5/7/2013. Patrick Nolan, DO, FACE
|
|
|
- Alexina Margaret Pearson
- 5 years ago
- Views:
Transcription
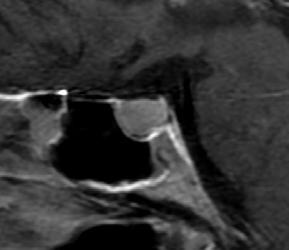
1 Patrick Nolan, DO, FACE Patient: T.W. 83 year old male 9/18/2012 AM sudden onset of Vertigo ER visit Had MRI, some labs Home on Zofran and medicines Complete resolution of sx after 2 days MRI chronic sinus inflammation mm pituitary lesion R above sella solid mass R cavernous sinus extension, up to diaphragm on R No hemorrhage Some infundibulum deviation to L Referral made No physical signs of Cushings, Acromegaly or Hypopituitarism No sx of D.I. Poor erectile competence for years Lab ACTH 40 (0 46 pg/ml) Cortisol 10.9 ( mg/dl) Free T ( mg/dl) TSH 3.94 ( uiv/ml) Testosterone 142 ( ng/dl) Prolactin ( ng/ml) IgF 1 59 ( ng/ml) GH 0.02 ( ng/ml) VS Stable BP 138/78 both arms Pulse 80 Wt 222# Height approx 6 1 Visual Field grossly nl Testes normal 1

2 Rx Cabergoline 0.5mg po twice weekly No further C/O Felt well No new symptoms Follow up MRI Dec 17, 2012 Pituitary mass now 10 mm x 9 mm and noticeably smaller with less supra sellar extension. Patient had no symptoms. Lab Dec 13, 2012 Prolactin 14.7 Testosterone 150 Normal chemistry Normal TFT s Rx Cabergoline 0.5mg weekly Testosterone gel to be titrated F/U in 4 6 months 2
3 3


4 44 year old male referred by Urology with low Testosterone No complaints by either him or his wife Teddy Bear syndrome Did everything his wife ever wanted of him. No libido or sexual desire whatsoever No erections in > 8 years No sexual attempts Fathered child 14 years previously 4
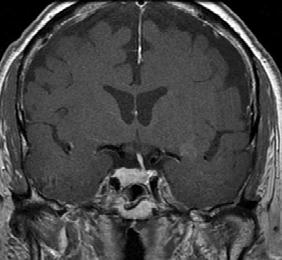
5 Exam Very pale ( pituitary pallor ) BP 100/64; HR 50 Regular; Wt 168#; Ht 5 11 Standing BP 90/50; HR 50 Regular No palp thyroid. Mild gynecomastia. Testes small bilat, normal genitalia otherwise Lab Panhypopituitary CMP nl CBC mild normocytic anemia LH/FSH not measurable Testosterone not measurable ACTH < 2 Cortisol < 2 mcg/dl Free T 4 < 0.2 ( ng/dl) TSH < 0.01 IgF 1 < 25 Prolactin 490 ng/ml Dilute > 40,000 ng/ml even to last dilution DX Severe panhypopituitarism Macro adenoma prolactinoma MRI Very large pituitary mass Above (surrounding) optic chiasm Invades bilateral cavernous sinuses and surrounds both carotids No field cuts! 5
 Return libido and sexual function Testosterone 600 s Tapered")
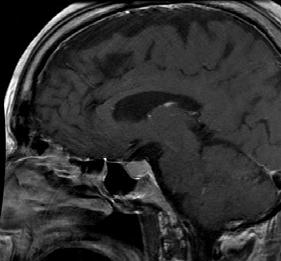
6 Plans High dose Cabergoline po Counseling psychologist regarding anticipated hyper sexual response Other hormones, LT 4, Cortisone po Watched for DI on Cortisone Follow Up: 3 months MRI > 60% reduction size No need for surgery Wife is malpractice threat divorce Prolactin diluted 46 Normal spontaneous erections ( unbelievable ) Return libido and sexual function Testosterone 600 s Tapered off all med except Cabergoline Moved to Michigan with girlfriend TSH, Free T 4 nl CMP, CBC nl Testes nl Genitalia nl 6
7 38 year old male C/O fatigue, muscle weakness, sleepiness, huge appetite, lack of NRG, weight gain No definite medical history Family History Obesity, Hypertension, Type II Diabetes/Metabolic Syndrome Patient wants to take his health seriously Can t figure out what is wrong Habits 3 meals/day, no meds Probably 4 6,000 calories/day Minimal activity Minimal erections, not sustained Desires sex, but cannot function Wife unhappy, Children (x2) not happy, Dog not happy Exam Obese male wt 296#, ht 5 11 Referral by LMD low testosterone 196 AM 222 AM Normal Prolactin Normal LH/FSH Mild elevation 24 Urine Cortisol TSH, Free T 4 nl CMP, CBC nl Testes nl, Genitalia nl 7

8 Plan Counseled him and wife Weight loss support group Serious wt loss effort Intense, no tolerance diet & exercising Trial for 3 months No TOLERANCE for mistakes No Excuses Should do sleep study Follow Up: 4 months 25# wt loss, approx 87,500 calorie debt Improving clinically More NRG + function Testosterone 390 Plan Same Serious lifestyle changes 8
9 26 year old male ER Visit Shoulder injury Xray Normal 14 Y/O shoulder MD thought it strange Radiologist thought it interesting LMD referral to Endocrine for GH deficiency Ht 6 3 Wt 180# Poor muscle mass Testes tiny small penis 6cm Never had erection No libido/girlfriend Introvert personality Testosterone < 25 LH/FSH 65/80 Thyroid/Pituitary fx all nl Karyotype 47 XXY Dx Klinefelter s Syndrome 9

10 Elected to start testosterone replacement Not insured elected to self administer depo testosterone q 2 wks IM Patrick Nolan, D.O., F.A.C.E. 10

 There is no well established benefit")
11 Review: Physiology Pathology Physical Exam Laboratory Measurements Therapeutic Options Areas of Uncertainty There is no general agreement on the acceptable normal range of testosterone John J McGill, M.D. (Review, Cleveland Clinic Journal of Medicine, November 2012) There is no well established benefit of testosterone administration in normal aging males (Committee of Institute of Medicine, 2004) 11
12 Somatic: gynecomastia, decreased body hair, anemia, muscle loss, fatigue, bone loss, hot flashes. Psychological: depressed mood, impaired cognition/memory/energy, irritability. Sexual: decreased libido, ED Changes in normal aging men are similar to hypogonadism Peter Snyder, MD (Up To Date 2013) Testes Size (4 7cm normal) Are testes descended? Gynecomastia Body hair Loss of body hair Muscle mass Scalp hair recession Arm span greater than height Anosmia Signs of chronic illness (poor nutrition, alcoholism, liver disease, chronic renal failure, RA) 12
13 Primary Hypogonadism Karyotype abnormality (e.g. Klinefelter syndrome) Toxin exposure (chemotherapy) Congenital defect Orchitis Testicular trauma or infarction Hemochromatosis Medications (e.g. ketoconazole) Increased temperature of testicular environment Secondary Hypogonadism Kallmann syndrome Gonadotropin releasing hormone (GnRH) receptor mutation or deficiency Genetic mutation associated with pituitary hormone deficiency Obesity, insulin resistance Type 2 Diabetes Obstructive sleep apnea Aging Hemochromatosis Secondary Hypogonadism Estrogen excess Anabolic steroid abuse Anorexia nervosa Acute illness Human immunodeficiency virus infection Chronic medical conditions Alcohol abuse Severe primary hypothyroidism 13
14 Secondary Hypogonadism Sellar mass of infiltrative lesion Metastatic lesion Trauma (head injury) Radiation exposure Surgery Stalk severance Pituitary apoplexy Semen Analysis 15 million/cc (40 million total) 40% motile is normal. Consider repeating 2 4 times for full assessment. Testosterone: June December orders (Providence Lab) June December orders (Providence Lab) Providence Lab Total Testosterone: $140 LH: $108 FSH: $86 Mayo Clinic Bioavailable Testosterone: $177 Free Testosterone: $135 Prolactin: $99 Jil Jefson, Providence Lab 14
15 Physicians in the U.S. = 700,000 Accidental deaths caused by physicians per year = 120,000 Accidental deaths per physician is Statistics courtesy of U.S. Dept of Health & Human Services Gun owners in the U.S. = 80,000,000 (Yes, that s 80 million!) Accidental gun deaths per year (all age groups) =1,500 Accidental deaths per gun owner is Statistics courtesy of FBI Statistically, doctors are approximately 9,000 times more dangerous than gun owners. Remember, Guns don t kill people, doctors do. Not everyone has a gun, but almost everyone has at least one doctor. This means you are over 9,000 times more likely to be killed by a doctor than a gun owner. 15
16 Please alert your friends to this alarming threat. We must ban doctors before this gets completely out of hand! Out of concern for the public at large, we withheld the statistics on lawyers for fear the shock would cause people to panic and seek medical attention! 50 66% drop in testosterone with age (20 y.o. 80 y.o.) 30% drop during day (8am 8pm) Do not measure during hospitalization or acute illness (low T may be a marker of poor health?) UpToDate
17 Statistics remember regression toward the mean. Testosterone repeat twice if low at 8am Free testosterone (calculated from T, SHBG, albumin formula varies) Bioavailable testosterone(not precipitated by ammomium sulfate) Gold Standard equilibrium dialysis Bioavailable or free testosterone if suspect low SHBG: obesity, cirrhosis, advanced age, nephrosis, endocrinopathy (diabetes, hypothyroidism, corticosteroid use, acromegaly) Or if suspect elevated SHBG: weight loss, hyperthyroidism, estrogen LH, FSH T 4, TSH Prolactin Fe/TIBC 17
18 Low or normal LH with Testosterone below 150 Increased prolactin Headache, visual loss Low T 4 with low/normal TSH Do not measure testosterone: Acute illness/hospitalization Severe obesity with fatigue Evaluate and treat sleep apnea first If Exclude treatable condition (disorder of thyroid, prolactin, corticosteroid, iron, pituitary lesion, sleep apnea) If Symptoms are present If (2) 8am tests are less than ng/dl (consider age: or 15 20% below cut point) Do CBC at baseline (rule out erythrocytosis) Discuss prostate, cardiovascular, sleep apnea risks, and transmission risks of topical preps. Oral preparations are not used because of liver toxicity, tumors. Parenteral (IM $24/month for 100mg/week) (50 100mg IM q week (300mg q 3 weeks) Transdermal ($ /month, average dose) Common usage liquid (Axiron) 2 4 actuations per day in axilla 18
19 Gel (Androgel) 1% 2.5 5g packets one per day (4 pumps/day) Other: Androderm, testoderm, testopatch patches, testim, fortesta gels Also available: Subcutaneous pellets (testopel) pellets per 3 6 months (requires surgery, up to 12% extrusion) Buccal (gum, STRIANT) bid; 16% gum irritation At initiation Acne, gynecomastia, aggressiveness, closure of epiphyses Increased BPH symptoms Increased sleep apnea Erythrocytosis (measure CBC at baseline and after 3 6 months of therapy, especially with IM forms) Skin rashes (patches) Transmission (gels, rare), cardiovascular events higher in some studies meta analysis of 51 randomized trials: No increase prostate cancer, need for prostate biopsy, urinary symptoms compared to placebo. No benefit when testosterone added to PDE5 inhibitors in patients with low testosterone levels Long term effects not yet evaluated (WHI like study has not yet been performed Weight lifting as effective testosterone in HIV population in increasing muscle strength 19
20 20
Hypogonadism 4/27/2018. Male Hypogonadism -- Definition. Epidemiology. Objectives HYPOGONADISM. Men with Hypogonadism. 95% untreated.
 Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Testosterone Therapy in Men with Hypogonadism
 Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Recognizing and Managing Testosterone Deficiency
 Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Testosterone Treatment: Myths Vs Reality. Fadi Al-Khayer, M.D, F.A.C.E
 Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients
 Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
6/14/2010. GnRH=Gonadotropin-Releasing Hormone.
 Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
GUIDELINES ON. Introduction. G.R. Dohle, S. Arver, C. Bettocchi, S. Kliesch, M. Punab, W. de Ronde
 GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
Mechanism of hyperprolactinemia
 Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
ANDROGEN DEFICIENCY Update on Evaluation and Management
 ANDROGEN DEFICIENCY Update on Evaluation and Management Kristen Gill Hairston, MD, MPH Associate Professor of Internal Medicine Section of Endocrinology and Metabolism Wake Forest University School of
ANDROGEN DEFICIENCY Update on Evaluation and Management Kristen Gill Hairston, MD, MPH Associate Professor of Internal Medicine Section of Endocrinology and Metabolism Wake Forest University School of
Androgen deficiency. Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital
 Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
GUIDELINES ON MALE HYPOGONADISM
 GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Androderm patch, AndroGel packets and pump, Axiron solution, First- Testosterone, First-Testosterone MC, Fortesta gel, Testim gel, Vogelxo
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
More than meets the eye
 More than meets the eye Ana Paula Abreu, MD, PhD American Association of Clinical Endocrinologists New England Chapter Annual Meeting September 8, 2018 Disclosures No conflict of interest or significant
More than meets the eye Ana Paula Abreu, MD, PhD American Association of Clinical Endocrinologists New England Chapter Annual Meeting September 8, 2018 Disclosures No conflict of interest or significant
GA KS KY LA MD NJ NV NY TN TX WA Applicable X X N/A N/A X N/A X X X X X X N/A N/A NA *FHK- Florida Healthy Kids. Androgens
 Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
OVERVIEW OF PRESENTATION
 Thanh D. Hoang, DO, FACP, FACE Division of Endocrinology Department of Internal Medicine WRNMMC 13 Aug 2018 OVERVIEW OF PRESENTATION Take Home Points Definition of Hypogonadism Clinical Manifestations
Thanh D. Hoang, DO, FACP, FACE Division of Endocrinology Department of Internal Medicine WRNMMC 13 Aug 2018 OVERVIEW OF PRESENTATION Take Home Points Definition of Hypogonadism Clinical Manifestations
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male
: female / male") 1. Patient personal details Institute code: Physician code: Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male 2. Changes in acromegaly-specific medical
1. Patient personal details Institute code: Physician code: Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male 2. Changes in acromegaly-specific medical
Laboratory Investigation of Male Gonadal Function. Dr N Oosthuizen Dept of Chemical Pathology UP 2010
 Laboratory Investigation of Male Gonadal Function Dr N Oosthuizen Dept of Chemical Pathology UP 2010 1 Figure 1. Hypothalamic-pituitary pituitary-testicular testicular axis 2 Testosterone (T) measurement
Laboratory Investigation of Male Gonadal Function Dr N Oosthuizen Dept of Chemical Pathology UP 2010 1 Figure 1. Hypothalamic-pituitary pituitary-testicular testicular axis 2 Testosterone (T) measurement
Androgens. Medication Strengths Quantity Limit Comments Androderm (testosterone patch) 1% pump 2 pump bottles per Non-Preferred
 1% pump 2 pump bottles per Non-Preferred") Market DC Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Androderm (testosterone patch) AndroGel (testosterone
Market DC Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Androderm (testosterone patch) AndroGel (testosterone
Imaging pituitary gland tumors
 November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY
 JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution?
 Case Reports in Radiology Volume 2015, Article ID 268974, 5 pages http://dx.doi.org/10.1155/2015/268974 Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution? Devon
Case Reports in Radiology Volume 2015, Article ID 268974, 5 pages http://dx.doi.org/10.1155/2015/268974 Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution? Devon
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
TESTOSTERONE DEFINITION
 DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
43 year old man with low libido. Katie Stanley, MD August 16, 2012
 43 year old man with low libido Katie Stanley, MD August 16, 2012 HPI 43 yo M with history of heroin addiction on methadone maintenance Reported low libido to PCP PCP checked testosterone and found to
43 year old man with low libido Katie Stanley, MD August 16, 2012 HPI 43 yo M with history of heroin addiction on methadone maintenance Reported low libido to PCP PCP checked testosterone and found to
14 Girl with Cushing s Disease: An Update. Kristen Dillard, MD Endorama October 17, 2013
 14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE
 Authoriser: Moya O Doherty Page 1 of 7 BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE The purpose of this protocol is to describe common tests used for the investigation
Authoriser: Moya O Doherty Page 1 of 7 BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE The purpose of this protocol is to describe common tests used for the investigation
Hypogonadism and Testosterone Replacement Therapy: Pharmacist
 Hypogonadism and Testosterone Replacement Therapy: Practical Insights for the Pharmacist Roger G. Hefflinger, PharmD Associate Professor of Pharmacy Practice and Administrative Services Idaho State University,
Hypogonadism and Testosterone Replacement Therapy: Practical Insights for the Pharmacist Roger G. Hefflinger, PharmD Associate Professor of Pharmacy Practice and Administrative Services Idaho State University,
Male Hypogonadism. Types and causes of hypogonadism. What is male hypogonadism? Symptoms. Testosterone production. Patient Information.
 Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN
 International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:
![Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:](/thumbs/75/72057018.jpg "Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:") Clinical Policy: (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date: 07.25.17 Last Review Date: 11.17 Line of Business: Commercial Coding Implications Revision Log See Important Reminder
Clinical Policy: (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date: 07.25.17 Last Review Date: 11.17 Line of Business: Commercial Coding Implications Revision Log See Important Reminder
panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013
 panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013 PITUITARY GLAND (HYPOPHYSIS CEREBRI) The master of endocrine glands master of endocrine glands It is a small oval
panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013 PITUITARY GLAND (HYPOPHYSIS CEREBRI) The master of endocrine glands master of endocrine glands It is a small oval
GLMS CME- Cell Group 5 10 April Greenlane Medical Specialists Pui-Ling Chan Endocrinologist
 GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
Late onset hypogonadism
 Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Pituitary for the General Practitioner. Marilyn Lee Consultant physician and endocrinologist
 Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
62-year-old woman with severe headache. Celeste Thomas November 1, 2012
 62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
NANOS Patient Brochure
 NANOS Patient Brochure Pituitary Tumor Copyright 2015. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
NANOS Patient Brochure Pituitary Tumor Copyright 2015. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
What we will cover. Evaluation of the Child with Suspected Pituitary Disease. ituitary
 Evaluation of the Child with Suspected Pituitary Disease Craig Alter, MD University of Pennsylvania Children s Hospital of Philadelphia What we will cover * What laboratory tests to order * MRI: common
Evaluation of the Child with Suspected Pituitary Disease Craig Alter, MD University of Pennsylvania Children s Hospital of Philadelphia What we will cover * What laboratory tests to order * MRI: common
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly
 Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly Dr. Peter Igaz MD PhD DSc 2nd Department of Medicine Semmelweis University Fields of Endocrinology Diseases
Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly Dr. Peter Igaz MD PhD DSc 2nd Department of Medicine Semmelweis University Fields of Endocrinology Diseases
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology
 Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction
 Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction Mohammad Talha Rauf, MD Internal Medicine Resident PGY3 Dania AbuShanab, MD Julie Samantray,
Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction Mohammad Talha Rauf, MD Internal Medicine Resident PGY3 Dania AbuShanab, MD Julie Samantray,
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel ANDROID (methyltestosterone) oral capsule ANDROXY (fluoxymesterone) oral tablet AXIRON transdermal
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel ANDROID (methyltestosterone) oral capsule ANDROXY (fluoxymesterone) oral tablet AXIRON transdermal
Clinical evaluation of infertility
 Clinical evaluation of infertility DR. FARIBA KHANIPOUYANI OBSTETRICIAN & GYNECOLOGIST PRENATOLOGIST Definition: inability to achieve conception despite one year of frequent unprotected intercourse. Male
Clinical evaluation of infertility DR. FARIBA KHANIPOUYANI OBSTETRICIAN & GYNECOLOGIST PRENATOLOGIST Definition: inability to achieve conception despite one year of frequent unprotected intercourse. Male
UW MEDICINE PATIENT EDUCATION. Acromegaly Symptoms and treatments. What is acromegaly? DRAFT. What are the symptoms? How is it diagnosed?
 UW MEDICINE PATIENT EDUCATION Acromegaly Symptoms and treatments This handout explains a health condition called acromegaly. It describes tests that are used to diagnose the condition and gives basic instructions
UW MEDICINE PATIENT EDUCATION Acromegaly Symptoms and treatments This handout explains a health condition called acromegaly. It describes tests that are used to diagnose the condition and gives basic instructions
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on the Approach to Pediatric Anemia and Pallor. These podcasts are designed to give medical students an overview of key
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on the Approach to Pediatric Anemia and Pallor. These podcasts are designed to give medical students an overview of key
Managing Testosterone Deficiency: A Practical Guide. John Grantmyre MD Professor of Urology Dalhousie University
 Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA
 Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015
 66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015 HPI 66 M presenting as a referral for erectile dysfunction and abnormal labs Has been seeing a facility specializing in
66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015 HPI 66 M presenting as a referral for erectile dysfunction and abnormal labs Has been seeing a facility specializing in
A dro r gen e R e R p e lac a e c m e e m n e t t T her e a r p a y Androgen Replacement Therapy in the Aging O j b ecti t ve v s Male
 Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Reproductive Health and Pituitary Disease
 Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Functional Pituitary Adenomas. Fawn M. Wolf, MD 2/2/2018
 Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Consent for Testosterone Therapy-Men Revised 4/10/18
 Consent for Testosterone Therapy in Men You have been diagnosed with or have an increased risk of having a hormone deficiency and your provider has recommended treatment with bio-identical hormone replacement
Consent for Testosterone Therapy in Men You have been diagnosed with or have an increased risk of having a hormone deficiency and your provider has recommended treatment with bio-identical hormone replacement
15 month-old female with a cystic brain lesion. Magdalena Dumin, MD Pediatric Endocrinology Fellow University of Chicago December 4, 2014
 + 15 month-old female with a cystic brain lesion Magdalena Dumin, MD Pediatric Endocrinology Fellow University of Chicago December 4, 2014 + Chief Complaint 15 month-old female admitted to PICU for concern
+ 15 month-old female with a cystic brain lesion Magdalena Dumin, MD Pediatric Endocrinology Fellow University of Chicago December 4, 2014 + Chief Complaint 15 month-old female admitted to PICU for concern
Growth hormone therapy in a girl with Turner syndrome showing a large increase over the initially predicted ht of 4 5
 Disorders of Growth and Puberty: How to Recognize the Normal Variants vs Patients Who Need to be Evaluated Paul Kaplowitz, M.D Pediatric Endocrinology. VCU School of Medicine Interpretation of Growth Charts
Disorders of Growth and Puberty: How to Recognize the Normal Variants vs Patients Who Need to be Evaluated Paul Kaplowitz, M.D Pediatric Endocrinology. VCU School of Medicine Interpretation of Growth Charts
Male History, Clinical Examination and Testing
 Male History, Clinical Examination and Testing Dirk Vanderschueren, MD, PhD Case Jan is 29 years old and consults for 1 year primary subfertility partner 28 years old and normal gynaecological investigation
Male History, Clinical Examination and Testing Dirk Vanderschueren, MD, PhD Case Jan is 29 years old and consults for 1 year primary subfertility partner 28 years old and normal gynaecological investigation
Dr John Quin. Royal Sussex County Hospital, Brighton. BHIVA AUTUMN CONFERENCE 2013 Including CHIVA Parallel Sessions. None
 BHIVA AUTUMN CONFERENCE 2013 Including CHIVA Parallel Sessions Dr John Quin Royal Sussex County Hospital, Brighton COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Dr John Quin None
BHIVA AUTUMN CONFERENCE 2013 Including CHIVA Parallel Sessions Dr John Quin Royal Sussex County Hospital, Brighton COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Dr John Quin None
Late onset Hypogonadism. Dr KhooSay Chuan Department of Urology Penang General Hospital
 Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
Pathology of pituitary gland. By: Shifaa Qa qa
 Pathology of pituitary gland By: Shifaa Qa qa Sella turcica Adenohypophysis (80%): - epithelial cells - acidophil, basophil, chromophobe - Somatotrophs, Mammosomatotrophs, Corticotrophs, Thyrotrophs, Gonadotrophs
Pathology of pituitary gland By: Shifaa Qa qa Sella turcica Adenohypophysis (80%): - epithelial cells - acidophil, basophil, chromophobe - Somatotrophs, Mammosomatotrophs, Corticotrophs, Thyrotrophs, Gonadotrophs
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Men Getting Older Will Testosterone Keep Him Young?
 Men Getting Older Will Testosterone Keep Him Young? Alvin M. Matsumoto, M.D. Associate Director, GRECC V.A. Puget Sound Health Care System Professor, Department of Medicine Division of Gerontology and
Men Getting Older Will Testosterone Keep Him Young? Alvin M. Matsumoto, M.D. Associate Director, GRECC V.A. Puget Sound Health Care System Professor, Department of Medicine Division of Gerontology and
Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline
 CLINICAL PRACTICE GUIDELINE Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline Shalender Bhasin, 1 Juan P. Brito, 2 Glenn R. Cunningham, 3 Frances J. Hayes,
CLINICAL PRACTICE GUIDELINE Testosterone Therapy in Men With Hypogonadism: An Endocrine Society* Clinical Practice Guideline Shalender Bhasin, 1 Juan P. Brito, 2 Glenn R. Cunningham, 3 Frances J. Hayes,
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY)
") HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
Challenging Pituitary Cases. Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine
 Challenging Pituitary Cases Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine 1 34 yo male has incidental finding of large macroadenoma, with prolactin
Challenging Pituitary Cases Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine 1 34 yo male has incidental finding of large macroadenoma, with prolactin
Testosterone Therapy in Men with Androgen Deficiency Syndromes: An Endocrine Society Clinical Practice Guideline
 SPECIAL FEATURE Clinical Practice Guideline Testosterone Therapy in Men with Androgen Deficiency Syndromes: An Endocrine Society Clinical Practice Guideline Shalender Bhasin, Glenn R. Cunningham, Frances
SPECIAL FEATURE Clinical Practice Guideline Testosterone Therapy in Men with Androgen Deficiency Syndromes: An Endocrine Society Clinical Practice Guideline Shalender Bhasin, Glenn R. Cunningham, Frances
Pituitary Apoplexy. Updated: April 22, 2018 CLINICAL RECOGNITION
 Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
TEST REPORT # SB. Patient Name: Comprehensive Male Profile I Patient Phone Number: TEST NAME RESULTS 08/12/18 RANGE
 TEST REPORT Ordering Provider: David Getuwell, MD 8605 SW Creekside Place Beaverton, OR 97008 Phone: 503-466-2445 Fax: 503-466-1636 Samples Received 08/15/2018 Report Date 08/20/2018 Samples Collected
TEST REPORT Ordering Provider: David Getuwell, MD 8605 SW Creekside Place Beaverton, OR 97008 Phone: 503-466-2445 Fax: 503-466-1636 Samples Received 08/15/2018 Report Date 08/20/2018 Samples Collected
Pituitary Disease Resident Tutorial 2017
 Pituitary Disease Resident Tutorial 2017 Sarat Sunthornyothin MD Division of Endocrinology and Metabolism King Chulalongkorn Memorial Hospital Pituitary Anatomy hypophyseal portal system direct arterial
Pituitary Disease Resident Tutorial 2017 Sarat Sunthornyothin MD Division of Endocrinology and Metabolism King Chulalongkorn Memorial Hospital Pituitary Anatomy hypophyseal portal system direct arterial
Didactic Series. Hypogonadism and HIV. Daniel Lee, MD UCSD Medical Center, Owen Clinic July 28, 2016
 Didactic Series Hypogonadism and HIV Daniel Lee, MD UCSD Medical Center, Owen Clinic July 28, 2016 This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department
Didactic Series Hypogonadism and HIV Daniel Lee, MD UCSD Medical Center, Owen Clinic July 28, 2016 This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department
ROLE OF HORMONAL ASSAY IN DIAGNOSING PCOD DR GAANA SREENIVAS (JSS,MYSURU)
") ROLE OF HORMONAL ASSAY IN DIAGNOSING PCOD DR GAANA SREENIVAS (JSS,MYSURU) In 1935, Stein and Leventhal described 7 women with bilateral enlarged PCO, amenorrhea or irregular menses, infertility and masculinizing
ROLE OF HORMONAL ASSAY IN DIAGNOSING PCOD DR GAANA SREENIVAS (JSS,MYSURU) In 1935, Stein and Leventhal described 7 women with bilateral enlarged PCO, amenorrhea or irregular menses, infertility and masculinizing
Hormone Balance - Female Report SAMPLE. result graph based on Luteal Phase. result graph based on Luteal Phase
 Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Therapeutic Use Exemptions
 APPENDIX I Therapeutic Use Exemptions The NFL recognizes that within the list of prohibited substances there are medications that are appropriate for the treatment of specific medical conditions. For athletes
APPENDIX I Therapeutic Use Exemptions The NFL recognizes that within the list of prohibited substances there are medications that are appropriate for the treatment of specific medical conditions. For athletes
PATIENT INFORMATION HYPOPITUITARISM YOUR QUESTIONS ANSWERED
 PATIENT INFORMATION HYPOPITUITARISM YOUR QUESTIONS ANSWERED Contents What is hypopituitarism? 1 What causes hypopituitarism? 2 What are the symptoms and signs of hypopituitarism? 4 How is hypopituitarism
PATIENT INFORMATION HYPOPITUITARISM YOUR QUESTIONS ANSWERED Contents What is hypopituitarism? 1 What causes hypopituitarism? 2 What are the symptoms and signs of hypopituitarism? 4 How is hypopituitarism
Why is my body not changing? Conflicts of interest. Overview 11/9/2015. None
 Why is my body not changing? Murthy Korada Pediatrician, Pediatric Endocrinologist Ridge Meadows Hospital Surrey Memorial Hospital None Conflicts of interest Overview Overview of normal pubertal timing
Why is my body not changing? Murthy Korada Pediatrician, Pediatric Endocrinologist Ridge Meadows Hospital Surrey Memorial Hospital None Conflicts of interest Overview Overview of normal pubertal timing
CYSTIC PROLACTINOMA: A SURGICAL DISEASE?
 AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
Testosterone Injection / Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Testosterone Injection / Implant Page: 1 of 9 Last Review Date: December 5, 2014 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Testosterone Injection / Implant Page: 1 of 9 Last Review Date: December 5, 2014 Testosterone
, David Stultz, MD. Erectile Dysfunction. David Stultz, MD September 10, 2001
 Erectile Dysfunction David Stultz, MD September 10, 2001 Case Presentation A 66 year old male presents to your office requesting Viagra. He states that for the past year he has had difficulty forming
Erectile Dysfunction David Stultz, MD September 10, 2001 Case Presentation A 66 year old male presents to your office requesting Viagra. He states that for the past year he has had difficulty forming
Point-Counterpoint: Late Onset Hypogonadism (LOH)
") Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary Tumor Apoplexy
 Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 817603, 4 pages http://dx.doi.org/10.1155/2013/817603 Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary
Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 817603, 4 pages http://dx.doi.org/10.1155/2013/817603 Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary
Testosterone Therapy in Men An update
 Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
47 Year-Old Female with Headache. Olesya Krivospitskaya, MD Second year endocrinology fellow
 47 Year-Old Female with Headache Olesya Krivospitskaya, MD Second year endocrinology fellow HPI: 47 y.o. female presented to ER with c/o acute onset of headache at the vertex of her head and retro-orbital
47 Year-Old Female with Headache Olesya Krivospitskaya, MD Second year endocrinology fellow HPI: 47 y.o. female presented to ER with c/o acute onset of headache at the vertex of her head and retro-orbital
Pituitary Stalk Interruption Syndrome. Leena Shahla, MD, PGY5 Endocrinology, Diabetes and Metabolism Fellowship University of Massachusetts
 Pituitary Stalk Interruption Syndrome Leena Shahla, MD, PGY5 Endocrinology, Diabetes and Metabolism Fellowship University of Massachusetts 11/12/2016 Case: NP, 42 year old female, from Dominican Republic.
Pituitary Stalk Interruption Syndrome Leena Shahla, MD, PGY5 Endocrinology, Diabetes and Metabolism Fellowship University of Massachusetts 11/12/2016 Case: NP, 42 year old female, from Dominican Republic.
FAILURE IS NOT AN OPTION HOPE IS NOT A PLAN
 FAILURE IS NOT AN OPTION HOPE IS NOT A PLAN Doctors' Secrets What Men Want - Testosterone - Sharing the Secrets of Men s Health Donald M. McLeod M.D. and Philip A White M.D. CONTENTS SECTION I Introduction
FAILURE IS NOT AN OPTION HOPE IS NOT A PLAN Doctors' Secrets What Men Want - Testosterone - Sharing the Secrets of Men s Health Donald M. McLeod M.D. and Philip A White M.D. CONTENTS SECTION I Introduction
Table of Contents. What Is Hypopituitarism? What Causes Hypopituitarism? What It Means to You... 4
 Hypopituitarism Table of Contents What Is Hypopituitarism?... 2 What Causes Hypopituitarism?... 4 What It Means to You... 4 I. Thyroid-Stimulating Hormone (TSH) Deficiency... 4 II. Adrenocorticotrophic
Hypopituitarism Table of Contents What Is Hypopituitarism?... 2 What Causes Hypopituitarism?... 4 What It Means to You... 4 I. Thyroid-Stimulating Hormone (TSH) Deficiency... 4 II. Adrenocorticotrophic
Hormone Replacement Therapy
 Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
What Is the Low T Syndrome? Is Testosterone Supplementation Safe?
 What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone
Assessment and management of male androgen disorders: an update
 Irene Chan Mark Ng Tang Fui Jeffrey D Zajac Mathis Grossmann Assessment and management of male androgen disorders: an update Background Male hypogonadism, caused by intrinsic pathology of the hypothalamic
Irene Chan Mark Ng Tang Fui Jeffrey D Zajac Mathis Grossmann Assessment and management of male androgen disorders: an update Background Male hypogonadism, caused by intrinsic pathology of the hypothalamic
Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君
 Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君 Williams text book of endocrinology 11 th e Anterior pituitary hormone 10-20% of pituitary cells, increase to 40% during AP PRL releasing factors: TRH, oxytocin,
Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君 Williams text book of endocrinology 11 th e Anterior pituitary hormone 10-20% of pituitary cells, increase to 40% during AP PRL releasing factors: TRH, oxytocin,
Prior Authorization Criteria Update: Androgens, Topical and Parenteral
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
HYPOTHALAMO PITUITARY GONADAL AXIS
 HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
Male Hypogonadism. More than just a low testosterone? KM Pantalone Endocrinology
 Male Hypogonadism More than just a low testosterone? KM Pantalone Endocrinology Conflicts of Interest None to declare Case 1 A 54 year old man is referred for evaluation of low testosterone The patient
Male Hypogonadism More than just a low testosterone? KM Pantalone Endocrinology Conflicts of Interest None to declare Case 1 A 54 year old man is referred for evaluation of low testosterone The patient
Endocrine Update Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh
 Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
ANDROGEN DEFICIENCY A GUIDE TO MALE HORMONES A BOOKLET IN THE SERIES OF CONSUMER GUIDES ON MALE REPRODUCTIVE HEALTH FROM
 ANDROGEN DEFICIENCY A GUIDE TO MALE HORMONES A BOOKLET IN THE SERIES OF CONSUMER GUIDES ON MALE REPRODUCTIVE HEALTH FROM First published in July 2003 by Andrology Australia 5th Edition, December 2015 Copyright
ANDROGEN DEFICIENCY A GUIDE TO MALE HORMONES A BOOKLET IN THE SERIES OF CONSUMER GUIDES ON MALE REPRODUCTIVE HEALTH FROM First published in July 2003 by Andrology Australia 5th Edition, December 2015 Copyright