Resonance Disorders and Velopharyngeal Dysfunction: Evaluation and Treatment
|
|
|
- Oswin Dickerson
- 6 years ago
- Views:
Transcription
1 Resonance Disorders and Velopharyngeal Dysfunction: Evaluation and Treatment Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center
2 Resonance Disorders and Velopharyngeal Dysfunction Normal resonance Normal velopharyngeal function Velopharyngeal dysfunction (VPD) Velopharyngeal insufficiency (VPI) Velopharyngeal incompetence (VPI) Abnormal resonance Effects of cleft palate and VPI on speech/resonance Velopharyngeal mislearning
3 Evaluation and Treatment Evaluation Perceptual evaluation Intra-oral evaluation Treatment Surgical procedures Prosthetic devices Speech therapy Referrals

4 NORMAL RESONANCE
5 What is resonance for speech? Modification of the sound that is generated from the vocal cords Provides the quality of perceived sound during speech
6 What determines resonance for speech? Size and shape of the resonating cavities pharyngeal cavity oral cavity nasal cavity Function of the velopharyngeal valve
7 Size and Shape of Cavities Resonance is affected by the following: Length and volume of pharynx Size and shape of oral cavity Configuration of nasal cavity
8 Science Experiment
9 Science Experiment
10 Size and Shape of Cavities Shorter/smaller cavities: enhance higher formants Longer/larger cavities: enhance lower formants
11 Size and Shape of Cavities Differences between children and adults men and women tall people and short people Makes voice quality unique to individual
")
12 Resonance and Vowels Vowels are resonance sounds They are produced by changing the size and shape of the oral (resonating) cavity
13 NORMAL VELOPHARYNGEAL FUNCTION
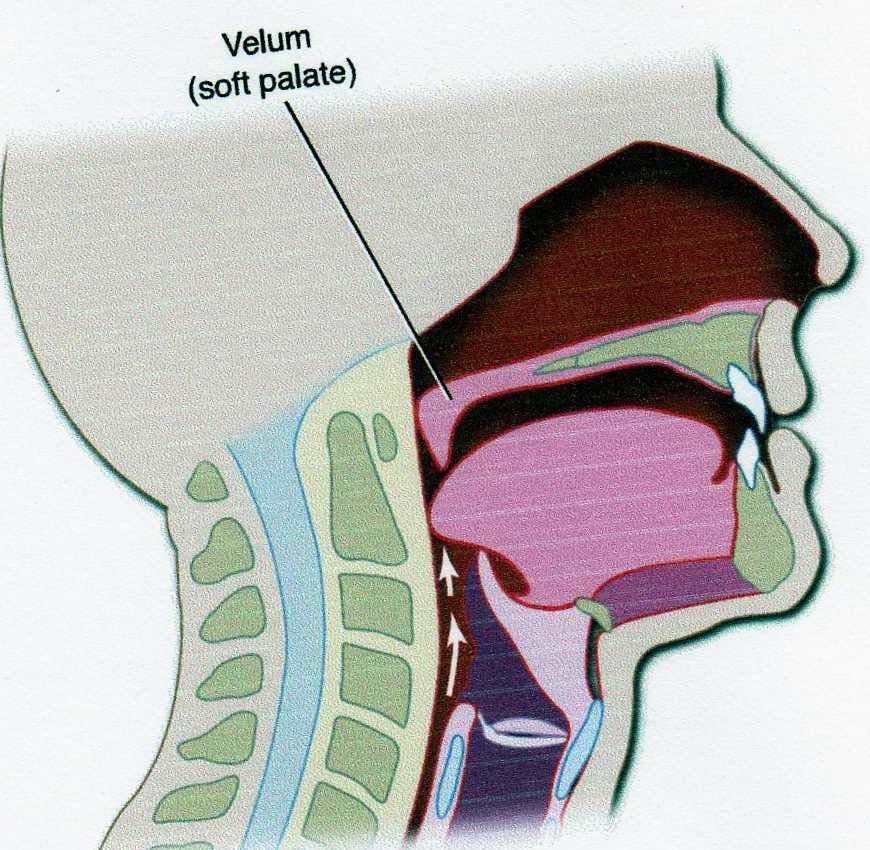
14 Structures Active in VP Closure Velum (Soft Palate) Lateral Pharyngeal Walls (LPWs) Posterior Pharyngeal Wall (PPW)
15 Velum: Rest
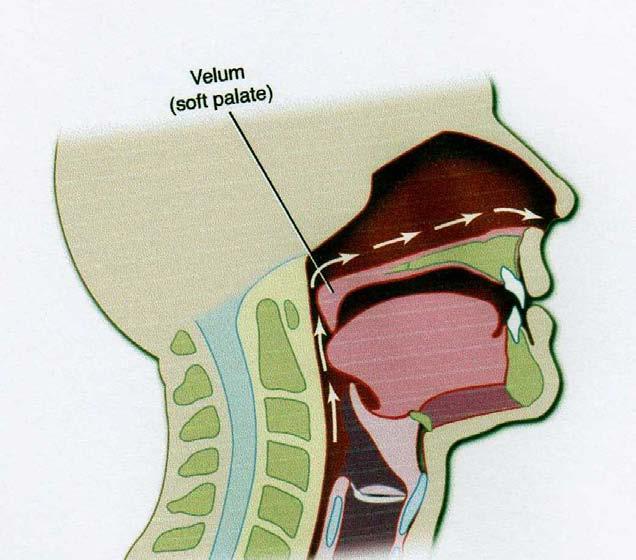
16 Velum (Soft Palate) Moves in a superior and posterior direction Has a type of knee action Moves toward the posterior pharyngeal wall
17 Velum: During Speech

18 Physics and Flow Water (and air) flow in a forward direction until something stops it An obstructing object will redirect the flow
19 Velopharyngeal Valve and Flow Due to the physics of airflow, even a small opening will be symptomatic for speech.
20 Lateral Pharyngeal Walls (LPWs) Move medially to close against the velum or in some cases, behind the velum
21 Posterior Pharyngeal Wall (PPW) Moves anteriorly toward the velum In some speakers, there s a bulge called a Passavant s ridge


22 Passavant s Ridge
23 VP Valve during Speech Velopharyngeal valve is closed for oral sounds Most consonants (air pressure sounds) All vowels (resonance sounds) Velopharyngeal valve is open for nasal sounds (m, n, ng)

24 Purpose of VP Valve Directs transmission of sound energy and air flow in the oral and nasal cavities during speech
25 Video: Normal VP Closure (Videofluoroscopy)
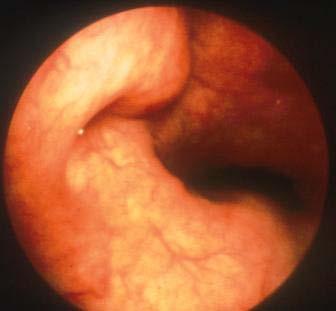
26 Normal VP Closure (Nasopharyngoscopy)
27 Video: Normal VP Closure (Nasopharyngoscopy)
28 Variations in VP Closure Non-Pneumatic: gagging, vomiting, swallowing Pneumatic: blowing, whistling, speech (+ pressure) sucking, kissing (- pressure)
29 Normal Velopharyngeal Function Learning (Articulation) Anatomy (Structure) Physiology (Movement)
30 VELOPHARYNGEAL DYSFUNCTION Articulation/Speech Learning (Velopharyngeal Mislearning) Anatomy (Velopharyngeal Insufficiency) Physiology (Velopharyngeal Incompetence)
31 VPI: Velopharyngeal Insufficiency and Incompetence
32 Velopharyngeal Insufficiency (VPI)

33 Video: VP Insufficiency

34 Video: VP Insufficiency
35 Causes of VP Insufficiency History of cleft palate or submucous cleft Deep pharynx Irregular adenoids Enlarged tonsils

36 History of Cleft Palate Velum may be too short or may be irregular following repair

37 Submucous Cleft Nasal Surface
")
38 Deep Pharynx Can be due to cranial base or cervical spine anomalies (i.e., Klippel-Feil syndrome or craniosynostosis)
39 Adenoids Positioned in usual site of VP contact Closure is velo-adenoidal in kids Normal VP closure requires a tight seal


40 Irregular Adenoids Adenoid irregularity (marked indentation or protrusion) prevents a tight seal Can cause small gap and nasal emission
41 Video: Irregular Adenoids


42 Enlarged Tonsils Can extend into pharynx, interfering with LPW and velar movement or preventing a tight VP seal
43 VP Insufficiency Following Surgery or Treatment Adenoidectomy Maxillary advancement Treatment of nasopharyngeal tumors
44 Adenoidectomy Sudden increase in the nasopharyngeal dimension can cause VPI Often temporary and resolves within 6 weeks Permanent VPI is a risk, especially with history of cleft or submucous cleft
45 VPI Post Adenoidectomy Caused by a change in the structure Speech therapy CANNOT change structure Exercises don t work because the problem is not the muscles Surgical correction is indicated
46 Velopharyngeal Incompetence (VPI)
47 Video: VP Incompetence (Note hypernasality)
48 Causes of VP Incompetence Velopharyngeal hypotonia, paralysis or paresis Neurological injury (i.e.,tbi) or dysfunction (i.e., neuromuscular disorders) Occurs as a characteristic of dysarthria Velopharyngeal incoordination can occur with apraxia of speech
49 Video: Dysarthria
50 Video: Apraxia
51 Abnormal Resonance Hypernasality Hyponasality (denasality) Cul de sac resonance Mixed resonance
52 Hypernasality Too much sound resonating in the nasal cavity Usually due to VPI or fistula Most perceptible on vowels
53 Hypernasality Voiced oral consonants become nasalized (m/b, n/d, etc.) Obligatory distortion Other consonants may be substituted by nasals Compensatory production
54 Hyponasality Not enough nasal resonance on nasal sounds (m, n, ng) Due to nasal obstruction Nasal phonemes sound similar to oral cognates (b/m, d/n, g/ng) Also noticeable on vowels
, but cannot get out Due to blockage in the")
55 Cul de Sac Resonance Sound resonates in a cavity (oral, pharyngeal or nasal), but cannot get out Due to blockage in the vocal tract
56 Cul de Sac Resonance Voice sounds muffled and low in volume Sound is absorbed (like a sponge) in the cavity
57 Cul de Sac Resonance Types and Causes Oral cul de sac resonance Nasal cul de sac resonance Pharyngeal cul de sac resonance
58 Oral Cul de Sac Resonance Sound stays in the oral cavity Due to small oral cavity size or small mouth opening (microstomia) Parents describe speech as mumbling (which is not opening the mouth very much) Speech is low in volume


59 To increase volume
60 Nasal Cul de Sac Resonance Sound is mostly in the nasal cavity Due to VPI and nasal obstruction from: a deviated septum stenotic nares maxillary retrusion Common with cleft palate and craniofacial anomalies

61 Pharyngeal Cul de Sac Resonance Sound stays in the pharynx Common in patients with very large tonsils

62 Pharyngeal Cul de Sac Resonance Has been called potato-in-the-mouth speech Enlarged tonsils are the potatoes

63 Enlarged Tonsils Tonsils block sound transmission to oral cavity

64 *Cul de Sac Residence
65 Mixed Resonance Hypernasality/nasal emission on oral sounds and hyponasality on nasal sounds Due to VPI and obstruction or apraxia
66 Effects of Cleft Palate and VPI on Speech and Resonance 1. Abnormal resonance Hypernasality due to VPI or fistula Hyponasality or cul de sac resonance with cleft palate or craniofacial anomalies due to blockage
67 Effects of Cleft Palate and VPI on Speech and Resonance 2. Nasal air emission, which can cause Weak or omitted consonants Short utterance length Occasionally a nasal grimace Compensatory articulation productions 3. Dysphonia
68 Nasal Air Emission Air leaks through the valve Occurs on high pressure consonants, particularly voiceless consonants Occurs with or without hypernasality
69 Types of Nasal Emission Large opening Small opening Nasal Rustle (Turbulence)
70 Nasal Emission with Large Opening No impedance to airflow Soft, low intensity sound Affects articulation and utterance length

71 Nasal Emission with Large Opening Can also cause: Weak or omitted consonants Short utterance length Occasionally a nasal grimace Compensatory articulation productions
72 Compensatory Productions for VPI or Fistula Manner of production is maintained Placement is in pharynx to take advantage of air pressure VP valve will be open, so there will be nasal emission
73 Compensatory Productions for Palatal Fistula Plosives (Stops) Velar plosive (backing of anterior sounds) Fricatives Velar fricative

74 Velar Fricative
75 Compensatory Productions for VPI Plosives (Stops) Pharyngeal plosives Glottal stops Fricatives Pharyngeal fricatives Posterior nasal fricatives Glottal fricative (/h/) Nasal sniff
76 Pharyngeal Plosive
77 Glottal Stop Can be Co-Articulated
78 Pharyngeal Fricative

79 Posterior Nasal Fricative
80 Posterior Nasal Fricative Back of tongue articulates against velum Air pressure forced into pharynx VP valve opens for release of air pressure Causes phoneme-specific nasal air emission (PSNAE)
81 Glottal Fricative (/h/) Substituted for oral fricatives
82 Nasal Sniff Occurs as a substitution for sibilants, particularly /s/ Usually occurs in the final word position
83 Compensatory Productions for VPI Are produce in the pharynx Production results in an open VP valve Nasal emission is due to production, so persists, even after surgery for VPI Speech therapy is needed postoperatively to correct placement (which will eliminate nasal emission)
84 Nasal Emission with Small Opening Air forced through the small opening causes friction and bubbling of secretions (nasal rustle)/ nasal turbulence Distortion is loud and distracting Has no effect on consonants or utterance length
85 Nasal Emission with Small Opening Occurs inconsistently Patient can usually close with effort Opening increases with motoric demands and fatigue Can correct in therapy - but child will not be able to maintain it Therefore, even a small structural gap will require surgical correction
86 Dysphonia Hoarseness Breathiness Abnormal pitch

87 Dysphonia Vocal cord nodules due to strain in the vocal tract with VPI Laryngeal anomalies with craniofacial syndromes Compensatory strategy Breathiness and low volume mask hypernasality and nasal emission
88 Examples of Effect of Gap Size

89 Video: Large Gap Note: Nasal emission, weak consonants, short utterance length, nasal grimace

90 Video: Mid Sized Gap Note: Distortion is worse when opening becomes smaller

91 Video: Small Gap Note: Rustle (AKA Turbulence)
92 VELOPHARYNGEAL MISLEARNING
93 Velopharyngeal Mislearning Causes: Hearing Loss/Deafness Secondary to VPI: Learned compensatory productions secondary to VPI Mislearning: Misarticulations that cause nasal emission unrelated to a VPI
94 Hearing Loss/Deafness Need auditory feedback because there is no tactile-kinesthetic feedback of VP movement Results in a mixture of hyper- and hyponasality

95 Hypernasality due to Misarticulations Nasalization of vowels Back of tongue too high on vowels Can be phoneme-specific on the high vowel /i/
96 Hypernasality due to Misarticulations Substitution of nasal consonants for oral consonants (i.e. ng/l, ng/r)
97 Nasal Emission due to Misarticulation Due to pharyngeal or posterior nasal fricatives Causes phoneme-specific nasal air emission (PSNAE) Usually occurs on sibilants, particularly s/z Child is usually stimulable

98 Video: PSNAE
99 Recommendations for VP Mislearning Speech therapy because this is an articulation disorder Surgery is NOT indicated!!! Differential diagnosis is very important!

100 Evaluation and Treatment: using low-tech and no tech procedures
101 Evaluation of VP Function Child needs: Connected speech Ability to cooperate for stimulablity testing and instrumental assessment Big enough for a good airway No recent airway concerns Usually around the age of 3

102 Caveat: Don t wait too long! Critical period of brain development Need to intervene during critical period
103 Caveat: Don t wait too long! Consequences of waiting too long Correction will take longer Prognosis is negatively affected Can affect social and emotional development
104 What to Evaluate Speech sound production Airflow/air pressure and presence of nasal emission Resonance Voice (phonation)
105 Speech Sound Production Placement errors Phonological (pattern) errors Developmental errors Obligatory or compensatory errors
106 Obligatory Errors Placement is correct, but structure is abnormal Nasalization of oral phonemes (m/b, n/d, ng/g) Nasal emission Weak or omitted consonants Short utterance length
107 Compensatory Errors Placement is incorrect to compensate for abnormal structure Glottal stops Pharyngeal fricatives Pharyngeal plosives Note: These misarticulations can also be due to mislearning in the absence of VPI
108 Nasal Emission Characteristics of a large gap versus small gap
109 Nasal Emission- Large Gap Nasal emission is barely audible or even inaudible Nasal emission causes: Weak or omitted consonants Short utterance length Nasal grimace
110 Nasal Emission- Small Gap Usually in the form of a nasal rustle Note: Nasal rustle can also be due to a misarticulation which causes phoneme-specific nasal air emission
111 Nasal Rustle Can be structural or functional Structural Defect Occurs inconsistently, but on all pressure sounds, including /p/, /t/ and /k/ Functional Error Occurs consistently, but only on certain sibilants (i.e. s/z)
112 Resonance Need to determine the type: normal resonance right balance of oral and nasal resonance hypernasality hyponasality cul de sac resonance mixed resonance
113 Resonance Severity Rating scales: Seven point scale Normal, mild, moderate, severe Present or absent
114 Phonation Evaluate for signs of dysphonia: Hoarseness Breathiness Low or high pitch Low intensity
115 How?


116 Speech Samples Single word articulation test NOT good!!!
117 Speech Samples Prolongation of sounds Repetition of syllables Counting Repetition of sentences with pressuresensitive consonants Connected speech
118 Repetition of Single Sounds Oral sound to test hypernasality: vowels, particularly /ah/ and /eee/ Oral sounds to test nasal emission: prolonged /s/ Nasal sound to test hyponasality: prolonged /m/
119 Repetition of Syllables To test hypernasality or nasal emission, use oral consonants with high and low vowels: pa, pa, pa, pa ta, ta, ta, ta ka, ka, ka, ka sa, sa, sa, sa pi, pi, pi, pi ti, ti, ti, ti ki, ki, ki, ki si, si, si, si sha, sha, sha, sha shi, shi, shi, shi
120 Repetition of Syllables To test hyponasality, use nasal sounds with high and low vowels: ma, ma, ma, ma na, na, na, na mi, mi, mi, mi ni, ni, ni, ni
121 Counting To test nasal emission: Count from 60 to 70 Repeat 60 or 66 over and over 66 = SIKSTY SIKS Good combination of plosives and fricatives in blends
122 Counting To test hyponasality: Count from 90 to 99 Repeat 99 over and over
123 Repetition of Sentences p/b: Popeye plays baseball. t/d: Take Teddy to town. Do it for Daddy. k/g: Give Kate the cake. Go get the wagon. f/v: Fred has five fish. Drive the van. s/z: I see the sun in the sky. sh: She went shopping. ch: I ride a choo choo train. j: John told a joke to Jim. l: Look at the lady. r: Run down the road. I have a red fire truck. th: Thank you for the toothbrush. Blends: splash, sprinkle, street
124 Stimulability and Consistency Does change in placement change VP function? Stimulability is a good prognostic indicator for improvement or correction with therapy

125 Key to Perceptual Assessment Listen very carefully!!!
126 Low-Tech/ No-Tech Procedures Use same type of speech samples to»see»feel»hear

127 See: Mirror Test

128 See: Air Paddle

129 See: See-Scape

130 Feel: Sides of Nose

131 Hear: Nose Plugging Listen to oral sounds and sentences with nose open and then closed If there is a difference, there is an open VP valve If there is no difference, the test is inconclusive
132 Hear: Stethoscope Take off the drum Put the tip of the tube at the entrance of a nostril Listen for air or sound through the scope during oral sounds

133 Hear: Straw Same as stethoscope Straw is always available, cheap and disposable!

134 Hear: Listening Tube
135 Prediction of Gap Size based on perceptual features Hypernasality, inaudible nasal emission, weak consonants, short utterance length, compensatory productions Hypernasality, audible nasal emission, weak consonants, may have compensatory productions Possibly mild hypernasality and audible nasal emission Normal resonance, but inconsistent nasal rustle (turbulence)

136 INTRA-ORAL EVALUATION
137 Intra-Oral Evaluation Can evaluate oral structures and oral function Cannot evaluate velopharyngeal structure or VP function View is well below area of closure
138 Intra-Oral Evaluation Signs of a submucous cleft Position of the uvula during phonation Size of the tonsils Signs of upper airway obstruction Signs of oral-motor dysfunction
139 Intra-Oral Evaluation Need to see to the tip of the uvula Avoid using a tongue blade


140 Say aaaah as in bat and protrude the tongue
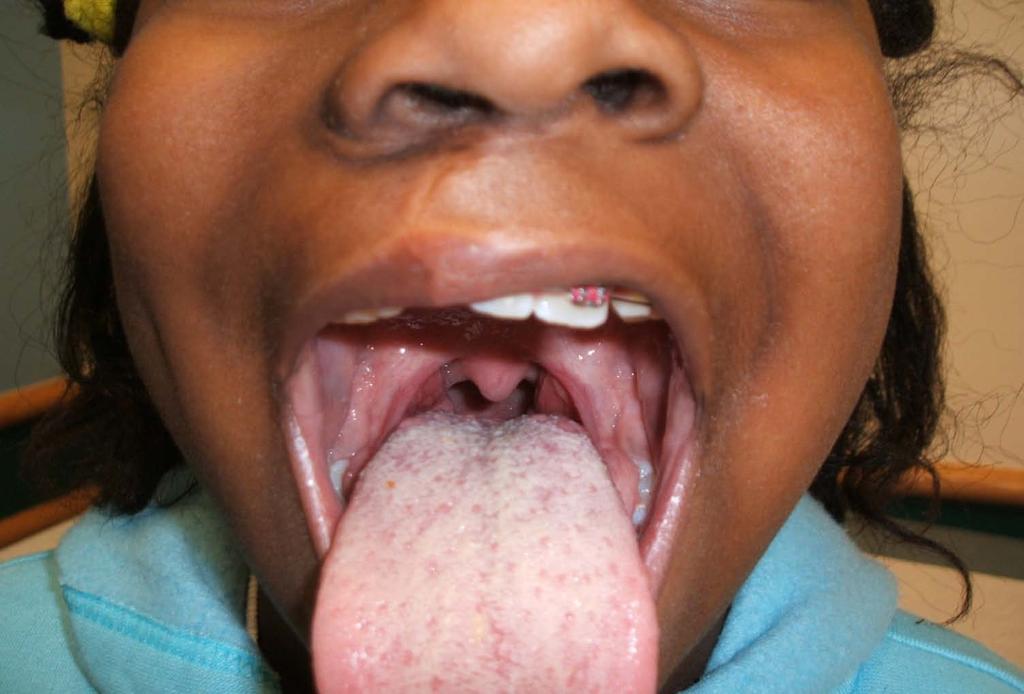
141 Aaaah

142 Video: Submucous Cleft

143 Submucous Cleft
144 Instrumental Evaluation of VP Function Direct Procedures You can see it, but you can t quantify it. Videofluoroscopy and nasopharyngoscopy Indirect Procedures You can quantify it, but you can t see it Aerodynamics (pressure-flow) and Nasometry

145 Nasometry (KayPentax) Analyzes acoustic energy from oral and nasal cavities Gives an objective nasalance score
146 Measured Value called Nasalance Computes a percentage of nasal acoustic energy in speech Nasal Acoustic Energy Total (nasal + oral) Acoustic Energy

147 SNAP Test: Sibilants Passage Normal Speech
148 SNAP Test: Suzy Passage Nasal Rustle
149 SNAP Test: Velars Passage Nasal Rustle
150 Need to Determine Probable Cause Velopharyngeal insufficiency (VPI) Velopharyngeal incompetence (VPI) Velopharyngeal mislearning
151 Velopharyngeal Insufficiency (structural abnormality) Surgery (speech therapy postoperatively) Prosthetics- speech bulb (if surgery is not an option) Speech therapy is appropriate AFTER the surgery to eliminate compensatory articulation errors Note: Speech therapy CANNOT change abnormal structure!
152 Velopharyngeal Incompetence (neurophysiological cause) Surgery (speech therapy postoperatively) Prosthetics- palatal lift Speech therapy
153 Velopharyngeal Mislearning Speech therapy only
154 TREATMENT OF VPI Surgery Prosthetics Speech therapy

155 Surgery for VPI Pharyngeal augmentation Furlow Z plasty Sphincter pharyngoplasty Pharyngeal flap Note: These do not always work the first time. May need revision or even re-do.
156 Factors in Surgical Procedure Selection Cause: irregular adenoids versus short velum Size of the opening Risk of airway obstruction Location, Location, Location Need to find the hole and find the right procedure to fill it!

157 Prosthetic Devices Palatal lift Palatal obturator Speech bulb
158 Limitations of Prosthetic Devices Require insertion and removal Have to redo periodically due to growth Can be lost or damaged May be very uncomfortable Compliance is often poor Don t permanently correct the problem Most centers use only if surgery is not possible
159 Speech Therapy With Structural Anomalies Speech therapy CANNOT change abnormal structure Speech therapy CANNOT correct VPI
160 Speech Therapy With Structural Anomalies Speech therapy CAN change abnormal function Compensatory errors secondary to abnormal structure (i.e., malocclusion or VPI) Mislearning (in absence of structural anomalies) Oral-motor dysfunction (apraxia)
161 Speech Therapy With Structural Anomalies Speech therapy CAN improve the function of the VP structures AFTER surgical correction of the structure Changing structure does not change function

162 Speech Therapy While waiting for surgery to correct VPI: Use nose plugging technique Gives the child increased oral pressure to work on articulation Child should wear nose plug at home as much as possible

163 Speech Therapy For hypernasality or nasal emission after surgery for VPI: Use auditory feedback Nasal tube or ONL will provide feedback
* * Super Duper")
164 Auditory Feedback: Oral & Nasal Listener (ONL)* * Super Duper Publications- 2007
165 Speech Therapy for VP Mislearning Glottal stops Nasalized vowels or ng/l Nasalized /r/ Pharyngeal plosives Palatal-dorsal production (lateral lisp) Pharyngeal or posterior nasal fricatives
166 Video: Speech Therapy for phoneme-specific nasal emission due to misarticulation
167 General Principles Do not use blowing or sucking exercises, velar exercises or oral-motor exercises!!! Do not PINCH the nose to improve VP function None of these have any evidence of efficacy and they don t work!!!
168 General Principles Use general articulation procedures to establish appropriate placement Incorporate motor learning principles
169 Motor Learning Necessary for learning to perform all complicated motor movements and sequences without conscious thought Dependent on feedback and practice Results in brain reorganization due to neural plasticity
170 Feedback Done in speech therapy to shape appropriate production of the speech sound
171 Practice Done first in therapy, and then at home Drill work is VERY important The number of correct responses elicited (in therapy and at home) is directly related to the rate of progress.
172 Examples of Motor Learning Playing an instrument: piano Ballroom dancing: salsa, swing Sports: shooting a basketball Speech

173 Motor Learning Speech therapy is like piano lessons if you don t practice at home, you don t learn to play the piano!
174 Goal of Treatment Normal speech and resonance No evidence of nasality Acceptable speech is not acceptable
175 Referrals Check Around... This is a specialty area for all disciplines (ENT, surgery and speech path) Refer to a craniofacial team Check with American Cleft Palate- Craniofacial Association (ACPA) for professionals with experience in this area (

176 Team Approach: Cincinnati Craniofacial Center

177 Thanks for your interest!
Financial Disclosures
 Resonance Disorders and Velopharyngeal Dysfunction: Evaluation and Treatment Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center Employment: Financial Disclosures Cincinnati Children
Resonance Disorders and Velopharyngeal Dysfunction: Evaluation and Treatment Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center Employment: Financial Disclosures Cincinnati Children
Evaluation and Treatment: using low-tech and no tech procedures
 Evaluation and Treatment: using low-tech and no tech procedures 6. Perceptual Evaluation When, What, How, and Why When the evaluation should be done for the most reliable results and maximum benefit for
Evaluation and Treatment: using low-tech and no tech procedures 6. Perceptual Evaluation When, What, How, and Why When the evaluation should be done for the most reliable results and maximum benefit for
Resonance Disorders & Velopharyngeal Dysfunction
 Resonance Disorders & Velopharyngeal Dysfunction Cincinnati Children s Normal Velopharyngeal Function Structures Active in Velopharyngeal Closure Velum (soft palate) - The velum moves in a superior and
Resonance Disorders & Velopharyngeal Dysfunction Cincinnati Children s Normal Velopharyngeal Function Structures Active in Velopharyngeal Closure Velum (soft palate) - The velum moves in a superior and
Cleft Palate Speech-Components and Assessment Voice and Resonance Disorders-ASLS-563. Key Components of Cleft Palate Speech.
 Cleft Palate Speech-Components and Assessment Voice and Resonance Disorders-ASLS-563 Key Components of Cleft Palate Speech Disorder Type of Disorder/ Causes Hypernasality Resonance Disorder insufficiency
Cleft Palate Speech-Components and Assessment Voice and Resonance Disorders-ASLS-563 Key Components of Cleft Palate Speech Disorder Type of Disorder/ Causes Hypernasality Resonance Disorder insufficiency
Cleft Lip and Palate: The Effects on Speech and Resonance
 Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Cleft lip and/or palate can have a negative impact on both speech and resonance. The following is a summary of normal anatomy, the types and causes of
Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Cleft lip and/or palate can have a negative impact on both speech and resonance. The following is a summary of normal anatomy, the types and causes of
VPD Clinic: Using Nasopharyngoscopy to Evaluate Velopharyngeal Dysfunction and so much more!
 VPD Clinic: Using Nasopharyngoscopy to Evaluate Velopharyngeal Dysfunction and so much more! Brenda Sitzmann, MA, CCC-SLP Speech Language Pathologist Jill Arganbright, MD Assistant Professor, Pediatric
VPD Clinic: Using Nasopharyngoscopy to Evaluate Velopharyngeal Dysfunction and so much more! Brenda Sitzmann, MA, CCC-SLP Speech Language Pathologist Jill Arganbright, MD Assistant Professor, Pediatric
Speech/Resonance Disorders due to Clefts and Craniofacial Anomalies
 Speech/Resonance Disorders due to Clefts and Craniofacial Anomalies Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center Royalties: Financial Disclosures Book: Kummer, AW. Cleft Palate
Speech/Resonance Disorders due to Clefts and Craniofacial Anomalies Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center Royalties: Financial Disclosures Book: Kummer, AW. Cleft Palate
CLEFT PALATE & MISARTICULATION
 CLEFT PALATE & MISARTICULATION INTRODUCTION o Between the 6th and 12th weeks of fetal gestation,the left and right sides of the face and facial skeleton fuse in the midddle. When they do fail to do so,
CLEFT PALATE & MISARTICULATION INTRODUCTION o Between the 6th and 12th weeks of fetal gestation,the left and right sides of the face and facial skeleton fuse in the midddle. When they do fail to do so,
Speech Sound Disorders Alert: Identifying and Fixing Nasal Fricatives in a Flash
 Speech Sound Disorders Alert: Identifying and Fixing Nasal Fricatives in a Flash Judith Trost-Cardamone, PhD CCC/SLP California State University at Northridge Ventura Cleft Lip & Palate Clinic and Lynn
Speech Sound Disorders Alert: Identifying and Fixing Nasal Fricatives in a Flash Judith Trost-Cardamone, PhD CCC/SLP California State University at Northridge Ventura Cleft Lip & Palate Clinic and Lynn
Kerry Callahan Mandulak, PhD, CCC-SLP Department of Speech and Hearing Sciences Portland State University, Portland, OR
 Kerry Callahan Mandulak, PhD, CCC-SLP Department of Speech and Hearing Sciences Portland State University, Portland, OR Adriane Baylis, PhD, CCC-SLP Nationwide Children s Hospital, Columbus, OH Anna Thurmes,
Kerry Callahan Mandulak, PhD, CCC-SLP Department of Speech and Hearing Sciences Portland State University, Portland, OR Adriane Baylis, PhD, CCC-SLP Nationwide Children s Hospital, Columbus, OH Anna Thurmes,
Developmental communication disorders
 Part I Developmental communication disorders 1 Cleft lip and palate and other craniofacial anomalies John E. Riski 1.1 Introduction Despite reports from the Centers for Disease Control and Prevention
Part I Developmental communication disorders 1 Cleft lip and palate and other craniofacial anomalies John E. Riski 1.1 Introduction Despite reports from the Centers for Disease Control and Prevention
Speech: Something We Can Really Fix
 CHAPTER 2 Speech: Something We Can Really Fix As we have just seen, speech impairment is one of the most common findings in VCFS, occurring in at least 70% of cases (Shprintzen & Golding-Kushner, 2009).
CHAPTER 2 Speech: Something We Can Really Fix As we have just seen, speech impairment is one of the most common findings in VCFS, occurring in at least 70% of cases (Shprintzen & Golding-Kushner, 2009).
TEMPORAL CHARACTERISTICS OF ALVEOLAR STOP CONSONANTS PRODUCED BY CHILDREN WITH VARYING LEVELS OF VELOPHARYNGEAL DYSFUNCTION.
 TEMPORAL CHARACTERISTICS OF ALVEOLAR STOP CONSONANTS PRODUCED BY CHILDREN WITH VARYING LEVELS OF VELOPHARYNGEAL DYSFUNCTION Meredith Gaylord A thesis submitted to the faculty of the University of North
TEMPORAL CHARACTERISTICS OF ALVEOLAR STOP CONSONANTS PRODUCED BY CHILDREN WITH VARYING LEVELS OF VELOPHARYNGEAL DYSFUNCTION Meredith Gaylord A thesis submitted to the faculty of the University of North
Place and Manner of Articulation Sounds in English. Dr. Bushra Ni ma
 Place and Manner of Articulation Sounds in English Dr. Bushra Ni ma Organs of Speech Respiratory System Phonatory System Articulatory System Lungs Muscles of the chest Trachea Larynx Pharynx Lips Teeth
Place and Manner of Articulation Sounds in English Dr. Bushra Ni ma Organs of Speech Respiratory System Phonatory System Articulatory System Lungs Muscles of the chest Trachea Larynx Pharynx Lips Teeth
THE DEVIL KNOWS MORE FOR BEING OLD THAN FOR BEING THE DEVIL
 V P I A CHALLENGE 40 YEARS A PHYSICIAN 37 YEARS TREATING PATIENTS WITH V P I THE DEVIL KNOWS MORE FOR BEING OLD THAN FOR BEING THE DEVIL NO CP CENTER IN THE WORLD CAN CLAIM 0% PREVALENCE OF V P I AFTER
V P I A CHALLENGE 40 YEARS A PHYSICIAN 37 YEARS TREATING PATIENTS WITH V P I THE DEVIL KNOWS MORE FOR BEING OLD THAN FOR BEING THE DEVIL NO CP CENTER IN THE WORLD CAN CLAIM 0% PREVALENCE OF V P I AFTER
Def. - the process of exchanging information and ideas
 What is communication Def. - the process of exchanging information and ideas All living things communicate. Acquiring Human Communication Humans communicate in many ways What is a communication disorder?
What is communication Def. - the process of exchanging information and ideas All living things communicate. Acquiring Human Communication Humans communicate in many ways What is a communication disorder?
Speech (Sound) Processing
 Processing") 7 Speech (Sound) Processing Acoustic Human communication is achieved when thought is transformed through language into speech. The sounds of speech are initiated by activity in the central nervous system,
7 Speech (Sound) Processing Acoustic Human communication is achieved when thought is transformed through language into speech. The sounds of speech are initiated by activity in the central nervous system,
It is important to understand as to how do we hear sounds. There is air all around us. The air carries the sound waves but it is below 20Hz that our
 Phonetics. Phonetics: it is a branch of linguistics that deals with explaining the articulatory, auditory and acoustic properties of linguistic sounds of human languages. It is important to understand
Phonetics. Phonetics: it is a branch of linguistics that deals with explaining the articulatory, auditory and acoustic properties of linguistic sounds of human languages. It is important to understand
Mark Hakel, Ph.D., CCC-SLP, Julie Marshall, D.D.S., M.S. Monica McHenry, Ph.D. CCC-SLP. November 20, 2009
 Mark Hakel, Ph.D., CCC-SLP, Julie Marshall, D.D.S., M.S. Monica McHenry, Ph.D. CCC-SLP November 20, 2009 Inadequate tissue with good innervation Classically associated with cleft palate Inadequate tissue
Mark Hakel, Ph.D., CCC-SLP, Julie Marshall, D.D.S., M.S. Monica McHenry, Ph.D. CCC-SLP November 20, 2009 Inadequate tissue with good innervation Classically associated with cleft palate Inadequate tissue
Communication disorders in individuals with cleft lip and palate: An overview
 Review Article Free full text on www.ijps.org DOI: 10.4103/0970-0358.57199 Communication disorders in individuals with cleft lip and palate: An overview Roopa Nagarajan, V. H. Savitha, B. Subramaniyan
Review Article Free full text on www.ijps.org DOI: 10.4103/0970-0358.57199 Communication disorders in individuals with cleft lip and palate: An overview Roopa Nagarajan, V. H. Savitha, B. Subramaniyan
LINGUISTICS 221 LECTURE #3 Introduction to Phonetics and Phonology THE BASIC SOUNDS OF ENGLISH
 LINGUISTICS 221 LECTURE #3 Introduction to Phonetics and Phonology 1. STOPS THE BASIC SOUNDS OF ENGLISH A stop consonant is produced with a complete closure of airflow in the vocal tract; the air pressure
LINGUISTICS 221 LECTURE #3 Introduction to Phonetics and Phonology 1. STOPS THE BASIC SOUNDS OF ENGLISH A stop consonant is produced with a complete closure of airflow in the vocal tract; the air pressure
UNIVERSITY OF CINCINNATI
 UNIVERSITY OF CINCINNATI Date: I,, hereby submit this work as part of the requirements for the degree of: in: It is entitled: This work and its defense approved by: Chair: Speech Outcomes following Surgical
UNIVERSITY OF CINCINNATI Date: I,, hereby submit this work as part of the requirements for the degree of: in: It is entitled: This work and its defense approved by: Chair: Speech Outcomes following Surgical
Let s start by tuning our ears!
 Craniofacial Speech Disorders: How to Identify, Transcribe & Plan Treatment Let s start by tuning our ears! Judith Trost-Cardamone, PhD - CCC/SLP, FASHA Professor, California State University-Northridge
Craniofacial Speech Disorders: How to Identify, Transcribe & Plan Treatment Let s start by tuning our ears! Judith Trost-Cardamone, PhD - CCC/SLP, FASHA Professor, California State University-Northridge
Longitudinal outcome of pharyngoplasty
 Archives of Orofacial Sciences (2009), 4(1): 17-21 CASE REPORT Longitudinal outcome of pharyngoplasty Peter J. Anderson*, Roslynn K. Sells, David. J. David Australian Craniofacial Unit, Women s and Children
Archives of Orofacial Sciences (2009), 4(1): 17-21 CASE REPORT Longitudinal outcome of pharyngoplasty Peter J. Anderson*, Roslynn K. Sells, David. J. David Australian Craniofacial Unit, Women s and Children
Asia Pacific Journal of Research ISSN (Print) : ISSN (Online) :
 : ISSN (Online) :") CLEFT SPEECH A TELLTALE SIGN OF OCCULT SUBMUCOUS CLEFT: A CASE STUDY MS. ARPITA CHATTERJEE SHAHI AUDIOLOGIST AND SPEECH LANGUAGE PATHOLOGIST ALI YAVAR JUNG NATIONAL INSTITUTE FOR THE HEARING HANDICAPPED
CLEFT SPEECH A TELLTALE SIGN OF OCCULT SUBMUCOUS CLEFT: A CASE STUDY MS. ARPITA CHATTERJEE SHAHI AUDIOLOGIST AND SPEECH LANGUAGE PATHOLOGIST ALI YAVAR JUNG NATIONAL INSTITUTE FOR THE HEARING HANDICAPPED
CINERADIOGRAPHIC ASSESSMENT OF COMBINED ISLAND FLAP PUSHBACK AND PHARYNGEAL FLAP IN THE SURGICAL MANAGEMENT OF SUBMUCOUS CLEFT PALATE 1
 CINERADIOGRAPHIC ASSESSMENT OF COMBINED ISLAND FLAP PUSHBACK AND PHARYNGEAL FLAP IN THE SURGICAL MANAGEMENT OF SUBMUCOUS CLEFT PALATE 1 By JOHN E. HOOPES, M.D., z A. LEE DELLON, 3 JACOB I. FABRIKANT, M.D.,
CINERADIOGRAPHIC ASSESSMENT OF COMBINED ISLAND FLAP PUSHBACK AND PHARYNGEAL FLAP IN THE SURGICAL MANAGEMENT OF SUBMUCOUS CLEFT PALATE 1 By JOHN E. HOOPES, M.D., z A. LEE DELLON, 3 JACOB I. FABRIKANT, M.D.,
The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (9), Page
 Vol. 73 (9), Page") The Egyptian Journal of Hospital Medicine (October 18) Vol. 73 (9), Page 7604-7609 Role of MRI in Detection of Repaired Cleft Palate Muscles and Correlation to Speech Amro Mahmoud Abdelrahman Ali, Mahmoud
The Egyptian Journal of Hospital Medicine (October 18) Vol. 73 (9), Page 7604-7609 Role of MRI in Detection of Repaired Cleft Palate Muscles and Correlation to Speech Amro Mahmoud Abdelrahman Ali, Mahmoud
Critical Review: Is videonasopharyngoscopy biofeedback therapy effective in improving velopharyngeal closure in patients with cleft palate?
 Critical Review: Is videonasopharyngoscopy biofeedback therapy effective in improving velopharyngeal closure in patients with cleft palate? Brenna Singer M.Cl.Sc (SLP) Candidate University of Western Ontario:
Critical Review: Is videonasopharyngoscopy biofeedback therapy effective in improving velopharyngeal closure in patients with cleft palate? Brenna Singer M.Cl.Sc (SLP) Candidate University of Western Ontario:
Speech Generation and Perception
 Speech Generation and Perception 1 Speech Generation and Perception : The study of the anatomy of the organs of speech is required as a background for articulatory and acoustic phonetics. An understanding
Speech Generation and Perception 1 Speech Generation and Perception : The study of the anatomy of the organs of speech is required as a background for articulatory and acoustic phonetics. An understanding
ASU Speech and Hearing Clinic Spring Testing. Adult Speech and Language Evaluation
 Adult Speech and Language Evaluation ASU Speech and Hearing Clinic Spring Testing Name: DOB:_ Gender: Examiner:_ Date: Instructions: Administer the following screening tools and standardized tests/batteries.
Adult Speech and Language Evaluation ASU Speech and Hearing Clinic Spring Testing Name: DOB:_ Gender: Examiner:_ Date: Instructions: Administer the following screening tools and standardized tests/batteries.
Surgery for Pediatric Velopharyngeal Insufficiency
 oks ==> freeinebo Advances Oto-Rhino-Laryngology Editor: G. Randolph Vol. 76 Surgery for Pediatric Velopharyngeal Insufficiency Editors N. Raol C.J. Hartnick Surgery for Pediatric Velopharyngeal Insufficiency
oks ==> freeinebo Advances Oto-Rhino-Laryngology Editor: G. Randolph Vol. 76 Surgery for Pediatric Velopharyngeal Insufficiency Editors N. Raol C.J. Hartnick Surgery for Pediatric Velopharyngeal Insufficiency
Assignment #4: Speech Target /p/ By: Robyn Black STAGE MODALITY STRATEGIES/TECHNIQUES MATERIALS
 Assignment #4: Speech Target /p/ By: Robyn Black Target phoneme: /p/ Manner: Plosive Description: A plosive is a speech sound produced by the closure of the oral passage followed by a release accompanied
Assignment #4: Speech Target /p/ By: Robyn Black Target phoneme: /p/ Manner: Plosive Description: A plosive is a speech sound produced by the closure of the oral passage followed by a release accompanied
Cleft Lip and Palate. February 21, February 28, /17/2015
 Cleft Lip and Palate Dianne M. Altuna, M.S./CCC-SLP Region X ESC November 20, 2015 paltuna@aol.com 214.763.7388 February 21, 2014 Diagnosis/Types Common craniofacial syndromes associated with cleft lip
Cleft Lip and Palate Dianne M. Altuna, M.S./CCC-SLP Region X ESC November 20, 2015 paltuna@aol.com 214.763.7388 February 21, 2014 Diagnosis/Types Common craniofacial syndromes associated with cleft lip
Phonetics is the study of vocal sounds. Phonetics and flight safety - An orodental view point. Gp Capt K Ravishankar *, Air Cmde GP Singh VSM +
 Phonetics Methods and in flight Aerospace safety - Medicineethods An orodental view point: Aerospace Ravishankar Medicine K ABSTRACT Phonetics and flight safety - An orodental view point Gp Capt K Ravishankar
Phonetics Methods and in flight Aerospace safety - Medicineethods An orodental view point: Aerospace Ravishankar Medicine K ABSTRACT Phonetics and flight safety - An orodental view point Gp Capt K Ravishankar
Sibilants Have Similar Sound Production
 The Entire World of Sibilants Christine Ristuccia, M.S. CCC-SLP Sibilants Have Similar Sound Production Related sounds. They are produced at or just behind alveolar ridge (bumpy gum area behind front teeth).
The Entire World of Sibilants Christine Ristuccia, M.S. CCC-SLP Sibilants Have Similar Sound Production Related sounds. They are produced at or just behind alveolar ridge (bumpy gum area behind front teeth).
Clinical experience from primary palatoplasty and studies of velopharyngeal
 The Effect of Intravelar Veloplasty on Velopharyngeal Competence Following Pharyngeal Flap Surgery Bennie L. Jarvis, M.D. Wicuiam C. Trier, M.D. Clinical experience from primary palatoplasty and studies
The Effect of Intravelar Veloplasty on Velopharyngeal Competence Following Pharyngeal Flap Surgery Bennie L. Jarvis, M.D. Wicuiam C. Trier, M.D. Clinical experience from primary palatoplasty and studies
LINGUISTICS 130 LECTURE #4 ARTICULATORS IN THE ORAL CAVITY
 LINGUISTICS 130 LECTURE #4 ARTICULATORS IN THE ORAL CAVITY LIPS (Latin labia ) labial sounds bilabial labiodental e.g. bee, my e.g. fly, veal TEETH (Latin dentes) dental sounds e.g. think, they ALVEOLAR
LINGUISTICS 130 LECTURE #4 ARTICULATORS IN THE ORAL CAVITY LIPS (Latin labia ) labial sounds bilabial labiodental e.g. bee, my e.g. fly, veal TEETH (Latin dentes) dental sounds e.g. think, they ALVEOLAR
 - speech-~echanism Assessment tion, a small dental mirror and gauze pads may be necessary. Before putting the gloves on, clean the table with disinfectant and wash your hands thoroughly with antibacterial
- speech-~echanism Assessment tion, a small dental mirror and gauze pads may be necessary. Before putting the gloves on, clean the table with disinfectant and wash your hands thoroughly with antibacterial
Objectives. Oromyofunction & Oral Health Gum Gardeners April 28, 2014 Linda D Onofrio, MS, CCC-SLP
 Oromyofunction & Oral Health Gum Gardeners April 28, 2014 Linda D Onofrio, MS, CCC-SLP 503-808-9919 linda@donofrioslp.com My clinical experience & scope of practice n Be able to conduct an oromyofunctional
Oromyofunction & Oral Health Gum Gardeners April 28, 2014 Linda D Onofrio, MS, CCC-SLP 503-808-9919 linda@donofrioslp.com My clinical experience & scope of practice n Be able to conduct an oromyofunctional
G l o s s a r y. The lack of closure of a normal body orifice or. passage
 A P P E N D I XE G l o s s a r y Allergic rhinitis Swelling of the membrane in the nasal chamber due to allergic reactions; the condition may obstruct breathing Alveolar ridge The bony arches of the maxilla
A P P E N D I XE G l o s s a r y Allergic rhinitis Swelling of the membrane in the nasal chamber due to allergic reactions; the condition may obstruct breathing Alveolar ridge The bony arches of the maxilla
Associations between speech features and phenotypic severity in Treacher Collins syndrome
 Åsten et al. BMC Medical Genetics 2014, 15:47 RESEARCH ARTICLE Open Access Associations between speech features and phenotypic severity in Treacher Collins syndrome Pamela Åsten 1*, Harriet Akre 2,3 and
Åsten et al. BMC Medical Genetics 2014, 15:47 RESEARCH ARTICLE Open Access Associations between speech features and phenotypic severity in Treacher Collins syndrome Pamela Åsten 1*, Harriet Akre 2,3 and
Speech and Language Therapy. Kerrie McCarthy Senior Speech and Language Therapist
 Speech and Language Therapy Kerrie McCarthy Senior Speech and Language Therapist Contents 1. Voice disorders 2. Swallow disorders 3. Videofluroscopy 4. Adult Acquired Communication Disorders 5. How to
Speech and Language Therapy Kerrie McCarthy Senior Speech and Language Therapist Contents 1. Voice disorders 2. Swallow disorders 3. Videofluroscopy 4. Adult Acquired Communication Disorders 5. How to
o Spectrogram: Laterals have weak formants around 250, 1200, and 2400 Hz.
 Ch. 10 Places of articulation 1) Primary places of articulation a) Labials: made with one or both lips i) Bilabial: two lips. Bilabial stops and nasals are common, while fricatives are uncommon. ii) Labiodental:
Ch. 10 Places of articulation 1) Primary places of articulation a) Labials: made with one or both lips i) Bilabial: two lips. Bilabial stops and nasals are common, while fricatives are uncommon. ii) Labiodental:
Velopharyngeal oclusion in people who were submitted to nasoendoscopy at The Center of Health Education (CEPS)
") to nasoendoscopy at The Center of Health (CEPS) Lais Odila Silveira Camargo 1 Carla Meliso Rodrigues 2 Juliana Arbex Avelar 3 Received on 12/5/00 Approved on 8/10/00 Salusvita, Bauru, ABSTRACT 1 to 3 -
to nasoendoscopy at The Center of Health (CEPS) Lais Odila Silveira Camargo 1 Carla Meliso Rodrigues 2 Juliana Arbex Avelar 3 Received on 12/5/00 Approved on 8/10/00 Salusvita, Bauru, ABSTRACT 1 to 3 -
Longitudinal Evaluation of Articulation and Velopharyngeal
 _ Longitudinal Evaluation of Articulation and Velopharyngeal Competence of Patients with Pharyngeal Flaps D. R. Van Demark, PH.D. M. A. Harpin, PH.D. In this study, 129 patients with cleft palate who had
_ Longitudinal Evaluation of Articulation and Velopharyngeal Competence of Patients with Pharyngeal Flaps D. R. Van Demark, PH.D. M. A. Harpin, PH.D. In this study, 129 patients with cleft palate who had
how stopped air is released when released with puff of air = aspirated when release is unaspirated, captured air is released into vowel (i.e.
 1 STOP CONSONANTS also referred to as plosives labeled to describe manner of production a speech sound with closure or stopping of airstream within the oral cavity interruption of airflow has two phases:
1 STOP CONSONANTS also referred to as plosives labeled to describe manner of production a speech sound with closure or stopping of airstream within the oral cavity interruption of airflow has two phases:
Historical study of a program of systematic obturator reduction for palatal incompetence
 University of Montana ScholarWorks at University of Montana Graduate Student Theses, Dissertations, & Professional Papers Graduate School 1980 Historical study of a program of systematic obturator reduction
University of Montana ScholarWorks at University of Montana Graduate Student Theses, Dissertations, & Professional Papers Graduate School 1980 Historical study of a program of systematic obturator reduction
Temporal Characteristics of Aerodynamic Segments in the Speech of Children and Adults
 Temporal Characteristics of Aerodynamic Segments in the Speech of Children and Adults Objectives: The primary purpose of this study was to determine the temporal characteristics of aerodynamic segments
Temporal Characteristics of Aerodynamic Segments in the Speech of Children and Adults Objectives: The primary purpose of this study was to determine the temporal characteristics of aerodynamic segments
Carolinas Center for Cleft Lip & Palate Surgery
 Carolinas Center for Cleft Lip & Palate Surgery Carolinas Center for Oral & Facial Surgery 8840 Blakeney Professional Drive Suite 300 Charlotte NC 28277 P: 704.716.9840 F: 704.716.9841 Clinical Coordinator
Carolinas Center for Cleft Lip & Palate Surgery Carolinas Center for Oral & Facial Surgery 8840 Blakeney Professional Drive Suite 300 Charlotte NC 28277 P: 704.716.9840 F: 704.716.9841 Clinical Coordinator
1 Announcing Your Speaking Voice 2 Current Trends More Program choices and increased specialization increase in importance of one-to-one contact
 1 Announcing Your Speaking Voice 2 Current Trends More Program choices and increased specialization increase in importance of one-to-one contact between announcer and audience ongoing regulatory debate
1 Announcing Your Speaking Voice 2 Current Trends More Program choices and increased specialization increase in importance of one-to-one contact between announcer and audience ongoing regulatory debate
Plastic and Jaw Department, United Sheffield Hospitals
 THE EXAMINATION OF IMPERFECT SPEECH FOLLOWING CLEFT-PALATE OPERATIONS By WILFRED HYNES, F.R.C.S Plastic and Jaw Department, United Sheffield Hospitals THE results of cleft-palate operations can be difficult
THE EXAMINATION OF IMPERFECT SPEECH FOLLOWING CLEFT-PALATE OPERATIONS By WILFRED HYNES, F.R.C.S Plastic and Jaw Department, United Sheffield Hospitals THE results of cleft-palate operations can be difficult
Comparative Study between Superiorly Based Pharyngeal Flap and Sphincteroplasty in Treatment of Velopharyngeal Insufficiency after Cleft Palate Repair
 Egypt, J. Plast. Reconstr. Surg., Vol. 29, No. 2, July: 149-156, 2005 Comparative Study between Superiorly Based Pharyngeal Flap and Sphincteroplasty in Treatment of Velopharyngeal Insufficiency after
Egypt, J. Plast. Reconstr. Surg., Vol. 29, No. 2, July: 149-156, 2005 Comparative Study between Superiorly Based Pharyngeal Flap and Sphincteroplasty in Treatment of Velopharyngeal Insufficiency after
Overview. Acoustics of Speech and Hearing. Source-Filter Model. Source-Filter Model. Turbulence Take 2. Turbulence
 Overview Acoustics of Speech and Hearing Lecture 2-4 Fricatives Source-filter model reminder Sources of turbulence Shaping of source spectrum by vocal tract Acoustic-phonetic characteristics of English
Overview Acoustics of Speech and Hearing Lecture 2-4 Fricatives Source-filter model reminder Sources of turbulence Shaping of source spectrum by vocal tract Acoustic-phonetic characteristics of English
A Simple Technique for Determining Velopharyngeal Status during Speech Production
 A Simple Technique for Determining Velopharyngeal Status during Speech Production Kate Bunton, Ph.D., CCC-SLP, 1 Jeannette D. Hoit, Ph.D., CCC-SLP, 1 and Keegan Gallagher 1 ABSTRACT Clinical evaluation
A Simple Technique for Determining Velopharyngeal Status during Speech Production Kate Bunton, Ph.D., CCC-SLP, 1 Jeannette D. Hoit, Ph.D., CCC-SLP, 1 and Keegan Gallagher 1 ABSTRACT Clinical evaluation
EVALUATION AND MANAGEMENT OF PATIENTS WITH CLEFT LIP AND PALATE
 EVALUATION AND MANAGEMENT OF PATIENTS WITH CLEFT LIP AND PALATE DEFINING TERMS PRIMARY PALATE- Structures anterior to the incisive foramen Includes the nose, lip alveolus, and hard palate back to the incisive
EVALUATION AND MANAGEMENT OF PATIENTS WITH CLEFT LIP AND PALATE DEFINING TERMS PRIMARY PALATE- Structures anterior to the incisive foramen Includes the nose, lip alveolus, and hard palate back to the incisive
rcgftffi$ehffih!htr Claudia Yun,tA Grainiofacial Center
 Treatment of Gom pensatory Articulation Errors rcgftffi$ehffih!htr Claudia Yun,tA Grainiofacial Center chans "+##ffilhospitar =X}H 6JhEFSHIM+,L. Com pensatory m isarticulations are substitution errors
Treatment of Gom pensatory Articulation Errors rcgftffi$ehffih!htr Claudia Yun,tA Grainiofacial Center chans "+##ffilhospitar =X}H 6JhEFSHIM+,L. Com pensatory m isarticulations are substitution errors
Prosthetic Rehabilitation of a Velopharyngeal Defect: A Case Report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 4 Ver. X (Apr. 2015), PP 01-05 www.iosrjournals.org Prosthetic Rehabilitation of a Velopharyngeal
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 4 Ver. X (Apr. 2015), PP 01-05 www.iosrjournals.org Prosthetic Rehabilitation of a Velopharyngeal
Slide 1. Slide 2. Slide 3. Introduction to the Electrolarynx. I have nothing to disclose and I have no proprietary interest in any product discussed.
 Slide 1 Introduction to the Electrolarynx CANDY MOLTZ, MS, CCC -SLP TLA SAN ANTONIO 2019 Slide 2 I have nothing to disclose and I have no proprietary interest in any product discussed. Slide 3 Electrolarynxes
Slide 1 Introduction to the Electrolarynx CANDY MOLTZ, MS, CCC -SLP TLA SAN ANTONIO 2019 Slide 2 I have nothing to disclose and I have no proprietary interest in any product discussed. Slide 3 Electrolarynxes
Understanding 22q11.2 Deletion Syndrome
 Understanding 22q11.2 Deletion Syndrome 22q11.2 Deletion Syndrome ( 22q11.2 ) is a genetic disorder that is also referred to as Velo- Cardio-Facial Syndrome ( VCFS ), Shprintzen Syndrome, and/or DiGeorge
Understanding 22q11.2 Deletion Syndrome 22q11.2 Deletion Syndrome ( 22q11.2 ) is a genetic disorder that is also referred to as Velo- Cardio-Facial Syndrome ( VCFS ), Shprintzen Syndrome, and/or DiGeorge
Introduction to Standard Esophageal Speech. Texas Laryngectomy Association 2018
 Introduction to Standard Esophageal Speech Texas Laryngectomy Association 2018 Disclosure Objectives At the end of this presentation the participant will be able to: Describe the production of standard
Introduction to Standard Esophageal Speech Texas Laryngectomy Association 2018 Disclosure Objectives At the end of this presentation the participant will be able to: Describe the production of standard
SYLLABUS FOR PH.D ENTRANCE TEST IN SPEECH AND HEARING
 SYLLABUS FOR PH.D ENTRANCE TEST IN SPEECH AND HEARING 1) ADVANCES IN SPEECH SCIENCE. a) Life span changes in speech mechanism including developmental milestones b) Physiology of Speech production: Respiratory
SYLLABUS FOR PH.D ENTRANCE TEST IN SPEECH AND HEARING 1) ADVANCES IN SPEECH SCIENCE. a) Life span changes in speech mechanism including developmental milestones b) Physiology of Speech production: Respiratory
VOICE LESSON #6. Resonance: Creating Good Vocal Vibes. The Soft Palate
 VOICE LESSON #6 Resonance: Creating Good Vocal Vibes Voice Lesson #6 - Resonance Page 1 of 7 RESONANCE is the amplification and enrichment of tones produced by the voice. When we talk about resonance,
VOICE LESSON #6 Resonance: Creating Good Vocal Vibes Voice Lesson #6 - Resonance Page 1 of 7 RESONANCE is the amplification and enrichment of tones produced by the voice. When we talk about resonance,
Objectives. Module A2: Upper Airway Anatomy & Physiology. Function of the Lungs/Heart. The lung is for gas exchange. Failure of the Lungs/Heart
 Module A2: Upper Airway Anatomy & Physiology Objectives Classify epithelial tissue based on cell type and tissue layers. Identify location of tissue epithelium in the respiratory system. Describe the major
Module A2: Upper Airway Anatomy & Physiology Objectives Classify epithelial tissue based on cell type and tissue layers. Identify location of tissue epithelium in the respiratory system. Describe the major
What s New in Cleft Palate and Velopharyngeal Dysfunction Management?
 CME What s New in Cleft Palate and Velopharyngeal Dysfunction Management? Sanjay Naran, M.D. Matthew Ford, C.C.C.-S.L.P. Joseph E. Losee, M.D. Pittsburgh, Pa. Learning Objectives: After studying this article,
CME What s New in Cleft Palate and Velopharyngeal Dysfunction Management? Sanjay Naran, M.D. Matthew Ford, C.C.C.-S.L.P. Joseph E. Losee, M.D. Pittsburgh, Pa. Learning Objectives: After studying this article,
(1) TONSILS & ADENOIDS
 TONSILS & ADENOIDS") (1) TONSILS & ADENOIDS (2) Your child has been referred to have his tonsils and adenoids removed. This operation is commonly called an adenotonsillectomy and is one of the most common major operations
(1) TONSILS & ADENOIDS (2) Your child has been referred to have his tonsils and adenoids removed. This operation is commonly called an adenotonsillectomy and is one of the most common major operations
Pressure-Flow Characteristics of /m/ and /p/ Production in Speakers Without Cleft Palate: Developmental Findings
 Pressure-Flow Characteristics of /m/ and /p/ Production in Speakers Without Cleft Palate: Developmental Findings Objective: The purpose of this study was to describe the pressure-flow characteristics of
Pressure-Flow Characteristics of /m/ and /p/ Production in Speakers Without Cleft Palate: Developmental Findings Objective: The purpose of this study was to describe the pressure-flow characteristics of
Speech production: disordered EPG data
 Speech production: disordered EPG data F.E. Gibbon QMUC, Edinburgh VISPP Summer School - Palmse, Estonia August 10-15 2005 aims of lecture 2 recognise EPG patterns produced by those with speech disorders
Speech production: disordered EPG data F.E. Gibbon QMUC, Edinburgh VISPP Summer School - Palmse, Estonia August 10-15 2005 aims of lecture 2 recognise EPG patterns produced by those with speech disorders
By JAMES CALNAN, F.R.C.S. 1 Plastic Surgeon, University of Oxford
 BLOWING TESTS AND SPEECH By JAMES CALNAN, F.R.C.S. 1 Plastic Surgeon, University of Oxford and CATHERINE E. RENFREW, F.C.S.T. Chief Speech Therapist, United Oxford Hospitals " Is the mechanism competent?
BLOWING TESTS AND SPEECH By JAMES CALNAN, F.R.C.S. 1 Plastic Surgeon, University of Oxford and CATHERINE E. RENFREW, F.C.S.T. Chief Speech Therapist, United Oxford Hospitals " Is the mechanism competent?
Respiratory System. Functional Anatomy of the Respiratory System
 Respiratory System Overview of the Respiratory System s Job Major Duty Respiration Other important aspects ph control Vocalization Processing incoming air Protection Metabolism (ACE) What structures allow
Respiratory System Overview of the Respiratory System s Job Major Duty Respiration Other important aspects ph control Vocalization Processing incoming air Protection Metabolism (ACE) What structures allow
Speech and Swallowing in KD: Soup to Nuts. Neil C. Porter, M.D. Assistant Professor of Neurology University of Maryland
 Speech and Swallowing in KD: Soup to Nuts Neil C. Porter, M.D. Assistant Professor of Neurology University of Maryland Disclosures I will not be speaking on off-label use of medications I have no relevant
Speech and Swallowing in KD: Soup to Nuts Neil C. Porter, M.D. Assistant Professor of Neurology University of Maryland Disclosures I will not be speaking on off-label use of medications I have no relevant
The Clinical Swallow Evaluation: What it can and cannot tell us. Introduction
 The Clinical Swallow Evaluation: What it can and cannot tell us Debra M. Suiter, Ph.D., CCC-SLP, BCS-S Director, Voice & Swallow Clinic Associate Professor, Division of Communication Sciences & Disorders
The Clinical Swallow Evaluation: What it can and cannot tell us Debra M. Suiter, Ph.D., CCC-SLP, BCS-S Director, Voice & Swallow Clinic Associate Professor, Division of Communication Sciences & Disorders
PARENT CONCERNS A 3 YEAR OLD CHILD WITH TONGUE THRUSTING AND AN OPEN BITE. Robert M. Mason, DMD, PhD
 PARENT CONCERNS A 3 YEAR OLD CHILD WITH TONGUE THRUSTING AND AN OPEN BITE Robert M. Mason, DMD, PhD ABSTRACT: A parent s questions about a 3 year old with tongue thrusting and an anterior open bite are
PARENT CONCERNS A 3 YEAR OLD CHILD WITH TONGUE THRUSTING AND AN OPEN BITE Robert M. Mason, DMD, PhD ABSTRACT: A parent s questions about a 3 year old with tongue thrusting and an anterior open bite are
Speech Spectra and Spectrograms
 ACOUSTICS TOPICS ACOUSTICS SOFTWARE SPH301 SLP801 RESOURCE INDEX HELP PAGES Back to Main "Speech Spectra and Spectrograms" Page Speech Spectra and Spectrograms Robert Mannell 6. Some consonant spectra
ACOUSTICS TOPICS ACOUSTICS SOFTWARE SPH301 SLP801 RESOURCE INDEX HELP PAGES Back to Main "Speech Spectra and Spectrograms" Page Speech Spectra and Spectrograms Robert Mannell 6. Some consonant spectra
Velopharyngeal dysfunction (VPD) occurs
 occurs") Clinical Experience The Effect of Timing of Surgery for Velopharyngeal Dysfunction on Speech Devra B. Becker, MD,* Lynn M. Grames, SLP-CCC,* Thomas Pilgram, PhD,* Alex A. Kane, MD,* Jeffrey L. Marsh, MD
Clinical Experience The Effect of Timing of Surgery for Velopharyngeal Dysfunction on Speech Devra B. Becker, MD,* Lynn M. Grames, SLP-CCC,* Thomas Pilgram, PhD,* Alex A. Kane, MD,* Jeffrey L. Marsh, MD
Tyler Phillips Levee M.Cl.Sc (SLP) Candidate University of Western Ontario: School of Communication Sciences and Disorders
 Candidate University of Western Ontario: School of Communication Sciences and Disorders") Critical Review: Which Speech Symptoms Contribute Most to Reduced Intelligibility in Individuals with Ataxic Dysarthria Secondary to Friedreich s Disease? Tyler Phillips Levee M.Cl.Sc (SLP) Candidate University
Critical Review: Which Speech Symptoms Contribute Most to Reduced Intelligibility in Individuals with Ataxic Dysarthria Secondary to Friedreich s Disease? Tyler Phillips Levee M.Cl.Sc (SLP) Candidate University
Orofacial Myofunctional Therapy and it s Role in Dental Health and SDB. By: Jennie Herklotz, MA, CCC-SLP
 Orofacial Myofunctional Therapy and it s Role in Dental Health and SDB By: Jennie Herklotz, MA, CCC-SLP What is an Orofacial Myofunctional Disorder (OMD)? Includes at least one of the following: Open mouth
Orofacial Myofunctional Therapy and it s Role in Dental Health and SDB By: Jennie Herklotz, MA, CCC-SLP What is an Orofacial Myofunctional Disorder (OMD)? Includes at least one of the following: Open mouth
CASE STUDIES CONTENTS PART REINKE' S EDEMA, 3 VOCAL CORD DYSFUNCTION, 7. fiabit COUGH, 15 MUSCLE TENSION DYSPHONIA, 18 PUBERPHONIA, 33
 CONTENTS PART I CASE STUDIES REINKE' S EDEMA, 3 CASE STUDY 1-1: Postoperative Reinke's Edema, 4 VOCAL CORD DYSFUNCTION, 7 CASE STUDY 2-1: Vocal Cord Dysfunction, 8 CASE STUDY 2-2: Vocal Cord Dysfunction,
CONTENTS PART I CASE STUDIES REINKE' S EDEMA, 3 CASE STUDY 1-1: Postoperative Reinke's Edema, 4 VOCAL CORD DYSFUNCTION, 7 CASE STUDY 2-1: Vocal Cord Dysfunction, 8 CASE STUDY 2-2: Vocal Cord Dysfunction,
Morphological variations of soft palate and influence of age on it: A digital cephalometric study
 Original Research Article Morphological variations of soft palate and influence of age on it: A digital cephalometric study C. Vani 1*, T. Vinila Lakshmi 2, V. Dheeraj Roy 3 1 Professor, 2 Post graduate
Original Research Article Morphological variations of soft palate and influence of age on it: A digital cephalometric study C. Vani 1*, T. Vinila Lakshmi 2, V. Dheeraj Roy 3 1 Professor, 2 Post graduate
study. The subject was chosen as typical of a group of six soprano voices methods. METHOD
 254 J. Physiol. (I937) 9I, 254-258 6I2.784 THE MECHANISM OF PITCH CHANGE IN THE VOICE BY R. CURRY Phonetics Laboratory, King's College, Neweastle-on-Tyne (Received 9 August 1937) THE object of the work
254 J. Physiol. (I937) 9I, 254-258 6I2.784 THE MECHANISM OF PITCH CHANGE IN THE VOICE BY R. CURRY Phonetics Laboratory, King's College, Neweastle-on-Tyne (Received 9 August 1937) THE object of the work
Videofluorography and the assessment of velopharyngeal competence.
 University of Montana ScholarWorks at University of Montana Graduate Student Theses, Dissertations, & Professional Papers Graduate School 1977 Videofluorography and the assessment of velopharyngeal competence.
University of Montana ScholarWorks at University of Montana Graduate Student Theses, Dissertations, & Professional Papers Graduate School 1977 Videofluorography and the assessment of velopharyngeal competence.
Communication and Swallowing with PSP/CBD. Megan DePuy, MBA, MS, CCC-SLP Private Speech Pathologist
 Communication and Swallowing with PSP/CBD Megan DePuy, MBA, MS, CCC-SLP Private Speech Pathologist A Speech Therapist? Why? Swallowing (Dysphagia) Speech (Dysarthria, Dysphonia) Language (Aphasia) An Experienced
Communication and Swallowing with PSP/CBD Megan DePuy, MBA, MS, CCC-SLP Private Speech Pathologist A Speech Therapist? Why? Swallowing (Dysphagia) Speech (Dysarthria, Dysphonia) Language (Aphasia) An Experienced
Understanding your child s videofluoroscopic swallow study report
 Understanding your child s videofluoroscopic swallow study report This leaflet is given to you during your child s appointment in order to explain some of the words used by the speech and language therapist
Understanding your child s videofluoroscopic swallow study report This leaflet is given to you during your child s appointment in order to explain some of the words used by the speech and language therapist
Evaluation of the Toronto Palatal Lift Prosthesis for Patients with Hypernasal Resonance Disorders.
 Evaluation of the Toronto Palatal Lift Prosthesis for Patients with Hypernasal Resonance Disorders. by Brett William Ayliffe A thesis submitted in conformity with the requirements for the degree of Masters
Evaluation of the Toronto Palatal Lift Prosthesis for Patients with Hypernasal Resonance Disorders. by Brett William Ayliffe A thesis submitted in conformity with the requirements for the degree of Masters
SLHS 1301 The Physics and Biology of Spoken Language. Practice Exam 2. b) 2 32
 2 32") SLHS 1301 The Physics and Biology of Spoken Language Practice Exam 2 Chapter 9 1. In analog-to-digital conversion, quantization of the signal means that a) small differences in signal amplitude over time
SLHS 1301 The Physics and Biology of Spoken Language Practice Exam 2 Chapter 9 1. In analog-to-digital conversion, quantization of the signal means that a) small differences in signal amplitude over time
Department of Pediatric Otolarygnology. ENT Specialty Programs
 Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Speech Therapy. 4. Therapy is used to achieve significant, functional improvement through specific diagnosisrelated
 Speech Therapy I. Policy Speech therapy services include the diagnosis and treatment of communication impairment(s) and swallowing disorders. Services include speech/language therapy, swallowing/feeding
Speech Therapy I. Policy Speech therapy services include the diagnosis and treatment of communication impairment(s) and swallowing disorders. Services include speech/language therapy, swallowing/feeding
Tracheostomy and Ventilator Education Program Module 10: Communication Supplies
 Tracheostomy and Ventilator Education Program Module 10: Communication Supplies Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who
Tracheostomy and Ventilator Education Program Module 10: Communication Supplies Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who
The Throat. Image source:
 The Throat Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The Throat consists of three parts: 1. The Nasopharynx is the upper part of the throat and it is situated behind
The Throat Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The Throat consists of three parts: 1. The Nasopharynx is the upper part of the throat and it is situated behind
International Confederation for Cleft Lip and Palate and Related Craniofacial Anomalies Task Force Report: Speech Assessment
 The Cleft Palate Craniofacial Journal 51(6) pp. e138 e145 November 2014 Ó Copyright 2014 American Cleft Palate Craniofacial Association BRIEF COMMUNICATION International Confederation for Cleft Lip and
The Cleft Palate Craniofacial Journal 51(6) pp. e138 e145 November 2014 Ó Copyright 2014 American Cleft Palate Craniofacial Association BRIEF COMMUNICATION International Confederation for Cleft Lip and
Voice Evaluation. Area of Concern:
 Name : Lilly Tulip File Number : 1002 Age : xx years D.O.B. : 9-9-1999 Address : 9999 9 th St NW D.O.E. : 11-30-2012 Minot, ND 59992 Referral : Dr. Andrew Hetland Phone : (701) 899-9999 Code : 784.40 Area
Name : Lilly Tulip File Number : 1002 Age : xx years D.O.B. : 9-9-1999 Address : 9999 9 th St NW D.O.E. : 11-30-2012 Minot, ND 59992 Referral : Dr. Andrew Hetland Phone : (701) 899-9999 Code : 784.40 Area
The Respiratory System
 13 PART A The Respiratory System PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Organs of the Respiratory
13 PART A The Respiratory System PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Organs of the Respiratory
Downloaded on T04:25:43Z. Title. Abnormal patterns of tongue-palate contact in the speech of individuals with cleft palate
 Title Abnormal patterns of tongue-palate contact in the speech of individuals with cleft palate Author(s) Gibbon, Fiona E. Publication date 2004-08 Original citation Type of publication Link to publisher's
Title Abnormal patterns of tongue-palate contact in the speech of individuals with cleft palate Author(s) Gibbon, Fiona E. Publication date 2004-08 Original citation Type of publication Link to publisher's
Audiology Curriculum Foundation Course Linkages
 Audiology Curriculum Foundation Course Linkages Phonetics (HUCD 5020) a. Vowels b. Consonants c. Suprasegmentals d. Clinical transcription e. Dialectal variation HUCD 5140 HUCD 6360 HUCD 6560 HUCD 6640
Audiology Curriculum Foundation Course Linkages Phonetics (HUCD 5020) a. Vowels b. Consonants c. Suprasegmentals d. Clinical transcription e. Dialectal variation HUCD 5140 HUCD 6360 HUCD 6560 HUCD 6640
Snoring and Obstructive Sleep Apnea: Patient s Guide to Minimally Invasive Treatments Chapter 2
 Snoring and Obstructive Sleep Apnea: Patient s Guide to Minimally Invasive Treatments Chapter 2 CAUSES OF SNORING AND SLEEP APNEA We inhale air through our nose and mouth. From the nostrils, air flows
Snoring and Obstructive Sleep Apnea: Patient s Guide to Minimally Invasive Treatments Chapter 2 CAUSES OF SNORING AND SLEEP APNEA We inhale air through our nose and mouth. From the nostrils, air flows
Made available courtesy of the Acoustical Society of America:
 Controlling changes in vocal tract resistance By: Donald W. Warren, Anne Putnam Rochet, Rodger M. Dalston, and Robert Mayo Warren, D.W., Roceht, A.P., Dalston, R.M., and Mayo, R. (1992). Controlling changes
Controlling changes in vocal tract resistance By: Donald W. Warren, Anne Putnam Rochet, Rodger M. Dalston, and Robert Mayo Warren, D.W., Roceht, A.P., Dalston, R.M., and Mayo, R. (1992). Controlling changes
NURSE-UP RESPIRATORY SYSTEM
 NURSE-UP RESPIRATORY SYSTEM FUNCTIONS OF THE RESPIRATORY SYSTEM Pulmonary Ventilation - Breathing Gas exchanger External Respiration between lungs and bloodstream Internal Respiration between bloodstream
NURSE-UP RESPIRATORY SYSTEM FUNCTIONS OF THE RESPIRATORY SYSTEM Pulmonary Ventilation - Breathing Gas exchanger External Respiration between lungs and bloodstream Internal Respiration between bloodstream
11 Music and Speech Perception
 11 Music and Speech Perception Properties of sound Sound has three basic dimensions: Frequency (pitch) Intensity (loudness) Time (length) Properties of sound The frequency of a sound wave, measured in
11 Music and Speech Perception Properties of sound Sound has three basic dimensions: Frequency (pitch) Intensity (loudness) Time (length) Properties of sound The frequency of a sound wave, measured in
Research Article Measurement of Voice Onset Time in Maxillectomy Patients
 e Scientific World Journal, Article ID 925707, 4 pages http://dx.doi.org/10.1155/2014/925707 Research Article Measurement of Voice Onset Time in Maxillectomy Patients Mariko Hattori, 1 Yuka I. Sumita,
e Scientific World Journal, Article ID 925707, 4 pages http://dx.doi.org/10.1155/2014/925707 Research Article Measurement of Voice Onset Time in Maxillectomy Patients Mariko Hattori, 1 Yuka I. Sumita,
Dr.ALI AL BAZZAZ PLASTIC SURGON CLEFT LIP AND PALATE
 Dr.ALI AL BAZZAZ PLASTIC SURGON CLEFT LIP AND PALATE Cleft lip (cheiloschisis) and cleft palate (palatoschisis), which can also occur together as cleft lip and palate, are variations of a type of clefting
Dr.ALI AL BAZZAZ PLASTIC SURGON CLEFT LIP AND PALATE Cleft lip (cheiloschisis) and cleft palate (palatoschisis), which can also occur together as cleft lip and palate, are variations of a type of clefting