UPDATE: DIAGNOSIS & MANAGEMENT OF RLS
|
|
|
- Julianna Rice
- 6 years ago
- Views:
Transcription


1 UPDATE: DIAGNOSIS & MANAGEMENT OF RLS Beenish K. Khwaja, D.O. Legacy Medical Group--Neurology & Sleep Medicine Director, Legacy Mt. Hood Sleep Center
2 Outline Definition & Diagnostic Criteria Epidemiology of RLS Pathophysiology of RLS Etiology of RLS Differential Diagnosis of RLS Diagnosis of RLS in Adults and Children Clinical Course & Complication of RLS Impact of RLS Management Approach & Treatment of RLS
3 Essential Features Urge to move or the unpleasant leg sensation begins or worsens during periods of rest or inactivity such as lying down or sitting. Patients describe exacerbation of symptoms in situations such as watching television, driving or flying long distances, or attending meetings. Symptoms also worsen in association with a decrease in central nervous system (CNS) activity that leads to a decrease in alertness.
4 Essential Features Patients with RLS report an urge to move associated with dysesthesia when they are at rest. Some say that the sensations are uncomfortable and unpleasant, and others use specific terms such as creepycrawly, jittery, internal itch, or shock-like feelings. Up to 50% of RLS patients describe their sensations as painful. Some people, however, describe only an urge to move, and they are unaware of a sensory component.
5 Essential Features Symptoms are usually felt over large areas of the thighs or calves (or both) and are usually experienced as coming from deep within the legs rather than as superficial. The disorder can also involve the arms and other body parts. Symptoms in the legs usually precede involvement of the arms by several years. Arm paresthesias have been associated with a higher severity of the disorder. The involvement of the arms without any involvement in the legs rarely occurs.
6 Essential Features Urge to move and the unpleasant leg sensations are relieved by activity. When symptoms occur, patients may move their legs vigorously, flexing, stretching, or crossing them one over the other. In severe cases, they might walk around for hours in the evening or during the night to relieve the discomfort. The relief is generally described as beginning immediately or soon after the activity begins and this relief usually persists as long as the activity continues.
7 Essential Features Symptoms are worse in the evening. Three factors that can contribute to this phenomena are: Increased sleepiness in the evening compared to the daytime. Decrease in motor activity in the evening compared to the daytime. There is a manifestation of an intrinsic circadian rhythm in RLS symptoms.

8 Supportive Clinical Features Positive Family History Positive response to dopaminergic therapy. Nearly all patients with RLS show at least an initial positive therapeutic response to either L-dopa or dopamine receptor agonist. Presence of periodic limb movements (PLM) Occur in 80% of people with RLS. PLM in sleep are also common in some other disorders and among the elderly and are not specific for RLS. Recent genetic studies suggest that there may be a strong genetic connection between PLM and RLS and in the future, a specific form of RLS with PLM may be described.
. Can begin at any age even young children.")
9 Epidemiology Prevalence of RLS is approximately 5% to 10%. Most common movement disorder and among the most common sleep-related disorders. Most studies have also shown notable gender differences Women 9% v. Men 5.4% Has been found to occur across most every population (less so in Asians). Can begin at any age even young children. Up to 25% of primary care patients have RLS symptoms. Prevalence of severe RLS (at least moderate symptoms 3 or more times a week): 2.7% Women 3.7% v. Men 1.7% Increases in each decade of life
10 RLS and Age
11 Pathophysiology Dopamine Has been hypothesized as the main neurotransmitter in the pathophysiology because dopaminergic mechanisms are involved in spinal flexor reflex control and dopamine agonists provide symptomatic relief of RLS and PLMD. However, imaging studies (PET and SPECT ) scrutinizing either the dopamine type 2 (D 2 )-receptor or dopamine transporter have yielded mixed results, with three demonstrating reduced synaptic activity and two showing no difference from controls.
12 Pathophysiology Proteins involved in dopamine transmission exhibit circadian rhythms, possibly providing an explanation for the circadian character of RLS. The similarities in treatment response suggest a potential shared pathophysiology between RLS and Parkinson's disease. However, current evidence does not convincingly show more than a casual association.
13 Pathophysiology Iron Given the similar circadian rhythms of serum iron levels, the proteins involved in dopamine transmission, and RLS symptoms, it is difficult not to hypothesize a connection. Iron is a cofactor for tyrosine hydroxylase, the rate-limiting enzyme for dopamine synthesis. Decrease in iron may decrease dopamine synthesis. However, studies in iron-deficient animals have also demonstrated a decrease in D 1 - and D 2 -receptor, a decrease in dopamine transporter function, but an elevation in extra-cellular dopamine. Clearly, if there is an iron-dopamine connection in RLS, it is complex and it will need to be elucidated.

14 Etiology of RLS Primary (Idiopathic) RLS Accounts for most cases 50% of all cases are familial Inheritance is autosomal dominant with 5 genetic loci identified Seen in younger patients, or patients have a history of onset at a young age. Secondary RLS Pregnancy 11-33% Iron Deficiency Anemia 25% Peripheral Neuropathy 36% ESRD 20-57% Parkinson s Disease 21% Other Metabolic Deficiencies: B12, Folate, Thyroid
15 Secondary RLS Iron Deficiency Recent studies have shown that decreased iron stores (indicated by serum ferritin levels below 50 ng per ml [50 μg per L] can exacerbate RLS symptoms. Patients with newly diagnosed RLS or RLS patients with a recent exacerbation of symptoms should have their serum ferritin levels measured. Neurologic Lesions RLS has been reported in association with spinal cord and peripheral nerve lesions, although an exact pathologic mechanism has not been identified. RLS also may occur in patients with vertebral disk disease/radiculopathy. Other Neurologic Conditions Associate with RLS: Parkinson s CMT 2 SCA 1-2-3
16 Secondary RLS Pregnancy 20-25% of pregnant women experience RLS. If new onset (more than half) generally occur in last half of pregnancy. Symptoms stop soon after or even before delivery. Speculated etiologies include iron deficiency, folate deficiency, hormonal changes. May be a risk factor for later development of RLS. The more # of children a woman has, the higher the risk of RLS.
17 Secondary RLS Uremia Renal failure patient have a higher prevalence of RLS than general population: %. Associated with anemia and peripheral neuropathy or independently. Dialysis does NOT markedly improve RLS symptoms; in fact, may dialysis patients discontinue dialysis due to RLS. Kidney transplantation has a strong and positive influence on RLS symptoms in hemodialysis patients.
18 Secondary RLS Drug-Induced RLS symptoms may be induced or exacerbated by medications such as: Tricyclic antidepressants Selective serotonin reuptake inhibitors (SSRIs) Lithium Dopamine antagonists (e.g. Raglan, Compazine and Antipsychotics) Alcohol Antihistamines Caffeine Nicotine
19 Differential Diagnosis of RLS Disorders of Restlessness Neuroleptic-induced akathisia Positional discomfort Nervous leg shaking Involuntary leg movements (PLM, priopriospinal myoclonus at sleep onset, rhythmic movement disorder) Disorders of Leg Discomfort Peripheral Neuropathy Nocturnal Leg Cramps Intermittent Claudication or arterial insufficiency Arthritic leg discomfort Painful myopathies Varicose veins or venous insufficiency Deep vein thrombosis Fasciculations Disorders of Both Restlessness and Leg Discomfort Painful legs and moving toes Hypnic jerks
20 Diagnosing RLS History: main method of diagnosis Neurologic examination: normal in idiopathic; mainly used to look for secondary causes Lab testing: CBC, serum ferritin, percent iron saturation Added testing for peripheral neuropathy: B12, Chemistries (BUN, Cr), Glucose/A1c, EMG/NCS Consider PSG (not required or recommended) Insufficient sleep and sleep disorders such as sleep apnea might exacerbate symptoms of RLS.

21

22
23 RLS in Children 4 essential adult criteria + description in child s own words consistent with leg discomfort (urge to move is not enough) OR 4 essential adult criteria + 2 supportive criteria Supportive criteria in children: Sleep disturbance for age Biological parent or sibling with RLS Sleep study documenting PLM index > 5/hr Studies have found that RLS/PLMS in children is more prevalent in ADHD and vice versa. Treatment of RLS in Children: Gabapentin Clonazepam Clonidine (may be a good choice in patient with RLS and ADHD)
24 Clinical Course The intensity of sensory and motor symptoms varies greatly from one case to another; it also fluctuates throughout a patient's lifetime. Onset of RLS in patients younger than 30 tends to be more insidious and may not become troublesome until middle or later age. When the age of onset is 50 years or older, symptoms often appear more abruptly. Sudden remissions, lasting for months or even years, are as difficult to explain as are relapses, which appear without any apparent reason.
25 Complications of RLS Discomfort and pain Major cause of sleep disturbance (e.g. difficulty initiating and maintaining sleep) May lead to daytime fatigue/sleepiness Poor functioning at home or job due to restlessness Impaired social interactions Feelings of frustration, anxiety, depression, embarrassment
26 Impact of RLS REST Study: looked at epidemiology and impact of RLS People with RLS have impaired quality of life comparable to other chronic conditions. Wisconsin Sleep Cohort Study: People with RLS symptoms every night are much more likely to have cardiovascular disease. National Sleep Foundation in America Poll 2005: Those with RLS symptoms are more likely to report drowsy driving and missing social events due to discomfort.
27 Treatment of RLS Intermittent : RLS that is troublesome enough when present to justify treatment but does not occur frequently enough to necessitate daily therapy. Symptoms when not treated would occur on average <2/week for the past year with at least 5 lifetime events. Daily : RLS that is frequent and troublesome enough to require daily therapy. Symptoms when not treated would occur on average at least 2x/week for the past year. Refractory : Daily RLS treated with at least one dopamine agonist at usual dose with one or more the following outcomes: Inability to achieve a satisfactory response. Response that has become unsatisfactory with time despite increasing doses. Intolerable adverse effects. Augmentation that is not controllable with adjustment of agonist doses.
28 Target Symptoms for RLS Therapy Dysesthesia: reduce to the lowest level possible throughout the 24 hours. Sleep: normalize sleep onset, sleep maintenance, and daytime alertness. Periodic Leg Movements: reduce to asymptomatic level for patients and bed partner. Timing of treatment before significant onset of symptoms. Side Effects should be minimized.
29 Behavior Modification for RLS Avoid caffeine, chocolate, and MSG Aerobic exercise, but before 7:00 PM Limit use of centrally active stimulants: decongestants, antihistamines, nicotine, appetite suppressants, etc. Avoid SSRI anti-depressants, unless only effective treatment (possibly better: bupropion or nefazodone). Counter stimuli: socks, stretching, hot baths or showers, ice pack etc.
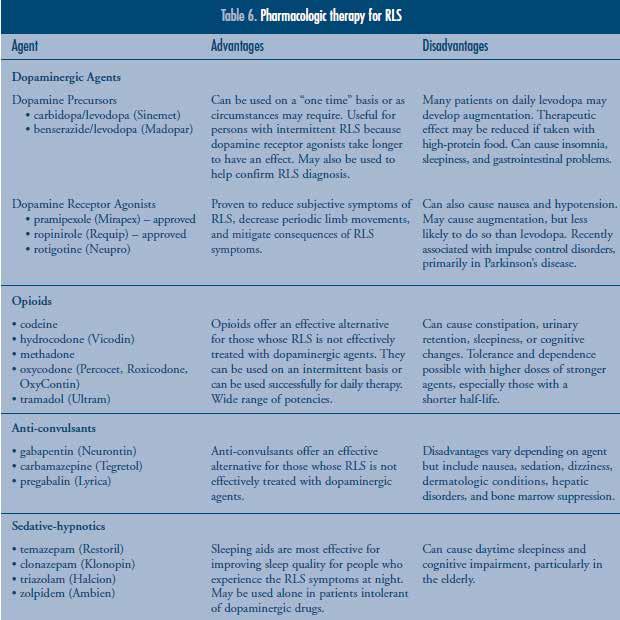
30 Pharmacologic Treatment for RLS Pharmacologic treatment options FDA Approved Medications Levadopa Dopamine Agonists Pramiprexole (Mirapex) Ropinirole (Requip) Non-FDA Approved Medications Anticonvulsants (GBP, Carbamazepine, Lyrica) Opioids (Codeine, Propoxyphene, Oxycodone, Tramadol, Hydrocodone, Methadone) Benzodiazepines (Clonazepam, Oxazepam, Triazolam) Iron Therapy
31 Treatment of RLS: Levodopa Several open-label and placebo-controlled studies have documented the short-term efficacy and long-term benefit of levodopa, given with carbidopa, in idiopathic RLS and RLS associated with uremia. Several adverse effects were reported including: Nausea/vomiting Tachycardia Orthostatic hypotension Hallucinations Insomnia Daytime fatigue Daytime sleepiness
32 Treatment of RLS: Levodopa 2 adverse effects were more specifically studied including morning rebound and RLS augmentation. Morning rebound is characterized by the presence of RLS symptoms occurring de novo as a consequence of evening or nighttime treatment. Augmentation is characterized by an earlier onset of symptoms by at least 4 hours or by an earlier onset between 2 and 4 hours plus at least one of the following: shorter latency to symptoms when at rest, extension of symptoms to other body parts, greater intensity of symptoms, and shorter duration of relief from treatment. One group found augmentation in 81% patients treated with levodopa. Increased severity of RLS and higher dosage of levodopa were associated with higher risk of developing augmentation. Mild augmentation may be treated by earlier administration of the drug, but in severe cases the medication should be discontinued.
33 Treatment of RLS: Dopamine Agonists Dopamine agonists are now considered the firstline treatment for RLS. More effective and produce fewer adverse effects (especially augmentation). Sleepiness might be seen during treatment with dopamine agonists, but it is much less problematic than in Parkinson's disease, and no cases of sudden onset of sleep have been reported. Small percentage of RLS patients treated with dopaminergic medications have noted increased urges and time spent gambling and increased sexual desire, a side-effect previously reported in Parkinson's disease.
34 Treatment of RLS: Opioids Opioids are often prescribed for severe cases, especially in patients unresponsive to other treatments. Opioids are also very useful during withdrawal from dopaminergic agents in patients who have developed severe augmentation. Opioids should also be used cautiously in patients who snore and are at risk for having sleep apnea syndrome.
35 Treatment of RLS: Anticonvulsants Studies of anticonvulsants have focused on gabapentin. Several open-label trials and one placebo-controlled study showed subjective improvements with gabapentin at doses of 300 to 2400 mg a day. Gabapentin is considered more potent and produces fewer adverse effects than dopaminergic agonists, except for mild daytime somnolence. Recommended for the treatment of neuropathic RLS and in general for patients who use pain as a descriptor for their leg sensations.
36 Treatment of RLS: Benzodiazepines Several studies showed that benzodiazepines improve the quality of sleep and reduce PLMS and associated arousals. However, the therapeutic effects of benzodiazepines on subjective ratings of RLS symptoms were either modest or not significant. Therefore benzodiazepines are mostly used to improve sleep continuity in patients with RLS. Because dopaminergic agents often have a stimulating effect and worsen insomnia, benzodiazepines are often used as an adjunctive treatment.
37 Treatment of RLS: Iron Supplementation Ferritin < 18, percent saturation < 16% However, ferritin levels less than 50ng/ml have been associated with increased symptoms The goal of therapy maintain ferritin > 50 ng/ml Treatment: Ferrous Sulfate 325 mg PLUS 100mg Vitamin C 1 hour or at least 2 hours after a meal up to 3x/daily Severe iron deficiency Ferritin <10 ng/ml Treatment: IV iron infusions of mg at least 2 days apart Iron dextran has higher anaphylactic risk than iron sucrose, iron gluconate or ferumoxytol However, the dextran maintains high peripheral iron availability much longer than does the sucrose. Optimal parental iron therapy is unclear.
38 Treatment of RLS & Pregnancy 1 st option is to increase iron, vitamin B12, folate, and magnesium levels. 2 nd option is oxycodone 5mg in 2 nd and 3 rd trimester. Pramipexole and GBP are pregnancy category C. Gabapentin can be used during breastfeeding as there is very little penetration into breast milk. Other options in breast feeding including benzodiazepines like Clonazepam, Diazepam or even Methadone (monitor the infant for sedation and poor suckling). Oxycodone and codeine can enter breast milk. Dopamine agonists suppress prolactin production.
39 Case Study # 1 54 y/o woman with 20+ year history of RLS. PMHx: CKD with creatinine of 2.1, stable. Hospitalized for major depression 4 yrs ago; currently taking fluoxetine at 40 mg/d. My legs are driving me nuts. Inside they crawl and hurt. I just have to move them. I can t live this way any longer. I would be better off dead. Taking carbidopa/levodopa ER 50/200 qid for 8 months. Relief of 1-2 hours, otherwise 24-hour RLS.
40 Case Study # 1 Did anything help you? I slept with oxycodone (taken for 3 days after dental work). Sinemet CR helped for 2 months and then it wouldn t last so I took more. Re-check of creatinine, hemoglobin and hematocrit, B12, folate, and Ferritin. No changes were found.
41 Augmentation Shift of RLS symptoms by two or more hours to an earlier onset compared to the patient s baseline. Levodopa produces augmentation in 30-85% of RLS patients (onset typically at 1-3 months). Dopamine agonists (DA) estimated to produce augmentation in 15-35% of patients (onset typically >6-12 months).
42 Management Options for Augmentation Change the schedule of drug administration. For example, split the dose in two first dose at about 6pm and the second half at bedtime. For levodopa, taper off then switch to a dopamine agonist. If DA, consider earlier dosing (as above). Observe for further augmentation. In the severe patient, shift to high potency opiate. Consider gabapentin, clonazepam or other therapy.
43 Case Study # 1: Treatment Approach Taper carbidopa/levodopa ER 50/200 by one tablet every 2 days, beginning in the evening, to prevent augmentation. To reduce augmentation, substitute ropinirole 0.25 mg for each of the doses every 2 days. Oxycodone 5 mg p.o. h.s. for acute symptom relief and to improve sleep. Emphasize complexity, need for daily contact.
44 Treatment Course Day 1-10 Day 1: I slept 5 hours. Day 6: The legs are 30% better, but I m only sleeping 4 hours or so. Response: Increase ropinirole doses # 3 & 4 to 0.50 mg. Day 10: My legs are OK until about 11:00 and then they act up. The medicine makes me really sick (nauseated). Response: Nausea should get better. Increase ropinorole at noon to 0.5 mg.
45 Treatment Course Day Day 11: I m sick all day. I didn t sleep. Response: Discontinue a.m. ropinirole. Day 12: You got to do something. Response: Reduce ropinirole to 0.25 mg noon & 6:00 pm, continue 0.5 mg at 10:00 pm. Day 14: I m not as sick but my legs are worse. Is this ever going to get better? Response: Add oxycodone 5 mg at 6:00 p.m. (and h.s.). Reduce ropinirole to 0.25 mg TID.
46 Treatment Course Day Day 21: I m 50 % better. I even slept 6 hours one night. RL starts at about noon. Response: Increase ropinirole to 0.5 mg with lunch. Day 24 That stuff makes me sick. I decreased it (back to 0.25 mg at noon). My legs were getting puffy. Response: Checked chemistries and renal function. No acute changes.
47 Treatment Course Day Day 26: Doc, I think the dope works the best. The fluid was making my legs hurt. Response: Stopped ropinirole Changed oxycodone to METHADONE 5 mg at 6:00 p.m. and 10:00 p.m. Day 35: Doc, it s amazing. I don t feel my legs jumping and I slept for five nights straight. Edema resolved.
48 Treatment Course Day 35 + Depression remained moderate with low energy & motivation; moderate sadness. PCP agreed to my request to discontinue Prozac. Wellbutrin SR 150 mg was started and increased to a.m. and noon one week later. Four weeks later, clonazepam 0.5 mg h.s. was added due to feeling a bit nervous. At eight weeks, he slept >6 hours nightly and said I feel pretty good. He has remained so for 3+ years on methadone, buproprion XL and clonazepam.
49 Conclusions Treat symptoms identified as problems by patient. Treat iron deficiency. Dopamine agonists are the first line. Target therapy before the onset of syptoms. Carbidopa Levodopa causes augmentation. Best used prn. [Arbitrary limit: 3 tabs of 25/100)] Opiates reserved for severe patients. High potency agents can be used (methadone, hydromorphone) but caution for EDS and SDB. Gabapentin is variably effective. Best with pain. Depression and anxiety are common and require treatment when present. Buproprion preferred.

50
51

52


53
Basics of Restless Legs Syndrome (Willis-Ekbom Disease)
") Basics of Restless Legs Syndrome (Willis-Ekbom Disease) Michael H. Silber, M.B.Ch.B. Professor of Neurology Mayo Clinic College of Medicine Objectives Understand how RLS is diagnosed Understand what we
Basics of Restless Legs Syndrome (Willis-Ekbom Disease) Michael H. Silber, M.B.Ch.B. Professor of Neurology Mayo Clinic College of Medicine Objectives Understand how RLS is diagnosed Understand what we
Walters AS. Toward a better definition of the restless legs syndrome. The International Restless Legs Syndrome Study Group..
 Restless Legs Syndrome: Impact, Recognition, and Management Pierre Bou-Khalil Khalil, MD, FCCP, D ABSM What is RLS and what is its impact? Definition of RLS RLS is characterized by disagreeable leg sensations
Restless Legs Syndrome: Impact, Recognition, and Management Pierre Bou-Khalil Khalil, MD, FCCP, D ABSM What is RLS and what is its impact? Definition of RLS RLS is characterized by disagreeable leg sensations
AUGMENTATION SUFFERING AND WHAT CAN BE DONE ABOUT IT. John W. Winkelman MD PhD Massachusetts General Hospital Harvard Medical School Boston, MA
 AUGMENTATION SUFFERING AND WHAT CAN BE DONE ABOUT IT John W. Winkelman MD PhD Massachusetts General Hospital Harvard Medical School Boston, MA Disclosure Information Type of Affiliation Commercial Entity
AUGMENTATION SUFFERING AND WHAT CAN BE DONE ABOUT IT John W. Winkelman MD PhD Massachusetts General Hospital Harvard Medical School Boston, MA Disclosure Information Type of Affiliation Commercial Entity
Case 1. A. Insomnia B. Restless leg syndrome C. Peripheral neuropathy D. Osteoarthritis of the hip. Disclosures. Diagnosis for trouble falling asleep
 Disclosures I have no disclosures Case 1 Liza Ashbrook, MD Assistant Clinical Professor UCSF Department of Neurology History of Present Illness Diagnosis for trouble falling asleep 70-year-man with obstructive
Disclosures I have no disclosures Case 1 Liza Ashbrook, MD Assistant Clinical Professor UCSF Department of Neurology History of Present Illness Diagnosis for trouble falling asleep 70-year-man with obstructive
Restless Leg Syndrome What does it mean to you in the middle of the night?
 S Restless Leg Syndrome What does it mean to you in the middle of the night? David A. Weed, DO, FCCP, D, ABSM Sleep Disorders Center ~ The Aroostook Medical Center Presque Isle, Maine S 1990 S 22 year
S Restless Leg Syndrome What does it mean to you in the middle of the night? David A. Weed, DO, FCCP, D, ABSM Sleep Disorders Center ~ The Aroostook Medical Center Presque Isle, Maine S 1990 S 22 year
Restless Legs Syndrome: Is This a Pain Issue?
 Restless Legs Syndrome: Is This a Pain Issue? Kathy Lattavo, RN, MSN, ACNS- BC, RN-BC Objectives Describe the pathophysiology of RLS. Evaluate treatment for RLS. Compare & contrast RLS & pain. Definitions
Restless Legs Syndrome: Is This a Pain Issue? Kathy Lattavo, RN, MSN, ACNS- BC, RN-BC Objectives Describe the pathophysiology of RLS. Evaluate treatment for RLS. Compare & contrast RLS & pain. Definitions
Christopher J. Earley, MB, BCh, PhD Professor Department of Neurology Johns Hopkins School of Medicine
 Christopher J. Earley, MB, BCh, PhD Professor Department of Neurology Johns Hopkins School of Medicine 1. Medication working well but do you still need it? 2. Medication working well but do you really
Christopher J. Earley, MB, BCh, PhD Professor Department of Neurology Johns Hopkins School of Medicine 1. Medication working well but do you still need it? 2. Medication working well but do you really
Restless Legs Syndrome. Brian Koo, M.D. University Hospitals
 Restless Legs Syndrome Brian Koo, M.D. University Hospitals Outline of Talk Diagnosis/classification Symptomatology Evaluation PLMS Epidemiology Prevalence Risk factor Effect of Quality of Life Pathophysiology
Restless Legs Syndrome Brian Koo, M.D. University Hospitals Outline of Talk Diagnosis/classification Symptomatology Evaluation PLMS Epidemiology Prevalence Risk factor Effect of Quality of Life Pathophysiology
RESTLESS LEGS SYNDROME IN CHILDREN AND ADOLESCENTS
 RESTLESS LEGS SYNDROME IN CHILDREN AND ADOLESCENTS Tracy Carbone, MD Medical Director of Sleep Medicine Lee Health Golisano Children s Hospital of Southwest Florida Fort Myers, FL OVERVIEW Although the
RESTLESS LEGS SYNDROME IN CHILDREN AND ADOLESCENTS Tracy Carbone, MD Medical Director of Sleep Medicine Lee Health Golisano Children s Hospital of Southwest Florida Fort Myers, FL OVERVIEW Although the
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
The Management of Restless Legs Syndrome in Adults in Primary Care Version 1.1 February 2019
 The Management of Restless Legs Syndrome in Adults in Primary Care Version 1.1 February 2019 VERSION CONTROL Version Number Date Amendments made 1.0 December 2015 1.1 February 2019 Version 1. Approved
The Management of Restless Legs Syndrome in Adults in Primary Care Version 1.1 February 2019 VERSION CONTROL Version Number Date Amendments made 1.0 December 2015 1.1 February 2019 Version 1. Approved
Author: Colleen Symanski-Sanders, RN, Forensic Nurse Specialist. Objectives: Upon completion of this CNE article, the reader will be able to
 Restless Leg Syndrome Expires Wednesday, October 31, 2018 Nursing Colleen Symanski-Sanders, RN Objectives 1. Describe the three different categories of restless legs syndrome. 2. Explain the main symptoms
Restless Leg Syndrome Expires Wednesday, October 31, 2018 Nursing Colleen Symanski-Sanders, RN Objectives 1. Describe the three different categories of restless legs syndrome. 2. Explain the main symptoms
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute
 Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Dr Alex Bartle. Medical Director Sleep Well Clinic Christchurch
 Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 8:30-9:25 WS #191: Sleep Disorders in The Elderly 9:35-10:30 WS #203: Sleep Disorders in The Elderly (Repeated) REM - Rapid Eye Movement
Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 8:30-9:25 WS #191: Sleep Disorders in The Elderly 9:35-10:30 WS #203: Sleep Disorders in The Elderly (Repeated) REM - Rapid Eye Movement
New data show sustained 5-year benefit of Neupro (Rotigotine Transdermal System) for symptoms of Restless Legs Syndrome
 for symptoms of Restless Legs Syndrome") New data show sustained 5-year benefit of Neupro (Rotigotine Transdermal System) for symptoms of Restless Legs Syndrome Latest safety and efficacy results for rotigotine in the treatment of moderate to
New data show sustained 5-year benefit of Neupro (Rotigotine Transdermal System) for symptoms of Restless Legs Syndrome Latest safety and efficacy results for rotigotine in the treatment of moderate to
Movement Disorders. Eric Kraus, MD! Neurology!
 Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
Options for Treating Restless Legs Syndrome. A Review of the Research for Adults
 Options for Treating Restless Legs Syndrome A Review of the Research for Adults Is This Information Right for Me? Yes, this information is for you if: Your doctor* has told you that you have restless legs
Options for Treating Restless Legs Syndrome A Review of the Research for Adults Is This Information Right for Me? Yes, this information is for you if: Your doctor* has told you that you have restless legs
Can valium help restless leg syndrome
 Can valium help restless leg syndrome The Borg System is 100 % Can valium help restless leg syndrome Mar 1, 2012. Fortunately, certain lifestyle strategies can help you manage milder forms of RLS, and
Can valium help restless leg syndrome The Borg System is 100 % Can valium help restless leg syndrome Mar 1, 2012. Fortunately, certain lifestyle strategies can help you manage milder forms of RLS, and
RESTLESS LEG SYNDROME: DETECTION AND MANAGEMENT IN PRIMARY CARE
 RESTLESS LEG SYNDROME: DETECTION AND MANAGEMENT IN PRIMARY CARE By Marietta Farrell, RN, BSN The contents of this course are taken from the National Center on Sleep Disorders Research, National Institutes
RESTLESS LEG SYNDROME: DETECTION AND MANAGEMENT IN PRIMARY CARE By Marietta Farrell, RN, BSN The contents of this course are taken from the National Center on Sleep Disorders Research, National Institutes
Restless Legs Syndrome: Associated Conditions. William Ondo, MD Methodist Neurological Institute
 Restless Legs Syndrome: Associated Conditions William Ondo, MD Methodist Neurological Institute Clinical Definition Urge to move the legs with or without paresthesias Symptoms worse during inactivity Symptoms
Restless Legs Syndrome: Associated Conditions William Ondo, MD Methodist Neurological Institute Clinical Definition Urge to move the legs with or without paresthesias Symptoms worse during inactivity Symptoms
Does oxycodone cause restless legs
 Does oxycodone cause restless legs 15-12-2015 Restless legs syndrome: Oxycodone/naloxone oxycodone /naloxone for restless legs syndrome should have their no apparent underlying cause. 8-11-2013 An oxycodone
Does oxycodone cause restless legs 15-12-2015 Restless legs syndrome: Oxycodone/naloxone oxycodone /naloxone for restless legs syndrome should have their no apparent underlying cause. 8-11-2013 An oxycodone
SLEEP DISORDERS. Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children
 SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
GREEN. Ropinirole Other PD treatments Benzodiazepines Opioids low potency Anticonvulsants Clonidine
 New Medicine Report (Adopted by the CCG until review and futher notice) Document Status Traffic Light Decision PRAMIPEXOLE For restless legs syndrome Post Suffolk D&TC GREEN Prescribers Rating Possibly
New Medicine Report (Adopted by the CCG until review and futher notice) Document Status Traffic Light Decision PRAMIPEXOLE For restless legs syndrome Post Suffolk D&TC GREEN Prescribers Rating Possibly
Elavil (amitriptyline)
") Generic name: Amitriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets; 10 mg/ml injection Available in generic: Yes Drug class: Tricyclic antidepressant General Information
Generic name: Amitriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets; 10 mg/ml injection Available in generic: Yes Drug class: Tricyclic antidepressant General Information
Healthy Sleep Tips Along the Way!
 Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
AGING CHANGES IN SLEEP
 OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
TOP 10 LIST OF SLEEP QUESTIONS. Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children
 TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
Sleep and Parkinson's Disease
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Overview. Sleep Related Movement Disorders - Restless Leg Syndrome - Periodic Limb movements in Sleep
 The Structure of Sleep The Parasomnias - in REM - in Non-REM - Narcolepsy Overview Sleep Related Movement Disorders - Restless Leg Syndrome - Periodic Limb movements in Sleep Circadian Rhythm disorders
The Structure of Sleep The Parasomnias - in REM - in Non-REM - Narcolepsy Overview Sleep Related Movement Disorders - Restless Leg Syndrome - Periodic Limb movements in Sleep Circadian Rhythm disorders
Depression & Anxiety. What can I do? What are other possible treatments? What is this? Why does this happen? KEY POINTS
 Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
WHY CAN T I SLEEP? Deepti Chandran, MD
 WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
Many people with physical
 FACTSHEET How to Sleep Better Many people with physical disabilities suffer from sleep disturbances, and sleep tends to become more disrupted as we get older. Not sleeping well can negatively impact your
FACTSHEET How to Sleep Better Many people with physical disabilities suffer from sleep disturbances, and sleep tends to become more disrupted as we get older. Not sleeping well can negatively impact your
INSOMNIA IN GERIATRICS. Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow
 INSOMNIA IN GERIATRICS Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow Insomnia Insomnia is the inability to fall asleep, the inability to stay asleep, or waking up earlier than desired. To
INSOMNIA IN GERIATRICS Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow Insomnia Insomnia is the inability to fall asleep, the inability to stay asleep, or waking up earlier than desired. To
Weaning off requip. Cari untuk: Cari Cari
 Cari untuk: Cari Cari Weaning off requip Weaning Off Mirapex. Readers have updated us on their weaning efforts. Mirapex has. I do not want to replace this med with Requip,. The pramipexole is the same
Cari untuk: Cari Cari Weaning off requip Weaning Off Mirapex. Readers have updated us on their weaning efforts. Mirapex has. I do not want to replace this med with Requip,. The pramipexole is the same
Sleeping with PD. Jean Tsai, MD PhD September 27, 2014
 Sleeping with PD Jean Tsai, MD PhD September 27, 2014 Evaluation of sleep Assessment at least annually recommended by Agency for Healthcare Research and Quality (AHRQ) of the US Dept of Health and Human
Sleeping with PD Jean Tsai, MD PhD September 27, 2014 Evaluation of sleep Assessment at least annually recommended by Agency for Healthcare Research and Quality (AHRQ) of the US Dept of Health and Human
Norpramin (desipramine)
") Generic name: Desipramine Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets Available in generic: Yes Drug class: Tricyclic antidepressant General Information Norpramin (desipramine)
Generic name: Desipramine Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets Available in generic: Yes Drug class: Tricyclic antidepressant General Information Norpramin (desipramine)
PACKAGE LEAFLET: INFORMATION FOR USER ROPINIROLE 2 mg FILM-COATED TABLETS. Ropinirole
 PACKAGE LEAFLET: INFORMATION FOR USER ROPINIROLE 0.25 mg FILM-COATED TABLETS ROPINIROLE 0.5 mg FILM-COATED TABLETS ROPINIROLE 1 mg FILM-COATED TABLETS ROPINIROLE 2 mg FILM-COATED TABLETS Ropinirole Read
PACKAGE LEAFLET: INFORMATION FOR USER ROPINIROLE 0.25 mg FILM-COATED TABLETS ROPINIROLE 0.5 mg FILM-COATED TABLETS ROPINIROLE 1 mg FILM-COATED TABLETS ROPINIROLE 2 mg FILM-COATED TABLETS Ropinirole Read
Learning Objectives. Sleep and Sleep Disorders NOT called Sleep Apnea. Socioeconomic Consequences. Socioeconomic Consequences
 Sleep and Sleep Disorders NOT called Sleep Apnea Jerrold Kram, MD, FCCP, FAASM Medical Director, California Center for Sleep Disorders Board of Directors, National Sleep Foundation Learning Objectives
Sleep and Sleep Disorders NOT called Sleep Apnea Jerrold Kram, MD, FCCP, FAASM Medical Director, California Center for Sleep Disorders Board of Directors, National Sleep Foundation Learning Objectives
Tofranil and Tofranil-PM (imipramine)
") Tofranil and Tofranil-PM (imipramine) Generic name: Imipramine Available strengths: 10 mg, 25 mg, 50 mg tablets; 75 mg, 100 mg, 125 mg, 150 mg capsules (Tofranil-PM) Available in generic: Yes Drug class:
Tofranil and Tofranil-PM (imipramine) Generic name: Imipramine Available strengths: 10 mg, 25 mg, 50 mg tablets; 75 mg, 100 mg, 125 mg, 150 mg capsules (Tofranil-PM) Available in generic: Yes Drug class:
Revised October A Publication for Healthcare Providers
 Revised October 2005 R L S M E D I C A L B U L L E T I N 2 0 0 5 A Publication for Healthcare Providers A B S T R A C T Restless legs syndrome (RLS) is a sensorimotor disorder characterized by a distressing
Revised October 2005 R L S M E D I C A L B U L L E T I N 2 0 0 5 A Publication for Healthcare Providers A B S T R A C T Restless legs syndrome (RLS) is a sensorimotor disorder characterized by a distressing
Insomnia. Learning Objectives. Disclosure 6/7/11. Research funding: NIH, Respironics, Embla Consulting: Elsevier
 Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Common Antidepressant Medications for Adults
 (and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
(and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
Sleep in the Patient with Diabetes
 Sleep in the Patient with Diabetes ANDREA RINN, DO SEPTEMBER, 2017 Learning Objectives 1. Recognize the correlation between sleep apnea and diabetes 2. Review potential relationships between sleep and
Sleep in the Patient with Diabetes ANDREA RINN, DO SEPTEMBER, 2017 Learning Objectives 1. Recognize the correlation between sleep apnea and diabetes 2. Review potential relationships between sleep and
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
Wellbutrin/Wellbutrin-SR/ Wellbutrin-XL (bupropion)
") Wellbutrin/Wellbutrin-SR/ Wellbutrin-XL (bupropion) Generic name: Bupropion Available strengths: 75 mg, 100 mg immediate-release tablets; 100 mg, 150 mg, 200 mg sustained-release tablets (Wellbutrin-SR);
Wellbutrin/Wellbutrin-SR/ Wellbutrin-XL (bupropion) Generic name: Bupropion Available strengths: 75 mg, 100 mg immediate-release tablets; 100 mg, 150 mg, 200 mg sustained-release tablets (Wellbutrin-SR);
Quick Guide to Common Antidepressants-Adults
 Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
R E S T L E S S L E G S S Y N D R O M E. Causes, diagnosis and treatment. For the patient living with restless legs syndrome (RLS)
") R E S T L E S S L E G S S Y N D R O M E Causes, diagnosis and treatment For the patient living with restless legs syndrome (RLS) www.rls.org RESTLESS LEGS SYNDROME Restless legs syndrome (RLS), also called
R E S T L E S S L E G S S Y N D R O M E Causes, diagnosis and treatment For the patient living with restless legs syndrome (RLS) www.rls.org RESTLESS LEGS SYNDROME Restless legs syndrome (RLS), also called
Drug Review Rozerem (ramelteon)
") Drug Review Rozerem (ramelteon) Introduction 1 Ramelteon is a melatonin receptor agonist with affinity for MT 1 and MT 2 and selectivity over the MT 3 receptor. The activity at the MT 1 and MT 2 receptors
Drug Review Rozerem (ramelteon) Introduction 1 Ramelteon is a melatonin receptor agonist with affinity for MT 1 and MT 2 and selectivity over the MT 3 receptor. The activity at the MT 1 and MT 2 receptors
Pamelor (nortriptyline)
") Generic name: Nortriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg capsules; 10 mg/5 ml oral solution Available in generic: Yes Drug class: Tricyclic antidepressant General Information Pamelor
Generic name: Nortriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg capsules; 10 mg/5 ml oral solution Available in generic: Yes Drug class: Tricyclic antidepressant General Information Pamelor
SIFROL Composition Properties Indication
 SIFROL Boehringer Composition 1 tablet contains: 0.125, 0.25 or 1.0 mg, (S)-2- amino-4,5,6,7-tetrahydro-6-propylamino-benzothiazole dihydrochloride monohydrate equivalent to 0.088, 0.18 or 0.7 mg pramipexole
SIFROL Boehringer Composition 1 tablet contains: 0.125, 0.25 or 1.0 mg, (S)-2- amino-4,5,6,7-tetrahydro-6-propylamino-benzothiazole dihydrochloride monohydrate equivalent to 0.088, 0.18 or 0.7 mg pramipexole
OBJECTIVES. The psychiatric, medical, and neurologic causes of sleep problems. Office-based and objective methods of evaluating sleep
 SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
Modern Management of Sleep Disorders. If Only I Could Sleep Like I Did Before
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
Neupro (rotigotine) showed significant benefit on early morning motor control, sleep and nocturnal symptoms in patients with Parkinson s disease
 showed significant benefit on early morning motor control, sleep and nocturnal symptoms in patients with Parkinson s disease") For the attention of accredited medical writers only Neupro (rotigotine) showed significant benefit on early morning motor control, sleep and nocturnal symptoms in patients with Parkinson s disease Detailed
For the attention of accredited medical writers only Neupro (rotigotine) showed significant benefit on early morning motor control, sleep and nocturnal symptoms in patients with Parkinson s disease Detailed
Medications for the Treatment of Neuropathic Pain
 Medications for the Treatment of Neuropathic Pain February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation Neuropathic Pain Pain, paresthesias, and sensory
Medications for the Treatment of Neuropathic Pain February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation Neuropathic Pain Pain, paresthesias, and sensory
Best Medical Treatments for Parkinson s disease
 Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Mirtazapine GENERAL INFORMATION. 15-mg, 30-mg, and 40-mg orally disintegrating tablets (SolTab) Available in generic
 Available in generic") Mirtazapine Generic name Available brands Available strengths and formulations Available in generic Mirtazapine Remeron, Remeron SolTab 7.5-mg, 15-mg, 30-mg, and 45-mg tablets 15-mg, 30-mg, and 40-mg orally
Mirtazapine Generic name Available brands Available strengths and formulations Available in generic Mirtazapine Remeron, Remeron SolTab 7.5-mg, 15-mg, 30-mg, and 45-mg tablets 15-mg, 30-mg, and 40-mg orally
Non Malignant Pain: Symptom Management
 Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO?
 ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO? You may have noticed a change... Levodopa is a common treatment for Parkinson s, and doctors have relied on it for decades. Over time as Parkinson s progresses,
ARE YOUR LEVODOPA PILLS WORKING LIKE THEY USED TO? You may have noticed a change... Levodopa is a common treatment for Parkinson s, and doctors have relied on it for decades. Over time as Parkinson s progresses,
Sleep and a Healthy Heart
 Sleep and a Healthy Heart Dr. R. John Kimoff, MD, FRCP(C) Professor of Medicine, Respiratory Division Director, Sleep Laboratory, MCI-McGill University Health Centre Montréal, Québec, Canada Women s Healthy
Sleep and a Healthy Heart Dr. R. John Kimoff, MD, FRCP(C) Professor of Medicine, Respiratory Division Director, Sleep Laboratory, MCI-McGill University Health Centre Montréal, Québec, Canada Women s Healthy
Patients with Parkinson s disease treated with Neupro (rotigotine) showed low rates of dyskinesias with long term treatment
 showed low rates of dyskinesias with long term treatment") For the attention of accredited medical writers only Patients with Parkinson s disease treated with Neupro (rotigotine) showed low rates of dyskinesias with long term treatment Data presented at the 7
For the attention of accredited medical writers only Patients with Parkinson s disease treated with Neupro (rotigotine) showed low rates of dyskinesias with long term treatment Data presented at the 7
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Depression and RLS. John W. Winkelman MD, PhD Departments of Psychiatry and Neurology Massachusetts General Hospital
 Depression and RLS John W. Winkelman MD, PhD Departments of Psychiatry and Neurology Massachusetts General Hospital Associate Professor of Psychiatry Harvard Medical School A 42 year old man has a three
Depression and RLS John W. Winkelman MD, PhD Departments of Psychiatry and Neurology Massachusetts General Hospital Associate Professor of Psychiatry Harvard Medical School A 42 year old man has a three
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
continuing education for pharmacists
 continuing education for pharmacists Restless Legs Syndrome and Management Volume XXX, No. 2 Thomas A. Gossel, R.Ph., Ph.D., Professor Emeritus, Ohio Northern University, Ada, Ohio and J. Richard Wuest,
continuing education for pharmacists Restless Legs Syndrome and Management Volume XXX, No. 2 Thomas A. Gossel, R.Ph., Ph.D., Professor Emeritus, Ohio Northern University, Ada, Ohio and J. Richard Wuest,
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
What s new for diagnosing and treating Parkinson s Disease?
 What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
Modern Management of Sleep Disorders
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over)
") Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
Restless Legs Syndrome: What is Ferritin & Why Do We Want To Be Iron Man or Iron Woman
 Restless Legs Syndrome: What is Ferritin & Why Do We Want To Be Iron Man or Iron Woman Focus Fall 2017 Conference Poughkeepsie, NY Dr. Steven A Thau MD Director, Pulmonary and Sleep Medicine Phelps Memorial
Restless Legs Syndrome: What is Ferritin & Why Do We Want To Be Iron Man or Iron Woman Focus Fall 2017 Conference Poughkeepsie, NY Dr. Steven A Thau MD Director, Pulmonary and Sleep Medicine Phelps Memorial
Data presented at major international congress
 Neupro (rotigotine transdermal system) significantly improved wellbeing and daily activities impaired due to limb pain associated with Restless Legs Syndrome Data presented at major international congress
Neupro (rotigotine transdermal system) significantly improved wellbeing and daily activities impaired due to limb pain associated with Restless Legs Syndrome Data presented at major international congress
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia
 Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
TIAGABINE. THERAPEUTICS Brands Gabitril see index for additional brand names. Generic? Yes
 TIAGABINE THERAPEUTICS Brands Gabitril see index for additional brand names Generic? Yes Class Anticonvulsant; selective GABA reuptake inhibitor (SGRI) Commonly Prescribed for (bold for FDA approved) Partial
TIAGABINE THERAPEUTICS Brands Gabitril see index for additional brand names Generic? Yes Class Anticonvulsant; selective GABA reuptake inhibitor (SGRI) Commonly Prescribed for (bold for FDA approved) Partial
Insomnia. Dr Terri Henderson MBChB FCPsych
 Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
MEDICATION GUIDE DUOPA (Do-oh-pa) (carbidopa and levodopa) enteral suspension
 (carbidopa and levodopa) enteral suspension") MEDICATION GUIDE DUOPA (Do-oh-pa) (carbidopa and levodopa) enteral suspension Read this Medication Guide before you start using DUOPA and each time you get a refill. There may be new information. This
MEDICATION GUIDE DUOPA (Do-oh-pa) (carbidopa and levodopa) enteral suspension Read this Medication Guide before you start using DUOPA and each time you get a refill. There may be new information. This
SLEEP UPDATE 2008 SLEEP HYPNOGRAM. David Claman, MD UCSF Sleep Disorders Center
 SLEEP UPDATE 2008 SLEEP HYPNOGRAM David Claman, MD UCSF Sleep Disorders Center Insomnia Case A 40 year old man c/o insomnia at sleep onset. He worries about sleep at night, and takes 2-3 hrs to fall asleep.
SLEEP UPDATE 2008 SLEEP HYPNOGRAM David Claman, MD UCSF Sleep Disorders Center Insomnia Case A 40 year old man c/o insomnia at sleep onset. He worries about sleep at night, and takes 2-3 hrs to fall asleep.
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
Bupropion HCl, bupropion hydrobromide Wellbutrin SR, Wellbutrin XL, Zyban, Aplenzin, Forfivo XL
 Bupropion Generic names Available brands Available strengths and formulations Available in generic Bupropion HCl, bupropion hydrobromide Wellbutrin SR, Wellbutrin XL, Zyban, Aplenzin, Forfivo XL 75-mg
Bupropion Generic names Available brands Available strengths and formulations Available in generic Bupropion HCl, bupropion hydrobromide Wellbutrin SR, Wellbutrin XL, Zyban, Aplenzin, Forfivo XL 75-mg
Treating Insomnia in Primary Care. Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team
 Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
SUBOXONE (buprenorphine and naloxone) sublingual film (CIII) IMPORTANT SAFETY INFORMATION
 sublingual film (CIII) IMPORTANT SAFETY INFORMATION") SUBOXONE (buprenorphine and naloxone) sublingual film (CIII) IMPORTANT SAFETY INFORMATION What is the most important information I should know about SUBOXONE Film? Keep SUBOXONE Film in a secure place
SUBOXONE (buprenorphine and naloxone) sublingual film (CIII) IMPORTANT SAFETY INFORMATION What is the most important information I should know about SUBOXONE Film? Keep SUBOXONE Film in a secure place
Sleep Symptoms & History
 Sleep Symptoms & History In your own words, please tell us what brings you to the sleep clinic today? How long have you been experiencing your sleep problems? yrs. mos. To give us a precise understanding
Sleep Symptoms & History In your own words, please tell us what brings you to the sleep clinic today? How long have you been experiencing your sleep problems? yrs. mos. To give us a precise understanding
The Prevention & Treatment of Augmentation
 The Prevention & Treatment of Augmentation MARK J BUCHFUHRER, MD S T A N F O R D U N I VERSITY S L E E P M E D I C IN E C E N T ER, R E D W O O D C I T Y, C A P R I VATE P R ACTICE, D O W N E Y, C A 2017
The Prevention & Treatment of Augmentation MARK J BUCHFUHRER, MD S T A N F O R D U N I VERSITY S L E E P M E D I C IN E C E N T ER, R E D W O O D C I T Y, C A P R I VATE P R ACTICE, D O W N E Y, C A 2017
Sleep and Traumatic Brain Injury (TBI)
") Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Where do you get most of your information about medications?
 DRUG ACTION AND RLS Jacquelyn Bainbridge, Pharm.D., FCCP Professor Pei Shieen Wong, Pharm.D., BCPS University of Colorado Anschutz Medical Campus, Skaggs School of Pharmacy and Pharmaceutical Sciences,
DRUG ACTION AND RLS Jacquelyn Bainbridge, Pharm.D., FCCP Professor Pei Shieen Wong, Pharm.D., BCPS University of Colorado Anschutz Medical Campus, Skaggs School of Pharmacy and Pharmaceutical Sciences,
CONCORD INTERNAL MEDICINE. Peripheral Neuropathy. April 22, 2012
 CONCORD INTERNAL MEDICINE Peripheral Neuropathy Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe, III, MD April 22, 2012 The information contained in this protocol should never
CONCORD INTERNAL MEDICINE Peripheral Neuropathy Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe, III, MD April 22, 2012 The information contained in this protocol should never
The Medical Letter. on Drugs and Therapeutics. Usual Adult Hypnotic Dose 1,2 Some Adverse Effects Comments Cost 3
 The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
Parkinson s Founda.on
 Parkinson s Founda.on PD ExpertBriefing: Sleep and Parkinson s Led By: Aleksandar Videnovic, M.D., M.Sc. Associate Professor of Neurology; Director, MGH Program on Sleep, Circadian Biology and NeurodegeneraDon
Parkinson s Founda.on PD ExpertBriefing: Sleep and Parkinson s Led By: Aleksandar Videnovic, M.D., M.Sc. Associate Professor of Neurology; Director, MGH Program on Sleep, Circadian Biology and NeurodegeneraDon
Drugs, Sleep & Wakefulness. Brian Koo Reena Mehra MD MS Kingman Strohl MD
 Drugs, Sleep & Wakefulness Brian Koo Reena Mehra MD MS Kingman Strohl MD Things To Keep In Mind Many drugs effect sleep either causing insomnia or sedation Disruption of sleep and wakefulness may not be
Drugs, Sleep & Wakefulness Brian Koo Reena Mehra MD MS Kingman Strohl MD Things To Keep In Mind Many drugs effect sleep either causing insomnia or sedation Disruption of sleep and wakefulness may not be
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University
 Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Chronic Insomnia: DSM - V. Insomnia DSM - V. Patient Symptoms. Insomnia: Assessment and Overview of Management. Insomnia Management in the Digital Age
 Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
ZOPICLONE Product Monograph Page 34 of 38
 PART III: CONSUMER INFORMATION Pr ZOPICLONE Zopiclone Tablets 5 mg and 7.5 mg House Standard This leaflet is part III of a three-part "Product Monograph" published when ZOPICLONE was approved for sale
PART III: CONSUMER INFORMATION Pr ZOPICLONE Zopiclone Tablets 5 mg and 7.5 mg House Standard This leaflet is part III of a three-part "Product Monograph" published when ZOPICLONE was approved for sale
Parkinson s Disease Medications: Professionals Edition
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Insomnia. F r e q u e n t l y A s k e d Q u e s t i o n s
 Insomnia Q: What is insomnia? A: Insomnia is a common sleep disorder. If you have insomnia, you may: Lie awake for a long time and have trouble falling asleep Wake up a lot and have trouble returning to
Insomnia Q: What is insomnia? A: Insomnia is a common sleep disorder. If you have insomnia, you may: Lie awake for a long time and have trouble falling asleep Wake up a lot and have trouble returning to
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
SIFROL â. Contraindications Hypersensitivity to pramipexole or any other component of the product.
 SIFROL â Composition 1 tablet contains 0.088, 0.18 & 0.7 mg (S) 2 amino 4,5,6,7-tetrahydro-6-propylamino-benzothiazole (= pramipexole base) equivalent to 0.125, 0.25 & 1 mg of pramipexole dihydrochloride
SIFROL â Composition 1 tablet contains 0.088, 0.18 & 0.7 mg (S) 2 amino 4,5,6,7-tetrahydro-6-propylamino-benzothiazole (= pramipexole base) equivalent to 0.125, 0.25 & 1 mg of pramipexole dihydrochloride
LEGS SYNDROME RESTLESS D ETECTION MANAGEMENT. National Center on Sleep Disorders Research and Office of Prevention, Education, and Control AND
 National Center on Sleep Disorders Research and Office of Prevention, Education, and Control RESTLESS LEGS SYNDROME D ETECTION AND MANAGEMENT IN PRIMARY CARE N A T I O N A L I N S T I T U T E S O F H E
National Center on Sleep Disorders Research and Office of Prevention, Education, and Control RESTLESS LEGS SYNDROME D ETECTION AND MANAGEMENT IN PRIMARY CARE N A T I O N A L I N S T I T U T E S O F H E