Parkinson s disease Dementia Clinical Features and Treatments
|
|
|
- Joleen Knight
- 5 years ago
- Views:
Transcription

1 Parkinson s disease Dementia Clinical Features and Treatments Dr Susan H Fox MRCP (UK), PhD Associate Professor Neurology University of Toronto Movement Disorders Clinic, Toronto Western Hospital JAN 22 nd 2015
2 Objectives To review the clinical features of cognitive impairment in PD To review treatment options for cognitive problems.
3 Neuropsychiatric symptoms in PD a) Mood: Anxiety, Depression, irritability, panic attacks, apathy, fatigue b) Psychotic symptoms; Euphoria, agitation, hallucinations, delusions, paranoia c) Cognitive dysfunction: Dementia; Mild cognitive impairment (MCI)
4 Neuropsychiatric manifestations in Parkinson's Disease are a major cause of morbidity. 14,354 Medicare beneficiaries with YOPD Compared to the general population of medically disabled Americans, those with YOPD were more likely to receive medical care for depression (OR: 1.89, ), dementia (OR: 7.73, ), substance abuse/dependence (OR: 3.00, ) psychosis (OR: 3.36, ), personality/impulse control disorders (OR: 4.56, ) psychosocial dysfunction (OR: 3.85, ). Willis et al Parkinsonism and Related Disord 2013 Feb;19(2):202-6.
5 PD Dementia Dementia is common Affects 30-80% of advanced PD. Hely MA, et al. The Sydney multicenter study of Parkinson's disease: the inevitability of dementia at 20 years. Mov Disord 2008;23: Aarsland D, Kurz MW. The epidemiology of dementia associated with Parkinson disease. J Neurol Sci 2010;289(1-2):18-22.

6 Dementia as Milestone marker of PD Four milestones in progression of PD 1. Falls 2. Hallucinations 3. Dementia 4. Nursing home care progression Once milestone is reached the average time to death is the same about 5y regardless of age-ofdisease onset Kempster PA, et al Brain 2010;133:
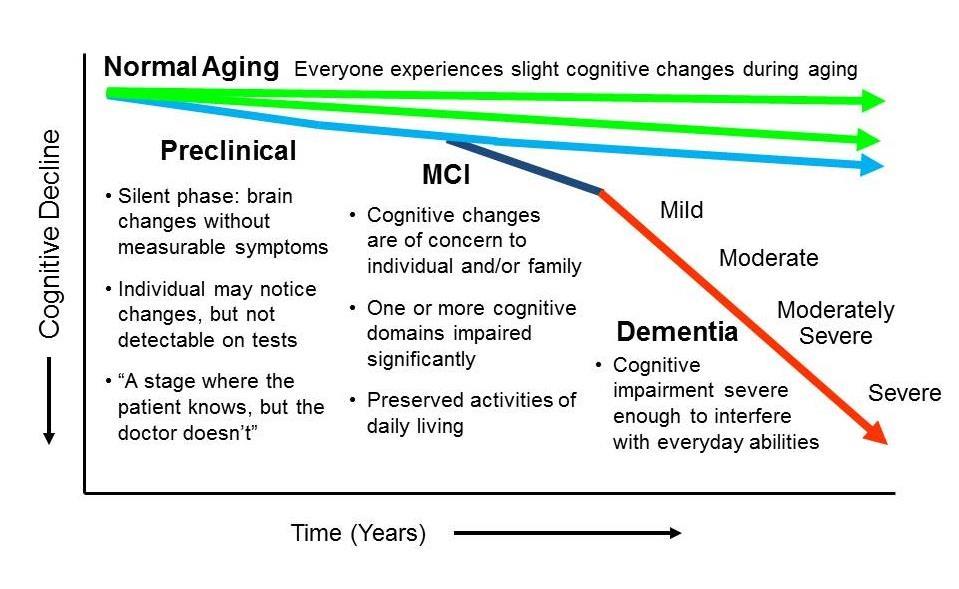
7 What is Dementia in PD? Gradual cognitive decline within the context of Parkinson Disease Decline in function what was (premorbid) baseline? Heterogeneous cognitive domains affected Executive function; attention, learning and memory, verbal fluency, visuospatial abilities > 1 domain affected Severe enough to impact Activities of Daily Living
8 Diagnostic Criteria for PDD Emre et al Mov Disord 2007;22:
 No significant functional impairment as a result of cognitive deficit Affects 15-30% of early PD patients")
9 Mild Cognitive Impairment (MCI) Definition 1) A complaint of cognitive dysfunction 2) Scores of at least 1.5 standard deviations below the agecorrected mean on one or more core psychological tests 3) No significant functional impairment as a result of cognitive deficit Affects 15-30% of early PD patients Litvan et al Mov Disord 2012;27: Yarnall et el. Characterizing mild cognitive impairment in incident Parkinson disease; the ICICLE-PD Study : Neurology ;82(4):308-16
10 How to assess cognitive function in PD 1. Cognitive Screening Tests 2. Neuropsychological Assessments 3. Research studies Diagnostic Criteria/Imaging studies ( Dr Monchi)

11 1. Cognitive Screening Tests Marras et al Mov Disor 2014;29:
12 1. Cognitive Screening Tests MOCA is possibly better screen than MMSE MoCA possibly better due to ability to detect executive dysfunction; a relative deficiency of the MMSE Quick screens? Incorrect hippo response Pill questionnaire Head-Turning Sign
13 Incorrect response = Hippo rather than Rhino
14 The incorrect Hippo response can predict an abnormal MoCA 117 non-demented PD subjects 27 (23%) incorrectly responded hippo to the rhinoceros naming item on the MoCA Hippo responders scored significantly lower on the MoCA and MMSE. Poor scores on tasks requiring visuospatial and executive abilities across testing modalities. Armstrong, Fox, Marras et al ParkRel Dis2013 The meaning of a "hippo" response on the Montreal Cognitive Assessment in Parkinson's disease.

15 The Pill Questionnaire did not show sensitivity or specificity enough to be used as a single screen However inaccurate reporting is associated with deficits in many cognitive domains an should be an alerting factor
16 Head-Turning Sign
17 PD-specific Cognitive Screens Longer to administer Not fully evaluated for reliability in PD, as yet Marras et al Mov Disord 2014;29:
18 2. Neuropsychological Assessments 1. Estimate of premorbid function/intelligence 2. Language 3. Attention 4. Processing speed 5. Executive function 6. Learning and Memory 7. Visuo-spatial Gold Standard Neuropsychology/Trained administrator Long Time = 2h Affected by: Time of day Medications Co-morbidities - depression etc.
19 Symptoms that are often associated or preludes to cognitive decline in PD Depression and Anxiety Apathy Psychosis- visual hallucinations


20 Psychosis Features Vivid dreams/nightmares Illusions Hallucinations Paranoid delusions
21 Hallucinations in PD Visual most common Can affect up to 50% of PD patients Typically are well-formed hallucinations of people, animals, insects; Veridical Usually occur on going to sleep and on awakening Frequently stable, and chronic Rarely auditory; tactile
22 Parkinson's disease Dementia vs Dementia with Lewy Bodies Parkinson's disease Dementia (PDD) Later onset dementia Occurs after many years of typical levodopa-responsive PD Pathological- alpha synuclein deposition Dementia with Lewy Bodies (DLB) Early onset dementia, before or within one year of motor symptoms Fluctuations with pronounced variations in attention and alertness Visual hallucinations ++ Older age Autonomic symptoms ++ REM sleep behavior disorder Very sensitive to drugs esp any neuroleptics Cortical Lewy Body Disease (CLBD) = pathological term for extensive alpha synuclein deposition in cortex
23 DLB Alzheimer Disease PD PD Dementia Extrapyramidal symptoms Often more symmetric Rare, usually mild in late stages Initially often asymmetric Initially often asymmetric PIGD subtype 69% - 38% 88% - TD subtype 31% - 62% 12% Hypomimia 48.5% 4.2% - Hypophonia 30.8% 3.4% - Rigidity 44.6% 9.8% - Impaired posture/gait 43.1% 14.2% - Bradykinesia 55.4% 19.3% - Impaired chair rise 28.9% 15.4% - Postural instability 26.2% 12.5% - Resting tremor 13.9% 3.2% - Action/postural tremor 12.3% 6.2% Cognitive impairment Early disturbances in attention & Early impairment of declarative Impaired executive and Impaired executive and visuoperceptive functions memory & attention visuoperceptive functions visuoperceptive functions Fluctuations in cognition Neuropsychiatric symptoms Prominent, early second to hourly variations Moderate day to day variations Mild day to day variations Mild day to day variations Visual hallucinations Typical, early & persistent Sometimes, late course Often present drugs trigger Often present drugs trigger Delusions Typical Usually present Present Present Depression Usually present Usually present Usually present Usually present
24 Treating Cognitive problems in PD

25 UPDATED: 2013: Treatments for Non-Motor Symptoms of PD

26 Can J Neurol Sci. 2012;39: Suppl 4: S1-20; 26
27 Randomized Controlled Trials in PDD Cholinesterase inhibitors (daily dose) Donepezil (2.5 10mg) Outcome vs. placebo (n receiving active) (duration) POSITIVE MMSE, NEGATIVE CIBIC (n = 14) (10w) POSITIVE DRS (n = 16) ; (18w) NEGATIVE ADaSCog ; POSITIVE MMSE ((n = 22); (10w) NEGATIVE ADASCog /CGI ; POSITIVE MMSE ; (n = 550) (24 w) Refs Aarsland et al 2002 Leroi et al 2004 Ravina et al 2005 Dubois et al 2012 Rivastigmine (3 12mg) POSITIVE (ADCS-CGI and ADASCog (n = 541) (24 w) Emre et al 2004 Glutamate antagonists Memantine (10 20 mg) Outcome vs. placebo (n receiving active) (duration) NEGATIVE DRS, MMSE (n = 25) POSITIVE CGI (n = 72 ) POSITIVE ADCS-CGIC in DLB not PDD (n = 195) References Lerois et al 2009 Aarsland et al 2009 Emre et al 2010
28 6 Trials using Donepezil, Rivastigmine; n = 1236 subjects AEs more common in rivastigmine groups = Nausea and vomiting
29
30 Safety and tolerability of cholinesterase inhibitors? ECG before starting risk of prolonged QTc interval Nausea and vomiting up to 30% of patients Rivastigmine patch may be better tolerated
31 Safety and tolerability of cholinesterase inhibitors? Worsening of Parkinsonism? More patients on rivastigmine vs. placebo reported tremor as an AE but not UPDRS III» Rolinski et al Cochrane Review 2012 Open label safety study of rivastigmine oral vs patch for 76 w in PD dementia Tremor = 24% oral vs 10% patch No significant worsening of motor UPDRS in both Discontinuation rate due to worse motor scores 2% in both» Emre et al Clin Neuropharm 2014

32 Conclusions: PD Dementia Treatments - Interventions assessed in MDS EBM Reviews - Cholinesterase inhibitors Donepezil Rivastigmine Galantamine Glutamate antagonists Practice implications Possibly useful Clinically useful Possibly useful Practice implications Memantine Possibly useful
33
34 Treatments for PD-MCI? Therapy Mechanism of action Studies Donepezil Cholinesterase inhibitor (MUSTARDD-PD (NCT )- suspended due to low recruitment). DASH-PD in Japan; recruiting early PD subjects and following over 3y Rivastigmine Galantamine + Allosteric modulator of nicotinic cholinergic receptors Ongoing study using patch (NCT ) Negative DBRCT in non-demented PD (Grace et al 2009) Rasagiline Mono amine oxidase B inhibitor (MAOB-I) Safinamide MAOB-I/Glutamate release inhibition Atomoxetine Noradrenaline and serotonin reuptake inhibitor Cognitive Speed Training Positive on attention and verbal fluency (Hanagasi et al 2011) NCT and NCT ongoing Ongoing study (NCT ) Ongoing study vs donepezil for attention in nondemented PD (NCT ) Ongoing vs placebo in PD MCI (NCT ) NCT ; NCT ; NCT ongoing Positive outcomes in non-demented PD (Edwards et al 2013)
35 Management of PD Psychosis Vaughan and Goldman, Movement Disorder Emergencies: Diagnosis and Treatment, ed. S. Frucht
36 Specific treatments for psychosis in PD Atypical antipsychotic agents Quetiapine mg start with half a tablet (25mg) at night and titrate according to response Clozapine mg - Very effective start with half a tablet (25mg) at night and titrate according to response (average 50 mg) Parkinson Study Group NEJM;1999 Mar 11;340(10): Pollack et al. J Neurol Neurosurg Psychiatry May;75(5):689-95
37 Safety issues: Side effects: Clozapine for PD sedation, increased drooling, occasional Orthostatic hypotension Leukopenia: regular blood counts required (initially weekly 2 weekly 2 monthly) 1-2% in the pre-cnr period vs. 382 / (=0.38%) pts treated with CLZ with 12 leukopenia-related deaths (= %) * 6 / 187 pts with psychosis in PD included into RCTs (transient) *Honigfeld et al., J Clin Psychiatry; 1998 (CNR database ) CNR = Clozaril National Registry
38 Safety issues with using atypical antipsychotics for psychosis in PD general safety issues to consider in elderly patients: antipsychotics (including atypicals) are associated with a similarly increased risk for all-cause mortality cerebrovascular events in elderly patients with dementia Trifiro G et al. Use of antipsychotics in elderly patients with dementia: do atypical and conventional agents have a similar safety profile? Pharmacol Res. 2009;59:1 12. Bullock R. Treatment of behavioural and psychiatric symptoms in dementia: implications of recent safety warnings. Curr Med Res Opin. 2005;21:1 10.
39 Avoid other atypical neuroleptics Olanzapine Risperdone Aripiprezole All worsen PD Goetz et al Olanzapine and clozapine: comparative effects on motor function in hallucinating PD patients. Neurology 2000 Sep 26;55(6): Friedmnan et al. Open-label flexible-dose pilot study to evaluate the safety and tolerability of aripiprazole in patients with psychosis associated with Parkinson's disease. Mov Disord 2006 Dec;21(12):
40 DLB Treatment options Cholinesterase inhibitors help Hallucinations and cognition Quetiapine or Clozapine Help sleep and Hallucinations Minimise non-essential centrally acting drugs very poorly tolerated
41 Clinical pearls for cognitive dysfunction in PD Simple in clinic screens head-turning sign; Pill Questionnaire Watch out for younger PD patient with work-related anxiety - multitasking jobs a common reason for stopping work. Maybe a prelude to cognitive decline Depression /anxiety are often a prelude to dementia Subjects with MOCA < 25 should stop driving PD patients with dementia are extremely sensitive to medications per se; Reduce drug load to minimum Social support networks and education of care givers are important for long term care of PD Dementia
42 Support Alzheimer Society's website at or contact your local Alzheimer Society. For more information on PD, please visit the Parkinson Society Canada Additional Resources: Alzheimer s Association: Alzheimer Europe: europe.org/dementia/other-forms-of-dementia/neuro-degenerative- Diseases/Dementia-in-Parkinson-s-disease-PDD?#fragment-1 Alzheimer s Society UK: ttp:// entid=135



43 Parkinson s disease Dementia: Research and non-medication treatments exploration Oury Monchi, PhD, Tourmaline Oil Chair in Parkinson s disease, Movement Disorders Program, Departments of Clinical Neurosciences and Radiology, Hotchkiss Brain Institute, Cumming School of Medecine, University of Calgary.

44 Parkinson s Disease

45 Non-motor deficits Benjamin Ball, France 1855 Visual hallucinations in PD Intellectual perturbation is not Just a coincidence nor irritability linked to the diagnosis, but an Integral part of the disease Largely forgotten until end of 20 th century

46 End of 1980 s


47 Cognitive deficits Executive deficits: higher order processes that are used when planning, problem-solving initiating a new task. Attention difficulties: Problems in focusing or dividing attention in complex situations. In real life, this may translate into difficulties in resisting to distraction

48 Cognitive Deficits Visio-spatial problems: Problems in estimating distances, Discriminating and acting on visual information. This can sometimes increase the risk of falls. In real life this may translate in difficulties in orientation in an environment with complex visual stimuli, such as finding a specific isle in a supermarket. At the later stages of the disease, illusions or little hallucinations are observed in some patients only.

49 Cognitive Deficits Language dysfunction: Word finding and naming deficits. Memory: Retrieving information that has already been learned. In PD the problem is mostly with recall, and not with pure semantic or encoding like can occur in Alzheimer s disease. Using a notepad can help IMPORTANT: Not all these symptoms are present in patients, and great differences exist between them.


50 Depression and Anxiety Depression is common in PD patients. A depressed person has trouble experimenting joy, may stop hobbies enjoyed before, and may not want to perform his daily routine. Diagnosis of Parkinson's disease can certainly cause stress and sadness, but depression can occur independently. Indeed a large number of patients with PD have experienced depression before they had the diagnosis Anxiety often occurs with depression in PD. They may have excessive worry about everyday things they can not control. Some people have outbreaks of anxiety called "panic attacks".
51

52 MCI very heterogeneous in Parkinson s Disease Caviness et al. (2007)
53 Prevalence longitudinal studies Broeders et al., Neurology, 2013
54 Neuroimaging anatomical MRI studies Movement Disorders, 2011


55 Method 17 PD patients with MCI 15 PD patients without MCI 18 Healthy Controls MRI 3T FreeSurfer Cortical thickness Subcortical segmentation 20 months Time 1 Time 2 Neuropsychological evaluation + MRI Neuropsychological evaluation + MRI MCI = Mild Cognitive Impairment PD = Parkinson s disease


56 Results - thickness Blue clusters = increased rate of cortical thinning PD-MCI PD-non-MCI HCs -1.34% -0.67% -0.34% Hanganu et al., Brain 2014
57 Results subcortical Mean percentage of change over time PD-MCI PD-non-MCI HCs Thalamus -1.51% -1.80% -3.71% Caudate -1.92% % Putamen -1.64% % Hippocampus -2.07% % -6.05% Amygdala -6.05% % -5.98% N. Accumbens -5.98% % Ventral striatum has an increased degradation Hanganu et al., Brain 2014
58 Neuroimaging studies fmri

59 fmri WCST Results in Young Controls: Shift-planning Isolation of a cognitive cortico-striatal loop including the ventrolateral PFC in the planning of a set-shift Monchi et al., 2001: Journal of Neuroscience, editor s choice Science and Nature Reviews Neuroscience
60 fmri WCST Results in PD-OFF and matched Controls: Shift-planning Controls PD patients Decreased activity in PD in the cognitive cortico-striatal loop during planning the set-shift Monchi et al., Journal of Neuroscience 2004 Highlighted in This Week in the Journal


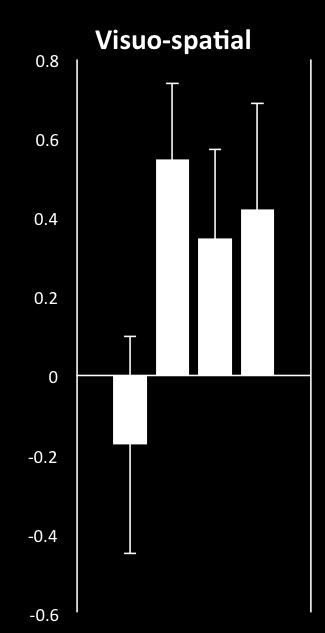
61 fmri WCST MCI vs. NON MCI OFF Negative Feedback PD NON MCI PD MCI Shift Planning vs. Control Feedback T-stat Z = +4 Z = +4 Effect more pronounced in patients with MCI
 use more the MTL eventhough it is not required")
62 Correlation with retrieval list of RAVLT T-stat 4.4 Shift Execution 3 Y=-30 Patients with better scores (memory) use more the MTL eventhough it is not required for the task Nagano-Saito et al.,2014, Neurobiology of Aging

63 Hippocampal compensation hypothesis Could the lack of MTL compensation be a marker of dementia in PD?




64 Longitudinal study fmri WCST All PD T1 correlated with MOCA evolution, Planning set-shift T-stat X=-34 X=+36 T-stat Z=+8

65 Genotypes and cognitive deficits
66 Conclusion part I Cognitive decline is very heterogeneous in PD PD dementia may occur from mixed pathologies, including some associated with AD. Studies currently taking place to find out longitudinally the differences between PD-MCI and nonpd-mci Other factors such as age, neuropsychiatric symptoms and genetics also play a role in the occurrence of dementia in PD
67 Cognitive training in PD
68 Exercise programs in PD
69

70 New possible treatments Transcranial Magnetic Stimulation (TMS)


71 Fronto-striatal connectivity during rest TBS of PFC and resting-state fmri


72 itbs and rsfmri correlation analysis L caudate nucleus seed Pre-iTBS Sham TBC Post-iTBS T-stat Z = -2 Y = -4 Z = -2 Loop affected in PD-MCI

73 Therapeutical TMS trial in PD-MCI


74 Preliminary results 10 patients active itbs neuropsychological tests


75 Preliminary results 10 patients active itbs neuropsychological tests p<0.05 * * * * *
76 Conclusion Part II Data on non-medication treatment is not yet conclusive Not enough studies Lack of guidelines Which is more beneficial? Confounding factor, being taken care of, placebo effect, social effect.. In need of proper large-scale clinical trials like for medication Nevertheless, get involved always some benefits and keep active mentally and physically as much as possible Regularity more important than intensity
The Spectrum of Lewy Body Disease: Dementia with Lewy Bodies and Parkinson's Disease Dementia
 Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Parkinsonian Disorders with Dementia
 Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University
 Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University Design of trials in DLB and PDD What has been learnt from previous trials in these indications and other dementias? Overview
Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University Design of trials in DLB and PDD What has been learnt from previous trials in these indications and other dementias? Overview
Nature, prevalence and clinical significance. Barcelona, Spain
 Nature, prevalence and clinical significance Jaime Kulisevsky Barcelona, Spain 1 Non motor (neuropsychiatric) symptoms are an integral part of Parkinson s s disease (PD) Affective disorders And are associated
Nature, prevalence and clinical significance Jaime Kulisevsky Barcelona, Spain 1 Non motor (neuropsychiatric) symptoms are an integral part of Parkinson s s disease (PD) Affective disorders And are associated
Behavioral Aspects of Parkinson s Disease
 Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Neurocognitive Disorders Research to Emerging Therapies
 Neurocognitive Disorders Research to Emerging Therapies Edward Huey, MD Assistant Professor of Psychiatry and Neurology The Taub Institute for Research on Alzheimer s Disease and the Aging Brain Columbia
Neurocognitive Disorders Research to Emerging Therapies Edward Huey, MD Assistant Professor of Psychiatry and Neurology The Taub Institute for Research on Alzheimer s Disease and the Aging Brain Columbia
Psychosis and Agitation in Dementia
 Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Coordinating Care Between Neurology and Psychiatry to Improve the Diagnosis and Treatment of Parkinson s Disease Psychosis
 Coordinating Care Between Neurology and Psychiatry to Improve the Diagnosis and Treatment of Parkinson s Disease Psychosis Jeff Gelblum, MD Senior Attending Neurologist Mt. Sinai Medical Center Miami,
Coordinating Care Between Neurology and Psychiatry to Improve the Diagnosis and Treatment of Parkinson s Disease Psychosis Jeff Gelblum, MD Senior Attending Neurologist Mt. Sinai Medical Center Miami,
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Appendix N: Research recommendations
 Appendix N: recommendations N.1 First-line treatment of motor symptoms recommendation 1 Interventions What is the effectiveness of initial levodopa monotherapy versus initial levodopa-dopamine agonist
Appendix N: recommendations N.1 First-line treatment of motor symptoms recommendation 1 Interventions What is the effectiveness of initial levodopa monotherapy versus initial levodopa-dopamine agonist
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Revised criteria for the clinical diagnosis of dementia with Lewy. Dementia with Lewy bodies. (Dementia with Lewy Bodies)
") Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Dementia in Parkinson s disease:
 Dementia in Parkinson s disease: A 20 year Prospective Neuropsychological Study Sydney Multicentre Study Associate Professor Wayne GJ Reid PhD FAPS 149 newly diagnosed community living Parkinson s Disease
Dementia in Parkinson s disease: A 20 year Prospective Neuropsychological Study Sydney Multicentre Study Associate Professor Wayne GJ Reid PhD FAPS 149 newly diagnosed community living Parkinson s Disease
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias. Aaron H. Kaufman, MD
 Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Alison Charleston 1 st September 2016
 Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE
 CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask. Presented By: Tuesday, March 22, 2011 at 1:00 PM ET
 PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018
 Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Cognitive enhancers PINCH ME. Anticholinergic burden BPSD. Agitation, Aggression and antipsychotics
 Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
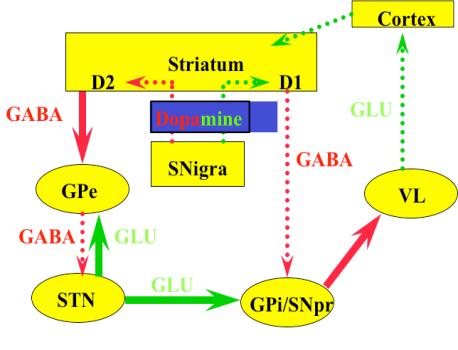
Basal ganglia motor circuit
 Parkinson s Disease Basal ganglia motor circuit 1 Direct pathway (gas pedal) 2 Indirect pathway (brake) To release or augment the tonic inhibition of GPi on thalamus Direct pathway There is a tonic inhibition
Parkinson s Disease Basal ganglia motor circuit 1 Direct pathway (gas pedal) 2 Indirect pathway (brake) To release or augment the tonic inhibition of GPi on thalamus Direct pathway There is a tonic inhibition
How to Diagnose Early (Prodromal) Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.
 Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.") How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
DEMENTIA IN PARKINSON`S DISEASE. DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD
 Director-Parkinson`s Disease Service for the Older Person HNELHD") DEMENTIA IN PARKINSON`S DISEASE DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD DEMENTIA IN PD The concept of Non Motor Symptoms in PD Dementia in Parkinson`s
DEMENTIA IN PARKINSON`S DISEASE DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD DEMENTIA IN PD The concept of Non Motor Symptoms in PD Dementia in Parkinson`s
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA
 BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Psychiatric aspects of Parkinson s disease an update
 Psychiatric aspects of Parkinson s disease an update Dr Chris Collins 027 2787593 chris.collins@cdhb.health.nz Disclosures: none Non-motor aspects physical Sensory anosmia, visual symptoms Speech and
Psychiatric aspects of Parkinson s disease an update Dr Chris Collins 027 2787593 chris.collins@cdhb.health.nz Disclosures: none Non-motor aspects physical Sensory anosmia, visual symptoms Speech and
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
The place for treatments of associated neuropsychiatric and other symptoms
 The place for treatments of associated neuropsychiatric and other symptoms Luca Pani dg@aifa.gov.it London, 25 th November 2014 Workshop on Alzheimer s Disease European Medicines Agency London, UK Public
The place for treatments of associated neuropsychiatric and other symptoms Luca Pani dg@aifa.gov.it London, 25 th November 2014 Workshop on Alzheimer s Disease European Medicines Agency London, UK Public
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Disclosure. Speaker Bureaus. Grant Support. Pfizer Forest Norvartis. Pan American Health Organization/WHO NIA HRSA
 Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
NEUROPSYCHOMETRIC TESTS
 NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
Enhanced Primary Care Pathway: Parkinson s Disease
 Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
Parkinson s Disease Psychosis: Hallucinations Delusions and Paranoia
 Parkinson s Disease Psychosis: Hallucinations Delusions and Paranoia Christopher G. Goetz, MD Professor of Neurological Sciences Professor of Pharmacology Rush University Medical Center Parkinson s Foundation
Parkinson s Disease Psychosis: Hallucinations Delusions and Paranoia Christopher G. Goetz, MD Professor of Neurological Sciences Professor of Pharmacology Rush University Medical Center Parkinson s Foundation
Clinical Trial Designs for RCTs focussing on the Treatment of Agitation in people with Alzheimer s disease
 Clinical Trial Designs for RCTs focussing on the Treatment of Agitation in people with Alzheimer s disease Professor Clive Ballard Dr Byron Creese University of Exeter, UK Guardian guide for 2018: Top
Clinical Trial Designs for RCTs focussing on the Treatment of Agitation in people with Alzheimer s disease Professor Clive Ballard Dr Byron Creese University of Exeter, UK Guardian guide for 2018: Top
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care.
 Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Any interventions, where RCTs in PD are not available, are not included in the tables.
 Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
PROJECTION: Worlds dementia population is expected to triple by 2050
 DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Cognitive-Motor Interference in Persons with Parkinson Disease
 Cognitive-Motor Interference in Persons with Parkinson Disease Tara L. McIsaac, PhD, PT Associate Professor of Physical Therapy A.T. Still University Arizona School of Health Sciences October 11, 2014
Cognitive-Motor Interference in Persons with Parkinson Disease Tara L. McIsaac, PhD, PT Associate Professor of Physical Therapy A.T. Still University Arizona School of Health Sciences October 11, 2014
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Greg Jicha, M.D., Ph.D. Associate Professor of Neurology The Robert T. & Nyles Y. McCowan Chair in Alzheimer s Research University of Kentucky
 Greg Jicha, M.D., Ph.D. Associate Professor of Neurology The Robert T. & Nyles Y. McCowan Chair in Alzheimer s Research University of Kentucky Alzheimer s Disease Center and the Sanders-Brown Center on
Greg Jicha, M.D., Ph.D. Associate Professor of Neurology The Robert T. & Nyles Y. McCowan Chair in Alzheimer s Research University of Kentucky Alzheimer s Disease Center and the Sanders-Brown Center on
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Update on First Psychotic Episodes in Childhood and Adolescence. Cheryl Corcoran, MD Assistant Professor of Psychiatry Columbia University
 Update on First Psychotic Episodes in Childhood and Adolescence Cheryl Corcoran, MD Assistant Professor of Psychiatry Columbia University Childhood-Onset Psychosis 8% of psychiatrically referred youth
Update on First Psychotic Episodes in Childhood and Adolescence Cheryl Corcoran, MD Assistant Professor of Psychiatry Columbia University Childhood-Onset Psychosis 8% of psychiatrically referred youth
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
PPMI Cognitive-Behavioral Working Group. Daniel Weintraub, MD
 PPMI Cognitive-Behavioral Working Group Daniel Weintraub, MD PPMI Annual Meeting - May 6-7, 2014 Membership Daniel Weintraub WG Chair Tanya Simuni Steering Committee Shirley Lasch IND Chris Coffey, Chelsea
PPMI Cognitive-Behavioral Working Group Daniel Weintraub, MD PPMI Annual Meeting - May 6-7, 2014 Membership Daniel Weintraub WG Chair Tanya Simuni Steering Committee Shirley Lasch IND Chris Coffey, Chelsea
SCIENTIFIC DISCUSSION
 London, 2 March 2006 Product name: Prometax Procedure number: EMEA/H/C/255/II/33 SCIENTIFIC DISCUSSION 7 Westferry Circus, Canary Wharf, London, E14 4HB, UK Tel. (44-20) 74 18 84 00 Fax (44-20) 74 18 86
London, 2 March 2006 Product name: Prometax Procedure number: EMEA/H/C/255/II/33 SCIENTIFIC DISCUSSION 7 Westferry Circus, Canary Wharf, London, E14 4HB, UK Tel. (44-20) 74 18 84 00 Fax (44-20) 74 18 86
Alzheimer Disease and Related Dementias
 Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Alzheimer Disease and Related Dementias Defining Generic Key Terms and Concepts Mild cognitive impairment: (MCI) is a state of progressive memory loss after the age of 50 that is beyond what would be expected
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good?
 ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good? STEPHANIE M. OZALAS, PHARMD, BCPS, BCGP VA MARYLAND HEALTH CARE SYSTEM BALTIMORE, MD DISCLOSURES Off-label use of medications will be
ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good? STEPHANIE M. OZALAS, PHARMD, BCPS, BCGP VA MARYLAND HEALTH CARE SYSTEM BALTIMORE, MD DISCLOSURES Off-label use of medications will be
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Rational Medication Use in Dementia
 Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Non-motor symptoms as a marker of. Michael Samuel
 Non-motor symptoms as a marker of progression in Parkinson s s disease Michael Samuel London, UK 1 Definitions and their problems Non-motor symptoms as a marker of progression Non-motor symptoms (NMS)
Non-motor symptoms as a marker of progression in Parkinson s s disease Michael Samuel London, UK 1 Definitions and their problems Non-motor symptoms as a marker of progression Non-motor symptoms (NMS)
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
Approach to Cognitive Disorders in Primary Care
 Approach to Cognitive Disorders in Primary Care What can reasonably be done in an office visit? What about screening for cognitive disorders? USPSTF (2014) doesn t recommend screening: magnitude of clinically
Approach to Cognitive Disorders in Primary Care What can reasonably be done in an office visit? What about screening for cognitive disorders? USPSTF (2014) doesn t recommend screening: magnitude of clinically
Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations
 Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations Pari Deshmukh MD Triple board-certified psychiatrist (Boards of psychiatry, addiction medicine, integrative
Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations Pari Deshmukh MD Triple board-certified psychiatrist (Boards of psychiatry, addiction medicine, integrative
Parkinson s Disease. Gillian Sare
 Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
USING ANTIPSYCHOTICS TO TREAT THE BEHAVIORAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA (BPSD)- WHAT IS THE EVIDENCE?
- WHAT IS THE EVIDENCE?") USING ANTIPSYCHOTICS TO TREAT THE BEHAVIORAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA (BPSD)- WHAT IS THE EVIDENCE? Mugdha Thakur, MD Associate Professor of Psychiatry and Behavioral Sciences Duke University
USING ANTIPSYCHOTICS TO TREAT THE BEHAVIORAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA (BPSD)- WHAT IS THE EVIDENCE? Mugdha Thakur, MD Associate Professor of Psychiatry and Behavioral Sciences Duke University
Non-motor subtypes of Early Parkinson Disease in the Parkinson s Progression Markers Initiative
 Non-motor subtypes of Early Parkinson Disease in the Parkinson s Progression Markers Initiative Samay Jain, MD MSc Seo Young Park, PhD University of Pittsburgh Department of Neurology and Center for Research
Non-motor subtypes of Early Parkinson Disease in the Parkinson s Progression Markers Initiative Samay Jain, MD MSc Seo Young Park, PhD University of Pittsburgh Department of Neurology and Center for Research
Behavioral and Psychological Symptoms of dementia (BPSD)
") Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Part 2: Early detection, assessment and treatment in relation to the new guidelines. Christopher Patterson McMaster University
 Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Prof Tim Anderson. Neurologist University of Otago Christchurch
 Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
Commonly encountered medications and their side effects - what the generalist needs to know
 Commonly encountered medications and their side effects - what the generalist needs to know Jeremy Cosgrove Consultant Neurologist Leeds Teaching Hospitals NHS Trust Outline: Parkinson s medications and
Commonly encountered medications and their side effects - what the generalist needs to know Jeremy Cosgrove Consultant Neurologist Leeds Teaching Hospitals NHS Trust Outline: Parkinson s medications and
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Date of Referral: Enhanced Primary Care Pathway: Parkinson s Disease
 Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
Drugs used to relieve behavioural and psychological symptoms in dementia
 alzheimers.org.uk Drugs used to relieve behavioural and psychological symptoms in dementia People with dementia may develop behavioural and psychological symptoms including restlessness, aggression, delusions,
alzheimers.org.uk Drugs used to relieve behavioural and psychological symptoms in dementia People with dementia may develop behavioural and psychological symptoms including restlessness, aggression, delusions,
Psychotropic Strategies Handout Package
 Psychotropic Strategies Handout Package Psychotropic Strategies Learning Objectives Utilize all clinical information available Assess the patient s overall condition this is essential Basic Principles
Psychotropic Strategies Handout Package Psychotropic Strategies Learning Objectives Utilize all clinical information available Assess the patient s overall condition this is essential Basic Principles
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Acetylcholinesterase inhibitors: donepezil, rivastigmine, tacrine or galantamine for non-alzheimer s dementia
 STEER 2002; Vol 2: No.2 Acetylcholinesterase inhibitors: donepezil, rivastigmine, tacrine or galantamine for non-alzheimer s dementia Bunmi Fajemisin Evidence search date: November 2001 www.signpoststeer.org
STEER 2002; Vol 2: No.2 Acetylcholinesterase inhibitors: donepezil, rivastigmine, tacrine or galantamine for non-alzheimer s dementia Bunmi Fajemisin Evidence search date: November 2001 www.signpoststeer.org