Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
|
|
|
- Erica McCarthy
- 6 years ago
- Views:
Transcription
1 Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
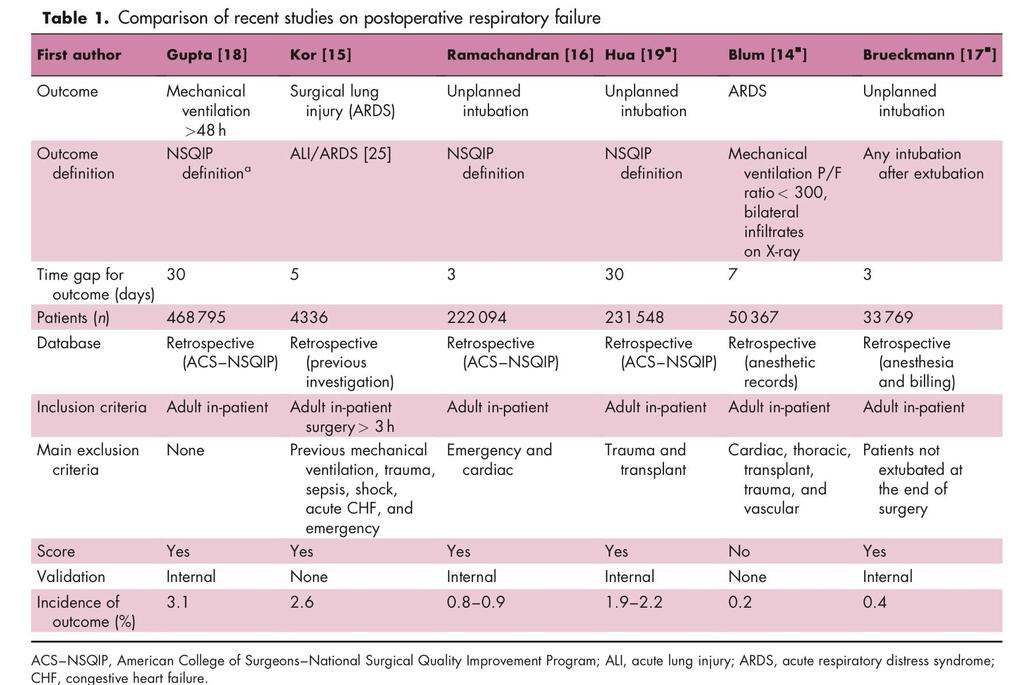
2 Is it really or/only a postoperative issue Multi hit theory first hits second hits
3 Definition Pulmonary gas exchange impairment that presents after a surgical procedure and as a result of the changes induced by anesthesia and surgery with ABG,s measurement providing the grounds for diagnosis: PaO2< 60 mmhg (Fio ) Pco2 > 50 mm of hg P/F < 300 mm of hg
4 ACS-NSQIP definition of PRF Unplanned intubation during surgery or postoperatively Reintubation once extubated Mechanical ventilation for > 48 h postoperatively.
5
6 Severity According to the recent international consensus on ARDS, PRF may be classified as Mild (PaO2/FIO2 300mmHg and>200mmhg) Moderate (PaO2/ FIO2 200 mmhg and > 100 mmhg) Severe (PaO2/FIO2 100 mmhg)
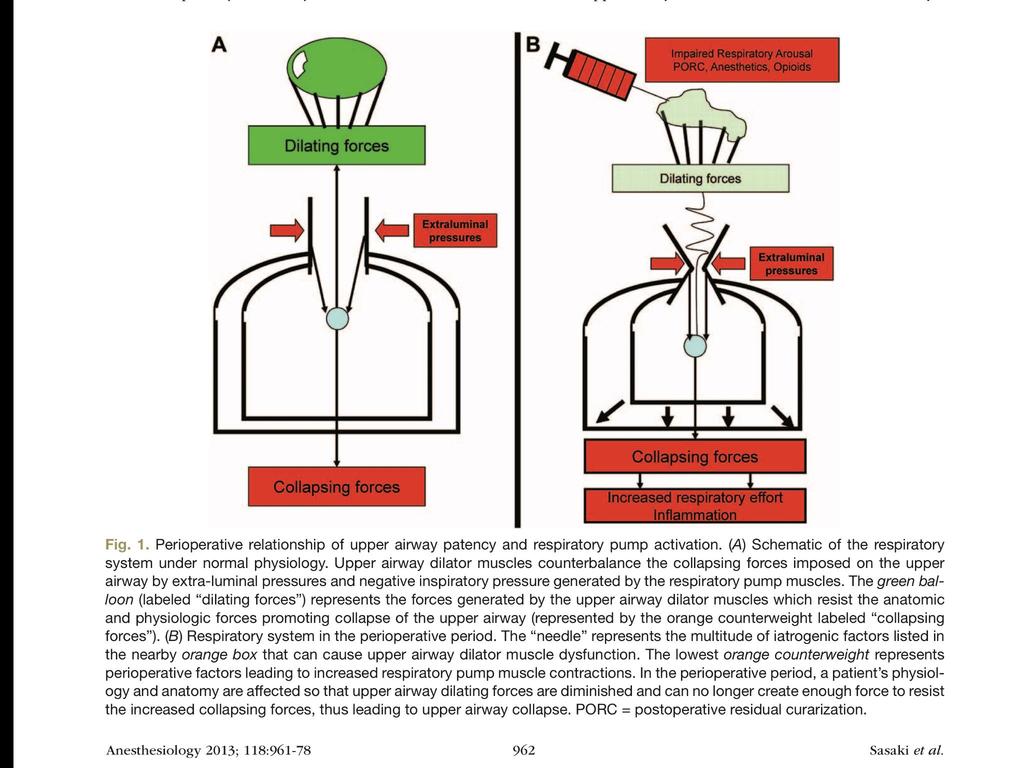
7 Pathogenesis Primarily reduction of respiratory muscle tone leading to abnormal gas exchange and ventilation-perfusion mismatch and shunt aggravated by factors such as hypoventilation due to the residual effects of anesthetics, lung edema, laryngospasm, and bronchospasm and increased Fio2 > 80% during surgery and manipulation of structures above or below the diaphragm during surgery
8
9
10
11 PRF PREDICTORS FIRST HITS Threats associated with the patient s condition and the foreseen procedure (preoperative information). SECOND HITS Intraoperative events, which would modulate first-hit risk and indicate the patient s definitive risk.
12 Preoperative Age Male ASA of at least 3 FUNCTIONAL DEPENDENCY Sepsis/sep tic shock CHF COPD Prolonged hospitalization DM GERD Alcohol abuse Current smoker Liver disease Weight loss cancer Dyspnea HTN Renal failure Surgery Cardiac Vascular Thoracic Upper abdominal Emergenc y Neck Urology Neurosurgery General Burn Transplant High risk surgery INTRAOPERATIVE Pulmonary driving pressure Inspired oxygen fraction Volume of crystalloid administration Erythrocyte transfusion Duration of surgery No. of anesthetics during admission
13 PREVENTION OF POSTOPERATIVE RESPIRATORY FAILURE
14 VENTILATORY( LUNG PROTECTIVE VENTILATION) Accurate FIO2( upto 80% does not promote atelectasis) Avoid volume trauma by 1) limit plateau pressure to 20 cm of h20 2) limit tidal volume to 6ml/kg in all non-risk and high risk patients Avoid Atelectrauma 1)Peep 2)Recruitment maneuvers after intubation,disconnection, durring hypoxia and before extubation Severgnini P, Selmo G, Lanza C, et al. Protective mechanical ventilation during general anesthesia for open abdominal surgery improves postoperative pulmonary function. Anesthesiology 2013; 118: A comprehensive ventilation strategy (low tidal volumes, PEEP, and recruitment maneuvers) can improve postoperative pulmonary function. Futier E, Constantin JM, Paugam-Burtz C, et al. A trial of intraoperative low-tidalvolume ventilation in abdominal surgery. N Engl J Med 2013; 369:
15 NON VENTILATORY Anesthetic technique (i) Choose neuroaxial or regional techniques (ii) Inhaled anesthetics to decrease pulmonary inflammatory response to mechanical ventilation (iii) Accurate administration and monitoring of neuromuscular block Emergence (i) Complete reversal of the neuromuscular Blockade (ii) No atelectasis (iii) Adequate postoperative analgesia (iv) Avoid overuse of opiates and excessive sedation Restrictive use of fluids Avoid transfusion (i) Alleviate preoperative anemia (ii) Apply blood saving strategies Decrease risk of pulmonary infection (i) Antibiotic prophylaxis (ii) Tooth brushing and oral decontamination (iii) Orotracheal tube management Check cuff pressure Appropriate cuff shape Appropriate material (iv) Avoid nasogastric tubes Surgical technique (i) Choose a thoracoscopic or laparoscopic Approach (ii) Reduce surgical duration (iii) Defer surgery whenever possible
16 POSTOPERATIVE NOINVASIVE VENTILATION Use in selected patient groups may reduce the incidence of postoperative hypoxia, respiratory failure, rates of reintubation, incidence of pneumonia, ICU and hospital length of stay, and potentially mortality. NIV must be delivered via a tight-fitting mask or helmet. Problems with interface fit, leakage, and patient discomfort are frequently encountered The question of treating with NIV can become a balance of the costs incurred through equipment, disposables, staffing, and critical care bed provision against the potential savings made by preventing complications and reducing length of stay.
17 HIGH-FLOW NASAL OXYGEN Delivery of air oxygen mixtures at inspiratory flow rates of up to 60 L/min, which reduces the amount of ambient air entrainment and allows a more reliable and predictable FiO2 delivery to patients Pharyngeal dead-space washout, alveolar recruitment, and reduced airflow resistance and variable degree of PEEP, 3 7 cm H20 which all promote enhanced respiratory parameters and gas exchange Improved oxygenation and 90-day survival in patients with acute hypoxic RF when compared to NIV Reduced extubation failure and reintubation rates in postoperative patients and icu as well
18 Physiotherapy Techniques Multimodal specialty including early assisted mobilization, exercise, thoracic expansion exercises, incentive spirometry, and airway clearance techniques. PEP therapy patients generate an expiratory pressure of up to 20 cm H20 by breathing against a mouthpiece valve device, may also be used postoperatively to increase functional residual capacity and mobilize secretions NO strong evidence to suggest that PEP is beneficial when applied routinely. However, physiologically in postoperative patients with increased sputum production, or to ameliorate sputum retention, especially in patients with dynamic airway collapse or atelectasis.
19 A 75y/M, know case of uncontrolled DM, severe COPD with FEV 1 <30% and corpulmonale has small swelling of Rt lower arm(probably lipoma) which is asymptomatic with no pain or any neurovascular involvement. You did preoperative assessment, following which you went to surgeon to discuss the plan of surgery and anesthesia. What will be most appropriate plan for this pt? 1. GA with lung protective ventilation 2. Iv sedation with local application 3. Supraclavicular block 4. Defer the surgery 5. GA with high tidal volumes
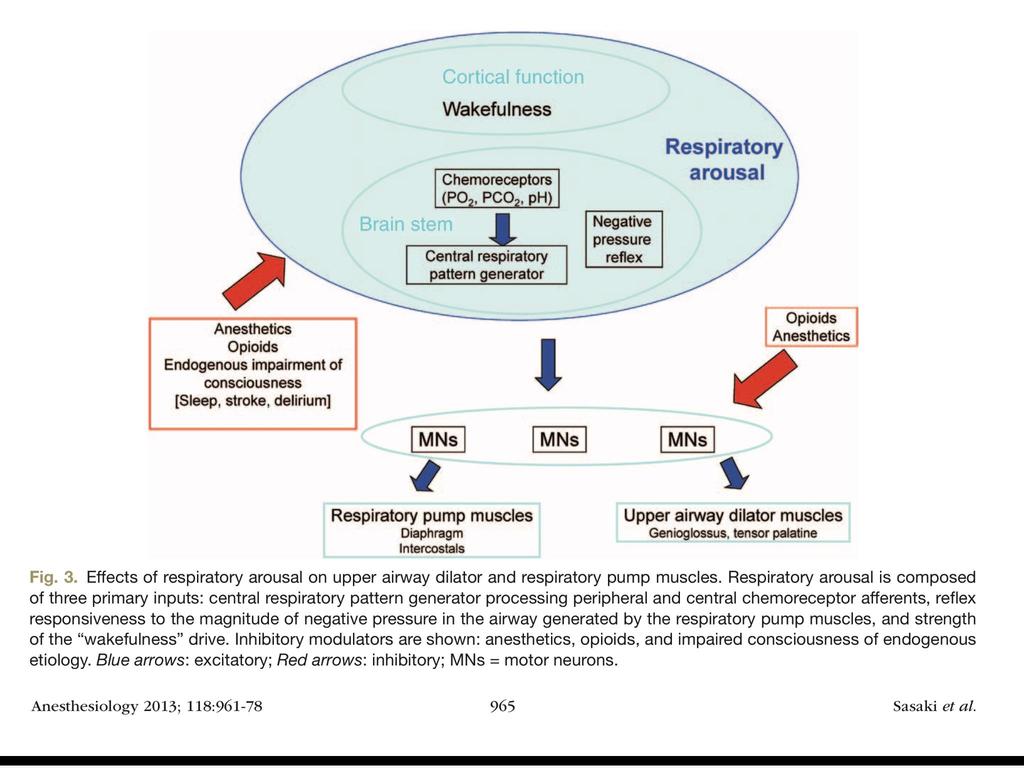
20 Uncoupling of the link between unconsciousness and upper airway dilator muscle hypotonia is by 1. Etomidate 2. Propofol 3. Thiopental 4. Midazolam 5. None of the above
21 Respiratory arousal is not characterized by 1. Increased chemo responsiveness to hypoxia 2. Increased chemo responsiveness to hypercarbia 3. Suppression of reflex responsiveness to negative upper airway pressure 4. Increase in the magnitude of wakefulness
22 Regarding role of muscles in PRF 1. In awake pt upper airways muscles have constrictor(narrowing) effect 2. Expiratory pump muscles have no role in development of PRF 3. Tensor palatine is involved in Negative pressure reflex. 4. Genioglossus has no phasic neuronal input during respiratory cycle 5. Tone of respiratory pump muscles increases FRC BY 0.8L
23
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Charisma High-flow CPAP solution
 Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Protecting the Lungs
 Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Perioperative Pulmonary Management. Objectives
 Citywide Resident Perioperative Medical Consult Conference Perioperative Pulmonary Management Frank Jacono, MD May 5, 2017 Objectives Definition of post-operative pulmonary complications (PPC) Risk factors
Citywide Resident Perioperative Medical Consult Conference Perioperative Pulmonary Management Frank Jacono, MD May 5, 2017 Objectives Definition of post-operative pulmonary complications (PPC) Risk factors
Fariba Rezaeetalab Associate Professor,Pulmonologist
 Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
Trial protocol - NIVAS Study
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
What s New About Proning?
 1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
Lung Injury and Protection in the Perioperative Period
 J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1).
.") PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
Assessing perioperative risk
 Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery. By: Lillian Han
 Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
NI 60. Non-invasive ventilation without compromise. Homecare Pneumology Neonatology Anaesthesia. Sleep Diagnostics Service Patient Support
 NI 60 Non-invasive ventilation without compromise Homecare Pneumology Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support NI 60 Non-invasive ventilation without
NI 60 Non-invasive ventilation without compromise Homecare Pneumology Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support NI 60 Non-invasive ventilation without
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Non-invasive Ventilation
 Non-invasive Ventilation 163 29 Non-invasive Ventilation AM BHAGWATI Artificial ventilatory support has became an integral component in the management of critically ill patients in the intensive care units.
Non-invasive Ventilation 163 29 Non-invasive Ventilation AM BHAGWATI Artificial ventilatory support has became an integral component in the management of critically ill patients in the intensive care units.
Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning
 CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Supplementary Online Content 2
 Supplementary Online Content 2 van Meenen DMP, van der Hoeven SM, Binnekade JM, et al. Effect of on demand vs routine nebulization of acetylcysteine with salbutamol on ventilator-free days in intensive
Supplementary Online Content 2 van Meenen DMP, van der Hoeven SM, Binnekade JM, et al. Effect of on demand vs routine nebulization of acetylcysteine with salbutamol on ventilator-free days in intensive
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
High Flow Oxygen Therapy in Acute Respiratory Failure. Laurent Brochard Toronto
 High Flow Oxygen Therapy in Acute Respiratory Failure Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical research projects from the
High Flow Oxygen Therapy in Acute Respiratory Failure Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical research projects from the
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
11/20/2015. Beyond CPAP. No relevant financial conflicts of interest. Kristie R Ross, M.D. November 12, Describe advanced ventilation options
 Beyond CPAP Kristie R Ross, M.D. November 12, 2015 No relevant financial conflicts of interest Sponsored by The Warren Alpert Medical School of Brown University Describe advanced ventilation options Compare
Beyond CPAP Kristie R Ross, M.D. November 12, 2015 No relevant financial conflicts of interest Sponsored by The Warren Alpert Medical School of Brown University Describe advanced ventilation options Compare
LAS VEGAS Case Report Form 1 Intra-Operative
 LAS VEGAS Case Report Form 1 Intra-Operative Patient Informed Consent 1. Informed consent applicable: yes no (choose no if waived by local EC) 1.1 If applicable; was consent obtained? yes no 1.2 If yes,
LAS VEGAS Case Report Form 1 Intra-Operative Patient Informed Consent 1. Informed consent applicable: yes no (choose no if waived by local EC) 1.1 If applicable; was consent obtained? yes no 1.2 If yes,
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Concerns and Controversial Issues in NPPV. Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation
 : Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
: Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
Preoperative Pulmonary Evaluation. Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine
 Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
C l i n i c a lcpap. Advanced Solutions in Acute Respiratory Care
 C l i n i c a lcpap Advanced Solutions in Acute Respiratory Care This is tex which explains in moderate clinicsal detail, the background and structure of the patient indication for CPAP. This is tex which
C l i n i c a lcpap Advanced Solutions in Acute Respiratory Care This is tex which explains in moderate clinicsal detail, the background and structure of the patient indication for CPAP. This is tex which
Effects of PPV on the Pulmonary System. Chapter 17
 Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
High Flow Humidification Therapy, Updates.
 High Flow Humidification Therapy, Updates. Bernardo Selim, M.D. I have no relevant financial relationships to disclose. Assistant Professor, Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic What
High Flow Humidification Therapy, Updates. Bernardo Selim, M.D. I have no relevant financial relationships to disclose. Assistant Professor, Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic What
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Disclosures. Objectives. Defining Adult Obesity. Body Mass Index vs. Central Obesity 9/6/2017
 Disclosures Why is the Morbidly Obese Patient at Increased Risk for Perioperative Morbidity? Lisa R. Farmer, MD Associate Professor No conflicts of interests concerning the content of this presentation
Disclosures Why is the Morbidly Obese Patient at Increased Risk for Perioperative Morbidity? Lisa R. Farmer, MD Associate Professor No conflicts of interests concerning the content of this presentation
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Supplementary Online Content
 1 Supplementary Online Content Leme AC, Hajjar LA, Volpe MS, et al. Effect of intensive vs moderate alveolar recruitment strategies added to lung-protective ventilation on postoperative pulmonary complications:
1 Supplementary Online Content Leme AC, Hajjar LA, Volpe MS, et al. Effect of intensive vs moderate alveolar recruitment strategies added to lung-protective ventilation on postoperative pulmonary complications:
Postoperative pulmonary complications
 British Journal of Anaesthesia, 118 (3): 317 34 (2017) doi: 10.1093/bja/aex002 Review Article Postoperative pulmonary complications A. Miskovic and A. B. Lumb* Department of Anaesthesia, St James s University
British Journal of Anaesthesia, 118 (3): 317 34 (2017) doi: 10.1093/bja/aex002 Review Article Postoperative pulmonary complications A. Miskovic and A. B. Lumb* Department of Anaesthesia, St James s University
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion
 How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Non-Invasive Ventilation
 Khusrav Bajan Head Emergency Medicine, Consultant Intensivist & Physician, P.D. Hinduja National Hospital & M.R.C. 112 And the Lord God formed man of the dust of the ground and breathed into his nostrils
Khusrav Bajan Head Emergency Medicine, Consultant Intensivist & Physician, P.D. Hinduja National Hospital & M.R.C. 112 And the Lord God formed man of the dust of the ground and breathed into his nostrils
Problem Based Learning. Problem. Based Learning
 Problem 2013 Based Learning Problem Based Learning Your teacher presents you with a problem in anesthesia, our learning becomes active in the sense that you discover and work with content that you determine
Problem 2013 Based Learning Problem Based Learning Your teacher presents you with a problem in anesthesia, our learning becomes active in the sense that you discover and work with content that you determine
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Mechanical Ventilation of the Patient with Neuromuscular Disease
 Mechanical Ventilation of the Patient with Neuromuscular Disease Dean Hess PhD RRT Associate Professor of Anesthesia, Harvard Medical School Assistant Director of Respiratory Care, Massachusetts General
Mechanical Ventilation of the Patient with Neuromuscular Disease Dean Hess PhD RRT Associate Professor of Anesthesia, Harvard Medical School Assistant Director of Respiratory Care, Massachusetts General
1.40 Prevention of Nosocomial Pneumonia
 1.40 Prevention of Nosocomial Pneumonia Purpose Audience Policy Statement: The guideline is designed to reduce the incidence of pneumonia and other acute lower respiratory tract infections. All UTMB healthcare
1.40 Prevention of Nosocomial Pneumonia Purpose Audience Policy Statement: The guideline is designed to reduce the incidence of pneumonia and other acute lower respiratory tract infections. All UTMB healthcare
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE
 VAPOTHERM POCKET GUIDE") Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
7 Initial Ventilator Settings, ~05
 Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Lab 4: Respiratory Physiology and Pathophysiology
 Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Basics of NIV. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Mechanical ventilation in the emergency department
 Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial
. A randomized controlled trial") CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial Backgrounds Postoperative pulmonary complications are most frequent after cardiac surgery and lead to increased
CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial Backgrounds Postoperative pulmonary complications are most frequent after cardiac surgery and lead to increased
Does the Use of Positive End Expiratory Pressure (PEEP) During Surgery Decrease Respiratory Complications Twenty-Four Hours Post Operative?
 During Surgery Decrease Respiratory Complications Twenty-Four Hours Post Operative?") Rhode Island College Digital Commons @ RIC Master's Theses, Dissertations, Graduate Research and Major Papers Overview Master's Theses, Dissertations, Graduate Research and Major Papers 2016 Does the Use
Rhode Island College Digital Commons @ RIC Master's Theses, Dissertations, Graduate Research and Major Papers Overview Master's Theses, Dissertations, Graduate Research and Major Papers 2016 Does the Use
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
November 2012 Critical Care Case of the Month: I Just Can t Do It Captain! I Can t Get the Sats Up!
 November 2012 Critical Care Case of the Month: I Just Can t Do It Captain! I Can t Get the Sats Up! Bridgett Ronan, MD Department of Pulmonary Medicine Mayo Clinic Arizona Scottsdale, AZ History of Present
November 2012 Critical Care Case of the Month: I Just Can t Do It Captain! I Can t Get the Sats Up! Bridgett Ronan, MD Department of Pulmonary Medicine Mayo Clinic Arizona Scottsdale, AZ History of Present
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
PULMONARY FUNCTION TESTING. Purposes of Pulmonary Tests. General Categories of Lung Diseases. Types of PF Tests
 PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?