Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
|
|
|
- Sandra Hampton
- 5 years ago
- Views:
Transcription
1 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
2 Nothing to disclose
3 Dementia Progressive deterioration in mental function including; Cognition (learning, memory, attention), language, social skills Personality and behavior Executive functions Visual perceptual functions (vision)
4 Classification Degenerative Alzheimer s Disease Lewy Body Disease Frontoemporal Dementia Non-Degenerative Vascular Paraneoplastic Autoimmune Inflammatory Prion Disordes (CJD)
5 Alzheimer s Disease In 2015, 5.3 million American had Alzheimer s Disease (AD) 5.1 million are over the age of 65 and less than age 65 Two thirds of persons with AD are women Older African-American and Hispanics more likely to have AD. By 2025 the number of people with AD n the United States expected to rise to 7.5 million (40% increase) and to 13.8 million by 2050
6 Risk Factors Age (Mild Cognitive Impairment) Family history Genetics Apoe-e4 allele Presenile 1 (PS1) Presenile 2 (PS2) Amyloid Precusor Protein (APP) Traumatic Brain Injury Hypertension, hypercholesterolemia, diabetes, stroke, heart disease
7 Four Presentation Variants of AD Amnestic (Main deficit is memory) Visual (Main deficit is vision, Posterior Cortical Atrophy) Aphasic (Main deficit is language) Behavioral (Main deficit is behavioral changes) Each presentation is associated with a specific pattern of amyloid and tau deposition

")

8 BvAD Logopenic dementia (LaAD) Amnestic AD PCA
9 Normal Cognitive Continuum Mild Cognitive Impairment Alzheimer's Disease CP
10 Successful aging MCI Typical aging Function Dementia Time

11 Mild Cognitive Impairment MCI AD 12%/yr Control AD 1-2%/yr 50 Initial exam Months 50 Initial exam Months Petersen RC et al: Arch Neurol 56: , 1999 CP
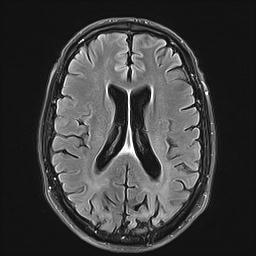
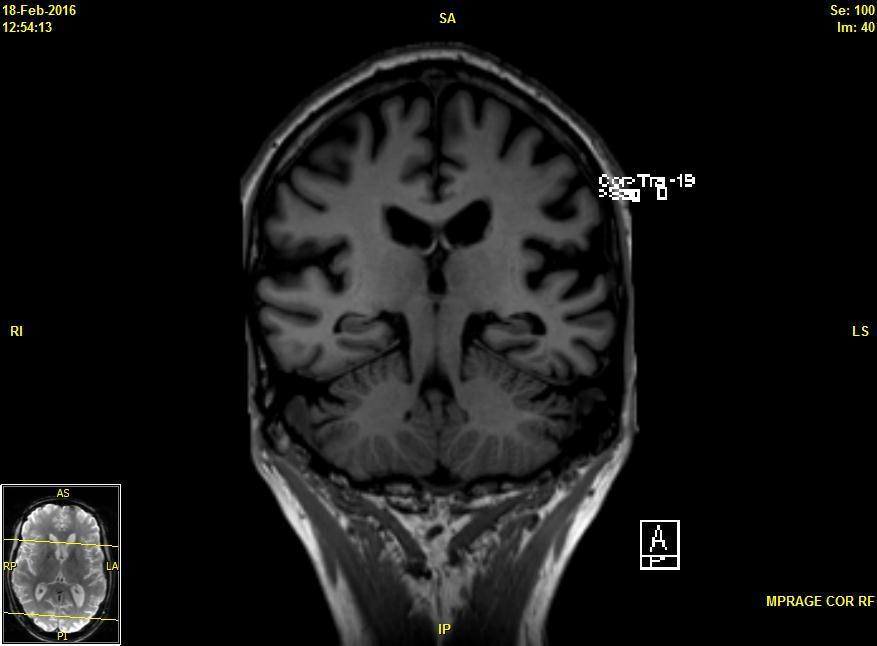
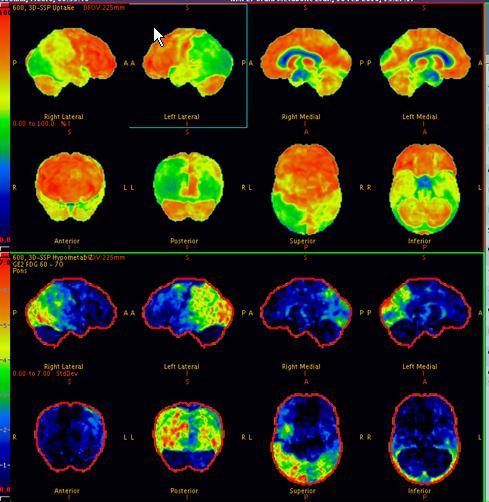
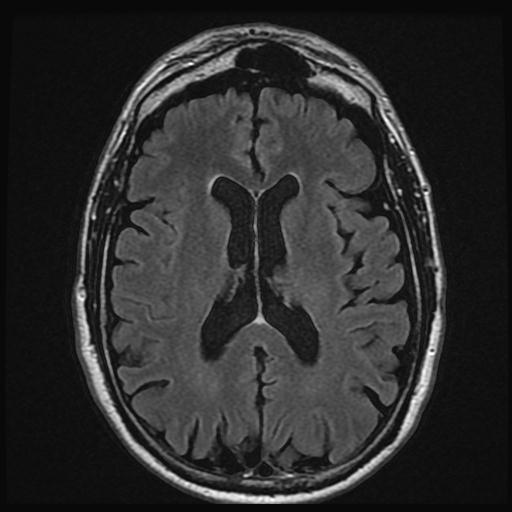
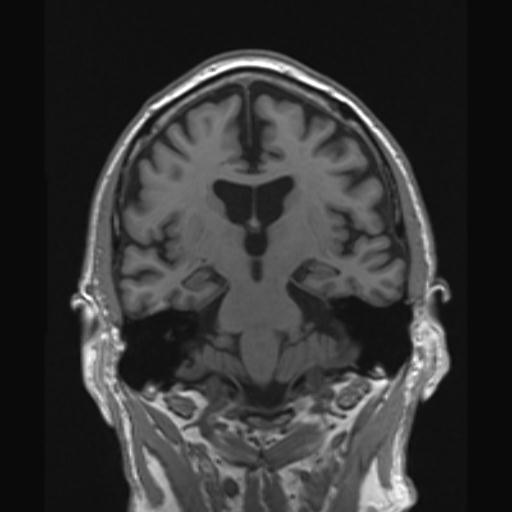
12 Diagnosis of Alzheimer s Disease History Neurological Exam Neuropsychological Testing (can quantify and characterize cognitive domains affected) Neuroimaging Structural; CT and MRI Functional; SPECT and PET Amyloid Imaging; CSF markers
13
14

15 Alzheimer s Disease Amyloid Scan

16 CSF Markers of Alzheimer s Disease
17 Treatment of Alzheimer s Disease Only two FDA approved meds Cholinesterase Inhibitors Donepezil, Rivastigmine, Galantamine Inhibits the enzyme acetylcholinesterase from breaking down acetylcholine, increasing the level and duration of action of the neurotransmitter acetylcholine Provides a window of symptomatic improvement Do not slow down the rate of progression Seem to lose effect after a few years Memantine; May be helpful in patients with severe Alzheimer s Disease
18 Lewy Body Disease The terms Dementia with Lewy Body (DLB) and Lewy Body Dementia (LBD) often used interchangeable. Second most frequent cause of dementia Incidence 3.5 per 100K, prevalence 1.3 million Neuropathology closely related to Parkinson s Disease (alpha synuclein deposition)
19 LBD Symptoms (Criteria) Central Feature Dementia (different from Alzheimer s Disease) Core Features Fluctuating cognition Complex visual hallucinations Parkinsonism (rigidity, bradikiniesia, etc) Suggestive Features REM Behavior Disorder Hypersensitivity to Neuroleptics Low dopamine transporter uptake in the basal ganglia (DAT SPECT)
20 Supportive Features Repeated falls and syncope (fainting). Transient, unexplained loss of consciousness. Autonomic dysfunction. Hallucinations of other senses, like touch or hearing. Visuospatial abnormalities. Other psychiatric disturbances.
21 REM sleep behavior disorder A parasomnia featuring: Violent dreaming, often described as being chased or attacked by people or animals Leads to violent physical activities during sleep Thrashing about in sleep Falling out of bed Striking bed partner Physical injuries A powerful predictor of subsequent DLB (or multiple system atrophy), up to 10 years later

22
23
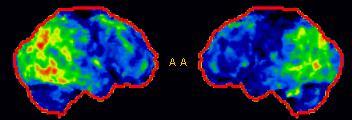
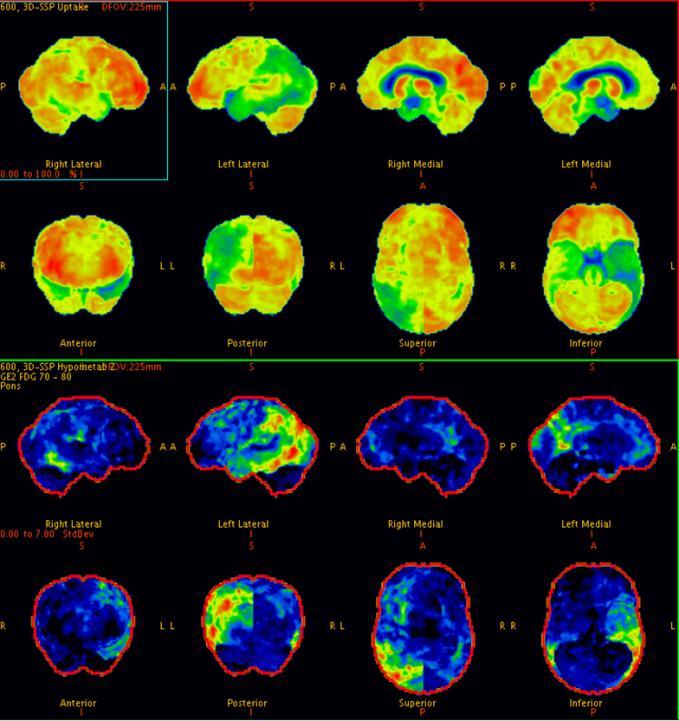
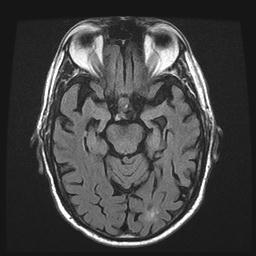
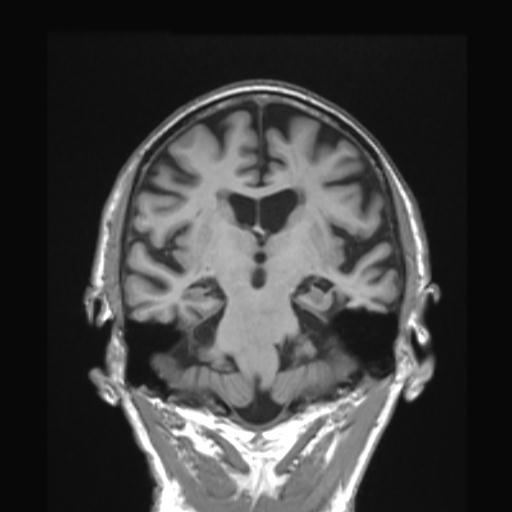
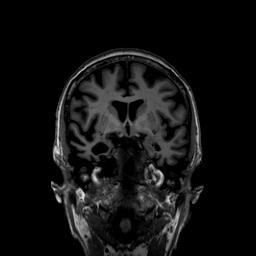
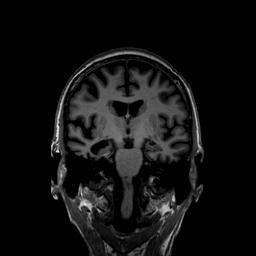
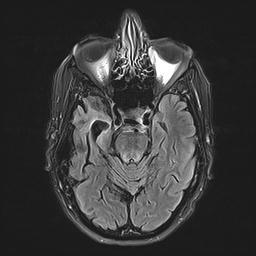
24 LBD
25

26 DATScan (high affinity for dopamine transporters)
27 Interwoven therapy of DLB Cognition Movement disorder Visual Hallucinations Sleep disorder Depression Orthostatic hypotension incontinence cholinesterase inhibitor levodopa antipsychotic clonazepam antidepressant midodrine anticholinergics Excessive daytime sleepiness?
28 Fronto-temporal Dementia Third most frequent cause of dementia Three variants, each with relatively specific brain localization (as per MRI and PET) Behavioral Language (Aphasia) Semantic Dementia (loss of word meaning) Three mutations have been associated with FTD Progranulin on Chromosome 17 C9orf72 on Chromosome 9 Microtubule Associated Protein tau on Chromosome 17 VCP Three proteins Phosphorylated Tau TAR-DNA-binding protein 43 (TDP-43) Fused in sarcoma (FUS) protein
29 Percentage Clinical syndrome by protein FTLD-tau FTLD-TDP 0 bvftd (n=128) FTD-MND (n=32) agppa (n=27) SD (n=18) PSPS (n=35) CBS (n=34) Clinical diagnosis

 lvppa logopenic variant MAPT GRN C9ORF72 MAPT Corticobasal Syndrome Progressive")
30 The FTD spectrum has been linked to genetic causes FTD -Motor Neuron Disease/ALS ALS Behavioral Variant FTD C9ORF72 GRN FUS OPTN PNF1 SOD1 TARDBP UBQLN2 VCP C9ORF72 GRN TARDBP FUS VCP C9ORF72 GRN MAPT VCP CHMP2B svppa semantic variant Sporadic nappa Nonfluent/ agrammatic variant GRN C9ORF72 MAPT-unclear (AD) lvppa logopenic variant MAPT GRN C9ORF72 MAPT Corticobasal Syndrome Progressive Supranuclear Palsy

31 Behavioral variant of FTD Most common clinical syndrome associated with FTLD Characterized by changes in behavior & personality & executive dysfunction Can be familial Can be associated with MND Variable degrees of R & L frontotemporal atrophy & hypometabolism R L Neary et al. Neurology. 1998; Rascovsky et al. Brain. 2011
32
33 Social Cognition and BvFTD Theory of Mind Understand and predict how another person thinks, feels and behaves when faced with a particular situation Empathy: perhaps one of the most magnificent of human abilities Deceit: putting ourselves in the mind of our enemies so as to prepare an ambush
34 Neurobiology of TOM There is a well defined brain system that becomes active with TOM functions There are some areas of the brain which seem to be highly dedicated to TOM functions BvFTD can affect TOM very early in its course.

35 Vollm, B. A., A. N. Taylor, et al. (2006). "Neuronal correlates of theory of mind and empathy: a functional magnetic resonance imaging study in a nonverbal task." Neuroimage 29(1): 90-8
36 Progressive non-fluent aphasia Speech output is hesitant and non-fluent Some cases familial Typically associated with atrophy of the left perisylvian region However, non-fluency was not more specifically defined and could have been secondary to word finding difficulties resulting in pauses, or to speech production impairment (apraxia of speech, AOS)



37 Semantic dementia Multimodal disorder with aphasia and agnosia Loss of word meaning Not familial Not associated with MND When aphasia is the dominant feature it is referred to as the semantic variant of PPA Left anterior medial temporal lobe atrophy Right temporal variant is usually misdiagnosed as bvftd R R L L Warrington. Q J Exp Psychol. 1975; Neary et al. Neurology. 1998; Gorno-Tempini et al. Neurology. 2011

38 Frontotemporal dementia with motor neuron disease (FTD-MND) Combines features of FTD (behavioral dyscontrol, executive dysfunction, agrammatic aphasia) with features of lower motor neuron disease Cognitive and behavioral symptoms predate motor symptoms If motor symptoms predate the cognitive symptoms, we use the term ALS- dementia R L Mitsuyama. J Neurol Neurosurg Psychiatry. 1984
39 Summary The neurodegenerative dementias include AD, LBD and FTD Each has a specific clinical and pathological spectrum Definitive diagnosis can only be made with neuropathological analysis Functional and structural findings as well as biomarkers can narrow the diagnosis

40 Dementia with Lewy Bodies Case 1 Case 2
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer
 The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
! slow, progressive, permanent loss of neurologic function.
 UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia
 Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia Bradley F. Boeve, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Alzheimer s Disease
Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia Bradley F. Boeve, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Alzheimer s Disease
LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION
 LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION Murray Grossman University of Pennsylvania Support from NIH (AG17586, AG15116, NS44266, NS35867, AG32953, AG38490), IARPA, ALS Association, and the
LANGUAGE AND PATHOLOGY IN FRONTOTEMPORAL DEGENERATION Murray Grossman University of Pennsylvania Support from NIH (AG17586, AG15116, NS44266, NS35867, AG32953, AG38490), IARPA, ALS Association, and the
Objectives. Objectives continued: 3/24/2012. Copyright Do not distribute or replicate without permission 1
 Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Biomarkers: Translating Research into Clinical Practice
 Biomarkers: Translating Research into Clinical Practice AFTD Education Conference San Diego, April 2015 Nadine Tatton, PhD Scientific Director, AFTD HelpLine 866-5507-7222 u info@theaftd.org u www.theaftd.org
Biomarkers: Translating Research into Clinical Practice AFTD Education Conference San Diego, April 2015 Nadine Tatton, PhD Scientific Director, AFTD HelpLine 866-5507-7222 u info@theaftd.org u www.theaftd.org
I do not have any disclosures
 Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Frontotemporal Dementia: Towards better diagnosis. Frontotemporal Dementia. John Hodges, NeuRA & University of New South Wales, Sydney.
 I.1 I.2 II.1 II.2 II.3 II.4 II.5 II.6 III.1 III.2 III.3 III.4 III.5 III.6 III.7 III.8 III.9 III.10 III.11 III.12 IV.1 IV.2 IV.3 IV.4 IV.5 Frontotemporal Dementia: Towards better diagnosis Frontotemporal
I.1 I.2 II.1 II.2 II.3 II.4 II.5 II.6 III.1 III.2 III.3 III.4 III.5 III.6 III.7 III.8 III.9 III.10 III.11 III.12 IV.1 IV.2 IV.3 IV.4 IV.5 Frontotemporal Dementia: Towards better diagnosis Frontotemporal
3/7/2017. Alzheimer s and Dementia Research: An Advanced Discussion. Alzheimer s and Dementia Research: An Advanced Discussion
 Alzheimer s and Dementia Research: An Advanced Discussion Brad Boeve, MD Department of Neurology Mayo Clinic Alzheimer s and Dementia Research: An Advanced Discussion Theoretical Constructs in Aging/Dementia
Alzheimer s and Dementia Research: An Advanced Discussion Brad Boeve, MD Department of Neurology Mayo Clinic Alzheimer s and Dementia Research: An Advanced Discussion Theoretical Constructs in Aging/Dementia
Ruolo dei biomarcatori come criterio di supporto nella diagnostica delle demenze ad esordio precoce
 Ruolo dei biomarcatori come criterio di supporto nella diagnostica delle demenze ad esordio precoce ALESSANDRO MARTORANA UOC NEUROLOGIA-CENTRO ALZHEIMER POLICLINICO TOR VERGATA-UNIVERSITÀ DI ROMA TOR VERGATA
Ruolo dei biomarcatori come criterio di supporto nella diagnostica delle demenze ad esordio precoce ALESSANDRO MARTORANA UOC NEUROLOGIA-CENTRO ALZHEIMER POLICLINICO TOR VERGATA-UNIVERSITÀ DI ROMA TOR VERGATA
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Objectives. RAIN Difficult Diagnosis 2014: A 75 year old woman with falls. Case History: First visit. Case History: First Visit
 Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
FTD basics! Etienne de Villers-Sidani, MD!
 FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Frontotemporal dementia:
 Frontotemporal dementia: Where we ve been What s on the horizon Howard Rosen, M.D. UCSF Department of Neurology Memory and Aging Center www.memory.ucsf.edu None Disclosures Overview FTD, What is it? Origins
Frontotemporal dementia: Where we ve been What s on the horizon Howard Rosen, M.D. UCSF Department of Neurology Memory and Aging Center www.memory.ucsf.edu None Disclosures Overview FTD, What is it? Origins
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
Form A3: Subject Family History
 Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
2016 Programs & Information
 Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Sandra Weintraub, PhD Clinical Core Leader and Professor
 Sandra Weintraub, PhD Clinical Core Leader and Professor Northwestern Cognitive Neurology and Alzheimer s Disease Center (CNADC) Chicago, Illinois www.brain.northwestern.edu Why is it so difficult to diagnose
Sandra Weintraub, PhD Clinical Core Leader and Professor Northwestern Cognitive Neurology and Alzheimer s Disease Center (CNADC) Chicago, Illinois www.brain.northwestern.edu Why is it so difficult to diagnose
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Introduction, use of imaging and current guidelines. John O Brien Professor of Old Age Psychiatry University of Cambridge
 Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Moving Targets: An Update on Diagnosing Dementia in the Clinic
 Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Do not copy or distribute without permission. S. Weintraub, CNADC, NUFSM, 2009
 Sandra Weintraub, Ph.D. Clinical Core Director, Cognitive Neurology and Alzheimer s Disease Center Northwestern University Feinberg School of Medicine Chicago, Illinois Dementia: a condition caused by
Sandra Weintraub, Ph.D. Clinical Core Director, Cognitive Neurology and Alzheimer s Disease Center Northwestern University Feinberg School of Medicine Chicago, Illinois Dementia: a condition caused by
Clinical Genetics & Dementia
 Clinical Genetics & Dementia Dr Nayana Lahiri Consultant in Clinical Genetics & Honorary Senior Lecturer Nayana.lahiri@nhs.net Aims of the Session To appreciate the potential utility of family history
Clinical Genetics & Dementia Dr Nayana Lahiri Consultant in Clinical Genetics & Honorary Senior Lecturer Nayana.lahiri@nhs.net Aims of the Session To appreciate the potential utility of family history
Update on functional brain imaging in Movement Disorders
 Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Neuro degenerative PET image from FDG, amyloid to Tau
 Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Diagnosis before NIA AA The impact of FDG PET in. Diagnosis after NIA AA Neuropathology and PET image 2015/10/16
 The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Medications and Non-Pharma Approaches to Treatment. David J. Irwin, MD Penn Frontotemporal Degeneration Center
 Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
NIH Public Access Author Manuscript Semin Neurol. Author manuscript; available in PMC 2014 November 14.
 NIH Public Access Author Manuscript Published in final edited form as: Semin Neurol. 2013 September ; 33(4): 386 416. doi:10.1055/s-0033-1359312. Neuroimaging Biomarkers of Neurodegenerative Diseases and
NIH Public Access Author Manuscript Published in final edited form as: Semin Neurol. 2013 September ; 33(4): 386 416. doi:10.1055/s-0033-1359312. Neuroimaging Biomarkers of Neurodegenerative Diseases and
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Clinicopathologic and genetic aspects of hippocampal sclerosis. Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA
 Clinicopathologic and genetic aspects of hippocampal sclerosis Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA The hippocampus in health & disease A major structure of the medial temporal
Clinicopathologic and genetic aspects of hippocampal sclerosis Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA The hippocampus in health & disease A major structure of the medial temporal
Differentiating Dementia Diagnoses
 Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
DEMENTIA ANDREA BERG, MD
 DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia. Amber Eker, MD. Assistant Professor Near East University Department of Neurology
 Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Prof Tim Anderson. Neurologist University of Otago Christchurch
 Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
UDS version 3 Summary of major changes to UDS form packets
 UDS version 3 Summary of major changes to UDS form packets from version 2 to VERSION 3 february 18 final Form A1: Subject demographics Updated question on principal referral source to add additional options
UDS version 3 Summary of major changes to UDS form packets from version 2 to VERSION 3 february 18 final Form A1: Subject demographics Updated question on principal referral source to add additional options
Phenotypic Variability in ALS
 Phenotypic Variability in ALS Michael A. Elliott, MD, FAAN Medical Director, ALS Clinic Swedish Neuroscience Institute 1 Outline ALS Background Description Typical Presentation Clinical Phenotype Motor
Phenotypic Variability in ALS Michael A. Elliott, MD, FAAN Medical Director, ALS Clinic Swedish Neuroscience Institute 1 Outline ALS Background Description Typical Presentation Clinical Phenotype Motor
Part 2: Early detection, assessment and treatment in relation to the new guidelines. Christopher Patterson McMaster University
 Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Presenter Disclosure Information. I have no financial relationships to disclose:
 Sandra Weintraub, Ph.D. Cognitive Neurology and Alzheimer s Disease Center Northwestern University, Feinberg School of Medicine Chicago, Illinois http://www.brain.northwestern.edu/dementia/ppa/index.html
Sandra Weintraub, Ph.D. Cognitive Neurology and Alzheimer s Disease Center Northwestern University, Feinberg School of Medicine Chicago, Illinois http://www.brain.northwestern.edu/dementia/ppa/index.html
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
The Spectrum of Lewy Body Disease: Dementia with Lewy Bodies and Parkinson's Disease Dementia
 Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Comprehensive Approach to DLB Management
 Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Confronting the Clinical Challenges of Frontotemporal Dementia
 Confronting the Clinical Challenges of Frontotemporal Dementia A look at FTD s symptoms, pathophysiology, subtypes, as well as the latest from imaging studies. By Zac Haughn, Senior Associate Editor Ask
Confronting the Clinical Challenges of Frontotemporal Dementia A look at FTD s symptoms, pathophysiology, subtypes, as well as the latest from imaging studies. By Zac Haughn, Senior Associate Editor Ask
NCRAD. Single Gene Implicated in FTD/ALS UCSF Memory and Aging Center, San Francisco, California
 The National Cell Repository for Alzheimer s Disease (NCRAD) is a data and specimen collection source for families with Alzheimer disease (AD) or serious memory loss. Families having two or more living
The National Cell Repository for Alzheimer s Disease (NCRAD) is a data and specimen collection source for families with Alzheimer disease (AD) or serious memory loss. Families having two or more living
FRONTO TEMPORAL DEMENTIA
 FRONTO TEMPORAL DEMENTIA Dr. Diana Paleacu Kertesz Neurology Service and Memory Clinic Abarbanel Mental Health Center Department of Neurology, Tel Aviv University DAT: 55-60% VD: 15-20% DLBD: 15-20% FTD:
FRONTO TEMPORAL DEMENTIA Dr. Diana Paleacu Kertesz Neurology Service and Memory Clinic Abarbanel Mental Health Center Department of Neurology, Tel Aviv University DAT: 55-60% VD: 15-20% DLBD: 15-20% FTD:
FRONTO TEMPORAL DEMENTIA
 FRONTO TEMPORAL DEMENTIA Dr. Diana Paleacu Kertesz Neurology Service and Memory Clinic Abarbanel Mental Health Center Department of Neurology, Tel Aviv University Fronto-Temporal Lobe Dementia (FTLD) DAT:
FRONTO TEMPORAL DEMENTIA Dr. Diana Paleacu Kertesz Neurology Service and Memory Clinic Abarbanel Mental Health Center Department of Neurology, Tel Aviv University Fronto-Temporal Lobe Dementia (FTLD) DAT:
Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases
 Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases Keith A. Josephs, MD, MST, MSc Professor of Neurology 13th Annual Mild Cognitive Impairment (MCI) Symposium: Alzheimer and Non-Alzheimer
Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases Keith A. Josephs, MD, MST, MSc Professor of Neurology 13th Annual Mild Cognitive Impairment (MCI) Symposium: Alzheimer and Non-Alzheimer
Revised criteria for the clinical diagnosis of dementia with Lewy. Dementia with Lewy bodies. (Dementia with Lewy Bodies)
") Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
White matter hyperintensities correlate with neuropsychiatric manifestations of Alzheimer s disease and frontotemporal lobar degeneration
 White matter hyperintensities correlate with neuropsychiatric manifestations of Alzheimer s disease and frontotemporal lobar degeneration Annual Scientific Meeting Canadian Geriatric Society Philippe Desmarais,
White matter hyperintensities correlate with neuropsychiatric manifestations of Alzheimer s disease and frontotemporal lobar degeneration Annual Scientific Meeting Canadian Geriatric Society Philippe Desmarais,
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Overview of the non-alzheimer Dementias
 Overview of the non-alzheimer Dementias Chiadi U. Onyike, MD, MHS FTD/Young-Onset Dementias Program Johns Hopkins Neuropsychiatry Disclaimer Dr. Onyike is a principal investigator for the Baltimore site
Overview of the non-alzheimer Dementias Chiadi U. Onyike, MD, MHS FTD/Young-Onset Dementias Program Johns Hopkins Neuropsychiatry Disclaimer Dr. Onyike is a principal investigator for the Baltimore site
Dementia: A Comprehensive Update Neuroimaging, CSF, and genetic biomarkers in dementia
 Dementia: A Comprehensive Update 2016 Neuroimaging, CSF, and genetic biomarkers in dementia Bradford C. Dickerson, M.D. Associate Professor of Neurology, Harvard Medical School Departments of Neurology
Dementia: A Comprehensive Update 2016 Neuroimaging, CSF, and genetic biomarkers in dementia Bradford C. Dickerson, M.D. Associate Professor of Neurology, Harvard Medical School Departments of Neurology
Brain imaging for the diagnosis of people with suspected dementia
 Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Early Onset Dementia From the background to the foreground
 Early Onset Dementia From the background to the foreground Dr Jeremy Isaacs Consultant Neurologist St George s Hospital Excellence in specialist and community healthcare Themes of my talk The early onset
Early Onset Dementia From the background to the foreground Dr Jeremy Isaacs Consultant Neurologist St George s Hospital Excellence in specialist and community healthcare Themes of my talk The early onset
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
FTD: Improving Outcomes & Outreach
 2nd Annual Frontotemporal Degeneration Caregiver Education Conference Raleigh, NC 7.25.12 FTD: Improving Outcomes & Outreach Dan Kaufer, MD Associate Professor, Neurology Director, Memory Disorders Program
2nd Annual Frontotemporal Degeneration Caregiver Education Conference Raleigh, NC 7.25.12 FTD: Improving Outcomes & Outreach Dan Kaufer, MD Associate Professor, Neurology Director, Memory Disorders Program
Navigating The Cognitive Internet: Introduction. Wendy Lemere DNP, GNP-BC Gerontological Nurse Practitioner Henry Ford Health System
 Navigating The Cognitive Internet: Introduction Wendy Lemere DNP, GNP-BC Gerontological Nurse Practitioner Henry Ford Health System What s so hard about diagnosing dementia? Diagnosis relies on synthesis
Navigating The Cognitive Internet: Introduction Wendy Lemere DNP, GNP-BC Gerontological Nurse Practitioner Henry Ford Health System What s so hard about diagnosing dementia? Diagnosis relies on synthesis
Erin Cullnan Research Assistant, University of Illinois at Chicago
 Dr. Moises Gaviria Distinguished Professor of Psychiatry, University of Illinois at Chicago Director of Consultation Liaison Service, Advocate Christ Medical Center Director of the Older Adult Program,
Dr. Moises Gaviria Distinguished Professor of Psychiatry, University of Illinois at Chicago Director of Consultation Liaison Service, Advocate Christ Medical Center Director of the Older Adult Program,
Dementia. Team Members: Abdulaziz Alsalem, Khalid Al-Qahtani, Dania Alkelabi, Sarah Alshamrani
 Dementia Objectives: differentiate delirium from dementia differentiate Mild Cognitive Impairment from Dementia become familiar with common dementia syndromes, and available treatments Team Members: Abdulaziz
Dementia Objectives: differentiate delirium from dementia differentiate Mild Cognitive Impairment from Dementia become familiar with common dementia syndromes, and available treatments Team Members: Abdulaziz
La neurosonologia. Ecografia cerebrale e nuove applicazioni nelle malattie neurodegenerative. Nelle patologie degenerative e vascolari cerebrali
 La neurosonologia Nelle patologie degenerative e vascolari cerebrali Andrea Pilotto Ecografia cerebrale e nuove applicazioni nelle malattie neurodegenerative Prof. Daniela Berg Department of Neurodegeneration
La neurosonologia Nelle patologie degenerative e vascolari cerebrali Andrea Pilotto Ecografia cerebrale e nuove applicazioni nelle malattie neurodegenerative Prof. Daniela Berg Department of Neurodegeneration
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss
 Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss Incidence of Common Neurological Diseases Incidence New Cases Disease (per 100,000) (per
Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss Incidence of Common Neurological Diseases Incidence New Cases Disease (per 100,000) (per
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
Paper Title Theme Presentation Type Poster Presentatio n Day
 A NOVEL PROBE OF FUNCTIONAL NETWORK ARCHITECTURE IN PROTEINOPATHIES: SPECTRAL DCM IN SEMANTIC DEMENTIA Blood and imaging biomarkers Poster and Data Blitz Monday 1 M1 PATHWAYS PREDICTION & RISK-GENE PRIORITIZATION
A NOVEL PROBE OF FUNCTIONAL NETWORK ARCHITECTURE IN PROTEINOPATHIES: SPECTRAL DCM IN SEMANTIC DEMENTIA Blood and imaging biomarkers Poster and Data Blitz Monday 1 M1 PATHWAYS PREDICTION & RISK-GENE PRIORITIZATION
Frontotemporal Degeneration
 #96100 Frontotemporal Degeneration COURSE #96100 2 CONTACT/CLOCK HOURS Release Date: 11/01/15 Expiration Date: 10/31/18 Frontotemporal Degeneration HOW TO RECEIVE CREDIT Read the enclosed course. Complete
#96100 Frontotemporal Degeneration COURSE #96100 2 CONTACT/CLOCK HOURS Release Date: 11/01/15 Expiration Date: 10/31/18 Frontotemporal Degeneration HOW TO RECEIVE CREDIT Read the enclosed course. Complete
Regulatory Challenges across Dementia Subtypes European View
 Regulatory Challenges across Dementia Subtypes European View Population definition including Early disease at risk Endpoints in POC studies Endpoints in pivotal trials 1 Disclaimer No CoI The opinions
Regulatory Challenges across Dementia Subtypes European View Population definition including Early disease at risk Endpoints in POC studies Endpoints in pivotal trials 1 Disclaimer No CoI The opinions
ASYMMETRICAL CORTICAL DEGENERATIVE SYNDROMES
 ASYMMETRICAL CORTICAL DEGENERATIVE SYNDROMES Richard Caselli, MD Professor & Chair, Department of Neurology Mayo Clinic Arizona & Clinical Core Director, Arizona Alzheimer s Disease Center Objectives:
ASYMMETRICAL CORTICAL DEGENERATIVE SYNDROMES Richard Caselli, MD Professor & Chair, Department of Neurology Mayo Clinic Arizona & Clinical Core Director, Arizona Alzheimer s Disease Center Objectives:
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Biology 3201 Nervous System # 7: Nervous System Disorders
 Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
Neuroimaging Biomarkers of Neurodegenerative Diseases and Dementia
 386 Neuroimaging Biomarkers of Neurodegenerative Diseases and Dementia Shannon L. Risacher, PhD 1 Andrew J. Saykin, PsyD 1 1 Center for Neuroimaging, Department of Radiology and Imaging Sciences, and Indiana
386 Neuroimaging Biomarkers of Neurodegenerative Diseases and Dementia Shannon L. Risacher, PhD 1 Andrew J. Saykin, PsyD 1 1 Center for Neuroimaging, Department of Radiology and Imaging Sciences, and Indiana
8/24/18. Dementia. Risk of Dementia Following Traumatic Brain Injury: A Review of the Literature. Media Presence. Media Presence
 Risk of Dementia Following Traumatic Brain Injury: A Review of the Literature Media Presence Carlos Marquez de la Plata, Ph.D. & Jeff Schaffert, M.S. Media Presence Dementia What is dementia? Dementia
Risk of Dementia Following Traumatic Brain Injury: A Review of the Literature Media Presence Carlos Marquez de la Plata, Ph.D. & Jeff Schaffert, M.S. Media Presence Dementia What is dementia? Dementia
Dementia the A,B,Cs. Dr. Frank Molnar. Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital
 Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
How to Diagnose Early (Prodromal) Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.
 Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.") How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
Dementia: Diagnosis and Treatment
 Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
Brain Advance Access published February 25, doi: /brain/awu024 Brain 2014: Page 1 of 17 1
 Brain Advance Access published February 25, 2014 doi:10.1093/brain/awu024 Brain 2014: Page 1 of 17 1 BRAIN A JOURNAL OF NEUROLOGY Asymmetry and heterogeneity of Alzheimer s and frontotemporal pathology
Brain Advance Access published February 25, 2014 doi:10.1093/brain/awu024 Brain 2014: Page 1 of 17 1 BRAIN A JOURNAL OF NEUROLOGY Asymmetry and heterogeneity of Alzheimer s and frontotemporal pathology
DEFINING THE NEUROPSYCHOLOGICAL AND NEUROIMAGING PHENOTYPE OF BEHAVIOURAL VARIANT FRONTOTEMPORAL DEMENTIA SUBMITTED TO UNIVERSITY COLLEGE LONDON
 DEFINING THE NEUROPSYCHOLOGICAL AND NEUROIMAGING PHENOTYPE OF BEHAVIOURAL VARIANT FRONTOTEMPORAL DEMENTIA SUBMITTED TO UNIVERSITY COLLEGE LONDON FOR THE DEGREE OF DOCTOR OF PHILOSOPHY LAURA EMILY DOWNEY
DEFINING THE NEUROPSYCHOLOGICAL AND NEUROIMAGING PHENOTYPE OF BEHAVIOURAL VARIANT FRONTOTEMPORAL DEMENTIA SUBMITTED TO UNIVERSITY COLLEGE LONDON FOR THE DEGREE OF DOCTOR OF PHILOSOPHY LAURA EMILY DOWNEY
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status. Case 1 4/7/11. Which of the following evaluations is your next step?
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco