OSA and Hypertension Scope of the Problem
|
|
|
- Kathlyn Jordan
- 6 years ago
- Views:
Transcription

1 OSA and Hypertension Scope of the Problem Dr Ahmad Izuanuddin Ismail Senior Lecturer & Respiratory Physician Faculty of Medicine, Universiti Teknologi MARA
2 Outline Does OSA cause daytime HTN, and if so, by what mechanism How to diagnose OSA in patients with HTN, and vice versa Does increased BP in OSA affect target organs Does treatment of OSA decrease BP Which antihypertensive should be use to treat HTN in OSA patients MSH 2014
3 OSA is an independent risk for hypertension and effective CPAP therapy can reduce the blood pressure MSH 2014

4 Obstructive Sleep Apnoea Intermittent hypoxia, sleep fragmentation, increased respiratory efforts Intermittent Hypoxia Reduction or cessation of flow Increase in respiratory effort Cardiovascular activation Arousal MSH 2014

5 Clinical OSA: Just the Tip of the Iceberg Clinical OSA Diagnosed cases Subclinical OSA Undiagnosed cases millions at risk Obesity and ageing; lack of awareness; scgma MSH2014
6 Prevalence of OSA US adults (Punjabi 2008, Young 1997, Hu 1999) 9 50% of males and 4 17% of females reported snoring Clinically significant OSA 3-7% for adult males and 2-5% for adult females 75% of severe OSA remains undiagnosed MSH 2014
 ESS>11 OSAS- loud snoring, breathing")
7 Snoring and breathing pauses during sleep in the Malaysian popula4on Kamil et al Respirology 2007 N= 1611 adults years old, cross secconal populacon based survey DefiniCon: Snoring- self report with confirmacon from bed partner Habitual snoring snores 3 or more nights a week Loud habitual snoring louder than talking Excessive daycme sleepiness (EDS) ESS>11 OSAS- loud snoring, breathing pauses (with or without without choking or gasping) and EDS Male (n = 853) Female (n = 758) All respondents (n = 1611) Non-snoring Snoring* Habitual snoring** Loud habitual snoring** Sleeping pauses** Excessive daytime sleepiness* Clinically suspected OSAS* Univariate analysis for comparison between genders. *P < 0.05, **P <
8 Sleep apnoea prevalence in CV diseases MSH 2014 Courtesy of Patrick Levy, ERS2012
9 Sleep Apnoea Cardiovascular Risk Several Ongoing Epidemiological Studies 1. Sleep Heart Health Study Community dwelling middle-aged men and women across the United States 2. Wisconsin Sleep Cohort Study Population based sample of working men and women from Wisconsin MSH 2014
10 The Sleep Heart Health Study Design: Prospective cohort study Multi-center Assessment of sleep on to ongoing cohort studies of cardiovascular and respiratory disease Wide geographic and ethnic representation of middle-aged and older US adults Quan et al: The Sleep Heart Health Study: Design, Methods, Rationale Sleep 1997; 20(12)
11 The SHHS: Field Sites Baseline N = 6441 Minneapolis (1085) Framingham (1000) Sacramento (501) South Dakota (201) Pittsburgh (398) Hagerstown (1184) New York (760) Phoenix (201) Tucson (911) Oklahoma (200) National Heart Lung and Blood Institute (NHLBI). The Sleep Heart Health Study: Manuals of Operation. demographics/01jul02received/shhs1demo1jul02.pdf. Accessed July 18, 2007.
12 Outcome and Covariate Data Prevalent disease Cardiovascular disease, myocardial infarction, stroke, angina, PTCA, congestive heart failure, hypertension, diabetes, asthma and COPD Demographic Age, race, education, marital status, occupation, etc. Health Habits Smoking, alcohol use, caffeine, etc. Quan et al: The Sleep Heart Health Study: Design, Methods, Rationale Sleep 1997; 20(12)
13 Outcome and Covariate Data Anthropometrics (BMI, waist girth, hip circumferences) Medication use (prescription and non-prescription) Electrocardiogram Subset of the cohort Echocardiogram Holter data Head MRI scans Physical activity Serum (fasting, non-fasting, post glucose challenge) Spirometry Quan et al: The Sleep Heart Health Study: Design, Methods, Rationale Sleep 1997; 20(12)
14 SHHS: Longitudinal Design Baseline PSG (N = 6441) Follow-up PSG (N = 3291) Continuous Outcome Surveillance Outcome Surveillance Censoring Date April 1, 2006 End of Follow-up MSH 2014
15 Sleep Apnoea and Hypertension Adjusted odds ratio for prevalent hypertension AHI (events/hr) Odds ratio 95% CI < Reference > Adjusted for age, sex, ethnicity, BMI, neck, waist/hip ratio, alcohol use, and smoking Nieto et al. Association of Sleep-disordered breathing, sleep apnea, and hypertension in a large community-based sample. JAMA 2000; 283(14):

16 Sleep apnea and Incident Hypertension O Connor et al. Am J Respir Crit Care Med Vol 179. pp , 2009 MSH 2014

17 Sleep apnea and Incident Hypertension O Connor et al. Am J Respir Crit Care Med Vol 179. pp , 2009
18 Incident Hypertension in SDB n=1889 Marin J. JAMA 2012; 307:2169
19 % controlled HT OSA and refractory hypertension < > HT - Relationship between OSA and HT severity 80% of OSA patients among refractory HT Grote, J Hypertens Logan, Hypertension /90 mm Hg 160/95 mm Hg
20 Outline Does OSA cause daytime HTN, and if so, by what mechanism How to diagnose OSA in patients with HTN, and vice versa Does increased BP in OSA affect target organs Does treatment of OSA decrease BP Which antihypertensive should be use to treat HTN in OSA patients MSH 2014


21 Mechanisms of Hypertension in OSA Foster GE et al. Exp Physiol 2007;92;51-65
22 OSA Causes Increased Sympathetic Tone MSH 2014 Somers VK. J C. J Clin Invest :189
23 OSA Intermittent hypoxia Sleep fragmentation Intrathoracic pressure swings Hypercapnia? Obesity Oxidative stress Systemic inflammation Sympathetic excitation Endothelial dysfunction Metabolic dysregulation Cardiovascular disease MSH 2014 Levy et al Eur Respir Rev 2013
24 Outline Does OSA cause daytime HTN, and if so, by what mechanism How to diagnose OSA in patients with HTN, and vice versa Does increased BP in OSA affect target organs Does treatment of OSA decrease BP Which antihypertensive should be use to treat HTN in OSA patients MSH 2014
 EVALUATION CLASSIFICATION OF BLOOD BRESSURE (BP)* CATEGORY SBP MMHG DBP MMHG Normal <120 and <80 Prehypertension 120-139 or 80-89 Hypertension, stage 1 140-159 or 90-99")

25 Reference Card from the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) Sleep Apnea is an Identifiable Cause of Hypertension NIH, JNC7 (2003) EVALUATION CLASSIFICATION OF BLOOD BRESSURE (BP)* CATEGORY SBP MMHG DBP MMHG Normal <120 and <80 Prehypertension or Hypertension, stage or Hypertension, stage 2 >_ or >_ Key: SBP = systolic blood pressure DBP = diastolic blood pressure DIAGNOSTIC WORKUP OF HYPERTENSION Assess risk factors and comorbidities. Reveal identifiable causes of hypertension. Assess presence of target organ damage. Conduct history and physical examination. Obtain laboratory tests; urinalysis, blood glucose, hematocrit and lipid panel, serum potassium, creatinine, and calcium. Optional: urinary albumin/ creatinine ratio. Obtain electrocardiogram. ASSESS FOR MAJOR CARDIOVASCULAR DISEASE (CVD) RISK FACTORS Hypertension Physical inactivity Obesity Microalbuminuria, estimated (body mass index >_ 30 kg/m 2 glomerular filtration rate <60 ml/min Dyslipidemia Age (>55 for men, >65 for women) Diabetes mellitus Family history of premature CVD Cigarette smoking (men age <55, women age <65) ASSESS FOR IDENTIFIABLE CAUSES OF HYPERTENSION Sleep apnea Drug induced/related Cushing s syndrome or steroid therapy Chronic kidney disease Pheochromocytoma Primary aldosteronism Coarctation of aorta Renovascular disease Thyroid/parathyroid disease TREATMENT PRINCIPLES OF HYPERTENSION TREATMENT Treat to BP <140/90 mmhg or BP <130/80 mmhg in patients with diabetes or chronic kidney disease. Majority of patients will require two medications to reach goal. ALGORITHM FOR TREATMENT OF HYPERTENSION Stage 1 Hypertension (SBP or DBP mmhg) Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. LIFESTYLE MODIFICATIONS Not at Goal Blood Pressure (<140/90 mmhg) (<130/80 mmhg for patients with diabetes or chronic kidney disease) Without Compelling Indications INITIAL DRUG CHOICES Stage 2 Hypertension (SBP >_ 160 or DBP >_ 100 mmhg) 2-drug combination for most (usually thiazidetype diuretic and ACEI, or ARB, or BB, or CCB). With Compelling Indications Drug(s) for the compelling indications See Compelling Indications for Individual Drug Classes Other antihpertensive drugs (diuretics, ACEI, ARB, BB CCB) as needed. NOT AT GOAL BLOOD PRESSURE Optimize dosages or add additional drugs until goal blood pressure is achieved. Consider consultation with hypertension specialist. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health National Heart, Lung, and Blood Institute
 Sleep apnoea")

26 February 2008 MOH/P/PAK/ (GU) Table 2. Secondary causes of hypertension Clinical Practice Guidelines Management of Hypertension (3rd Edition) Sleep apnoea Drug-induced or drug-related Chronic kidney disease Primary aldosteronism Renovascular disease Chronic steroid therapy and Cushing syndrome Phaeochromocytoma Acromegaly Thyroid or parathyroid disease Coarctation of the aorta Takayasu Arteritis Ministry of Health Malaysia Academy of Medicine of Malaysia Malaysian Society of Hypertension
27 OSAHS A or B, and C Obstructive Sleep Apnoea Hypopnoea Syndrome A Excessive Daytime Sleepiness B At least two of the following items Nocturnal gasping or breathing arrests Frequent awakenings Unrefreshing sleep Daytime fatigue Loss of concentration C - > 5 obstructive breathing episodes per hour during sleep MSH 2014

28 ERS/ESH Task Force Report 2013 MSH 2014
29 Outline Does OSA cause daytime HTN, and if so, by what mechanism What is the best method to measure BP in OSA patients Does increased BP in OSA affect target organs Does treatment of OSA decrease BP Which antihypertensive should be use to treat HTN in OSA patients MSH 2014

30 Gottlieb et al. Circulation 2010; 122:
31 Sleep Apnea: Incident CVD Men: Age < 70 years Outcome Predictor Variable Hazard Ratio 95 % CI Incident CVD AHI < 5 vs. AHI > AHI continuous (per 10 unit increase) Gottlieb et al. Circulation 2010; 122:
32 Prospective Study of OSA and Incident CHD and HF Sleep Heart and Health Study OSA have a 58% higher adjusted risk of incident HF Gottlieb DJ et al. Circulation. 2010;122:

33 Cardiovascular mortality
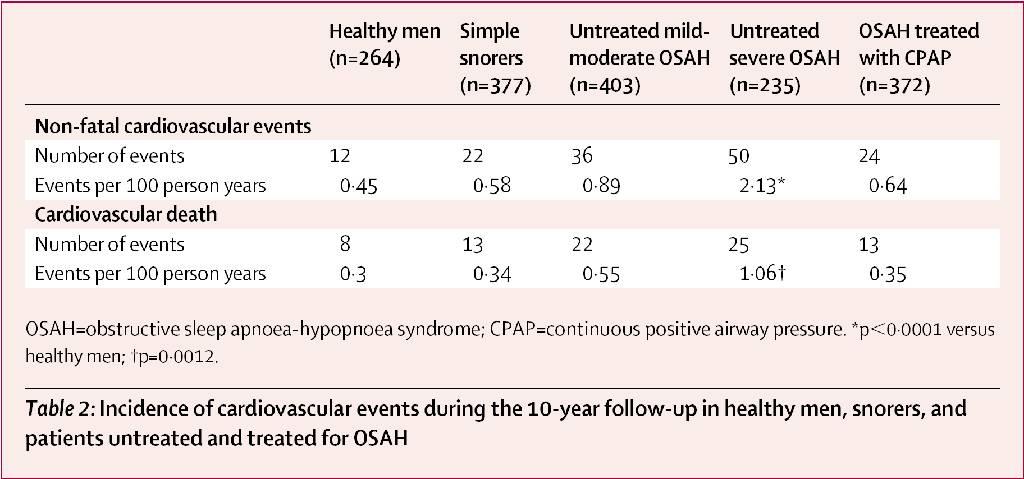
34 Sleep Apnea and Fatal Cardiovascular Events Months Marin et al. Lancet 2005
35 Effects of CPAP Therapy on CVD Marin et al. Lancet 2005 MSH 2014
36 Sleep Apnea and CVD Cross-sectional data suggest a significant and independent association between sleep apnea and prevalent CAD and CHF Untreated sleep apnea is associated with increased odds of developing CAD and CHF In patients with CAD, untreated sleep apnea is associated with increased death rate MSH 2014
37 Outline Does OSA cause daytime HTN, and if so, by what mechanism What is the best method to measure BP in OSA patients Does increased BP in OSA affect target organs Does treatment of OSA decrease BP Which antihypertensive should be use to treat HTN in OSA patients MSH 2014
38 Randomized Clinical Trial of CPAP on BP Double-blind randomized trial (118 men) Sleep Apnea: ODI > 10 events/hr + Epworth score > 9 Sub-therapeutic vs. therapeutic CPAP 24-hr ambulatory blood pressure (baseline and 4-wks post Rx) Mean BP: 2.5 mmhg (CPAP) vs mmhg (sham) Pepperell et al. Lancet. 2002;359(9302):
39 Before CPAP intervention After CPAP intervention
 Becker HF.")
40 CPAP Lowers BP in SDB 9 Weeks CPAP (n=16) Placebo (n=16) Becker HF. Circulation; 2003; 107:68
41 Effect Of CPAP On Incident Hypertension Or CV Events In SDB Without EDS (n=725) Barbé F. JAMA 2012; 307:2161
42 ." CPAP and Blood Pressure Meta-Analysis Haentjens P, Arch Intern Med 2007
43 Significant correla4on between the improvement in night- 4me blood BP and the dura4on of CPAP use
44 Factors affecting BP reduction by CPAP therapy in OSA patients Presence or absence of daytime sleepiness OSA severity Blood pressure levels before treatment Resistant hypertension Patients age and sex Duration of treatment CPAP proper titration Patients compliance with CPAP treatment MSH 2014
45 Outline Does OSA cause daytime HTN, and if so, by what mechanism What is the best method to measure BP in OSA patients Does increased BP in OSA affect target organs Does treatment of OSA decrease BP Which antihypertensive should be use to treat HTN in OSA patients MSH 2014
46 Antihypertensives for OSA patients In patients with untreated OSA and hypertension, BP lowering drugs effectively reduced daytime BP, without clear differences between different classes of medications (Zou et al Sleep Med 2010) Normalisation of BP during daytime can be easily achieved, but CPAP treatment is necessary to eliminate BP fluctuations at night MSH 2014
47 Addi4ve effects of CPAP and Valsartan a) SBP mmhg b) DBP mmhg :00 11:00 13:00 15:00 17:00 19:00 21:00 23:00 01:00 03:00 05:00 07:00 09:00 Time h Pepin AJRCCM 2010
48 Take Home Message Obstructive sleep apnea is an independent risk factor for the development of systemic hypertension Hypertension associated with obstructive sleep apnea may be relatively resistant to drug therapy In hypertensive patients with obstructive sleep apnea, specific therapy of obstructive sleep apnea may reduce blood pressure MSH 2014

49 Quantity and Quality of Sleep are Paramount for Human Health

50 MSH 2014
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Heart Failure and Sleep Disordered Breathing (SDB) Unhappy Bedfellows
 Unhappy Bedfellows") Question Heart Failure and Sleep Disordered Breathing (SDB) Unhappy Bedfellows 1 ResMed 2012 07 2 ResMed 2012 07 Open Airway 3 ResMed 2012 07 Flow Limitation Snore 4 ResMed 2012 07 Apnoea 5 ResMed 2012
Question Heart Failure and Sleep Disordered Breathing (SDB) Unhappy Bedfellows 1 ResMed 2012 07 2 ResMed 2012 07 Open Airway 3 ResMed 2012 07 Flow Limitation Snore 4 ResMed 2012 07 Apnoea 5 ResMed 2012
General Outline. General Outline. Pathogenesis of Metabolic Dysfunction in Sleep Apnea: The Role of Sleep Fragmentation and Intermittent Hypoxemia
 Pathogenesis of Metabolic in Sleep Apnea: The Role of Sleep Fragmentation and Intermittent Hypoxemia Naresh M. Punjabi, MD, PhD Associate Professor of Medicine and Epidemiology Johns Hopkins University,
Pathogenesis of Metabolic in Sleep Apnea: The Role of Sleep Fragmentation and Intermittent Hypoxemia Naresh M. Punjabi, MD, PhD Associate Professor of Medicine and Epidemiology Johns Hopkins University,
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Sleep apnea as a risk factor for cardiovascular disease
 Sleep apnea as a risk factor for cardiovascular disease Malcolm Kohler Chair Respiratory Medicine, Clinical Director, Department of Pulmonology, University Hospital Zurich Incidence of fatal cardiovascular
Sleep apnea as a risk factor for cardiovascular disease Malcolm Kohler Chair Respiratory Medicine, Clinical Director, Department of Pulmonology, University Hospital Zurich Incidence of fatal cardiovascular
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential
DECLARATION OF CONFLICT OF INTEREST Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Co-Morbidities Associated with OSA
 Co-Morbidities Associated with OSA Dr VK Vijayan MD (Med), PhD (Med), DSc, FCCP, FICC, FAPSR, FAMS Advisor to Director General, ICMR Bhopal Memorial Hospital and Research Centre & National Institute for
Co-Morbidities Associated with OSA Dr VK Vijayan MD (Med), PhD (Med), DSc, FCCP, FICC, FAPSR, FAMS Advisor to Director General, ICMR Bhopal Memorial Hospital and Research Centre & National Institute for
Obstructive sleep apnoea How to identify?
 Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential conflict of interest None Obstructive
Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential conflict of interest None Obstructive
Sleep Apnea: Vascular and Metabolic Complications
 Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Obstructive sleep apnea and hypertension: why treatment does not consistently improve blood pressure?
 Martino F. Pengo MD, PhD 7 & 8 décembre 2018, Berlin Obstructive sleep apnea and hypertension: why treatment does not consistently improve blood pressure? Sleep Disorder Center Department of Cardiovascular,
Martino F. Pengo MD, PhD 7 & 8 décembre 2018, Berlin Obstructive sleep apnea and hypertension: why treatment does not consistently improve blood pressure? Sleep Disorder Center Department of Cardiovascular,
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Circadian Variations Influential in Circulatory & Vascular Phenomena
 SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
Snoring and Its Outcomes
 Disclosures None Snoring and Its Outcomes Jolie Chang, MD Otolaryngology, Head and Neck Surgery University of California, San Francisco February 14, 2014 Otolaryngology Head Outline Snoring and OSA Acoustics
Disclosures None Snoring and Its Outcomes Jolie Chang, MD Otolaryngology, Head and Neck Surgery University of California, San Francisco February 14, 2014 Otolaryngology Head Outline Snoring and OSA Acoustics
Obstructive Sleep Apnea
 Obstructive Sleep Apnea Definition: Repetitive episodes of upper airway obstruction (complete or partial) that occur during sleep and are associated with arousals or desaturations +/or daytime sleepiness.
Obstructive Sleep Apnea Definition: Repetitive episodes of upper airway obstruction (complete or partial) that occur during sleep and are associated with arousals or desaturations +/or daytime sleepiness.
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Management of OSA in the Acute Care Environment. Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018
 Management of OSA in the Acute Care Environment Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018 1 Learning Objectives Upon completion, the participant should be able to: Understand pathology
Management of OSA in the Acute Care Environment Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018 1 Learning Objectives Upon completion, the participant should be able to: Understand pathology
MCOEM Spring Chapter Meeting April 5, Sleep Apnea An Overview with Emphasis on Cardiovascular Correlations Jacques Conaway, MD
 MCOEM Spring Chapter Meeting April 5, 2014 Sleep Apnea An Overview with Emphasis on Cardiovascular Correlations Jacques Conaway, MD Case Presentation History of Present Illness 57 year old man with ihh/
MCOEM Spring Chapter Meeting April 5, 2014 Sleep Apnea An Overview with Emphasis on Cardiovascular Correlations Jacques Conaway, MD Case Presentation History of Present Illness 57 year old man with ihh/
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Sleep Apnea in Women: How Is It Different?
 Sleep Apnea in Women: How Is It Different? Grace Pien, MD, MSCE Division of Pulmonary and Critical Care Department of Medicine Johns Hopkins School of Medicine 16 February 2018 Outline Prevalence Clinical
Sleep Apnea in Women: How Is It Different? Grace Pien, MD, MSCE Division of Pulmonary and Critical Care Department of Medicine Johns Hopkins School of Medicine 16 February 2018 Outline Prevalence Clinical
The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome
 The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome Natsios Georgios University Hospital of Larissa, Greece Definitions Obstructive Sleep Apnea (OSA)
The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome Natsios Georgios University Hospital of Larissa, Greece Definitions Obstructive Sleep Apnea (OSA)
Sleep and the Heart. Physiologic Changes in Cardiovascular Parameters during Sleep
 Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart. Rami N. Khayat, MD
 Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Sleep Disordered Breathing: Beware Snoring! Dr T A McDonagh Consultant Cardiologist Royal Brompton Hospital London. UK
 Sleep Disordered Breathing: Beware Snoring! Dr T A McDonagh Consultant Cardiologist Royal Brompton Hospital London. UK Sleep Disordered Breathing in CHF Erratic breathing during sleep known for years e.g.
Sleep Disordered Breathing: Beware Snoring! Dr T A McDonagh Consultant Cardiologist Royal Brompton Hospital London. UK Sleep Disordered Breathing in CHF Erratic breathing during sleep known for years e.g.
Mario Kinsella MD FAASM 10/5/2016
 Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Sleep Apnoea : its impact outside the chest. Dr Tom Mackay Consultant Respiratory Physician Royal Infirmary Edinburgh
 Sleep Apnoea : its impact outside the chest Dr Tom Mackay Consultant Respiratory Physician Royal Infirmary Edinburgh Body Mass Index < 20 kg/m 2 20-25 kg/m 2 25-30 kg/m 2 > 30 kg/m 2 underweight normal
Sleep Apnoea : its impact outside the chest Dr Tom Mackay Consultant Respiratory Physician Royal Infirmary Edinburgh Body Mass Index < 20 kg/m 2 20-25 kg/m 2 25-30 kg/m 2 > 30 kg/m 2 underweight normal
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
PVDOMICS. Sleep Core. Cleveland Clinic Cleveland, Ohio
 PVDOMICS Sleep Core Rawan Nawabit, Research Coordinator and Polysomnologist Joan Aylor, Research Coordinator Dr. Reena Mehra, Co-Investigator, Sleep Core Lead Cleveland Clinic Cleveland, Ohio 1 Obstructive
PVDOMICS Sleep Core Rawan Nawabit, Research Coordinator and Polysomnologist Joan Aylor, Research Coordinator Dr. Reena Mehra, Co-Investigator, Sleep Core Lead Cleveland Clinic Cleveland, Ohio 1 Obstructive
Blood Pressure Monitoring in Chronic Kidney Disease
 Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
GOALS. Obstructive Sleep Apnea and Cardiovascular Disease (OVERVIEW) FINANCIAL DISCLOSURE 2/1/2017
 FINANCIAL DISCLOSURE 2/1/2017") Obstructive Sleep Apnea and Cardiovascular Disease (OVERVIEW) 19th Annual Topics in Cardiovascular Care Steven Khov, DO, FAAP Pulmonary Associates of Lancaster, Ltd February 3, 2017 skhov2@lghealth.org
Obstructive Sleep Apnea and Cardiovascular Disease (OVERVIEW) 19th Annual Topics in Cardiovascular Care Steven Khov, DO, FAAP Pulmonary Associates of Lancaster, Ltd February 3, 2017 skhov2@lghealth.org
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
OSA and cardiovascular disease what is the evidence? Mohan Edupuganti, MD, FACC. Baptist Health Cardiology. Disclosures: None
 OSA and cardiovascular disease what is the evidence? Mohan Edupuganti, MD, FACC. Baptist Health Cardiology. Disclosures: None 1 OSA basics Affects 20-30% of males and 10-15% of females in North America
OSA and cardiovascular disease what is the evidence? Mohan Edupuganti, MD, FACC. Baptist Health Cardiology. Disclosures: None 1 OSA basics Affects 20-30% of males and 10-15% of females in North America
In-Patient Sleep Testing/Management Boaz Markewitz, MD
 In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Sleep Apnea: Diagnosis & Treatment
 Disclosure Sleep Apnea: Diagnosis & Treatment Lawrence J. Epstein, MD Sleep HealthCenters Harvard Medical School Chief Medical Officer for Sleep HealthCenters Sleep medicine specialty practice group Consultant
Disclosure Sleep Apnea: Diagnosis & Treatment Lawrence J. Epstein, MD Sleep HealthCenters Harvard Medical School Chief Medical Officer for Sleep HealthCenters Sleep medicine specialty practice group Consultant
Sleep Apnea and Heart Failure
 Sleep Apnea and Heart Failure Micha T. Maeder, MD Cardiology Division Kantonsspital St. Gallen Switzerland micha.maeder@kssg.ch Sleep Disordered Breathing (SDB) in HFrEF 700 HFrEF patients (LVEF
Sleep Apnea and Heart Failure Micha T. Maeder, MD Cardiology Division Kantonsspital St. Gallen Switzerland micha.maeder@kssg.ch Sleep Disordered Breathing (SDB) in HFrEF 700 HFrEF patients (LVEF
Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease
 1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
2/19/2013. Cardiovascular Disease Prevention International Symposium. Cardiovascular Disease and Sleep Apnea. Still Controversial?
 Cardiovascular Disease Prevention International Symposium Cardiovascular Disease and Sleep Apnea February 16, 2013 Jonathan A. Fialkow, M.D., FACC, FAHA Medical Director, Clinical Cardiology, Baptist Cardiac
Cardiovascular Disease Prevention International Symposium Cardiovascular Disease and Sleep Apnea February 16, 2013 Jonathan A. Fialkow, M.D., FACC, FAHA Medical Director, Clinical Cardiology, Baptist Cardiac
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
TIP. Documentation and coding guide. Disease definitions* Prevalence and statistics associated with HTN**
 Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Sleep-disordered breathing in the elderly: is it distinct from that in the younger or middle-aged populations?
 Editorial Sleep-disordered breathing in the elderly: is it distinct from that in the younger or middle-aged populations? Hiroki Kitakata, Takashi Kohno, Keiichi Fukuda Division of Cardiology, Department
Editorial Sleep-disordered breathing in the elderly: is it distinct from that in the younger or middle-aged populations? Hiroki Kitakata, Takashi Kohno, Keiichi Fukuda Division of Cardiology, Department
Portable Sleep Testing in Hospitalized Patients
 1 Portable Sleep Testing in Hospitalized Patients Rami Khayat, MD Heart Failure AND Public Health 6 million Americans with heart failure (>2% population 20 million people with asymptomatic cardiac impairment
1 Portable Sleep Testing in Hospitalized Patients Rami Khayat, MD Heart Failure AND Public Health 6 million Americans with heart failure (>2% population 20 million people with asymptomatic cardiac impairment
Hypertension and obesity. Dr Wilson Sugut Moi teaching and referral hospital
 Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Sleep and the Heart. Sleep Stages. Sleep and the Heart: non REM 8/31/2016
 Sleep and the Heart Overview of sleep Hypertension Arrhythmias Ischemic events CHF Pulmonary Hypertension Cardiac Meds and Sleep Sleep Stages Non-REM sleep(75-80%) Stage 1(5%) Stage 2(50%) Stage 3-4*(15-20%)
Sleep and the Heart Overview of sleep Hypertension Arrhythmias Ischemic events CHF Pulmonary Hypertension Cardiac Meds and Sleep Sleep Stages Non-REM sleep(75-80%) Stage 1(5%) Stage 2(50%) Stage 3-4*(15-20%)
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Apnea-Hypopnea- Index The new old biomarker for Sleep-Disordered Breathing. Alan S Maisel MD
 Apnea-Hypopnea- Index The new old biomarker for Sleep-Disordered Breathing Alan S Maisel MD Triumvirate of Health-public awareness 1.8% Sleep Physical Fitness Nutrition 91.3% 99.9% Sleep is important to
Apnea-Hypopnea- Index The new old biomarker for Sleep-Disordered Breathing Alan S Maisel MD Triumvirate of Health-public awareness 1.8% Sleep Physical Fitness Nutrition 91.3% 99.9% Sleep is important to
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD
 New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Sleep Apnea induced Endothelial Dysfunction: could it be reversible?
 Orofacial Pain and Oral Medicine Course: OFPM #723 Motor/Sleep Disorders and Oral Physiology in OFPOM Lecture #3a Dr. Glenn Clark Professor of Diagnostic Sciences Assistant Dean of Distance Education Director
Orofacial Pain and Oral Medicine Course: OFPM #723 Motor/Sleep Disorders and Oral Physiology in OFPOM Lecture #3a Dr. Glenn Clark Professor of Diagnostic Sciences Assistant Dean of Distance Education Director
2/11/2019 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES DUALITY OF INTEREST
 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
3/10/2014. Pearls to Remember. 1) Consequences of OSA related to both arousals and hypoxia. 2) Arousals provoke increased
 Consequences of OSA related to both arousals and hypoxia. 2) Arousals provoke increased") Cardiovascular disease and Sleep Disorders Timothy L. Grant, M.D.,F.A.A.S.M. Medical Director Baptist Sleep Center at Sunset Medical Director Baptist Sleep Education Series Medical Director Sleep Division
Cardiovascular disease and Sleep Disorders Timothy L. Grant, M.D.,F.A.A.S.M. Medical Director Baptist Sleep Center at Sunset Medical Director Baptist Sleep Education Series Medical Director Sleep Division
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
( ) 28 kg/ m 2, OSAHS, BMI < 24 kg/ m 2 10
 28 kg/ m 2, OSAHS, BMI < 24 kg/ m 2 10") 2013 9 12 5 http: / / www. cjrccm. com 435 ;, ( sleep apneahypopnea syndrome, SAHS) 20 80,, SAHS /, SAHS, [ 1 ] SAHS ( obstructive sleep apnea-hypopnea syndrome, OSAHS) OSAHS [ 2-4 ], 50% 92% OSAHS, 30%
2013 9 12 5 http: / / www. cjrccm. com 435 ;, ( sleep apneahypopnea syndrome, SAHS) 20 80,, SAHS /, SAHS, [ 1 ] SAHS ( obstructive sleep apnea-hypopnea syndrome, OSAHS) OSAHS [ 2-4 ], 50% 92% OSAHS, 30%
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Simple diagnostic tools for the Screening of Sleep Apnea in subjects with high risk of cardiovascular disease
 Cardiovascular diseases remain the number one cause of death worldwide Simple diagnostic tools for the Screening of Sleep Apnea in subjects with high risk of cardiovascular disease Shaoguang Huang MD Department
Cardiovascular diseases remain the number one cause of death worldwide Simple diagnostic tools for the Screening of Sleep Apnea in subjects with high risk of cardiovascular disease Shaoguang Huang MD Department
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
IMET 2000 PAL International Medical Education Trust Palestine What the GP Should Know about Hypertension
 What the GP Should Know about Hypertension Raed Abu Sham a, M.D Internist and Cardiologist Cardiac Pacing and Electrophysiologist Impact of Age on Blood Pressure Prevalence of HTN according to Age Fast
What the GP Should Know about Hypertension Raed Abu Sham a, M.D Internist and Cardiologist Cardiac Pacing and Electrophysiologist Impact of Age on Blood Pressure Prevalence of HTN according to Age Fast
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker