DEMENTIA. Szabolcs Szatmári. Tg. Mureş Marosvásárhely Romania 4/18/ :59 AM
|
|
|
- Dinah Glenn
- 5 years ago
- Views:
Transcription

1 DEMENTIA Szabolcs Szatmári Tg. Mureş Marosvásárhely Romania
2
3 Dementia from Latin de- "apart, away" + mens (genitive mentis) "mind"
4
5 MORE GRAY HAIR AND LESS GRAY MATTER Daryl R. Gress
6 Cognitive decline minor neurocognitive disorder major neurocognitive disorder PREDEMENTIA DEMENTIA

7 DSM-IV criteria for the diagnosis of dementia The development of multiple cognitive deficits manifested by both memory impairment and at least one of the following: aphasia apraxia agnosia executive dysfunction causing significant impairment in social or occupational functioning and which do not exclusively occur during delirium
8 CAUSES OF DEMENTIA INTRACRANIAL: DEGENERATIV: Alzheimer, Pick, Lewy, Parkinson, Huntington, VASCULAR, POST-STROKE TUMORS, POST-TRAUMATIC, Tumor, metastasis, subdural haematoma, hydrocephalus INFECTIONS AIDS, prion: Creutzfeldt-Jakob, PESS, neurosyphilis, Lyme, meningitis
9 CAUSES OF DEMENTIA EXTRACRANIAL: INTOXICATIONS Alcohol, drogs, CO GENETIC Wilson ORGAN INSUFF. liver, renal failure, cardiac, thyroid DEFICIENCY STATES B12, folate
10
11 When to assess the patient for cognitive impairment? memory complaints family alerted other diseases (hospitalized elderly patients) sent by the family doctor screening!!!
12 Minimal program for investigation of cognitive impairment anamnesis and heteroanamnesis general exam neurological exam psychiatric exam Mini Mental State Examination and/or other short cognitive test laboratory tests CT or MRI REPEAT IF NECESSARY DEPENDING ON THE EVOLUTION!!!
13 DSM-IV criteria for the diagnosis of dementia The development of multiple cognitive deficits manifested by both memory impairment and at least one of the following: aphasia apraxia agnosia executive dysfunction causing significant impairment in social or occupational functioning and which do not exclusively occur during delirium
14 History, anamnesis, heteroanamnesis: risk factors: alcohol, hypertension, stroke, diabetes mellitus, atrial fibrillation, dislipidemia head trauma depression dementia in the family
15 History, anamnesis, heteroanamnesis: activity of daily living: alimentation, washing, dressing, shopping, handling money, orientation, accommodation incontinency urine, fecal emotional education, prior level of knowledge
16 Questions to ask family members about patients with memory problems Can you give some examples of times when the patient had trouble with memory? Does he or she have trouble remembering names or faces of familiar people? Has he or she got lost while driving or walking in familiar areas?
17 Questions to ask family members to determine the nature of cognitive impairment in patients with memory loss Aphasia Does the patient: have any difficulties with finding the right word to say? use frequently what-d ye-call-it instead of names? break off in midsentence? use circumlocutions in his/her speech?
18 Questions to ask family members to determine the nature of cognitive impairment in patients with memory loss Apraxia Does he or she have any difficulty with: dressing or bathing alone? using a brush or comb? feeding himself or herself?
19 Questions to ask family members to determine the nature of cognitive impairment in patients with memory loss Agnosia Does he or she have any trouble recognizing: familiar people or places? familiar objects or personal items?
20 Executive dysfunction Has he or she had any difficulty understanding what is going on around him or her, such as following a church activity or planning an upcoming event? Has he or she had any problems figuring out how to use familiar objects, such as appliances or tools, or how to operate with new devices, such as a new television remote control or microwave oven?
21 Minimal program for investigation of cognitive impairment anamnesis and heteroanamnesis general exam neurological exam psychiatric exam Mini Mental State Examination and/or other short cognitive test laboratory tests CT or MRI REPEAT IF NECESSARY DEPENDING ON THE EVOLUTION!!!
22 Maximum score Score Orientation 5 What is the (year) (season) (date) (day) (month)? 5 Where are we: (state) (county) (town or city) (hospital) (floor)? Registration 3 Name three common objects (e.g., "apple," "table," "penny"): Attention and calculation 5 Spell "world" backwards. The score is the number of letters in correct order. (D L R O W ) Recall 3 Ask for the three objects repeated above. Language 2 Name a "pencil" and "watch." Repeat the following: "No ifs ands or buts." 1 Follow a three-stage command: 3 "Take a paper in your right hand, fold it in half and put it on the floor." 1 Close your eyes. 1 Write a sentence. 1 Mini-Mental State Examination Folstein MF, Folstein SE, McHugh PR 1975 Copy the following design. Total score

23 Clock Drawing Test "Without looking at your watch, draw the face of a clock, and mark the hands to show 10 minutes to 11:00." This task requires intact memory, visuospatial skills, and executive functioning. Scoring: the clock numbers are generally intact (6 to 10 points) not intact (1 to 5 points). a score of 5 or less is suggestive of dementia
24
25
26
27 Minimal program for investigation of cognitive impairment anamnesis and heteroanamnesis general exam neurological exam psychiatric exam Mini Mental State Examination and/or other short cognitive test laboratory tests CT or MRI REPEAT IF NECESSARY DEPENDING ON THE EVOLUTION!!!
28 LABORATORY TESTS FOR THE EVALUATION OF DEMENTIA Thyroid function tests Serum vitamin B 12 Serum glucose level Complete blood cell count Serum electrolyte levels Serum liver function tests Serum kidney function tests Erythrocyte sedimentation rate Chest radiography Electrocardiography Toxicology screening Urinalysis and microscopy Serologic tests for syphilis
29 Additional Tests to Consider in the Diagnostic Work-Up of Dementia Test Electroencephalography Lumbar puncture Heavy metal screen Indication Possible seizures; Creutzfeldt-Jakob disease Onset of dementia within the preceding six months; dementia rapidly progressive History of potential exposure Human immunodeficiency virus History of potential exposure Lyme disease titer Ceruloplasmin, arylsulfatase, electrophoresis Slit lamp examination Apolipoprotein E Genetic testing for Alzheimer genes, other dementia genes History of exposure and compatible clinical picture Wilson's disease, metachromatic leukodystrophy, multiple myeloma History and examination suggest Wilson's disease Need to increase likelihood that diagnosis of Alzheimer's disease is correct Family history is strong, and confirmation is clinically necessary
30 Genetic testing and counselling???? Testing positive for APOE ε4 does not mean a person will definitely develop late onset Alzheimer's disease. Testing negative for APOE ε4 does not guarantee that they will be free from Alzheimer's presenilin when family history is +
31 Minimal program for investigation of cognitive impairment anamnesis and heteroanamnesis general exam neurological exam psychiatric exam Mini Mental State Examination and/or other short cognitive test laboratory tests CT or MRI REPEAT IF NECESSARY DEPENDING ON THE EVOLUTION!!!
32 Neuroradiology - CT/MRI Focal neurological signs Suspected cerebral lesion tumors subdural haematoma hydrocephalus stroke! acute, subacute onset trauma weeks ago general signs of malignancy

33 Dr. Gary W. Small
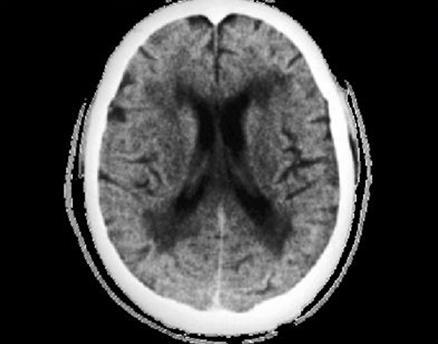
34 ALZHEIMER s DISEASE Characteristic: dementia no other causes slow progression cortical signs no neurological signs CT/MRI: atrophy Not characteristic: acute onset, focal signs, epilepsy, other CT/MRI signs


35 Alzheimer s disease: narrow gyri, large sulci
36


37 Alzheimer s disease: atrophy


38 Pathology: neurofibrillary tangles, neuritic plaques, amiloid depositions

39 Pathology: Lewy-body Clinical criteria Dementia Attention Visuospatial Executive Characteristic: Fluctuation Hallucinations parkinsonism

40 Lewis, KA et al: Abnormal neurites containing C-terminally truncated α - synuclein are present in Alzheimer s disease without conventional Lewy body pathology. The American Journal of Pathology 177(6) , 2010

41 Pathology: Pick-cells
42 VASCULAR DEMENTIA Dementia Cerebrovascular disease (risk factors, stroke, CT/MRI) relationship
43 VASCULAR DEMENTIA Commonly: multiinfarct (MID), multilacunar Characteristic: anamnestic: stroke, TIA Signs after stroke: neurological exam and CT/MRI Pseudobulbar syndrome, Incontinency: emotional, urine gait disorders (astasia, abasia), depression Not characteristic: normal CT/MRI, lack of vascular risk factors

44 CT: multiple lacunar infarcts Hegedűs, 2001
45 VASCULAR DEMENTIA Special: Binswanger s disease (encephalitis subcorticalis chronica progressiva) hypertension, dementia, unsteady gait, incontinency leucoaraiosis CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leucoencephalopathy)

46 Leucoaraiosis
 metabolic alcohol drugs Pseudodementia (depression)")
47 Potentially reversible causes of dementia subdural hematoma tumor (frontal) metabolic alcohol drugs Pseudodementia (depression) hydrokephalus

48 Potentially reversible causes of dementia hydrokephalus dementia unsteady gait incontinency
49 Features Distinguishing Delirium and Dementia Delirium Dementia Onset Acute Insidious Duration Days/weeks Months/years Attention Distracted Usually normal Level of Consciousness Increased/decreased Usually normal Cognition Disorganized Impoverished
50 Features Distinguishing Dementia and Depressive Pseudodementia: Dementia Pseudodementia Precise onset Unusual Usual Duration Long Short Complaints Variable Usual psych history Uncommon Common "Don't know" Uncommon Common Affect Labile, blunted Depressed
51 Mini-Mental State Examination (MMSE) Natural history of Alzheimer s disease 30 Early diagnosis Mild-tomoderate Severe 25 Symptoms 20 Diagnosis Loss of functional independence Behavioural problems Nursing home placement Death Time (years) Reproduced from Feldman and Gracon, 1996
52
53 Acetylcholinesterase Inhibitors Used in the Treatment of Dementia Drug Dosage Target dosage Minimum therapeutic dosage Donepezil (Aricept) Start at 5 mg once daily, taken at bedtime; after 6 weeks, increase to 10 mg once daily. 10 mg once daily 5 mg daily Rivastigmine (Exelon) Start at 1.5 mg twice daily, taken with food; at 2-week intervals, increase each dose by 1.5 mg, up to a dosage of 6 mg twice daily. 6 mg twice daily 3 mg twice daily Galantamine (Reminyl) Start at 4 mg twice daily with food; at 4-week intervals, increase each dose by 4 mg, up to a dosage of 12 mg twice daily. 12 mg twice daily 8 mg twice daily
54 N-methyl-D-aspartat (NMDA) antagonist Memantine (Ebixa) for treatment of moderate-to-severe AD Recommended dose: 2x10 mg per day Start at 1x5 mg per day Increase with 5mg per day each week to max. 2x10 mg per day
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Introduction to Dementia: Diagnosis & Evaluation. Created in March 2005 Duration: about 15 minutes
 Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Understanding Dementia
 Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
STUDENT GUIDELINES FOR DIAGNOSIS OF DEMENTIA
 STUDENT GUIDELINES FOR DIAGNOSIS OF DEMENTIA What is dementia? Dementia is characterised by a slow, sometimes stepwise, deterioration in the elderly person s mental, physical and social functioning. It
STUDENT GUIDELINES FOR DIAGNOSIS OF DEMENTIA What is dementia? Dementia is characterised by a slow, sometimes stepwise, deterioration in the elderly person s mental, physical and social functioning. It
Causes of Transient Incontinence. Geriatrics: Urinary Incontinence, Dementia, and Delirium. Classification of Established Incontinence
 Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
MINI-MENTAL STATE EXA MINATION (M MSE)
") MINI-MENTAL STATE EXA MINATION (M MSE) M axim u m Score Score 5 5 Orientation What is the (day of week) (day of month) (month) (year) (season)? Where are we: (state) (county) (town) (facility) (floor)?
MINI-MENTAL STATE EXA MINATION (M MSE) M axim u m Score Score 5 5 Orientation What is the (day of week) (day of month) (month) (year) (season)? Where are we: (state) (county) (town) (facility) (floor)?
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Cognitive Assessment. Part Two: Assessing Capacity, Beyond The Basics. Using Information To Make Decisions (Appreciating) What s s The Correct Method?
 What s s The Correct Method?") AUTONOMY, CAPACITY AND UNDUE INFLUENCE: KEMP Page 1 of 9 Part Two: Assessing Capacity, Beyond The Basics Cognitive Assessment Bryan Kemp, Ph. D. Center of Excellence in Elder Abuse and Neglect UC Irvine
AUTONOMY, CAPACITY AND UNDUE INFLUENCE: KEMP Page 1 of 9 Part Two: Assessing Capacity, Beyond The Basics Cognitive Assessment Bryan Kemp, Ph. D. Center of Excellence in Elder Abuse and Neglect UC Irvine
Vascular Dementia. Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center
 Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
If you have dementia, you may have some or all of the following symptoms.
 About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
Differentiating Dementia Diagnoses
 Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Resources: Types of dementia
 1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
COGNITIVE ALTERATIONS IN CHRONIC KIDNEY DISEASE K K L E E
 COGNITIVE ALTERATIONS IN CHRONIC KIDNEY DISEASE K K L E E Attention Problem Solving Language Cognitive Domains Decision Making Memory Reasoning The Cardiovascular Health Cognition Study shows higher S
COGNITIVE ALTERATIONS IN CHRONIC KIDNEY DISEASE K K L E E Attention Problem Solving Language Cognitive Domains Decision Making Memory Reasoning The Cardiovascular Health Cognition Study shows higher S
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
FACTORS AFFECTING CAPACITY
 FACTORS AFFECTING CAPACITY Psychosocial Factors Affecting Capacity Psychosocial factors include one s surroundings, way of life & things that affect relationships between the adult and their environment.
FACTORS AFFECTING CAPACITY Psychosocial Factors Affecting Capacity Psychosocial factors include one s surroundings, way of life & things that affect relationships between the adult and their environment.
MINI MENTAL STATE EXAM
 MINI MENTAL STATE EXAM ID NUMBER: FORM CODE: M M E DATE: 06/01/2011 Version 2.0 ADMINISTRATIVE INFORMATION 0a. Completion Date: / / 0b. Staff ID: Month Day Year Materials: Black pen, pencil, wrist watch,
MINI MENTAL STATE EXAM ID NUMBER: FORM CODE: M M E DATE: 06/01/2011 Version 2.0 ADMINISTRATIVE INFORMATION 0a. Completion Date: / / 0b. Staff ID: Month Day Year Materials: Black pen, pencil, wrist watch,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
Dementia. Amber Eker, MD. Assistant Professor Near East University Department of Neurology
 Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Dementia: Diagnosis and Treatment
 Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center
 Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care.
 Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Alzheimer Disease and Related Dementias. Alzheimer Society of Manitoba Dr. David Strang
 Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
Is PET/CT really helpful in diagnosing Alzheimer s Disease?
 Is PET/CT really helpful in diagnosing Alzheimer s Disease? J. Rudolf MD Ph.D. Consultant in Neurology, Dept. of Neurology, General Hospital Papageorgiou Thessaloniki, Greece Conflict of Interest PET/CT
Is PET/CT really helpful in diagnosing Alzheimer s Disease? J. Rudolf MD Ph.D. Consultant in Neurology, Dept. of Neurology, General Hospital Papageorgiou Thessaloniki, Greece Conflict of Interest PET/CT
Brain Health and Risk Factors for Dementia
 Welcome To Brain Health and Risk Factors for Dementia Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa April 4, 2018 10:00 11:00
Welcome To Brain Health and Risk Factors for Dementia Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa April 4, 2018 10:00 11:00
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Cognitive Assessment 4/29/2015. Learning Objectives To be able to:
 Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event
 Cumbria Partnership NHS Foundation Trust Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event Andrew Milburn Occupational Therapy Clinical Lead, Dementia Pathways
Cumbria Partnership NHS Foundation Trust Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event Andrew Milburn Occupational Therapy Clinical Lead, Dementia Pathways
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
DEMENTIA ANDREA BERG, MD
 DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 diagnosis and assessment bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
diagnosis and assessment bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
BHIVA Best Practice Management Session
 BHIVA Best Practice Management Session CNS (The brain) - I keep forgetting things DEMENTIA DIAGNOSIS, CLASSIFICATION AND INVESTIGATIONS Paul Holmes Consultant Neurologist Guy s and St Thomas Hospitals
BHIVA Best Practice Management Session CNS (The brain) - I keep forgetting things DEMENTIA DIAGNOSIS, CLASSIFICATION AND INVESTIGATIONS Paul Holmes Consultant Neurologist Guy s and St Thomas Hospitals
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Old Age and Stress. Disorders of Aging and Cognition. Disorders of Aging and Cognition. Chapter 18
 Disorders of Aging and Cognition Chapter 18 Slides & Handouts by Karen Clay Rhines, Ph.D. Northampton Community College Comer, Abnormal Psychology, 8e Disorders of Aging and Cognition Dementia deterioration
Disorders of Aging and Cognition Chapter 18 Slides & Handouts by Karen Clay Rhines, Ph.D. Northampton Community College Comer, Abnormal Psychology, 8e Disorders of Aging and Cognition Dementia deterioration
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
Name at birth. Address. MMSE: CASE: Cognigram. MMSE (Folstein and coll., 1975) Temporal Orientation Day: Date: Month: Season: Year: /5
 Temporal Orientation Day: Date: Month: Season: Year: /5") CASE Cognitive Assessment Scale for the Elderly Daniel Geneau - Daniel Taillefer Institution Examiner Date of exam Age Education Date of birth Room File No y m d Name at birth Usual name or spouse name
CASE Cognitive Assessment Scale for the Elderly Daniel Geneau - Daniel Taillefer Institution Examiner Date of exam Age Education Date of birth Room File No y m d Name at birth Usual name or spouse name
Alzheimer Disease and Related Dementias
 Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
RECOGNITION AND MANAGEMENT OF DEMENTIA IN THE ACUTE CARE SETTING
 RECOGNITION AND MANAGEMENT OF DEMENTIA IN THE ACUTE CARE SETTING Alex Hishaw, MD Department of Neurology University of Arizona Objectives: Recognize the impact of history and presentation on the diagnosis
RECOGNITION AND MANAGEMENT OF DEMENTIA IN THE ACUTE CARE SETTING Alex Hishaw, MD Department of Neurology University of Arizona Objectives: Recognize the impact of history and presentation on the diagnosis
Encephalopathy. David M. Ermak, DO Assistant Professor of Neurology
 Encephalopathy David M. Ermak, DO Assistant Professor of Neurology Objectives Conduct a proper evaluation of mental status Evaluate and investigate encephalopathy and the common causes Appreciate documentation
Encephalopathy David M. Ermak, DO Assistant Professor of Neurology Objectives Conduct a proper evaluation of mental status Evaluate and investigate encephalopathy and the common causes Appreciate documentation
Alzheimer's Disease. Dementia
 Alzheimer's Disease Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s Disease
Alzheimer's Disease Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s Disease
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Donepezil, galantamine, rivastigmine and memantine for the treatment of Alzheimer's disease (Review of TA 111) Appraisal
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Donepezil, galantamine, rivastigmine and memantine for the treatment of Alzheimer's disease (Review of TA 111) Appraisal
Significance A Busy Clinician's Guide to Seniors with Memory Loss
 Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Dementia is not normal aging!
 The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
ASSESSMENT MILD COGNITIVE IMPAIRMENT. (i) Is the forgetfulness or confusion acute or chronic?
 Is the forgetfulness or confusion acute or chronic?") The main pathological hallmarks of AD are the Betaamyloid plaques and neurofibrillary tangles. The risk factors for the development of this pathology include advanced age, family history, vascular risk
The main pathological hallmarks of AD are the Betaamyloid plaques and neurofibrillary tangles. The risk factors for the development of this pathology include advanced age, family history, vascular risk
CHAPTER 15: NEUROCOGNITIVE DISORDERS KEY TERMS. Acetylcholine A neurotransmitter that appears to be involved in learning and memory.
 CHAPTER 15: NEUROCOGNITIVE DISORDERS KEY TERMS Acetylcholine A neurotransmitter that appears to be involved in learning and memory. Adult Memory and Information Processing Battery (AMIPB) A neuropsychological
CHAPTER 15: NEUROCOGNITIVE DISORDERS KEY TERMS Acetylcholine A neurotransmitter that appears to be involved in learning and memory. Adult Memory and Information Processing Battery (AMIPB) A neuropsychological
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Dementia NICE Guidelines Update. Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018
 26 September 2018") Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
EARLY DEMENTIA. University of Hawaii Geriatric Medicine Department
 EARLY DEMENTIA University of Hawaii Geriatric Medicine Department INTRODUCTION Dementia is very prevalent Screening and early diagnosis is important Evaluation Dementia Management DEMENTIA IS VERY PREVALENT
EARLY DEMENTIA University of Hawaii Geriatric Medicine Department INTRODUCTION Dementia is very prevalent Screening and early diagnosis is important Evaluation Dementia Management DEMENTIA IS VERY PREVALENT
Alzheimer s Disease without Dementia
 Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Delirium, Dementia, and Amnestic Disorders. Dr.Al-Azzam 1
 Delirium, Dementia, and Amnestic Disorders Dr.Al-Azzam 1 Introduction Disorders in which a clinically significant deficit in cognition or memory exists The number of people with these disorders is growing
Delirium, Dementia, and Amnestic Disorders Dr.Al-Azzam 1 Introduction Disorders in which a clinically significant deficit in cognition or memory exists The number of people with these disorders is growing
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Understanding dementia
 Dementia handbook for carers Essex Understanding dementia About this handbook 1 What is dementia 3 Summary of dementia symptoms 6 Medication and treatment 7 About this handbook This handbook aims to summarise
Dementia handbook for carers Essex Understanding dementia About this handbook 1 What is dementia 3 Summary of dementia symptoms 6 Medication and treatment 7 About this handbook This handbook aims to summarise
Managing Patients with Dementia using a Collaborative and Strength-based Approach
 Managing Patients with Dementia using a Collaborative and Strength-based Approach Therapy Network Seminars, Inc. Nicole Dawson, PT, PhD, GCS Learning Objectives The Participant will be able to: Identify
Managing Patients with Dementia using a Collaborative and Strength-based Approach Therapy Network Seminars, Inc. Nicole Dawson, PT, PhD, GCS Learning Objectives The Participant will be able to: Identify
Dementia is a syndrome in which the progressive
 UNDERSTANDING THE BURDEN OF MENTAL HEALTH Photo: Digital Stock. Recognizing Dementia: The Importance of an Accurate Diagnosis BY JOE MAIER,JR. Dementia is a syndrome in which the progressive deterioration
UNDERSTANDING THE BURDEN OF MENTAL HEALTH Photo: Digital Stock. Recognizing Dementia: The Importance of an Accurate Diagnosis BY JOE MAIER,JR. Dementia is a syndrome in which the progressive deterioration
Dementia: general overview
 132 CHAPTER 5 Organic illness Dementia: general overview Essence Dementia is a syndrome characterized by progressive, usually irreversible, global cognitive deficits. Often memory impairment is the first
132 CHAPTER 5 Organic illness Dementia: general overview Essence Dementia is a syndrome characterized by progressive, usually irreversible, global cognitive deficits. Often memory impairment is the first
Alzheimer s Disease. Fact Sheet. Fact Sheet. Fact Sheet. What Causes AD?
 2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
Dementia and Delirium
 Dementia and Delirium LPT Gondar Mental Health Group www.le.ac.uk Dementia and Delirium WTINP Chapter 4.6 Introduction - areas to be covered Delirium Definition and causes Clinical features Management
Dementia and Delirium LPT Gondar Mental Health Group www.le.ac.uk Dementia and Delirium WTINP Chapter 4.6 Introduction - areas to be covered Delirium Definition and causes Clinical features Management
4/11/2017. The impact of Alzheimer s disease. Typical changes. The impact of Alzheimer s disease. Problematic changes. Problematic changes
 The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
DSM-5 MAJOR AND MILD NEUROCOGNITIVE DISORDERS (PAGE 602)
") SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
Dementia is an overall term for a set of symptoms that is caused by disorders affecting the brain.
 Vascular Dementia Vascular Dementia Other Dementias This information sheet provides an overview of a type of dementia known as vascular dementia. In this information sheet you will find: An overview of
Vascular Dementia Vascular Dementia Other Dementias This information sheet provides an overview of a type of dementia known as vascular dementia. In this information sheet you will find: An overview of
What is dementia? alzheimers.org.uk
 alzheimers.org.uk What is dementia? If you, or a friend or relative, have been diagnosed with dementia, you may be feeling anxious or confused. You may not know what dementia is. This factsheet should
alzheimers.org.uk What is dementia? If you, or a friend or relative, have been diagnosed with dementia, you may be feeling anxious or confused. You may not know what dementia is. This factsheet should
In-Service Education. workbook 3. by Hartman Publishing, Inc. second edition
 In-Service Education workbook 3 second edition by Hartman Publishing, Inc. Alzheimer s Disease Dignity Diabetes Restraints and Restraint Alternatives Abuse and Neglect Death and Dying Managing Stress Perf
In-Service Education workbook 3 second edition by Hartman Publishing, Inc. Alzheimer s Disease Dignity Diabetes Restraints and Restraint Alternatives Abuse and Neglect Death and Dying Managing Stress Perf
Evaluations. Alzheimer s Disease A Public Health Response. Viewer Call-In. July 19, Guest Speakers. Thanks to our Sponsors:
 Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Dementia, Depression, and Delirium 2.0 Contact Hours Presented by: CEU Professor
 Dementia, Depression, and Delirium 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Dementia, Depression, and Delirium 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Evaluation and Treatment of Dementia
 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Dr Roger Cable NHS Dumfries and Galloway
 Dr Roger Cable NHS Dumfries and Galloway Young Onset Dementia Statistics What is dementia Diagnosing dementia History Examination Tests Subtypes of dementia 315000 Cost of dementia (Alzheimer s society)
Dr Roger Cable NHS Dumfries and Galloway Young Onset Dementia Statistics What is dementia Diagnosing dementia History Examination Tests Subtypes of dementia 315000 Cost of dementia (Alzheimer s society)
Cal MediConnect Dementia Awareness CMC Annual Training
 Cal MediConnect 2017 Dementia Awareness 2017 CMC Annual Training Definition Overview of Dementia Training Diagnosis of Dementia Signs and Symptoms Risk Factors Stages of Dementia Types of Dementia: Reversible/Irreversible
Cal MediConnect 2017 Dementia Awareness 2017 CMC Annual Training Definition Overview of Dementia Training Diagnosis of Dementia Signs and Symptoms Risk Factors Stages of Dementia Types of Dementia: Reversible/Irreversible
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
Assessment and treatment of cognitive deficits in dementia Julia Gifford MB BCh and Roy Jones BSc, FRCP, DipPharmMed
 Assessment and treatment of cognitive deficits in dementia Julia Gifford MB BCh and Roy Jones BSc, FRCP, DipPharmMed SPL Our series Prescribing in older people gives practical advice for successful management
Assessment and treatment of cognitive deficits in dementia Julia Gifford MB BCh and Roy Jones BSc, FRCP, DipPharmMed SPL Our series Prescribing in older people gives practical advice for successful management
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Alzheimer s disease. The facts in brief
 Alzheimer s disease Dementia is an umbrella term used to describe various conditions which damage brain cells and lead to a loss of brain function over time. Dementia causes a progressive decline in a
Alzheimer s disease Dementia is an umbrella term used to describe various conditions which damage brain cells and lead to a loss of brain function over time. Dementia causes a progressive decline in a
Forgetfulness: Knowing When to Ask for Help
 National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
Dementia the A,B,Cs. Dr. Frank Molnar. Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital
 Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)