Introduction. v Insomnia is very prevalent in acute (30-50%) and chronic forms (10-15%). v Insomnia is often ignored as a symptom of other disorders.
|
|
|
- Albert Thompson
- 6 years ago
- Views:
Transcription
1 Introduction v Insomnia is very prevalent in acute (30-50%) and chronic forms (10-15%). v Insomnia is often ignored as a symptom of other disorders. v Insomnia is a risk factor for psychiatric and medical morbidity. v CBT for insomnia has moderate to large effect sizes which are equivalent to medical interventions for insomnia. 1
2 Definition of Insomnia v World Health Organization - problem initiating/maintaining sleep or non-refreshing sleep that occurs three nights/week and is associated with daytime distress or impairment. v DSM-IV calls it primary insomnia if the difficulty sleeping is not associated with any medical or psychiatric disorders. v ICSD calls it psychopysiological insomnia - a disorder of somatized tension and learned sleep preventing associations that result in insomnia and decreased functioning during the day. 2
3 Duration of Illness v Acute - less than one month - usually associated with clearly defined precipitants (stress, pain, substance abuse). v Chronic - symptoms persist for > one month, more typically > six months. v Transition from acute to chronic occurs when patient stops causally linking original precipitant to insomnia 3
4 Severity of Illness v Intensity - greater than 30 minutes to fall asleep or wakefulness during the night is usually considered the threshold between normal and abnormal sleep. v Total sleep time of less than 6 to 6.5 hours. TST threshold is not clearly established due to individual variation in sleep need. Also, sleep need may be met even though insomnia is present. v Frequency- usually symptom occurance of 3 or more nights per week. 4
5 Diagnostic Process v Two step process for diagnosing primary insomnia. v First rule out psychiatric disorders. This can be difficult due to significant overlap of symptoms of insomnia and depression and anxiety. Inadequately treated psychaitric disorders must be considered. v Second, rule out and other primary sleep disorders which cause insomnia symptoms for example circadian rhythm disorders or PLMD. 5
6 Common Medical/Psychiatric Rule Outs v Medical disorders which may cause insomnia - chronic pain, chronic obstructive pulmonary disease, gastroesophageal reflux disease, renal disease, hyperthyroidism, dementia. v Psychiatric disorders which cause insomnia - primarily major depression, bipolar depression, and anxiety disorders (generalized anxiety disorder, PTSD, panic disorder). 6
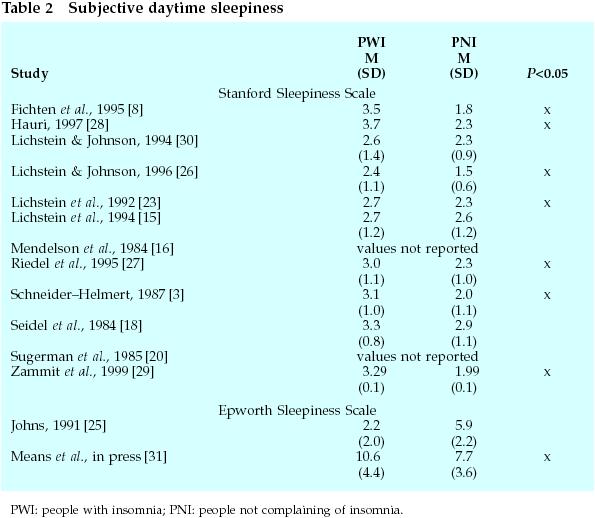
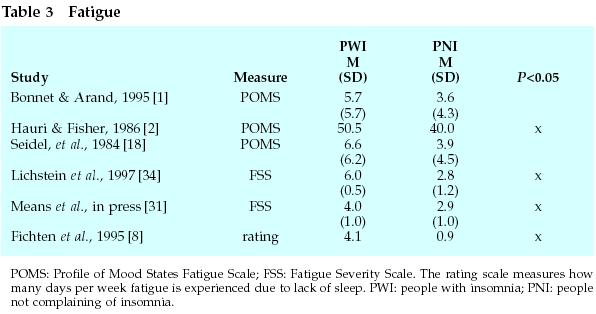
7 Common Sleep Disorder Rule Outs v Sleep Apnea (particularly central sleep apnea), narcolepsy, restless legss syndrome, periodic limb movement disorder. v It is important to disguish between fatigue and sleepiness sleepiness. v Fatigue - physical or mental weariness, feeling worn out. v Sleepiness - may or may not include fatigue, but patient indicates that they are struggling to stay awake. 7
8 Common Sleep Disorder Rule Outs - cont. v Most commonly, patients with insomnia report difficulty with fatigue, but less commonly sleepiness. v Sleepiness is more commonly associated with sleep apnea, narcolepsy, PLMD and RLS. v Circadian rhythm disorders, such as delayed sleep phase (sleep onset difficulty) or advanced sleep phase (early morning awakening), may present as insomnia. 8
9 Common Sleep Disorder Rule Outs - cont. v External factors may also cause or exacerbate insomnia. v These include, most commonly, insomnia associated with medication, drug or alcohol use. v Insomnia may be a side effect of some medications and should be considered. Timing and dosage should be considered for necessary medications. v Common problem is rebound insomnia after discontinuation of hypnotic medication. 9
10 Evaluation of Insomnia v Sleep is the outcome of a complex set of physiological and psychological processes o Assessment is not haphazard o Researchers have identified factors that commonly are associated with poor sleep o A comprehensive evaluation considers these factors o Idiosyncratic patient perceptions and meanings assigned to symptoms are also considered 10
11 Evaluation of Insomnia v A few insomnia complaints are associated with many diagnoses v Trouble falling asleep may be due to: o delayed sleep phase o learned sleep preventing associations o major depression, generalized anxiety Factors may vary from one night to the next in a patient 11
12 Evaluation - cont. v Evaluation begins before the first visit o Materials are sent to the patient prior to coming to the clinic o This serves to inform the patient that the evaluation will be comprehensive o Also allows the clinician to be efficient when the patient is being evaluated in the clinic 12
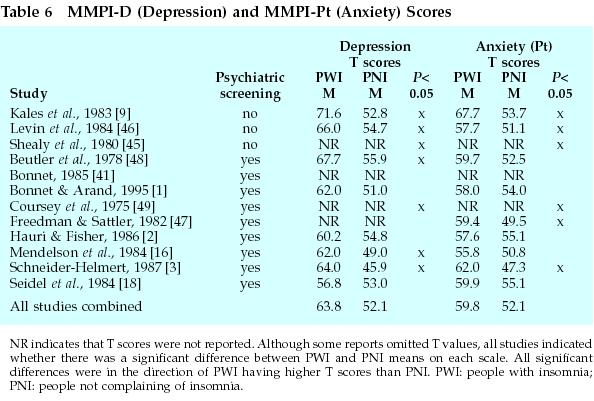
13 Depression Depression is commonly found in patients with insomnia and needs to be thoroughly evaluated o Depression inventories such as the Beck can be used in the initial evaluation o Depression can cause insomnia,, but insomnia can also cause mood disturbance,, so it is important to keep this issue open during treatment 13
14 Anxiety Anxiety disorders are common in insomnia Anxiety may manifest as either somatic or cognitive arousal that will interfere with the process of winding down before bed. Brief scales are available with which anxiety can be measured (e.g. state-trait anxiety inventory) Anxiety may be sub-clinical in many cases 14
15 Cognitive beliefs The beliefs that the patient hold regarding the functions sleep and the consequences of sleeplessness affect the course of the insomnia and the response to treatment. Scales are available which can be administered prior to treatment to assess dysfunctional beliefs and attitudes. 15
16 Sleep hygiene Assessment of basic sleep hygiene practices are sometimes overlooked as explanations for sleep difficulty. Assessment of basic sleep hygiene practices such as caffeine use, tobacco use, exercise patterns, eating habits should be included in the evaluation 16
17 Sleep Log A sleep log provides a systematic, subjective portrayal of key features of the sleep pattern (bed time, waketime, sleep onset latency, etc) o Patients should not use clock to record information as this might interfere more with sleep o Sometimes patients resist keeping a sleep log because believe the pattern is always the same or there is no rhyme or reason to the pattern o Patients are often surprised by the results of their log-they see that they are getting more sleep then they thought 17
18 18
19 Sleep History v The evolution of the sleep problem helps the clinician better understand the current problem v Sleep history involves understanding the predisposing, precipitating and perpetuating factors in the sleep problem. v Treatment is usually focussed on treating the perpetuating factors,, such as the behavioral adaptations to poor sleep or changes in thinking v The sleep complaint points to the part of the night that is most troubling and how often the problem occurs 19
20 Sleep Wake Pattern v The pattern of sleep is usually obtained in the sleep log and involves the following information: o Type, dosage, frequency and timing of sleep medicine o Time and activities around bedtime o Time of lights out o Estimated sleep latency o Frequency, timing, duration, cause and consequences of nocturnal awakenings 20
21 Sleep Wake Pattern - cont. o Final wake-up and rise time (out of bed) o Quality of sleep o Frequency, timing, duration of naps o daytime consequences such as fatigue or cognitive alertness This list simplifies the nature of obtaining this information as sleep may follow a branching pattern such as with and without medication, good vs. bad nights.. An assessment may need to be done for each branch. 21
22 Sleep Related Cognitions v Worries, apprehension about not sleeping and cognitive hyperarousal may set off a self- fulfilling prophecy v Obsessional thinking will preclude sleep as the mind remains on alert rehearsing responses to crises v Sometimes no particular distressing thoughts can be described, but the patients mind flits from one mundane thought to another. 22
23 Sleep Related Cognitions - cont. v How does the insomnia appear to the insomniac? v What is the form of the cognitions? Obsessive fixture on one thought or unable to focus on one thought? v What is the emotional tone? Anger and agitation or resignation and detachment? 23
24 Social Determinants v Social intrusions prior to going to bed may effect sleep. Telephone may ring Nightly news headlines Internet chat rooms, instant messaging v People with chronic sleep difficulties vary in their approaches to dealing with social intrusions Some are very protective of their sleep Others may follow a night-owl pattern v Understanding the social context will be helpful in planning treatment 24
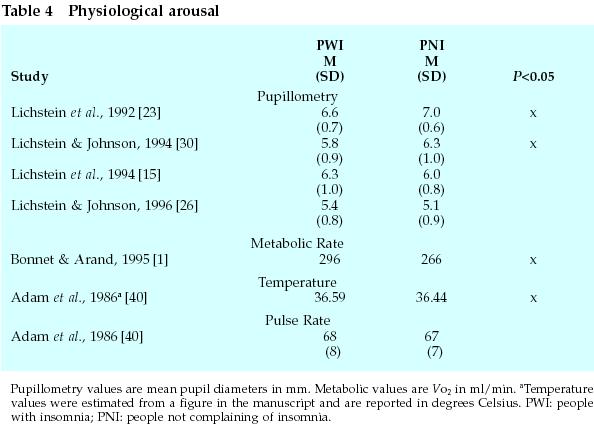
25 Physiological Hyperarousal v Heightened physiological arousal is present in individuals with sleeping problems and this arousal inhibits sleep. v Techniques are available to measure heart rate, body temperature and muscle tension,, but no levels are known above which insomnia is triggered. v There are no suitable assessment instruments for quantifying hyperarousal in the clinical setting 25
26 26
27 Circadian Rhythms v The circadian system promotes sleep as well as wakefulness. v Knowing the phase position of the endogenous rhythm can help to explain a particular sleep problem. v No direct assessments are available for measurement of the circadian system. v Indirect measures include the Horne-Ostberg morningness-eveningness scale, preferred sleep time when no time constraints exist 27
28 Sleep Disorders v Restless Legs Syndrome can be diagnosed by patient report. Sleep onset insomnia is common with RLS v Periodic Limb Movement Disorder- - can be a subtle writhing of the foot to distinct rapid jerks.. These movements occur, by definition, during sleep, so the patient may not be aware of them. v PLMD can only be diagnosed with overnight PSG and may include difficulty maintaining sleep because of fragmented sleep due to arousals. 28
29 29
30 30
31 Sleep Disorders - cont. v Respiratory disturbance during sleep may produce fragmented sleep and complaint of insomnia. v Daytime sleepiness is the far more common complaint in sleep disordered breathing. v Sleep apnea is part of the differential diagnosis for insomnia 31
32 Objective Tests for Insomnia v PSG is used if the clinician suspects that some other primary sleep disorder (besides insomnia) is causing insomnia.. Symptoms of RLS, PLMD or sleep apnea would be sufficient to require PSG testing. v If a patient is unresponsive to behavioral or pharmacological treatment, a PSG may be necessary. v PSG may be used to confirm a diagnosis of sleep state misperception 32
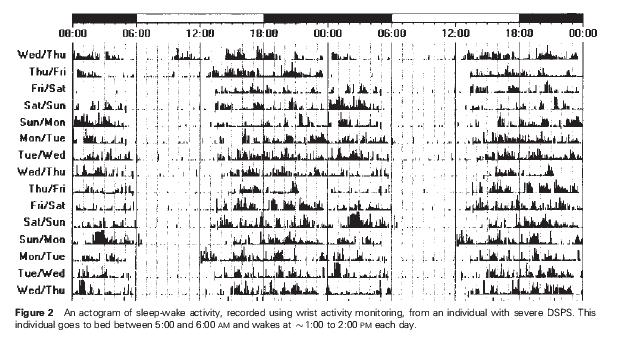
33 Objective Tests for Insomnia - cont. v Physical exam - several medical disorders may be responsible for insomnia, however most commonly, behavioral and psychological factors are responsible and there are few indications of any medical problem. v Actigraphy - Behavioral quiescence is a defining characteristic of sleep, and actigraphy which measures movement may be useful to assess sleep patterns. v When used in conjunction with sleep logs, actigraphy can detail the sleep pattern over many days or weeks. 33
34 Trial Treatment as Evaluation v If RLS or PLMD is suspected,, an overnight PSG is the only definitive way to diagnose the disorder. v However, dopaminergic agents are commonly used to treat these disorders and can be used on a trial basis. v If the patients symptoms are resolved,, with Mirapex or Sinemet,, then diagnostic certainty is high. 34
35 Cognitive-Behavioral Perspective on Insomnia v Behavioral perspective Predisposing factors - personality factors, physiologic arousal, genetic predisposition, etc. Precipitating factors - situational stress, acute injury, bereavement, etc. Perpetuating factors - any form of compensatory strategies a patient used to cope with insomnia - napping, spending too much time in bed, variable schedule 35
36 Cognitive-Behavioral Perspective on Insomnia v Cognitive perspective - two types of cognitive problems: Beliefs and attitudes toward sleep o Unrealistic views about what constitutes adequate sleep and catastrophic beliefs about the consequences of insomnia Cognitive processes like intrusive thoughts and worry. o Perseverative problem-solving about mundane daily activities or work or relationships. 36
37 Cognitive-Behavioral Perspective on Insomnia v Neurocognitive perspective - dysfunctional beliefs and worry are epiphenomena. v In chronic insomnia cognition occurs secondary to conditioned arousal. v Arousal is conditioned cortical arousal observed as high frequency EEG activity (14-45 Hz) at or around sleep onset and during non-rem sleep. v High frequency EEG activity allows for more sensory processing and memory formation and difficulty with perceiving sleep. 37
38 Cognitive-Behavioral Treatment of Insomnia v Most common cognitive-behavioral therapies (CBT) are: Sleep hygiene education Stimulus control Sleep restriction Relaxation therapy Cognitive therapy v Most behavioral sleep medicine clinicians use a multi-modal approach - combining the techniques above. 38
39 Cognitive-Behavioral Treatment of Insomnia v Therapeutic regimen - usually therapy requires 4-8 weeks of, in most cases, face-to-face meeting with the provider. Sessions last minutes. v Stimulus control and sleep restriction are implemented during the first 2-3 sessions. Additional sessions are used to upwardly titrate sleep time v Adjunctive therapies such as cognitive therapy, relaxation training and relapse prevention occur during the balance of the sessions. 39
40 Stimulus Control Therapy v Stimulus control therapy limits the amount of time that patients spend awake in the bed. v They are designed to decondition pre-sleep arousal and re-associate the bed with rapid well consolidated sleep. v Typical instructions include: o o o o o Keep a fixed wake time 7 days a week avoid any behavior in the bed besides sleep sleep nowhere else except the bedroom leave the bedroom after being awake for longer than 15 minutes return to bed only when sleepy 40
41 Sleep Restriction Therapy v Recommended for both sleep initiation and maintenance problems. v Procedure entails three steps: Establish a fixed waketime. Decrease sleep opportunity to average total sleep time. Increase time in bed by 15 minutes per week as sleep efficiency (TST/TIB) increases. v May be contraindicated in patients with bipolar or seizure disorder. 41
42 Sleep Hygiene Education v Addresses a variety of behaviors that may influence the quality and quantity of sleep. v Common suggestions include: Exercise regularly, Make bedroom a comfortable temperature and free of noise and light, Cut down on caffeine and tobacco products Avoid alcohol, especially in the evening, Don t go to bed hungry 42
43 Cognitive Therapy v Based on the observation that people with insomnia have negative thoughts and beliefs about their condition and its consequences. v Challenging these beliefs can decrease anxiety and arousal associated with insomnia. v Cognitive restructuring focuses on catastrophic thinking and the belief that poor sleep will have devastating consequences. v These beliefs are challenged with evidence collected by the patient of how often these horrible consequences have occurred (not often). 43
44 Relaxation Training and Phototherapy v Relaxation training specifically targets the physiological arousal experienced by the patient. v Any technique (progressive muscle relaxation, deep breathing, autogenic training) with which the patient is comfortable can be used. It may need to be practiced out of bed because of performance anxiety. v Phototherapy,, although not a behavioral therapy, can be used in conjunction with CBT when a patients sleep difficulty has a circadian rhythm component. 44
45 Treatment Complinace v The single most important complicating factor in CBT is poor treatment compliance. v Patients expectations should be managed with a thoughtful rationale for each aspect of treatment to help increase compliance v Patients should be advised that sleep may get somewhat worse before improvement is appreciated 45
46 CBT and Sedative/Hypnotics v CBT may be combined with hypnotics to take advantage of the strengths of each: the rapid reduction in symptoms with medicine and the long lasting effects of CBT. v The best method of combining therapy has yet to be established. v For patients who are currently taking hypnotics, collaborating with their physician to withdraw them may be most useful. 46
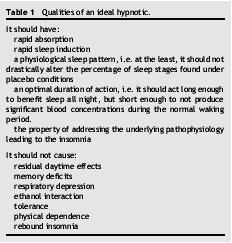
47 Pharmacologic Treatment Options v Most common hypnotics are benzodiazepines (temazepam, flurazepam) ) and benzodiazepines receptor agonists (zolpidem, zaleplon). v These medicines have mostly been studied as short-term treatments.. Thus the effects of long- term use is undocumented. v Physicians often have some concern with tolerance, side-effects and rebound insomnia. v Daytime functioning is not improved with hypnotic medication. 47

48 Recettore GABAA 48
49 Pharmacologic Treatment Options - cont. v Sedating anti-depressant medications are often used to treat primary insomnia. v There exists a paucity of data on the use of sedating anti-depressants for insomnia. v These medicines are thought to have a low abuse profile and may be useful in treating occult depression and are considered a better long term treatment for primary insomnia by some physicians. 49
50 50
51 51
52 52
53 53
54 54
55 55
56 56
57 57
58 58
59 59
60 60
61 61
62
63 63
64 64
65 65
66 66
67 67
68 68
69 69
70 70
71 71
72 72
Insomnia. Learning Objectives. Disclosure 6/7/11. Research funding: NIH, Respironics, Embla Consulting: Elsevier
 Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Cognitive-Behavioral Therapy for Insomnia
 Wisconsin Department of Health Services Wisconsin Public Psychiatry Network Teleconference (WPPNT) This teleconference is brought to you by the Wisconsin Department of Health Services (DHS) Bureau of Prevention,
Wisconsin Department of Health Services Wisconsin Public Psychiatry Network Teleconference (WPPNT) This teleconference is brought to you by the Wisconsin Department of Health Services (DHS) Bureau of Prevention,
Chronic Insomnia: DSM - V. Insomnia DSM - V. Patient Symptoms. Insomnia: Assessment and Overview of Management. Insomnia Management in the Digital Age
 Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
Optimal Sleep Using NeurOptimal -Insomnia Studies
 Optimal Sleep Using NeurOptimal -Insomnia Studies Edward B. O'Malley, PhD, FAASM Diplomate, American Board of Sleep Medicine Managing Director, Sleep HealthCare of CT Fairfield, CT eomalley@sleephelathcarect.com
Optimal Sleep Using NeurOptimal -Insomnia Studies Edward B. O'Malley, PhD, FAASM Diplomate, American Board of Sleep Medicine Managing Director, Sleep HealthCare of CT Fairfield, CT eomalley@sleephelathcarect.com
INDEX. Group psychotherapy, described, 97 Group stimulus control, 29-47; see also Stimulus control (group setting)
") Index Abdominal breathing, 70; see also Breathing; Relaxation therapy Activation, sleep drive/responsivity, 6-9 Age level; see also Elderly circadian rhythms and, 68-69 delayed sleep phase syndrome and,
Index Abdominal breathing, 70; see also Breathing; Relaxation therapy Activation, sleep drive/responsivity, 6-9 Age level; see also Elderly circadian rhythms and, 68-69 delayed sleep phase syndrome and,
INSOMNIAS. Stephan Eisenschenk, MD Department of Neurology
 INSOMNIAS INSOMNIAS General criteria for insomnia A. Repeated difficulty with sleep initiation, duration, consolidation or quality. B. Adequate sleep opportunity, persistent sleep difficulty and associated
INSOMNIAS INSOMNIAS General criteria for insomnia A. Repeated difficulty with sleep initiation, duration, consolidation or quality. B. Adequate sleep opportunity, persistent sleep difficulty and associated
Cognitive Behavioral Therapy for Insomnia. Melanie K. Leggett, PhD, CBSM Duke University Medical Center
 Cognitive Behavioral Therapy for Insomnia Melanie K. Leggett, PhD, CBSM Duke University Medical Center Disclosures I have no relevant financial relationship with the manufacturers of any commercial products
Cognitive Behavioral Therapy for Insomnia Melanie K. Leggett, PhD, CBSM Duke University Medical Center Disclosures I have no relevant financial relationship with the manufacturers of any commercial products
Treating Insomnia in Primary Care. Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team
 Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
WHY CAN T I SLEEP? Deepti Chandran, MD
 WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
Sleep and Traumatic Brain Injury (TBI)
") Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Sleep and Ageing. Siobhan Banks PhD. Body and Brain at Work, Centre for Sleep Research University of South Australia
 Sleep and Ageing Siobhan Banks PhD Body and Brain at Work, Centre for Sleep Research University of South Australia Health and Active Ageing, 22 nd September 2015 Sleep and Aging How does sleep change as
Sleep and Ageing Siobhan Banks PhD Body and Brain at Work, Centre for Sleep Research University of South Australia Health and Active Ageing, 22 nd September 2015 Sleep and Aging How does sleep change as
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia
 Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
 Sleep This factsheet is available in a downloadable PDF here. Table of Contents Introduction Insomnia How Long does Insomnia Last? How much Sleep should You get? Symptoms of Insomnia Causes of Insomnia
Sleep This factsheet is available in a downloadable PDF here. Table of Contents Introduction Insomnia How Long does Insomnia Last? How much Sleep should You get? Symptoms of Insomnia Causes of Insomnia
Insomnia % of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences)
") 10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
Guideline for Adult Insomnia
 Guideline for Adult Insomnia Exclusions This guideline does not apply to: Children under the age of 18 Pregnant and lactating women Geriatric patients: While the general principles of the diagnosis and
Guideline for Adult Insomnia Exclusions This guideline does not apply to: Children under the age of 18 Pregnant and lactating women Geriatric patients: While the general principles of the diagnosis and
6/3/2015. Insomnia An Integrative Approach. Objectives. Why An Integrative Approach? Integrative Model. Definition. Short-term Insomnia
 Insomnia An Integrative Approach Jeffrey S. Jump, M.D. Medical Director CHI Memorial Integrative Medicine Associates Objectives Understand the importance of sleep to health Identify patients with insomnia
Insomnia An Integrative Approach Jeffrey S. Jump, M.D. Medical Director CHI Memorial Integrative Medicine Associates Objectives Understand the importance of sleep to health Identify patients with insomnia
Dr Alex Bartle. Sleep Well Clinic
 Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Faculty/Presenter Disclosure
 A Little CBT I With My Tea Please: Cognitive Behavioural Therapy for insomnia (CBT I) and Its Use In the Treatment of Sleeplessness W. Jerome Alonso, MD Medical Director, Canadian Sleep Consultants Clinical
A Little CBT I With My Tea Please: Cognitive Behavioural Therapy for insomnia (CBT I) and Its Use In the Treatment of Sleeplessness W. Jerome Alonso, MD Medical Director, Canadian Sleep Consultants Clinical
HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS. To educate participants regarding the sleep wake cycle.
 HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS Talk about the relationship between depression, sleep, and health problems. To educate participants regarding the sleep wake cycle. To provide
HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS Talk about the relationship between depression, sleep, and health problems. To educate participants regarding the sleep wake cycle. To provide
TOP 10 LIST OF SLEEP QUESTIONS. Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children
 TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
SLEEP DISORDERS. Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children
 SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
WHEN COUNTING SHEEP FAILS: ADMINISTERING SINGLE-SESSION COGNITIVE-BEHAVIORAL THERAPY FOR INSOMNIA IN A GROUP PSYCHOEDUCATIONAL FORMAT
 WHEN COUNTING SHEEP FAILS: ADMINISTERING SINGLE-SESSION COGNITIVE-BEHAVIORAL THERAPY FOR INSOMNIA IN A GROUP PSYCHOEDUCATIONAL FORMAT Kristin E. Eisenhauer, PhD. Trinity University San Antonio, Texas I
WHEN COUNTING SHEEP FAILS: ADMINISTERING SINGLE-SESSION COGNITIVE-BEHAVIORAL THERAPY FOR INSOMNIA IN A GROUP PSYCHOEDUCATIONAL FORMAT Kristin E. Eisenhauer, PhD. Trinity University San Antonio, Texas I
Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
 COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems. Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems. Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
AGING CHANGES IN SLEEP
 OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
Insomnia. Dr Terri Henderson MBChB FCPsych
 Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
Article printed from
 What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
Sleep & Relaxation. Session 1 Understanding Insomnia Sleep improvement techniques Try a new technique
 Sleep & Relaxation Sleep & Relaxation Session 1 Understanding Insomnia Sleep improvement techniques Try a new technique Session 2 Dealing with unhelpful thoughts Putting these techniques together for better
Sleep & Relaxation Sleep & Relaxation Session 1 Understanding Insomnia Sleep improvement techniques Try a new technique Session 2 Dealing with unhelpful thoughts Putting these techniques together for better
John McLachlan. Clinical Lead Pulmonary Physiology & Sleep Medicine. President Elect, WA Branch Thoracic Society of Australia & NZ
 John McLachlan Respiratory & Sleep Physician @FSH Clinical Lead Pulmonary Physiology & Sleep Medicine Sleep Physician x 27 years Interest in Insomnia management President Elect, WA Branch Thoracic Society
John McLachlan Respiratory & Sleep Physician @FSH Clinical Lead Pulmonary Physiology & Sleep Medicine Sleep Physician x 27 years Interest in Insomnia management President Elect, WA Branch Thoracic Society
KU LEUVEN. Liesbet Van Houdenhove Clinical Psychologist Student Health Center KU Leuven
 SLEEPLESS @ KU LEUVEN Liesbet Van Houdenhove Clinical Psychologist Student Health Center KU Leuven Background Impaired sleep is a frequent and important health problem in college students Prevalence rates
SLEEPLESS @ KU LEUVEN Liesbet Van Houdenhove Clinical Psychologist Student Health Center KU Leuven Background Impaired sleep is a frequent and important health problem in college students Prevalence rates
THIBODAUX REGIONAL SLEEP DISORDERS CENTER 604 N ACADIA ROAD, Suite 210 THIBODAUX, LA 70301
 Name:_ Date: Address: Phone (home): Work: Marital Status: Date of Birth: Height: Weight: In case of emergency contact: ************************************************************************ Social Security#:
Name:_ Date: Address: Phone (home): Work: Marital Status: Date of Birth: Height: Weight: In case of emergency contact: ************************************************************************ Social Security#:
The Wellbeing Plus Course
 The Wellbeing Plus Course Resource: Good Sleep Guide The Wellbeing Plus Course was written by Professor Nick Titov and Dr Blake Dear The development of the Wellbeing Plus Course was funded by a research
The Wellbeing Plus Course Resource: Good Sleep Guide The Wellbeing Plus Course was written by Professor Nick Titov and Dr Blake Dear The development of the Wellbeing Plus Course was funded by a research
Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER
 Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER Disclosure: Financial - none Non-Financial - none Selected Topics Sleep epidemiology Sleep
Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER Disclosure: Financial - none Non-Financial - none Selected Topics Sleep epidemiology Sleep
Improving Your Sleep Course. Session 1 Understanding Sleep and Assessing Your Difficulties
 Improving Your Sleep Course Session 1 Understanding Sleep and Assessing Your Difficulties Course Information Session Details Sessions Session 1 Session 2 Session 3 Session 4 Optional Review Session 5 Session
Improving Your Sleep Course Session 1 Understanding Sleep and Assessing Your Difficulties Course Information Session Details Sessions Session 1 Session 2 Session 3 Session 4 Optional Review Session 5 Session
Iowa Sleep Disturbances Inventory (ISDI)
") Department of Psychological & Brain Sciences Publications 1-1-2010 Iowa Sleep Disturbances Inventory (ISDI) Erin Koffel University of Iowa Copyright 2010 Erin Koffel Comments For more information on the
Department of Psychological & Brain Sciences Publications 1-1-2010 Iowa Sleep Disturbances Inventory (ISDI) Erin Koffel University of Iowa Copyright 2010 Erin Koffel Comments For more information on the
Insomnia. F r e q u e n t l y A s k e d Q u e s t i o n s
 Insomnia Q: What is insomnia? A: Insomnia is a common sleep disorder. If you have insomnia, you may: Lie awake for a long time and have trouble falling asleep Wake up a lot and have trouble returning to
Insomnia Q: What is insomnia? A: Insomnia is a common sleep disorder. If you have insomnia, you may: Lie awake for a long time and have trouble falling asleep Wake up a lot and have trouble returning to
Modern Management of Sleep Disorders
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Insomnia treatment. Sleep hygiene education sleep hygiene teaches good sleeping habits. This includes:
 Insomnia treatment INSOMNIA OVERVIEW insomnia is defined as difficulty falling asleep, difficulty staying asleep, or waking up early in the morning and not being able to return to sleep. In general, people
Insomnia treatment INSOMNIA OVERVIEW insomnia is defined as difficulty falling asleep, difficulty staying asleep, or waking up early in the morning and not being able to return to sleep. In general, people
Get on the Road to Better Health Recognizing the Dangers of Sleep Apnea
 Get on the Road to Better Health You Will Learn About The importance and benefits of sleep Sleep deprivation and its consequences The prevalence, symptoms, and treatments for major sleep problems/ disorders
Get on the Road to Better Health You Will Learn About The importance and benefits of sleep Sleep deprivation and its consequences The prevalence, symptoms, and treatments for major sleep problems/ disorders
HOW TO DEAL WITH SLEEP PROBLEMS
 The Handbook on Successful Ageing HOW TO DEAL WITH SLEEP PROBLEMS Up to 50% of the elderly complain of insomnia, but although such complaints are prevalent and are often accompanied by higher rates of
The Handbook on Successful Ageing HOW TO DEAL WITH SLEEP PROBLEMS Up to 50% of the elderly complain of insomnia, but although such complaints are prevalent and are often accompanied by higher rates of
WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?)
") Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?) CATHERINE MCCALL, MD
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?) CATHERINE MCCALL, MD
Earl J. Soileau, MD, FSAHM Asst Professor, Family Medicine LSU HSC Medical School New Orleans at Lake Charles
 Earl J. Soileau, MD, FSAHM Asst Professor, Family Medicine LSU HSC Medical School New Orleans at Lake Charles Sleep Disorders Restless Legs Syndrome (RLS) and Periodic Limb Movement Disorder (PLMD) Sleep
Earl J. Soileau, MD, FSAHM Asst Professor, Family Medicine LSU HSC Medical School New Orleans at Lake Charles Sleep Disorders Restless Legs Syndrome (RLS) and Periodic Limb Movement Disorder (PLMD) Sleep
Biopsychosocial Characteristics of Somatoform Disorders
 Contemporary Psychiatric-Mental Health Nursing Chapter 19 Somatoform and Sleep Disorders Biopsychosocial Characteristics of Somatoform Disorders Unconscious transformation of emotions into physical symptoms
Contemporary Psychiatric-Mental Health Nursing Chapter 19 Somatoform and Sleep Disorders Biopsychosocial Characteristics of Somatoform Disorders Unconscious transformation of emotions into physical symptoms
A good night s sleep
 A good night s sleep Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm A good night
A good night s sleep Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm A good night
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abuse sleep physiology effects of, 880 882 substance, in adolescents, sleep problems and, 929 946. See also Substance use and abuse, in adolescents,
Note: Page numbers of article titles are in boldface type. A Abuse sleep physiology effects of, 880 882 substance, in adolescents, sleep problems and, 929 946. See also Substance use and abuse, in adolescents,
Insomnia Disorder A Journey to the Land of No Nod
 Insomnia Disorder A Journey to the Land of No Nod JACQUELINE D. KLOSS, PH.D. P S Y C H O L O G I S T B R Y N M A W R P S Y C H O L O G I C A L A S S O C I A T E S B E H A V I O R A L S L E E P M E D I
Insomnia Disorder A Journey to the Land of No Nod JACQUELINE D. KLOSS, PH.D. P S Y C H O L O G I S T B R Y N M A W R P S Y C H O L O G I C A L A S S O C I A T E S B E H A V I O R A L S L E E P M E D I
SLEEP-WAKE DISORDERS: INSOMNIA. Prof. Paz Gía-Portilla
 SLEEP-WAKE DISORDERS: INSOMNIA Prof. Paz Gía-Portilla SLEEP-WAKE DISORDERS AND ICD-10 Chapter V: Mental and Behavioural Disorders F51. Non-organic sleep disorders Chapter VI: Nervous System Illnesses G47.
SLEEP-WAKE DISORDERS: INSOMNIA Prof. Paz Gía-Portilla SLEEP-WAKE DISORDERS AND ICD-10 Chapter V: Mental and Behavioural Disorders F51. Non-organic sleep disorders Chapter VI: Nervous System Illnesses G47.
Modern Management of Sleep Disorders. Case. Introduction. Topics Covered. Douglas C. Bauer, MD University of California, San Francisco
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Participant ID: If you had no responsibilities, what time would your body tell you to go to sleep and wake up?
 What does your sleep look like on a typical week? Total Sleep Time: Bedtime:, Sleep onset latency:, Number of Awakenings:, Wake time after sleep onset:, Rise time:, Out of bed:, Naps:? Notes: Is your sleep
What does your sleep look like on a typical week? Total Sleep Time: Bedtime:, Sleep onset latency:, Number of Awakenings:, Wake time after sleep onset:, Rise time:, Out of bed:, Naps:? Notes: Is your sleep
Sleep and Parkinson's Disease
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Question #1. Disclosures. CAPA 2015 Annual Conference. All of the following occur as we get older EXCEPT: Evaluating Patients with Insomnia
 Evaluating Patients with Roger D. Seheult, M.D. Pulmonary Critical Care Physician - Beaver Medical Group, Redlands California Assistant Clinical Professor of Medicine - Loma Linda University School of
Evaluating Patients with Roger D. Seheult, M.D. Pulmonary Critical Care Physician - Beaver Medical Group, Redlands California Assistant Clinical Professor of Medicine - Loma Linda University School of
Modern Management of Sleep Disorders. If Only I Could Sleep Like I Did Before
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
OPTIMIZING SLEEP TO PERFORM, RECOVER AND THRIVE. Shona Halson, PhD Senior Physiologist Australian Institute of Sport
 OPTIMIZING SLEEP TO PERFORM, RECOVER AND THRIVE Shona Halson, PhD Senior Physiologist Australian Institute of Sport Sleep Elite Sport and Elite Military Vin Walsh, 2014- If one considers the challenges
OPTIMIZING SLEEP TO PERFORM, RECOVER AND THRIVE Shona Halson, PhD Senior Physiologist Australian Institute of Sport Sleep Elite Sport and Elite Military Vin Walsh, 2014- If one considers the challenges
RETT SYNDROME AND SLEEP
 2015 A good night s sleep promotes learning, improved mood, general good health, and a better quality of life for both your child and the whole family. This article written for Rettsyndrome.org by Dr Daniel
2015 A good night s sleep promotes learning, improved mood, general good health, and a better quality of life for both your child and the whole family. This article written for Rettsyndrome.org by Dr Daniel
Milena Pavlova, M.D., FAASM Department of Neurology, Brigham and Women's Hospital Assistant Professor of Neurology, Harvard Medical School Medical
 Milena Pavlova, M.D., FAASM Department of Neurology, Brigham and Women's Hospital Assistant Professor of Neurology, Harvard Medical School Medical Director, Faulkner EEG and Sleep Testing Center Course
Milena Pavlova, M.D., FAASM Department of Neurology, Brigham and Women's Hospital Assistant Professor of Neurology, Harvard Medical School Medical Director, Faulkner EEG and Sleep Testing Center Course
Facts about Sleep. Circadian rhythms are important in determining human sleep patterns/ sleep-waking cycle
 Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Healthy Sleep Tips Along the Way!
 Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
CPT David Shaha, MC US Army
 CPT David Shaha, MC US Army None Thoughts and comments are my own and do not represent the official policy of the Department of the Army, Department of Defense, or United States Government. Clinical Case
CPT David Shaha, MC US Army None Thoughts and comments are my own and do not represent the official policy of the Department of the Army, Department of Defense, or United States Government. Clinical Case
Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment
 Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment Session 1: Introduction and sleep assessment -Assess sleep problem (option: have client complete 20-item sleep questionnaire).
Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment Session 1: Introduction and sleep assessment -Assess sleep problem (option: have client complete 20-item sleep questionnaire).
Many people with physical
 FACTSHEET How to Sleep Better Many people with physical disabilities suffer from sleep disturbances, and sleep tends to become more disrupted as we get older. Not sleeping well can negatively impact your
FACTSHEET How to Sleep Better Many people with physical disabilities suffer from sleep disturbances, and sleep tends to become more disrupted as we get older. Not sleeping well can negatively impact your
Sweet Dreams: The Relationship between Sleep Health and Your Weight
 Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
RECIPES FOR A GOOD NIGHT S SLEEP
 RECIPES FOR A GOOD NIGHT S SLEEP Maribeth Gallagher, PMHNP-BC, MS Hospice of the Valley Objectives: Describe the most common changes in sleep that occur in older adults. Discuss the possible negative effects
RECIPES FOR A GOOD NIGHT S SLEEP Maribeth Gallagher, PMHNP-BC, MS Hospice of the Valley Objectives: Describe the most common changes in sleep that occur in older adults. Discuss the possible negative effects
YOU REALLY NEED TO SLEEP: Several methods to improve your sleep
 YOU REALLY NEED TO SLEEP: Several methods to improve your sleep Sleep is essential to our well-being. When humans fail to get good sleep over a period of time, numerous problems can occur. CAN T SLEEP!!
YOU REALLY NEED TO SLEEP: Several methods to improve your sleep Sleep is essential to our well-being. When humans fail to get good sleep over a period of time, numerous problems can occur. CAN T SLEEP!!
Sleep and mental wellbeing: exploring the links
 Sleep and mental wellbeing: exploring the links Like most physiological functions, the length and quality of sleep is influenced by a host of biological, environmental and lifestyle factors. Across all
Sleep and mental wellbeing: exploring the links Like most physiological functions, the length and quality of sleep is influenced by a host of biological, environmental and lifestyle factors. Across all
OBJECTIVES. The psychiatric, medical, and neurologic causes of sleep problems. Office-based and objective methods of evaluating sleep
 SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
A GUIDE TO BETTER SLEEP. Prepared by Dr Grant Willson Director, Sleep and Lifestyle Solutions
 A GUIDE TO BETTER SLEEP Prepared by Dr Grant Willson Director, Sleep and Lifestyle Solutions A GUIDE TO BETTER SLEEP Good sleep is one of life s pleasures. Most people can think of a time when they slept
A GUIDE TO BETTER SLEEP Prepared by Dr Grant Willson Director, Sleep and Lifestyle Solutions A GUIDE TO BETTER SLEEP Good sleep is one of life s pleasures. Most people can think of a time when they slept
Sleep Hygiene. William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA
 Sleep Hygiene William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA Why Is Sleep Important? Symptoms of Sleep Deprivation: Irritability / Poor Stress
Sleep Hygiene William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA Why Is Sleep Important? Symptoms of Sleep Deprivation: Irritability / Poor Stress
Cognitive behavioural therapy for insomnia
 Cognitive behavioural therapy for insomnia Item type Authors Citation Publisher Journal Article Ruth, Alan Ruth A. Cognitive behavioural therapy for insomnia. Nurs Gen Prac 2014 May 29-30, 32 Nursing in
Cognitive behavioural therapy for insomnia Item type Authors Citation Publisher Journal Article Ruth, Alan Ruth A. Cognitive behavioural therapy for insomnia. Nurs Gen Prac 2014 May 29-30, 32 Nursing in
Pediatric Sleep History
 Fax 423-431-2983 Pediatric Sleep History Patient/ Child s Name: Date of Birth: Parent Name: Last 4 of Social Security No: Gender: Male Female Height: Weight: Age: Race: Street Address: City: State: Zip:
Fax 423-431-2983 Pediatric Sleep History Patient/ Child s Name: Date of Birth: Parent Name: Last 4 of Social Security No: Gender: Male Female Height: Weight: Age: Race: Street Address: City: State: Zip:
Disclosures. Speaker: Teva, UCB, Purdue Advisory Board: Welltrinsic Sleep Network Consultant: Vapotherm, Inc. National Interpretor: Novasom
 So PAP Doesn t Work Rochelle Goldberg, MD, FAASM, FCCP Diplomat, American Board of Sleep Medicine Director Sleep Medicine Services Main Line Health Systems Lankenau Medical Center and Paoli Hospital Disclosures
So PAP Doesn t Work Rochelle Goldberg, MD, FAASM, FCCP Diplomat, American Board of Sleep Medicine Director Sleep Medicine Services Main Line Health Systems Lankenau Medical Center and Paoli Hospital Disclosures
HEALTHY LIFESTYLE, HEALTHY SLEEP. There are many different sleep disorders, and almost all of them can be improved with lifestyle changes.
 HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
September 15, 2017 Pierre, SD End the Insomnia Struggle: An Individualized Approach to Treating Insomnia Using CBT-I and ACT
 September 15, 2017 Pierre, SD End the Insomnia Struggle: An Individualized Approach to Treating Insomnia Using CBT-I and ACT Alisha L. Brosse, Ph.D. Boulder Center for Cognitive & Behavioral Therapies,
September 15, 2017 Pierre, SD End the Insomnia Struggle: An Individualized Approach to Treating Insomnia Using CBT-I and ACT Alisha L. Brosse, Ph.D. Boulder Center for Cognitive & Behavioral Therapies,
Index SLEEP MEDICINE CLINICS. Note: Page numbers of article titles are in boldface type.
 299 SLEEP MEDICINE CLINICS Sleep Med Clin 1 (2006) 299 303 Note: Page numbers of article titles are in boldface type. A Acid reflux, sleep disturbances in older adults related to, 238 Aging, alterations
299 SLEEP MEDICINE CLINICS Sleep Med Clin 1 (2006) 299 303 Note: Page numbers of article titles are in boldface type. A Acid reflux, sleep disturbances in older adults related to, 238 Aging, alterations
Sleep problems 4/10/2014. Normal sleep (lots of variability at all ages) 2 phases of sleep. Quantity. Quality REM. Non-REM.
 2 phases of sleep. Quantity. Quality REM. Non-REM.") Sleep problems Normal sleep (lots of variability at all ages) Quantity Newborns: 16-20 hrs/day 1-yr olds: 12 hrs/day 6-12 yr olds: 10-11 hrs/day Quality Newborns: distributed between day and night 3-months:
Sleep problems Normal sleep (lots of variability at all ages) Quantity Newborns: 16-20 hrs/day 1-yr olds: 12 hrs/day 6-12 yr olds: 10-11 hrs/day Quality Newborns: distributed between day and night 3-months:
Contents. Page. Can t sleep 3. Insomnia 4. Sleep 5. How long should we sleep? 8. Sleep problems 9. Getting a better night s sleep 11
 I Cannot Sleep Contents Page Can t sleep 3 Insomnia 4 Sleep 5 How long should we sleep? 8 Sleep problems 9 Getting a better night s sleep 11 Treatment for insomnia 15 For more information 19 2 Can t sleep
I Cannot Sleep Contents Page Can t sleep 3 Insomnia 4 Sleep 5 How long should we sleep? 8 Sleep problems 9 Getting a better night s sleep 11 Treatment for insomnia 15 For more information 19 2 Can t sleep
일차진료에서불면증치료 김종우. Primary Insomnia : DSM-IV criteria 경희대학교의과대학정신과학교실 MEMO. Diagnostic Criteria for Insomnia (ICSD-2) 개원의와함께하는임상강좌
 개원의와함께하는임상강좌") 개원의와함께하는임상강좌 2011 일차진료에서불면증치료 경희대학교의과대학정신과학교실 김종우 Diagnostic Criteria for Insomnia (ICSD-2) International Classification of Sleep Disorders, 2nd Edition (ICSD-2) Primary Insomnia : DSM-IV criteria A. The
개원의와함께하는임상강좌 2011 일차진료에서불면증치료 경희대학교의과대학정신과학교실 김종우 Diagnostic Criteria for Insomnia (ICSD-2) International Classification of Sleep Disorders, 2nd Edition (ICSD-2) Primary Insomnia : DSM-IV criteria A. The
노인병원에서 Light Therapy 의 활용 박 기 형 진주삼성병원 송도병원 신경과
 Light Therapy 1 : 15 / 63 (23.8%) 1 : 7 2 : 8 : 6 / 86 (7%) 1, : 48 / 205 (23.4%) 1 : 43 2 : 5 Sleep in Geriatrics Prevalence NIH survey of 9000 american senior above age 65 ; 88% had sleep disturbances
Light Therapy 1 : 15 / 63 (23.8%) 1 : 7 2 : 8 : 6 / 86 (7%) 1, : 48 / 205 (23.4%) 1 : 43 2 : 5 Sleep in Geriatrics Prevalence NIH survey of 9000 american senior above age 65 ; 88% had sleep disturbances
Grade: 66.7% Attempt Number: 1/3 Questions Attempted: 27/27
 1. While assessing a client, the nurse notes that the client s body language seems to convey a message of helplessness, as if the client were saying, Take care of me. Which theory describes somatization
1. While assessing a client, the nurse notes that the client s body language seems to convey a message of helplessness, as if the client were saying, Take care of me. Which theory describes somatization
Managing Insomnia Disorder A Review of the Research for Adults
 Managing Insomnia Disorder A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional said you have insomnia disorder (said
Managing Insomnia Disorder A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional said you have insomnia disorder (said
RESTore TM. Clinician Manual for Single User. Insomnia and Sleep Disorders. A step by step manual to help you guide your clients through the program
 RESTore TM Insomnia and Sleep Disorders Clinician Manual for Single User A step by step manual to help you guide your clients through the program Version 10 July, 2016 Table of Contents Introduction...
RESTore TM Insomnia and Sleep Disorders Clinician Manual for Single User A step by step manual to help you guide your clients through the program Version 10 July, 2016 Table of Contents Introduction...
Sleep in ME/CFS and FM. W. Jerome Alonso, MD, CCFP, DABFM (Sleep Medicine)
") Sleep in ME/CFS and FM W. Jerome Alonso, MD, CCFP, DABFM (Sleep Medicine) Medical Director, Canadian Sleep Consultants Clinical Assistant Professor, University of Calgary Board Certified in Sleep Medicine,
Sleep in ME/CFS and FM W. Jerome Alonso, MD, CCFP, DABFM (Sleep Medicine) Medical Director, Canadian Sleep Consultants Clinical Assistant Professor, University of Calgary Board Certified in Sleep Medicine,
A good night s sleep. The aim of this booklet A Practical Guide: About A good night s sleep is to assist people get a better night s sleep.
 59124- F-A Sleep ENG 5/8/05 8:38 AM Page 1 A practical guide about: A good night s sleep (ENGLISH) A Division of the Diversity Health Institute The aim of this booklet A Practical Guide: About A good night
59124- F-A Sleep ENG 5/8/05 8:38 AM Page 1 A practical guide about: A good night s sleep (ENGLISH) A Division of the Diversity Health Institute The aim of this booklet A Practical Guide: About A good night
Not Sleeping Well? Chronic physical conditions. There May Be a Medical Cause. Diabetes. Heartburn
 Not Sleeping Well? There May Be a Medical Cause People who feel they sleep perfectly well may still be troubled by excessive daytime sleepiness because of a variety of underlying medical illnesses. A sleep
Not Sleeping Well? There May Be a Medical Cause People who feel they sleep perfectly well may still be troubled by excessive daytime sleepiness because of a variety of underlying medical illnesses. A sleep
Sleep Management
 www.working-minds.org.uk Sleep Management Working Minds UK: Dovey Wilday Consultancy Contact: 07941 196379 SLEEP MANAGEMENT Sleep problems occur frequently in people suffering from depression/anxiety.
www.working-minds.org.uk Sleep Management Working Minds UK: Dovey Wilday Consultancy Contact: 07941 196379 SLEEP MANAGEMENT Sleep problems occur frequently in people suffering from depression/anxiety.
CONQUERING INSOMNIA & ACHIEVING SLEEP WELLNESS
 CONQUERING INSOMNIA & ACHIEVING SLEEP WELLNESS "Sleep is the golden chain that ties health and our bodies together." ~ Thomas Dekker ~ Under recognized & Under treated Insomnia Facts Negatively Affects
CONQUERING INSOMNIA & ACHIEVING SLEEP WELLNESS "Sleep is the golden chain that ties health and our bodies together." ~ Thomas Dekker ~ Under recognized & Under treated Insomnia Facts Negatively Affects
8/29/2013. Discuss Relation of Fatigue to Sleep Disturbance. Assessing and Treating Factors Contributing to Fatigue and Sleep Disturbance
 Timothy Pearman, Ph.D. Director, Supportive Oncology Robert H. Lurie Comprehensive Cancer Center Associate Professor of Medical Social Sciences and Psychiatry Northwestern University Feinberg School of
Timothy Pearman, Ph.D. Director, Supportive Oncology Robert H. Lurie Comprehensive Cancer Center Associate Professor of Medical Social Sciences and Psychiatry Northwestern University Feinberg School of
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute
 Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Clinical Guideline for the Evaluation and Management of Chronic Insomnia in Adults
 Special Article Clinical Guideline for the Evaluation and Management of Chronic Insomnia in Adults Sharon Schutte-Rodin, M.D. 1 ; Lauren Broch, Ph.D. 2 ; Daniel Buysse, M.D. 3 ; Cynthia Dorsey, Ph.D. 4
Special Article Clinical Guideline for the Evaluation and Management of Chronic Insomnia in Adults Sharon Schutte-Rodin, M.D. 1 ; Lauren Broch, Ph.D. 2 ; Daniel Buysse, M.D. 3 ; Cynthia Dorsey, Ph.D. 4
Pittsburgh Insomnia Rating Scale University of Pittsburgh School of Medicine, Department of Psychiatry, All Rights Reserved.
 Pittsburgh Insomnia Rating Scale University of Pittsburgh School of Medicine, Department of Psychiatry, 2001. All Rights Reserved. Name ID# Date A. Overall sleep quality: Consider the quality of your sleep
Pittsburgh Insomnia Rating Scale University of Pittsburgh School of Medicine, Department of Psychiatry, 2001. All Rights Reserved. Name ID# Date A. Overall sleep quality: Consider the quality of your sleep
Objectives. Disclosure. APNA 26th Annual Conference Session 2017: November 8, Kurtz 1. The speaker has no conflicts of interest to disclose
 Christine Kurtz, DNP, PMHCNS BC Valparaiso University Disclosure The speaker has no conflicts of interest to disclose Objectives The learner will Describe the rationale for and five therapies of CBT I
Christine Kurtz, DNP, PMHCNS BC Valparaiso University Disclosure The speaker has no conflicts of interest to disclose Objectives The learner will Describe the rationale for and five therapies of CBT I
Original Sleep Hygiene Rules*
 Original Sleep Hygiene Rules* 1. Sleep as much as needed to feel refreshed and healthy during the following day, but not more. Curtailing time in bed a bit seems to solidify sleep; excessively long times
Original Sleep Hygiene Rules* 1. Sleep as much as needed to feel refreshed and healthy during the following day, but not more. Curtailing time in bed a bit seems to solidify sleep; excessively long times
Zopiclone Orion. Date: , Version 1.2 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN
 Zopiclone Orion Date: 16-11-2016, Version 1.2 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Insomnia (i.e. sleeplessness) is a common
Zopiclone Orion Date: 16-11-2016, Version 1.2 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Insomnia (i.e. sleeplessness) is a common
th Ave NE Suite F Bellevue, WA Phone: (425) Fax: (425) Excessive Daytime Sleepiness
 Fax: (425) Excessive Daytime Sleepiness") 1414 116 th Ave NE Suite F Bellevue, WA 98004 Phone: (425) 451-8417 Fax: (425) 455-4089 Excessive Daytime Sleepiness Nearly everyone has days when they feel sleepy. But for some people, excessive sleepiness
1414 116 th Ave NE Suite F Bellevue, WA 98004 Phone: (425) 451-8417 Fax: (425) 455-4089 Excessive Daytime Sleepiness Nearly everyone has days when they feel sleepy. But for some people, excessive sleepiness
Sleep Disorders. Guidance for Primary Care. National Advisory Group for Respiratory Managed Clinical Networks
 Sleep Disorders Guidance for Primary Care National Advisory Group for Respiratory Managed Clinical Networks Presentation Patient complaining of difficulty sleeping, ongoing fatigue, poor concentration
Sleep Disorders Guidance for Primary Care National Advisory Group for Respiratory Managed Clinical Networks Presentation Patient complaining of difficulty sleeping, ongoing fatigue, poor concentration
How to Help Your Clients Get Better Sleep
 How to Help Your Clients Get Better Sleep Bonus Video 1 10-Point Checklist for Getting Better Sleep with Rubin Naiman, PhD How to Help Your Clients Get Better Sleep 2 10-Point Checklist for Getting Better
How to Help Your Clients Get Better Sleep Bonus Video 1 10-Point Checklist for Getting Better Sleep with Rubin Naiman, PhD How to Help Your Clients Get Better Sleep 2 10-Point Checklist for Getting Better
Objectives. Types of Sleep Problems in Developmental Disorders
 Objectives Sleep Problems in the Child with Neurodevelopmental Disorders AACPDM September 11, 2014 BRK-3 Golda Milo-Manson MD, MHSc, FRCP(C) Holland Bloorview Kids Rehabilitation Hospital Toronto, Canada
Objectives Sleep Problems in the Child with Neurodevelopmental Disorders AACPDM September 11, 2014 BRK-3 Golda Milo-Manson MD, MHSc, FRCP(C) Holland Bloorview Kids Rehabilitation Hospital Toronto, Canada
PRACTICAL MANAGEMENT OF INSOMNIA IN THE OFFICE
 PRACTICAL MANAGEMENT OF INSOMNIA IN THE OFFICE NORAH VINCENT, PHD., C. PSYCH. PSYCHOLOGIST, WINNIPEG REGIONAL HEALTH AUTHORITY PROFESSOR, DEPARTMENT OF CLINICAL HEALTH PSYCHOLOGY, UNIVERSITY OF MANITOBA
PRACTICAL MANAGEMENT OF INSOMNIA IN THE OFFICE NORAH VINCENT, PHD., C. PSYCH. PSYCHOLOGIST, WINNIPEG REGIONAL HEALTH AUTHORITY PROFESSOR, DEPARTMENT OF CLINICAL HEALTH PSYCHOLOGY, UNIVERSITY OF MANITOBA
Diagnosis and treatment of sleep disorders
 Diagnosis and treatment of sleep disorders Normal human sleep Sleep cycle occurs about every 90 minutes, approximately 4-6 cycles occur per major sleep episode NREM (70-80%) slow wave sleep heart rate,
Diagnosis and treatment of sleep disorders Normal human sleep Sleep cycle occurs about every 90 minutes, approximately 4-6 cycles occur per major sleep episode NREM (70-80%) slow wave sleep heart rate,
Dr Alex Bartle. Director Sleep Well Clinic
 Dr Alex Bartle Director Sleep Well Clinic 1 Fatigue in the Workforce The structure of sleep Fatigue and sleep Consequences of fatigue Management of Shiftwork Conclusion Sleep Architecture REM NREM Rapid
Dr Alex Bartle Director Sleep Well Clinic 1 Fatigue in the Workforce The structure of sleep Fatigue and sleep Consequences of fatigue Management of Shiftwork Conclusion Sleep Architecture REM NREM Rapid
Sleep. Information booklet. RDaSH. Adult Mental Health Services
 Sleep Information booklet RDaSH Adult Mental Health Services Sleep problems are often referred to as insomnia. They are very common, particularly in women, children and people over 65, so it is quite normal
Sleep Information booklet RDaSH Adult Mental Health Services Sleep problems are often referred to as insomnia. They are very common, particularly in women, children and people over 65, so it is quite normal