Respiratory insufficiency in bariatric patients
|
|
|
- Dulcie Robinson
- 5 years ago
- Views:
Transcription

1 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015
2 Definition of obesity Underweight BMI< 18 Normal weight BMI Overweight BMI > 25 Obesity BMI > 30 Morbid obesity BMI > 40 or comorbidities
 Compared to 800 mio starving 20-30% of ICU patients have a BMI > 30")
3 Perspective Globally 1,9 billion are overweight (BMI>25) 600 mio are obese (BMI>30) Compared to 800 mio starving 20-30% of ICU patients have a BMI > 30 WHO 2015
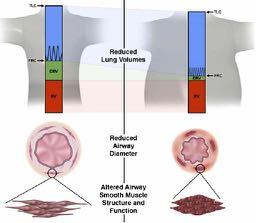
4 Physiology in the obese Increased abdominal pressure and thoracic weight Reduced compliance worsened in suppine position and during sedation Changes in diaphragma Weight of heart Increased thoracic blood volume Increased FiO 2 Loss of muscle tone/power
5
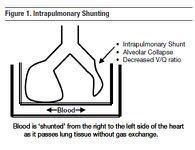
6 Physiology in the obese Reduction in end expiratory lung volumes Reduction in functional residual volume FRC: 2 liters at BMI 25; 1 liter at BMI 35 Reduction of EELV below closing capacity causes collapse of bronchioli Atelectasis impaired gas exchange, ie shunt and hypoxemia Compliance reduced: - 75 cmh2o at BMI 25; 50 at BMI 35
7
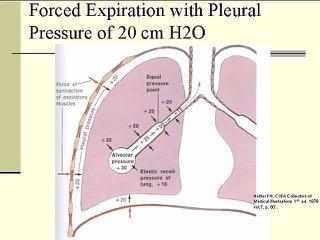
8 Complications to mechanical ventilation Expiratory flow limitation: airway collapse (PEEPi) Prolonged expiration Increased incidence of asthma and bronchospasm VILI ventilator induced lung injury caused by repetetive opening and closing of og collapsed alveoli
 When Intubation is needed postoperatively, increased risk of ARDS (not")
9 Complications to anesthesia not ICU Postoperative complications 5 % in Morbidly obese are not increased (except 1 study) When Intubation is needed postoperatively, increased risk of ARDS (not mortality)
10 Ventilator strategy No evidence for particular ventilator mode KEEP THE LUNG OPEN Lowest FiO 2 to mantain physiologic oxygenation PEEP (10-15) after RM (up to cmh 2 O 6-8 secs) Sighs Vt? IBW 6-8 ml/kg The lung does not grow with increased Body Mass
. A CT scan 1 cm above the diaphragm in the three different groups at all four time points.")
11 From: Prevention of Atelectasis in Morbidly Obese Patients during General Anesthesia and Paralysis:A Computerized Tomography Study Anesthesiology. 2009;111(5): doi: /aln.0b013e3181b87edb Figure Legend: Fig. 3. Representative computerized tomography (CT). A CT scan 1 cm above the diaphragm in the three different groups at all four time points. Note the sustained effect of RM + PEEP and the transient effect of RM + ZEEP. PEEP = positive end-expiratory pressure; RM = recruitment maneuver; ZEEP = zero end-expiratory pressure. Date of download: 10/25/2015 Copyright 2015 American Society of Anesthesiologists. All rights reserved.
12 To PEEP or not to PEEP

13 Beware of hyperinflation Zimbabwe 2008
14 Co morbidities Obesity is correlated to a wide range of other diseases Anxiety depression Ischemic heart disease, hypertension COPD Diabetes mellitus Chronic inflammatory state Increased risk of acute kidney injury oedema

15 Special considerations Obesity hypoventilation Syndrome OHS PaCO 2 > 5,9 kpa (45 mmhg) + BMI > 30 Exclusion of other reasons for hypercapnia Malignant OHS When BMI > 40 Obesity supine death syndrome
16
17 Prepare for extubation Minimal sedation Protocolized sedation and weaning Prevent neuromuscular weakness because of prolonged ventilation Treat prolonged expiration to avoid increased WOB and fatigue Optimize fluid status



18 Positioning Position in sitting or halfsitting Obesity supine death syndrome McKenzie Anesth Analg 1980 Jan; 59(1):81
19 Postextubation NIV could reduce respiratory insufficiency in terms of reduced LOS in ICU and hospital. Mortality reduction in patients with hypercapnia El Sohl; Eur Respir J 2006; Common reintubation what rate is acceptable
20 Outcomes Overweight is not related to increased mortality but Longer length of stay (LOS) 1,5 day and Ventilator 1 day Low BMI increases mortality! Moderately overweight (BMI 30-40) might have a lower mortality RR 0,86 (CI 0,81-0,91; p < 0,001) Akkinusi et al CCM Metaanalysis

21
22 Special considerations Prevent or treat overt pain and anxiety A priori higher PEEP. Allow for longer expiration Prepare before mobilization and exercise Optimize blood pressure and cardiac output. Increase oxygen supply and ventilation if needed. Treat bronchospasm as needed. Evaluate thoroughly before weaning and extubation Consider NIV for postextubation profylaxis Especially with hypercapnia or for exercise
23 Key Points Generally same challenges in obese patients as those with normal weight. The obese patient with respiratory insufficiency has an increased risk of a more difficult weaning from the ventilator and thus longer time on mechanical ventilation We need to take precautions in order to avoid further complications. These are the same measures as in any other patient with difficult weaning Though a longer stay in the ICU the bariatric patient does not have an excess mortality (overweight might even be protective).
24 Thank you
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
 Dr.Ahmad farooq") Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
Disclosures. Objectives. Defining Adult Obesity. Body Mass Index vs. Central Obesity 9/6/2017
 Disclosures Why is the Morbidly Obese Patient at Increased Risk for Perioperative Morbidity? Lisa R. Farmer, MD Associate Professor No conflicts of interests concerning the content of this presentation
Disclosures Why is the Morbidly Obese Patient at Increased Risk for Perioperative Morbidity? Lisa R. Farmer, MD Associate Professor No conflicts of interests concerning the content of this presentation
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Ventilation de l obèse: les 10 points clés
 Ventilation de l obèse: les 10 points clés Samir JABER Department of Critical Care Medicine and Anesthesiology (DAR B) Saint Eloi University Hospital and Montpellier School of Medicine; INSERM U1046 University
Ventilation de l obèse: les 10 points clés Samir JABER Department of Critical Care Medicine and Anesthesiology (DAR B) Saint Eloi University Hospital and Montpellier School of Medicine; INSERM U1046 University
Charisma High-flow CPAP solution
 Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial
. A randomized controlled trial") CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial Backgrounds Postoperative pulmonary complications are most frequent after cardiac surgery and lead to increased
CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial Backgrounds Postoperative pulmonary complications are most frequent after cardiac surgery and lead to increased
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Does the Use of Positive End Expiratory Pressure (PEEP) During Surgery Decrease Respiratory Complications Twenty-Four Hours Post Operative?
 During Surgery Decrease Respiratory Complications Twenty-Four Hours Post Operative?") Rhode Island College Digital Commons @ RIC Master's Theses, Dissertations, Graduate Research and Major Papers Overview Master's Theses, Dissertations, Graduate Research and Major Papers 2016 Does the Use
Rhode Island College Digital Commons @ RIC Master's Theses, Dissertations, Graduate Research and Major Papers Overview Master's Theses, Dissertations, Graduate Research and Major Papers 2016 Does the Use
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Measuring End Expiratory Lung Volume after cardiac surgery
 (Acta Anaesth. Belg., 2012, 63, 115-120) Measuring End Expiratory Lung Volume after cardiac surgery G. MICHIELS (*), V. MARCHAL (**), D. LEDOUX (*) and P. DAMAS (*) Abstract. Background : The aim of this
(Acta Anaesth. Belg., 2012, 63, 115-120) Measuring End Expiratory Lung Volume after cardiac surgery G. MICHIELS (*), V. MARCHAL (**), D. LEDOUX (*) and P. DAMAS (*) Abstract. Background : The aim of this
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
Alveolar Recruitment Maneuvers and Noninvasive Positive Pressure Ventilation in Obese Patients: A Quality Improvement Project
 The University of Southern Mississippi The Aquila Digital Community Doctoral Projects Fall 10-1-2018 Alveolar Recruitment Maneuvers and Noninvasive Positive Pressure Ventilation in Obese Patients: A Quality
The University of Southern Mississippi The Aquila Digital Community Doctoral Projects Fall 10-1-2018 Alveolar Recruitment Maneuvers and Noninvasive Positive Pressure Ventilation in Obese Patients: A Quality
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Fariba Rezaeetalab Associate Professor,Pulmonologist
 Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Mechanical Ventilation Strategies in Anesthesia
 Mechanical Ventilation Strategies in Anesthesia PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University
Mechanical Ventilation Strategies in Anesthesia PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
One Lung Ventilation in Obese patients
 One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT
, RPSGT") BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
VENTILATING CHILDREN- a quick recap. Dr Despina Demopoulos Paediatric Intensivist
 VENTILATING CHILDREN- a quick recap Dr Despina Demopoulos Paediatric Intensivist Introduction Six Tricks Case Scenarios Goals of ventilation Modes of ventilation Different diseases Conclusion OVERVIEW
VENTILATING CHILDREN- a quick recap Dr Despina Demopoulos Paediatric Intensivist Introduction Six Tricks Case Scenarios Goals of ventilation Modes of ventilation Different diseases Conclusion OVERVIEW
Dr. AM MAALIM KPA 2018
 Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
QuickLung Breather Patient Settings
 The QuickLung Breather is capable of simulating a spontaneously breathing patient in a variety of modes and patterns. In response to customer requests, we have compiled five common respiratory cases below.
The QuickLung Breather is capable of simulating a spontaneously breathing patient in a variety of modes and patterns. In response to customer requests, we have compiled five common respiratory cases below.
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
Effect of peak inspiratory pressure on the development. of postoperative pulmonary complications.
 Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Respiratory Complications of Obesity. Diana Wilson, M.D. ACP Educational Session September 16, 2017
 Respiratory Complications of Obesity Diana Wilson, M.D. ACP Educational Session September 16, 2017 1 Prevalence of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2011 Prevalence
Respiratory Complications of Obesity Diana Wilson, M.D. ACP Educational Session September 16, 2017 1 Prevalence of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2011 Prevalence
TSANZ meeting 01 Apr Physiology of respiratory failure in COPD & OHS. Bhajan Singh MBBS FRACP PhD
 TSANZ meeting 01 Apr 2015 Physiology of respiratory failure in & OHS Bhajan Singh MBBS FRACP PhD Head of Department, Pulmonary Physiology & Sleep Medicine, Sir Charles Gairdner Hospital Director, West
TSANZ meeting 01 Apr 2015 Physiology of respiratory failure in & OHS Bhajan Singh MBBS FRACP PhD Head of Department, Pulmonary Physiology & Sleep Medicine, Sir Charles Gairdner Hospital Director, West
A simple case of.. Acute severe asthma. MasterclassIC Schiermonnikoog 2017
 A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
Biphasic Capnogram in a Single Lung Transplant Recipient A Case Report
 TITLE PAGE Biphasic Capnogram in a Single Lung Transplant Recipient A Case Report Authors: Hardeep S. Rai, MD, Cleveland Clinic, Respiratory Institute, Cleveland, OH 44195 Justin Boehm, RRT, Cleveland
TITLE PAGE Biphasic Capnogram in a Single Lung Transplant Recipient A Case Report Authors: Hardeep S. Rai, MD, Cleveland Clinic, Respiratory Institute, Cleveland, OH 44195 Justin Boehm, RRT, Cleveland
Lung Injury and Protection in the Perioperative Period
 J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
Preoperative Pulmonary Evaluation. Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine
 Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
AVOIDING THE CRASH 3: RELAX, OPTIMAL POST-AIRWAY MANAGEMENT AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Mechanical ventilation in the emergency department
 Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
R Y. P r. r w. e s s u r e O A T. e A i. i v. i t P o s I R S P. u s. u o i n n t C o R E. Boussignac CPAP. Breathe easy, recover effectively
 S P I R u s O A T i t P o s R Y i v e A i r w a y P r e s s u r e R E u o i n n t C o Breathe easy, recover effectively (1, 2) What is CPAP? Continuous Positive Airway Pressure, (CPAP), is the conservation
S P I R u s O A T i t P o s R Y i v e A i r w a y P r e s s u r e R E u o i n n t C o Breathe easy, recover effectively (1, 2) What is CPAP? Continuous Positive Airway Pressure, (CPAP), is the conservation
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
EPO 2 Evaluation of the preoxygenation in! morbidly obese. Optimal position and ventilation mode!
 EPO 2 Evaluation of the preoxygenation in! morbidly obese. Optimal position and ventilation mode! Antony Carrier-Boucher! PGY 3 Anesthesiology! Laval University! None! Conflict of interest! 2. Anesth Analg
EPO 2 Evaluation of the preoxygenation in! morbidly obese. Optimal position and ventilation mode! Antony Carrier-Boucher! PGY 3 Anesthesiology! Laval University! None! Conflict of interest! 2. Anesth Analg
Respiratory failure Dr. Kamaran
 Respiratory failure Dr. Kamaran Respiratory failure refers to a condition in which pulmonary gas exchange fails to maintain normal arterial oxygen and carbon dioxide. Respiratory failure is a condition
Respiratory failure Dr. Kamaran Respiratory failure refers to a condition in which pulmonary gas exchange fails to maintain normal arterial oxygen and carbon dioxide. Respiratory failure is a condition
Instellen van beademingsparameters bij de obese pa3ent. MDO Nynke Postma
 Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
You are caring for a patient who is intubated and. pressure control ventilation. The ventilator. up to see these scalars
 Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Assessing perioperative risk
 Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
Tissue is the Issue. PEEP CPAP FiO2 HFNC PSV HFNC. DO 2 = CO [(Hb x 1.34) SaO PaO 2 ] perfusione
![Tissue is the Issue. PEEP CPAP FiO2 HFNC PSV HFNC. DO 2 = CO [(Hb x 1.34) SaO PaO 2 ] perfusione](/thumbs/79/78902905.jpg "Tissue is the Issue. PEEP CPAP FiO2 HFNC PSV HFNC. DO 2 = CO [(Hb x 1.34) SaO PaO 2 ] perfusione") Tissue is the Issue perfusione PEEP CPAP FiO2 HFNC PSV HFNC DO 2 = CO [(Hb x 1.34) SaO 2 + 0.003 PaO 2 ] O2 HFNC PEEP CPAP PSV ARF ACPE HIGH FLOW NASAL CANNULA High and Exact FiO2, High Flow heating and
Tissue is the Issue perfusione PEEP CPAP FiO2 HFNC PSV HFNC DO 2 = CO [(Hb x 1.34) SaO 2 + 0.003 PaO 2 ] O2 HFNC PEEP CPAP PSV ARF ACPE HIGH FLOW NASAL CANNULA High and Exact FiO2, High Flow heating and
Ambulatory Anesthesia for the Obese Patient
 Ambulatory Anesthesia for the Obese Patient Disclosures I have nothing to disclose Brian M Keech, MD FAAP University of Colorado School of Medicine Director, Ambulatory Anesthesia Denver Health Medical
Ambulatory Anesthesia for the Obese Patient Disclosures I have nothing to disclose Brian M Keech, MD FAAP University of Colorado School of Medicine Director, Ambulatory Anesthesia Denver Health Medical
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Airway pressure release ventilation (APRV) in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital
 in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital") Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Journal Club American Journal of Respiratory and Critical Care Medicine. Zhang Junyi
 Journal Club 2018 American Journal of Respiratory and Critical Care Medicine Zhang Junyi 2018.11.23 Background Mechanical Ventilation A life-saving technique used worldwide 15 million patients annually
Journal Club 2018 American Journal of Respiratory and Critical Care Medicine Zhang Junyi 2018.11.23 Background Mechanical Ventilation A life-saving technique used worldwide 15 million patients annually
Protecting the Lungs
 Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
PREVENT COMPLICATIONS IN MAJOR SURGERY
 PREVENT COMPLICATIONS IN MAJOR SURGERY Dept of Anesthesia and ICM (Prof. G. Della Rocca) Azienda Ospedaliero-Universitaria University of Udine. Udine, Italy CLINICAL TRIAL OF SURVIVORS CARDIORESPIRATORY
PREVENT COMPLICATIONS IN MAJOR SURGERY Dept of Anesthesia and ICM (Prof. G. Della Rocca) Azienda Ospedaliero-Universitaria University of Udine. Udine, Italy CLINICAL TRIAL OF SURVIVORS CARDIORESPIRATORY
High Flow Humidification Therapy, Updates.
 High Flow Humidification Therapy, Updates. Bernardo Selim, M.D. I have no relevant financial relationships to disclose. Assistant Professor, Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic What
High Flow Humidification Therapy, Updates. Bernardo Selim, M.D. I have no relevant financial relationships to disclose. Assistant Professor, Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic What
Concerns and Controversial Issues in NPPV. Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation
 : Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
: Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
Basics for mechanical ventilation
 Basics for mechanical ventilation Lorx András Semmelweis University Dept. of Anaesthesiology and Intensive Therapy 1 Normal breathing negativ pressure during inspiration zero EEP or 3-4 H2Ocm dynamic PEEP
Basics for mechanical ventilation Lorx András Semmelweis University Dept. of Anaesthesiology and Intensive Therapy 1 Normal breathing negativ pressure during inspiration zero EEP or 3-4 H2Ocm dynamic PEEP
Web Appendix 1: Literature search strategy. BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up. Sources to be searched for the guidelines;
 write-up. Sources to be searched for the guidelines;") Web Appendix 1: Literature search strategy BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up Sources to be searched for the guidelines; Cochrane Database of Systematic Reviews (CDSR) Database of
Web Appendix 1: Literature search strategy BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up Sources to be searched for the guidelines; Cochrane Database of Systematic Reviews (CDSR) Database of
«Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic?
 1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients CASE REPORT FORM
 INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
Non-Invasive Ventilation
 Khusrav Bajan Head Emergency Medicine, Consultant Intensivist & Physician, P.D. Hinduja National Hospital & M.R.C. 112 And the Lord God formed man of the dust of the ground and breathed into his nostrils
Khusrav Bajan Head Emergency Medicine, Consultant Intensivist & Physician, P.D. Hinduja National Hospital & M.R.C. 112 And the Lord God formed man of the dust of the ground and breathed into his nostrils