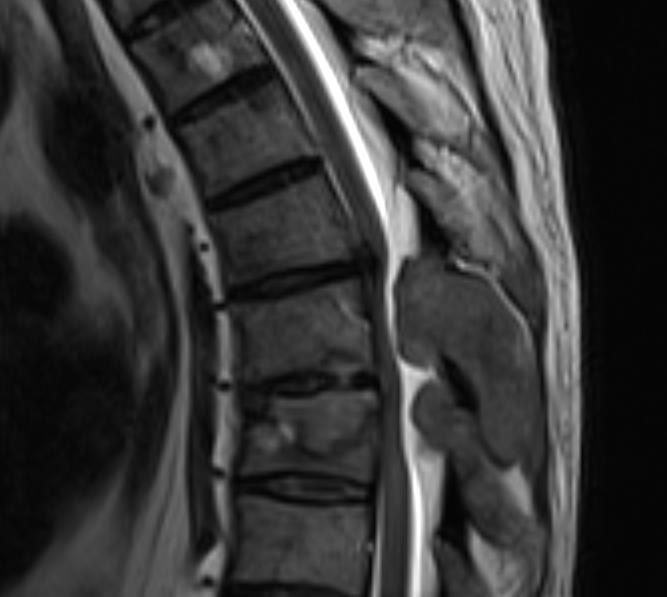
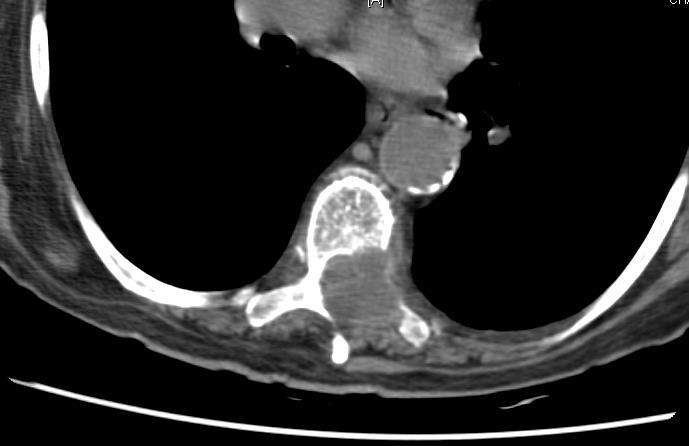
12 (Impending) cord compression on current imaging - refer for advice Imaging essential to define level MRI ideal If found on CT etc - that is fine If in doubt - phone We might treat without an MRI scan
13
14 Treatment of MSCC Steroids Steroids improve functional outcome with RT* No agreement on optimal dose/schedule More complications with higher doses Use 16 mg dexamethasone/24 hours (8mg bd) Continue during RT then taper rapidly (< 2/52) Eg. 8 mg od 3/7, 4 mg od 3/7, 2 mg od 3/7, stop? * Sorensen et al Eur J Cancer 1994; 30A:22-27
15 Steroid side effects GI ulcers / bleeding / perforation Psychosis Osteoporosis / fractures Proximal myopathy Skin thinning / ulcers Diabetes
16 Reducing Steroid regimen for Day Spinal Cord Compression Dexamethasone daily dose Administration mg 16mg OD or 8mg BD (8am & 12noon) 4-6 8mg 8mg OD 7-9 4mg 4mg OD mg 2mg OD 13 Discontinue While the patient is on steroids commence PPI (e.g. Lansoprazole) for gastric protection. A slower reducing regimen may be required for patients who have received previous courses of steroids.
17 Treatment of MSCC Surgery + RT vs RT alone Patchell et al Proc Am Soc Clin Oncol 21:1, 2003 (abstr 2) Regine WF, Tibbs PA, Young A, et al. Int J Radiat Oncol Biol Phys 2003; 57 (suppl 2): S125 Randomised trial Decompressive surgery + RT vs RT alone 30 Gy in 10# both arms 101 patients (terminated at 50% accrual) Median ambulation 126 v 35 days (p=0.006) 3/16 (19%) v 9/16 (58%) paraparetic pts regained ambulation Better pain control Trend toward better survival with surgery (p=0.08)

18 RT is the treatment of choice for some cord compressions but oncologists need to think of spinal surgery first
19 ECOG (WHO) PS 0 Fully active and able to carry out pre-disease activities without restriction 1 Restricted in strenuous activity but ambulatory and able to carry out light work 2 Ambulatory and self-caring, but unable to do light work. Up and about more than 50% of the time 3 Limited self care. In bed for more than 50% of the time 4 Unable to self care. Confined to bed or chair
20 Prognosis? Two best predictors probably History of the cancer in that patient Nick factor - from the end of the bed
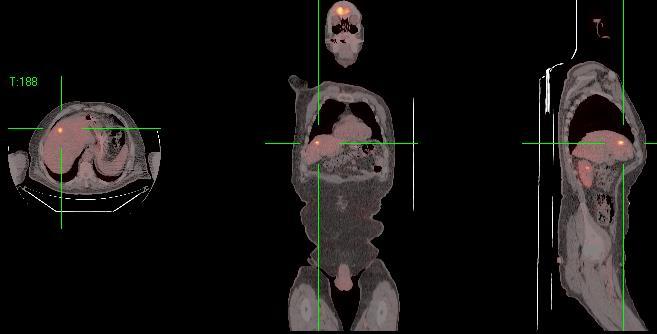
21 Oligometastases A few metastases - <5? May be picked up much earlier than in the past with new imaging eg PET-CT Stage migration - everyone a winner Means we are seeing a different population with metastatic disease who need innovative approaches
22
23 Prognosis Good: ambulatory, radiosensitive, 1 level of compression Not good: multiple levels, brain/liver mets, lung cancer, etc
24 Prognosis Median survival historically 3-6 months Recurrence occurs in 10-25% of patients Recurrence in 50% of 2 year survivors; nearly all 3-year survivors
25 Ambulation post RT Deficit before RT Ambulatory after RT Ambulatory 92% Assistance needed 65% Paraparetic 43% Paraplegic 14%





26 Radiotherapy Technical capabilities have advanced more than our biological knowledge Can put RT dose (not DXT) exactly where you want it


27 Radiotherapy for MSCC Palliative - often need to be quick and simple High dose per fraction as not so concerned about late effects eg 8/1, 20/5, 30/10 Solitary metastases?


28 Radiotherapy for MSCC No limit to radiation dose An excellent pain killer Can help preserve continence
29 Solitary metastasis


 Treat (2 min) Move")
30 What does RT for MSCC entail? Move patient from bed to hard CT couch Scan (or simulate) Move patient back to bed 1hr calculation time Move patient from bed to hard Linac couch Align (5 min) Treat (2 min) Move patient back to bed



31 Need to know about your AOS No perfect patient selection tool - but patient selection is the most important decision Radiotherapy technically advanced, biologically limited but a good painkiller
32 The ideal pathway Patient with metastatic cancer knows of warning symptoms Warning symptoms spotted by patient - contacts coordinator MRI within a few days - shows cord comp Oncologist alerted - liases with spinal surgeon as appropriate RT starts that day within clinical trial (SCORAD) Remains an outpatient
33
34

35 We can and do give out of hours RT but it takes some organising 8.30am - 8pm Mon-Fri On call Sat 9-5 On call Sun 9-1
36 We can give radiotherapy more than once Balance of potential benefits and risks May well be worth re-treatment RT is worth repeating if it worked before and you are likely to do more good than harm
37 Other considerations Bed rest V mobilisation Rehabilitation Braces & collars Psychological issues Urinary catheter Bowel function Nutrition Discharge issues
38 Constipation Factors Autonomic dysfunction Limited mobility Opiate analgesic Risk of perforation Masked by corticosteroids Bowel regimen needed
39 Anticoagulation High tumour burden Possible value in prophylaxis against VTE If patient not mobile subcutaneous low molecular weight heparin
40 Best Supportive Care Once neurological function lost, recovery unlikely. If disease elsewhere is advanced, may be appropriate not to treat actively. Steroids, physiotherapy, analgesia, good nursing care
41 Multidisciplinary care Rehabilitation Nursing care pressure sores Personal dignity - Lack of autonomy End stage of illness If discharge planned, OT/PT and SW input Keeping patient and family informed Financial assistance (DS1500) Gold Standards Framework
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Recognition & Treatment of Malignant Spinal Cord Compression
 Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Malignant Spinal cord Compression. Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania
 Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE
 THE CHRISTIE, GREATER MANCHESTER & CHESHIRE") PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
Management of Acute Oncological emergencies
 Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Spinal Cord Compression Diagnosis and Management. Information for Shared Care Centres and Community Staff
 Reference: CG1412 Written by: Dr Daniel Yeomanson Peer reviewer Dr Jeanette Payne Approved: August 2016 Approved by D&TC: 10 th June 2016 Review Due: August 2019 Intended Audience This document contains
Reference: CG1412 Written by: Dr Daniel Yeomanson Peer reviewer Dr Jeanette Payne Approved: August 2016 Approved by D&TC: 10 th June 2016 Review Due: August 2019 Intended Audience This document contains
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION
 CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway
 Clinical guidelines and pathway") Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Update on Management of Malignant Spinal Cord Compression. Heino Hugel Consultant in Palliative Medicine University Hospital Aintree
 Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Spinal cord compression as a first presentation of cancer: A case report
 J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
CP80 Version: V01. Acute Oncology Management Service Date approved: 8 th May 2015 Date ratified: 1 st June 2015 Review date: 1 st June 2017
 STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator
 Clinical Advisor Coordinator") Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
Suspected spinal cord compression form
 Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Rehabilitation and Metastatic Spinal Cord Compression
 Rehabilitation and Metastatic Spinal Cord Compression Pradeep Thumbikat MS, MSc, FRCS Consultant in Spinal Cord Injuries Sheffield Teaching Hospitals 1 Evidence for Rehabilitation Differences and similarities
Rehabilitation and Metastatic Spinal Cord Compression Pradeep Thumbikat MS, MSc, FRCS Consultant in Spinal Cord Injuries Sheffield Teaching Hospitals 1 Evidence for Rehabilitation Differences and similarities
Radiotherapy for lymphoma
 Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
Palliative Care Emergencies
 Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
The Role of Radiotherapy in Metastatic Breast Cancer. Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health
 The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Guidelines for the Management. Malignant Spinal Cord Compression. Final Guideline
 Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Spinal cord compression: what it means and how it can be treated
 Spinal cord compression: what it means and how it can be treated Patient Information Oncology Department Author ID: Acute Oncology Nurse Specialist Leaflet Number: CC 036 Version: 2.1 Name of Leaflet:
Spinal cord compression: what it means and how it can be treated Patient Information Oncology Department Author ID: Acute Oncology Nurse Specialist Leaflet Number: CC 036 Version: 2.1 Name of Leaflet:
Spinal cord compression
 Spinal cord compression Urology Department Patient Information Leaflet Introduction If you have been diagnosed with cancer, you need to know about spinal cord compression and the warning signs. This leaflet
Spinal cord compression Urology Department Patient Information Leaflet Introduction If you have been diagnosed with cancer, you need to know about spinal cord compression and the warning signs. This leaflet
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression. Tuesday 17 th September 2013
 Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
AND CHEMOTHERAPY IN PALLIATIVE CARE
 THE ROLE OF RADIOTHERAPY AND CHEMOTHERAPY IN PALLIATIVE CARE Top Ten Cancers in Public Hospital KNH 2008 (CTC) Multidisciplinary Approach Radiotherapist Radiologist Medical Oncologist PALLIATIVE CARE/ONCOLOGY
THE ROLE OF RADIOTHERAPY AND CHEMOTHERAPY IN PALLIATIVE CARE Top Ten Cancers in Public Hospital KNH 2008 (CTC) Multidisciplinary Approach Radiotherapist Radiologist Medical Oncologist PALLIATIVE CARE/ONCOLOGY
Developing spinal cord compression care guidelines at WPH
 Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Dr Bernie Foran, Suzanne Hodson, Liz Kirkham, Rebecca Mills, Jan Siddall, Rebecca Walsh,
Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Dr Bernie Foran, Suzanne Hodson, Liz Kirkham, Rebecca Mills, Jan Siddall, Rebecca Walsh,
A new score predicting the survival of patients with spinal cord compression from myeloma
 Douglas et al. BMC Cancer 2012, 12:425 RESEARCH ARTICLE Open Access A new score predicting the survival of patients with spinal cord compression from myeloma Sarah Douglas 1, Steven E Schild 2 and Dirk
Douglas et al. BMC Cancer 2012, 12:425 RESEARCH ARTICLE Open Access A new score predicting the survival of patients with spinal cord compression from myeloma Sarah Douglas 1, Steven E Schild 2 and Dirk
Emergency Neurological Life Support Spinal Cord Compression
 Emergency Neurological Life Support Spinal Cord Compression Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Spinal Cord Compression Table of Contents Emergency Neurological Life Support...
Emergency Neurological Life Support Spinal Cord Compression Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Spinal Cord Compression Table of Contents Emergency Neurological Life Support...
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Developing spinal cord compression care guidelines at WPH
 Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Bernie Foran, Suzanne Hodson, Jane Mason, Rebecca Mills, Jan Siddall, Rebecca Walsh, Clare
Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Bernie Foran, Suzanne Hodson, Jane Mason, Rebecca Mills, Jan Siddall, Rebecca Walsh, Clare
42 y/o woman with unwitnessed episode of loss of consciousness and urinary incontinence
 Top Five Neurological Emergencies: When To Refer February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 CASE 1 42 y/o woman with unwitnessed episode
Top Five Neurological Emergencies: When To Refer February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 CASE 1 42 y/o woman with unwitnessed episode
Suspecting Tumors, or Could it be cancer?
 Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
A prospective study of patients with impending spinal cord compression treated with palliative radiotherapy alone
 A prospective study of patients with impending spinal cord compression treated with palliative radiotherapy alone Item Type Article Authors O'Sullian, L.;Clayton-Lea, A.;McArdle, O.;McGarry, M.;Kenny,
A prospective study of patients with impending spinal cord compression treated with palliative radiotherapy alone Item Type Article Authors O'Sullian, L.;Clayton-Lea, A.;McArdle, O.;McGarry, M.;Kenny,
Metastatic spinal cord compression (MSCC) What happens? MSCC. MSCC is a palliative care emergency. Signs/symptoms
 What happens? MSCC. MSCC is a palliative care emergency. Signs/symptoms") A patient with suspected metastatic spinal cord compression and the dilemma of non-resident status Sandra Notley CNS-Palliative Care 1 Metastatic spinal cord compression (MSCC) Is indentation, displacement
A patient with suspected metastatic spinal cord compression and the dilemma of non-resident status Sandra Notley CNS-Palliative Care 1 Metastatic spinal cord compression (MSCC) Is indentation, displacement
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
agreed MSCC pathways and guidelines).
.") Referral of Patients with Spinal Metastatic Disease and Suspected Metastatic Spinal Cord Compression (to be used in association with locally West Midlands Clinical Networks and Clinical Senate Coversheet
Referral of Patients with Spinal Metastatic Disease and Suspected Metastatic Spinal Cord Compression (to be used in association with locally West Midlands Clinical Networks and Clinical Senate Coversheet
Palliative treatments for lung cancer: What can the oncologist do?
 Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
DOCTOR DISCUSSION GUIDE
 DOCTOR DISCUSSION GUIDE BE PREPARED For the best outcome from a visit with your doctor, it s important to be prepared. The more completely and clearly you describe the pain you re experiencing, the easier
DOCTOR DISCUSSION GUIDE BE PREPARED For the best outcome from a visit with your doctor, it s important to be prepared. The more completely and clearly you describe the pain you re experiencing, the easier
Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH
 Document Control Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH Author Author s job title Consultant T&O Directorate Scheduled Care Department
Document Control Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH Author Author s job title Consultant T&O Directorate Scheduled Care Department
Disclosures. Disclosures 27/01/2019. Modern approach and pitfalls in metastatic spine surgery. None.. Jeremy Reynolds
 Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures
 Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Analysis of Malignant Spinal Cord Compression Patients Treated In a Radiotherapy Centre
 Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2013; 1(6):906-910 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2013; 1(6):906-910 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Dorsal root ganglion block / Transforaminal epidural / Nerve root block
 Information sheet for adult patients undergoing: Dorsal root ganglion block / Transforaminal epidural / Nerve root block What is the aim of this information sheet? for the Treatment of Pain The aim of
Information sheet for adult patients undergoing: Dorsal root ganglion block / Transforaminal epidural / Nerve root block What is the aim of this information sheet? for the Treatment of Pain The aim of
Palliative Care Emergencies
 Palliative Care Emergencies Dr. T. Thirukkumaran Palliative Care Services Northwest Tasmania What are the emergencies in Palliative Medicine? Palliative Emergencies (a) Disease related or Symptom related
Palliative Care Emergencies Dr. T. Thirukkumaran Palliative Care Services Northwest Tasmania What are the emergencies in Palliative Medicine? Palliative Emergencies (a) Disease related or Symptom related
Cancer of Unknown Primary Service
 Cancer of Unknown Primary Service Dr Maurice Fernando Consultant In Specialist Palliative Care and CUP lead Doncaster and Bassetlaw Hospitals NHS FT Wakefield meeting -14-07-2016 CUP service CUP MDT
Cancer of Unknown Primary Service Dr Maurice Fernando Consultant In Specialist Palliative Care and CUP lead Doncaster and Bassetlaw Hospitals NHS FT Wakefield meeting -14-07-2016 CUP service CUP MDT
INJECTION FOR YOUR BACK & NECK
 INJECTION FOR YOUR BACK & NECK CERVICAL EPIDURAL CERVICAL FACET BLOCKS LUMBAR EPIDURAL FACET BLOCKS ROOT BLOCKS INJECTIONS FOR YOUR BACK A lumbar caudal epidural steroid injection is an outpatient procedure
INJECTION FOR YOUR BACK & NECK CERVICAL EPIDURAL CERVICAL FACET BLOCKS LUMBAR EPIDURAL FACET BLOCKS ROOT BLOCKS INJECTIONS FOR YOUR BACK A lumbar caudal epidural steroid injection is an outpatient procedure
HISTORY PAPERWORK FOR APPOINTMENTS WITH DAVID A. PROPST, D.O.
 HISTORY PAPERWORK FOR APPOINTMENTS WITH DAVID A. PROPST, D.O. Name: Age: Room Number: Sex: MALE or FEMALE Dominant Hand: RIGHT or LEFT Height Weight Blood pressure HISTORY 1. Did your first symptoms begin
HISTORY PAPERWORK FOR APPOINTMENTS WITH DAVID A. PROPST, D.O. Name: Age: Room Number: Sex: MALE or FEMALE Dominant Hand: RIGHT or LEFT Height Weight Blood pressure HISTORY 1. Did your first symptoms begin
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
North West London Trauma Network Spinal Pathway and Protocols
 North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
Benefits of Radiation Therapy in the Palliative Cancer Patient
 Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Standard care plan for Prophylactic Cranial Irradiation for Limited Stage (stage I-III) Small Cell Lung Cancer (25Gy in 10 fractions) References
 Small Cell Lung Cancer (25Gy in 10 fractions) References") CHEMOTHERAPY CARE PLAN Document Title: Document Type: Subject: Approved by: Prophylactic Cranial Irradiation for Limited-stage Small Cell Lung Cancer (20Gy in 5 fractions) Clinical Guideline Standard Care
CHEMOTHERAPY CARE PLAN Document Title: Document Type: Subject: Approved by: Prophylactic Cranial Irradiation for Limited-stage Small Cell Lung Cancer (20Gy in 5 fractions) Clinical Guideline Standard Care
Integrating Pain Metrics into Oncologic Clinical and Regulatory Decision-Making. Charles Cleeland MD Anderson Cancer Center
 Integrating Pain Metrics into Oncologic Clinical and Regulatory Decision-Making Charles Cleeland MD Anderson Cancer Center Panelists Charles Cleeland, Department Chair, Department of Symptom Research,
Integrating Pain Metrics into Oncologic Clinical and Regulatory Decision-Making Charles Cleeland MD Anderson Cancer Center Panelists Charles Cleeland, Department Chair, Department of Symptom Research,
Disclosure. Thoracolumbar Tumors. Intraspinal Tumor Removal Options 6/4/2011. Minimally Invasive Approaches for Spinal Tumors
 Minimally Invasive Approaches for Spinal Tumors Praveen V. Mummaneni, M.D. Disclosure Medtronic (Consultant, Grants) DePuy (Consultant, Other Financial Support) Associate Professor Dept. of Neurosurgery
Minimally Invasive Approaches for Spinal Tumors Praveen V. Mummaneni, M.D. Disclosure Medtronic (Consultant, Grants) DePuy (Consultant, Other Financial Support) Associate Professor Dept. of Neurosurgery
Patient Treatment Date/time: Diagnosis: Treatment Regimen:
 Name: Address: DOB: HCRN: Consultant: Ward: Assessment: Pre Systematic Anti Cancer Therapy (SACT) Continuation *This assessment is for patients on multiday regimens Patient Treatment Date/time: Diagnosis:
Name: Address: DOB: HCRN: Consultant: Ward: Assessment: Pre Systematic Anti Cancer Therapy (SACT) Continuation *This assessment is for patients on multiday regimens Patient Treatment Date/time: Diagnosis:
Cancer Survivorship NEURO-ONCOLOGY PATIENT SURVIVORSHIP PLAN. Resources and Tools for the Multidisciplinary Team
 NEURO-ONCOLOGY PATIENT SURVIVORSHIP PLAN Cancer Survivorship Resources and Tools for the Multidisciplinary Team Your survivorship care plan is a summary of your tumor treatments and recommendations for
NEURO-ONCOLOGY PATIENT SURVIVORSHIP PLAN Cancer Survivorship Resources and Tools for the Multidisciplinary Team Your survivorship care plan is a summary of your tumor treatments and recommendations for
Emergencies in Palliative Medicine
 Emergencies in Palliative Medicine Objectives Recognise palliative care emergencies Be aware of their existence Recognise signs and symptoms of common emergencies Anticipate occurrence of emergencies Manage
Emergencies in Palliative Medicine Objectives Recognise palliative care emergencies Be aware of their existence Recognise signs and symptoms of common emergencies Anticipate occurrence of emergencies Manage
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Jackie Turnpenney Version: Accountable Committee:
BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Jackie Turnpenney Version: Accountable Committee:
Open repair of Abdominal Aortic Aneurysms (AAA)
") Open repair of Abdominal Aortic Aneurysms (AAA) Exceptional healthcare, personally delivered Ask 3 Questions Preparation for your Appointments We want you to be active in your healthcare. By telling us
Open repair of Abdominal Aortic Aneurysms (AAA) Exceptional healthcare, personally delivered Ask 3 Questions Preparation for your Appointments We want you to be active in your healthcare. By telling us
The surgical treatment of metastatic disease of the spine
 The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
Difficult Diagnosis: Case History. 7 months prior, she happened to have undergone a C-spine MRI after a car accident
 Relevant Disclosures: None Difficult Diagnosis: Recent Advances in Neurology 2013 Jeffrey M. Gelfand, MD Assistant Professor UCSF Neuroinflammation and MS Center UCSF Department of Neurology Case History
Relevant Disclosures: None Difficult Diagnosis: Recent Advances in Neurology 2013 Jeffrey M. Gelfand, MD Assistant Professor UCSF Neuroinflammation and MS Center UCSF Department of Neurology Case History
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
Radiotherapy in oncological emergencies. Is it still a mainstay?
 Radiotherapy in oncological emergencies. Is it still a mainstay? Paweł Potocki, MD Jagiellonian University Medical College Kraków University Hospital Departament of Clinical Oncology ppotocki@su.krakow.pl
Radiotherapy in oncological emergencies. Is it still a mainstay? Paweł Potocki, MD Jagiellonian University Medical College Kraków University Hospital Departament of Clinical Oncology ppotocki@su.krakow.pl
Gamma Knife Radiosurgery A tool for treating intracranial conditions. CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop
 Gamma Knife Radiosurgery A tool for treating intracranial conditions CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop ANGELA McBEAN Gamma Knife CNC State-wide Care Coordinator Gamma Knife
Gamma Knife Radiosurgery A tool for treating intracranial conditions CNSA Annual Congress 2016 Radiation Oncology Pre-congress Workshop ANGELA McBEAN Gamma Knife CNC State-wide Care Coordinator Gamma Knife
The in-hospital management of COPD-exacerbation includes three core processes:
 Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Appendix 1A. Process flow for in-hospital management of COPDexacerbation The in-hospital management of COPD-exacerbation includes three core processes: 1. Diagnostic assessment 2. Pharmacological management
Thoracic Recurrences. Soft tissue recurrence
 Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Spinal injury. Structure of the spine
 Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Palliative RT. Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University
 Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Epidural steroid injection
 Information sheet for adult patients undergoing: Epidural steroid injection for the Treatment of Pain What is the aim of this information sheet? The aim of this information sheet is to provide you with
Information sheet for adult patients undergoing: Epidural steroid injection for the Treatment of Pain What is the aim of this information sheet? The aim of this information sheet is to provide you with
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Treating your abdominal aortic aneurysm by open repair (surgery)
") Patient information Abdominal aortic aneurysm open surgery Treating your abdominal aortic aneurysm by open repair (surgery) Introduction This leaflet tells you about open repair of abdominal aortic aneurysm,
Patient information Abdominal aortic aneurysm open surgery Treating your abdominal aortic aneurysm by open repair (surgery) Introduction This leaflet tells you about open repair of abdominal aortic aneurysm,
9:00-9:10 am Metastatic Epidural Cervical Spinal Cord Compression CSRS San Diego, 2015 Michael G. Fehlings, MD
 9:00-9:10 am Metastatic Epidural Cervical Spinal Cord Compression CSRS San Diego, 2015 Michael G. Fehlings, MD 1 BACKGROUND After the lungs and the liver, metastases most frequently arise in osseous tissues;
9:00-9:10 am Metastatic Epidural Cervical Spinal Cord Compression CSRS San Diego, 2015 Michael G. Fehlings, MD 1 BACKGROUND After the lungs and the liver, metastases most frequently arise in osseous tissues;
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested is: Please check the indication (reason) for this procedure
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested is: Please check the indication (reason) for this procedure
Evaluation for Epilepsy Surgery
 Evaluation for Epilepsy Surgery What is pre-surgery evaluation? Surgery is one of the therapies to treat epilepsy. In order to decide if surgery will be helpful for you, your doctor needs to evaluate the
Evaluation for Epilepsy Surgery What is pre-surgery evaluation? Surgery is one of the therapies to treat epilepsy. In order to decide if surgery will be helpful for you, your doctor needs to evaluate the
Bone metastases of solid tumors Diagnosis and management by
 Bone metastases of solid tumors Diagnosis and management by Dr/RASHA M Abd el Motagaly oncology consultant Nasser institute adult oncology unit 3/27/2010 1 Goals 1- Know the multitude of problem of bone
Bone metastases of solid tumors Diagnosis and management by Dr/RASHA M Abd el Motagaly oncology consultant Nasser institute adult oncology unit 3/27/2010 1 Goals 1- Know the multitude of problem of bone
Stereotactic Ablative Body Radiotherapy for Spinal Metastases using CyberKnife UHB is a no smoking Trust
 Stereotactic Ablative Body Radiotherapy for Spinal Metastases using CyberKnife UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Stereotactic Ablative Body Radiotherapy for Spinal Metastases using CyberKnife UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
The research questions are presented in priority order, and are further elaborated with lay summaries and three-part questions where applicable.
 Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Lumbar Disc Prolapse. Dr. Ahmed Salah Eldin Hassan. Professor of Neurosurgery & Consultant spinal surgeon
 Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Interventions for the treatment of metastatic extradural spinal cord compression in adults (Review)
") Interventions for the treatment of metastatic extradural spinal cord compression in adults (Review) George R, Jeba J, Ramkumar G, Chacko AG, Leng M, Tharyan P This is a reprint of a Cochrane review, prepared
Interventions for the treatment of metastatic extradural spinal cord compression in adults (Review) George R, Jeba J, Ramkumar G, Chacko AG, Leng M, Tharyan P This is a reprint of a Cochrane review, prepared
bone HEALTH IN FOCUS UNDERSTANDING THE IMPORTANCE OF BONE HEALTH WHEN LIVING WITH METASTATIC BREAST CANCER
 bone HEALTH IN FOCUS UNDERSTANDING THE IMPORTANCE OF BONE HEALTH WHEN LIVING WITH METASTATIC BREAST CANCER IF YOU VE BEEN DIAGNOSED WITH METASTATIC BREAST CANCER (ALSO KNOWN AS STAGE IV BREAST CANCER),
bone HEALTH IN FOCUS UNDERSTANDING THE IMPORTANCE OF BONE HEALTH WHEN LIVING WITH METASTATIC BREAST CANCER IF YOU VE BEEN DIAGNOSED WITH METASTATIC BREAST CANCER (ALSO KNOWN AS STAGE IV BREAST CANCER),
TOTAL HIP ARTHROPLASTY (Total Hip Replacement)
") (Total Hip Replacement) The Hip Joint The hip is a ball and socket joint. The joint is formed by the head of the femur (thighbone) and the acetabulum (pelvis). The bones are coated in cartilage, which
(Total Hip Replacement) The Hip Joint The hip is a ball and socket joint. The joint is formed by the head of the femur (thighbone) and the acetabulum (pelvis). The bones are coated in cartilage, which
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
A Patient s Guide to Intraoperative Monitoring
 A Patient s Guide to Intraoperative Monitoring 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Intraoperative Monitoring 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Paul Allan Regional Clinical Lead - South. Lumbar Spine. Assessment & Differential Diagnosis
 Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
Nursing the spinal patient
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Nursing the spinal patient Author : Lisa Thompson Categories : RVNs Date : November 1, 2009 Lisa Thompson DipAVN(surg), looks
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Nursing the spinal patient Author : Lisa Thompson Categories : RVNs Date : November 1, 2009 Lisa Thompson DipAVN(surg), looks
3/3/2016. International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI)
") International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
Red Flags for serious spinal pathology: A collaborative approach
 Red Flags for serious spinal pathology: A collaborative approach Professor James Selfe DSc, PhD, MA, GD Phys (Distinction), FCSP Serious Spinal Pathology Background Collaboration Communication Solutions
Red Flags for serious spinal pathology: A collaborative approach Professor James Selfe DSc, PhD, MA, GD Phys (Distinction), FCSP Serious Spinal Pathology Background Collaboration Communication Solutions
Malignant epidural spinal cord compression: the role of external beam radiotherapy
 REVIEW C URRENT OPINION Malignant epidural spinal cord compression: the role of external beam radiotherapy Tanya Holt a, Peter Hoskin b, Ernesto Maranzano c, Arjun Sahgal d, Steven E. Schild e, Samuel
REVIEW C URRENT OPINION Malignant epidural spinal cord compression: the role of external beam radiotherapy Tanya Holt a, Peter Hoskin b, Ernesto Maranzano c, Arjun Sahgal d, Steven E. Schild e, Samuel
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Facet Injection Please check the indication (reason)
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Facet Injection Please check the indication (reason)
A Case of Metastatic Lung Adenocarcinoma EGFR ve, ALK +
 ESMO Preceptorship Programme Dr Najihah Abu Bakar University Malaya Medical Centre, Kuala Lumpur, Malaysia A Case of Metastatic Lung Adenocarcinoma EGFR ve, ALK + HISTORY Mr TT/ 65yo/ Male/ Non smoker/no
ESMO Preceptorship Programme Dr Najihah Abu Bakar University Malaya Medical Centre, Kuala Lumpur, Malaysia A Case of Metastatic Lung Adenocarcinoma EGFR ve, ALK + HISTORY Mr TT/ 65yo/ Male/ Non smoker/no