Dementia. Amber Eker, MD. Assistant Professor Near East University Department of Neurology
|
|
|
- Bridget Pitts
- 5 years ago
- Views:
Transcription

1 Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology
2 Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social or occupational functioning
3 Classification of Dementias Primary versus secondary based on the pathophysiology leading to damaged brain tissue Cortical versus sub-cortical depending on the cerebral location of the primary deficits Reversible versus irreversible depending on optimal treatment expectations Early (before age 65) versus late onset
4 Dementias Most Common Dementias Degenerative Dementias 1-Alzheimer Disease 2-Lewy Body Dementia 3- Vaskular Dementia Alzheimer Disease Lewy Body Dementia Frontal Lobe Dementia Parkinsonism and Dementia
5
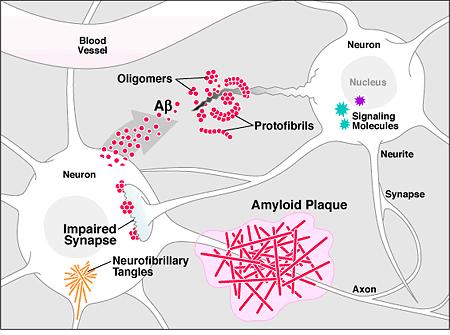
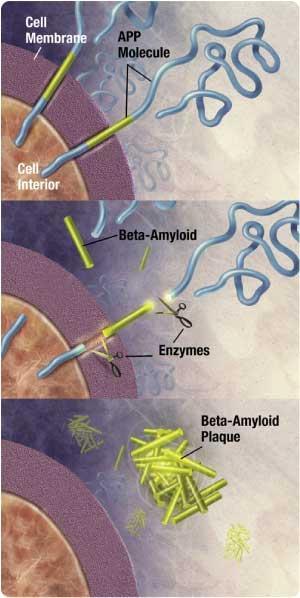
6 Alzheimer s Disease In 1901, a German psychiatrist named Alois Alzheimer observed a patient named Mrs. Auguste D. This 51-year-old woman suffered from a loss of shortterm memory and some behavioral symptoms in 1906, the patient died, and Dr. Alzheimer sent her brain to a laboratory. Pathologic evaluation identify amyloid plaques and neurofibrillary tangles. Dr. Alzheimer discribed was the first time the pathology and the clinical symptoms of the disorder in 1906 and published his findings in 1907
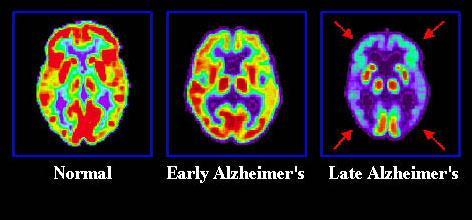
7 Alzheimer s Disease The most common form of dementia AD affects about million people in the world, and that number is projected to reach 80 million by the year 2050 Prevalance >65 ;%5-10, >85 %25-50 Oldest old / Graying population / Modern epidemia
 1950 50 yrs 2012 79")
8 Demografics of Aging >85 is fastest growing demographic group 20% of population by 2030 will be over 65 There will be more women than men Life expectancy: (F > M) yrs yrs
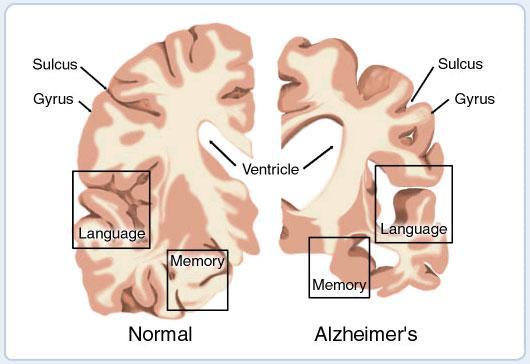
9 Alzheimer s Disease Short-term memory impairment AND At least one of the following: Aphasia - language impairments Apraxia - motor memory impairments Agnosia - sensory memory impairments Abstract thinking / Exec. function impairments Impairment in social and/or occupational functions
10 Aphasia Characterized initially by a fluent aphasia - Able to initiate and maintain a conversation - Impaired comprehension - Intact grammar but paraphasias - circumlocutions, tangential and often using nonspecific phrases ( the thing ) Later language can be severely impaired with mutism, echolalia.
11 Apraxia Inability to carry out motor activities despite intact motor function Agnosia The inability to recognize or identify objects despite intact sensory function Can be visual or tactile
12 Impaired Executive Function Difficulty with planning, initiating, sequencing, monitoring or stopping complex behaviors. Contributes to loss of intrumental activities such as shopping, meal preparation, driving and managing finances.
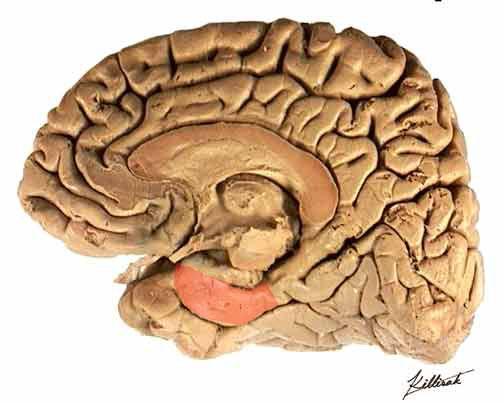
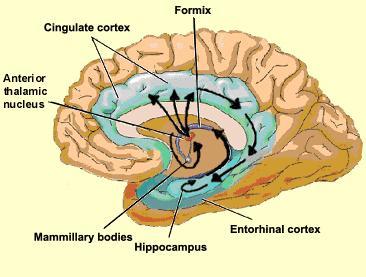
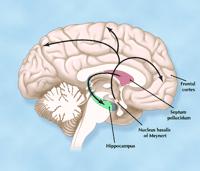
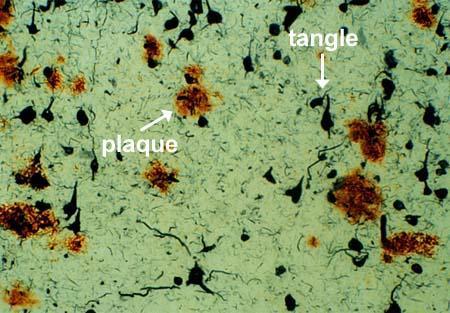
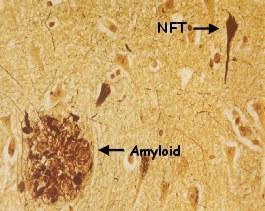
13 Pathology Neuropathological hallmarks: Amyloid-rich neuritic plaques -extracellular - abnormal insoluble amyloid (beta) protein fragments Neurofibrillary tangles - intracellular - disturbed taumicrotubule complexes (hyperphosphorylated tau) Cholinergic system degeneration with significant loss of neurons in certain areas (such as Nucleus Basalis of Meynert) Degeneration often begins in entorhinal cortex and progresses to other limbic structures
14
15 Pathology
16
17
18
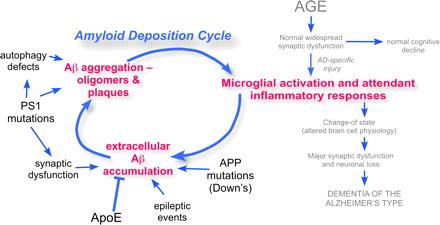
19 Pathophysiology Altered amyloid and tau protein metabolism Inflammation Oxidative stress Hormonal changes (Estrogen loss)
20 Risk Factors for AD Age Family history APOE 4 genotype Vascular risk factors Down s syndrome (trisomy 21) Head Trauma (esp. late in life) Late-onset depression (after age 65) Mild Cognitive Impairment (MCI)
21 Alzheimer Disease Most cases of AD are sporadic Familial forms of AD: Autosomal dominant AD, less than 5%
22 Genetic risk factors Chromosome 19 - autosomal recessive - Apolipoprotein E-4 allele - associated with late-onset disease Chromosome 1, 14, 21 - autosomal dominant mutations - associated with early-onset/familial cases. Amyloid processing genes. The amyloid precursor protein (APP) gene on chromosome 21 The presenilin-1 (PS1) gene on chromosome 14 The presenilin-2 (PS2) gene on chromosome 1
23 Education APO E 2 Protective Factors in AD Statin use? Anti-inflammatory agents? Estrogen replacement therapy??
24 Diagnosis Definitive diagnosis of AD : an autopsy or brain biopsy In clinical practice, the diagnosis is usually made on the basis of the history and findings on Mental Status Examination and radiologic evaluation ; Probable or possible AD
25 Alzheimer s Disease Short-term memory impairment AND At least one of the following: Aphasia - language impairments Apraxia - motor memory impairments Agnosia - sensory memory impairments Abstract thinking / Exec. function impairments Impairment in social and/or occupational functions At least one supportive test CSF Amyloid β, total tau, fosfo tau levels Retention in Amyloid PET Medial temporal lobe atrophy in MRI Temporoparietal hypometabolism in FDG PET Not explainable by another disorder
26
27 Treatment Symptomatic therapies Cholinesterase inhibitors These drugs block the esterase-mediated metabolism of acetylcholine to choline and acetate. This results in: Increased acetylcholine in the synaptic cleft Partial N -methyl-d-aspartate (NMDA) antagonist
28 Treatment Treatment of secondary symptoms of AD (depression, agitation, psychosis and sleep disorders)
29
30 MCI Some congnitive dysfunctions Functional activities are largely preserved MCI does not meet the criteria for dementia
31 Dementia with Lewy Bodies (DLB) 1. The central feature : Progressive cognitive decline with social or occupational dysfunction 2. Two of the following core features are essential for a diagnosis of probable DLB, and one is essential for possible DLB. Fluctuating cognition with pronounced variations in attention and alertness Recurrent visual hallucinations that are typically well formed and detailed Spontaneous motor features of parkinsonism 3. Features supportive of the diagnosis are repeated falls syncope transient loss of consciousness neuroleptic sensitivity systematized delusions hallucinations in other modalities.
 The main structural component is alphasynuclein, a presynaptic protein, the function of which is unknown Neurofilament proteins and ubiquitin are other important constituents")
32 Lewy Body Pathology Concentric spheres found within vacuoles (eosinophilic cytoplasmic inclusions) Seen in cortex, midbrain and brainstem neurons in patients especially with Lewy Body dementias (also idiopathic parkinsonism) The main structural component is alphasynuclein, a presynaptic protein, the function of which is unknown Neurofilament proteins and ubiquitin are other important constituents of LBs
 Infarcts on cerebral")
33 Vascular Dementia The onset of cognitive deficits associated with a stroke Abrupt onset of symptoms followed by stepwise deterioration Findings on neurologic examination consistent with prior stroke(s) Infarcts on cerebral imaging
 in the")
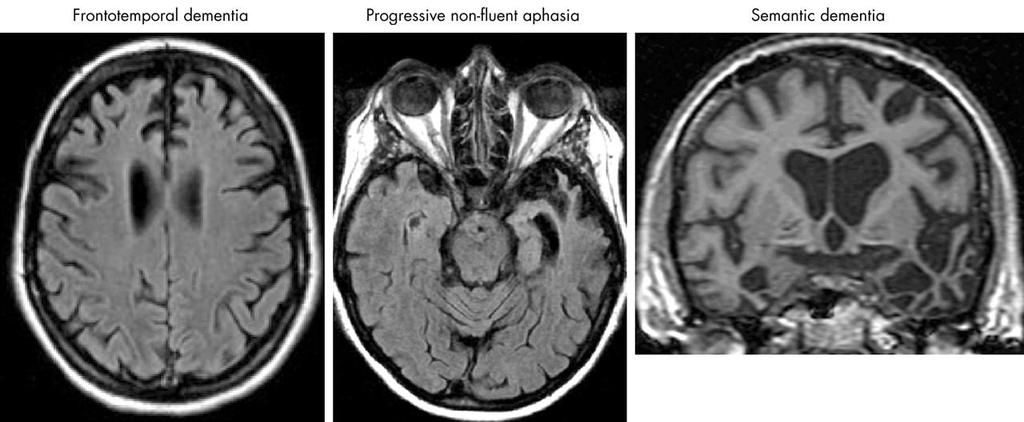
34 Frontotemporal Dementia Characterized by focal atrophy of the frontal and temporal lobes Clinically, presents with language abnormalities and behavioral disturbances. Pick's disease was the first recognized subtype of FTD, one that is characterized pathologically by the presence of Pick bodies (silver staining intracytoplasmic inclusions) in the neocortex and hippocampus.
35 Frontotemporal Dementia Occurs between the ages of 35 and 75 years, and only rarely after age 75; the mean age of onset is the sixth decade Both sexes are equally affected. Familial occurrence occurs in 20 to 40 percent of cases and may be associated with a variety of identified mutations in the tau gene on chromosome 17 Tau gene mutation also have seen in progressive supranuclear palsy (PSP), [13] corticobasal degeneration, and the amyotrophic lateral sclerosis (ALS)
36 Frontotemporal Lobe Dementia Core Features Insidious onset and gradual progression Early decline in social/interpersonal conduct Early impairment in personal conduct Early loss of insight Early emotional blunting Supportive Features Behavior disorder hygiene, grooming, mental rigidity, dietary changes, perseverative behavior Speech and language perseveration, mutism, economy of speech Physical signs akinesis, rigidity, tremor, labile BP
37
38 Parkinsonism and Dementia Parkinson Disease Dementia (PDD) Dementia with CBD, MSA, PSP


39 Normal-Pressure Hydrocephalus A condition of pathologically enlarged ventricular size with normal opening pressures on lumbar puncture Triad; dementia gait disturbance urinary incontinence Reversible by the placement of a ventriculoperitoneal shunt
40 Dementia associated with infectious diseases HIV Prion diseases Neurosyphilis PML Encephalitis ( Toxo, Criptococus, CMV, Herpes, Tbc, Lyme, Wipple, Brucella) SSPE
41 Metabolic Toxic Dementias Endocrinopathies: Hypotiroidism. Hypoparatiroidism, Cushing disease, Liver dysfunction Uremia Vitamine deficiencies (B12, Tiamin) Drugs; Anticholinergic, antihystaminic Alcohol abuse Heavy metals (arsenic, lead, mercury) Organic toxins (i insecticides, spreys)
42 Other Etiologies for Dementia Posttraumatic Slowly progressive intracranial mass Paraneoplastic
43 Reversible Reasons B12 deficiency Hypotiroidsm Other metabolic reasons NPH Some brain tumors Subdural hematoma
44 Pseudodementia Depression Schizophrenia Mental Reterdation is not dementia
45 Steps to take in Dementia Evaluation History Physical and Neurological Exam Cognitive Screening Test Rule out Reversible Causes Neuroimaging Consider the Etiology Treatment
46 History Taking and Examinations Get history also from caregiver or spouse Ask activities of daily living (Telephone, travel, shopping, meals, housework, medicine, money, bathing, dressing, grooming, toileting) Importance of Cognitive Screening Establish a baseline level of functioning Allows for objective documentation of cognition
47 Labwork Electrolytes BUN CBC Liver Enzymes TSH B12 Level Syphilis? Others only if clinical suspicion high
48 Neuroimaging CT, MRI Functional Imaging--not in initial workup
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Introduction to Dementia: Diagnosis & Evaluation. Created in March 2005 Duration: about 15 minutes
 Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Dementia: Diagnosis and Treatment
 Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Differentiating Dementia Diagnoses
 Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Dementia. Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 Dementia Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine What is Dementia? Dementia is a general term referring to a decline in cognitive/mental functioning; this decline
Dementia Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine What is Dementia? Dementia is a general term referring to a decline in cognitive/mental functioning; this decline
I do not have any disclosures
 Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
! slow, progressive, permanent loss of neurologic function.
 UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
FTD basics! Etienne de Villers-Sidani, MD!
 FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Form A3: Subject Family History
 Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Dementia and Healthy Ageing : is the pathology any different?
 Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
The Aging Brain The Aging Brain
 The Aging Brain The Aging Brain R. Scott Turner, MD, PhD Director, Memory Disorders Program Professor, Department of Neurology Georgetown University Washington, DC memory.georgetown.edu rst36@georgetown.edu
The Aging Brain The Aging Brain R. Scott Turner, MD, PhD Director, Memory Disorders Program Professor, Department of Neurology Georgetown University Washington, DC memory.georgetown.edu rst36@georgetown.edu
DIFFERENTIAL DIAGNOSIS OF NEUROCOGNITIVE DISORDERS
 DIFFERENTIAL DIAGNOSIS OF NEUROCOGNITIVE DISORDERS Maria D. Llorente MD Associate Chief of Staff, Mental Health Washington DC VA Medical Center Professor of Psychiatry, Georgetown University School of
DIFFERENTIAL DIAGNOSIS OF NEUROCOGNITIVE DISORDERS Maria D. Llorente MD Associate Chief of Staff, Mental Health Washington DC VA Medical Center Professor of Psychiatry, Georgetown University School of
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Neuropathology of Neurodegenerative Disorders Prof. Jillian Kril
 Neurodegenerative disorders to be discussed Alzheimer s disease Lewy body diseases Frontotemporal dementia and other tauopathies Huntington s disease Motor Neuron Disease 2 Neuropathology of neurodegeneration
Neurodegenerative disorders to be discussed Alzheimer s disease Lewy body diseases Frontotemporal dementia and other tauopathies Huntington s disease Motor Neuron Disease 2 Neuropathology of neurodegeneration
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status. Case 1 4/7/11. Which of the following evaluations is your next step?
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Introduction, use of imaging and current guidelines. John O Brien Professor of Old Age Psychiatry University of Cambridge
 Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Alzheimer s Disease - Dementia
 - Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
- Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
DEMENTIA. Szabolcs Szatmári. Tg. Mureş Marosvásárhely Romania 4/18/ :59 AM
 DEMENTIA Szabolcs Szatmári Tg. Mureş Marosvásárhely Romania Dementia from Latin de- "apart, away" + mens (genitive mentis) "mind" MORE GRAY HAIR AND LESS GRAY MATTER Daryl R. Gress Cognitive decline
DEMENTIA Szabolcs Szatmári Tg. Mureş Marosvásárhely Romania Dementia from Latin de- "apart, away" + mens (genitive mentis) "mind" MORE GRAY HAIR AND LESS GRAY MATTER Daryl R. Gress Cognitive decline
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
212 Index C-SB-13,
 Index A Acetylcholinesterase inhibitor, treatment, 15 Age-associated memory impairment (AAMI), 5 Alzheimer s disease (AD), 40, 95 96 apolipoprotein E genotype and risk for, 58 cellular neurodegeneration
Index A Acetylcholinesterase inhibitor, treatment, 15 Age-associated memory impairment (AAMI), 5 Alzheimer s disease (AD), 40, 95 96 apolipoprotein E genotype and risk for, 58 cellular neurodegeneration
Dr Roger Cable NHS Dumfries and Galloway
 Dr Roger Cable NHS Dumfries and Galloway Young Onset Dementia Statistics What is dementia Diagnosing dementia History Examination Tests Subtypes of dementia 315000 Cost of dementia (Alzheimer s society)
Dr Roger Cable NHS Dumfries and Galloway Young Onset Dementia Statistics What is dementia Diagnosing dementia History Examination Tests Subtypes of dementia 315000 Cost of dementia (Alzheimer s society)
Fact Sheet Alzheimer s disease
 What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
Clinical Genetics & Dementia
 Clinical Genetics & Dementia Dr Nayana Lahiri Consultant in Clinical Genetics & Honorary Senior Lecturer Nayana.lahiri@nhs.net Aims of the Session To appreciate the potential utility of family history
Clinical Genetics & Dementia Dr Nayana Lahiri Consultant in Clinical Genetics & Honorary Senior Lecturer Nayana.lahiri@nhs.net Aims of the Session To appreciate the potential utility of family history
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
RECOGNITION AND MANAGEMENT OF DEMENTIA IN THE ACUTE CARE SETTING
 RECOGNITION AND MANAGEMENT OF DEMENTIA IN THE ACUTE CARE SETTING Alex Hishaw, MD Department of Neurology University of Arizona Objectives: Recognize the impact of history and presentation on the diagnosis
RECOGNITION AND MANAGEMENT OF DEMENTIA IN THE ACUTE CARE SETTING Alex Hishaw, MD Department of Neurology University of Arizona Objectives: Recognize the impact of history and presentation on the diagnosis
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer
 The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
Dementia. Dr Maria Foundas Consultant Physician. Training support Skills development Competency Assessment Scholarships Education
 Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
Roger E. Kelley, M.D. Professor and Chairman Department of Neurology Tulane University School of Medicine New Orleans, Louisiana
 Roger E. Kelley, M.D. Professor and Chairman Department of Neurology Tulane University School of Medicine New Orleans, Louisiana FINANCIAL DISCLOSURE No potential conflict of interest to disclose. OBJECTIVES
Roger E. Kelley, M.D. Professor and Chairman Department of Neurology Tulane University School of Medicine New Orleans, Louisiana FINANCIAL DISCLOSURE No potential conflict of interest to disclose. OBJECTIVES
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
FDG-PET e parkinsonismi
 Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Dementia: The Role of Neuropsychology and Finding the Right Diagnosis
 Dementia: The Role of Neuropsychology and Finding the Right Diagnosis Robert E. Cohen, PsyD Director - Department of Neuropsychology Orlando Health Memory Disorder Clinic OBJECTIVES: Discuss the role of
Dementia: The Role of Neuropsychology and Finding the Right Diagnosis Robert E. Cohen, PsyD Director - Department of Neuropsychology Orlando Health Memory Disorder Clinic OBJECTIVES: Discuss the role of
Caring Sheet #13: Frontotemporal Dementia:
 CARING SHEETS: Caring Sheet #13: Frontotemporal Dementia: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet
CARING SHEETS: Caring Sheet #13: Frontotemporal Dementia: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet
Diagnosis before NIA AA The impact of FDG PET in. Diagnosis after NIA AA Neuropathology and PET image 2015/10/16
 The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
Objectives. RAIN Difficult Diagnosis 2014: A 75 year old woman with falls. Case History: First visit. Case History: First Visit
 Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
ALZHEIMER S DISEASE FACTOIDS & STATISTICS
 ALZHEIMER S DISEASE FACTOIDS & STATISTICS ~ 4 million affected in US alone 6-8% if 65+ years old, 30-50% if 80+ By 2030, in US >65 million people >65+ (---> ~14 million with AD) AD is one of the top 10
ALZHEIMER S DISEASE FACTOIDS & STATISTICS ~ 4 million affected in US alone 6-8% if 65+ years old, 30-50% if 80+ By 2030, in US >65 million people >65+ (---> ~14 million with AD) AD is one of the top 10
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Diagnosis and management of Dementia
 Diagnosis and management of Dementia Dr. Jahnavi Kedare Associate Professor Dept. of Psychiatry, T. N. Medical College B. Y. L. Nair Hospital, Mumbai Prevalence of Dementia Lower than developed countries
Diagnosis and management of Dementia Dr. Jahnavi Kedare Associate Professor Dept. of Psychiatry, T. N. Medical College B. Y. L. Nair Hospital, Mumbai Prevalence of Dementia Lower than developed countries
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss
 Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss Incidence of Common Neurological Diseases Incidence New Cases Disease (per 100,000) (per
Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss Incidence of Common Neurological Diseases Incidence New Cases Disease (per 100,000) (per
Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases
 Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases Keith A. Josephs, MD, MST, MSc Professor of Neurology 13th Annual Mild Cognitive Impairment (MCI) Symposium: Alzheimer and Non-Alzheimer
Role of TDP-43 in Non-Alzheimer s and Alzheimer s Neurodegenerative Diseases Keith A. Josephs, MD, MST, MSc Professor of Neurology 13th Annual Mild Cognitive Impairment (MCI) Symposium: Alzheimer and Non-Alzheimer
Clinicopathologic and genetic aspects of hippocampal sclerosis. Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA
 Clinicopathologic and genetic aspects of hippocampal sclerosis Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA The hippocampus in health & disease A major structure of the medial temporal
Clinicopathologic and genetic aspects of hippocampal sclerosis Dennis W. Dickson, MD Mayo Clinic, Jacksonville, Florida USA The hippocampus in health & disease A major structure of the medial temporal
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre
 Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre Today Introduction to CT Introduction to MRI Introduction to nuclear medicine Imaging the dementias The Brain ~ 1.5
Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre Today Introduction to CT Introduction to MRI Introduction to nuclear medicine Imaging the dementias The Brain ~ 1.5
Delirium, Dementia, and Amnestic Disorders. Dr.Al-Azzam 1
 Delirium, Dementia, and Amnestic Disorders Dr.Al-Azzam 1 Introduction Disorders in which a clinically significant deficit in cognition or memory exists The number of people with these disorders is growing
Delirium, Dementia, and Amnestic Disorders Dr.Al-Azzam 1 Introduction Disorders in which a clinically significant deficit in cognition or memory exists The number of people with these disorders is growing
DEMENTIA ANDREA BERG, MD
 DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
Chapter 94 Delirium and Dementia Episode Overview
 Chapter 94 Delirium and Dementia Episode Overview Core questions: 1. List the four key diagnostic criteria for delirium. 2. List six strong predisposing or precipitating factors for delirium. 3. List 15
Chapter 94 Delirium and Dementia Episode Overview Core questions: 1. List the four key diagnostic criteria for delirium. 2. List six strong predisposing or precipitating factors for delirium. 3. List 15
review of existing studies on ASL in dementia Marion Smits, MD PhD
 review of existing studies on ASL in dementia Marion Smits, MD PhD Associate Professor of Neuroradiology Department of Radiology, Erasmus MC, Rotterdam (NL) Alzheimer Centre South-West Netherlands, Rotterdam
review of existing studies on ASL in dementia Marion Smits, MD PhD Associate Professor of Neuroradiology Department of Radiology, Erasmus MC, Rotterdam (NL) Alzheimer Centre South-West Netherlands, Rotterdam
The Spectrum of Lewy Body Disease: Dementia with Lewy Bodies and Parkinson's Disease Dementia
 Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Objectives. Objectives continued: 3/24/2012. Copyright Do not distribute or replicate without permission 1
 Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
DEMENTIA 9/29/16. Introduction. Introduction. Signs and Symptom. Epidemiology. Dementia. Dr. Yotin Chinvarun M.D. Ph.D.
 Introduction DEMENTIA Dr. Yotin Chinvarun M.D. Ph.D. Neurology, Pramongkutklao hospital In 1901 Auguste Deter, a woman in her early 50s, became 1 st person diagnosed with Alzheimer's disease, a form of
Introduction DEMENTIA Dr. Yotin Chinvarun M.D. Ph.D. Neurology, Pramongkutklao hospital In 1901 Auguste Deter, a woman in her early 50s, became 1 st person diagnosed with Alzheimer's disease, a form of
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Neuroimaging for dementia diagnosis. Guidance from the London Dementia Clinical Network
 Neuroimaging for dementia diagnosis Guidance from the London Dementia Clinical Network Authors Dr Stephen Orleans-Foli Consultant Psychiatrist, West London Mental Health NHS Trust Dr Jeremy Isaacs Consultant
Neuroimaging for dementia diagnosis Guidance from the London Dementia Clinical Network Authors Dr Stephen Orleans-Foli Consultant Psychiatrist, West London Mental Health NHS Trust Dr Jeremy Isaacs Consultant
10 Facts We All Need to Know About Dementia (MNCD) in Old Age
 in Old Age") 10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
Dementia. Team Members: Abdulaziz Alsalem, Khalid Al-Qahtani, Dania Alkelabi, Sarah Alshamrani
 Dementia Objectives: differentiate delirium from dementia differentiate Mild Cognitive Impairment from Dementia become familiar with common dementia syndromes, and available treatments Team Members: Abdulaziz
Dementia Objectives: differentiate delirium from dementia differentiate Mild Cognitive Impairment from Dementia become familiar with common dementia syndromes, and available treatments Team Members: Abdulaziz
brain MRI for neuropsychiatrists: what do you need to know
 brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
Brain imaging for the diagnosis of people with suspected dementia
 Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Dementia and Delirium:
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive
CASE 49. What type of memory is available for conscious retrieval? Which part of the brain stores semantic (factual) memories?
 memories?") CASE 49 A 43-year-old woman is brought to her primary care physician by her family because of concerns about her forgetfulness. The patient has a history of Down syndrome but no other medical problems.
CASE 49 A 43-year-old woman is brought to her primary care physician by her family because of concerns about her forgetfulness. The patient has a history of Down syndrome but no other medical problems.
New life Collage of nursing Karachi
 New life Collage of nursing Karachi Presenter: Zafar ali shah Faculty: Raja khatri Subject: Pathophysiology Topic :Alzheimer s Disease Post RN BScN semester 2 nd Objective Define Alzheimer s Describe pathophysiology
New life Collage of nursing Karachi Presenter: Zafar ali shah Faculty: Raja khatri Subject: Pathophysiology Topic :Alzheimer s Disease Post RN BScN semester 2 nd Objective Define Alzheimer s Describe pathophysiology
2016 Programs & Information
 Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Update on functional brain imaging in Movement Disorders
 Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
DEMENTIA IN PARKINSON`S DISEASE. DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD
 Director-Parkinson`s Disease Service for the Older Person HNELHD") DEMENTIA IN PARKINSON`S DISEASE DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD DEMENTIA IN PD The concept of Non Motor Symptoms in PD Dementia in Parkinson`s
DEMENTIA IN PARKINSON`S DISEASE DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD DEMENTIA IN PD The concept of Non Motor Symptoms in PD Dementia in Parkinson`s
Moving Targets: An Update on Diagnosing Dementia in the Clinic
 Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures