Sleep-Disordered Breathing and Risk of Sudden Death in Multiple System Atrophy
|
|
|
- Simon Russell
- 5 years ago
- Views:
Transcription
1 Sleep-Disordered Breathing and Risk of Sudden Death in Multiple System Atrophy Lisa Cutchen MD Sleep Medicine Fellow University of New Mexico Sleep Disorders Center New Mexico Thoracic Society February 27, 2016
2 Objectives 1. Describe the three clinical syndromes known as multiple system atrophy. 2. Recognize the clinical features of multiple system atrophy. 3. Understand the management strategies for sleep-disordered breathing in patients with multiple system atrophy.
3 Case Study 54-year-old woman presents to her primary care physician and reports a disturbing noise that she makes during sleep with inspiration. Her husband reports that it began a year ago, but has become worse since then, now continuous throughout the night. The noise is described as a strange, high-pitched sound like the bray of a donkey. Her husband also describes episodes during sleep in which she has sudden violent movements which seem to be dream enactments. She has also had urinary frequency and urgency, although testing has not revealed a urinary tract infection. She recently fell on a walk with her husband which she attributed to clumsiness.
4 Multiple System Atrophy A fatal adult-onset neurodegenerative disorder characterized by autonomic failure, parkinsonism, cerebellar abnormalities, and corticospinal degeneration The pathological process in the brain affects the central autonomic, striatonigral, and olivopontocerebellar systems
5 Multiple System Atrophy Estimated annual incidence in population >50 years old is approximately 3 per 100,000 Estimated annual prevalence is between 2 to 5 cases per 100,000 Mean age of onset 54 years (range 31-78) Men = Women
6 Multiple System Atrophy There are three syndromes that are captured by the term Multiple System Atrophy Striatonigral degeneration Olivopontocerebellar atrophy Shy-Drager Syndrome
7 Multiple System Atrophy There are three syndromes that are captured by the term Multiple System Atrophy MSA-P Striatonigral degeneration MSA-C Olivopontocerebellar atrophy Shy-Drager syndrome Shy-Drager syndrome
8 Multiple System Atrophy There are three syndromes that are captured by the term Multiple System Atrophy MSA-P predominant parkinsonism MSA-C predominant cerebellar ataxia Shy-Drager syndrome Predominant autonomic failure
9 MSA Clinical Features The neuropathologic changes probably begin several years before the disease becomes symptomatic The onset of the disease is marked by the initial clinical manifestation of one of its characteristic features, motor or autonomic
10 Multiple System Atrophy Clinical Features Parkinsonism Bradykinesia Resting tremor Rigidity Postural instability Gait changes Cerebellar Ataxia Gait ataxia Ataxic dysarthria Limb ataxia Sustained gaze-evoked nystagmus
11 Multiple System Atrophy Clinical Features Autonomic Dysfunction Orthostatic hypotension Light-headedness, altered vision, nausea, weakness, fatigue, and coat-hanger distribution pain only while standing Bowel and bladder disturbances Urinary urgency, frequency, and incontinence not due to a non-neurological cause Sexual dysfunction Erectile dysfunction
12 Multiple System Atrophy The initial motor symptom determines the morphological phenotype in an individual case MSA-P predominant parkinsonism MSA-C predominant cerebellar ataxia Shy-Drager syndrome Predominant autonomic failure
13 MSA Clinical Features MSA P: The predominant motor feature is parkisonism MSA C: The predominant motor feature is cerebellar ataxia MSA-P outnumbers MSA-C by between 2 and 4 to one in Europe and North America MSA-C more common in Japan
14 Kollensperger M, Geser F, Ndayisaba J, et al. Presentation, diagnosis, and management of multiple system atrophy in Europe: final analysis of the European multiple system atrophy registry, Movement Disorders 2010;25(15): Multiple System Atrophy Neuropsychiatric Features and Sleep Disturbance Depression 41% Psychotic symptoms 6% Hallucinations 5.5% Delusions 2% Dementia 4.5% Psychotic symptoms MSA-P > MSA-C Insomnia 19% Excessive daytime sleepiness 17% Restless legs 10%
15 Multiple System Atrophy Sleep Symptoms in MSA Obstructive sleep apnea, with upper airway obstruction mainly at the level of the larynx Laryngeal stridor Central hypoventilation Reduced and fragmented sleep Excessive daytime sleepiness Periodic limb movements and restless legs syndrome REM sleep behavior disorder
16 Neuropathology of Multiple System Atrophy (MSA) MSA is one of the alpha-synucleinopathies alpha-synuclein Microscopically, glial cytoplasmic inclusions of aggregates of misfolded alpha-synuclein Macroscopically, cerebellar atrophy or pronounced pallor of the substantia nigra The underlying neuropathology contributes to the sleep disorders associated with MSA Abbott SM, Videnovic A. Sleep disorders in atypical parkinsonism, Movement disorders clinical practice 2014;1(2): Jellinger KA. Neuropathology of multiple system atrophy: new thoughts about pathogenesis, Movement Disorders 2014;29(14):
17 Alpha-Synucleinopathies Multiple System Atrophy Parkinson Disease Lewy Body Dementia
18 Respiratory Manifestations of Multiple System Atrophy MSA affects the brainstem areas involved in respiratory rhythmogenesis, chemosensitivity, and control of laryngeal function Brainstem areas controlling ventilation Dorsolateral pons Nucleus of the solitary tract Ventrolateral medulla Benarroch EE. Brainstem respiratory control: substrates of respiratory failure of multiple system atrophy, Movement Disorders 2007;22(2):
19 Respiratory Manifestations of Multiple System Atrophy Brainstem areas controlling ventilation Dorsolateral pons Nucleus of the solitary tract Ventrolateral medulla The neurons in these areas are involved in Respiratory rhythm Respiratory reflexes Control of cranial neurons that drive the muscles of the upper respiratory airway Control of spinal neurons that drive the muscles of the respiratory pump Benarroch EE. Brainstem respiratory control: substrates of respiratory failure of multiple system atrophy, Movement Disorders 2007;22(2):
20 Respiratory Manifestations of Multiple System Atrophy In addition, there are neurons near the ventral medulla that are responsive to CO 2 /ph, hypoxia, or both Drive automatic respiration, especially during sleep Benarroch EE. Brainstem respiratory control: substrates of respiratory failure of multiple system atrophy, Movement Disorders 2007;22(2):

21 Respiratory Manifestations of Multiple System Atrophy α-synuclein depositions cause neurodegeneration in multiple areas: Substantia nigra Cerebellum Pontine and medullary nuclei Spinal cord Benarroch EE. Brainstem respiratory control: substrates of respiratory failure of multiple system atrophy, Movement Disorders 2007;22(2):
22 Respiratory Manifestations of Multiple System Atrophy Respiratory Rhythm Generated in the pre-botzinger complex Respiratory Chemosensitivity Carotid bodies (mainly oxygen sensitive) Rostral ventrolateral medulla (hypoxia-activated) The main chemosensitive role of the brainstem depends on neurons sensitive to ph (CO 2 /H + ) Benarroch EE. Brainstem respiratory control: substrates of respiratory failure of multiple system atrophy, Movement Disorders 2007;22(2):
23 Respiratory Manifestations of Multiple System Atrophy Laryngeal muscles are innervated by vagal motoneurons located in the nucleus ambiguus Posterior cricoarytenoid muscle activated during inspiration causes laryngeal abduction Thyroarytenoid muscle activated during expiration causes laryngeal adduction Benarroch EE. Brainstem respiratory control: substrates of respiratory failure of multiple system atrophy, Movement Disorders 2007;22(2):
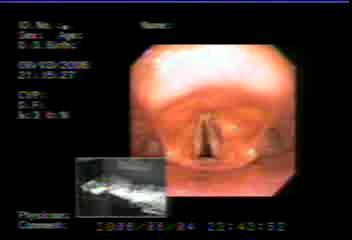
24 Laryngeal Dysfunction
25 Laryngeal Stridor in MSA Paralysis of abductor vocal cord muscles Sustained tonic activity of adductor vocal cord muscles Laryngoscopic evaluation during wakefulness may not show laryngeal narrowing in these patients Selective denervation atrophy of the posterior cricoarytenoid muscle possible Impaired laryngeal function alone may not account for the high incidence of sudden death in MSA patients Benarroch EE. Brainstem respiratory control: substrates of respiratory failure of multiple system atrophy, Movement Disorders 2007;22(2):
26 Sleep and MSA Leading cause of death in MSA Bronchopneumonia (48%) Bulbar palsy predisposes patients to aspiration pneumonia Sudden death (21%) Laryngeal obstruction Central hypoventilation with a blunted CO 2 response curve resulting in hypercapnic respiratory failure Cardiac arrhythmia related to dysautonomia Silber MH, Levine S. Stridor and death in multiple system atrophy. Movement Disorders, 2000;15(4):
27 Predictors of Survival in MSA Retrospective research study published 2015 All cases of MSA evaluated at Mayo Clinic, Rochester, between January 1998 and December 2012 Individuals excluded if there was secondary cause of parkinsonism or ataxia or if clinical or laboratory features suggested alternative diagnosis to MSA 685 patients identified 594 probable MSA 91 possible MSA Coon EA, Sletten DM, Suarez MD, et al. Clinical features and autonomic testing predict survival in multiple system atrophy, Brain 2015:138:
28 Predictors of Survival in MSA Patient Demographics 685 total 330 (48%) female vs. 355 (52%) male MSA-P 430 patients (63%) MSA-P: 203 (47%) female vs. 227 (52%) male MSA-C 255 patients (37%) MSA-C: 127 (50%) female vs. 128 (50%) male Mean age of onset 61 years (range years) MSA-C earlier at 58.4 years vs. MSA-P at 62.3 years Median time from onset of symptoms to initial evaluation at Mayo was 3.07 years Median time from onset of symptoms to death was 7.51 years Median time from diagnosis to death was 3.33 years Coon EA, Sletten DM, Suarez MD, et al. Clinical features and autonomic testing predict survival in multiple system atrophy, Brain 2015:138:
29 Predictors of Survival in MSA No difference in survival between motor subtypes There was symptom overlap of parkinsonism and ataxia, although parkinsonism was more likely to occur in MSA-C than was ataxia to occur in MSA- P. No difference in survival between MSA-P and MSA-C Either from time of symptom onset or time of diagnosis Sleep symptoms of dream enactment and stridor were similar between MSA-P and MSA-C Of 304 patients with reported dream enactment behavior, it preceded onset Coon of EA, motor Sletten DM, Suarez and MD, autonomic et al. Clinical features and autonomic testing predict survival in symptoms in 34% multiple system atrophy, Brain 2015:138:
30 Predictors of Survival in MSA Factors Not Associated with Survival MSA subtype (adjusted for age of onset) Classification as probable vs. possible MSA Gender Coon EA, Sletten DM, Suarez MD, et al. Clinical features and autonomic testing predict survival in multiple system atrophy, Brain 2015:138:
31 Predictors of Survival in MSA Factors associated with shortened survival included Later age at onset Early autonomic symptoms The presence of bladder symptoms Early need for urinary catheterization Early falls (considered a motor symptom) Stridor Severity of autonomic dysfunction Coon EA, Sletten DM, Suarez MD, et al. Clinical features and autonomic testing predict survival in multiple system atrophy, Brain 2015:138:
32 Predictors of Survival in MSA Six variables were maintained in the final model as independent predictors of shortened survival The strongest predictor was falls occurring within 3 years of symptom onset Four of the other five independent predictors related to autonomic symptoms or degree of autonomic impairment Stridor was not maintained as an independent predictor, possibly due to significant associations between stridor and several other predictors Coon EA, Sletten DM, Suarez MD, et al. Clinical features and autonomic testing predict survival in multiple system atrophy, Brain 2015:138:
33 Predictors of Survival in MSA Did recognition of stridor during evaluation for MSA prompt treatment that may have affected survival? In earlier studies, stridor was shown to be a good prognostic indicator of survival. Silber MH, Levine S. Stridor and death in multiple system atrophy, Movement Disorders, 2000;15(4):

34 Predictors of Survival in MSA Coon EA, Sletten DM, Suarez MD, et al. Clinical features and autonomic testing predict survival in multiple system atrophy, Brain 2015:138:
35 Predictors of Survival in MSA Retrospective research study published in autopsy-confirmed cases at the Mayo Clinic, Rochester 16 women, 33 men Mean age of onset 56.1 years Symptoms at onset 50% autonomic 30% parkinsonism 20% cerebellar Figueroa JJ, Singer W, Parsaik A, et al. Multiple system atrophy: prognostic indicators of survival, Movement Disorders
36 Predictors of Survival in MSA Prognostic indicators for shorter survival were Older age at onset (hazard ratio 1.04, P = 0.03) Early requirement of bladder catheterization (hazard ratio 7.9, P = 0.004) 7 vs. 9.8 years Early generalized (CASS 6) autonomic failure (hazard ratio 2.8, P = 0.047) 7.3 vs years
37 Composite Autonomic Severity Score (CASS) A validated instrument for laboratory quantitation of autonomic failure derived from the Autonomic Reflex Screen and Thermoregulatory Sweat Testing. 1 to 3, mild and limited 4 to 6, moderate 7 to 10, severe and generalized
38 Composite Autonomic Severity Score (CASS) Autonomic Reflex Screen The Quantitative Sudomotor Axon Reflex Test at proximal and distant standard sites to assess sympathetic postganglionic sudomotor axon function Heart rate responses to deep breathing and the Valsalva maneuver to assess cardiovagal function Beat-to-beat blood pressure responses to the Valsalva maneuver and head-up tilt to assess sympathetic adrenergic function
39 Composite Autonomic Severity Score (CASS) Thermoregulatory Sweat Testing (TST) Assesses the integrity of central and peripheral sudomotor pathways involved in the thermoregulatory response to changes in environmental temperature by providing quantitative evaluation of the proportion of anterior body surface that does not sweat. A TST of 40% or greater indicates moderate to severe anhidrosis and a TST of 100% indicates complete anhidrosis.
40 Predictors of Survival in MSA The medullary serotonergic neurons modulate the micturition reflex and are central respiratory chemosensors that participate in the regulation of arousal, respiratory rhythmogenesis, and ventilatory response to hypoxemia and hypercarbia. They are also involved in sympathetically mediated thermoregulation. Figueroa JJ, Singer W, Parsaik A, et al. Multiple system atrophy: prognostic indicators of survival, Movement Disorders
41 Treatment of Stridor and Laryngeal Dysfunction Direct laryngoscopy during sleep without pharmacologic sedation documented inspiratory adduction of the vocal cords with downward displacement of the larynx Application of CPAP resulted in improvement in stridor, distension of the hypopharynx, abduction of the vocal cords, and reduction of the downward displacement of the larynx Kuzniar TJ, Morgenthaler TI, Prakash U, et al. Effects of continuous positive airway pressure on stridor in multiple system atrophy sleep laryngoscopy, J Clin Sleep Med 2009;5(1):65-67.
42 Treatment of Stridor and Laryngeal Dysfunction Retrospective review of 38 patients seen at the Mayo Clinic, Rochester, from 1975 to 2010 who had MSA and had received otolaryngologic examination Mean age at diagnosis 68.0 years +/- 8.2 years Median age at diagnosis 67.3 years (range ) Median age at symptom onset 63.7 years (range ) Median age at diagnosis of true vocal fold impairment 66.2 years (range ) Lalich IJ, Ekbom DC, Starkman SJ, et al. Vocal fold motion impairment in multiple system atrophy, Laryngoscope 2014;124:
43 Treatment of Stridor and Laryngeal Dysfunction Median duration of vocal or respiratory symptoms (stridor, dysphonia, respiratory difficulty) prior to diagnosis of MSA was 12 months (range 1-60 months) Median duration of MSA symptoms prior to diagnosis of MSA was 36 months (range months) Stridor was present in 25 (68%) of the patients Lalich IJ, Ekbom DC, Starkman SJ, et al. Vocal fold motion impairment in multiple system atrophy, Laryngoscope 2014;124:
44 Treatment of Stridor and Laryngeal Dysfunction True vocal fold paralysis in 15 (39.5%) patients True vocal fold paresis in 21 (55.3%) patients True vocal fold mixed paresis/paralysis in 2 (5.3%) patients Included with the paralysis group for analysis Median survival after diagnosis with vocal fold motion impairment was 51.6 months Survival of those with stridor was not significantly different from those without stridor 24.9 months vs months, P = Lalich IJ, Ekbom DC, Starkman SJ, et al. Vocal fold motion impairment in multiple system atrophy, Laryngoscope 2014;124:
45 Treatment of Stridor and Laryngeal Dysfunction Decreased survival rate in patients with shorter duration of voice symptoms (stridor, dysphonia, respiratory difficulty) before the diagnosis of VFMI (P = ). Decreased survival rate in patients with shorter duration of any MSA-related symptom before MSA diagnosis (P = ). These associations likely related to symptom severity or disease velocity Lalich IJ, Ekbom DC, Starkman SJ, et al. Vocal fold motion impairment in multiple system atrophy, Laryngoscope
46 Treatment of Stridor and Laryngeal Dysfunction There was not a significant relationship between stridor and survival There was decreased survival associated with unilateral or bilateral vocal cord paralysis on laryngoscopy (P = ). Vocal fold motion impairment rather than stridor carries the implication of poor prognosis Lalich IJ, Ekbom DC, Starkman SJ, et al. Vocal fold motion impairment in multiple system atrophy, Laryngoscope 2014;124:
47 Treatment of Stridor and Laryngeal Dysfunction CPAP is effective therapy for eliminating stridor during sleep. Median survival time not significantly different between subjects without stridor and those with stridor treated with only CPAP. However, if the patient develops daytime stridor, and it is not treated with tracheostomy, then mean life expectancy is 0.8 years. Iranzo A, Santamaria J; Tolosa E, et al. Long-term effect of CPAP in the treatment of nocturnal stridor in multiple system atrophy, Neurology 2004;63(5): Silber MH, Levine S. Stridor and death in multiple
48 Treatment of Stridor and Laryngeal Dysfunction Besides CPAP and tracheostomy, there is surgery of the larynx a sampling: laryngofissure cord lateralization Cymetra injection bilateral type I thyroplasty carbon dioxide laser left transverse cordotomy partial arytenoidectomy and vocal fold lateralization This study too small to detect impact on survival of these airway interventions
49 Nocturnal Sudden Death in MSA Seems to be caused by a mechanism other than upper airway obstruction Even if treated with CPAP or tracheostomy, there is still risk of sudden death Tracheostomy has been known to make central sleep apnea worse Likely involves dysfunction of the respiratory regulation center
50 Recommended Reading Abbott SM, Videnovic A. Sleep disorders in atypical parkinsonism, Movement disorders clinical practice 2014;1(2): Benarroch EE. Brainstem respiratory control: substrates of respiratory failure of multiple system atrophy, Movement Disorders 2007;22(2): Iranzo A. Sleep and breathing in multiple system atrophy, Current Treatment Options in Neurology 2007;9: Kollensperger M, Geser F, Ndayisaba J, et al. Presentation, diagnosis, and management of multiple system atrophy in Europe: final analysis of the European multiple system atrophy registry, Movement Disorders 2010;25(15):
MSA. Sleep disorders MULTIPLE SYSTEM ATROPHY AND NOCTURNAL STRIDOR 1/26/2015. Alex Iranzo Neurology Service Hospital Clinic de Barcelona Spain
 MULTIPLE SYSTEM ATROPHY AND NOCTURNAL STRIDOR Alex Iranzo Neurology Service Hospital Clinic de Barcelona Spain MSA Neurodegenerative disease Parkinsonism, cerebellar, dysautonomia Mean survival is less
MULTIPLE SYSTEM ATROPHY AND NOCTURNAL STRIDOR Alex Iranzo Neurology Service Hospital Clinic de Barcelona Spain MSA Neurodegenerative disease Parkinsonism, cerebellar, dysautonomia Mean survival is less
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Drunk When You re Not A 67 year old male presents with feeling off balance
 Drunk When You re Not A 67 year old male presents with feeling off balance Kiera McElrone, DO Internal Medicine/Pediatrics Residency Maine Medical Center September 2017 ACP Bar Harbor Meeting Chief Complaint
Drunk When You re Not A 67 year old male presents with feeling off balance Kiera McElrone, DO Internal Medicine/Pediatrics Residency Maine Medical Center September 2017 ACP Bar Harbor Meeting Chief Complaint
Multiple System Atrophy
 Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute
 Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy
 Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Joint Session with ACOFP and Mayo Clinic. Parkinson's Disease: 5 Pearls. Jay Van Gerpen, MD
 Joint Session with ACOFP and Mayo Clinic Parkinson's Disease: 5 Pearls Jay Van Gerpen, MD Parkinson s Disease: 5 Pearls J.A. van Gerpen, MD Sections of Movement Disorders and Clinical Neurophysiology
Joint Session with ACOFP and Mayo Clinic Parkinson's Disease: 5 Pearls Jay Van Gerpen, MD Parkinson s Disease: 5 Pearls J.A. van Gerpen, MD Sections of Movement Disorders and Clinical Neurophysiology
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
M Nakajima, 1 H Kojima, 2 Y Takazawa, 3 N Yahagi, 4 K Harada, 1 K Takahashi, 1 K Unuma, 1 K Yoshida 1. Case report
 1 Department of Forensic Medicine, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan; 2 Tokyo Metropolitan Institute for Neuroscience, Tokyo, Japan; 3 Department of Pathology, Graduate
1 Department of Forensic Medicine, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan; 2 Tokyo Metropolitan Institute for Neuroscience, Tokyo, Japan; 3 Department of Pathology, Graduate
Functional Distinctions
 Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Comprehensive Approach to DLB Management
 Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
A guide to Multiple System Atrophy for: General Practitioners
 Introduction Prevalence Duration Initial presentation Red flags and symptoms Key management problems GP support The MSA Trust A guide to Multiple System Atrophy for: General Practitioners This document
Introduction Prevalence Duration Initial presentation Red flags and symptoms Key management problems GP support The MSA Trust A guide to Multiple System Atrophy for: General Practitioners This document
Autonomic Dysfunction
 Autonomic Dysfunction Unique anatomy PRE-GANGLIONIC POST-GANGLIONIC PRE-GANGLIONIC POST-GANGLIONIC Bradbury-Eggleston Postural hypotension with cardiovascular, GI, urogenital, thermoregulatory, sudomotor
Autonomic Dysfunction Unique anatomy PRE-GANGLIONIC POST-GANGLIONIC PRE-GANGLIONIC POST-GANGLIONIC Bradbury-Eggleston Postural hypotension with cardiovascular, GI, urogenital, thermoregulatory, sudomotor
Pietro Cortelli. IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna
 Pietro Cortelli IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna HYSTORY 1900 description of OPCA (Dejerine, Thomas) 1960 description of Shy-Drager
Pietro Cortelli IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna HYSTORY 1900 description of OPCA (Dejerine, Thomas) 1960 description of Shy-Drager
DISORDERS OF THE MOTOR SYSTEM. Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
CN V! touch! pain! Touch! P/T!
 CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
6/5/2017. Mellar P Davis MD FCCP FAAHPM Geisinger Medical Center Danville, PA
 Mellar P Davis MD FCCP FAAHPM Geisinger Medical Center Danville, PA Opioids adversely influence respiration in five distinct ways Opioids cause complex sleep disordered breathing consisting of central
Mellar P Davis MD FCCP FAAHPM Geisinger Medical Center Danville, PA Opioids adversely influence respiration in five distinct ways Opioids cause complex sleep disordered breathing consisting of central
Atypical parkinsonism
 Atypical parkinsonism Wassilios Meissner Service de neurologie et CMR atrophie multisystématisée, CHU de Bordeaux Institut des Maladies Neurodégénératives, Université Bordeaux 2, CNRS UMR 5293 Parkinsonism?
Atypical parkinsonism Wassilios Meissner Service de neurologie et CMR atrophie multisystématisée, CHU de Bordeaux Institut des Maladies Neurodégénératives, Université Bordeaux 2, CNRS UMR 5293 Parkinsonism?
Multiple choice questions: ANSWERS
 Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Circadian Variations Influential in Circulatory & Vascular Phenomena
 SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
MULTI SYSTEM ATROPHY: REPORT OF TWO CASES Dipu Bhuyan 1, Rohit Kr. Chandak 2, Pankaj Kr. Patel 3, Sushant Agarwal 4, Debjanee Phukan 5
 MULTI SYSTEM ATROPHY: REPORT OF TWO CASES Dipu Bhuyan 1, Rohit Kr. Chandak 2, Pankaj Kr. Patel 3, Sushant Agarwal 4, Debjanee Phukan 5 HOW TO CITE THIS ARTICLE: Dipu Bhuyan, Rohit Kr. Chandak, Pankaj Kr.
MULTI SYSTEM ATROPHY: REPORT OF TWO CASES Dipu Bhuyan 1, Rohit Kr. Chandak 2, Pankaj Kr. Patel 3, Sushant Agarwal 4, Debjanee Phukan 5 HOW TO CITE THIS ARTICLE: Dipu Bhuyan, Rohit Kr. Chandak, Pankaj Kr.
RESPIRATORY PROBLEMS IN MND RICHARD HARRISON MND RESPIRATORY ASSESSMENT SERVICE LUNG HEALTH UNIVERSITY HOSPITAL OF NORTH TEES
 RESPIRATORY PROBLEMS IN MND RICHARD HARRISON MND RESPIRATORY ASSESSMENT SERVICE LUNG HEALTH UNIVERSITY HOSPITAL OF NORTH TEES A TYPICAL HISTORY: NON BULBAR ONSET Difficulty walking Weak hands and arms
RESPIRATORY PROBLEMS IN MND RICHARD HARRISON MND RESPIRATORY ASSESSMENT SERVICE LUNG HEALTH UNIVERSITY HOSPITAL OF NORTH TEES A TYPICAL HISTORY: NON BULBAR ONSET Difficulty walking Weak hands and arms
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy
 By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy 1 By the end of the lecture, students will be able to : Distinguish the internal structure of the components of the brain stem in different levels and the specific
By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy 1 By the end of the lecture, students will be able to : Distinguish the internal structure of the components of the brain stem in different levels and the specific
Sleep Dysfunction in Multiple System Atrophy DR CALLUM DUPRE NEUROLOGY/SLEEP MEDICINE CAPITAL HEALTH SYSTEM
 Sleep Dysfunction in Multiple System Atrophy DR CALLUM DUPRE NEUROLOGY/SLEEP MEDICINE CAPITAL HEALTH SYSTEM Categories of Disturbance Sleep Breathing Disorders Parasomnias Sleepiness Insomnia Breathing?
Sleep Dysfunction in Multiple System Atrophy DR CALLUM DUPRE NEUROLOGY/SLEEP MEDICINE CAPITAL HEALTH SYSTEM Categories of Disturbance Sleep Breathing Disorders Parasomnias Sleepiness Insomnia Breathing?
Index SLEEP MEDICINE CLINICS. Note: Page numbers of article titles are in boldface type.
 299 SLEEP MEDICINE CLINICS Sleep Med Clin 1 (2006) 299 303 Note: Page numbers of article titles are in boldface type. A Acid reflux, sleep disturbances in older adults related to, 238 Aging, alterations
299 SLEEP MEDICINE CLINICS Sleep Med Clin 1 (2006) 299 303 Note: Page numbers of article titles are in boldface type. A Acid reflux, sleep disturbances in older adults related to, 238 Aging, alterations
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
:{ic0fp'16. Geriatric Medicine: Blood Pressure Monitoring in the Elderly. Terrie Ginsberg, DO, FACOI
 :{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
:{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
Non-Motor Symptoms of Parkinson s Disease
 Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease and other related movement disorders a video guide to diagnosis
 Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
Brainstem. Steven McLoon Department of Neuroscience University of Minnesota
 Brainstem Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Change in Lab Sequence Week of Oct 2 Lab 5 Week of Oct 9 Lab 4 2 Goal Today Know the regions of the brainstem. Know
Brainstem Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Change in Lab Sequence Week of Oct 2 Lab 5 Week of Oct 9 Lab 4 2 Goal Today Know the regions of the brainstem. Know
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
CONTROL OF MOVEMENT BY THE BRAIN A. PRIMARY MOTOR CORTEX:
 CONTROL OF MOVEMENT BY THE BRAIN A. PRIMARY MOTOR CORTEX: - responsible for - like somatosensory cortex, primary motor cortex show (motor homunculus) - amount of cortex devoted to different parts of body
CONTROL OF MOVEMENT BY THE BRAIN A. PRIMARY MOTOR CORTEX: - responsible for - like somatosensory cortex, primary motor cortex show (motor homunculus) - amount of cortex devoted to different parts of body
Index SLEEP MEDICINE CLINICS. Note: Page numbers of article titles are in boldface type. Cerebrospinal fluid analysis, for Kleine-Levin syndrome,
 165 SLEEP MEDICINE CLINICS Index Sleep Med Clin 1 (2006) 165 170 Note: Page numbers of article titles are in boldface type. A Academic performance, effects of sleepiness in children on, 112 Accidents,
165 SLEEP MEDICINE CLINICS Index Sleep Med Clin 1 (2006) 165 170 Note: Page numbers of article titles are in boldface type. A Academic performance, effects of sleepiness in children on, 112 Accidents,
A. PRIMARY MOTOR CORTEX: - responsible for - like somatosensory cortex, primary motor cortex show (motor homunculus) - amount of cortex devoted to
 - amount of cortex devoted to") CONTROL OF MOVEMENT BY THE BRAIN A. PRIMARY MOTOR CORTEX: - responsible for - like somatosensory cortex, primary motor cortex show (motor homunculus) - amount of cortex devoted to different parts of body
CONTROL OF MOVEMENT BY THE BRAIN A. PRIMARY MOTOR CORTEX: - responsible for - like somatosensory cortex, primary motor cortex show (motor homunculus) - amount of cortex devoted to different parts of body
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Accidents, risk of, with insufficient sleep, 318 Acquired immunodeficiency syndrome (AIDS), comorbid with narcolepsy, 298 299 Actigraphy, in
Note: Page numbers of article titles are in boldface type. A Accidents, risk of, with insufficient sleep, 318 Acquired immunodeficiency syndrome (AIDS), comorbid with narcolepsy, 298 299 Actigraphy, in
Multiple System Atrophy Manifested by Bilateral Vocal Cord Palsy as an Initial Sign
 Korean J Crit Care Med 2015 May 30(2):123-127 / ISSN 2383-4870 (Print) ㆍ ISSN 2383-4889 (Online) Case Report Multiple System Atrophy Manifested by Bilateral Vocal Cord Palsy as an Initial Sign Yuri Seo,
Korean J Crit Care Med 2015 May 30(2):123-127 / ISSN 2383-4870 (Print) ㆍ ISSN 2383-4889 (Online) Case Report Multiple System Atrophy Manifested by Bilateral Vocal Cord Palsy as an Initial Sign Yuri Seo,
BILATERAL ABDUCTOR VOCAL CORD PALSY. Dr NITYA G Final year PG KIMS
 BILATERAL ABDUCTOR VOCAL CORD PALSY Dr NITYA G Final year PG KIMS INTRODUCTION Vocal cord paralysis is a sign of a disease It results from dysfunction of Recurrent laryngeal nerves on both sides Paralysis
BILATERAL ABDUCTOR VOCAL CORD PALSY Dr NITYA G Final year PG KIMS INTRODUCTION Vocal cord paralysis is a sign of a disease It results from dysfunction of Recurrent laryngeal nerves on both sides Paralysis
Early Clinical Features of Parkinson s Disease and Related Disorders. Dr. Alastair Noyce
 1 Specialist Registrar in Neurology, London Deanery Parkinson s UK Doctoral Research Fellow Project lead for PREDICT-PD Declarations Salary: Parkinson's UK, Barts and the London NHS Trust Grants: Parkinson's
1 Specialist Registrar in Neurology, London Deanery Parkinson s UK Doctoral Research Fellow Project lead for PREDICT-PD Declarations Salary: Parkinson's UK, Barts and the London NHS Trust Grants: Parkinson's
Sleeping with PD. Jean Tsai, MD PhD September 27, 2014
 Sleeping with PD Jean Tsai, MD PhD September 27, 2014 Evaluation of sleep Assessment at least annually recommended by Agency for Healthcare Research and Quality (AHRQ) of the US Dept of Health and Human
Sleeping with PD Jean Tsai, MD PhD September 27, 2014 Evaluation of sleep Assessment at least annually recommended by Agency for Healthcare Research and Quality (AHRQ) of the US Dept of Health and Human
Mario Kinsella MD FAASM 10/5/2016
 Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Unit VIII Problem 4 Physiology lab: Brain Stem Lesions
 Unit VIII Problem 4 Physiology lab: Brain Stem Lesions - Motor and sensory somatotopy: Pre-central gyrus: is the motor area. Post-central gyrus: is the sensory area. Somatotopy: there is a map of thee
Unit VIII Problem 4 Physiology lab: Brain Stem Lesions - Motor and sensory somatotopy: Pre-central gyrus: is the motor area. Post-central gyrus: is the sensory area. Somatotopy: there is a map of thee
Parts of the motor circuits
 MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
Parkinson s Disease Initial Clinical and Diagnostic Evaluation. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Upper and Lower Motoneurons for the Head Objectives
 Upper and Lower Motoneurons for the Head Objectives Know the locations of cranial nerve motor nuclei Describe the effects of motor cranial nerve lesions Describe how the corticobulbar tract innervates
Upper and Lower Motoneurons for the Head Objectives Know the locations of cranial nerve motor nuclei Describe the effects of motor cranial nerve lesions Describe how the corticobulbar tract innervates
Premotor PD: autonomic failure
 Premotor PD: autonomic failure Division of Neurobiology Department of Neurology Medical University of Innsbruck Non-motor symptoms in PD Autonomic OH, constipation, impotence, urinary incontinence or retention,
Premotor PD: autonomic failure Division of Neurobiology Department of Neurology Medical University of Innsbruck Non-motor symptoms in PD Autonomic OH, constipation, impotence, urinary incontinence or retention,
1. The cerebellum coordinates fine movement through interactions with the following motor-associated areas:
 DENT/OBHS 131 2009 Take-home test 4 Week 6: Take-home test (2/11/09 close 2/18/09) 1. The cerebellum coordinates fine movement through interactions with the following motor-associated areas: Hypothalamus
DENT/OBHS 131 2009 Take-home test 4 Week 6: Take-home test (2/11/09 close 2/18/09) 1. The cerebellum coordinates fine movement through interactions with the following motor-associated areas: Hypothalamus
Cerebellum. Steven McLoon Department of Neuroscience University of Minnesota
 Cerebellum Steven McLoon Department of Neuroscience University of Minnesota 1 Anatomy of the Cerebellum The cerebellum has approximately half of all the neurons in the central nervous system. The cerebellum
Cerebellum Steven McLoon Department of Neuroscience University of Minnesota 1 Anatomy of the Cerebellum The cerebellum has approximately half of all the neurons in the central nervous system. The cerebellum
Reticular Formation George R. Leichnetz, Ph.D.
 Reticular Formation George R. Leichnetz, Ph.D. OBJECTIVES 1. To understand the anatomical and functional organization of the brainstem reticular formation into three general regions: median (raphe), medial
Reticular Formation George R. Leichnetz, Ph.D. OBJECTIVES 1. To understand the anatomical and functional organization of the brainstem reticular formation into three general regions: median (raphe), medial
Nsci 2100: Human Neuroanatomy 2017 Examination 3
 Name KEY Lab Section Nsci 2100: Human Neuroanatomy 2017 Examination 3 On this page, write your name and lab section. On your bubble answer sheet, enter your name (last name, space, first name), internet
Name KEY Lab Section Nsci 2100: Human Neuroanatomy 2017 Examination 3 On this page, write your name and lab section. On your bubble answer sheet, enter your name (last name, space, first name), internet
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
Vocal Fold Motion Impairment. Surgical options 10/17/2008. Voice Changes after Treatment for Bilateral Vocal Fold Motion Impairment
 Voice Changes after Treatment for Bilateral Vocal Fold Motion Impairment Betty S. Tsai, MD Mark S. Courey, MD Sarah L. Schneider, MS, CCC-SLP Soha Al-Jurf, MS, CCC-SLP UCSF Department of Otolaryngology
Voice Changes after Treatment for Bilateral Vocal Fold Motion Impairment Betty S. Tsai, MD Mark S. Courey, MD Sarah L. Schneider, MS, CCC-SLP Soha Al-Jurf, MS, CCC-SLP UCSF Department of Otolaryngology
What is SDB? Obstructive sleep apnea-hypopnea syndrome (OSAHS)
") Have a Good Sleep? Estimated 70 million Americans have clinically significant sleep problems Chronic insomnias report decreased quality of life, memory and attention problems, decreased physical health
Have a Good Sleep? Estimated 70 million Americans have clinically significant sleep problems Chronic insomnias report decreased quality of life, memory and attention problems, decreased physical health
Respiratory/Sleep Disorder Breathing (SDB) SDB is highly prevalent, under recognized, under reported and under treated
 SDB is highly prevalent, under recognized, under reported and under treated") Respiratory/Sleep Disorder Breathing (SDB) Definitions SDB is highly prevalent, under recognized, under reported and under treated Central 1. Central sleep apnea (CSA) is defined by the cessation of air
Respiratory/Sleep Disorder Breathing (SDB) Definitions SDB is highly prevalent, under recognized, under reported and under treated Central 1. Central sleep apnea (CSA) is defined by the cessation of air
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Assistant Professor of Neurology and Psychiatry University of Colorado Denver Goals 1) What are the most common non-motor
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Assistant Professor of Neurology and Psychiatry University of Colorado Denver Goals 1) What are the most common non-motor
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Unit VIII Problem 5 Physiology: Cerebellum
 Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
PARKINS ON CENTER. Parkinson s Disease: Diagnosis and Management. Learning Objectives: Recognition of PD OHSU. Disclosure Information
 OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Title. CitationCerebellum, 14(6): Issue Date Doc URL. Rights. Type. File Information. Author(s) Mitsuru; Sasaki, Hidenao
: Issue Date Doc URL. Rights. Type. File Information. Author(s) Mitsuru; Sasaki, Hidenao") Title Epidemiology of Multiple System Atrophy in Hokkaido, Sakushima, Ken; Nishimoto, Naoki; Nojima, Masanori; Author(s) Mitsuru; Sasaki, Hidenao CitationCerebellum, 14(6): 682-687 Issue Date 2015-12 Doc
Title Epidemiology of Multiple System Atrophy in Hokkaido, Sakushima, Ken; Nishimoto, Naoki; Nojima, Masanori; Author(s) Mitsuru; Sasaki, Hidenao CitationCerebellum, 14(6): 682-687 Issue Date 2015-12 Doc
Regulation of respiration
 Regulation of respiration Breathing is controlled by the central neuronal network to meet the metabolic demands of the body Neural regulation Chemical regulation Respiratory center Definition: A collection
Regulation of respiration Breathing is controlled by the central neuronal network to meet the metabolic demands of the body Neural regulation Chemical regulation Respiratory center Definition: A collection
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
MOTOR NEURONE DISEASE
 MOTOR NEURONE DISEASE Dr Arun Aggarwal Department of Rehabilitation Medicine, RPAH Department of Neurology, Concord Hospital. Motor Neurone Disease Umbrella term in UK and Australia (ALS in USA) Neurodegenerative
MOTOR NEURONE DISEASE Dr Arun Aggarwal Department of Rehabilitation Medicine, RPAH Department of Neurology, Concord Hospital. Motor Neurone Disease Umbrella term in UK and Australia (ALS in USA) Neurodegenerative
Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal:
 Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal: mainly from area 6 area 6 Premotorarea: uses external
Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal: mainly from area 6 area 6 Premotorarea: uses external
Sleep and Sleep Hygiene in an Occupational Health & Safety Context
 Sleep and Sleep Hygiene in an Occupational Health & Safety Context Glenn Legault Ph.D. Center for Research in Occupational Safety and Health, Laurentian University Nov. 12, 2014 Overview: Sleep what is
Sleep and Sleep Hygiene in an Occupational Health & Safety Context Glenn Legault Ph.D. Center for Research in Occupational Safety and Health, Laurentian University Nov. 12, 2014 Overview: Sleep what is
1.1. Parkinson disease
 1.TREMOR 1.1. Parkinson disease Parkinson Disease Progressive disorder: tremor, rigidity, and slowness of movements Neuronal loss of the substantia nigra Non motor features (dementia and dysautonomia),
1.TREMOR 1.1. Parkinson disease Parkinson Disease Progressive disorder: tremor, rigidity, and slowness of movements Neuronal loss of the substantia nigra Non motor features (dementia and dysautonomia),
Causes and Consequences of Respiratory Centre Depression and Hypoventilation
 Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Indications and Uses of Testing. Laboratory Testing of Autonomic Function. Generalized Autonomic Failure. Benign Disorders 12/30/2012.
 Indications and Uses of Testing Laboratory Testing of Autonomic Function Conditions of generalized autonomic failure Help define the degree of autonomic dysfunction and distinguish more benign from life
Indications and Uses of Testing Laboratory Testing of Autonomic Function Conditions of generalized autonomic failure Help define the degree of autonomic dysfunction and distinguish more benign from life
The Respiratory System
 Elaine N. Marieb Katja Hoehn Human Anatomy & Physiology SEVENTH EDITION C H A P T E R PowerPoint Lecture Slides prepared by Vince Austin, Bluegrass Technical and Community College 22P A R T B The Respiratory
Elaine N. Marieb Katja Hoehn Human Anatomy & Physiology SEVENTH EDITION C H A P T E R PowerPoint Lecture Slides prepared by Vince Austin, Bluegrass Technical and Community College 22P A R T B The Respiratory
Parkinson s Founda.on
 Parkinson s Founda.on PD ExpertBriefing: Sleep and Parkinson s Led By: Aleksandar Videnovic, M.D., M.Sc. Associate Professor of Neurology; Director, MGH Program on Sleep, Circadian Biology and NeurodegeneraDon
Parkinson s Founda.on PD ExpertBriefing: Sleep and Parkinson s Led By: Aleksandar Videnovic, M.D., M.Sc. Associate Professor of Neurology; Director, MGH Program on Sleep, Circadian Biology and NeurodegeneraDon
Autonomic Function Tests: Some Clinical Applications
 REVIEW J Clin Neurol 213;9:1-8 Print ISSN 1738-6586 / On-line ISSN 25-513 http://dx.doi.org/1.3988/jcn.213.9.1.1 Open Access Autonomic Function Tests: Some Clinical Applications Phillip A. Low, a Victoria
REVIEW J Clin Neurol 213;9:1-8 Print ISSN 1738-6586 / On-line ISSN 25-513 http://dx.doi.org/1.3988/jcn.213.9.1.1 Open Access Autonomic Function Tests: Some Clinical Applications Phillip A. Low, a Victoria
Sleep Medicine. Maintenance of Certification Examination Blueprint. Purpose of the exam
 Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Brainstem. By Dr. Bhushan R. Kavimandan
 Brainstem By Dr. Bhushan R. Kavimandan Development Ventricles in brainstem Mesencephalon cerebral aqueduct Metencephalon 4 th ventricle Mylencephalon 4 th ventricle Corpus callosum Posterior commissure
Brainstem By Dr. Bhushan R. Kavimandan Development Ventricles in brainstem Mesencephalon cerebral aqueduct Metencephalon 4 th ventricle Mylencephalon 4 th ventricle Corpus callosum Posterior commissure
Identification number: TÁMOP /1/A
 Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Sleep Disorders The Effect on our Lives Every Day
 Sleep Disorders The Effect on our Lives Every Day Julie Hatleli, RN Sheri Krenz, RN Regional Sleep Disorders Center-Mankato, MN 2016 MFMER slide-1 Agenda Sleep Stages Sleep Apnea Sleep Disorders DOT requirements
Sleep Disorders The Effect on our Lives Every Day Julie Hatleli, RN Sheri Krenz, RN Regional Sleep Disorders Center-Mankato, MN 2016 MFMER slide-1 Agenda Sleep Stages Sleep Apnea Sleep Disorders DOT requirements
Faculty of Clinical Forensic Medicine Committee 1/2018
 Guideline Subject: Clinical Forensic Assessment and Management of Non-Fatal Strangulation Approval Date: January 2018 Review Date: January 2021 Review By: Number: Faculty of Clinical Forensic Medicine
Guideline Subject: Clinical Forensic Assessment and Management of Non-Fatal Strangulation Approval Date: January 2018 Review Date: January 2021 Review By: Number: Faculty of Clinical Forensic Medicine
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
2. List seven functions performed by the respiratory system?
 The Respiratory System C23 Study Guide Tortora and Derrickson 1. In physiology we recognize that the word respiration has three meanings. What are the three different meanings of the word respiration as
The Respiratory System C23 Study Guide Tortora and Derrickson 1. In physiology we recognize that the word respiration has three meanings. What are the three different meanings of the word respiration as
I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts.
 Descending Tracts I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts. III: To define the upper and the lower motor neurons. 1. The corticonuclear
Descending Tracts I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts. III: To define the upper and the lower motor neurons. 1. The corticonuclear
GENERAL PRINCIPLES OF NEUROLOGY- John W. Day, M.D., Ph.D.
 I. TAKE HOME POINTS FOR THIS LECTURE A. Localizing the disease is the first step in diagnosing a neurological disorder. B. Time course of the disease (acute, subacute, or chronic) indicates the pathophysiological
I. TAKE HOME POINTS FOR THIS LECTURE A. Localizing the disease is the first step in diagnosing a neurological disorder. B. Time course of the disease (acute, subacute, or chronic) indicates the pathophysiological
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y
 Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
PD AND FALLS J U MALLYA FALLS AWARENESS MEETING
 PD AND FALLS J U MALLYA FALLS AWARENESS MEETING 23-09-2016 PD Chronic Progressive neurodegenerative disease Motor system disorder Degeneration of Dopaminergic neurons in Substantia nigra in the midbrain.
PD AND FALLS J U MALLYA FALLS AWARENESS MEETING 23-09-2016 PD Chronic Progressive neurodegenerative disease Motor system disorder Degeneration of Dopaminergic neurons in Substantia nigra in the midbrain.
International Brain Bee Syllabus 2012 Department of Neurosciences, Universiti Sains Malaysia
 BRAIN DEVELOPMENT The cells of the nervous system connect with one another in trillions of remarkably specific patterns that form and change over the course of an organism s life. These connections develop
BRAIN DEVELOPMENT The cells of the nervous system connect with one another in trillions of remarkably specific patterns that form and change over the course of an organism s life. These connections develop