Characterizing Potentially Inappropriate Prescribing of Proton Pump Inhibitors in Older People in Primary Care in Ireland from 1997 to 2012.
|
|
|
- Milo Craig
- 5 years ago
- Views:
Transcription

1 Royal College of Surgeons in Ireland General Practice Articles Department of General Practice Characterizing Potentially Inappropriate Prescribing of Proton Pump Inhibitors in Older People in Primary Care in Ireland from 1997 to Frank Moriarty Royal College of Surgeons in Ireland, Kathleen Bennett Royal College of Surgeons in Ireland, Caitriona Cahir Royal College of Surgeons in Ireland Tom Fahey Royal College of Surgeons in Ireland Citation Moriarty F, Bennett K, Cahir C, Fahey T. Characterizing Potentially Inappropriate Prescribing of Proton Pump Inhibitors in Older People in Primary Care in Ireland from 1997 to Journal of the American Geriatrics Society. 2016;64(12): e291-e296. This Article is brought to you for free and open access by the Department of General Practice at It has been accepted for inclusion in General Practice Articles by an authorized administrator of e- For more information, please contact
2 Use Licence This work is licensed under a Creative Commons Attribution-Noncommercial-Share Alike 4.0 License. This article is available at e-publications@rcsi:
3 Characterising potentially inappropriate prescribing of proton pump inhibitors in older people in primary care in Ireland from 1997 to 2012 Frank Moriarty, MPharm 1, Kathleen Bennett, PhD 2, Caitriona Cahir, PhD 2, Tom Fahey, MD 1 1. HRB Centre for Primary Care Research, Department of General Practice, Royal College of Surgeons in Ireland, 123 St Stephens Green, Dublin 2, Ireland. 2. Division of Population Health Sciences, Royal College of Surgeons in Ireland, 123 St Stephens Green, Dublin 2, Ireland. This is the peer reviewed version of the following article: Moriarty, F., Bennett, K., Cahir, C., and Fahey, T. Characterizing Potentially Inappropriate Prescribing of Proton Pump Inhibitors in Older People in Primary Care in Ireland from 1997 to J Am Geriatr Soc. 2016; 64(12): e291-e296, which has been published in final form at This article may be used for noncommercial purposes in accordance with Wiley Terms and Conditions for Self-Archiving. Funding: This work was supported by the Health Research Board of Ireland (HRB) through the HRB PhD Scholars Programme in Health Services Research (grant no. PHD/2007/16) and the HRB Centre for Primary Care Research (grant no. HRC/2007/1). Previous presentations: This work was presented in part at the Society for Social Medicine Annual Scientific Meeting Corresponding author: 1
4 Frank Moriarty HRB Centre for Primary Care Research, Department of General Practice, Royal College of Surgeons in Ireland, 123 St Stephens Green, Dublin 2, Ireland. Tel: Fax: frankmoriarty@rcsi.ie Alternate corresponding author: Tom Fahey HRB Centre for Primary Care Research, Department of General Practice, Royal College of Surgeons in Ireland, 123 St Stephens Green, Dublin 2, Ireland. Tel: Fax: tomfahey@rcsi.ie Abbreviated title: Proton pump inhibitor use from 1997 to 2012 Key words: Proton pump inhibitors; potentially inappropriate prescribing; older persons; primary care; gastrointestinal bleeding Abstract: 275 Word count: 2614 Graphics: 3 (2 tables, 1 figure) References: 30 2
5 Abstract Background/objectives: Concerns have been raised regarding overprescribing of proton pump inhibitors (PPIs). This study characterises prescribing of PPIs and medicines which increase gastrointestinal bleeding risk (ulcerogenic) in older people from 1997 to 2012 and assesses factors associated with maximal-dose prescribing in long-term PPI users. Design: Repeated cross-sectional study of pharmacy claims data. Setting: Eastern Health Board region of Ireland. Participants: Individuals aged 65 from a means-tested scheme in 1997, 2002, 2007, and 2012 (range 78, ,884 individuals). Measurements: PPI prescribing prevalence was determined per study year, categorised by duration ( or >8 weeks), dosage (maximal or maintenance) and co-prescribed drugs. Logistic regression in long-term PPI users determined if age, gender, polypharmacy and ulcerogenic medicines use were associated with being prescribed a maximal dose rather than a maintenance dose. Adjusted odds ratios (OR) with 95% confidence intervals (CI) are presented. Results: Half of this older aged population received a PPI in 2007 and Long-term use (>8 weeks) of maximal doses rose from 0.8% of individuals in 1997 to 23.6% in While some ulcerogenic medicines and polypharmacy were significantly associated with maximal PPI doses, any NSAID use was significantly associated with lower odds of maximal PPI dose (adjusted OR 0.85, 95%CI ), as were aspirin use and increasing age. Adjusting for medication and demographic factors, odds of being prescribed a maximal PPI dose were significantly higher in 2012 compared to 1997 (adjusted OR 6.3, 95%CI ). 3
6 Conclusions: Long-term maximal dose PPI prescribing is highly prevalent in older populations and is not consistently associated with gastrointestinal bleeding risk factors. Interventions involving prescribers and patients may promote appropriate PPI use, reducing costs and adverse effects of PPI overprescribing. 4
7 Introduction Proton pump inhibitors (PPIs) were first marketed in the late 1980 s and since this time, the volume prescribed has surpassed other acid-suppressant agents such as H2 receptor antagonists (H2RA) due to superior pharmacokinetics and efficacy to make PPIs one of the most commonly prescribed drug classes.[1 3] They were initially marketed for the treatment and prevention of gastric acid-related symptoms and diseases, however, these indications do not fully account for the rising number of prescriptions observed in recent years.[4] Their widespread use has prompted concerns regarding overprescribing of PPIs and that their use by many patients may cause more harm than benefit, particularly in patients at low risk of gastrointestinal (GI) adverse events.[1,5] Use of PPIs for longer than indicated in older people is a particular source of concern, as illustrated by the addition of this prescribing to the recently updated Beers criteria.[6] The Screening Tool for Older Person s Prescriptions (STOPP) also defines use of PPIs at therapeutic dose or higher for longer than 8 weeks as potentially inappropriate for people aged 65 and over.[7] Studies suggest this is the optimal duration of high-dose prescribing to maximise ulcer healing and symptom resolution and minimise rebound acid secretion.[5] This is one of the most prevalent types of potentially inappropriate prescribing defined by STOPP in several European countries,[8] with a recent study showing that almost a quarter of older participants received this type of potentially inappropriate prescribing.[3] As PPIs are regarded as having a good safety profile and high efficacy,[5] such prescribing is often seen as a conservative approach to reduce the likelihood of GI bleeds in patients who are at elevated risk of such adverse events. However, using high doses for longer than indicated is 5
8 not cost-effective and, as well as increasing drug burden for patients, may also put patients at risk of other adverse events, including fractures and Clostridium difficile infection.[5,9,10] The objectives of this study are: (1) to characterise how PPI prescribing and co-prescribed ulcerogenic medicines have changed in community-dwelling older people in Ireland (aged 65 years) from 1997 to 2012 and (2) for long-term PPI users, to determine what coprescribed medications and demographic factors are associated with prescription of maximal dose (rather than maintenance dose) and which factors account for the increase in long-term use of maximal doses from 1997 to
9 Methods Study design This is a repeated cross-sectional study using administrative pharmacy claims data available from the Health Service Executive Primary Care Reimbursement Service (HSE-PCRS). The study population includes all individuals aged 65 years eligible for the General Medical Services (GMS) scheme in the former Eastern Health Board region of Ireland (representing one third of older people nationally) in the years 1997, 2002, 2007, and The GMS scheme is a form of public health cover in Ireland with means-tested eligibility, however, from 2002 to 2008 all people aged 70 years or over were automatically eligible for the scheme and since January 2009, a higher income threshold was applied to this age group compared to the general population still covering 96.5% of this population.[11] Analysis PPI use For each study year, we determined the percentage of the study population prescribed a PPI (ATC code A02BC and combinations), categorised by duration ( and > 8 weeks for shortand long-term use respectively) and for those prescribed a long-term PPI, the dosage prescribed for this period (either maximal i.e. treatment dosage or higher, or maintenance i.e. less than treatment dose). Individuals with long-term periods at both maximal and maintenance doses were categorised as the former. Treatment doses were classified as 40mg daily for omeprazole, pantoprazole, and esomeprazole, 30mg daily for lansoprazole and 20mg daily for rabeprazole, consistent with other studies and United Kingdom treatment guidelines.[12,13] These doses are in some cases higher than those indicated on 7
10 Food & Drug Administration (FDA) labels and so estimates of potential overprescribing are likely to be more conservative than if FDA dose recommendations had been used. For individuals prescribed a long-term PPI at maximal dose we also examined their concomitant use of medicines that can increase risk of GI bleeding (ulcerogenic agents including non-steroidal anti-inflammatory drugs (NSAIDs), aspirin, other antiplatelet or anticoagulant drugs, and oral corticosteroids prescribed for 3 months or greater). Concomitant use was classified as a dispensing of the ulcerogenic medicine within the period of long-term PPI use. Data were only available on doctor-prescribed drugs. We calculated prevalence estimates with 95% confidence intervals (CIs) for each of these scenarios as a percentage of all persons aged 65 years and over eligible for the GMS scheme in the final month of each study year. Factors associated with dosage of long-term PPIs Among long-term PPI users across all years, we used logistic regression to assess medication and demographic factors associated with being prescribed a maximal dose (considered potentially inappropriate prescribing) compared to a lower, more appropriate maintenance dose after 8 weeks. Factors included as explanatory variables were concomitant use of ulcerogenic medicines, age group (categorised as years (reference), years, or 75 years), gender, and level of polypharmacy (number of regular medication classes prescribed to an individual for 3 months or longer, categorised as 0-4 (reference), 5-9, or 10 or more regular medicines). Study year was also included to assess if risk of long-term users being prescribed a maximal dose changed with time, controlling for demographic and medication factors. Adjusted odds ratios (OR) with 95% CI are presented. Multicollinearity was assessed using the variance inflation factor. Some individuals may be included at 8
11 multiple time points, so a sensitivity analysis was undertaken to account for clustering/nonindependence of repeated observations of a patient in estimating standard errors. All analyses were performed using Stata version 12 (Stata Corporation, College Station, TX, USA) and significance was assumed at p<
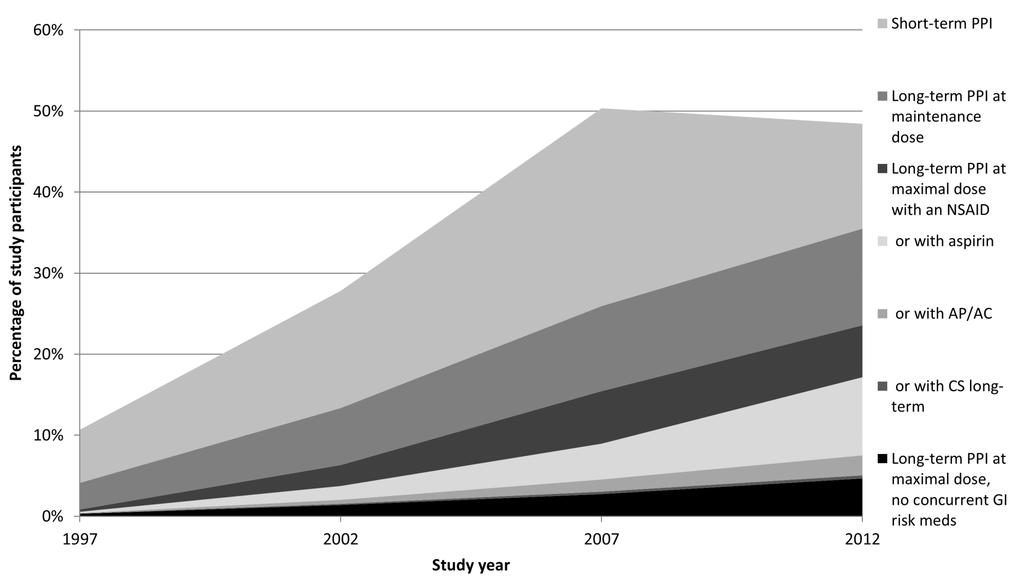
12 Results The number of individuals aged 65 years and over included in this study was 78,489 in 1997, 121,726 in 2002, 129,162 in 2007, and 133,884 in Previous analysis found the percentage of these older adults on five or more regular medicines (i.e. with polypharmacy) increased steadily from 17.8% in 1997 to 60.4% in 2012, while those on 10 or more regular medicines rose from 1.5% to 21.9% over this period.[3] Approximately half of participants were prescribed any PPI in 2007 and 2012, up from 10.7% in 1997 (see Table 1). Long-term prescribing became more common, with the percentage of participants on a PPI for greater than 8 weeks increasing from 4.1% in 1997 to 35.5% in The prevalence of potentially inappropriate prescription of a PPI (i.e. treatment dosage or higher for greater than 8 weeks) also rose over this period, from 0.8% of individuals in 1997 to 23.6% of those in Long-term use at maximal dosages increased both as a proportion of those prescribed any PPI and those on a long-term PPI, as illustrated in Figure 1 and in all cases the trend across years was statistically significant. Excluding individuals also receiving a concurrent prescription for an ulcerogenic agent, 4.7% of the 2012 study population were prescribed a potentially inappropriate PPI with no concurrent medicines that increase the risk of GI bleeding. The corresponding percentages were 0.3% of individuals in 1997, 1.4% in 2002, and 2.7% in 2007, a statistically significant trend. Adjusted logistic regression analysis of individuals prescribed a long-term PPI found that concurrent anticoagulant, antiplatelet (excluding aspirin), or long-term corticosteroid use, and being on five or more regular medicines were significantly associated with higher odds of being prescribed a potentially inappropriate maximal dose (Table 2). Concurrent NSAID (adjusted OR 0.87, 95% CI ) or aspirin use (OR 0.95, 95% CI ) as well as 10
13 female gender and older age were associated with lower odds of being prescribed a maximal dose among long-term PPI users. The increased odds of a long-term PPI user in 2012 being on a maximal dose compared to in 1997 remained significantly higher after adjusting for concomitant ulcerogenic medicines, age group, gender and polypharmacy in the multivariate model (adjusted OR 6.30, 95% CI , see Table 2). In sensitivity analysis, accounting for patient clustering of repeated observations across years did not significantly alter the results. 11
14 Discussion Principal findings and interpretation Although the proportion of older people in this study prescribed PPIs was four times higher in 2012 compared to 1997, the prevalence of potentially inappropriate long-term PPI at maximal dose increased almost thirtyfold over this period. Discounting instances where an ulcerogenic drug was co-prescribed (even though higher doses of PPIs would not necessarily be indicated for gastroprotection in such cases), there were still almost 5% of people on a potentially inappropriate PPI in It was hypothesised that long-term PPI users with GI bleeding risk factors would be more likely to be prescribed a maximal dose; however, maximal-dose use was not consistently associated with such risk factors, including aspirin and NSAID use and increasing age. The rise in potentially inappropriate PPI use from 1997 to 2012 was not fully explained by changes in demographics and medication co-prescribing over this time period. Behavioural economic theories may provide some explanation of the decision-making processes leading to increased use of maximal-dose PPIs long term. The availability heuristic, estimating the probability of events based on how easily one recalls similar events could play a role.[14] The threat of a GI bleed is well established and may be more widely recognised by prescribers than PPI-associated adverse effects such as Clostridium difficile infection and fracture, for which evidence is newer and mainly observational.[9,10] Omission bias, which leads to risks from acts of omission being underestimated relative to acts of commission, may also influence decision making.[14] The more passive approach of continuing a PPI at treatment dose may be favoured relative to the risk of the act of commission of dose reduction/discontinuation, for fear of adverse consequences of altering 12
15 the status quo.[15] Patient resistance to change due to beliefs that continuation is beneficial to their health may also impede deprescribing.[16] The unexpected association of NSAID use with lower doses of PPI could be due to the presence of confounding not measured in this study, for example a factor associated with the outcome of maximal-dose PPI prescribing and inversely associated with NSAID use, such as history of peptic ulcer disease (PUD) or symptomatic gastro-oesophageal reflux disease (GORD). Given that GI mucosal protective mechanisms are impaired with age, the relationship between increasing age and lower odds of maximal-dose PPI is also surprising and unlikely to be explained by confounding due to PUD/GORD.[17] Findings in the context of previous research Research has shown a consistent upward trend in PPI utilisation, up to a 13-fold increase in the 12 years up to 2006 in Australia.[18 21] A Dutch study found a rise in PPI prescribing to primary care patients initiated on low-dose aspirin or an NSAID from 2000 to 2012, and this increase was observed in patients across levels of risk for upper GI bleeding.[21] Regarding trends in maximal dose prescribing, a growing prevalence of high-intensity PPI use was noted in a Canadian study.[22] Considering prescribing between 1997 and 2004 in this Canadian research, polypharmacy was associated with use of high doses, while increasing age was associated with reduced odds, consistent with our study. Interestingly the authors concluded that severity of GORD symptoms was a weak predictor of maximal-dose use. An important finding was that demographics and concomitant ulcerogenic medicines dispensed did not account for much of the increase in maximal treatment dose prescribing from 1997 to This suggests that prescribing practices have changed independent of these factors and that many patients may not require this level of PPI prescribing. This is 13
16 consistent with other studies, where a small proportion of PPI prescribing (13.5%) was associated with regular indications of PUD or taking an NSAID in French nursing homes,[23] while non-specific morbidity accounted for 46% of new prescriptions in an English primarycare setting in 1995.[18] The former study concluded that much prescribing was probably inappropriately related to general health vulnerability, reflected by polypharmacy and comorbidities.[23] Strengths and limitations Strengths of this study are the large numbers included and their representativeness of older Irish adults. The long study duration provides better evidence of actual changes in prescribing practice rather than short-term fluctuations. Due to lack of clinical information, we were unable to include possible predictors of prolonged use of maximal-dose PPIs such as PUD, GORD, or GI bleeding history. However, with the exception of Barrett s oesophagus and Zollinger-Ellison (ZE) syndrome, long-term PPI use at higher treatment doses is no more effective than maintenance doses for these conditions.[22] The lack of data on the setting of initiation (i.e. hospital or ambulatory care) or the indication for PPI prescriptions precluded examination of potentially important contributors to PPI overuse such as stress ulcer prophylaxis.[5,24] Similar to concomitant ulcerogenic drugs, conditions such as PUD may offer some justification for maximal-dose use, however, this would still be contrary to treatment guidelines and unlikely to benefit patients.[13,22] The use of pharmacy claims data captured all prescribed medicines and allowed for medicines use of individuals to be analysed rather than population-level drug consumption. Although the primary focus was prescribing of these agents, it was assumed that dispensed medications were then consumed. While this is a limitation, long-term use indicated by 14
17 repeated dispensing here is more likely to indicate actual consumption compared to onceoff or intermittent dispensing. We lacked information on non-prescription use of medicines, including NSAIDs, aspirin, PPIs or alternative gastroprotective medicines (e.g. antacids, H2RA), however, patients would have to purchase these themselves; given the extra cost, this is probably uncommon. Although this is not the first study to examine factors associated with maximal-dose PPI use in older people, this does appear to be the first since the continued increase in long-term prescribing over the last decade. Clinical and policy implications Deprescribing of PPIs targeted at patients at low risk of GI bleeding, through dose reduction or discontinuation where tolerated, may help reduce the occurrence of PPI-associated adverse effects for patients and associated costs.[9] Sub-optimal use of PPIs has been identified as a significant source of drug expenditure and rationalising prescribing in this area could yield substantial cost savings.[12,20] A recent systematic review has shown interventions to improve PPI prescribing are feasible, with discontinuation rates without symptom control deterioration ranging from 14% to 64%.[25] Approaches to optimise prescribing more generally in older patients may also provide improvements. OPTI-SCRIPT, a multi-faceted intervention including academic detailing by a pharmacist and medication review with web-based treatment algorithms, targeted potentially inappropriate prescribing in Irish general practice and was effective in reducing the use of maximal-dose PPIs long term (OR 0.3, 95% CI , comparing the intervention group to control).[26] Reducing overuse needs involvement of both healthcare professionals, to discuss PPI use, offer alternative treatments and trial discontinuation, as well as patients, who if fully informed of the risks and benefits may be more likely to try other approaches such as 15
18 lifestyle changes.[4] Strategies to optimise such prescribing should extend beyond primary care as many long-term prescriptions are hospital initiated.[27] PPIs commenced in secondary care without appropriate indications, for example for stress ulcer prophylaxis, are often continued inappropriately following discharge, particularly if communication of indication at the transition of care is lacking.[1,24,28,29] Providing clear information to prescribers initiating or continuing PPIs regarding indicated dosage and duration of treatment may help reduce inappropriate long-term use in ambulatory care.[30] Conclusions This study contextualises the growing trend in potentially inappropriate PPI use in recent years and demonstrates that a significant portion of this maximal-dose PPI prescribing in older patients may not be justified. Further research should focus on determining the most effective interventions to optimise prescribing in this area and ways to implement these in practice in order to reduce PPI overuse while enhancing patient care. 16
19 ACKNOWLEDGMENTS The authors wish to thank the Health Service Executive Primary Care Reimbursement Service (HSE-PCRS) for providing the administrative pharmacy claims data utilised in this study. This work was supported by the Health Research Board of Ireland (HRB) through the HRB PhD Scholars Programme in Health Services Research (grant no. PHD/2007/16) and the HRB Centre for Primary Care Research (grant no. HRC/2007/1). Conflict of interest: The authors have no conflict of interest to report Conflict of Interest Disclosures: Elements of Financial/Personal Conflicts Employment or Affiliation FM KB CC TF Yes No Yes No Yes No Yes No X X X X Grants/Funds X X X X Honoraria X X X X Speaker Forum X X X X Consultant X X X X Stocks X X X X Royalties X X X X Expert Testimony X X X X Board Member X X X X Patents X X X X Personal Relationship X X X X *Authors can be listed by abbreviations of their names. For all Yes responses, provide a brief explanation here: 17
20 1. Financial conflicts: employment or affiliation, grants or funding, honoraria, speaker forum membership, consultant, stock ownership or options (excluding mutual funds), royalties, expert testimony, advisory board, or patents (pending, filed, or received) as they relate to the sponsoring agent, products, technology and/or methodologies involved in the papers submitted for publication. Medical education companies that are not owned or operated by the sponsoring agent or company associated with the product, technology or methodology described in the submitted paper(s) and serve to organize and prepare manuscripts for submission are generally not considered a potential conflict. 2. Personal conflicts: a close family or personal relationship with owners or employees of the sponsoring agent or company associated with product, technology or methodology described in the submitted paper. 3. Full or adequate disclosure: each author addresses each of the specific categories of financial and personal conflicts. 4. Potential conflict: any circumstance or competing interest that could be construed or perceived as influencing the interpretation of the results. The time period for applying the criteria for COI is 3 years prior to the time the manuscript is submitted (submission date) to thejournal. Author contributions: Moriarty: study concept and design, data analysis and interpretation, drafting and revision of manuscript. Bennett: data acquisition and interpretation, revision of manuscript. Cahir, Fahey: data interpretation, revision of manuscript. Sponsor s Role: The funder had no role in the design, methods, data collection and analysis, or preparation of this paper. 18
21 References [1] Forgacs I, Loganayagam A. Overprescribing proton pump inhibitors. BMJ 2008;336:2 3. [2] Hamzat H, Sun H, Ford JC, et al. Inappropriate prescribing of proton pump inhibitors in older patients. Drugs Aging 2012;29: [3] Moriarty F, Hardy C, Bennett K, et al. Trends and interaction of polypharmacy and potentially inappropriate prescribing in primary care over 15 years in Ireland: a repeated cross-sectional study. BMJ Open 2015;5:e [4] Katz MH. Failing the acid test: benefits of proton pump inhibitors may not justify the risks for many users. Arch Intern Med 2010;170: [5] Heidelbaugh JJ, Kim AH, Chang R, et al. Overutilization of proton-pump inhibitors: what the clinician needs to know. Therap Adv Gastroenterol 2012;5: [6] American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc 2015;63: [7] O Mahony D, O Sullivan D, Byrne S, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing 2015;44: [8] Gallagher P, Lang P, Cherubini A, et al. Prevalence of potentially inappropriate prescribing in an acutely ill population of older patients admitted to six European hospitals. Eur J Clin Pharmacol 2011;67:
22 [9] Wilhelm SM, Rjater RG, Kale-Pradhan PB. Perils and pitfalls of long-term effects of proton pump inhibitors. Expert Rev Clin Pharmacol 2013;6: [10] Schoenfield AJ, Grady D. Adverse effects associated with proton pump inhibitors. JAMA Intern Med 2016;176: [11] Health Service Executive. Primary Care Reimbursement Service Annual Report. Dublin: [12] Cahir C, Fahey T, Tilson L, et al. Proton pump inhibitors: potential cost reductions by applying prescribing guidelines. BMC Health Serv Res 2012;12:408. [13] National Institute for Health and Clinical Excellence. Dyspepsia and gastrooesophageal reflux disease: investigation and management of dyspepsia, symptoms suggestive of gastro-oesophageal reflux disease, or both. Clinical Guideline 184. London, NICE: [14] Bornstein BH, Emler AC. Rationality in medical decision making: a review of the literature on doctors decision-making biases. J Eval Clin Pract 2001;7: [15] Anderson K, Stowasser D, Freeman C, et al. Prescriber barriers and enablers to minimising potentially inappropriate medications in adults: a systematic review and thematic synthesis. BMJ Open 2014;4:e e [16] Reeve E, To J, Hendrix I, et al. Patient barriers to and enablers of deprescribing: a systematic review. Drugs Aging 2013;30: [17] Newton JL. Changes in upper gastrointestinal physiology with age. Mech Ageing Dev 2004;125:
23 [18] Bashford JN, Norwood J, Chapman SR. Why are patients prescribed proton pump inhibitors? Retrospective analysis of link between morbidity and prescribing in the General Practice Research Database. BMJ 1998;317: [19] Hollingworth S, Duncan EL, Martin JH. Marked increase in proton pump inhibitors use in Australia. Pharmacoepidemiol Drug Saf 2010;19: [20] Johansen ME, Huerta TR, Richardson CR. National Use of Proton Pump Inhibitors From 2007 to JAMA Intern Med 2014;174: [21] Warle-van Herwaarden MF, Koffeman AR, Valkhoff VE, et al. Time-trends in the prescribing of gastroprotective agents to primary care patients initiating low-dose aspirin or non-steroidal anti-inflammatory drugs: a population-based cohort study. Br J Clin Pharmacol 2015;80: [22] Targownik LE, Metge C, Roos L, et al. The prevalence of and the clinical and demographic characteristics associated with high-intensity proton pump inhibitor use. Am J Gastroenterol 2007;102: [23] de Souto Barreto P, Lapeyre-Mestre M, Mathieu C, et al. Prevalence and associations of the use of proton-pump inhibitors in nursing homes: a cross-sectional study. J Am Med Dir Assoc 2013;14: [24] Thomas L, Culley EJ, Gladowski P, et al. Longitudinal analysis of the costs associated with inpatient initiation and subsequent outpatient continuation of proton pump inhibitor therapy for stress ulcer prophylaxis in a large managed care organization. J Manag Care Pharm 2010;16:
24 [25] Haastrup P, Paulsen MS, Begtrup LM, et al. Strategies for discontinuation of proton pump inhibitors: a systematic review. Fam Pract 2014;31: [26] Clyne B, Smith SM, Hughes CM, et al. Effectiveness of a multifaceted intervention on potentially inappropriate prescribing in older patients in primary care: a cluster randomised controlled trial (the OPTI-SCRIPT study). Ann Fam Med 2015;13: [27] Feely J, Chan R, McManus J, et al. The influence of hospital-based prescribers on prescribing in general practice. Pharmacoeconomics 1999;16: [28] Zink DA, Pohlman M, Barnes M, et al. Long-term use of acid suppression started inappropriately during hospitalization. Aliment Pharmacol Ther 2005;21: [29] Moran N, Jones E, O Toole A, et al. The appropriateness of a proton pump inhibtor prescription. Ir Med J 2014;107: [30] Wermeling M, Himmel W, Behrens G, et al. Why do GPs continue inappropriate hospital prescriptions of proton pump inhibitors? A qualitative study. Eur J Gen Pract 2014;20:
25 Figure 23
26 Figure 1 Prescribing of PPIs and ulcerogenic medicines to General Medical Services scheme-eligible population of Eastern Health Board region of Ireland aged 65 years in 1997, 2002, 2007 and Abbreviations: PPI = proton pump inhibitor; NSAID = non-steroidal anti-inflammatory drug; AP = antiplatelet drug (excluding aspirin); AC = anticoagulant drug; CS= corticosteroid; GI = gastrointestinal 24
27 Tables Table 1 Number and Percentage of Individuals Prescribed a Proton Pump Inhibitor (PPI) in 1997, 2002, 2007 and 2012, Categorised by Duration of Use, Dosage and Concurrent Medications Use 1997 (n=78,489) a 2002 (n=121,726) a 2007 (n=129,162) a 2012 (n=133,884) a n % prevalence n % prevalence n % prevalence n % prevalence (95% CI) (95% CI) (95% CI) (95% CI) Prescribed a PPI (10.5, 10.9) (27.6, 28.1) (50.1, 50.6) (48.2, 48.7) Short-term PPI ( 8 weeks) (6.4, 6.7) (14.3, 14.7) (24.2, 24.6) (12.8, 13.1) Long-term PPI (>8 weeks) (4.0, 4.3) (13.2, 13.5) (25.7, 26.2) (35.2, 35.8) Long-term PPI, maintenance dose b (3.2, 3.4) (6.9, 7.2) (10.3, 10.7) (11.8, 12.1) Long-term PPI, maximal dose b (0.8, 0.9) (6.2, 6.5) (15.2, 15.6) (23.3, 23.8) - with an NSAID c (0.3, 0.3) (2.5, 2.7) (6.3, 6.6) (6.3, 6.5) - with aspirin c (0.2, 0.3) (2.9, 3.1) (8.5, 8.8) (13.0, 13.4) - with an antiplatelet d or (0.1, 0.1) (1.2, 1.3) (4.2, 4.4) (5.9, 6.2) anticoagulant drug c 25
28 1997 (n=78,489) a 2002 (n=121,726) a 2007 (n=129,162) a 2012 (n=133,884) a n % prevalence n % prevalence n % prevalence n % prevalence (95% CI) (95% CI) (95% CI) (95% CI) - with a long-term ( 3 months) (0.1, 0.1) (0.6, 0.7) (1.3, 1.4) (1.8, 1.9) corticosteroid c Long-term PPI, maximal dose b, (0.3, 0.3) (1.3, 1.5) (2.7, 2.8) (4.6, 4.8) none of above medicines a Total number of people aged 65 years eligible for General Medical Services scheme in Eastern Health Board region for each study year b Dose classified as maximal i.e. greater than or equal to treatment dosage recommend by the United Kingdom National Institute for Clinical and Care Excellence (40mg daily for omeprazole, pantoprazole, and esomeprazole, 30mg daily for lansoprazole and 20mg daily for rabeprazole), or maintenance i.e. less than treatment dose.[13] c Categories not mutually exclusive, individuals may have been co-prescribed more than one type of ulcerogenic medicine d Antiplatelet drugs excluding aspirin 26
29 Table 2 Unadjusted and adjusted odds ratios and 95% CIs for factors associated with maximal dose compared to maintenance dose in long-term PPI users Unadjusted OR (95% CI) Adjusted OR (95% CI) b Concurrent aspirin 1.13 (1.11, 1.16) 0.95 (0.92, 0.97) Concurrent NSAID 0.84 (0.82, 0.86) 0.87 (0.85, 0.89) Concurrent antiplatelet a /anticoagulant 1.64 (1.59, 1.69) 1.36 (1.31, 1.41) Concurrent corticosteroid for 3 months 1.19 (1.13, 1.24) 1.09 (1.04, 1.15) Age group years (reference) years 0.90 (0.86, 0.94) 0.90 (0.86, 0.93) 75+ years 0.94 (0.91, 0.97) 0.86 (0.83, 0.89) Female (vs male) 0.89 (0.87, 0.91) 0.90 (0.88, 0.92) Level of polypharmacy 0-4 medicines (reference) medicines 1.45 (1.40, 1.50) 1.28 (1.24, 1.34) 10+ medicines 2.39 (2.30, 2.49) 1.91 (1.83, 2.00) Study year 1997 (reference) (3.20, 3.83) 3.28 (2.99, 3.59) (5.24, 6.25) 4.86 (4.45, 5.32) (7.04, 8.39) 6.30 (5.76, 6.88) a Antiplatelet drugs excluding aspirin. b Mean variance inflation factor for all included covariates was 4.05 indicating no serious multicollinearity. 27
Measuring and Evaluating Indicators of Appropriate Prescribing in Older. Populations
 HRB PhD Scholar Division of Population Health Sciences RCSI Measuring and Evaluating Indicators of Appropriate Prescribing in Older Cost-Effective Proton Pump Populations Potential Strategies for more
HRB PhD Scholar Division of Population Health Sciences RCSI Measuring and Evaluating Indicators of Appropriate Prescribing in Older Cost-Effective Proton Pump Populations Potential Strategies for more
Proton Pump Inhibitor De-prescribing Guidance
 Amendment History Proton Pump Inhibitor De-prescribing Guidance VERSION DATE AMENDMENT HISTORY 1.0 2013 Previous version 2.0 September 2015 Comments Amendment to Flow chart and addition of Rationale page
Amendment History Proton Pump Inhibitor De-prescribing Guidance VERSION DATE AMENDMENT HISTORY 1.0 2013 Previous version 2.0 September 2015 Comments Amendment to Flow chart and addition of Rationale page
High use of maintenance therapy after triple therapy regimes in Ireland
 High use of maintenance therapy after triple therapy regimes in Ireland K Bennett, H O Connor, M Barry, C O Morain, J Feely Department of Pharmacology & Therapeutics Department of Gastroenterology Trinity
High use of maintenance therapy after triple therapy regimes in Ireland K Bennett, H O Connor, M Barry, C O Morain, J Feely Department of Pharmacology & Therapeutics Department of Gastroenterology Trinity
Royal College of Surgeons in Ireland Coláiste Ríoga na Máinleá in Éirinn
 Royal College of Surgeons in Ireland Coláiste Ríoga na Máinleá in Éirinn Prescribing indicators to assess potentially inappropriate prescribing (PIP): Overview of current criteria and development of the
Royal College of Surgeons in Ireland Coláiste Ríoga na Máinleá in Éirinn Prescribing indicators to assess potentially inappropriate prescribing (PIP): Overview of current criteria and development of the
Proton Pump Inhibitors:
 Proton Pump Inhibitors: How bad could they be? Andrea Flanagan, Pharm.D. Iowa City VA Medical Center PGY-1 Pharmacy Resident Objectives for Pharmacists At the end of this presentation PHARMACISTS should
Proton Pump Inhibitors: How bad could they be? Andrea Flanagan, Pharm.D. Iowa City VA Medical Center PGY-1 Pharmacy Resident Objectives for Pharmacists At the end of this presentation PHARMACISTS should
Rpts. GENERAL General Schedule (Code GE) Program Prescriber type: Dental Medical Practitioners Nurse practitioners Optometrists Midwives
 Program Prescriber type: Dental Medical Practitioners Nurse practitioners Optometrists Midwives") Esomeprazole 20mg Name, Restriction, Manner of esomeprazole 20 mg enteric tablet, 30 (8886Q) (029W) Gastric ulcer Peptic ulcer Treatment Phase: Initial treatment The therapy must be for initial treatment
Esomeprazole 20mg Name, Restriction, Manner of esomeprazole 20 mg enteric tablet, 30 (8886Q) (029W) Gastric ulcer Peptic ulcer Treatment Phase: Initial treatment The therapy must be for initial treatment
Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist
 Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist") Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist Disclosures I have no actual or potential conflicts of interest to report in relation to this
Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist Disclosures I have no actual or potential conflicts of interest to report in relation to this
PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW
 PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW DATE OF AUTHORISATION: AUTHORISING GP: PRESCRIBING SUPPORT TECHNICIAN: SUMMARY Dyspepsia refers to a broad range of symptoms related
PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW DATE OF AUTHORISATION: AUTHORISING GP: PRESCRIBING SUPPORT TECHNICIAN: SUMMARY Dyspepsia refers to a broad range of symptoms related
Have COX-2 inhibitors influenced the co-prescription of anti-ulcer drugs with NSAIDs?
 et al. DOI:10.1111/j.1365-2125.2003.02012.x British Journal of Clinical Pharmacology Have COX-2 inhibitors influenced the co-prescription of anti-ulcer drugs with NSAIDs? Mary Teeling, Kathleen Bennett
et al. DOI:10.1111/j.1365-2125.2003.02012.x British Journal of Clinical Pharmacology Have COX-2 inhibitors influenced the co-prescription of anti-ulcer drugs with NSAIDs? Mary Teeling, Kathleen Bennett
DRUG UTILIZATION STUDIES TO GUIDE BETTER HOSPITAL PHARMACEUTICAL POLICY
 DRUG UTILIZATION STUDIES TO GUIDE BETTER HOSPITAL PHARMACEUTICAL POLICY Dr. G. Parthasarathi Professor, Pharmacy Practice JSS University, Mysore 30 October 2011 ACPE6 Beijing, 2011 1 Presentation Outline
DRUG UTILIZATION STUDIES TO GUIDE BETTER HOSPITAL PHARMACEUTICAL POLICY Dr. G. Parthasarathi Professor, Pharmacy Practice JSS University, Mysore 30 October 2011 ACPE6 Beijing, 2011 1 Presentation Outline
Survey on repeat prescribing for acid suppression drugs in primary care in Cornwall and the Isles of Scilly
 Aliment Pharmacol Ther 1999; 13: 813±817. Survey on repeat prescribing for acid suppression drugs in primary care in Cornwall and the Isles of Scilly R. BOUTET, M. WILCOCK & I. MACKENZIE 1 Department of
Aliment Pharmacol Ther 1999; 13: 813±817. Survey on repeat prescribing for acid suppression drugs in primary care in Cornwall and the Isles of Scilly R. BOUTET, M. WILCOCK & I. MACKENZIE 1 Department of
The Appropriateness of Acid Suppressive Medications Use in a Tertiary Hospital in Kedah
 Human Journals Research Article July 2016 Vol.:6, Issue:4 All rights are reserved by Kirubakaran Ranita et al. The Appropriateness of Acid Suppressive Medications Use in a Tertiary Hospital in Kedah Keywords:
Human Journals Research Article July 2016 Vol.:6, Issue:4 All rights are reserved by Kirubakaran Ranita et al. The Appropriateness of Acid Suppressive Medications Use in a Tertiary Hospital in Kedah Keywords:
Identifying patients who may benefit from stepping down PPI treatment
 CLINICAL AUDIT Identifying patients who may benefit from stepping down PPI treatment Valid to January 2024 bpac nz better medicin e This audit identifies patients who are prescribed the proton pump inhibitor
CLINICAL AUDIT Identifying patients who may benefit from stepping down PPI treatment Valid to January 2024 bpac nz better medicin e This audit identifies patients who are prescribed the proton pump inhibitor
Oral proton pump inhibitors (PPIs)
") Treatment Guideline Oral proton pump inhibitors (PPIs) Introduction The high efficacy and low toxicity of proton pump inhibitors (PPIs) has contributed to their frequent prescription worldwide, often without
Treatment Guideline Oral proton pump inhibitors (PPIs) Introduction The high efficacy and low toxicity of proton pump inhibitors (PPIs) has contributed to their frequent prescription worldwide, often without
Prescribing of anti-osteoporotic therapies following the use of Proton Pump Inhibitors in general practice
 Prescribing of anti-osteoporotic therapies following the use of Proton Pump Inhibitors in general practice B. McGowan, K. Bennett, J. Feely Department of Pharmacology & Therapeutics, Trinity Centre for
Prescribing of anti-osteoporotic therapies following the use of Proton Pump Inhibitors in general practice B. McGowan, K. Bennett, J. Feely Department of Pharmacology & Therapeutics, Trinity Centre for
NSAIDs Change Package 2017/2018
 NSAIDs Change Package 2017/2018 Aim: To Reduce harm to patients from Non-Steroidal Anti-inflammatory Drugs (NSAIDs) in primary care Background A key aim of the Safety in Practice programme is to reduce
NSAIDs Change Package 2017/2018 Aim: To Reduce harm to patients from Non-Steroidal Anti-inflammatory Drugs (NSAIDs) in primary care Background A key aim of the Safety in Practice programme is to reduce
Disclosures. Proton Pump Inhibitors Deprescribing? Deprescribing PPI Objectives. Deprescribing. Proton Pump Inhibitors (PPI) 5/28/2018.
 5/28/2018.") Proton Pump Inhibitors Deprescribing? None Disclosures Chad Burski, MD Assistant Professor of Medicine UAB Gastroenterology Deprescribing PPI Objectives AR Why? Who? How? The mechanism of action of Proton
Proton Pump Inhibitors Deprescribing? None Disclosures Chad Burski, MD Assistant Professor of Medicine UAB Gastroenterology Deprescribing PPI Objectives AR Why? Who? How? The mechanism of action of Proton
Management of Dyspepsia
 MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
The Role of Pharmacists achieving international best practice standards and realising key opportunities.
 The Role of Pharmacists achieving international best practice standards and realising key opportunities. Dr. Stephen Byrne Senior Lecturer in Clinical Pharmacy & Director of the MSc in Clinical Pharmacy
The Role of Pharmacists achieving international best practice standards and realising key opportunities. Dr. Stephen Byrne Senior Lecturer in Clinical Pharmacy & Director of the MSc in Clinical Pharmacy
Developing Evidence-Based Best Practices for the Prescribing and Use of Proton Pump Inhibitors in Canada
 Developing Evidence-Based Best Practices for the Prescribing and Use of Proton Pump Inhibitors in Canada Presented by: Sumeet R. Singh, COMPUS April 4, 2006 Background COMPUS Objective: To identify and
Developing Evidence-Based Best Practices for the Prescribing and Use of Proton Pump Inhibitors in Canada Presented by: Sumeet R. Singh, COMPUS April 4, 2006 Background COMPUS Objective: To identify and
Proton pump inhibitors: potential cost reductions by applying prescribing guidelines
 Cahir et al. BMC Health Services Research 2012, 12:408 RESEARCH ARTICLE Open Access Proton pump inhibitors: potential cost reductions by applying prescribing guidelines Caitriona Cahir 1*, Tom Fahey 1,
Cahir et al. BMC Health Services Research 2012, 12:408 RESEARCH ARTICLE Open Access Proton pump inhibitors: potential cost reductions by applying prescribing guidelines Caitriona Cahir 1*, Tom Fahey 1,
MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD)
") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
Guidelines for the Management of Dyspepsia and GORD. Gastroenterology/ Acute Adult Governance. Drugs and Therapeutics Committee
 Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Screening tools for elderly patients in primary care
 Screening tools for elderly patients in primary care Cristín Ryan 1 Prof. Julia Kennedy 1 Dr. Denis O Mahony 2 Dr. Stephen Byrne 1 Co-Investigator: Dr. Paul Gallagher 2 1 Pharmaceutical Care Research Group,
Screening tools for elderly patients in primary care Cristín Ryan 1 Prof. Julia Kennedy 1 Dr. Denis O Mahony 2 Dr. Stephen Byrne 1 Co-Investigator: Dr. Paul Gallagher 2 1 Pharmaceutical Care Research Group,
Pharmacoeconomic analysis of proton pump inhibitor therapy and interventions to control Helicobacter pylori infection Klok, Rogier Martijn
 University of Groningen Pharmacoeconomic analysis of proton pump inhibitor therapy and interventions to control Helicobacter pylori infection Klok, Rogier Martijn IMPORTANT NOTE: You are advised to consult
University of Groningen Pharmacoeconomic analysis of proton pump inhibitor therapy and interventions to control Helicobacter pylori infection Klok, Rogier Martijn IMPORTANT NOTE: You are advised to consult
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU
 Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Policy Evaluation: Proton Pump Inhibitors (PPIs)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The PROMPT criteria: Development and validation of prescribing indicators in middle-aged adults
 The PROMPT criteria: Development and validation of prescribing indicators in middle-aged adults Dr. Janine Cooper, Professor Carmel Hughes, Dr. Cristín Ryan, Professor Susan Smith, Dr. Emma Wallace, Dr.
The PROMPT criteria: Development and validation of prescribing indicators in middle-aged adults Dr. Janine Cooper, Professor Carmel Hughes, Dr. Cristín Ryan, Professor Susan Smith, Dr. Emma Wallace, Dr.
Proton Pump Inhibitors. Description. Section: Prescription Drugs Effective Date: July 1, 2014
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.09.01 Subject: Proton Pump Inhibitors Page: 1 of 7 Last Review Date: June 12, 2014 Proton Pump Inhibitors
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.09.01 Subject: Proton Pump Inhibitors Page: 1 of 7 Last Review Date: June 12, 2014 Proton Pump Inhibitors
Omeprazole 10mg. Name, Restriction, Manner of administration and form OMEPRAZOLE omeprazole 10 mg enteric tablet, 30 (8332M) Max. Qty.
 Max. Qty.") Omeprazole 10mg Name, Restriction, Manner of administration and form omeprazole 10 mg enteric tablet, 30 (8332M) Gastro-oesophageal reflux disease Name, Restriction, Manner of administration and form omeprazole
Omeprazole 10mg Name, Restriction, Manner of administration and form omeprazole 10 mg enteric tablet, 30 (8332M) Gastro-oesophageal reflux disease Name, Restriction, Manner of administration and form omeprazole
Drug Class Monograph
 Drug Class Monograph Class: Proton Pump Inhibitors Drugs: Aciphex Sprinkle (rabeprazole), Dexilant (dexlansoprazole), Lansoprazole, Nexium (esomeprazole capsule, esomeprazole granules), Omeprazole, Pantoprazole,
Drug Class Monograph Class: Proton Pump Inhibitors Drugs: Aciphex Sprinkle (rabeprazole), Dexilant (dexlansoprazole), Lansoprazole, Nexium (esomeprazole capsule, esomeprazole granules), Omeprazole, Pantoprazole,
COMPUS OPTIMAL THERAPY REPORT. Supporting Informed Decisions. À l appui des décisions éclairées. Proton Pump Inhibitor Project Overview: Summaries
 OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 1 March 2007 Proton Pump Inhibitor Project Overview: Summaries Supporting Informed Decisions À l appui des décisions éclairées This Executive Summary is based
OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 1 March 2007 Proton Pump Inhibitor Project Overview: Summaries Supporting Informed Decisions À l appui des décisions éclairées This Executive Summary is based
Rpts. GENERAL General Schedule (Code GE)
") Pantoprazole 20mg Name, Restriction, Manner of administration and form Pantoprazole 20mg enteric tablet, 30 (8399C) Gastro-oesophageal reflux disease Name, Restriction, Manner of administration and form
Pantoprazole 20mg Name, Restriction, Manner of administration and form Pantoprazole 20mg enteric tablet, 30 (8399C) Gastro-oesophageal reflux disease Name, Restriction, Manner of administration and form
The Nottingham eprints service makes this work by researchers of the University of Nottingham available open access under the following conditions.
 Othman, Fatmah and Card, Timothy R. and Crooks, Colin J. (2016) Proton pump inhibitor prescribing patterns in the UK: a primary care database study. Pharmacoepidemiology and Drug Safety, 25 (9). pp. 1079-1087.
Othman, Fatmah and Card, Timothy R. and Crooks, Colin J. (2016) Proton pump inhibitor prescribing patterns in the UK: a primary care database study. Pharmacoepidemiology and Drug Safety, 25 (9). pp. 1079-1087.
A C A D E M I C D E TA I L I N G C H O O S I N G W I S E LY C O N F E R E N C E O C T 2 1, PA M M C L E A N - V E Y S E Y B S C P H A R M D R
 PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
a newsletter detailing appropriate indications of IV PPI was sent to physicians;
 Inappropriate use of intravenous pantoprazole: extent of the problem and successful solutions Kaplan G G, Bates D, McDonald D, Panaccione R, Romagnuolo J Record Status This is a critical abstract of an
Inappropriate use of intravenous pantoprazole: extent of the problem and successful solutions Kaplan G G, Bates D, McDonald D, Panaccione R, Romagnuolo J Record Status This is a critical abstract of an
The first stop for professional medicines advice. Community Pharmacy NSAID Gastro-Intestinal Safety Audit
 Community Pharmacy NSAID Gastro-Intestinal Safety Audit Working with Primary Care Commissioning, Strategy and Innovation Directorate The first stop for professional medicines advice www.sps.nhs.uk Community
Community Pharmacy NSAID Gastro-Intestinal Safety Audit Working with Primary Care Commissioning, Strategy and Innovation Directorate The first stop for professional medicines advice www.sps.nhs.uk Community
COMPUS OPTIMAL THERAPY REPORT. Supporting Informed Decisions. À l appui des décisions éclairées
 OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 6 March 2007 Gap Analysis Report for the Prescribing and Use of Proton Pump Inhibitors (PPIs) Supporting Informed Decisions À l appui des décisions éclairées
OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 6 March 2007 Gap Analysis Report for the Prescribing and Use of Proton Pump Inhibitors (PPIs) Supporting Informed Decisions À l appui des décisions éclairées
Royal College of Surgeons in Ireland Barbara Clyne Royal College of Surgeons in Ireland
 Royal College of Surgeons in Ireland e-publications@rcsi General Practice Articles Department of General Practice 2-6-2016 Sustained effectiveness of a multifaceted intervention to reduce potentially inappropriate
Royal College of Surgeons in Ireland e-publications@rcsi General Practice Articles Department of General Practice 2-6-2016 Sustained effectiveness of a multifaceted intervention to reduce potentially inappropriate
Management of dyspepsia and of Helicobacter pylori infection
 Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Proton pump inhibitors and the risk of pneumonia: a comparison of cohort and self-controlled case series designs
 Ramsay et al. BMC Medical Research Methodology 2013, 13:82 RESEARCH ARTICLE Open Access Proton pump inhibitors and the risk of pneumonia: a comparison of cohort and self-controlled case series designs
Ramsay et al. BMC Medical Research Methodology 2013, 13:82 RESEARCH ARTICLE Open Access Proton pump inhibitors and the risk of pneumonia: a comparison of cohort and self-controlled case series designs
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients
 A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients") There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
Proton Pump Inhibitors (PPIs) (Sherwood Employer Group)
 (Sherwood Employer Group)") Proton Pump Inhibitors (PPIs) (Sherwood Employer Group) BCBSKS will review Prior Authorization requests Prior Authorization Form: https://www.bcbsks.com/customerservice/forms/pdf/priorauth-6058ks-st-ippi.pdf
Proton Pump Inhibitors (PPIs) (Sherwood Employer Group) BCBSKS will review Prior Authorization requests Prior Authorization Form: https://www.bcbsks.com/customerservice/forms/pdf/priorauth-6058ks-st-ippi.pdf
Complications of Proton Pump Inhibitor Therapy. Gastroenterology 2017; 153:35-48 발표자 ; F1 김선화
 Complications of Proton Pump Inhibitor Therapy Gastroenterology 2017; 153:35-48 발표자 ; F1 김선화 Background Proton pump inhibitors (PPIs) are among the most commonly prescribed medicines for gastroesophageal
Complications of Proton Pump Inhibitor Therapy Gastroenterology 2017; 153:35-48 발표자 ; F1 김선화 Background Proton pump inhibitors (PPIs) are among the most commonly prescribed medicines for gastroesophageal
Briefing Document on Medication use and Falls
 Briefing Document on Medication use and Falls This document is intended as a briefing document and is not to be regarded as a document offering definitive legal advice in relation to the subject matter.
Briefing Document on Medication use and Falls This document is intended as a briefing document and is not to be regarded as a document offering definitive legal advice in relation to the subject matter.
COMPUS OPTIMAL THERAPY REPORT. Supporting Informed Decisions. À l appui des décisions éclairées. Proton Pump Inhibitor Project Overview: Summaries
 OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 1 March 2007 Proton Pump Inhibitor Project Overview: Summaries Supporting Informed Decisions À l appui des décisions éclairées This Executive Summary is based
OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 1 March 2007 Proton Pump Inhibitor Project Overview: Summaries Supporting Informed Decisions À l appui des décisions éclairées This Executive Summary is based
Perplexed by PPI s Should I be Worried? James R Gray Gastroenterology Vancouver
 Perplexed by PPI s Should I be Worried? James R Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Perplexed by PPI s Should I be Worried? James R Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Proton Pump Inhibitors. Description
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.01 Subject: Proton Pump Inhibitors Page: 1 of 6 Last Review Date: June 24, 2015 Proton Pump Inhibitors
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.01 Subject: Proton Pump Inhibitors Page: 1 of 6 Last Review Date: June 24, 2015 Proton Pump Inhibitors
LONG -TERM USE OF PPIS: INDICATIONS, BENEFITS AND HARMS. Jihane Naous, M.D.
 LONG -TERM USE OF PPIS: INDICATIONS, BENEFITS AND HARMS Jihane Naous, M.D. Objectives Identify the conditions supported by AGA/ACG guidelines necessitating long-term use of daily PPIs, Recognize which
LONG -TERM USE OF PPIS: INDICATIONS, BENEFITS AND HARMS Jihane Naous, M.D. Objectives Identify the conditions supported by AGA/ACG guidelines necessitating long-term use of daily PPIs, Recognize which
Optimising Safe & Appropriate Medicines Use and Deprescribing. Katie Smith, Director, East Anglia Medicines Information Service February 2014
 Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5),
,") Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5), 268-271 Copyright: This is an Accepted Manuscript of an article published by Taylor
Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5), 268-271 Copyright: This is an Accepted Manuscript of an article published by Taylor
CYP2C19-Proton Pump Inhibitors
 CYP2C19-Proton Pump Inhibitors Cameron Thomas, Pharm.D. PGY2 Clinical Pharmacogenetics Resident St. Jude Children s Research Hospital February 1, 2018 Objectives: CYP2C19-PPI Implementation Review the
CYP2C19-Proton Pump Inhibitors Cameron Thomas, Pharm.D. PGY2 Clinical Pharmacogenetics Resident St. Jude Children s Research Hospital February 1, 2018 Objectives: CYP2C19-PPI Implementation Review the
PPIs: Good or Bad? 1. Basics of PPIs. Gastric Acid Basics. Outline. Gastric Acid Basics. Proton Pump Inhibitors (PPI)
") Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
A Prospective Observational Study on Evidence-Based and Unlicensed Indications for Proton Pump Inhibitors in Inpatients of a Tertiary Care Hospital
 Research Article A Prospective Observational Study on Evidence-Based and Unlicensed Indications for Proton Pump Inhibitors in Inpatients of a Tertiary Care Hospital B. Blessy Ruth Mounika 1, P. Saranya
Research Article A Prospective Observational Study on Evidence-Based and Unlicensed Indications for Proton Pump Inhibitors in Inpatients of a Tertiary Care Hospital B. Blessy Ruth Mounika 1, P. Saranya
MY PATIENT HAS READ THAT HIS PPI S MAY BE TROUBLE. NOW WHAT?
 MY PATIENT HAS READ THAT HIS PPI S MAY BE TROUBLE. NOW WHAT? Clarence Wong MD FRCPC Associate Professor FACULTY/PRESENTER DISCLOSURE Faculty: Clarence Wong Relationships with commercial interests: Grants/Research
MY PATIENT HAS READ THAT HIS PPI S MAY BE TROUBLE. NOW WHAT? Clarence Wong MD FRCPC Associate Professor FACULTY/PRESENTER DISCLOSURE Faculty: Clarence Wong Relationships with commercial interests: Grants/Research
Proton Pump Inhibitors Drug Class Prior Authorization Protocol
 Proton Pump Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review
Proton Pump Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review
Source of effectiveness data The effectiveness data were derived from a review and synthesis of completed studies.
 Economic evaluation of maintenance therapies for reflux esophagitis: comparison between step-up therapies and step-down therapies Sugano K, Kobayashi M Record Status This is a critical abstract of an economic
Economic evaluation of maintenance therapies for reflux esophagitis: comparison between step-up therapies and step-down therapies Sugano K, Kobayashi M Record Status This is a critical abstract of an economic
Inappropriate use of proton pump inhibitors among medical inpatients: a questionnaire-based observational study
 RESEARCH Inappropriate use of proton pump inhibitors among medical inpatients: a questionnaire-based observational study Muhammad Haroon 1 Faiza Yasin 2 Syed K M Gardezi 1 Fahd Adeeb 1 Frank Walker 1 1
RESEARCH Inappropriate use of proton pump inhibitors among medical inpatients: a questionnaire-based observational study Muhammad Haroon 1 Faiza Yasin 2 Syed K M Gardezi 1 Fahd Adeeb 1 Frank Walker 1 1
Do calcium antagonists contribute to gastro-oesophageal reflux disease and concomitant noncardiac chest pain?
 DOI:10.1111/j.1365-2125.2007.02851.x British Journal of Clinical Pharmacology Do calcium antagonists contribute to gastro-oesophageal reflux disease and concomitant noncardiac chest pain? Jeff Hughes,
DOI:10.1111/j.1365-2125.2007.02851.x British Journal of Clinical Pharmacology Do calcium antagonists contribute to gastro-oesophageal reflux disease and concomitant noncardiac chest pain? Jeff Hughes,
Setting The setting was primary care. The economic analysis was conducted in Glasgow, UK.
 Helicobacter pylori eradication for peptic ulceration: an observational study in a Scottish primary care setting Forrest E H, MacKenzie J F, Stuart R C, Morris A J Record Status This is a critical abstract
Helicobacter pylori eradication for peptic ulceration: an observational study in a Scottish primary care setting Forrest E H, MacKenzie J F, Stuart R C, Morris A J Record Status This is a critical abstract
Pharmacoepidemiology and economic evaluation of measures of potentially inappropriate prescribing
 Royal College of Surgeons in Ireland e-publications@rcsi PhD theses Theses and Dissertations 1-1-2016 Pharmacoepidemiology and economic evaluation of measures of potentially inappropriate prescribing Frank
Royal College of Surgeons in Ireland e-publications@rcsi PhD theses Theses and Dissertations 1-1-2016 Pharmacoepidemiology and economic evaluation of measures of potentially inappropriate prescribing Frank
FARMACI E ALTE VIE DIGESTIVE NELL ANZIANO: UTILITÀ E LIMITI
 FARMACI E ALTE VIE DIGESTIVE NELL ANZIANO: UTILITÀ E LIMITI Edoardo V. Savarino, MD, PhD Professor of Gastroenterology Department of Surgery, Oncology and Gastroenterology University of Padua Italy COMMON
FARMACI E ALTE VIE DIGESTIVE NELL ANZIANO: UTILITÀ E LIMITI Edoardo V. Savarino, MD, PhD Professor of Gastroenterology Department of Surgery, Oncology and Gastroenterology University of Padua Italy COMMON
Deprescribing: A Practical Guide
 Deprescribing: A Practical Guide The information in this booklet should be used as a pragmatic decision aid, in conjunction with other relevant patient specific data. Useful resource links http://www.derbyshiremedicinesmanagement.nhs.uk/assets/clinical_guidelines/clinical_guidelines_fr
Deprescribing: A Practical Guide The information in this booklet should be used as a pragmatic decision aid, in conjunction with other relevant patient specific data. Useful resource links http://www.derbyshiremedicinesmanagement.nhs.uk/assets/clinical_guidelines/clinical_guidelines_fr
Practical Guide to Safety of PPIs What to Tell Your Patient. Proton Pump Inhibitors
 Practical Guide to Safety of PPIs What to Tell Your Patient Joel E Richter, MD, FACP, MACG Professor and Director Division of Digestive Diseases and Nutrition Joy Culverhouse Center for Esophageal Diseases
Practical Guide to Safety of PPIs What to Tell Your Patient Joel E Richter, MD, FACP, MACG Professor and Director Division of Digestive Diseases and Nutrition Joy Culverhouse Center for Esophageal Diseases
Katee Kindler, PharmD, BCACP
 Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
SELECTED ABSTRACTS. Figure. Risk Stratification Matrix A CLINICIAN S GUIDE TO THE SELECTION OF NSAID THERAPY
 SELECTED ABSTRACTS A CLINICIAN S GUIDE TO THE SELECTION OF NSAID THERAPY The authors of this article present a 4-quadrant matrix based on 2 key clinical parameters: risk for adverse gastrointestinal (GI)
SELECTED ABSTRACTS A CLINICIAN S GUIDE TO THE SELECTION OF NSAID THERAPY The authors of this article present a 4-quadrant matrix based on 2 key clinical parameters: risk for adverse gastrointestinal (GI)
11/19/2012. Comparison between PPIs G CELL. Risk ratio (95% CI) Patient subgroup. gastrin. S-form of omeprazole. Acid sensitive. coated.
 Patient subgroup. gastrin. S-form of omeprazole. Acid sensitive. coated.") REGULATION OF GASTRIC ACID SECRETION Comparison between PPIs Omeprazole Lansoprazole Rabeprazole Pantoprazole Esomeprazole gastrin G CELL + Acid sensitive Yes T1/2 30-60 minutes Main elimination Enteric
REGULATION OF GASTRIC ACID SECRETION Comparison between PPIs Omeprazole Lansoprazole Rabeprazole Pantoprazole Esomeprazole gastrin G CELL + Acid sensitive Yes T1/2 30-60 minutes Main elimination Enteric
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 PROTON PUMP INHIBITORS, NON-PREFERRED FORMS: ACIPHEX (rabeprazole sodium EC) oral tablet ACIPHEX SPRINKLE (rabeprazole sodium DR) oral capsule ESOMEPRAZOLE STRONTIUM (esomeprazole strontium DR) oral capsule
PROTON PUMP INHIBITORS, NON-PREFERRED FORMS: ACIPHEX (rabeprazole sodium EC) oral tablet ACIPHEX SPRINKLE (rabeprazole sodium DR) oral capsule ESOMEPRAZOLE STRONTIUM (esomeprazole strontium DR) oral capsule
Conflict of interest declaration and sources of funding
 Potentially Inappropriate Prescribing immediately prior to Long-Term Care admission (PIP in LTC): Validation of tools for their future use across Ontario Bruyère CLRI Webinar March 24 th, 2016 and Bruyère
Potentially Inappropriate Prescribing immediately prior to Long-Term Care admission (PIP in LTC): Validation of tools for their future use across Ontario Bruyère CLRI Webinar March 24 th, 2016 and Bruyère
COMPUS OPTIMAL THERAPY REPORT. Supporting Informed Decisions. À l appui des décisions éclairées
 OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 5 March 2007 Current Practice Analysis Report for the Prescribing and Use of Proton Pump Inhibitors (PPIs) Supporting Informed Decisions À l appui des décisions
OPTIMAL THERAPY REPORT COMPUS Volume 1, Issue 5 March 2007 Current Practice Analysis Report for the Prescribing and Use of Proton Pump Inhibitors (PPIs) Supporting Informed Decisions À l appui des décisions
II. Angiotensin Receptor Blockers (ARBs) Drug Class Review
 Drug Class Review") DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE DOD BENEFICIARY ADVISORY PANEL I. Uniform Formulary Review Process Under 10 U.S.C. 1074g, as implemented by 32 C.F.R. 199.21,
DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE DOD BENEFICIARY ADVISORY PANEL I. Uniform Formulary Review Process Under 10 U.S.C. 1074g, as implemented by 32 C.F.R. 199.21,
Overlap of Frailty, Comorbidity, Disability, and Poor Self-Rated Health in Community-Dwelling Near-Centenarians and Centenarians
 Title Overlap of Frailty, Comorbidity, Disability, and Poor Self-Rated Health in Community-Dwelling Near-Centenarians and Centenarians Author(s) Lau, HP; Kwan, SKJ; Cheung, KSL Citation Journal of the
Title Overlap of Frailty, Comorbidity, Disability, and Poor Self-Rated Health in Community-Dwelling Near-Centenarians and Centenarians Author(s) Lau, HP; Kwan, SKJ; Cheung, KSL Citation Journal of the
Database of Abstracts of Reviews of Effects (DARE) Produced by the Centre for Reviews and Dissemination Copyright 2017 University of York.
 Produced by the Centre for Reviews and Dissemination Copyright 2017 University of York.") A comparison of the cost-effectiveness of five strategies for the prevention of non-steroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling Brown
A comparison of the cost-effectiveness of five strategies for the prevention of non-steroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling Brown
Setting The setting was secondary care. The economic study was carried out in Hong Kong, China.
 Cost-effectiveness of Helicobacter pylori "test and treat" for patients with typical reflux symptoms in a population with a high prevalence of H. pylori infection: a Markov model analysis You J H, Wong
Cost-effectiveness of Helicobacter pylori "test and treat" for patients with typical reflux symptoms in a population with a high prevalence of H. pylori infection: a Markov model analysis You J H, Wong
Indigestion (dyspepsia)
") Commissioning pathways Indigestion (dyspepsia) Supplementary information to be read in conjunction with the pathway Reference Supplementary Information 1.1 Symptom Description Annual incidence 40%. Prevalence
Commissioning pathways Indigestion (dyspepsia) Supplementary information to be read in conjunction with the pathway Reference Supplementary Information 1.1 Symptom Description Annual incidence 40%. Prevalence
Concurrent use of alcohol interactive medications and alcohol in older adults: a systematic review of prevalence and associated adverse outcomes
 Concurrent use of alcohol interactive medications and alcohol in older adults: a systematic review of prevalence and associated adverse outcomes Alice Holton Royal College of Surgeons in Ireland 21 September
Concurrent use of alcohol interactive medications and alcohol in older adults: a systematic review of prevalence and associated adverse outcomes Alice Holton Royal College of Surgeons in Ireland 21 September
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Proton Pump Inhibitors- Questions & Controversies. Farah Kablaoui, PharmD, BCPS, BCCCP
 Proton Pump Inhibitors- Questions & Controversies Farah Kablaoui, PharmD, BCPS, BCCCP Disclosure Information Proton Pump Inhibitors: Questions & Controversies Farah Kablaoui I have no financial relationship
Proton Pump Inhibitors- Questions & Controversies Farah Kablaoui, PharmD, BCPS, BCCCP Disclosure Information Proton Pump Inhibitors: Questions & Controversies Farah Kablaoui I have no financial relationship
Shared decision making for stepdown and stopping decisions. Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes
 Shared decision making for stepdown and stopping decisions Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes 1 Disclosures I have had travel and lodging paid for
Shared decision making for stepdown and stopping decisions Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes 1 Disclosures I have had travel and lodging paid for
Cost-effectiveness of apremilast (Otezla )
") Cost-effectiveness of apremilast (Otezla ) alone or in combination with Disease Modifying Antirheumatic Drugs (DMARDs) for the treatment of active psoriatic arthritis in adult patients who have had an
Cost-effectiveness of apremilast (Otezla ) alone or in combination with Disease Modifying Antirheumatic Drugs (DMARDs) for the treatment of active psoriatic arthritis in adult patients who have had an
THE EFFECTS OF LONG- TERM PROTON PUMP INHIBITORS USE AND MISUSE
 THE EFFECTS OF LONG- TERM PROTON PUMP INHIBITORS USE AND MISUSE CONTENTS Overview Indications Over-prescribed in inappropriate conditions Side effects of long-term PPI use Conclusion OVERVIEW INDICATIONS
THE EFFECTS OF LONG- TERM PROTON PUMP INHIBITORS USE AND MISUSE CONTENTS Overview Indications Over-prescribed in inappropriate conditions Side effects of long-term PPI use Conclusion OVERVIEW INDICATIONS
Study population The study population comprised a hypothetical cohort of patients with confirmed reflux oesophagitis.
 Cost effectiveness of esomeprazole compared with omeprazole in the acute treatment of patients with reflux oesophagitis in the UK Wahlqvist P, Junghard O, Higgins A, Green J Record Status This is a critical
Cost effectiveness of esomeprazole compared with omeprazole in the acute treatment of patients with reflux oesophagitis in the UK Wahlqvist P, Junghard O, Higgins A, Green J Record Status This is a critical
From medicines reconciliation to medicines review. Dr. Fatma Karapinar Hospital pharmacistepidemiologist
 From medicines reconciliation to medicines review Dr. Fatma Karapinar Hospital pharmacistepidemiologist Conflict of interest Nothing to disclose Questions Medication review is more important than medicines
From medicines reconciliation to medicines review Dr. Fatma Karapinar Hospital pharmacistepidemiologist Conflict of interest Nothing to disclose Questions Medication review is more important than medicines
Bleeding Prevention in an Era of Expanding Combination Antithrombotic Therapies
 Bleeding Prevention in an Era of Expanding Combination Antithrombotic Therapies Muthiah Vaduganathan, MD MPH Cardiovascular Medicine Brigham and Women s Hospital December 8 th, 2017 Disclosures None Key
Bleeding Prevention in an Era of Expanding Combination Antithrombotic Therapies Muthiah Vaduganathan, MD MPH Cardiovascular Medicine Brigham and Women s Hospital December 8 th, 2017 Disclosures None Key
British Journal of Clinical Pharmacology. Frank Moriarty 1, Kathleen Bennett 2, Caitriona Cahir 2,RoseAnneKenny 3 and Tom Fahey 1
 British Journal of Clinical Pharmacology Br J Clin Pharmacol (2016) 82 849 857 849 PHARMACOEPIDEMIOLOGY Potentially inappropriate prescribing according to STOPP and START and adverse outcomes in community-dwelling
British Journal of Clinical Pharmacology Br J Clin Pharmacol (2016) 82 849 857 849 PHARMACOEPIDEMIOLOGY Potentially inappropriate prescribing according to STOPP and START and adverse outcomes in community-dwelling
Disclosure. The elderly at risk: reducing medications safely to meet life s changes. Relevant financial relationships.
 The elderly at risk: reducing medications safely to meet life s changes Barbara Farrell BScPhm, PharmD, FCSHP European Society of Hospital Pharmacists Conference March 2017 Disclosure Relevant financial
The elderly at risk: reducing medications safely to meet life s changes Barbara Farrell BScPhm, PharmD, FCSHP European Society of Hospital Pharmacists Conference March 2017 Disclosure Relevant financial
All Indiana Medicaid Prescribers and Pharmacy Providers
 P R O V I D E R B U L L E T I N BT200148 NOVEMBER 28, 2001 To: All Indiana Medicaid Prescribers and Pharmacy Providers Subject: Note: The information in this bulletin regarding prior authorization payment
P R O V I D E R B U L L E T I N BT200148 NOVEMBER 28, 2001 To: All Indiana Medicaid Prescribers and Pharmacy Providers Subject: Note: The information in this bulletin regarding prior authorization payment
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY
 TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
ARIC Manuscript Proposal #2493. PC Reviewed: 2/10/15 Status: A Priority: 2 SC Reviewed: Status: Priority:
 ARIC Manuscript Proposal #2493 PC Reviewed: 2/10/15 Status: A Priority: 2 SC Reviewed: Status: Priority: 1. a. Full Title: Potentially inappropriate medication use in older people: Prevalence and outcomes.
ARIC Manuscript Proposal #2493 PC Reviewed: 2/10/15 Status: A Priority: 2 SC Reviewed: Status: Priority: 1. a. Full Title: Potentially inappropriate medication use in older people: Prevalence and outcomes.
Patient Safety in Older Adults
 Patient Safety in Older Adults Scott Martin Vouri, PharmD, MSCI, BCPS, BCGP, FASCP St. Louis College of Pharmacy Faculty Disclosure Dr. Vouri is funded by the Washington University Institute of Clinical
Patient Safety in Older Adults Scott Martin Vouri, PharmD, MSCI, BCPS, BCGP, FASCP St. Louis College of Pharmacy Faculty Disclosure Dr. Vouri is funded by the Washington University Institute of Clinical
Setting The setting was the community. The economic study was carried out in the USA.
 Cost-effectiveness analysis of NSAIDs, NSAIDs with concomitant therapy to prevent gastrointestinal toxicity, and COX-2 specific inhibitors in the treatment of rheumatoid arthritis Yun H R, Bae S C Record
Cost-effectiveness analysis of NSAIDs, NSAIDs with concomitant therapy to prevent gastrointestinal toxicity, and COX-2 specific inhibitors in the treatment of rheumatoid arthritis Yun H R, Bae S C Record
Patient Safety in Older Adults
 Patient Safety in Older Adults Scott Martin Vouri, PharmD, MSCI, BCPS, BCGP, FASCP St. Louis College of Pharmacy Faculty Disclosure Dr. Vouri is funded by the Washington University Institute of Clinical
Patient Safety in Older Adults Scott Martin Vouri, PharmD, MSCI, BCPS, BCGP, FASCP St. Louis College of Pharmacy Faculty Disclosure Dr. Vouri is funded by the Washington University Institute of Clinical
The presence and development of gastric ulcers. Evaluation of Stress Ulcer Prophylaxis in a Family Medicine Residency Inpatient Service
 Evaluation of Stress Ulcer Prophylaxis in a Family Medicine Residency Inpatient Service Heather A. Kehr, PharmD, BCPS, Carrie L. Griffiths, PharmD, R. Wesley Haynes, PharmD, Sonia Everhart, PharmD, BCPS,
Evaluation of Stress Ulcer Prophylaxis in a Family Medicine Residency Inpatient Service Heather A. Kehr, PharmD, BCPS, Carrie L. Griffiths, PharmD, R. Wesley Haynes, PharmD, Sonia Everhart, PharmD, BCPS,
Assessment of Drug Therapy in Geriatric Patients Using Beer s Criteria
 Original Article Assessment of Drug Therapy in Geriatric Patients Using Beer s Criteria RJ Lihite *, M Lahkar **, S Roy * Abstract Aim: Inappropriate medication use (IMU) in the elderly population has
Original Article Assessment of Drug Therapy in Geriatric Patients Using Beer s Criteria RJ Lihite *, M Lahkar **, S Roy * Abstract Aim: Inappropriate medication use (IMU) in the elderly population has
The significance of Helicobacter pylori in the approach of dyspepsia in primary care Arents, Nicolaas Lodevikus Augustinus
 University of Groningen The significance of Helicobacter pylori in the approach of dyspepsia in primary care Arents, Nicolaas Lodevikus Augustinus IMPORTANT NOTE: You are advised to consult the publisher's
University of Groningen The significance of Helicobacter pylori in the approach of dyspepsia in primary care Arents, Nicolaas Lodevikus Augustinus IMPORTANT NOTE: You are advised to consult the publisher's
Stress ulcer prophylaxis (SUP) is commonly used
 is commonly used") Efforts to Reduce Stress Ulcer Prophylaxis Use in Non-Critically Ill Hospitalized Patients by Internal Medicine Residents: A Single-Institution Experience Gaurav Jain, MD, Sayeeda A. Jabeen, MD, and Srikanth
Efforts to Reduce Stress Ulcer Prophylaxis Use in Non-Critically Ill Hospitalized Patients by Internal Medicine Residents: A Single-Institution Experience Gaurav Jain, MD, Sayeeda A. Jabeen, MD, and Srikanth
Medication safety in vulnerable patient groups - Elderly patients -
 Woodennature/CC-BY-SA-3.0 http://theintelligence.de Medication safety in vulnerable patient groups - Elderly patients - 20th Congress of EAHP 25-27 March, 2015, Hamburg, Germany Dr. rer. nat. Beate Wickop
Woodennature/CC-BY-SA-3.0 http://theintelligence.de Medication safety in vulnerable patient groups - Elderly patients - 20th Congress of EAHP 25-27 March, 2015, Hamburg, Germany Dr. rer. nat. Beate Wickop
Physician specialty and the outcomes and cost of admissions for end-stage liver disease Ko C W, Kelley K, Meyer K E
 Physician specialty and the outcomes and cost of admissions for end-stage liver disease Ko C W, Kelley K, Meyer K E Record Status This is a critical abstract of an economic evaluation that meets the criteria
Physician specialty and the outcomes and cost of admissions for end-stage liver disease Ko C W, Kelley K, Meyer K E Record Status This is a critical abstract of an economic evaluation that meets the criteria
The Sustainability of Irish Pharmaceutical Expenditure. Valerie Walshe Ph.D. Economist
 The Sustainability of Irish Pharmaceutical Expenditure Valerie Walshe Ph.D. Economist valerie.walshe@hse.ie February 2015 Content Overview of Irish Health Services Community Drug Prescribing Trends Driving
The Sustainability of Irish Pharmaceutical Expenditure Valerie Walshe Ph.D. Economist valerie.walshe@hse.ie February 2015 Content Overview of Irish Health Services Community Drug Prescribing Trends Driving