Parkinson s Disease Prescribing Guidelines for use in Primary and Secondary Care
|
|
|
- Stephany Craig
- 6 years ago
- Views:
Transcription

1 Parkinson's Disease Prescribing Guidelines for use in Primary and Secondary Care 2017 Parkinson s Disease Prescribing Guidelines for use in Primary and Secondary Care Document Description Document Type Prescribing Guidance Service Application Primary and Secondary Care Version 2.2 Ratification date July 2017 Review date July 2019 Lead Author(s) Dr Janine Barnes Dr Alistair Lewthwaite Neurology Specialist Pharmacist Consultant Neurologist, DGoH Change History Version Date Comments /1/10 Developed by Dr Barnes and Dr Etti /1/10 Updated with comments from Mehul Amin, Team Leader of Primary Care Neurology Team 0.3 9/2/10 Amended by Clair Huckerby-Pharmaceutical Advisor /2/10 Updated with comments from AMMC 0.5 April 2010 Final comments from neurology consultants 0.6 June 2010 Changes to formatting 1.0 Sept 2010 Final Ratified edition 2.0 Oct 2012 Guidelines reviewed Ropinirole XL info updated due to license change 2.1 May 2015 Amended by Dr Barnes 2.2 April 2017 Amended by Dr Barnes-Following publication of new NICE guidance 1
2 Link with Care Quality Commission Essential Standards of Quality & Safety Regulation 10, Outcome 16- Assessing and monitoring the quality of service provision. Regulation 13, Outcome 9- Management of medicines. Link with Trust Purpose and Values statements These guidelines are aimed to improve the health and wellbeing of our local community. They link with: We will support, deliver and develop our staff We will work to continuously improve services. 2
3 Reviewers - This Document has been reviewed by Version Date Name Title/Responsibility 2.1 May 2015 Dr J Barnes Neurology Specialist Pharmacist 2.2 April 2017 Dr J Barnes Neurology Specialist Pharmacist Approvals - This document has been approved by Version Date Name Title/Responsibility 2.2 Sept Dr D Jenkins Chair, Area Clinical Effectiveness 2017 Sub-committee DOCUMENT STATUS: This is a controlled document. Whilst this document may be printed, the electronic version posted on the intranet is the controlled copy. Any printed copies of the document are not controlled. Related Documents Reference No. Document Title Version Applicable Legislation Glossary of Terms Term Acronym Definition Clinical Commissioning Group CCG 3
4 Summary Sheet These guidelines have been drawn up to promote the safe, effective and economic use of medication for Parkinson s disease patients, aiming to improve the quality of patient experience for this group of patients. Recommendations for prescribing are based on NICE and SIGN guidance and from consultations with clinicians from both primary and secondary care in the Dudley Health Economy. These guidelines are for use by all staff within the Dudley Health Economy, who manage patients with Parkinson s disease. Produced in consultation with: Dr R Etti Dr M Douglas Clair Huckerby Jane Elvidge Mehul Amin Dr J Stellman Dr S Duja Dr A. Banerjee Dr A McGrath Dr A Michael Primary Care Neurology team AMMC members Practice based Commissioning Clusters Consultant Neurologist, DGoH Consultant Neurologist, DGoH Pharmaceutical Adviser, Dudley PCT Principal Pharmacist, DGoH Team Leader, Primary Care Neurology Team Elderly Care consultant, DGoH Elderly Care consultant, DGoH Elderly Care consultant, DGoH Elderly Care consultant, DGoH Elderly Care consultant, DGoH The guidelines will be subject to review in two years time or sooner depending on changes in national guidance. Contents Introduction 5 Treatment pathway for Parkinson s disease 6 Levodopa: Co-careldopa, Co-beneldopa 7 Dopamine agonists: Ropinirole, Pramipexole, Rotigotine 11 Monoamine oxidase B inhibitors: Rasagiline, Selegiline, Safinamide 14 Antimuscarinics: Trihexyphenidyl 15 COMT (catechol-o-methyl-transferase) inhibitors: Entacapone, 15 Opicapone Stanek(Levodopa/Carbidopa/Entacapone) 16 Amantadine 16 Apomorphine 16 References 17 Pg No 4
5 Introduction Aims To provide a simple pathway for the treatment of Parkinson s disease To promote the safe, effective and economic use of Parkinson s disease medication To minimise the risk of medication related side effects experienced by this patient group Principles of Treatment This guidance is based on the best available evidence but its application must be modified by professional judgement The pathway and prescribing guidelines are produced as an aide to prescribing for GPs and specialists within Dudley although often it is not possible to identify a universal first choice therapy for patients with early or late Parkinson s disease and so the choice of drug prescribed should take into account: Clinical and lifestyle characteristics Patient preference Roles and Responsibilities It is essential that in order for these guidelines to be implemented that they are easily and conveniently accessible to all healthcare professionals. Specialist Initiation: Where specialist initiation of a drug is suggested, this refers to consultant neurologists, consultants within the elderly care team and prescribers within the neurology primary care team. Identified Standards These guidelines should be read in association with NICE 2 and SIGN 3 clinical guidelines. Auditing The Prescribing and Medicines Management team working with the Primary Care Neurology team and Dudley group of hospitals, will be responsible for the audit of the prescribing guidelines. 5
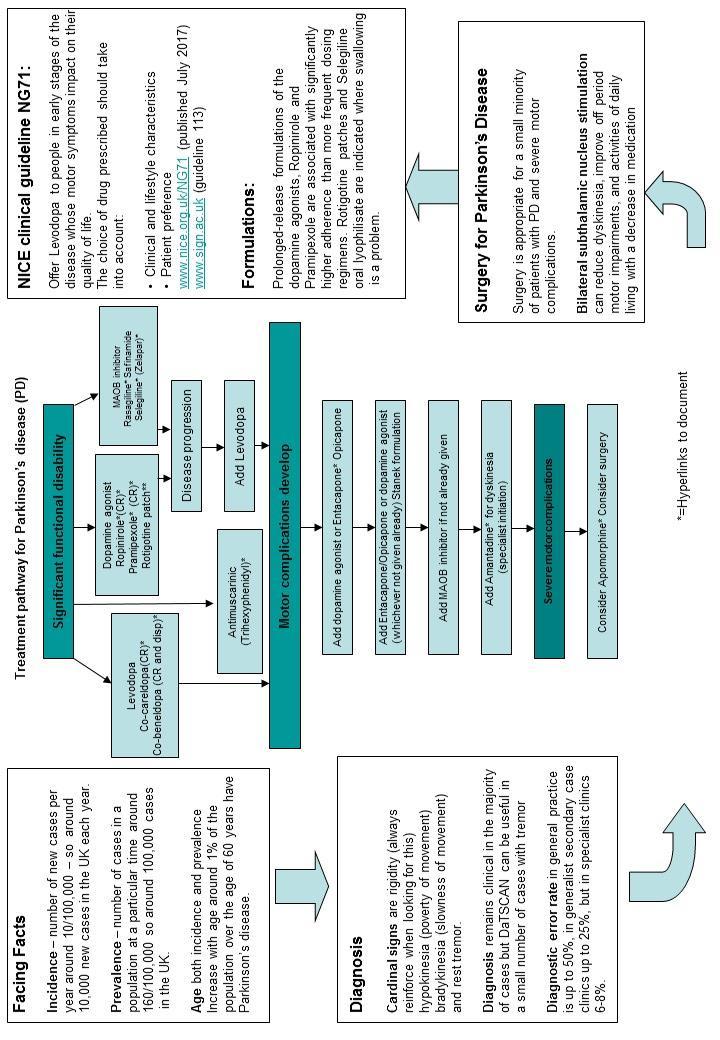
6 6

7 A. Levodopa: Levodopa Formulations Co-careldopa, Co-beneldopa (specialist initiation recommended) Levodopa is the amino-acid precursor of dopamine, acts by replenishing depleted striatal dopamine; is given with an extracerebral dopa-decarboxylase inhibitor that reduces the peripheral conversion of levodopa to dopamine allowing less side effects and lower doses of levodopa to be used. The extracerebral dopa-decarboxylase inhibitors used with levodopa are benserazide (co-beneldopa) and carbidopa (co-careldopa). These combinations are used in the elderly or frail, in patients with other significant illnesses, and in those with more severe symptoms. The preparations are effective and well-tolerated in most patients. Levodopa therapy should be initiated at a low dose and increased in small steps, with the final dose as low as possible. Intervals between doses should be suited to the individual patient needs. Levodopa treatment is associated with the development of potentially troublesome motor complications including response fluctuations and dyskinesias. Response fluctuations are characterised by large variations in motor performance, with normal function during the on period, and weakness 7
8 and restricted mobility during the off period. End-of-dose deterioration also occurs, where the duration of benefit after each dose becomes progressively shorter. Modified-release preparations may help with end-of-dose deterioration or nocturnal immobility and rigidity. Motor complications are particularly problematic in young patients treated with levodopa. Co-careldopa: Indicated for Parkinsonism (but not drug-induced extrapyramidal symptoms) Dose Dose Frequency Dose Titration Maximum dose Expressed as levodopa, initially 100 mg (with carbidopa 25 mg) up to 800 mg (with carbidopa 200 mg) daily in divided doses or initially mg (with carbidopa mg) or initially 125 mg (with carbidopa 12.5 mg, as ½ tablet of cocareldopa 25/250) 3 times daily increased by mg (with carbidopa mg) daily or on alternate days response 3 4 times daily increased by mg daily or on alternate days response 1 2 times daily increased by 125 mg (with carbidopa 12.5 mg) daily or on alternate days response up to 800 mg (with carbidopa mg) daily in divided doses NB. At least 70 mg carbidopa daily is necessary to achieve full inhibition of peripheral dopa-decarboxylase. When transferring patients from another levodopa/dopa-decarboxylase inhibitor preparation, the previous preparation should be discontinued at least 12 hours before. 8
9 Co-beneldopa: Indicated for Parkinsonism (but not drug-induced extrapyramidal symptoms) Dose Dose Frequency Dose Titration Maintenance dose Expressed as levodopa, initially 50mg 3-4 times daily (100mg 3 times daily in advanced disease) increased by 100 mg daily once or twice weekly according to response mg daily in divided doses Dose for elderly patients initially 50 mg once or twice daily increased by 50 mg daily every 3 4 days response NB. When transferring patients from another levodopa/dopa-decarboxylase inhibitor preparation, the previous preparation should be discontinued 12 hours before (although interval can be shorter). Levodopa controlled release formulations: Co-careldopa, Co-beneldopa Indicated for idiopathic Parkinson's disease, in particular to reduce off-period in patients who previously have been treated with levodopa/decarboxylase inhibitors, or with levodopa alone and who have experienced motor fluctuations. The experience is limited with 'Sinemet CR' and 'Half Sinemet CR' in patients who have not been treated with Levodopa before. In clinical trials, patients with motor fluctuations experienced reduced 'off'-time with 'Sinemet CR' when compared with 'Sinemet'. The reduction of the 'off'-time is rather small (about 10%) and the incidence of dyskinesias increases slightly after administration of 'Sinemet CR' compared to standard 'Sinemet'. Global ratings of improvement and activities of daily living in the 'on' and 'off' state, as assessed by both patient and physician, were better during therapy with 'Sinemet CR' than with 'Sinemet'. Patients considered 'Sinemet CR' to be more helpful for their clinical fluctuations, and preferred it over 'Sinemet'. In patients without motor fluctuations, 'Sinemet CR under controlled conditions, provided the same therapeutic benefit with less frequent dosing than with 'Sinemet'. Generally, there was no further improvement of other symptoms of Parkinson's disease. (see BNF for prescribing advice¹) 9
10 Co-careldopa CR: (Caramet CR, Half Sinemet CR and Sinemet CR) Co-careldopa CR preparation: (strength expressed as carbidopa:levodopa) Caramet CR co-careldopa 25/100 50/200 Dose for patients not receiving levodopa/dopadecarboxylase inhibitor preparations, expressed as levodopa, initially mg Dose frequency twice daily (at least 6 hours between doses) Dose titration dose adjusted response at intervals of at least 2 days Sinemet CR 50/200 initially, 1 Sinemet CR tablet twice daily both dose and interval then adjusted response at intervals of not less than 3 days Co-careldopa CR preparation: (strength expressed as carbidopa:levodopa) Caramet CR co-careldopa 25/100 50/200 Sinemet CR 50/200 Patients transferring from immediaterelease levodopa/dopadecarboxylase inhibitor preparations, discontinue previous preparation at least 12 hours before first dose of Caramet CR; 1 Sinemet CR tablet twice daily can be substituted for a daily dose of levodopa mg in immediaterelease Sinemet tablets Dose frequency substitute Caramet CR to provide a similar amount of levodopa daily and extend dosing interval by 30 50%; (substitute Sinemet CR to provide approx. 10% more levodopa per day and extend dosing interval by 30 50%); Dose titration dose then adjusted response at intervals of at least 2 days dose and interval then adjusted response at intervals of not less than 3 days 10
11 Co-beneldopa CR: (Madopar) Co-beneldopa CR preparation: (strength expressed as 25/100 beneldopa:levodopa) Dose and frequency Maximum dose Dose titration Dose for patients not receiving levodopa/dopadecarboxylase inhibitor preparations, Patients transferring from immediaterelease levodopa/dopadecarboxylase inhibitor preparations, initially 1 capsule 3 times daily initially 1 capsule substituted for every 100 mg of levodopa and given at same dosage frequency 6 capsules daily increased every 2 3 days response; average increase of 50% needed over previous levodopa dose and titration may take up to 4 weeks Supplementary dose of immediate-release Madopar may be needed with first morning dose; if response still poor to total daily dose of Madopar CR plus Madopar corresponding to 1.2 g levodopa, consider alternative therapy. Levodopa dispersible formulation: Co-beneldopa: Patients requiring a more rapid onset of action, e.g., from early morning or afternoon akinesia, or who exhibit delayed on or wearing off phenomena, are more likely to benefit from Co-beneldopa dispersible. (see BNF for prescribing advice 1 ) The tablets can be dispersed in water or orange squash (not orange juice) or swallowed whole. B. Dopamine Agonists: (specialist initiation recommended) Ropinirole: Licensed to treat Parkinson s disease, either used alone or as an adjunct to levodopa with a dopa-decarboxylase inhibitor. When administered as adjunct to levodopa, concurrent dose of levodopa may be reduced by approx. 20%. 11
12 Dose Dose Frequency Dose Titration Maximum dose initially 750 micrograms daily in 3 divided doses 24 mg daily increased by increments of 750 micrograms at weekly intervals to 3 mg daily further increased by increments of up to 3 mg at weekly intervals response; usual range 9 16 mg daily (but higher doses may be required if used with levodopa); Ropinirole XL prescribed as Ipinnia XL brand: Stable Parkinson s disease in patients transferring from ropinirole immediaterelease tablets, initially Ipinnia XL once daily substituted for total daily dose equivalent of ropinirole immediate-release tablets; if control not maintained after switching, in patients receiving less than 8 mg once daily, increase in steps of 2 mg at intervals of at least 1 week to 8 mg once daily response; in patients receiving 8 mg once daily or more, increase in steps of 2 mg at intervals of at least 2 weeks response; max. 24 mg once daily. Patients can also be initiated on Ipinnia XL with a usual starting dose of 2mg once daily. After a week this dose can be increased to 4mg once daily, when a therapeutic response may be seen. If sufficient symptom control is not achieved or maintained, the daily dose may be increased by 2mg at weekly or longer intervals. NB. When administered as adjunct to levodopa, concurrent dose of levodopa may be reduced. Pramipexole: Licensed to treat Parkinson s disease, used alone or as an adjunct to levodopa with dopa-decarboxylase inhibitor. NB. Doses and strengths are stated in terms of pramipexole (base); equivalent strengths in terms of pramipexole dihydrochloride monohydrate (salt) are as follows: 88 micrograms base 125 micrograms salt; 180 micrograms base 250 micrograms salt; 350 micrograms base 500 micrograms salt; 700 micrograms base 1 mg salt Dose Dose Frequency Dose Titration Maximum dose Initially 88 micrograms 3 times daily dose doubled every 5 7 days if tolerated to 3.3 mg daily in 3 divided doses 12
13 350 micrograms 3 times daily; further increased if necessary by 180 micrograms 3 times daily at weekly intervals During pramipexole dose titration and maintenance, levodopa dose may be reduced. Pramipexole has been associated with somnolence and episodes of sudden sleep onset in a rare number of cases. Patients should be informed of this and advised to exercise caution when driving or operating machinery during treatment with the medication. Pramipexole prolonged release prescribed as Pipexus brand: The majority of patients are able to switch from immediate release Pramipexole to the prolonged release formulation without the need for dose adjustment. Rotigotine patch: 4,5 (specialist initiation recommended) Licensed to treat Parkinson s disease, either used alone or as an adjunct to levodopa with dopa-decarboxylase inhibitor. monotherapy adjunctive therapy with levodopa Dose Frequency Dose Titration Maximum dose 2 mg/24 hours increased in 8 mg/24 hours patch to dry, nonirritated steps of 2 mg/24 skin on hours at weekly torso, thigh, or intervals if upper arm, required removing after 24 hours and siting replacement patch on a different area (avoid using the same area for 14 days) apply 4 mg/24 hours patch to dry, non-irritated skin on torso, thigh, or upper arm, removing after 24 hours and siting replacement increased in steps of 2 mg/24 hours at weekly intervals if required 16 mg/24 hours 13
14 patch on a different area (avoid using the same site for 14 days); Rotigotine patches (Neupro ) are licensed as a monotherapy or as an adjunct to Levodopa with a dopa-decarboxylase inhibitor and it is a useful product where the transdermal route facilitates treatment. C. Monoamine oxidase B inhibitors: (specialist initiation recommended) Rasagiline, Selegiline, Safinamide Rasagiline: Licensed to treat Parkinson s disease, used alone or as adjunct to levodopa with dopa-decarboxylase inhibitor. Dose-1mg daily. Selegiline: Licensed to treat Parkinson s disease, used alone or as adjunct to levodopa with dopa-decarboxylase inhibitor. Dose-10 mg in the morning, or 5 mg at breakfast and midday. To avoid initial confusion and agitation, it may be appropriate to start treatment with a dose of 2.5 mg daily, particularly in the elderly. Selegiline oral lyophilisate: 6 (Zelapar) (specialist initiation recommended) The lyophilisate (1.25mg) can be taken daily before breakfast. The tablets should be placed on the tongue and allowed to dissolve. The patient should be advised not to drink, rinse or wash mouth out for 5 minutes after taking the tablet. NB. Patients receiving the 10mg conventional Selegiline tablet can be switched to Zelapar 1.25mg. The lyophilisate may be useful for patients who have difficulty in swallowing as Zelapar dissolves completely within 10 seconds of placing on the tongue and, in contrast to conventional tablets, Selegiline is absorbed primarily pregastrically. 14
15 Safinamide 7 : (specialist initiation recommended) Licensed for the treatment of adult patients with idiopathic Parkinson s disease as add-on therapy to a stable dose of levodopa alone or in combination with other medicinal products for Parkinson s disease in mid to late-stage fluctuating patients. Dose-Treatment should be started at one 50mg tablet per day. The dose may be increased to 100mg/day on the basis of individual clinical need. No change in dose is required for elderly patients. D. Antimuscarinics: Trihexyphenidyl: 8 (specialist initiation recommended) Found to be useful in treating severe tremor in younger Parkinson s disease patients. Drug may also be useful in reducing sialorrhoea-but has little effect on bradykinesia and propensity for causing neuropsychiatric side effects. E. COMT (catechol-o-methyl-transferase) inhibitors: (specialist initiation recommended) Entacapone and tolcapone prevent the peripheral breakdown of levodopa, by inhibiting catechol-o-methyltransferase, allowing more levodopa to reach the brain. They are licensed for use as an adjunct to co-beneldopa or cocareldopa for patients with Parkinson s disease who experience end-of-dose deterioration and cannot be stabilised on these combinations. Due to the risk of hepatotoxicity, tolcapone should be prescribed under specialist supervision only, when other catechol-o-methyltransferase inhibitors combined with cobeneldopa or co-careldopa are ineffective. Entacapone: Licensed as adjunct to levodopa with dopa-decarboxylase inhibitor in Parkinson s disease and end-of-dose motor fluctuations. Dose-200 mg with each dose of levodopa with dopa-decarboxylase inhibitor; max. 2 g daily. Opicapone 9,10,11 (specialist initiation recommended) Licensed as adjunctive therapy to preparations of levodopa/dopa decarboxylase inhibitors in adult patients with Parkinson s disease and endof-dose motor fluctuations who cannot be stabilised on those combinations. 15
16 Dose-50mg daily, taken at bedtime, at least one hour before or after levodopa combinations. Opicapone enhances the effects of levodopa. Hence, it is often necessary to adjust levodopa dosage within the first days to first weeks after initiating treatment with opicapone. Stanek : (Levodopa/Carbidopa/Entacapone) Licensed for Parkinson s disease and end of dose motor fluctuations not adequately controlled with levodopa and dopa decarboxylase treatment. Only 1 tablet to be taken for each dose. See BNF 1 for maximum amount of tablets daily as depends on strength of tablet. Patients receiving standardrelease co-careldopa or co-beneldopa alone, initiate Stanek at a dose that provides similar (or slightly lower) amount of levodopa Patients with dyskinesia or receiving more than 800 mg levodopa daily, introduce entacapone before transferring to Stanek (levodopa dose may need to be reduced by 10 30% initially). Patients receiving entacapone and standardrelease co-careldopa or co-beneldopa, initiate Stanek at a dose that provides similar (or slightly higher) amount of levodopa. Stanek is most cost effective at higher doses. F. Amantadine: 12 (specialist initiation recommended) Licensed for Parkinson s disease (but not drug-induced extrapyramidal symptoms). Dose-Parkinson s disease, 100 mg daily increased after one week to 100 mg twice daily, usually in conjunction with other treatment; some patients may require higher doses, max. 400 mg daily; elderly 65 years and over, 100 mg daily adjusted response. G. Apomorphine: 13,14 (specialist initiation recommended) (intermittent injection, pre-filled syringe. ampoule) Licensed for refractory motor fluctuations in Parkinson s disease ( off episodes) inadequately controlled by levodopa with dopa-decarboxylase inhibitor or other dopaminergics (for capable and motivated patients under specialist supervision). Dose-By subcutaneous injection, usual range (after initiation as below) 3 30 mg daily in divided doses; subcutaneous infusion may be preferable in those requiring division of injections into more than 10 doses daily; max. single dose 10 mg; child and adolescent under 18 years not recommended. 16
17 By continuous subcutaneous infusion (those requiring division into more than 10 injections daily) initially 1 mg/hour daily increased response (not more often than every 4 hours) in max. steps of 500 micrograms/hour, to usual rate of 1 4 mg/hour (14 60 micrograms/kg/hour); change infusion site every 12 hours and give during waking hours only (24-hour infusions not advised unless severe night-time symptoms) intermittent bolus boosts also usually needed; child and adolescent under 18 years not recommended. NB Total daily dose by either route (or combined routes) max. 100 mg. Requirements for initiation: Hospital admission and at least 2 days of pretreatment with domperidone for nausea and vomiting, after at least 3 days withhold existing antiparkinsonian medication overnight to provoke off episode, determine threshold dose, reestablish other antiparkinsonian drugs, determine effective apomorphine regimen, teach to administer by subcutaneous injection into lower abdomen or outer thigh at first sign of off episode, discharge from hospital, monitor frequently and adjust dosage regimen as appropriate (domperidone may normally be withdrawn over several weeks or longer) for full details of initiation requirements, consult product literature. References: 1. British National Formulary (2017) British National Formulary 73. Available at (Accessed 27 July 2017). 2. National Institute for Clinical excellence (20017) NICE clinical guideline 71 Parkinson s disease in adults. Available at : (Accessed 27 July 2017). 3. Scottish Intercollegiate Guidelines Network (2010) SIGN 113 Diagnosis and pharmacological management of Parkinson s disease. Available at: (Accessed 10 September 2012). 4. Giladi, N., Boroojerdi, B., Ko/>rczyn, A.D., Burn, D.J., Clark, C.E., Schapira, A.H.V. (2007) Rotigotine transdermal patch in early Parkinson s disease: A randomized, double-blind, controlled study versus placebo and ropinirole. Movement Disorders, 22(16), pp Poewe, W.H., Rascol, O., Quinn, N., Tolosa, E., Oertel, W.H., Martignoni, E., Rupp, M., Boroojerdi, B. (2007) Efficacy of pramipexole and transdermal rotigotine in advanced Parkinson s disease: a double-blind, double-dummy, randomised controlled trial. Lancet Neurology, 6, pp
18 6. Lew, M.F., Pawha, R., Leehey, M., Bertoni, J., Kricorian, G., Zydis Selegiline Study, (2007) Safety and efficacy of newly formulated selegiline orally disintegrating tablets as an adjunct to levodopa in the management of off episodes in patients with Parkinson s disease. Current Medical Research and Opinion, 23(4) pp National Institute for Clinical excellence (2017) Parkinson s disease with motor fluctuations:safinamide. Evidence summary (ES6). Available at : (Accessed 20 March 2017) 8. Martin, W.E., Loewenson, R.B., Resch, J.A., Baker, A.B. (1974) A controlled study comparing trihexyphenidyl hydrochloride plus levodopa with placebo plus levodopa in patients with Parkinson s disease. Neurology, 24/10 (912-9), Ferreira, J.J., Lees, A., Rocha, J.F., Poewe, W., Rascol, O., Soares-da- Silva, P. (2015) Opicapone as an adjunct to levodopa in patients with Parkinson s disease and end-of-dose motor fluctuations: a randomised, double-blind, controlled trial. Lancet Neurology. 10. Lees, A.J., Ferreira, J., Rascol, O., Poewe, W., Rocha, J.F., McCrory, M., et al., (2016) Opicapone as Adjunct to Levodopa Therapy in Patients With Parkinson s Disease and Motor Fluctuations: A Randomised Clinical Trial. JAMA Neurology. 11. National Institute for Clinical excellence (2017) Parkinson s disease with end of dose motor fluctuations: opicapone: Evidence summary (ES9). Available at : (Accessed 20 March 2017) 12. Verhagen Metman, L., Del Dotto, P., Van Den Munckhof, P., Fang, J., Mouradian, M.M., Chase, T.N. (1998) Amantadine as treatment for dyskinesias and motor fluctuations in Parkinson s disease. Neurology, 50/5 ( ), Chen, J.J., Obering, C. (2005) A review of intermittent subcutaneous apomorphine injections for the rescue management of motor fluctuations associated with advanced Parkinson s disease. Clinical Therapeutics, 27(11), pp Ruiz, P.J.G., Ignacio, A.S., Pensado, B.A., Garcia, A.C., Frech, F.A., Lopez, M.A.., Gonzalez, J.A., Octavio, J.B. (2008) Efficacy of long-term continuous subcutaneous apomorphine infusion in advanced Parkinson s disease with motor fluctuations : a multicenter study. Movement Disorders, 23(8) pp
New Medicines Committee Briefing July 2011
 New Medicines Committee Briefing July 2011 Pramipexole immediate-release (Mirapexin ) and Pramipexole modifiedrelease (Mirapexin prolonged release) for the treatment of Parkinson s Disease Pramipexole
New Medicines Committee Briefing July 2011 Pramipexole immediate-release (Mirapexin ) and Pramipexole modifiedrelease (Mirapexin prolonged release) for the treatment of Parkinson s Disease Pramipexole
Re-Submission. Scottish Medicines Consortium. rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd.
 (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd.") Scottish Medicines Consortium Re-Submission rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd 10 November 2006 The Scottish Medicines Consortium (SMC) has completed
Scottish Medicines Consortium Re-Submission rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd 10 November 2006 The Scottish Medicines Consortium (SMC) has completed
Guidelines for acute treatment of patients with Parkinson s disease including those who are nil by mouth
 Index No: MMG48 Guidelines for acute treatment of patients with Parkinson s disease including those who are nil by mouth Version: 2.0 Date ratified: November 2017 Ratified by: (Name of Committee) Name
Index No: MMG48 Guidelines for acute treatment of patients with Parkinson s disease including those who are nil by mouth Version: 2.0 Date ratified: November 2017 Ratified by: (Name of Committee) Name
PARKINSON S MEDICATION
 PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
Acute management of in-patient Parkinson s Disease patients
 Acute management of in-patient Parkinson s Disease patients Contents Pages Introduction and Admission advice 2 Nil by Mouth Guidance 3 5 Complex therapy advice (Apomorphine, DBS, Duodopa) 6 Surgical peri-operative
Acute management of in-patient Parkinson s Disease patients Contents Pages Introduction and Admission advice 2 Nil by Mouth Guidance 3 5 Complex therapy advice (Apomorphine, DBS, Duodopa) 6 Surgical peri-operative
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University
 Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Parkinson s disease. Information for patients and carers. The Leeds Teaching Hospitals NHS Trust
 n The Leeds Teaching Hospitals NHS Trust Parkinson s disease Information for patients and carers in partnership with Leeds Community Healthcare NHS Trust The symptoms of Parkinson s appear when the levels
n The Leeds Teaching Hospitals NHS Trust Parkinson s disease Information for patients and carers in partnership with Leeds Community Healthcare NHS Trust The symptoms of Parkinson s appear when the levels
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to
 parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
Clinical Policy: Safinamide (Xadago) Reference Number: CP.CPA.308 Effective Date: Last Review Date: Line of Business: Commercial
 Reference Number: CP.CPA.308 Effective Date: Last Review Date: Line of Business: Commercial") Clinical Policy: Safinamide (Xadago) Reference Number: CP.CPA.308 Effective Date: 05.16.17 Last Review Date: 08.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy
Clinical Policy: Safinamide (Xadago) Reference Number: CP.CPA.308 Effective Date: 05.16.17 Last Review Date: 08.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy
ACUTE MANAGEMENT OF PARKINSON S PATIENTS WHO ARE NIL BY MOUTH (NBM) OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM
 OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM") ACUTE MANAGEMENT OF PARKINSON S PATIENTS WHO ARE NIL BY MOUTH (NBM) OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM 1 CONTENTS: TOPIC PAGE Introduction 3 What should you do when a PD
ACUTE MANAGEMENT OF PARKINSON S PATIENTS WHO ARE NIL BY MOUTH (NBM) OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM 1 CONTENTS: TOPIC PAGE Introduction 3 What should you do when a PD
Medications used to treat Parkinson s disease
 Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Final Appraisal Report. ) for the treatment of idiopathic Parkinson s disease. Ropinirole prolonged-release (Requip XL. GlaxoSmithKline UK
 for the treatment of idiopathic Parkinson s disease. Ropinirole prolonged-release (Requip XL. GlaxoSmithKline UK") Final Appraisal Report Ropinirole prolonged-release (Requip XL ) for the treatment of idiopathic Parkinson s disease GlaxoSmithKline UK Advice No: 1409 August 2009 Recommendation of AWMSG Ropinirole prolonged-release
Final Appraisal Report Ropinirole prolonged-release (Requip XL ) for the treatment of idiopathic Parkinson s disease GlaxoSmithKline UK Advice No: 1409 August 2009 Recommendation of AWMSG Ropinirole prolonged-release
Scottish Medicines Consortium
 Scottish Medicines Consortium rotigotine 2mg/24 hours, 4mg/24 hours, 6mg/24 hours, 8mg/24 hours transdermal patch (Neupro ) (No: 289/06) Schwarz Pharma Ltd. 7 July 2006 The Scottish Medicines Consortium
Scottish Medicines Consortium rotigotine 2mg/24 hours, 4mg/24 hours, 6mg/24 hours, 8mg/24 hours transdermal patch (Neupro ) (No: 289/06) Schwarz Pharma Ltd. 7 July 2006 The Scottish Medicines Consortium
Clinical Guideline for the management of inpatients with Parkinson s disease
 Clinical Guideline for the management of inpatients with Parkinson s disease Introduction: Parkinson s disease (PD) is the second most common neurodegenerative disorder, characterised by bradykinesia,
Clinical Guideline for the management of inpatients with Parkinson s disease Introduction: Parkinson s disease (PD) is the second most common neurodegenerative disorder, characterised by bradykinesia,
TRANSPARENCY COMMITTEE OPINION. 18 March 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 March 2009 REQUIP LP 2 mg extended-release tablet Box of 21 tablets (CIP: 379 214-8) Box of 28 tablets (CIP: 379
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 March 2009 REQUIP LP 2 mg extended-release tablet Box of 21 tablets (CIP: 379 214-8) Box of 28 tablets (CIP: 379
CENTENE PHARMACY AND THERAPEUTICS NEW DRUG REVIEW 3Q17 July August
 BRAND NAME Xadago GENERIC NAME Safinamide MANUFACTURER Newron Pharmaceuticals SpA holds license; granted approval. US WorldMeds, LLC exclusive licensee and distributor in the U.S. DATE OF APPROVAL March
BRAND NAME Xadago GENERIC NAME Safinamide MANUFACTURER Newron Pharmaceuticals SpA holds license; granted approval. US WorldMeds, LLC exclusive licensee and distributor in the U.S. DATE OF APPROVAL March
Effective Shared Care Agreement for the treatment of severe motor complications in people with Parkinson Disease with apomorphine (APO-go )
") Effective Shared Care Agreement for the treatment of severe motor complications in people with Parkinson Disease with apomorphine (APO-go ) This shared care agreement outlines the ways in which the responsibilities
Effective Shared Care Agreement for the treatment of severe motor complications in people with Parkinson Disease with apomorphine (APO-go ) This shared care agreement outlines the ways in which the responsibilities
Management of Parkinson s Disease in Primary and Secondary care for patients with compromised swallow or those patients deemed Nil By Mouth.
 Management of Parkinson s Disease in Primary and Secondary care for patients with compromised swallow or those patients deemed Nil By Mouth. To aid the management and treatment of Parkinson s Patients
Management of Parkinson s Disease in Primary and Secondary care for patients with compromised swallow or those patients deemed Nil By Mouth. To aid the management and treatment of Parkinson s Patients
Dorset Medicines Advisory Group SHARED CARE GUIDELINES FOR PRESCRIBING ENTACAPONE (INCLUDING IN COMBINATION) OR OPICAPONE IN PARKINSON S DISEASE
 OR OPICAPONE IN PARKINSON S DISEASE") SHARED CARE GUIDELINES FOR PRESCRIBING ENTACAPONE (INCLUDING IN COMBINATION) OR OPICAPONE IN PARKINSON S DISEASE INDICATION By inhibiting metabolism of levodopa, entacapone or opicapone allow a reduction
SHARED CARE GUIDELINES FOR PRESCRIBING ENTACAPONE (INCLUDING IN COMBINATION) OR OPICAPONE IN PARKINSON S DISEASE INDICATION By inhibiting metabolism of levodopa, entacapone or opicapone allow a reduction
Appendix 2: Admissions checklists for people with Parkinson s
 Appendix 2: Admissions checklists for people with Parkinson s This document is intended to form the basis of a locally developed tool and so it has been built to be amended with relevant local information,
Appendix 2: Admissions checklists for people with Parkinson s This document is intended to form the basis of a locally developed tool and so it has been built to be amended with relevant local information,
Parkinson s Disease Medications: Professionals Edition
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease. Gillian Sare
 Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
MANAGEMENT OF PATIENTS WITH PARKINSON S DISEASE WHO ARE NIL BY MOUTH OR WITH A COMPROMISED SWALLOW
 MANAGEMENT OF PATIENTS WITH PARKINSON S DISEASE WHO ARE NIL BY MOUTH OR WITH A COMPROMISED SWALLOW Author: Gordon W Duncan Status: Approved Authorised by: Clinical Policy Group Version: 1.0 Review date:
MANAGEMENT OF PATIENTS WITH PARKINSON S DISEASE WHO ARE NIL BY MOUTH OR WITH A COMPROMISED SWALLOW Author: Gordon W Duncan Status: Approved Authorised by: Clinical Policy Group Version: 1.0 Review date:
Anticholinergics. COMT* Inhibitors. Dopaminergic Agents. Dopamine Agonists. Combination Product
 Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
Best Medical Treatments for Parkinson s disease
 Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
An Overview of Parkinson s Medication used in Multiple System Atrophy
 Introduction The cause of Parkinson s symptoms The types of Parkinson s drugs used in MSA Finding the best medication Additional medication Drugs to avoid Further information An Overview of Parkinson s
Introduction The cause of Parkinson s symptoms The types of Parkinson s drugs used in MSA Finding the best medication Additional medication Drugs to avoid Further information An Overview of Parkinson s
Commonly encountered medications and their side effects - what the generalist needs to know
 Commonly encountered medications and their side effects - what the generalist needs to know Jeremy Cosgrove Consultant Neurologist Leeds Teaching Hospitals NHS Trust Outline: Parkinson s medications and
Commonly encountered medications and their side effects - what the generalist needs to know Jeremy Cosgrove Consultant Neurologist Leeds Teaching Hospitals NHS Trust Outline: Parkinson s medications and
Communicating About OFF Episodes With Your Doctor
 Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Advanced Therapies for Motor Symptoms in PD. Matthew Boyce MD
 Advanced Therapies for Motor Symptoms in PD Matthew Boyce MD Medtronic Education Teva Speakers Bureau Acadia Speakers Bureau Disclosures Discuss issues in advanced PD Adjunct therapies to levo-dopa Newer
Advanced Therapies for Motor Symptoms in PD Matthew Boyce MD Medtronic Education Teva Speakers Bureau Acadia Speakers Bureau Disclosures Discuss issues in advanced PD Adjunct therapies to levo-dopa Newer
Update in the Management of Parkinson s Disease
 Update in the Management of Parkinson s Disease What s standard? What s new? What s coming? Bruno V. Gallo, M.D. Assistant Professor of Neurology, FIU Wertheim College of Medicine Director, Parkinson &
Update in the Management of Parkinson s Disease What s standard? What s new? What s coming? Bruno V. Gallo, M.D. Assistant Professor of Neurology, FIU Wertheim College of Medicine Director, Parkinson &
Drug Therapy of Parkinsonism. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
An Overview of Parkinson s Medication used in Multiple System Atrophy
 Introduction Cause of Parkinson s symptoms Parkinson s drug use in MSA Finding the best medication Other medication - Interaction Drugs to avoid Further information An Overview of Parkinson s Medication
Introduction Cause of Parkinson s symptoms Parkinson s drug use in MSA Finding the best medication Other medication - Interaction Drugs to avoid Further information An Overview of Parkinson s Medication
Rotigotine patches (Neupro) in early Parkinson s disease Edited by AdRes Health Economics & Outcomes Research
 in early Parkinson s disease Edited by AdRes Health Economics & Outcomes Research") Rotigotine patches (Neupro) in early Parkinson s disease Edited by AdRes Health Economics & Outcomes Research Synthetic DRUG PROFILE Introduction Parkinson s disease (PD) is a neurodegenerative disorder
Rotigotine patches (Neupro) in early Parkinson s disease Edited by AdRes Health Economics & Outcomes Research Synthetic DRUG PROFILE Introduction Parkinson s disease (PD) is a neurodegenerative disorder
Shared Care Agreement Apomorphine For use in Parkinson s Disease
 Shared Care Agreement Apomorphine For use in Parkinson s Disease This shared care agreement outlines suggested ways in which the prescribing responsibilities can be shared between the specialist and GP.
Shared Care Agreement Apomorphine For use in Parkinson s Disease This shared care agreement outlines suggested ways in which the prescribing responsibilities can be shared between the specialist and GP.
Cardinal Features of Parkinson s. Management of Parkinson s Disease. Drug Induced Parkinson s. Other Parkinson s Symptoms.
 Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Prior Authorization with Quantity Limit Program Summary
 Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Continuous dopaminergic stimulation
 Continuous dopaminergic stimulation Angelo Antonini Milan, Italy GPSRC CNS 172 173 0709 RTG 1 As PD progresses patient mobility becomes increasingly dependent on bioavailability of peripheral levodopa
Continuous dopaminergic stimulation Angelo Antonini Milan, Italy GPSRC CNS 172 173 0709 RTG 1 As PD progresses patient mobility becomes increasingly dependent on bioavailability of peripheral levodopa
European Commission approves ONGENTYS (opicapone) a novel treatment for Parkinson s disease patients with motor fluctuations
 a novel treatment for Parkinson s disease patients with motor fluctuations") July 6, 2016 European Commission approves ONGENTYS (opicapone) a novel treatment for Parkinson s disease patients with motor fluctuations Porto, 5 July 2016 BIAL announced that the medicinal product ONGENTYS
July 6, 2016 European Commission approves ONGENTYS (opicapone) a novel treatment for Parkinson s disease patients with motor fluctuations Porto, 5 July 2016 BIAL announced that the medicinal product ONGENTYS
History Parkinson`s disease. Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson
 Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
SHARED CARE PRESCRIBING GUIDELINE. TOLCAPONE for the Treatment of IDIOPATHIC PARKISON S DISEASE.
 WORKING IN PARTNERSHIP WITH Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex
WORKING IN PARTNERSHIP WITH Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
The symptoms of the Parkinson s disease may vary from person to person. The symptoms might include the following:
 1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
CLINICAL GUIDELINE FOR THE MANAGEMENT OF INPATIENTS WITH PARKINSON S DISEASE
 CLINICAL GUIDELINE FOR THE MANAGEMENT OF INPATIENTS WITH PARKINSON S DISEASE 1. Aim/Purpose of this Guideline To assist all doctors and nurses in the care of inpatients with Parkinson s disease. This guideline
CLINICAL GUIDELINE FOR THE MANAGEMENT OF INPATIENTS WITH PARKINSON S DISEASE 1. Aim/Purpose of this Guideline To assist all doctors and nurses in the care of inpatients with Parkinson s disease. This guideline
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
PDL Class: Parkinson s Drugs
 Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review: September 2013 Date of Last Review:
Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review: September 2013 Date of Last Review:
Opicapone is a peripheral, selective and reversible catechol-o-methyltransferase (COMT) inhibitor 1.
 inhibitor 1.") New Medicines Committee Briefing June 2017 Opicapone (Ongentys ) as adjunctive therapy in adult patients with Parkinson s disease and end-of-dose motor fluctuations Opicapone (Ongentys ) is to be reviewed
New Medicines Committee Briefing June 2017 Opicapone (Ongentys ) as adjunctive therapy in adult patients with Parkinson s disease and end-of-dose motor fluctuations Opicapone (Ongentys ) is to be reviewed
Parkinson's Disease and how you can make a difference with medication
 Parkinson's Disease and how you can make a difference with medication Alyson Franks Parkinson's and Movement Disorder Nurse Specialist Royal Hallamshire Hospital No treatment all Complementary Therapy
Parkinson's Disease and how you can make a difference with medication Alyson Franks Parkinson's and Movement Disorder Nurse Specialist Royal Hallamshire Hospital No treatment all Complementary Therapy
What is the best medical therapy for early Parkinson's disease? Medications Commonly Used for Parkinson's Disease
 FPIN's Clinical Inquiries Treatment of Early Parkinson's Disease Clinical Question What is the best medical therapy for early Parkinson's disease? Evidence-Based Answer Treatment of early Parkinson's disease
FPIN's Clinical Inquiries Treatment of Early Parkinson's Disease Clinical Question What is the best medical therapy for early Parkinson's disease? Evidence-Based Answer Treatment of early Parkinson's disease
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
SHARED CARE PRESCRIBING GUIDELINE
 WORKING IN PARTNERSHIP WITH Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath) North East Hampshire & Farnham CCG, Crawley CCG, Horsham & Mid-Sussex
WORKING IN PARTNERSHIP WITH Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath) North East Hampshire & Farnham CCG, Crawley CCG, Horsham & Mid-Sussex
COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date)
") COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Drug, Treatment, Device name Co-careldopa 2000mg/500mg intestinal gel (Duodopa, Solvay Pharmaceuticals)
COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Drug, Treatment, Device name Co-careldopa 2000mg/500mg intestinal gel (Duodopa, Solvay Pharmaceuticals)
APOMORPHINE (Adults) Shared Care Guidelines DRUG:
 Shared Care Guidelines DRUG:") Shared Care Guidelines DRUG: APOMORPHINE (Adults) Indication: Treatment of motor fluctuations in patients with Parkinson's disease which is not sufficiently controlled by oral anti-parkinson medication.
Shared Care Guidelines DRUG: APOMORPHINE (Adults) Indication: Treatment of motor fluctuations in patients with Parkinson's disease which is not sufficiently controlled by oral anti-parkinson medication.
XADAGO (safinamide) oral tablet
 oral tablet") XADAGO (safinamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
XADAGO (safinamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
The Use of Amantadine HCL in Clinical Practice: A Study of Old and New Indications
 The Use of Amantadine HCL in Clinical Practice: A Study of Old and New Indications Carlos Singer, MD* Spiridon Papapetropoulos, MD, PhD* Gadith Uzcategui, BA Lydia Vela, MD * Department of Neurology, University
The Use of Amantadine HCL in Clinical Practice: A Study of Old and New Indications Carlos Singer, MD* Spiridon Papapetropoulos, MD, PhD* Gadith Uzcategui, BA Lydia Vela, MD * Department of Neurology, University
Drugs for Parkinson s Disease
 This Clinical Resource gives subscribers additional insight related to the Recommendations published in July 2017 ~ Resource #330705 Drugs for Parkinson s Disease Parkinson s disease is characterized by
This Clinical Resource gives subscribers additional insight related to the Recommendations published in July 2017 ~ Resource #330705 Drugs for Parkinson s Disease Parkinson s disease is characterized by
The Shaking Palsy of 1817
 The Shaking Palsy of 1817 A Treatment Update on Parkinson s Disease Dr Eitzaz Sadiq Neurologist CH Baragwanath Acadamic Hospital Parkinson s Disease O Premature death of dopaminergic neurons O Symptoms
The Shaking Palsy of 1817 A Treatment Update on Parkinson s Disease Dr Eitzaz Sadiq Neurologist CH Baragwanath Acadamic Hospital Parkinson s Disease O Premature death of dopaminergic neurons O Symptoms
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Treatment of Parkinson s Disease and of Spasticity. Satpal Singh Pharmacology and Toxicology 3223 JSMBS
 Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
GUIDELINES FOR THE MANAGEMENT OF PATIENTS WITH PARKINSON S DISEASE (PD) ADMITTED TO HOSPITAL. Reviewer s Name, Title & address:
 ADMITTED TO HOSPITAL. Reviewer s Name, Title & address:") GUIDELINES FOR THE MANAGEMENT OF PATIENTS WITH PARKINSON S DISEASE (PD) ADMITTED TO HOSPITAL Record Type Clinical Guideline elibrary ID Reference No: CG 1813 Newly developed and approved Trust-wide Clinical
GUIDELINES FOR THE MANAGEMENT OF PATIENTS WITH PARKINSON S DISEASE (PD) ADMITTED TO HOSPITAL Record Type Clinical Guideline elibrary ID Reference No: CG 1813 Newly developed and approved Trust-wide Clinical
Recent Advances in the cause and treatment of Parkinson disease. Anthony Schapira Head of Dept. Clinical Neurosciences UCL Institute of Neurology UCL
 Recent Advances in the cause and treatment of Parkinson disease Anthony Schapira Head of Dept. Clinical Neurosciences UCL Institute of Neurology UCL SOME BACKGROUND incidence rate (per 100.000 person years)
Recent Advances in the cause and treatment of Parkinson disease Anthony Schapira Head of Dept. Clinical Neurosciences UCL Institute of Neurology UCL SOME BACKGROUND incidence rate (per 100.000 person years)
Parkinson s disease: diagnosis and current management
 n DRUG REVIEW Parkinson s disease: diagnosis and current management Lucy Collins MPhil, Gemma Cummins MRCPI and Roger A Barker PhD, MRCP SPL Treatment for Parkinson s should be tailored to the needs of
n DRUG REVIEW Parkinson s disease: diagnosis and current management Lucy Collins MPhil, Gemma Cummins MRCPI and Roger A Barker PhD, MRCP SPL Treatment for Parkinson s should be tailored to the needs of
Clinical Trial Results Posting
 RD..3.2 V1. Page/Seite 1 of/von 5 CT Registry ID#: NCT2428 (ClinicalTrials.gov Identifier number) These results are supplied for informational purposes only. Prescribing decisions should be made based
RD..3.2 V1. Page/Seite 1 of/von 5 CT Registry ID#: NCT2428 (ClinicalTrials.gov Identifier number) These results are supplied for informational purposes only. Prescribing decisions should be made based
Literature Scan: Anti-Parkinson s Agents
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Suffolk PCT Drug & Therapeutics Committee New Medicine Report (Adopted by the CCG until review and futher notice)
") Suffolk PCT Drug & Therapeutics Committee New Medicine Report (Adopted by the CCG until review and futher notice) This drug has been reviewed because it is a product that may be prescribed in primary care.
Suffolk PCT Drug & Therapeutics Committee New Medicine Report (Adopted by the CCG until review and futher notice) This drug has been reviewed because it is a product that may be prescribed in primary care.
Shared Care Guideline
 Shared Care Guideline Rotigotine Executive Summary Indication: Parkinson s disease, either alone or as an adjunct to co-beneldopa or co-careldopa. Patient Group: Patients with early-stage idiopathic Parkinson
Shared Care Guideline Rotigotine Executive Summary Indication: Parkinson s disease, either alone or as an adjunct to co-beneldopa or co-careldopa. Patient Group: Patients with early-stage idiopathic Parkinson
Guideline for the Management of Parkinson s Disease Medication Trust Reference B26/2017
 Guideline for the Management of Parkinson s Disease Medication Trust Reference B26/2017 1. INTRUCTION 1.1 Guideline for the management of Parkinson s Disease Medication in adult patients presenting to
Guideline for the Management of Parkinson s Disease Medication Trust Reference B26/2017 1. INTRUCTION 1.1 Guideline for the management of Parkinson s Disease Medication in adult patients presenting to
New Medicine Recommendation Opicapone (Ongentys ) 50mg hard capsules. For
 50mg hard capsules. For") New Medicine Recommendation Opicapone (Ongentys ) 50mg hard capsules. For adjunctive therapy to preparations of levodopa/ DOPA decarboxylase inhibitors (DDCI) in adult patients with Parkinson's disease
New Medicine Recommendation Opicapone (Ongentys ) 50mg hard capsules. For adjunctive therapy to preparations of levodopa/ DOPA decarboxylase inhibitors (DDCI) in adult patients with Parkinson's disease
What s new for diagnosing and treating Parkinson s Disease?
 What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
Report on New Patented Drugs Azilect
 Report on New Patented Drugs Azilect Under its transparency initiative, the PMPRB publishes the results of the reviews of new patented drugs by Board Staff, for purposes of applying the Board s Excessive
Report on New Patented Drugs Azilect Under its transparency initiative, the PMPRB publishes the results of the reviews of new patented drugs by Board Staff, for purposes of applying the Board s Excessive
Drug Management of Parkinsonism. By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.)
; MSc. (Ped.); MHPE (Ed.)") Drug Management of Parkinsonism By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.) Drug management of Parkinsonism Levodopa Ergot derivatives noamine Oxidaes Inhibitors Catechol-Omethyl
Drug Management of Parkinsonism By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.) Drug management of Parkinsonism Levodopa Ergot derivatives noamine Oxidaes Inhibitors Catechol-Omethyl
05-Nov-15. Impact of Parkinson s Disease in Australia. The Nature of Parkinson s disease 21st Century
 Peter Silburn Professor Clinical Neuroscience University of Queensland Queensland Brain Institute Neurosciences Queensland Impact of in Australia Second most common neurodegenerative disorder Up to 64,000
Peter Silburn Professor Clinical Neuroscience University of Queensland Queensland Brain Institute Neurosciences Queensland Impact of in Australia Second most common neurodegenerative disorder Up to 64,000
Summary of Patient < 3y at Visit 11 (90 months)
") Summary of Patient < 3y at 11 (90 months) Clinician Scoring Page Direct online data entry available? Medication 378 Yes BPW 382 Yes Diagnostic Features 383 Yes UPDRS Clinician 388 Yes CISI-PD 397 Yes MoCA
Summary of Patient < 3y at 11 (90 months) Clinician Scoring Page Direct online data entry available? Medication 378 Yes BPW 382 Yes Diagnostic Features 383 Yes UPDRS Clinician 388 Yes CISI-PD 397 Yes MoCA
NI Formulary: Chapter 4 Central Nervous system
 Hypnotics Anxiolytics Acute state Non drug treatment Temazepam tablets 10mg, 20mg; oral solution 10mg/5ml or Zolpidem tablets 5mg, 10mg or Zopiclone 3.75mg, 7.5mg Non drug treatment Diazepam tablets 2mg,
Hypnotics Anxiolytics Acute state Non drug treatment Temazepam tablets 10mg, 20mg; oral solution 10mg/5ml or Zolpidem tablets 5mg, 10mg or Zopiclone 3.75mg, 7.5mg Non drug treatment Diazepam tablets 2mg,
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
Margo J Nell Dept Pharmacology
 Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
SIFROL â. Contraindications Hypersensitivity to pramipexole or any other component of the product.
 SIFROL â Composition 1 tablet contains 0.088, 0.18 & 0.7 mg (S) 2 amino 4,5,6,7-tetrahydro-6-propylamino-benzothiazole (= pramipexole base) equivalent to 0.125, 0.25 & 1 mg of pramipexole dihydrochloride
SIFROL â Composition 1 tablet contains 0.088, 0.18 & 0.7 mg (S) 2 amino 4,5,6,7-tetrahydro-6-propylamino-benzothiazole (= pramipexole base) equivalent to 0.125, 0.25 & 1 mg of pramipexole dihydrochloride
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
PL CE LIVE July 2015 Forum
 July 2015 PL CE LIVE Rachel Maynard, PharmD Associate Editor Pharmacist s Letter/Pharmacy Technician s Letter CE Information Pharmacist's Letter / Therapeutic Research Center is accredited by the Accreditation
July 2015 PL CE LIVE Rachel Maynard, PharmD Associate Editor Pharmacist s Letter/Pharmacy Technician s Letter CE Information Pharmacist's Letter / Therapeutic Research Center is accredited by the Accreditation
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N.
 PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
BORDEAUX MDS WINTER SCHOOL FOR YOUNG
 BORDEAUX MDS WINTER SCHOOL FOR YOUNG NEUROLOGISTS INFUSION THERAPIES IN PARKINSON S DISEASE Apomorphine, T. Henriksen Tove Henriksen, MD MDS Clinic University Hospital of Bispebjerg, Copenhagen MOTOR FLUCTUATIONS
BORDEAUX MDS WINTER SCHOOL FOR YOUNG NEUROLOGISTS INFUSION THERAPIES IN PARKINSON S DISEASE Apomorphine, T. Henriksen Tove Henriksen, MD MDS Clinic University Hospital of Bispebjerg, Copenhagen MOTOR FLUCTUATIONS
Guidance on Safe Prescribing of Melatonin for Sleep Disorders in Children, Young People and Adults
 Guidance on Safe Prescribing of Melatonin for Sleep Disorders in Children, Young People and Adults Ref: PHARM-0025-v3 Status: FINAL Document type: Guidelines Guidance on Safe Prescribing of Melatonin Page
Guidance on Safe Prescribing of Melatonin for Sleep Disorders in Children, Young People and Adults Ref: PHARM-0025-v3 Status: FINAL Document type: Guidelines Guidance on Safe Prescribing of Melatonin Page
9/26/18. Objectives. Disclosures. Parkinson s Disease Update Clinical and Operational Considerations
 Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Drug treatment of early Parkinson s disease (motor symptoms)
") 5 Drug treatment of early Parkinson s disease (motor symptoms) 5.1 When should treatment be started for a patient with Parkinson s disease? 67 5.2 Are there guidelines for the treatment of Parkinson s
5 Drug treatment of early Parkinson s disease (motor symptoms) 5.1 When should treatment be started for a patient with Parkinson s disease? 67 5.2 Are there guidelines for the treatment of Parkinson s
Drugs used in Parkinsonism
 Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Novel approaches to the pharmacological treatment of Parkinson s disease. Peter Jenner King s College UK
 Novel approaches to the pharmacological treatment of Parkinson s disease Peter Jenner King s College UK Disclosures and Disclaimers Speakers fees and consultancy fees have been received from Britannia
Novel approaches to the pharmacological treatment of Parkinson s disease Peter Jenner King s College UK Disclosures and Disclaimers Speakers fees and consultancy fees have been received from Britannia
2-The age at onset of PD is variable, usually between 50 and 80 years, with a mean onset of 55 years (1).
.") Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Evidence-Based Medical Review Update: Pharmacological and Surgical Treatments of Parkinson s Disease: 2001 to 2004
 Movement Disorders Vol. 20, No. 5, 2005, pp. 523 539 2005 Movement Disorder Society Research Review Evidence-Based Medical Review Update: Pharmacological and Surgical Treatments of Parkinson s Disease:
Movement Disorders Vol. 20, No. 5, 2005, pp. 523 539 2005 Movement Disorder Society Research Review Evidence-Based Medical Review Update: Pharmacological and Surgical Treatments of Parkinson s Disease:
Medicines Management and the Unwell Parkinson s Patient
 Medicines Management and the Unwell Parkinson s Patient Belinda Kessel Geriatrician and Movement Disorder Specialist Princess Royal University Hospital Orpington, Kent The Society for Acute Medicine, 7
Medicines Management and the Unwell Parkinson s Patient Belinda Kessel Geriatrician and Movement Disorder Specialist Princess Royal University Hospital Orpington, Kent The Society for Acute Medicine, 7
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
Effective Shared Care Agreement (ESCA) for drugs used in dementia- Donepezil, Galantamine, Rivastigmine and Memantine
 for drugs used in dementia- Donepezil, Galantamine, Rivastigmine and Memantine") Effective Shared Care Agreement (ESCA) for drugs used in dementia- Donepezil, Galantamine, Rivastigmine and Memantine for the treatment of dementia AREAS OF RESPONSIBILITY FOR THE SHARING OF CARE This
Effective Shared Care Agreement (ESCA) for drugs used in dementia- Donepezil, Galantamine, Rivastigmine and Memantine for the treatment of dementia AREAS OF RESPONSIBILITY FOR THE SHARING OF CARE This
Rasagiline and Rapid Symptomatic Motor Effect in Parkinson s Disease: Review of Literature
 Neurol Ther (2014) 3:41 66 DOI 10.1007/s40120-013-0014-1 REVIEW Rasagiline and Rapid Symptomatic Motor Effect in Parkinson s Disease: Review of Literature Michele Pistacchi Francesco Martinello Manuela
Neurol Ther (2014) 3:41 66 DOI 10.1007/s40120-013-0014-1 REVIEW Rasagiline and Rapid Symptomatic Motor Effect in Parkinson s Disease: Review of Literature Michele Pistacchi Francesco Martinello Manuela