Update on the Treatment of Parkinson s Disease. Neurotherapeutics for Rehab Professionals November 6 th, 2015
|
|
|
- Jared White
- 5 years ago
- Views:
Transcription
1 Brent Bluett, DO Dr. Brent Bluett completed medical school at Touro Unviersity Nevada College of Osteopathic Medicine, neurology residency at the University of Texas Southwestern at Austin, and a Movement Disorders Fellowship at the University of California San Diego. He returns to the Las Vegas area as a Movement Disorders specialist at the Cleveland Clinic Nevada Lou Ruvo Center for Brain Health (CCLRCBH). His expertise is in Movement Disorders such as Parkinson s Disease, Atypical Parkinsonism (Progressive Supranuclear Palsy), Dystonia, Ataxia, and Tremors. Dr. Bluett is fellowship trained in therapeutic interventions such as Botulinum toxin injections and Deep Brain Programming Stimulation, and leads the Botulinum toxin for Dystonia clinic at the CCLRCBH. He recently completed the first large research study on predicting and preventing falls in Progressive Supranuclear Palsy, and intends to expand the findings to reduce falls in other Movement Disorders. His other research interests include transcranial direct-current stimulation to improve motor function in Parkinson s disease and Dystonia, and neuroimaging utilizing the cutting edge imaging modalities at the Lou Ruvo Center for Brain Health. Note: Dr. Bluett has no relationship which, in the context of his presentation, could be perceived as a potential conflict of interest.
2 Update on the Treatment of Parkinson s Disease Neurotherapeutics for Rehab Professionals November 6 th, 2015
3 Therapeutic principles of treatment
4 1) No proven protective/restorative effects with medications as of yet MAO-B inhibitors have shown promise in modifying disease progression Exercise reduces loss of dopamine neurons in MPTP lesioned rats Induces growth factors (GDNF, BDNF)
5 2) Encourage patients to remain active and mobile Decreased motivation, increased passivity in PD -> active exercise program may help PT/exercise useful in all stages of the disease Better motor performance seen in patients w/ PD who exercise intensely and regularly
6 3) Keep the patient functioning independently as long as possible Drugs help symptoms but don t stop disease progression 75% of patients have serious complications of Levodopa tx 5 Major responses > 5 years of Levodopa therapy: 1) Troublesome fluctuations (43%) 2) Smooth, good response (25%) 3) Troublesome dyskinesias (20%) 4) Total or substantial loss of efficacy (8%) 5) Toxicity at therapeutic/sub therapeutic dose (4%)
7 3) Keep the patient functioning independently as long as possible Levodopa therapy: Younger patients are more likely to develop motor fluctuations and dyskinesias Older patients are more likely to develop confusion, psychosis, sleep-wake alterations from medications
8 4) Individualize therapy Consider each patient s symptoms, degree of functional impairment, and expected risks/benefits of treatment agents Determine issues by asking the patient to list the specific symptoms that trouble them the most. Then attempt to treat the most troublesome symptoms This will maximize the patient s quality of life
9 Pharmacologic Treatment of Parkinson s Disease
10 Patient with Parkinson s Disease - OFF medication

11 Same patient ON medication
12 Therapeutic Options 1) MAO-B Inhibitors 2) Dopamine Agonists 3) Carbidopa-Levodopa 4) IPX-066 5) Duodopa 6) Botulinum Toxin injections 7) Deep Brain Stimulation
13 MAO-B Inhibitors
14 DATATOP trial Deprenyl and Tocopherol Antioxidative Therapy of Parkinsonism Selegiline (5mg PO bid) delayed symptomatic treatment by 9 months Helps avoid Levodopa induced motor complications
15 BLIND-DATE trial Subjects on Selegiline required lower dosage of levodopa Had slower rate of worsening of symptoms and signs of PD, and less freezing of gait
16 TEMPO and ADAGIO trials Rasagaline can reduce the rate of clinical worsening in patients with early PD TEMPO: 2mg Rasagaline had superior result > 1 mg ADAGIO: Only the 1mg dose was superior to placebo
17 Recommend start treatment in Early PD with MAO-Inihbitor <10mg/day Selegiline < 2mg/day Rasagiline
18 Dopamine Agonists
19 Oral: Ropinirole (Requip and Requip XL) Pramipexole (Mirapex and Mirapex ER) Transdermal: Rotigotine (Neupro) Dopamine Agonist monotherapy is rarely successful > 3 years
20 Nausea DA Agonist common side effects Orthostatic hypotension Common cause of falls Important to assess BP Supine, Sitting, Standing, Standing after 3 minutes Timed up and go *Advise caution when standing or sitting up Somnolence Ask pt s about sleep attacks, may require Modafinil Hallucinations
21 DA Agonist common side effects: Impulse Control Disorder Compulsive gambling, shopping, sexual behavior Impulsive patients may attempt to walk faster than they re capable of, or stand up too quickly Leg edema (later) Compression stockings Elevate feet above level of heart
22 Dopamine Agonist Withdrawal Syndrome (DAWS) Not relieved by Levodopa Symptoms: Anxiety, panic, agoraphobia, depression, diaphoresis, OH, fatigue, pain, drug cravings *Advise physician if patient showing signs Gradually reduce DA Agonist. Do not discontinue immediately. May need to restart DA Agonist at low dose
23 Carbidopa-Levodopa (Sinemet)
24 Sinemet IR 10/100, 25/100, 25/250 mg Start with 25/100 mg, increase by 25/100 mg q week until reach desired outcome Usually 25/100 mg tid Bradykinesia and Rigidity respond best Tremor may be more resistant Reasonable high dose of levodopa before concluding inefficacy = 2,000 mg/day
25 Sinemet CR: Useful as a first line drug in pts > 70 y/o Lowers peak plasma level, less drowsiness or confusion Pre-bedtime dose may increase nighttime mobility, but can have an excess delayed response Severe, sustained dyskinesias, less predictable response with CR
26 Nausea Carbidopa-Levodopa side effects and complications of therapy Orthostatic Hypotension Midodrine, Fludrocortisone (Florinef), Droxidopa (Northera) Supine hypertension Elevate head of bed 30 degrees Somnolence Hallucinations Dyskinesias Amantadine
27 Carbidopa-Levodopa side effects and complications of therapy Fluctuations: OFF vs. ON Duration of Levodopa dose becomes shorter as PD worsens Pharmacokinetic ½ life is 90 minutes Clinical ½ life: Stage 1: 262 minutes Stage 2: 142 minutes Stage 3: 54 minutes
28 Carbidopa-Levodopa side effects and complications of therapy Fluctuations: Entacapone COMT inhibitor, prolongs ½ life of Levodopa Increased risk of dyskinesias earlier on when used with Sinemet Sinemet CR Not shown to avoid fluctuations Better to use small, divided doses of Sinemet IR
29 IPX-066 (Rytary)
30 Contains immediate release and extended-release beads Dissolves in GI tract at varying rates Specific amount of Carbidopa and levodopa in a 1:4 ratio Carbidopa/Levodopa: 23.75mg/95mg 36.25mg/145mg 48.75mg/195mg 61.25mg/245mg Provides both initial and extended levodopa plasma concentrations
31 1 393 PD patients with > 2.5 hours off-time per day IPX066 (given 3-6 times a day) vs. Carbidopa/Levodopa IR Reduced off-time by 1.17 hours/day Final daily dose of IPX066 was approximately double that of Carbidopa/Levodopa IR Adverse events over 13 week period: 43% with IPX066 40% with Carbidopa/Levodopa IR
32 Conclusions: Many PD patients with motor fluctuations can be switched from Carbidopa-Levodopa IR to IPX066 with: Reduced dosing frequency Reduced off-time Improved functionality Improvement in some measures of quality of life
33 Conversion from Carbidopa-Levodopa IR to Rytary
34 Comparison of the pharmacokinetics of an oral extended-release capsule formulation of carbidopalevodopa (IPX066) with immediate-release carbidopalevodopa (Sinemet), sustained-release carbidopalevodopa (Sinemet CR), and carbidopa-levodopaentacapone (Stalevo) Hsu, A., Yao, H.-M., Gupta, S. and Modi, N. B. (2015), Journal of Clinical Pharma, 55: doi: /jcph.514
35 Study Conclusions Carbidopa-Levodopa IR: Reached peak concentrations (C max ) at 1 hour LD concentrations then decreased rapidly and were less than 10% of peak by 5 hours. Sinemet CR and Stalevo (Carbidopa-Levodopa-Entacapone): Reached peak concentration (C max ) at 1.5 hours LD concentrations were less than 10% of peak by 6.3 (Sinemet CR) and 7.5 hours (Stalevo) IPX066 (Rytary): Reached peak concentration (C max ) at 4.5 hours LD concentrations were less than 10% of peak by 10.1 hours
36 Anecdotal Clinical Observations of Rytary Decreases fluctuations Patient s don t get initial kick of Sinemet IR Less dyskinesias Takes time to convert dosing properly Take delayed onset and sustained benefit into account when assessing patients Determining if patient is OFF or ON may be more difficult
37 Levodopa/Carbidopa Intestinal Gel (LCIG) or Duodopa
38 Intrajejunal percutaneous gastrostomy tube LCIG provides continuous drug delivery in order to provide a stable plasma LD concentration Goal: continuously stimulate striatal dopamine receptors Non-oral route avoids fluctuations in absorption due to delayed gastric emptying and competition for GI uptake

39 Duodopa Pump
40 Clinical Indications for Duodopa: Advanced Parkinson s Disease Severe motor fluctuations and dyskinesias resistant to conventional therapy Satisfactory response to Levodopa Ability to tolerate surgery and have social support to handle postoperative care Contraindications to Duodopa: Pronounced dementia Medical contraindications to abdominal surgery
41 Anecdotal Clinical Observations of Duodopa Reserved for advanced PD patients Does help reduce fluctuations and dyskinesias Patients must initially come to clinic for full day to adjust bolus and maintenance doses Patients need caretakers to assist with administration Tube can become dislodged Requires coordination with GI specialist
42 Botulinum Toxin Injections

43 How Botox Works
44 Indications in Parkinson s Disease Dystonia Sustained muscle contractions, frequently causing twisting and repetitive movements, or abnormal postures Sialorrhea Excessive salivation and drooling Overproduction and reduced swallowing

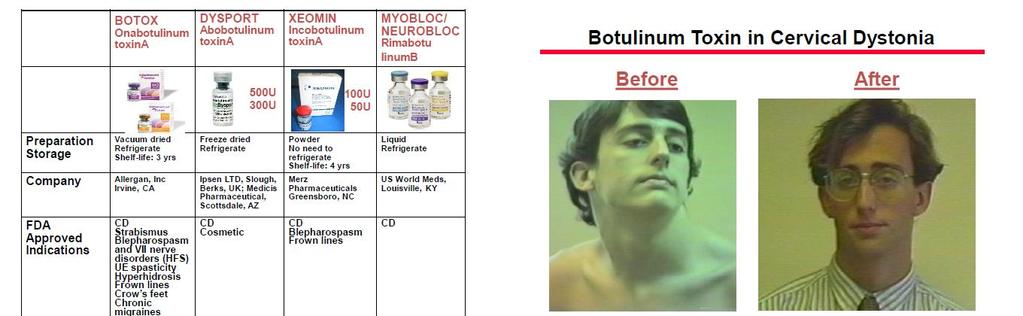
45 Cervical Dystonia

46 Focal Foot Dystonia

47 Dystonia in Parkinson s Disease
48
49 Botulinum Toxin for Dystonia Focal Dystonia Standard dosage = Units Sialorrhea Standard dosage = 40 Units Clinical improvement generally begins within the first two weeks after injection Maximum clinical benefit at approximately six weeks post-injection. Most patients return to pre-treatment status by 3 months post-treatment.
50 Physical therapy program for cervical dystonia: a study of 20 cases Botulinum toxin (BTX) is the best therapeutic option in patients with cervical dystonia (CD) Physical therapy (PT) can be added to the treatment to achieve better results. Combination of: Motor Learning Exercises Kinesiotherapy Functional Electrical Stimulation of antagonist muscles Botox + PT group showed greater improvement than Botox alone in pain and disability
51 Special Considerations in Therapy for Dystonia Prolonged immobilization of a limb can cause a peripheral dystonia Botulinum toxin adjunctive therapies should focus on decreasing pain and improving functionality Monitor for excessive weakness, especially in patients who receive botulinum toxin in lower extremities Speech therapy important to monitor for dysphagia/dysarthria after botulinum toxin injections for cervical dystonia Important to manage patient expectations
52 Deep Brain Stimulation for Parkinson s Disease
53 Before and After DBS
54 How DBS works Non-destructive and reversible means of disrupting the abnormal function of thalamic and basal ganglia nuclei and their circuits Stimulation parameters are programmed non-invasively, postsurgery Adjustments made to deliver the appropriate level of stimulation Amplitude Frequency Pulse Width
55 FDA Indication for Parkinson s Disease Indicated for bilateral stimulation of the globus pallidus interna (Gpi) or the Subthalamic nucleus (STN) as an adjunctive therapy in reducing some of the symptoms of advanced, levodopa-responsive Parkinson s Disease that are not adequately controlled with medication Ventral intermedius nucleus (Vim) of the thalamus can be targeted to reduce tremor in PD
56 Inclusion criteria for DBS in Parkinson s Disease Idiopathic Parkinson s Disease Troublesome motor symptoms despite optimal pharmacologic treatment Intolerable side effects to antiparkinsonian medication Patient still has clear motor improvement with Levodopa Generally > 30% improvement in UPDRS III Motor exam ON vs. OFF
57 Exclusion criteria for DBS in Parkinson s Disease Significant medical conditions that prevent surgery Dementia Moderate to severe depression Age > 70 Levodopa-unresponsive gait and balance abnormalities Intellectual impairment
58 DBS Multidisciplinary Evaluation UPDRS III Motor examination both OFF and ON Levodopa Physical Therapy/Occupational Therapy/Speech Therapy Provide input regarding patient s overall status, potential areas of improvement, limitations, risks/benefits PT: Gait disability/tendency to fall OT: Manual dexterity, potential functional disorder? ST: Dysarthria, dysphagia, aphasia Neuropsychiatric evaluation MRI Brain Systemic comorbidities Social circumstances
59 Important considerations in DBS Gait unlikely to improve May worsen postural instability STN vs. GPI: STN: Greater benefits, greater risk Can cause disinhibition, personality changes, induce dyskinesias Therapists can be of great benefit in setting programming parameters Overstimulation can cause: Dysarthria (bilateral Gpi) Muscle contraction (Gpi) Dysequilibrium and gait ataxia (STN) Please advise physician responsible for DBS programming
60 Conclusions Therapists are vital to management of Parkinson s Disease Medications and surgery only go so far! Two most feared complications of PD: Falls Dysphagia Monitor for complications of medical/surgical therapy Team approach Communication between physician and therapist is key Respect each other s areas of expertise Encourage exercise Optimize patient s quality of life
61 References 1) Fahn S, Jankovic J, Hallett M. Principles and Practices of Movement Disorders 2011, Elsevier Saunders. 2) Robert Hauser, Ann Hsu, Sherron Kell, Alberto Espay, Kapil Sethi, Mark Stacy, William Ondo, Martin O Connell, Suneel Gupta, for the IPX066 Advance-PD investigators. Extended-release carbidopalevodopa (IPX066) compared with immediate-release carbidopalevodopa in patients with Parkinson s disease and motor fluctuations: a phase 3 randomised, double-blind trial Lancet Neurology, 2013:12: ) Hsu, A., Yao, H.-M., Gupta, S. and Modi, N. B. Comparison of the pharmacokinetics of an oral extended-release capsule formulation of carbidopa-levodopa (IPX066) with immediate-release carbidopalevodopa (Sinemet), sustained-release carbidopa-levodopa (Sinemet CR), and carbidopa-levodopa-entacapone (Stalevo). 2015, Journal of Clinical Pharma, 55: doi: /jcph.514
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
PD: Key Treatment Considerations
 PD: Key Treatment Considerations 2018 Management of Neurologic and Neurosurgical Disorders in Daily Practice Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 11/27/2018 1 Outline Treatment
PD: Key Treatment Considerations 2018 Management of Neurologic and Neurosurgical Disorders in Daily Practice Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 11/27/2018 1 Outline Treatment
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Best Medical Treatments for Parkinson s disease
 Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Medications used to treat Parkinson s disease
 Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Communicating About OFF Episodes With Your Doctor
 Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University
 Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Prior Authorization with Quantity Limit Program Summary
 Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N.
 PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to
 parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
Deep Brain Stimulation: Patient selection
 Deep Brain Stimulation: Patient selection Halim Fadil, MD Movement Disorders Neurologist Kane Hall Barry Neurology Bedford/Keller, TX 1991: Thalamic (Vim) DBS for tremor Benabid AL, et al. Lancet. 1991;337(8738):403-406.
Deep Brain Stimulation: Patient selection Halim Fadil, MD Movement Disorders Neurologist Kane Hall Barry Neurology Bedford/Keller, TX 1991: Thalamic (Vim) DBS for tremor Benabid AL, et al. Lancet. 1991;337(8738):403-406.
The Shaking Palsy of 1817
 The Shaking Palsy of 1817 A Treatment Update on Parkinson s Disease Dr Eitzaz Sadiq Neurologist CH Baragwanath Acadamic Hospital Parkinson s Disease O Premature death of dopaminergic neurons O Symptoms
The Shaking Palsy of 1817 A Treatment Update on Parkinson s Disease Dr Eitzaz Sadiq Neurologist CH Baragwanath Acadamic Hospital Parkinson s Disease O Premature death of dopaminergic neurons O Symptoms
Medication Management & Strategies When the levodopa honeymoon is over
 Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Deep Brain Stimulation: Indications and Ethical Applications
 Deep Brain Stimulation Overview Kara D. Beasley, DO, MBe, FACOS Boulder Neurosurgical and Spine Associates (303) 562-1372 Deep Brain Stimulation: Indications and Ethical Applications Instrument of Change
Deep Brain Stimulation Overview Kara D. Beasley, DO, MBe, FACOS Boulder Neurosurgical and Spine Associates (303) 562-1372 Deep Brain Stimulation: Indications and Ethical Applications Instrument of Change
Advanced Therapies for Motor Symptoms in PD. Matthew Boyce MD
 Advanced Therapies for Motor Symptoms in PD Matthew Boyce MD Medtronic Education Teva Speakers Bureau Acadia Speakers Bureau Disclosures Discuss issues in advanced PD Adjunct therapies to levo-dopa Newer
Advanced Therapies for Motor Symptoms in PD Matthew Boyce MD Medtronic Education Teva Speakers Bureau Acadia Speakers Bureau Disclosures Discuss issues in advanced PD Adjunct therapies to levo-dopa Newer
Parkinson s Disease Medications: Professionals Edition
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
10/13/2017. Disclosures. Deep Brain Stimulation in the Treatment of Movement Disorders. Deep Brain Stimulation: Objectives.
 Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Objectives. Emerging Treatments in Parkinson s s Disease. Pathology. As Parkinson s progresses it eventually affects large portions of the brain.
 Objectives Emerging Treatments in Parkinson s s Disease 1) Describe recent developments in the therapies for Parkinson s Disease Jeff Kraakevik MD Assistant Professor OHSU/Portland VAMC Parkinson s Center
Objectives Emerging Treatments in Parkinson s s Disease 1) Describe recent developments in the therapies for Parkinson s Disease Jeff Kraakevik MD Assistant Professor OHSU/Portland VAMC Parkinson s Center
Welcome and Introductions
 Parkinson s Disease Spotlight on Treatment Advances Tuesday, January 26, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing American Parkinson Disease Association 1
Parkinson s Disease Spotlight on Treatment Advances Tuesday, January 26, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing American Parkinson Disease Association 1
PARKINSON S MEDICATION
 PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
Parkinson's Disease KP Update
 Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
8/28/2017. Behind the Scenes of Parkinson s Disease
 BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s Disease. Gillian Sare
 Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
Literature Scan: Anti-Parkinson s Agents
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Anticholinergics. COMT* Inhibitors. Dopaminergic Agents. Dopamine Agonists. Combination Product
 Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
What is Parkinson s Disease?
 2018 Update in Parkinson s Disease: Treatments and Future Plans Arita McCoy, MSN, CRNP Johns Hopkins Parkinson s Disease and Movement Disorder Center A National Parkinson Foundation Center of Excellence
2018 Update in Parkinson s Disease: Treatments and Future Plans Arita McCoy, MSN, CRNP Johns Hopkins Parkinson s Disease and Movement Disorder Center A National Parkinson Foundation Center of Excellence
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Issues for Patient Discussion
 onmotor complications radykinesia Screening Tools asked PD micrographia eurodegeneration Designed for Use by Family Practitioners remor on-off opamine agonists tiffness depression ostural instability wearing
onmotor complications radykinesia Screening Tools asked PD micrographia eurodegeneration Designed for Use by Family Practitioners remor on-off opamine agonists tiffness depression ostural instability wearing
The symptoms of the Parkinson s disease may vary from person to person. The symptoms might include the following:
 1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
PARKINSON S SYMPTOM TRACKER
 PARKINSON S SYMPTOM You can help your doctor make good treatment decisions by tracking your symptoms. A well-kept Symptom Tracker provides a clear picture of when you are taking your medications, when
PARKINSON S SYMPTOM You can help your doctor make good treatment decisions by tracking your symptoms. A well-kept Symptom Tracker provides a clear picture of when you are taking your medications, when
Cardinal Features of Parkinson s. Management of Parkinson s Disease. Drug Induced Parkinson s. Other Parkinson s Symptoms.
 Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Surgical Management of Parkinson s Disease
 Surgical Management of Parkinson s Disease Shyamal H. Mehta MD, PhD Assistant Professor of Neurology, Movement Disorders Division Mayo Clinic College of Medicine Mayo Clinic, Arizona 2016 MFMER slide-1
Surgical Management of Parkinson s Disease Shyamal H. Mehta MD, PhD Assistant Professor of Neurology, Movement Disorders Division Mayo Clinic College of Medicine Mayo Clinic, Arizona 2016 MFMER slide-1
Motor Fluctuations in Parkinson s Disease
 Motor Fluctuations in Parkinson s Disease Saeed Bohlega, MD, FRCPC Senior Distinguished Consultant Department of Neurosciences King Faisal Specialist Hospital & Research Centre Outline Type of fluctuations
Motor Fluctuations in Parkinson s Disease Saeed Bohlega, MD, FRCPC Senior Distinguished Consultant Department of Neurosciences King Faisal Specialist Hospital & Research Centre Outline Type of fluctuations
Key Concepts and Issues in Parkinson s Disease in 2016
 Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
What s new for diagnosing and treating Parkinson s Disease?
 What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Parkinson s Disease Update
 Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Deep Brain Stimulation for Parkinson s Disease & Essential Tremor
 Deep Brain Stimulation for Parkinson s Disease & Essential Tremor Albert Fenoy, MD Assistant Professor University of Texas at Houston, Health Science Center Current US Approvals Essential Tremor and Parkinsonian
Deep Brain Stimulation for Parkinson s Disease & Essential Tremor Albert Fenoy, MD Assistant Professor University of Texas at Houston, Health Science Center Current US Approvals Essential Tremor and Parkinsonian
Scottish Medicines Consortium
 Scottish Medicines Consortium rotigotine 2mg/24 hours, 4mg/24 hours, 6mg/24 hours, 8mg/24 hours transdermal patch (Neupro ) (No: 289/06) Schwarz Pharma Ltd. 7 July 2006 The Scottish Medicines Consortium
Scottish Medicines Consortium rotigotine 2mg/24 hours, 4mg/24 hours, 6mg/24 hours, 8mg/24 hours transdermal patch (Neupro ) (No: 289/06) Schwarz Pharma Ltd. 7 July 2006 The Scottish Medicines Consortium
Welcome and Introductions
 Parkinson s Disease Spotlight on Addressing Motor and Non-Motor Symptoms The Changing Landscape Wednesday, March 8, 2017 Welcome and Introductions Stephanie Paul Vice President Development and Marketing
Parkinson s Disease Spotlight on Addressing Motor and Non-Motor Symptoms The Changing Landscape Wednesday, March 8, 2017 Welcome and Introductions Stephanie Paul Vice President Development and Marketing
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Clinical Policy: Safinamide (Xadago) Reference Number: CP.CPA.308 Effective Date: Last Review Date: Line of Business: Commercial
 Reference Number: CP.CPA.308 Effective Date: Last Review Date: Line of Business: Commercial") Clinical Policy: Safinamide (Xadago) Reference Number: CP.CPA.308 Effective Date: 05.16.17 Last Review Date: 08.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy
Clinical Policy: Safinamide (Xadago) Reference Number: CP.CPA.308 Effective Date: 05.16.17 Last Review Date: 08.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Punit Agrawal, DO Clinical Assistant Professor of Neurology Division of Movement Disorders OSU Department of Neurology
 Deep Brain Stimulation for Movement Disorders Punit Agrawal, DO Clinical Assistant Professor of Neurology Division of Movement Disorders OSU Department of Neurology History of DBS 1 History of DBS 1987
Deep Brain Stimulation for Movement Disorders Punit Agrawal, DO Clinical Assistant Professor of Neurology Division of Movement Disorders OSU Department of Neurology History of DBS 1 History of DBS 1987
Treatment of Parkinson s Disease and of Spasticity. Satpal Singh Pharmacology and Toxicology 3223 JSMBS
 Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
ACUTE MANAGEMENT OF PARKINSON S PATIENTS WHO ARE NIL BY MOUTH (NBM) OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM
 OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM") ACUTE MANAGEMENT OF PARKINSON S PATIENTS WHO ARE NIL BY MOUTH (NBM) OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM 1 CONTENTS: TOPIC PAGE Introduction 3 What should you do when a PD
ACUTE MANAGEMENT OF PARKINSON S PATIENTS WHO ARE NIL BY MOUTH (NBM) OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM 1 CONTENTS: TOPIC PAGE Introduction 3 What should you do when a PD
With Time, The Pathology of PD Spreads Throughout the Brain
 With Time, The Pathology of PD Spreads Throughout the Brain Braak s staging of Parkinson s disease pathology dm co sn mc hc fc 1 Hubert H. Fernandez, MD, FAAN Professor of Medicine (Neurology) Cleveland
With Time, The Pathology of PD Spreads Throughout the Brain Braak s staging of Parkinson s disease pathology dm co sn mc hc fc 1 Hubert H. Fernandez, MD, FAAN Professor of Medicine (Neurology) Cleveland
Pharmacological treatment of Parkinson's disease
 Pharmacological treatment of Parkinson's disease Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon PD PROGRESSION DISABILITY instability
Pharmacological treatment of Parkinson's disease Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon PD PROGRESSION DISABILITY instability
CENTENE PHARMACY AND THERAPEUTICS NEW DRUG REVIEW 3Q17 July August
 BRAND NAME Xadago GENERIC NAME Safinamide MANUFACTURER Newron Pharmaceuticals SpA holds license; granted approval. US WorldMeds, LLC exclusive licensee and distributor in the U.S. DATE OF APPROVAL March
BRAND NAME Xadago GENERIC NAME Safinamide MANUFACTURER Newron Pharmaceuticals SpA holds license; granted approval. US WorldMeds, LLC exclusive licensee and distributor in the U.S. DATE OF APPROVAL March
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition Joint Session with ACOFP and Cleveland
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition Joint Session with ACOFP and Cleveland
Re-Submission. Scottish Medicines Consortium. rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd.
 (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd.") Scottish Medicines Consortium Re-Submission rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd 10 November 2006 The Scottish Medicines Consortium (SMC) has completed
Scottish Medicines Consortium Re-Submission rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd 10 November 2006 The Scottish Medicines Consortium (SMC) has completed
Parkinsons Disease update. Sindhu R Srivatsal MD MPH Virginia Mason Medical Center
 Parkinsons Disease update Sindhu R Srivatsal MD MPH Virginia Mason Medical Center PARKINSONISM Vs PARKINSON S Parkinsonism Bradykinesia: slowness of movements (essential feature) PLUS one of Tremor: resting
Parkinsons Disease update Sindhu R Srivatsal MD MPH Virginia Mason Medical Center PARKINSONISM Vs PARKINSON S Parkinsonism Bradykinesia: slowness of movements (essential feature) PLUS one of Tremor: resting
Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016
 Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016") Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016 What is Parkinson s? Parkinson's is a progressive neurological condition. People
Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016 What is Parkinson s? Parkinson's is a progressive neurological condition. People
Novel approaches to the pharmacological treatment of Parkinson s disease. Peter Jenner King s College UK
 Novel approaches to the pharmacological treatment of Parkinson s disease Peter Jenner King s College UK Disclosures and Disclaimers Speakers fees and consultancy fees have been received from Britannia
Novel approaches to the pharmacological treatment of Parkinson s disease Peter Jenner King s College UK Disclosures and Disclaimers Speakers fees and consultancy fees have been received from Britannia
EMERGING TREATMENTS FOR PARKINSON S DISEASE
 EMERGING TREATMENTS FOR PARKINSON S DISEASE Katerina Markopoulou, MD, PhD Director Neurodegenerative Diseases Program Department of Neurology NorthShore University HealthSystem Clinical Assistant Professor
EMERGING TREATMENTS FOR PARKINSON S DISEASE Katerina Markopoulou, MD, PhD Director Neurodegenerative Diseases Program Department of Neurology NorthShore University HealthSystem Clinical Assistant Professor
Update in the Management of Parkinson s Disease
 Update in the Management of Parkinson s Disease What s standard? What s new? What s coming? Bruno V. Gallo, M.D. Assistant Professor of Neurology, FIU Wertheim College of Medicine Director, Parkinson &
Update in the Management of Parkinson s Disease What s standard? What s new? What s coming? Bruno V. Gallo, M.D. Assistant Professor of Neurology, FIU Wertheim College of Medicine Director, Parkinson &
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
05-Nov-15. Impact of Parkinson s Disease in Australia. The Nature of Parkinson s disease 21st Century
 Peter Silburn Professor Clinical Neuroscience University of Queensland Queensland Brain Institute Neurosciences Queensland Impact of in Australia Second most common neurodegenerative disorder Up to 64,000
Peter Silburn Professor Clinical Neuroscience University of Queensland Queensland Brain Institute Neurosciences Queensland Impact of in Australia Second most common neurodegenerative disorder Up to 64,000
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Update on Parkinson s disease and other Movement Disorders October 2018
 Update on Parkinson s disease and other Movement Disorders October 2018 DR. JONATHAN EVANS CONSULTANT IN NEUROLOGY QUEEN S MEDICAL CENTRE NOTTINGHAM Disclosures: Honoraria UCB, Britannia, Allergan, AbbVie
Update on Parkinson s disease and other Movement Disorders October 2018 DR. JONATHAN EVANS CONSULTANT IN NEUROLOGY QUEEN S MEDICAL CENTRE NOTTINGHAM Disclosures: Honoraria UCB, Britannia, Allergan, AbbVie
Clinical Guideline for the management of inpatients with Parkinson s disease
 Clinical Guideline for the management of inpatients with Parkinson s disease Introduction: Parkinson s disease (PD) is the second most common neurodegenerative disorder, characterised by bradykinesia,
Clinical Guideline for the management of inpatients with Parkinson s disease Introduction: Parkinson s disease (PD) is the second most common neurodegenerative disorder, characterised by bradykinesia,
MAXIMIZING FUNCTION IN PARKINSON S DISEASE
 1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
PL CE LIVE July 2015 Forum
 July 2015 PL CE LIVE Rachel Maynard, PharmD Associate Editor Pharmacist s Letter/Pharmacy Technician s Letter CE Information Pharmacist's Letter / Therapeutic Research Center is accredited by the Accreditation
July 2015 PL CE LIVE Rachel Maynard, PharmD Associate Editor Pharmacist s Letter/Pharmacy Technician s Letter CE Information Pharmacist's Letter / Therapeutic Research Center is accredited by the Accreditation
Parkinson s Disease Update. Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015
 Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Drug Therapy of Parkinsonism. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
BORDEAUX MDS WINTER SCHOOL FOR YOUNG
 BORDEAUX MDS WINTER SCHOOL FOR YOUNG NEUROLOGISTS INFUSION THERAPIES IN PARKINSON S DISEASE Apomorphine, T. Henriksen Tove Henriksen, MD MDS Clinic University Hospital of Bispebjerg, Copenhagen MOTOR FLUCTUATIONS
BORDEAUX MDS WINTER SCHOOL FOR YOUNG NEUROLOGISTS INFUSION THERAPIES IN PARKINSON S DISEASE Apomorphine, T. Henriksen Tove Henriksen, MD MDS Clinic University Hospital of Bispebjerg, Copenhagen MOTOR FLUCTUATIONS
Non-Motor Symptoms of Parkinson s Disease
 Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
PDL Class: Parkinson s Drugs
 Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review: September 2013 Date of Last Review:
Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review: September 2013 Date of Last Review:
Advances in Parkinson s Disease Treatment. Ryan J. Uitti, M.D. Professor of Neurology Mayo Clinic, Jacksonville, FL
 Advances in Parkinson s Disease Treatment Ryan J. Uitti, M.D. Professor of Neurology Mayo Clinic, Jacksonville, FL Uitti.ryan@mayo.edu Ryan J. Uitti, MD Disclosure receives research support from NIH/NINDS,
Advances in Parkinson s Disease Treatment Ryan J. Uitti, M.D. Professor of Neurology Mayo Clinic, Jacksonville, FL Uitti.ryan@mayo.edu Ryan J. Uitti, MD Disclosure receives research support from NIH/NINDS,
See Policy CPT/HCPCS CODE section below for any prior authorization requirements
 Effective Date: 1/1/2019 Section: SUR Policy No: 395 1/1/19 Medical Policy Committee Approved Date: 8/17; 2/18; 12/18 Medical Officer Date APPLIES TO: Medicare Only See Policy CPT/HCPCS CODE section below
Effective Date: 1/1/2019 Section: SUR Policy No: 395 1/1/19 Medical Policy Committee Approved Date: 8/17; 2/18; 12/18 Medical Officer Date APPLIES TO: Medicare Only See Policy CPT/HCPCS CODE section below
The Fresco Institute for Parkinson's and Movement Disorders
 The Fresco Institute for Parkinson's and Movement Disorders Follow Up Patient Questionnaire Name: Date: Accompanied by: Do you smoke? CURRENT PAST NEVER Which neurological symptom bothers you most right
The Fresco Institute for Parkinson's and Movement Disorders Follow Up Patient Questionnaire Name: Date: Accompanied by: Do you smoke? CURRENT PAST NEVER Which neurological symptom bothers you most right
Drugs used in Parkinsonism
 Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Surgical Treatment of Movement Disorders. Surgical Treatment of Movement Disorders. New Techniques: Procedure is safer and better
 Surgical Treatment of Movement Stephen Grill, MD, PHD Johns Hopkins University and Parkinson s and Movement Center of Maryland Surgical Treatment of Movement Historical Aspects Preoperative Issues Surgical
Surgical Treatment of Movement Stephen Grill, MD, PHD Johns Hopkins University and Parkinson s and Movement Center of Maryland Surgical Treatment of Movement Historical Aspects Preoperative Issues Surgical
Deep Brain Stimulation. Is It Right for You?
 Deep Brain Stimulation Is It Right for You? Northwestern Medicine Deep Brain Stimulation What is DBS? Northwestern Medicine Central DuPage Hospital is a regional destination for the treatment of movement
Deep Brain Stimulation Is It Right for You? Northwestern Medicine Deep Brain Stimulation What is DBS? Northwestern Medicine Central DuPage Hospital is a regional destination for the treatment of movement
History Parkinson`s disease. Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson
 Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinson s disease. Information for patients and carers. The Leeds Teaching Hospitals NHS Trust
 n The Leeds Teaching Hospitals NHS Trust Parkinson s disease Information for patients and carers in partnership with Leeds Community Healthcare NHS Trust The symptoms of Parkinson s appear when the levels
n The Leeds Teaching Hospitals NHS Trust Parkinson s disease Information for patients and carers in partnership with Leeds Community Healthcare NHS Trust The symptoms of Parkinson s appear when the levels
ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO?
 ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO? You may have noticed a change... Levodopa is a common treatment for Parkinson s, and doctors have relied on it for decades. Over time as Parkinson s progresses,
ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO? You may have noticed a change... Levodopa is a common treatment for Parkinson s, and doctors have relied on it for decades. Over time as Parkinson s progresses,
9/26/18. Objectives. Disclosures. Parkinson s Disease Update Clinical and Operational Considerations
 Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Any interventions, where RCTs in PD are not available, are not included in the tables.
 Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Individual Study Table Referring to Part of Dossier: Volume: Page:
 Synopsis Abbott Laboratories Name of Study Drug: DUODOPA Intestinal Gel Name of Active Ingredient: Levodopa-carbidopa Individual Study Table Referring to Part of Dossier: Volume: Page: (For National Authority
Synopsis Abbott Laboratories Name of Study Drug: DUODOPA Intestinal Gel Name of Active Ingredient: Levodopa-carbidopa Individual Study Table Referring to Part of Dossier: Volume: Page: (For National Authority
TRANSPARENCY COMMITTEE OPINION. 18 March 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 March 2009 REQUIP LP 2 mg extended-release tablet Box of 21 tablets (CIP: 379 214-8) Box of 28 tablets (CIP: 379
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 March 2009 REQUIP LP 2 mg extended-release tablet Box of 21 tablets (CIP: 379 214-8) Box of 28 tablets (CIP: 379
Depression & Anxiety. What can I do? What are other possible treatments? What is this? Why does this happen? KEY POINTS
 Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
PARKINS ON CENTER. Parkinson s Disease: Diagnosis and Management. Learning Objectives: Recognition of PD OHSU. Disclosure Information
 OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant: