Procedures in the Sleep Laboratory
|
|
|
- Morgan Miles
- 6 years ago
- Views:
Transcription

1 AAST Technologist Fundamentals Date: May 7, 2017 Focus Conference Location: Orlando, Florida Workshop Procedures in the Sleep Laboratory Laree Fordyce, RST, RPSGT, CCRP
2 Conflict of Interest Disclosures for Speakers X 1. I do not have any potential conflicts to disclose. 2. I wish to disclose the following potential conflicts of interest: Type of Potential Conflict Details of Potential Conflict Grant/Research Support Consultant Speakers Bureaus Financial support Other 3. The material presented in this lecture has no relationship with any of these potential conflicts, OR 4. This talk presents material that is related to one or more of these potential conflicts, and the following objective references are provided as support for this lecture:

3 Objectives 1. Review the American Academy of Sleep Medicine practice parameters for testing; and 2. Discuss recording, documentation and reporting techniques for Polysomnography, MSLT, MWT and Home Sleep Apnea Testing (HSAT).


4 AASM Practice Parameters for Testing PSG MSLT MWT HSAT
5 PSG
6 Recording Polysomnography When starting a study, we need to make sure that we have a history, physical exam, previous test results, referral and insurance information, physician s orders, etc.) The sleep technologist prepares for and monitors the recording, requiring expertise in normal and abnormal sleep and multiple technical and medical monitors. The sleep technologist verifies and maintains the quality of the recording and can decipher artifact from true physiological signals. The technologist can recognize when medical intervention is required and responds according to the protocols provided by the medical director. Therefore, attended polysomnography by a trained sleep technologist produces the highest quality clinical tool.

7 Documentation The sleep technologist is the eyes and ears of the interpreting sleep physician.

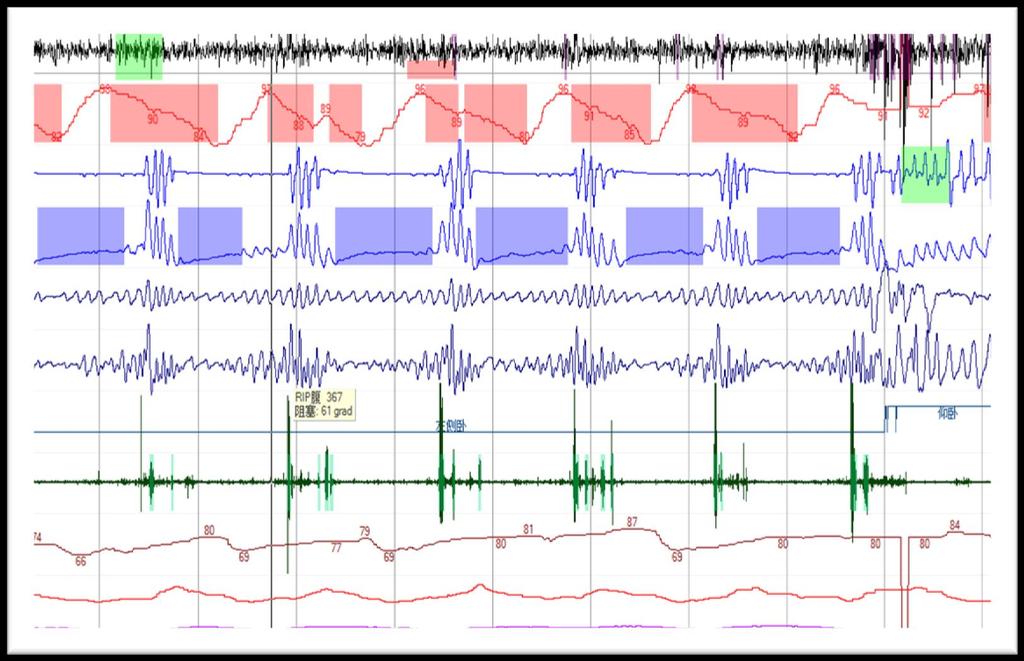
8 What do you see?

9 Sweat artifact TECH NOTE: Pt sweating +++, turned on Fan
10 What is happening here?
11 Poor impedance of M2 electrode

12 Documentation The sleep technologist is the eyes and ears of the interpreting sleep physician. Document everything you observe. Document any changes that you make throughout the recording.

13 Reporting The standard diagnostic PSG requires the recording and evaluation of sleep stages and arousals, respiration, limb movements, snoring, oximetry, body position, and cardiac rhythm disturbances. The resulting documentation is used to diagnose or assess the treatment of sleep disorders

14 Version 2.4
15 STAGES OF SLEEP Stage W Stage N1 Stage N2 Wakefulness NREM1 NREM2 Stage N3 NREM3 Stage R REM
16 The Polysomnographic Report Patient Information: Name: Ht-cm: Interpreting Physician: Age: Wt-kg: Referral Provider: DOB : BMI: Recorded By: Sex: Neck Circumference: Study Indication: PHN : Study # : Polysomnography was conducted on the night of 24/03/2016. The following parameters were monitored: frontal, central and occipital EEG, electro-oculogram (EOG), sub-mental EMG, nasal and oral airflow, anterior tibialis EMG, body position and electrocardiogram. Additionally, thoracic and abdominal movements were recorded by inductance plethysmography. Oxygen saturation (SpO2) was monitored using a pulse oximeter. The tracing was scored using 30 second epochs. Hypopneas were scored per AASM definition VIII4.B (3% desaturation). Tech Comments:
17 Sleep Summary Lights Out: 8:30:17 PM Stage Duration % TST Lights On: 5:53:47 AM N1 3.5 min 0.6% Total Recording Time (TIB): min N min 48.5% Total Sleep Time (TST): min N min 28.9% Sleep Period Time: min R min 21.9% Sleep Onset: 8:35:47 PM Sleep Efficiency: 97.4 % Latencies From Lights Out From Sleep Onset Wake After Sleep Onset (WASO): 9.0 min N1 5.5 min 0.0 min Wake During Sleep 6.5 min N2 7.0 min 17.0 min Total Wake Time: 14.5 min N min 17.0 min % Wake Time: 2.6 R min
18 Respiratory Summary Central Mixed Obstructive Avg Max # Avg Max # Avg Max # Apneas, NREM: Apneas, REM: Apneas, Total: Event Statistics Total WAI # W/O AI Apneas: Hypopneas: A + H Total: 65 AHI: Oximetry Data Min SpO2 value TST: 87% Average SpO2 (TIB): 96% Min SpO2 w/ Respiratory Event: 89% Average SpO2 (TST): 96% Desaturations #: 4 Desaturation Index: 0.4/hr
19 Periodic Leg Movements Total # Limb Movement 83 Limb Movement Index 9.0 Total # PLMS 28 PLMS Index 3.0 Total # PLMS Arousals: 7 PLMS Arousal Index: Arousals Respiratory: Leg Movements: Snore: Spontaneous: Total: Arousal Index: REM: NREM: Arousals:

20 MSLT
21 MSLT Box 1 Recommendations for the MSLT Protocol (Adapted from Carskadon and colleagues, Guidelines for the multiple sleep latency test (MSLT): a standard measure of sleepiness 9. Modified by collective expert opinion using Rand/UCLA Appropriateness Method) 1. The MSLT consists of five nap opportunities performed at two hour intervals. The initial nap opportunity begins 1.5 to 3 hours after termina- tion of the nocturnal recording. A shorter four-nap test may be performed but this test is not reliable for the diagnosis of narcolepsy unless at least two sleep onset REM periods have occurred. 2. The MSLT must be performed immediately following polysomnography recorded during the individual s major sleep period. The use of MSLT to support a diagnosis of narcolepsy is suspect if TST on the prior night sleep is less than 6 hours. The test should not be performed after a split- night sleep study (combination of diagnostic and therapeutic studies in a single night). 3. Sleep logs may be obtained for 1 week prior to the MSLT to assess sleep-wake schedules. 4. Standardization of test conditions is critical for obtaining valid results. Sleep rooms should be dark and quiet during testing. Room tempera- ture should be set based on the patient s comfort level. 5. Stimulants, stimulant-like medications, and REM suppressing medications should ideally be stopped 2 weeks before MSLT. Use of the patient s other usual medications (e.g., antihypertensives, insulin, etc.) should be thoughtfully planned by the sleep clinician before MSLT testing so that undesired influences by the stimulating or sedating properties of the medications are minimized. Drug screening may be indicated to ensure that sleepiness on the MSLT is not pharmacologically induced. Drug screening is usually performed on the morning of the MSLT but its timing and the circumstances of the testing may be modified by the clinician. Smoking should be stopped at least 30 minutes prior to each nap opportunity. Vigorous physical activity should be avoided during the day and any stimulating activities by the patient should end at least 15 minutes prior to each nap opportunity. The patient must abstain from any caffeinated beverages and avoid unusual exposures to bright sunlight. A light breakfast is rec- ommended at least 1 hour prior to the first trial, and a light lunch is recommended immediately after the termination of the second noon trial. 6. Sleep technologists who perform MSLTs should be experienced in conducting the test. 7. The conventional recording montage for the MSLT includes central EEG (C3-A2, C4-A1) and occipital (O1-A2, O2-A1) derivations, left and right eye electrooculograms (EOGs), mental/submental electromyogram (EMG), and electrocardiogram (EKG). 8.. Prior to each nap opportunity, the patient should be asked if they need to go to the bathroom or need other adjustments for comfort. Standard instructions for bio-calibrations (i.e., patient calibrations) prior to each nap include: (1) lie quietly with your eyes open for 30 seconds, (2) close both eyes for 30 seconds, (3) without moving your head, look to the right, then left, then right, then left, right and then left, (4) blink eyes slow- ly for 5 times, and (5) clench or grit your teeth tightly together. 9. With each nap opportunity the subject should be instructed as follows: Please lie quietly, assume a comfortable position, keep your eyes closed and try to fall asleep. The same instructions should be given prior to every test. Immediately after these instructions are given, bedroom lights are turned off, signaling the start of the test. Between naps, the patient should be out of bed and prevented from sleeping. This generally requires continuous observation by a laboratory staff member. 10. Sleep onset for the clinical MSLT is determined by the time from lights out to the first epoch of any stage of sleep, including stage 1 sleep. Sleep onset is defined as the first epoch of greater than 15 sec of cumulative sleep in a 30-sec epoch. The absence of sleep on a nap opportunity is recorded as a sleep latency of 20 minutes. This latency is included in the calculation of mean sleep latency (MSL). In order to assess for the occurrence of REM sleep, in the clinical MSLT the test continues for 15 minutes from after the first epoch of sleep. The duration of 15 minutes is determined by clock time, and is not determined by a sleep time of 15 minutes. REM latency is taken as the time of the first epoch of sleep to the beginning of the first epoch of REM sleep regardless of the intervening stages of sleep or wakefulness. 11. A nap session is terminated after 20 minutes if sleep does not occur. 12. The MSLT report should include the start and end times of each nap or nap opportunity, latency from lights out to the first epoch of sleep, mean sleep latency (arithmetic mean of all naps or nap opportunities), and number of sleep-onset REM periods (defined as greater than 15 sec of REM sleep in a 30-sec epoch). 13. Events that represent deviation from standard protocol or conditions should be documented by the sleep technologist for review by the inter- preting sleep clinician.
22 Multiple Sleep Latency Test - Recording 4-5 nap opportunities performed at 2 hour intervals Following a PSG» follow patient s habitual schedule (sleep logs)» use for narcolepsy diagnosis is suspect if TST < 6 hours, usefulness» not after split night study with CPAP First test: hrs. after lights on Stimulants, stimulant-like medications and REM suppressing medications should be stopped 2 weeks prior to MSLT Drug screening may be indicated Smoking stopped at least 30 minutes prior to each nap No caffeine No sleep/dozing between tests
23 Multiple Sleep Latency Test - Documentation Montage (EEG, EOG, EMG and EKG) Bio-cals prior to each nap. Instruct patient to Please lie quietly, in a comfortable position with your eyes closed Sleep onset:» first epoch of any stage of sleep» Nap will be terminated after 15 minutes from sleep onset» if no sleep, latency is 20 min
24 MSLT - Reporting The MSLT report should include: - the start and end times of each nap or nap opportunity, - latency from lights out to the first epoch of sleep, - mean sleep latency (arithmetic mean of all naps or nap opportunities), - number of sleep-onset REM periods (defined as greater than 15 sec of REM sleep in a 30-sec epoch).

25 SLEEP ONSET (Clinical MSLT, AASM recommends for PSG)
26 MWT Box 2 Recommendations for the MWT protocol (Developed from methods of Doghramji and colleagues, A normative study of the maintenance of wakefulness test (MWT), Modified by collective expert opinion using Rand/UCLA Appropriateness Method) 1. The 4-trial MWT 40-minute protocol is recommended. The MWT consists of four trials performed at two hour intervals, with the first trial beginning about 1.5 to 3 hours after the patient s usual wake-up time. This usually equates to a first trial starting at 0900 or 1000 hours. 2. Performance of a PSG prior to MWT should be decided by the clinician based on clinical circumstances. 3. Based on the Rand/UCLA Appropriateness Method, no consensus was reached regarding the use of sleep logs prior to the MWT; there are instances, based on clinical judgment, when they may be indicated. 4. The room should be maximally insulated from external light. The light source should be positioned slightly behind the subject s head such that it is just out of his/her field of vision, and should deliver an illuminance of lux at the corneal level (a 7.5 W night light can be used, placed 1 foot off the floor and 3 feet laterally removed from the subject s head). Room temperature should be set based on the patient s com- fort level. The subject should be seated in bed, with the back and head supported by a bedrest (bolster pillow) such that the neck is not uncom- fortably flexed or extended. 5. The use of tobacco, caffeine and other medications by the patient before and during MWT should be addressed and decided upon by the sleep clinician before MWT. Drug screening may be indicated to ensure that sleepiness/wakefulness on the MWT is not influenced by substances other than medically prescribed drugs. Drug screening is usually performed on the morning of the MWT but its timing and the circumstances of the testing may be modified by the clinician. A light breakfast is recommended at least 1 hour prior to the first trial, and a light lunch is rec- ommended immediately after the termination of the secondnoon trial. 6. Sleep technologists who perform the MWT should be experienced in conducting the test. 7. The conventional recording montage for the MWT includes central EEG (C3-A2, C4-A1) and occipital (O1-A2, O2-A1) derivations, left and right eye electrooculograms (EOGs), mental/submental electromyogram (EMG), and electrocardiogram (EKG). 8. Prior to each trial, the patient should be asked if they need to go to the bathroom or need other adjustments for comfort. Standard instructions for bio-calibrations (i.e., patient calibrations) prior to each trial include: (1) sitlie quietly with your eyes open for 30 seconds, (2) close both eyes for 30 seconds, (3) without moving your head, look to the right, then left, then right, then left, right and then left, (4) blink eyes slowly for 5 times, and (5) clench or grit your teeth tightly together. 9. Instructions to the patient consist of the following: Please sit still and remain awake for as long as possible. Look directly ahead of you, and do not look directly at the light. Patients are not allowed to use extraordinary measures to stay awake such as slapping the face or singing. 10. Sleep onset is defined as the first epoch of greater than 15 sec of cumulative sleep in a 30-sec epoch. 11. Trials are ended after 40 minutes if no sleep occurs, or after unequivocal sleep, defined as three consecutive epochs of stage 1 sleep, or one epoch of any other stage of sleep. 12. The following data should be recorded: start and stop times for each trial, sleep latency, total sleep time, stages of sleep achieved for each trial, and the mean sleep latency (the arithmetic mean of the four trials). 13. Events that represent deviation from standard protocol or conditions should be documented by the sleep technologist for review by the sleep specialist.
27 Maintenance of Wakefulness Test - Recording 4 Trial opportunities performed at 2 hour intervals A PSG prior to the MWT will be decided by the clinician based on circumstances» First test: hrs. after lights on The room should be maximally insulated from external light. The light source should be positioned slightly behind the subject s head but outt of his/her field of vision The use of tobacco, caffeine and other medications by the patient before and during MWT should be addressed and decided upon by the sleep clinician before MWT. Drug screening may be indicated to ensure that sleepiness/wakefulness on the MWT is not influenced by substances other than medically prescribed drugs.
28 Maintenance of Wakefulness Test - Documentation Montage (EEG, EOG, EMG and EKG) Bio-cals prior to each nap. Instruct patient to Please sit still and remain awake for as long as possible. Look directly ahead of you, and do not look directly at the light. Sleep onset:» Trial is 40 minutes» first epoch of any stage of sleep, trial is terminated» if no sleep, latency is 40 min
29 MWT - Reporting The MWT data should be recorded: - start and stop times for each trial, - sleep latency, total sleep time, - stages of sleep achieved for each trial, - the mean sleep latency (the arithmetic mean of the four trials).
30 HSAT
31 What is a Home Sleep Apnea Test? Type 2 PM: full unattended polysomnography ( 7 channels) Type 3 PM: limited channel devices (usually 4 7 channels) Must include airflow and effort channels Type 4 PM: 1 or 2 channels usually including oximetry as one of the parameters
32 HSAT Indicated for adult patients with a high pretest probability of moderate to severe OSA. HSAT is not appropriate and is contraindicated for: - pediatric patients - patients with comorbid medical conditions including, but not limited to, moderate to severe pulmonary disease, neuromuscular disease, or congestive heart failure, and patients suspected of having other sleep disorders HSAT is also contraindicated for patients with medical or cognitive issues that impact the safety of a patient using the device unattended. HSAT should not be used for general screening.

33 AASM Guidelines for PM JCSM Journal of Clinical Sleep Medicine, Vol. 3, No. 7, 2007

34 What device do I use?

35 The PM device used for HSAT by a sleep center should be chosen carefully for its intended purpose by the technical staff and medical director. - Factors to consider are ease of use by the patient, - recording parameters - the ability to customize the raw data view, - the ability to customize reports, - Cost; the device, the cost of consumables (cannulas, disposable sensors, batteries), database features, and the availability of technical support.
36 Physiological and Recording For Type 2 devices only: Parameters EEG electrodes should be placed according to the International system of Electrode Placement (3). The recommended EEG derivation is F4-M1, C4-M1, and O2-M1 recorded at a minimum sampling rate of 200 Hz with impedances of 5 KΩ or less. The recommended sampling rate is 500 Hz; filter settings for this parameter are LFF 0.3 Hz and HFF 35 Hz. EOG electrodes should be placed at E1 and E2 according to AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications standards (4). The recommended EOG derivation is E1-M2, E2-M2 recorded at a minimum sampling rate of 200 Hz with impedances of 5 KΩ or less. The recommended sampling rate is 500 Hz filter settings for this parameter are LFF 0.3 Hz and HFF 35 Hz. Chin EMG electrodes should be placed above and below the mandible on the mental and submental muscles of the chin as specified in the AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications standards. The derivation for recording chin EMG consists of a submental electrode referred to the electrode placed above the mandible on the mental muscle. The minimum sampling rate is 200 Hz. The recommended sampling rate is 500 Hz. Filter settings for this parameter are LFF 10 Hz and HFF 100 Hz.
37 HSAT Devices Type 2 4 Recording Parameters A nasal air pressure transducer is the most common mode of recording airflow in portable monitoring. The recommended respiratory effort sensor is calibrated or un-calibrated respiratory inductance plethysmography (RIP). The minimum acceptable sampling rate is 25 Hz. The preferred sampling rate is 100 Hz. Filter settings for the respiratory data are LFF 0.1 Hz, HFF 15 Hz. The recommended blood oxygen sensor is a pulse oximeter with an averaging time of < 3 seconds. Finger probes can be reusable or disposable. A slipped or disconnected oximeter probe is one of the more common reasons for PM failure. The minimum recommended sampling rate is 10 Hz. The preferred sampling rate is 25 Hz, which improves the ability to recognize artifact.
38 A pulse rate is generally obtained from the pulse oximeter. The minimum acceptable sampling rate is 10 Hz. The preferred sampling rate is 25 Hz, which improves the ability to recognize artifact. Modified Lead II is the recommended placement for recording the electrocardiogram (ECG). The minimum acceptable sampling rate is 200 Hz. The recommended sampling rate of 500 Hz improves waveform definition. Filter settings for ECG are LFF 0.3, HFF 70 Hz. Snoring can be derived from the nasal air pressure transducer signal, or can be recorded as a separate channel with a microphone device The minimum acceptable sampling rate for the collection of snoring sound or vibration data is 200 Hz. The preferred sampling rate is 500Hz. Filter settings are LFF 10 Hz, HFF 100 Hz.
39 Version 2.4
40 Initializing the HSAT Device - Re-charging or replacing the batteries for every test. - Previous data must be cleared before a new recording can be acquired. - Enter patient information can be entered and the device initialized to collect new data. - Devices can be set to start at a pre-set time, or can be manually started by the patient at bedtime. * It is important to know the maximum recording time capability, which might range from one to seven or more nights of recording time.
41 HSAT - Recording the patient picks up the PM device and is instructed how to apply it at home. Take a history, updated meds, changes in sleep patterns. Make sure the patient has take home instructions on how to apply the PM device. - Written instructions with pictorial diagrams of each component and step in the process - Many manufacturers provide video instruction accessible online or on a pre-recorded disk. - A demonstration on video or by the technologist educator can be followed by having the patient apply the device and sensors themselves. It is important for the patient to be given a 24-hour access phone number for technical support if any questions or problems arise.
42 HSAT - Documentation As with PSG, the sleep technologist is responsible for ensuring that all required documentation (history, physical exam, previous test results, referral and insurance information, physician s orders, etc.) is available and reviewed prior to dispensing the PM device for testing. Patient ID verification and insurance verification should be completed at intake, as well as the documentation that the privacy notice was made available to the patient. The sleep center may require the patient to sign a return agreement stating when and where to return the device that includes device replacement or late fee terms. A form that includes pre-sleep and post-sleep questions should be dispensed to the patient with the device and returned for the interpreting physician s review. A comprehensive database should be kept to track HSAT procedures, diagnosis codes, turnaround time, and failure rates. Optimally, this data should be tied to patient outcomes.
43 HSAT - Documentation DEVICE RETURN AND DATA UPLOAD the data should be checked for minimal adequacy (required signals recorded for a minimum time set by the center) and re-dispensed at the same visit when a failure is detected. Document any issues the patient had during the night.
44

45 HSAT - Reporting The scoring technologist evaluates whether the minimum data collection requirement has been met (set by the sleep center). The manufacturer may provide an automated analysis of the raw data, an experienced and qualified technologist must manually edit and verify the results. At minimum, respiratory events by type, oxygen desaturations, and fail periods must be accurately marked. Scoring should be performed in accordance with the AASM scoring manual (3). The scorer prepares a scoring report, which should indicate that the study was manually edited, and communicates any limitations to the recorded data, including failures. The scoring report and scored raw data is then made available to the interpreting sleep specialist for interpretation.

46 HSAT - Other All technical personnel must be trained by the Medical Director of the sleep center, a board certified sleep specialist, or a registered sleep technologist with the RST or RPSGT credential. Quality Assurance Equipment Safety Infection Control Equipment Decontamination

47

48 AASM Practice Parameters for Testing PSG MSLT MWT HSAT

49

50 What Factor does not matter when selecting a PM device? A. Ease of use by the patient B. Cost of consumables C. the ability to auto score the study D. the ability to customize reports

51 During an MSLT a patient has REM on Naps 2 and 3. Is a fifth nap needed? A. Yes B. No

52 Without any sleep, a MWT is performed for? A. 20 minutes B. 40 minutes C. 15 minutes D. 30 seconds

53 The recommended averaging time of a pulse oximeter is? A. < 1 second B. < 2 seconds C. < 3 seconds D.< 1 minute

54 When performing any study, which of the following is most important? A. Recording techniques B. Documentation techniques C. Reporting techniques D. All of the above


55 Questions??
Milena Pavlova, M.D., FAASM Department of Neurology, Brigham and Women's Hospital Assistant Professor of Neurology, Harvard Medical School Medical
 Milena Pavlova, M.D., FAASM Department of Neurology, Brigham and Women's Hospital Assistant Professor of Neurology, Harvard Medical School Medical Director, Faulkner EEG and Sleep Testing Center Course
Milena Pavlova, M.D., FAASM Department of Neurology, Brigham and Women's Hospital Assistant Professor of Neurology, Harvard Medical School Medical Director, Faulkner EEG and Sleep Testing Center Course
Out of Center Sleep Testing (OCST) - Updated July 2012
 - Updated July 2012") Out of Center Sleep Testing (OCST) - Updated July 2012 SUMMARY: Out of center sleep testing (OCST) can be used as an alternative to full, attended polysomnography (PSG) for the diagnosis of obstructive
Out of Center Sleep Testing (OCST) - Updated July 2012 SUMMARY: Out of center sleep testing (OCST) can be used as an alternative to full, attended polysomnography (PSG) for the diagnosis of obstructive
MWT PROTOCOL PURPOSE POLICY
 PURPOSE A standard MWT protocol that is consistent with AASM practice parameters promotes consistency, allows comparisons between tests, and ensures accurate interpretations that are consistent with published
PURPOSE A standard MWT protocol that is consistent with AASM practice parameters promotes consistency, allows comparisons between tests, and ensures accurate interpretations that are consistent with published
NATIONAL COMPETENCY SKILL STANDARDS FOR PERFORMING POLYSOMNOGRAPHY/SLEEP TECHNOLOGY
 NATIONAL COMPETENCY SKILL STANDARDS FOR PERFORMING POLYSOMNOGRAPHY/SLEEP TECHNOLOGY Polysomnography/Sleep Technology providers practice in accordance with the facility policy and procedure manual which
NATIONAL COMPETENCY SKILL STANDARDS FOR PERFORMING POLYSOMNOGRAPHY/SLEEP TECHNOLOGY Polysomnography/Sleep Technology providers practice in accordance with the facility policy and procedure manual which
Split Night Protocols for Adult Patients - Updated July 2012
 Split Night Protocols for Adult Patients - Updated July 2012 SUMMARY: Sleep technologists are team members who work under the direction of a physician practicing sleep disorders medicine. Sleep technologists
Split Night Protocols for Adult Patients - Updated July 2012 SUMMARY: Sleep technologists are team members who work under the direction of a physician practicing sleep disorders medicine. Sleep technologists
Basics of Polysomnography. Chitra Lal, MD, FCCP, FAASM Assistant professor of Medicine, Pulmonary, Critical Care and Sleep, MUSC, Charleston, SC
 Basics of Polysomnography Chitra Lal, MD, FCCP, FAASM Assistant professor of Medicine, Pulmonary, Critical Care and Sleep, MUSC, Charleston, SC Basics of Polysomnography Continuous and simultaneous recording
Basics of Polysomnography Chitra Lal, MD, FCCP, FAASM Assistant professor of Medicine, Pulmonary, Critical Care and Sleep, MUSC, Charleston, SC Basics of Polysomnography Continuous and simultaneous recording
Appendix 1. Practice Guidelines for Standards of Adult Sleep Medicine Services
 Appendix 1 Practice Guidelines for Standards of Adult Sleep Medicine Services 1 Premises and Procedures Out-patient/Clinic Rooms Sleep bedroom for PSG/PG Monitoring/Analysis/ Scoring room PSG equipment
Appendix 1 Practice Guidelines for Standards of Adult Sleep Medicine Services 1 Premises and Procedures Out-patient/Clinic Rooms Sleep bedroom for PSG/PG Monitoring/Analysis/ Scoring room PSG equipment
Coding for Sleep Disorders Jennifer Rose V. Molano, MD
 Practice Coding for Sleep Disorders Jennifer Rose V. Molano, MD Accurate coding is an important function of neurologic practice. This section of is part of an ongoing series that presents helpful coding
Practice Coding for Sleep Disorders Jennifer Rose V. Molano, MD Accurate coding is an important function of neurologic practice. This section of is part of an ongoing series that presents helpful coding
Pediatric Considerations in the Sleep Lab
 AAST Technologist Fundamentals Date: May 7, 2017 Focus Conference Location: Orlando, Florida Workshop Pediatric Considerations in the Sleep Lab By Joel Porquez, BS, RST/RPSGT, CCSH X X X X X X Conflict
AAST Technologist Fundamentals Date: May 7, 2017 Focus Conference Location: Orlando, Florida Workshop Pediatric Considerations in the Sleep Lab By Joel Porquez, BS, RST/RPSGT, CCSH X X X X X X Conflict
A 74-year-old man with severe ischemic cardiomyopathy and atrial fibrillation
 1 A 74-year-old man with severe ischemic cardiomyopathy and atrial fibrillation The following 3 minute polysomnogram (PSG) tracing was recorded in a 74-year-old man with severe ischemic cardiomyopathy
1 A 74-year-old man with severe ischemic cardiomyopathy and atrial fibrillation The following 3 minute polysomnogram (PSG) tracing was recorded in a 74-year-old man with severe ischemic cardiomyopathy
Polysomnography Course Session: Sept 2017
 Polysomnography Course Session: Sept 2017 General Information Polysomnography course will be held at SLEEP AND ALERTNESS CLINIC Med-West Medical centre 750 Dundas St. W., Suite 2-259 (Conference Room)
Polysomnography Course Session: Sept 2017 General Information Polysomnography course will be held at SLEEP AND ALERTNESS CLINIC Med-West Medical centre 750 Dundas St. W., Suite 2-259 (Conference Room)
The AASM Manual for the Scoring of Sleep and Associated Events
 The AASM Manual for the Scoring of Sleep and Associated Events Summary of Updates in Version 2.1 July 1, 2014 The American Academy of Sleep Medicine (AASM) is committed to ensuring that The AASM Manual
The AASM Manual for the Scoring of Sleep and Associated Events Summary of Updates in Version 2.1 July 1, 2014 The American Academy of Sleep Medicine (AASM) is committed to ensuring that The AASM Manual
Polysomnography Artifacts and Updates on AASM Scoring Rules. Robin Lloyd, MD, FAASM, FAAP 2017 Utah Sleep Society Conference
 Polysomnography Artifacts and Updates on AASM Scoring Rules Robin Lloyd, MD, FAASM, FAAP 2017 Utah Sleep Society Conference x Conflict of Interest Disclosures for Speakers 1. I do not have any relationships
Polysomnography Artifacts and Updates on AASM Scoring Rules Robin Lloyd, MD, FAASM, FAAP 2017 Utah Sleep Society Conference x Conflict of Interest Disclosures for Speakers 1. I do not have any relationships
(To be filled by the treating physician)
") CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
Artifact Recognition and Troubleshooting
 Artifact Recognition and Troubleshooting 2017 Focus Fall Super Session The Best of the Best For Respiratory Therapists and Sleep Technologists The Doubletree Hilton Hotel Pittsburgh, PA Thursday Sept.
Artifact Recognition and Troubleshooting 2017 Focus Fall Super Session The Best of the Best For Respiratory Therapists and Sleep Technologists The Doubletree Hilton Hotel Pittsburgh, PA Thursday Sept.
Sleep 101. Kathleen Feeney RPSGT, RST, CSE Business Development Specialist
 Sleep 101 Kathleen Feeney RPSGT, RST, CSE Business Development Specialist 2016 Why is Sleep Important More than one-third of the population has trouble sleeping (Gallup) Obstructive Sleep Apnea Untreated
Sleep 101 Kathleen Feeney RPSGT, RST, CSE Business Development Specialist 2016 Why is Sleep Important More than one-third of the population has trouble sleeping (Gallup) Obstructive Sleep Apnea Untreated
The AASM Manual for the Scoring of Sleep and Associated Events
 The AASM Manual for the Scoring of Sleep and Associated Events The 2007 AASM Scoring Manual vs. the AASM Scoring Manual v2.0 October 2012 The American Academy of Sleep Medicine (AASM) is committed to ensuring
The AASM Manual for the Scoring of Sleep and Associated Events The 2007 AASM Scoring Manual vs. the AASM Scoring Manual v2.0 October 2012 The American Academy of Sleep Medicine (AASM) is committed to ensuring
Assessment of Sleep Disorders DR HUGH SELSICK
 Assessment of Sleep Disorders DR HUGH SELSICK Goals Understand the importance of history taking Be able to take a basic sleep history Be aware the technology used to assess sleep disorders. Understand
Assessment of Sleep Disorders DR HUGH SELSICK Goals Understand the importance of history taking Be able to take a basic sleep history Be aware the technology used to assess sleep disorders. Understand
Excessive Daytime Sleepiness Associated with Insufficient Sleep
 Sleep, 6(4):319-325 1983 Raven Press, New York Excessive Daytime Sleepiness Associated with Insufficient Sleep T. Roehrs, F. Zorick, J. Sicklesteel, R. Wittig, and T. Roth Sleep Disorders and Research
Sleep, 6(4):319-325 1983 Raven Press, New York Excessive Daytime Sleepiness Associated with Insufficient Sleep T. Roehrs, F. Zorick, J. Sicklesteel, R. Wittig, and T. Roth Sleep Disorders and Research
AASM guidelines, when available. Does this mean if our medical director chooses for us to use an alternative rule that our accreditation is at risk?
 GENERAL G.1. I see that the STANDARDS FOR ACCREDITATION state that we are to use the recommended AASM guidelines, when available. Does this mean if our medical director chooses for us to use an alternative
GENERAL G.1. I see that the STANDARDS FOR ACCREDITATION state that we are to use the recommended AASM guidelines, when available. Does this mean if our medical director chooses for us to use an alternative
Sleep Studies: Attended Polysomnography and Portable Polysomnography Tests, Multiple Sleep Latency Testing and Maintenance of Wakefulness Testing
 Portable Polysomnography Tests, Multiple Sleep Latency Testing and Maintenance of Wakefulness Testing MP9132 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated
Portable Polysomnography Tests, Multiple Sleep Latency Testing and Maintenance of Wakefulness Testing MP9132 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated
The International Franco - Palestinian Congress in Sleep Medicine
 The International Franco - Palestinian Congress in Sleep Medicine Temporomandibular Disorders and Sleep Apnea 26 and 27 October, 2017 Notre Dame Hotel, Jerusalem Polysomnography Reports Interpreting the
The International Franco - Palestinian Congress in Sleep Medicine Temporomandibular Disorders and Sleep Apnea 26 and 27 October, 2017 Notre Dame Hotel, Jerusalem Polysomnography Reports Interpreting the
PORTABLE OR HOME SLEEP STUDIES FOR ADULT PATIENTS:
 Sleep Studies: Attended Polysomnography and Portable Polysomnography Tests, Multiple Sleep Latency Testing and Maintenance of Wakefulness Testing MP9132 Covered Service: Prior Authorization Required: Additional
Sleep Studies: Attended Polysomnography and Portable Polysomnography Tests, Multiple Sleep Latency Testing and Maintenance of Wakefulness Testing MP9132 Covered Service: Prior Authorization Required: Additional
Polysomnography (PSG) (Sleep Studies), Sleep Center
 (Sleep Studies), Sleep Center") Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
linkedin.com/in/lizziehillsleeptechservices 1
 BSS2015 Hands-On Tech Breakfast SCORING SLEEP USING AASM GUIDELINES: A BRIEF INTRODUCTION Lizzie Hill BSc RPSGT EST Specialist Respiratory Clinical Physiologist, Royal Hospital for Sick Children, Edinburgh
BSS2015 Hands-On Tech Breakfast SCORING SLEEP USING AASM GUIDELINES: A BRIEF INTRODUCTION Lizzie Hill BSc RPSGT EST Specialist Respiratory Clinical Physiologist, Royal Hospital for Sick Children, Edinburgh
3/13/2014. Home Sweet Home? New Trends in Testing for Obstructive Sleep Apnea. Disclosures. No relevant financial disclosures
 2014 Big Sky Pulmonary Conference Home Sweet Home? New Trends in Testing for Obstructive Sleep Apnea Eric Olson, MD Associate Professor of Medicine Co-Director, Center for Sleep Medicine Mayo Clinic olson.eric@mayo.edu
2014 Big Sky Pulmonary Conference Home Sweet Home? New Trends in Testing for Obstructive Sleep Apnea Eric Olson, MD Associate Professor of Medicine Co-Director, Center for Sleep Medicine Mayo Clinic olson.eric@mayo.edu
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: October 15, 2018 Related Policies: 2.01.18 Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome Polysomnography for Non-Respiratory Sleep Disorders
FEP Medical Policy Manual Effective Date: October 15, 2018 Related Policies: 2.01.18 Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome Polysomnography for Non-Respiratory Sleep Disorders
Questions: What tests are available to diagnose sleep disordered breathing? How do you calculate overall AHI vs obstructive AHI?
 Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
Simplest method: Questionnaires. Retrospective: past week, month, year, lifetime Daily: Sleep diary What kinds of questions would you ask?
 Spencer Dawson Simplest method: Questionnaires Retrospective: past week, month, year, lifetime Daily: Sleep diary What kinds of questions would you ask? Did you nap during the day? Bed time and rise time
Spencer Dawson Simplest method: Questionnaires Retrospective: past week, month, year, lifetime Daily: Sleep diary What kinds of questions would you ask? Did you nap during the day? Bed time and rise time
Medicare CPAP/BIPAP Coverage Criteria
 Medicare CPAP/BIPAP Coverage Criteria For any item to be covered by Medicare, it must 1) be eligible for a defined Medicare benefit category, 2) be reasonable and necessary for the diagnosis or treatment
Medicare CPAP/BIPAP Coverage Criteria For any item to be covered by Medicare, it must 1) be eligible for a defined Medicare benefit category, 2) be reasonable and necessary for the diagnosis or treatment
Patterns of Sleepiness in Various Disorders of Excessive Daytime Somnolence
 Sleep, 5:S165S174 1982 Raven Press, New York Patterns of Sleepiness in Various Disorders of Excessive Daytime Somnolence F. Zorick, T. Roehrs, G. Koshorek, J. Sicklesteel, *K. Hartse, R. Wittig, and T.
Sleep, 5:S165S174 1982 Raven Press, New York Patterns of Sleepiness in Various Disorders of Excessive Daytime Somnolence F. Zorick, T. Roehrs, G. Koshorek, J. Sicklesteel, *K. Hartse, R. Wittig, and T.
CHANGING SHAPE OF SLEEP STUDIES
 CHANGING SHAPE OF SLEEP STUDIES JAMES C. O BRIEN MD FCCP, FAASM MEDICAL DIRECTOR, PROHEALTH PHYSICIANS SLEEP CENTERS 10/19/2107 GOALS OF MY TALK-- Review the types of sleep studies Provide clinical information
CHANGING SHAPE OF SLEEP STUDIES JAMES C. O BRIEN MD FCCP, FAASM MEDICAL DIRECTOR, PROHEALTH PHYSICIANS SLEEP CENTERS 10/19/2107 GOALS OF MY TALK-- Review the types of sleep studies Provide clinical information
Measuring sleep and sleepiness with mobile devices
 Measuring sleep and sleepiness with mobile devices Rebecca M. C. Spencer, PhD Personal Health Monitoring University of Massachusetts, Amherst Sleep IALS Why measure sleep? Memory Decisionmaking Stress
Measuring sleep and sleepiness with mobile devices Rebecca M. C. Spencer, PhD Personal Health Monitoring University of Massachusetts, Amherst Sleep IALS Why measure sleep? Memory Decisionmaking Stress
EFFICACY OF MODAFINIL IN 10 TAIWANESE PATIENTS WITH NARCOLEPSY: FINDINGS USING THE MULTIPLE SLEEP LATENCY TEST AND EPWORTH SLEEPINESS SCALE
 EFFICACY OF MODAFINIL IN 10 TAIWANESE PATIENTS WITH NARCOLEPSY: FINDINGS USING THE MULTIPLE SLEEP LATENCY TEST AND EPWORTH SLEEPINESS SCALE Shih-Bin Yeh 1 and Carlos Hugh Schenck 2,3 1 Department of Neurology
EFFICACY OF MODAFINIL IN 10 TAIWANESE PATIENTS WITH NARCOLEPSY: FINDINGS USING THE MULTIPLE SLEEP LATENCY TEST AND EPWORTH SLEEPINESS SCALE Shih-Bin Yeh 1 and Carlos Hugh Schenck 2,3 1 Department of Neurology
Web-Based Home Sleep Testing
 Editorial Web-Based Home Sleep Testing Authors: Matthew Tarler, Ph.D., Sarah Weimer, Craig Frederick, Michael Papsidero M.D., Hani Kayyali Abstract: Study Objective: To assess the feasibility and accuracy
Editorial Web-Based Home Sleep Testing Authors: Matthew Tarler, Ph.D., Sarah Weimer, Craig Frederick, Michael Papsidero M.D., Hani Kayyali Abstract: Study Objective: To assess the feasibility and accuracy
In-Patient Sleep Testing/Management Boaz Markewitz, MD
 In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
Medical Policy Original Effective Date:01/23/2019
 Page 1 of 17 Disclaimer Description Refer to the member s specific benefit plan and Schedule of Benefits to determine coverage. This may not be a benefit on all plans or the plan may have broader or more
Page 1 of 17 Disclaimer Description Refer to the member s specific benefit plan and Schedule of Benefits to determine coverage. This may not be a benefit on all plans or the plan may have broader or more
Frequently Asked Questions
 Q- What is Sleep Apnea? Frequently Asked Questions A- Sleep Apnea, sometimes known as the "silent killer" although there is usually nothing silent about it. It is associated with periodic loud snoring
Q- What is Sleep Apnea? Frequently Asked Questions A- Sleep Apnea, sometimes known as the "silent killer" although there is usually nothing silent about it. It is associated with periodic loud snoring
PEDIATRIC PAP TITRATION PROTOCOL
 PURPOSE In order to provide the highest quality care for our patients, our sleep disorders facility adheres to the AASM Standards of Accreditation. The accompanying policy and procedure on pediatric titrations
PURPOSE In order to provide the highest quality care for our patients, our sleep disorders facility adheres to the AASM Standards of Accreditation. The accompanying policy and procedure on pediatric titrations
Summary of Features and Performance
 MICHELE SLEEP SCORING SYSTEM Summary of Features and Performance Suite PE438, Princess Elizabeth Building 1 Morley Ave / Winnipeg, Manitoba / R3L 2P4 Canada phone 1 877 949 3202 / fax 204 943 6295 Table
MICHELE SLEEP SCORING SYSTEM Summary of Features and Performance Suite PE438, Princess Elizabeth Building 1 Morley Ave / Winnipeg, Manitoba / R3L 2P4 Canada phone 1 877 949 3202 / fax 204 943 6295 Table
New Government O2 Criteria and Expert Panel. Jennifer Despain, RPSGT, RST, AS
 New Government O2 Criteria and Expert Panel Jennifer Despain, RPSGT, RST, AS Lead Sleep Technologist, Central Utah Clinic Sleep Disorders Center; Provo, Utah Objectives: Review new government O2 criteria
New Government O2 Criteria and Expert Panel Jennifer Despain, RPSGT, RST, AS Lead Sleep Technologist, Central Utah Clinic Sleep Disorders Center; Provo, Utah Objectives: Review new government O2 criteria
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA)
") PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
Western Hospital System. PSG in History. SENSORS in the field of SLEEP. PSG in History continued. Remember
 SENSORS in the field of SLEEP Mrs. Gaye Cherry: Scientist in Charge Department of Sleep and Respiratory Medicine Sleep Disorders Unit Western Hospital PSG in History 1875: Discovery of brain-wave activity
SENSORS in the field of SLEEP Mrs. Gaye Cherry: Scientist in Charge Department of Sleep and Respiratory Medicine Sleep Disorders Unit Western Hospital PSG in History 1875: Discovery of brain-wave activity
Arousal detection in sleep
 Arousal detection in sleep FW BES, H KUYKENS AND A KUMAR MEDCARE AUTOMATION, OTTHO HELDRINGSTRAAT 27 1066XT AMSTERDAM, THE NETHERLANDS Introduction Arousals are part of normal sleep. They become pathological
Arousal detection in sleep FW BES, H KUYKENS AND A KUMAR MEDCARE AUTOMATION, OTTHO HELDRINGSTRAAT 27 1066XT AMSTERDAM, THE NETHERLANDS Introduction Arousals are part of normal sleep. They become pathological
Diagnosis and treatment of sleep disorders
 Diagnosis and treatment of sleep disorders Normal human sleep Sleep cycle occurs about every 90 minutes, approximately 4-6 cycles occur per major sleep episode NREM (70-80%) slow wave sleep heart rate,
Diagnosis and treatment of sleep disorders Normal human sleep Sleep cycle occurs about every 90 minutes, approximately 4-6 cycles occur per major sleep episode NREM (70-80%) slow wave sleep heart rate,
Your physician has ordered a sleep study for you on. Your arrival time is scheduled for.
 Dear Patient: Your physician has ordered a sleep study for you on. Your arrival time is scheduled for. The Texas State Sleep Lab is located in the Health Professions Building on the Texas State University
Dear Patient: Your physician has ordered a sleep study for you on. Your arrival time is scheduled for. The Texas State Sleep Lab is located in the Health Professions Building on the Texas State University
Diagnostic Accuracy of the Multivariable Apnea Prediction (MAP) Index as a Screening Tool for Obstructive Sleep Apnea
 Index as a Screening Tool for Obstructive Sleep Apnea") Original Article Diagnostic Accuracy of the Multivariable Apnea Prediction (MAP) Index as a Screening Tool for Obstructive Sleep Apnea Ahmad Khajeh-Mehrizi 1,2 and Omid Aminian 1 1. Occupational Sleep
Original Article Diagnostic Accuracy of the Multivariable Apnea Prediction (MAP) Index as a Screening Tool for Obstructive Sleep Apnea Ahmad Khajeh-Mehrizi 1,2 and Omid Aminian 1 1. Occupational Sleep
SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS
 SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS Laugh and the world laughs with you; snore and you sleep alone. These words by novelist Anthony Vergess ring true with all too many
SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS Laugh and the world laughs with you; snore and you sleep alone. These words by novelist Anthony Vergess ring true with all too many
SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
 DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY") SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
Types of Sleep Studies 8/28/2018. Ronald S. Prehn, ThM, DDS. Type 1 Attended in-lab polysomnography (PSG) 18 leads
 18 leads") Ronald S. Prehn, ThM, DDS rprehn@tmjtexas.com Board Certified in Dental Sleep Medicine Board Certified in Orofacial Pain Types of Sleep Studies Type 1 Attended in-lab polysomnography (PSG) 18 leads Type
Ronald S. Prehn, ThM, DDS rprehn@tmjtexas.com Board Certified in Dental Sleep Medicine Board Certified in Orofacial Pain Types of Sleep Studies Type 1 Attended in-lab polysomnography (PSG) 18 leads Type
PEDIATRIC SLEEP GUIDELINES Version 1.0; Effective
 MedSolutions, Inc. Clinical Decision Support Tool Diagnostic Strategies This tool addresses common symptoms and symptom complexes. Requests for patients with atypical symptoms or clinical presentations
MedSolutions, Inc. Clinical Decision Support Tool Diagnostic Strategies This tool addresses common symptoms and symptom complexes. Requests for patients with atypical symptoms or clinical presentations
 Sleep Studies Sleep studies are tests that measure how well you sleep and how your body responds to sleep problems. These tests can help your doctor find out whether you have a sleep disorder and how severe
Sleep Studies Sleep studies are tests that measure how well you sleep and how your body responds to sleep problems. These tests can help your doctor find out whether you have a sleep disorder and how severe
SLEEP DISORDERED BREATHING The Clinical Conditions
 SLEEP DISORDERED BREATHING The Clinical Conditions Robert G. Hooper, M.D. In the previous portion of this paper, the definitions of the respiratory events that are the hallmarks of problems with breathing
SLEEP DISORDERED BREATHING The Clinical Conditions Robert G. Hooper, M.D. In the previous portion of this paper, the definitions of the respiratory events that are the hallmarks of problems with breathing
Sleep diagnostics systems
 Sleep diagnostics systems DeVilbiss Healthcare introduces the SleepDoc Porti diagnostics systems powered by the technology and expertise of Dr Fenyves und Gut. From a 5 channel respiratory screener up
Sleep diagnostics systems DeVilbiss Healthcare introduces the SleepDoc Porti diagnostics systems powered by the technology and expertise of Dr Fenyves und Gut. From a 5 channel respiratory screener up
Practice Parameters for the Indications for Polysomnography and Related Procedures
 Sleep. 20(6):406-422 1997 American Sleep Disorders Association and Sleep Research Society An American Sleep Disorders Association Report " Practice Parameters for the Indications for Polysomnography and
Sleep. 20(6):406-422 1997 American Sleep Disorders Association and Sleep Research Society An American Sleep Disorders Association Report " Practice Parameters for the Indications for Polysomnography and
Polysomnography and Sleep Studies
 Polysomnography and Sleep Studies Policy Number: Original Effective Date: MM.02.016 09/14/2004 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 05/01/2014 Section: Medicine Place(s)
Polysomnography and Sleep Studies Policy Number: Original Effective Date: MM.02.016 09/14/2004 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 05/01/2014 Section: Medicine Place(s)
HEALTHY LIFESTYLE, HEALTHY SLEEP. There are many different sleep disorders, and almost all of them can be improved with lifestyle changes.
 HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
MOVEMENT RULES. Dr. Tripat Deep Singh (MBBS, MD, RPSGT, RST) International Sleep Specialist (World Sleep Federation program)
 International Sleep Specialist (World Sleep Federation program)") MOVEMENT RULES Dr. Tripat Deep Singh (MBBS, MD, RPSGT, RST) International Sleep Specialist (World Sleep Federation program) 1. Scoring Periodic Limb Movement in Sleep (PLMS) A. The following rules define
MOVEMENT RULES Dr. Tripat Deep Singh (MBBS, MD, RPSGT, RST) International Sleep Specialist (World Sleep Federation program) 1. Scoring Periodic Limb Movement in Sleep (PLMS) A. The following rules define
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: January 15, 2018 Related Policies: 2.01.18 Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome Diagnosis and Medical Management of Obstructive
FEP Medical Policy Manual Effective Date: January 15, 2018 Related Policies: 2.01.18 Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome Diagnosis and Medical Management of Obstructive
INFORMATION SOCIETY TECHNOLOGIES (IST) PROGRAMME
 PROGRAMME") INFORMATION SOCIETY TECHNOLOGIES (IST) PROGRAMME SENSATION 507231 Report on definition of home care needs, security requirements, literacy and educational level, and attitudes of average patients in the
INFORMATION SOCIETY TECHNOLOGIES (IST) PROGRAMME SENSATION 507231 Report on definition of home care needs, security requirements, literacy and educational level, and attitudes of average patients in the
International Journal of Scientific & Engineering Research Volume 9, Issue 1, January ISSN
 International Journal of Scientific & Engineering Research Volume 9, Issue 1, January-2018 342 The difference of sleep quality between 2-channel ambulatory monitor and diagnostic polysomnography Tengchin
International Journal of Scientific & Engineering Research Volume 9, Issue 1, January-2018 342 The difference of sleep quality between 2-channel ambulatory monitor and diagnostic polysomnography Tengchin
OSA - Obstructive sleep apnoea What you need to know if you think you might have OSA
 OSA - Obstructive sleep apnoea What you need to know if you think you might have OSA Obstructive sleep apnoea, or OSA, is a breathing problem that happens when you sleep. It can affect anyone men, women
OSA - Obstructive sleep apnoea What you need to know if you think you might have OSA Obstructive sleep apnoea, or OSA, is a breathing problem that happens when you sleep. It can affect anyone men, women
SleepView. SleepView. Monitor + SleepViewSM. Portal Clinical Validation Summary. CliniCal validation
 CliniCal validation Monitor + SM Portal Clinical Validation Summary 2007 AASM established guidelines for proper Portable Monitoring (PM) methodology to be used in home sleep apnea diagnosis Clinical Guidelines
CliniCal validation Monitor + SM Portal Clinical Validation Summary 2007 AASM established guidelines for proper Portable Monitoring (PM) methodology to be used in home sleep apnea diagnosis Clinical Guidelines
Smith Seminars Online Continuing Education AARC-Approved for 2 CRCE Polysomnography and Obstructive Sleep Apnea
 Smith Seminars Online Continuing Education AARC-Approved for 2 CRCE Polysomnography and Obstructive Sleep Apnea Objectives Understand the importance of polysomnography in diagnosing obstructive sleep apnea.
Smith Seminars Online Continuing Education AARC-Approved for 2 CRCE Polysomnography and Obstructive Sleep Apnea Objectives Understand the importance of polysomnography in diagnosing obstructive sleep apnea.
Polysomnography and Sleep Disorders
 23 Polysomnography and Sleep Disorders Jean K. Matheson, Randip Singh, and Andreja Packard Summary The classification of sleep disorders is based both on clinical and neurophysiological criteria and is
23 Polysomnography and Sleep Disorders Jean K. Matheson, Randip Singh, and Andreja Packard Summary The classification of sleep disorders is based both on clinical and neurophysiological criteria and is
Updates on Accreditation Laura A Linley RPSGT Advanced Sleep Management; VP of Operations AAST Immediate Past President
 Updates on Accreditation Laura A Linley RPSGT Advanced Sleep Management; VP of Operations AAST Immediate Past President Conflict of Interest Disclosures Speaker: X 1. I do not have any potential conflicts
Updates on Accreditation Laura A Linley RPSGT Advanced Sleep Management; VP of Operations AAST Immediate Past President Conflict of Interest Disclosures Speaker: X 1. I do not have any potential conflicts
Helpful hints for filing
 Helpful hints for filing Respiratory Assist Devices HCPCS Code E0470 E0471 Overview The following information describes the Durable Medical Equipment Medicare Administrative Contractors' (DME MACs) medical
Helpful hints for filing Respiratory Assist Devices HCPCS Code E0470 E0471 Overview The following information describes the Durable Medical Equipment Medicare Administrative Contractors' (DME MACs) medical
Basic Standards for Osteopathic Fellowship Training in Sleep Medicine
 Basic Standards for Osteopathic Fellowship Training in Sleep Medicine American Osteopathic Association and the American College of Osteopathic Neurologists and Psychiatrists and the American College of
Basic Standards for Osteopathic Fellowship Training in Sleep Medicine American Osteopathic Association and the American College of Osteopathic Neurologists and Psychiatrists and the American College of
Clinical Practice Guideline on the Use of Actigraphy for the Evaluation of Sleep Disorders and Circadian Rhythm Sleep-Wake Disorders
 Clinical Practice Guideline on the Use of Actigraphy for the Evaluation of Sleep Disorders and Circadian Rhythm Sleep-Wake Disorders An American Academy of Sleep Medicine Clinical Practice Guideline Introduction:
Clinical Practice Guideline on the Use of Actigraphy for the Evaluation of Sleep Disorders and Circadian Rhythm Sleep-Wake Disorders An American Academy of Sleep Medicine Clinical Practice Guideline Introduction:
Disclosures. Acknowledgements. Sleep in Autism Spectrum Disorders: Window to Treatment and Etiology NONE. Ruth O Hara, Ph.D.
 Sleep in Autism Spectrum Disorders: Window to Treatment and Etiology Ruth O Hara, Ph.D. Associate Professor, Department of Psychiatry and Behavioral Sciences, Stanford University School of Medicine Disclosures
Sleep in Autism Spectrum Disorders: Window to Treatment and Etiology Ruth O Hara, Ph.D. Associate Professor, Department of Psychiatry and Behavioral Sciences, Stanford University School of Medicine Disclosures
Rediscover the power of sleep
 Rediscover the power of sleep Patient Copy Apnea solutions for all ages Mobile Sleep Services Who We Are An experienced and well trained team of sleep care professionals consisting of Registered Sleep
Rediscover the power of sleep Patient Copy Apnea solutions for all ages Mobile Sleep Services Who We Are An experienced and well trained team of sleep care professionals consisting of Registered Sleep
Obstructive Sleep Apnea Syndrome. Common sleep disorder causes high blood pressure and heart attacks
 Obstructive Sleep Apnea Syndrome Common sleep disorder causes high blood pressure and heart attacks Message: Sleep apnea is very common. It is estimated that 158 million people worldwide suffer from sleep
Obstructive Sleep Apnea Syndrome Common sleep disorder causes high blood pressure and heart attacks Message: Sleep apnea is very common. It is estimated that 158 million people worldwide suffer from sleep
Physician Dentist Collaboration
 Physician Dentist Collaboration Ronald S. Prehn, ThM, DDS Legal Perspective MD CAN LEGALLY MAKE PROPER DIAGNOSIS DDS CAN LEGALLY FABRICATE DENTAL SLEEP APPLIANCES Legal Perspective TWO PROFESSIONS WORK
Physician Dentist Collaboration Ronald S. Prehn, ThM, DDS Legal Perspective MD CAN LEGALLY MAKE PROPER DIAGNOSIS DDS CAN LEGALLY FABRICATE DENTAL SLEEP APPLIANCES Legal Perspective TWO PROFESSIONS WORK
Special Article. Division of Pulmonary and Critical Care Medicine, Johns Hopkins University, Baltimore, MD; 2 James A. Haley VA Hospital, Tampa, FL; 3
 Special Article Clinical Guidelines for the Use of Unattended Portable Monitors in the Diagnosis of Obstructive Sleep Apnea in Adult Patients Portable Monitoring Task Force of the American Academy of Sleep
Special Article Clinical Guidelines for the Use of Unattended Portable Monitors in the Diagnosis of Obstructive Sleep Apnea in Adult Patients Portable Monitoring Task Force of the American Academy of Sleep
Basic Standards for Fellowship Training in Sleep Medicine
 Basic Standards for Fellowship Training in Sleep Medicine American Osteopathic Association and American College of Osteopathic Neurologists and Psychiatrists and American College of Osteopathic Internists
Basic Standards for Fellowship Training in Sleep Medicine American Osteopathic Association and American College of Osteopathic Neurologists and Psychiatrists and American College of Osteopathic Internists
FAQ CODING & REIMBURSEMENT. WatchPAT TM Home Sleep Test
 FAQ CODING & REIMBURSEMENT WatchPAT TM Home Sleep Test TABLE OF CONTENTS PATIENT SELECTION CRITERIA 3 CODING & MODIFIERS 4-6 PLACE OF SERVICE 6 FREQUENCY 7 ACCREDITATION 7 SLEEP MEDICINE GLOSSARY AND ACRONYMS
FAQ CODING & REIMBURSEMENT WatchPAT TM Home Sleep Test TABLE OF CONTENTS PATIENT SELECTION CRITERIA 3 CODING & MODIFIERS 4-6 PLACE OF SERVICE 6 FREQUENCY 7 ACCREDITATION 7 SLEEP MEDICINE GLOSSARY AND ACRONYMS
RETT SYNDROME AND SLEEP
 2015 A good night s sleep promotes learning, improved mood, general good health, and a better quality of life for both your child and the whole family. This article written for Rettsyndrome.org by Dr Daniel
2015 A good night s sleep promotes learning, improved mood, general good health, and a better quality of life for both your child and the whole family. This article written for Rettsyndrome.org by Dr Daniel
TOP 10 LIST OF SLEEP QUESTIONS. Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children
 TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
SLEEP DISORDERS. Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children
 SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome
 Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome Policy Number: 2.01.18 Last Review: 9/2018 Origination: 1/2006 Next Review: 1/2019 Policy Blue Cross and Blue Shield of Kansas City
Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome Policy Number: 2.01.18 Last Review: 9/2018 Origination: 1/2006 Next Review: 1/2019 Policy Blue Cross and Blue Shield of Kansas City
Robert E. McMichael, M.D. Medical Director Patient Instructions for a Diagnostic Sleep Study
 NORTH TEXAS SLEEP DISORDERS CENTER Neurology Associates of Arlington, P.A 811 West Interstate 20, Suite G12 Arlington, Texas 76017 (817) 419-6375 Fax (817) 419-6371 Robert E. McMichael, M.D. Medical Director
NORTH TEXAS SLEEP DISORDERS CENTER Neurology Associates of Arlington, P.A 811 West Interstate 20, Suite G12 Arlington, Texas 76017 (817) 419-6375 Fax (817) 419-6371 Robert E. McMichael, M.D. Medical Director
1/28/2015 EVALUATION OF SLEEP THROUGH SCALES AND LABORATORY TOOLS. Marco Zucconi
 EVALUATION OF SLEEP THROUGH SCALES AND LABORATORY TOOLS Marco Zucconi Sleep Disorders Centre, Dept of Clinical Neurosciences, San Raffaele Hospital, Milan, Italy INDAGINI STRUMENTALI DEL CICLO SONNO-VEGLIA
EVALUATION OF SLEEP THROUGH SCALES AND LABORATORY TOOLS Marco Zucconi Sleep Disorders Centre, Dept of Clinical Neurosciences, San Raffaele Hospital, Milan, Italy INDAGINI STRUMENTALI DEL CICLO SONNO-VEGLIA
Littleton, CO Welcome Packet 8151 Southpark Lane, Suite 200 Littleton, CO 80120
 Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
Non-contact Screening System with Two Microwave Radars in the Diagnosis of Sleep Apnea-Hypopnea Syndrome
 Medinfo2013 Decision Support Systems and Technologies - II Non-contact Screening System with Two Microwave Radars in the Diagnosis of Sleep Apnea-Hypopnea Syndrome 21 August 2013 M. Kagawa 1, K. Ueki 1,
Medinfo2013 Decision Support Systems and Technologies - II Non-contact Screening System with Two Microwave Radars in the Diagnosis of Sleep Apnea-Hypopnea Syndrome 21 August 2013 M. Kagawa 1, K. Ueki 1,
Periodic Leg Movement, L-Dopa, 5-Hydroxytryptophan, and L-Tryptophan
 Sleep 10(4):393-397, Raven Press, New York 1987, Association of Professional Sleep Societies Short Report Periodic Leg Movement, L-Dopa, 5-Hydroxytryptophan, and L-Tryptophan C. Guilleminault, S. Mondini,
Sleep 10(4):393-397, Raven Press, New York 1987, Association of Professional Sleep Societies Short Report Periodic Leg Movement, L-Dopa, 5-Hydroxytryptophan, and L-Tryptophan C. Guilleminault, S. Mondini,
Sleep Center. Have you had a previous sleep study? Yes No If so, when and where? Name of facility Address
 Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
About VirtuOx. Was marketed exclusively by Phillips Healthcare division, Respironics for 3 years
 About VirtuOx VirtuOx, Inc. assists physicians and Durable Medical Equipment (DME)( companies diagnose respiratory diseases and qualify patients for home respiratory equipment under the guidelines of CMS
About VirtuOx VirtuOx, Inc. assists physicians and Durable Medical Equipment (DME)( companies diagnose respiratory diseases and qualify patients for home respiratory equipment under the guidelines of CMS
OSA and COPD: What happens when the two OVERLAP?
 2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
Sleep Medicine. Maintenance of Certification Examination Blueprint. Purpose of the exam
 Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Standards for Accreditation of Sleep Disorders Centers. Accreditation by the American Academy of Sleep Medicine (AASM) is a voluntary
 is a voluntary") s for Accreditation of Sleep Disorders Centers Introduction Accreditation by the American Academy of Sleep Medicine (AASM) is a voluntary program offered to Sleep Disorders Centers and Laboratories for
s for Accreditation of Sleep Disorders Centers Introduction Accreditation by the American Academy of Sleep Medicine (AASM) is a voluntary program offered to Sleep Disorders Centers and Laboratories for
* Cedars Sinai Medical Center, Los Angeles, California, U.S.A.
 Sleep. 18(2):115-126 1995 American Sleep Disorders Association and Sleep Research Society Home Monitoring-Actimetry Assessment of Accuracy and Analysis Time of a Novel Device to Monitor Sleep and Breathing
Sleep. 18(2):115-126 1995 American Sleep Disorders Association and Sleep Research Society Home Monitoring-Actimetry Assessment of Accuracy and Analysis Time of a Novel Device to Monitor Sleep and Breathing
Sweet Dreams: The Relationship between Sleep Health and Your Weight
 Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
Polysomnography - Sleep Studies
 Polysomnography - Sleep Studies Policy Number: Original Effective Date: MM.02.016 09/14/2004 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 12/21/2012 Section: Medicine Place(s) of Service:
Polysomnography - Sleep Studies Policy Number: Original Effective Date: MM.02.016 09/14/2004 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 12/21/2012 Section: Medicine Place(s) of Service:
INTRINSIC SLEEP DISORDERS. Excessive daytime sleepiness (EDS) is a common complaint. Causes of EDS are numerous and include:
 is a common complaint. Causes of EDS are numerous and include:") INTRINSIC SLEEP DISORDERS Introduction Excessive daytime sleepiness (EDS) is a common complaint. Causes of EDS are numerous and include: Intrinsic sleep disorders (e.g. narcolepsy, obstructive sleep apnoea/hypopnea
INTRINSIC SLEEP DISORDERS Introduction Excessive daytime sleepiness (EDS) is a common complaint. Causes of EDS are numerous and include: Intrinsic sleep disorders (e.g. narcolepsy, obstructive sleep apnoea/hypopnea
Denver, CO Welcome Packet
 Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
EEG Arousals: Scoring Rules and Examples. A Preliminary Report from the Sleep Disorders Atlas Task Force of the American Sleep Disorders Association
 EEG Arousals: Scoring Rules and Examples A Preliminary Report from the Sleep Disorders Atlas Task Force of the American Sleep Disorders Association Sleep in patients with a number of sleep disorders and
EEG Arousals: Scoring Rules and Examples A Preliminary Report from the Sleep Disorders Atlas Task Force of the American Sleep Disorders Association Sleep in patients with a number of sleep disorders and
IMPORTANT INFORMATION
 Joint Commission Accredited to Perform Medicare, NV Medicaid, HPN Medicaid and Tricare Military Sleep Studies You have been scheduled for an overnight sleep study at our facility. The following important
Joint Commission Accredited to Perform Medicare, NV Medicaid, HPN Medicaid and Tricare Military Sleep Studies You have been scheduled for an overnight sleep study at our facility. The following important