Pediatric obstructive sleep apnea Adenotonsillectomy and beyond (a surgeon s perspective)
|
|
|
- Katrina Malone
- 6 years ago
- Views:
Transcription


1 Pediatric obstructive sleep apnea Adenotonsillectomy and beyond (a surgeon s perspective) Tony Kille, MD Associate Professor Pediatric Otolaryngology American Family Children s Hospital Madison, WI
2 Disclosures None
3 Outline Evaluation and management of sleep-disordered breathing in routine pediatric patients Tonsillectomy & adenoidectomy outcomes Thoughts on the role of polysomnography (PSG) Evaluation and management of pediatric patients with persistent OSA after T&A
4 Basic approach OSA is state-specific obstruction (or partial obstruction) at some point (or points) of upper airway from tip of nose to trachea Find obstruction Alleviate obstruction
5 Sleep-disordered breathing A spectrum of disease (primary snoring OSA); differentiated by PSG Similar presenting signs/symptoms Most otolaryngologists treat SDB and not necessarily OSA Approx 90% of T&A without pre-op PSG Most common reason for PSG = doubt about diagnosis Reasons for not obtaining PSG = Long wait time, cost, availability (Mitchell, Laryngoscope, 2006)
6 Clinical History Patient/family history not highly predictive of abnormal PSG However, variety of questionnaires available as fairly reliable diagnostic tools Pediatric Sleep Questionnaire (PSQ) Sleep Related Breathing Disorders portion 22-item closed response questionnaire Breathing Sleep quality including daytime sleepiness Behavior/attention 85% sensitivity and 81% specificity for diagnosis of OSA 7/22 positive responses predictive of OSA (Chervin, Sleep Medicine, 2000)
7 Clinical History Snores? How long has this been a problem? Every night? Parts of nights? Associated with increased effort? Gasps or changes/pauses in breathing pattern? Mouth breathing? Restless? Wakes because of breathing abnormality? Unusual sleep positions/neck hyperextension? Daytime symptoms Bedwetting? Effect on behavior and/or QOL? Review of other ENT signs/symptoms Swallow Stridor Epistaxis Sinonasal Allergies? Other medical issues Down syndrome Neuromuscular issues (diminished tone) Craniofacial abnormalities Obesity
8 Physical Exam BMI Head & neck exam Flexible endoscopic exam (?)

")

9 Nasal Exam External deformity (projection, deviation, etc) Inferior turbinates Nasal septum Other (polyps, masses, etc)

10 Oral cavity Exam Retrognathia High arched palate/dental crowding Tonsil size Tongue-palate position
11 Flexible endoscopy? If tonsils small or absent Co-existing symptoms Stridor Nosebleeds Dysphagia Hoarseness
12 Initial decision-making Surgery (tonsillectomy & adenoidectomy) Medical management Sleep study Observation
13 Initial decision-making Surgery (tonsillectomy & adenoidectomy) Medical management Sleep study Observation What does the data say?
14 Tonsillectomy and adenoidectomy Very common ~500,000 T&A s/year in US Most are for sleep-disordered breathing Average age: 4-6 years ~90% T&A > 15 years old for chronic tonsillitis AAP guidelines: If OSA and exam consistent with adenotonsillar hypertrophy, T&A is first line therapy
15 Outcomes of T&A Effects on sleep parameters as measured by PSG Effects on quality of life Effects on behavior Effects on healthcare utilization
16 T&A for OSA 79 children with OSA studied with pre- & post-op PSG AHI improved in all children after surgery All children with pre-op AHI <10 normalized 73% with pre-op AHI >10 normalized Caregivers reported snoring at 3 months follow-up in all patients with persistent OSA (Mitchell, Laryngoscope, 2007).
17 T&A in obese children with OSA 72 subjects: 33 obese, 39 normal weight Similar mean ages (6-7) and PSG-surgery intervals More Hispanic children in obese group Significant differences (p <.001) in pre-op PSG parameters between groups: AHI: obese 23.4 ( ), normal 17.1 ( ) Apnea index: obese 6.2, normal 2.2 Hypopnea index: obese 13.5, normal 12.5 Arousal index: obese 24.8, normal 10.8 REM %: obese 12.2%, normal 20% No differences between pre-op SpO2 nadir (80%) (Mitchell and Kelly, J. Otolaryngology Head & Neck Surgery, 2007).
18 Population Pre-operative Surgery Post-operative Obese children with OSA n = 33 Normalweight children with OSA n = 39 Mild OSA 10% (n=3) Moderate OSA 20% (n=6) Severe OSA 70% (n=24) Mild OSA 5% (n=2) Moderate OSA 36% (n=14) T & A No OSA 24% (n=8) Mild OSA 46% (n=15) Moderate OSA 15% (n=5) Severe OSA 15% (n=5) T & A No OSA 72% (n=28) Mild OSA 18% (n=7) Moderate OSA 10% (n=4) Severe OSA 59% (n=23) Severe OSA 0% (n=0)
19 T&A for Quality of Life QOL of children with OSA significantly worse than those of healthy children without OSA QOL of children with OSA similar to children with asthma or juvenile rheumatoid arthritis
20 T&A for QOL 60 children with OSA completed OSA-18 QOL survey before and 3 months after T&A Changes in total scores and all domain scores significantly improved postop (Mitchell, Arch Otolaryngology Head & Neck Surgery, 2004).
 Pre-op QOL diminished for both OSA and mild SDB groups QOL improved in all domains regardless of severity of pre-op PSG (Mitchell, Otolaryngology Head & Neck")
21 T&A for QOL 61 patients with OSA & SDB tested with pre- and post-op OSA-18 QOL tool 43 with OSA (AHI range 5-46, mean = 21/hr) 18 with mild SDB (AHI range 0-4.9, mean = 3/hr) Pre-op QOL diminished for both OSA and mild SDB groups QOL improved in all domains regardless of severity of pre-op PSG (Mitchell, Otolaryngology Head & Neck Surgery, 2005).
22 OSA and Neurocognitive & Behavioral Issues

23 OSA and Neurocognitive & Behavioral Issues
24 OSA and Neurocognitive & Behavioral Issues Several studies have shown increased behavior problems in children with OSA Approx 30% with OSA score abnormal range with standard behavioral instruments Both externalizing symptoms (hyperactivity, aggression, attention) and internalizing symptoms (anxiety, depression, somatization) Several studies have shown reduced neurocognitive performance in children with OSA and primary snoring as compared with normal healthy children without OSA or PS (Blunden, Journal of Clinical & Experimental Neuropsychology, 2000). (Kennedy, Pediatric Pulmonology, 2004). (O Brien, Pediatrics, 2004).
25 T&A for Behavior 52 children (mean age 7) with OSA (mean AHI = 16.2/hr) assessed with pre- and post-op Behavior Assessment System for Children (BASC) Improvements measured after T&A in all areas regardless of sex, age, ethnicity, parental eduation, parental income, or relative severity of OSA (Mitchell & Kelly, Laryngoscope, 2005).
26 Health care utilization Children with OSA had significantly more hospital and outpatient visits and more use of antibiotics resulting in 215% elevated healthcare use compared to controls (Tarasiuk A, et al. American Journal Respiratory & Critical Care Medicine, 2007). Following T&A, total healthcare costs were reduced by 1/3 (change not seen in control or untreated group) Most of decreased cost due to reduction in upper respiratory tract infections, antibiotics (and other medications), doctor visits (Chang JJ, et al. Journal of Pediatrics, 2014).
27 T&A versus observation ChildHood AdenoTonsillectomy study (CHAT) Inclusion: (Marcus, NEJM, 2013). 5-9 year old, AHI > 2, T&A candidate Exclusion: Significant comorbidities, severe OSA, morbid obesity 460 pts with PSG-proven OSA Baseline exam, neuropsych eval, QOL survey T&A 230 Obs 230 Baseline exam, neuropsych eval, QOL survey
28 CHAT study patient selection 1244 considered T&A candidates by peds ENT; screened with PSG *** 594 (48%) had AHI>2 Mean AHI = (3%) of 594 excluded for severe OSA 460 randomized to T&A versus watchful waiting
29 T&A versus observation CHAT study PSG results After 7 months: T&A: AHI Observation: AHI normalizes (AHI < 2) over 7 months in 46% of children without T&A and in 79% with T&A In obese/overweight, normalization in 29% of observation and in 68% of T&A Predictors of OSA resolution: Low AHI Not obese Not African American
30 T&A versus observation CHAT study: cognitive, behavior, & QOL After 7 months: No significant difference in attention or executive function between T&A and observation groups Significant difference in behavior (as measured by caregivers and teachers) and quality of life 72% of patients in T&A group had both AHI normalization and symptom resolution Only 20% of patients in observation group had both AHI normalization and symptom resolution
31 CHAT summary T&A is highly effective at normalizing AHI and symptom resolution Observation is somewhat effective in normalizing AHI and poor at symptom reduction Pediatric Adenotonsillectomy Trial for Snoring (PATS) is underway for patients with AHI < 3 May be game-changer in terms of patient management and role of PSG
32 Role of PSG? PSG considered gold standard for diagnosis of OSA But Similar morbidity and benefit of treatment between primary snoring and mild OSA in terms of CV impact, quality of life, neurocognition, and behavior Using PSG results as sole metric for effectiveness of T&A may neglect other benefits that are important to patients and families PSG may not capture full breadth of disease Distinction between primary snoring and OSA is an arbitrary one defined by the test itself
33 Medical management CPAP Pro: It works! Addresses both mechanical and functional obstruction Non-specific Con: Only works if you wear it
34 Medical management OSA shown to have increased inflammatory mediators Growing literature showing some success with use of: Topical nasal steroids Montelukast Oromyofunctional therapy Rapid maxillary expansion/oral appliances Weight loss
35 Persistent OSA after T&A Long history of success The low hanging fruit for surgical management Generally favorable risk-benefit ratio Can be curative in many cases However Failure (based on abnormal post-op PSG) ranges from 10-40% Risk factors for persistent OSA after T&A: Obesity Severe pre-op OSA Down syndrome Craniofacial abnormalities Achondroplasia Neurologic issues (hypotonia, cerebral palsy, etc) Teenager Asthma/reactive airway disease (Imanguli, Laryngoscope, 2016)
36 Approach to persistent OSA after T&A Review sleep study Review symptoms Room for improvement with medical approach? Poorly controlled environmental allergies Nasal steroid & saline for significant chronic rhinitis Leukotriene receptor antagonist Is PAP an option?
37 Physical Exam General: Voice Stridor Mouth-breathing BMI Midface and mandibular hypoplasia Nasal: Structural integrity Septal deviation Mucosal edema Inferior turbinate hypertrophy Polyps/masses
38 Physical Exam Oral cavity: Tonsils Palate Tongue (size & position) Lingual tonsil (?) Posterior pharyngeal mass
39 Physical Exam Flexible fiberoptic exam Posterior nasal passage Adenoid re-growth Pharynx asymmetry, collapse, lesions Tongue base lingual tonsil, masses Larynx laryngomalacia, masses, cord mobility
40 Limitations Anatomy during office exam anatomy during sleep Patient position Pharyngeal & laryngeal tone Poor cooperation


41 State-specific examinations Use of pharmacologic agents for sedation Goal of reproducing upper airway behavior similar to natural sleep ( simulated sleep Drug-induced sleep endoscopy (DISE) Cine MRI
42 Anesthetic technique Dexmedetomidine α 2 adrenergic agonist Sedative, anxiolytic, and analgesic effects Simulates non-rem sleep well Slower onset (need 10 min loading dose) Longer half-life Less muscular relaxation More normal respiratory effort and reflexes Ketamine NMDA receptor antagonist Causes dissociative anesthesia Does not compromise respiratory drive or airway tone Potential for hallucinations, nightmares, emergence delirium as side effect Counteracts hypotension/bradycardia associated with dex Propofol Global CNS depression via GABA and NMDA receptors Fast onset Short acting Decreases genioglossus neuromuscular activity Tongue base collapse Airway obstruction oxygen desats at increased doses
43 Anesthetic technique Agents that adversely affect airway dynamics: Benzodiazepines Barbituates Opioids Inhalational agents Topical lidocaine
44 DISE technique No pre-medication No topical decongestants or topical anesthetics Mask induction; IV placed Titrate IV anesthetic to tolerate trans-nasal endoscopy, yet maintain respiratory reflexes No oral airway; avoid jaw thrust; avoid oxygen Examine all levels of airway Photo and video documentation
45 DISE what are we looking at? Nose Septal deviation Turbinate size Other Adenoid Velum Assessing anterior-posterior obstruction Lateral pharyngeal wall Tonsil size (if present) Dynamic collapse/extrinsic compression Tongue base Assess anterior-posterior obstruction Lingual tonsils Supraglottis Static or functional obstruction For each location, assess view obtained at most and least obstructed points in respiratory cycle. Evaluate sites with & without jaw thrust as well as with body position changes.
.")
46 Grading system Adenoid 0 = Absent adenoids 1 = 0-50% Obstruction of choana 2 = 50%-99% Obstruction of choana 3 = Complete obstruction of choana (Chan, et al. JAMA Otolaryngol Head Neck Surg, 2014).
 3 = Complete closure against posterior pharyngeal wall (Chan, et al.")
47 Grading system Velum 0 = No obstruction (complete view of tongue base and/or larynx) 1 = 0-50% Anterior-posterior closure (some view of tongue base/larynx) 2 = 50%-99% Anterior-posterior closure (no view of tongue base/larynx, but not against posterior pharyngeal wall) 3 = Complete closure against posterior pharyngeal wall (Chan, et al. JAMA Otolaryngol Head Neck Surg, 2014).

48 Grading system Lateral pharyngeal wall 0 = No obstruction 1 = 0-50% Lateral obstruction 2 = 50%-99% Lateral obstruction 3 = Complete obstruction (Chan, et al. JAMA Otolaryngol Head Neck Surg, 2014).
 3 = Complete obstruction (epiglottis against posterior pharyngeal wall) (Chan, et al.")
49 Grading system Tongue base 0 = No obstruction (complete view of vallecula) 1 = 0-50% Obstruction (vallecula not visible) 2 = 50%-99% Obstruction (epiglottis not contacting posterior pharyngeal wall) 3 = Complete obstruction (epiglottis against posterior pharyngeal wall) (Chan, et al. JAMA Otolaryngol Head Neck Surg, 2014).
 3 = Complete obstruction (glottic opening not seen) (Chan, et al.")
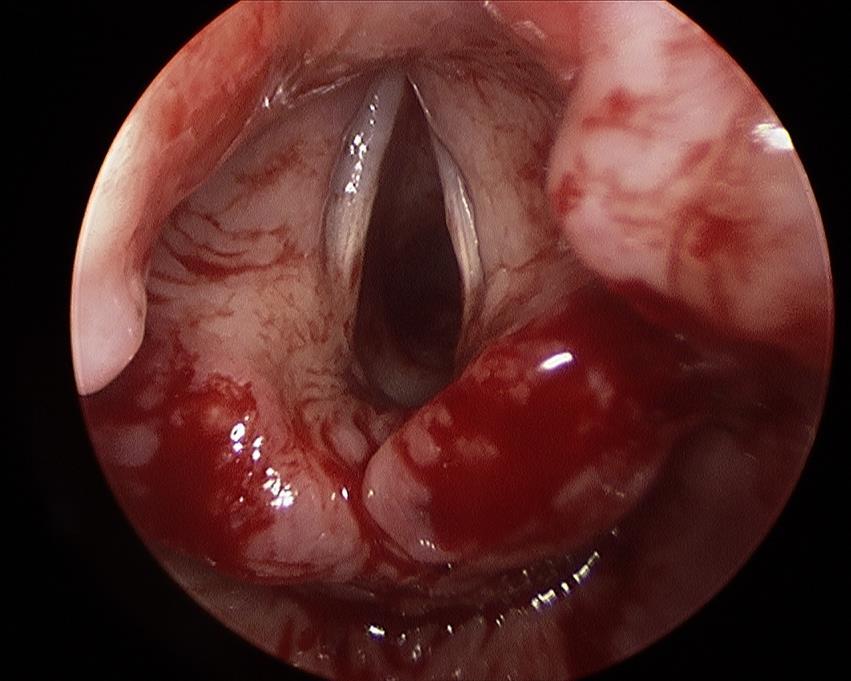
50 Grading system Supraglottis 0 = No obstruction (full view of vocal cords) 1 = 0-50% Obstruction (vocal cords partially obscured but >50% visible) 2 = 50%-99% Obstruction (>50% of vocal cords obscured) 3 = Complete obstruction (glottic opening not seen) (Chan, et al. JAMA Otolaryngol Head Neck Surg, 2014).
51 DISE outcomes DISE evaluations in children with OSA are significantly different compared to those without SDB More severe OSA is associated with more severe obstruction seen on DISE (Steinhart, Acta Otolaryngolog, 2000) More severe OSA associated with DISE showing obstruction at multiple sites; mild OSA associated with single site obstruction (Ulualp, Laryngoscope, 2013) Lots of research ongoing on this topic!
 Can see depth of tissues (e.g. lingual tonsil hypertrophy vs macroglossia/glossoptosis) Good at viewing: Oropharynx Nasopharynx Retroglossal Supraglottis Not good at viewing: Nasal passage")
52 Cine MRI 128 high resolution images over 2 minutes during snoring or oxygen desats ( cine because it looks like movie) With sedation, but less needed (no airway instrumentation) Static and dynamic images Can assess multiple levels of airway concomitantly Look at in multiple orientations (usu sagittal and axial) Can see depth of tissues (e.g. lingual tonsil hypertrophy vs macroglossia/glossoptosis) Good at viewing: Oropharynx Nasopharynx Retroglossal Supraglottis Not good at viewing: Nasal passage
53 DISE vs cine MRI Cine MRI Pro: Examine multiple levels simultaneously No airway instrumentation Can see depth of lingual tonsil and adenoid Con: Surgeon not present No positional maneuvers Poor view of nasal passage and larynx Anesthesiology comfort level DISE Pro: OR setting with anesthesiologist and surgeon working together Can proceed to directed surgery Can assess positional maneuvers Examine entire airway Con: View only one level at a time Level of sedation needed for instrumentation may exacerbate collapse (i.e. false positives)
54 Surgery beyond T&A Most studies find persistent obstruction is at level of tongue base or supraglottis Frequently, obstruction at multiple sites Numerous options: Adenoidectomy revision Inferior turbinate reduction Septoplasty Uvulopalatopharyngoplasty Lingual tonsillectomy Midline posterior glossectomy Hyoid suspension Supraglottoplasty Epiglottopexy Maxillary/mandibular distraction Upper airway neurostimulation (hypoglossal)

55 Nasal/Nasopharyngeal Revision adenoidectomy Re-growth not common, but more likely in those undergoing primary adenoidectomy age <3 and with environmental allergies Inferior turbinate reductions No peds studies on nasal surgery alone for OSA Retrospective review, 51 children age 3-12 yrs 28 T&A only, 23 T&A w/itr Statistically significant reduction in AHI and increase in nasal cross-sectional area (Cheng, Laryngoscope, 2012)
56 Palate Pillar closure at time of T&A is not helpful and increases chance of swallow/speech problems Limited peds data on UPPP




57 Tongue & tongue base Lingual tonsillectomy Relatively common site of obstruction Higher incidence in Down syndrome, obese, GERD Risk profile similar to standard (palatal) tonsillectomy Can be difficult to determine if concomitant macroglossia Systematic review of 6 studies 141 patients with lingual tonsillectomy alone Mean age: 9.7 years Mean AHI: pre-op 13.9 post-op 8.0 Success: AHI < 5: 60% AHI < 1: 20% (Manickam, Laryngoscope, 2016). (From: Kille & Lewoczko. Operative Techniques Otolaryngol, 2015)
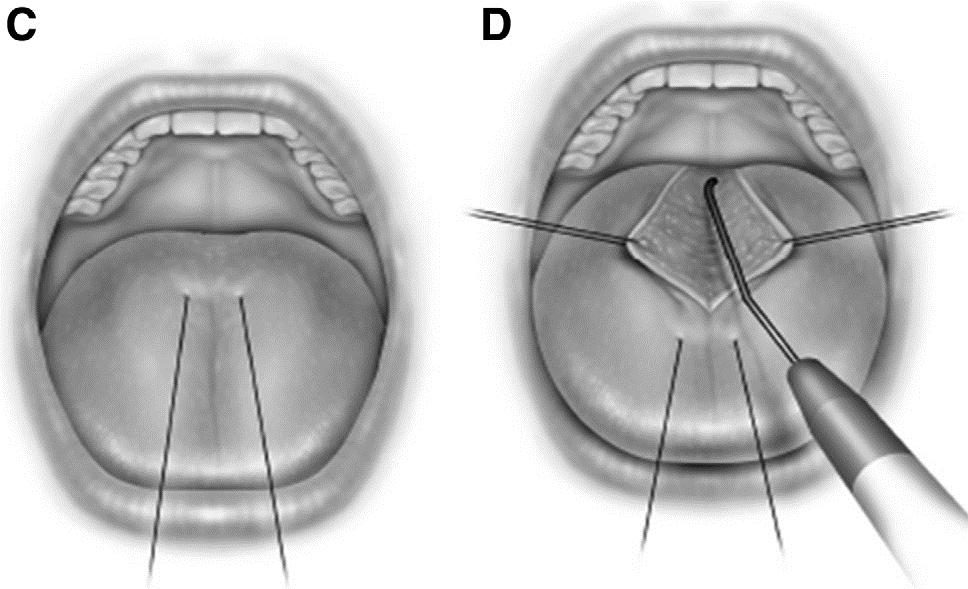
58 Midline glossectomy Tongue suspension
59 Laryngomalacia Classic/congenital Infants Inspiratory stridor Worse with feeding, agitation Treatment: Mild - Observation, reflux management, weight checks Severe (FTT or scary breathing) - supraglottoplasty
60 Laryngomalacia Sleep-variant or occult Prevalence of 3.9% among children with OSA Presents as snore, though occasionally snore described as unusual or with stridor component Arytenoid complex collapse > epiglottic collapse Approx 50% of occult laryngomalacia have neuromotor delay with hypotonia Occasionally history of congenital laryngomalacia symptoms
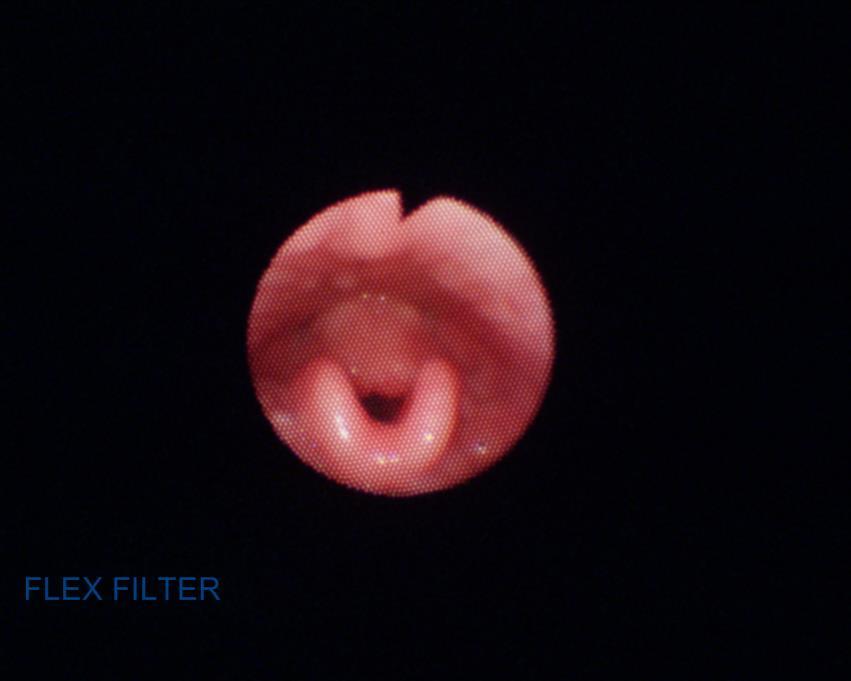
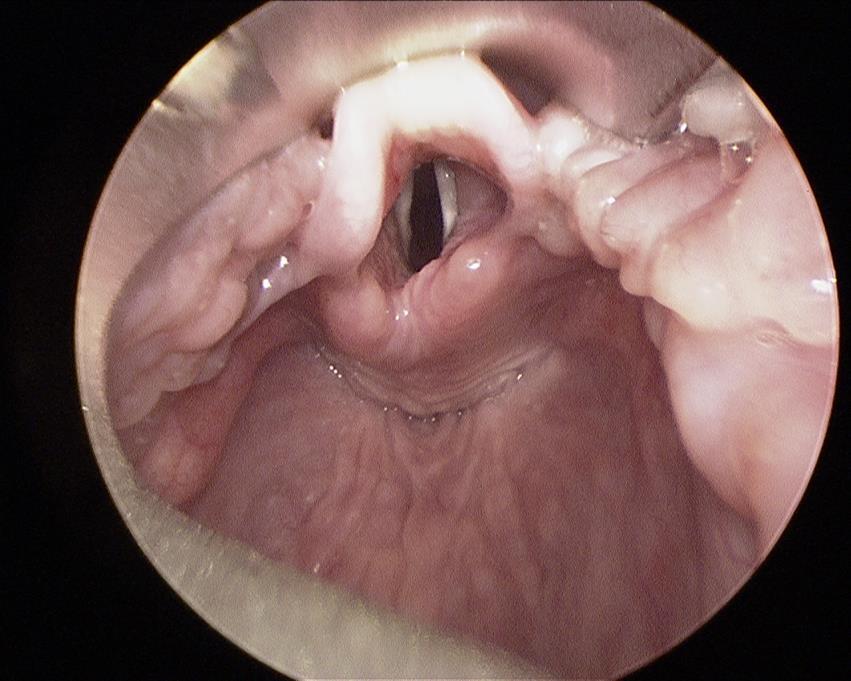
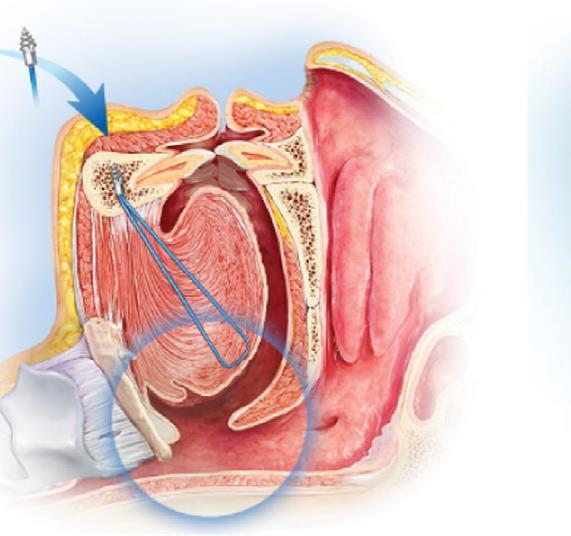
61 Supraglottoplasty
62 Supraglottoplasty outcomes for OSA Systematic review of 4 studies Total of 77 patients Mean age = 5.7 years Mean AHI: pre-op 12.1 post-op 4.4 Success: AHI < 5: 58% AHI < 1: 16% (Manickam, Laryngoscope, 2016).
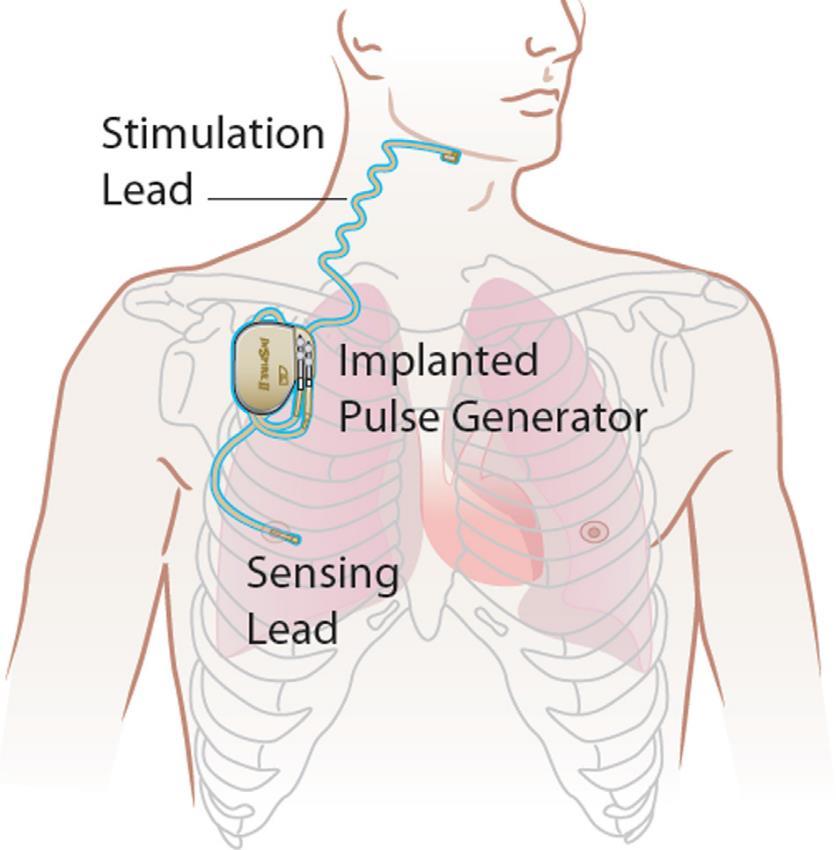
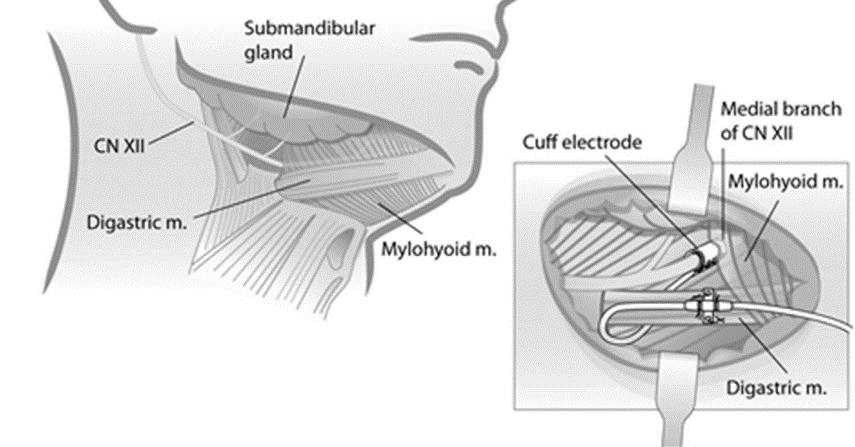
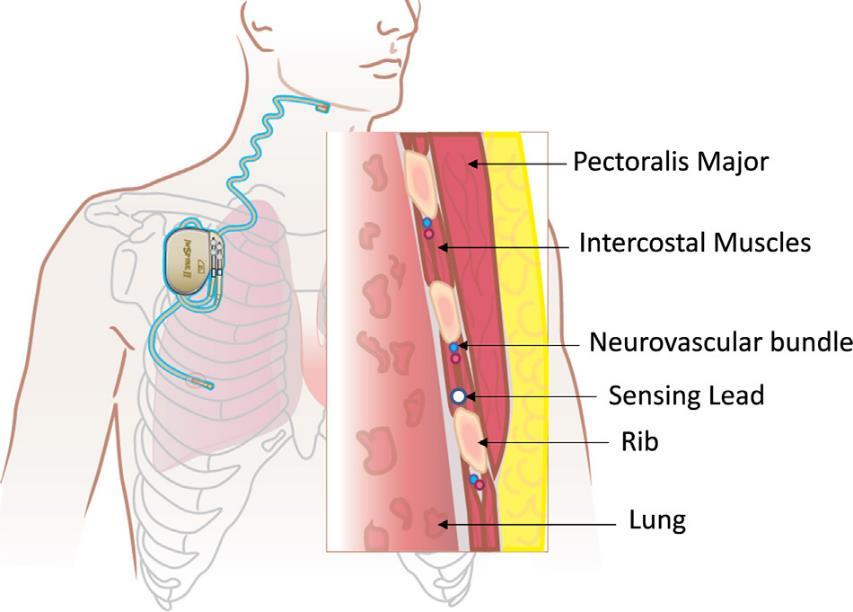
63 Hypoglossal Nerve Stimulator (Inspire)
64 Hypoglossal Nerve Stimulator (Inspire) Excellent results seen in adults thus far (STAR trial) Current multi-institutional study in peds population: Down syndrome Prior T&A Failed CPAP Age years AHI 10-65/hr BMI percentile 95% Excluded if: need MRI, active cardiac disease, swallow issues
65 Tracheostomy Highly effective Useful in children with multiple levels of obstruction or neurological impairment Increased risk profile and care requirements

66 Questions?
Pediatric Obstructive Sleep apnea An update What else is there to know?
 Pediatric Obstructive Sleep apnea An update What else is there to know? Garani S. Nadaraja, MD, FAAP Medical Director BCH-Oakland Clinical Assistant Professor Division of Pediatric Otolaryngology UCSF
Pediatric Obstructive Sleep apnea An update What else is there to know? Garani S. Nadaraja, MD, FAAP Medical Director BCH-Oakland Clinical Assistant Professor Division of Pediatric Otolaryngology UCSF
CHALLENGES IN PEDIATRIC OBSTRUCTIVE SLEEP APNEA. Amy S. Whigham, MD Assistant Professor
 CHALLENGES IN PEDIATRIC OBSTRUCTIVE SLEEP APNEA Amy S. Whigham, MD Assistant Professor Disclosures I have nothing to disclose. Outline Epidemiology Diagnosis Adenotonsillectomy Failure Treatment of Refractory
CHALLENGES IN PEDIATRIC OBSTRUCTIVE SLEEP APNEA Amy S. Whigham, MD Assistant Professor Disclosures I have nothing to disclose. Outline Epidemiology Diagnosis Adenotonsillectomy Failure Treatment of Refractory
Pediatric Airway Disorders Speaker Disclosure Outline
 Pediatric Airway Disorders G. Paul Digoy, M.D. Director of Pediatric Otolaryngology OU Health Sciences Center Paul-Digoy@ouhsc.edu Office: 405 271-5504 Speaker Disclosure Speakers, moderators, or panelists
Pediatric Airway Disorders G. Paul Digoy, M.D. Director of Pediatric Otolaryngology OU Health Sciences Center Paul-Digoy@ouhsc.edu Office: 405 271-5504 Speaker Disclosure Speakers, moderators, or panelists
11/19/2012 ก! " Varies 5-86% in men 2-57% in women. Thailand 26.4% (Neruntarut et al, Sleep Breath (2011) 15: )
 15: )") Snoring ก Respiratory sound generated in the upper airway during sleep that typically occurs during inspiration but may occur during expiration ICSD-2, 2005..... ก ก! Prevalence of snoring Varies 5-86%
Snoring ก Respiratory sound generated in the upper airway during sleep that typically occurs during inspiration but may occur during expiration ICSD-2, 2005..... ก ก! Prevalence of snoring Varies 5-86%
Persistent Obstructive Sleep Apnea After Tonsillectomy. Learning Objectives. Mary Frances Musso, DO Pediatric Otolaryngology
 Persistent Obstructive Sleep Apnea After Tonsillectomy Mary Frances Musso, DO Pediatric Otolaryngology Learning Objectives Recognize indications for tonsillectomy List patients at risk for persistent OSA
Persistent Obstructive Sleep Apnea After Tonsillectomy Mary Frances Musso, DO Pediatric Otolaryngology Learning Objectives Recognize indications for tonsillectomy List patients at risk for persistent OSA
Anesthesia Considerations for Dynamic Upper Airway Evaluation
 Anesthesia Considerations for Dynamic Upper Airway Evaluation Mohamed Mahmoud MD Associate Professor of Anesthesia & Pediatrics Cincinnati Children s Hospital Medical Center Objectives Diagnosis of Sleep
Anesthesia Considerations for Dynamic Upper Airway Evaluation Mohamed Mahmoud MD Associate Professor of Anesthesia & Pediatrics Cincinnati Children s Hospital Medical Center Objectives Diagnosis of Sleep
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Accidents. See Motor vehicle accidents. Acetazolamide, in OSA therapy, 531 Acetylcholinesterase inhibitors, in OSA therapy, 532 533 Acromegaly,
Note: Page numbers of article titles are in boldface type. A Accidents. See Motor vehicle accidents. Acetazolamide, in OSA therapy, 531 Acetylcholinesterase inhibitors, in OSA therapy, 532 533 Acromegaly,
Pediatric OSA. Pediatric OSA: Treatment Options Beyond AT. Copyright (c) 2012 Boston Children's Hospital 1
 2012 Boston Children's Hospital 1") Pediatric OSA Treatments Options Beyond AT Report of Financial Relationships (past 12 months) with commercial entities producing, marketing, re selling, or distributing health care goods or services consumed
Pediatric OSA Treatments Options Beyond AT Report of Financial Relationships (past 12 months) with commercial entities producing, marketing, re selling, or distributing health care goods or services consumed
Pediatric Sleep Disorders
 Pediatric Sleep Disorders S. SHAHZEIDI, MD, FAAP, FCCP, FAASM GRAND HEALTH INSTITUTE Objectives Discuss the importance of screening for snoring Explain the signs and symptoms of parasomnias and sleep apnea
Pediatric Sleep Disorders S. SHAHZEIDI, MD, FAAP, FCCP, FAASM GRAND HEALTH INSTITUTE Objectives Discuss the importance of screening for snoring Explain the signs and symptoms of parasomnias and sleep apnea
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea
 Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update
 OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
Obstructive Sleep Apnea- Hypopnea Syndrome and Snoring: Surgical Options
 Obstructive Sleep Apnea- Hypopnea Syndrome and Snoring: Surgical Options Joshua L. Kessler, MD, FACS Boston ENT Associates Clinical Instructor, Otology and Laryngology Harvard Medical School Why Consider
Obstructive Sleep Apnea- Hypopnea Syndrome and Snoring: Surgical Options Joshua L. Kessler, MD, FACS Boston ENT Associates Clinical Instructor, Otology and Laryngology Harvard Medical School Why Consider
Obstructive Sleep Disordered Breathing in children and Growth
 Obstructive Sleep Disordered Breathing in children and Growth Diana Marangu Kenya Paediatric Association Respiratory Symposium Wednesday, 26 th April 2017 Outline Obstructive sleep disordered breathing
Obstructive Sleep Disordered Breathing in children and Growth Diana Marangu Kenya Paediatric Association Respiratory Symposium Wednesday, 26 th April 2017 Outline Obstructive sleep disordered breathing
Sleep Disordered Breathing
 Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012
 Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
Anesthetic Risks of Obstructive Sleep Apnea in Children
 Anesthetic Risks of Obstructive Sleep Apnea in Children Dawn M. Sweeney, M.D. Associate Professor of Anesthesiology and Pediatrics University of Rochester Medical Center Risk Factors for OSA in Children
Anesthetic Risks of Obstructive Sleep Apnea in Children Dawn M. Sweeney, M.D. Associate Professor of Anesthesiology and Pediatrics University of Rochester Medical Center Risk Factors for OSA in Children
Snoring and Obstructive Sleep Apnea: Patient s Guide to Minimally Invasive Treatments Chapter 2
 Snoring and Obstructive Sleep Apnea: Patient s Guide to Minimally Invasive Treatments Chapter 2 CAUSES OF SNORING AND SLEEP APNEA We inhale air through our nose and mouth. From the nostrils, air flows
Snoring and Obstructive Sleep Apnea: Patient s Guide to Minimally Invasive Treatments Chapter 2 CAUSES OF SNORING AND SLEEP APNEA We inhale air through our nose and mouth. From the nostrils, air flows
Goal of Evaluation. Overview. Characterize disorder to guide effective treatment 1/10/2018. Disclosures
 to Identify Sites of Obstruction in Patients with OSA Eric J. Kezirian, MD, MPH Professor, Otolaryngology Head & Neck Surgery President, International Surgical Sleep Society Sleep-Doctor.com Eric.Kezirian@med.usc.edu
to Identify Sites of Obstruction in Patients with OSA Eric J. Kezirian, MD, MPH Professor, Otolaryngology Head & Neck Surgery President, International Surgical Sleep Society Sleep-Doctor.com Eric.Kezirian@med.usc.edu
4/11/2013. Objective
 Sleep nasopharyngoscopy py in children: rationale and facts Hamdy El-Hakim FRCS(Ed) FRCS(ORL) Associate Professor Pediatric Otolaryngology Division of Otolaryngology Head & Neck Surgery The Stollery Children
Sleep nasopharyngoscopy py in children: rationale and facts Hamdy El-Hakim FRCS(Ed) FRCS(ORL) Associate Professor Pediatric Otolaryngology Division of Otolaryngology Head & Neck Surgery The Stollery Children
Suchada Sritippayawan, MD Div. Pulmonology & Critical Care Dept. Pediatrics, Faculty of Medicine
 Management of pediatric OSA Suchada Sritippayawan, MD Div. Pulmonology & Critical Care Dept. Pediatrics, Faculty of Medicine Chulalongkorn University Treatment modalities Surgery Medications NIV during
Management of pediatric OSA Suchada Sritippayawan, MD Div. Pulmonology & Critical Care Dept. Pediatrics, Faculty of Medicine Chulalongkorn University Treatment modalities Surgery Medications NIV during
Roles of Surgery in OSA MASM Annual Fall Conference 2017 October 14, 2017 Kathleen Yaremchuk, MD, MSA Chair, Department of Otolaryngology/Head and
 Roles of Surgery in OSA MASM Annual Fall Conference 2017 October 14, 2017 Kathleen Yaremchuk, MD, MSA Chair, Department of Otolaryngology/Head and Neck Surgery Senior Staff Sleep Medicine Henry Ford Hospital
Roles of Surgery in OSA MASM Annual Fall Conference 2017 October 14, 2017 Kathleen Yaremchuk, MD, MSA Chair, Department of Otolaryngology/Head and Neck Surgery Senior Staff Sleep Medicine Henry Ford Hospital
Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome
 Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome Director, Sleep Laboratory Center for Pediatric Sleep Disorders Boston Children s Hospital Copyright 2014 Boston Children s Hospital
Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome Director, Sleep Laboratory Center for Pediatric Sleep Disorders Boston Children s Hospital Copyright 2014 Boston Children s Hospital
Snoring. Forty-five percent of normal adults snore at least occasionally and 25
 Snoring Insight into sleeping disorders and sleep apnea Forty-five percent of normal adults snore at least occasionally and 25 percent are habitual snorers. Problem snoring is more frequent in males and
Snoring Insight into sleeping disorders and sleep apnea Forty-five percent of normal adults snore at least occasionally and 25 percent are habitual snorers. Problem snoring is more frequent in males and
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Obstructive Sleep Apnea These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Obstructive Sleep Apnea These podcasts are designed to give medical students an overview of key topics in pediatrics.
Alexandria Workshop on
 Alexandria Workshop on 1 Snoring & OSA Surgery Course Director: Yassin Bahgat MD Claudio Vicini MD Course Board: Filippo Montevecchi MD Pietro Canzi MD Snoring & Obstructive ti Sleep Apnea The basic information
Alexandria Workshop on 1 Snoring & OSA Surgery Course Director: Yassin Bahgat MD Claudio Vicini MD Course Board: Filippo Montevecchi MD Pietro Canzi MD Snoring & Obstructive ti Sleep Apnea The basic information
Copyright (c) 2012 Boston Children's Hospital 1
 2012 Boston Children's Hospital 1") SURGICAL MANAGEMENT OF PEDIATRIC OBSTRUCTIVE SLEEP RELATED BREATHING DISORDERS Gi Soo Lee, M.D. Ed.M. Department of Otolaryngology and Communication Enhancement Boston Children s Hospital REPORT OF FINANCIAL
SURGICAL MANAGEMENT OF PEDIATRIC OBSTRUCTIVE SLEEP RELATED BREATHING DISORDERS Gi Soo Lee, M.D. Ed.M. Department of Otolaryngology and Communication Enhancement Boston Children s Hospital REPORT OF FINANCIAL
An update on childhood sleep-disordered breathing
 An update on childhood sleep-disordered breathing แพทย หญ งวนพร อน นตเสร ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร มหาว ทยาล ยสงขลานคร นทร Sleep-disordered breathing Primary snoring Upper airway resistance syndrome
An update on childhood sleep-disordered breathing แพทย หญ งวนพร อน นตเสร ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร มหาว ทยาล ยสงขลานคร นทร Sleep-disordered breathing Primary snoring Upper airway resistance syndrome
Questions: What tests are available to diagnose sleep disordered breathing? How do you calculate overall AHI vs obstructive AHI?
 Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
SURGERY FOR SNORING AND MILD OBSTRUCTIVE SLEEP APNOEA
 SURGERY FOR SNORING AND MILD OBSTRUCTIVE SLEEP APNOEA INTRODUCTION Snoring with or without excessive daytime somnolence, restless sleep and periods of apnoea are all manifestations of sleep disordered
SURGERY FOR SNORING AND MILD OBSTRUCTIVE SLEEP APNOEA INTRODUCTION Snoring with or without excessive daytime somnolence, restless sleep and periods of apnoea are all manifestations of sleep disordered
Surgical Treatment of OSA. Han-Soo Bae, MD Monroe Ear Nose and Throat Associates May 5, 2017
 Surgical Treatment of OSA Han-Soo Bae, MD Monroe Ear Nose and Throat Associates May 5, 2017 Disclosure None Treatment of OSA PAP Oral appliance Surgery OSA and Mortality Surgical Treatment of OSA Surgery
Surgical Treatment of OSA Han-Soo Bae, MD Monroe Ear Nose and Throat Associates May 5, 2017 Disclosure None Treatment of OSA PAP Oral appliance Surgery OSA and Mortality Surgical Treatment of OSA Surgery
Sleep Diordered Breathing (Part 1)
") Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Overview. Goal of Evaluation. DISE: Identifying the Sites of Obstruction in OSA. Characterize disorder to guide effective treatment.
 DISE: Identifying the Sites of Obstruction in OSA Eric J. Kezirian, MD, MPH Director, Division of Sleep Surgery Otolaryngology Head and Neck Surgery University of California, San Francisco ekezirian@ohns.ucsf.edu
DISE: Identifying the Sites of Obstruction in OSA Eric J. Kezirian, MD, MPH Director, Division of Sleep Surgery Otolaryngology Head and Neck Surgery University of California, San Francisco ekezirian@ohns.ucsf.edu
Perioperative Care in OSA Surgery
 Perioperative Care in OSA Surgery Overview Estimate of Major Peri-Op Complications Risk Factors for Airway Complications Peri-Operative Planning Avoidance of Complications Andrew N. Goldberg, MD, MSCE
Perioperative Care in OSA Surgery Overview Estimate of Major Peri-Op Complications Risk Factors for Airway Complications Peri-Operative Planning Avoidance of Complications Andrew N. Goldberg, MD, MSCE
Updated Friedman Staging System for Obstructive Sleep Apnea
 Updated Friedman Staging System for Obstructive Sleep Apnea Michael Friedman a, b Anna M. Salapatas b Lauren B. Bonzelaar c a Section of Sleep Surgery, Rush University Medical Center, and b Section of
Updated Friedman Staging System for Obstructive Sleep Apnea Michael Friedman a, b Anna M. Salapatas b Lauren B. Bonzelaar c a Section of Sleep Surgery, Rush University Medical Center, and b Section of
Review Article Sleep Endoscopy in the Evaluation of Pediatric Obstructive Sleep Apnea
 Hindawi Publishing Corporation International Journal of Pediatrics Volume 2012, Article ID 576719, 6 pages doi:10.1155/2012/576719 Review Article Sleep Endoscopy in the Evaluation of Pediatric Obstructive
Hindawi Publishing Corporation International Journal of Pediatrics Volume 2012, Article ID 576719, 6 pages doi:10.1155/2012/576719 Review Article Sleep Endoscopy in the Evaluation of Pediatric Obstructive
Evaluation, Management and Long-Term Care of OSA in Adults
 Evaluation, Management and Long-Term Care of OSA in Adults AUGUST 2015 Providing diagnostic tools and therapies that are evidence-based is a key part of a successful sleep practice. This resource outlines
Evaluation, Management and Long-Term Care of OSA in Adults AUGUST 2015 Providing diagnostic tools and therapies that are evidence-based is a key part of a successful sleep practice. This resource outlines
Abdussalam Alahmari ENT Resident R2 KAUH 15/12/2015
 Abdussalam Alahmari ENT Resident R2 KAUH 15/12/2015 Physiology of sleep Snoring mechanism, causes, sites, symptoms, and management. Sleep apnea definitions, pathophysiology, risk factors, evaluation of
Abdussalam Alahmari ENT Resident R2 KAUH 15/12/2015 Physiology of sleep Snoring mechanism, causes, sites, symptoms, and management. Sleep apnea definitions, pathophysiology, risk factors, evaluation of
PEDIATRIC OBSTRUCTIVE SLEEP
 ORIGINAL ARTICLE Drug-Induced Sleep Endoscopy in Persistent Pediatric Sleep-Disordered Breathing After Adenotonsillectomy Megan L. Durr, MD; Anna K. Meyer, MD; Eric J. Kezirian, MD, MPH; Kristina W. Rosbe,
ORIGINAL ARTICLE Drug-Induced Sleep Endoscopy in Persistent Pediatric Sleep-Disordered Breathing After Adenotonsillectomy Megan L. Durr, MD; Anna K. Meyer, MD; Eric J. Kezirian, MD, MPH; Kristina W. Rosbe,
BTS sleep Course. Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith)
") BTS sleep Course Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith) S1: Overview of OSA Definition History Prevalence Pathophysiology Causes Consequences
BTS sleep Course Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith) S1: Overview of OSA Definition History Prevalence Pathophysiology Causes Consequences
Pre-Operative Services Teaching Rounds 11 March 2011
 Pre-Operative Services Teaching Rounds 11 March 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 11 March 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
OSA in children. About this information. What is obstructive sleep apnoea (OSA)?
?") About this information This information explains all about sleep-related breathing problems in children, focusing on the condition obstructive sleep apnoea (OSA). It tells you what the risk factors are
About this information This information explains all about sleep-related breathing problems in children, focusing on the condition obstructive sleep apnoea (OSA). It tells you what the risk factors are
IEHP considers the treatment of obstructive sleep apnea (OSA) medically necessary according to the criteria outlined below:
 medically necessary according to the criteria outlined below:") : Positive Airway Pressure, Oral Appliances, and Surgical Interventions Policy: Obstructive sleep apnea (OSA) is characterized by an interruption of breathing during sleep most commonly due to extra or
: Positive Airway Pressure, Oral Appliances, and Surgical Interventions Policy: Obstructive sleep apnea (OSA) is characterized by an interruption of breathing during sleep most commonly due to extra or
Obstructive Sleep Apnea Syndrome
 SMGr up Obstructive Sleep Apnea Syndrome Alper Dilci, Handan Koyuncu and Vural Fidan* Otorhinolaryngology Department, Yunus Emre Government Hospital, Turkey *Corresponding author: Vural Fidan, Otorhinolaryngology
SMGr up Obstructive Sleep Apnea Syndrome Alper Dilci, Handan Koyuncu and Vural Fidan* Otorhinolaryngology Department, Yunus Emre Government Hospital, Turkey *Corresponding author: Vural Fidan, Otorhinolaryngology
Using Questionnaire Tools to Predict Pediatric OSA outcomes. Vidya T. Raman, MD Nationwide Children s Hospital October 201
 Using Questionnaire Tools to Predict Pediatric OSA outcomes Vidya T. Raman, MD Nationwide Children s Hospital October 201 NCH Conflict of Interest SASM $10,000 Grant NCH intramural/interdepartmental $38,000
Using Questionnaire Tools to Predict Pediatric OSA outcomes Vidya T. Raman, MD Nationwide Children s Hospital October 201 NCH Conflict of Interest SASM $10,000 Grant NCH intramural/interdepartmental $38,000
Sleep-Disordered Breathing in Children and a Critical Review of T&A. Objectives. No disclosures
 Sleep-Disordered Breathing in Children and a Critical Review of T&A No disclosures Anna Meyer, MD, FAAP Pediatric Otolaryngology Otolaryngology-Head & Neck Surgery UCSF February 2014 1 Objectives Summarize
Sleep-Disordered Breathing in Children and a Critical Review of T&A No disclosures Anna Meyer, MD, FAAP Pediatric Otolaryngology Otolaryngology-Head & Neck Surgery UCSF February 2014 1 Objectives Summarize
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Recognizing the Difficult Airway in Pediatric Patients. Nancy L. Glass, MD, MBA,
 Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Medicare C/D Medical Coverage Policy
 Medicare C/D Medical Coverage Policy Surgical Treatment of Obstructive Sleep Apnea Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January, 2019 DESCRIPTION OF PROCEDURE OR SERVICE
Medicare C/D Medical Coverage Policy Surgical Treatment of Obstructive Sleep Apnea Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January, 2019 DESCRIPTION OF PROCEDURE OR SERVICE
SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
 DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY") SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
Clinical Practice Guideline: Tonsillectomy in Children, Baugh et al Otolaryngology Head and Neck Surgery, 2011 J and: 144 (1 supplement) S1 30.
 S1 30.") Pediatric ENT Guidelines Jane Cooper, FNP, CORLN References: Clinical Practice Guideline: Tympanostomy tubes in children, Rosenfeld et al., American Academy of Otolaryngology Head and Neck Surgery Foundation
Pediatric ENT Guidelines Jane Cooper, FNP, CORLN References: Clinical Practice Guideline: Tympanostomy tubes in children, Rosenfeld et al., American Academy of Otolaryngology Head and Neck Surgery Foundation
Management of OSA. saurabh maji
 Management of OSA saurabh maji INTRODUCTION Obstructive sleep apnea is a major public health problem Prevalence of OSAS in INDIA is 2.4% to 4.96% in men and 1% to 2 % in women In the rest of the world
Management of OSA saurabh maji INTRODUCTION Obstructive sleep apnea is a major public health problem Prevalence of OSAS in INDIA is 2.4% to 4.96% in men and 1% to 2 % in women In the rest of the world
PEDIATRIC SLEEP GUIDELINES Version 1.0; Effective
 MedSolutions, Inc. Clinical Decision Support Tool Diagnostic Strategies This tool addresses common symptoms and symptom complexes. Requests for patients with atypical symptoms or clinical presentations
MedSolutions, Inc. Clinical Decision Support Tool Diagnostic Strategies This tool addresses common symptoms and symptom complexes. Requests for patients with atypical symptoms or clinical presentations
Childhood Obstructive Sleep Apnea
 Childhood Obstructive Sleep Apnea 1 PROF. RAJESHWAR DAYAL MD, FAMS,FIAP,DNB, DCH (LONDON) NATIONAL CONVENOR,IAP SLEEP PROGRAM NATIONAL VICE PRESIDENT IAP 2011 HEAD DEPARTMENT OF PAEDIATRICS S. N. MEDICAL
Childhood Obstructive Sleep Apnea 1 PROF. RAJESHWAR DAYAL MD, FAMS,FIAP,DNB, DCH (LONDON) NATIONAL CONVENOR,IAP SLEEP PROGRAM NATIONAL VICE PRESIDENT IAP 2011 HEAD DEPARTMENT OF PAEDIATRICS S. N. MEDICAL
Department of Pediatric Otolarygnology. ENT Specialty Programs
 Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Outline. Major variables contributing to airway patency/collapse. OSA- Definition
 Outline Alicia Gruber Kalamas, MD Associate Clinical Professor of Anesthesia & Perioperative Care University of California, San Francisco September 2011 Definition Pathophysiology Patient Risk Factors
Outline Alicia Gruber Kalamas, MD Associate Clinical Professor of Anesthesia & Perioperative Care University of California, San Francisco September 2011 Definition Pathophysiology Patient Risk Factors
SLEEP APNEA. Multimedia Health Education. Disclaimer
 Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of Sleep Apnea must be made in conjunction with your Physician or
Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of Sleep Apnea must be made in conjunction with your Physician or
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
5, 2002 RESIDENT PHYSICIAN: W.
 TITLE: Adult and Pediatric Obstructive Sleep Apnea SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: June 5, 2002 RESIDENT PHYSICIAN: W. Kevin Katzenmeyer, MD FACULTY PHYSICIAN: Ronald
TITLE: Adult and Pediatric Obstructive Sleep Apnea SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: June 5, 2002 RESIDENT PHYSICIAN: W. Kevin Katzenmeyer, MD FACULTY PHYSICIAN: Ronald
An Update on the Management of Pediatric Obstructive Sleep Apnea Benjamin J. Rubinstein, MD 1 Cristina M. Baldassari, MD, FAAP, FACS 1,2,*
 Curr Treat Options Peds (2015) 1:211 223 DOI 10.1007/s40746-015-0022-8 Otolaryngology (EM Arjmand and D Sidell, Section Editors) An Update on the Management of Pediatric Obstructive Sleep Apnea Benjamin
Curr Treat Options Peds (2015) 1:211 223 DOI 10.1007/s40746-015-0022-8 Otolaryngology (EM Arjmand and D Sidell, Section Editors) An Update on the Management of Pediatric Obstructive Sleep Apnea Benjamin
Polysomnography (PSG) (Sleep Studies), Sleep Center
 (Sleep Studies), Sleep Center") Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Anyone of any shape or size may snore, but there are certain features which significantly increase the chance of snoring.
 Snoring Snoring is a common sleep related problem affecting more than 20% of the population at some stage in their lives. Snoring occurs when various parts of the throat, including the soft palate, tonsils
Snoring Snoring is a common sleep related problem affecting more than 20% of the population at some stage in their lives. Snoring occurs when various parts of the throat, including the soft palate, tonsils
Upper Airway Stimulation for Obstructive Sleep Apnea
 Upper Airway Stimulation for Obstructive Sleep Apnea Background, Mechanism and Clinical Data Overview Seth Hollen RPSGT 21 May 2016 1 Conflicts of Interest Therapy Support Specialist, Inspire Medical Systems
Upper Airway Stimulation for Obstructive Sleep Apnea Background, Mechanism and Clinical Data Overview Seth Hollen RPSGT 21 May 2016 1 Conflicts of Interest Therapy Support Specialist, Inspire Medical Systems
Comparing Upper Airway Stimulation to Expansion Sphincter Pharyngoplasty: A Single University Experience
 771395AORXXX10.1177/0003489418771395Annals of Otology, Rhinology & LaryngologyHuntley et al research-article2018 Original Article Comparing Upper Airway Stimulation to Expansion Sphincter Pharyngoplasty:
771395AORXXX10.1177/0003489418771395Annals of Otology, Rhinology & LaryngologyHuntley et al research-article2018 Original Article Comparing Upper Airway Stimulation to Expansion Sphincter Pharyngoplasty:
Pediatric Considerations in the Sleep Lab
 AAST Technologist Fundamentals Date: May 7, 2017 Focus Conference Location: Orlando, Florida Workshop Pediatric Considerations in the Sleep Lab By Joel Porquez, BS, RST/RPSGT, CCSH X X X X X X Conflict
AAST Technologist Fundamentals Date: May 7, 2017 Focus Conference Location: Orlando, Florida Workshop Pediatric Considerations in the Sleep Lab By Joel Porquez, BS, RST/RPSGT, CCSH X X X X X X Conflict
Hypoglossal Nerve Stimulator Surgery for treatment of OSA. Disclosures. Hypoglossal Nerve Stimulation 11/9/2016
 Hypoglossal Nerve Stimulator Surgery for treatment of OSA olando Molina MD South Florida ENT Associates A Disclosures I do not have any relevant financial disclosures at this time. Hypoglossal Nerve Stimulation
Hypoglossal Nerve Stimulator Surgery for treatment of OSA olando Molina MD South Florida ENT Associates A Disclosures I do not have any relevant financial disclosures at this time. Hypoglossal Nerve Stimulation
Disclosures. Learning Objectives. Obstructive sleep apnea and snoring 3/19/2014. None
 Obstructive sleep apnea and snoring Ashutosh Kacker, MD, FACS Professor of Clinical Otolaryngology Department of Otorhinolaryngology Weill Medical College of Cornell University New York Presbyterian Hospital
Obstructive sleep apnea and snoring Ashutosh Kacker, MD, FACS Professor of Clinical Otolaryngology Department of Otorhinolaryngology Weill Medical College of Cornell University New York Presbyterian Hospital
Unilateral Supraglottoplasty for Severe Laryngomalacia in Children. Nasser A Fageeh, MD, FRCSC, FACS*
 Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA)
") PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
Home Video to Assess the Snoring Child
 Home Video to Assess the Snoring Child Federico Murillo-González Consider the following case: a 5 year-old child who snores and constantly wakesup every night, breathes through the mouth during the day,
Home Video to Assess the Snoring Child Federico Murillo-González Consider the following case: a 5 year-old child who snores and constantly wakesup every night, breathes through the mouth during the day,
Sleep-disordered breathing (SDB) is a relatively common
 is a relatively common") The effect of tonsillectomy and adenoidectomy on inattention and impulsivity as measured by the Test of Variables of Attention (TOVA) in children with obstructive sleep apnea syndrome GALIT AVIOR, MD,
The effect of tonsillectomy and adenoidectomy on inattention and impulsivity as measured by the Test of Variables of Attention (TOVA) in children with obstructive sleep apnea syndrome GALIT AVIOR, MD,
DOWNLOAD OR READ : TREATMENT FOR SNORING PROBLEMS PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : TREATMENT FOR SNORING PROBLEMS PDF EBOOK EPUB MOBI Page 1 Page 2 treatment for snoring problems treatment for snoring problems pdf treatment for snoring problems problem, presenting
DOWNLOAD OR READ : TREATMENT FOR SNORING PROBLEMS PDF EBOOK EPUB MOBI Page 1 Page 2 treatment for snoring problems treatment for snoring problems pdf treatment for snoring problems problem, presenting
Sleep Apnea. Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa
 Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
The Ear, Nose and Throat in MPS
 The Ear, Nose and Throat in MPS Annerose Keilmann Voice Care Center Bad Rappenau, Germany Preciptorship program on MPS Wiesbaden, November 2 nd 2015 Alterations of the outer and middle ear in MPS I narrowing
The Ear, Nose and Throat in MPS Annerose Keilmann Voice Care Center Bad Rappenau, Germany Preciptorship program on MPS Wiesbaden, November 2 nd 2015 Alterations of the outer and middle ear in MPS I narrowing
THE PATIENT STRONGLY MOTIVATED TOWARDS THE TREATMENT? & ENT
 SNORING & OSAHS SURGERY International Workshop Preoperative Diagnostic Protocol < 15 min Filippo Montevecchi M.D. Department of Special Surgery Head & Neck Surgery, Oral Surgery Unit (Head: C.Vicini) G.B.
SNORING & OSAHS SURGERY International Workshop Preoperative Diagnostic Protocol < 15 min Filippo Montevecchi M.D. Department of Special Surgery Head & Neck Surgery, Oral Surgery Unit (Head: C.Vicini) G.B.
Learning Objectives. And it s getting worse. The Big Picture. Dr. Roger Roubal
 Learning Objectives How to screen for sleep apnea; questions to ask your patients Industry treatment guidelines; when to consider an oral appliance vs. a CPAP What goals/thresholds to set for successful
Learning Objectives How to screen for sleep apnea; questions to ask your patients Industry treatment guidelines; when to consider an oral appliance vs. a CPAP What goals/thresholds to set for successful
National Sleep Disorders Research Plan
 Research Plan Home Foreword Preface Introduction Executive Summary Contents Contact Us National Sleep Disorders Research Plan Return to Table of Contents SECTION 5 - SLEEP DISORDERS SLEEP-DISORDERED BREATHING
Research Plan Home Foreword Preface Introduction Executive Summary Contents Contact Us National Sleep Disorders Research Plan Return to Table of Contents SECTION 5 - SLEEP DISORDERS SLEEP-DISORDERED BREATHING
Proposed GLOSSARY: Different sedative agents: Midazolam (M); Propofol (P) Different degrees of sedation (Minimal, Moderate, Deep) Proposal:
; Propofol (P) Different degrees of sedation (Minimal, Moderate, Deep) Proposal:") SNORING & OSAHS SURGERY International Workshop Sleep Endoscopy > 15 min Filippo Montevecchi M.D. Department of Special Surgery Head & Neck Surgery, Oral Surgery Unit (Head: C.Vicini) G.B. Morgagni L.Pierantoni
SNORING & OSAHS SURGERY International Workshop Sleep Endoscopy > 15 min Filippo Montevecchi M.D. Department of Special Surgery Head & Neck Surgery, Oral Surgery Unit (Head: C.Vicini) G.B. Morgagni L.Pierantoni
Research Article Drug-Induced Sleep Endoscopy Changes the Treatment Concept in Patients with Obstructive Sleep Apnoea
 BioMed Research International Volume 2016, Article ID 6583216, 5 pages http://dx.doi.org/10.1155/2016/6583216 Research Article Drug-Induced Sleep Endoscopy Changes the Treatment Concept in Patients with
BioMed Research International Volume 2016, Article ID 6583216, 5 pages http://dx.doi.org/10.1155/2016/6583216 Research Article Drug-Induced Sleep Endoscopy Changes the Treatment Concept in Patients with
NASAL CONTINUOUS POSITIVE AIRWAY PRESSURE FOR OBSTRUCTIVE SLEEP APNEA IN CHILDREN. Dr. Nguyễn Quỳnh Anh Department of Respiration 1
 1 NASAL CONTINUOUS POSITIVE AIRWAY PRESSURE FOR OBSTRUCTIVE SLEEP APNEA IN CHILDREN Dr. Nguyễn Quỳnh Anh Department of Respiration 1 CONTENTS 2 1. Preface 2. Definition 3. Etiology 4. Symptoms 5. Complications
1 NASAL CONTINUOUS POSITIVE AIRWAY PRESSURE FOR OBSTRUCTIVE SLEEP APNEA IN CHILDREN Dr. Nguyễn Quỳnh Anh Department of Respiration 1 CONTENTS 2 1. Preface 2. Definition 3. Etiology 4. Symptoms 5. Complications
Anna & John J. Sie Center for Down Syndrome Affiliates
 Anna & John J. Sie Center for Down Syndrome Affiliates Types of Medical Research Bench or basic research: done in a controlled laboratory setting using nonhuman subjects Clinical research: answer questions
Anna & John J. Sie Center for Down Syndrome Affiliates Types of Medical Research Bench or basic research: done in a controlled laboratory setting using nonhuman subjects Clinical research: answer questions
Upper Airway Muscle Stimulation for Obstructive Sleep Apnea
 Upper Airway Muscle Stimulation for Obstructive Sleep Apnea M. Safwan Badr, MD, MBA Chair, Department of Medicine, Wayne State University School of Medicine. Staff Physician, John D. Dingell VA Medical
Upper Airway Muscle Stimulation for Obstructive Sleep Apnea M. Safwan Badr, MD, MBA Chair, Department of Medicine, Wayne State University School of Medicine. Staff Physician, John D. Dingell VA Medical
Association of Palatine Tonsil Size and Obstructive Sleep Apnea in Adults
 The Laryngoscope VC 2017 The American Laryngological, Rhinological and Otological Society, Inc. Association of Palatine Tonsil Size and Obstructive Sleep Apnea in Adults Sebastian M. Jara, MD ; Edward
The Laryngoscope VC 2017 The American Laryngological, Rhinological and Otological Society, Inc. Association of Palatine Tonsil Size and Obstructive Sleep Apnea in Adults Sebastian M. Jara, MD ; Edward
Nasal Evaluation & Non-surgical Nasal Therapy in SDB
 Nasal Evaluation & Non-surgical Nasal Therapy in SDB Edward M. Weaver, MD, MPH Seattle VA Medical Center University of Washington Harborview Medical Center Acknowledgments This material is the result of
Nasal Evaluation & Non-surgical Nasal Therapy in SDB Edward M. Weaver, MD, MPH Seattle VA Medical Center University of Washington Harborview Medical Center Acknowledgments This material is the result of
Brian Palmer, D.D.S, Kansas City, Missouri, USA. April, 2001
 Brian Palmer, D.D.S, Kansas City, Missouri, USA A1 April, 2001 Disclaimer The information in this presentation is for basic information only and is not to be construed as a diagnosis or treatment for any
Brian Palmer, D.D.S, Kansas City, Missouri, USA A1 April, 2001 Disclaimer The information in this presentation is for basic information only and is not to be construed as a diagnosis or treatment for any
New Guidelines for Tonsillectomy Daniel C. Chelius, Jr., MD Pediatric Otolaryngolo Pediatric Otolary gy--head Head and Neck S and Neck u S rgery
 New Guidelines for Tonsillectomy Daniel C. Chelius, Jr., MD Pediatric Otolaryngology-Head and Neck Surgery November 16, 2011 EXIT Procedures Sinus surgery/skull base surgery Head and Neck Cancers Thyroid/Parathyroid
New Guidelines for Tonsillectomy Daniel C. Chelius, Jr., MD Pediatric Otolaryngology-Head and Neck Surgery November 16, 2011 EXIT Procedures Sinus surgery/skull base surgery Head and Neck Cancers Thyroid/Parathyroid
Obstructive sleep apnea Is it time for personalized medicine?
 Obstructive sleep apnea Is it time for personalized medicine? CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep
Obstructive sleep apnea Is it time for personalized medicine? CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep
Nasal Mass Presenting as Obstructive Sleep Apnea Syndrome
 ORIGINAL ARTICLE pissn 2093-9175 / eissn 2233-8853 http://dx.doi.org/10.17241/smr.2015.6.2.54 Nasal Mass Presenting as Obstructive Sleep Apnea Syndrome Seung Hoon Lee, MD, PhD, In Sik Song, MD, Jae Woo
ORIGINAL ARTICLE pissn 2093-9175 / eissn 2233-8853 http://dx.doi.org/10.17241/smr.2015.6.2.54 Nasal Mass Presenting as Obstructive Sleep Apnea Syndrome Seung Hoon Lee, MD, PhD, In Sik Song, MD, Jae Woo
Complications of Sleep-Disordered Breathing
 Complications of Sleep-Disordered Breathing Similarities between Pediatrics and Adults CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center
Complications of Sleep-Disordered Breathing Similarities between Pediatrics and Adults CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center
Emerging Nursing Roles in Collaborative Management of Sleep Disordered Breathing and Obstructive Sleep Apnoea
 Emerging Nursing Roles in Collaborative Management of Sleep Disordered Breathing and Obstructive Sleep Apnoea Sigma Theta Tau International 28th International Nursing Research Congress 27-31 July 2017
Emerging Nursing Roles in Collaborative Management of Sleep Disordered Breathing and Obstructive Sleep Apnoea Sigma Theta Tau International 28th International Nursing Research Congress 27-31 July 2017
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update
 OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosres: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosres: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
(1) TONSILS & ADENOIDS
 TONSILS & ADENOIDS") (1) TONSILS & ADENOIDS (2) Your child has been referred to have his tonsils and adenoids removed. This operation is commonly called an adenotonsillectomy and is one of the most common major operations
(1) TONSILS & ADENOIDS (2) Your child has been referred to have his tonsils and adenoids removed. This operation is commonly called an adenotonsillectomy and is one of the most common major operations
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 23 Caring for Clients with Upper Respiratory Disorders Rhinitis Inflammation of Nasal Cavities Types
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 23 Caring for Clients with Upper Respiratory Disorders Rhinitis Inflammation of Nasal Cavities Types
Ped e iat a r t i r c c S lee e p e A p A nea e a Surg r er e y
 Airway Imaging in Pediatric OSA Kasey Li, MD, DDS, FACS Stanford University Sleep Medicine Program The airway is smaller in children with OSA compared to controls The adenoid and tonsils are larger and
Airway Imaging in Pediatric OSA Kasey Li, MD, DDS, FACS Stanford University Sleep Medicine Program The airway is smaller in children with OSA compared to controls The adenoid and tonsils are larger and
in China Shanghai Office Beijing Office (+86) (+86)
 (+86)") SLEEP Apnea in China Guide 2018-2019 Shanghai Office (+86) 21 2426 6400 Beijing Office (+86) 010 6464 0611 www.pacificprime.cn Follow us on WeChat t A comprehensive overview of sleep apnea Perhaps you
SLEEP Apnea in China Guide 2018-2019 Shanghai Office (+86) 21 2426 6400 Beijing Office (+86) 010 6464 0611 www.pacificprime.cn Follow us on WeChat t A comprehensive overview of sleep apnea Perhaps you
JMSCR Vol 05 Issue 01 Page January 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i1.161 Risk of Failure of Adenotonsillectomy
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i1.161 Risk of Failure of Adenotonsillectomy
Children s Hospital of Pittsburgh Continuity Clinic Curriculum Week of November 7, Stacey Cook, MD, PhD
 Children s Hospital of Pittsburgh Continuity Clinic Curriculum Week of November 7, 2016 Stacey Cook, MD, PhD Topic: Sleep disorders: Obstructive Sleep Apnea Syndrome (OSAS) Learning Objectives: After completing
Children s Hospital of Pittsburgh Continuity Clinic Curriculum Week of November 7, 2016 Stacey Cook, MD, PhD Topic: Sleep disorders: Obstructive Sleep Apnea Syndrome (OSAS) Learning Objectives: After completing
Obstructive sleep apnea (OSA) is a common disorder
 is a common disorder") Original Research Sleep Medicine and Surgery Drug-Induced Sedation Endoscopy in the Evaluation of OSA Patients with Incomplete Oral Appliance Therapy Response Otolaryngology Head and Neck Surgery 2015,
Original Research Sleep Medicine and Surgery Drug-Induced Sedation Endoscopy in the Evaluation of OSA Patients with Incomplete Oral Appliance Therapy Response Otolaryngology Head and Neck Surgery 2015,