PROPOSED REVISIONS OF ISMA BRAIN DEATH GUIDELINES
|
|
|
- Sheena Casey
- 6 years ago
- Views:
Transcription
1 RESOLUTION Introduced by: Action: PROPOSED REVISIONS OF ISMA BRAIN DEATH GUIDELINES Emil Weber, MD Adopted as Amended RESOLVED, that ISMA adopt updated brain death guidelines for adults and children, as provided by the Ad Hoc Committee to establish Brain Death Guidelines for the state of Indiana for 2017.
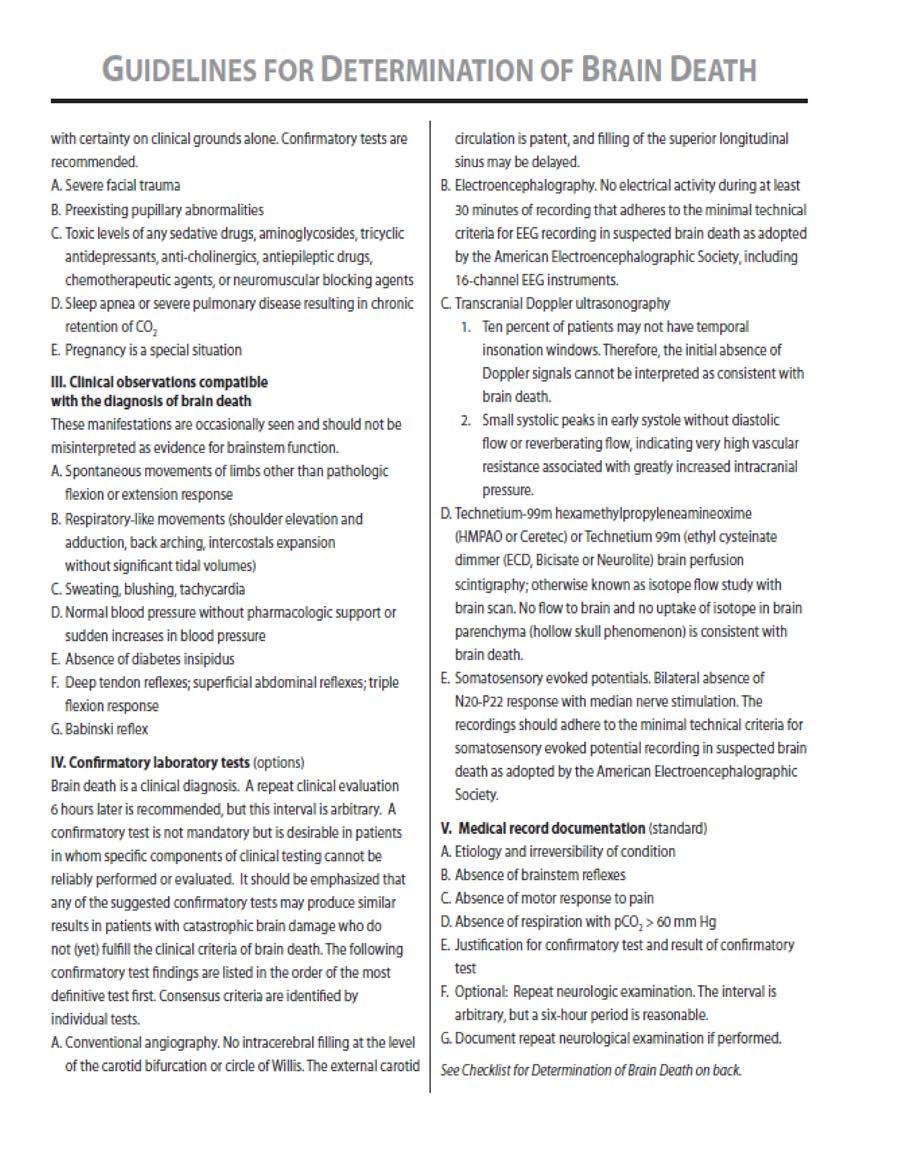
2 Proposed Revision of ISMA Adult Brain Death Guidelines of 2017 ADULT GUIDELINES FOR DETERMINATIN OF BRAIN DEATH ADULT DIAGNOSTIC CRITERIA- PATIENTS ABOVE 18 YEARS OF AGE I. Diagnostic criteria for clinical diagnosis of brain death. A. Prerequisites. Brain death is the absence of clinical brain function when the proximate cause is known and demonstrably irreversible. 1. Clinical or neuroimaging evidence of an acute CNS catastrophe that is compatible with the clinical diagnosis of brain death. 2. Exclusion of complicating medical conditions that may confound clinical assessment (no severe electrolyte, acidbase, or endocrine disturbance) 3. No drug intoxication or poisoning. 4. Core temperature > 32 0 C (90 o F). 5. In any patient who has a recorded core body temperature of 34 o C or lower, prior to or during hospitalization, a cerebral blood flow study must be performed which shows no cerebral blood flow before brain death can be declared by physical examination. A core body temperature of 36 o C or higher should be maintained for at least 24 hours prior to initiating the brain death examination. B. The three cardinal findings in brain death are coma or unresponsiveness, 3. Apnea-testing performed as follows: a) Prerequisites I. Core temperature >36 o C or 97 o F II. Systolic blood pressure> 90 mm HG III. Euvolemia. Option: positive fluid balance in the previous 6 hours IV. Normal pco2, Option: arterial pco2 > 40 mm Hg V. Normal po2. Option: preoxygenation to obtain arterial po2 > 200 mm Hg b) Connect a pulse oximeter and disconnect the ventilator. c). c) If oxygen saturation falls to 85 % or less, abort the apnea test and reconnect the respirator; otherwise, continue with apnea test. d) Look closely for respiratory movements (abdominal or chest excursions that produce adequate tidal volumes). e) Measure arterial po2, pco2 and ph after approximately 8 minutes and reconnect the ventilator. f) If respiratory movements are absent and arterial pco2is > 60 mm Hg
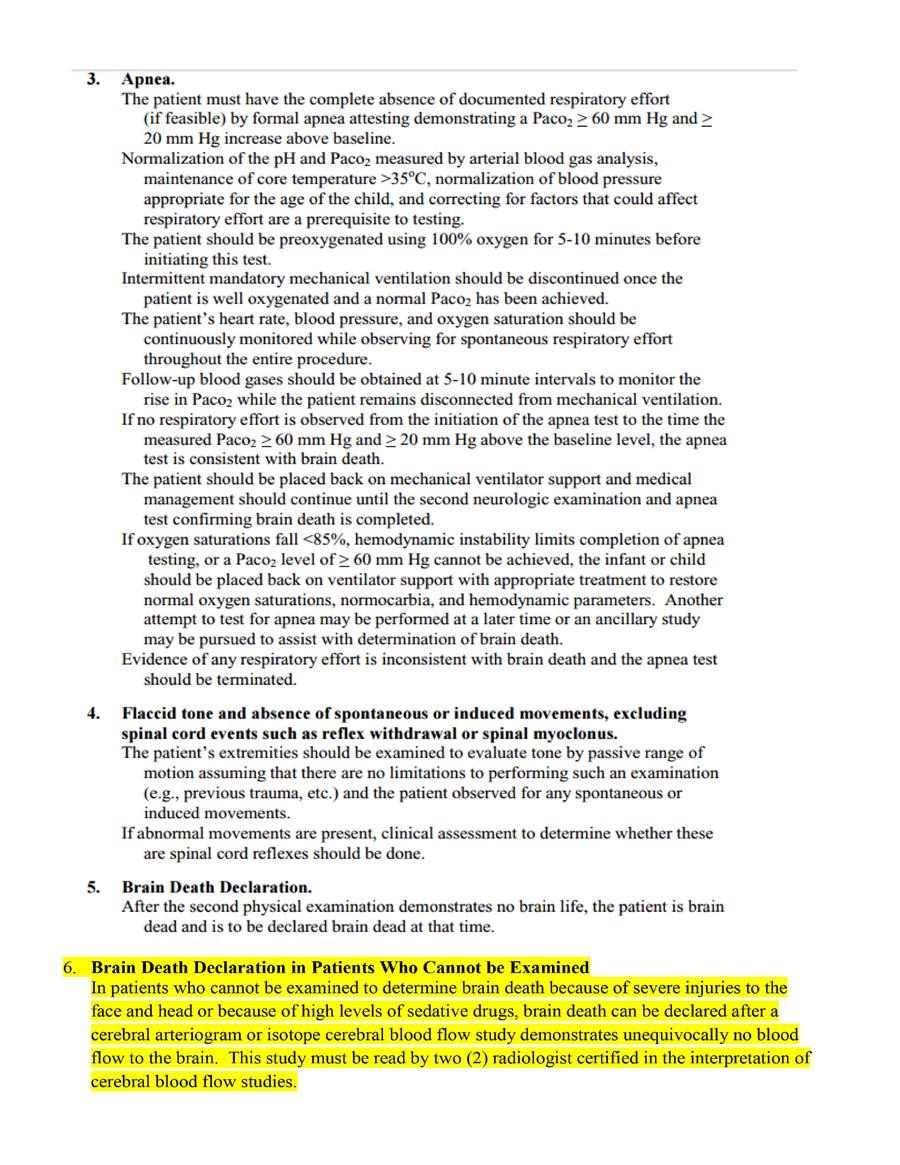
3 absence of brainstem reflexes and apnea. 1. Coma or unresponsiveness-no cerebral motor response to pain in all extremities (nail-bed pressure and supraorbital pressure). 2. Absence of brainstem reflexes a) Pupils i. No response to bright light ii. Size: midposition (4mm) to dilated (9mm). b) Ocular movement i. No oculocephalic reflex (testing only when no fracture or instability of the cervical spine is apparent) ii. No deviation of the eyes to irrigation in each ear with 50 ml of cold water (allow 1 minute after injection and at least 5 minutes between testing on each side) c) Facial sensation and facial motor response i. No corneal reflex to touch with a throat swab ii. No jaw reflex iii. No grimacing to deep pressure on nail bed, supraorbital ridge, or temporomandibular joint d) Pharyngeal and tracheal reflexes i. No response after stimulation of the posterior pharynx with tongue blade ii. No cough response to bronchial suctioning (option: 20 mm Hg increase in pco2 over a baseline normal pco2), the apnea test result is positive (i.e., it supports the diagnosis of brain death). g) If respiratory movements are observed, the apnea test result is negative (i.e., it does not support the clinical diagnosis of brain death), and the test should be repeated. h) Connect the ventilator if, during testing, the systolic blood pressure becomes < 90 mm Hg or the pulse oximeter indicates significant oxygen desaturation and cardiac arrhythmias are present; immediately draw an arterial blood sample and analyze arterial blood gas. If pco2 is > 60 mm Hg or pco2 increase is < 20 mm Hg over baseline normal pco2, the result is indeterminate, and an additional confirmatory test can be considered. C. Brain Death Declaration in Patients Who Cannot Be Examined. In patients who cannot be examined to determine brain death because of severe injuries to the face and head or because of high levels of sedative drugs, brain death can be declared after a cerebral arteriogram or isotope cerebral blood flow study demonstrates
4 unequivocally there is no blood flow to the brain. This study must be read by two (2) radiologists certified in the interpretation of cerebral blood flow studies. II. Pitfalls in the diagnosis of brain death The following conditions may interfere with the clinical diagnosis of brain death, so that the diagnosis cannot be made
5

6
7
8
9
10

11
12
13
14 The content of these Brain Death Guidelines is largely excerpted from an article published in Critical Care Medicine 2011 Vol. 39, No. 9, entitled Guidelines for the determination of brain death in infants and children; An update of the 1987 Task Force recommendations. For documentation and supportive information, including an extensive bibliography, please refer to the aforementioned publication.
GUIDELINES: The following guidelines for determining brain death in adults are accepted practice parameters of the American Academy of Neurology 1
 Page 1 of 5 PURPOSE: The purpose of this policy is to provide licensed staff and medical personnel with a guideline to determine when a patient on a ventilator demonstrates clinical brain death. POLICY
Page 1 of 5 PURPOSE: The purpose of this policy is to provide licensed staff and medical personnel with a guideline to determine when a patient on a ventilator demonstrates clinical brain death. POLICY
Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin
 Prepared by Reviewed By Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin Dr. M. Salim Khan Medical Director Approved by Dr. Manzoor H Qazi Chief Executive
Prepared by Reviewed By Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin Dr. M. Salim Khan Medical Director Approved by Dr. Manzoor H Qazi Chief Executive
Hospital of the University of Pennsylvania POLICY MANUAL
 Page 1 of 8 KEY WORDS: Brain Death Coma # 1-6-11 Procedures Following Patient Death # 1-6-13 Organ Donation and Anatomical Donation and Pennsylvania s Anatomical Gift Act #1-6-17 Withholding and Withdrawing
Page 1 of 8 KEY WORDS: Brain Death Coma # 1-6-11 Procedures Following Patient Death # 1-6-13 Organ Donation and Anatomical Donation and Pennsylvania s Anatomical Gift Act #1-6-17 Withholding and Withdrawing
DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010
 Chicago, Illinois PAGE: 1 of 7 DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010 Key Content Expert: Medical Center Ethics Committee in consultation with Chiefs of Service for Neurology
Chicago, Illinois PAGE: 1 of 7 DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010 Key Content Expert: Medical Center Ethics Committee in consultation with Chiefs of Service for Neurology
Determination of Death
 Policy Legal Standard UTMB physicians will determine death in accordance with this policy which is based on Texas law and the practice parameters recommended by the American Academy of Neurology for adults
Policy Legal Standard UTMB physicians will determine death in accordance with this policy which is based on Texas law and the practice parameters recommended by the American Academy of Neurology for adults
Brain Death Determination: Outline. Definition. Brain Death Determination. Brain Death Determination. No conflict of interest
 No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria
 Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria A. SUBJECT: Guidelines for the Determination of Death: Including Death by Neurologic Criteria B. POLICY: The Medical
Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria A. SUBJECT: Guidelines for the Determination of Death: Including Death by Neurologic Criteria B. POLICY: The Medical
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL
 YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
Neurological Determination of Death Adult
 Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
Brain Death Examination Importance and Pitfalls. Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota
 Brain Death Examination Importance and Pitfalls Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota Conflict No Conflicts to report Will not discuss off label use of any medication. Presentation
Brain Death Examination Importance and Pitfalls Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota Conflict No Conflicts to report Will not discuss off label use of any medication. Presentation
Declaring Brain Death. Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery
 Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine
 Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine") Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine 2016 MFMER 3583421-1 Brain Death or 2016 MFMER 3583421-2 Where
Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine 2016 MFMER 3583421-1 Brain Death or 2016 MFMER 3583421-2 Where
NEW YORK CITY HEALTH AND HOSPITALS CORPORATION CORPORATE BRAIN DEATH POLICY
 NEW YORK CITY HEALTH AND HOSPITALS CORPORATION CORPORATE BRAIN DEATH POLICY PURPOSE: To describe the guidelines, procedure, and documentation requirements for: Initiation of a brain death evaluation, Determination
NEW YORK CITY HEALTH AND HOSPITALS CORPORATION CORPORATE BRAIN DEATH POLICY PURPOSE: To describe the guidelines, procedure, and documentation requirements for: Initiation of a brain death evaluation, Determination
Take A Breath: Pulmonary Management of the Organ Donor. Whitni Noyes, RN, CPTC Midwest Transplant Network
 Take A Breath: Pulmonary Management of the Organ Donor Whitni Noyes, RN, CPTC Midwest Transplant Network Objectives Recognize MTN referral criteria. Be familiar with the apnea test for brain death pronouncement.
Take A Breath: Pulmonary Management of the Organ Donor Whitni Noyes, RN, CPTC Midwest Transplant Network Objectives Recognize MTN referral criteria. Be familiar with the apnea test for brain death pronouncement.
Clinical Report Guidelines for the Determination of Brain Death in Infants and Children: An Update of the 1987 Task Force Recommendations
 Guidance for the Clinician in Rendering Pediatric Care Clinical Report Guidelines for the Determination of Brain Death in Infants and Children: An Update of the 1987 Task Force Recommendations abstract
Guidance for the Clinician in Rendering Pediatric Care Clinical Report Guidelines for the Determination of Brain Death in Infants and Children: An Update of the 1987 Task Force Recommendations abstract
Policy No: Title: Determination of Death by Brain Criteria Department: PATIENT CARE. Originated: May 1992
 Title: Determination of Death by Brain Criteria Department: PATIENT CARE Policy No: Page 1 of 6 Revised: April 2009 Previous revisions: 9/96, 7/99, 7/07 Reviewed: August 2010 Originated: May 1992 I. POLICY:
Title: Determination of Death by Brain Criteria Department: PATIENT CARE Policy No: Page 1 of 6 Revised: April 2009 Previous revisions: 9/96, 7/99, 7/07 Reviewed: August 2010 Originated: May 1992 I. POLICY:
GUIDELINE for the diagnosis and confirmation of death within Adult Critical Care
 Guideline for the diagnosis and confirmation of death within adult critical care 1. Introduction Death occurs when there is permanent loss of capacity for consciousness and loss of all brainstem functions.
Guideline for the diagnosis and confirmation of death within adult critical care 1. Introduction Death occurs when there is permanent loss of capacity for consciousness and loss of all brainstem functions.
Diagnosis and Declaration of Death: A Dilemma
 Review Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/392 Diagnosis and Declaration of Death: A Dilemma Niranjan Kumar Verma 1, Ashutosh Ranjan 2, Alok Kumar Singh 3 1 Professor
Review Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/392 Diagnosis and Declaration of Death: A Dilemma Niranjan Kumar Verma 1, Ashutosh Ranjan 2, Alok Kumar Singh 3 1 Professor
Determination of Death by Brain Death Criteria in Adults Page 1 of 10. All attending physicians certified to determine brain death.
 Page 1 of 10 Scope: All attending physicians certified to determine brain death. Statutory Background Uniform Determination of Death Act (Adopted in various forms in most states including Connecticut)
Page 1 of 10 Scope: All attending physicians certified to determine brain death. Statutory Background Uniform Determination of Death Act (Adopted in various forms in most states including Connecticut)
The Determination of Brain Death. James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY
 The Determination of Brain Death James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY James.Zisfein@nychhc.org The early history of brain death Until recently, death was determined
The Determination of Brain Death James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY James.Zisfein@nychhc.org The early history of brain death Until recently, death was determined
Last printed 9/15/2016 9:51 AM. Departmental/Patient Care Page 1 of 6. Origination Date: 6/18/2014. Grady Memorial Hospital Brain Death Policy
 Last printed 9/15/2016 9:51 AM Departmental/Patient Care Page 1 of 6 Grady Memorial Hospital Brain Death Policy Origination Date: 6/18/2014 Revision Date: 2/2/2015 I. POLICY STATEMENT: Mission statement:
Last printed 9/15/2016 9:51 AM Departmental/Patient Care Page 1 of 6 Grady Memorial Hospital Brain Death Policy Origination Date: 6/18/2014 Revision Date: 2/2/2015 I. POLICY STATEMENT: Mission statement:
Brain Death and Disorders of Consciousness. John Banja, PhD Center for Ethics Emory University
 Brain Death and Disorders of Consciousness John Banja, PhD Center for Ethics Emory University jbanja@emory.edu Five kinds of catastrophic neurological injury Minimal Responsiveness Persistent Vegetative
Brain Death and Disorders of Consciousness John Banja, PhD Center for Ethics Emory University jbanja@emory.edu Five kinds of catastrophic neurological injury Minimal Responsiveness Persistent Vegetative
Examination Approach. Examination Approach. Case 1: Mental Status. The Neurological Exam In the ICU: High Yield Techniques 5/8/2015
 The Neurological Exam In the ICU: High Yield Techniques Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests and techniques S.
The Neurological Exam In the ICU: High Yield Techniques Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests and techniques S.
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY. Procedural Sedation Questions
 Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Med 536 Communicating About Prognosis Workshop. Case 2
 Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Pronouncing brain death Contemporary practice and safety of the apnea test
 Pronouncing brain death Contemporary practice and safety of the apnea test Eelco F.M. Wijdicks, MD, PhD Alejandro A. Rabinstein, MD Edward M. Manno, MD John D. Atkinson, MD Address correspondence and reprint
Pronouncing brain death Contemporary practice and safety of the apnea test Eelco F.M. Wijdicks, MD, PhD Alejandro A. Rabinstein, MD Edward M. Manno, MD John D. Atkinson, MD Address correspondence and reprint
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Experiences as a Donation Support Physician. Dead or not Dead? Are the following statements consistent with neurological
 Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
Deceased donor. Solid organ transplantation
 Deceased donor Solid organ transplantation Deceased donor donation process 1. Potential donor detection 2. Brain death diagnosis 3. Donor management 4. Organ allocation 5. Organ retrieval Brain death Irreversible
Deceased donor Solid organ transplantation Deceased donor donation process 1. Potential donor detection 2. Brain death diagnosis 3. Donor management 4. Organ allocation 5. Organ retrieval Brain death Irreversible
Module 2: Facilitator instructions for Airway & Breathing Skills Station
 Module 2: Facilitator instructions for Airway & Breathing Skills Station 1. Preparation a. Assemble equipment beforehand. b. Make sure that you have what you need and that it is functioning properly. 2.
Module 2: Facilitator instructions for Airway & Breathing Skills Station 1. Preparation a. Assemble equipment beforehand. b. Make sure that you have what you need and that it is functioning properly. 2.
First Person Consent Uniform Anatomical Gift Act of 1968
 Andrew Wilson, Medicolegal Death Investigator Not-for-profit Organ Procurement Organization (OPO) & Tissue Recovery Agency Regulated by Centers for Medicaid and Medicare Services (CMS) and FDA Offices
Andrew Wilson, Medicolegal Death Investigator Not-for-profit Organ Procurement Organization (OPO) & Tissue Recovery Agency Regulated by Centers for Medicaid and Medicare Services (CMS) and FDA Offices
Respiratory Care and Organ Donation
 Respiratory Care and Organ Donation Whitni Noyes, RN, OPTC Midwest Transplant Network Midwest Transplant Network CMS requires every accredited hospital to have an agreement with an OPO. MTN is the first
Respiratory Care and Organ Donation Whitni Noyes, RN, OPTC Midwest Transplant Network Midwest Transplant Network CMS requires every accredited hospital to have an agreement with an OPO. MTN is the first
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Ethical Dilemmas Brain Death and Overdose. Disclosures
 Ethical Dilemmas Brain Death and Overdose Ross W. Sullivan MD Director Toxicology Consultation Service Medical Toxicology Fellowship Director Assistant Professor Emergency Medicine SUNY Upstate Hospital,
Ethical Dilemmas Brain Death and Overdose Ross W. Sullivan MD Director Toxicology Consultation Service Medical Toxicology Fellowship Director Assistant Professor Emergency Medicine SUNY Upstate Hospital,
Appendix E Choose the sign or symptom that best indicates severe respiratory distress.
 Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
Legal Determination of Brain Death
 Research and Reviews Legal Determination of Brain Death JMAJ 54(6): 363 367, 2011 Yoshihiro NATORI* 1 Abstract Revisions to the Organ Transplant Act have made it possible for the organs of a brain-dead
Research and Reviews Legal Determination of Brain Death JMAJ 54(6): 363 367, 2011 Yoshihiro NATORI* 1 Abstract Revisions to the Organ Transplant Act have made it possible for the organs of a brain-dead
Sedation-Analgesia Patient Evaluation
 Getting Started A health care provider with current privileges to administer sedation-analgesia must conduct a pre-procedure evaluation, and obtain informed consent for sedation-analgesia Only patients
Getting Started A health care provider with current privileges to administer sedation-analgesia must conduct a pre-procedure evaluation, and obtain informed consent for sedation-analgesia Only patients
How to Diagnose Brainstem Death. Akhmad Imron Dept./SMF Bedah Saraf FK.Unpad/RSHS
 How to Diagnose Brainstem Death Akhmad Imron Dept./SMF Bedah Saraf FK.Unpad/RSHS RSUP Dr. Hasan Sadikin Bandung Jalan Pasteur No. 38 Bandung telephone.62-022-2034953/57 Fax.62-022-2032216 Diagnosis of
How to Diagnose Brainstem Death Akhmad Imron Dept./SMF Bedah Saraf FK.Unpad/RSHS RSUP Dr. Hasan Sadikin Bandung Jalan Pasteur No. 38 Bandung telephone.62-022-2034953/57 Fax.62-022-2032216 Diagnosis of
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Committee on Organ Donor Intervention Research
 National Academics of Science, Engineering, Medicine Committee on Organ Donor Intervention Research Galen V. Henderson, MD Director, Neurocritical Care Brigham and Women s Hospital Harvard Medical School
National Academics of Science, Engineering, Medicine Committee on Organ Donor Intervention Research Galen V. Henderson, MD Director, Neurocritical Care Brigham and Women s Hospital Harvard Medical School
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Practice variability in brain death determination A call to action
 Practice variability in brain death determination A call to action Claire N. Shappell, BA Jeffrey I. Frank, MD Khalil Husari, MD Matthew Sanchez, BS Fernando Goldenberg, MD Agnieszka Ardelt, MD, PhD Correspondence
Practice variability in brain death determination A call to action Claire N. Shappell, BA Jeffrey I. Frank, MD Khalil Husari, MD Matthew Sanchez, BS Fernando Goldenberg, MD Agnieszka Ardelt, MD, PhD Correspondence
VIDEOFLUOROSCOPIC SWALLOWING EXAM
 VIDEOFLUOROSCOPIC SWALLOWING EXAM INDENTIFYING INFORMATION May include the following: Name, ID/medical record number, date of birth, date of exam, referred by, reason for referral HISTORY/SUBJECTIVE INFORMATION
VIDEOFLUOROSCOPIC SWALLOWING EXAM INDENTIFYING INFORMATION May include the following: Name, ID/medical record number, date of birth, date of exam, referred by, reason for referral HISTORY/SUBJECTIVE INFORMATION
Unit VIII Problem 4 Physiology lab: Brain Stem Lesions
 Unit VIII Problem 4 Physiology lab: Brain Stem Lesions - Motor and sensory somatotopy: Pre-central gyrus: is the motor area. Post-central gyrus: is the sensory area. Somatotopy: there is a map of thee
Unit VIII Problem 4 Physiology lab: Brain Stem Lesions - Motor and sensory somatotopy: Pre-central gyrus: is the motor area. Post-central gyrus: is the sensory area. Somatotopy: there is a map of thee
The updated guidelines for the determination of brain
 Developing a Standard Method for Apnea Testing in the Determination of Brain Death for Patients on Venoarterial Extracorporeal Membrane Oxygenation: A Pediatric Case Series Rima J. Jarrah, MD 1 ; Samuel
Developing a Standard Method for Apnea Testing in the Determination of Brain Death for Patients on Venoarterial Extracorporeal Membrane Oxygenation: A Pediatric Case Series Rima J. Jarrah, MD 1 ; Samuel
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Airway Management From Brady s First Responder (8th Edition) 82 Questions
 82 Questions") Airway Management From Brady s First Responder (8th Edition) 82 Questions 1. What color will cyanotic skin be? p. 119 *A.) Blue B.) Red C.) Yellow D.) Green 2. Which is the primary path for air to enter
Airway Management From Brady s First Responder (8th Edition) 82 Questions 1. What color will cyanotic skin be? p. 119 *A.) Blue B.) Red C.) Yellow D.) Green 2. Which is the primary path for air to enter
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol
 Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Simulation-Based Training In Brain Death Determination
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2015 Simulation-Based Training In Brain Death Determination
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2015 Simulation-Based Training In Brain Death Determination
a central pulse located at the apex of the heart Apical pulse Apical-radial pulse a complete absence of respirations Apnea
 Afebrile absence of a fever Apical pulse a central pulse located at the apex of the heart Apical-radial pulse measurement of the apical beat and the radial pulse at the same time Apnea a complete absence
Afebrile absence of a fever Apical pulse a central pulse located at the apex of the heart Apical-radial pulse measurement of the apical beat and the radial pulse at the same time Apnea a complete absence
Ethical Challenges With Documenting Brain Death
 Ethical Challenges With Documenting Brain Death William Reitsma, BSN, CPTC Consultant AOPO Accreditation Surveyor 2015 Doug Miller Symposium Wisconsin Dells, Wisconsin When are You Dead? History of Brain
Ethical Challenges With Documenting Brain Death William Reitsma, BSN, CPTC Consultant AOPO Accreditation Surveyor 2015 Doug Miller Symposium Wisconsin Dells, Wisconsin When are You Dead? History of Brain
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions
 83 Questions") Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Bilaga 4 till rapport 1 (17)
") Bilaga 4 Tabeller, beskrivning av studier Bilaga 4 till rapport 1 (17) Bilddiagnostik vid misstanke om total hjärninfarkt en systematisk litteraturöversikt, rapport 282 (2018) SBU Statens beredning för
Bilaga 4 Tabeller, beskrivning av studier Bilaga 4 till rapport 1 (17) Bilddiagnostik vid misstanke om total hjärninfarkt en systematisk litteraturöversikt, rapport 282 (2018) SBU Statens beredning för
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Pediatric advanced life support. Management of decreased conscious level in children. Virgi ija Žili skaitė 2017
 Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Home Pulse Oximetry for Infants and Children
 Last Review Date: April 21, 2017 Number: MG.MM.DM.12aC2v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: April 21, 2017 Number: MG.MM.DM.12aC2v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
PEDIATRIC INITIAL ASSESSMENT - ALS
 PEDIATRIC INITIAL ASSESSMENT - ALS I. SCENE SIZE-UP A. Protect from body substance through isolation (glasses, gloves, gown and mask). B. Assess the scene for safety and take appropriate steps. C. Determine
PEDIATRIC INITIAL ASSESSMENT - ALS I. SCENE SIZE-UP A. Protect from body substance through isolation (glasses, gloves, gown and mask). B. Assess the scene for safety and take appropriate steps. C. Determine
Shock. Perfusion. The cardiovascular system s circulation of blood and oxygen to all the cells in different tissues and organs of the body
 Shock Chapter 10 Shock State of collapse and failure of the cardiovascular system Leads to inadequate circulation Without adequate blood flow, cells cannot get rid of metabolic wastes The result- hypoperfusion
Shock Chapter 10 Shock State of collapse and failure of the cardiovascular system Leads to inadequate circulation Without adequate blood flow, cells cannot get rid of metabolic wastes The result- hypoperfusion
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
HPR 475- Medical Aspects
 HPR 475- Medical Aspects Evidence-Based Practice Knowledge and Skills: EBP-12 EBP-13 EBP-14 Describe the types of outcomes measures for clinical practice (patient-based and clinician-based) as well as
HPR 475- Medical Aspects Evidence-Based Practice Knowledge and Skills: EBP-12 EBP-13 EBP-14 Describe the types of outcomes measures for clinical practice (patient-based and clinician-based) as well as
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Chapter 12 - Vital_Signs_and_Monitoring_Devices
 Introduction to Emergency Medical Care 1 OBJECTIVES 12.1 Define key terms introduced in this chapter. Slides 13 15, 17, 21 22, 26, 28, 30, 32 33, 35, 44, 47 48, 50, 55, 60 12.2 Identify the vital signs
Introduction to Emergency Medical Care 1 OBJECTIVES 12.1 Define key terms introduced in this chapter. Slides 13 15, 17, 21 22, 26, 28, 30, 32 33, 35, 44, 47 48, 50, 55, 60 12.2 Identify the vital signs
Medical First Responder Program Protocols
 Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
Variability of brain death determination guidelines in leading US neurologic institutions
 Variability of brain death determination guidelines in leading US neurologic institutions David M. Greer, MD, MA Panayiotis N. Varelas, MD, PhD Shamael Haque, DO, MPH Eelco F.M. Wijdicks, MD, PhD Address
Variability of brain death determination guidelines in leading US neurologic institutions David M. Greer, MD, MA Panayiotis N. Varelas, MD, PhD Shamael Haque, DO, MPH Eelco F.M. Wijdicks, MD, PhD Address
PHYSIOLOHY OF BRAIN STEM
 PHYSIOLOHY OF BRAIN STEM Learning Objectives The brain stem is the lower part of the brain. It is adjoining and structurally continuous with the spinal cord. 1 Mid Brain 2 Pons 3 Medulla Oblongata The
PHYSIOLOHY OF BRAIN STEM Learning Objectives The brain stem is the lower part of the brain. It is adjoining and structurally continuous with the spinal cord. 1 Mid Brain 2 Pons 3 Medulla Oblongata The
COMA & INTENSIVE CARE
 COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
Outline. Common causes of loss of consciousness. How to assess loss of consciousness. Emergency management of a patient with loss of consciousness.
 Outline Common causes of loss of consciousness. How to assess loss of consciousness. Emergency management of a patient with loss of consciousness. Common causes of loss of consciousness Alterations in
Outline Common causes of loss of consciousness. How to assess loss of consciousness. Emergency management of a patient with loss of consciousness. Common causes of loss of consciousness Alterations in
Neurologic Determination of Death. Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015
 Neurologic Determination of Death Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015 Format Definition of Brain Death Historical Perspectives International consistency / inconsistency
Neurologic Determination of Death Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015 Format Definition of Brain Death Historical Perspectives International consistency / inconsistency
Medicine I: Part 1: Medical Physical Examination. Kanchan Ganda, MD. Physical Examination: Detailed Discussion
 1. Kanchan Ganda, MD 2. Physical Examination: Detailed Discussion Page - 1 3. Physical Examination 4. Physical Examination (P.E): Steps Page - 2 5. General Appearance 6. Left Parotid Enlargement Page -
1. Kanchan Ganda, MD 2. Physical Examination: Detailed Discussion Page - 1 3. Physical Examination 4. Physical Examination (P.E): Steps Page - 2 5. General Appearance 6. Left Parotid Enlargement Page -
Assessment and Scoring Tools
 Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Vital Signs and SAMPLE History
 CHAPTER 9 Vital Signs and SAMPLE History Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
CHAPTER 9 Vital Signs and SAMPLE History Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
Frontline First Aid First Responder Session Quizzes
 Session 1 1. One of the 4 parts of the Patient Assessment Model is: a. Injury Survey b. Patient Survey c. Critical Survey d. Ongoing Survey 2. One of the Secondary responsibilities of the First Responder
Session 1 1. One of the 4 parts of the Patient Assessment Model is: a. Injury Survey b. Patient Survey c. Critical Survey d. Ongoing Survey 2. One of the Secondary responsibilities of the First Responder
Head Trauma Protocol
 Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
CAE Healthcare Human Patient Simulator (HPS)
") CAE Healthcare Human Patient Simulator (HPS) The Human Patient Simulator, HPS, is a tethered simulator that is capable of patient assessment and treatment including mechanical ventilation and anesthesia.
CAE Healthcare Human Patient Simulator (HPS) The Human Patient Simulator, HPS, is a tethered simulator that is capable of patient assessment and treatment including mechanical ventilation and anesthesia.
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery. By: Lillian Han
 Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: ASSESSMENT Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: ASSESSMENT Revised: 11/2013 DEFINITIONS General Impression - EMT develops a plan of action from the
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: ASSESSMENT Revised: 11/2013 DEFINITIONS General Impression - EMT develops a plan of action from the
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
CAE Healthcare istan. Neurological Features Anatomy, Physiology and Clinical signs
 CAE Healthcare istan NYSIM has two wireless istans available for your sessions. We also have them preprogrammed with the NLN Nursing These are available for you to review at the NYSIM Center. They can
CAE Healthcare istan NYSIM has two wireless istans available for your sessions. We also have them preprogrammed with the NLN Nursing These are available for you to review at the NYSIM Center. They can
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition)
") 2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
Non-Invasive Monitoring
 Grey Nuns and Misericordia Community Hospital Approved by: Non-Invasive Monitoring Neonatal Policy & Procedures Manual : Assessment : Oct 2015 Date Effective Oct 2015 Gail Cameron Senior Director Operations,
Grey Nuns and Misericordia Community Hospital Approved by: Non-Invasive Monitoring Neonatal Policy & Procedures Manual : Assessment : Oct 2015 Date Effective Oct 2015 Gail Cameron Senior Director Operations,
PHYSIOLOGY OF THE BRAIN STEM
 PHYSIOLOGY OF THE BRAIN STEM Dr Syed Shahid Habib Professor & Consultant Clinical Neurophysiology Dept. of Physiology College of Medicine & KKUH King Saud University OBJECTIVES At the end of this lecture
PHYSIOLOGY OF THE BRAIN STEM Dr Syed Shahid Habib Professor & Consultant Clinical Neurophysiology Dept. of Physiology College of Medicine & KKUH King Saud University OBJECTIVES At the end of this lecture
68W COMBAT MEDIC POCKET GUIDE
 GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: Shock Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: Shock Revised: 11/2013 DEFINITIONS Aerobic metabolism is energy using oxygen into cells. Anaerobic
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: Shock Revised: 11/2013 DEFINITIONS Aerobic metabolism is energy using oxygen into cells. Anaerobic
PRE-HOSPITAL EMERGENCY CARE COURSE.
 PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PEPP Course: PEPP BLS Pretest
 PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
FIRST AID WRITTEN EXAM. Team Name: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. a. TRUE b. FALSE
 is mandatory. a. TRUE b. FALSE") 2015 NEW IBERIA MINE RESCUE CONTEST FIRST AID WRITTEN EXAM Name: Date: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. 2. The use of accessory muscles in the chest, abdomen
2015 NEW IBERIA MINE RESCUE CONTEST FIRST AID WRITTEN EXAM Name: Date: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. 2. The use of accessory muscles in the chest, abdomen
Administrative Policies and Procedures. Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916
 Administrative Policies and Procedures Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916 Title: Sedation Cross Reference: Date Issued: 05/09 Date Reviewed: 04/11 Date: Revised:
Administrative Policies and Procedures Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916 Title: Sedation Cross Reference: Date Issued: 05/09 Date Reviewed: 04/11 Date: Revised:
Anesthesia Monitoring. D. J. McMahon rev cewood
 Anesthesia Monitoring D. J. McMahon 150114 rev cewood 2018-01-19 Key Points Anesthesia Monitoring: - Understand the difference between guidelines & standards - ASA monitoring Standard I states that an
Anesthesia Monitoring D. J. McMahon 150114 rev cewood 2018-01-19 Key Points Anesthesia Monitoring: - Understand the difference between guidelines & standards - ASA monitoring Standard I states that an
General Medical Procedure. Emergency Airway Techniques (General Airway Protocol)
") General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
Anesthesia Monitoring
 Anesthesia Monitoring Horatiu V. Vinerean, DVM, DACLAM Anesthesia Monitoring Anesthesia can be divided into four progressive phases. The signs relating to a certain phase are based upon the presence or
Anesthesia Monitoring Horatiu V. Vinerean, DVM, DACLAM Anesthesia Monitoring Anesthesia can be divided into four progressive phases. The signs relating to a certain phase are based upon the presence or
Control of Respiration
 Control of Respiration Graphics are used with permission of: adam.com (http://www.adam.com/) Benjamin Cummings Publishing Co (http://www.awl.com/bc) Page 1. Introduction The basic rhythm of breathing is
Control of Respiration Graphics are used with permission of: adam.com (http://www.adam.com/) Benjamin Cummings Publishing Co (http://www.awl.com/bc) Page 1. Introduction The basic rhythm of breathing is
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
BRAIN DEATH. Frequently Asked Questions 04for the General Public
 BRAIN DEATH Frequently Asked Questions 04for the General Public Neurocritical Care Society BRAIN DEATH FAQ s FOR THE GENERAL PUBLIC NEUROCRITICAL CARE SOCIETY 1. Q: Why was this FAQ created? A: Several
BRAIN DEATH Frequently Asked Questions 04for the General Public Neurocritical Care Society BRAIN DEATH FAQ s FOR THE GENERAL PUBLIC NEUROCRITICAL CARE SOCIETY 1. Q: Why was this FAQ created? A: Several