Question #1. Disclosures. CAPA 2015 Annual Conference. All of the following occur as we get older EXCEPT: Evaluating Patients with Insomnia
|
|
|
- Gordon Wilson
- 6 years ago
- Views:
Transcription

1 Evaluating Patients with Roger D. Seheult, M.D. Pulmonary Critical Care Physician - Beaver Medical Group, Redlands California Assistant Clinical Professor of Medicine - Loma Linda University School of Medicine CAPA Conference Palm Springs 2015 Disclosures Off Label mentions: -amitriptyline, tradazone, triazolam, lorazepam, quazepam Question #1 All of the following occur as we get older EXCEPT: A) increased awakenings, arousals, and stage shifts B) decreased Stage 3+4 (N3) C) reduced sleep efficiency D) phase advancement (go to and get up from bed earlier) E) more sensitive to sleepiness and sleep deprivation 1
2 Question #2 An initial trial of medication for insomnia should last A) As long as the patient needs it B) For the rest of their life C) While they have reduced sleep efficiency D) 6 weeks with cbt then taper the medication E) 12 months then reassess in your clinic Question #3 Which of the following medications is FDA approved for sleep onset insomnia and is not habit forming. A) zolpidem (Ambien) B) zaleplon (Sonata) C) eszopiclone (Lunesta) D) ramelton (Rozerem) E) lorazepam (Ativan) Question #4 A physician from NY is feeling jet-lagged in a conference in HI, what can he do to speed up acclimatization after arriving. A) Expose his eyes to bright light at 0100 B) Avoid afternoon sun exposure (1400) C) Early afternoon sun exposure (1400) D) Sleep as much as he can E) Early afternoon melatonin administration 2
 I have a sleep specialist B) I do not have a sleep specialist Oh sleep, Oh gentle sleep, Nature's soft nurse How have I frighted thee?")
3 Question #5 How many of you have a Sleep Specialist that you can refer to in your practice? A) I have a sleep specialist B) I do not have a sleep specialist Oh sleep, Oh gentle sleep, Nature's soft nurse How have I frighted thee? That though no more will weigh mine eyelids down And sleep my senses in forgetfulness? 1) Sleep changes with normal aging 2) -Pathophysiology -Management -Behavioral -Medication 3) Circadian Rhythm 3

4 Normal Aging Stages of Sleep 1 transition (N1) 2 light sleep (N2) 3,4 physically restorative sleep (N3) REM mentally restorative sleep (R) Normal Aging Most of these changes occur by the age of 40 or 50 Sleep remains pretty constant from age except for.. Sleep efficiency decreases steadily from 95% to 80% as one ages to 80 years of age Middle Age: -increased awakenings, arousals, and stage shifts -decreased Stage 3+4 (N3) -reduced sleep efficiency -phase advancement (go to and get up from bed earlier) -resistance to sleepiness and sleep deprivation Circadian Rhythm Disorder Normal Aging 4

5 Normal Aging DLMO Temp nadir Normal Aging M L L M 5
6 increases as we age years = 14% years = 15% years = 20% years = 25% * Older Adults (mean age = 74 years) -waking too early = 19% -trouble falling asleep = 19% -daytime napping = 25% -insomnia = 29% -both initiating/maintaining sleep = 43% What are the factors contributing to insomnia in the elderly? -medical illness (getting up to urinate) -psychiatric illness (depression) -medication/polypharmacy -alcohol, caffeine, nicotine, -BP meds, decongestants, psych meds -antihistamines, antidepressants (during day) -circadian rhythm disturbances -going to bed too early and get up too early -not enough light exposure (no circadian rhythm) -primary sleep disorders Treatment is individualized depending on what type of is seen: -for patient with insomnia the cause was found to be: -35% psychiatric illness (depression) -15% psychophysiological (performance anxiety) -12% drug and ETOH dependency -12% RLS -10% circadian rhythm sleep disorder -9% paradoxical sleep disorder (not a problem) 6

7 Hard to go to sleep or Hard to stay asleep 3Ps -predisposing factors biological, genetic, worrying -precipitating factors environment, stress, -perpetuating factors behaviors adopted by patient that works against them (see Sleep Hygiene) 7

8 Recommendations: 1) Screen for during health examinations 2) In-dept History and Physical is important if insomnia is found (more) 3) May need to use PSG but do not use routinely 4) Instruments such as questionnaires, logs, checklists may be helpful Symptoms to screen for: -heightened arousal assoc with insomnia -depression, anxiety, OCD -restless leg syndrome (U.R.G.E.) -sleep/wake schedule disorders -snoring or other symptoms of OSA -drug or alcohol abuse -current medication use General Approach: -treat any medical or psychiatric illness, substance disorder or sleep disorder found -counsel on sleep hygiene and stimulus control (BT) 8
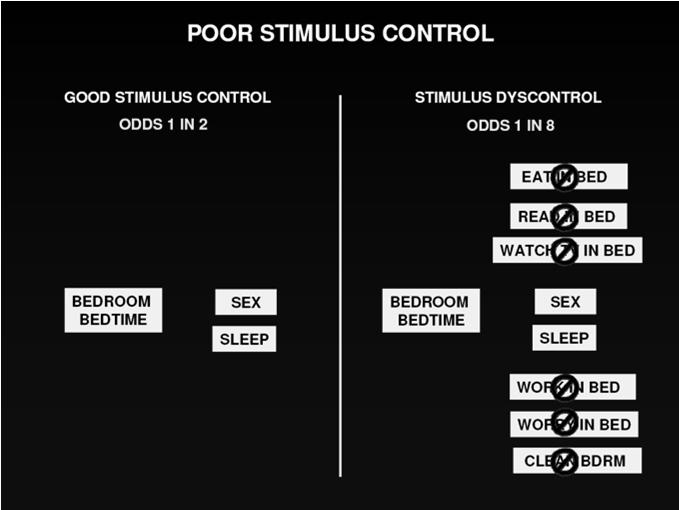
9 Sleep Hygiene Stimulus Control 1) Sleep until rested then get up 1) Go to bed only when sleepy 2) Keep a regular sleep schedule 2) Use bed for sleep and sex only! 3) Do not force sleep -no television, reading, eating 4) Exercise regularly for 20 min, 4-5 hours before bedtime 5) Avoid caffeinated drinks in afternoon 3) Get out of bed if not able to sleep in 20 minutes -return to bed only when sleepy -repeat as many times as nec. 6) Avoid ETOH at bedtime 4) Wake up at same time each day 7) Avoid smoking in PM -use an alarm clock if nec. 8) Do not go to bed hungry 5) No napping 9) Adjust bedroom environment 10) Deal with worries before bedtime General Approach: -treat any medical or psychiatric illness, substance disorder or sleep disorder found -counsel on sleep hygiene and stimulus control (BT) -what about medication first off? Flow chart: General Approach Look for diseases Do Hygiene and Stimulus Behavioral Therapy Medication 9

 Do not force sleep -no television, reading, eating 4) Exercise regularly for 20 min, 4-5 hours before bedtime 5) Avoid caffeinated drinks in afternoon 3) Get out of bed if not able to sleep in 20")
10 General Approach: -treat any medical or psychiatric illness, substance disorder or sleep disorder found -counsel on sleep hygiene and stimulus control (BT) -what about medication first off? CBT-I is at least as effective for treating insomnia when compared with sleep medications, and its effects may be more durable than medications. Sleep Hygiene Stimulus Control 1) Sleep until rested then get up 1) Go to bed only when sleepy 2) Keep a regular sleep schedule 2) Use bed for sleep and sex only! 3) Do not force sleep -no television, reading, eating 4) Exercise regularly for 20 min, 4-5 hours before bedtime 5) Avoid caffeinated drinks in afternoon 3) Get out of bed if not able to sleep in 20 minutes -return to bed only when sleepy -repeat as many times as nec. 6) Avoid ETOH at bedtime 4) Wake up at same time each day 7) Avoid smoking in PM -use an alarm clock if nec. 8) Do not go to bed hungry 5) No napping 9) Adjust bedroom environment 10) Deal with worries before bedtime 10


11 11


12 Flow chart: General Approach Look for diseases Do Hygiene and Stimulus Behavioral Therapy Medication 12
13 For patients that continue to have insomnia: Behavioral Therapy Medications (in addition to Sleep Hygiene and StimulusControl) 1) Relaxation 1) Benzodiazepines 2) Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3) Cognitive Therapy 3) Melatonin agonists 4) Cognitive Behavioral Therapy 4) Antidepressants Target of BT Behavioral Therapy (in addition to Sleep Hygiene and StimulusControl) Relaxation Therapy Medications 1) Relaxation 1) Benzodiazepines 2) Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3) Cognitive Therapy 3) Melatonin agonists 4) Cognitive Behavioral Therapy 4) Antidepressants Progressive relaxation -relax one muscle at a time until the whole body is relaxed -start in face: contract muscles for 1-2 sec -repeat for 45 minutes Relaxation Response -lying down, close eyes -allow relaxation to spread throughout entire body -turn thoughts to more peaceful things 13
 Melatonin agonists 4) Cognitive Behavioral Therapy 4) Antidepressants Sleep Restriction Therapy (de-fragmentation therapy) -insomnia stay in bed longer circ shift & homeostatic drive (vicious")

14 Behavioral Therapy Medications (in addition to Sleep Hygiene and StimulusControl) 1) Relaxation 1) Benzodiazepines 2) Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3) Cognitive Therapy 3) Melatonin agonists 4) Cognitive Behavioral Therapy 4) Antidepressants Sleep Restriction Therapy (de-fragmentation therapy) -insomnia stay in bed longer circ shift & homeostatic drive (vicious cycle) -purpose is to increase sleep drive and consolidate sleep and sleep efficiency -add up all fragments (no less than 5 h) and count back from target wake time -patient is allowed to go to bed only at that time until sleep efficiency > 85% -once this happens, patient allowed to go to bed 15 minutes earlier until > 85% -keep going back until excessive daytime sleepiness improves -NO NAPPING. 14
 Behavioral Therapy Medications (in addition to Sleep Hygiene and StimulusControl) 1) Relaxation 1) Benzodiazepines 2) Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3)")
 -purpose is to increase sleep drive and consolidate sleep and sleep efficiency -add up all fragments (no less than 5 h) and count back from target wake time -patient is allowed")
15 -Restrict to the number of hours in bed = average TST -5 Hours should be the minimum -PTTB and PTOB are inflexible -Review ways to stay awake -Keep diary -Titration based on diary data (85% or more versus less) Behavioral Therapy Medications (in addition to Sleep Hygiene and StimulusControl) 1) Relaxation 1) Benzodiazepines 2) Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3) Cognitive Therapy 3) Melatonin agonists 4) Cognitive Behavioral Therapy 4) Antidepressants Sleep Restriction Therapy (de-fragmentation therapy) -insomnia stay in bed longer circ shift & homeostatic drive (vicious cycle) -purpose is to increase sleep drive and consolidate sleep and sleep efficiency -add up all fragments (no less than 5 h) and count back from target wake time -patient is allowed to go to bed only at that time until sleep efficiency > 85% -once this happens, patient allowed to go to bed 15 minutes earlier until > 85% -keep going back until excessive daytime sleepiness improves -must monitor these patient very carefully for sleep deprivation. 1 1) Kyle DS et al. Sleep restriction therapy for insomnia is associatedwith reduced objective total sleep time, increaseddaytime somnolence, and objectively impaired vigilance: implications for the clinical management of insomnia disorder. Sleep 2014; 37:229 Behavioral Therapy Medications (in addition to Sleep Hygiene and StimulusControl) 1) Relaxation 1) Benzodiazepines 2) Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3) Cognitive Therapy 3) Melatonin agonists 4) Cognitive Behavioral Therapy 4) Antidepressants Cognitive Therapy -prevent people from making a mountain out of a molehill -catastrophic thinking -establishing realistic expectations 15
 Relaxation 1) Benzodiazepines 2) Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3)")
 NIH State ofthe Science Conferencestatement on Manifestations and Management of Chronic in Adults, June 13-15, 2005. Sleep 2005; 28:1049 2) McCurry SM, et al.")
16 Behavioral Therapy (in addition to Sleep Hygiene and StimulusControl) Cognitive-Behavioral Therapy -combination of the preceding -education, stimulus control, sleep restriction, cognitive therapy, sleep hygiene -provides patients tools for the future -very few can do a good job Medications 1) Relaxation 1) Benzodiazepines 2) Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3) Cognitive Therapy 3) Melatonin agonists 4) Cognitive Behavioral Therapy 4) Antidepressants -proven effective 1 to improve sleep quality and decrease awake time during the night. 2 1) NIH State ofthe Science Conferencestatement on Manifestations and Management of Chronic in Adults, June 13-15, Sleep 2005; 28:1049 2) McCurry SM, et al. Evidence-based psychological treatments for insomnia in older adults. Psychol Aging 2007; 22:18 Medications 16
17 Behavioral Therapy Medications (in addition to Sleep Hygiene and StimulusControl) 1) Relaxation 1) Benzodiazepines 2) Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3) Cognitive Therapy 3) Melatonin agonists 4) Cognitive Behavioral Therapy 4) Antidepressants Medications in general -usual improvement in daytime function, better QOL, few comorbidities -risks include side effects and addiction with long term use Risks go up in -pregnancy: fetal malformations -alcohol consuption -kidney disease, liver, or pulmonary disease -sleep apnea -nighttime decision makers* -elderly (75+ years) WHICH ONE DO I CHOOSE? Has to do with what type of insomnia. Sleep onset or maintenance? Benzodiazepines Binds to several GABA A receptors (longer) SL, N2, TST, REM, impair memory anxiety, anticonvulsant -SE: daytime sleepiness, motor, cognitive, dependence, complex sleep-related behaviors triazolam (Halcion) estazolam (Prosom) lorazepam (Ativan) temazepam (Restoril) flurazepam (Dalmane) quazepam (Doral) Medications 1) Benzodiazepines 2) Nonbenzodiazepines sedatives 3) Melatonin agonists 4) Antidepressants Nonbenzodiazepines Targets GABA A receptor specifically SL, N2, TST, REM, impair memory Less anxiety, less anticonvulsant -SE: less daytime sleepiness, motor, cognitive, dependence,, complex sleep-related behaviors zolpidem (Ambien) t 1/2 = 2h* zolpidem (Ambien-CR) t 1/2 = 2h** zaleplon (Sonata) t 1/2 = 1h eszopiclone (Lunesta) t 1/2 = 6 h 17

18 FDA warning 1/2013: Zolpidem (Ambien) -recommend use of a lower dose in women then previously recommended, consider this also in men Zolpidem (Ambien CR) -recommend use of a lower dose in women then previously recommended, consider this also in men - patients should not drive or engage in other activities that require complete mental alertness the day after taking zolpidem extended release because zolpidem levels can remain high enough the next day to impair these activities. 1) Medications WHICH ONE DO I CHOOSE? Has to do with what type of insomnia. Sleep onset or maintenance? 1) Benzodiazepines 2) Nonbenzodiazepines sedatives 3) Melatonin agonists 4) Antidepressants Melatonin agonists ramelton (Rozerem) -bind to M receptors tighter than melatonin (t 1/2 = hours) -better for sleep onset insomnia (give 30 minutes before bedtime) -fewer side effects then B or NB; no hypnotic SE (next day) -cleared through the liver, contraindicated with fluvoxamine -not habit forming -may prolactin and testosterone (don t need to monitor unless symptoms) -not a scheduled drug with the FDA - SL by minutes, TST by minutes lasted for up to 1 year or more 18
19 Medications WHICH ONE DO I CHOOSE? Has to do with what type of insomnia. Sleep onset or maintenance? 1) Benzodiazepines 2) Nonbenzodiazepines sedatives 3) Melatonin agonists 4) Antidepressants Antidepressants (doxepine, amitriptyline, trazadone) -Doxepine: only 3 and 6 mg dose is FDA approved -amitriptyline and trazadone (antihistamine, anticholinergic effects) -use in depressed patients with insomnia -not depressed? doxepine 3 mg versus placebo: WASO, TST, Sleep efficiency, Sleep quality trazadone versus zolpidem: no difference 1 -the routine use of sedating antidepressants other than low dose doxepine is not recommendeddue to side effects 1) Walsh etal. Subjective hypnotic efficacyoftrazadone and zolpidem in DSM-III-R primary insomnia. Hun Psychopharmacol 1998; 13:191 Medications WHICH ONE DO I CHOOSE? Has to do with what type of insomnia. Sleep onset or maintenance? 1) Benzodiazepines 2) Nonbenzodiazepines sedatives 3) Melatonin agonists 4) Antidepressants Not recommended 1 -Diphenhydramine no evidence it improves insomnia, next day SE alterness, cognitive, dry mouth -Antipsychotics few trials and many SE -Barbiturates - few trials and many SE -Over the Counter -Valerian - SL < 1 min, hepatic SE, no regulation -Melatonin works in delayed sleep phase syndrome and low melatonin levels** -Alcohol short term SL. Promotes sleep disturbance later in the night, OSA, dependence, interaction with other meds. 1) NIH Stateof the ScienceConferencestatementon ManifestationsandManagement ofchronic in Adults, June 13-15, Sleep2005; 28:1049 More about Side effects: Older adults: -in 60 years plus pharmacotherapy: - sleep quality, TST, freq awakening 1-2-5x adverse cognitive or psychomotor events (falls, fractures) Mortality: -observational studies connect sedative hypnotics and all-cause mortality! -OR: !!!! -other studies than adjusted for confounders did not -need prospective study to look as causality 1) Glass et al. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits. BMJ 2005; 331:
 Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3) Cognitive Therapy 3) Melatonin agonists 4) Cognitive Behavioral Therapy 4) Antidepressants Combination Therapy -CBT +")
20 Flow chart: General Approach Look for diseases Do Hygiene and Stimulus Behavioral Therapy Medication Behavioral Therapy Medications (in addition to Sleep Hygiene and StimulusControl) 1) Relaxation 1) Benzodiazepines 2) Sleep restriction Therapy 2) Nonbenzodiazepines sedatives 3) Cognitive Therapy 3) Melatonin agonists 4) Cognitive Behavioral Therapy 4) Antidepressants Combination Therapy -CBT + Medication for 6-8 weeks -taper the medication and continue the CBT Study: Morin et el. 20
21 Combination Therapy -CBT + Medication for 6-8 weeks -taper the medication and continue the CBT Flow chart: General Approach Look for diseases Do Hygiene and Stimulus Behavioral Therapy Medication (6 wks) Sleep Specialist? 21
 2300 Go to Sleep 0500 Core body temperature nadir 0700 wake up 8 hours -light")
 Questionnaire 2) Sleep diary / actigraphy for at least 7 days 3) Core body temperature 4)")
22 Pineal SCN Melatonin Output Sleep/Wake Cycle Circadian Rhythm Facts: -body temperature, melatonin secretion, sleep onset and waking up are all on the clock and related to each other 2100 Dim light melatonin onset (DLMO) 2300 Go to Sleep 0500 Core body temperature nadir 0700 wake up 8 hours -light exposure after nadir advances rhythm (1-2 h before wake) -light exposure before nadir delays rhythm (2h before sleep) -melatonin administration 5-7 hours before sleep time advances rhythm Things to measure: 1) Questionnaire 2) Sleep diary / actigraphy for at least 7 days 3) Core body temperature 4) Melatonin levels 22


23 Circadian Rhythm Disorders Delayed Sleep Phase -22 year old female medical student can t fall asleep until 3AM with difficulty waking up in the morning. -struggled through college to make it to morning classes -zolpidem helps only intermittently 23

24 Advanced Sleep Phase -78 year old woman with early morning awakening and excessive daytime sleepiness over the last 2 years -falls asleep at 8PM but would like to stay up until 10:30PM -gets up at 3AM but scheduled wake up time is 6AM 24

25 Advanced Sleep Phase -50 year old physician goes to a medical conference in Kona, HI and has difficulty staying awake at dinner but finds himself having no difficulty making the 7AM breakfast. -he is going to take a vacation in HI at the end of the conference and realizes that he is a bit jet lagged. What is the best option to get on schedule here and also when he gets back to the mainland so he minimizes work loss? From Mainland to HI H A S T P D T M M D T M C D T M E D T M From HI back to Mainland H A S T M P D T M D T C D T E D T M
 Circadian Rhythm")
26 1) Sleep changes with normal aging 2) -Pathophysiology -Management -Behavioral -Medication 3) Circadian Rhythm Questions? 26
27 Question #1 All of the following occur as we get older EXCEPT: A) increased awakenings, arousals, and stage shifts B) decreased Stage 3+4 (N3) C) reduced sleep efficiency D) phase advancement (go to and get up from bed earlier) E) more sensitive to sleepiness and sleep deprivation Question #2 An initial trial of medication for insomnia should last A) As long as the patient needs it B) For the rest of their life C) reduced sleep efficiency D) 6 weeks with cbt then taper the medication E) 12 months then reassess in your clinic Question #3 Which of the following medications is FDA approved for sleep onset insomnia and is not habit forming. A) zolpidem (Ambien) B) zaleplon (Sonata) C) eszopiclone (Lunesta) D) ramelton (Rozerem) E) lorazepam (Ativan) 27
28 Question #4 A physician from NY is feeling jet-lagged in a conference in HI, what can he do to speed up acclimatization after arriving. A) Expose his eyes to bright light at 0100 B) Avoid afternoon sun exposure (1400) C) Early afternoon sun exposure (1400) D) Sleep as much as he can E) Early afternoon melatonin administration 28
Insomnia. Learning Objectives. Disclosure 6/7/11. Research funding: NIH, Respironics, Embla Consulting: Elsevier
 Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Pharmacological Help for a Good Night s s Sleep. Thomas Owens, MD
 Pharmacological Help for a Good Night s s Sleep Thomas Owens, MD Objectives 1. Define insomnia and characterize the symptoms and array of causes. 2. Describe traditional and new pharmacologic approaches
Pharmacological Help for a Good Night s s Sleep Thomas Owens, MD Objectives 1. Define insomnia and characterize the symptoms and array of causes. 2. Describe traditional and new pharmacologic approaches
Insomnia treatment. Sleep hygiene education sleep hygiene teaches good sleeping habits. This includes:
 Insomnia treatment INSOMNIA OVERVIEW insomnia is defined as difficulty falling asleep, difficulty staying asleep, or waking up early in the morning and not being able to return to sleep. In general, people
Insomnia treatment INSOMNIA OVERVIEW insomnia is defined as difficulty falling asleep, difficulty staying asleep, or waking up early in the morning and not being able to return to sleep. In general, people
Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER
 Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER Disclosure: Financial - none Non-Financial - none Selected Topics Sleep epidemiology Sleep
Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER Disclosure: Financial - none Non-Financial - none Selected Topics Sleep epidemiology Sleep
Managing Insomnia Disorder A Review of the Research for Adults
 Managing Insomnia Disorder A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional said you have insomnia disorder (said
Managing Insomnia Disorder A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional said you have insomnia disorder (said
Insomnia: Updates in Medical Management. Michael Newnam M.D.
 Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Insomnia treatment in primary care
 Insomnia treatment in primary care Daniel J. Buysse, MD UPMC Professor of Sleep Medicine Professor of Psychiatry and Clinical and Translational Science University of Pittsburgh School of Medicine buyssedj@upmc.edu
Insomnia treatment in primary care Daniel J. Buysse, MD UPMC Professor of Sleep Medicine Professor of Psychiatry and Clinical and Translational Science University of Pittsburgh School of Medicine buyssedj@upmc.edu
Insomnia % of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences)
") 10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
Dr Alex Bartle. Sleep Well Clinic
 Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Learning Objectives. Management of Insomnia. Impact of Chronic Insomnia. Insomnia: Definitions. Measurement of Goals. Goals of Therapy 9/29/2017
 Learning Objectives Characterize insomnia and its negative effects Management of Insomnia Discuss the goals of treatment Summarize guidelines of management of insomnia including non-pharmacologic and pharmacologic
Learning Objectives Characterize insomnia and its negative effects Management of Insomnia Discuss the goals of treatment Summarize guidelines of management of insomnia including non-pharmacologic and pharmacologic
INSOMNIA IN THE GERIATRIC POPULATION. Shannon Bush, MS4
 INSOMNIA IN THE GERIATRIC POPULATION Shannon Bush, MS4 CHANGES IN SLEEP ARCHITECTURE 2 Reduction in slow wave sleep (stage 3 and 4) Increase in lighter stages of sleep (stage 1 and 2) Decrease in REM sleep
INSOMNIA IN THE GERIATRIC POPULATION Shannon Bush, MS4 CHANGES IN SLEEP ARCHITECTURE 2 Reduction in slow wave sleep (stage 3 and 4) Increase in lighter stages of sleep (stage 1 and 2) Decrease in REM sleep
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia
 Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
Sleep and Parkinson's Disease
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Insomnia: habits, help, and hazards
 Insomnia: habits, help, and hazards Balanced data about medications www.rxfacts.org Copyright 2010 by The Alosa Foundation www.rxfacts.org November 2010 2 www.rxfacts.org Author: Leslie Jackowski, B.Sc.,
Insomnia: habits, help, and hazards Balanced data about medications www.rxfacts.org Copyright 2010 by The Alosa Foundation www.rxfacts.org November 2010 2 www.rxfacts.org Author: Leslie Jackowski, B.Sc.,
Insomnia Agents (Sherwood Employer Group)
") Insomnia Agents (Sherwood Employer Group) BCBSKS will review Prior Authorization requests Prior Authorization Form: https://www.bcbsks.com/customerservice/forms/pdf/priorauth-6058ks-st-ippi.pdf Link to
Insomnia Agents (Sherwood Employer Group) BCBSKS will review Prior Authorization requests Prior Authorization Form: https://www.bcbsks.com/customerservice/forms/pdf/priorauth-6058ks-st-ippi.pdf Link to
How to Manage Insomnia with and without medications
 How to Manage Insomnia with and without medications Tatyana Gurvich, Pharm.D. USC School of Pharmacy UC Irvine SeniorHealth Center Insomnia: How common is it? 26-50% of adult population complain of insomnia
How to Manage Insomnia with and without medications Tatyana Gurvich, Pharm.D. USC School of Pharmacy UC Irvine SeniorHealth Center Insomnia: How common is it? 26-50% of adult population complain of insomnia
Chronic Insomnia: DSM - V. Insomnia DSM - V. Patient Symptoms. Insomnia: Assessment and Overview of Management. Insomnia Management in the Digital Age
 Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
CPT David Shaha, MC US Army
 CPT David Shaha, MC US Army None Thoughts and comments are my own and do not represent the official policy of the Department of the Army, Department of Defense, or United States Government. Clinical Case
CPT David Shaha, MC US Army None Thoughts and comments are my own and do not represent the official policy of the Department of the Army, Department of Defense, or United States Government. Clinical Case
Available Strengths Limits. 200 mg tablets PA. 50 mg, 150 mg, 200 mg, 250 mg tablets. 500 mg/ml solution PA
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY Sleeping Disorders P&T DATE: 12/14/2016 THERAPEUTIC CLASS Psychiatric Disorders REVIEW HISTORY: 2/16, 5/15, 2/12 LOB AFFECTED
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY Sleeping Disorders P&T DATE: 12/14/2016 THERAPEUTIC CLASS Psychiatric Disorders REVIEW HISTORY: 2/16, 5/15, 2/12 LOB AFFECTED
Insomnia. F r e q u e n t l y A s k e d Q u e s t i o n s
 Insomnia Q: What is insomnia? A: Insomnia is a common sleep disorder. If you have insomnia, you may: Lie awake for a long time and have trouble falling asleep Wake up a lot and have trouble returning to
Insomnia Q: What is insomnia? A: Insomnia is a common sleep disorder. If you have insomnia, you may: Lie awake for a long time and have trouble falling asleep Wake up a lot and have trouble returning to
CBT for Insomnia: Past, Present, and Future Directions
 CBT for Insomnia: Past, Present, and Future Directions J. Todd Arnedt, Ph.D. Associate Professor of Psychiatry and Neurology Director, Behavioral Sleep Medicine Program Acting Director, Sleep and Circadian
CBT for Insomnia: Past, Present, and Future Directions J. Todd Arnedt, Ph.D. Associate Professor of Psychiatry and Neurology Director, Behavioral Sleep Medicine Program Acting Director, Sleep and Circadian
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
AGING CHANGES IN SLEEP
 OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
Insomnia. Dr Terri Henderson MBChB FCPsych
 Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
INSOMNIAS. Stephan Eisenschenk, MD Department of Neurology
 INSOMNIAS INSOMNIAS General criteria for insomnia A. Repeated difficulty with sleep initiation, duration, consolidation or quality. B. Adequate sleep opportunity, persistent sleep difficulty and associated
INSOMNIAS INSOMNIAS General criteria for insomnia A. Repeated difficulty with sleep initiation, duration, consolidation or quality. B. Adequate sleep opportunity, persistent sleep difficulty and associated
Healthy Sleep Tips Along the Way!
 Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Sleep and Ageing. Siobhan Banks PhD. Body and Brain at Work, Centre for Sleep Research University of South Australia
 Sleep and Ageing Siobhan Banks PhD Body and Brain at Work, Centre for Sleep Research University of South Australia Health and Active Ageing, 22 nd September 2015 Sleep and Aging How does sleep change as
Sleep and Ageing Siobhan Banks PhD Body and Brain at Work, Centre for Sleep Research University of South Australia Health and Active Ageing, 22 nd September 2015 Sleep and Aging How does sleep change as
WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?)
") Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?) CATHERINE MCCALL, MD
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?) CATHERINE MCCALL, MD
HEALTHY LIFESTYLE, HEALTHY SLEEP. There are many different sleep disorders, and almost all of them can be improved with lifestyle changes.
 HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
The Medical Letter. on Drugs and Therapeutics. Usual Adult Hypnotic Dose 1,2 Some Adverse Effects Comments Cost 3
 The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
INDEX. Group psychotherapy, described, 97 Group stimulus control, 29-47; see also Stimulus control (group setting)
") Index Abdominal breathing, 70; see also Breathing; Relaxation therapy Activation, sleep drive/responsivity, 6-9 Age level; see also Elderly circadian rhythms and, 68-69 delayed sleep phase syndrome and,
Index Abdominal breathing, 70; see also Breathing; Relaxation therapy Activation, sleep drive/responsivity, 6-9 Age level; see also Elderly circadian rhythms and, 68-69 delayed sleep phase syndrome and,
6/3/2015. Insomnia An Integrative Approach. Objectives. Why An Integrative Approach? Integrative Model. Definition. Short-term Insomnia
 Insomnia An Integrative Approach Jeffrey S. Jump, M.D. Medical Director CHI Memorial Integrative Medicine Associates Objectives Understand the importance of sleep to health Identify patients with insomnia
Insomnia An Integrative Approach Jeffrey S. Jump, M.D. Medical Director CHI Memorial Integrative Medicine Associates Objectives Understand the importance of sleep to health Identify patients with insomnia
Modern Management of Sleep Disorders. If Only I Could Sleep Like I Did Before
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
Introduction. v Insomnia is very prevalent in acute (30-50%) and chronic forms (10-15%). v Insomnia is often ignored as a symptom of other disorders.
 and chronic forms (10-15%). v Insomnia is often ignored as a symptom of other disorders.") Introduction v Insomnia is very prevalent in acute (30-50%) and chronic forms (10-15%). v Insomnia is often ignored as a symptom of other disorders. v Insomnia is a risk factor for psychiatric and medical
Introduction v Insomnia is very prevalent in acute (30-50%) and chronic forms (10-15%). v Insomnia is often ignored as a symptom of other disorders. v Insomnia is a risk factor for psychiatric and medical
You May Be at Risk. You are taking one of the following sedative-hypnotic medications: Diazepam (Valium ) Estazolam. Flurazepam.
 Estazolam. Flurazepam.") You May Be at Risk You are taking one of the following sedative-hypnotic medications: Alprazolam (Xanax ) Diazepam (Valium ) Temazepam (Restoril ) Chlorazepate Estazolam Triazolam (Halcion ) Chlordiazepoxide
You May Be at Risk You are taking one of the following sedative-hypnotic medications: Alprazolam (Xanax ) Diazepam (Valium ) Temazepam (Restoril ) Chlorazepate Estazolam Triazolam (Halcion ) Chlordiazepoxide
Psychopharmacology of Sleep Disorders
 Psychopharmacology of Sleep Disorders John W. Winkelman MD, PhD Chief, Sleep Disorders Clinical Research Program Departments of Psychiatry and Neurology Massachusetts General Hospital Professor of Psychiatry
Psychopharmacology of Sleep Disorders John W. Winkelman MD, PhD Chief, Sleep Disorders Clinical Research Program Departments of Psychiatry and Neurology Massachusetts General Hospital Professor of Psychiatry
SLEEP-WAKE DISORDERS: INSOMNIA. Prof. Paz Gía-Portilla
 SLEEP-WAKE DISORDERS: INSOMNIA Prof. Paz Gía-Portilla SLEEP-WAKE DISORDERS AND ICD-10 Chapter V: Mental and Behavioural Disorders F51. Non-organic sleep disorders Chapter VI: Nervous System Illnesses G47.
SLEEP-WAKE DISORDERS: INSOMNIA Prof. Paz Gía-Portilla SLEEP-WAKE DISORDERS AND ICD-10 Chapter V: Mental and Behavioural Disorders F51. Non-organic sleep disorders Chapter VI: Nervous System Illnesses G47.
Sleep History Questionnaire
 Location South Loop Katy Steeplechase Fort Bend NAME ADDRESS PHONE SEX DOB AGE HEIGHT WEIGHT NECK COLLAR SIZE (inches) Do you have difficulty falling asleep? Is your sleep restless or disturbed? Do you
Location South Loop Katy Steeplechase Fort Bend NAME ADDRESS PHONE SEX DOB AGE HEIGHT WEIGHT NECK COLLAR SIZE (inches) Do you have difficulty falling asleep? Is your sleep restless or disturbed? Do you
SEDATIVE-HYPNOTIC AGENTS
 SEDATIVE-HYPNOTIC AGENTS Documentation A. FDA approved indications 1. Insomnia 2. Sedation for an agitated patient in an inpatient setting Documentation B. Non-FDA approved, commonly used indications 1.
SEDATIVE-HYPNOTIC AGENTS Documentation A. FDA approved indications 1. Insomnia 2. Sedation for an agitated patient in an inpatient setting Documentation B. Non-FDA approved, commonly used indications 1.
Many people with physical
 FACTSHEET How to Sleep Better Many people with physical disabilities suffer from sleep disturbances, and sleep tends to become more disrupted as we get older. Not sleeping well can negatively impact your
FACTSHEET How to Sleep Better Many people with physical disabilities suffer from sleep disturbances, and sleep tends to become more disrupted as we get older. Not sleeping well can negatively impact your
Insomnia. St. Joseph s Annual Family Practice Refresher March 1, Robert J. Ostrander, M.D
 St. Joseph s Annual Family Practice Refresher March 1, 2018 Robert J. Ostrander, M.D If in bed I say, When shall I arise? then the night drags on; I am filled with restlessness until the dawn. Job 7:4
St. Joseph s Annual Family Practice Refresher March 1, 2018 Robert J. Ostrander, M.D If in bed I say, When shall I arise? then the night drags on; I am filled with restlessness until the dawn. Job 7:4
Earl J. Soileau, MD, FSAHM Asst Professor, Family Medicine LSU HSC Medical School New Orleans at Lake Charles
 Earl J. Soileau, MD, FSAHM Asst Professor, Family Medicine LSU HSC Medical School New Orleans at Lake Charles Sleep Disorders Restless Legs Syndrome (RLS) and Periodic Limb Movement Disorder (PLMD) Sleep
Earl J. Soileau, MD, FSAHM Asst Professor, Family Medicine LSU HSC Medical School New Orleans at Lake Charles Sleep Disorders Restless Legs Syndrome (RLS) and Periodic Limb Movement Disorder (PLMD) Sleep
Insomnia Disorder A Journey to the Land of No Nod
 Insomnia Disorder A Journey to the Land of No Nod JACQUELINE D. KLOSS, PH.D. P S Y C H O L O G I S T B R Y N M A W R P S Y C H O L O G I C A L A S S O C I A T E S B E H A V I O R A L S L E E P M E D I
Insomnia Disorder A Journey to the Land of No Nod JACQUELINE D. KLOSS, PH.D. P S Y C H O L O G I S T B R Y N M A W R P S Y C H O L O G I C A L A S S O C I A T E S B E H A V I O R A L S L E E P M E D I
Insomnia Treatment in Brief
 Insomnia Treatment in Brief Project ECHO May 7, 2015 Jonathan Emens, M.D. Associate Professor, Departments of Psychiatry and Internal Medicine Oregon Health & Science University Staff Physician and Sleep
Insomnia Treatment in Brief Project ECHO May 7, 2015 Jonathan Emens, M.D. Associate Professor, Departments of Psychiatry and Internal Medicine Oregon Health & Science University Staff Physician and Sleep
3/24/2016 DISCLOSURE STATEMENT PHARMACIST OBJECTIVES OVERVIEW TECHNICIAN OBJECTIVES PREVALENCE OF INSOMNIA THE WRONG SIDE OF THE BED: CHRONIC INSOMNIA
 DISCLOSURE STATEMENT I do not have any actual or potential conflict of interest in relation to this presentation THE WRONG SIDE OF THE BED: CHRONIC INSOMNIA DANIELLE ROWAN, PHARMD, MBA PGY1 PHARMACY PRACTICE
DISCLOSURE STATEMENT I do not have any actual or potential conflict of interest in relation to this presentation THE WRONG SIDE OF THE BED: CHRONIC INSOMNIA DANIELLE ROWAN, PHARMD, MBA PGY1 PHARMACY PRACTICE
Guideline for Adult Insomnia
 Guideline for Adult Insomnia Exclusions This guideline does not apply to: Children under the age of 18 Pregnant and lactating women Geriatric patients: While the general principles of the diagnosis and
Guideline for Adult Insomnia Exclusions This guideline does not apply to: Children under the age of 18 Pregnant and lactating women Geriatric patients: While the general principles of the diagnosis and
WHY CAN T I SLEEP? Deepti Chandran, MD
 WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
You May Be at Risk. You are taking one of the following sedative-hypnotic medications:
 You May Be at Risk You are taking one of the following sedative-hypnotic medications: Alprazolam (Xanax ) Bromazepam (Lectopam ) Chlorazepate Chlordiazepoxideamitriptyline Clidinium-chlordiazepoxide Clobazam
You May Be at Risk You are taking one of the following sedative-hypnotic medications: Alprazolam (Xanax ) Bromazepam (Lectopam ) Chlorazepate Chlordiazepoxideamitriptyline Clidinium-chlordiazepoxide Clobazam
LEARNING OBJECTIVES SLEEP APNEA
 LEARNING OBJECTIVES List key differences between insomnia and obstructive sleep apnea Identify at least two appropriate pharmacologic treatment options for insomnia INSOMNIA VS. SLEEP APNEA Morganne Smyth,
LEARNING OBJECTIVES List key differences between insomnia and obstructive sleep apnea Identify at least two appropriate pharmacologic treatment options for insomnia INSOMNIA VS. SLEEP APNEA Morganne Smyth,
Article printed from
 What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
What is sleep? o Sleep is a body s rest cycle.
 What is sleep? o Sleep is a state when our senses and motor actvity are relatively suspended; there is a total or partial unconsciousness and all voluntary muscles are inactive. o Sleep is a body s rest
What is sleep? o Sleep is a state when our senses and motor actvity are relatively suspended; there is a total or partial unconsciousness and all voluntary muscles are inactive. o Sleep is a body s rest
Treating Insomnia in Primary Care. Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team
 Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
14. Percent Mellinger GD et al. Arch Gen Psychiatry. 1985;42: ICSD III
 4:45 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau
4:45 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau
Sleep and Insomnia 2/8/2018. Presented by. Marie Rataj, MSN, APRN, ANP. Objectives. Everything you wanted to know
 Sleep and Insomnia Everything you wanted to know Presented by Marie Rataj, MSN, APRN, ANP Objectives Develop a basic knowledge of normal sleep and differentiate from abnormal sleep Develop basic understanding
Sleep and Insomnia Everything you wanted to know Presented by Marie Rataj, MSN, APRN, ANP Objectives Develop a basic knowledge of normal sleep and differentiate from abnormal sleep Develop basic understanding
Modern Management of Sleep Disorders. Case. Introduction. Topics Covered. Douglas C. Bauer, MD University of California, San Francisco
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Addressing the Multiple Causes and Lifestyle Impacts of Insomnia: A Guide for Patient Counseling
 Addressing the Multiple Causes and Lifestyle Impacts of Insomnia: A Guide for Patient Counseling Educational Objectives: At the completion of this knowledge-based activity, participants will be able to:
Addressing the Multiple Causes and Lifestyle Impacts of Insomnia: A Guide for Patient Counseling Educational Objectives: At the completion of this knowledge-based activity, participants will be able to:
Modern Management of Sleep Disorders
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Cognitive Behavioral Therapy for Insomnia. Melanie K. Leggett, PhD, CBSM Duke University Medical Center
 Cognitive Behavioral Therapy for Insomnia Melanie K. Leggett, PhD, CBSM Duke University Medical Center Disclosures I have no relevant financial relationship with the manufacturers of any commercial products
Cognitive Behavioral Therapy for Insomnia Melanie K. Leggett, PhD, CBSM Duke University Medical Center Disclosures I have no relevant financial relationship with the manufacturers of any commercial products
Insomnia. Arturo Meade MD
 Insomnia Arturo Meade MD Goals Definition Prevalence Pathophysiology The role of Orexin Orexin receptor blockers Consequences: Daily Functioning Insomnia: Consequences Decreased quality of life
Insomnia Arturo Meade MD Goals Definition Prevalence Pathophysiology The role of Orexin Orexin receptor blockers Consequences: Daily Functioning Insomnia: Consequences Decreased quality of life
Dr Alex Bartle. Medical Director Sleep Well Clinic Christchurch
 Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 11:00-11:55 WS #113: Circadian Sleep Disorders 12:05-13:00 WS #125: Circadian Sleep Disorders (Repeated) Overview The Structure of Sleep
Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 11:00-11:55 WS #113: Circadian Sleep Disorders 12:05-13:00 WS #125: Circadian Sleep Disorders (Repeated) Overview The Structure of Sleep
Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
 COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems. Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems. Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
Sleep and Traumatic Brain Injury (TBI)
") Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Treatment of Insomnia for Clinicians
 Treatment of Insomnia for Clinicians Larry Pawluk, M.D., FRCPC Diplomate, American Board of Sleep Medicine Clinical Professor of Psychiatry, Sleep Medicine Program, University of Alberta What is Insomnia?
Treatment of Insomnia for Clinicians Larry Pawluk, M.D., FRCPC Diplomate, American Board of Sleep Medicine Clinical Professor of Psychiatry, Sleep Medicine Program, University of Alberta What is Insomnia?
SLEEP UPDATE 2008 SLEEP HYPNOGRAM. David Claman, MD UCSF Sleep Disorders Center
 SLEEP UPDATE 2008 SLEEP HYPNOGRAM David Claman, MD UCSF Sleep Disorders Center Insomnia Case A 40 year old man c/o insomnia at sleep onset. He worries about sleep at night, and takes 2-3 hrs to fall asleep.
SLEEP UPDATE 2008 SLEEP HYPNOGRAM David Claman, MD UCSF Sleep Disorders Center Insomnia Case A 40 year old man c/o insomnia at sleep onset. He worries about sleep at night, and takes 2-3 hrs to fall asleep.
Sleep Disorders: Assessment and Therapeutic Options
 Sleep Disorders: Assessment and Therapeutic Options John W. Winkelman MD, PhD Chief, Sleep Disorders Clinical Research Program Departments of Psychiatry and Neurology Massachusetts General Hospital Professor
Sleep Disorders: Assessment and Therapeutic Options John W. Winkelman MD, PhD Chief, Sleep Disorders Clinical Research Program Departments of Psychiatry and Neurology Massachusetts General Hospital Professor
Drug Review Rozerem (ramelteon)
") Drug Review Rozerem (ramelteon) Introduction 1 Ramelteon is a melatonin receptor agonist with affinity for MT 1 and MT 2 and selectivity over the MT 3 receptor. The activity at the MT 1 and MT 2 receptors
Drug Review Rozerem (ramelteon) Introduction 1 Ramelteon is a melatonin receptor agonist with affinity for MT 1 and MT 2 and selectivity over the MT 3 receptor. The activity at the MT 1 and MT 2 receptors
TOP 10 LIST OF SLEEP QUESTIONS. Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children
 TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
SLEEP DISORDERS. Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children
 SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
Insomnia Restoring Restful Sleep
 Insomnia Restoring Restful Sleep written by Harvard Medical School www.patientedu.org Nearly everyone has spent at least one night lying in bed wishing for sleep. But for many people, it s a nightly struggle.
Insomnia Restoring Restful Sleep written by Harvard Medical School www.patientedu.org Nearly everyone has spent at least one night lying in bed wishing for sleep. But for many people, it s a nightly struggle.
Cognitive-Behavioral Therapy for Insomnia
 Wisconsin Department of Health Services Wisconsin Public Psychiatry Network Teleconference (WPPNT) This teleconference is brought to you by the Wisconsin Department of Health Services (DHS) Bureau of Prevention,
Wisconsin Department of Health Services Wisconsin Public Psychiatry Network Teleconference (WPPNT) This teleconference is brought to you by the Wisconsin Department of Health Services (DHS) Bureau of Prevention,
You May Be at Risk. You are currently taking a sedative-hypnotic drug. Please Bring This Information With You To Your Next Medical Appointment
 You are currently taking a sedative-hypnotic drug Alprazolam Chlordiazepoxide Clonazepam Diazepam Estazolam Flurazepam Lorazepam Oxazepam Temazepam Triazolam Eszopiclone Zaleplon Zolpidem Please Bring
You are currently taking a sedative-hypnotic drug Alprazolam Chlordiazepoxide Clonazepam Diazepam Estazolam Flurazepam Lorazepam Oxazepam Temazepam Triazolam Eszopiclone Zaleplon Zolpidem Please Bring
14. Percent
 4:30 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau
4:30 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau
Faculty/Presenter Disclosure
 A Little CBT I With My Tea Please: Cognitive Behavioural Therapy for insomnia (CBT I) and Its Use In the Treatment of Sleeplessness W. Jerome Alonso, MD Medical Director, Canadian Sleep Consultants Clinical
A Little CBT I With My Tea Please: Cognitive Behavioural Therapy for insomnia (CBT I) and Its Use In the Treatment of Sleeplessness W. Jerome Alonso, MD Medical Director, Canadian Sleep Consultants Clinical
Sleep in the Patient with Diabetes
 Sleep in the Patient with Diabetes ANDREA RINN, DO SEPTEMBER, 2017 Learning Objectives 1. Recognize the correlation between sleep apnea and diabetes 2. Review potential relationships between sleep and
Sleep in the Patient with Diabetes ANDREA RINN, DO SEPTEMBER, 2017 Learning Objectives 1. Recognize the correlation between sleep apnea and diabetes 2. Review potential relationships between sleep and
Contents. Page. Can t sleep 3. Insomnia 4. Sleep 5. How long should we sleep? 8. Sleep problems 9. Getting a better night s sleep 11
 I Cannot Sleep Contents Page Can t sleep 3 Insomnia 4 Sleep 5 How long should we sleep? 8 Sleep problems 9 Getting a better night s sleep 11 Treatment for insomnia 15 For more information 19 2 Can t sleep
I Cannot Sleep Contents Page Can t sleep 3 Insomnia 4 Sleep 5 How long should we sleep? 8 Sleep problems 9 Getting a better night s sleep 11 Treatment for insomnia 15 For more information 19 2 Can t sleep
Facts about Sleep. Circadian rhythms are important in determining human sleep patterns/ sleep-waking cycle
 Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Temazepam 30 mg sleeping pills
 Temazepam 30 mg sleeping pills The sedative effects of temazepam may last longer in older adults. Accidental falls are common in elderly patients who take benzodiazepines. Use caution to avoid falling
Temazepam 30 mg sleeping pills The sedative effects of temazepam may last longer in older adults. Accidental falls are common in elderly patients who take benzodiazepines. Use caution to avoid falling
Sleep Hygiene. William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA
 Sleep Hygiene William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA Why Is Sleep Important? Symptoms of Sleep Deprivation: Irritability / Poor Stress
Sleep Hygiene William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA Why Is Sleep Important? Symptoms of Sleep Deprivation: Irritability / Poor Stress
 Sleep This factsheet is available in a downloadable PDF here. Table of Contents Introduction Insomnia How Long does Insomnia Last? How much Sleep should You get? Symptoms of Insomnia Causes of Insomnia
Sleep This factsheet is available in a downloadable PDF here. Table of Contents Introduction Insomnia How Long does Insomnia Last? How much Sleep should You get? Symptoms of Insomnia Causes of Insomnia
ADULT PRIMARY INSOMNIA
 Clinical Practice Guideline Adult Primary Insomnia: Diagnosis to Management 2007 Update This guideline was developed by a Clinical Practice Guidelines Working Group to assist physicians in the management
Clinical Practice Guideline Adult Primary Insomnia: Diagnosis to Management 2007 Update This guideline was developed by a Clinical Practice Guidelines Working Group to assist physicians in the management
Sleep and Students. John Villa, DO Medical Director
 Sleep and Students John Villa, DO Medical Director Objectives: Importance and Benefits of Sleep States and Stages of the Sleep Cycle Sleep Needs, Patterns and Characteristics for All Ages Healthy Sleep
Sleep and Students John Villa, DO Medical Director Objectives: Importance and Benefits of Sleep States and Stages of the Sleep Cycle Sleep Needs, Patterns and Characteristics for All Ages Healthy Sleep
OUTLINE SLEEP UPDATE 2011 DISCLOSURES. David Claman, MD. Formerly on Lunesta Speakers Bureau Resigned 2011
 SLEEP UPDATE 2011 David Claman, MD Professor of Medicine UCSF Sleep Disorders Center DISCLOSURES Formerly on Lunesta Speakers Bureau Resigned 2011 Former Consultant for Provent Consulting activity was
SLEEP UPDATE 2011 David Claman, MD Professor of Medicine UCSF Sleep Disorders Center DISCLOSURES Formerly on Lunesta Speakers Bureau Resigned 2011 Former Consultant for Provent Consulting activity was
Sleeping Pills and Natural Sleep Aids
 Sleeping Pills and Natural Sleep Aids Prescription and Over-the-Counter Products It s the middle of the night, and you re staring at the ceiling, thinking about work, or bills, or the kids. Sleep just
Sleeping Pills and Natural Sleep Aids Prescription and Over-the-Counter Products It s the middle of the night, and you re staring at the ceiling, thinking about work, or bills, or the kids. Sleep just
HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS. To educate participants regarding the sleep wake cycle.
 HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS Talk about the relationship between depression, sleep, and health problems. To educate participants regarding the sleep wake cycle. To provide
HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS Talk about the relationship between depression, sleep, and health problems. To educate participants regarding the sleep wake cycle. To provide
Sedative Hypnotics. Description
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.60.11 Subject: Sedative Hypnotics Page: 1 of 7 Last Review Date: December 8, 2017 Sedative Hypnotics
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.60.11 Subject: Sedative Hypnotics Page: 1 of 7 Last Review Date: December 8, 2017 Sedative Hypnotics
John McLachlan. Clinical Lead Pulmonary Physiology & Sleep Medicine. President Elect, WA Branch Thoracic Society of Australia & NZ
 John McLachlan Respiratory & Sleep Physician @FSH Clinical Lead Pulmonary Physiology & Sleep Medicine Sleep Physician x 27 years Interest in Insomnia management President Elect, WA Branch Thoracic Society
John McLachlan Respiratory & Sleep Physician @FSH Clinical Lead Pulmonary Physiology & Sleep Medicine Sleep Physician x 27 years Interest in Insomnia management President Elect, WA Branch Thoracic Society
OBJECTIVES. The psychiatric, medical, and neurologic causes of sleep problems. Office-based and objective methods of evaluating sleep
 SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
Sedative Hypnotics. Description
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.60.11 Subject: Sedative Hypnotics Page: 1 of 8 Last Review Date: September 15, 2016 Sedative Hypnotics
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.60.11 Subject: Sedative Hypnotics Page: 1 of 8 Last Review Date: September 15, 2016 Sedative Hypnotics
Anxiolytic and Hypnotic drugs
 Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
Sleep Issues for Adults with ADHD. Robert Myers, PhD Clinical Psychologist Associate Clinical Professor, Psychiatry & Human Behavior
 Sleep Issues for Adults with ADHD Robert Myers, PhD Clinical Psychologist Associate Clinical Professor, Psychiatry & Human Behavior Sleep Disorders are Prevalent in ADHD 30% in children 60% to 80% in adults
Sleep Issues for Adults with ADHD Robert Myers, PhD Clinical Psychologist Associate Clinical Professor, Psychiatry & Human Behavior Sleep Disorders are Prevalent in ADHD 30% in children 60% to 80% in adults
continuing education for pharmacists
 continuing education for pharmacists General Insomnia Disorder in Adults and Treatment Guidelines Amanda R. Kriesen, R.Ph., PharmD Volume XXXV, No. 9 Dr. Amanda Kriesen has no relevant financial relationships
continuing education for pharmacists General Insomnia Disorder in Adults and Treatment Guidelines Amanda R. Kriesen, R.Ph., PharmD Volume XXXV, No. 9 Dr. Amanda Kriesen has no relevant financial relationships
RETT SYNDROME AND SLEEP
 2015 A good night s sleep promotes learning, improved mood, general good health, and a better quality of life for both your child and the whole family. This article written for Rettsyndrome.org by Dr Daniel
2015 A good night s sleep promotes learning, improved mood, general good health, and a better quality of life for both your child and the whole family. This article written for Rettsyndrome.org by Dr Daniel
Treating sleep disorders
 Treating sleep disorders Sue Wilson Centre for Neuropsychopharmacology Imperial College London sue.wilson@imperial.ac.uk Suggested algorithm for treatment of insomnia Diagnosis of insomnia Associated with
Treating sleep disorders Sue Wilson Centre for Neuropsychopharmacology Imperial College London sue.wilson@imperial.ac.uk Suggested algorithm for treatment of insomnia Diagnosis of insomnia Associated with
Addressing Pharmacologic Issues in. DSM-5 Sleep-Wake. Insomnia. Disorders. DSM-5 Insomnia Disorder. Insomnia. Disorder
 Addressing Pharmacologic Issues in David N. Neubauer, MD Associate Professor of Psychiatry and Behavioral Sciences Johns Hopkins School of Medicine Baltimore, Maryland Restless Legs Syndrome Substance/
Addressing Pharmacologic Issues in David N. Neubauer, MD Associate Professor of Psychiatry and Behavioral Sciences Johns Hopkins School of Medicine Baltimore, Maryland Restless Legs Syndrome Substance/
Session 5. Bedtime Relaxation Techniques and Lifestyle Practices for Improving Sleep
 Session 5 Bedtime Relaxation Techniques and Lifestyle Practices for Improving Sleep Lesson 1: Relaxation Techniques at Night and Lifestyle Practices That Improve Sleep Using Relaxation Techniques to Aid
Session 5 Bedtime Relaxation Techniques and Lifestyle Practices for Improving Sleep Lesson 1: Relaxation Techniques at Night and Lifestyle Practices That Improve Sleep Using Relaxation Techniques to Aid
Sleep. Basic concepts and applications for athletes. Michael A. Grandner PhD MTR
 Sleep Basic concepts and applications for athletes Michael A. Grandner PhD MTR Director, Sleep and Health Research Program Director, Behavioral Sleep Medicine Program Assistant Professor of Psychiatry,
Sleep Basic concepts and applications for athletes Michael A. Grandner PhD MTR Director, Sleep and Health Research Program Director, Behavioral Sleep Medicine Program Assistant Professor of Psychiatry,
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Non-Benzodiazepine Insomnia Reference Number: CP.PMA_10.11.23 Effective Date: 07.16 Last Review Date: 04.18 Line of Business: Medicaid- Arizona (AHCS, CIC) Revision Log See Important Reminder
Clinical Policy: Non-Benzodiazepine Insomnia Reference Number: CP.PMA_10.11.23 Effective Date: 07.16 Last Review Date: 04.18 Line of Business: Medicaid- Arizona (AHCS, CIC) Revision Log See Important Reminder
Sedative/Hypnotic Agents. Sedative/Hypnotic Agents. Central Nervous System Depressants. Sedative/Hypnotic Agents(cont d) Sleep
 Sleep") Central Nervous System Depressants Sedative Drugs that have an inhibitory effect on the CNS to the degree that they reduce: Nervousness, excitability, irritability Without causing sleep Hypnotics Calm
Central Nervous System Depressants Sedative Drugs that have an inhibitory effect on the CNS to the degree that they reduce: Nervousness, excitability, irritability Without causing sleep Hypnotics Calm
Disclosures. Speaker: Teva, UCB, Purdue Advisory Board: Welltrinsic Sleep Network Consultant: Vapotherm, Inc. National Interpretor: Novasom
 So PAP Doesn t Work Rochelle Goldberg, MD, FAASM, FCCP Diplomat, American Board of Sleep Medicine Director Sleep Medicine Services Main Line Health Systems Lankenau Medical Center and Paoli Hospital Disclosures
So PAP Doesn t Work Rochelle Goldberg, MD, FAASM, FCCP Diplomat, American Board of Sleep Medicine Director Sleep Medicine Services Main Line Health Systems Lankenau Medical Center and Paoli Hospital Disclosures