European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section WEAN SAFE. Data Collection Forms
|
|
|
- Phoebe Greer
- 6 years ago
- Views:
Transcription
 Acute")

1 European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section WEAN SAFE Data Collection Forms
2
3
4 Study ID: Date of Data collection: FORM 0: - ORGANIZATIONAL DATA OF THE PARTICIPATING ICU TO BE FILLED ONLY ONCE FOR THE STUDY 0.1 Name of the INSTITUTION: 0.2 Mailing Address: 0.3 Phone 0.4 Contact person #1: Contact person #2: ICU Medical Director: 0.9 Open ICU Closed ICU [ONE SELECTION ONLY] 0.10 Type of hospital: University/Academic Non-University [ONE SELECTION ONLY] Type of ICU (check all that apply): 0.11 Medical 0.12 Respiratory ICU 0.13 Surgical 0.14 Cardiothoracic 0.15 Neurosurgical 0.16 Other specialty 0.17 Total number of beds in the hospital: 0.18 Number of beds in use in the ICU at commencement of study: 0.19 Total number of admissions to the ICU in last calendar year: 0.20 Total number of ICU beds in the hospital (including all ICUs, also not involved in this study, excluding intermediate care): 0.21 Was this ICU involved in research activities (other than surveys) in the last 5 years? YES NO [ONE SELECTION ONLY] 0.22 Is there a step-down/intermediate care unit in your hospital? YES NO [ONE SELECTION ONLY] 0.23 Does this hospital have a dedicated weaning facility within the hospital? YES NO [ONE SELECTION ONLY] 4
5 Average number of Health Professionals present in the ICU 1 : Staff Physicians Doctors in training/non-staff Nurses/Nurse practitioners Physician assistants Occupational Therapists Physiotherapists Pharmacists Respiratory Therapists Daytime Night time Which UNITS are used for the following: 0.40 Noradrenaline/norepinephrine: mcg/min mcg/kg/min mg/hour [ONE SELECTION ONLY] 0.41 Adrenaline/epinephrine: mcg/min mcg/kg/min mg/hour [ONE SELECTION ONLY] 0.42 Dopamine: mcg/min mcg/kg/min mg/hour [ONE SELECTION ONLY] 0.43 Dobutamine: mcg/min mcg/kg/min mg/hour [ONE SELECTION ONLY] 0.44 Blood gases? mmhg kpa [ONE SELECTION ONLY] 0.45 Platelets: 10^3/mm3 10^9/L [ONE SELECTION ONLY] 0.46 Hemoglobin: g/100 ml g/l mmol/l [ONE SELECTION ONLY] 0.47 Height: inch cm [ONE SELECTION ONLY] 0.48 Weight: lbs kg [ONE SELECTION ONLY] 0.49 Do you use written/electronic sedation protocols? YES NO [ONE SELECTION ONLY] 0.50 Do you use a sedation scale? YES NO [ONE SELECTION ONLY] 0.51 (IF YES: SAS RASS Ramsay Other ) 0.52 Does your ICU have weaning protocols for patients ventilated > 24 hours? YES NO [ONE SELECTION ONLY] 0.53 If yes: Physician driven Nurses driven RT driven [ONE SELECTION ONLY] 0.54 Please upload your protocol Do you use automated weaning system? YES NO [ONE SELECTION ONLY] 0.56 If yes, please indicate which one: 1 This number may be less than 1.0, particularly for allied health professionals such as physiotherapists. If so, please estimate amount of time as a proportion of a full working day spent by these personnel in the ICU. 5
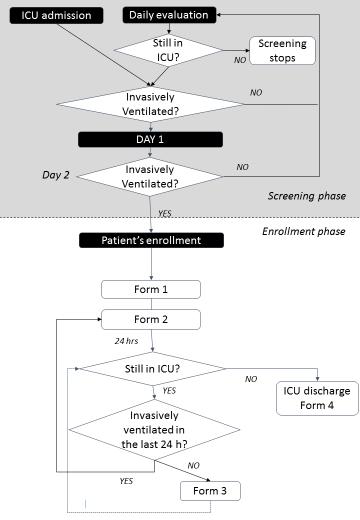
6 Study ID: Date of Data collection: DAILY SCREENING FORM Patient s initials: Gender: M F Year of Birth: First day of ventilation in the present ICU [FIRST DAY OF VENTILATION] Are there any exclusion Criteria present? Yes No Date Is this patient in ICU today? Is this patient receiving Invasive Mechanical Ventilation today [FIRST DAY OF VENTILATION] +1 Yes No Yes No [FIRST DAY OF VENTILATION] +2 Yes No Yes No If Yes PATIENT ENROLLED! ICU Outcome (non-enrolled Patients) Alive at ICU Discharge: Yes No 6
7 FORM 1: - TO BE COMPLETED FOR ALL INVASIVELY VENTILATED PATIENTS ON STUDY DAY 1 Sub Form GENERAL 1.1 Date of enrollment (between 7AM and 10AM on study day 1): / / [FILLED AUTOMATICALLY FROM THE FORM BEFORE] 1.2 Date and hour of commencement of IMV: / / (DD/MM/Year) 1.3 at (24 hour clock) 1.4 Date of ICU admission in the current episode: / /201 _ (DD/MM/Year) 1.5 Gender: M F [ONE SELECTION ONLY] 1.6 Age: What was the main category of ICU admission? (SELECT ONLY ONE OPTION) 1.7 Medical 1.8 Scheduled Surgery 1.9 Emergency surgery (excluding Trauma) 1.10 Trauma [with or without surgery] 1.11 Monitoring (e.g. in situ thrombolysis, desensitization), or post non-surgical procedure (including PCI, bronchoscopy) Hospital Admission 1.12 Date of presentation in current Hospital: / / 201 _ (DD/MM/Year) 1.13 Height (first documented at ICU admission): 1.14 Weight (first documented at ICU admission): 1.15 Residence Status prior to hospital admission [ONE SELECTION ONLY] Home Other healthcare facility Nursing home Unknown Homeless 1.16 Admission Source: [ONE SELECTION ONLY] Other ICU Ward ER OR/Recovery Other, please specify 1.17 Was the patient previously intubated for greater than 24 hours during this hospital admission prior to enrollment? YES NO [ONE SELECTION ONLY] 1.18 Was the patient previously enrolled in this study? YES NO [ONE SELECTION ONLY] 1.19 (If yes, indicate the patient s previous study number ) Co-morbidities present before ICU admission (check all that apply): 1.20 COPD (If known, GOLD: I II III IV) 1.21 Interstitial Lung Disease 1.22 Other chronic lung disease 7
8 1.23 Asthma requiring home inhaled or oral medications 1.24 Active solid organ Neoplasm Hematologic neoplasm 1.26 Bone marrow transplant 1.27 Diabetes Mellitus requiring insulin or oral hypoglycaemic therapy therapy 1.28 Heart failure: NYHA classes III-IV 1.29 Chronic Renal Failure ( if selected: 1.29a Requiring dialysis) 1.30 Immunosuppression Chronic liver failure (1.32 Child-Pugh Class C) 1.33 Congenital/Acquired Myopathies/Neuropathies 1.34 alcohol abuse 1.35 active smoker 1.36 pulmonary hypertension 1.37 kyphoscoliosis with respiratory dysfunction 1.38 Pregnancy [ONE SELECTION ONLY] Yes No Unknown 1.39 Known or suspected diagnosis of dementia? [ONE SELECTION ONLY] None Mild Moderate/severe 1.40 Clinical Frailty Scale Score (in the 2 months prior to first ICU admission) [ONE SELECTION ONLY] 1. Very fit robust, active, energetic, well motivated and fit; exercise regularly; most fit group for their age 2. Well without active disease, but less fit than people in category 1 3. Managing Well, with treated comorbid disease disease symptoms are well controlled 4. Apparently Vulnerable not frankly dependent, patients slowed up or have disease symptoms 5. Mildly Frail with limited dependence on others for instrumental activities of daily living 6. Moderately Frail help is needed with all outside activities and with keeping house, i.e. in both instrumental and non-instrumental activities of daily living 7. Severely frail completely dependent on others for personal care, from whatever cause (physical or cognitive). 8. Very Severely Frail Completely dependent, approaching the end of life. Terminally Ill life expectancy < 6 months, whether or not evidently frail. What is/are the cause(s) of the patient s ICU admission (check all that apply)? 1.41 Hypercapnic Respiratory Failure 1.42 Hypoxaemic Respiratory Failure 1.43 Sepsis/septic shock 1.44 Cardiogenic pulmonary edema 1.45 Cardiac arrest 1.46 Emergency surgery 1.47 Elective surgery (1.48 CARDIAC 1.49 ABDOMINAL 1.50 THORACIC 1.51 NEUROSURGICAL 1.52 Other ) 1.53 Shock (other than septic) 1.54 Trauma 1.55 Neurologic impairment 1.56 Drug overdose 1.57 Airway protection 1.58 Other ( ) 1.59 Metabolic/electrolyte 2 Excluding non-melanoma skin cancer 3 Includes drugs such as cyclosporine, azathioprine, rituximab or cancer chemotherapy, steroids (except for adrenal insufficiency replacement) 8
9 Study ID: Date of Data collection: FORM 2: - DAILY DATA COLLECTION FORM THIS FORM HAS TO BE FILLED EVERY DAY, REPORTING DATA COLLECTED BETWEEN 7-10 am 2.1a Was this patient in the ICU in the last 24 hours? YES NO (Go to form 4) [ONE SELECTION ONLY] 2.1b Was Patient invasively ventilated in the last 24 hours? YES NO (Go to form 3) [ONE SELECTION ONLY] 2.2 Patient s interface: ETT Tracheostomy Not invasively ventilated anymore [ONE SELECTION ONLY] 2.3 Sedation level (before sedation interruption): [ONE SELECTION ONLY] RASS SASS RAMSAY Not measured 2.4 Was there a sedation interruption in the last 24 hours: [ONE SELECTION ONLY] Yes No What is the current (at the time of evaluation) level of ventilator assistance received (if on separation attempt, please give prior level of assistance)? Full support: Volume A/C PC/BIPAP/APRV SIMV PRVG Partial support: PSV NAVA Minimal support: CPAP T-Tube Other (specify) Please record ventilator settings: 2.14 Peak 2.15 Plateau (if different) 2.16 RR (set) 2.17 RR (total) 2.18 PEEP (cmh2o) 2.21 FiO Actual Tidal volume 2.23 p0.1 (if measured) Arterial Blood Gas (as close as possible to above vent settings, if measured): 2.24 ph: PaO 2: 2.26 PaCO 2: 2.27 Lactate If no Arterial Blood Gas Analysis: Pulse Oximeter SpO2: % 2.29 What is the lowest level of assistance received in the last 24 hours? IF DIFFERENT FROM ABOVE [ONE SELECTION ONLY] Assistance level not different from above Full support: Volume A/C PC/BIPAP/APRV SIMV PRVG Partial support: PSV NAVA Minimal support: CPAP T-Tube Other (specify) Extubation: Accidental Extubation Planned Extubation 2.30 Peak 2.31 Plateau (if different) [if cmv] 2.31 Pressure support level [if PSV] 2.32 RR (set) 2.33 RR (total) 2.34 PEEP (cmh2o) 2.35 FiO Actual Tidal volume 2.37 p0.1 (if measured) 2.38 How long was this level maintained for? hours Start time 9
10 2.39 What was the reason for termination of lower level of support? Pre-planned termination Patient deterioration Other (Specify) Arterial Blood Gas (if measured during reduced support): 2.40 ph: PaO 2: 2.42 PaCO 2: 2.43 Lactate If no Arterial Blood Gas Analysis: Pulse Oximeter SpO2: % 2.45 Was this a spontaneous breathing trial (SBT), to predict success in separating the patient from the ventilator? YES NO [ONE SELECTION ONLY] 10
11 SOFA Score (every third day from day 1, 4, etc.) Values NOT AVAILABLE (Please give worst value in the last 24 hours) Glasgow Coma Scale (3-15) 2.46 motor 2.47 eye 2.48 verbal Platelet Count(UNITS) 2.50 Total Bilirubin (if measured) 2.51 Creatinine (if measured) 2.52 OR Urine Output (ml/day) 2.53 Mean Arterial Pressure (mmhg) 2.54 Dopamine infusion 2.55 Dobutamine infusion 2.56 Noradrenaline infusion 2.57 Adrenaline infusion 2.58 Others vasopressors? (Yes/No) or dosage? 2.59 PDE inhibitors (Yes/No) or dosage? In the last 24 hours, did the patient receive any of the following drugs: 2.60 Sedatives[ONE SELECTION ONLY]: Continuous Intermittent None 2.61 Opioids[ONE SELECTION ONLY]: Continuous Intermittent None 2.62 NM blockers[one SELECTION ONLY]: Continuous Intermittent None 2.63 Steroids[ONE SELECTION ONLY]: High dose Low dose None 2.64 Diuretics[ONE SELECTION ONLY]: High dose Low dose None 2.65 Renal replacement therapy [ONE SELECTION ONLY] YES NO 2.66 Is the patient receiving ECMO/ECCO2R YES NO Blood flow l/min 11
12 PART B: - TO BE FILLED FOR PATIENTS WITH PEEP < 10 cm H2O, and FiO2 < 50%, if they are not receiving neuromuscular blockers or high doses of vasopressors (> 0.2 mcg/kg/min of noradrenaline or equivalent) What are the reasons for not separating the patient from the ventilator according to the attending physician (check all that apply)? 2.67 Unresolved surgical condition 2.68 Unresolved respiratory failure 2.69 Upper airway protection 2.70 Decreased level of consciousness 2.71 Agitation/ delirium 2.72 Cardiac failure / Fluid Overload 2.73 Hemodynamic instability 2.74 Muscle weakness 2.75 Planned intervention requiring airway protection 2.76 Failed spontaneous breathing trial 2.77 Recent [< 24 hours] re-intubation 2.78 Excessive secretion 2.79 Weak cough 2.80 Maximum Inspiratory Pressure (if measured in the last 24 hours) cmh2o 2.81 Is this patient considered in weaning phase according to the attending physician? Yes No Uncertain Unknown [ONE SELECTION ONLY] 2.82 Amount of secretions: none/mild moderate abundant [ONE SELECTION ONLY] 2.83 Cough strength: weak intermediate normal/strong NOT RECORDED [ONE SELECTION ONLY] 2.84 Was the patient out of the bed last 24 hours? Yes No [ONE SELECTION ONLY] 2.85 Did the patient do mobility exercise last 24 hours? Yes, active Yes, passive No [ONE SELECTION ONLY] 2.86 Current heart rate 2.87 Current systolic blood pressure 2.88 Current diastolic blood pressure 2.89 Fluid balance in last 24 hours 12
13 Study ID: Date of Data collection: FORM 3: - DAILY DATA COLLECTION FORM FOR PATIENTS NOT CONNECTED TO THE VENTILATOR IN THE LAST 24 HOURS IN THE LAST 24 HOURS DID THE PATIENT RECEIVE ANY OF THE FOLLOWING? (Check all that apply) 3.1 Face mask/nasal cannula low flow oxygen (<15) 3.2 NIV/CPAP via Helmet interface 3.3 NIV/CPAP via Face/Nose Mask interface 3.4 High Flow nasal cannula 3.5 None of the above IF YES, WHAT WAS THE REASON? (Check all that apply) 3.6 Hypoxia 3.7 Hypercapnia 3.8 Respiratory distress 3.9 Prophylaxis 3.10 Restoration of home ventilatory support (including Sleep Apnea Syndrome) 13
14 Study ID: Date of Data collection: FORM 4: - OUTCOMES ICU DISCHARGE/DEATH ICU Outcome 4.1 Alive Dead [ONE SELECTION ONLY] 4.2 Date of ICU discharge/death: / / (DD/MM/Year) For pts discharged alive 4.3 Discharged to: [ONE SELECTION ONLY] This Hospital: Other ICU Intermediate Care Unit Weaning unit Hospital Ward Other Hospital: ICU Intermediate Care Unit Weaning unit Hospital Ward Other Location: Home Rehabilitation facility Other (Specify) Respiratory status at ICU Discharge (check all that apply): 4.4 Intubated 4.5 Tracheostomy 4.6 Non-invasive ventilation 4.7 Oxygen therapy 4.8 No oxygen therapy 4.9 Level of physical Dependence (at discharge) [ONE SELECTION ONLY] Independent Partially Dependent Completely Dependent Changes in Goals of Care 4.10 Was there a pre-existing order limiting life-sustaining measures prior to ICU admission? (E.g. no CPR/withhold/withdraw) 4.11 Was there a decision to limit a life sustaining measure at any time during the ICU stay? Yes No Not legally available [ONE SELECTION ONLY] If answer to 4.11= yes What was the life sustaining measure limited? [CHECK ALL THAT APPLY] 4.12 No CPR 4.13 No re-intubation 4.14 No re-admission to ICU 4.15 ICU trial 4.16 Full comfort care [i.e. no organ support] 4.17 Extubation with full comfort and/or palliative care Did a difficulty in weaning influence the decision to limit life-sustaining measures? [ONE SELECTION ONLY] No Yes Sole/major reason Yes One of a number of reasons 4.19 Date of decision for No CPR measures in event of cardiac arrest: / / 4.20 Date of decision to withhold/withdraw other life sustaining measures: / / Co-Enrollment in another Study 4.21 Was this patient co-enrolled in another study Yes No [ONE SELECTION ONLY] 4.22 If patient was co-enrolled, was there a protocol for weaning from mechanical ventilation Yes No [ONE SELECTION ONLY] 14
15 If ICU outcome= alive Hospital (or 90 day) Outcome (whichever event occurs first) 4.23 Alive Dead [ONE SELECTION ONLY] 4.24 Date of hospital discharge: / / 15
WorldwidE AssessmeNt of Separation of patients From ventilatory assistance WEAN SAFE
 European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section ESICM Trial Group WorldwidE AssessmeNt of Separation of patients From ventilatory assistance WEAN SAFE Data Collection
European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section ESICM Trial Group WorldwidE AssessmeNt of Separation of patients From ventilatory assistance WEAN SAFE Data Collection
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
SECTION 1: INCLUSION/EXCLUSION CRITERIA INCLUSION CRITERIA Please put a cross in the Yes or No box for each question
 Site Number Patient s Initials SECTION 1: INCLUSION/EXCLUSION CRITERIA INCLUSION CRITERIA Please put a cross in the Yes or No box for each question Yes No 1.1 Is the patient receiving invasive mechanical
Site Number Patient s Initials SECTION 1: INCLUSION/EXCLUSION CRITERIA INCLUSION CRITERIA Please put a cross in the Yes or No box for each question Yes No 1.1 Is the patient receiving invasive mechanical
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients CASE REPORT FORM
 INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders
![Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders](/thumbs/83/87321224.jpg "Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders") Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
MECHANICAL VENTILATION PROTOCOLS
 GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
CASE REPORT FORM (v )
") INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM (v 1.2 30.09.18) SITE INFORMATION
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM (v 1.2 30.09.18) SITE INFORMATION
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION
 SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
POLICY. Number: Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE. Authorization
 POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
LAS VEGAS Case Report Form 1 Intra-Operative
 LAS VEGAS Case Report Form 1 Intra-Operative Patient Informed Consent 1. Informed consent applicable: yes no (choose no if waived by local EC) 1.1 If applicable; was consent obtained? yes no 1.2 If yes,
LAS VEGAS Case Report Form 1 Intra-Operative Patient Informed Consent 1. Informed consent applicable: yes no (choose no if waived by local EC) 1.1 If applicable; was consent obtained? yes no 1.2 If yes,
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME
 FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
Guide to completing the MODET study CRF
 Guide to completing the MODET study CRF Please record ND for not documented, NA for not applicable and UK for unknown rather than leave blank fields. CRF PAGE 1. Time of injury Complete the time of injury
Guide to completing the MODET study CRF Please record ND for not documented, NA for not applicable and UK for unknown rather than leave blank fields. CRF PAGE 1. Time of injury Complete the time of injury
EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM
 REFERRAL FORM") Patient Label This form is accessible on www.royalpapworth.nhs.uk Intensive Care Unit EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM Please always phone Papworth ECMO Coordinator on 01480 830541,
Patient Label This form is accessible on www.royalpapworth.nhs.uk Intensive Care Unit EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM Please always phone Papworth ECMO Coordinator on 01480 830541,
Web Appendix 1: Literature search strategy. BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up. Sources to be searched for the guidelines;
 write-up. Sources to be searched for the guidelines;") Web Appendix 1: Literature search strategy BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up Sources to be searched for the guidelines; Cochrane Database of Systematic Reviews (CDSR) Database of
Web Appendix 1: Literature search strategy BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up Sources to be searched for the guidelines; Cochrane Database of Systematic Reviews (CDSR) Database of
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Admission Criteria Clinical Practice Policy
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Admission Criteria Clinical Practice Policy Original Date: 04/2011 Purpose: To specify physiologic criteria for appropriate
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Admission Criteria Clinical Practice Policy Original Date: 04/2011 Purpose: To specify physiologic criteria for appropriate
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Non-invasive Positive Pressure Mechanical Ventilation: NIPPV: CPAP BPAP IPAP EPAP. My Real Goals. What s new in 2018? OMG PAP?
 Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
Addendum/database Part 1 demographics
 Addendum/database Part 1 demographics Part 1 General demographics Section finished? Date Time of alarm 08.00-17.00h 17.00-23.00h 23.00-08.00h Transport unit MICU / ITW IC ambulance Standard ambulance Helicopter
Addendum/database Part 1 demographics Part 1 General demographics Section finished? Date Time of alarm 08.00-17.00h 17.00-23.00h 23.00-08.00h Transport unit MICU / ITW IC ambulance Standard ambulance Helicopter
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
(Non)-invasive ventilation: transition from PICU to home. Christian Dohna-Schwake
-invasive ventilation: transition from PICU to home. Christian Dohna-Schwake") (Non)-invasive ventilation: transition from PICU to home Christian Dohna-Schwake Increased use of NIV in PICUs over last 15 years First choice of respiratory support in many diseases Common temporary indications:
(Non)-invasive ventilation: transition from PICU to home Christian Dohna-Schwake Increased use of NIV in PICUs over last 15 years First choice of respiratory support in many diseases Common temporary indications:
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1).
.") PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
Concerns and Controversial Issues in NPPV. Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation
 : Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
: Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION
 SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date (DD/MMM/YYYY) (DD/MMM/YYYY) Gender Female Male Date of surgery (DD/MMM/YYYY)
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date (DD/MMM/YYYY) (DD/MMM/YYYY) Gender Female Male Date of surgery (DD/MMM/YYYY)
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning
 CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
PAPER DE LA VNI EN LA RETIRADA DE LA VENTILACIÓ INVASIVA I FRACÀS D EXTUBACIÓ
 PAPER DE LA VNI EN LA RETIRADA DE LA VENTILACIÓ INVASIVA I FRACÀS D EXTUBACIÓ Dr. Miquel Ferrer UVIIR, Servei de Pneumologia, Hospital Clínic, IDIBAPS, CibeRes, Barcelona. E- mail: miferrer@clinic.ub.es
PAPER DE LA VNI EN LA RETIRADA DE LA VENTILACIÓ INVASIVA I FRACÀS D EXTUBACIÓ Dr. Miquel Ferrer UVIIR, Servei de Pneumologia, Hospital Clínic, IDIBAPS, CibeRes, Barcelona. E- mail: miferrer@clinic.ub.es
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Spontaneous Breathing Trial and Mechanical Ventilation Weaning Process
 Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล
 Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Trial protocol - NIVAS Study
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
(To be filled by the treating physician)
") CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
4. Which survey program does your facility use to get your program designated by the state?
 TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
2. To provide an ethical, moral and practical framework for decision-making during a public health emergency.
 November 2010 TABLE TOP EXERCISE PARTICIPANT GUIDE When Routine Critical Care Resources Are Not Available Time expectations for each session: SECTION ACTIVITY TIME I Introduction 5 minutes II Exercise
November 2010 TABLE TOP EXERCISE PARTICIPANT GUIDE When Routine Critical Care Resources Are Not Available Time expectations for each session: SECTION ACTIVITY TIME I Introduction 5 minutes II Exercise
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS
 RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Hospital Resource and Clinical Management Guidelines for Hospital Healthcare Providers When Routine Critical Care Resources Are Not Available
 Hospital Resource and Clinical Management Guidelines for Hospital Healthcare Providers When Routine Critical Care Resources Are Not Available Medical College of Wisconsin Center for Medical Incident Management
Hospital Resource and Clinical Management Guidelines for Hospital Healthcare Providers When Routine Critical Care Resources Are Not Available Medical College of Wisconsin Center for Medical Incident Management
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Proportional Assist Ventilation (PAV) (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure
 (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure") Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
 Dr.Ahmad farooq") Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
High Flow Oxygen Therapy in Acute Respiratory Failure. Laurent Brochard Toronto
 High Flow Oxygen Therapy in Acute Respiratory Failure Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical research projects from the
High Flow Oxygen Therapy in Acute Respiratory Failure Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical research projects from the
Home Mechanical Ventilation. Anthony Bateman
 Home Mechanical Ventilation Anthony Bateman What is Long Term Ventilation? LTV is the provision of respiratory support to individuals with non-acute respiratory failure Progression of expected disease
Home Mechanical Ventilation Anthony Bateman What is Long Term Ventilation? LTV is the provision of respiratory support to individuals with non-acute respiratory failure Progression of expected disease
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Potential Conflicts of Interest
 Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Making vasopressors safer
 Making vasopressors safer Requirements for safe vaspressor use In an ideal world 1. Knowledge of what constitutes optimal vasopressor dosing 2. A culture of cautiousness regarding vasopressors What do
Making vasopressors safer Requirements for safe vaspressor use In an ideal world 1. Knowledge of what constitutes optimal vasopressor dosing 2. A culture of cautiousness regarding vasopressors What do
RESPIRATORY COMPLICATIONS AFTER SCI
 SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
Icu-cpr PICTURE QUIZ march 2014
 Department of surgery Icu-cpr PICTURE QUIZ march 2014 Prepared by Dr. Karam Kamal Younis Assistant professor and consultant surgeon Convener of the Department of Surgery College of Medicine University
Department of surgery Icu-cpr PICTURE QUIZ march 2014 Prepared by Dr. Karam Kamal Younis Assistant professor and consultant surgeon Convener of the Department of Surgery College of Medicine University
Acute NIV in COPD and what happens next. Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital
 Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Clinical Practice Guidelines for Cases with Pneumonia associated with Pandemic H1N infection As of 7 August 2009
 Clinical Practice Guidelines for Cases with Pneumonia associated with Pandemic H1N1 2009 infection As of 7 August 2009 This Clinical Practice Guideline contains basic information to be considered when
Clinical Practice Guidelines for Cases with Pneumonia associated with Pandemic H1N1 2009 infection As of 7 August 2009 This Clinical Practice Guideline contains basic information to be considered when
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Care Unit (FELLOW)
") Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Journal Club American Journal of Respiratory and Critical Care Medicine. Zhang Junyi
 Journal Club 2018 American Journal of Respiratory and Critical Care Medicine Zhang Junyi 2018.11.23 Background Mechanical Ventilation A life-saving technique used worldwide 15 million patients annually
Journal Club 2018 American Journal of Respiratory and Critical Care Medicine Zhang Junyi 2018.11.23 Background Mechanical Ventilation A life-saving technique used worldwide 15 million patients annually
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
BTS Guideline for Home Oxygen use in adults Appendix 9 (online only) Key Questions - PICO 10 December 2012
 Key Questions - PICO 10 December 2012") BTS Guideline for Home Oxygen use in adults Appendix 9 (online only) Key Questions - PICO 10 December 2012 Evidence base for Home Oxygen therapy in COPD, non-copd respiratory disease and nonrespiratory
BTS Guideline for Home Oxygen use in adults Appendix 9 (online only) Key Questions - PICO 10 December 2012 Evidence base for Home Oxygen therapy in COPD, non-copd respiratory disease and nonrespiratory
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Supplementary Online Content 2
 Supplementary Online Content 2 van Meenen DMP, van der Hoeven SM, Binnekade JM, et al. Effect of on demand vs routine nebulization of acetylcysteine with salbutamol on ventilator-free days in intensive
Supplementary Online Content 2 van Meenen DMP, van der Hoeven SM, Binnekade JM, et al. Effect of on demand vs routine nebulization of acetylcysteine with salbutamol on ventilator-free days in intensive
Charisma High-flow CPAP solution
 Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Respiratory Failure how the respiratory physicians deal with airway emergencies
 Respiratory Failure how the respiratory physicians deal with airway emergencies Dr Michael Davies MD FRCP Consultant Respiratory Physician Respiratory Support and Sleep Centre Papworth Hospital NHS Foundation
Respiratory Failure how the respiratory physicians deal with airway emergencies Dr Michael Davies MD FRCP Consultant Respiratory Physician Respiratory Support and Sleep Centre Papworth Hospital NHS Foundation
Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital
 Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital Objectives Upon completion of this module, the learner will be able to: Identify types of airways and indications
Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital Objectives Upon completion of this module, the learner will be able to: Identify types of airways and indications
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
An Overview of the Chronic Critical Illness Syndrome (CCIS) and Weaning the PMV Patient
 and Weaning the PMV Patient") An Overview of the Chronic Critical Illness Syndrome (CCIS) and Weaning the PMV Patient Fall 2011 CCIS has been known for some time HISTORICAL PRECURSORS INCLUDE: SIRS Systemic Inflammatory Response Syndrome
An Overview of the Chronic Critical Illness Syndrome (CCIS) and Weaning the PMV Patient Fall 2011 CCIS has been known for some time HISTORICAL PRECURSORS INCLUDE: SIRS Systemic Inflammatory Response Syndrome
APACHE II: A Severity of Disease Classification System Standard Operating Procedure for Accurate Calculations
 BACKGROUND APACHE II: A Severity of Disease Classification System Standard Operating Procedure for Accurate Calculations The APACHE prognostic scoring system was developed in 1981 at the George Washington
BACKGROUND APACHE II: A Severity of Disease Classification System Standard Operating Procedure for Accurate Calculations The APACHE prognostic scoring system was developed in 1981 at the George Washington